Embed Size (px)
Citation preview
Break-Out Session
Management of Heart Failure
Nathan Dwyer & Graeme Bleach
National Heart Foundation of Australia1
1. Krum H, et al. Med J Aust. 2011 Apr; 194(8):405-409.
• Last updated October 2011
• Similar to European and US guideline recommendations except for recent (2016) changes
• Will require updating to reflect changes in HF management
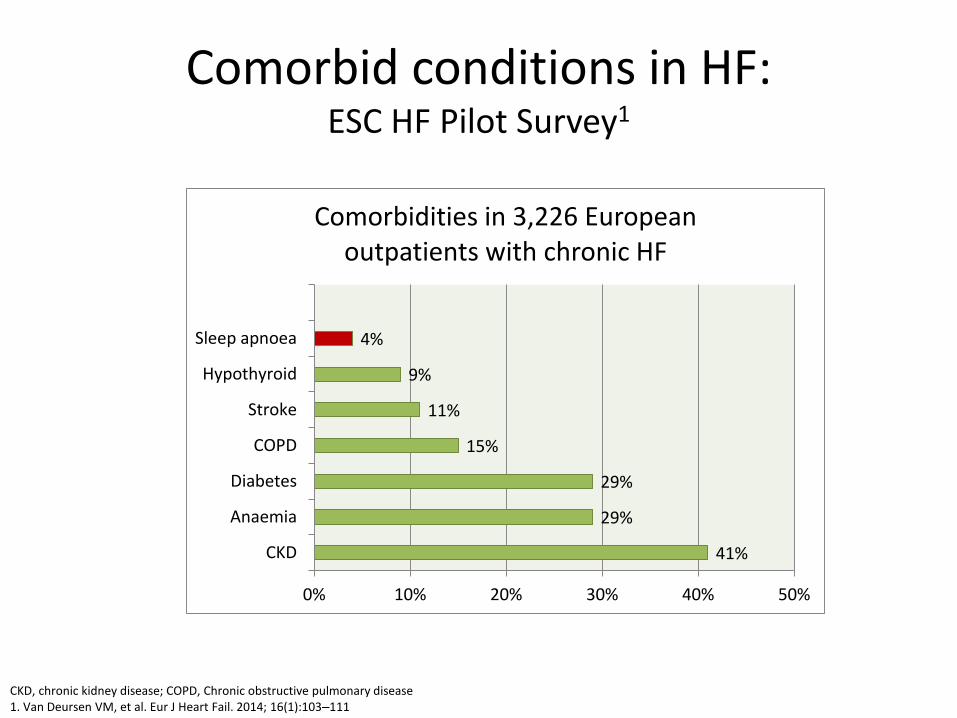
Comorbid conditions in HF: ESC HF Pilot Survey1
41%
29%
29%
15%
11%
9%
4%
CKD
Anaemia
Diabetes
COPD
Stroke
Hypothyroid
Sleep apnoea
0% 10% 20% 30% 40% 50%
Comorbidities in 3,226 European outpatients with chronic HF
CKD, chronic kidney disease; COPD, Chronic obstructive pulmonary disease1. Van Deursen VM, et al. Eur J Heart Fail. 2014; 16(1):103‒111

TREATMENTS
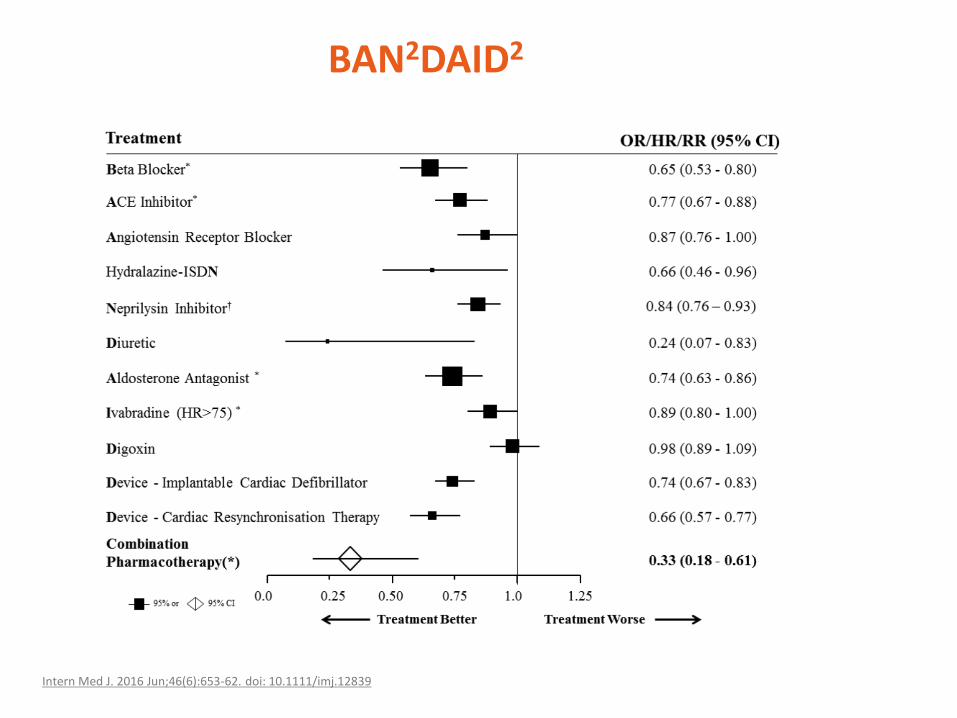
BAN2DAID2
Intern Med J. 2016 Jun;46(6):653-62. doi: 10.1111/imj.12839
Ivabradine
1. National Heart Foundation Australia. Guidelines for the prevention, detection and management of chronic heart failure in Australia. 2011. 2. eMC. Summary of Product Characteristics: Procoralan. 2015. 3. Ponikowski P, et al. Eur Heart J. 2016; doi: 10.1093/eurheartj/ehw128 (Web Addenda).
Ivabradine has a role in certain HF-REF patients1
Indication:
• Patients with impaired systolic function and a recent heart failure hospitalisation, who are in sinus rhythm where heart rate remains ≥70 bpm despite efforts to maximise dosage of background beta-blockade1
Potential uses: • Patients with stable symptomatic HF (NYHA class II–IV) and EF ≤35% and resting heart
rate ≥70 bpm despite guideline-recommended treatment (maximal tolerated dose of ACEi or ARB, beta-blocker and an MRA3
Reported patient outcomes:• Reduce cardiovascular mortality1,3
• Reduce the risk of HF hospitalisation1,3Reported patient outcomes
Potential uses
Indication
If - channel blocker1
Key issues for use1
• Should be considered for CHF patients with impaired systolic function and who are in sinus rhythm where their heart rate remains > 77 bpm despite efforts to maximise dosage of background beta-blockade
Key trial data2
• SHIFT study
Mode of action3
• Slows HR through inhibition of the lf channel in the sinus node
Safety considerations3
• Use with caution in severe (class IV) HF or during exacerbation of HF
• Monitor HR during treatment
• May worsen retinitis pigmentosa
• Drug interactions include drugs that may cause bradycardia (discontinue verapamil, diltiazem); drugs that are strong inhibitors of CYP3A4– Antifungals such as ketoconazole, macrolide antibiotics (clarithromycin), HIV protease inhibitors ritonavir. See
labelling for other contraindications
1.National Heart Foundation of Australia. Guidelines for the prevention, detection and management of chronic heart failure in Australia. October 2011. 2. Swedberg K, et al. J Am Coll Cardiol. 2012; 59(22):1938‒1945. 3. Ponikowski P, et al. Eur Heart J, 2016. doi:10.1093/eurheartj/ehw128.

lf - channel blocker1
1. Ponikowski P, et al. Eur Heart J, 2016. doi:10.1093/eurheartj/ehw128
Drugs in this category Starting dose (mg) Target dose (mg)
Ivabradine 5 BID 7.5 BID
Dosage considerations:• Start with low dose• In patients >75 years of age, 2.5 mg BID starting dose may be used• Modify dose based on patient’s resting heart rate. Aim for targeted dose, or
highest tolerated dose based on resting HR (50 to 60 BPM target)

ARNIs
1. eMC. Summary of Product Characteristics: Entresto. 2016. 2. Ponikowski P, et al. Eur Heart J. 2016; doi: 10.1093/eurheartj/ehw128.
ARNIs have a role in selected HF-REF patients
Indication:
• Treatment of symptomatic chronic HF-REF1
Potential uses:
• A replacement for an ACEi to further reduce the risk of HF hospitalisation and death in ambulatory patients with HF-REF who remain symptomatic despite optimal treatment with an ACEi, beta-blocker and an MRA2
• In ambulatory patients with symptomatic HF-REF, ARNIs:2
– Reduce hospitalisations for worsening HF– Reduce cardiovascular mortality and overall mortality
Reported patient outcomes
Potential uses
Indication
Angiotensin receptor neprilysin inhibitor (ARNI)
Key issues for use
• Recommended as a replacement for an ACEi in patients with HF-REF who remain symptomatic despite optimised ACEi + beta-blocker + MRA1
Key trial data
• PARADIGM-HF2
Mode of action
• RAAS inhibition; inhibition of neprilysin increases bioavailability of natriuretic peptides1
Safety considerations1
• To minimise risk of angio-oedema, withhold ACEi for ≥36 hours before initiating ARNI therapy
• Combined treatment of ARNI with ACEi or ARB is contraindicated
1. Ponikowski P, et al. Eur Heart J, 2016. doi:10.1093/eurheartj/ehw128. 2. McMurray JJ, et al. N Engl J Med. 2014; 17(3):242‒247.
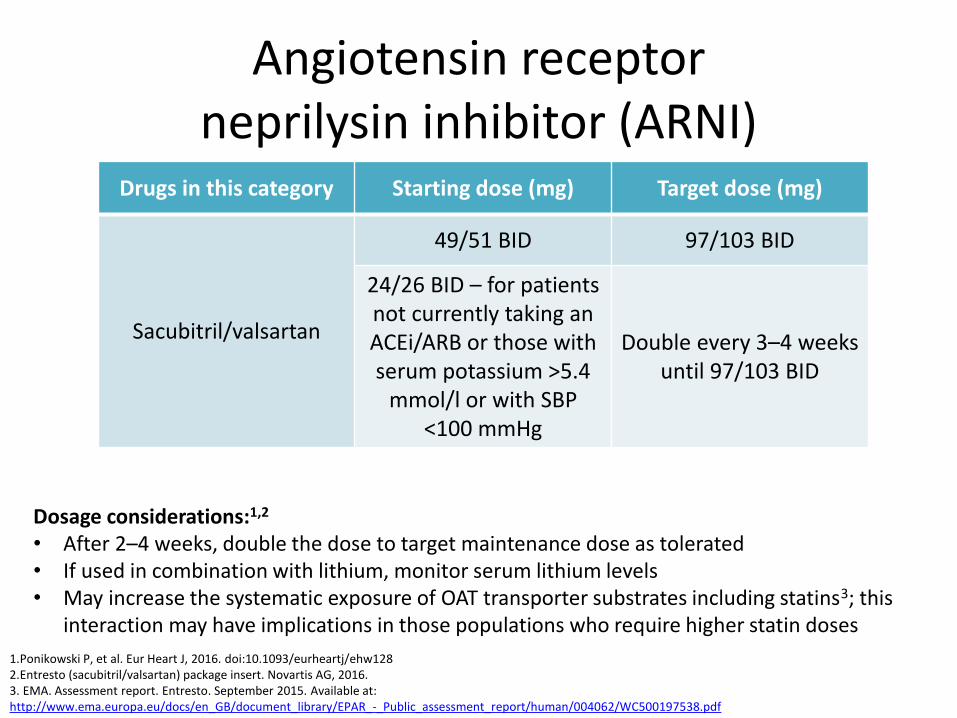
Angiotensin receptor neprilysin inhibitor (ARNI)
1.Ponikowski P, et al. Eur Heart J, 2016. doi:10.1093/eurheartj/ehw1282.Entresto (sacubitril/valsartan) package insert. Novartis AG, 2016.3. EMA. Assessment report. Entresto. September 2015. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/004062/WC500197538.pdf
Drugs in this category Starting dose (mg) Target dose (mg)
Sacubitril/valsartan
49/51 BID 97/103 BID
24/26 BID – for patientsnot currently taking an ACEi/ARB or those with serum potassium >5.4
mmol/l or with SBP <100 mmHg
Double every 3–4 weeks until 97/103 BID
Dosage considerations:1,2
• After 2–4 weeks, double the dose to target maintenance dose as tolerated• If used in combination with lithium, monitor serum lithium levels• May increase the systematic exposure of OAT transporter substrates including statins3; this
interaction may have implications in those populations who require higher statin doses
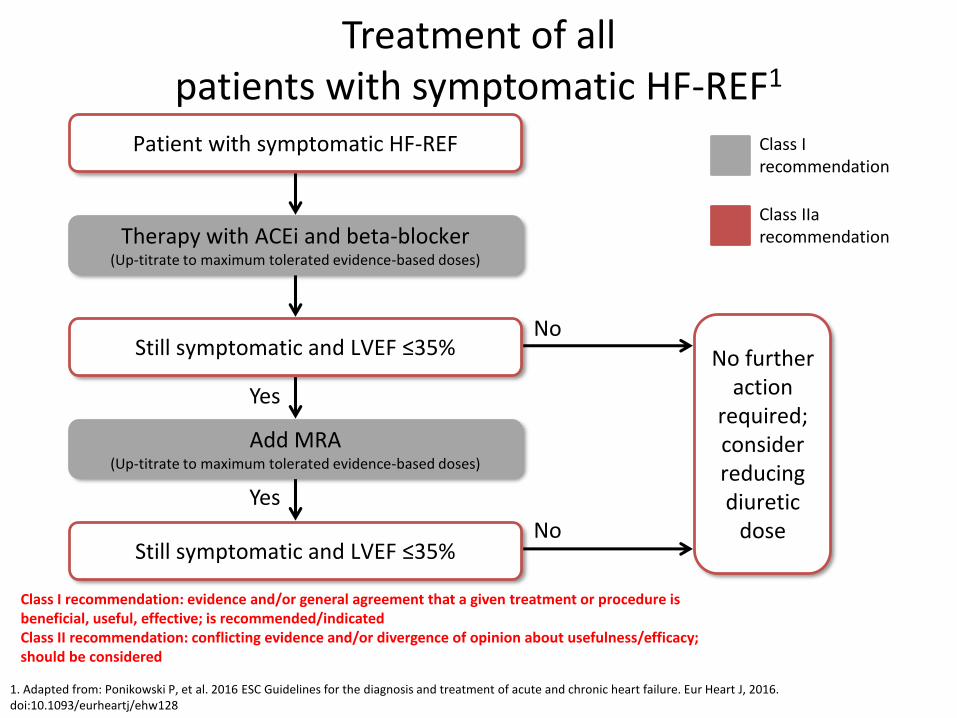
Treatment of all patients with symptomatic HF-REF1
1. Adapted from: Ponikowski P, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J, 2016. doi:10.1093/eurheartj/ehw128
Patient with symptomatic HF-REF
Therapy with ACEi and beta-blocker (Up-titrate to maximum tolerated evidence-based doses)
Still symptomatic and LVEF ≤35%
Add MRA(Up-titrate to maximum tolerated evidence-based doses)
Still symptomatic and LVEF ≤35%
No
No
Yes
Yes
No further action
required; consider reducing diuretic
dose
Class I recommendation
Class IIarecommendation
Class I recommendation: evidence and/or general agreement that a given treatment or procedure is beneficial, useful, effective; is recommended/indicated Class II recommendation: conflicting evidence and/or divergence of opinion about usefulness/efficacy; should be considered
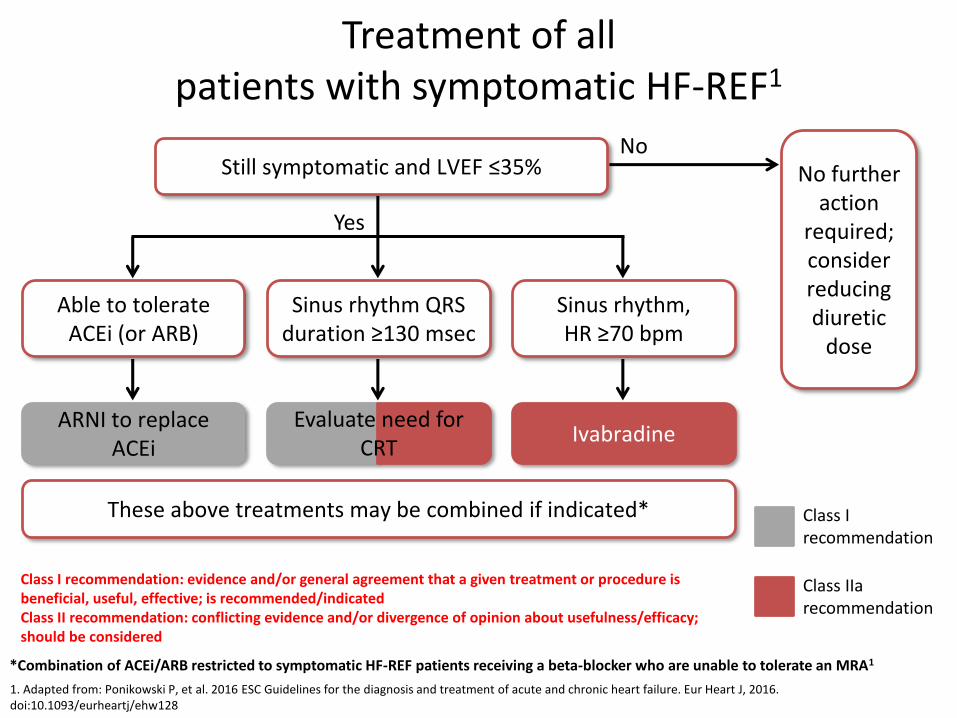
1. Adapted from: Ponikowski P, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J, 2016. doi:10.1093/eurheartj/ehw128
*Combination of ACEi/ARB restricted to symptomatic HF-REF patients receiving a beta-blocker who are unable to tolerate an MRA1
Yes
Sinus rhythm QRS duration ≥130 msec
Sinus rhythm, HR ≥70 bpm
Able to tolerate ACEi (or ARB)
ARNI to replace ACEi
IvabradineEvaluate need for
CRT
These above treatments may be combined if indicated* Class I recommendation
Class IIarecommendation
Still symptomatic and LVEF ≤35%No
No further action
required; consider reducing diuretic
dose
Class I recommendation: evidence and/or general agreement that a given treatment or procedure is beneficial, useful, effective; is recommended/indicated Class II recommendation: conflicting evidence and/or divergence of opinion about usefulness/efficacy; should be considered
Treatment of all patients with symptomatic HF-REF1
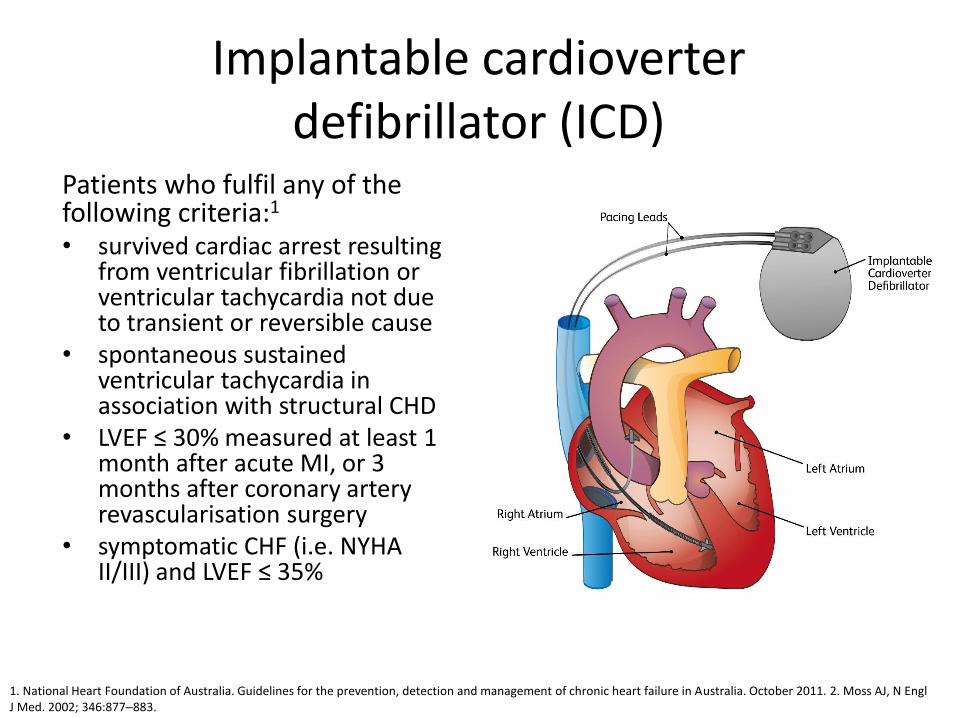
Implantable cardioverter defibrillator (ICD)
Patients who fulfil any of the following criteria:1
• survived cardiac arrest resulting from ventricular fibrillation or ventricular tachycardia not due to transient or reversible cause
• spontaneous sustained ventricular tachycardia in association with structural CHD
• LVEF ≤ 30% measured at least 1 month after acute MI, or 3 months after coronary artery revascularisation surgery
• symptomatic CHF (i.e. NYHA II/III) and LVEF ≤ 35%
1. National Heart Foundation of Australia. Guidelines for the prevention, detection and management of chronic heart failure in Australia. October 2011. 2. Moss AJ, N Engl J Med. 2002; 346:877‒883.
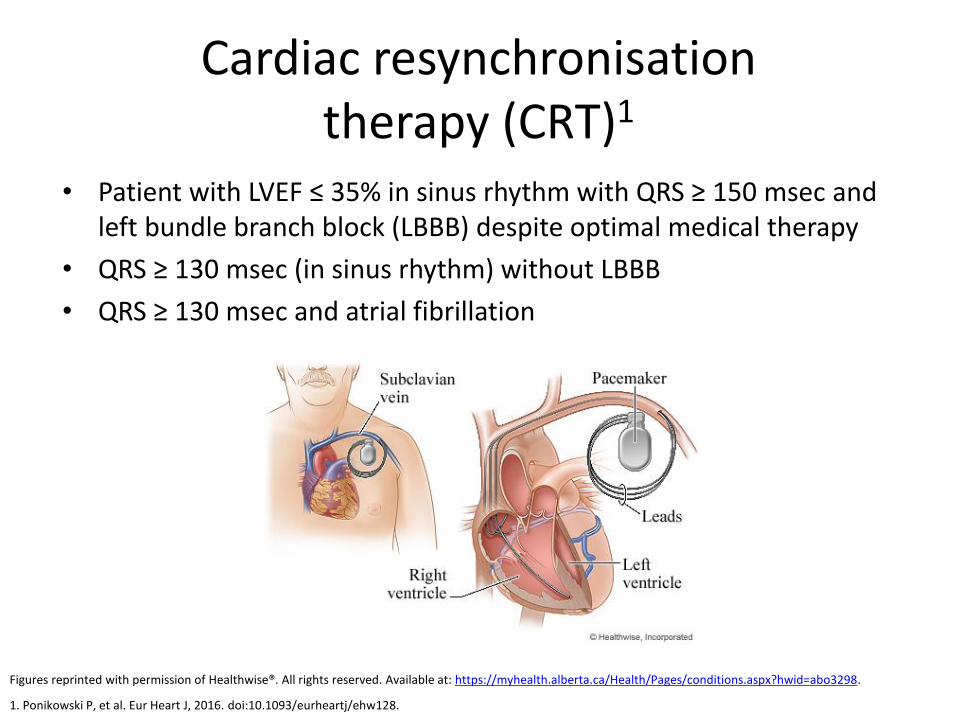
Cardiac resynchronisation therapy (CRT)1
• Patient with LVEF ≤ 35% in sinus rhythm with QRS ≥ 150 msec and left bundle branch block (LBBB) despite optimal medical therapy
• QRS ≥ 130 msec (in sinus rhythm) without LBBB
• QRS ≥ 130 msec and atrial fibrillation
1. Ponikowski P, et al. Eur Heart J, 2016. doi:10.1093/eurheartj/ehw128.
Figures reprinted with permission of Healthwise®. All rights reserved. Available at: https://myhealth.alberta.ca/Health/Pages/conditions.aspx?hwid=abo3298.

Left ventricular assist devices (LVAD)1
• End-stage: bridge to candidacy for transplant or bridge to transplant1,2
• Patients on LVAD have improved survival while awaiting transplant1
• Therapy is intended to be short-term, but due to long waits for organs the reality is that many patients will have lifelong LVAD1
1. Ponikowski P, et al. Eur Heart J, 2016. doi:10.1093/eurheartj/ehw128 2. Moss AJ, N Engl J Med. 2002; 346:877‒883. 2. National Heart Foundation of Australia. Guidelines for the prevention, detection and management of chronic heart failure in Australia. October 2011.
Figure reprinted with permission of Mayo Foundation for Medical Education and Research. All rights reserved. Available at: http://www.mayoclinic.org/tests-procedures/ventricular-assist-device/multimedia/left-ventricular-assist%20device/img-20006714.
Treatment of HF-PEF (LVEF ≥50%)
“No treatment has been shown, convincingly, to reduce morbidity or mortality in patients with HF-PEF...” 1
However
Despite the lack of “treatment” evidence, multidisciplinary management programs reduce mortality and hospitalisations regardless of the type of HF2
Recommendations for treating HF-PEF• Use treatment to improve QoL and alleviate symptoms1
• Diuretic therapy to improve congestion, symptoms, signs1
• Potential benefit for use of beta-blocker, MRA, ARB or ACEi1
• Treat cardiovascular and non-cardiovascular comorbidities:1
– AF: anticoagulant (avoid antiplatelet therapy in this population)
– Hypertension: treat according to hypertension guidelines– Diabetes: treat with metformin; some data exist for
empagliflozin– Exercise training: endurance/resistance training
1. Ponikowski P, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J, 2016. doi:10.1093/eurheartj/ehw128


ECHOCARDIOGRAPHY
Understanding Echo Reports
• Check date of study• Reason for test
– Laboratory best answer physician’s question– Type and diameter of prosthetic valves to quantify function– Results of previous studies help determine trends
• Image quality– Excellent, good, satisfactory– Difficult, fair or poor may lead to measurement errors
• Rate and Rhythm– AF, brady, or tachy interfere with functional assessment
• Chamber sizes• Hypertrophy
– Septal bulge common in elderly
• LV Systolic Function– Wall motion: global (CM) or regional (ischaemia)

Understanding Echo Reports
• LV diastolic dysfunction– Normal or Grade 1-4
• Valves– Morphology– Regurgitation or Stenosis
• Mass or thrombus– LAA not visualised on TTE
• ASD or VSD• Pericardium
– Thickened or calcified– Effusion
• Aortic dilatation or aneurysm• Incidental Findings
– Pleural effusions– Hepatic masses– Extracardiac mass compressing the heart
• Conclusions– Summary of important findings– Suggestions for follow-up or other investigations
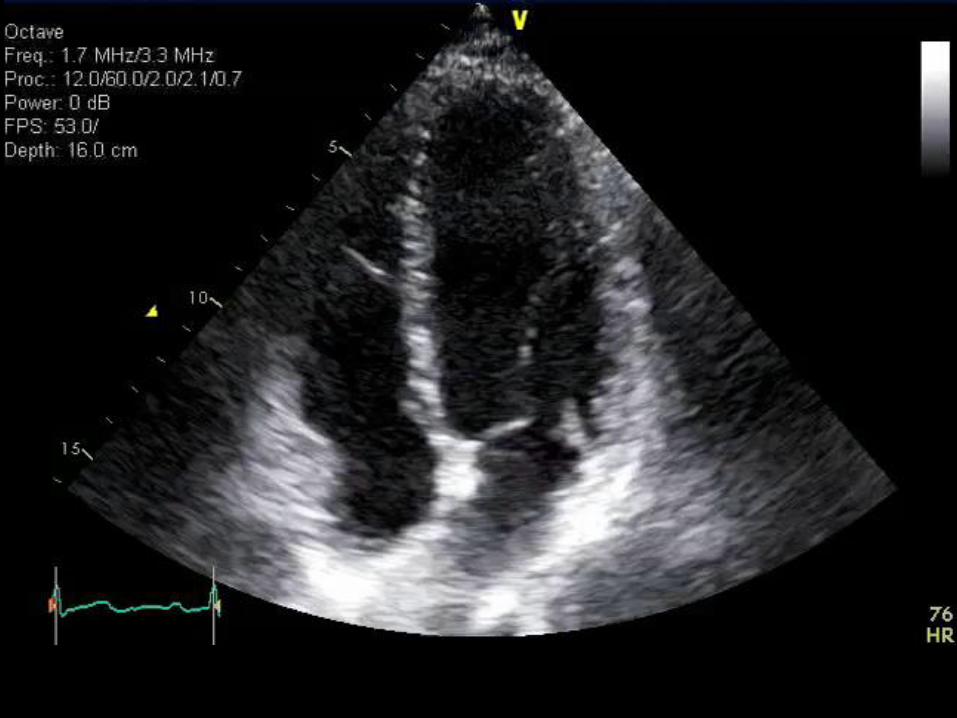
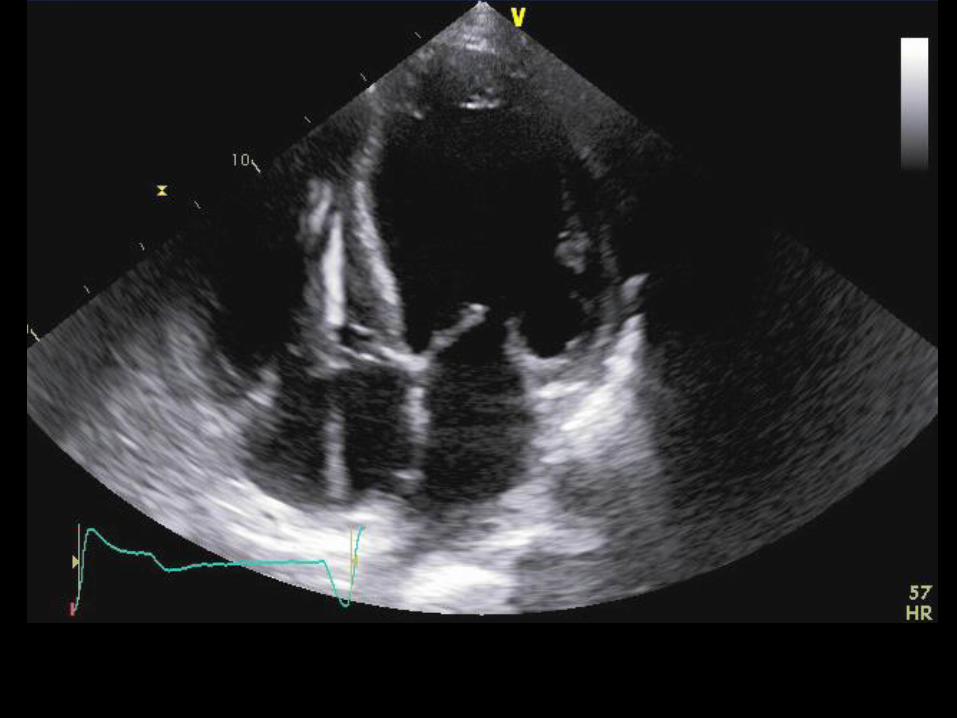

DIASTOLOGY
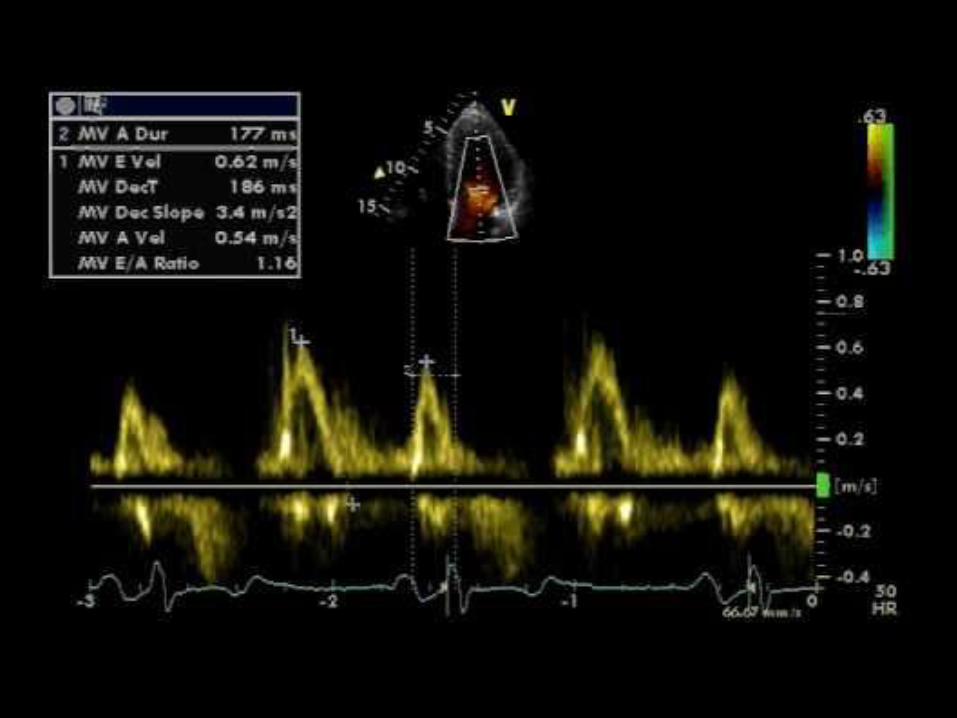

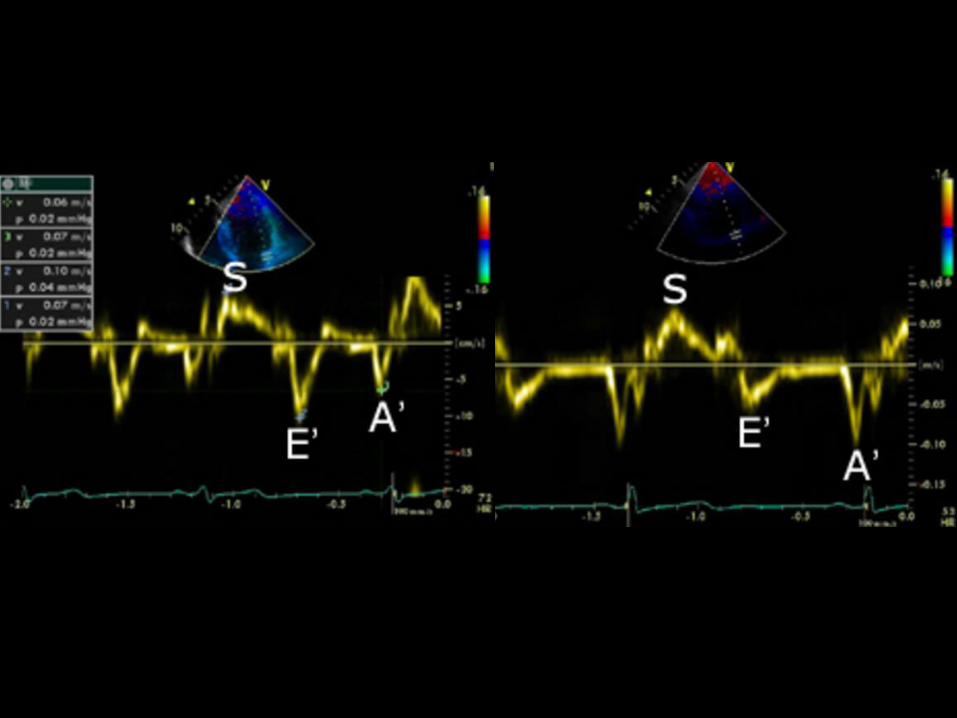
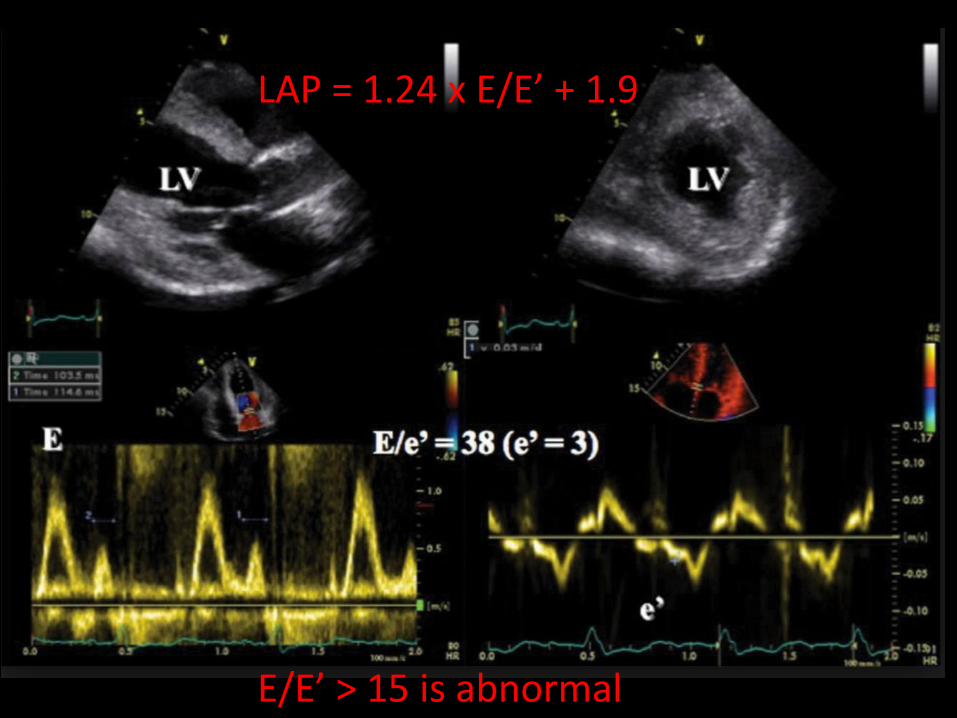
LAP = 1.24 x E/E’ + 1.9
E/E’ > 15 is abnormal
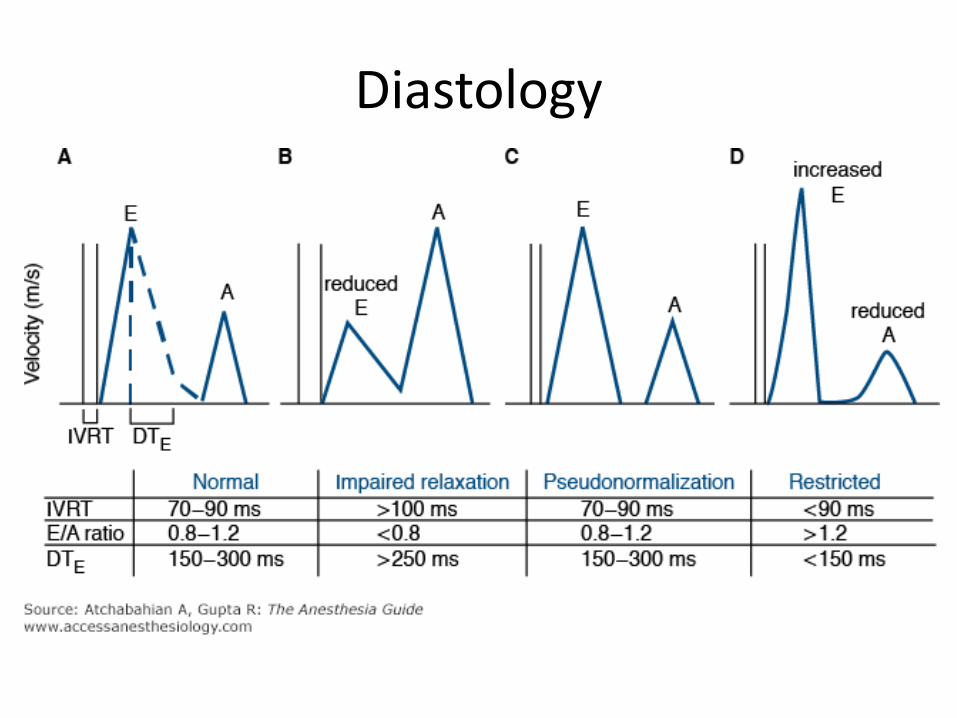
Diastology

INVESTIGATIONS


Biomarkers
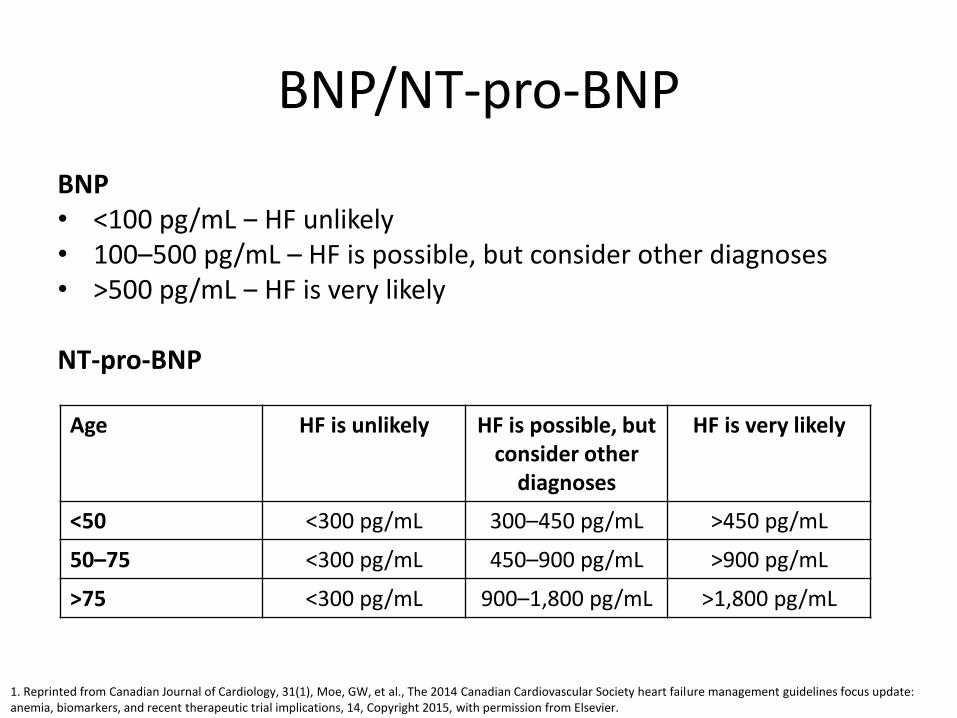
BNP/NT-pro-BNP
BNP• <100 pg/mL ‒ HF unlikely• 100–500 pg/mL – HF is possible, but consider other diagnoses• >500 pg/mL ‒ HF is very likely
NT-pro-BNP
1. Reprinted from Canadian Journal of Cardiology, 31(1), Moe, GW, et al., The 2014 Canadian Cardiovascular Society heart failure management guidelines focus update: anemia, biomarkers, and recent therapeutic trial implications, 14, Copyright 2015, with permission from Elsevier.
Age HF is unlikely HF is possible, but consider other
diagnoses
HF is very likely
<50 <300 pg/mL 300–450 pg/mL >450 pg/mL
50–75 <300 pg/mL 450–900 pg/mL >900 pg/mL
>75 <300 pg/mL 900–1,800 pg/mL >1,800 pg/mL

BNP/NT-pro-BNP
• When BNP/NT-pro-BNP levels are normal:– As an initial diagnostic test, especially when
echocardiography is not immediately available1
– As a rule-out test1
• When BNP/NT-pro-BNP levels are elevated:– Use to guide patient referrals for specialist assessment
(primary care)2
– Confirmatory imaging (as appropriate)• Echocardiography2
• CMR, tomography, angiography
1. Ponikowski P, et al. Eur Heart J. 2016; doi:10.1093/eurheartj/ehw128. 2. Chronic heart failure. Costing report, 2010. NICE clinical guideline 108. Available at: www.nice.org.uk/guidance/cg108/resources/costing-report-134800813.

Audience poll
Have you ever used BNP as part of HF monitoring?
No, this is only used in clinical trials
Yes, as part of a clinical trial
Yes, I use this marker in clinical practice
How might BNP guide treatment?
Determine treatment targets
Determine whether therapy has improved clinical status
Add a drug therapy based on lack of improvement in BNP
Adjust a dosage based on lack of BNP improvement
Predict worsening disease status or risk

Role of serum BNP, NT-pro-BNP in HF monitoring and follow-up
US guidelines1
• Measurement of BNP or NT-pro-BNP is useful to support clinical judgement for the diagnosis of HF
• Measurement of BNP or NT-pro-BNP is useful for establishing prognosis or disease severity in chronic HF and acutely decompensated HF
European guidelines2
• Measurement of natriuretic peptides can be used as an initial diagnostic test, especially in the non-acute setting when echocardiography is not immediately available
• Natriuretic peptides can identify those who require further cardiac investigations
1. Yancy CW, et al. 2013 ACCF/AHA guideline. Circulation. 2013; 128(16):1810–1852. 2. Ponikowski P, et al. Eur Heart J. 2016; doi:10.1093/eurheartj/ehw128.

Iron Deficiency
• Fe essential
– Oxygen uptake, transport and storage
– Oxidative metabolism in skeletal and cardiac muscle
– Erythropoiesis
• Clinical consequences in absence of anaemia
– Repletion of Fe in those without anaemia improves cognitive, symptomatic, and exercise performance.
CASE VIGNETTES
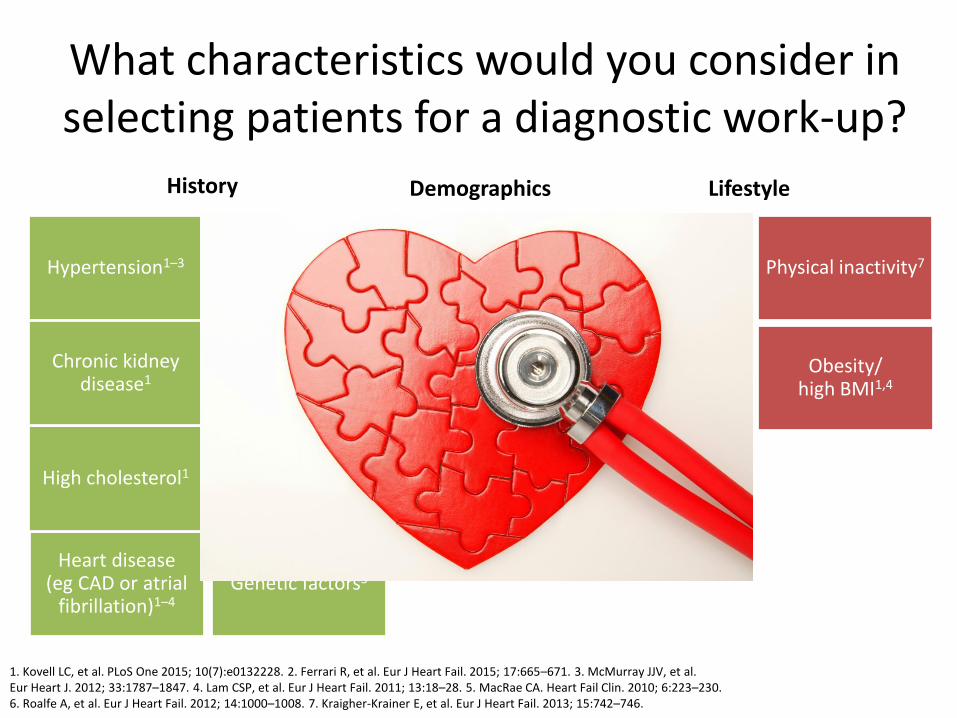
What characteristics would you consider in selecting patients for a diagnostic work-up?
Prior myocardial infarction (MI)1
Heart disease (eg CAD or atrial
fibrillation)1–4
Old age2
Gender (male: HF-REF6;
female: HF-PEF2)
Genetic factors5
Smoking1Hypertension1–3
High cholesterol1
Physical inactivity7
Obesity/high BMI1,4
High blood glucose/
diabetes1–4
High sodium intake1
Chronic kidney disease1
Alcohol use1,3Prior infection3
1. Kovell LC, et al. PLoS One 2015; 10(7):e0132228. 2. Ferrari R, et al. Eur J Heart Fail. 2015; 17:665–671. 3. McMurray JJV, et al. Eur Heart J. 2012; 33:1787–1847. 4. Lam CSP, et al. Eur J Heart Fail. 2011; 13:18–28. 5. MacRae CA. Heart Fail Clin. 2010; 6:223–230. 6. Roalfe A, et al. Eur J Heart Fail. 2012; 14:1000–1008. 7. Kraigher-Krainer E, et al. Eur J Heart Fail. 2013; 15:742–746.
History Demographics Lifestyle
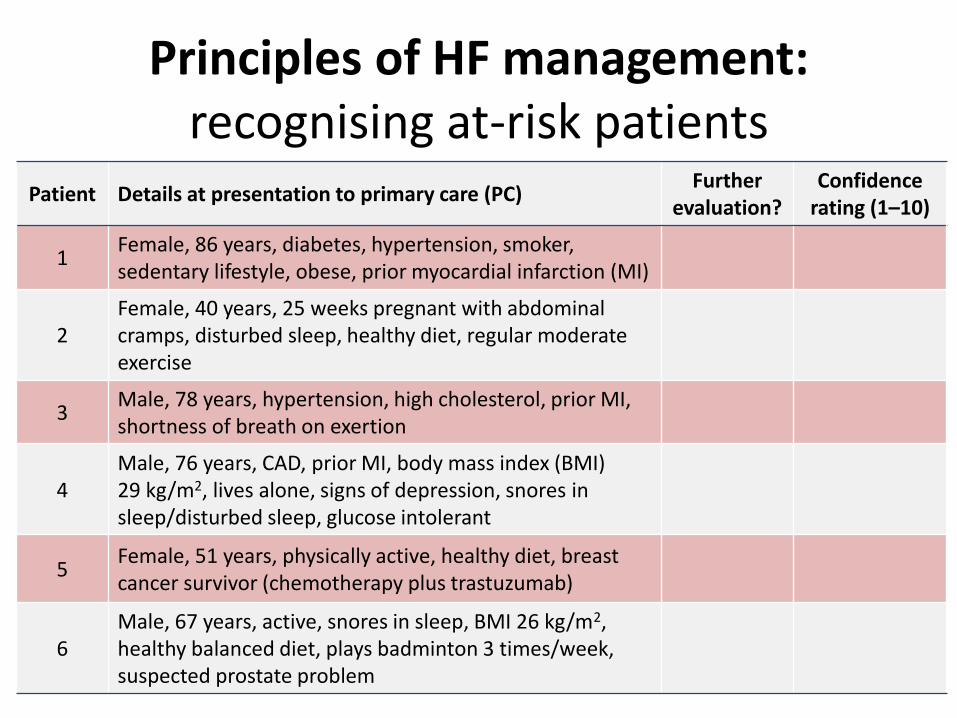
Principles of HF management:recognising at-risk patients
Patient Details at presentation to primary care (PC)Further
evaluation?Confidence
rating (1–10)
1Female, 86 years, diabetes, hypertension, smoker, sedentary lifestyle, obese, prior myocardial infarction (MI)
YES ?
2Female, 40 years, 25 weeks pregnant with abdominal cramps, disturbed sleep, healthy diet, regular moderate exercise
NO ?
3Male, 78 years, hypertension, high cholesterol, prior MI, shortness of breath on exertion
YES ?
4Male, 76 years, CAD, prior MI, body mass index (BMI) 29 kg/m2, lives alone, signs of depression, snores in sleep/disturbed sleep, glucose intolerant
YES ?
5Female, 51 years, physically active, healthy diet, breast cancer survivor (chemotherapy plus trastuzumab)
YES ?
6Male, 67 years, active, snores in sleep, BMI 26 kg/m2, healthy balanced diet, plays badminton 3 times/week, suspected prostate problem
NO ?
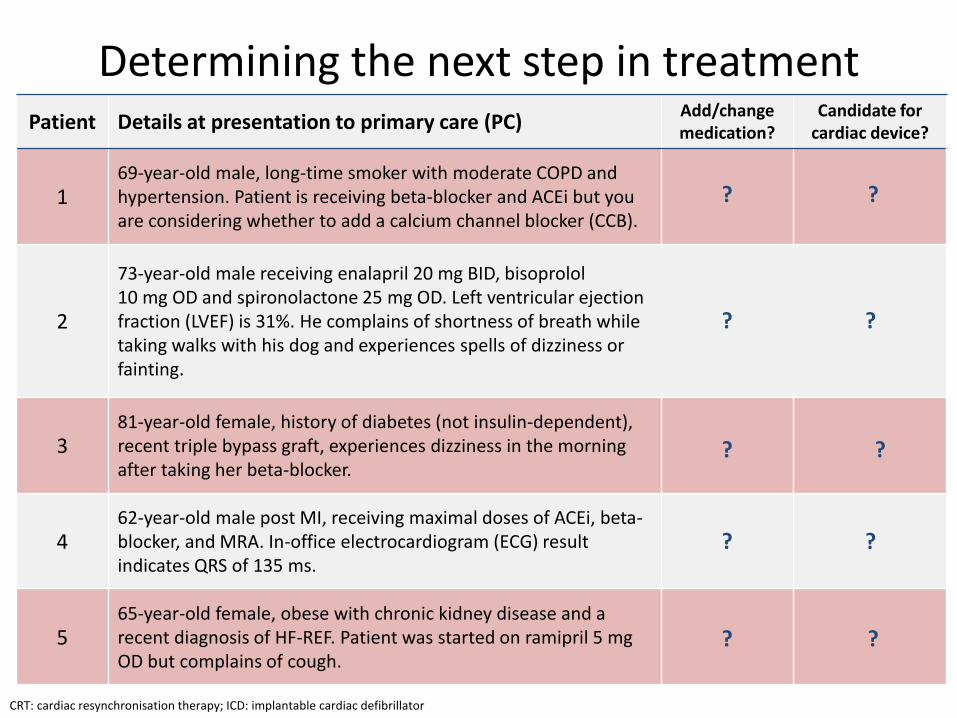
Determining the next step in treatmentPatient Details at presentation to primary care (PC)
Add/change medication?
Candidate for cardiac device?
169-year-old male, long-time smoker with moderate COPD and hypertension. Patient is receiving beta-blocker and ACEi but you are considering whether to add a calcium channel blocker (CCB).
Yes: increase ACEi dose or
add CCBNo
2
73-year-old male receiving enalapril 20 mg BID, bisoprolol 10 mg OD and spironolactone 25 mg OD. Left ventricular ejection fraction (LVEF) is 31%. He complains of shortness of breath while taking walks with his dog and experiences spells of dizziness or fainting.
Considerchanging
ACEi to ARNI if
hypertension persists
Yes: possibly ICD for primary prevention of sudden death
381-year-old female, history of diabetes (not insulin-dependent),recent triple bypass graft, experiences dizziness in the morning after taking her beta-blocker.
Possiblychange beta-blocker dose
No
462-year-old male post MI, receiving maximal doses of ACEi, beta-blocker, and MRA. In-office electrocardiogram (ECG) result indicates QRS of 135 ms.
NoYes: consider CRT if LVEF
<35%
565-year-old female, obese with chronic kidney disease and a recent diagnosis of HF-REF. Patient was started on ramipril 5 mg OD but complains of cough.
Yes: consider changing
medicationNo
? ?
??
? ?
? ?
? ?
CRT: cardiac resynchronisation therapy; ICD: implantable cardiac defibrillator
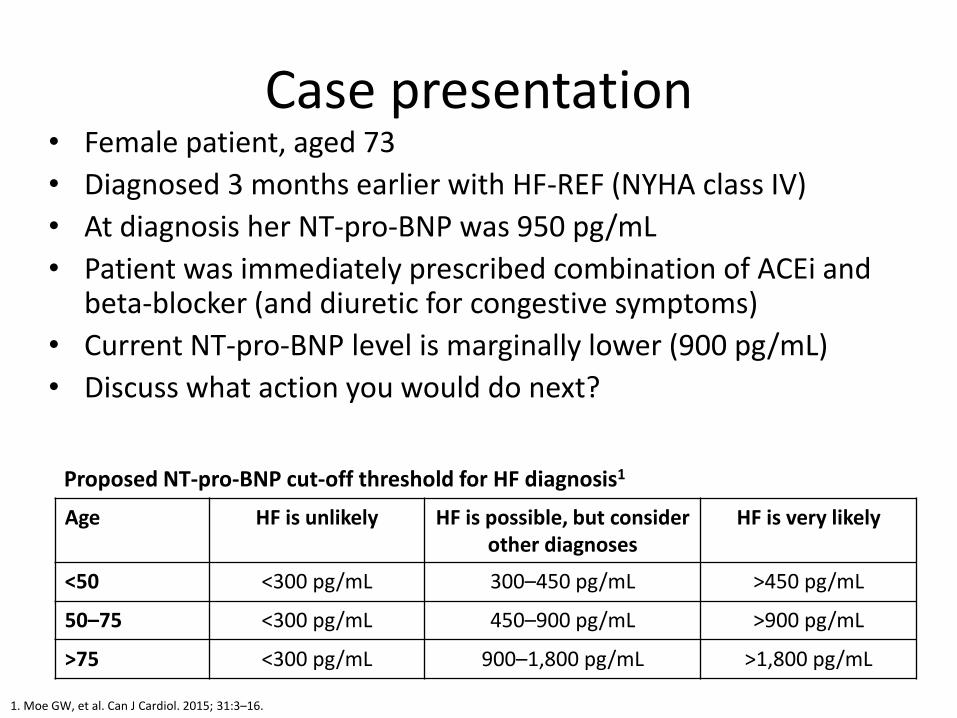
Case presentation• Female patient, aged 73
• Diagnosed 3 months earlier with HF-REF (NYHA class IV)
• At diagnosis her NT-pro-BNP was 950 pg/mL
• Patient was immediately prescribed combination of ACEi and beta-blocker (and diuretic for congestive symptoms)
• Current NT-pro-BNP level is marginally lower (900 pg/mL)
• Discuss what action you would do next?
Age HF is unlikely HF is possible, but consider other diagnoses
HF is very likely
<50 <300 pg/mL 300–450 pg/mL >450 pg/mL
50–75 <300 pg/mL 450–900 pg/mL >900 pg/mL
>75 <300 pg/mL 900–1,800 pg/mL >1,800 pg/mL
1. Moe GW, et al. Can J Cardiol. 2015; 31:3–16.
Proposed NT-pro-BNP cut-off threshold for HF diagnosis1

Comorbid conditions
Stage 3 kidney disease, insulin-dependent diabetes, BMI 24 kg/m2
Patient is currently taking maximum tolerated doses of ACEi and beta blocker and MRA (spironolactone)
Recent hospitalisations for worsening symptoms, significant hepatic congestion
History of sick sinus node syndrome
• Are beta-blockers contraindicated in this patient?• How should therapy be adjusted to account for kidney disease?• If the patient develops microalbuminuria, what course of action should
be taken? Should the patient be taken off any of his medications?
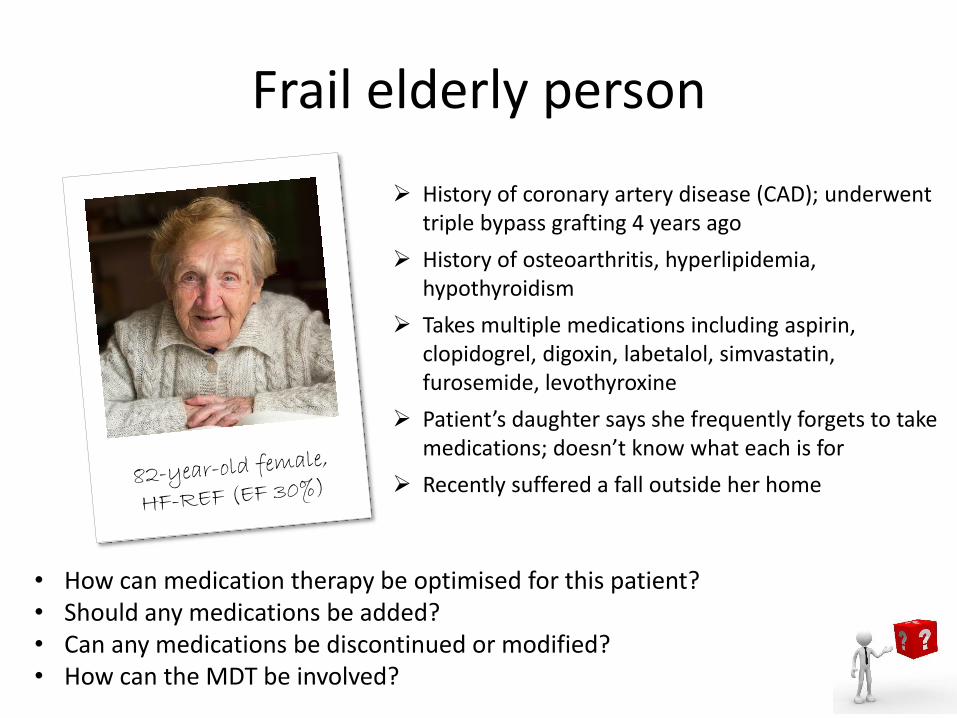
Frail elderly person
History of coronary artery disease (CAD); underwent triple bypass grafting 4 years ago
History of osteoarthritis, hyperlipidemia, hypothyroidism
Takes multiple medications including aspirin, clopidogrel, digoxin, labetalol, simvastatin, furosemide, levothyroxine
Patient’s daughter says she frequently forgets to take medications; doesn’t know what each is for
Recently suffered a fall outside her home
• How can medication therapy be optimised for this patient?• Should any medications be added?• Can any medications be discontinued or modified?• How can the MDT be involved?

Case study: Is this patient decompensated?
• Patient previously diagnosed with HF who presents to her PCP with progressive dyspnoea, chest pain and orthopnoea over previous 2 weeks
• Examination reveals normal body temp, rapid breathing, low volume pulse, BP 110/70, evident sacral oedema, pansystolic murmur and late inspiratory crackles noted in both lungs
73-year-old female with prior MI and
HF diagnosis
What tests will you order?
Complete blood count (CBC) with electrolytes
Serum brain natriuretic peptide (BNP)
Electrocardiogram (ECG)
Echo
Troponin
Other
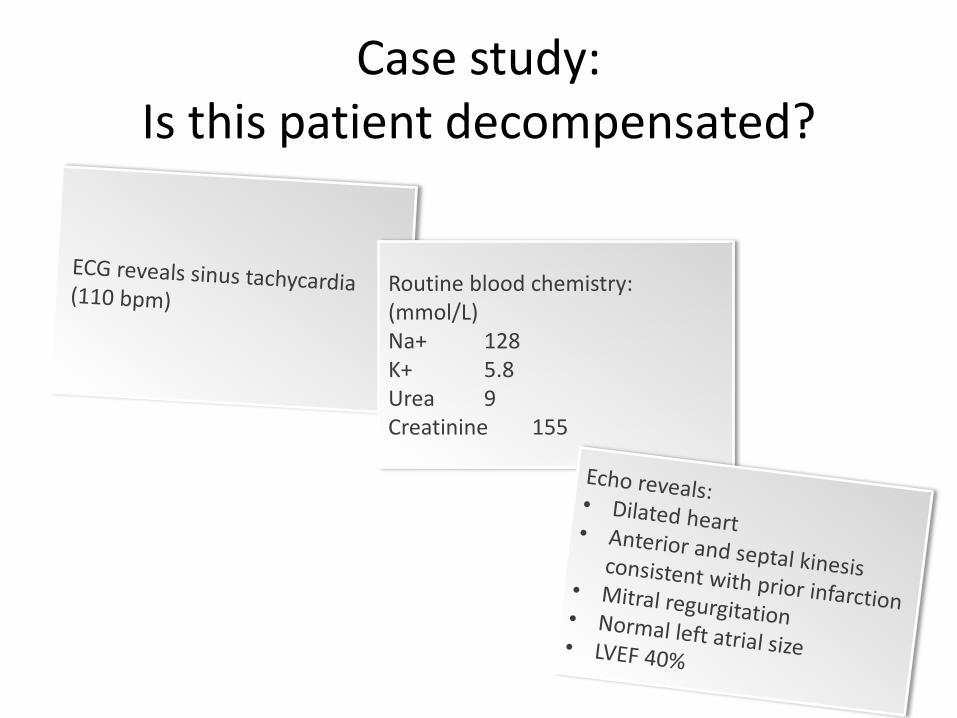
Case study: Is this patient decompensated?
Routine blood chemistry: (mmol/L)Na+ 128K+ 5.8Urea 9Creatinine 155
Case study: Is this patient decompensated?
What does your evaluation suggest? (Select all that apply)
Acute decompensated HF
Stable HF
Does the ECG result suggest a cardiac cause for the patient’s dyspnoea symptoms?
Yes
No
Not enough information to decide
What course of action would you take?
Hospitalise the patient
Change therapies Consider ______
Case study: Frail, elderly patient
Known comorbid conditions: • Hypertension, coronary artery disease
(history of triple-vessel bypass graft), osteoarthritis, hyperlipidaemia and renal dysfunction
Medications:• ACEi (lisinopril), beta-blocker
(carvedilol), antithrombotic (aspirin, clopidogrel), statin (simvastatin), diuretic (furosemide), inhaled corticosteroid/long-acting beta-agonist (fluticasone/salmeterol)
84-year-old male with HF and EF 30%

Case study: Frail, elderly patient
Slight weight loss since last visit 3 months ago
No chest pain or shortness of breath reported
Case study: Frail, elderly patient
Can therapy be optimised per evidence-based guidelines?
Add therapies
Discontinue therapies
Adjust therapies
Should further evaluations be considered?
Can proactive steps can be taken to prevent clinical event or worsening?
What advice can you give the patient and his caregivers?

How would you adjust therapies for these patients?
Anaemia
Determine underlying cause of anaemia (kidney disease, iron deficiency)
Testing: CBC, iron, ferritin, reticulocytes, faecal occult blood
Is oral iron supplementation sufficient? Is IV indicated?
Chronic kidney disease (CKD)
Use loop diuretic rather than thiazide diuretic for treating hypertension
Avoid aldosterone blockers (eg spironolactone) in severe CKD due to rise in potassium
ACEis and ARBs can be used in mild CKD. How should therapy be adjusted in case of rising serum creatinine?
How should beta-blocker doses be adjusted in CKD?
Presenting symptoms
• 6-week history of shortness of breath when trying to walk his dog
• 4-week history of swollen ankles
Background
• 67-year-old retiree, widowed and lives alone. Children live interstate
Medical history
• MI (18 months ago)
• Hypertension – diagnosed 2005
• Obese (weight 109 kg, BMI 36, Waist 110 cm)
• Osteoarthritis – diagnosed 2010
• Ex-smoker
• quit at 60 (~40 pack/year smoker)
BMI: body mass index; GP: general practitioner; MI: myocardial infarction.
GRAHAMPRESENTED TO HIS GP
GRAHAMPRESENTED TO HIS GP
Clinical examination
• BP 148/95
• HR 90
• Bilateral pitting oedema to knees
• JVP is elevated at 6 cm
• Lungs are clear to auscultation
• Soft systolic murmur audible on auscultation of heart sounds
• Abdominal examination non-contributory
Medications at presentation
• CCB/Statin – High/Mid
• NSAID - Salicylates
• ACEi – High dose
• NSAID – COX 2 selective
• Benzodiazepine PRN
BP: blood pressure; GP: general practitioner; HR: heart rate; JVP: jugular venous pressure; PRN: when required.
DOES GRAHAM HAVE HEART FAILURE?
WHAT ARE YOUR NEXT STEPS FOR GRAHAM?
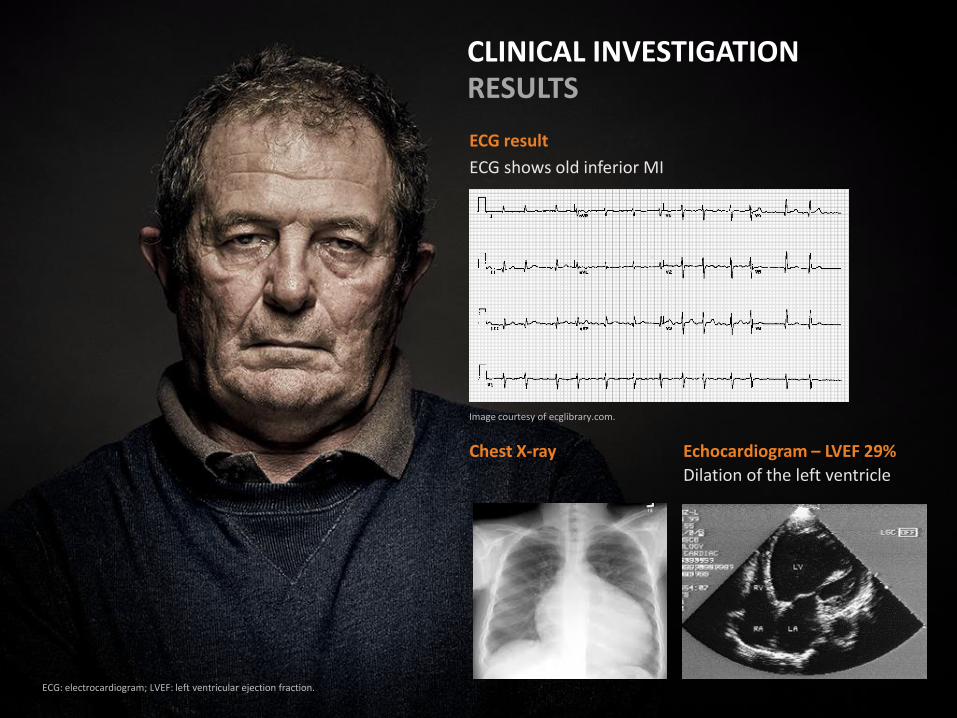
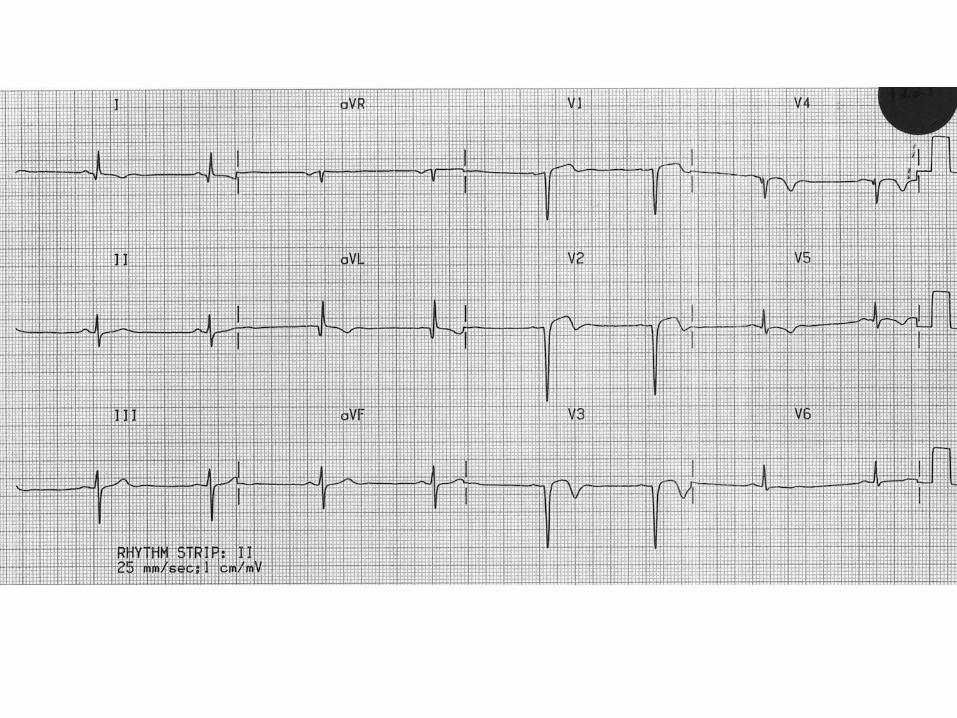
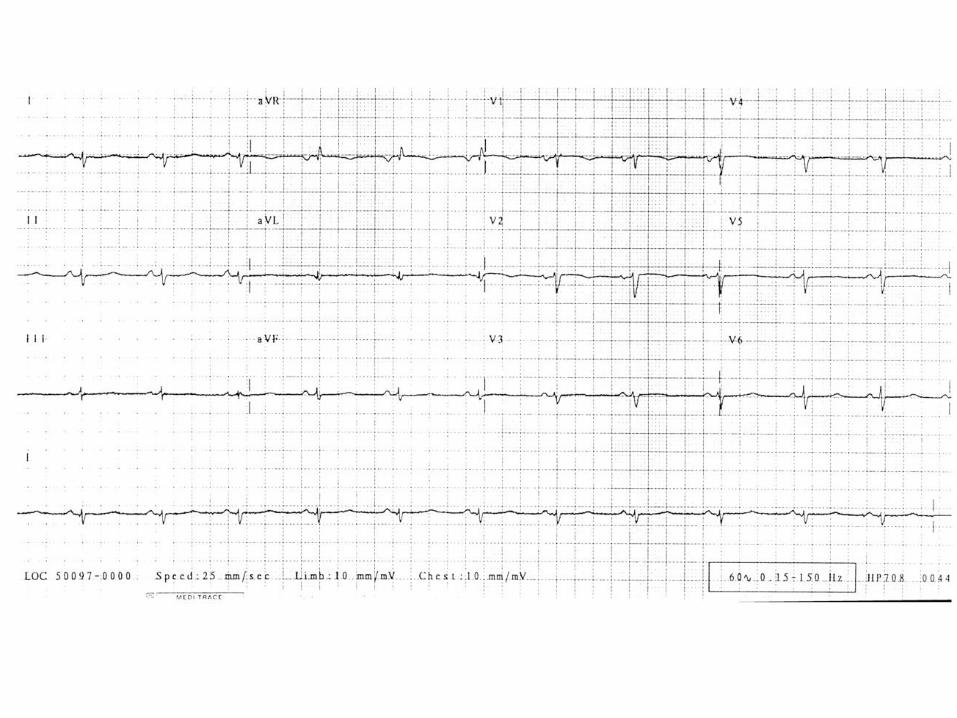
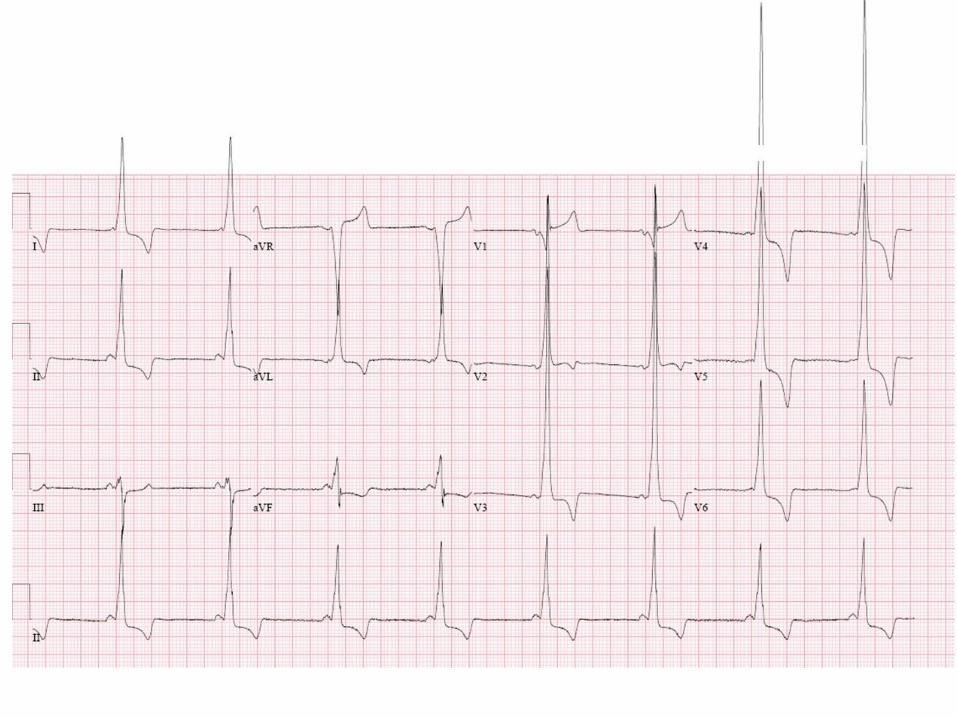
ECG result
ECG shows old inferior MI
CLINICAL INVESTIGATION RESULTS
Chest X-ray Echocardiogram – LVEF 29%
Dilation of the left ventricle
ECG: electrocardiogram; LVEF: left ventricular ejection fraction.
Image courtesy of ecglibrary.com.

WHAT IS YOUR DIAGNOSIS?
HEART FAILURE WITH REDUCED EJECTION FRACTION

WHAT NON-PHARMACOLOGICAL AND PHARMACOLOGICAL INTERVENTIONS SHOULD BE INITIATED WITH GRAHAM?
Background
• 67-year-old retiree, widowed and lives alone. Children live interstate.
Medical history
• MI (18 months ago)
• Hypertension – diagnosed 2005
• Obese (weight 109 kg, BMI 36, Waist 110 cm)
• Osteoarthritis – diagnosed 2010
• Ex-smoker
• quit at 60 (~40 pack/year smoker)
Medications at presentation
• CCB/Statin – High/Mid dose
• NSAID - Salicylates
• ACEi – high dose
• NSAID – COX 2 selective
• Benzodiazepine PRN
Clinical investigations confirmed heart failure with reduced ejection fraction
BMI: body mass index; MI: myocardial infarction; PRN: when required.
GRAHAM IS NOW TREATED WITH GUIDELINE-RECOMMENDED THERAPIES
Current medications
• ACEi – High dose
• β – Blocker – Cardio selective- Mid dose
• Diuretic - Low dose
• MRA - Low dose
• CCB/Statin – High/Mid dose
• NSAID - Salicylate
• Simple analgesic
• Benzodiazepine PRN
Non-pharmacological interventions
• Exercise phys. and dietician referral
• Fluid restriction
• Salt restriction
• Daily weighing
• Weight loss advised
MR: modified release; PRN: when required.
WHAT ARE THE GOALS FOR GRAHAM’S ONGOING MANAGEMENT?
• Multidisciplinary care?
• Self-care?
• Medication optimisation?
• Management of co-morbidities?
• Any others?

• Free, expert-led education in heart failure• Designed for the whole multidisciplinary team: cardiologists, GPs,
nurses and any healthcare professionals involved in the management of heart failure
• Small, local and highly interactive roundtable meetings • For more information visit: www.corehearteducation.com
Register here: mms.corehearteducation.com
CORE is supported by funding from Novartis Pharma AG. All educational content and materials are created by the CORE Steering Committee in collaboration with PCM Scientific, the medical education company acting as secretariat. The financial supporter has had no involvement in the creation or development of the educational content.

• Increasing prompt diagnosis of heart failure• Improving the use of appropriate intervention in heart failure• Improving disease management through better comorbidity
competence• Increasing multidisciplinary collaboration and communication
including referral to, and interaction with, cardiac rehabilitation and palliative care services
• For more information visit:
www.corehearteducation.com

• Introduction to heart failure• Diagnosis of heart failure• Planning and initiating treatment in heart failure• Monitoring and adapting treatment in heart failure• Long-term management of heart failure• Working together in heart failure management
• For more information visit:
www.corehearteducation.com





























