Embed Size (px)
Citation preview
Br HeartY 1995;73:139-144
Heart rate variability in left ventricularhypertrophy
Mahendra K Mandawat, David R Wallbridge, Stuart D Pringle, Abdulla A S Riyami,Shahid Latif, Peter W Macfarlane, A Ross Lorimer, StuartM Cobbe
Departnent ofMedical Cardiology,Royal Infirmary,GlasgowM K MandawatD R WallbridgeS D PringleA A S RiyamiS LatifP W MacfarlaneA R LorimerS M CobbeCorrespondence to:Dr D R Walbridge,Department of MedicalCardiology, Royal Infirmary,10 Alexandra Parade,Glasgow, Scotland,G31 2ER.Accepted for publication24 August 1994
AbstractBackground-Electrocardiographic leftventricular hypertrophy and strain areassociated with increased cardiacmorbidity and mortality. Impaired car-diac autonomic function, assessed non-invasively by spontaneous heart ratevariability on Holter monitoring, is asso-ciated with an increased risk of suddendeath after myocardial infarction.Aim-To study the effect of left ventricu-lar hypertrophy on heart rate variability.Patients-36 controls and 154 patientswith left ventricular hypertrophy (94 withhypertension and 60 with aortic valvedisease).Setting-Tertiary referral centre.Methods-Heart rate variability wasmeasured on 24 h Holter recordings bynon-spectral methods. Left ventricularmass index and fractional shorteningwere measured by echocardiography.Results-Patients with left ventricularhypertrophy had a higher left ventricularmass index (P < 0.001) and reduced heartrate variability (P < 0.001) comparedwith those of the controls. A continuousinverse relation was apparent betweenheart rate variability and left ventricularmass index (r = - 0-478, P < 0.001). Heartrate variability was not affected by age,the presence of coronary artery disease inpatients with left ventricular hypertro-phy, or /1 blocker treatment for hyperten-sion. Multivariate analysis showed thatleft ventricular mass index is the mostimportant determinant ofheart rate vari-ability.Conclusion-Heart rate variability is sig-nificantly reduced in patients with leftventricular hypertrophy secondary tohypertension or aortic valve disease. Acontinuous inverse relation existsbetween heart rate variability and leftventricular mass index. Impaired cardiacautonomic function in left ventricularhypertrophy may contribute to the mech-anism of sudden death.
(Br Heart J 1995;73:139-144)
Keywords: left ventricular hypertrophy, heart ratevariability.
Electrocardiographic left ventricular hypertro-phy and strain are associated with increasedcardiovascular mortality and sudden death.
This risk is independent of the level of bloodpressure and other cardiovascular risk fac-tors,' 2 but an increased incidence of ventricu-lar arrhythmia has been reported.34Experimental and clinical evidence each sug-gests that impaired cardiac autonomic controlmay be a risk factor for sudden cardiac death.Increased sympathetic activity is associatedwith a reduced threshold for ventricular fibril-lation, and thereby potentially increases mor-tality, whilst increased parasympatheticactivity has the opposite effect, increasing thethreshold for ventricular fibrillation.56Recently, attention has focused on sponta-neous heart rate variability on Holter moni-toring as a non-invasive measure of cardiacautonomic function.7 8 Decreased heart ratevariability, indicating either increased sympa-thetic activity or reduced vagal activity, isassociated with increased risk of sudden deathin coronary artery disease.9 A reduction inheart rate variability has been reported inpatients with diabetes mellitus,'0 heart fail-ure," and after myocardial infarction,'2 13 butthere is little experience in patients with leftventricular hypertrophy.14 15The present study was undertaken to
compare heart rate variability in a controlpopulation with that in patients having elec-trocardiographic left ventricular hypertrophyand strain secondary to either hypertension oraortic valve disease. Possible reasons for anydifference, including left ventricular mass,coronary artery disease and ventricular func-tion are explored as are the possible conse-quences on ventricular arrhythmia.
Patients and methodsThere were three study groups: controls,patients with hypertension, and those withaortic valve disease.
Thirty six asymptomatic volunteers wererecruited on the basis of age from a largercohort of local government employeesundergoing non-invasive cardiac assessment.The age range of these volunteers waschosen so that the mean age would match thatof the patients. By definition, there was nohistory of diabetes or hypertension, and noroutine medication. Physical examinationand resting electrocardiogram (ECG) werenormal.
Ninety four patients were selected from anongoing study investigating the mechanismsof sudden cardiac death in 102 subjects withelectrocardiographic left ventricular hyper-trophy and strain presenting consecutively to
139 on 18 A
ugust 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.73.2.139 on 1 F
ebruary 1995. Dow
nloaded from

Mandawat, Wallbnidge, Pringle, Riyami, Latif, Macfarlane, Lorimer, Cobbe
the hypertension clinic. 16 All patients hadessential hypertension and inclusion in thepresent study was determined by the availabil-ity of a suitable 24 h ambulatory ECG (ofadequate quality; no atrial fibrillation, atrio-ventricular block, or sick sinus syndrome; andno permanent pacemaker). Five patients hadsuffered a previous myocardial infarctionmore than 1 year before the study and all buteight continued their usual medication,including ,B blockers, during the investigation.
Sixty patients (32 aortic stenosis, 10 aorticincompetence, and 18 mixed aortic valve dis-ease) were selected from a separate ongoingstudy of 90 consecutive patients requiringinvasive assessment for significant aortic valvedisease.17 Inclusion was determined by theavailability of a suitable 24 h ambulatoryECG (as described earlier). Regular medica-tion was continued, but no patient was receiv-ing ,B blocker or antiarrhythmic treatment.
All patients underwent 24 h ambulatoryECG monitoring. Echocardiography was per-formed to assess left ventricular mass'8 andfractional shortening. Coronary angiographywas undertaken in all patients with aorticvalve disease. This technique was consideredin all patients with hypertension, except thosewho were thought to be too old or frail, andperformed in 47.The study was approved by the Ethical
Committee of Glasgow Royal Infirmary.Written informed consent was obtained forinvasive procedures and verbal consent forother investigations.
ELECTROCARDIOGRAPHYA 12 lead ECG was recorded and measuredusing the Glasgow CARE (computer assistedreporting of electrocardiogram) system.'9 Leftventricular hypertrophy and strain wasdefined as ST segment depression > 002 mVand T wave inversion of 0-1 mV or more inone of leads I, aVL, V5 or V6 in the presenceof voltage criteria (SV1 + RV5 > 3.5 mV) forleft ventricular hypertrophy.
ECHOCARDIOGRAPHYThe echocardiograms were obtained with an
Ultramark 8 machine (Advanced TechnologyLaboratories, Bathell, USA) with a 3 MHztransducer. Patients were positioned in the450 left lateral position and views giving bestdelineation of the interventricular septum andleft ventricular posterior wall were chosen inthe parasternal long axis view. Measurementswere made according to the recommendationsof the Penn convention.20 The left ventricularmass was calculated by the anatomically vali-dated formula of Devereux and Reicheck'8:
LVM = 1-04 [(IVS + PWLV + LVIDD)3 - (LVIDD)3] - 13-6 g
where LVM is the left ventricular mass (g),IVS is the interventricular septal thickness(cm), PWLV is the thickness of the posteriorwall of left ventricle (cm), and LVIDD is theleft ventricular internal dimension at the endof diastole (cm).The ventricular mass was divided by body
surface area to obtain the left ventricular mass
index (LVMI). The body surface area wasobtained from the equation21:
BSA= 0-0001 x 71-84 x Wt0425 x Ht0725
where BSA is body surface area (m2), Wt isweight (kg), and Ht is height (cm).
Echocardiographic left ventricular hyper-trophy was diagnosed when left ventricularmass index exceeded 131 g/m2 in men and108 g/m2 in women.'8 Fractional shorteningwas taken as a measure of left ventricularfunction and was obtained as follows22:
Fractional shortening (%) = (LVIDd - LVIDs)/LVIDd
where LVIDd and LVIDs are the left ventricu-lar internal diameters at end diastole and endsystole, respectively.
AMBULATORY ELECTROCARDIOGRAPHYTwenty four h ambulatory ECGs wererecorded using bipolar leads CM5 and a mod-ified V2 on a Medilog II FM device (OxfordInstruments, Oxford, UK). Tapes wereanalysed by a single experienced technicianusing a computer assisted technique.23Significant ventricular arrhythmia was definedas the presence of > 30 ventricular extrasys-toles per h, complicated ventricular extrasys-tole (couplets, triplets, or R-on-T), orventricular tachycardia.'4
HEART RATE VARIABILITYAmbulatory ECG tapes were replayed using aPathfinder II (Reynolds Medical, Hertford,UK) high speed analyser at 60 times theoriginal speed. The analysis system, initiallytrained by an operator, differentiated betweennormal and abnormal QRS complexes. Thetriggering level for abnormal QRS complexeswas adjusted by the same operator throughoutthe study in an identical manner to minimisethe differences between successive analyses.All abnormal QRS complexes and their adja-cent intervals were excluded from the calcula-tion of heart rate variability. The signals onthe oscilloscope were closely monitoredthroughout by the operator to exclude tapeswith intermittent atrial fibrillation and othernon-sinus rhythms. The Pathfinder generatedan external impulse synchronous with eachQRS complex identified and another if theQRS complex was normal in configuration.This digitised information was passed to anECG analyser interface unit. This prolongedthe duration of the external impulses whichwere transferred via a parallel link to an IBMcompatible personal computer that effectivelystored each RR interval. Cycle lengths differ-ing by less than 20% from the preceding sinuscycle length (NN) were stored for furtheranalysis.
Heart rate variability was calculated as:1. SDNN, which is the standard deviation
of all NN intervals over 24 h.'52. Triangular index, which was calculated
by dividing the total number ofNN intervalsby the modal NN interval frequency.26
3. SDANN, which is the standard devia-tion of the mean NN interval for all 5 minsegments of a 24 h recording.
140
on 18 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.73.2.139 on 1 February 1995. D
ownloaded from
Heart rate variability in left ventricular hypertrophy
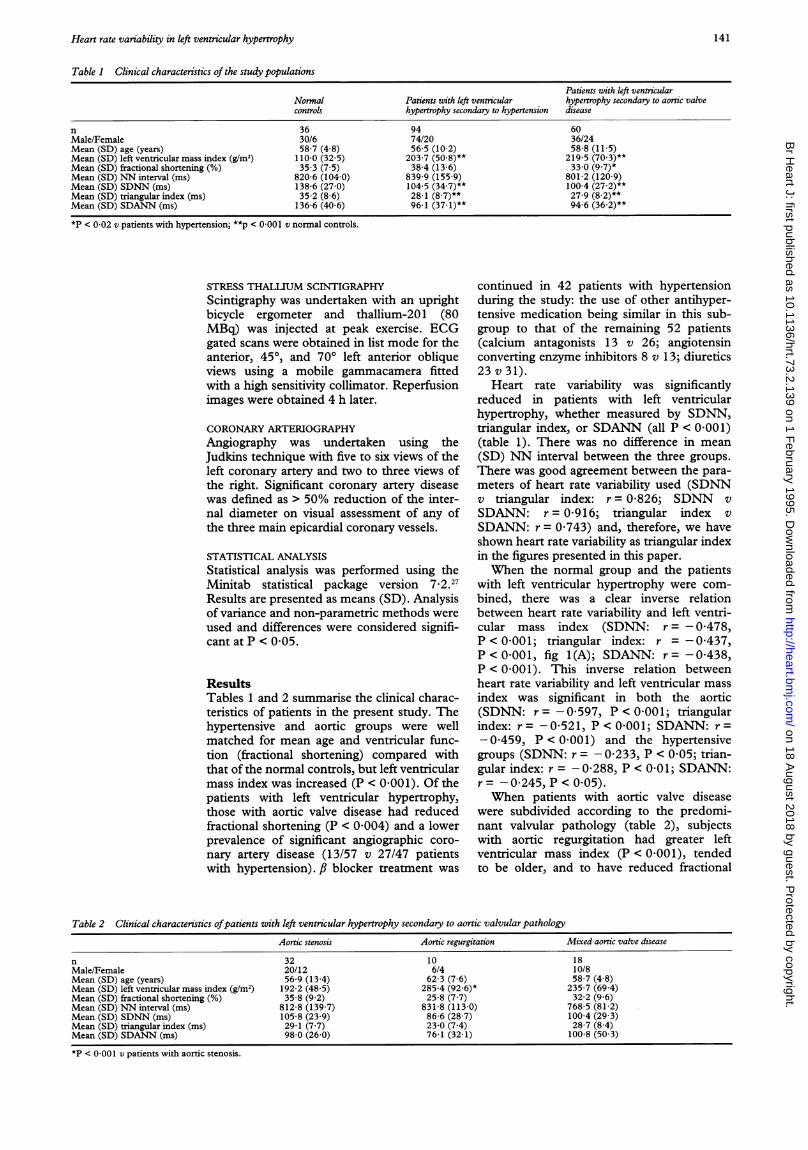
Table 1 Clinical characteristics of the study populations
Patients with left ventricularNormal Patients with left ventricular hypertrophy secondary to aortic valvecontrols hypertrophy secondary to hypertension disease
n 36 94 60Male/Female 30/6 74/20 36/24Mean (SD) age (years) 58-7 (4 8) 56 5 (10 2) 58 8 (11-5)Mean (SD) left ventricular mass index (g/m2) 110-0 (32-5) 203 7 (50 8)** 219-5 (70 3)**Mean (SD) fractional shortening (%) 35-3 (7-5) 38-4 (13-6) 33-0 (9 7)*Mean (SD) NN interval (ms) 820-6 (104-0) 839-9 (155-9) 801-2 (120-9)Mean (SD) SDNN (ms) 138-6 (27 0) 104-5 (34 7)** 100-4 (27 2)**Mean (SD) triangular index (ms) 35-2 (8-6) 28-1 (8.7)** 27-9 (8.2)**Mean (SD) SDANN (ms) 136-6 (40 6) 96-1 (37-1)** 94-6 (36.2)**
*P < 0 02 v patients with hypertension; **p < 0 001 v normal controls.
STRESS THALLIUM SCINTIGRAPHYScintigraphy was undertaken with an uprightbicycle ergometer and thallium-201 (80MBq) was injected at peak exercise. ECGgated scans were obtained in list mode for theanterior, 450, and 700 left anterior obliqueviews using a mobile gammacamera fittedwith a high sensitivity collimator. Reperfusionimages were obtained 4 h later.
CORONARY ARTERIOGRAPHYAngiography was undertaken using theJudkins technique with five to six views of theleft coronary artery and two to three views ofthe right. Significant coronary artery diseasewas defined as > 50% reduction of the inter-nal diameter on visual assessment of any ofthe three main epicardial coronary vessels.
STATISTICAL ANALYSIS
Statistical analysis was performed using theMinitab statistical package version 7.2.27Results are presented as means (SD). Analysisof variance and non-parametric methods were
used and differences were considered signifi-cant at P < 0O05.
ResultsTables 1 and 2 summarise the clinical charac-teristics of patients in the present study. Thehypertensive and aortic groups were wellmatched for mean age and ventricular func-tion (fractional shortening) compared withthat of the normal controls, but left ventricularmass index was increased (P < 0 001). Of thepatients with left ventricular hypertrophy,those with aortic valve disease had reducedfractional shortening (P < 0 004) and a lowerprevalence of significant angiographic coro-
nary artery disease (13/57 v 27/47 patientswith hypertension). ,B blocker treatment was
continued in 42 patients with hypertensionduring the study: the use of other antihyper-tensive medication being similar in this sub-group to that of the remaining 52 patients(calcium antagonists 13 v 26; angiotensinconverting enzyme inhibitors 8 v 13; diuretics23 v 31).
Heart rate variability was significantlyreduced in patients with left ventricularhypertrophy, whether measured by SDNN,triangular index, or SDANN (all P < 0 001)(table 1). There was no difference in mean
(SD) NN interval between the three groups.There was good agreement between the para-
meters of heart rate variability used (SDNNv triangular index: r = 0-826; SDNN v
SDANN: r = 0-916; triangular index v
SDANN: r = 0 743) and, therefore, we haveshown heart rate variability as triangular indexin the figures presented in this paper.
When the normal group and the patientswith left ventricular hypertrophy were com-
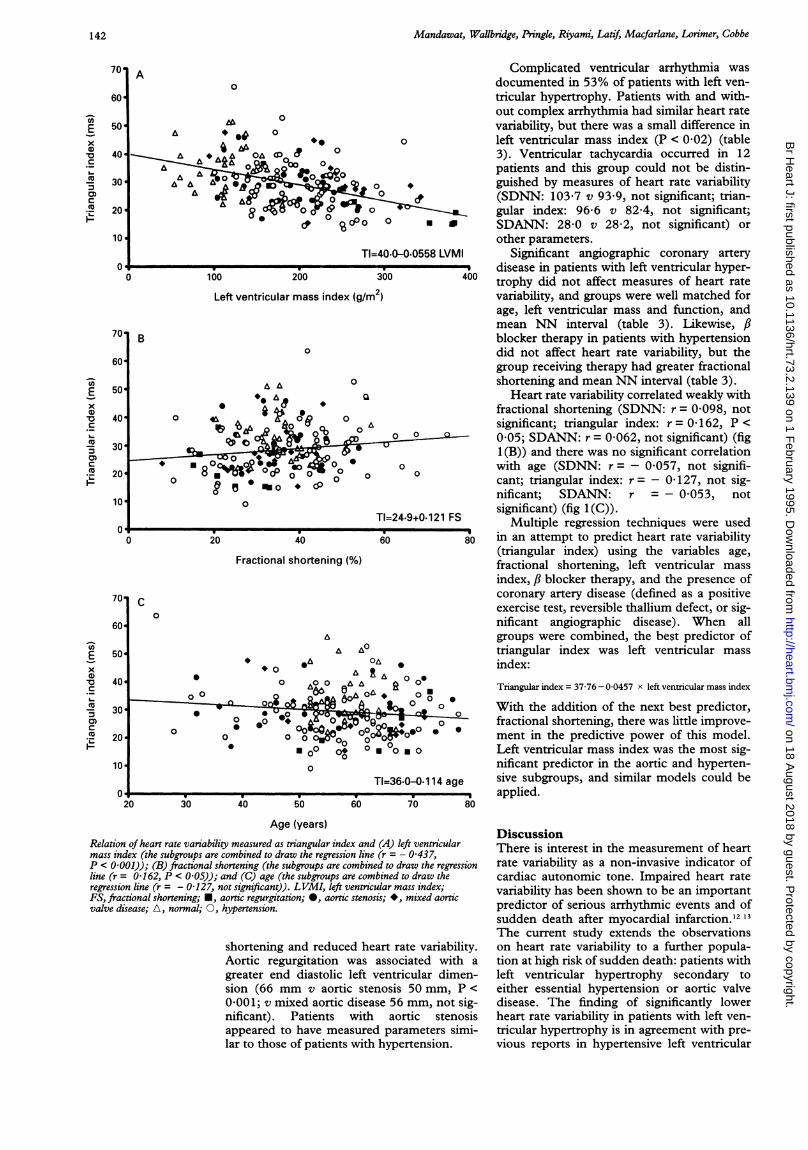
bined, there was a clear inverse relationbetween heart rate variability and left ventri-cular mass index (SDNN: r = - 0478,P < 000O1; triangular index: r = -0437,P < 0X001, fig 1(A); SDANN: r =-0X438,P < 0 001). This inverse relation betweenheart rate variability and left ventricular mass
index was significant in both the aortic(SDNN: r = -0597, P < 0 001; triangularindex: r -0-521, P<0001; SDANN: r=-0A459, P < 0 001) and the hypertensivegroups (SDNN: r = - 0233, P < 0-05; trian-gular index: r = -0-288, P < 0 01; SDANN:r = - 0-245, P < 0 05).When patients with aortic valve disease
were subdivided according to the predomi-nant valvular pathology (table 2), subjectswith aortic regurgitation had greater leftventricular mass index (P < 0O001), tendedto be older, and to have reduced fractional
Table 2 Clinical characteristics ofpatients with left ventricular hypertrophy secondary to aortic valvular pathologyAortic stenosis Aortic regurgitation Mixed aortic valve disease
n 32 10 18Male/Female 20/12 6/4 10/8Mean (SD) age (years) 56-9 (13-4) 62-3 (7 6) 58-7 (4 8)Mean (SD) left ventricular mass index (g/m2) 192-2 (48 5) 285-4 (92 6)* 235-7 (69 4)Mean (SD) fractional shortening (%) 358 (9 2) 25-8 (7 7) 32-2 (9 6)Mean (SD) NN interval (ms) 812 8 (139-7) 831-8 (113-0) 768-5 (81 2)Mean (SD) SDNN (ms) 105-8 (23 9) 86-6 (28-7) 100-4 (29 3)Mean (SD) triangular index (ms) 29-1 (7 7) 23-0 (7 4) 28-7 (8 4)Mean (SD) SDANN (ms) 98-0 (26-0) 76-1 (32 1) 100-8 (50 3)
*P < 0-001 v patients with aortic stenosis.
141
on 18 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.73.2.139 on 1 February 1995. D
ownloaded from
Mandawat, Wallbridge, Pringle, Riyami, Latif) Macfarlane, Lorimer, Cobbe
Left ventricular mass index (g/m2)
Fractional shortening (%)
80
Age (years)
Relation of heart rate variability measured as triangular index and (A) left ventricularmass index (the subgroups are combined to draw the regression line (r = - 0 437,P < 0 001)); (B) fractional shortening (the subgroups are combined to draw the regressionline (r = 0 162, P < 0 05)); and (C) age (the subgroups are combined to draw theregression line (r = - 0 127, not significant)). LVMI, left ventricular mass index;FS, fractional shortening; *, aortic regurgitation; *, aortic stenosis; *, mixed aorticvalve disease; A, normal; 0, hypertension.
shortening and reduced heart rate variability.Aortic regurgitation was associated with a
greater end diastolic left ventricular dimen-sion (66 mm v aortic stenosis 50 mm, P <
0 001; v mixed aortic disease 56 mm, not sig-nificant). Patients with aortic stenosisappeared to have measured parameters simi-lar to those of patients with hypertension.
Complicated ventricular arrhythmia wasdocumented in 53% of patients with left ven-tricular hypertrophy. Patients with and with-out complex arrhythmia had similar heart ratevariability, but there was a small difference inleft ventricular mass index (P < 0-02) (table3). Ventricular tachycardia occurred in 12patients and this group could not be distin-guished by measures of heart rate variability(SDNN: 103-7 v 93 9, not significant; trian-gular index: 96-6 v 82-4, not significant;SDANN: 28-0 v 28&2, not significant) orother parameters.
Significant angiographic coronary arterydisease in patients with left ventricular hyper-trophy did not affect measures of heart ratevariability, and groups were well matched forage, left ventricular mass and function, andmean NN interval (table 3). Likewise, fiblocker therapy in patients with hypertensiondid not affect heart rate variability, but thegroup receiving therapy had greater fractionalshortening and mean NN interval (table 3).
Heart rate variability correlated weakly withfractional shortening (SDNN: r = 0-098, notsignificant; triangular index: r = 0<162, P <0'05; SDANN: r = 0-062, not significant) (fig1 (B)) and there was no significant correlationwith age (SDNN: r = - 0057, not signifi-cant; triangular index: r= - 0-127, not sig-nificant; SDANN: r =- 0053, notsignificant) (fig 1(G)).
Multiple regression techniques were usedin an attempt to predict heart rate variability(triangular index) using the variables age,fractional shortening, left ventricular massindex, fi blocker therapy, and the presence ofcoronary artery disease (defined as a positiveexercise test, reversible thallium defect, or sig-nificant angiographic disease). When allgroups were combined, the best predictor oftriangular index was left ventricular massindex:
Triangular index = 37-76 - 0-0457 x left venticular mass index
With the addition of the next best predictor,fractional shortening, there was little improve-ment in the predictive power of this model.Left ventricular mass index was the most sig-nificant predictor in the aortic and hyperten-sive subgroups, and similar models could beapplied.
DiscussionThere is interest in the measurement of heartrate variability as a non-invasive indicator of
cardiac autonomic tone. Impaired heart ratevariability has been shown to be an importantpredictor of serious arrhythmic events and ofsudden death after myocardial infarction.'2 13
The current study extends the observationson heart rate variability to a further popula-tion at high risk of sudden death: patients withleft ventricular hypertrophy secondary toeither essential hypertension or aortic valvedisease. The finding of significantly lowerheart rate variability in patients with left ven-
tricular hypertrophy is in agreement with pre-vious reports in hypertensive left ventricular
x0.
'a
c
0)C
-
Ex0)
V
'a
C
._
CuI-
x
0)
I-
142
on 18 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.73.2.139 on 1 February 1995. D
ownloaded from

Heart rate variability in left ventricular hypertrophy
Table 3 Influence of significant ventricular arrhythmia (> 30 ventricular extrasystoleslh, complex ventricular extrasystole, or ventricular tachycardia),angiographic coronary artery disease in patients with left ventricular hypertrophy, and 1)-blocker treatment in patients with hypertension on heart ratevariability
Significant ventricular arrhythmia Coronary artery disease ,B Blocker therapy
No Yes No Yes No Yes
n 73 81 64 40 52 42Mean (SD) age (years) 56-0 (11-1) 58-7 (10-4) 56-2 (11 0) 58-6 (9-0) 58-1 (8 9) 54-6 (11-5)Mean (SD) left ventricular mass index (g/m2) 200-4 (63 9) 218-8 (54-1)* 214-1 (65 6) 201-0 (51-7) 208-1 (53 6) 198-5 (47 4)Mean (SD) fractional shortening (%) 37-2 (11-5) 35-5 (13-3) 34-6 (10-1) 36-4 (12-5) 35-4 (14-3) 42-1 (119)**Mean (SD) NN interval (ms) 833-3 (131-9) 817-6 (154-8) 798-2 (119-5) 812-5 (142-8) 772 3 (123-2) 923-6 (152 5)***Mean (SD) SDNN (ms) 104-1 (27-1) 101 9 (35 9) 101-1 (32 0) 97 4 (21-6) 101-6 (36 0) 108-1 (33 0)Mean (SD) triangular index (ms) 28-9 (7 9) 27-2 (9 0) 28-2 (8 9) 27-0 (7 2) 27-1 (7 9) 29-4 (9-6)Mean (SD) SDANN (ms) 98-7 (36-1) 92-7 (37 2) 95 7 (40 5) 88-7 (23-1) 95 0 (40-1) 97 5 (33 5)
*P < 0 02 v no significant ventricular arrhythmia; **P < 0 005 v no fl-blocker treatment; ***P < 0 001 v no fl-blocker treatment.
hypertrophy assessed by spectral analysismethods'5 and in animal studies.28 There areno published data on heart rate variability inaortic valve disease, but Airaksinen et a129have reported altered autonomic function insuch patients and this is also our experience(AAS Riyami, unpublished data). Heart ratevariability was similarly reduced in patientswith left ventricular hypertrophy due to pres-sure overload from either aortic stenosis orhypertension.We have demonstrated a continuous
inverse relation between heart rate variabilityand left ventricular mass index. This relationis apparent for measurement of heart ratevariability by SDNN, triangular index, andSDANN. The correlation was better inpatients with aortic valve disease than in thosewith hypertension, and this may be attribut-able to a wider range of left ventricular massindex values in the former group because ofthe inclusion of patients with aortic regurgita-tion.
Previous studies have demonstrated areduction in heart rate variability with increas-ing age,'03' in patients with coronary arterydisease,2532 and in those with impaired leftventricular function." In the present study ofpatients with left ventricular hypertrophy,multivariate analysis demonstrated that leftventricular mass index was the single mostimportant determinant of heart rate variabil-ity. Fractional shortening was a much weakerpredictor and added little to the power of themultivariate model. Heart rate variability wasnot affected by angiographic coronary arterydisease, patient age, or fi blocker treatment,although the latter observation is com-pounded by between group differences infractional shortening and the mean NN inter-val.The observation of an increased prevalence
of ventricular ectopy and ventricular tachy-cardia in patients with hypertensive left ven-tricular hypertrophy is consistent with anarrhythmic mechanism as the cause of suddendeath.'4 We were unable to demonstrate anydifference in heart rate variability in the leftventricular hypertrophy group betweenpatients with and without complex ventriculararrhythmia. Likewise, no differences in heartrate variability were seen in patients with ven-tricular tachycardia, although the numbers are
small. There is an association betweenreduced heart rate variability and an increasedincidence of ventricular arrhythmia aftermyocardial infarction,'4 but the relation inpatients with left ventricular hypertrophy isless certain. 14 The relation of ventriculararrhythmia, left ventricular mass, and heartrate variability requires further exploration.The study has several potential limitations.
It is accepted that SDNN, triangular index,and SDANN, derived directly from heart rateintervals, are broadly based measures of heartrate variability. SDNN, for example, corre-lates positively with the low frequency compo-nent on power spectral analysis (r = 085)'5and conveys important prognostic informa-tion.25 Analysis of heart rate variability bypower spectral methods may provide addi-tional information in patients with left ventric-ular hypertrophy. Whilst multifactorialanalysis suggested that left ventricular massindex was the most important determinant ofheart rate variability, inclusion of a largerpatient population may have permitted morethorough examination of the possible com-pounding effects of age, fractional shortening,coronary artery disease, and fi blocker med-ication. Information pertaining to ejectionfraction is not available for patients in this study.
In conclusion, heart rate variability isreduced significantly in patients with left ven-tricular hypertrophy secondary to eitherhypertension or aortic valve disease. There isa continuous inverse relation between heartrate variability and left ventricular mass index.Multivariate analysis demonstrates that leftventricular mass index is the most importantdeterminant of heart rate variability.Disturbances in cardiac autonomic functionmay contribute to the mechanism of suddendeath in patients with left ventricular hyper-trophy, and assessment of heart rate variabil-ity may prove important in the riskstratification of such patients. Future workshould examine the relation between heartrate variability and mortality in patients withleft ventricular hypertrophy, and the effect onheart rate variability of changes in left ventric-ular mass index due to antihypertensive treat-ment or after aortic valve replacement.
DRW is a British Heart Foundation Friends' ProvidentResearch Fellow. We thank Miss S C McLaughlin for statisticalsupport.
143
on 18 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.73.2.139 on 1 February 1995. D
ownloaded from
Mandawat, Wallbridge, Pringle, Riyami, Latif, Macfarlane, Lorimer, Cobbe
1 Kannel WB, Gorden T, Offun D. Left ventricular hyper-trophy by electrocardiogram: prevalence, incidence andmortality in the Framingham study. Ann Intern Med1969;71:89-105.
2 Kannel WB, Sorlie P. Left ventricular hypertrophy inhypertension: prognostic and pathogenetic implications(the Framingham study). In: Strauer BE, ed. The heart inhypertension (Boehringer, Mannheim symposium series).Berlin: Springer Verlag, 1981:223-42.
3 Messerli FH, Ventura HO, Elizard DJ, Dunn FG, FrolichED. Hypertension and sudden death: increased ventricu-lar ectopic activity in left ventricular hypertrophy. Am JfMed 1984;77: 18-22.
4 McLenachan JM, Esther M, Morris KI, Dargie HJ.Ventricular arrhythmia in patients with left ventricularhypertrophy. N EnglJ Med 1987;317:787-92.
5 Lown B, Verrier R. Neural activity and ventricular fibrilla-tion. N EnglJ Med 1976;294;1165-70.
6 Zipes DP, Levi MN, Cobb LA, Julius S, Peter G,Kaufman PG, et al. Task force 2: sudden cardiac death.Neural and cardiac interactions. Circulation 1987;76(suppl 1):202-7.
7 Schwartz PJ, Randall WC, Anderson EA, Engle BT,Friedman M, Hartley LH, et al. Task force 4. Suddencardiac death. Non pharmacologic interventions.Circulation 1987;76(suppl 1):215-9.
8 Ewing DJ. Heart rate variability: an important new riskfactor in patients following myocardial infarction. ClinCardiol 1991;14:683-5.
9 Martin GJ, Magid NM, Myers G, Barnett PS, Schaad JW,Weiss JS, et al. Heart rate variability and sudden deathsecondary to coronary artery disease during ambulatoryelectrocardiographic monitoring. Am J7 Cardiol 1987;60:86-9.
10 Ewing DJ, Neilson JM, Shapiro CM, Steward JA, Reid W.Twenty four hour heart rate variability: effect of posture,sleep, and time of day in healthy controls and comparisonwith bed side tests of autonomic function in diabeticpatients. BrHeartJ 1991;65:239-44.
11 Woo MA, William RN, Stevenson G, Mosar DK. Pattern ofbeat to beat heart rate variability in advanced heart failure.Am HeartJ 1992;123:704-10.
12 Kleiger RE, Miller JP, Bigger JT, Moss AJ and MulticenterPostinfarction Research Group. Decreased heart ratevariability and its association with increased mortalityafter acute myocardial infarction. Am Jf Cardiol 1987;59:256-62.
13 Pipilis A, Flather M, Ormerod 0, Sleight P. Heart ratevariability in acute myocardial infarction and its associa-tion with infarct site and clinical course. Am Cardiol1991;67:1137-9.
14 Cardillo C, Musumevu V. Heart rate variability and ven-tricular ectopic activity in hypertensive patients.JHypertens 1989;7(suppl 6):534-5.
15 Coumel JS, Hermida JS, Wennerblom B, Leenhardts A,Maison-Blanche P, Cauchemez B. Heart rate variabilityin left ventricular hypertrophy and heart failure, andeffects of betablockade. Eur HeartJ 199 1;12:412-22.
16 Pringle SD, Dunn FG, Tweddel AC, Martin W,MacFarlane PW, McKillop, JH, et al. Symptomatic andsilent myocardial ischaemia in hypertensive patients withleft ventricular hypertrophy. BrHeartJ 1992;67:377-82.
17 Riyami AAS. Potential predictors of sudden death in aorticvalve disease [PhD thesis]. Glasgow: University ofGlasgow, 1991.
18 Devereux RB, Reicheck N. Echocardiographic determina-tion of left ventricular mass in man: anatomic validationof method. Circulation 1977;55:613-8.
19 Macfarlane PW, Devine B, Latif S, McLaughlin S, ShoatDB, Watts MP. Methodology of ECG interpretation inthe Glasgow Program. Methods InfMed 1990;29:354-61.
20 Devereux RB, Lutas EM, Casale PN. Standardisation ofM mode echocardiographic left ventricular anatomicmeasurements. JAm Coll Cardiol 1984;4: 1222-30.
21 DuBois D, DuBois EF. A formula to estimate approximatesurface area if height and weight be known. Arch InternMed 1916;17:863-71.
22 McDonald IG, Feigenbaum H, Chang S. Analysis of leftventricular wall motion by reflected ultrasound.Application to assessment of myocardial function.Circulation 1972;46: 14-25.
23 Macfarlane PW, McLung JM, Irving A, Watts MP.Computer assisted analysis of dynamic (24 hours)electrocardiograms. In: Macfarlane PW, ed. Progress inelectrocardiology. London: Pitman, 1979:123-6.
24 Lown B, Wolf M. Approaches to sudden death from coro-nary heart disease. Circulation 1971;41:130-40.
25 Bigger JT, Kleiger RE, Fleiss J, Rolnitzky LM, SteinmanRC, Miller JP, and the Multicenter PostinfarctionResearch Group. Component of heart rate variabilitymeasured during the healing of acute myocardial infarc-tion. Am Cardiol 1988;61:208-15.
26 Cripps TR, Malik M, Farrell TG, Camm AJ. Prognosticvalue of reduced heart rate variability after myocardialinfarction. Clinical evaluation of new analysis method.BrHeartJ 1991;65:14-9.
27 Ryan BF, Brian U, Thomas AR. Minitab hand book.Boston, MA: PWS Kent Publishing, 1985.
28 Friberg P, Karlsson B, Nordlander M. Sympathetic andparasympathetic influence on blood pressure and heartrate variability in Wistar-Kyoto and spontaneouslyhypertensive rats. Hypertens 1988;6:S58-60.
29 Airaksinen KEJ, Ikaheimo NJ, Koistinen MJ, TakkunenJT. Impaired vagal heart rate control in aortic valvestenosis. Eur Heart
_J 1988;9:1126-30.30 Hrushesky WJM, Fader D, Schmitt 0, Gilbertson V. The
respiratory sinus arrythmia. A measure of cardiac age.Science 1984;224: 1001-4.
31 Masaoka S, Lev-Ran A, Hill LR, Gita V, Edward HG.Heart rate variability in diabetes. Relationship to age andduration of disease. Diabetes Care 1985;8:64-8.
32 Hayano J, Sakakibara V, Yamada M, Ohte N, Fujinami T,Yokoyama K, et al. Decreased magnitude of heart ratespectral component in coronary artery disease; its rela-tion to angiographic severity. Circulation 1990;81:1217-24.
33 Nolan J, Flapan AD, Capewell S, MacDonald TM,Neilson JMM, Ewind DJ. Decreased cardiac parasympa-thetic activity in chronic heart failure and its relation toleft ventricular function. Br HeartJ 1992;67:482-5.
34 Farrell TG, Bashir Y, Cripps T, Malik M, Poloniecki J,Bennett ED, et al. Risk stratification for arrhythmicevents in post infarction patients based on heart ratevariability, ambulatory electrocardiographic variablesand signal average electrocardiogram. JAm Coll Cardiol1991;18:687-97.
35 Kleiger RE, Bigger JT, Bosner MS, Chung MK, Cook JR,Rolnitzky LM, et al. Stability over time of variables mea-suring heart rate variability in normal subjects. Am JCardiol 1991;68:626-30.
144
on 18 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.73.2.139 on 1 February 1995. D
ownloaded from





























