Embed Size (px)
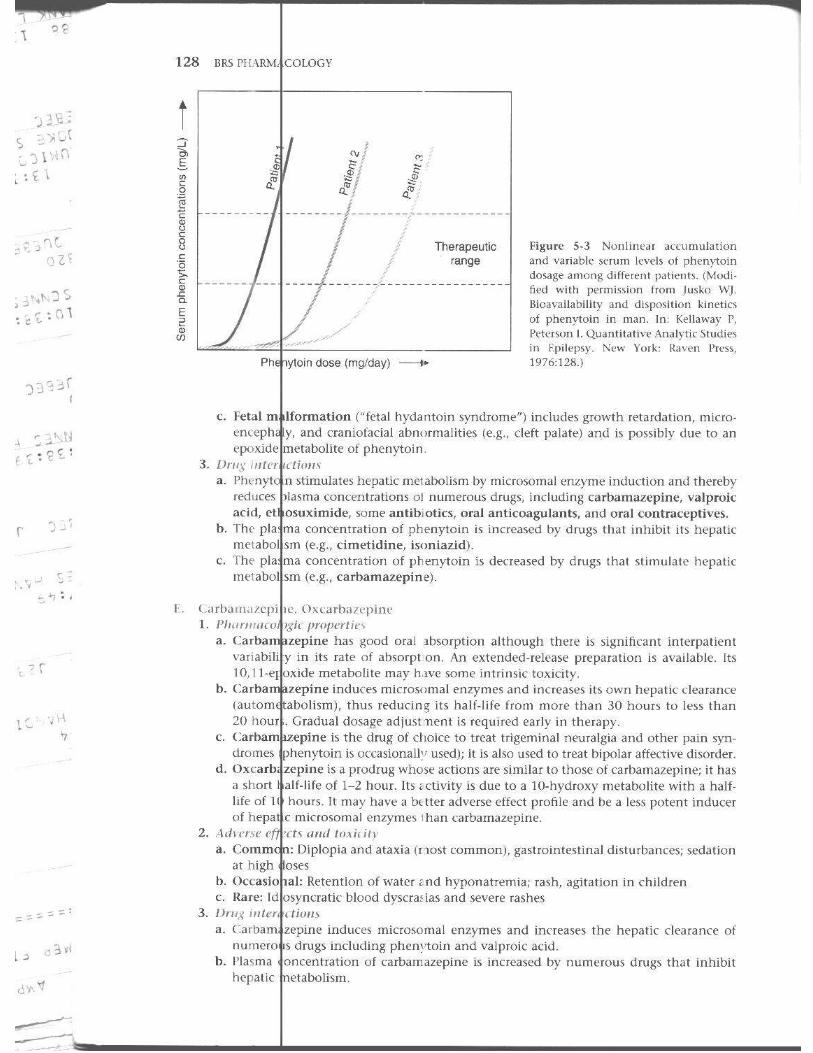
DESCRIPTION
USMLE pharm
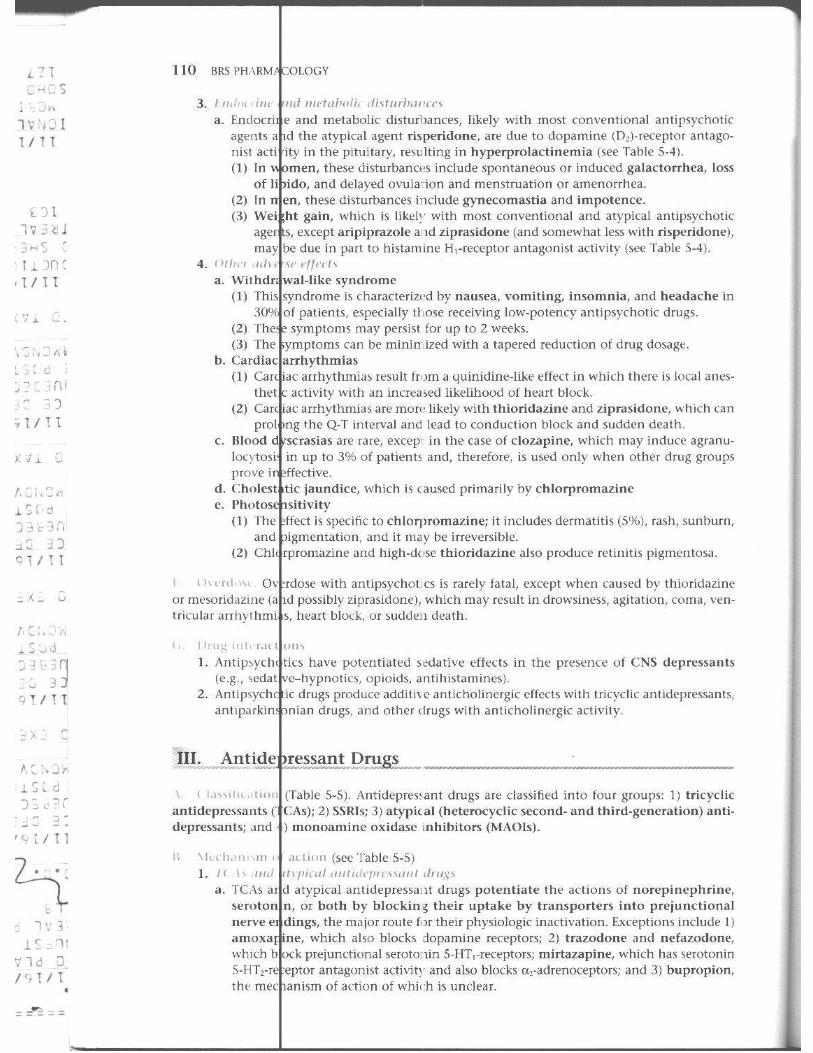
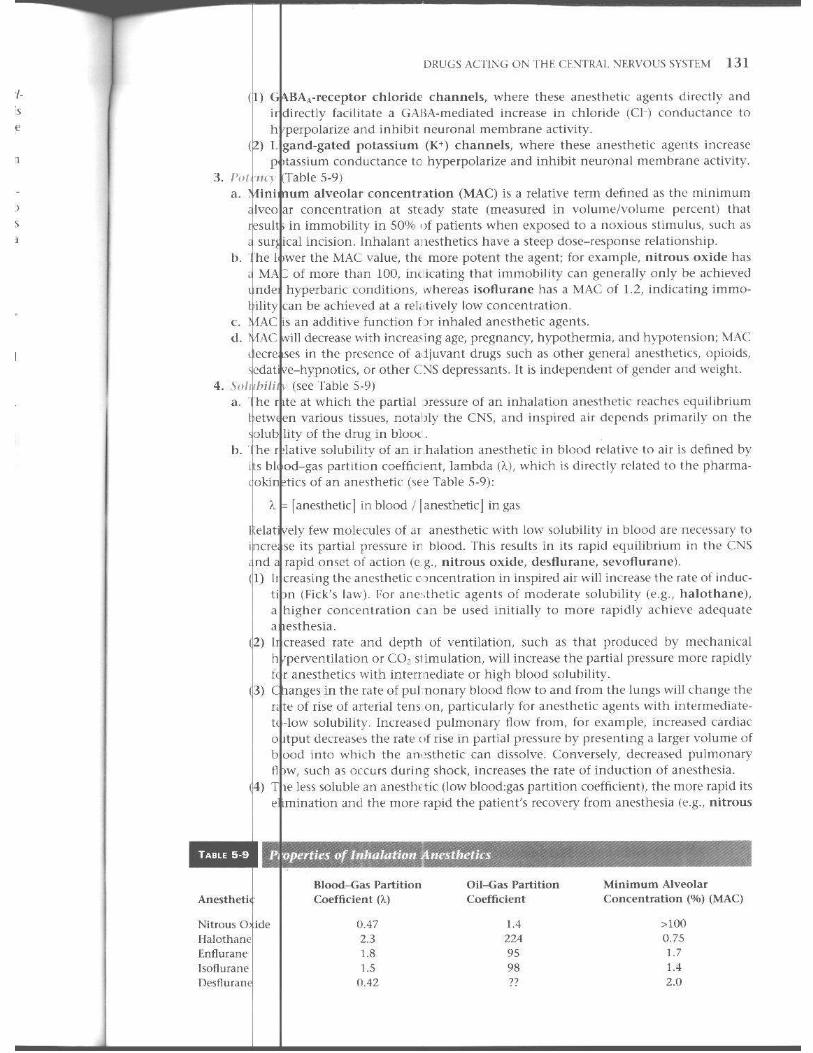
Citation preview
Log on 10'
resources Use the code ntnvlrtl~rt to access the r*sour for BRS 4th edition.
~1 , Point,~ Where Teaching, learning, & Technology Click ./ I
LWW's Online Resources for bOl students and faculty, all housed I one robust, easy-to-access websit
http://thePoint.lww.co
Point , provides flexible leami
solutions and resources to snldems
using BRS Phamuu;ology, 4th editi
• All Q&A from the book is also provided online.
• All images and tables from the book are also
provided online.
Scratch off the sticker with care! Note: Book CMHIM , ......... 1M ,. .. 1 ia ICratch.d 01
4TH
GaIT C. ProfesSor Department .md
COLOGY
1'11.0.
Integra tin> Biology ~ nd Pharmacology
Graduate s .• : h+o. of Biomedical Scie,c{'s i\ssl stanl for Education Programs
Medical School at Houston
Dm'id Loose, 1'11.0. Associate ""'1"'"' Departmen t . Integrated [liology and Pharmacology ilnd Graduat(' Seh,,101 of Biomedical SciellCl's Univer~ity of Medical School . .It Iioustoll I [ OU~I Otl,
With sp,celat contributions by
Medilla IIshell, ,\I.D.
Will iam B~'~:I;~:,~~~HOSPital Royal Oak,
Todd \. William B~'~ ~t~;,~~~H OSPital Royal Oak,
.\J.D., 1'11.1).
~. •
Williams & Wilkins Kluwer busines s
~.-
Acquisitions Editor: Ix,run,M. Balado Managing Editor: L. Sebring Marketins, Linkin'> Production Montalb,!no
Designer: DOUg .~~t:;,~::~:; Compo.litor; Circle Inc. Printer: Courin
Copyright © 20071 I,'pin""tt \-Villiams & V\ ilkins
351 \-Vest Camden Raltimo[t', MLJ 21
530 Walnut St reet Philadt'lphi.1, PA 1
All rights [t'served. hook is protected b:; copyright. No part of this book may be reproduced in any form or by,j" means, including pho :ocopying, or utilized by any information storage and retrieval system written pt'rmission from the copyright owner.
The publisher is responsihle (as a matter of product liability, negligence, or otht'rwise l for any injury resulting any materia l containt'ti hert'in. This puhlication contains information relat-
ing to gl;'ne'i·,;',\1 ~;0.'tf!I::~,O~I': 'in~"~d;:I;~,;a~1 cart' that should not he construed as ,pt'cific instruct ions for individual product information and package inserts should be rt'vit'wt'd for current including contrain.tic"ations. dosages, and precautions.
I'riflted in 1111' U"If<'1St",,, of America
Third Edition,
Library of C'"'~''' Cataloging-In-Puhlication Data
Rosenfeld, Ga ry C. Pharmacology /
Kushell, Todd A. p. ;
Includes index. ISfiN-13:
Loose, David .
C. Rosenfeld, Dav d S. Loose; with special contributions by Medina I. ted.
(alk. paper) I. Pharmacology-Examinations, questions, etc. l. . TIl. St'ries.
IDNL\1: I. I'll f",>¥,w,ogy-Ex,mln,,!icmQucstions. QV 18.2 RSI3p 20061
RM3'UO~;,:~~:j~' 615'.1
2006009983
The publi.l!rers evcry c(tbrt to lrace 1111' cupyrisht holdl'f5 for borrowed I1wterial. If" tlley Ira...,! inadvertentl,. "t,"d,,,I',," any, till}' will he p/"Clsed to mak.e tile IIc(cs.mry arrangemcnls al lire first opportlill ity.
To purchase '~dil;'ln'll (·opies of this book, call our customer service department at (SOO) 6:{S-3030 or fax (301) 223-2320. Intemational customers should ca!i (301) 223-2300.
Vhit L:'r:.,';::::l.::,f:::::":;& Wilkins on tile Tnterm:t: http://www.LWiV.com.LippincottWilliams & Wilkim representatives a ·e available from 8:30 am to 6:00 pm, EST.
07 08 09 \0
345678910

This conci se and others for !
tiuns of the mual lati on of
e to the Fourth Edition
of medical pharmacology is designed for medical students, dental students. health care professions. It is intended primarily to help students prepare
such as the Un ited States Medical Licensing Examination Step 1 examinations. This book presents condensed and succinct descrip
and current Boord·dJiven information pertaining to pharmacology without -j details. 11 is not rneant to be a sub~titute for the comprehensive presen·
and difficu lt (oncepts found in standard pharmacology l{?xtS.
The fourth - ion begins with a chap:er devoted to the general principles of dru~ action, followed b')Yu~:~:l~:~ concerned with dLlgs acting on the major body systems. Other chapters discuss a " e rgots, antiinflamnatory and Immunosuppressive agents, drugs used to treat anem ias disorders of hemos asis, infeCl ious d iseases, ca nccr. and tOXicology.
Each indudes a presentali)n of specific drugs with a d iscussion of their general propert ies, n ism of action, pharmacologic effects, thcrapeutic uses, and ad,'crsc effects. A drug lisl, and figures surnmaTizc essential drug information included in all chapters,
Clinical ly USMLE·style rfview questions and answers with cxplanations follow each chapter help students assess their understa nd ing of the info rmation, Similarly, a com· prehen:.i,"e comisting of USMLE-stylc questions is included at the end of the book. serve. as a self-a.\scssment tool to help ~tudents determine their fund of knowledge diagnose any weakr esses in pharmacology.
• current drug infurmat ic'il • review tests feat ure updatr.-d USMI.F..~tyle questions • 2·colo! ""'"" summarize (sscntial lnformation for qukk recall • Drug !iSH
• Addiltonal comprehellSi\-e examination questions and explanatIons
Gary C. Rosl'lI{,eld, PII.o.
Dm'ill S. i (K)\C, Pl!.lJ.
v

Acknowledgments
The aullmrs a 'knowledge and thank our coll('agllt!~ for their .'IUppor! allll contributions to this boo!.. and our medical students fo)r bein g OUf hars hest critic~ .
vii
Contents
Preface v Acknowledgn cn ts vii
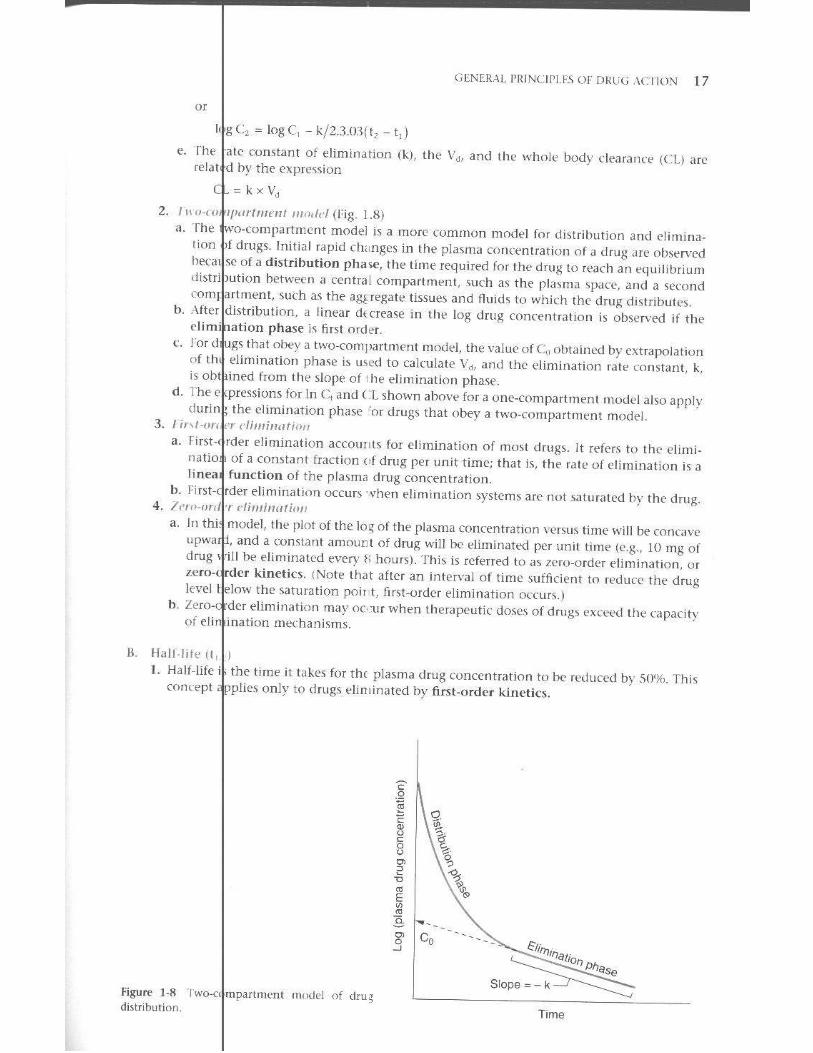
1 Gener I Principles of [)rug Action ......... . . .. . .. . . . . .. 1 I. D( se-Response Relation ;hips 1 II . 0 g Absorption 6 III . Dr g Dist ribu tion 9 IV. Dr g Elimin ation and Tt'rmin at ion of Action 10 V. Bl )tramforma l ion (Met,bolism) of Drugs 11 VI. E --ret lon of Drug.. \.; VII . P rmacokinct in. 16 Re , ·iew cs t 19
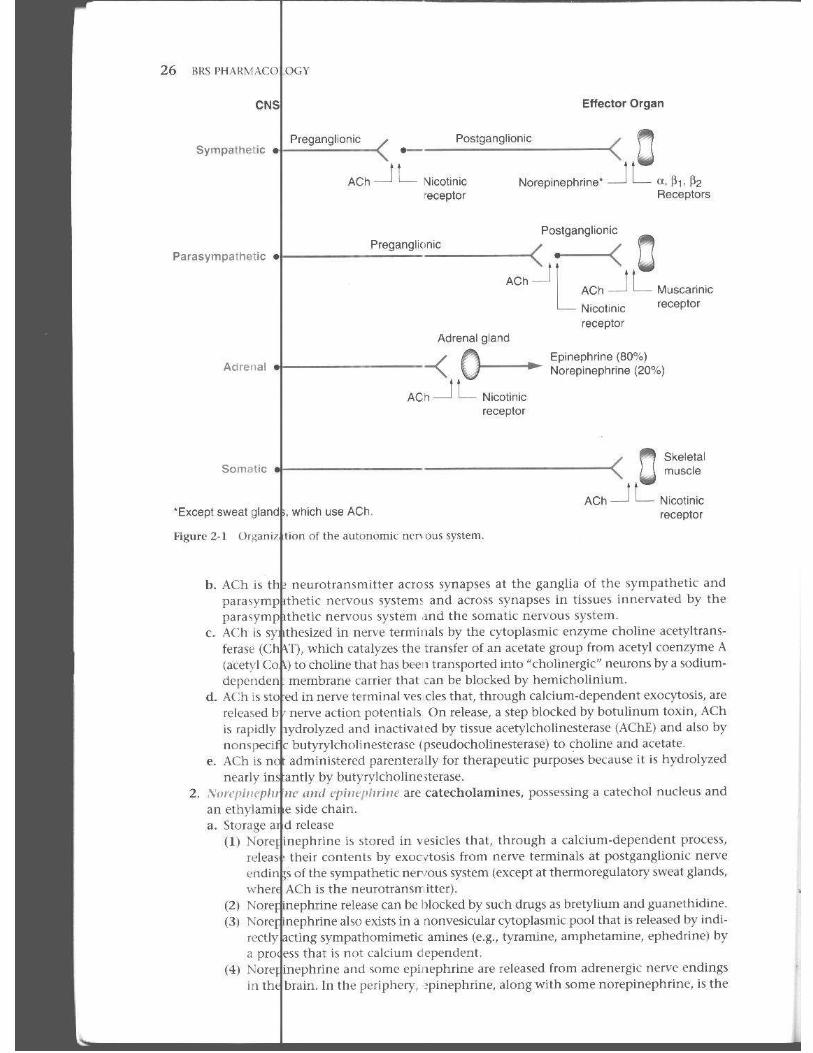
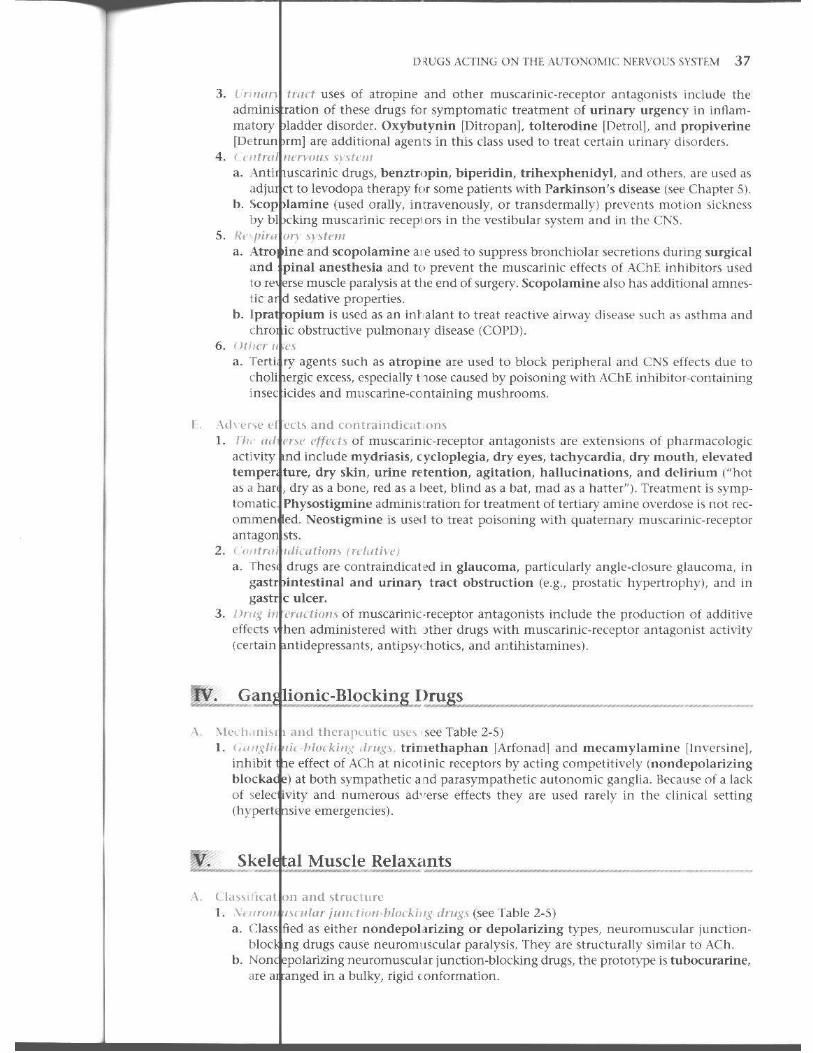
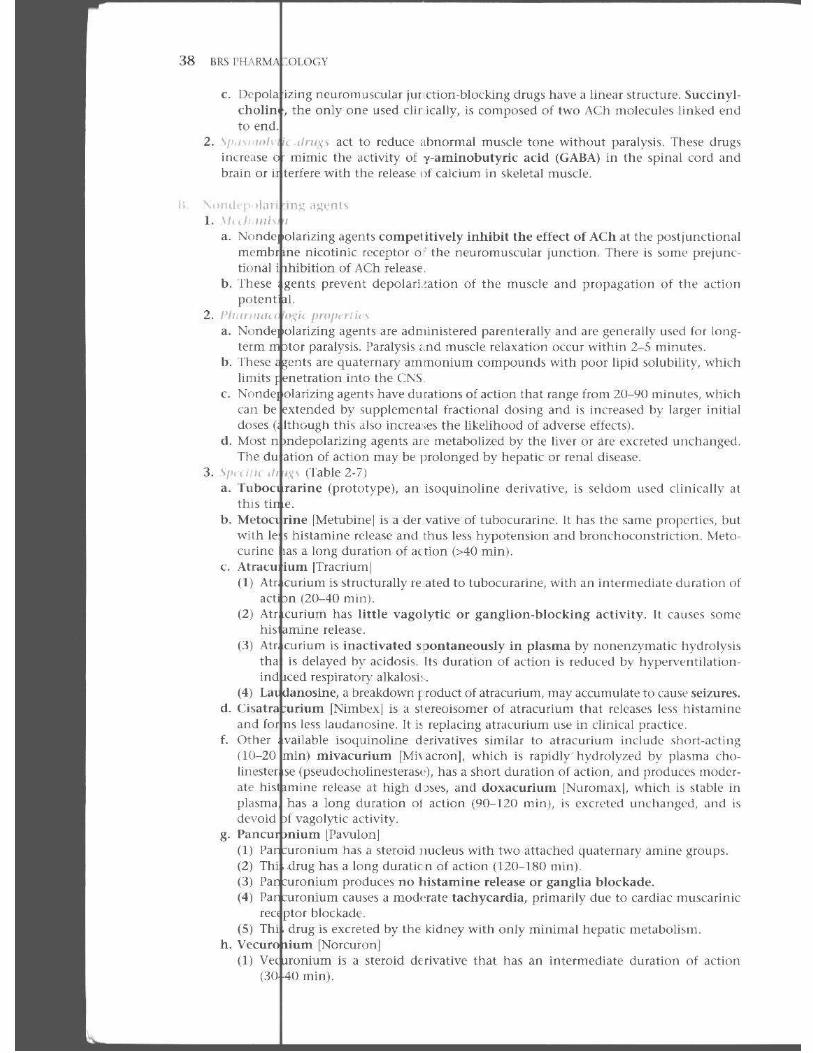
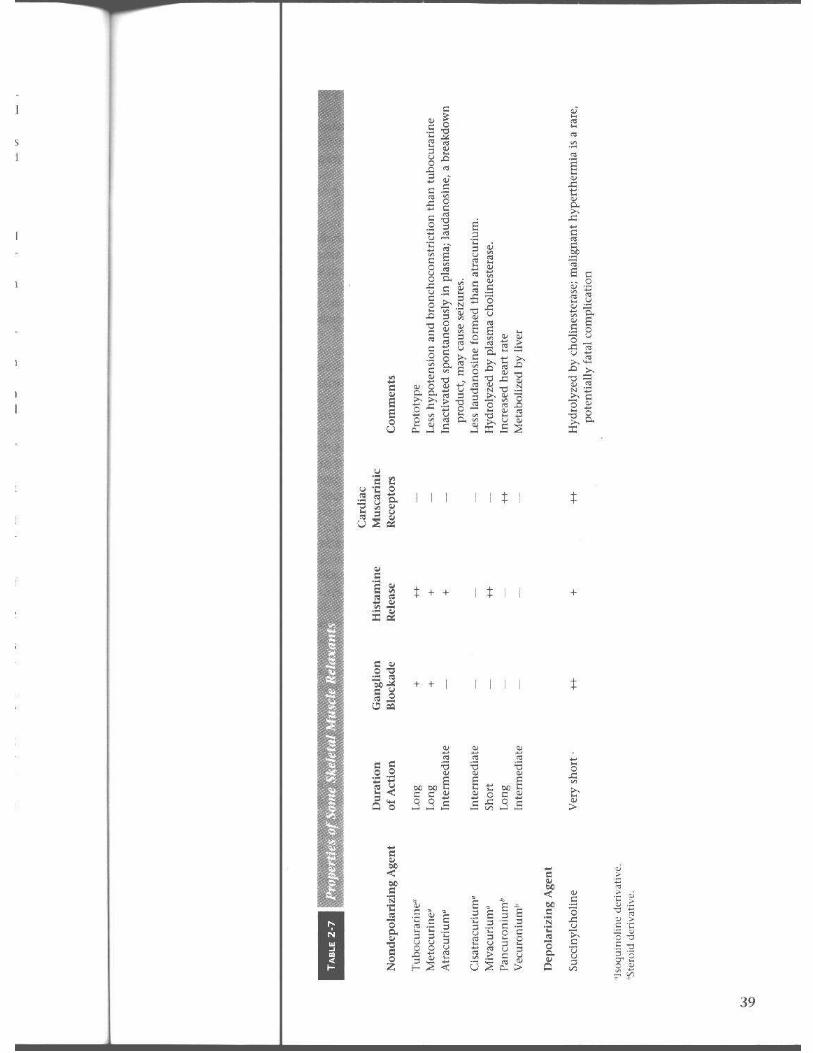
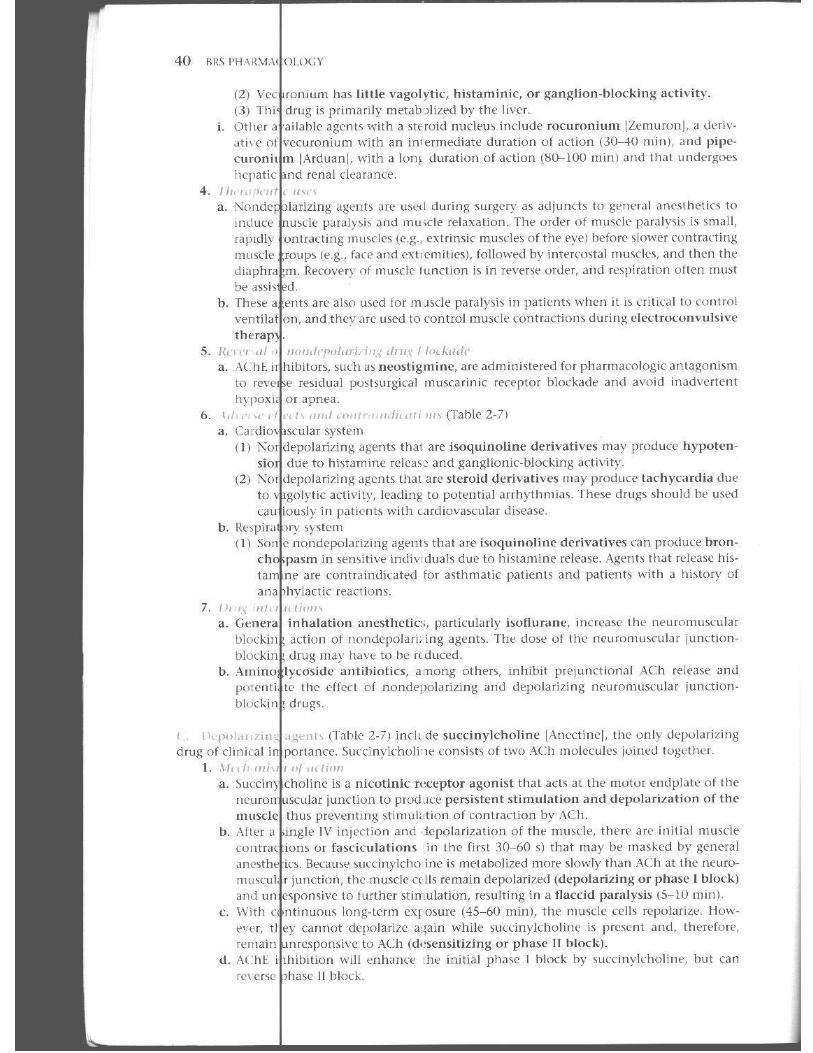
2 Drugs cting on the Autonomic Nervous System .... 25 I. TI Peripheral Efferent Nervous System 2S II . Pa asympat homimetit: Crug.. 10 III . :V1 scari ni c·Receptor Antagonists .15 IV. G< nglionic-Blocking On. gs 3 7 V. Sk 'leta! Muscle Relaxanl'i 37 VI . Sy npathomimetic nrug~ 42 VII . A energic Ikceptor Antlgonhls 47 Review re :<ol 53
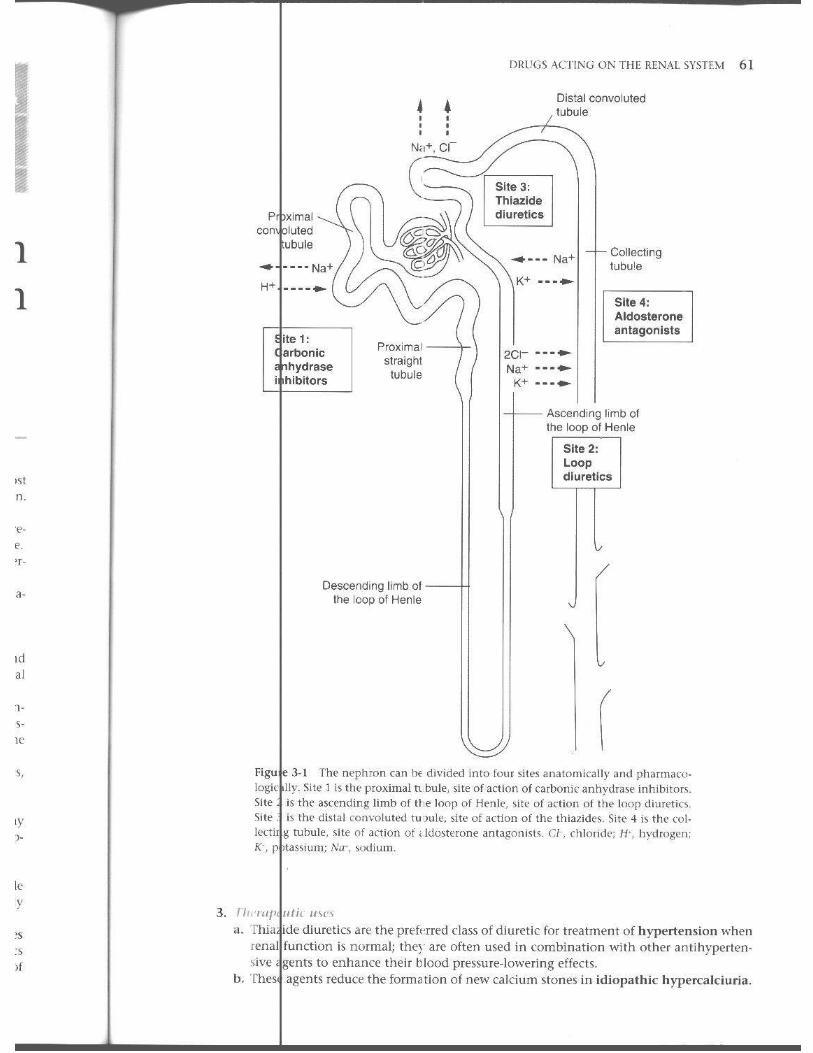
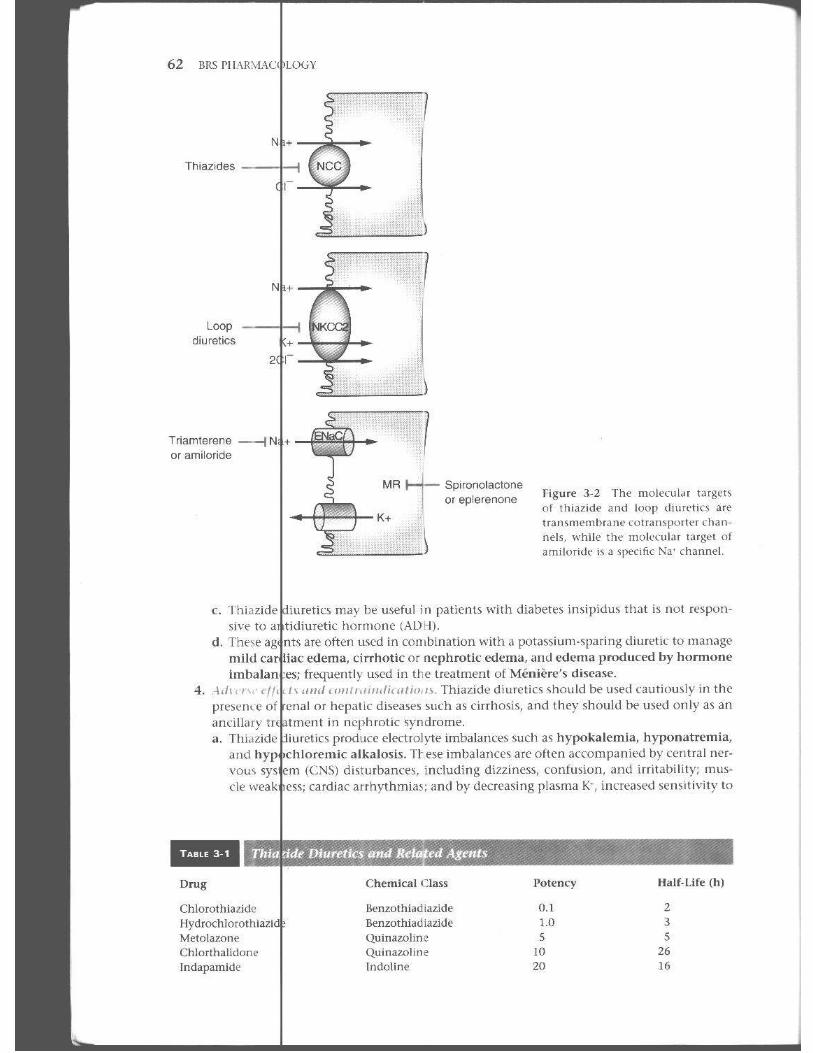
3 Drugs cling on the R(~nal System ................ . . ... 60 I. Oi retics 60 II . N ndiuretic Inhi bi tors o · Tubular Transpurt 66 Re view cst 69
~ Drugs cting on the Cardiovascular System · . . . . . .. . ... 73 I. A~ 'nh Used to Treat Congestive Ileart J:ailure (CHF) 73 II . AI i a rrh~'1:hm i( Dm gs 79 III. A ia ngi nal Agenh 81 IV. A ihypertcnsin' Drug~ 86 v. Dr Igs that Lower Plasma Li pids 92 Review est 96
ix
X CONTF,NT~
5 Drugs on the Central Nervous System · .......... 101 I. .. Drugs 101 II. .. (Neuroleptic) Drugs 106 III . Drugs ItO IV. I1 S V. Analgesics dnd An t,lgon ists L 16 VI . Drugs and Drugs Used to Treat Alzhdnll' r's Dise<lSl' 123 VII . 12. VIII . 1JO IX. ns X. 117 Review 148
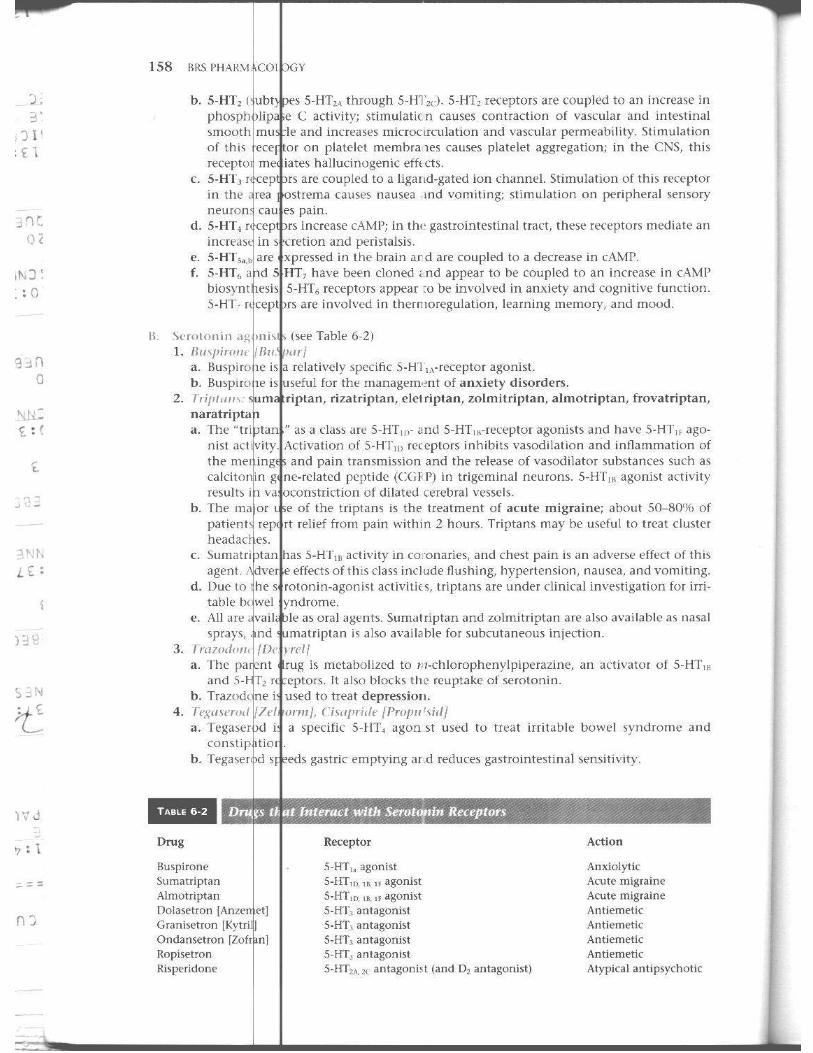
6 Ergots, Antiinflammatory Agents, and Apnts ········ ········ IS3 I. and Anti histam ines 153 II. and Seroto nin A ltagonists 157 Ill. 1 S9 IV. V. VI. VII .
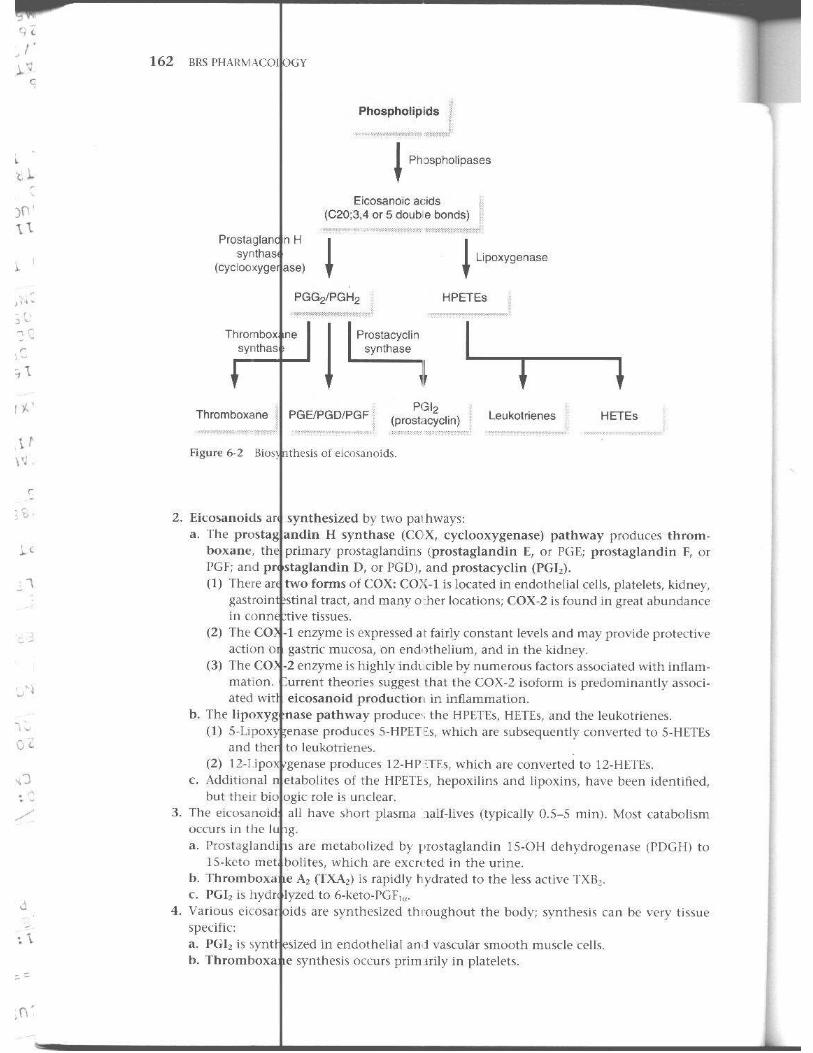
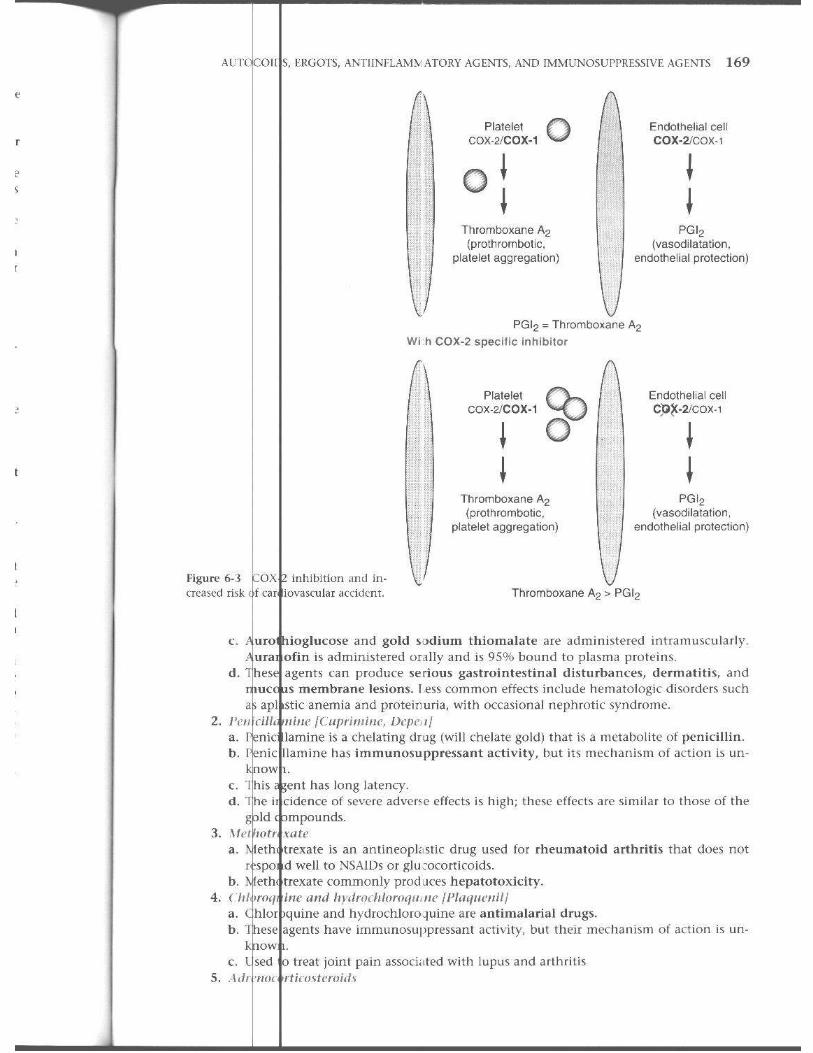
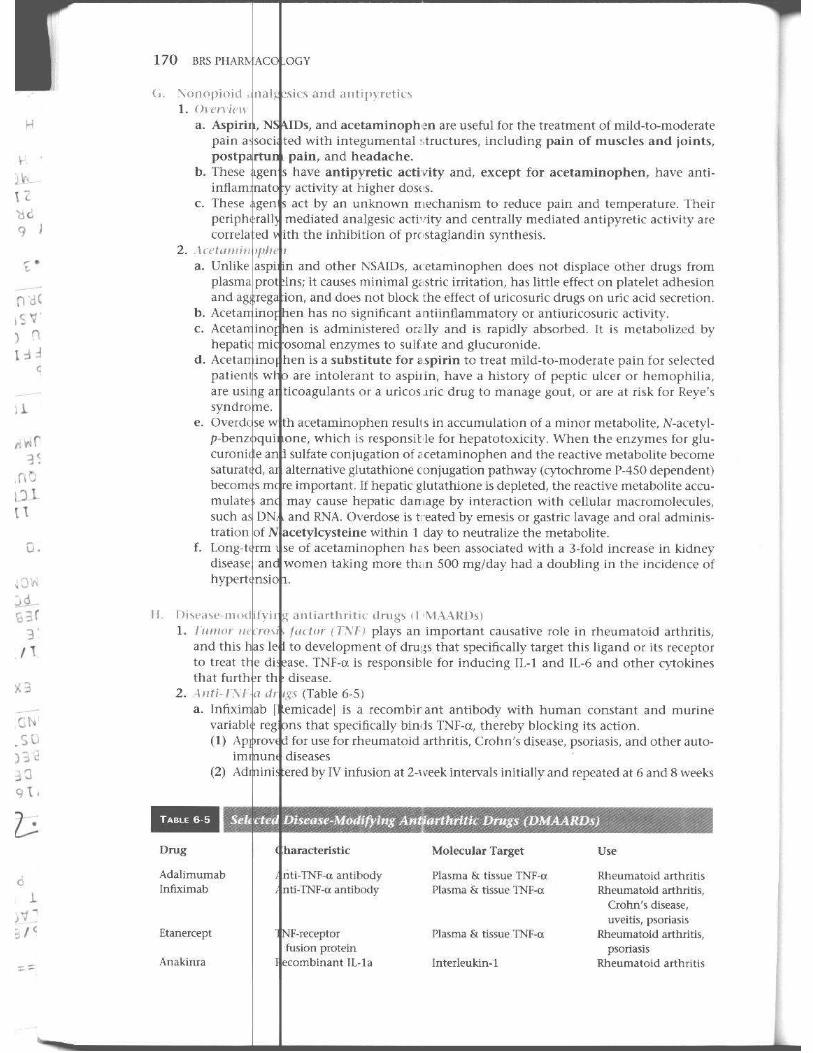
~rilf:~,~~\~~',:6 1 161 Antiinflammatory D rugs (:-.JSAIDs) 164
Used for Gout 171 VIII . Imnilm'''''PI'''''''''' Agent-, 172
177
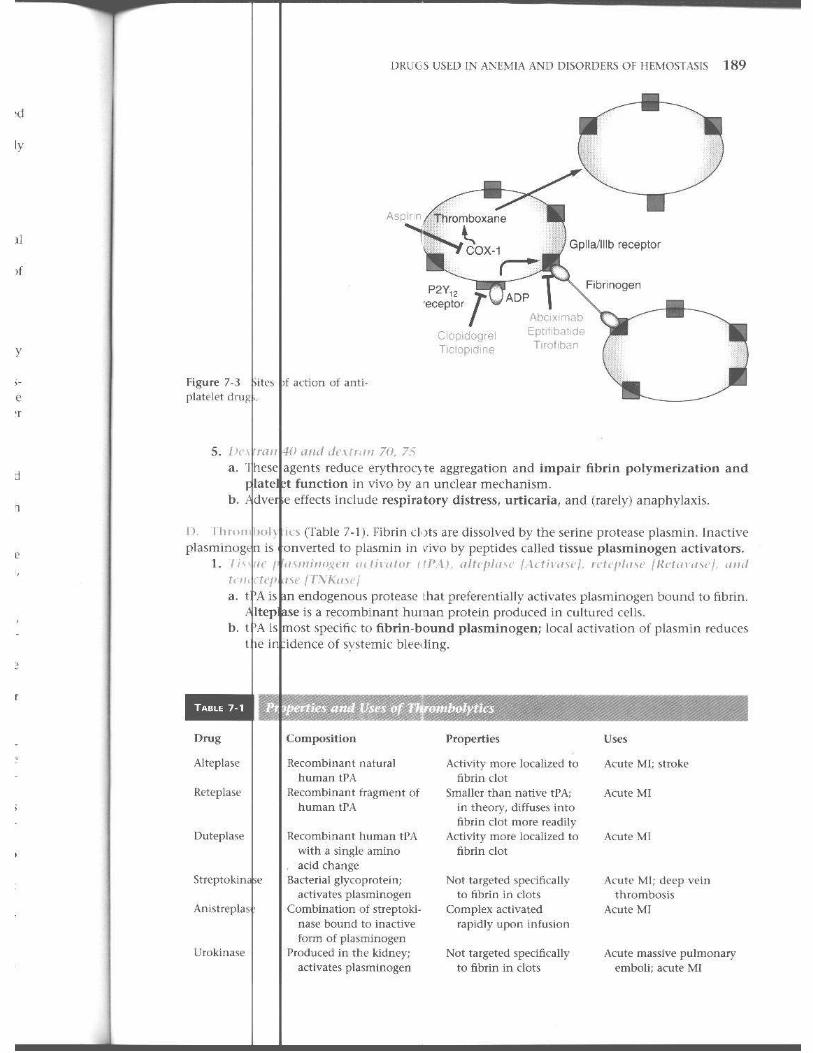
7 u,eo in Anemia and Disorders of Hemostasis .... 180 Used in the Treatme It o f Anem ia~ ISO Acting o n \-fyelo id (ells 184
III. USN in Hemostatic )iso rders 184
Review 192
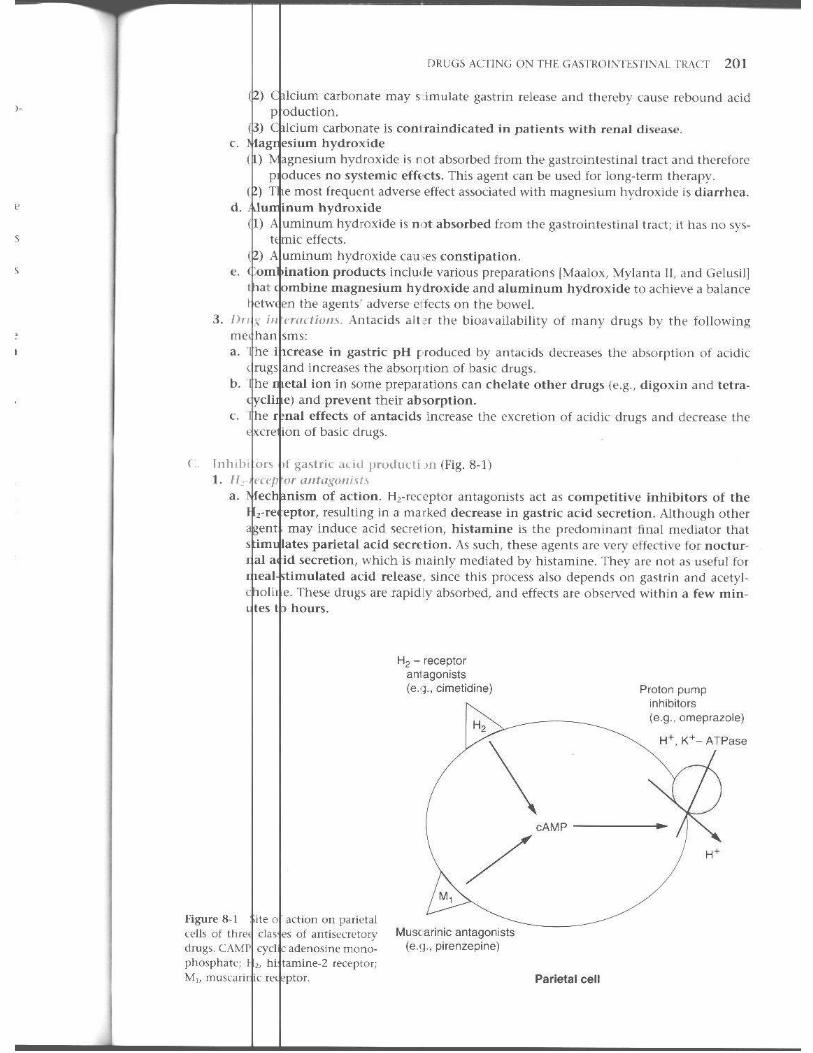
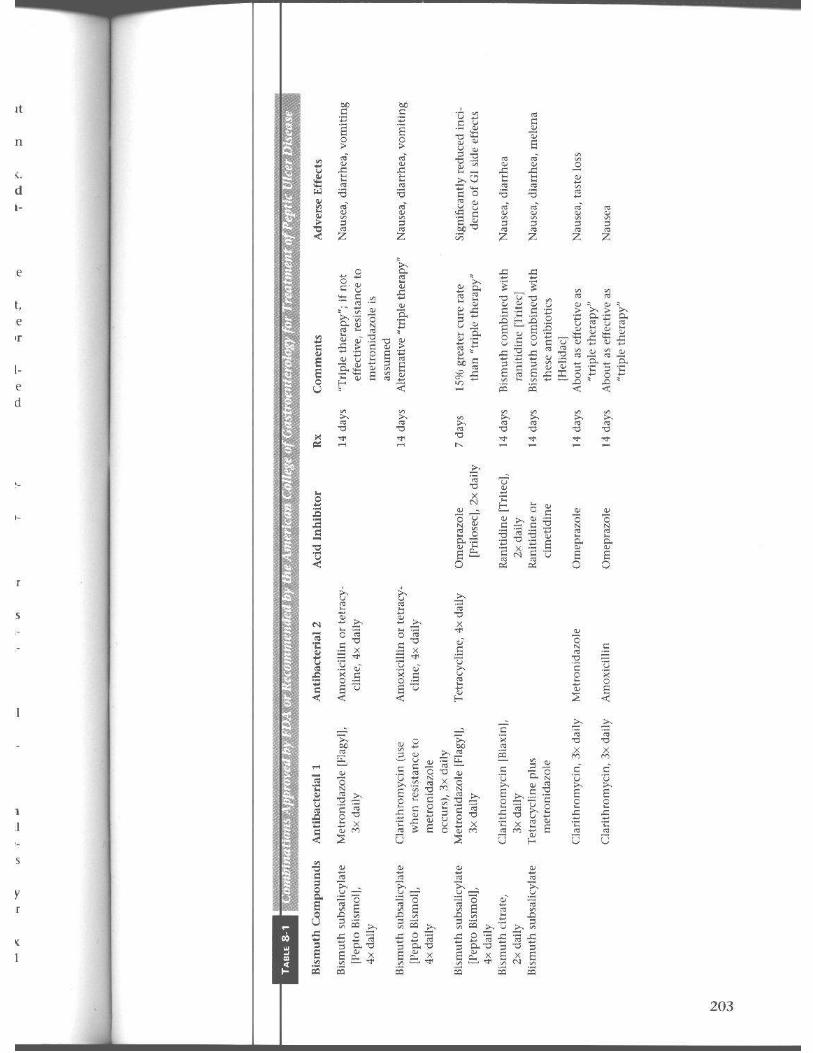
8 Drugs on the Gast rointestinaJ Tract · ........... 197 I. and Antiemet ics 197 II . and Appet it" En hancers 199 III . for Upper Gas :ro intestinai !"ract ])i~orders 200 IV. Agents 205 V. Used to Disso lve Gallston es 20:5 VI. VII .
D~I~~j:;~.~ Enzyme Hepl acements 20:5 A that Act on th e LmH'r Gast rointestinal Tract 206
Review 210
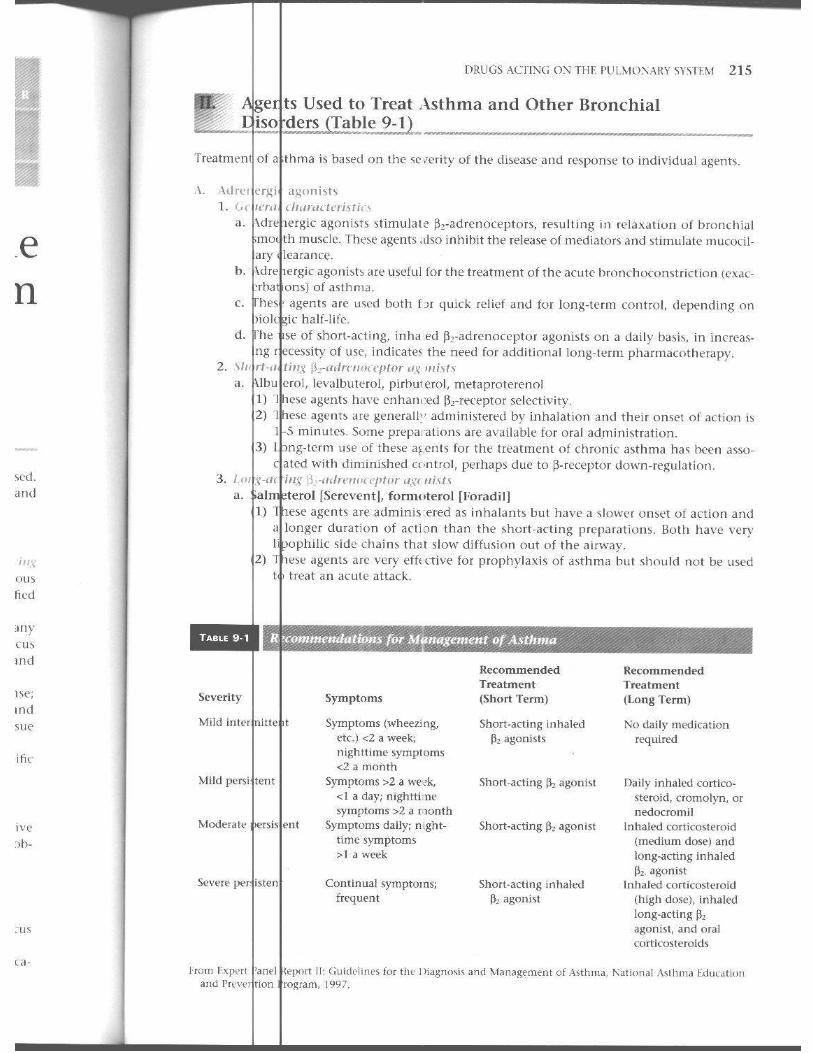
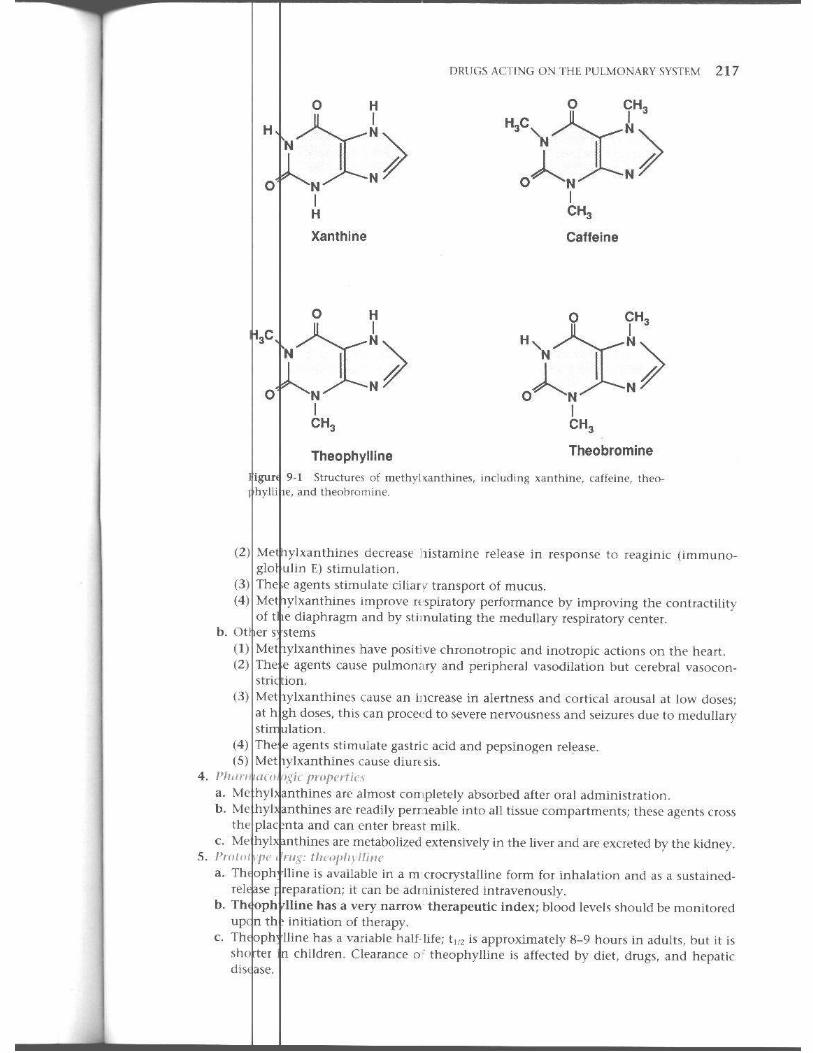
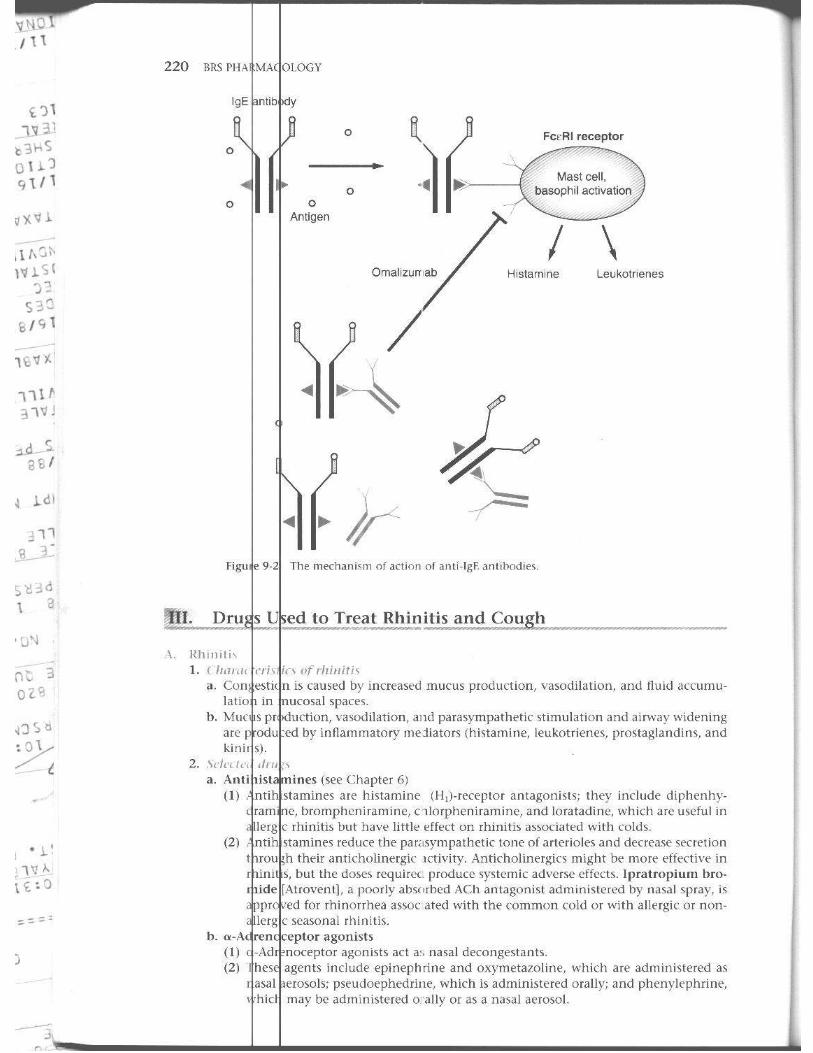
9 Drugs on the Pulmonary System ............... 214 I. 10 to Pulmonary l)isorders 2 14 II . Used to Treat Asthma and Other Bronch ia l I)isorders 21 S III. Used to Treat Rhi n it S and Cough 220
Re view 223
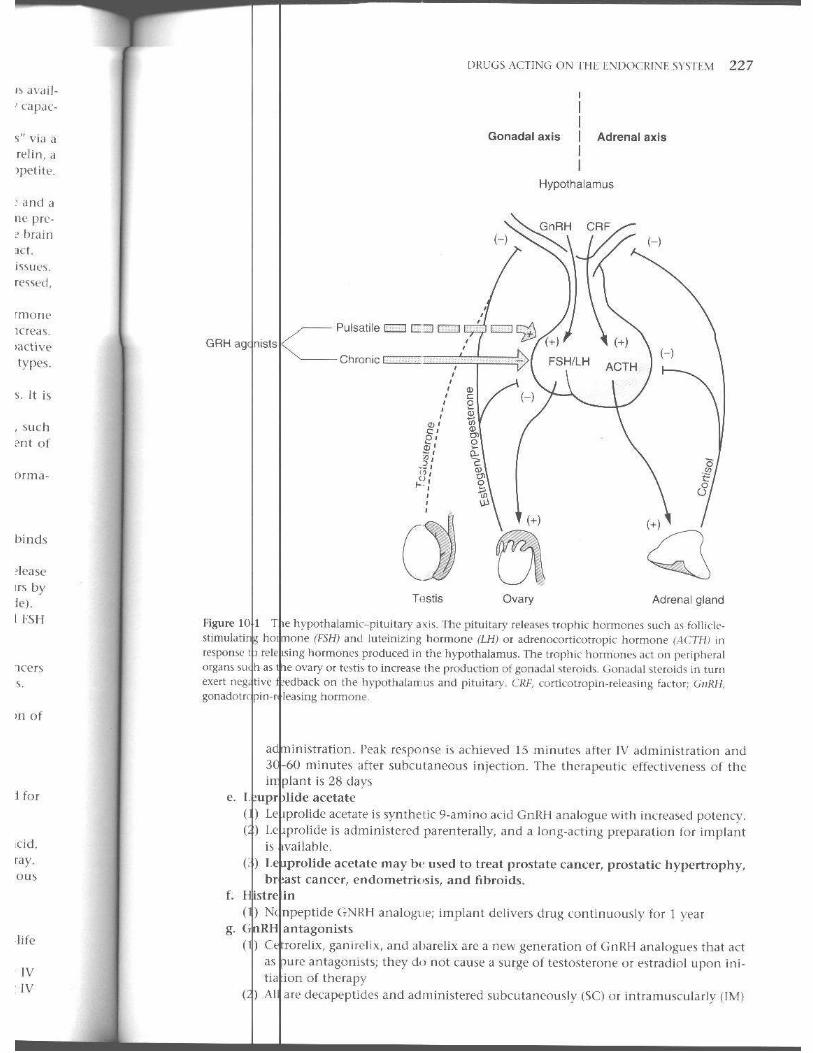
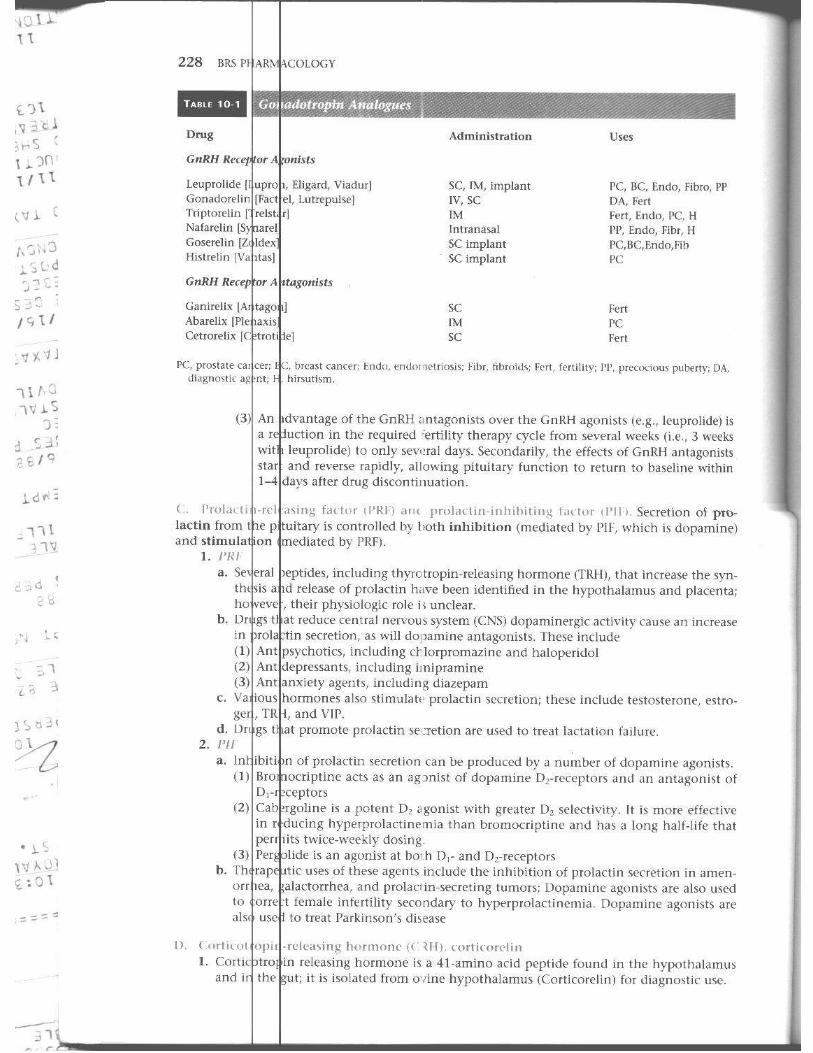
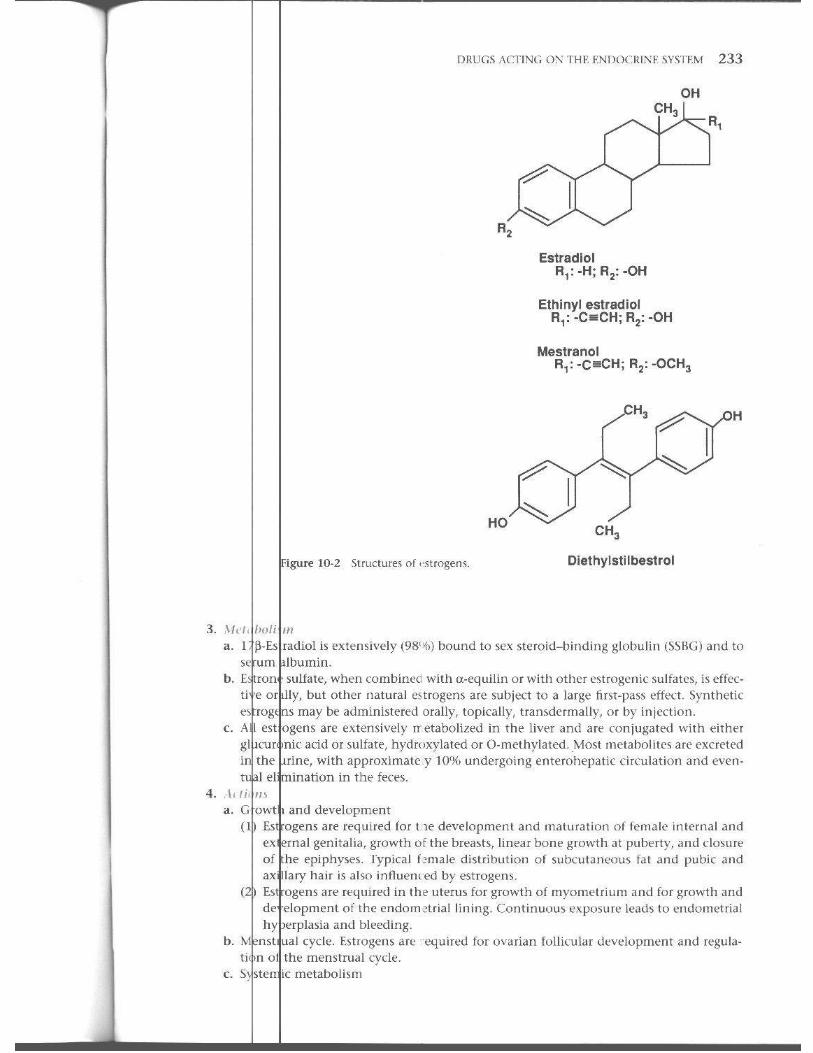
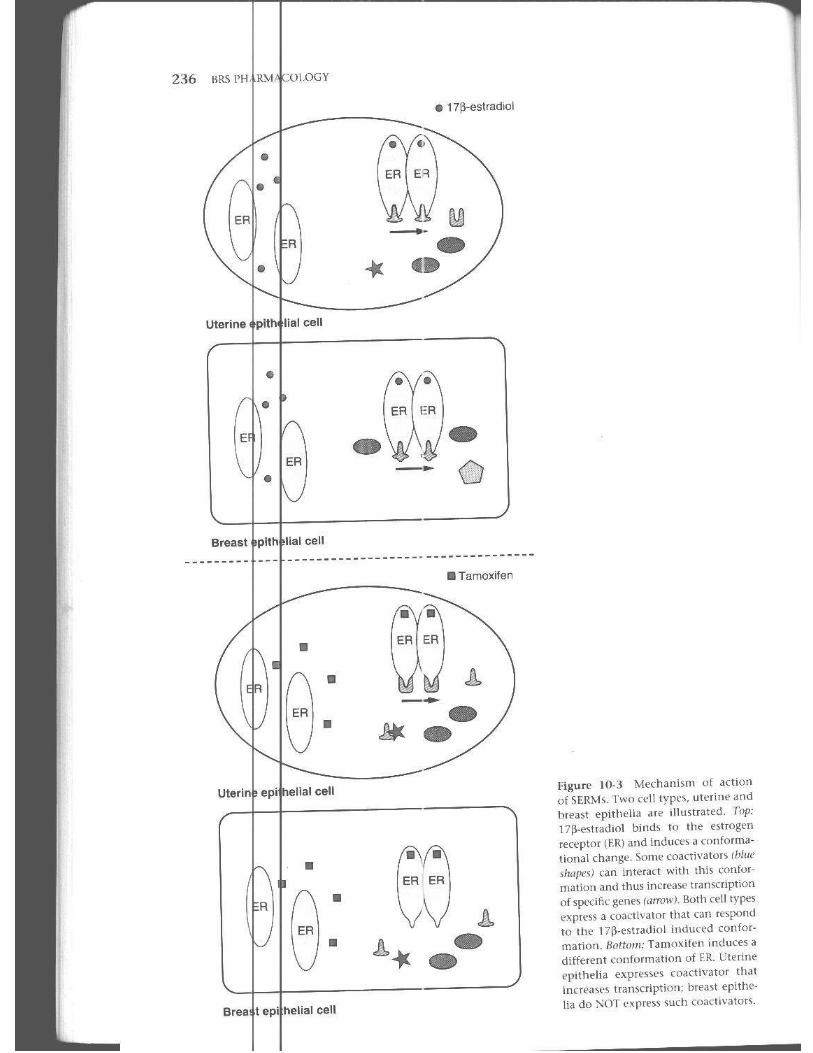
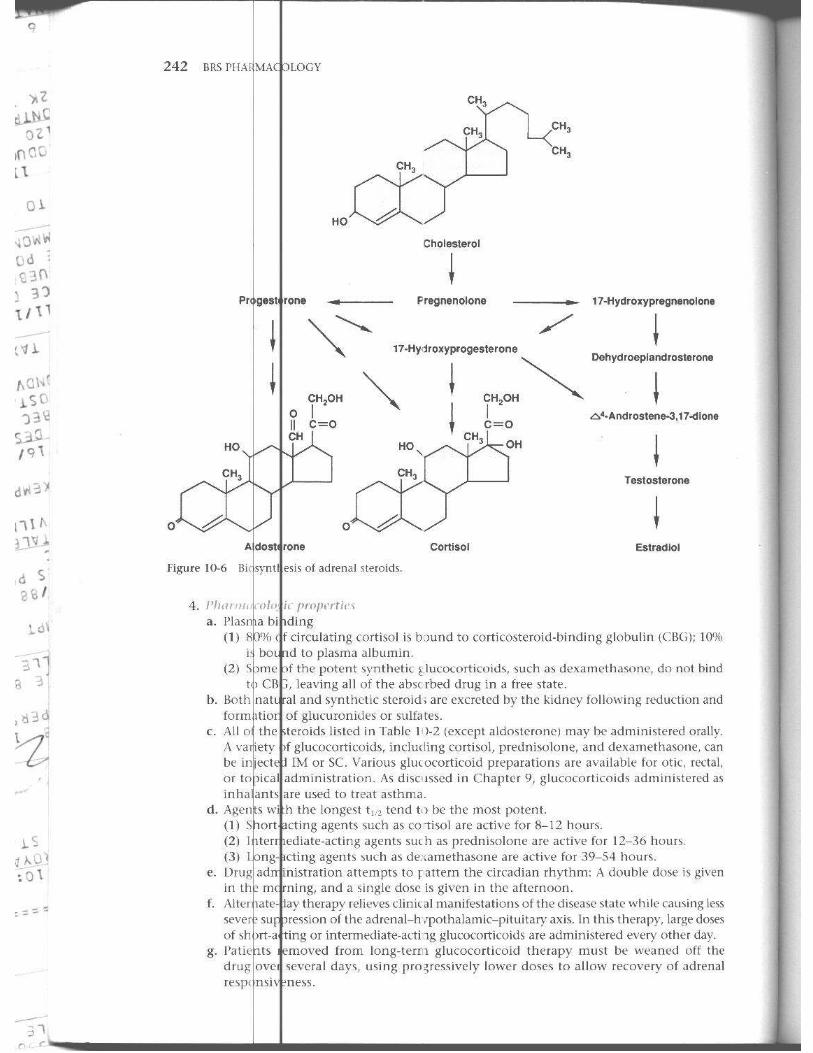
10 Drugs on the Endoc;rine System ................ 225 I. Recepto<s 22: II . The 225 Ill. The. IV . Th('
f~~t~;~~, l'ituitary 229 , Pituitary :!31
c ot\, F. :,\'TS xi
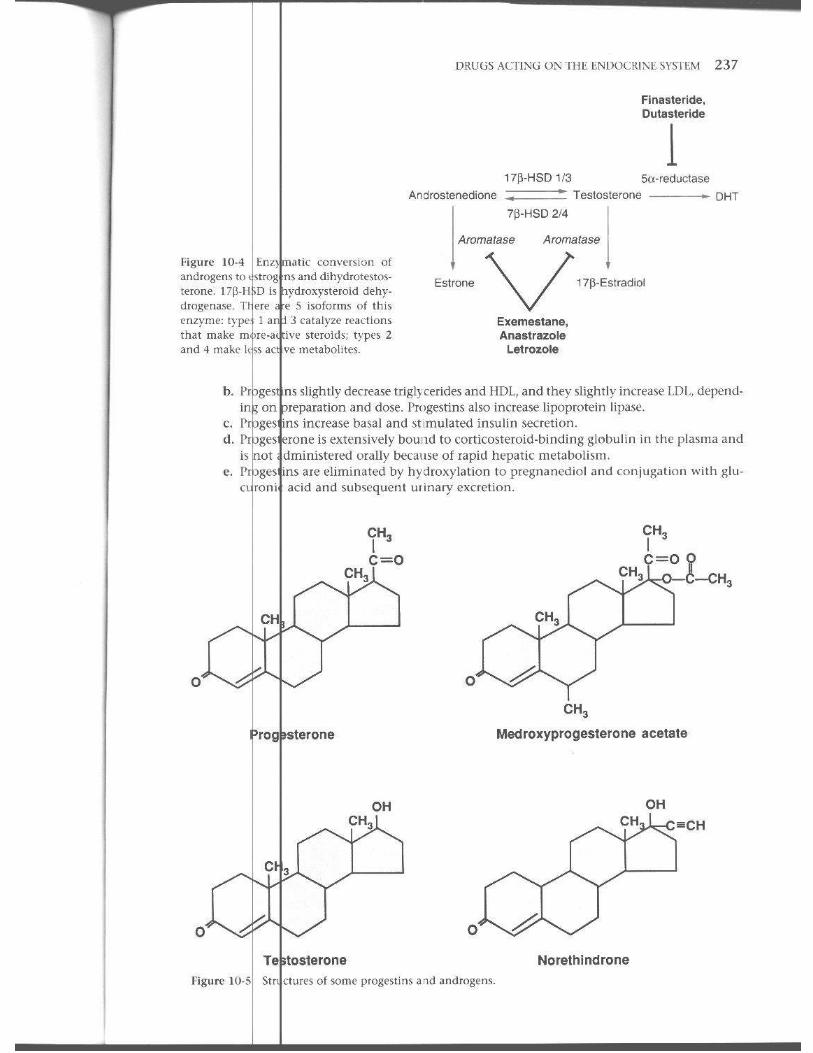
V. !rugs Acting on th e G'Jnadai and Reproductive Sys tem 232 VI . h e Adrenal Cortex 2-11 VII. he Thyroid 245 VIII. - he Pan creas and GlueJsc Homeost a~ i s 2-1 7 IX . he Ca lcium Ho meost.lt ic System 252 x. I etino ie Acid and Deri ' atives 256 Revie Test 260
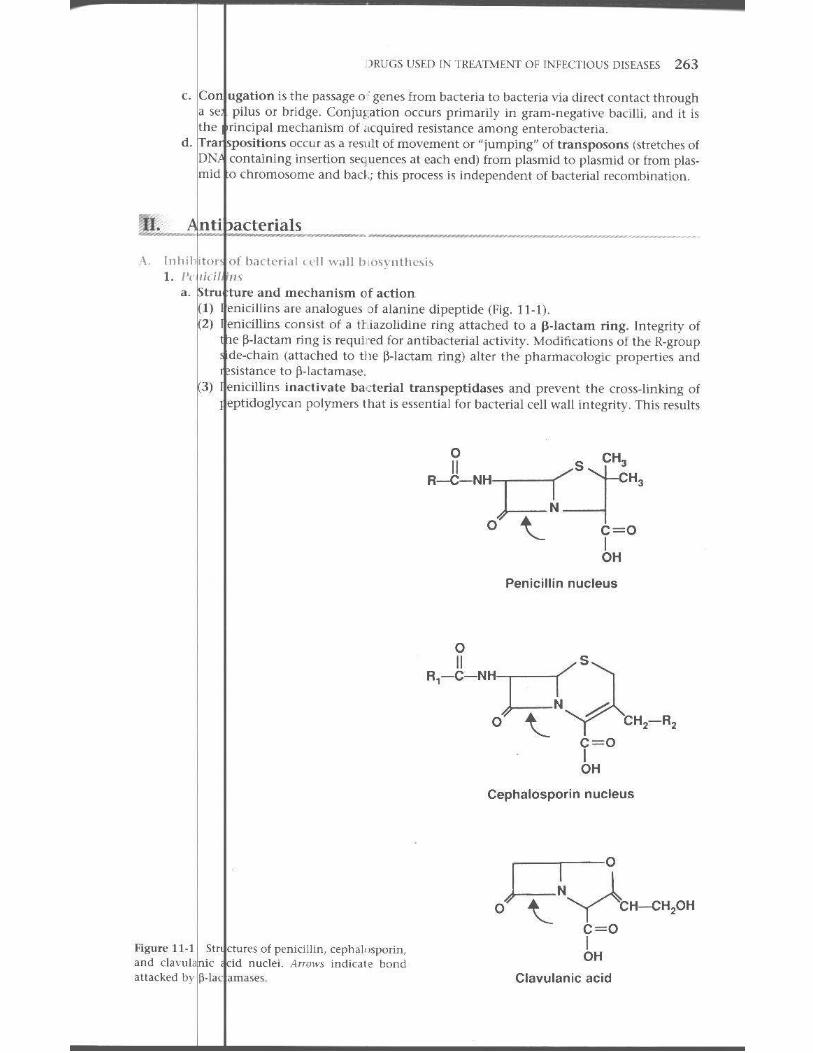
11 Dru Used in Treatm.ent of Infectious Diseases ... . .... 262 I. l l fcc tioLLS Di sease Tht'lapy 262 II . ntibacterials 263 III . . ntimycobacterial Age1 b 276 IV. f n tifungal Agent s ;~80
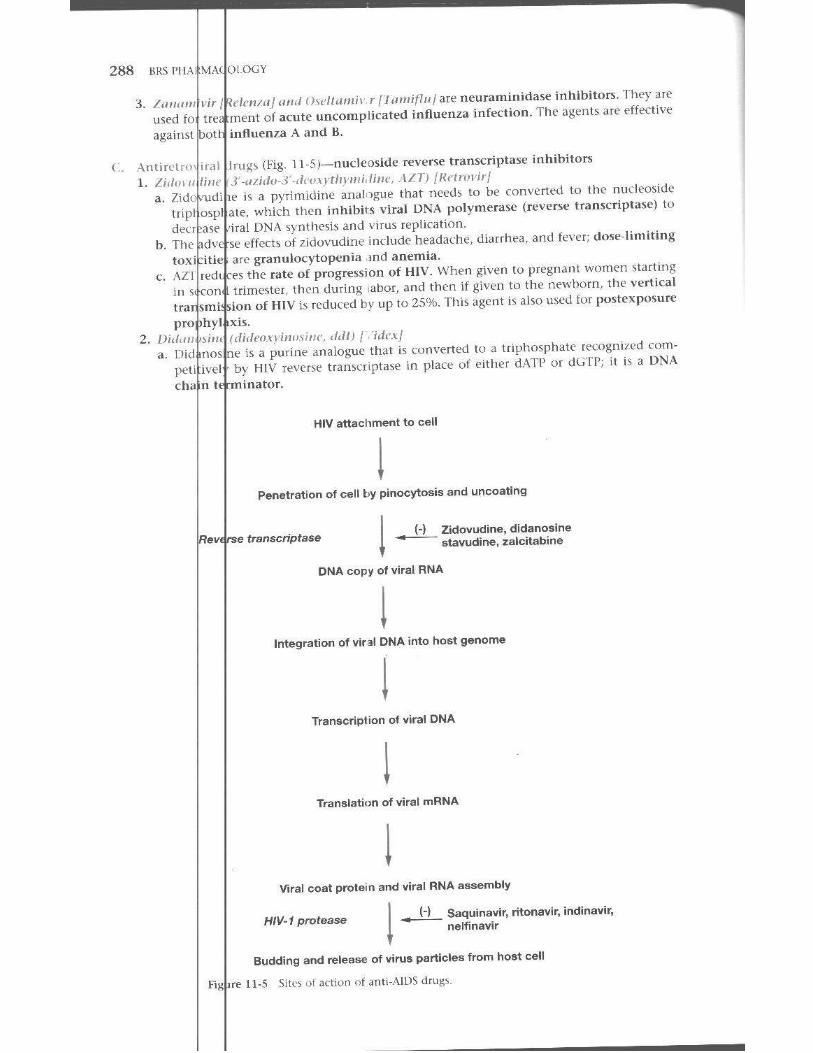
v. ntiparasit ic Drugs 282 VI. I n ti viral Drugs 2R6
Rcvie Test 293
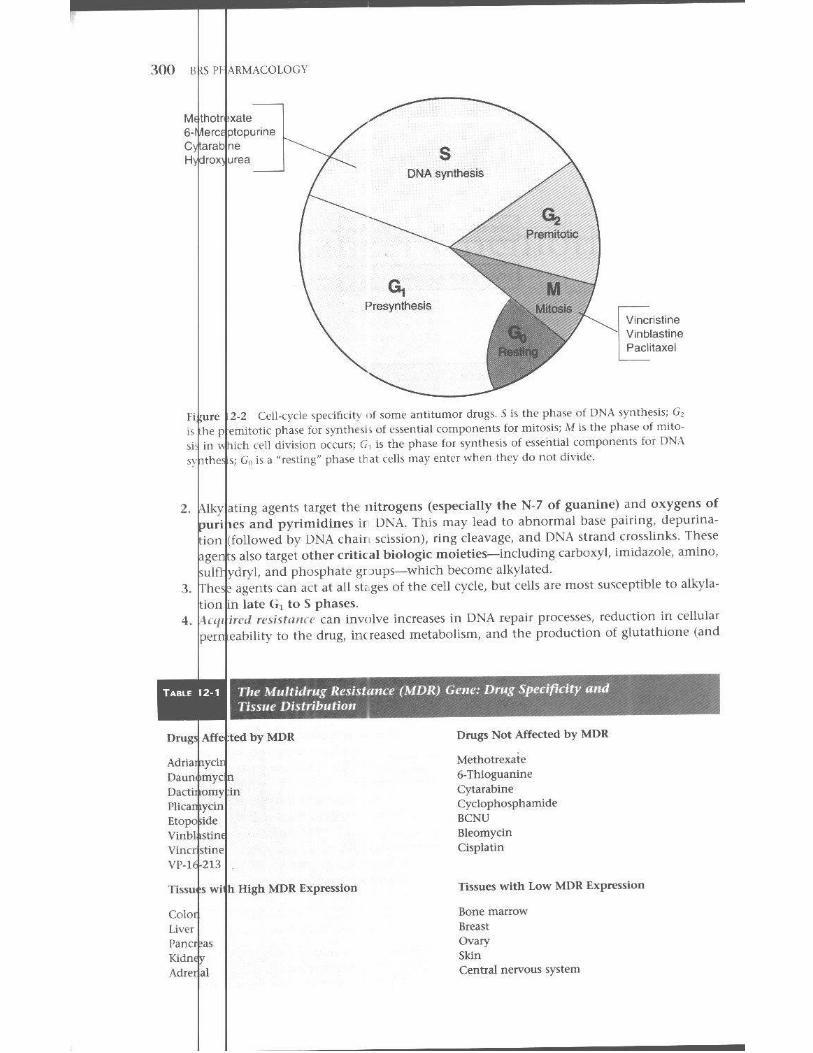
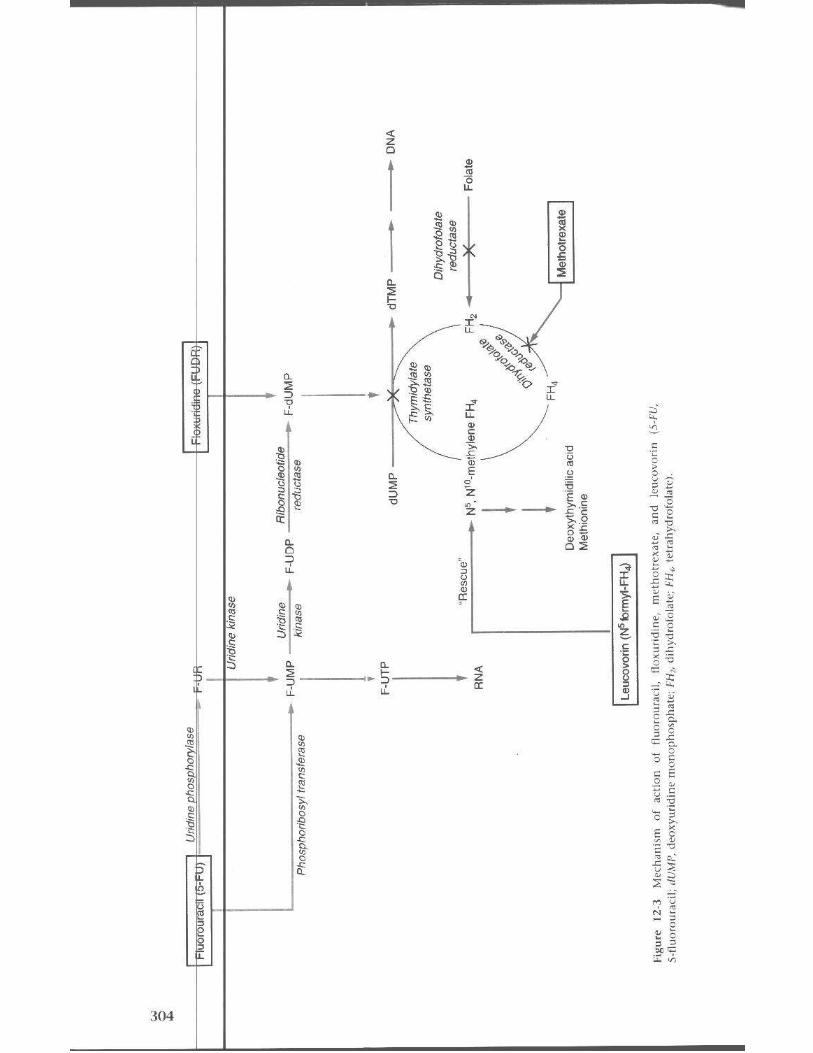
12 Cane r Chemotherapy ........................... . .... 298
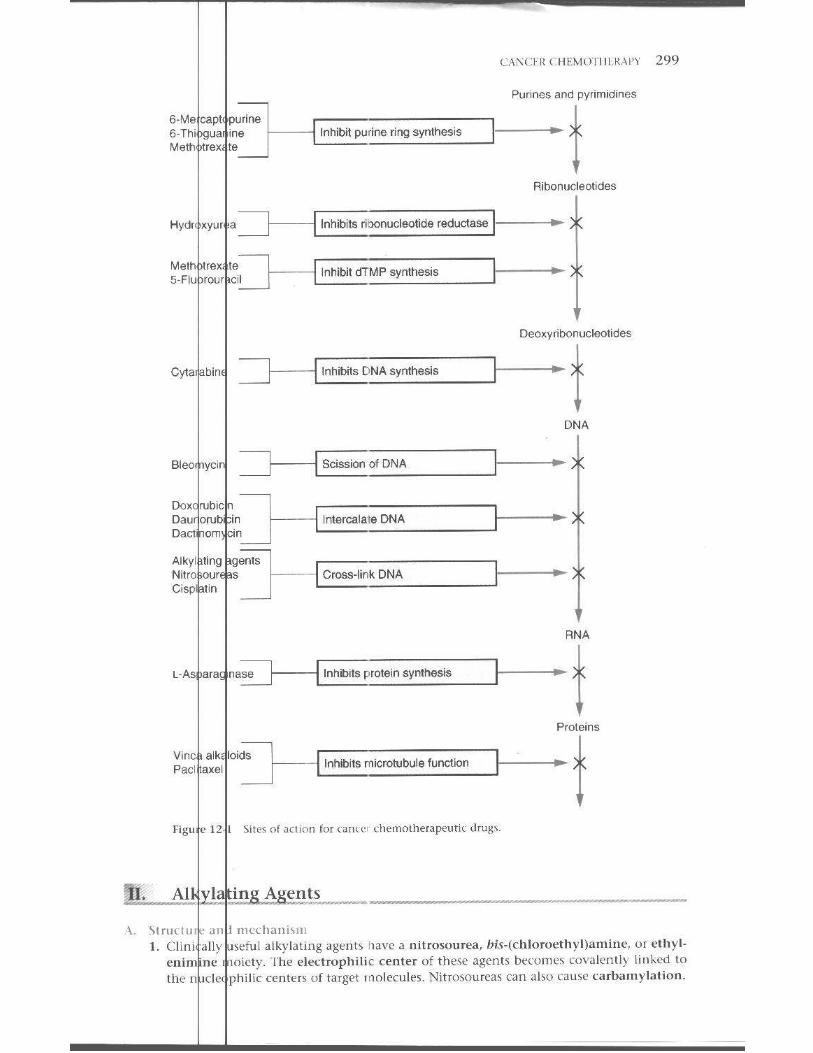
I. r rinciples of Cancer Chemotherapy 29S II . lkylat ing Agents 299 III . t nt imetabolites 30:; IV. atural l'rodm1s 1[6 V. I iscellaneous Agents 308 VI . . ewid Hormo nes an d 4..ntagon ists and Related Drugs 3 t 1 VIT. d junct Agen ts 3 13 Revie ' Test 315
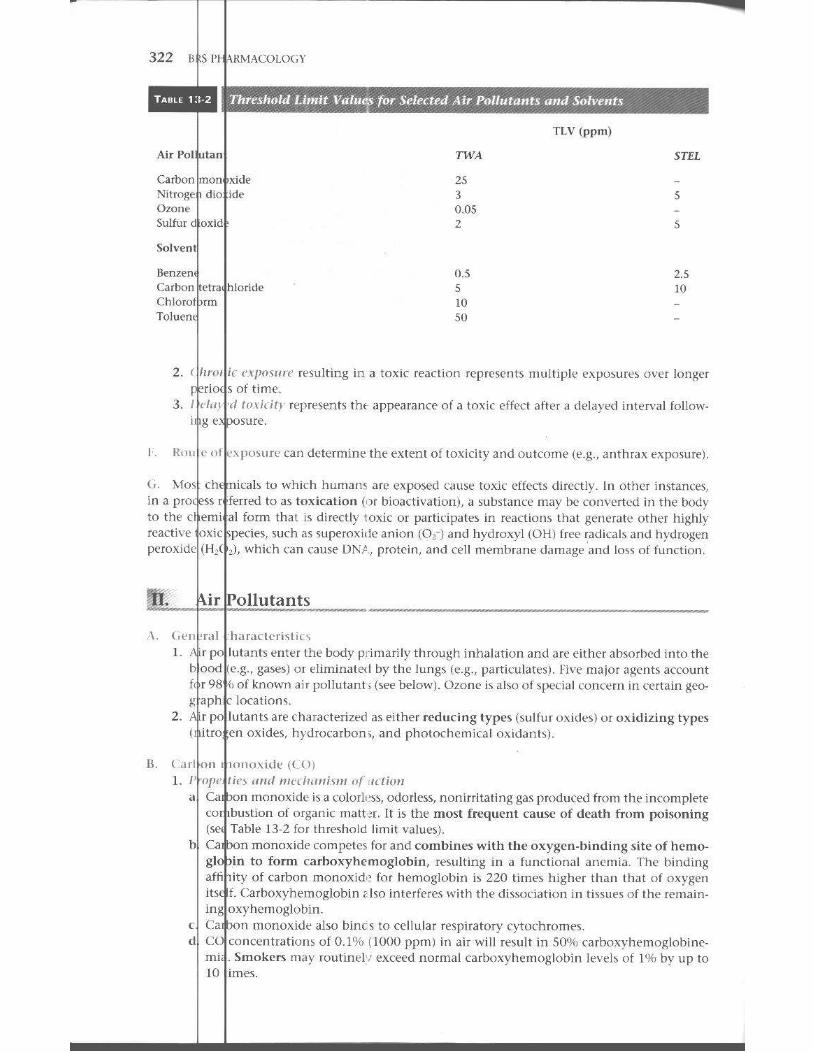
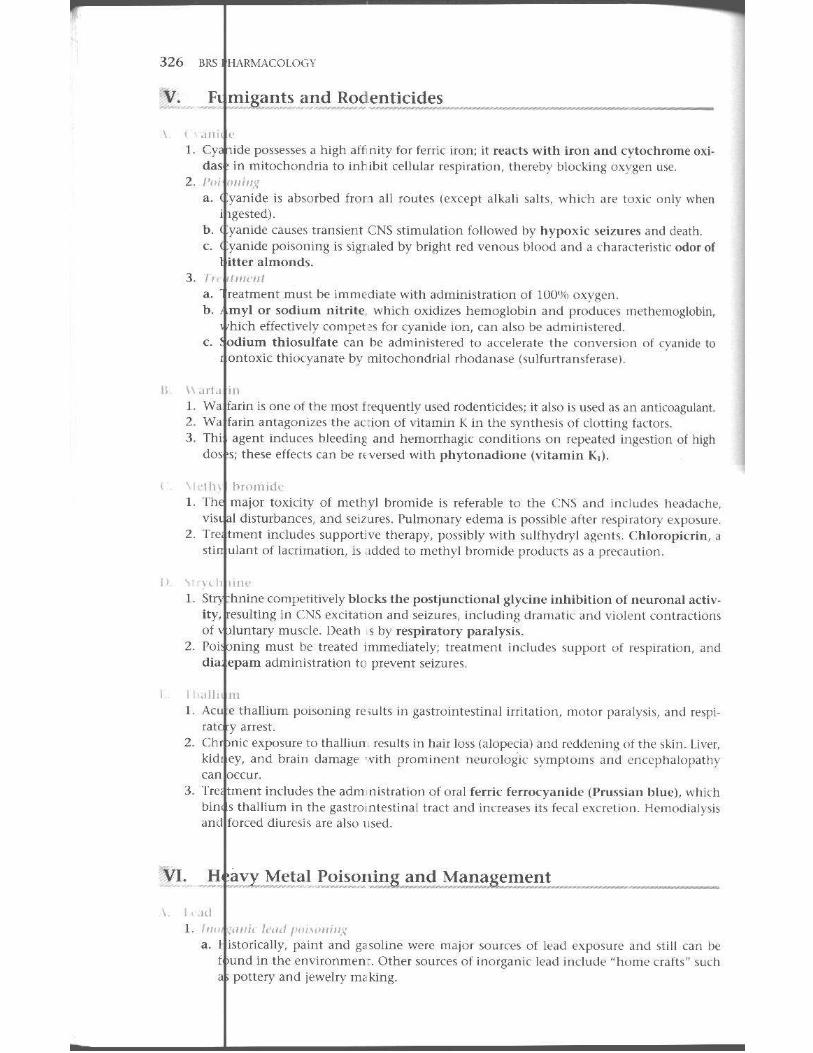
13 'foxi logy . . . . ................... . ..... . . . . . . .. ..... 320 I. I inci ples am i Tl'rminology 320 II , ir Pollutan b 322 III . S )Ivents 324 IV. J lsec ticides and lIerbi Cld es 324 V. F Jlll igants and Rodenticides .326 VI . ~ ravy Metal POisoning and Ma n agrm l'nt ~i26 VII. l rug Poison ing 330 Revic Test 333
Com rehensive Examination ............... , .. . . . .. . . 335
lode .. ... .... ..... · ·.·.· . ··.···· .. · . ··.· ·. ····.·· · · 353
I
) I
General Principles of Drug Action
",,"_~nos-Response Relati onships
.\ nlU~ (' fh 1\ are producl'd by alteJing the normal funclions of c('l1~ and tb~lIe, in the body via orl\' o f fou general mechanisms:
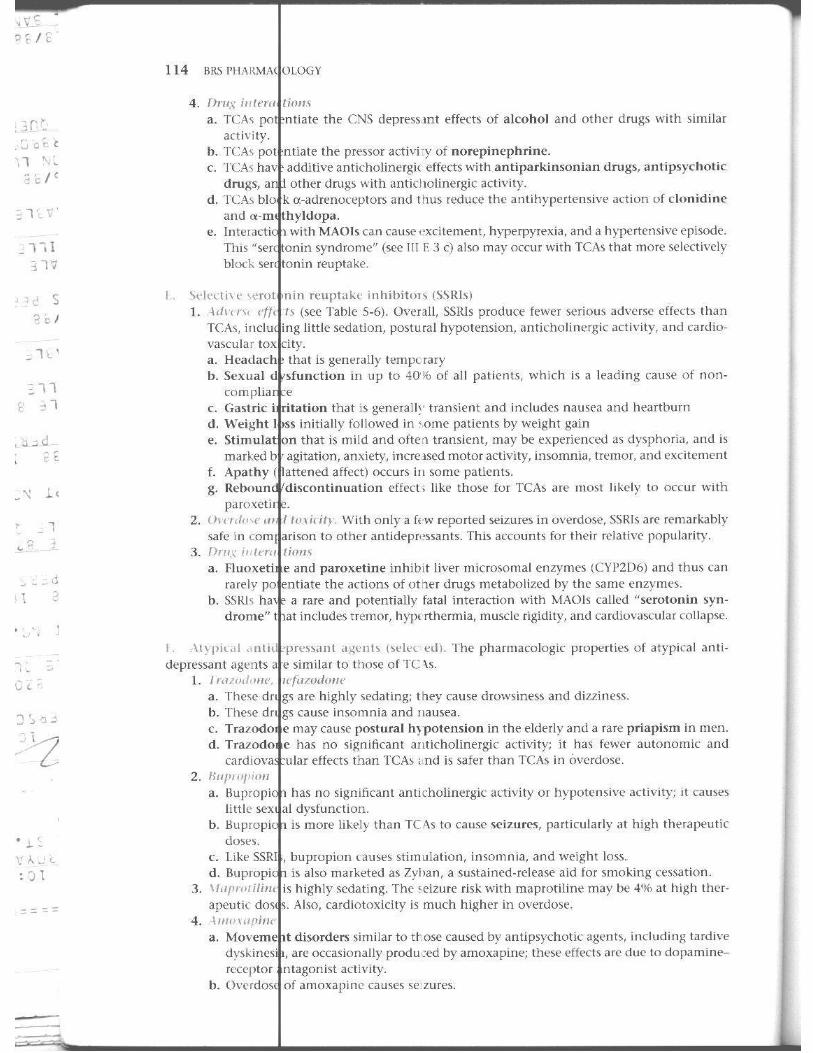
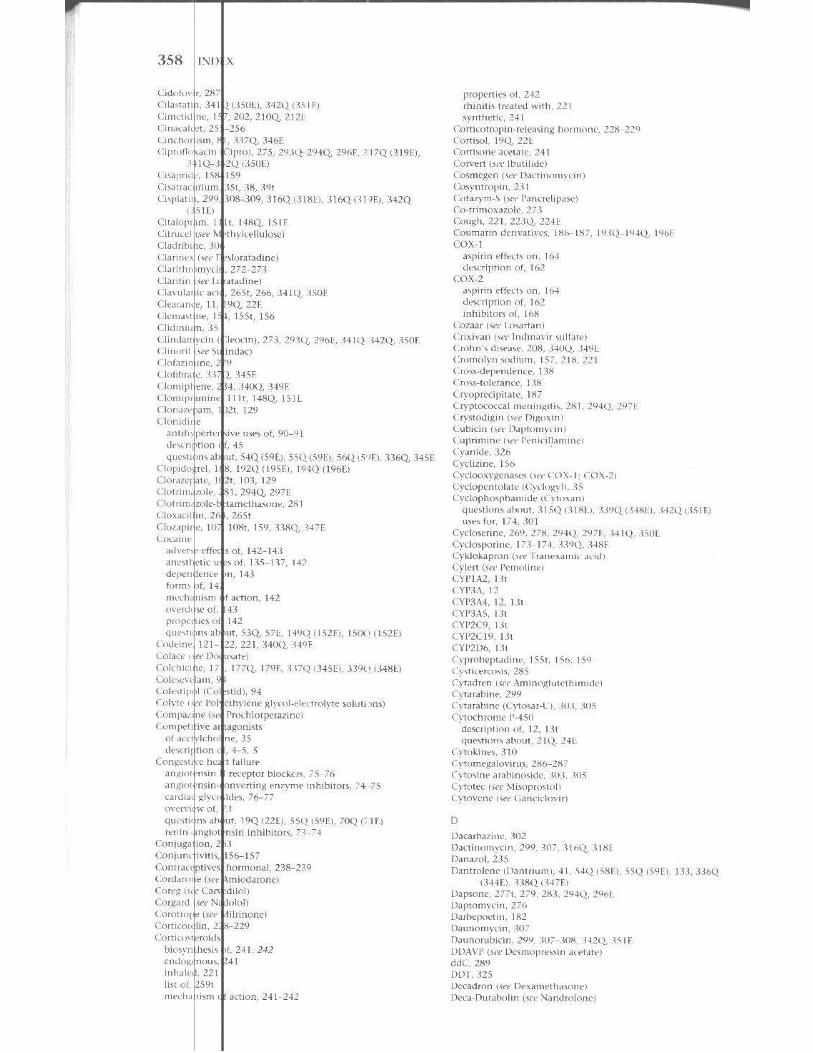
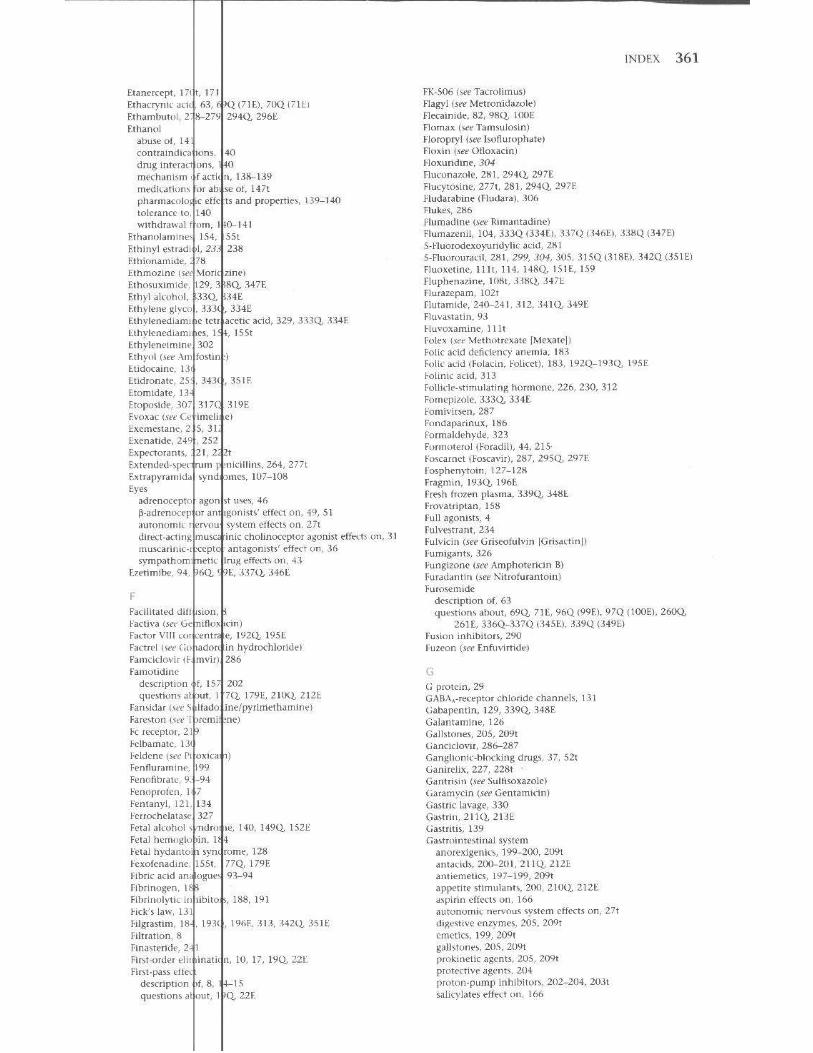
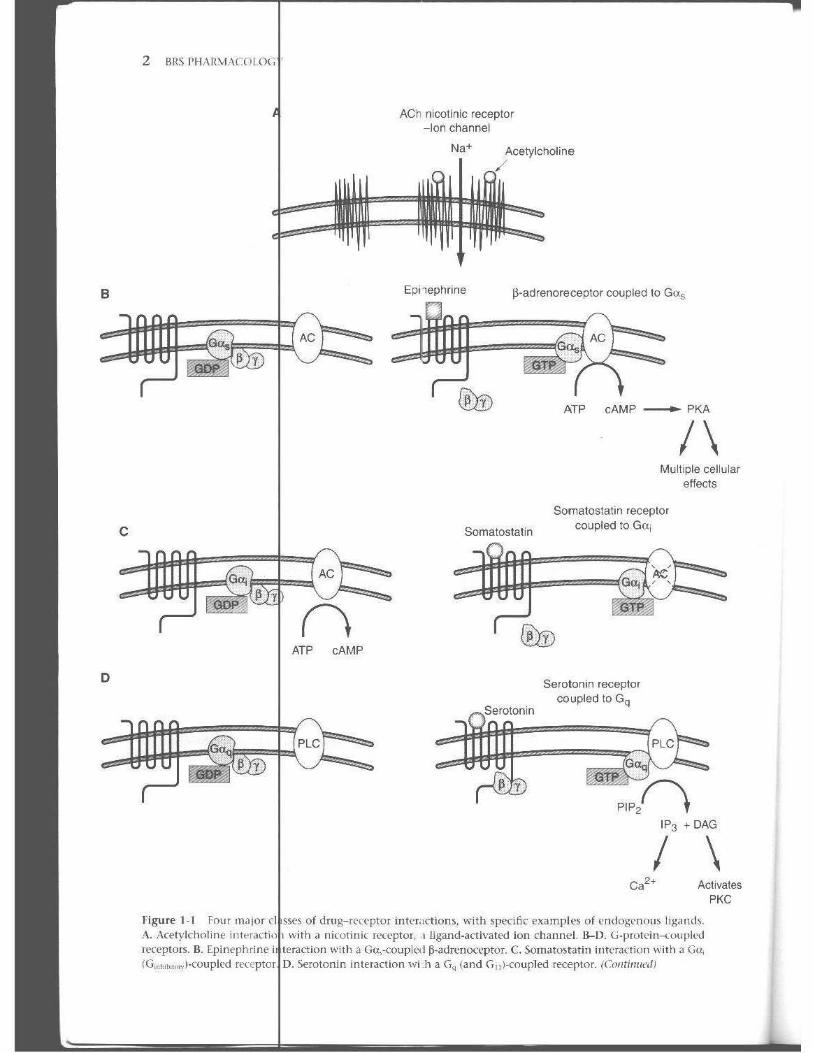
I. /1111'1 <14 i OIl IIi'" rn,p/on, n ,lturally occurring target macrornolccule~ th,lt mediate th£' cffe('l s )f endogenous physiolo!,iC suu)tanoc's such as neurotrallSmitters and hor!llone~ a. figu e 1-1 illustrat t:'s the four majm e la s)e) of drug-receptor intl' TKtions. using specific
cxar lples of endogenous li gands. (1) .iga nd-acti\'atcd ion dlannels. Figure J-IA illustrates aC{,I)' lcholi ne interacting
ilh a n icotinic receptor ttlat b a nonspecific Na' (K' tr<lmmembranc ion channt'!. teract ion of a moltlllie :If acetylcholine with each subunit of Ihe channel produces conformational change that permits the passage of Na' and K'. Ot her ch,m nels that re ta rgets for \ariou~ dru~s include SpKifK Cab and K chan neb.
(2) ;-pro lc in--<oupled rcctplOrs (Fig. l -I B- lJ). G-protcitl-(:o ll pled reu!ptors com· ose the largest l· l a~s of receptors. The receptors al l have 7 tra n smembrane scglents, 3 intracellular 10Jps, and an intracellul,H t·arboxy-terminal tail. The bioglc activit} of the r{'('ertors is rnaliated via interaction with a number o f G (GTP
I inding)-proteins . ·1) Ga,-coupled receptors. Figure I-IB il lustrates a B-adn.': IH.Kef)W r, which when
<Ktivated h} ligand linding (e,g., epi nephrine) eXChanges GD P for GTI'. This faci l itate~ the migrat on of Get., (Gu,"m"l"'o,,) and its interactio n with adenylyl t·}"dase rAC). Cru.,-bound AC ca\alyzc~ the pnxh,il"lion of cAM l' from ATP; cAMP activates protein kin;.se 1\ , whirh ~ubsequentl}' acts to phosphorylate and activate a number of effe ctor proteins. The [iy dim er may a lso :Ktivate some efte<:t o r~. Hydrolysis of th ~ GTP bound to the Go. to GOP terminates the signal.
) GOI I (G1nhobowr,)-i.:ouplet.l rt'Ccptors (Fig. I- IC). Ligand binding (e.g., somatostatin), to Gu; (Ga,nIub,,,,,, )<Ol pled ft'(·eptors, simi larly €.\(hangt'!> G'I I' for li DI', but Go, inh ihi l ~ adenylyl ere asc, leading to reduced cAM l' prOOuftion.
{-l G~ (and G Il)-coupletl ft'ceptors (Fig. 1-1.D). G~ (and G,,) interact with ligand (e .g., seroton in )-,Kti " ated receptors and increa se th e 3cth ity of phospholi pa'ie C (PLC). PLe: cI 'aves the membrane phosp hOlipid phosphatidylinmitol 4,5-bispho~phatt' (Pil l) to diacylglycerol (DAG) and inositoll,4,S-triphosphate (II'; ). lJAG activate~ protein kinase C. which can subsequently phosphorylate and acti\aie a n umb. 'f of cellula r proteins; II'. cau'ies the release of Ca2• fro m the endoplasmic ret icu lum into the cytoplasm, where it can activate many cellu lar processes.
B
o
c
Figure 1-1 Four m,liar A. Acetylcholine i
[l'Captors. B. Epinephrine (G",h,b<,C<"·J-<..'oupil'd
ATP cAMP
ACh nicotinic receptor -Ion channel
Na+ Acetylcholine
Epi lephrine l5-adrenoreceptor coupled to Gas
Somatostatin
ATP cAMP _ PKA
/\ Multiple cellular
effects
Somatostatin receptor coupled to Gaj
Serotonin receptor coupled to Gq
P1P2f'\ IP, +DAG
/ \ Ca2+ Activates
PKe
of drug-I('n:'ptor inter.Ktiam, with specific examples of l'mlog<.'num ligillids. with a nilOtinic [('(cpIO! , I ligand-activated ion channel. IJ-O. (j·protdn ...... uupll'd
i Witll a GCI.,-coupled p-<1drenoceptur. C. Soil1Jtu~tatin jTlIl'[J(liOrl with J G()'
Serotonin interaction wLh a G" (and G il l-coupled receptor. (Colltinucd)
\ ,liuta. ,
"" ""
G
\ :tlVates PKe
E
I u tin receptor
00 y y
F
HSP90 !
o A
ti r" r~AL I'RI",C!l'L1'5 OF DRU( , Acno:'\ 3
Ins Jlin receptor-activated tyrOSlr'le kinase activity
Insu lin
C>
po, 00 po, y y
IRSf\ IRS - P04
\ PI3·K
\ AKT
I \ :Orlisol actIVatIOn of
9 ucocor1lcold receptor
0 Cortisol
: \ "{
\ e ~ HSP90
Pol II
:
~-4-------~) CoA
NA NA
Transcription
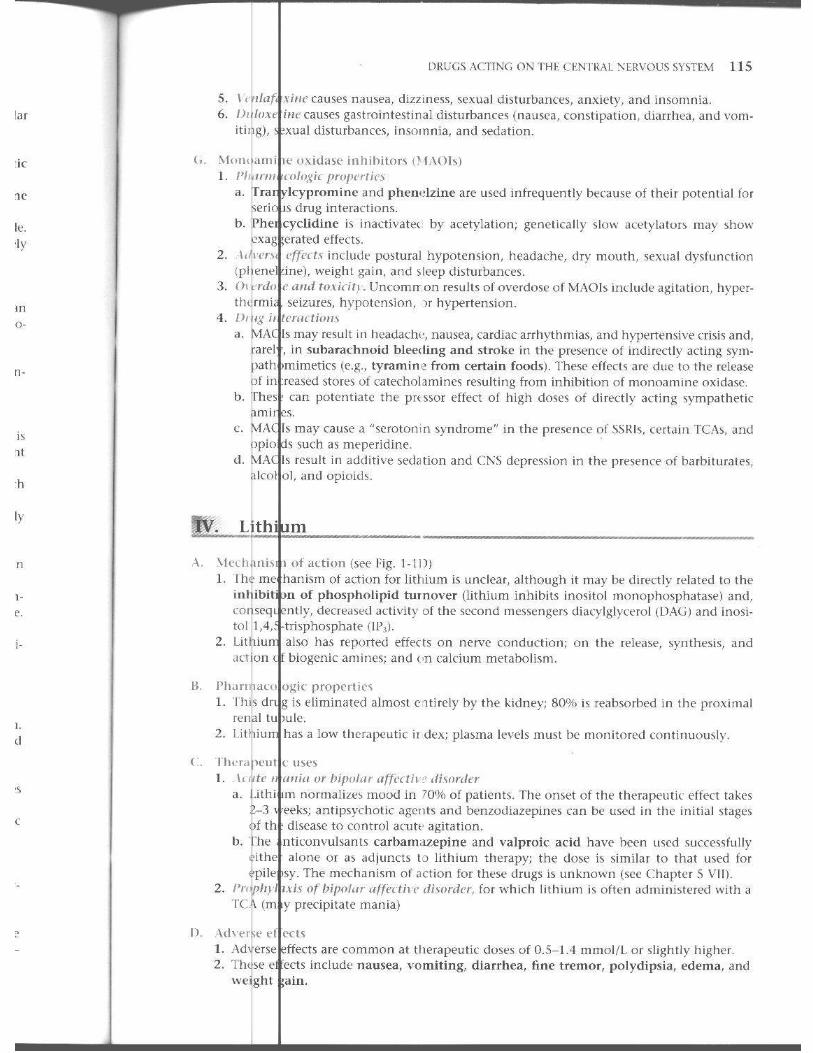
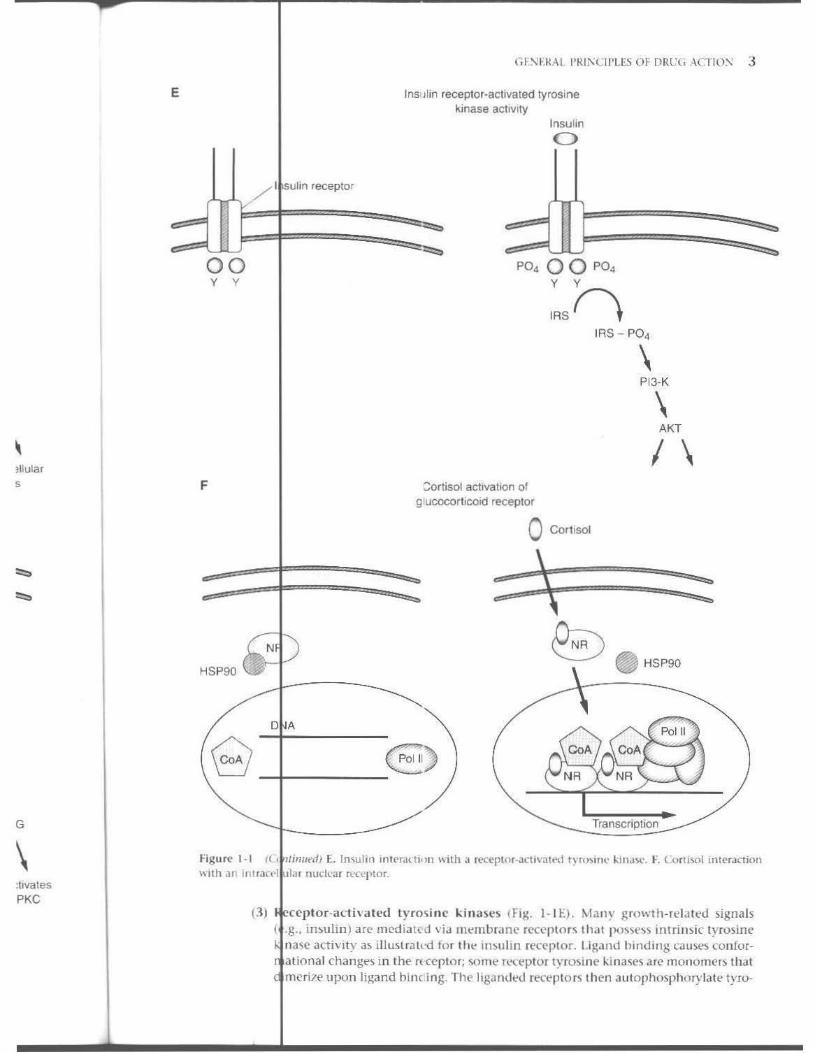
figure 1· 1 t(, "imlt'n) E. In\u lin inlf'ral"ti. )11 w ith a f('ceplor-3cli\a1t~1 trn»iUl' l in,IS('. F. COIIJ'101 interact ion "ith an In\ .3r.'1 la r nudear R'O"pLor_
(3) ccptor-acthated tyrm inc l;:inaSel> (Fig. I- IE). Many growth-rt'la ted signals .g .. in~ulin ) a re med ia ted via m <;,mbr;mi..' rCCCplor\ that I )(I~~(':,>~ intri nsic tyros ine nasI" acthLty a~ iIIuslra l('d f{) r the Ifl~uhn ren·ptor. Liga nd hi nding CillN'S confor
t al ional changes in the n ccptor; '>O fH e fl-'('eptor tyrosim,' l,:inascs arc rnOllOmE'r:'> that mcrilt> upon ligand hilK ing. The liga ndl-d recepto rs then autophosphorylatt> tyro-
4 URS I'IIARM',I('LO~Y
(4)
sine "~Id"", which recruits cytoplasmiC proteim to the plasma membrane where aho tyrosine phosphor.dated and aClh'aled .
'n''''''t'",,, nudear receptor.; (Fig. l - lF). Ugand~ (e.g .. corliwl) fo r nuclear receplipophilic and can diffuse rapidly IhrouRh the plasma membrane. In Ihe of ligand. nuclear receptors are inaClh'e bccau\(' o f their inleranion ,,-Uh
proteins such as h eal -shock pro teins like IISP-90. Binding of ligand prochanges in the receptor thai facili la te d i ~wciat ion of chaperones.
receptors in lo the nuclt-us, hetcfo- or homodilllt'li l Jtion of receptor" .• md
~~~:~:'~:~::: interaction with tl e lJ:'\IA of tarRet genes. I>NA-bou nd nuclear rt"(:epla rs to recruit a d iverse numix' r of prOteins called coacti\'a lors. wh ich suh-
act to increa'>C t ramcripUon of the target gene. 2. \lft'1<I1 i"" III <It I il'i/I "/ ! 1//1/1/," t y activation or inhibition of 111(' ell l-rllle 's catalytic
activity 3. III/illll'/.,/mii ! in which the dnlg. acting a~ a nonfunctiona l analo),:ue of a naturally
interferes with m 'rmal metabolism 4. \"II'lh', iii" 'I I or pIli ,;uil ;111,'. ,I< ti u //\ such a~ those caused by antacids. osmotic
agents. and
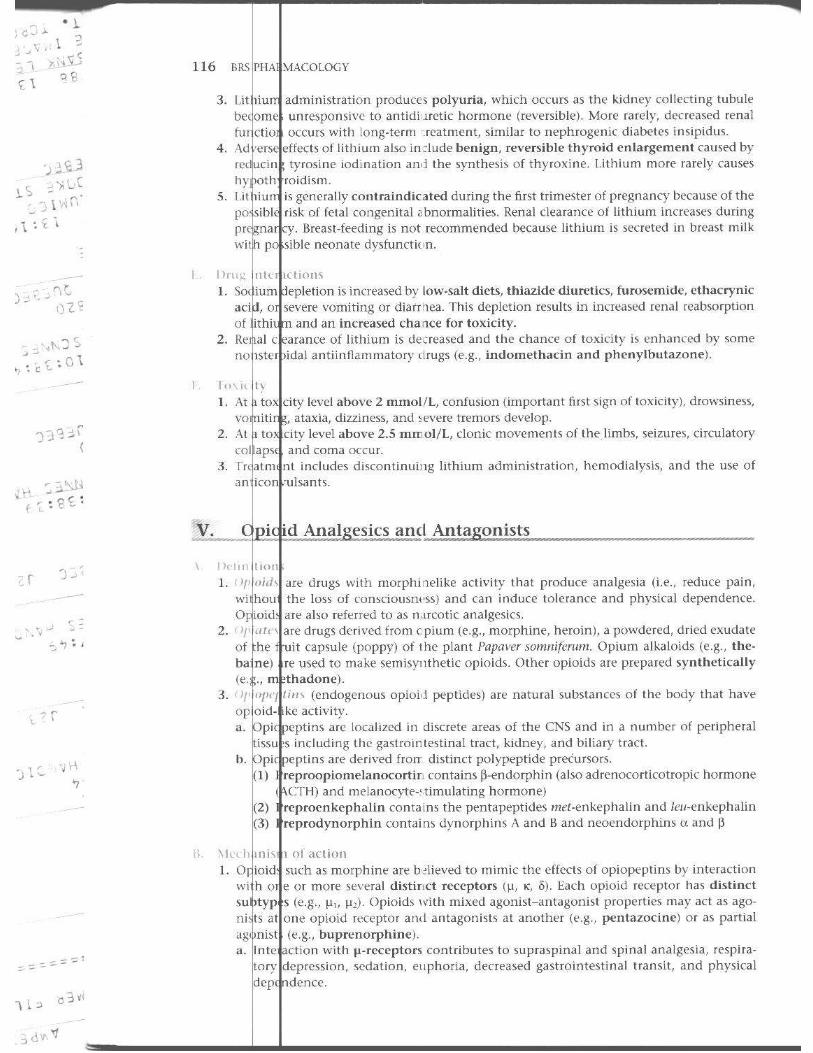
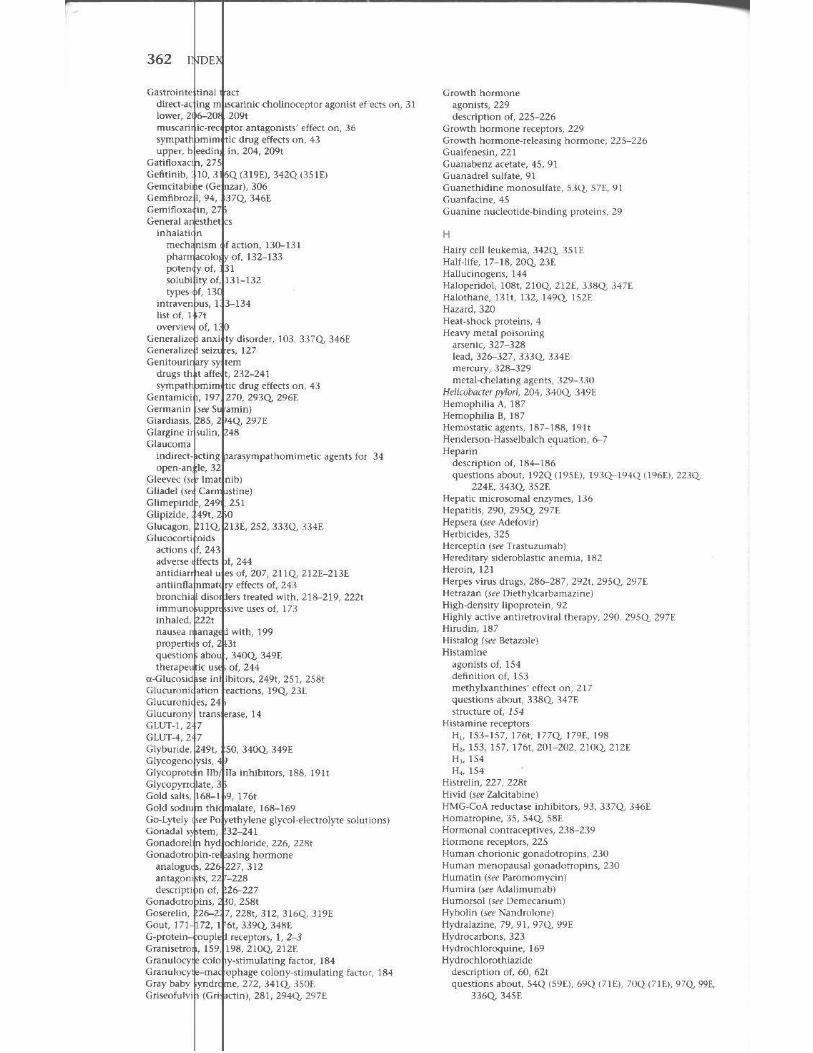
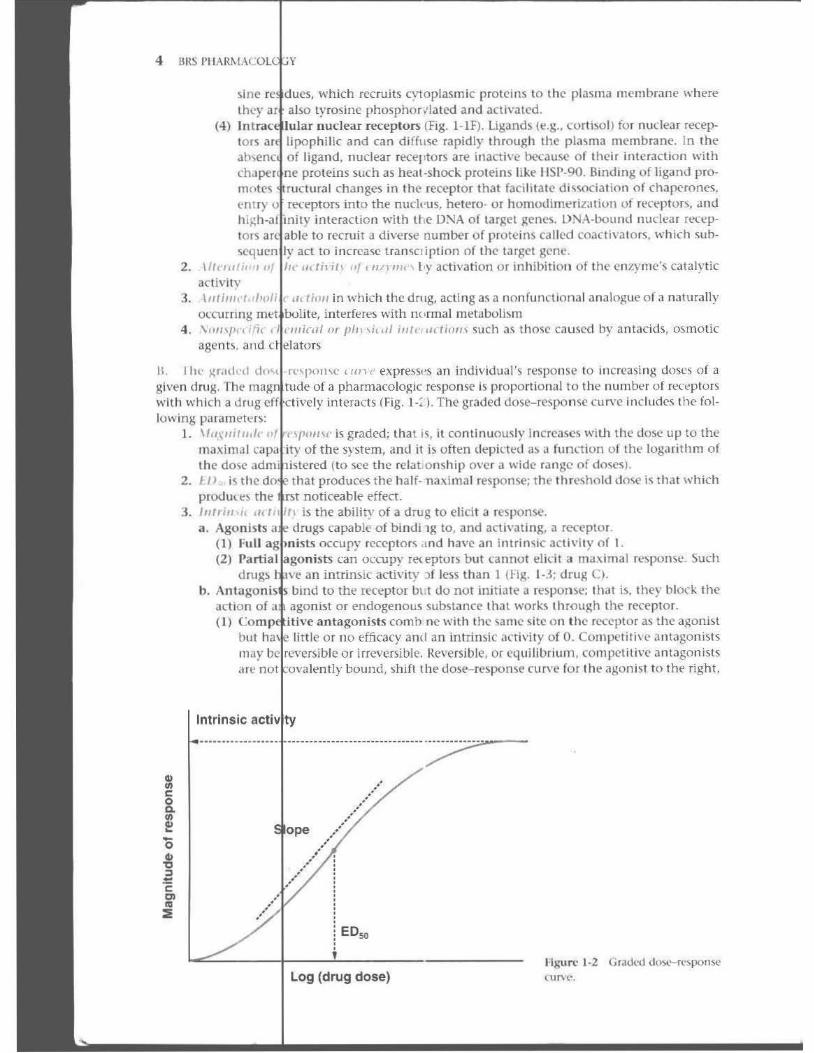
II. II\(' ,l(r.Hkd rt"I)(1!l\e ,1111 " e,'press,·s al1 individual 's response to increasing doses of a
given dHl,g, Tl""'n::;;;~~~;:~:~O:f a pharmacologic response is proportlon"l to the number of lereptors "'Ith which a d I interacts (Fig. 1 -~ 1. The graded dose-re~ponse curve Includes the following paramel<;,r~:
1. \I(/'''l/ifU'~'~. iiir:i;;;!':~~', is graded; that is, it continuOll~ly lncrea~e' willl the dose lip to the maximal of the system. ami it is often lIt'pirtt'd a~ a func-l ion of Ihe logMithrn of the dose (to see the relat on~hip O \ '{'T a " 'ide range of doses ).
2. II) is the that produces the half-lla.\;. imal response; the thrt'Shold doS<' is that wh ich
:1. noticeable effect .
I lltrill,i, ' /1 is the ability of a drug to e lici t a response. a .
b,
Agonists (I) Full (2)
drugs
cap.lble o f bindi 19 to, and activating, a receptor. OCCUP}' receptoT<; ,md have an intrin~ic activity of I .
can ou;upy rl'lt'ptors but (annot elidt a ma.\ima l r~ponse_ Such I an intrinsic activitY ::lf less than 1 (Fig. l -.{; drug C).
",",g' <ni ' i' bind to the receptor Ul t do not in itiate a response; Ih.lt is. they block the agonist or endogenous substance that works through the receplor.
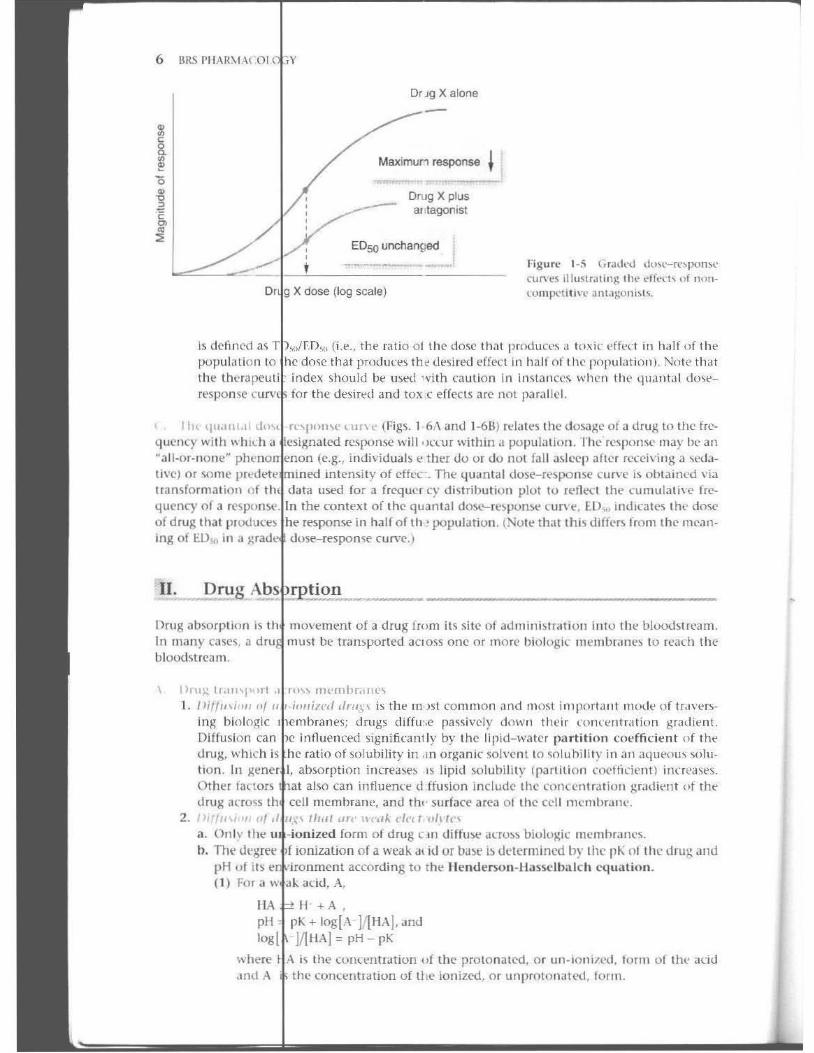
e"m,,,,tiliY' antagonists comb ne " 'ith the same site on the t('<eptor as the a),:onist little or 110 efficacy and an intrinsit' activity of O. COrllpcliti\(' antagonists
>n"vb, iccYC"iblcor irreversible. Reversible, or equilibrium. competitive antagonists "'" no' f·"y"''''''y "OIm".,hift the dose- respome cucve for the agonist to the cight.
Intrinsic ac,;vt'y
EO~
log (drug dose) rigun:' 1-2 GrJ,kd d()~-"-r(·wonfrl."
flUV(-" .
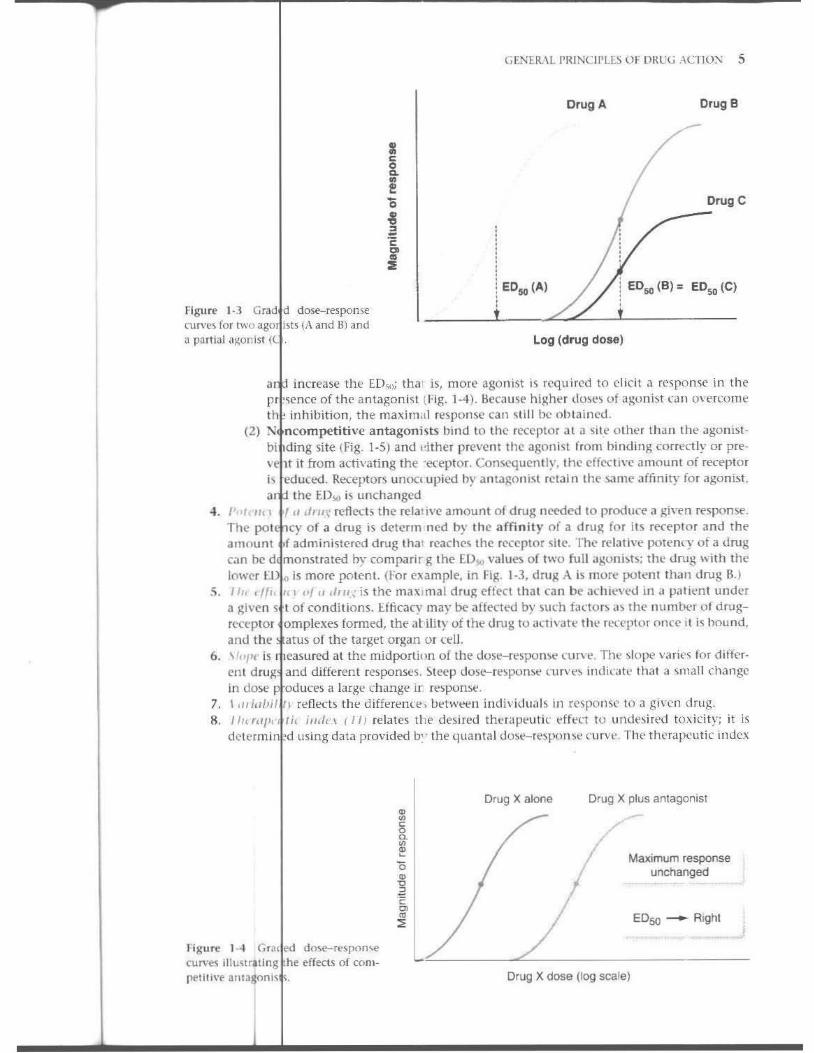
Flgun." ) ·1 Grad d do:;e.-r{"!;pome cur\'C~ for two ago! i~t~ (A and Bl and a parti~1 <l 1/;()nist ( I.
GF-NEIl\!: ('IUNCH'LES Of DRUG ACTIO); 5
Drug A Drug B
DrogC
ED50 (A) EDso (B) = EDso (C)
log (drug dose)
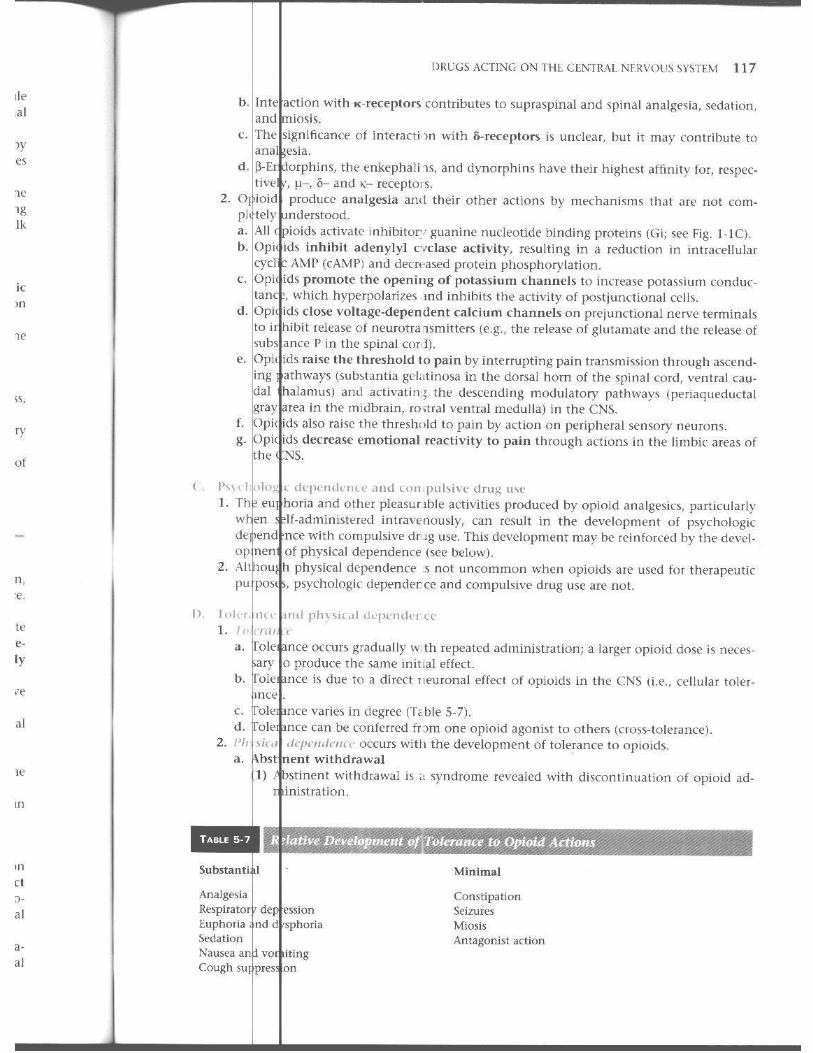
a intTease tht ED'i<'; tha is, more agonist is required to dicit a r('<;pollSe in the pr ',ence of the antagonist (I'ig. 1-4). Hccaust hightr do~t') of agonist ,all overcome til ! inhibition , th e maxim,!! response can 'i tilll~ ob tai nl'd .
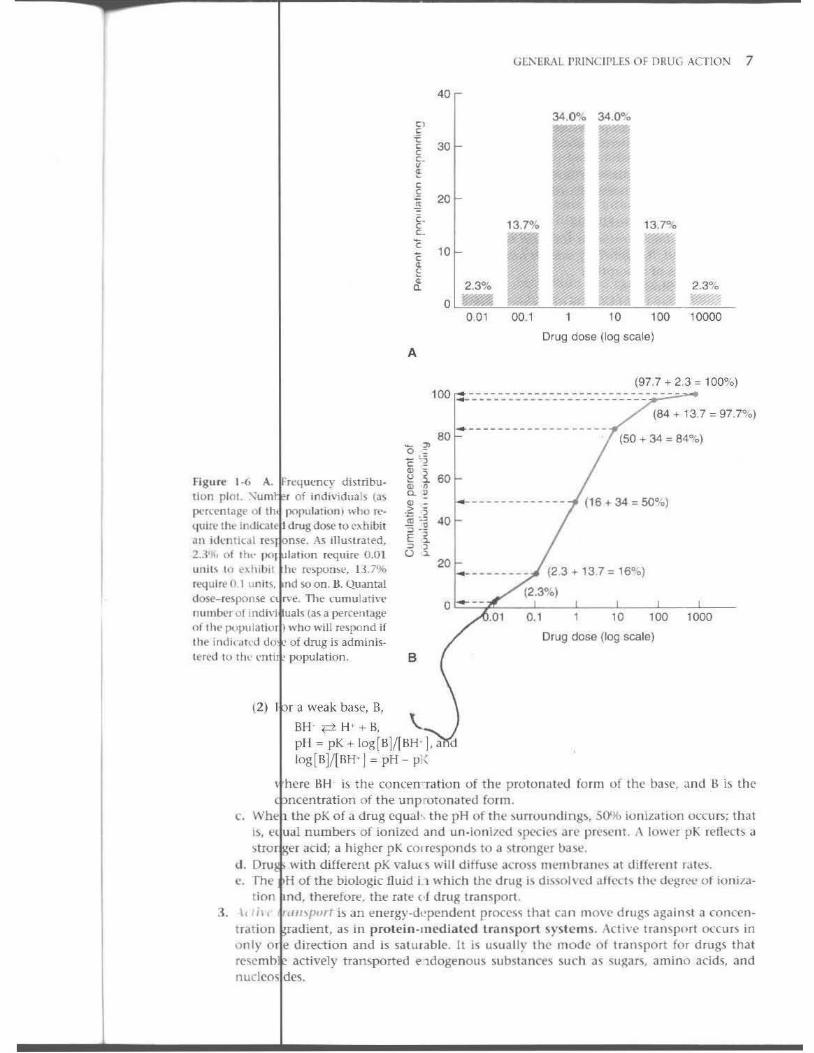
(2) N ncompetitive antagonists bind to the rccl'ptor a t a si te o ther than the agonistbi ding site (Fig. 1-5) and Pi ther preven t the agoni~t from binding correctly or pre\ 1t it from activating the '('(eptor. Con<.<'quen tly, the effcct i\'(' amou nt of receptor is educed. Receptors unocl upied hy antagon i~ t retain the same affmity for agonist , a the ED,',(J is unchanged
4 . ",,/, /III I" .11'11,\ reflects the re lative amount of drug nceded 10 produce a gil'en response. The pol cy of a d rug is determ ned by the affinity of a drug for its recepto r and the amount .f admin istered drug thaI reach('~ the r('Ceptar si te. The re lath'e potenry of a drug can be d monstrated by comparir g the f.D'io) values of two fuJI agonbt); lhe dnlg \\ ith the lower E is mo re potent. (for exampl(', in Fig. 1-3. drug A is more potellllhall drug H. )
S. , I" 1'f/1. ,., <If ,/ ,/111.,: is the maXIma l d ru)! eff('cI tha t can be achl('\'N.1 in a p.llit'n t under a given s t of conditions. I:.fti.cacy may be .lffec\('(\ by stlt"h fano r) ,I~ tilE' num ber o f d rugf('Ceptor omplexes formed, the at ility o f the d rug 10 , , ~ 11\ "fe the receptor OIlC(' \t is hound. and the . atus of the target organ or reil.
6. \ '''I't' is t easured at the mid portion of the dose- rtspumt' run·t. TIll' ~k)l)(' varifs for different drug. and different responses. Steep dose-re~pon~ l'urvt"~ inliil',!\(' that a ~mal1 change in dose p oduces a large change ir respon~t .
7. I ,,,ia/li/', refled.s the differenre , bttwetn illdividual s in r('spOrlSC to a given drug. R. III( '''1.'' Ih illdt·\ (1/) relates the desired thtrapt uti c tfftr t \(J ulldl'~iTed toxicity; it is
dctl'rmin 'd using data provided b" the quantal dO~i.'--Tt'sponw cur\'\'. The therapeutic index
1 (gurl' 1_4 GrJ{ ed do\e- respoo\e ('UI'\'es iIIustrltlng he effeCl~ of COlll[It'tl l l\'p aIllJ$oni\
Drug X alone Drug X plus antagonist
MaJ;;mum response unchanged
ED50 - Rtg hl
Drug X dose (log scale)
6 BRS 1'11"","0"'1'''
Is dcflllcd a, )X!pullltion 10
th~
respome '
Dr J9 X alone
MaximuM response ~
DOJ9 X plus al tagonlst
ED5Q unchanged
X dose (log scale)
FigUT{· 1-5 (.I~(kd dU~<'-n:~J-lOm<'
curyt's Ulu~lralitlg 111,' "ff, .. __ I,,,f "0"lOl11].X'ti tin ' antag:oni,I,.
the ratio o[ th" cto~" that pmduce, ,\ tU'I;ir l'ffl'ct in h,llf uf tile Illal produn'~ the desired effect in hall of I he population). Nu\(' that
i index should be u~t'd ' vith caution In in~ tan cc\ wilen tile qH,mtd l du'>t'tor the desirt'd and tox ( effects arc not )laralll'l.
I h< qU,IILI,LI [ rl'\jloLL \(' < Ul\ e (Figs. I 6'\ and J-6BJ rda les Ihe dosage of J drug to the fre-
quency with \\~":U~';h~~'~' ~ri:;~:~:;;~ response will 'Jl"(ur within" population. rhe re~pome may he an ~all -or· nont''' (e.g., i ndividual~ t' tht'f do Of do not fall askep after h'1,:ei\' ing a \£'<1.1-live) or \Ome in tensity of cffl'c . Tht;' quanta I dose- rt'sponse OHve is ohta ined via tramformalioll o f tlata used for a frcq uel c}' d i ~t rihuti(Jn plot 10 rt;'flt'{' t the cumulat i\(' Ire-quency of a tht' conted of Ihe quan tal doS<'- re'> pOflM> wn't', ED", indicates Ih ... dose of drug that p l ()(I U(:e~ response in haH of til > populatio ll . (Nolt' that th is differs from the mean-ing 01 EO", in a ' curve.)
II. ~g
Omg absorpt ioo is In many cases, a bloodstream .
1ll0vemt'nt of a drug from it, Sit" of admillhlratiOIl illlo the blOO(htream. must be t ran~ported aclO,S one or morC' bioklgi( nH'lI1brilne~ to rearh the
\ 1)l'u).:, tl',Ill'I'.,rl 1. /lit/lllj,,,, of
illl<; bio logic Diffusion ca n
1'0" ml'mhr,llll''i " I " drll.\'\ is tht' lTI)st (ommon and most important 1110d ... o f tfdvt'rs-1 drugs diffu',e paSSively down Ilwir cOlKl'ntra tion grMlient. influenced ~ignifirant l y by the lipid- wn ter partition cOl'ffident of the ratio of solubility in ,m organic soh'ent to ~olu hi lily ill JI1 ,1<l\leO\lS soll!
,en"'I'. ab<,orption incn2a,>t''> LS lipid solubility (pMtilion (tw!tiril' nt) innl'a,es. also can intlut'nt't' d ffu sion include the fOl1lelll ration gradit'!lt of the
dnll<; acro~s cell memilralll', and thl ' su rface area 0 1 the cell r)1el11br'HW . 2. I)il/ll,j·,,, Of tlr.1I "rt' lI("a l.. de,t (lh tn
a. On ly Ihe :~~r:~:~::~~fn7:rm of drug c II I diffU M> "(fOSS biologic Il)('mhralles. h, The dtgree of a weak dl id or bilse b determ ined hy Ihe pK nl Ill(" tim); all(l
pH of liS according to tht' lI t'ntierson -lI i1ssc lbalch equation, <I) . adtl, A,
H +A ,
pK + log(A- ]I(HA ]. and ]I1I1A] = pH - pK
i~ the cOllct'ntlation \I f the prolonatcd, or un·ioni /('d. form of till' ,Kid "the concentration of li re ionized, or unproto nated. form.
" ,
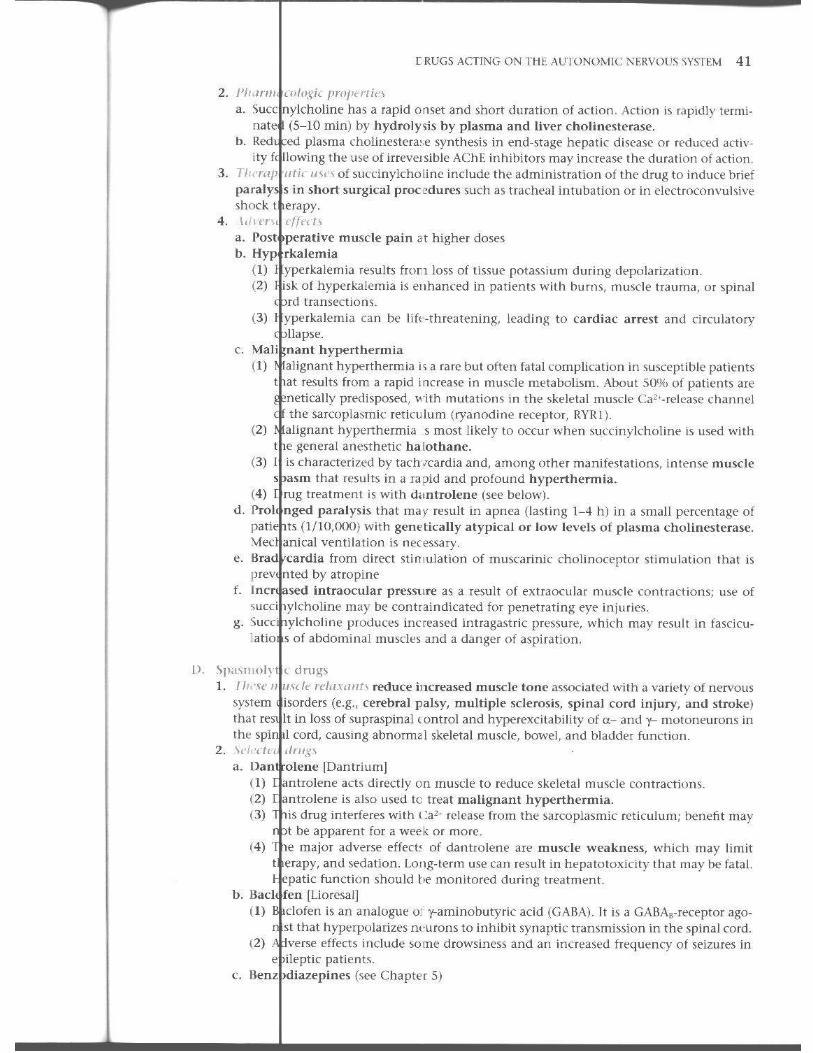
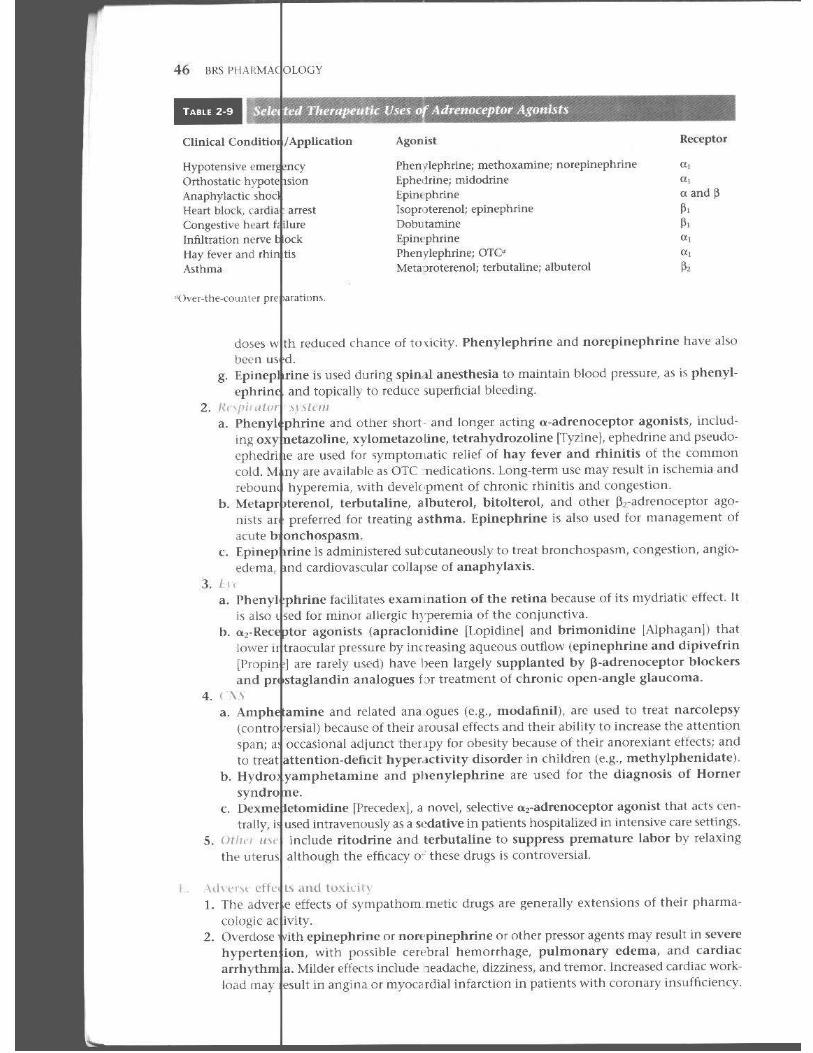
40
< , 30
! , 20
10
0
A
2.3% -001
Gt:KERAL I'RINClI'I.L~ OF I"lRU(, ACTION 7
13.7"{, i 13.7"1. -~ 2.3% ..... -,~, ~
00.1 10 100 10000
Drug dose (log scale)
(97.7 + 2.3 '" 100%) 100 _ -_-_-_-_-_-_-_-_-_-_-_-_-_-_-_-_-_-_-_-_-_-_-_-_- - - --
(84 + 13.7 '" 97.7~,,) --- -- -- -- -- -- -- -- ---
Figur~ I ·{, A. ·ft'4u .... m-y di~tribu
lion plot. ""um >r of individuals (a~ IX'rccllIagl' 0 1 Ih populat ion) who n"
\.jilin' lilt' InlllcalE I drug dose 10 c~ hl!.>it
all 1lli:lI1 i(JI ' l"~1 nsi'. As iIlmlfaled. 2 .. 1% of II .. , P"I ,Iilhon ' <'quirl' 0.01 "nil~ 10 .'"hi!.>i l Ill" n."~pomc, 1J.7% 't'(julrt> 0 1 li nit ~. nd so on. H. Quanta! dost"-r~Jlon~ Cl .\t'. TI'e tumulatin' !lltm ...... r of indhi uals (as a percenugl' of lIlt' pl.!pu[atiut ) who will rt'slxmd if thi' i!ll\",II<'u do . of dmg is adminis· tered w tlw cnti 'population.
(2) I r a weak base, B,
B"' ~H ' +B,
80
20
B
pI! = pK + log [BlI[BH ' ], a (1
log [Bl/[BH-l = pH - p)(
(SO + 34 '" 84%)
(16 + 34 '" SO"o)
_________ (23+137=1600)
(2.3"0)
.01 0.1 10 100 1000
Orug dose (log scale)
\ here HH is tilt' COTKl'n -ratiun of the protollatt'd form of the base, and B is the ncentration of tht! unp rotonatt'd form .
e Whe 1 the pK of a drug cquah the pH of th(> ~lIrro\lnd i ng~, 50')(' ionizat ion O(curs; that IS, l'l ual numbers of ionized and un·ioni7ed spC'Cies .:tre pn'st' ll t. A JOWl'T pK r(>fll;"{'h a ~tro 'er acid; a higher pK corresl>onds 10 a st ronSt.>r bast'.
J . Dru . with d ifferen t pK valu( s will diffuse across ml'1I1b ra lll'~ .It different hiles. C. rh(' H o f the biologic flu id i 1 wh ich the d rug i~ dl_~~ol\cd afl ('Ch t ile degree of ioniza
t ion IIld. th(' rcfort'. the ra te { f druK transport. 3. \,,' iI t fIIl/\fJj"" h an enl'rgy-dl'pcndcnt rroce~~ that ca n move drug~ again~ t a concen
t ril l ion ' radient, as in protein-mediated transport syste m s. /\cti\(' tramport (K'curs in only 0 1 e d irl'(:tion and is satutablc. It is usually the mode of tran~port for drug~ that rc~emh actively transported cldogenous substances such as sugars, ami no acids, and nuclem des.
8
It
"'" 4.
5.
" t.
2.
I i//'oI/i", ;, bulk flow of solvent and solute t tHough channel~ \j)()re\, in the membrane. with ~lIlati molenlles usua lly with a molecular " 'eight I('s~ than 100) th<lt pores. Some sumtamcs of greater molecular wdght, surh as (ert<lin pro-
filt ra tion can 1)<1» telll~, loan be through mtercetiu ar channels. Concentration gradicnh afft'i.1 the r3te of li ltra t lon. I ,I, " if",,, .. t .t" I"";"" is movement of <I ' ubstancc down a concent ration gradient_ Facilitated
medi<Itt'tI, ~pedfl\.:, a III saturable; it doc~ not requi re cn<'rgy. di ffu ~inn i~
'111\" PI ,a tlun 11/.// , is the most convenient, t'Conomk;II, .lIld common rou te of admin
I safe for most dru~. hlratlon; it is ,. Sites o f
( t ) (a)
(b)
(2)
(b)
I
and weak acids, which all: normillly un-ionized at the low to 2) of gastric cQ11IeTlts, may bt' ab)orbed directly from the stomach. bases and strong acids (PK = 2 to 3) are not normalJr absorbed from this
since they tend to be protonated at low pH.
small intt'stine is the primary site of ahsorption of most drugs bl'cause of th'~'''y l<lrge surface area a':ross which drug~. includ ing partially ionized weill-<
and ba~t'~. may rJiffust. nonnallyabwrllt"l.! more t'xtensi\,{'ly from the small intestine than from
even though the in testine has a higher pH (approximately 5). b. The
leaches lily of a lIrug is th,> fraction of drug (admini~tcrcd by any Tout~) that
unaltert'(1 lbioavallabillty = I for intravenous admin ist rat ion). refcr~ to the condit i()11 in whk h the plasma conc{,ll tralion VS. t ime pro
formulations ale it entkaL files of effect influenct'5 (h ug i1bsorption metabolism in the livcr or by (I) r he
biliary pd~S
the
."fter ahsorpt ion from Iht' :.tomar or small inlesti ne, a dru~ must the Ii"er before rNching the gell~rdl irt.ulat ion ;md its target site. If
of liver metabolic enzymes to inac t lv;i tht' drug i:. great, only limited . of active druK will escolpe the process. $om drugs ar .. metabolized so exten
,;,,",, ' , f<"SUIt of hepatic met.li-olism during the Ii ·t p..l) th,1I it j)H'('lud<"S thdr use. that may <lltef abs'Jrption from the ~to cll or small intestine illclude (2)
th e (,)
(b)
emptying time and Jassage of drug to thc in stine may be intluenced h~' ~",,·; ,eontent s and intes tinal motility . 'r wd emptying t im\:' gen-
decreases till;' rate of a11sorptlon because the intcstine is the major ahsorpfor rno~t orally adII ini5tert'd druH~.
";'l;:~:~::~~;:;.' (GI) blood flow plays an important role in lirug absorption b I ' Tliaintainin~ the concentration gradicnt across epithelial rTlCrTl-
b'" ~". "rhe absorption o f SIThlll, very lipid soluble molecules is "blood !low Ii Illwhereas high Iy polar Illolenllt') ,Ht' "blood flow independent."
(el !~:t~::::.~~~'~C:id and inactivati ng enlymes may destroy certain drugs. Enteric coatbrea\.;dowll of t Iblets by the acid p! I of the stomach.
(d ) with tood, ottl( T drugs, and other constit uents of the gastric milieu
«) influence absorption.
in oral preparat ions or t h~ spt'i.· i'll formut;lIion of those prepamay alter abwrptioll .
,. includes th ft"(' major rou l e~: intr(wcnous ( IV), intramuscular (1M), and (SC). Parenl<'ral administration generally r("iiu lt ~ in more pre· dic table ' than oral administ ration . a. Wit h IV , the drug is Inj<'Cted d irectly into th t: blOQ(btrea m (lOO'tJ bio-
available). represenh tbe most rapid means of IIl t roducing drugs in to the body and
';·"d :::;';,:::',~l'~n,usefu l in the treatllltnt of emerlo:encies when absolute control at dTug a' Is essential.
GENERAL I'RINCIPLES OF DRUG ACTION 9
b. !loftt 1M and SC admin istration, many drugs can enter thc capilla rics directly through ~por s" between endothelial cdls. Dt.<pot preparations fo r ~ustained release may be admin· ister by 1M or SC routes, b~ t SOUle preparations may cause ir ritat ion il lld pain.
3. Orill" I Itltt'~ "t /I,lmlllj\lruri oll a. lnh alio n results in ral}id ahsorption hecau~c of the large surface area and rich blOlXl
~up y of the alveoli. Inh alat ion is frequently used for gaseous ancsthetics, bu t it is gen· crall' no t practical. In hala tion may be useful fo r drugs that ac t on the airways, such as epin phrine and glucocort icc ids, which a re used to t rea t bronchial ast h ma.
b. Subl ngual administration i~ uscful for drugs \\·ith hi gh fi rst-pass Illetaholism , ~uch as n' roglycerin, sim.:e hepat ,c metabolism is bypassed.
c. Int r thecal admin istration i, useful for drugs that do n ot rtadily (ross tht' blood- brain barn r.
d . Reet I administration minimizes first-pilSS metabolislll ,llId !IIay bI; used to circum· vent the n ausea and vomilmg that sometimes result from oral administration. Use of rect admin istration may be limited by il1("Oliveniel1("t:' or patient noncompliance.
e. Top' al administration is u ',ed widely when a local effect is desired or 10 minimize sys! mic effects, espcria ll y ill dermatology .Hld ophtha lmu logy. Preparations rnu~t be noni riuting. Note th at drug' administered toplc,llly may sometimes produce systemic effec s.
'iiI. Dru Distribution
Drug disrnbuti )fl is th e movemen t of , drug from the blood~trea 1 to Ihe various tissues of the body
\. ()I \ tr ihuti 11 IIf drug~ IS the proces by which a drug leavcs I I bloodstream and enters the extracellular fl ids and ti~ues. A tlrug m ust di ffuSt! auoss cellular elllbranes if its site of act ion is in t ract'"llular. In this case, lipid solubi lity is important for effecti\ d istribut ion.
1. IIII/h'F" 1I< t' ,,/Mm,,1 0011
d. In m 'I tissul"S, d rugs can leav! the Circulatio n readily by dlffusio across or between capillaT) endothel ial cells. Thus. lhe initiail"dte of d istrib ut ' n of a rug depen ds heavily on <XXI flow to various org;ms (brain, Jj\'er, kidney> muse c, . n > fa t , bone).
b. At e uilibrium, or steady sta te, the alllOulli of drug in all organ b related to the mass of t organ and its properti~s, as well as to the properties of the specific drug.
Z. I "II/III. <II dhl ,UIII! iVII ( I .,) is tl e volume of to ta l body flu id into which a drug "appears" to distri ute. Volume of distribu1ion is determined by adrniniS1l'ring a known dose of drug (cxpres >d in uni ts of mass) iTltwvl;'nously and measUring tlw initial plasma ('onrentration (I;'x prl;'~ in units of mass/volume):
V,I '= ambunt of drug administered (m/g)!inilial plasma concentration (mwL)
Volurtlt of distribution is expres ;ed in units of vo lume. In most cases, the "initial" plasma concen ration, Co, is determinec by ext rapolation fromllle elimination phase (see IV). a. Stan ard va lues of volume~ of fluid t'ompartmenu in un ave r<l)!e 70-kg adult are as fol
lows plasma'" 3 liters; extracellular tluid = 12 lih: rs; and tutallKxly water'" 41 liters. b. Fea res of volume of distrib...ltion:
(1) "values for most drugs do not reprc~cn t their actual distribution in bodily flui Is. The use of V" values i~ prima rily conceptual; th;1\ is. dru/(s that distribute exten
vcly have relatively l arg ~ Vd values and viCe \'tr~. (2) j very low Vd \'a lue may indicatc extensive plasma protci n bindi ng oi the drug. A
\'ry h igh value may indi ;a te that the drug is ~x\(:nsi\'ely bou nd to l is~ue sit~.
(3) I mong o ther variables, \'~ rna)' be inOuenced by age, sex, weig ht, and disease I rocesses (e.g. , edema, a,ci tes).
3. IhllS It li~trilllltiOlI describes when thc rciati\·c d i~t rihu l ion of a drug in the hod}' changes with til Ie. This is usually seen with highly Jipophilk drug~ )tl("h a~ th iopental that initially elter tissues with h igh bl(oo flow (e .g., the brain) and then quickly redistribute to tis~ues jth lower blood flow (e.g., skeletalmusde and ildipoSl' th)ue).
4. 1I,/nit-" I ..
a. d i \ I rilml itm
(1 ) poorly
(2)
(3) Th£' b. Placental
( I ) with a ,
nature of the blood-brain barrie r, ioni7cd o r polar drug5 distribute including certlin chemotherapeutic ag\:' nt~ and toxil·l·ompounds,
must pass through, rather than hctw('('n, ('ndot ileliai cells. such as that resulling from meningitis, Illay iI1CIt'ast' tht' ability of solubl t' drugs to ,:ross th(' blood-bra in barrier.
barrit'r may no t b(' full y d('\·elopcd at the time of hirth .
drugs cross the pi, lcental oorrier more e,tsily tha n pola r drugs; drugs less ttan 600 pass the placental barrier hettcr than largt'[
(2) Thl' that drugs adm inistered to thl' mother may cross the placenta and reach fetus is always an important consideration in therapy.
(3) Drug '''in' PC""'" (e.g., the P-glycoprotein transporter) transfer dru~s out of the fetus.
1\ lIiudin;.: III \Irug\ pla~llIa pr"h'i m . Drugs in the plasma may exi~t in tl1(' free forlll or may be bound to plasma plo",'oo>OT otht'r blood components, such as red blood ("' Is.
t. ("·/1..,,,1/, ,/fill \ of /I/IIIII"'I"otri" 11I'.lii".~ a. plasma protein binding is highly variable and range~ fror virtually (jJt, to
mort: than bound, depending Oil the spedfic drug. IHnding i.~ gener lIy rewrsible. b. O nly the drug diffuses through \:apillary walls; ('xtemlve hinding tards the ratt'
at which drug reaches its site of .Ktion and may prolong durat ion 0 etion.
c . Some:'~::':;l proteins hind many di fferent drugs, whilt· o thcr proteins hin Iyone or a I number. 1;01 example, ·.erum albumin tends 10 b ind many acidic ugs, while g lycoprotein tends to lind many ba:.il" drugs.
d. There are if any, documented ehangl's in a drug's effect du(' to chang('s n I sma
pro tein bl'"'I'n".
\. \lnh,lrlL\rrl\ of 'dimin.Llion .lnd tl'rminalion pi O"llti(\ll 1. In most cases,
Inactive (or
other rouIC~ .
action of a drug is tC 'minatcd by enzym e-catalyzt'd conversion to an artive) compound and/or elimination from the body via the kidney or
2. drugs from the sitt' of a :tion may term inate the action of a drug, although
't~:::~l!,:;,:F~;O::',,~":,'~. mple, the action of the anestlle tic thiopental is termi)1 from Ihe hrain (where it initially accumulates as a result
solubility and the high blood now to that organ) to tilt' morl' poorly per-
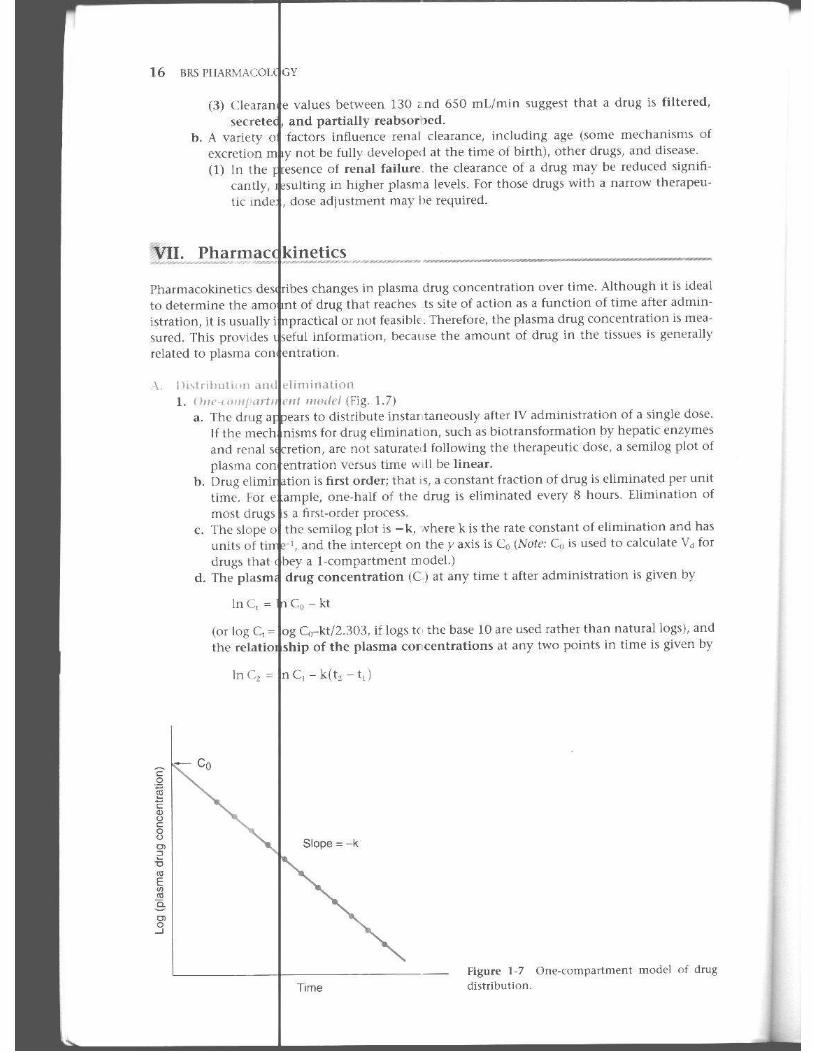
B 1{.Ih plllnr~ tWill t he IJodl I . F ir"·of./, I , .• . The eliminatior of most drugs at therapeutic doses I~ ~ firs t-order";
dcpend~ un the eonet'ntration of drug in the plasma. and is of th~ drug multiplied by a proportionality cOIutant:
from body (maSS/Time) = Constant x Dmgl " .. "" (mass/vol)
Because the eliminatio n is given in unit!> of m a!>!>{lime and concentration is in units of th t' units of the consta 'l t arc volume/time. Th is constant Is referred to as the IV C).
2. //"1" "1"./,., '"ull'l< ·,. Infrequent ly, the ra te of e limination of a drug is ;'zero-order. " In this case, thie' by which the body e liminates the drug (e.g., metabolism by hepatic enzymes, secretion in the kidne» is saturated. The rate of drug e limination from the body is constant and does not depend on plasma con centration .
L I:I'[R,\L PRINCI PI ~<; U I UlI. lX; \CTIO~ 11
( It .n UH.t {( I ). Conceptually, clearance is a measure o f the cap<l~~ity of the bod}' to remon ' a drug. ).Iathcm tkally, clearance h the poportionality constant that rd ;H~ the rate of drug elimi· nation 10 the )Iasma concentration of the drug. Thus, drugs with ~high " clearance are rapidly removed trom he body, and drugs with "low" clearance are removro Slowly. As noted in IV R, the units of clearal (e arc volume/time.
I. \/ ', , if I( o rXlll1 dew,III<.· is the c,lpaclty of an individual organ TO {'lil11in;lte a drug. SpeCific organ c ea rance may be dut to metaholism (e.g., "htpatic clearantC" by the liver) or exerelion (e . . , "rtnai clearance" by tlimination in the urine).
Rat( of elimination by organ " CL.""", x Drugpl.i..,.. pnf ..... ,,"'5'''
Cl ..... .. , :0 Rate of elimination t ~' ocganjDrug l ..... , .. I_""" ... n <p>
2. I I I, .. ,. "til ( , ... m"". is the cap.lcity of the body to eliminate tht' tlnlg by all rncchanbTII~. r hl.!H:f e, whole hody clearanct is equal to the sum of all of Ihe ~pt.'Cilic organ clearanl'e !I1l'chal bms by which the "Cliv( drug is eliminated from the body:
CL", ol< 1..,Jy '"' CL",g.>n I + CI , .. ,.,." + . , + CLo ,~n'
rh e ter 1 "dearancc" genera!ly J efer~ to whole body clearance UT!
in this a~e,
Rate f elimination from !xxI) .. CLwholttw, x Orug['lo"'"
and
CI. 0 Ra te o f elimination from bodyjDrug~
1. 1'/" IIII tl I" ,Iltmtl' h numericall~ the ~me as whole hody de .. r;ulcc, but thi~ I minology 1<' ~omt:' imes used Ix'Gtuse clearance may be viewed as the \'olu1ll t:' of pl' ('011 1 .. im thl' am( unt of drug removed pe ' unit time (re<:al! thaI the unih o f clearance are volurnt / lime) . I not specified, this term refer~ to the volum e of plasma "cleared" 01 drug by al! l)(x li Iy I lechanisms (Lt:'., whole hody cle,Hanct:'j , Thc term may ,11~o be appl ied to clt:'aranct by ~pcc C organs; for examplt, renal plasma dtarance is the volunw of plasma containl n~ the ITIlOunt of drug elimina1ed In the urine per unit time.
Biot nsformation etabolismLof Drugs_
-\. (,c11u,11 pi lpl' rlic<;
I. Biotran ormation is a major mechan i ~T11 for tJrug elimination; 1II0 ~1 drugs undergo biotransfor nation, or meta holism, " fter they cnter the body. Biolramfor1l1ation, which almo~t a lway~ oducts metabolites that Ire more polar thiln the parent drug, usually tt:'rmi nalcs I h(' pharma ologit' action of the part nt drug and. vi~ txcretion, incrt.'asc~ r('moval of the dnlg fro m til body. Howcvcr, Other {tmSCCjllcnces arE' possible. notably afit'r phase i reactiom, ind udi simililr or different pharmil('oiogic activity, or toxicologic activity.
2. Many d llg~ undergo severa l sequential biotransformation reacliom. Bio transformation is catal} .ed by specific en1.yrno! systems, which may also catal },1e Ihe lllt:'tabolislll of t'ndogel ous substances such as slt:'roid hormones.
:I. Th\, Ii\' ( is the major site o f hi )transformation, although ~pecifjc dru.l!~ may undergo blOt ran . ormation primarily or 2xtensivt'ly in other ti~sul's.
4. lhomlll 'ormation of drugs is viuiablt: and can be afferted by T11ilny pararnct ('r~. il1cluding pri or a( ministration of the drug in qut:'stion o r of ot her drugs; diet; hormonal status; ~(!nctic . : disease (e.g., decreased in cardiac and pulmonary dis~·'I~t,) ; age and devl'lop· 1l1t:lltal ·tatus (thc very t'lderly ,lnd V('fy young may he m ore Sl'llsitive to drugs, in part. hccause of decreascd or undcnloped I('wb of drug-mctabulilill/ol enzymes); and liver fun ctio (i n ca~es of ~evtre liver damagt, dosage adjustmertts mily be requirro for dru/ols l'Iimindt ~ largely via this route)
5. l'o~s ibl l;' onsequenccs of biotransformation indude the production of inaclh'c metaholites (n1l st common ), metabolite, with increa'>t:'U or decrea<,ed pOtendt's, llletaboJite~ with
12 ,"S 1'1I.',RM" ec' l o<iY
"
qUalitall\""';:'~Yjt::~: cent pharmacologic;: cUons, toxic mctaboli t e~, or active metaholites from inactive p
6. Metabolites olten more polar than the parent cOnl pound~ . Thi~ increased polarity may lead to a ' rapid ra te o f clearance X'cause of possible ~rct ion by acid or base carriers in the '"'n,,,1 it may also lead 10 deCieased tubu lar reabsorption.
1<I\~ ,ju .It._ III hio t r.lIlslurm atio n na( lion~
I. /,/,,'\, I tio ,',',J< tilm , joval\"{' enzyme-cata lyzed biotra nsformation o f the drug any conjugation s. rha~e I real'lions indmh.' oxi dat ions, reductions, and hydro l )'~ i s they frequen tly introduce a fum.1iona l KrouP (e.g .. -011 ) that sel"es 3!. the at live for sequential conjugation in a phase II reaction.
2. 1'/1,1\, 1/' ,\ ,,,1,,,,,,. j nm t i(ll/\ include conjugatio n react ions, v\'hich involn' the enzymt'-catalyn' d of a dmg (or drug mt'taboHtc) with an t'TldogeTlous sub<;tance. Phase 11 require a functiona l group-an active center-as tht' si tt' of conjugation with th\' sub,lanct'. Pha~c 11 readiom require t'nt'rgy indirectly for tht' ~yn-thesis of carriers," the form of the endogenous substam·c u~el1 in the con juga-tion reaction UDP-glucuronate).
( I lll\rnn ",,,,I,,,,,, phaR I hi (l lrd n~Jo rrn a li\Hl fI:,H li , ' n, Include cytochrome 1'-·1,.50,
aldt'hyde ,'m":'::I.;:~~,~jl l, dehYdrogenaSe, deaminases, esterases, amidases, and epoxlde hydratases. r.n ?ymc~ c. phase II biotransform'ltion reactio ns include glucuronyl transfera~e (gl u-curonidt' conj 5Ulfotransft'ra~ (sulfa!t' wnjugatioll), tram,Kylast's lamino acid wnjuga-t ion), a(!.'ty l 'lw~. la~es, methylases, and g utathione transferase. These enzymes are present in nUllleruu~ tb~ues; in plasma. Subcellular locat ions include cytosol, mitochondria.
I Only those enzymes loca ted In the endoplasmil· re ticu lum are inducible hy drug~
I . (.(11<11/ lilt
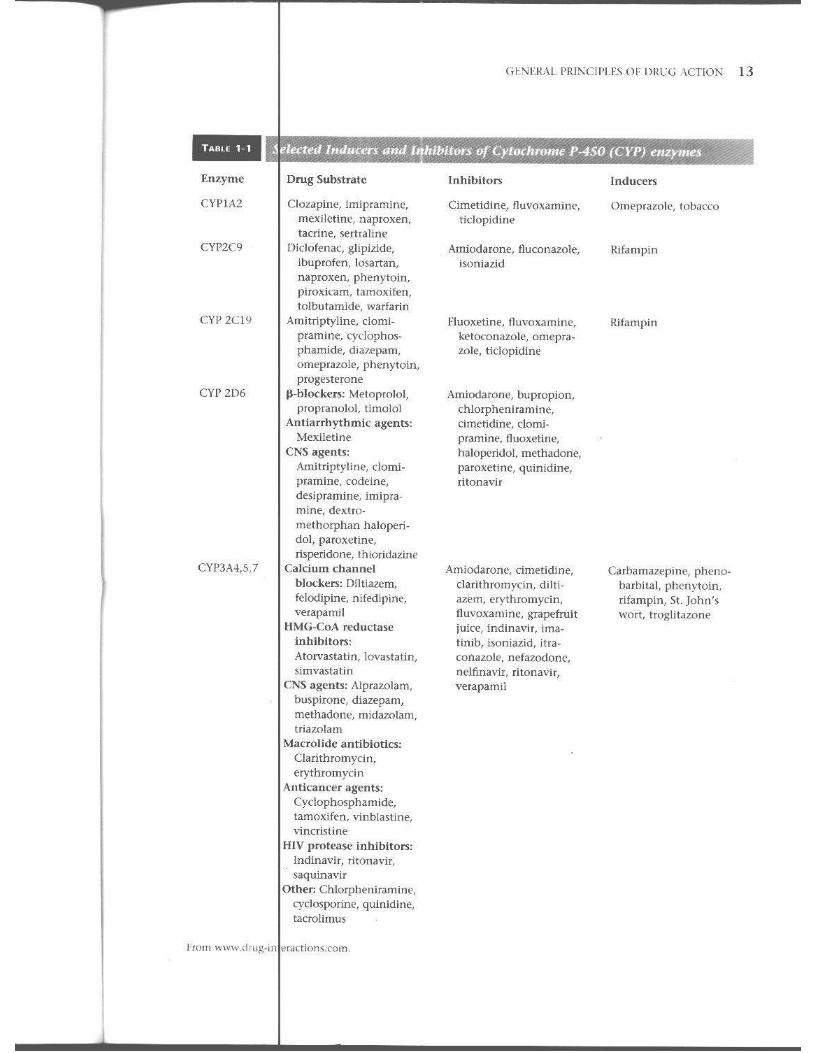
a. Gcncrdl . (Table I-I )
b.
c.
(I) P-4S0 monooxygenase plays a central rol~ in drug biotransfomlation.
12)
(3)
(4)
() )
numilcr of families tatl!a,t HI in mamma ls) of cytOChrome P· ... 50 (ahhrcn"I:VI''') en7yme'\ exists, e.ch member o f \~'hich cata lyzes the bio transforma
unique spectrum of drugs, with sonl(- overlap in the subs;t ra te specifici ties.
':::,e,1: ;,:~;~;,~y;s'tem is the one InO"t fr~quent!y ill\'olHd in pha~e J reaction s. T l'-4S0 families ar€' referred to using an arahic numeral, e.g., C¥Pl ,
C.g., Each family has a numilcr of suhfamilie~ denoted hy an upper case letter,
Cl'''''.A CYP2H, etc. The inllividual em:ynlCs within each subfamily arc denoted by (vtOll 1
,lIld '
numeral, e.g, C:YP:V, 1. CYP:iA2, ctc. , 1'-450 catalyzes Ill,merous reactions, Includ ing aromatic and aliphatiC
i ; dealkylations .Jt nitrogen, sulfur, and oxygen atoms; heteroatom at nitrogen and sulfur atoms; reductions al nitrogen atoms; and ester hydrolysis.
T'," ,d'P 'U~ubfallliJy b [espomible for up to half of the total cytcx:hrome P-4S0 in "'I' ""d :"':0,,"'" for approximately S09() of the met'lboli~Jl1 of clinically unpor
. CYP3A4 is a partin lally ilbundant enzymt>. tant
The cillc other
loca ti on of cytoclrome P-4S0 j~ th~ liver, whkh ha~ the grt'atl;~t spe· 1 i and t h.' highest to tal activity, but It is aho found in many
including the adrenals, oVarjes and teslis, and t issues invol\"ed in and ~te roid nit tabolism. The enzyme's suocellular location is the
reticulum . l.ipit membrane locat ion facilitates the metabolism of drugs.
of reaction (I) In o\"Crall reaction, the crug is OXidi7ed and oxygen is reduced to water.
equivalents are provi ded by n iCOtin amide adenine dinucleotide phosand generation of thiS cofactor is coupled to cytochrome P-450
\