Upload
florentina-adascalitei
View
213
Download
0
Tags:
Embed Size (px)
DESCRIPTION
Brain Tumors1
Citation preview
186
Conferences and Reviews
Brain TumorsModerator
KEITH L. BLACK, MD
DiscussantsJOHN C. MAZZIOTTA, MD, PhD, and DONALD P. BECKER, MD
An edited summary ofan Interdepartmental Conference arranged by the Department ofMedicine ofthe University ofCalifornia,Los Angeles, School ofMedicine. The Director of Conferences is William M. Pardridge, MD, Professor ofMedicine.
Recent advances in experimental tumor biology are being applied to critical clinical problems of primary brain tumors. Theexpression of peripheral benzodiazepine receptors, which are sparse in normal brain, is increased as much as 20-fold inbrain tumors. Experimental studies show promise in using labeled ligands to these receptors to identify the outer marginsof malignant brain tumors. Whereas positron emission tomography has improved the dynamic understanding of tumors,the labeled selective tumor receptors with positron emitters will enhance the ability to specifically diagnose and greatly aidin the pretreatment planning for tumors. Modulation of these receptors will also affect tumor growth and metabolism.Novel methods to deliver antitumor agents to the brain and new approaches using biologic response modifiers also holdpromise to further improve the management of brain tumors.(Black KL, Mazziotta JC, Becker DP: Brain tumors. West J Med 1991 Feb; 154:186-197)
Peripheral Benzodiazepine Receptors-Mechanisms in Brain Tumor Biology
EITH L. BLACK, MD*: There are two classes of benzo-Jdiazepine receptors in mammalian tissues. One class ofreceptors (the "central" receptor) is located on neurons andis the site at which benzodiazepine ligands are thought toexert their antianxiety, anticonvulsant, and muscle relaxanteffects. 1-3 These central binding sites are closely linked to 'y-aminobutyric acid (GABA) receptors, modulate the GABA-regulated anion channel, and are located on the cell mem-brane.2'4'5 The second class of benzodiazepine receptors (the"peripheral," nonneural receptor) is sparse in normal ner-vous tissue but prominent in many other tissues, such askidney, heart, platelets, and lymphocytes.6'8 High-affinitybinding by peripheral benzodiazepine ligands to rodent glialtumor was shown in homogenate studies.8'-2 Based on thesefindings, it was recently suggested that peripheral benzo-diazepine receptor ligands could be used specifically to im-age glial tumors in vivo and provide better definition oftumorborders and biologic character.'3'4 Second, but no less im-portant, the dramatic increase in the expression of peripheralbenzodiazepine receptors in brain tumors has recentlyprompted further investigation into a possible role of thesereceptors in brain tumor biology. Because the receptor wasshown to localize on the outer membrane of mitochondria,considerable work has focused on the modulation of cellmetabolism by the peripheral benzodiazepine receptor. Re-cent work has also suggested that selective peripheral benzo-
*Assistant Professor, Department of Surgery, Division of Neurosurgery, UCLASchool of Medicine.
diazepine ligands may act as mitogenic agents and increasetumor cell proliferation and DNA synthesis.Brain Tumor Imaging
Computed tomography (CT), magnetic resonance imag-ing (MRI), and positron emission tomography (PET) tech-niques currently used to image tumors in the central nervoussystem rely on differences in tissue attenuation characteris-tics, a breakdown of the blood-brain barrier to contrastagents, mass effect, or changes in glucose or amino acidtransport. 11 The limitations of these methods, most apparentin glial and other infiltrative tumors, are due to their failure toidentify tumor cells that reside beyond the borders of theimaging abnormality.16 An ability to image tumors with aligand that binds specifically to tumor cells and readilycrosses the intact blood-brain barrier might significantly im-prove tumor resolution in the brain and permit better identifi-cation of the outermost margin of tumor cells. Peripheralbenzodiazepine receptor ligands seem to fulfill both criteria:they are not barred by the blood-brain barrier, and they havehigh specific binding to glial tumors.
The possibility that a peripheral benzodiazepine receptorligand might be used specifically to image glial tumors wasfirst suggested by the findings of Starosta-Rubinstein andassociates. 13 Published findings from our laboratory were inagreement with this previous report that peripheral benzo-diazepine ligands bind selectively to glial tumors in rats, withlittle binding to normal brain or necrotic tissue.'4 The intra-venous administration of the selective peripheral benzo-diazepine ligand, [3H]PK 11195 (1-[2-chlorophenyl]-N-methyl-N-[ 1 -methylpropyl]-3-isoquinoline carboxamide),
This work was supported in part by National Institute of Neurological Disorders and Stroke grant No. NS15654 and Department of Energy contract No. DEACO3SF760001 3. DrMazziotta acknowledges the positron emission tomography investigators for their contribution.
Reprint requests to Keith L. Black, MD, Division of Neurosurgery, 74-140 Center for the Health Sciences, 10833 Le Conte Ave, UCLA School of Medicine, Los Angeles, CA90024-1749.
THE WESTERN JOURNAL OF MEDICINE * FEBRUARY 1991 * 154 * 2
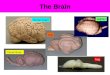
or the mixed peripheral and central ligand, [3H]flunitraze-pam (after pretreatment with clonazepam to block centralbinding sites), showed binding densities of peripheral benzo-diazepine receptors threefold to fivefold higher in experi-mental glial tumors compared with normal cortex. Periph-eral binding could be displaced by the preadministration ofexcess PK 11195. Topographic correlation was excellent be-tween areas of histologically verified tumor and high densi-ties of peripheral benzodiazepine binding (Figure 1). It wasfurther shown, however, that peripheral benzodiazepinebinding was not exclusive to tumors of glial origin but that, infact, substantial binding occurred in the experimental meta-static tumors. The nonexclusive binding of peripheral benzo-diazepines to glial tumors was further supported by in vitrofindings that peripheral ligands will bind to various tumors inhumans (Table 1), 17 which suggests that they may have lim-ited use as a marker to differentiate tumors. We did, however,find a significant correlation between high binding and thedegree of malignancy in gliomas in humans (Table 2). Invitro studies also showed that the number of receptors (Bmux)on C6 and Walker 256 tumors was increased rather than theaffinity of the ligand for the receptor site (Table 3). 18
Three-dimensional reconstructions were recently appliedto autoradiographic images of peripheral benzodiazepinebinding and compared with histologic images to confirm thespatial and structural accuracy of receptor mapping images inan experimental glial tumor. A close topographic correlationbetween histologic features and tumor binding was found.Similar techniques using positron-labeled peripheral benzo-A B
@>2f *'
flb ,v
diazepine receptor ligands are now being applied in humans.Although current PET resolution is limited, small clusters oftumor cells may be located using these techniques. Thiscould have important implications in identifying the surgicalmargins in subgroups of patients without diffuse spread ofglial tumor cells where radical resections may prove benefi-cial. Based on the intensity of uptake, insight may be ob-tained into the biologic behavior of the tumor to help inpreoperative planning and in determining prognosis.
Tumor BiologyThe biologic role of peripheral benzodiazepine receptors
in brain tumors is unclear. Unlike the central receptor, whichis located on the cell membrane, the peripheral binding site islocalized to the mitochondrial and nuclear subcellular frac-tions,1920 which implies a role for the receptor in oxidativemetabolism and ion fluxes.
Studies of the effects of peripheral-type ligands have alsoreported an inhibition ofthe proliferation ofthymoma cells,21the suppression of thymidine incorporation into the DNA ofglial cells,22 the blocking of mitogenesis in Swiss 3T3 cells,and the induction of differentiation in Friend erythroleuke-
Figure 1.-A digitized autoradiogram (A) and thionin-stained section (B) showRG-2 tumor after the administration of [3H]flunitrazepam with clonazepam.Binding to normal brain is slightly higher compared with [3H]PK 1 1 195 admin-istration. In magnified comparisons of the same autoradiogram (C) andthionin-stained section (D), tumor definition and correlation with histologicfeatures remain high. A fingerlike projection of invading cells (arrow) seen onthe magnified thionin-stained section (D) is also visualized on the magnifiedautoradiogram (C; arrow).
ABBREVIATIONS USED IN TEXTCT = computed tomographyED5s = median effective doseMRI = magnetic resonance imagingPET = positron emission tomography
TABLE 1.-Specific Binding of [HJPK 11195 toNonglial Human Brain Tumors'
Specific Binding,Histologic Tumor Type fmol/mg tissueSarcoma......................... 510.0Meningioma......................... 353.7 i93.6Hemangiopericytoma.................... 180.9Primitive neuroectodermal tumor, n = 2 ...... 154.3Craniopharyngioma ..................... 107.7Normal
..........................77.7 i28.4
'Values are expressed as the mean when n = 1. Standard deviation values are given whenn-2.
TABLE 2.-Specific Binding of [3H)PK 1195 toGlial Tumors in Humans'
Specific Binding,Histologic Tumor Type fmol/mg tissueNormal, nonneoplastic .... 77.7 28.4Necrosis.74.8 i 38.0Infiltrated.219.8 i 31.9Low-grade glioma.267.3 54.0High-grade glioma.452.1 46.5
'For statistical analysis (analysis of variance and unpaired Student's t test), regions ofinterest were defined as nonneoplastic (no neoplastic cells), necrotic (nonviable debris),infiltrated (tumor cells mixed with histologically appearing normal cells), low grade (gliomagrades I and 11), and high grade (glioma grades Ill and IV). The 3 necrotic sections were all frompatients with high-grade gliomas. Infiltrated sections included patients from the high- andlow-grade groups. Significant differences were found between nonneoplastic versus infil-trated (P
BRAIN TUMORS
mia cells.23 On the other hand, they enhance melanogenesisin melanoma cells24 and enhance the specific induction of c-fos messenger RNA and protein by nerve growth factor morethan 100-fold.25 Diwan and co-workers reported the promo-tion of hepatocellular carcinogenesis in B6C3F1 mice bydiazepam after initiation by N-nitrosodiethylamine.26 Theseeffects, however, were found at micromolar concentrations,whereas peripheral benzodiazepine receptors were saturatedat concentrations in the nanomolar range.9'2172
Because of the discrepancy between the dose of periph-eral benzodiazepines needed to show growth control andtheir binding constants, we recently investigated the effectsof peripheral benzodiazepines on cell proliferation of C6glioma and on the mitogenesis of Swiss 3T3 cells in culturewithin the concentrations at which receptor binding occurs .28We found that PK 11195 increased the growth rate of C6glioma cells by 20% to 30% in the nanomolar range in serum-free medium. Incorporating tritium-labeled thymidine intoC6 glioma cells also increased their growth rate 22% and25%, respectively, after treatment by the selective peripheralbenzodiazepine ligands, PK 11195 and Ro 5-4864. When theeffect of PK 11195 as a mitogenic agent was estimated by[3H]thymidine incorporation using Swiss 3T3 cells, PK11195 was found to increase DNA synthesis 170% over thatof control at 10 nmol per liter. Higher concentrations ofbenzodiazepines inhibited DNA synthesis. Peripheral ben-zodiazepine binding sites, however, were shown to decreasein number after exposure to serum-free medium or to 10nmol per liter of PK 11195.
It seems that peripheral benzodiazepine ligands have bi-phasic effects on cell proliferation. At concentrations in thenanomolar range, they stimulate [3H]thymidine incorpora-tion into DNA and increase cell proliferation in C6 glioma.They also show mitogenic activity in cell lines such as Swiss3T3 cells. At micromolar concentrations, however, theyinhibited DNA synthesis. Other authors, who have also sug-gested that peripheral benzodiazepines are involved in regu-lating cell proliferation,21-25 have indicated an antiprolif-erative effect of benzodiazepines at the micromolar range.Pawlikowski and colleagues reported an antiproliferativeaction of peripheral-type benzodiazepines on human gliomaat the micromolar range (1 to 100,mol per liter).22 A strongpositive correlation between the binding affinity of benzo-diazepines for the peripheral-type receptor and their antipro-liferative activities was reported in mouse thymoma cells,2'though there was no significant correlation between the ac-tivities of benzodiazepines and their reported degree of affin-ity.6'23'24'29 In Wang's experiments there was an approxi-mately 2,000-fold difference in dosage between receptorbinding and biologic effects21; the median effective dose(ED,.) for Ro 5-4864 in inhibiting [3H]thymidine incorpora-tion into thymoma cells was 16.1 /tmol per liter, whereas theintensity concentration where 50% of receptors were bound(IC50) was 8.5 nmol per liter. An in vitro binding assay usingautoradiography or cell homogenates showed that peripheralbenzodiazepine binding should be saturated at 10 to 20 nmolper liter.18'21 Clarke and Ryan used erythroleukemia cells intheir study and concluded that differentiation was induced bythe lipophilic properties of certain benzodiazepines.23 To thecontrary, the stimulation of cell growth of C6 cells and mito-genic activity of Swiss 3T3 cells were found in the nanomolarrange, which corresponded to the binding affinities of thecompounds for the peripheral benzodiazepine receptors.
Ruff and associates also reported that the chemotaxis of hu-man monocytes was enhanced with an ED50 of 10-13 mol perliter for Ro 5-4864, whereas a higher concentration (> 10-8mol per liter) resulted in a reduced chemotactic response.30These findings also support our conclusion that peripheralbenzodiazepines have a biphasic effect on cell proliferation.
Peripheral benzodiazepines, however, are not polypep-tide growth factors like epidermal growth factor or platelet-derived growth factor that has been found to be active on glialcells. Also, because receptors for peripheral benzodiaze-pines are thought to localize on the mitochondrial outermembrane,'9'20 it will be worthwhile to investigate in futurestudies whether this receptor-ligand complex will signifi-cantly affect the mitochondrial DNA or whether the activatedreceptor transmits mitogenic signals to the nucleus.Clinical Implications
Selective high-density binding by peripheral benzodiaze-pine ligands could be used clinically in several ways. First,these ligands are amenable to conjugation with potentiallycytotoxic compounds. The localization of binding sites tonuclear and mitochondrial fractions could increase theirtherapeutic advantage compared with targets on the cell sur-face. The effect of the modulation of the peripheral receptoritself on tumor growth and differentiation also remains to beexplored. Further, positron-labeled benzodiazepine ligands,such as carbon 11-labeled PK 11195, could potentially im-prove the definition of the outer border of tissues infiltratedwith malignant tumor cells or indicate residual tumor aftersurgical therapy. These novel concepts are currently beinginvestigated.Positron Emission Tomography in theStudy of Cerebral NeoplasmsApproaches to Brain Tumor ImagingJOHN C. MAZZIOTTA MD, PhD*: Although anatomicallybased imaging techniques have provided substantial informa-tion about cerebral gliomas, they can be inconclusive in de-tecting early tumors, in discriminating tumors from edema,the histologic grading of tumors, and in differentiating tumorrecurrence from radiation necrosis.3' Structural imagingtechniques, such as x-ray computed tomography and mag-netic resonance imaging, provide high-quality, high-resolu-tion images of the site of cerebral neoplasms and the distor-tions they induce in adjacent cerebral structures by the masseffects caused by their own volume and attendant edema. Inaddition, by using agents such as iodinated contrast materialin x-ray CT, alterations in the blood-brain barrier may also bedetected by these techniques. Distinguishing actual sites ofviable tumor from zones of necrosis or surrounding edema isdifficult with such methods, however. Similarly difficult isclinically differentiating recurrent tumor from radiation ne-crosis in a patient who has new signs and symptoms that arereferable to a site of previous tumor therapy.
Positron emission tomography measures a wide range ofphysiologic processes critical in understanding the patho-physiology of cerebral disorders.32135 These processes in-clude the ability to examine cerebral physiology, biochemis-try, hemodynamics, and pharmacokinetics in vivo in healthand disease. Critical to the understanding of tumor growthand strategies to limit or block suchgrowth is a knowledge of
*Associate Professor, Department of Neurology/Radiological Sciences, Reed Neu-rological Institute, UCLA School of Medicine, Laboratory of Nuclear Medicine.
188
THE WESTERN JOURNAL OF MEDICINE * FEBRUARY 1991 * 154 * 2
tumor metabolism, blood flow, protein synthesis, blood-brain barrier integrity, and the binding of specific com-pounds to receptors found on tumor cell surfaces. Each ofthese processes is important, but the study ofthe biochemicalrelations between the processes-that is, stoichiometry-may provide an even more sensitive indicator of tumor type,grade, and natural history.4 In addition, the effect of thetumor on adjacent or distant tissue is important in under-standing the constellation of signs and symptoms manifestedby a patient at a given point in time. Thus, tumor edema mayproduce dysfunction in adjacent tissue either directly or bysecondary ischemia. Simultaneously, functional deafferenta-tion and deafferentation of pathways leading to and from thezone oftumor and edema may disrupt normal neuronal activ-ity at far distant sites within and between the cerebral hemi-spheres and that affecting cerebrocerebellar neuronal con-nections.34 Positron emission tomography can identify suchlocal and distant functional disconnections.34
Because PET provides functional measures of neuronalactivity and biochemistry, we can map normal sites of cere-bral activity during behavior. Thus, patterns of cerebral me-tabolism and blood flow change when a subject is asked to dotasks that involve reading, listening, perceiving sensorystimuli, and movement.32 By having patients with brain tu-mors perform such tasks, it is possible to identify whethercritical neuronal networks, presumed to lie close to the site ofa planned tumor resection, will be adversely affected by thesurgical procedure, resulting in a major neurologic deficit forthe patient.Positron Emission Tomography
Positron emission tomography is an imaging techniquethat provides an accurate measurement of the concentrationsof trace amounts of compounds labeled with positron-emit-ting isotopes introduced into the body either by inhalation orintravenous administration.32 The imaging device producescross-sectional and planar images of the distribution of theadministered radiopharmaceutical agent. With the use of la-beled compounds to trace physiologic processes, it is possi-ble to use the local tissue concentrations, obtained from thePET images, to quantify these physiologic processes if themathematic relation between the process and the concentra-tion of the tracer in the tissue is understood. These mathe-matic relations are termed tracer kinetic models, and they areneeded to understand the behavior of compounds in the bodyand to interpret the resultant data validly. This usually re-quires both a measurement of the time course of the concen-tration of the administered tracer in the blood and sequentialimages of the organ of interest using PET to determine thetissue tracer concentration. Once the model is validated, theprocedure can be simplified and a single set of images can betaken at the end of a defined interval between administeringthe tracer and acquiring data.
Isotopes that emit positrons have several important quali-ties. Such isotopes include those of the natural elements ofthe body, such as nitrogen 13 ('3N; 10-minute half-life),carbon 11 ("C; 20-minute half-life), and oxygen 15 (lSO; 2-minute half-life). Because these are isotopes of natural bio-logic elements, they can be incorporated into compounds thatfaithfully mimic the chemical behavior of the natural com-pound, thereby minimizing the perturbation of the biologicsystems they are intended to trace. Because of the isotopes'short half-lifes, radiation doses to patients are low. A short
half-life, however, produces several practical challenges.First, the radiochemical synthesis of the tracer compoundmust be rapid for there to be enough isotope left at the end ofthe synthesis for reasonable imaging in a patient. Second, theshort half-life of a compound dictates that the isotopes andcompounds, in general, must be made at the site of the PETimaging instrument.
Isotopes used in PET studies are produced in charged-particle accelerators that include linear accelerators and cy-clotrons. At present, the usual approach is to build compactcyclotrons that are used for medical applications, such as theproduction of positron-emitting isotopes. More than 500compounds have been labeled with 15O, '3N, 'IC, and fluo-rine 18 ('8F) for use with PET.35"36 These compounds rangefrom simple labeled molecules such as water, carbon monox-ide, and oxygen gas to carbohydrates, amino acids, fattyacids, neurotransmitter analogues and precursors, as well asreceptor ligands.35'36
Positrons are emitted from unstable nuclei and travel ashort distance in tissue before coming to rest. Once at restthey combine with nearby electrons, resulting in their mutualannihilation. The resultant energy of annihilation results intwo photons emitted at an angle of 180 degrees to one an-other. These annihilation photons are detected by crystals inthe PET camera and are converted into voltages by the sys-tem's electronics. Because of the 180-degree emission pro-duced by positron annihilation, crystals on opposite sides ofthe patient are electronically linked (electronically colli-mated) to identify those events that take place in a giventomographic plane. This feature permits PET cameras tohave uniform, high spatial resolution (state-of-the-art cam-eras have 6- to 7-mm resolution in all three dimensions).37
Thus, with the unique features of PET, including the useof isotopes of natural elements, valid tracer kinetic models,and the unique physical properties of positron decay, it ispossible to quantify a wide range of physiologic, biochem-ical, and hemodynamic processes in the human body usingthis technique. When applied to the study of cerebral neo-plasms, we can use these methods to measure tumor metabo-lism, blood flow, protein synthesis, blood-brain-barrier in-tegrity, and the binding of specific ligands to membranereceptors. With this unique technique, we can collect previ-ously unavailable data about cerebral neoplasms, which hasproved useful in the management of patients with these disor-ders and in providing insights into the pathophysiology of theneoplastic process itself (Table 4). As these tumor propertiesare explored with PET, considerable studies have been doneand several reviews have been reported.3849
Glucose MetabolismTumors have an accelerated rate of glycolysis that can
exist despite adequate oxygenation.50-52 This property, oncethought to be unique to tumors, is characteristic of increases
TABLE 4.-Positron Emission Tomography and theManagement of Cerebral Gliomas
Determines tumor grade, which aids in management decisions andguides prognosis
Determines effect of tumor on adjacent and remote cerebral tissuesMonitors progression, change in grade, and therapy effectsHelps in choice of optimal site for biopsyDifferentiates radiation necrosis from tumor recurrence
189
BRAIN TUMORS
in intermediary metabolism seen with rapidly growing tissueof any type. Weber has shown a correspondence between therate of tumor metabolism and the growth rate of individualmalignant cells51; he has attributed this altered metabolism tochanges in the concentrations of certain key rate-controllingenzymes in the metabolic pathway. The accelerated glyco-lytic pathway can be shown with PET studies of glucosemetabolism using '8F-labeled fluorodeoxyglucose.53-55
In studies of experimentally induced gliomas in animals56and human PET studies,4'57"59 there was evidence of highglucose metabolism within the tumor itself. Hossmann andassociates injected intracerebral glioma cells into rats toshow that with tumor development, glucose use increasedout of proportion to cerebral blood flow.56 In addition, theyfound that blood flow decreases in the tissue immediatelysurrounding the tumor but not in the contralateral hemi-sphere.
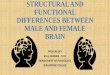
Studies by Di Chiro and colleagues at the National Insti-tutes of Health have shown a remarkable correlation betweenthe metabolic rate and histologic grade of gliomas.41 5765The most consistent finding is the appearance of "hot spots"of hypermetabolism in virtually all grade III and IV gliomas(Figure 2). Areas of hypermetabolism were only rare-ly seen in low-grade (I and II) tumors. On average, grade Iand II gliomas had metabolic rates similar to that of normalwhite matter, whereas grade III and IV tumors have meta-bolic rates comparable with or in excess of normal grey mat-ter (Figure 2).41 In all cases, peak values for tumor metabo-lism were used. Similar results were obtained for the gliomasof the upper cervical spinal cord and brain stem.59'65
In a separate study by Tyler and co-workers, fluorode-oxyglucose and PET were used to determine tumor glucosemetabolism versus tumor grade in 16 patients.66 Althoughthe highest metabolic rates found were among those patientswith grade IV tumors, there were examples of high-gradetumors that apparently had low metabolic rates; all thesepatients were untreated at the time of tumor metabolism mea-surements. Tyler and associates analyzed their data in com-parison to grey matter of the contralateral hemisphere,66whereas the group at the National Institutes of Health usedwhite matter as their reference tissue.41 58 Thus, there seemto be differences in the interpretation of results, owing in partto the fact that the latter study did not rely on visual inspec-tion of "hot spots" but rather averaged the entire tumor vol-ume and, in addition, studied patients who had been un-treated at the time of imaging. Although there is not completeagreement, there generally seems to be an excellent corre-spondence between the metabolic rate and tumor grade.
The metabolic grading of glioma malignancy has prog-nostic importance.67'68 In a study of 45 consecutive patientswith proven high-grade gliomas (grades III and IV) studied atthe National Institutes of Health, glucose metabolism wasevaluated as a measure of prognosis.67 All patients receivedradiation therapy before their entry into the study, 32 patientshad received chemotherapy, and most patients (41/45) hadcontrast enhancement of their tumors on x-ray CT. Glucoseuse in the tumor was compared with that of the contralateralside. A ratio of 1.4:1 of tumor to nontumor was found to bethe median level of glucose use, and patients were dividedinto two groups with regard to their survival (Figure 3).69Patients having tumors with high metabolism-ratios greaterthan 1.4-had a mean survival of 5 months; those with tu-mors having a ratio of less than 1.4 had a mean survival of 19
months. The histologic grade of tumors also correlated withsurvival, with the patients with grade III tumor survivinglonger than those with grade IV. The PET findings, however,were superior to histologic variables in predicting ultimateprognosis. Thus, patients with metabolic tumor ratiosgreater than 1.4 had short survival times, regardless of theirhistologic grade.
Measurements of glucose metabolism by PET in cerebralneoplasms are useful in identifying the grade of tumor withrespect to malignancy in the glioma series and in determiningthe prognosis for a patient. In addition, measurements ofglucose metabolism support the concept put forth by War-burg nearly 60 years ago that accelerated glycolysis is a char-acteristic of tumors and is proportional to their degree ofmalignancy.52Cerebral Blood Flow and Oxygen Use
Several investigators have examined the cerebral bloodflow and oxygen use of cerebral neoplasms.68"-1 Despite the
Figure 2.-High- and low-grade gliomas are differentiated with positron emis-sion tomographic (PET) determinations of glucose metabolism. The upper rowof images shows PET studies of glucose metabolism using [18F]fluorodeoxyglu-cose (FDG), the bottom left is a magnetic resonance imaging (MRI) study, andthe bottom right is an x-ray computed tomographic (CT) study after theadministration of iodinated contrast material. The patient depicted in the leftcolumn has a low-grade (grade 11) glioma of the frontoparietal cortex. Sur-rounding edema is obvious in the MRI scan. The glucose metabolism of thislesion is low and comparable with that of normal white matter. In contrast, thepatient whose studies are depicted in the right column shows the appearanceof a high-grade (grade IV) glioma in the frontal lobe. The x-ray CT study of thispatient shows a central area of low attenuation surrounded by a low-densityarea that extends throughout the frontal and into the parietal lobe. The latterdistribution is consistent with tumor-associated edema. The FDG-PET study ofthis patient shows a central area of low or absent metabolic activity consistentwith tumor necrosis and a surrounding area of high metabolic activity compa-rable with that of the normal grey matter and consistent with a highly malig-nant glioma. Surrounding the hypermetabolic zone is a more general reductionin glucose metabolism in the adjacent frontal cortex, which may represent theeffects of edema or pressure effects, or both, directly exerted by the tumor.Thus, while the site of these lesions, their attendant edema, and mass effectscan be shown by x-ray CT or MRI, information about the histologic nature oftumors is, in addition, provided by measurements of glucose metabolism withPET.
190
fact that cerebral gliomas have an accelerated rate of the useof glucose, reflecting their high glycolytic rate, they havedecreased oxygen use. These tumors shift away from oxida-tive metabolism (which supports the prediction of findings inanimals) where fast-growing tumors have augmentation ofthe Embden-Meyerhof pathways despite adequate oxygenavailability. These studies have included the measurements oflocal cerebral blood flow, oxygen use, and oxygen extractionfraction in cerebral gliomas and metastatic brain tumors us-ing 150-labeled compounds and PET (Figure 4).6871 Theseresults have been discussed by Beaney and associates withrespect to cerebral and systemic tumors.7374 In addition,these authors found that surgical decompression of brain tu-mors reduces the abnormalities in blood flow and oxygenuse, indicating a direct physiologic correlation with benefi-cial effects for this type of surgical treatment.
The stoichiometry of brain tumors indicates that theyhave enhanced glycolysis (increased glucose use), normal-to-mild reductions in cerebral blood flow but decreased cere-bral oxygen use despite an adequate supply of oxygen in thearterial blood (low oxygen extraction fractions). These dataare important in selecting the appropriate radiation orchemotherapeutic regimens for patients with tumors, partic-ularly as they can be measured in individual patients to deter-mine if their tumors are existing in oxygen-rich or oxygen-deprived environments. The use of PET to monitor theeffects of therapeutic modalities while doing stoichiometricstudies ofthe tumor can and should continue to play a signifi-cant role in the future understanding of the response of tu-mors to the maneuvers.
Blood-Brain-Barrier AlterationsThe initial PET studies of intracerebral neoplasms used
gallium 68 (68Ga)-labeled edetic acid to localize alteredblood-brain-barrier sites.75-78 These studies and others usingrubidium 82 (82Rb) resulted in discrete and precise localiza-tion of such tumors that correlated closely with iodinatedcontrast-enhanced x-ray CT images in the same patients.79Such studies have provided a quantitative model for calculat-ing molecular diffusion rates in and near tumors.78
ic
.a)Co
Metabolic Ratio of > 1.4oj I I0 4 8 12 16 20 24 28
MonthsFigure 3.-Glucose metabolism is correlated with prognosis in patients withhigh-grade gliomas. The ratio of glucose metabolism in tumor relative to thecontralateral brain tissue is termed the metabolic ratio. Patients having tumorswith ratios greater than 1.4 had a mean survival of 5 months, whereas thosewith tumors having ratios of less than 1.4 had a mean survival of 19 monthstfrom Patronas et al67; reproduced with permission).
Yen and associates used 82Rb to examine patients withcerebral gliomas and intracranial metastases.80 They showedthe advantages of using this isotope, which are related to theincreased mean residence time for rubidium relative to iodi-nated compounds, in addition to the rapid clearance of rubid-ium from the blood, which diminishes its recirculation.These authors concluded that 82Rb imaging was more sensi-tive than contrast CT in detecting blood-brain-barrier altera-tions because of its higher distribution volume and smallermolecular size, making the penetration of minimal blood-brain-barrier defects possible.
Rubidium 82 has also been used to examine the effects ofsteroids and whole brain irradiation on blood-brain-barrierfunction.8" It has been suggested that steroids decrease thepermeability of tumor capillaries to small hydrophilic mole-cules, including some chemotherapeutic agents, and that ste-roid pretreatment prevents abrupt increases in tumor capil-lary permeability after cranial irradiation. Within 24 hours ofadministration, giving high doses of methotrexate results inalterations in the blood-brain barrier, as shown with the useof rubidium 82, and widespread depressions of glucose me-tabolism as determined with the use of fluorodeoxyglucose.82These alterations of cerebral glucose metabolism were asso-ciated with changes in neuropsychologic performance,which were identified in the absence of systemic methotrex-ate toxicity.83
,;;Q %W_i,
Figure 4.-Tumor stoichiometry was done in a patient with a high-gradecerebral glioma located in the depth of the right cerebral hemisphere. Thispatient was evaluated with positron emission tomography to determine cere-bral blood flow (CBF), oxygen extraction ratio (OER), oxygen use (CMR02),glucose metabolism (CMRGLU), glucose extraction ratio (GER), and metabolicratio (MR) of oxygen to glucose use. Blood flow is modestly but heteroge-neously elevated in the tumor and suppressed in overlying cortical zones. Bothoxygen use and extraction are severely reduced in the tumor itself, and thelatter is moderately reduced in the overlying cortex. Glucose metabolism isincreased in these lesions, as is typical of high-grade gliomas, but suppressed inoverlying cortex, probably owing to edema and pressure effects. Glucose ex-traction is somewhat increased in the lesion, but the ratio of glucose to oxygenuse is low. This latter finding is consistent with the finding of acceleratedglycolysis in high-grade gliomas despite the adequate availability of oxygen,evidenced by the low extraction fraction of this lesion. Such a battery of studiesin an individual patient permits the determination of the biochemical signatureof lesions, such as cerebral gliomas, and the characterization of the biochemis-try that underlies their growth and response to therapy. Combined studies suchas these may prove critical in understanding the pathophysiology of tumorgrowth and may predict optimal approaches to their treatment (from Lam-mertsma et al6970; reproduced with permission).
THE WESTERN JOURNAL OF MEDICINE 9 FEBRUARY 1991 o 154 9 2 191
BRAIN TUMORS
Amino Acid IncorporationThe initial use of ["C]L-methionine with PET was re-
ported in 1983 by Bergstrom and colleagues in a single pa-tient with an anaplastic glioma.83 Since then, amino aciduptake has been used by this group to identify, for biopsyplacement, the site of low-grade gliomas that have minimalchanges in blood-brain-barrier permeability or glucose use(Figure 5).83 In addition, investigators at Johns Hopkins Uni-versity have used [11C]L-methionine and PET to evaluatebrain tumors in children. These studies are done withmethionine PET studies before and after a loading dose of acompeting nonradioactive amino acid, such as L-phenylal-anine, 100 mg per kg. The investigators noted a focal in-crease in the transport of methionine in all cases of pediatricastrocytomas and in one case of ependymoma.84 Phenylal-anine suppresses methionine uptake by the tumor, but thesuppression is greater in surrounding tissue altered by radia-tion gliosis or edema. Thus, preloading with an amino acidthat competes for the neutral amino acid carrier transportsystem results in a more specific and easily identifiable tumorsite using labeled methionine.
"C-Labeled L-leucine has also been used for estimates ofprotein synthesis in the human brain85 and in cerebral tumors(Figure 6). Because protein synthesis is enhanced in rapidlygrowing tissue, PET measurements of this process may be asensitive indicator of tumor cell growth and, hence, of prog-nosis and responsiveness to therapy.TumorpH
The pH of cerebral tumors has been determined usingweak acids, such as 'IC-labeled carbon dioxide and ITC-labeled dimethyloxazolidinedione.86-89 These studies indi-cate that there is no reduction in pH in the microenvironmentoftumors. Measurements oftumors in human subjects and inanimal models indicate that the tissue within and adjacent tocerebral neoplasms has a normal or a slightly alkaline pH.Measuring the tissue pH with PET seems a useful conceptbecause it may provide clinically relevant information aboutthe regional acid-base state and metabolism, which may havetherapeutic implications for the selection of chemotherapeu-tic agents and radiation therapy in patients with cerebraltumors.88
Figure 5.-The blood-brain-barrier integrity, glucose metabolism, and aminoacid uptake are shown in a low-grade cerebral glioma. This patient has a low-grade glioma situated at the same site as that of the patient described in Figure4, namely, deep in the right hemisphere. Blood-brain-barrier integrity is unal-tered by this lesion, as evidenced by the absence of extravasation of gallium 68edetic acid (EDTA), seen in the left image. Glucose metabolism is reduced byadministering carbon 11-labeled glucose. Amino acid uptake of the tumoris high compared with surrounding brain, as shown by carbon 11-labeledL-methionine. Such studies indicate that the uptake of compounds such asamino acids may be useful in identifying the sites of viable tumor, particularlyas a means of planning the optimal site of biopsy for such deep lesions insituations where contrast enhancement, as determined by positron emissiontomography or x-ray computed tomography, is minimal and uninformative(from Bergstrom et al85; reproduced with permission).
LigandsThe properties of tumor receptors and the ability to mea-
sure these receptors with radioisotope-tagged ligands are ar-eas of active research. This process can be simply extendedto PET for determining the receptor properties of humantumors measured externally with a PET instrument. "IC-Labeled ligands for peripheral benzodiazepine receptorcomplexes (for example, PK 11195), have already been de-veloped and should be but one of several possible radiophar-maceutic approaches to understanding the cell-surface recep-tors of tumors systemically and in the brain."3 90'91
Similarly, dopamine receptors have been visualized inpituitary adenomas using PET and "IC-labeled N-methylspi-perone.92 Patients were studied before and after haloperidolpretreatment to identify whether this compound would havesignificant blocking effects for dopamine receptors in pitui-tary adenomas. The tumor with the greatest uptake of theligand and the greatest blocking effect from haloperidol pre-treatment was in a patient with a hormonally active prolac-tinoma. Muhr and co-workers concluded that dopamine-re-ceptor binding can be identified in pituitary tumors in vivoand that this technique can be useful in understanding notonly the neuropharmacology of these tumors but also thevarying response of prolactinomas to dopamine agonists.92
In addition to using PET to identify the tumor cell-surfacereceptors, it is also possible to examine chemotherapeutic
ii
Figure 6.-Protein metabolism is shown in a high-grade (grade IV) cerebralglioma. The upper 6 images show the time course of uptake of [11C]L-leucine inthe brain of a patient with a right frontal grade IV glioma. The bottom imagesshow cerebral blood flow (CBF) measured with positron emission tomographyand iodinated contrast-enhanced x-ray computed tomography (XCT). The x-rayCT image shows two contrast-enhanced adjacent rings with central low atten-uation characteristics. Posterior to these lesions is an area of low attenuationthat extends into the white matter of the centrum semiovale. The cerebralblood flow study shows high flow in the areas of x-ray CT contrast enhance-ment with low or absent flow in the central zone. [IlC]Leucine uptake is higherin this lesion than in the normal adjacent brain. It shows a large ring patternwith a central zone of low uptake. Determinations of protein synthesis andamino acid uptake should parallel characteristics of tumor growth and mayprove to be important variables for characterizing such growth in response totherapeutic interventions.
192
THE WESTERN JOURNAL OF MEDICINE * FEBRUARY 1991 * 154 * 2 193
agents that have been labeled with positron-emitting iso-topes. An example of this approach is typified by the use of'IN-labeled cisplatin93 or 'IC-labeled carmustine (1,3-bis-[2-chloroethyl]-l-nitrosourea; BCNU), a lipophilic alkylat-ing agent.94 Using [11C]carmustine, Tyler and associateswere able to directly compare the pharmacokinetics of intra-venous versus superselective intra-arterial administration ofthe compound in patients with recurrent gliomas. Intra-arte-rial administration of the compound achieved concentrationsthat were, on the average, 50 times higher than thoseachieved with a comparable intravenous dose. The authorsconcluded that the degree of early metabolic trapping of car-mustine in tumors correlated with their clinical response tothis form of chemotherapy. Although the use of radiolabeledreceptor ligands and labeled chemotherapeutic agents has yetto provide definitive information about the pathophysiologyofcerebral neoplasms, these agents represent the tools availa-ble to neuro-oncologists for the study of these neoplastic pro-cesses. When these data are combined with the stoichiomet-ric information derived from studies with blood flow, bloodvolume, metabolism, protein synthesis, and pH, they providea broad set of biochemical and physiologic variables thatcharacterize the natural history of tumors and their responseto therapy.Adjacent and Distant Effects of Tumors asDetermined With Glucose Metabolism
All investigators who have examined tissue adjacent tocerebral neoplasms have noted reductions in glucose metabo-lism,41.61 95 blood flow, and oxygen use."3 With regard toglucose metabolism, 54 of 59 patients (92%) studied withPET had such reductions.4161'95 Overall metabolic rate re-ductions for glucose in peritumoral edema were48% 15%.The metabolic rate reduction was proportional to the totalvolume of the tumor and its edema and to the magnitude ofattenuation suppression measured by x-ray CT in edematoustissue. There was no correlation between the reduction in themetabolic rate in edematous tissue and tumor grade, tumormetabolic rate, tumor enhancement (with iodinated contraston x-ray CT), the severity or duration of neurologic symp-toms, the history of seizures, or the use of steroids or otheranticonvulsant medications.A wide range of destructive processes in the brain (for
example, cerebral infarction) have been shown by PET tocause distant effects presumably due to the disconnection ofafferent and efferent pathways traversing the site of tissuedamage.34 Cerebral neoplasms also show this phenomenon.Distant reductions in metabolism, typically linked with iden-tical reductions in blood flow, have been measured for glu-cose and oxygen use." '64,69,95 In patients with deep cerebralgliomas, suppression of glucose metabolism in the overlyingipsilateral cortex has been identified.41'6466 The reverse situ-ation is also true, and cases have been reported whereincortical tumors have resulted in a suppression of metabolicrates in the ipsilateral thalamus ofapproximately 20%. Whenblood flow has been combined with metabolic measure-ments, it has been found that reductions of a similar degree inboth variables occur in a coupled fashion.69 This is goodevidence that these distant effects are not a product of isch-emia, but rather reflect functional disconnection of onestructure from another.
reported29'34 and have a pattern similar to that seen in patientswith cerebral infarctions. In 21 such patients with supraten-torial tumors, 12 had contralateral suppression of cerebellarmetabolism ranging in magnitude from 8% to 34%. All ofthese patients had either a tumor or tumor edema involvingthe sensorimotor frontoparietal cortex with or without tha-lamic involvement. In the nine patients without contralateralcerebellar metabolic suppression, the tumors were at sitesother than those involving sensorimotor cortex. The degreeof cerebellar metabolic abnormality was related to the size ofthe tumor, to the presence of hemiparesis, and possibly to therapidity of growth of the tumor. The changes in cerebellarmetabolism did not seem to correlate with the duration ofsymptoms. The interesting phenomenon of cross-cerebellarflow and metabolic suppression represents an example of theability of PET functionally to show anatomic connectionsbetween the cerebral hemispheres and the posterior fossa.Similar results have been described in patients with otherdestructive lesions of the cerebral hemispheres as notedearlier.Tumor Recurrence Versus Radiation Necrosis
Radiation necrosis can occur in patients receiving 50 to60 grays (5,000 to 6,000 rads) of radiation to the brain.Neurologic signs and symptoms often occur months aftertherapy is completed. With the emergence of new or recur-rent symptoms referable to the same site as before tumortherapy, it is virtually impossible for clinicians to differenti-ate between the two inciting processes. Both radiation necro-sis and tumor recurrence are associated with mass effect,edema, and contrast enhancement using structural imagingmodalities such as x-ray CT or MRI; these modalities havebeen of little help in differentiating the two disorders.
Because necrotic brain does not metabolize glucose, ithas extraordinarily low metabolic rates and provides for rela-tively easy differentiation from recurrent high-grade tumorwhen measurements are made with fluorodeoxyglucose andPET (Figure 7). Recurrent high-grade tumors typically showglucose use with values similar to or in excess ofnormal greymatter. Irradiated but nonnecrotic brain tissue has severelyreduced glucose metabolic rates. Patronas and co-workersdescribed this phenomenon and accurately predicted biopsyor autopsy results in patients where this differential issue wasofclinical importance.63 Two patients had radiation necrosis,and three had recurrent tumors in this series.
In a separate and larger series by the same group, glucosemetabolism was examined in 95 patients who were referredfor the consideration of tumor recurrence versus radiationnecrosis. Of these patients, 10 were accurately diagnosed ashaving radiation necrosis and 85 were accurately diagnosedas having recurrent tumor.96 Similar results have been ob-tained in other laboratories.97 One study of34 patients had anoverall accuracy of 84% in differentiating tumor recurrencefrom radiation necrosis. This last study, however, differssomewhat from the other protocols in that many of thesepatients had brachyradiation therapy rather than conven-tional external-beam therapy.98
The value of being able to determine noninvasivelywhether new signs and symptoms in a previously treatedtumor patient represent recurrent tumor or radiation necrosisincludes the obvious advantage of avoiding biopsy in everypatient. Radiation necrosis can usually be managed medi-cally with drugs to reduce edema. Evidence of recurrent
Decreases in glucose metabolism for the cerebellar hemi-sphere contralateral to supratentorial gliomas have also been
THE WESTERN JOURNAL OF MEDICINE 9 FEBRUARY 1991 o 154 o 2 193
TUMORS~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
tumor and knowledge of its estimated histologic grade fromPET can dictate the strategy for future therapy, includingrepeat surgical resection or guided biopsy when clinicallyindicated.
Functional Activation of the Brain for Surgical PlanningIncreases in neuronal activity associated with behavioral
tasks can be determined using PET by defining blood flow orglucose metabolism.32 As noted earlier, the planning of sur-gical therapies for patients with brain tumors involves avoid-ing areas that are critical to the performance of key behaviortasks such as movement, audition, language, and vision (Fig-ure 8). By combining structural images from MRI or x-rayCT with metabolic or blood flow activation studies and PET,it is possible to identify the relation between tumor sites andadjacent or surrounding areas of functional activity. For ex-ample, consider a patient with a low-grade glioma in theposterior frontal lobe close to, but not specifically invading,the motor cortex for the hand (Figure 2). On neurologicexamination, the hand seems normal with only a minimaldegree ofclumsiness on complex testing. By measuring cere-bral blood flow or glucose metabolism while the subjectperforms a behavioral task with the hand, it is possible toidentify those cortical and subcortical structures that sub-serve the task in a given patient with cerebral tumor. Com-bining the distribution of the tumor identified from MRI, x-ray CT, or PET (the last using metabolism or tracers for
cell-surface receptors such as those for peripheral benzo-diazepine receptors), the three-dimensional spatial relationbetween the neuronal network subserving the motor task andthe tumor can be simultaneously identified. With this infor-mation, it is possible to plan the extent of the operation, thesite ofthe craniotomy, and the strategy for the resection. Suchapproaches should make surgical tumor treatment safer, re-sulting in lower morbidity as reflected by reduced neurologicdeficits postoperatively.
Clinical Strategies for Treating Malignant Brain TumorsDONALD P. BECKER, MD*: The prognosis is poor for patientswith primary malignant astrocytomas (Kernohan classifica-tion grades III and IV and World Health Organization classi-fication anaplastic astrocytoma and glioblastoma) despitesurgical excision and radiation or chemotherapy (or both).Malignant gliomas account for about half of the 9,000 newcases of primary brain tumors reported annually in theUnited States.99 These infiltrative tumors progress rapidly.Resection followed by external-beam irradiation remains thestandard treatment, yielding mean survival times of about 35weeks from the time of the operation.'00' 10 It is noteworthythat about 80% of patients have recurrence of the tumorwithin 2 cm of the initial tumor margin.102 Some workershave therefore suggested that improved local control couldlead to longer survival times.
The factors that have an important influence on patients'*Professor of Surgery, Division of Neurosurgery, UCLA School of Medicine.
Figure 7.-The upper level of images is from positron emission tomographicstudies of glucose metabolism using [18F]fluorodeoxyglucose, whereas the bot-tom images are x-ray computed tomography (XCT) scans after iodinated con-trast enhancement. The patient in the left column has radiation necrosis, andthe patient on the right has a recurrent high-grade glioma. Both x-ray CTstudies show contrast enhancement and surrounding low attenuation consis-tent with edema. A differential diagnosis based on x-ray CT alone, therefore,would not be possible, and such a decision would typically require a surgicalbiopsy. Glucose metabolism is low, or absent, in zones of radiation necrosis, asshown by the patient on the left. Recurrent tumor is evidenced by metabolismthat equals or exceeds that of normal grey matter, as shown by the patientdepicted in the right column. The patient on the right has a ring area ofhypermetabolism surrounding a central zone of tumor necrosis. The reductionin glucose metabolism in the overlying frontal cortex is probably due to edemaor pressure effects, or both.
Figure 8.-Glucose metabolic responses are shown of normal subjects per-forming behavioral tasks. The arrows indicate areas of high metabolic ratesindicative of increased neuronal activity. Normal patterns of metabolic re-sponses to behavioral tasks can be used to map critical sites of functionalneural networks in patients with cerebral tumors to avoid these areas duringtumor resection, as in the two patients whose positron emission tomographicstudies are shown in Figure 2. Both lesions are at or near the sensorimotor strip.Both of these patients have minimal signs of corticospinal tract dysfunction. Abehavioral mapping study to examine displacement and position of the func-tional motor cortex (as seen in the "motor" image of this figure) would beuseful in avoiding these critical areas during resection of the cerebral neo-plasms (from Phelps and Mazziotta32).
BRAIN TUMORS194
THE WESTERN JOURNAL OF MEDICINE * FEBRUARY 1991 * 154 * 2
survival with malignant gliomas include age, duration ofsymptoms, preirradiation performance state, tumor histol-ogy, accessibility to resection, extent of resection, radiother-apy, and a previous diagnosis of a low-grade glioma. Patientswith gross total resections live longer than those with partialresection, and patients with any degree of resection livelonger than those who undergo only a biopsy procedure.Also, patients with anaplastic gliomas in whom there was ahistory of low-grade glioma live considerably longer after thediagnosis of anaplastic glioma than do patients in whomanaplastic gliomas currently arose de novo. Some authorshave reported a difference in survival of only 19 weeks inpatients who have undergone biopsy to 76 weeks in patientswith gross total resections. Age is a strong predictor of sur-vival, with patients in the 18- to 44-year-old group having amedian survival of 107 weeks in comparison with patientsolder than 65 years who have a median survival of only 23weeks.
Recently thallium 201 (single photon emission CT) scanshave been shown to correlate with tumor histology in patientswith gliomas. A thallium index was developed based on theratio of thallium 201 uptake in the tumor versus the nonneo-plastic homologous area of brain. A thallium index of 1 rep-resented no uptake. In these patients, an index of 1.5 or lessshowed a 90% or higher accuracy of predicting which pa-tients will have low-grade gliomas versus an index of higherthan 1.5, where the tissue specimen almost always showeda grade III or grade IV glioma. In our experience, the thal-lium scan is more accurate than the CT or MRI scan in pre-dicting tissue histology because it does not rely merely on abreakdown of the blood-brain-barrier blood flow, but thethallium is recognized as a potassium analogue and is ac-tively pumped into tumor cells by sodium-potassium-adeno-sine phosphatase.503
A slight increase in the number of long-term survivors isobtained by treatment with carmustine. 04 Its full potential,however, may be limited by the delivery of high doses to thetumor site while avoiding systemic toxicity. Various attemptsto increase the concentrations of cytotoxic drugs in the brainhave proved disappointing. Other forms of regional treat-ment, including interstitial irradiation, have had some suc-cess at local control. A novel approach has recently beendeveloped to optimize local carmustine concentrations in theregion of the tumor by what has been termed "interstitialchemotherapy." A biodegradable polymer, manufactured byNova Pharmaceutical Corporation, Baltimore, Maryland,has been formulated into a solid wafer containing carmustinein the matrix. Encouraging results were obtained in a seriesof preclinical studies in rats, rabbits, and nonhuman primatesto establish the biocompatibility, biodistribution, and effi-cacy of carmustine-containing polymer wafers when im-planted intracerebrally.505"06 Phase I clinical trials haverecently been completed. In the first human study adminis-tering carmustine by interstitial chemotherapy using drug-loading polymer wafers, patients with malignant gliomas,for whom surgical therapy and radiation therapy or chemo-therapy, or both, were ineffective, underwent a second surgi-cal resection and the wafers were 'mplanted into the marginsof the surgical resection. The results of this study show thatthis may be a safe method for delivering chemotherapy intothe brain. The wafers have the advantage that they can deliverextremely high concentrations of chemotherapy into thebrain while avoiding the systemic side effects of the chemo-
therapeutic agent. In addition, there is prolonged exposure ofthe tumor cells to the chemotherapeutic compounds. Further,these wafers can be loaded with various antitumor modali-ties, so their full potential as a delivery tool for antitumorcompounds to treat brain tumors is just beginning to beexplored.
There has also been increasing interest in the impairedhumoral and cellular immune function in patients with pri-mary brain tumors. Recently there has been interest in thedevelopment of immune modifiers that stimulate the hostimmune system in patients with malignant brain tumors.Regimens using levamisole hydrochloride, poly IC, inter-feron, picibanial, or bacillus Calmette-Guerin vaccine havebeen attempted with limited success. A biologic responsemodifier, ImuVert (Cell Technology, Inc, Boulder, Colo-rado), prepared from the bacterium, Serratia marcescens,has recently been developed. ImuVert is known to stimulatethe activity of human natural killer cells in vitro, using astandard chromium-release cytotoxicity test. In addition, italso causes the release of interleukin 2, interferon, and tumornecrosis factor and stimulates lymphocytic activated killercells as well as antitumor macrophages. Because of thebroad-based immune stimulation of ImuVert, clinical trialshave recently begun testing its effects in patients with high-grade gliomas.
It is hoped that future treatment modalities may be able toconvert this universally fatal disease to a chronic diseaseprocess that can be controlled. Controlling recurrence at thesurgical margins and maintaining static growth of the tumorsby stimulating patients' immune systems might lengthen sur-vivals in these patients. Combinations of various therapiesbased on increasing knowledge of the biologic behavior ofthese tumors are currently being designed. A better defini-tion of the surgical margins is critically needed, and a way todeliver antitumor compounds successfully across the blood-brain barrier specifically to tumor cells will improve dramat-ically the effectiveness of current therapeutic modalities.
REFERENCES
1. Haefely W, Polc P, Pieri L: Neuropharmacology of benzodiazepines-Synapticmechanisms and neural basis of action, In Costa E (Ed): The Benzodiazepines: FromMolecular Biology to Clinical Practice. New York, NY, Raven Press, 1982, pp 21-66
2. Tallman JF, Paul SM, Skolnick P: Receptors for the age of anxiety: Pharmacol-ogy of the benzodiazepines. Science 1980; 207:274-281
3. Tallman JF, Gallager DW: The GABA-ergic system: A locus of benzodiazepineaction. Annu Rev Neurosci 1985; 8:21-44
4. Tallman JF, Thomas JW, Gallager DW: GABAergic modulation of benzodiaze-pine binding site sensitivity. Nature 1978; 274:383-385
5. Wastek GJ, Speth RC, Reisine TD, Yamamura HI: The effect of -y-aminobutyricacid on 3H-flunitrazepam binding in rat brain. Eur J Pharmacol 1978; 50:445447
6. Squires RF, Brastrup C: Benzodiazepine receptors in rat brain. Nature 1977;266:732-734
7. De Souza EB, Anholt RR, Murphy KM, Snyder SH, Kuhar MJ: Peripheral-typebenzodiazepine receptors in endocrine organs: Autoradiographic localization in ratpituitary, adrenal, and testis. Endocrinology 1985; 116:567-573
8. Marangos PJ, Patel J, Boulenger JP, Clark-Rosenberg R: Characterization ofperipheral-type benzodiazepine binding sites in brain using [3H]Ro 5-4864. Mol Phar-macol 1982; 22:26-32
9. Gallager DW, Mallorga P, Oertel W, Henneberry R, Tallman J: [3H]Diazepambinding in mammalian central nervous system: A pharmacological characterization. JNeurosci 1981; 1:218-225
10. Schoemaker H, Boles RG, Horst WD, Yamamura HI: Specific high-affinitybinding sites for [3H]Ro 5-4864 in rat brain and kidney. J Pharmacol Exp Ther 1983;225:61-69
11. Syapin PJ, Skolnick P: Characterization of benzodiazepine binding sites incultured cells of neural origin. J Neurochem 1979; 32:1047-1051
12. Wang JKT, Taniguchi T, Spector S: Structural requirements for the binding ofbenzodiazepine to their peripheral-type sites. Mol Pharmacol 1984; 25:349-351
13. Starosta-Rubinstein S, Ciliax BJ, Penney JB, McKeever P, Young AB: Imagingof a glioma using peripheral benzodiazepine receptor ligands. Proc NatI Acad Sci USA1987; 84:891-895
14. Black KL, Ikezaki K, Toga AW: Imaging of brain tumors using peripheralbenzodiazepine receptor ligands. J Neurosurg 1989; 71:113-118
195
BRAIN TUMORS
15. Hawkins RA, Phelps ME: Applications of positron emission tomography(PET) in tumor management, In Withers HR, Peters Li (Eds): Medical Radiology-Innovations in Radiation Oncology. Berlin, Springer-Verlag, 1988, pp 209-219
16. Eamest F 4th, Kelly PJ, Scheithauer BW, et al: Cerebral astrocytomas: Histo-pathologic correlation of MR and CT contrast enhancement with stereotactic biopsy.Radiology 1988; 166:823-827
17. Black KL, Ikezaki K, Santori E, Becker DP, Vinters HV: Specific high-affinitybinding of peripheral benzodiazepine receptor ligands to brain tumors in rat and man.Cancer 1990; 65:93-97
18. Ikezaki K, Black KL, Toga AW, et al: Imaging peripheral benzodiazepinereceptors in brain tumors of rats: In vitro binding characteristics. J Cereb Blood FlowMetab, in press
19. Anholt RR, Pedersen PL, De Souza EB, Snyder SH: The peripheral-typebenzodiazepine receptor: Localization to the mitochondrial outer membrane. J BiolChem 1986; 261:576-583
20. Basile AS, Skolnick P: Subcellular localization of 'peripheral-type' bindingsites for benzodiazepines in rat brain. J Neurochem 1986; 46:305-308
21. Wang JKT, Morgan JI, Spector S: Benzodiazepines that bind at peripheral sitesinhibit cell proliferation. Proc Natl Acad Sci USA 1984; 81:753-756
22. Pawlikowski M, Kunert-Radek J, Stepien H: Inhibition of cell proliferation ofhuman gliomas by benzodiazepines in vitro. Acta Neurol Scand 1988: 77:231-233
23. Clarke GD, Ryan PJ: Tranquillizers can block mitogenesis in 3T3 cells andinduce differentiation in Friend cells. Nature (London) 1980; 287:160-161
24. Matthew E, Laskin JD, Zimmerman EA, Weinstein IB, Hsu KC, EngelhardtDL: Benzodiazepines have high-affinity binding sites and induce melanogenesis inB16/C3 melanoma cells. Proc Natl Acad Sci USA 1981; 78:3935-3939
25. Curran T, Morgan JI: Superinduction of c-fos by nerve growth factor in thepresence of peripherally active benzodiazepines. Science 1985; 229:1265-1268
26. Diwan BA, Rice JM, Ward JM: Tumor-promoting activity of benzodiazepinetranquilizers diazepam and oxazepam in mouse liver. Carcinogenesis 1986; 7:789-794
27. Johnson MD, Wang JKT, Morgan JI, Spector S: Downregulation of [3HJRoS-4864 binding sites after exposure to peripheral-type benzodiazepines in vitro. J Phar-macol Exp Ther 1986; 238:855-859
28. Ikezaki K, Black KL: Stimulation of cell growth and DNA synthesis by periph-eral benzodiazepine (Letter). Cancer, in press
29. Hullihan JP, Spector S, Taniguchi T, Wang JK: The binding of [3H]-diazepamto guinea-pig ileal longitudinal muscle and the in vitro inhibition of contraction bybenzodiazepines. Br J Pharmacol 1983; 78:321-327
30. Ruff MR, Pert CB, Weber RJ, Wahl LM, Wahl SM, Paul SM: Benzodiazepinereceptor-mediated chemotaxis of human monocytes. Science 1985; 229:1281-1283
31. Di Chiro G, Brooks RA, Sokoloff L: Glycolytic rate and histologic grade ofhuman cerebral gliomas: A study with 8F-fluorodeoxyglucose and positron emissiontomography, In Heiss WD, Phelps ME (Eds): Positron Emission Tomography of theBrain. New York, NY, Springer Verlag, 1983, pp 182-201
32. Phelps ME, Mazziotta JC: Positron emission tomography: Human brain func-tion and biochemistry. Science 1985; 228:799-780
33. Phelps ME, Mazziotta JC, Shelbert HR: Positron Emission Tomography andAutoradiography. New York, NY, Raven Press, 1986
34. Mazziotta JC, Phelps ME: Positron Emission Tomography: Studies of theBrain. New York, NY, Raven Press, 1986, pp 493-580
35. Fowler JS, Wolf AP: Positron Emitted Labeled Compounds: Priorities andProblems. New York, NY, Raven Press, 1986, pp 391-450
36. Barrio JR: Biochemical Principles in Radiopharmaceuticals: Designs and Uti-lization. New York, NY, Raven Press, 1986, pp 451-492
37. Hoffman EJ, Phelps ME: Positron Emission Tomography: Principles andQuantitation. New York, NY, Raven Press, 1986, pp 237-28638. Fowler JS, Hoffman EJ, Larson SM, et al: Positron emission tomography in
oncology-Council on Scientific Affairs: Report of the Positron Emission TomographyPanel. JAMA 1988; 259:2126-2131
39. Thomas DG, Beaney RP, Brooks DJ: Positron emission tomography in thestudy of cerebral tumors. Neurosurg Rev 1984; 7:253-258
40. Wise RJ, Thomas DG, Lammertsma AA, Rhodes CG: PET scanning of humanbrain tumors. Prog Exp Tumor Res 1984; 27:154-169
41. Di Chiro G, DeLaPaz RL, Brooks RA, et al: Glucose utilization of cerebralgliomas measured by [18Fjfluorodeoxyglucose and positron emission tomography.Neurology (NY) 1982; 32:1323-1329
42. Hawkins RA, Phelps ME: PET in clinical oncology. Cancer Metastasis Rev1988; 7:119-142
43. Beaney RP: Positron emission tomography in the study of human tumors.Semin Nucl Med 1984; 14:324-341
44. Brooks DJ, Beaney RP, Thomas DG: The role ofpositron emission tomographyin the study of cerebral tumors. Semin Oncol 1986; 13:83-9345. Brownell GL, Kairento AL, Swartz M, Elmaleh DR: Positron emission tomog-
raphy in oncology-The Massachusetts General Hospital experience. Semin Nucl Med1985; 15:201-20946. Di Chiro G: Brain imaging of glucose utilization in cerebral tumors, In Soko-
loff L (Ed): Brain Imaging and Brain Function. New York, NY, Raven Press, 1985, pp185-197
47. Di Chiro G: Diagnostic and prognostic value of positron emission tomographyusing 18F-fluorodeoxyglucose in brain tumors, In Reivich M, Alavi A (Eds): PositronEmission Tomography. New York, NY, Alan R. Liss, 1985, pp 291-309
48. Di Chiro G: Positron emission tomography using 18F-fluorodeoxyglucose inbrain tumors: A powerful diagnostic and prognostic tool. Invest Radiol 1987; 22:360-37149. Miraldi F: Potential ofNMR and PET for determining tumor metabolism. Int J
Radiat Oncol Biol Phys 1986; 12:1033-103950. Larson S: Positron emission tomography in oncology and allied diseases, In
DeVita VT Jr, Hellman S, Rosenberg SA (Eds): Cancer: Principles and Practice ofOncology, 2nd ed. Philadelphia, Pa, JB Lippincott, 1989, pp 1-12
51. Weber G: Enzymology of cancer cells (pt I and 2). N Engl J Med 1977;296:486-492; 541-551
52. Warburg 0: The Metabolism of Tumors. London, Constable, 193053. Phelps ME, Huang SC, Hoffman EJ, Selin C, Sokoloff L, Kuhl DE: Tomo-
graphic measurement of local cerebral glucose metabolic rate in humans with (F- 18)2-fluoro-2-deoxyglucose: Validation of method. Ann Neurol 1979; 6:371-388
54. Sokoloff L, Reivich M, Kennedy C, et al: The ['4C]deoxyglucose method forthe measurement of local cerebral glucose utilization: Theory, procedure, and normalvalues in the conscious and anesthetized albino rat. J Neurochem 1977; 28:897-916
55. Reivich M, Kuhl D, Wolf A, et al: The 18F-fluorodeoxyglucose method for themeasurement of local cerebral glucose utilization in man. Circ Res 1979; 44:127-137
56. Hossmann Ka, Niebuhr I, Tamura M: Local cerebral blood flow and glucoseconsumption rate with experimental gliomas. J Cereb Blood Flow Metab 1982; 2:25-32
57. Di Chiro G, Brooks R, Patronas NJ, et al: Issues in the in vivo measurement ofglucose metabolism of human central nervous system tumors. Ann Neurol 1984;15(Suppl):S138-146
58. Di Chiro G, DeLaPaz R, Smith B, et al: 18F-2-Fluoro-2-deoxyglucose positronemission tomography of human cerebral gliomas. J Cereb Blood Flow Metab 1981;I(Suppl):SI l-S12
59. Di Chiro G, Oldfield E, Bairamian D, et al: In Vivo Glucose Utilization ofTumors of the Brain Stem and Spinal Cord. Proceedings of the VIlth Nobel Confer-ence, 1985, pp 351-362
60. Brooks RA, Di Chiro G, Tran AA, Petronas NJ, DeLaPaz RL: Measurement ofglucose-6-phosphatase in normal brain tissue (Abstr). Ann Neurol 1982; 12:91
61. DeLaPaz RL, Patronas NJ, Brooks RA, et al: A PET study of suppression ofglucose utilization in cerebral gray matter associated with brain tumor. J Cereb FlowMetab 1983; 3(Suppl):S21-S22
62. Patronas NJ, Brooks RA, DeLaPaz RL, Smith BH, Komblith PL, Di Chiro G:Glycolytic rate (PET) and contrast enhancement (CT) in human cerebral gliomas.AJNR 1983; 4:533-535
63. Patronas NJ, Di Chiro G, Brooks RA, et al: Work in progress: [18FJFluoro-deoxyglucose and positron emission tomography in the evaluation of radiation necrosisof the brain. Radiology 1982; 144:885-890
64. Patronas NJ, Di Chiro G, Smith BH, et al: Depressed cerebellar glucosemetabolism in supratentorial tumors. Brain Res 1984; 291:93-101
65. Di Chiro G, Oldfield E, Bairamian D, et al: Metabolic imaging of the brainstem and spinal cord: Studies with positron emission tomography using 18F-2-deoxy-glucose in normal and pathological cases. J Comput Assist Tomogr 1983; 7:937-945
66. Tyler JL, Diksic M, Villemure JG, et al: Metabolic and hemodynamic evalua-tion of gliomas using positron emission tomography. J Nucl Med 1987; 28:1123-1133
67. Patronas NJ, Di Chiro G, Kufta C, et al: Prediction of survival in gliomapatients by means of positron emission tomography. J Neurosurg 1985: 62:816-822
68. Alavi JB, Alavi A, Chawluk J, et al: Positroni emission tomography in patientswith glioma-A predictor of prognosis. Cancer 1988; 62:1074-1078
69. Lammertsma AA, Itoh M, McKenzie CG, et al: Quantitative tomographicmeasurements of regional cerebral blood flow and oxygen utilization in patients withbrain tumors using oxygen- 15 and positron emission tomography. J Cereb Blood FlowMetab 1981; 1 (Suppl):S567-S568
70. Lammertsma AA, Wise R. Gibbs J, et al: The pathophysiology of humancerebral tumors and surrounding white matter and remote cortex. J Cereb Blood FlowMetab 1983; 3(Suppl):S9-S10
71. Ito M, Lammertsma AA, Wise RJ, et al: Measurement of regional cerebralblood flow and oxygen utilisation in patients with cerebral tumours using 150 andpositron emission tomography: Analytical techniques and preliminary results.Neuroradiology 1982; 23:63-74
72. Rhodes CG, Wise RJ, Gibbs JM, et al: In vivo disturbance of the oxidativemetabolism of glucose in human cerebral gliomas. Ann Neurol 1983; 14:614-626
73. Beaney RP, Lammertsma AA, Jones T, McKenzie CG, Halnan KE: Positronemission tomography for in-vivo measurement of regional blood flow, oxygen utilisa-tion, and blood volume in patients with breast carcinoma. Lancet 1984; 1:131-134
74. Beaney RP, Brooks DJ, Leenders KL, Thomas DG, Jones T, Halnan KE: Bloodflow and oxygen utilisation in the contralateral cerebral cortex of patients with un-treated intracranial tumours as studied by positron emission tomography, with observa-tions on the effect of decompressive surgery. J Neurol Neurosurg Psychiatry 1985;48:310-319
75. Phelps ME, Hoffman EJ, Huang SC, et al: Design and performance character-istics of the ECAT positron tomography. J Comput Assist Tomogr 1978; 2:648
76. Thompson CJ, Yamamoto YL. Meyer E: Positrome II: A high efficiency PETdevice for dynamic studies. J Comput Assist Tomogr 1978; 2:650-651
77. Yamamoto YL, Thompson CJ, Meyer E, Robertson JS, Feindel W: Dynamicpositron emission tomography for study of cerebral hemodynamics in a cross section ofthe head using positron-emitting 68Ga-EDTA and 77Kr. J Comput Assist Tomogr 1977;1:43-55
78. Hawkins RA, Phelps Me, Huang SC: A kinetic evaluation of blood brainbarrier permeability in human brain tumors with 68Ga-EDTA and PET. J Cereb BloodFlow Metab 1984; 4:507-515
79. Jarden JO, Dhawan V, Kearfott KJ, Rottenberg DA: Measurement of brain/tumor capillary permeability using 82Rb and positron emission tomography (Abstr).Ann Neurol 1984; 16:131
80. Yen CK, Budinger TF, Friedland RP, Derenzo SE, Huesman RH, O'BrienMA: Brain tumor evaluation using Rb-82 and positron emission tomography. J NuclMed 1982; 23:532-537
81. Jarden JO, Dhawan V, Poltorak A, Posner JB, Rottenberg DA: Positron emis-sion tomographic measurement of blood-to-brain and blood-to-tumor transport of82Rb: The effect of dexamethasone and whole-brain radiation therapy. Ann Neurol1985; 18:636-646
82. Phillips PC, Dhawan V, Strother SC, et al: Reduced cerebral glucose metabo-lism and increased brain capillary permeability following high-dose methotrexate che-motherapy: A positron emission tomographic study. Ann Neurol 1987; 21:59-63
196
THE WESTERN JOURNAL OF MEDICINE * FEBRUARY 1991 * 154
83. Bergstrom M, Collins VP, Ehrin E, et al: Discrepancies in brain tumor extentas shown by computed tomography and positron emission tomography using[68GaJEDTA, [l 'C]glucose and ["Cimethionine. J Comput Assist Tomogr 1983;7:1062-1066
84. O'Tuama LA, Williams JA, La France ND, et al: Role of I"C-L-methioninepositron emission tomography in the case of children with brain tumors. Ann Neurol1986; 20:422
85. Hawkins RA, Huang SC, Barrio JR: Estimation of local cerebral proteinsynthesis rates with L-[I I'Cleucine and PET: Methods, model and results in animalsand humans. J Cereb Blood Flow Metab 1989: 9:446460
86. Amold JB, Kraig RP, Rottenberg DA: In vivo measurement of regional braintumor pH using [14Cldimethyloxazolidinedione and quantitative autoradiography-II:Characterization of the extracellular fluid compartment using pH-sensitive microelec-trodes and [14C]sucrose. J Cereb Blood Flow Metab 1986; 6:435-440
87. Brooks DJ, Beaney RP, Thomas DGT, Marshall J, Jones T: Studies on regionalcerebral pH in patients with cerebral tumours using continuous inhalation of ' ICO2 andpositron emission tomography. J Cereb Blood Flow Metab 1986; 6:529-535
88. Rottenberg DA, Ginos JZ, Kearfott KJ, Junck L, Dhawan V, Jarden JO: In vivomeasurement of brain tumor pH using [I ICJDMO and positron emission tomography.Ann Neurol 1985; 17:70-79
89. Mies G, Paschen W, Csiba L, et al: Comparison of regional tissue pH measuredwith umbelliferone and 14C-DMO in experimental brain tumours of rat. J Cereb BloodFlow Metab 1985; Suppl I
90. Richfield EK, Ciliax BJ, Starosta-Rubinstein SR, McKeever PE, Penney JB,Young AB: Comparison of 14C-deoxyglucose metabolism and peripheral benzodiaze-pine receptor binding in rat C6 glioma. Neurology 1988; 38:1255-1262
91. Junck L, Koeppe RA, Watkins GL, et al: Glioma imaging with a peripheralbenzodiazepine ligand (Abstr). Neurology 1988: 38(Suppl):307
92. Muhr C, Bergstrom M, Lundberg PO, et al: Dopamine receptors in pituitaryadenomas: PET visualization with "IC-N-methylspiperone. J Comput Assist Tomogr1986; 10:175-180
93. Ginos JZ, Cooper AJL, Dhawan V, et al: p['3N]Cisplatin PET to assess phar-macokinetics of intra-arterial versus intravenous chemotherapy for malignant braintumors. J Nucl Med 1987; 28:1844-1852
94. Tyler JL, Yamamoto YL, Diksic M, et al: Pharmacokinetics of superselectiveintra-arterial and intravenous I' IC]BCNU evaluated by PET. J Nucl Med 1986; 27:775-780
95. DeLaPaz RL, Patronas NJ, Brooks RA, et al: Positron emission tomographicstudy of suppression of gray-matter glucose utilization by brain tumors. AJNR 1983;4:826-829
96. Di Chiro G, Oldfield E, Wright DC, et al: Cerebral necrosis after radiotherapyand/or intraarterial chemotherapy for brain tumors: PET and neuropathologic studies.AJR 1988; 150:189-197
97. Doyle WK, Budinger TF, Valk PE, Levin VA, Gutin PH: Differentiation ofcerebral radiation necrosis from tumor recurrence by [18FJ-FDG and 82Rb positronemission tomography. J Comput Assist Tomogr 1987; 11:563-570
98. Valk PE, Budinger TF. Levin VA, Silver P, Gutin PH, Doyle WK: PET ofmalignant cerebral tumors after interstitial brachytherapy: Demonstration of metabolicactivity and correlation with clinical outcome. J Neurosurg 1988; 69:830-838
99. Wilson CG: Tumors of the central nervous system, In Horton J, Hill GH (Eds):Clinical Oncology. Philadelphia, Pa, WB Saunders, 1977, pp 588-617
100. Walker MD, Strike TA, Sheline GE: An analysis of dose-response relation-ship in the radiotherapy of malignant gliomas. Int J Radiat Oncol Biol Phys 1979;5:1725-1731
101. Winger NI, MacDonald DR, Kairncross JG: Supratentorial anaplasticgliomas in adults: The prognostic importance of extended resection in prior low-gradeglioma. J Neurosurg 1989; 71:487-493
102. Wallner KE, Galicich JH, Krol G, Arbit E, Malkin MG: Pattems of failurefollowing treatment for glioblastoma multiforme and anaplastic astrocytoma. Int JRadiat Oncol Biol Phys 1989; 16:1405-1409
103. Black KL, Hawkins RA, Kim KT, Becker DP, Lemer C, Marciano D: Use ofthallium-201 SpECT to quantitate malignancy grade of gliomas. J Neurosurg 1989;71:342-346
104. Wilson CB, Boldrey EB, Knot KJ: 1,3-Bis(2-chloroethyl)-l-nitrosourea(NSC-409962) in the treatment of brain tumors. Cancer Chemother Rep 1970; 54:273-281
105. Tamargo RJ, Epstein JI, Reinhard CS, Chasin M, Brem H: Brain biocompati-bility of a biodegradable controlled-release polymer in rats. J Biomed Mater Res 1989;23 :253-266
106. Grossman SA, Reinhard CS, Brem H, et al: The intracerebral delivery ofBCNU with surgically implanted bioerodible polymers: A quantitative autoradio-graphic study (Abstr). Proc Am Soc Clin Oncol 1988; 7:84
THE WESTERN JOURNAL OF MEDICINE 9 FEBRUARY 1991 e 154 197

![Characterization of Thread Proteins Expressed in ......ICANCERRESEARCH53,3823-3821,Augustis. ITO] Characterization of Thread Proteins Expressed in Neuroectodermal Tumors1 Yong-Yao](https://img.pdfslide.us/doc/110x75/5f5a2323a3458236c95847d0/characterization-of-thread-proteins-expressed-in-icancerresearch533823-3821augustis.jpg)



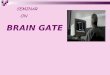



![of Established Tumors1 - Home | Cancer Researchcancerres.aacrjournals.org/content/canres/60/15/4152...[CANCER RESEARCH 60, 4152–4160, August 1, 2000] SU6668 Is a Potent Antiangiogenic](https://img.pdfslide.us/doc/110x75/5affd89b7f8b9a54578bb364/of-established-tumors1-home-cancer-cancer-research-60-41524160-august-1.jpg)