Embed Size (px)
DESCRIPTION
abses otak
Citation preview

Brain abscess
Kiking Ritarwan

Definition
• Brain abscess is a focal intracerebral infection that begin as a localized area of cerebritis and develops into a collection of pus surrounded by a weil-vascularized capsule.
• Abscess of the brain has been known for over 200 years, and surgical treatment started with MacEwen in 1893 [published:” pyogenic infective disease of the Brain”].

• Parenchymal brain infection can arise from hematogenous delivery of infected material, which often results in multiple abscess. Especially at risk are patients with congenital heart disease or valve infection.
• Pathogenesis: abscess begin with local cerebritis, causing necrosis and surronding edema.
• Epidemiology: 0,3 – 1,3 per 100.000 / tahun• Male to female ratio of 2:1 to 3:1

Common etiologic factorsCommon etiologic factors Distingushing
characteristics
Middle ear,paranasal sinus, or mastoid infection
Ear inf: temporal lobe abscess, sinus inf: frontal lobe abscess, mastoid inf: cerebellar abscess
Metastatic embolic from lung, pulmonary abscess, bronchietasis, or chronic empyema
Multiple abscess
Head trauma or Neurosurg. Gunshot wounds are the most common head trauma assc. With abscess
Endocarditis Drug abuser
Rare cause: dental procedures, Metastatic emboli from abdominal inf. Or PID, osteomyelitis of skull
-

Common etiologic factors Microorgnism involved
Aerobes Anaerob
Middle ear,paranasal sinus, or mastoid infection
Streptococci, Streptococci
Staph aureus Bacteriodes
Metastatic embolic from lung, pulmonary abscess, bronchietasis, or chronic empyema
Staph aureus, Klebsiela Streptococci,
S.Pneumoniae Fusobacteria
Head trauma or Neurosurg.
Staph aureus, streptococci
Pseudomonas
Endocarditis Staph aureus -
Rare cause: dental procedures, Metastatic emboli from abdominal inf. Or PID, osteomyelitis of skull
-

Neuropatologi (4 stages)
1. Early cerebritis ( days 1-3) infection of the brain with surronding white matter edema.2. Late cerebritis ( days 4-9) The core of the cerebritis becomes necrotic and enlarges
and capsular fibroblasts begin to form.3. Early capsule formation ( days10-13) The capsule is well developed, with proliferation of
fibroblasts, a surronding astrocytic proliferation, and edema4. Late capsule formation (days 14 or more). A mature, thick capsule surronds the central cavity
containing debris and PMN cells. There is usually marked cerebral edema in the surronding brain tissue in the presence of a mature abscess.

Gejala dan tanda klinis:
• Sakit kepala (70-90%)• Muntah (25-50%)• Kejang(30-50%)• Gejala pusing, vertigo, ataksia ( pd abses
cerebelli)• Ggn bicara (19,6%), hemianopsia (31%),
unilateral midriasis (20,5%)• Gejala fokal (61%) pd penderita abses
supratentorial.

Pemeriksaan utk Diagnosa:
• Glasgow coma scale : utk kesadaran penderita
• Rontgen foto kepala, sinus, mastoid, thoraks.
• EEG• CT Scan/ MRI• Angiografi : utk menentulan lokasi abses
(24%).• Lab: jlh leukosit 10.000-20.000/ cm3 (60-
70%) LED meningkat 45 mm/jam (75-90%).

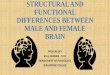
Head Ct San
A. Multiple brain abscesses associated with bacterial endocarditis (Staphylococcus aureus) in a55-year-old man. The large abscess in the left hemisphere shows a characteristic ring enhancement.
B. ContrastenhancedCT scan 4 months after institution of antibiotic treatment. The abscesses have resolved.
A B

Komplikasi Abses Otak
• Robeknya kapsul abses kedalam ventrikel atau keruangan subarakhnoid.
• Penyumbatan cairan serebrospinal hidrosefalus
• Edema otak• Herniasi tentorial oleh massa abses
otak.

11
Pengobatan abses otak
• Konservatif: - Pemberian AB yg tepat : 6-8 mgg mengecilkan abses. - Prinsip pemberian AB: bakterisid thdp organisme
hasil kultur, dapat melewati BBB. - Pemberian kortikosteroid: dewasa : loading dose 10-12 mg secara IV maintenance dose 4 mg secara IV setiap 6
jam anak : loading dose 10-12 mg/kg diberikan
satu kali IV maintenance dose 1-1,5 mg/kg/hari IV - Pemberian antikonvulsan• Operatif: Aspirasi dan eksisi. konsul Bedah Saraf , jika
terapi konservatif gagal.

Antibiotic treatment for brain abscess
Ear, mastoid, sinus
Streptococcal species, Ps anaerobes, Enterobaceteriacea
Metronidazole 7.5 mg IV every 6 h + Cefepime 2 gr IV every 6 h or meropenem 2gr IV every 8 h
Lung S. pneumoniae Same as above

AB treatment
Teeth, mouth Anaerobic streptococci, Eikenella, Prevotella, Actinomyces
Metro 7,5 mg/kg IV every 12 h + PNC G 4million units IV every 4 h or ceftizoxime 3 gr IV every 6 h
Post operative infection, furuncles or decubiti
Staphiloc Cefepime 2 gr IV every 8 h, or Nafcillin or oxacillin 2 g IV every 4 h