-
90MedGenet 1997;34:990-995
BRCA1 and BRCA2 mutation analysis in 86 earlyonset
breast/ovarian cancer patients
Alex M Garvin, Michele Attenhofer-Haner, Rodney J Scott
Human Genetics,Department ofResearch,Kantonsspital Basel,Basel
4031,SwitzerlandA M GarvinM Attenhofer-HanerR J Scott
Correspondence to:Professor Scott, Hunter AreaPathology Service,
LockedBag No 1, Hunter RegionalMail Centre, New SouthWales 2310,
Australia.
Received 28 May 1997Revised version accepted forpublication 23
July 1997
AbstractEighty-six women fulfilling specific selec-tion criteria
were studied for germlinemutations in two breast cancer
suscepti-bility genes, BRCA1 and BRCA2, usingthe protein truncation
test (PTT). Ninegermline mutations were identified, six inBRCA1 and
three in BRCA2. Of the sixBRCA1 mutations, three have
previouslybeen described and three are new, and forBRCA2, one is a
new mutation and theother two appear to occur at a site that
hasbeen described several times. Four kin-dreds were breast cancer
families, one abreast/ovarian cancer family, and thesixth an
ovarian cancer family. The threekindreds with BRCA2 mutations
wereclassified as one breast/ovarian cancerfamily, one breast
cancer family, and onefamily which harboured one early onsetbreast
cancer patient and two melanomapatients. The mutations in BRCA1
wereeither insertions, deletions, or transitionswhich all resulted
in a premature stopcodon. Mutations in BRCA2 were allframeshift
mutations as a result ofeither 2or 4 bp deletions. Two BRCA2
mutationswere identical, suggesting a Swiss foundereffect which was
confirmed by haplotypesharing. The 10% mutation detection rateis
compatible with the relaxed criteriaused for patient selection.
Considering therelative ease with which coding sequencescan be
screened by PTT, this assay is use-ful as a first screen for BRCA1
andBRCA2 mutations.(7Med Genet 1997;34:990-995)
Keywords: breast cancer; BRCA1; BRCA2; genetics
The most consistent factor associated with awoman's risk of
developing breast cancer is afamily history of disease. Hereditary
breastcancer is characterised by early onset, an excessof bilateral
disease, and in some families anover-representation of ovarian
cancer. Epide-miological studies have pointed to the exist-ence of
several breast cancer susceptibility
BRCA22 4 6
1 3 5 7
genes, two of which have been recently identi-fied, termed BRCA1
and BRCA2.' 2The locus for BRCA1 was identified in 1990
and the gene identified by positional cloningfour years later. '
The BRCA2 locus was iden-tified in 1994 and the gene identified
in1995.24 BRCA1 confers a lifetime risk ofapproximately 85% of
developing breast cancerand a 50% risk of developing ovarian
cancer.5BRCA2, however, confers a similar risk forbreast cancer
development but a different life-time risk of developing ovarian
cancer (onlyabout 10%) in comparison to BRCA1. Inaddition, BRCA2
appears to be associated withan increased risk of male breast
cancer whereasBRCA1 does not.6 It is currently not clear ifgermline
mutations in BRCA2 confer anincreased risk of cancers other than
breast andovary.The BRCA1 gene is located on chromosome
17q21 and codes for a 7.5 kb transcript whichis spread across
100 kb of genomic DNA. Thegene consists of 24 exons of which 22 are
cod-ing. The first 10 and last 13 exons are relativelysmall whereas
exon 11 represents over 60% ofthe entire coding sequence. The gene
codes fora 1863 amino acid zinc finger containingprotein of unknown
function, which hasrecently been shown to interact with
anadditional protein termed BARD1. Missensemutations in BRCA1
disrupt binding toBARD 1, suggesting that interaction withBARD 1 is
important in regulating BRCA1function.8 Eighty-six percent of BRCA1
muta-tions are either nonsense or frameshift muta-tions which
result in prematurely truncatedproteins that lead to a disruption
of BRCA1function.9BRCA2 is located on chromosome 13q1 2-13'
and codes for a 10.5 kb transcript. The geneconsists of 27 exons
and, like BRCA1, the first10 and last 16 exons are relatively
shortwhereas exon 11 represents approximately50% of the coding
sequence. The function ofthe gene remains elusive but the sequence
doeshave some similarities to BRCA1. Similar toBRCA1, most BRCA2
mutations result in pre-mature termination codons.
In this report we have investigated 86 earlyonset breast/ovarian
cancer patients for muta-tions in BRCA1 and BRCA2 using the
proteintruncation test (PTT). We have identified sixmutations in
BRCA1 and three mutations inBRCA2. All families harbouring
BRCA1mutations presented with typical disease char-acteristics for
this breast/ovarian cancer predis-position. Two of the three
families harbouringBRCA2 mutations presented with early onset
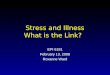
Exons 2-10 Exon 11 Exons 12-27
Figure 1 Diagrammatic representation of the coding sequence
ofBRCA2 indicating theseven overlapping segments that were
amplified using the primer sequences indicated intable 1.
990
on June 5, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.34.12.990 on 1 D
ecember 1997. D
ownloaded from
http://jmg.bmj.com/
-
BRCA1 and BRCA2 mutation analysis in early onset breastlovarian
cancer patients
Table 1 BRCA2 primers
Segment 5' 3' Size (bp)
1 external gccgggagaagcgtgagggg (101-120) tggtggtggctggccagctt
(1930-1911)1 internal T7-cctattggatccaaagaga (232-250)
tggtggtggctggccagctt (1930-1911) 17362 external
gaagatagtttttcattatg (1141-1160) cctttctattagctacttggaaag
(2922-2901)2 internal T7-aaaaatctacaaaaagtaaga (1180-1200)
gagaaaagttcttcagagtctgg (2879-2857) 17373 T7-ggtttattgcattcttctgtg
(2137-2157) ttctttaatctgagtgtttc (4374-4355) 22754
T7-ccaagctacatattgcagaag (3625-3645) ctcgttgtmttccttaatta
(5865-58460) 22785 T7-tcaaaaagtatctttttgaaa (5116-5136)
cccactaagataaggggctc (7070-7051) 11926 external
tctgtccaggtatcagatgc (6181-6200) ctcttttgttgggcctccac (8810-8791)6
internal T7-accaggcaagtcrtttccaaa (6247-6268) agatgatgtcttctccatcc
(8736-8717) 25277 external gaagattamtggtaagga (7921-7940)
cgctgaggtaaamgaaac (10620-10600)7 internal T7-ctcataccctccaatgatgg
(7987-8006) ggtttgaaattatattccag (10560-10541) 2611
The numbers in parentheses refer to the positions according to
Tavtigian et al,22 Genbank accession number U43746.
breast cancer and one case of ovarian cancer.The proband of the
third BRCA2 familypresented with early onset breast cancer andhad a
family history of skin cancer rather thanbreast cancer.
Patients and methodsPatients were ascertained as they
presentedwith disease at various clinics throughout theGerman and
Italian speaking parts of Switzer-land. At the time of diagnosis
the patients wereasked if they would be willing to participate ina
genetic screening study of BRCA1 andBRCA2 if they fulfilled any of
the followingminimum criteria: any woman under 40 yearsof age with
breast cancer and no other affectedfirst or second degree
relatives; any womenunder 50 years of age with a first degree
relativealso under 50 years of age with breast cancer;any woman
under 50 years of age with breastcancer and a first degree relative
with ovariancancer at any age; any woman with ovariancancer with a
first degree relative with ovariancancer at any age; any women with
bilateralbreast cancer both of which were identifiedbefore the age
of 60 years; and any women withbreast and ovarian cancer. Disease
status inprobands and affected relatives was confirmedin the
majority of patients by pathology reportsand in those cases where
these were unavailableby death certificates. All women entering
intothis study signed an informed consent declara-tion.
TEMPLATE PREPARATIONFor genomic DNA, patient peripheral
bloodlymphocytes (PBLs) were prepared from 10 mlEDTA blood and DNA
was isolated using thesalting out procedure.'0 Total RNA was
pre-Table 2 Summary of breast and ovarian cancer patientsin the
families of the 86 breast cancer patients
Index No of relanves No offamilies
Bilateral Brca
-
Garvin, Attenhofer-Haner, Scott
Table 3 BRCAl and BRCA2 mutations andfamily characteristics
Family Gene Exon Nucl cha-nge aa change Type Brca (age) * Ovca
(age) * Other
1686 BRCA1 1 11136insA 345 ter F - 5 (43-70)1604t BRCA1 11
61ldelC 502 ter F 5 (41-42) -1560t BRCA1 11 1648C- G Ser51OStop N 5
(33-42) -1564 BRCA1 11 2804delAA 901ter F 3 (33-59) 2 (37, 64)1668
BRCAI 11 3039delTT 990ter F 4 (40-65) 2 (?,?) Liver1540t BRCA1 11
3449insA 1114ter F 4 (39-48)0323 BRCA2 11 3036delACAA 958ter F 4
(31-60) - Testis1649 BRCA2 11 3036delACAA 958ter F 3 (35)41353
BRCA2 14 7297delCT 2358ter F 1 (32) - 2 mel
N=nonsense mutation, F=frameshift mutation, del=deletion,
ins=insertion, mel=melanoma.*When more than two patients affected,
age is given as a range.tReported previously."1tAge of the two
other relatives unknown.
testing on 63 women have previously beenreported but were
included in this study sinceBRCA2 analysis had not been performed.
Asummary of their family histories is shown intable 2.Both cDNA and
genomic DNA were used
for mutation detection studies. All samplesshowing premature
termination codons wereverified by direct sequencing of genomicDNA.
Two mutations were identified incDNA and the remaining in genomic
DNA. Asummary of all mutations identified is shownin table 3.BRCA1
analysis of the 23 women not
included in our previous study" showed threeadditional mutations
which were spreadthroughout exon 11 of BRCA1. The
mutationidentified in family 1668 was a 2 base pair (bp)deletion at
bp 3037 which resulted in a prema-ture stop at bp 3091. The family
history isremarkable in that there are two early onsetovarian
cancer patients, five early onset breastcancer patients, and one 50
year old liver can-cer patient who was unavailable for testing.
Inaddition, two unaffected carriers were identi-fied, one male
(aged 45 years), the other female(aged 42). Affected persons in
family 1564harboured a 2 bp deletion at position 2804which results
in a premature stop codon 18 bplater. This mutation has been
reported previ-ously but not published. Affected family mem-bers
all presented with breast cancer under theage of 60 years; however,
two of themdeveloped ovarian cancer at the ages of 37 and64 years.
As with the previous family, twounaffected carriers were
identified, one male(aged 27), the other female (aged 20).
Oneovarian cancer family without breast cancerwas also included in
this study. The mutationidentified in this family (1686) was an A
inser-tion at position 1129 ofBRCA1 which resultedin a stop codon
17 bp downstream and has not
Table 4 Haplotype sharing at the BRCA2 locus in families 0323
and 1649
Family 0323 Family 1649
Markers 1 2 3 4 5 6 7
D13S289 1 2 1 2 4 4 1 4 1 4 1 4 2 4D13S290 1 4 1 4 3 1 3 1 3 3 2
1 1 1D13S260 2 3 2 3 1 2 1 3 6 6 1 3 1 3D13S171 2 5 2 5 2 2 1 4 4 4
1 4 2 4 BRCA2D13S267 3 4 3 4 1 4 4 1 1 1 1 1 4 1
Patients 1-6 belong to family 0323 as indicated in fig 2A and
patient 7 belongs to family 1649 (fig2C). Common alleles in persons
harbouring the delACAA mutation (underlined) can be seenwithin
family 0323 which are present in patient 7 (family 1649).
Segregating alleles for markerDl 3S260 could not be determined, so
both alleles are underlined.
been reported previously. All patients withinthis family
presented with ovarian cancerunder the age of 70 years, the
youngest ofwhom was only 43 years of age whendiagnosed.
Since 80 of the selected families meeting ourinclusion
requirements did not appear toharbour mutations in BRCA1, BRCA2
screen-ing was performed. Three families were identi-fied as having
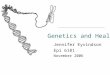
mutations in BRCA2. Affectedpersons in family 0323 harbour a 4 bp
deletion(ACAA) at position 3036 which results in astop codon 67 bp
downstream.Three patients with early onset breast
cancer harboured the 4 bp deletion and anobligate carrier was
identified who died ofovarian cancer three years after her
diagnosisat 66 years of age. In addition, a 60 year oldsister of
the ovarian cancer patient wasdiagnosed with breast cancer but did
not har-bour the mutation nor did her 40 year old sonwho suffered
from testicular carcinoma (fig2A). Family 1649 (fig 2B) harboured
an iden-tical mutation to that found in family 0323which was
associated only with early onsetbreast cancer. In this family,
three generationsofwomen developed early onset breast cancer.The
paternal grandmother of the proband alsodeveloped breast cancer
albeit at a later age,but she was unavailable for testing.
Haplotypeanalysis showed that these two families arerelated, as
common alleles were sharedbetween affected persons (table 4). The
muta-tion found in families 0323 and 1649 is simi-lar to that
reported previously" 2 in that itoccurred in a string of adenine
bases. Theexact location of the mutation, however, isimpossible to
determine since the surroundingsequence (GTGATAAACAAGCAA) does
notallow the differentiation between a deletionstarting at position
3034, 3035, or 3036.A 2 bp deletion at position 1297 in exon 14
ofBRCA2 resulting in a premature stop codon3 bp downstream of
the mutation was identi-fied in the index patient from family 1353
andis a new mutation. This woman was the onlybreast cancer patient
in the family (fig 2C).Additional family members suffered fromother
malignancies which included twomelanoma patients, one of whom
developeddisease at 30 years of age, and one basal cellcarcinoma
patient. Unfortunately, none ofthese patients was available for
analysis.
992
on June 5, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.34.12.990 on 1 D
ecember 1997. D
ownloaded from
http://jmg.bmj.com/
-
BRCA 1 and BRCA2 mutation analysis in early onset breastlovarian
cancer patients
A0323
Breast cancer 60 AbdominalHaplotyped disease
BRCA2 mutation -ve
Testicularcancer 40
B1649
Abdominalcancer
Suicide Infarct, Suicide, Ovarian Breast cancer 62 Spinal
Liver64 23 cancer 66 Haplotyped cord cancer
BRCA2 mutation -ve tumour, 4564
Suicide Breast cancer 48 Breast cancer 45 Oestrogen
BilateralHaplotyped Haplotyped \disorder breastBRCA2 BRCA2
cancer,
mutation +ve mutation +ve HaplotVped 31, 43BRCA2
Haplotypedmutation BRCA2
-ve mutation+ve
1353
Breast Breastcancer cancer
Breast Melanoma 30 Melanoma 65 Basal cellcancer carcinoma,
died at 60
Breast cancer 35 BreastHaplotyped cancer 32
BRCA2 mutation +ve
Figure 2 The three pedigrees with BRCA2 mutations. Persons
usedfor haplotyping analysis are as indicated. Those persons with
an asterisk above theirsymbol are the index patientsfrom each of
the families and have the same BRCA2 mutation (indicated as BRCA2
+ve). Age of diagnosis is indicatedwhere known.
DiscussionMost studies on breast cancer families havefocused on
large informative families wherethere is reasonably good pedigree
data. Rela-tively little is known about persons who haveminimal
family history of disease but havedeveloped disease at an unusually
early age. Inthis study we have addressed this issue byincluding in
the study persons who fulfil aminimal criteria. The carrier
frequency forBRCA1 is 1:833'3 and BRCA2 is approxi-mately the
same,6 suggesting 1:400 people inthe general population are
carriers. The twogenes are expected to account for approxi-mately
10% of the breast cancer cases under 45years of age.14 Therefore it
is to be expectedthat approximately half of the mutations wouldbe
the result of BRCA1 and half BRCA2. Inthis study the ratio of BRCA1
to BRCA2mutations was 3:1, indicating that BRCA1 ismore frequent in
the Swiss population thanBRCA2. Since, however, only a few
mutationswere detected, this result may be inaccurateowing to
sample size.
Because of the size of BRCA1 and BRCA2,efficient screening of
both genes remains prob-lematical. The PTT represents a relatively
use-ful alternative to more labour intensive screen-
ing strategies in that large amounts of codingsequence can be
quite rapidly examined. Amajor advantage of this method, in
comparisonto other detection strategies, is that anychanges
observed are likely to lead to a loss offunction. In this report
cDNA was used astemplate for the PTT which is generated frommRNA by
reverse transcriptase. Mutant mes-sage may be susceptible to the
actions of non-sense mediated decay and therefore may not
berepresented to the same extent as normalmessage" which would
result in the apparentabsence of detectable truncated products
bythe PTT. This, we believe, is unlikely sincebefore starting this
study we investigatedlymphoblastoid cell lines with known
muta-tions that had previously been reported asbeing susceptible to
the actions of nonsensemediated decay. These studies indicated that
aslong as mRNA was isolated from lymphocytesimmediately after
phlebotomy, sufficient mu-tant message was present for cDNA
conversionand hence mutation detection (results notshown). An
additional feature of the PTTwhich could lead to decreased
sensitivity of themethod is the amount of overlap between
therespective segments used for gene analysis. Ifinsufficient
overlap is designed into the
993
on June 5, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.34.12.990 on 1 D
ecember 1997. D
ownloaded from
http://jmg.bmj.com/
-
Garvin, Attenhofer-Haner, Scott
method, a loss of sensitivity is expected. In thisstudy fragment
overlap was approximately 200bp which is sufficient to ensure that
mutationsoccurring towards the ends of each segmentwould be
detected. There remain, however,limitations with respect to the
sensitivity of thePTT. It does not detect missense mutationswhich
have been shown to account for a smallbut significant proportion of
changes inBRCA1 and BRCA2. Preliminary results froma second
screening of 23 women included inthis study for additional BRCA1
mutationsshowed five polymorphisms of unknown sig-nificance (data
not shown), suggesting that thePTT should not be relied on as a
definitive test.Thus the PTT can be recommended for aninitial
screen for both BRCA1 and BRCA2;however, other more sensitive
screeningstrategies such as denaturing gradient gel
elec-trophoresis should also be used.6 Alter-natively, indirect
mutation detection methodscould be used, such as microsatellite
markeranalysis or restriction fragment length poly-morphism (RFLP)
analysis which could indi-cate the disease allele in cases where
therewere genomic deletions, rearrangements, pro-motor sequence
mutations, and missensemutations.Out of 86 breast cancer patients
who fulfilled
our inclusion criteria, only 10.5% were foundto harbour
mutations in either BRCA1 or 2.Interestingly, all persons with
either BRCA1 or2 mutations had a significant history of
cancer;however, it appears that BRCA2 mutationsmay be less tissue
specific than BRCA1 muta-tions.
If age restrictions are applied, then the con-tribution of an
inherited susceptibility to theoverall number ofbreast cancer
patients shouldincrease as age decreases.'7 In the familiesstudied
in this report only about 10% couldbe assigned to either BRCA1 or 2
which isclose to the predicted value.'7 These results arecomparable
to recently published data indicat-ing that BRCA1 and BRCA2 do not
accountfor all breast/ovarian cancer families.'6 18 Giventhe
selection criteria adopted for the presentstudy the mutation
detection rate of 10.5% isconsistent with other larger studies
usingslightly different inclusion requirements'6 18and suggests
that the Swiss population issimilar to others from the same region.
Thepaucity of genetic changes found in womenwho did not have a
family history of diseasesupports the notion that BRCA1 and
BRCA2are unlikely to be associated with de novomutations and
therefore represent a specialentity with respect to breast cancer
develop-ment.
Since BRCA1 has been linked to both breastand ovarian cancer it
was not surprising toidentify a germline BRCA1 mutation in
anovarian cancer family. The mutation occurs inthe 5' end of the
gene, thus providing furtherevidence that mutations towards the 5'
endappear to be associated with an increased ovar-ian cancer
risk.'" BRCA2 carriers, however, donot have the same risk of
ovarian cancer devel-opment but do nevertheless have a greater
riskthan the general population. Recently, it has
been shown that there is an ovarian cancer sus-ceptibility
region in BRCA2,7 somewherebetween nucleotide 4235 and 6504, known
asthe ovarian cancer cluster region (OCCR). TheBRCA2 family with
ovarian cancer identifiedhere harbours a mutation at 3036 which
haspreviously been reported'2 to be associatedwith ovarian cancer
and may therefore extendthe OCCR in BRCA2 by another 1200 bptowards
the 5' end.The spectrum of disease observed in families
harbouring BRCA2 mutations was differentfrom that associated
with mutations inBRCA1. It appears that mutations in BRCA2may
confer a broader range of disease suscepti-bility as compared to
BRCA1. Indeed it hasbeen shown that germline mutations inBRCA2
appear to be associated with pancre-atic cancer development.2' In
the current studywe observed two melanoma patients within onefamily
where only one isolated early onsetbreast cancer case was observed,
suggestingthat BRCA2 may confer increased risks forother types of
cancer than breast and ovary.Unfortunately, DNA was not available
forstudy from these two patients.Two families from different
regions of Swit-
zerland were identified harbouring the samegermline BRCA2
mutation (delACAA). As this4 bp deletion is not discernible, owing
to thenature of the surrounding sequence, fromthose reported at
positions 3034 or 3035, it isdifficult to determine if this region
represents acommon site for mutation or a foundermutation.
Haplotyping analysis of the twofamilies reported here suggests that
these twofamilies are related as common alleles areshared by all
affected persons. Since this muta-tion has been previously
described in familiesfrom different countries it remains
possiblethat it is either a founder mutation or is aregional
hotspot for mutations.The remaining 77 patients in whom germ-
line BRCA1 or BRCA2 mutations were notidentified represent a
significant problem withrespect to mutation detection and
geneticcounselling. Given that only a few familiestested positive,
it is to be expected that somemutations were not detected using the
PTT;however, it is unlikely that a significant numberhave been
missed, implying that there are othergenes responsible for the
increased risk ofbreast cancer development seen in this popula-tion
of women.
This work was supported in part by grants AKT332, AKT463from the
Swiss Cancer League, the Krebsliga Beider Basel, TheRoche Research
Foundation, the Ciba-Geigy Jubilaums Stif-tung and the Freiwillige
Medizinische Akademische Gesells-chaft.
1 Miki Y, Swensen J, Shattuck-Eidens D, et al. A strong
candi-date for the breast and ovarian cancer susceptibility
geneBRCA1. Science 1994;266:66-71.
2 Wooster R, Bignell G, Lancaster J, et al. Identification of
thebreast cancer susceptibility gene BRCA2. Nature
1995;378:789-92.
3 Hall JM, Lee MK, Newman B, et al. Linkage of
early-onsetfamilial breast cancer to chromosome 17q2 1. Science
1990;250:1684-49.
4 Wooster R, Neuhausen SL, Mangion J, et al. Localization ofa
breast cancer susceptibility gene BRCA2, to chromosome13ql2-13.
Science 1994;265:2088-90.
994
on June 5, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.34.12.990 on 1 D
ecember 1997. D
ownloaded from
http://jmg.bmj.com/
-
BRCAI and BRCA2 mutation analysis in early onset breastlovarian
cancer patients
5 Easton DF, Ford D, Bishop DT, Consortium BC. Breastand ovarian
cancer incidence in BRCAI-mutation carriers.AmJ7Hum Genet
1995;56:265-71.
6 Ford D, Easton DF. The genetics of breast and ovarian can-cer.
BrJ7 Cancer 1995;72:805-12.
7 Gayther SA, Mangion J, Russel P, et al. Variation of risks
ofbreast and ovarian cancer associated with differentgermline
mutations of the BRCA2 gene. Nat Genet1997;15: 103-5.
8 Wu LC, Wang ZW, Tsan JT, et al. Identification of a
RINGprotein that can interact in vivo with BRCA1 gene product.Nat
Genet 1996;14:430-40.
9 Shattuck-Eidens D, McClure M, Simard J, et al. A
collabo-rative survey of 80 mutations in the BRCA1 breast
andovarian cancer susceptibility gene: implications for
pre-symptomatic testing and screening. JAMA 1995;273:535-41.
10 Miller SA, Dykes DD, Polesky HF. A simple salting out
pro-cedure for extracting DNA from human nucleated cells.Nucleic
Acids Res 1988;53:739.
11 Garvin AM, Spycher M, Haner H, et al. BRCA1 mutationsin a
selected series of breast/ovarian cancer patients. 7 MedGenet
1996;33:721-5.
12 Lenoir et al, 1996. Breast Cancer Information Core
http://www.nchgr.nih.gov/Intramural_research/Lab_transfer/Bic/
13 Takahashi H, Chiu HC, Bandera CA, et al. Mutations of
theBRCA2 gene in ovarian carcinomas. Cancer Res
1996;56:2738-41.
14 Ford D, Easton DF, Peto J. Estimates of the gene frequencyof
BRCA1 and its contribution to breast and ovarian can-cer incidence.
Am _Hum Genet 1995;57:1457-62.
15 Fitzgerald MG, Macdonald DJ, Krainer M, et al. GermlineBRCA1
mutations in jewish and non-jewish women withearly-onset breast
cancer. N Engl _J Med 1996;334: 143-9.
16 Stoppa-Lyonnet D, Laurent-Puig P, Essioux L, et al.BRCA1
sequence variations in 160 individuals referred toa breast/ovarian
family cancer clinic. Ami I Hum Genet1997;60: 1021-30.
17 Friedman LS, Szabo CL, Ostermeyer EA, et al. Novelinherited
mutations and variable expressivity of BRCA1alleles, including
founder mutations 185 delAG inAshkenazi Jewish families.Am J Hum
Genet 1995;57:1284-97.
18 Hakansson S, Johannsson 0, Johansson U, et al.
Moderatefrequency of BRCA1 and BRCA2 germ-line mutations
inScandinavian familial breast cancer. Am J Hum Genet1997;60:
1068-78.
19 Langston AA, Malone KE, Thompson JD, Daling JR,Ostrander EA.
BRCA1 mutations in a population-basedsample of young women with
breast cancer. N Engl _J Med1996;334: 137-142.
20 Gayther SA, Warren W, Mazoyer S, et al. Germlinemutations of
the BRCA1 gene in breast and ovarian fami-lies provide evidence for
a genotype-phenotype correlation.Nat Genet 1996;11:428-33.
21 Goggins M, Schutte M, Lu J, et al. Germline BRCA2
genemutations in patients with apparently sporadic
pancreaticcarcinomas. Cancer Res 1996;56:5360-4.
22 Tavtigian S, Simard J, Rommens J, et al. The completeBRCA2
gene and mutations in chromosome 13q-linkedkindreds. Nat Genet
1996;12:333-7.
995
on June 5, 2021 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.34.12.990 on 1 D
ecember 1997. D
ownloaded from
http://jmg.bmj.com/