Embed Size (px)
Citation preview
Journal ol Neurology, Neurosurgery, and Psychiatry 1986;49:278-289
Brain stem auditory evoked potentials in patients withmultiple system atrophy with progressive autonomicfailure (Shy-Drager syndrome)
DEEPAK PRASHER,* ROGER BANNISTER
From the Medical Research Council Neuro-Otology{Unit, Institute of Neurology* and the National HospitalforNervous Diseases, London, UK
SUMMARY Brain stem potentials from three groups of patients, namely those with pure progressiveautonomic failure, Parkinson's disease and multisystem atrophy with progressive autonomic failure(Shy-Drager syndrome) were compared with each other and a group of normal subjects. In virtuallyall the patients with multisystem atrophy with progressive autonomic failure the brain stem poten-tials were abnormal in contrast to normal findings with Parkinson's disease. The closely associatedgroup of patients with progressive autonomic failure alone also revealed no abnormalities of theBAEP. This separation of the two groups, Parkinson's disease and progressive autonomic failurefrom multisystem atrophy with progressive autonomic failure is important clinically as multiplesystem atrophy of the Shy-Drager type has extra-pyramidal features closely resembling Parkin-sonism or a late onset cerebellar degeneration. From the abnormalities of the brain stem responsein multisystem atrophy with progressive autonomic failure, it is clear that some disruption of theauditory pathway occurs in the ponto-medullary region as in nearly all patients there is a significantdelay or reduction in the amplitude of components of the response generated beyond this region.The most likely area involved is the superior olivary complex.
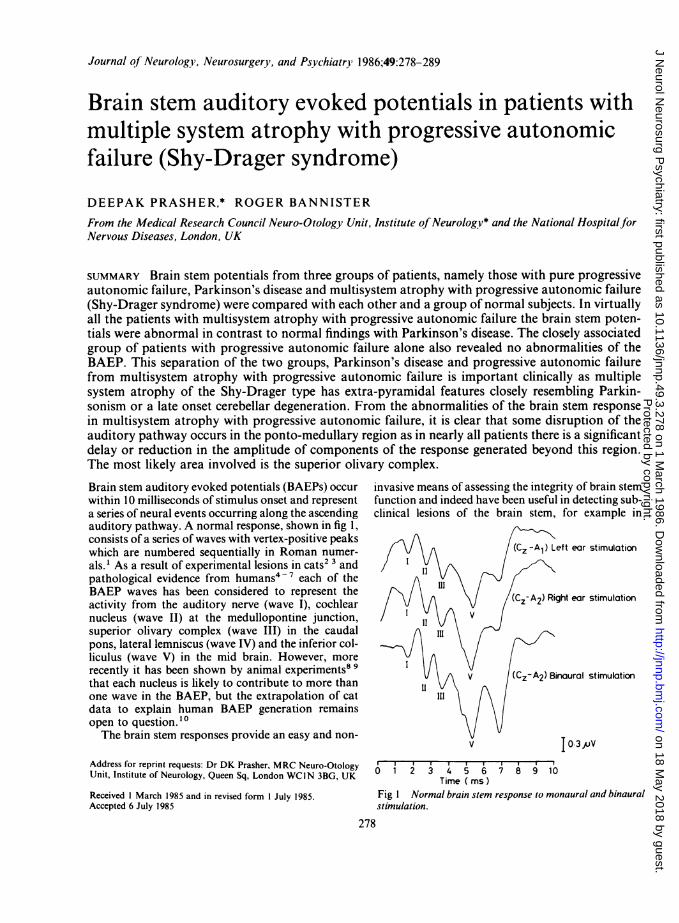
Brain stem auditory evoked potentials (BAEPs) occurwithin 10 milliseconds of stimulus onset and representa series of neural events occurring along the ascendingauditory pathway. A normal response, shown in fig 1,consists of a series of waves with vertex-positive peakswhich are numbered sequentially in Roman numer-als.' As a result of experimental lesions in cats2 3 andpathological evidence from humans4-7 each of theBAEP waves has been considered to represent theactivity from the auditory nerve (wave I), cochlearnucleus (wave II) at the medullopontine junction,superior olivary complex (wave I1I) in the caudalpons, lateral lemniscus (wave IV) and the inferior col-liculus (wave V) in the mid brain. However, morerecently it has been shown by animal experiments8 9that each nucleus is likely to contribute to more thanone wave in the BAEP. but the extrapolation of catdata to explain human BAEP generation remainsopen to question.l°The brain stem responses provide an easy and non-
Address for reprint requests: Dr DK Prasher, MRC Neuro-OtologyUnit, Institute of Neurology, Queen Sq. London WCIN 3BG. UK
Received I March 1985 and in revised form I JuIY 1985.Accepted 6 July 1985
invasive means of assessing the integrity of brain stemfunction and indeed have been useful in detecting sub-clinical lesions of the brain stem, for example in
(Cz -A) Left ear stimulation
(C-zA2) Right ear stimulation
V (Cz-A2) Binaural stimulation
Vv I0-3 V
0 1 2 3 4 5 6 7 8 9 10Time (ims)
Fig I Normal brain stem response to monaural and binauralstimulation.
278
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from
Brain stem auditory evoked potentials in patients with multiple systematrophy27Table 1 Group composition
Groups tested Male Female Age range Mean age (y)Normals n = 32 12 20 20-56 44Parkinson's disease n = 20 13 7 41-69 58Progressive autonomic failure n = 6 3 3 51-55 53Multiple system atrophy with progressive autonomic failure
(Shy-Drager syndrome) n = 14 9 5 43-71 59
Table 2 Pathology in groups tested
Regions of the brain Neuro-pathology Auditory pathway and origins ofinvolved pathologically brain stem response wavesMultiple system atrophy Parkinson's disease Progressivewith progressive, atnmcalrautonomicfailureaunmifilr(Shy-Drager syndrome)
Level of thalamus and basal gangliaCaudate nucleus + +Putamen + + Medial geniculate bodyGlobus pallidus + +Substantia nigra ++ + (Lewy bodies) + (Lewy bodies)
Level of brainstemEdinger-Westphal nucleus + Inferior colliculus Wave VTegmentum pontis + Lateral lemniscus Wave IVLocus coeruleus + + + Superior olivary
Complex Wave IIIPonto-cerebellar tract + Trapezoid bodyDorsal vagal nucleus + +Hypoglossal nucleus + Cochlear nucleus Wave IILateral cuneate nucleus +Inferior olive + + Auditory nerveNucleus ambiguus + + Spiral ganglion Wave I
patients with multiple sclerosis." 12 Abnormalities ofthe BAEP have also been reported in heredo-degenerative diseases such as Friedreich's ataxia'"and Charcot-Marie-Tooth disease.'4
There are conflicting reports at present regardingthe brain stem responses in Parkinson's disease.Gawel et al'5 reported prolongation of the latency ofwave V without any effect on its amplitude but Kriss(personal communication) was unable to confirmthese findings in a large group of patients. Tsuji et al'6and Chiappa'7 also report normal BAEPs in patientswith Parkinson's disease.
Similar anomalies exist with the visual evokedpotential (VEP) in that Bodis-Wollner et al'8 andGawel et al'5 reported VEP abnormalities in Parkin-son's disease whilst others'1920 have been unable toconfirm this. In this study, brain stem potentials fromthree different groups of patients, namely those withprogressive autonomic failure, Parkinson's diseaseand multiple system atrophy with progressive auto-nomic failure (Shy-Drager syndrome) were comparedwith each other and with a group of normal subjects.The main aim of the study was (a) to evaluate theusefulness of brain stem potentials in differentiatingbetween patients in the groups especially those withParkinson's disease from those with multisystem
atrophy with progressive autonomic failure and (b) torelate the extent of the brain stem involvement by thedisease in particular patients with the abnormalitiesof the brain stem potentials.
Methods
The brain stem potentials were recorded with conventionalEEG silver/silver chloride disc electrodes placed at the vertex(Cz) and upon each mastoid. The ground electrode ,wasplaced at the chin. Responses from Cz-AlI, and Cz-A2 wererecorded to ipsilateral, contralateral and binaural stimu-lation. The patient sat in a comfortable reclining chair in asound-proof chamber and listened through TDH 39 ear-phones to clicks (rectangular pulses of 100 us electricalduration) at an intensity level of 90 dB SL presented at a rateof 10 Hz. The electrical activity was amplified (x l0-'),filtered (3-2Hz to 3-2kHz), digitised every 10 ps for 1024points giving an analysis window of 10-24 ins. A total of1024 stimulus presentations were made for each average.T'he latencies of the waves were measured with a cursorunder program control. Responses were obtained twice foreach configuration in order to check the replicability. Fourof the 14 patients with multisystem atrophy with progressiveautonomic failure were retested after 2-6 months in order tocheck whether the response abnormalities were consistent orotherwise, over a period of time. The analysis of the BAEPrecordings was restricted to waves I, III and V as these are
279
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from
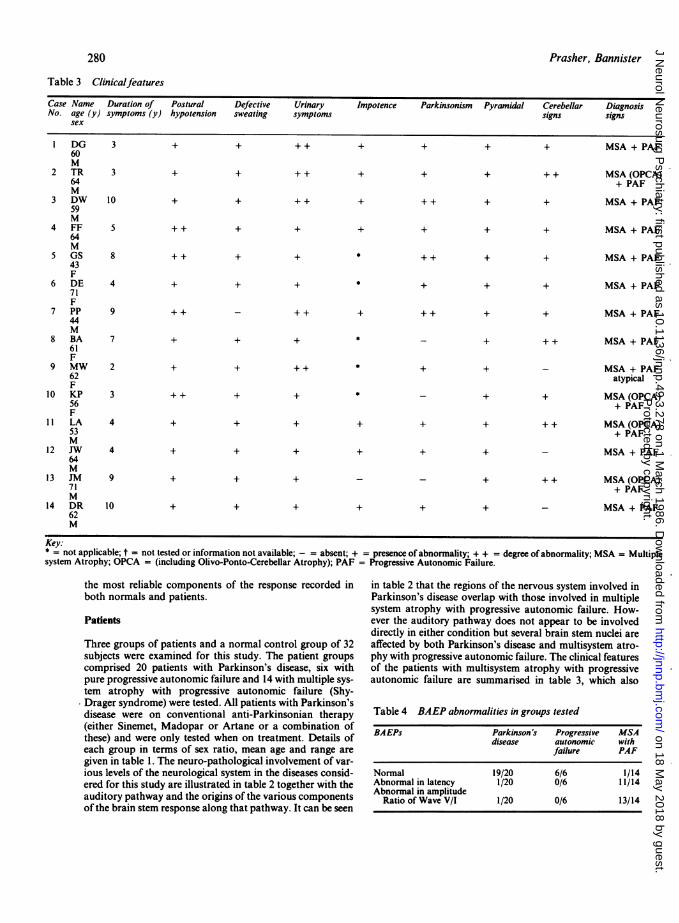
Table 3 Clinicalfeatures
Case Name Duration of Postural Defective Urinary Impotence Parkinsonism Pyramidal Cerebellar DiagnosisNo. age (y) symptoms (y) hypotension sweating symptoms signs signs
sex
1 DG 3 + + + + + + + + MSA + PAF60M
2 TR 3 + + + + + + + + + MSA (OPCA)64 + PAFM
3 DW 10 + + + + + + + + + MSA + PAF59M
4 FF 5 + + + + + + + + MSA + PAF64M
5 GS 8 + + + + * + + + + MSA + PAF43F
6 DE 4 + + + * + + + MSA + PAF71F
7 PP 9 + + - + + + + + + + MSA + PAF44M
8 BA 7 + + + * - + + + MSA + PAF61F
9 MW 2 + + ++ * + + - MSA + PAF62 atypicalF
10 KP 3 ++ + + * _ + + MSA (OPCA)56 + PAFF
11 LA 4 + + + + + + + + MSA(OPCA)53 + PAFM
12 JW 4 + + + + + + - MSA + PAF64M
13 JM 9 + + + - _ + + + MSA(OPCA)71 + PAFM
14 DR 10 + + + + + + - MSA + PAF62M
Key:* = not applicable; t = not tested or information not available; - = absent; + = presence of abnormality; + + = degree of abnormality; MSA = Multiplesystem Atrophy; OPCA = (including Olivo-Ponto-Cerebellar Atrophy); PAF = Progressive Autonomic Failure.
the most reliable components of the response recorded inboth normals and patients.
Patients
Three groups of patients and a normal control group of 32subjects were examined for this study. The patient groupscomprised 20 patients with Parkinson's disease, six withpure progressive autonomic failure and 14 with multiple sys-tem atrophy with progressive autonomic failure (Shy-Drager syndrome) were tested. All patients with Parkinson'sdisease were on conventional anti-Parkinsonian therapy(either Sinemet, Madopar or Artane or a combination ofthese) and were only tested when on treatment. Details ofeach group in terms of sex ratio, mean age and range aregiven in table 1. The neuro-pathological involvement of var-ious levels of the neurological system in the diseases consid-ered for this study are illustrated in table 2 together with theauditory pathway and the origins of the various componentsof the brain stem response along that pathway. It can be seen
in table 2 that the regions of the nervous system involved inParkinson's disease overlap with those involved in multiplesystem atrophy with progressive autonomic failure. How-ever the auditory pathway does not appear to be involveddirectly in either condition but several brain stem nuclei areaffected by both Parkinson's disease and multisystem atro-phy with progressive autonomic failure. The clinical featuresof the patients with multisystem atrophy with progressiveautonomic failure are summarised in table 3, which also
Table 4 BAEP abnormalities in groups tested
BAEPs Parkinson's Progressive MSAdisease autonomic with
failure PAF
Normal 19/20 6/6 1/14Abnormal in latency 1/20 0/6 11/14Abnormal in amplitude
Ratio of Wave V/I 1/20 0/6 13/14
280 Prasher, Bannister
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from
Brain stem auditory evoked potentials in patients with multiple system atrophy
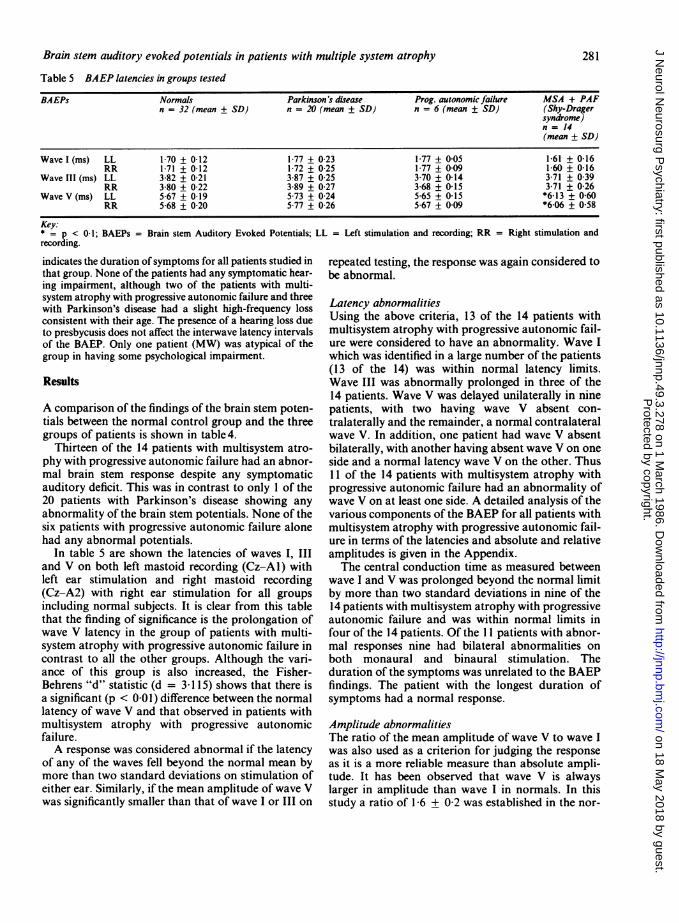
Table 5 BAEP latencies in groups tested
BAEPs Normals Parkinson's disease Prog. autonomic failure MSA + PAFn = 32 (mean + SD) n = 20 (mean + SD) n = 6 (mean + SD) (Shy-Drager
syndrome)n = 14(mean ± SD)
Wave I (ms) LL 1 70 + 0-12 1-77 + 0-23 1-77 + 005 1-61 + 0-16RR 1-71 + 0-12 1-72 + 0-25 1-77 + 0-09 1 60 0-16
Wave III (ms) LL 3-82 + 0-21 3-87 ± 0 25 3 70 ± 0-14 3-71 ± 039RR 3-80 + 0-22 3-89 + 0-27 3-68 + 0-15 3-71 + 0-26
Wave V (ms) LL 567 + 019 5.73 + 0-24 565 + 015 *6-13 + 060RR 5-68 + 0-20 5 77 + 0-26 5-67 + 009 *6-06 + 0 58
Key:* = p < 0-1; BAEPs = Brain stem Auditory Evoked Potentials; LL = Left stimulation and recording; RR = Right stimulation andrecording.
indicates the duration ofsymptoms for all patients studied inthat group. None of the patients had any symptomatic hear-ing impairment, although two of the patients with multi-system atrophy with progressive autonomic failure and threewith Parkinson's disease had a slight high-frequency lossconsistent with their age. The presence of a hearing loss dueto presbycusis does not affect the interwave latency intervalsof the BAEP. Only one patient (MW) was atypical of thegroup in having some psychological impairment.
Results
A comparison of the findings of the brain stem poten-tials between the normal control group and the threegroups of patients is shown in table4.
Thirteen of the 14 patients with multisystem atro-phy with progressive autonomic failure had an abnor-mal brain stem response despite any symptomaticauditory deficit. This was in contrast to only I of the20 patients with Parkinson's disease showing anyabnormality of the brain stem potentials. None of thesix patients with progressive autonomic failure alonehad any abnormal potentials.
In table 5 are shown the latencies of waves I, IIIand V on both left mastoid recording (Cz-Al) withleft ear stimulation and right mastoid recording(Cz-A2) with right ear stimulation for all groupsincluding normal subjects. It is clear from this tablethat the finding of significance is the prolongation ofwave V latency in the group of patients with multi-system atrophy with progressive autonomic failure incontrast to all the other groups. Although the vari-ance of this group is also increased, the Fisher-Behrens "d" statistic (d = 3 115) shows that there isa significant (p < 0 01) difference between the normallatency of wave V and that observed in patients withmultisystem atrophy with progressive autonomicfailure.A response was considered abnormal if the latency
of any of the waves fell beyond the normal mean bymore than two standard deviations on stimulation ofeither ear. Similarly, if the mean amplitude of wave Vwas significantly smaller than that of wave I or III on
repeated testing, the response was again considered tobe abnormal.
Latency abnormalitiesUsing the above criteria, 13 of the 14 patients withmultisystem atrophy with progressive autonomic fail-ure were considered to have an abnormality. Wave Iwhich was identified in a large number of the patients(13 of the 14) was within normal latency limits.Wave III was abnormally prolonged in three of the14 patients. Wave V was delayed unilaterally in ninepatients, with two having wave V absent con-tralaterally and the remainder, a normal contralateralwave V. In addition, one patient had wave V absentbilaterally, with another having absent wave V on oneside and a normal latency wave V on the other. Thus11 of the 14 patients with multisystem atrophy withprogressive autonomic failure had an abnormality ofwave V on at least one side. A detailed analysis of thevarious components of the BAEP for all patients withmultisystem atrophy with progressive autonomic fail-ure in terms of the latencies and absolute and relativeamplitudes is given in the Appendix.The central conduction time as measured between
wave I and V was prolonged beyond the normal limitby more than two standard deviations in nine of the14 patients with multisystem atrophy with progressiveautonomic failure and was within normal limits infour of the 14 patients. Of the 11 patients with abnor-mal responses nine had bilateral abnormalities onboth monaural and binaural stimulation. Theduration of the symptoms was unrelated to the BAEPfindings. The patient with the longest duration ofsymptoms had a normal response.
Amplitude abnormalitiesThe ratio of the mean amplitude of wave V to wave Iwas also used as a criterion for judging the responseas it is a more reliable measure than absolute ampli-tude. It has been observed that wave V is alwayslarger in amplitude than wave I in normals. In thisstudy a ratio of 1-6 + 0 2 was established in the nor-
281
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from
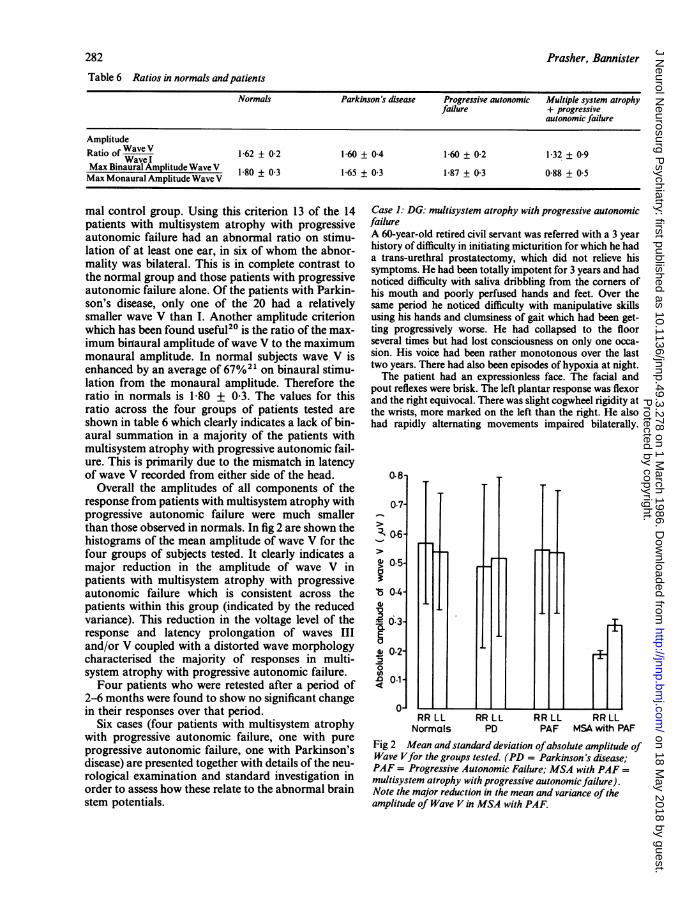
Table 6 Ratios in normals andpatients
Normals Parkinson's disease Progressive autonomic Multiple system atrophyfailure + progressive
autonomic failure
AmplitudeRatio of WaveV 1-62 + 0-2 1-60 + 04 1-60 + 0-2 132 + 09Wave IMax Binaural Amplitude Wave V 1-80 + 0-3 1-65 + 0-3 1-87 + 0-3 0-88 + 0 5Max Monaural Amplitude Wave V
mal control group. Using this criterion 13 of the 14patients with multisystem atrophy with progressiveautonomic failure had an abnormal ratio on stimu-lation of at least one ear, in six of whom the abnor-mality was bilateral. This is in complete contrast tothe normal group and those patients with progressiveautonomic failure alone. Of the patients with Parkin-son's disease, only one of the 20 had a relativelysmaller wave V than I. Another amplitude criterionwhich has been found useful20 is the ratio of the max-imum birnaural amplitude of wave V to the maximummonaural amplitude. In normal subjects wave V isenhanced by an average of 67%21 on binaural stimu-lation from the monaural amplitude. Therefore theratio in normals is 1 80 + 0 3. The values for thisratio across the four groups of patients tested areshown in table 6 which clearly indicates a lack of bin-aural summation in a majority of the patients withmultisystem atrophy with progressive autonomic fail-ure. This is primarily due to the mismatch in latencyof wave V recorded from either side of the head.
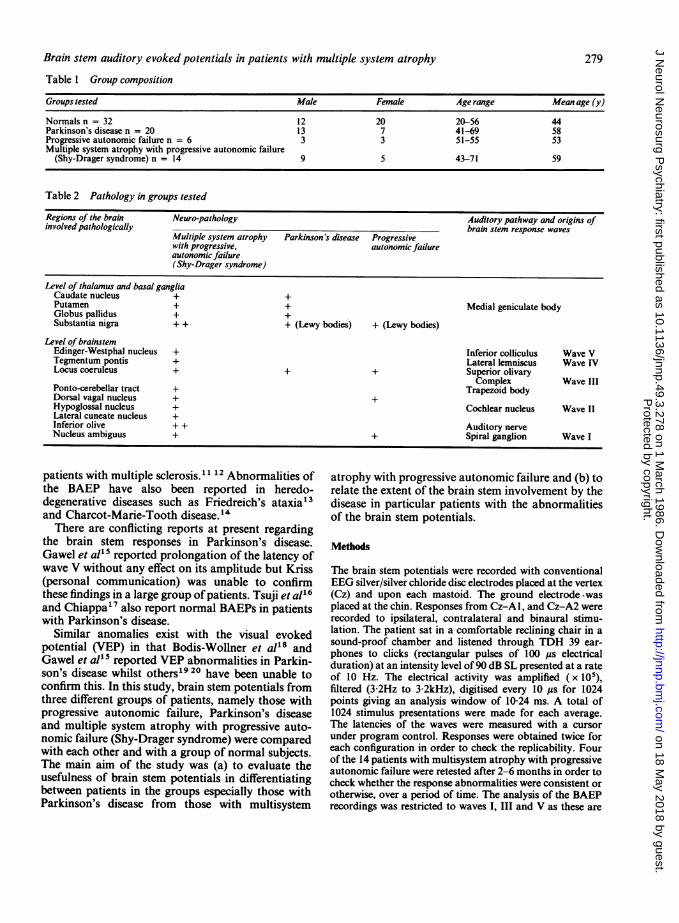
Overall the amplitudes of all components of theresponse from patients with multisystem atrophy withprogressive autonomic failure were much smallerthan those observed in normals. In fig 2 are shown thehistograms of the mean amplitude of wave V for thefour groups of subjects tested. It clearly indicates amajor reduction in the amplitude of wave V inpatients with multisystem atrophy with progressiveautonomic failure which is consistent across thepatients within this group (indicated by the reducedvariance). This reduction in the voltage level of theresponse and latency prolongation of waves IIIand/or V coupled with a distorted wave morphologycharacterised the majority of responses in multi-system atrophy with progressive autonomic failure.Four patients who were retested after a period of
2-6 months were found to show no significant changein their responses over that period.
Six cases (four patients with multisystem atrophywith progressive autonomic failure, one with pureprogressive autonomic failure, one with Parkinson'sdisease) are presented together with details of the neu-rological examination and standard investigation inorder to assess how these relate to the abnormal brainstem potentials.
Case 1: DG: multisystem atrophy with progressive autonomicfailureA 60-year-old retired civil servant was referred with a 3 yearhistory of difficulty in initiating micturition for which he hada trans-urethral prostatectomy, which did not relieve hissymptoms. He had been totally impotent for 3 years and hadnoticed difficulty with saliva dribbling from the corners ofhis mouth and poorly perfused hands and feet. Over thesame period he noticed difficulty with manipulative skillsusing his hands and clumsiness of gait which had been get-ting progressively worse. He had collapsed to the floorseveral times but had lost consciousness on only one occa-sion. His voice had been rather monotonous over the lasttwo years. There had also been episodes of hypoxia at night.The patient had an expressionless face. The facial and
pout reflexes were brisk. The left plantar response was flexorand the right equivocal. There was slight cogwheel rigidity atthe wrists, more marked on the left than the right. He alsohad rapidly alternating movements impaired bilaterally.
0.8-
07-
:''a6-
0GD 0.5-
't 04-'0
*5 0.3-
s 02-0
.0 0.1-: o-
RR LLNormals
RR LL RR LL RRLLPD PAF MSA with PAF
Fig 2 Mean and standard deviation ofabsolute amplitude ofWave Vfor the groups tested. (PD = Parkinson's disease;PAF = Progressive Autonomic Failure; MSA with PAF =multisystem atrophy with progressive autonomicfailure).Note the major reduction in the mean and variance of theamplitude of Wave V in MSA with PAF.
282 Prasher, Bannister
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from
Brain stem auditory evoked potentials in patients with multiple system atrophy
(Cz-AA) Left ea
I IIIV
(Cz- A2) Right ec
I II
V
II (CZ- AD) Binaural
V
17i 9 10Time (ims)
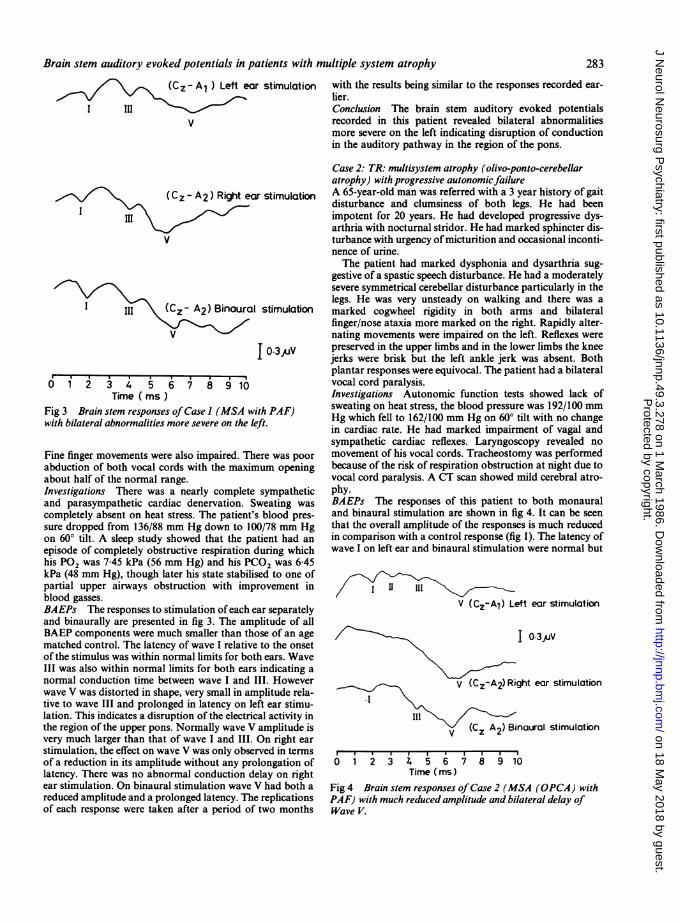
Fig 3 Brain stem responses ofCase I (MSA w
with bilateral abnormalities more severe on the I
Fine finger movements were also impaired. TI
abduction of both vocal cords with the maxiiabout half of the normal range.Investigations There was a nearly completeand parasympathetic cardiac denervation. 'completely absent on heat stress. The patient'sure dropped from 136/88 mm Hg down to 14
on 600 tilt. A sleep study showed that the p;episode of completely obstructive respirationhis P02 was 7-45 kPa (56 mm Hg) and his P4kPa (48 mm Hg), though later his state stabilipartial upper airways obstruction with imlblood gasses.BAEPs The responses to stimulation ofeachand binaurally are presented in fig 3. The amBAEP components were much smaller than thmatched control. The latency of wave I relativof the stimulus was within normal limits for boIII was also within normal limits for both earnormal conduction time between wave I andwave V was distorted in shape, very small in artive to wave III and prolonged in latency on 1lation. This indicates a disruption of the electriithe region of the upper pons. Normally wave Vvery much larger than that of wave I and III.stimulation, the effect on wave V was only obseof a reduction in its amplitude without any prilatency. There was no abnormal conduction dear stimulation. On binaural stimulation wavereduced amplitude and a prolonged latency. Thof each response were taken after a period of
ir stimulation with the results being similar to the responses recorded ear-lier.Conclusion The brain stem auditory evoked potentialsrecorded in this patient revealed bilateral abnormalitiesmore severe on the left indicating disruption of conductionin the auditory pathway in the region of the pons.
Case 2: TR: multisystem atrophy (olivo-ponto-cerebellaratrophy) with progressive autonomicfailure
ar stimulation A 65-year-old man was referred with a 3 year history of gaitdisturbance and clumsiness of both legs. He had beenimpotent for 20 years. He had developed progressive dys-arthria with nocturnal stridor. He had marked sphincter dis-turbance with urgency of micturition and occasional inconti-nence of urine.The patient had marked dysphonia and dysarthria sug-
gestive of a spastic speech disturbance. He had a moderatelysevere symmetrical cerebellar disturbance particularly in thelegs. He was very unsteady on walking and there was a
I stimulation marked cogwheel rigidity in both arms and bilateralfinger/nose ataxia more marked on the right. Rapidly alter-nating movements were impaired on the left. Reflexes were
T 0-3uV preserved in the upper limbs and in the lower limbs the kneejerks were brisk but the left ankle jerk was absent. Bothplantar responses were equivocal. The patient had a bilateralvocal cord paralysis.Investigations Autonomic function tests showed lack of
vith PAF) sweating on heat stress, the blood pressure was 192/100 mmleft. Hg which fell to 162/100 mm Hg on 600 tilt with no changein cardiac rate. He had marked impairment of vagal and
sympathetic cardiac reflexes. Laryngoscopy revealed nohere was poor movement of his vocal cords. Tracheostomy was performedmum opening because of the risk of respiration obstruction at night due to
vocal cord paralysis. A CT scan showed mild cerebral atro-sympathetic phy.
Sweating was BAEPs The responses of this patient to both monaural's blood pres- and binaural stimulation are shown in fig 4. It can be seen00/78 mm Hg that the overall amplitude of the responses is much reducedatient had an in comparison with a control response (fig 1). The latency ofduring which wave I on left ear and binaural stimulation were normal butC02 was 6 45ised to one ofprovement in I II1
ear separately V (CZ-Al) Left ear stimulation
plitude of alliose of an age __3I V,e to the onset,th ears. Waves indicating aIII. However V (Cz-A2)Right ear stimulationmplitude rela-eft ear stimu-ical activity in 1 /I amplitude is V (CZ A2) Binaural stimulationOn right ear-rvedinterms , , , ,olongation of 0 1 2 3 4 5 6 7 8 9 10lelay on right Time (ims)V had both a Fig 4 Brain stem responses ofCase 2 (MSA (OPCA) with.e replications PAF) with much reduced amplitude and bilateral delay off two months Wave V.
283
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from
284
(Cz-Al) Left ear stimulation
V
(Cz-A2) Right ear stimulationIII
V
(C,-A2) Binaural stimulation
To13,uVv 1.- {
O 1 2 3 4 5 6 7 8 9 10Time (ims)
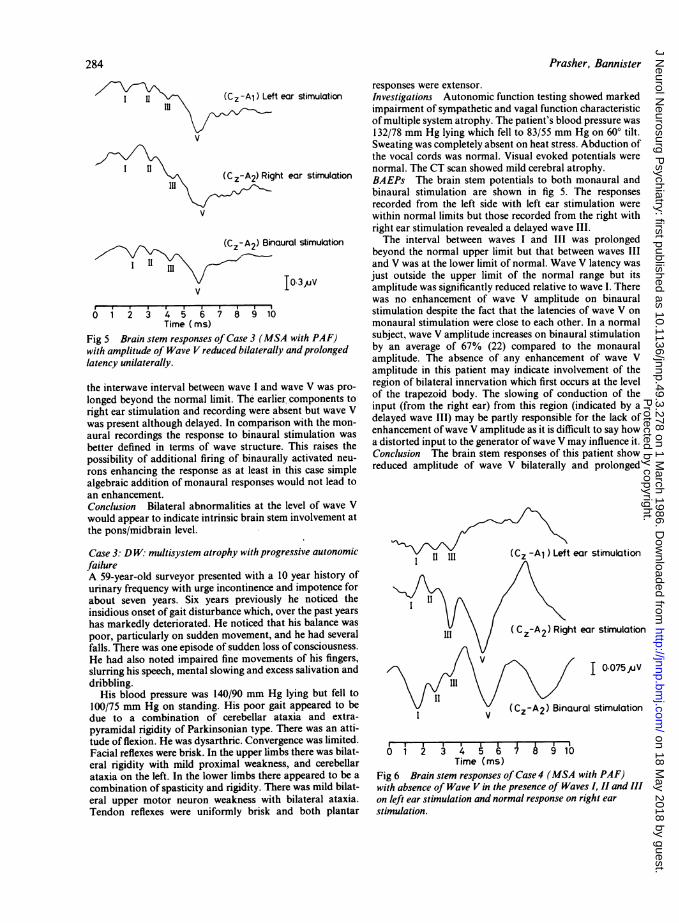
Fig 5 Brain stem responses of Case 3 (MSA with PAF)with amplitude of Wave V reduced bilaterally andprolongedlatency unilaterally.
the interwave interval between wave I and wave V was pro-longed beyond the normal limit. The earlier components toright ear stimulation and recording were absent but wave Vwas present although delayed. In comparison with the mon-aural recordings the response to binaural stimulation wasbetter defined in terms of wave structure. This raises thepossibility of additional firing of binaurally activated neu-rons enhancing the response as at least in this case simplealgebraic addition of monaural responses would not lead toan enhancement.Conclusion Bilateral abnormalities at the level of wave Vwould appear to indicate intrinsic brain stem involvement atthe pons/midbrain level.
Case 3: D W: multisystem atrophy with progressive autonomicfailureA 59-year-old surveyor presented with a 10 year history ofurinary frequency with urge incontinence and impotence forabout seven years. Six years previously he noticed theinsidious onset of gait disturbance which, over the past yearshas markedly deteriorated. He noticed that his balance waspoor, particularly on sudden movement, and he had severalfalls. There was one episode of sudden loss of consciousness.He had also noted impaired fine movements of his fingers,slurring his speech, mental slowing and excess salivation anddribbling.
His blood pressure was 140/90 mm Hg lying but fell to100/75 mm Hg on standing. His poor gait appeared to bedue to a combination of cerebellar ataxia and extra-pyramidal rigidity of Parkinsonian type. There was an atti-tude of flexion. He was dysarthric. Convergence was limited.Facial reflexes were brisk. In the upper limbs there was bilat-eral rigidity with mild proximal weakness, and cerebellarataxia on the left. In the lower limbs there appeared to be acombination of spasticity and rigidity. There was mild bilat-eral upper motor neuron weakness with bilateral ataxia.Tendon reflexes were uniformly brisk and both plantar
Prasher, Bannister
responses were extensor.Investigations Autonomic function testing showed markedimpairment of sympathetic and vagal function characteristicof multiple system atrophy. The patient's blood pressure was132/78 mm Hg lying which fell to 83/55 mm Hg on 600 tilt.Sweating was completely absent on heat stress. Abduction ofthe vocal cords was normal. Visual evoked potentials werenormal. The CT scan showed mild cerebral atrophy.BAEPs The brain stem potentials to both monaural andbinaural stimulation are shown in fig 5. The responsesrecorded from the left side with left ear stimulation werewithin normal limits but those recorded from the right withright ear stimulation revealed a delayed wave III.The interval between waves I and III was prolonged
beyond the normal upper limit but that between waves IIIand V was at the lower limit of normal. Wave V latency wasjust outside the upper limit of the normal range but itsamplitude was significantly reduced relative to wave I. Therewas no enhancement of wave V amplitude on binauralstimulation despite the fact that the latencies of wave V onmonaural stimulation were close to each other. In a normalsubject, wave V amplitude increases on binaural stimulationby an average of 67% (22) compared to the monauralamplitude. The absence of any enhancement of wave Vamplitude in this patient may indicate involvement of theregion of bilateral innervation which first occurs at the levelof the trapezoid body. The slowing of conduction of theinput (from the right ear) from this region (indicated by adelayed wave III) may be partly responsible for the lack ofenhancement ofwave V amplitude as it is difficult to say howa distorted input to the generator ofwave V may influence it.Conclusion The brain stem responses of this patient showreduced amplitude of wave V bilaterally and prolonged
II III (CZ -A1 ) LeftI /
6 i 2 3 4 5 6 7 8 9 lbTime (ms)
Fig 6 Brain stem responses of Case 4 (MSA with PAF)with absence of Wave V in the presence of Waves I, II and IIIon left ear stimulation and normal response on right earstimulation.
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from
Brain stem auditory evoked potentials in patients with multiple system atrophylatency unilaterally indicating bilateral involvement at thepons/midbrain level which is more severe on the right.
Case 4: JW: multisystem atrophy with progressive autonomicfailureA 64-year-old man presented with a four year history ofdifficulty with micturition and urge incontinence. A pros-tatectomy was performed but this aggravated his inconti-nence. Over the past three years his balance has steadilyworsened and in the last year he has been unable to walkmore than 20 or 30 yards without a rest. In the last 9 monthshis speech has become slurred and his writing less legible.The patient had an expressionless face and dysarthric
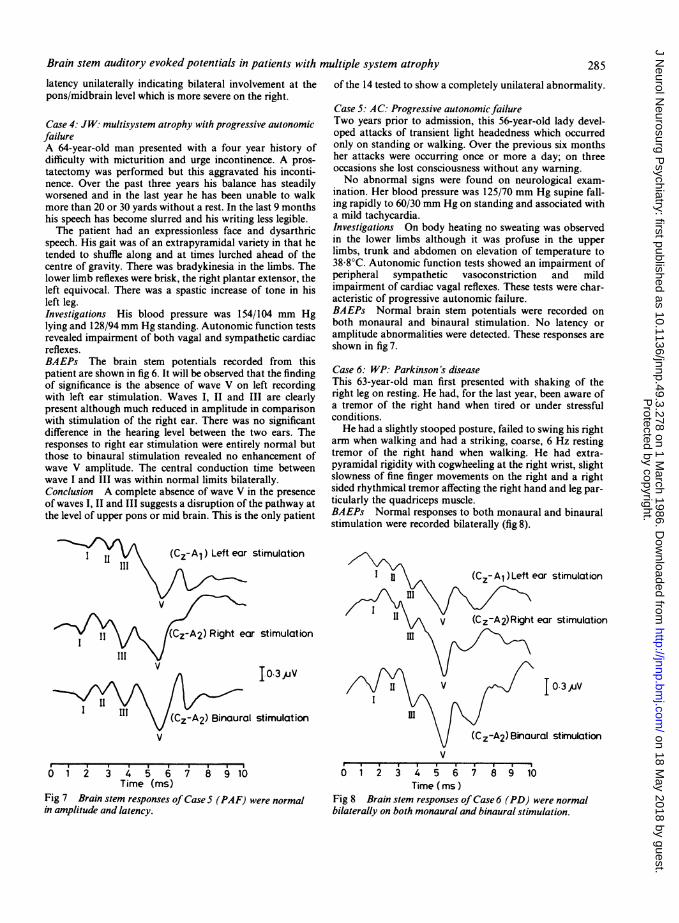
speech. His gait was of an extrapyramidal variety in that hetended to shuffle along and at times lurched ahead of thecentre of gravity. There was bradykinesia in the limbs. Thelower limb reflexes were brisk, the right plantar extensor, theleft equivocal. There was a spastic increase of tone in hisleft leg.Investigations His blood pressure was 154/104 mm Hglying and 128/94 mm Hg standing. Autonomic function testsrevealed impairment of both vagal and sympathetic cardiacreflexes.BAEPs The brain stem potentials recorded from thispatient are shown in fig 6. It will be observed that the findingof significance is the absence of wave V on left recordingwith left ear stimulation. Waves I, II and III are clearlypresent although much reduced in amplitude in comparisonwith stimulation of the right ear. There was no significantdifference in the hearing level between the two ears. Theresponses to right ear stimulation were entirely normal butthose to binaural stimulation revealed no enhancement ofwave V amplitude. The central conduction time betweenwave I and III was within normal limits bilaterally.Conclusion A complete absence of wave V in the presenceof waves I, II and III suggests a disruption of the pathway atthe level of upper pons or mid brain. This is the only patient
III I III
of the 14 tested to show a completely unilateral abnormality.
Case 5: AC: Progressive autonomicfailureTwo years prior to admission, this 56-year-old lady devel-oped attacks of transient light headedness which occurredonly on standing or walking. Over the previous six monthsher attacks were occurring once or more a day; on threeoccasions she lost consciousness without any warning.No abnormal signs were found on neurological exam-
ination. Her blood pressure was 125/70 mm Hg supine fall-ing rapidly to 60/30 mm Hg on standing and associated witha mild tachycardia.Investigations On body heating no sweating was observedin the lower limbs although it was profuse in the upperlimbs, trunk and abdomen on elevation of temperature to38 8°C. Autonomic function tests showed an impairment ofperipheral sympathetic vasoconstriction and mildimpairment of cardiac vagal reflexes. These tests were char-acteristic of progressive autonomic failure.BAEPs Normal brain stem potentials were recorded onboth monaural and binaural stimulation. No latency oramplitude abnormalities were detected. These responses areshown in fig 7.
Case 6: WP: Parkinson's diseaseThis 63-year-old man first presented with shaking of theright leg on resting. He had, for the last year, been aware ofa tremor of the right hand when tired or under stressfulconditions.He had a slightly stooped posture, failed to swing his right
arm when walking and had a striking, coarse, 6 Hz restingtremor of the right hand when walking. He had extra-pyramidal rigidity with cogwheeling at the right wrist, slightslowness of fine finger movements on the right and a rightsided rhythmical tremor affecting the right hand and leg par-ticularly the quadriceps muscle.BAEPs Normal responses to both monaural and binauralstimulation were recorded bilaterally (fig 8).
(Cz-A,) Left ear stimulation
r stimulation
I,03,V
stimulation
6 1 2 3 4 5 6 68 lbTime (ms)
Fig 7 Brain stem responses ofCase 5 (PAF) were normalin amplitude and latency.
V
0 1 2 3 4 5 6 7 8 9 10Time (ims)
Fig 8 Brain stem responses of Case 6 (PD) were normalbilaterally on both monaural and binaural stimulation.
285
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from

286
Discussion
This study has demonstrated that the brain stempotentials are virtually always abnormal in patientswith multisystem atrophy with progressive autonomicfailure (Shy-Drager syndrome) in contrast to the nor-mal findings in a majority of patients with Parkin-son's disease and the closely associated group ofpatients with only progressive autonomic failure.
In about one third of patients eventually proving tohave multisystem atrophy with progressive auto-nomic failure the wrong diagnosis is made initially(Parkinson's disease, or Parkinson's disease withprogressive autonomic failure, or progressive auto-nomic failure) and after some years the developmentof more obvious clinical features enables a correctdiagnosis to be made. Multisystem atrophy of theShy-Drager type is rare but it has extrapyramidal fea-tures closely resembling either idiopathic Parkin-sonism or a late onset cerebellar degeneration.22 23Making the correct diagnosis is important becausespecific treatment is sometimes possible and the prog-nosis of each syndrome is very different. Multisystematrophy patients have five years' mean survival timefrom diagnosis whereas Parkinson's patients have anearly normal life span. The use of BAEPs shouldmake it possible to make the correct diagnosis at anearlier stage.
Table 2 shows the widespread pathological changesdescribed in multisystem atrophy with progressiveautonomic failure, in Parkinson's disease and thoseobserved in progressive autonomic failure alone. Thedescription of a number of cases of progressive auto-nomic failure with close clinical relationship to Par-kinson's disease2425 and others with a more wide-spread neurological disorder has led to theconsideration of two separate syndromes.26 27Pathological changes confirm this distinction; inprogressive autonomic failure alone or with Parkin-son's disease, Lewy bodies are detected and degener-ative changes in the substantia nigra and locuscoeruleus have been found. In Parkinson's disease thepathological changes also occur in the caudatenucleus and putamen. In multisystem atrophy withprogressive autonomic failure, abnormalities aremuch more widespread including the inferior olivarynucleus, cerebellum, pons, substantia nigra, locuscoeruleus, putamen and globus pallidus. In multi-system atrophy with progressive autonomic failurethe striato-nigral degeneration occurs without thepresence of Lewy bodies.27 It is of interest that in oneprevious report of three patients with olivo-ponto-cerebellar atrophy28 in whom no specific tests ofautonomic function were reported, similar brain stemresponse abnormalities were detected. In this study nodistinction has been made between multisystem atro-
Prasher, Bannister
phy with or without olivo-ponto-cerebellar atrophy.In the majority of the patients with multisystem
atrophy with progressive autonomic failure the earliercomponents (wave I and II) of the brain stemresponse remained relatively unaffected in com-parison with waves III and V which were bothaffected indicating abnormalities at the level of thepons and midbrain. The overall amplitude of theresponses from these patients was reduced by about50% with the amplitude of wave V relative to wave Ibeing affected in 13 of the 14 patients and absence ofenhancement of wave V on binaural stimulation innine of the 14 patients. It is possible that cell loss andconsequent transneuronal degeneration and asyn-chronous firing of impulses may account for the dis-torted wave morphology, overall reduction in ampli-tude and prolongation of interwave intervals.With regard to the findings in patients with Parkin-
son's disease, our results are different from those ofGawel et all5 who reported a significant delay in themean latency of wave V for the Parkinson's patientsin comparison with a group of normals. However,Gawel et al"5 did not specify the age range of theircontrol group giving rise to the possibility of theresult being due to a comparison between two groupsof different ages. This is also considered as a possibleexplanation by Halliday29 for the delay reported byGowel et al.' 5 Tsuji et al"6 and Chiappa"7 also foundno abnormalities of BAEPs in patients with Parkin-son's disease.The present study has shown that in patients with
progressive autonomic failure alone the brain stemresponses are normal despite the commoninvolvement in multisystem atrophy with progressiveautonomic failure of brain stem nuclei coordinatingautonomic reflexes such as locus coeruleus, dorsalvagal nucleus and tractus solitarius most of which aremonoaminergic. The dorsal vagal nucleus and thenucleus ambiguous degenerate both in progressiveautonomic failure and multisystem atrophy withprogressive autonomic failure in the medulla close tothe site of the generator of wave II which is thecochlear nucleus. Therefore, with a sufficiently largelesion the possibility exists of a coincidental inter-ruption of the auditory pathway in the medulla. How-ever, in the absence of any abnormality of the brainstem response it is postulated that the involvement inprogressive autonomic failure of the dorsal vagalnucleus and nucleus ambiguous is restricted to thesenuclei.
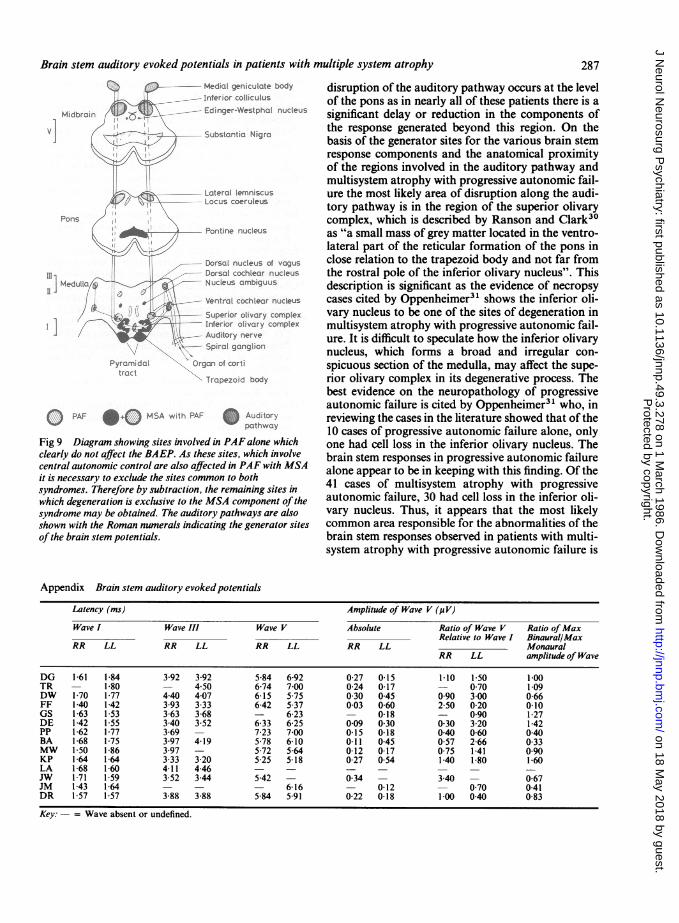
Figure 9 illustrates the auditory pathway and thenuclei and tracts in the brain stem involved in multi-ple system atrophy with progressive autonomic fail-ure. From the abnormalities of the brain stemresponse in patients with multisystem atrophy withprogressive autonomic failure, it is clear that some
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from
Brain stem auditory evoked potentials in patients with multiple system atrophyMedial gen culate body
Inferior colliculus
Midbro n ..k--D-- Edinger-Westpho. nucleus
Substartia Nigro
Lateral lemniscus-C --- Locus coeruleus
Pollss
Pont:ne nucleus
Dorsal nucleus ot vagus
Dorsal cochleor nucleuse / -
-- Nucleus ambiguus
/fi , ..----- Yentrol cochlecir nucleus
-- Super;or olivory complex
Interior olivary complexiAudtory nerve--Spiral gclng lion
Pyramidaltract
Orgar ot corti
Trapezoid body
PAF +0 MSA uth
PAF Au4tori,Fig 9 Diagram showing sites involved in PAF alone whichclearly do not affect the BAEP. As these sites, which involvecentral autonomic control are also affected in PAF with MSAit is necessary to exclude the sites common to bothsyndromes. Therefore by subtraction, the remaining sites inwhich degeneration is exclusive to the MSA component of thesyndrome may be obtained. The auditory pathways are alsoshown with the Roman numerals indicating the generator sitesof the brain stem potentials.
disruption of the auditory pathway occurs at the levelof the pons as in nearly all of these patients there is asignificant delay or reduction in the components ofthe response generated beyond this region. On thebasis of the generator sites for the various brain stemresponse components and the anatomical proximityof the regions involved in the auditory pathway andmultisystem atrophy with progressive autonomic fail-ure the most likely area of disruption along the audi-tory pathway is in the region of the superior olivarycomplex, which is described by Ranson and Clark30as "a small mass of grey matter located in the ventro-lateral part of the reticular formation of the pons inclose relation to the trapezoid body and not far fromthe rostral pole of the inferior olivary nucleus". Thisdescription is significant as the evidence of necropsycases cited by Oppenheimer3' shows the inferior oli-vary nucleus to be one of the sites of degeneration inmultisystem atrophy with progressive autonomic fail-ure. It is difficult to speculate how the inferior olivarynucleus, which forms a broad and irregular con-spicuous section of the medulla, may affect the supe-rior olivary complex in its degenerative process. Thebest evidence on the neuropathology of progressiveautonomic failure is cited by Oppenheimer3" who, inreviewing the cases in the literature showed that of the10 cases of progressive autonomic failure alone, onlyone had cell loss in the inferior olivary nucleus. Thebrain stem responses in progressive autonomic failurealone appear to be in keeping with this finding. Of the41 cases of multisystem atrophy with progressiveautonomic failure, 30 had cell loss in the inferior oli-vary nucleus. Thus, it appears that the most likelycommon area responsible for the abnormalities of thebrain stem responses observed in patients with multi-system atrophy with progressive autonomic failure is
Appendix Brain stem auditory evokedpotentials
Latency (ms) Amplitude of Wave V (p V)Wave I Wave III Wave V Absolute Ratio of Wave V Ratio ofMax
Relative to Wave I Binaural/MaxRR LL RR LL RR LL RR LL Monaural
RR LL amplitude of Wave
DG 1-61 1-84 3-92 3-92 5-84 6-92 0-27 0-15 1 10 1 50 1 00TR - 1-80 - 4 50 6-74 7 00 0-24 0-17 - 0 70 1 09DW 1 70 1 77 440 407 6-15 5 75 0 30 045 090 300 0-66FF 1-40 1 42 3-93 3 33 642 5-37 003 0-60 2 50 0 20 0 10GS 1-63 1-53 3-63 3 68 - 6 23 - 0-18 - 0 90 1-27DE 1 42 1-55 340 3-52 6-33 625 009 030 030 3-20 1-42PP 162 1-77 369 - 7-23 700 015 0-18 040 060 040BA 1-68 1-75 3-97 4-19 5-78 6-10 0 11 0-45 0-57 2 66 0 33MW 1 50 1-86 3-97 - 5-72 5-64 0-12 0-17 0-75 1-41 090KP 1-64 1-64 3-33 3 20 5-25 5-18 0-27 0-54 1-40 1-80 1-60LA 1-68 1-60 4-11 4 46 - - - - - - -JW 1 71 1-59 3 52 3-44 5-42 - 0-34 - 3 40 - 0-67JM 143 164 - - - 616 - 0-12 - 0 70 0 41DR 157 157 3-88 388 584 591 022 018 100 040 083
Key: -= Wave absent or undefined.
287
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from
288the ponto-medullary region involving both the supe-rior and the inferior olivary nuclei.
In conclusion, this study provides, by the recordingof brain stem auditory evoked potentials, a non-invasive means for differential diagnosis betweenprogressive autonomic failure alone or with Parkin-son's disease, and progressive autonomic failure withmultisystem atrophy (Shy-Drager syndrome).Although these conditions are different pathologicalentities with distinct histological appearances, theirclinical separation in the early stages is often difficult,if not impossible because of overlapping clinical fea-tures. Any additional information in this respect isvery valuable in the differential diagnosis. Patientsand their relatives need to know as accurate a diagno-sis as possible because it affects both treatment andprognosis. The prognosis of multisystem atrophywith progressive autonomic failure is so much worsethan progressive autonomic failure alone or with Par-kinson's disease. Brain stem auditory evoked poten-tials, by providing that additional information, mayhelp clarify the diagnosis in patients with eitherapparent Parkinson's disease and unusual featureswho may or may not have multisystem atrophy aswell as patients presenting with apparent pureprogressive autonomic failure alone. As far as theauthors are aware, there are no other closely relatedneurological conditions in which the BAEP dis-sociates so clearly between important differentialdiagnoses.
References
Jewett DL, Williston JS. Auditory evoked far fields aver-aged from the scalp of humans. Brain 1971;94:681-96.
2Buchwald FS, Huang CH. Far field acoustic response: ori-gins in the cat. Science 1975;189:382-4.
3Huang CM, Buchwald JS. Interpretation of the vertexshort latency acoustic response: A study of single neu-rons in the brain stem. Brain Res 1977;137:291-303.
4Stockard JJ, Rossiter VS. Clinical and pathological cor-relates of brain stem auditory response abnormalities.Neurology (Minneap) 1977;27:316-25.
sSohmer H, Feinmesser M, Szabo G. Sources of electro-cochleographic responses as studied in patients withbrain damage. Electroencephalogr Clin Neurophysiol1974;37:663-9.
6 Starr A, Achor LJ. Auditory brainstem responses in neu-rological disease. Arch Neurol 1975;32:761-8.
Starr A, Hamilton AE. Correlation between confirmedsites of neurological lesions and abnormalities of far-field auditory brainstem responses. ElectroencephalogrClin Neurophysiol 1976;41:595-618.
8Britt RH, Rossi GT. Neural generators of brain stem audi-tory evoked responses. Part I. Lesion studies. Neu-roscience Abstracts 1980;6:594.
9Achor LJ, Starr A. Auditory brainstem responses in the
Prasher, Bannister
cat II. Effects of lesions. Electroencephalogr Clin Neu-rophysiol 1980;48: 174-90.
0Kevanishvili Z. Sources of the human brainstem auditoryevoked potential. Scand Audiol 1980;9:75-82.
l Prasher DK, Gibson WPR. Brainstem auditory evokedpotentials. A comparative study of monaural vs. binau-ral stimulation in the detection of multiple sclerosis.Electroencephalogr Clin Neurophysiol 1980;50:247-53.
12Robinson K, Rudge P. Abnormalities of the auditory sys-tem in patients with multiple sclerosis. Brain 1977;100:19-40.
3Ell JJ, Prasher DK, Rudge P. Neuro-otological abnor-malities in Friedreich's Ataxia. J Neurol NeurosurgPsychiatry 1984;47:26-32.
14Satya-Murti S, Cacace A, Hanson P. Auditory dys-function in Friedreich's ataxia: result of spiral gangliondegeneration. Neurology (Minneap) 1980;30: 1047-53.
s Gawel MJ, Das P, Vincent S, Clifford Rose F. Visual andauditory evoked responses in patients with Parkinson'sdisease. J Neurol Neurosurg Psychiatry 198 1;44:227-32.
16Tsuji S, Muraoka S, Kuroiwa Y, Chen KM, GadusckCD. Auditory brain stem evoked response (ABSR) ofParkinson-dementia complex, and amyotrophic lateralsclerosis in Guam and Japan. Rinsho Shinkeigaku198 1;21:37-41.
7Chiappa K. Evoked Potentials in Clinical Medicine. NewYork: Raven Press, 1983.
18Bodis-Wollner I, Yahr MD. Measurements of visualevoked potentials in Parkinson's disease. Brain1978;101:661-71.
9Yaar I. The effect of Levodopa treatment on the visualevoked potentials in Parkinsonian patients. Electro-encephalogr Clin Neurophysiol 1980;50:267-4.
20 Ehle AL, Stewart M, Lellelid NE, Leventhal NA. Normalcheckerboard pattern reversal evoked potentials in Par-kinsonism. Electroencephalogr Clin Neurophysiol1982;54:336.
21Prasher DK, Sainz M, Gibson WPR. Binaural voltagesummation of brainstem auditory evoked potentials: Anadjunct to the diagnostic criteria for multiple sclerosis.Ann Neurol 1981;11:86-91.
22 Shy GM, Drager GA. A neurological syndrome associ-ated with orthostatic hypotension. Arch Neurol1960;2:511-27.
23 Bannister R, Oppenheimer DR. Degenerative diseases ofthe nervous system associated with autonomic failure.Brain 1972;95:457-4.
24Bannister R, Ardill L, Fentem P. Defective autonomiccontrol of blood vessels in idiopathic orthostatic hypo-tension. Brain 1967;90:725-46.
2'Thomas JE, Schirger A. Idiopathic orthostatic hypo-tension: A study of its natural history in 57 neuro-logically affected patients. Arch Neurol 1970;22:289-93.
26 Graham JG, Oppenheimer DR. Orthostatic hypotensionand nicotine sensitivity in a case of multiple system atro-phy. J Neurol Neurosurg Psyschiatry 1969;32:28-34.
27Spokes EGS, Bannister R, Oppenheimer DR. Multiplesystem atrophy with autonomic failure. Clinical, Histo-logical and Neurochemical observations of four cases. JNeurol Sci 1979;43:59-82.
28Gilroy J, Lynn GE. Computerised tomography andauditory evoked potentials. Use in the diagnosis of
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from

Brain stem auditory evoked potentials in patients with multiple system atrophy
olivo-ponto-cerebellar degeneration. Arch Neurol1978;35: 143-7.
29Halliday AM. Evoked Potentials in Clinical Testing.Churchill Livingstone, Edinburgh, 1982.
30 Ranson SW, Clark SL. Anatomy of the Nervous System.
289
WB Saunders and Co., 1953:185-208.31 Oppenheimer DR. Neuropathology of progressive auto-
nomic failure. In: Sir Roger Bannister, ed. AutonomicFailure. Oxford University Press, 1983:267-83.
Protected by copyright.
on 18 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.49.3.278 on 1 March 1986. D
ownloaded from