Embed Size (px)
Citation preview

I
Tbagvassthmaad
C
ddrpmdtfnd
I
fttwareo
C
mpe
A
MAGING TEACHING CASE
Brachial Artery Pseudoaneurysms Caused by Inadvertent HemodialysisAccess Needle Punctures
Annie Wang, MD,1 and James E. Silberzweig, MD2
INDEX WORDS: Pseudoaneurysm; brachial artery; iatrogenic pseudoaneurysm; arteriovenous fistula;interventional procedures.
tawe
aarwrmwtCbAsbthps
trpms
2
C
A1
LoE
he preferred access for hemodialysis is anative autogenous arteriovenous fistula
ecause fistulas have lower complication ratesnd better longevity compared with prostheticrafts.1 However, fistulas are inclined to de-elop such complications as aneurysm, pseudo-neurysm, venous stenosis, venous hyperten-ion, thrombosis, hemorrhage, arm edema, stealyndrome, and infection.2 Pseudoaneurysm inhe brachial artery is a rare complication ofemodialysis therapy. We report the case of aan who presented with several small brachial
rtery pseudoaneurysms because of repeated in-dvertent needle punctures of the brachial arteryuring access of the arteriovenous fistula.
CASE REPORT
linical History
A 55-year-old man with hypertension, insulin-depen-ent diabetes, and chronic kidney disease requiring hemo-ialysis was referred for a fistulogram to evaluate hisight-arm hemodialysis fistula. The fistula had been inlace for 12 months and used for hemodialysis for 6onths. Needle insertion for dialysis was noted to be
ifficult, and the access was “deep.” Physical examina-ion showed a markedly dilated vein at the antecubitalossa. A strong thrill in the mid arm at the sites of previouseedle punctures was present. However, the thrill waseep and the brachial vein was very difficult to palpate.
magingStudies
The site of maximal thrill in the mid arm was accessedor an angiographic study. Contrast injection showed thathe right brachial artery was inadvertently accessed. Mul-iple small pseudoaneurysms of the inflow brachial arteryere present. There was aneurysmal dilatation of the
rteriovenous anastomosis of the right brachial artery andight median cubital vein. Fistula outflow was through annlarged right brachial vein with no contrast opacificationf the basilic or cephalic veins (Fig 1).
linical Follow-up
Because of the presence of the arteriovenous anasto-otic pseudoaneurysm, the fistula was ligated and a new
rosthetic graft was placed in the contralateral upper
xtremity. We saw the patient 10 months later for graftmerican Journal of Kidney Diseases, Vol 53, No 2 (February), 20
hrombectomy. The extremity with the right brachialrtery pseudoaneurysms was asymptomatic at that time,ith normal pulses and no clinical evidence of distal
mbolization.
DISCUSSION
A focal vessel dilatation arising from anrteriovenous access could be either a trueneurysm or a pseudoaneurysm. A true aneu-ysm is a vascular dilatation containing all itsall layers intact. Conversely, a pseudoaneu-
ysm is a dilatation with disruption of 1 orore layers of its wall. A pseudoaneurysmall typically contains neointima and fibrous
issue and sometimes is lined with thrombus.linically, it may be difficult to differentiateetween an aneurysm and a pseudoaneurysm.neurysms that are fusiform in shape, develop
lowly over several years, and are locatedeneath intact nonulcerated skin usually arerue aneurysms and probably are secondary toigh flow, turbulent flow, and/or increasedressure caused by the presence of a distaltenosis.3
Venous pseudoaneurysms typically occur athe site of clustered needle punctures, withesultant degeneration of the vein wall. Venousseudoaneurysms are typically saccular andore prone to infection and rupture. Doppler
onography frequently is used as an initial
From 1New York Hospital Queens, Flushing; andDepartment of Radiology, St Luke’s-Roosevelt Hospitalenter, New York, NY.Received November 15, 2007. Accepted in revised form
ugust 6, 2008. Originally published online as doi:0.1053/j.ajkd.2008.08.008 on October 28, 2008.
Address correspondence to James E. Silberzweig, MD, Stuke’s-Roosevelt Hospital Center, Department of Radiol-gy, 4th Floor, 1000 Tenth Ave, New York, NY 10019.-mail: [email protected]© 2009 by the National Kidney Foundation, Inc.0272-6386/09/5302-0020$36.00/0
doi:10.1053/j.ajkd.2008.08.00809: pp 351-354 351

ipaptr2fri
rsUatatb
rvtlnaci
ls
reicsOoazes
wcteto
utpe
Wang and Silberzweig352
maging examination for evaluation of a pal-able mass in proximity to an arteriovenousccess. Sonography is useful in displaying theseudoaneurysm, including its relationship tohe normal vein, diameter of the pseudoaneu-ysm neck, and extent of mural thrombus (Fig). Conventional access angiography is per-ormed to define the site of the pseudoaneu-ysm and identify other abnormalities, includ-ng stenoses or additional pseudoaneurysms.
Arterial and venous traumatic pseudoaneu-ysms may arise after balloon angioplasty of atenosis4,5 or thrombectomy balloon inflation.6
se of a balloon catheter to eliminate the plugt the arterial anastomosis is a feature commono access thrombectomy procedures. A pseudo-neurysm may be caused by inadvertent disrup-ion of the vessel wall from overdilation by thealloon (Fig 3).A major cause of brachial artery pseudoaneu-
ysm is inadvertent arterial puncture duringenous cannulation for hemodialysis. Factorshat contribute to this complication are use ofarge-caliber needles, poor puncture tech-ique, and premature puncturing of the fistulafter surgery.7 Other reported causes of bra-hial artery pseudoaneurysms include penetrat-
Figure 1. Digital subtraction angiogram of the rightpper-extremity fistula shows (A) aneurysmal dilatation at
he arteriovenous anastomosis and (B) multiple smallseudoaneurysms (arrows) of the brachial artery and annlarged right brachial vein.
ng and blunt trauma, catheterization for vascu-rc
ar intervention, drug abuse, and arterial gasampling.7-11
Patients with brachial artery pseudoaneu-ysms may present weeks to months after pen-trating or blunt trauma.7,8 Common findingsnclude a pulsatile mass, systolic bruit by aus-ultation, and neuropathy and venous thrombo-is from pressure on adjacent nerves and veins.ther associated findings may include rupturef the pseudoaneurysm, infection, bleeding,nd distal arterial insufficiency. Distal emboli-ation of a mural thrombus within a pseudoan-urysm may result in hand ischemia. Diagno-is of a pseudoaneurysm may be confirmed by
Figure 2. A 33-year-old woman with low access flowith a pulsatile mass in the distal forearm. (A) Transverseolor Doppler sonogram image. The different colors withinhe pseudoaneurysm lumen indicate turbulent flow (differ-nt rates and directions of blood flow). (B) Digital subtrac-ion angiogram shows a saccular pseudoaneurysm (arrow)f the left cephalic vein immediately central to the left
adiocephalic anastomosis. Abbreviations: A, radial artery; V,ephalic vein.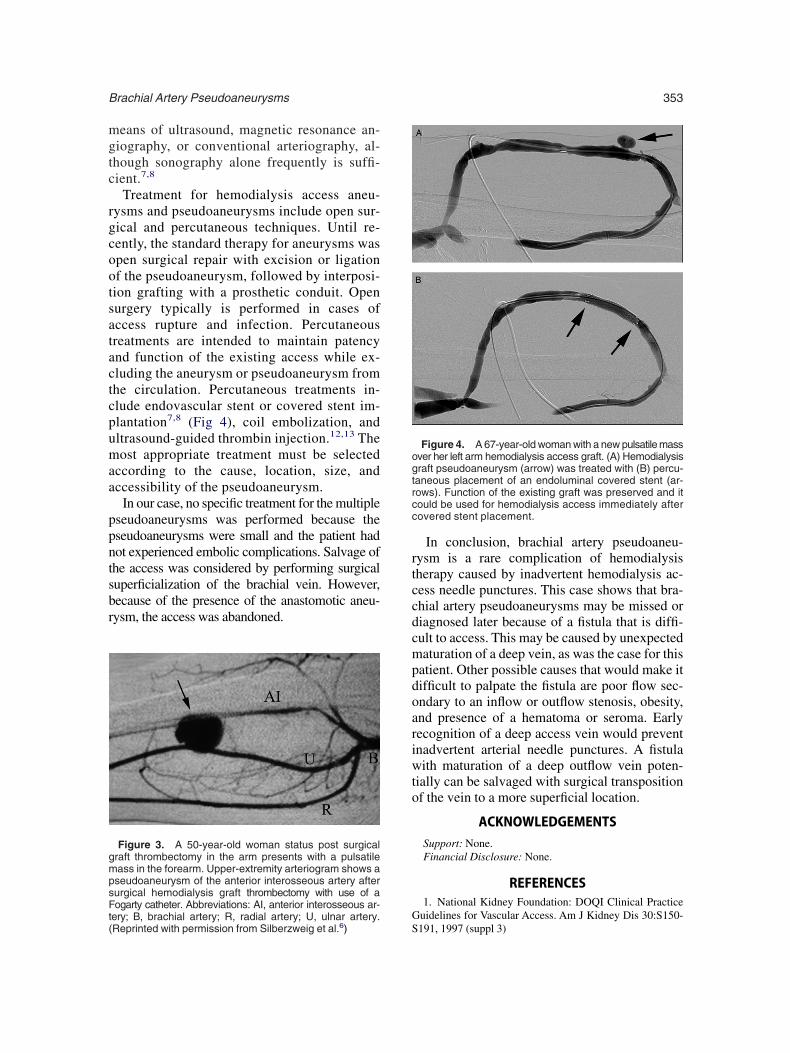
mgtc
rgcootsatactcpumaa
ppntsbr
rtccdcmpdoariwto
G
gmpsFt(
ogtrcc
Brachial Artery Pseudoaneurysms 353
eans of ultrasound, magnetic resonance an-iography, or conventional arteriography, al-hough sonography alone frequently is suffi-ient.7,8
Treatment for hemodialysis access aneu-ysms and pseudoaneurysms include open sur-ical and percutaneous techniques. Until re-ently, the standard therapy for aneurysms waspen surgical repair with excision or ligationf the pseudoaneurysm, followed by interposi-ion grafting with a prosthetic conduit. Openurgery typically is performed in cases ofccess rupture and infection. Percutaneousreatments are intended to maintain patencynd function of the existing access while ex-luding the aneurysm or pseudoaneurysm fromhe circulation. Percutaneous treatments in-lude endovascular stent or covered stent im-lantation7,8 (Fig 4), coil embolization, andltrasound-guided thrombin injection.12,13 Theost appropriate treatment must be selected
ccording to the cause, location, size, andccessibility of the pseudoaneurysm.
In our case, no specific treatment for the multipleseudoaneurysms was performed because theseudoaneurysms were small and the patient hadot experienced embolic complications. Salvage ofhe access was considered by performing surgicaluperficialization of the brachial vein. However,ecause of the presence of the anastomotic aneu-ysm, the access was abandoned.
Figure 3. A 50-year-old woman status post surgicalraft thrombectomy in the arm presents with a pulsatileass in the forearm. Upper-extremity arteriogram shows aseudoaneurysm of the anterior interosseous artery afterurgical hemodialysis graft thrombectomy with use of aogarty catheter. Abbreviations: AI, anterior interosseous ar-
Sery; B, brachial artery; R, radial artery; U, ulnar artery.Reprinted with permission from Silberzweig et al.6)
In conclusion, brachial artery pseudoaneu-ysm is a rare complication of hemodialysisherapy caused by inadvertent hemodialysis ac-ess needle punctures. This case shows that bra-hial artery pseudoaneurysms may be missed oriagnosed later because of a fistula that is diffi-ult to access. This may be caused by unexpectedaturation of a deep vein, as was the case for this
atient. Other possible causes that would make itifficult to palpate the fistula are poor flow sec-ndary to an inflow or outflow stenosis, obesity,nd presence of a hematoma or seroma. Earlyecognition of a deep access vein would preventnadvertent arterial needle punctures. A fistulaith maturation of a deep outflow vein poten-
ially can be salvaged with surgical transpositionf the vein to a more superficial location.
ACKNOWLEDGEMENTSSupport: None.Financial Disclosure: None.
REFERENCES1. National Kidney Foundation: DOQI Clinical Practice
uidelines for Vascular Access. Am J Kidney Dis 30:S150-
Figure 4. A 67-year-old woman with a new pulsatile massver her left arm hemodialysis access graft. (A) Hemodialysisraft pseudoaneurysm (arrow) was treated with (B) percu-aneous placement of an endoluminal covered stent (ar-ows). Function of the existing graft was preserved and itould be used for hemodialysis access immediately afterovered stent placement.
191, 1997 (suppl 3)

H42
vl
Rph1
g1
di3
t1
oI
r4
Mt
kt1
mhI
Cac
Wang and Silberzweig354
2. Basaran O, Karakayali H, Emiroglu R, Belli S,aberal M: Complications and long-term follow-up of416 vascular access procedures. Transplant Proc 35:2578-579, 20033. Pierce GE, Thomas JH, Fenton JR: Novel repair of
enous aneurysms secondary to arteriovenous dialysis fistu-ae. Vasc Endovascular Surg 41:55-60, 2007
4. Welber A, Schur I, Sofocleous CT, Cooper SG, PatelI, Peck SH: Endovascular stent placement for angio-lasty-induced venous rupture related to the treatment ofemodialysis grafts. J Vasc Interv Radiol 10:547-551,9995. Vesely TM: Use of stent grafts to repair hemodialysis
raft-related pseudoaneurysms. J Vasc Interv Radiol 16:1301-307, 20056. Silberzweig JE, Cooper JM, Ahn J, Mitty HA: Hemo-
ialysis graft thrombectomy complicated by Fogarty catheter-nduced arterial pseudoaneurysm. J Vasc Interv Radiol 9:329-31, 19987. Zibari GB, Rohr MS, Landreneau MD, et al: Complica-
ions from permanent hemodialysis vascular access. Surgery
04:681-686, 1988 l8. Yetkin U, Gurbuz A: Post-traumatic pseudoaneurysmf the brachial artery and its surgical treatment. Tex Heartnst J 30:293-297, 2003
9. Crawford DL, Yuschak JV, McCombs PR: Pseudoaneu-ysm of the brachial artery from blunt trauma. J Trauma2:327-329, 199710. Wing TS, Kwok KY, Hester YSC, Bonita KBL:anagement of brachial artery pseudoaneurysms secondary
o drug abuse. Ann Vasc Surg 19:657-661, 200511. Yildirim S, Nursal TZ, Yildirim T, Tarim A, Calis-
an K: Brachial artery pseudoaneurysm: A rare complica-ion after haemodialysis therapy. Acta Chir Belg 105:190-93, 200512. Clark TW, Abraham RJ: Thrombin injection for treat-ent of brachial artery pseudoaneurysm at the site of a
emodialysis fistula: Report of two patients. Cardiovascnterv Radiol 23:396-400, 2000
13. Wongwanit C, Ruangsetakit C, Sermsathanasawadi N,hinsakchai K, Mutirangura P: Treatment of iatrogenic pseudo-neurysm of brachial artery with percutaneous ultrasonographi-ally guided thrombin injection (PUGTI): A case report and a
iterature review. J Med Assoc Thai 90:1673-1679, 2007




























