Embed Size (px)
Citation preview

10/12/2015
1
Scott Brancato, MD, FHRSMedical Director, Cardiac Device ClinicProvidence Heart and Vascular Institute
Bradyarrhythmias – Permanent pacemakers
Tachyarrhythmias/Sudden death prevention –
Implantable Cardioverter Defibrillators (ICDs)
Cardiac rhythm monitoring – Implantable Loop Recorders (ILRs)

10/12/2015
2

10/12/2015
3

10/12/2015
4
Sinus node dysfunction
Symptomatic bradycardia (including pauses)
Symptomatic chronotropic incompetence
Heart Block
Asymptomatic advanced or complete AV block
Asymptomatic Mobitz Type II 2nd degree AV block
Symptomatic Mobitz Type I 2nd degree AV block
Cardiac resynchronization
CHF, LVEF 35% or less, with QRS>120ms or anticipated RV pacing >40%
Sinus bradycardia
Sinus pause
Conversion pause

10/12/2015
5
Mobitz 2 2nd degree
Mobitz 1 (Wenkebach)
Complete AV block
RBBB
Normal QRS
RV pacing QRS
LBBB
Conscious sedation
IV antibiotics
2” incision in deltopectoral groove
Access in axillary, cephalic or subclavian vein
Pacing leads are 6-7F (2-2.5mm diameter)
Leads advanced to RA/RV under fluoroscopy
Active fixation mechanisms (screws) extended
Leads connected to device
Incision closed

10/12/2015
6
RV and/or RA leads placed
Coronary sinus cannulated with introducer sheath
Venogram performed to identify CS branch
Lead advanced over wire into CS branch
Introducer sheath split
Infection
Hematoma
Pneumothorax
Hemothorax
Cardiac perforation
Contrast reaction
Lead dislodgement
Lead malfunction/failure
Overall
complication
rate 3-4%

10/12/2015
7
Complication
Lead dislodgement
Pneumothorax
Lead perforation
Venous thrombosis
Chronic lead failure
Hematoma requiring surgery
Erosion
Infection
Occurrence
2-4%
1%
<1%
1-3%
2-4% at 5 years
<0.5%
1%
1-2%
Extraction mortality 1%
In-hospital mortality for PPM infections 8.4%
The 15 month mortality rate is 36%
Hospital stay for PPM infection is 14.4 days
The incremental cost of PPM infection is estimated at $17-$25K
Unmet Clinical Needs
Access complications (pneumothorax, occlusion)
Pocket complications (Hematoma, Erosion, infections)
Lead complications (dislodgement, fracture, infections,
connection errors, interaction with vasculature & heart
structures, extraction complications)
Patient Preference
Cosmetic appeal (lack of pocket)
Minimally invasive approach
Pain and discomfort associated with pocket
Efficiency
Faster procedure?
Possibility for lower complications?
Increase Access to Brady Therapy
Availability of specialists in emerging markets

10/12/2015
8
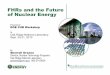
Intended for patients that have a Class I or II indication for a single-chamber ventricular pacemaker
Contraindicated in patients with current implanted cardiac devices which:
would interfere with the placement of the Micra device
are providing active cardiac therapy
• Pacing Mode: VVIR
• Volume: 0.75cc
• Mass: 2g
• Length: 24mm
• Width: 20Fr
• Bipolar sensing (17mm spacing)
• Programmable
• Capture Management
• Diagnostics: battery status,
pacing threshold, pacing
impedance, % paced
• 7.4/10.1 year longevity (2.0/1.5V
output, 60 bpm, 100% paced)
• MRI conditional
• RF communication with
programmer & Carelink
• Device can be deactivated
Proximal Retrieval
Feature
Anode (27mm2 )
Cathode (2.5mm2)
CapSure Sense
steroid eluting
Active Fixation “Tines”
Electrically Inactive

10/12/2015
9

10/12/2015
10
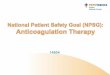
The Leadless Cardiac Pacemaker.

10/12/2015
11
Device-Related Serious Adverse Events.

10/12/2015
12
Single Chamber ICD Dual Chamber ICD
Biventricular ICD

10/12/2015
13
Subcutaneous ICD
LVEF<35% due to prior MI who are at least 40 days post MI (NYHA II-III)
LV dysfunction due to prior MI, LVEF < 30%, NYHA I
Survivors of Cardiac arrest due to VF or hemodynamically unstable sustained VT after evaluation to define the cause of event and excluding any reversible causes

10/12/2015
14
Primary prevention of sudden cardiac death
Cardiomyopathy (Ischemic, nonischemic)
Primary electrical disorders (Brugada, LQTS)
Secondary prevention of sudden cardiac death
Ventricular tachycardia
Ventricular fibrillation
Non-ischemic DCM LVEF < 35%, NYHA II-III
Non sustained VT due to prior MI, LVEF < 35% or inducible VF/FT on EPS
Structural heart disease and spontaneous sustained VT
Syncope of undetermined origin with clinically relevant sustained VT or VF induced at EPS
LQTS patients who experience syncope and/or VT while on b-Blockers
Reversible triggering factor for VT/VF
CAD patients without inducible or spontaneous VT undergoing bypass surgery
NYHA class IV drug refractory congestive heart failure, not candidates for transplant
Life expectancy less than 1 year
Significant behavioral disorders or psychiatric disorders

10/12/2015
15
Conscious sedation
IV antibiotics
2” incision in deltopectoral groove
Access in axillary, cephalic or subclavian vein
ICD leads are 7-8F (2.3-2.7mm diameter)
Leads advanced to RA/RV under fluoroscopy
Active fixation mechanisms (screws) extended
Leads connected to device
Incision closed
Defibrillaton threshold testing (rarely)
RV and/or RA leads placed
Coronary sinus cannulated with introducer sheath
Venogram performed to identify CS branch
Lead advanced over wire into CS branch
Introducer sheath split
Infection
Hematoma
Pneumothorax
Hemothorax
Cardiac perforation
Contrast reaction
Lead dislodgement
Lead malfunction/failure
Inappropriate shocks

10/12/2015
16
� The Danish Registry demonstrated that up to 15%
of ICD patients are at risk of a complication within
the first 6 months of implant.
� The majority of complications requiring invasive
intervention included:
� Lead related issues
� Infection
�Cardiac Perforation
�PneumothoraxKirkfeldt, R., et al. Complications after cardiac implantable electronic
device implantations: an analysis of a complete, nationwide cohort in
Denmark . European Heart Journal. Dec 2013
1. Maisel WH, Kramer DB. Implantable cardioverter defibrillator lead performance.
Circulation 2008;117:2721-2723. doi: 10.1161/CIRCULATION AHA. 108.776807.
Defibrillates without transvenous leads
Avoids lead related complications associated with traditional ICDs
Unlike traditional ICDs, it does not have the ability to function as a pacemaker

10/12/2015
17

10/12/2015
18

10/12/2015
19
No venous access (occluded or congenital)
High risk of complications for TV-ICD (dialysis, pediatric, immunocomprised)
Channelopathies (LQT, Brugada, HCM)
Previous device infections or lead failures
H/O endocarditis

10/12/2015
20
• Systolic heart failure and LBBB who are indicated for CRT
• Symptomatic bradycardia requiring pacemaker
• Recurrent sustained MVT for whom ATP is deemed appropriate
Cardiac implantable electronic devices have made possible incredible advances in patient care over the past several decades
Advances in technology continue to improve the size and functionality of these devices
Indications continue to evolve as the technology improves

10/12/2015
21