Embed Size (px)
Citation preview

Faculty of Bioscience Engineering
Academic year 2012-2013
Bovine brucellosis in Bangladesh: Estimationof true prevalence and diagnostic
test-characteristics
Suzanne SmitPromotor: Prof. Dr. Ir. Dirk Berkvens
Master’s dissertation submitted in partial fulfillment of the requirementsfor the degree of
Master of Science in Nutrition and Rural DevelopmentMain subject: Tropical Agriculture
Major: Animal Production

Copyright
“All rights reserved. The author and the promoters permit the use of this Master’s Disser-tation for consulting purposes and copying of parts for personal use. However, any otheruse fall under the limitations of copyright regulations, particularly the stringent obligationto explicitly mention the source when citing parts out of this Master’s Dissertation.”
Ghent University, Augustus 2013
Promoter The Author
Prof. Dr. Ir. Dirk Berkvens Suzanne Smit
contact: [email protected] contact: [email protected]

Acknowledgements
I would like to address my sincere gratitude to Prof. Dr. Ir. Dirk Berkvens for the oppor-tunity to conduct this master thesis and for all the support, education and useful feedbackthroughout its construction. Under the very helpful guidance of Dirk Berkvens the wholeprocess was one of “learning by doing”, which triggered my intellectual capabilities. Forme it was a great experience; it gave me the opportunity to combine my veterinary back-ground with new epidemiological- and mathematical skills. I have always had an interestin epidemiology, but the Veterinary Epidemiology course and subsequent Master Thesiseven further increased this sincere interest. I like the fact that it has a great balancebetween its theoretical part and its practical side with impact on a great scale.Special recognition is given to Dr. Anisur Rahman for the supply of information aboutthe study area, the field- and laboratory work, which resulted in the data used in thisstudy, and the valuable feedback.
In addition, my sincere thanks go my parents for the trust and support they havegiven me to successfully complete this Master of Science. In my struggle, during the lastfew years, to get myself back on track they have helped me enormously. Without theirlove and care i could never have reached where i am now. Thank you mum and dad foreverything. I would also like to thank my brother, Gerben, for being such a good friendand for insisting on fun times during the hard work. New years evening was the start ofa new beginning.. Further more, thanks to all my friends for making my life ”as awesomeas it can be” and for always being there for me.
i

Contents
Acknowledgements i
List of Tables v
List of Figures vi
List of abbreviations vii
Abstract ix
1 Introduction 1
2 Literature Review 32.1 Brucella spp. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2.1.1 Taxonomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32.1.2 Morphology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2.2 Brucellosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42.2.1 Brucellosis worldwide . . . . . . . . . . . . . . . . . . . . . . . . . . 42.2.2 Zoonotic capacity . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52.2.3 Bovine Brucellosis . . . . . . . . . . . . . . . . . . . . . . . . . . . 62.2.4 Brucellosis in Bangladesh . . . . . . . . . . . . . . . . . . . . . . . 7
2.3 Diagnosis of Brucella spp. . . . . . . . . . . . . . . . . . . . . . . . . . . . 82.3.1 Diagnostic methods . . . . . . . . . . . . . . . . . . . . . . . . . . . 82.3.2 Test characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . 92.3.3 Serological response to Brucella . . . . . . . . . . . . . . . . . . . . 102.3.4 Vaccination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122.3.5 Diagnostic tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
2.3.5.1 Agglutination tests . . . . . . . . . . . . . . . . . . . . . . 132.3.5.2 Acidified antigen modifications . . . . . . . . . . . . . . . 142.3.5.3 ELISA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
2.3.6 Conditional independence and dependence of diagnostic tests . . . . 152.3.7 Overparametrisation . . . . . . . . . . . . . . . . . . . . . . . . . . 16
3 Materials and Methods 193.1 Study area . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 193.2 Animal husbandry systems . . . . . . . . . . . . . . . . . . . . . . . . . . . 193.3 Sampling design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203.4 Ethics and consent of farm owner . . . . . . . . . . . . . . . . . . . . . . . 213.5 Processing of blood samples . . . . . . . . . . . . . . . . . . . . . . . . . . 213.6 Serological tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
ii

3.6.1 Indirect Enzyme-Linked Immunosorbent Assay (iELISA) . . . . . . 213.6.2 Rose Bengal Test (RBT) . . . . . . . . . . . . . . . . . . . . . . . . 223.6.3 Slow Agglutination Test (SAT) . . . . . . . . . . . . . . . . . . . . 22
3.7 Statistical analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223.7.1 Modeling approaches . . . . . . . . . . . . . . . . . . . . . . . . . . 23
3.7.1.1 The Hui and Walter model . . . . . . . . . . . . . . . . . 233.7.1.1.1 Deterministic estimation . . . . . . . . . . . . . . 233.7.1.1.2 Probabilistic estimation . . . . . . . . . . . . . . 23
3.7.1.2 Conditional independence . . . . . . . . . . . . . . . . . . 243.7.1.3 Conditional dependence . . . . . . . . . . . . . . . . . . . 24
3.7.1.3.1 Conditional dependence - Covariance scheme . . . 243.7.1.3.2 Conditional dependence - Berkvens et al. scheme 26
3.7.2 Meta analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 273.7.3 Bayesian p-value, PD and DIC . . . . . . . . . . . . . . . . . . . . 28
4 Results 314.1 Meta analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 314.2 Descriptive statistics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324.3 Calculations of the di!erent models . . . . . . . . . . . . . . . . . . . . . . 34
4.3.1 Hui and Walter Model . . . . . . . . . . . . . . . . . . . . . . . . . 344.3.2 Independent model . . . . . . . . . . . . . . . . . . . . . . . . . . . 344.3.3 Conditional dependence - Covariance scheme . . . . . . . . . . . . . 344.3.4 Conditional dependence - Berkvens et al. scheme . . . . . . . . . . 35
4.4 Overall results of the di!erent models . . . . . . . . . . . . . . . . . . . . . 36
5 Discussion 415.1 Comparison of Bayesian models . . . . . . . . . . . . . . . . . . . . . . . . 42
5.1.1 Bayesian p-value, PD and DIC . . . . . . . . . . . . . . . . . . . . 425.1.2 Independent test model . . . . . . . . . . . . . . . . . . . . . . . . . 425.1.3 Hui and Walter models . . . . . . . . . . . . . . . . . . . . . . . . . 435.1.4 Dependent test models . . . . . . . . . . . . . . . . . . . . . . . . . 43
5.2 Results of the model based on conditional dependence - Covariance scheme 445.3 Epidemiology of brucellosis . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
5.3.1 False positive serological cross-reactions . . . . . . . . . . . . . . . . 465.3.2 iELISA cut-o! . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 485.3.3 Comparison of the brucellosis prevalence in Mymensingh and at the
government farm . . . . . . . . . . . . . . . . . . . . . . . . . . . . 485.4 Strategy for control and eradication of brucellosis . . . . . . . . . . . . . . 50
6 Conclusion 55
References 57
Appendices 651 Hui and Walter scheme - deterministic estimation . . . . . . . . . . . . . . 652 Hui and Walter scheme (iELISA (cut-o! 7.5 IU/ml) and RBT) - proba-
bilistic estimation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 663 Conditional independance (Mymensingh - iELISA cut-o! 7.5 IU/ml) . . . . 67
Page iii

4 Conditional dependence - Covariance scheme(Mymensingh - iELISA cut-o! 7.5 IU/ml) . . . . . . . . . . . . . . . . . . 68
5 Conditional dependence - Berkvens et al. scheme (Mymensingh - iELISAcut-o! 7.5 IU/ml) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
6 Prior and posterior beta distributions . . . . . . . . . . . . . . . . . . . . . 72
Page iv

List of Tables
2.1 Two-by-two contingency table . . . . . . . . . . . . . . . . . . . . . . . . . 92.2 Common in use tests for the diagnosis of brucellosis . . . . . . . . . . . . . 13
3.1 Conditional probabilities . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
4.1 iELISA data for the meta-analysis . . . . . . . . . . . . . . . . . . . . . . . 314.2 RBT data for the meta-analysis . . . . . . . . . . . . . . . . . . . . . . . . 324.3 SAT data for the meta-analysis . . . . . . . . . . . . . . . . . . . . . . . . 324.4 Summary values of prior parameters . . . . . . . . . . . . . . . . . . . . . 324.5 Summary values of prior beta distribution parameters . . . . . . . . . . . . 324.6 Cross-classified test results for brucellosis in cattle in Mymensingh and the
government dairy farm based on iELISA, RBT and SAT with di!erentiELISA cut-o! values . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
4.7 Cross-classified test results in Mymensingh and at the government dairyfarm based on iELISA (with a cut-o! value of 7.5 IU/ml) and RBT . . . . 34
4.8 Estimated parameter values using an iELISA cut-o! at 2 units . . . . . . . 374.9 Estimated parameter values using an iELISA cut-o! at 5 units . . . . . . . 384.10 Estimated parameter values using an iELISA cut-o! at 7.5 units . . . . . . 394.11 Estimated parameter values at the government farm using the model based
on conditional dependence - covariance parametrisation with increasingiELISA cut-o! . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
5.1 Summary of Bayesian p-value, pD and DIC results from the di!erent mod-els and optimum values for DIC and pD obtainable from the data . . . . . 42
5.2 Estimates of prevalence and diagnostic test characteristics using the modelbased on conditional dependence - covariance parametrisation with increas-ing iELISA cut-o! . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
5.3 Summary values of posterior beta distribution parameters . . . . . . . . . 46
v

List of Figures
2.1 Worldwide incidence of human brucellosis . . . . . . . . . . . . . . . . . . 42.2 Transmission of Brucella to humans . . . . . . . . . . . . . . . . . . . . . . 52.3 Bovine placenta, containing numerous haemorrhagic cotyledons . . . . . . 72.4 Serological response to Brucella . . . . . . . . . . . . . . . . . . . . . . . . 112.5 Working mechanism of the indirect enzyme immunosorbentassay . . . . . . 15
3.1 Map of Bangladesh showing the study areas . . . . . . . . . . . . . . . . . 20
5.1 Government Farm: Estimates of prevalence and diagnostic test character-istics with increasing iELISA cut-o! . . . . . . . . . . . . . . . . . . . . . . 47
5.2 iELISA units (IU/ml) and status in function of age . . . . . . . . . . . . . 50
vi

List of abbreviations
AI Artificial inseminationBayesp Bayesian p-valueCCBDF Government owned Central cattle Breeding FarmEDTA Ethylenediaminetetraacetic acidcELISA Competitive enzyme-linked immunosorbent assayCI Credibility Intervaldevo Deviance of the observed datadevr Deviance of the sampled pseudo-dataDIC Deviance Information CriterionDT1 Dependent test - covariance parametrisationDT2 Dependent test - conditional parametrisationFPA Fluorescence polarization assayFPSR False positive serological cross-reactionsGovt. farm Government farmHW Hui and WalteriELISA Indirect enzyme-linked immunosorbent assayINF-! test Interferon gamma testIT Independent testsLPS LipopolysaccharideMym MymensinghOD Optical densityOIE World Organization for Animal HealthOPS O-polysacharidepD The e!ective number of estimated parametersprev PrevalenceRBT Rose Bengal TestSAT Slow Agglutination TestSe SensitivitysLPS Smooth-lipopolysaccharideSp SpecificityWHO World Health Organization
vii


Abstract
Brucellosis is a considerable problem worldwide; Brucella is a major bacterial zoonosis,the disease poses a barrier to trade of animals and animal products and can seriouslyimpair socioeconomic development of livestock owners. Bovine brucellosis causes greateconomic loss to livestock industries because it induces delayed œustrus, increased calv-ing interval, birth of weak calves, infectious abortion, infertility and subsequent culling.Furthermore, interruption of lactation may lead to a reduction in milk yield.In the absence of a gold standard, the true exposure prevalence to bovine brucellosis inthe Mymensingh district and the largest Government dairy farm of Bangladesh was esti-mated by means of combining three serological tests. In addition, the performance of thethree tests, namely the indirect enzyme-linked immunosorbent assay (iELISA) test, theRose Bengal Test (RBT) and the Slow Agglutination Test (SAT) was evaluated.
Since iELISA, RBT and SAT are based on similar biological events, namely the detec-tion of serum antibody response, the tests might be considered dependent on each othergiven the true disease status of subjects. However, the full model assuming conditional de-pendence has the implicit characteristic of being overparametrized. Hence, estimation ofthe true disease prevalence and test characteristics becomes either impossible or external(prior) information must be added by means of imposing constraints on the parameters.We imposed di!erent constraints onto four di!erent models; ranging from the assumptionof conditional independence and/or constancy of test parameters over di!erent popu-lations to the specification of prior distributions on parameters using expert opinion.External (prior) information (in the form of beta distributions) was generated by meansof a meta-analysis. By combining the data (test results) and the external information, theposterior means (and the 95% credibility intervals) of the true prevalence and diagnostictest characteristics of all three tests could be estimated at di!erent iELISA cut-o!s (2, 5,7.5, 10, 12.5, 15 and 20 IU/ml). Hence, we used a new way to incorporate expert opinionin the form of prior beta distributions for sensitivities and specificities to estimate the trueprevalence and test characteristics of the three tests in the absence of a gold standard andwe monitored the e!ect of this prior belief on the results.
We suggest that the covariance model, which assumes dependence between tests, is theappropriate model for brucellosis because it permitted us to use all the available prior in-formation. The prevalence decreased and the iELISA specificity increased with increasingiELISA cut-o!. This might be an indication for false positive serological cross-reactions(FPSR) due to cross-reacting antibodies. Comparison of the corrected iELISA ODs showsa dramatic di!erence between Mymensingh, where the iELISA units hardly exceeded 7.5IU/ml, and the government farm, showing much higher titres. In the Mymensingh areawe find a low prevalence and unpublished data show absence of correlation between Bru-cella infection and abortion in this area, which means probably another causative agent
ix

is involved. In contrast, at the government farm the prevalence is high and we mightbe dealing with normal infection dynamics. At a certain iELISA cut-o! all three testsshow a low specificity at the government farm when we compare this to the estimatesin the Mymensingh area, which might be due to higher FPSR prevalence and titers. Itdemonstrates that the test characteristics depend on the area in which the tests are used,and constancy of test characteristics cannot be assumed.Hence, there is reason to recommend using a higher iELISA cut-o! at the governmentfarm compared to the Mymensingh area. To avoid the FPSR problem, we therefore sug-gest to use the results obtained with the covariance model at an iELISA cuto! of 5 IU/mlin the Mymensingh area and 12.5 IU/ml at the government farm.
Further research is necessary to understand why we find such dramatic di!erences iniELISA titers, test characteristics and antibody prevalence between the Mymensingh areaand the government farm and to find the most appropriate cut-o! value. Overall, it wouldbe beneficial to further investigate and improve the diagnostic capabilities, especially sinceFPSR still interfere in serological diagnosis. In addition, further research is necessary tofind the origin of the FPSR and the absence of correlation between abortion and Brucellainfection.
Keywords: Epidemiology - brucellosis - bayesian estimation - prevalence - diagnostictest characteristics.
Page x

1Introduction
Bovine brucellosis is predominantly a disease of sexually mature animals (Rahman etal., 2011; 2012b). It is characteristically associated with abortion at the first gestation(“abortion storm” in naıve heifers) and is mainly caused by biovars (mainly biotype-1) ofBrucella abortus (Godfroid et al., 2010; OIE, 2009). Brucellosis is an enormous problemworldwide; it is endemic in most areas of the world, including Bangladesh (Pappas et al.,2006a; Rahman et al., unpublished).Brucella is a major bacterial zoonosis, the disease poses a barrier to trade of animalsand animal products and can seriously impair socioeconomic development of livestockowners (WHO, 2006). Bovine brucellosis causes great economic loss to livestock indus-tries because it induces delayed œustrus, increased calving interval, birth of weak calves,infectious abortion, infertility and subsequent culling. Furthermore, interruption of lac-tation may lead to a reduction in milk yield (Roth et al., 2003). In Bangladesh, peopleusually live in very close proximity of their livestock and rural income relies largely ondairy products and livestock breeding. Eighty percent of the rural people in the agro-based economy of Bangladesh are directly or indirectly involved in livestock rearing andlivestock contribute to 2.73% of the total GDP (Rahman et al., 2011).In many countries, eradication of the disease is a goal, with only a few countries nowclaiming to be o"cially brucellosis free (Godfroid et al., 2011).
To get a better picture on the current brucellosis situation in Bangladesh, the aimof this study is to estimate the true exposure prevalence to bovine brucellosis in natu-rally infected cattle in the Mymensingh district and the largest Government dairy farmof Bangladesh by applying three diagnostic antibody detection tests simultaneously. Inaddition, the performance of the three serological tests, namely the indirect enzyme-linkedimmunosorbent assay (iELISA) test, the Rose Bengal Test (RBT) and the Slow Agglu-tination Test (SAT), will be evaluated. These tests were previously used in serologicalstudies, although the performance of these tests has not been evaluated in naturally in-fected cattle of Bangladesh.It is traditionally assumed that the values of sensitivity (Se) and specificity (Sp), as sup-plied by the manufacturer of the test, apply to the population on which the test is used.
1

However, these Se and Sp values are usually not constant and universally applicable andassuming constancy of test parameters over di!erent populations may grossly misestimatethe true prevalence. In the absence of a gold standard test, alternative ways to get animproved estimation of Se, Sp and the true prevalence, is combining multiple imperfecttests (Berkvens et al., 2006; Rahman et al., unpublished).
An important consideration however, is whether or not these tests can be assumedconditionally independent. Since iELISA, RBT and SAT are based on similar biologicalevents, namely the detection of serum antibody response, the tests might be considereddependent on each other given the true disease status of subjects. Very few reports havebeen noted where authors considered test dependence in a multiple testing strategy forbrucellosis. Dependency of tests substantially changes the theoretical values of Se and Spof multiple combined tests compared with the values expected when tests are conditionallyindependent. However, the full model assuming conditional dependence has the implicitcharacteristic of being overparametrized. Hence, estimation of the true disease prevalenceand test characteristics becomes either impossible or external (prior) information mustbe added by means of imposing constraints on the parameters.
We will impose di!erent constraints on four di!erent models; ranging from the assump-tion of conditional independence and/or constancy of test parameters over populationsto the specification of prior distributions on parameters using expert opinion. We willstart by eliciting external (prior) information from di!erent publications by means of ameta-analysis. Then, by using the four di!erent models, we will combine the data (testresults) and the external information to obtain posterior means (and the 95% credibilityintervals) of the true prevalence and diagnostic test characteristics of all three tests.
Page 2

2Literature Review
2.1 Brucella spp.
2.1.1 Taxonomy
Brucellosis is caused by Gram-negative bacteria of the genus Brucella. The bacteria belongto the family Brucellaceae within the order Rhizobiales of the class "2-Proteobacteriacea(Garrity, 2001; Lopez-Goni and O’Callaghan, 2012). Although all members of the Bru-cella genus are closely related, the genus is divided into six classical species; Brucellamelitensis, Brucella abortus, Brucella suis, Brucella ovis, Brucella canis and Brucellaneotomae (Osterman and Moriyon, 2006). However, it was proposed to re-classify thegenus as a monospecific genus Brucella, i.e. combining the six species into a single specieswith several biotypes (Verger et al., 1985). In addition to the classical Brucella spp., thegenus has expanded to include marine isolates (Brucella ceti and Brucella pinnipedialis)and a species isolated from the common vole (Brucella microti) (Foster et al., 2007; Scholzet al., 2008). Recently, Brucella inopinata, which is the only species that has not beenisolated from an animal reservoir, was isolated from a breast implant infection in a womanwith clinical signs of brucellosis (Scholz et al., 2010). What led to the division of Brucellaspp. into the di!erent species is the di!erence in biochemical capabilities, susceptibilitiesto dyes and phages together with the di!erence in host preference (Cutler et al., 2005).Although Brucella spp. have a strong a"liation to specific natural hosts, they can infectheterogonous hosts (Boschiroli et al., 2001). The bacteria may a!ect a range of di!erentmammals including cattle, sheep, goats, swine, dogs, rodents, marine animals, severalwildlife species and men. The disease primarily infects the reproductive system in mosthost species, with concurrent loss in productivity (Cutler et al., 2005).
2.1.2 Morphology
Brucella are gram-negative facultative intracellular coccobacilli. These coccobacilli orshort rods measure 0.5 to 0.7 µm wide and 0.6 to 1.5 µm long. They are non-motile andare usually arranged singly, less frequently in pairs or small groups (OIE, 2009).
3

The understanding of the biology of Brucellae has made significant progress over theyears. However, we still seek to understand pathogenicity mechanisms and the details ofhost-microbial interactions (Cutler et al., 2005; Lopez-Goni and O’Callaghan, 2012). Theglobal picture from what is known about Brucella virulence is that it is able to manipulatekey aspects of host cell physiology and it has an extremely e"cient adaptation to shielditself from recognition by the immune system (Gorvel, 2008).
2.2 Brucellosis
2.2.1 Brucellosis worldwide
Brucellosis is an considerable problem worldwide (Figure 2.1). The economic and publichealth impacts remain of particular concern in developing countries. Brucella is a majorbacterial zoonosis, the disease poses a barrier to trade of animals and animal productsand can seriously impair socioeconomic development of livestock owners (WHO, 2006).
Review
Introduction Brucellosis is an old disease with minimal mortality. Yethuman brucellosis remains the commonest zoonoticdisease worldwide with more than 500 000 new casesannually,1–3 is associated with substantial residualdisability,4 and is an important cause of travel-associatedmorbidity.5 The global epidemiology of the disease hasdrastically evolved over the past decade. We focus on thecurrent global distribution of the disease and itsrelocation during the past decade, and attempt to explainthe rationale behind this evolution and its possiblefuture projections.
Global statusFigure 1 depicts the incidence of human brucellosisworldwide. Table 1 shows the countries with the highestannual incidence of human brucellosis from 2000onwards, as well as the incidence for selected othercountries.
USA Until the 1960s, most human cases in the USA wereattributed to Brucella abortus, reaching a high of6321 cases in 1947.27 A massive eradication campaignresulted in the elimination of cattle brucellosis and asubstantial decline in the incidence of human disease.During the 1970s brucellosis was mainly attributed toBrucella suis, prevalent among abattoir workers.28
According to annual reports from the Centers forDisease Control and Prevention (Atlanta, GA),17
2215 cases were reported in the period 1973–82, and1201 cases were reported between 1983 and 1992.1056 cases were reported for the period 1993–2002,more than half deriving from Texas and California. The136 cases and incidence of 0·48 cases per million for2001 represent respective peaks since 1985 and 1983. Asmall decline was noted in 2002. Table 2 shows theaverage annual incidence per state for 1993–2002, andfigure 2 depicts the incidence distribution per state.
Lancet Infect Dis 2006; 6: 91–99
GP, LC and EVT are at the FirstDivision of Internal Medicine ofthe Medical School at theUniversity of Ioannina, Greece;PP is at the PediatricsDepartment of the UniversityHospital of Ioannina, Greece; andNK is at the Internal MedicineDepartment of the GeneralHospital “G Hatzikosta”,Ioannina, Greece.
Correspondence to: Dr Georgios Pappas, InternalMedicine Department, UniversityHospital of Ioannina, 45110,Greece. Tel: +30 26510 49453;[email protected]
http://infection.thelancet.com Vol 6 February 2006 91
The epidemiology of human brucellosis, the commonest zoonotic infection worldwide, has drastically changed overthe past decade because of various sanitary, socioeconomic, and political reasons, together with the evolution ofinternational travel. Several areas traditionally considered to be endemic—eg, France, Israel, and most of LatinAmerica—have achieved control of the disease. On the other hand, new foci of human brucellosis have emerged,particularly in central Asia, while the situation in certain countries of the near east (eg, Syria) is rapidly worsening.Furthermore, the disease is still present, in varying trends, both in European countries and in the USA. Awarenessof this new global map of human brucellosis will allow for proper interventions from international public-healthorganisations.
The new global map of human brucellosisGeorgios Pappas, Photini Papadimitriou, Nikolaos Akritidis, Leonidas Christou, Epameinondas V Tsianos
Annual incidence of brucellosis per 1000 000 population
!50050–500 cases10–502–10"2Possibily endemic, no dataNon-endemic/no data
Figure 1: Worldwide incidence of human brucellosis
Figure 2.1: Worldwide incidence of human brucellosis (Pappas et al., 2006a)
It is endemic in most areas of the world, including Mediterranean Europe, Northernand Sub-Saharan Africa, the Middle East, South East Asia and many South Americancountries. Much of the developing world is still in the early stages of attempting to controlthe disease (Boschiroli et al., 2001; Corbel, 1997; Pappas et al., 2006a).For many countries, eradication of the disease is a goal, with only a few countries nowclaiming to be o"cially brucellosis free, including 12 countries in the EU. In these coun-tries, control has been achieved through the combination of vaccination and test-and-slaughter programs coupled with e!ective disease surveillance, animal movement controland milk pasteurization (McDermott and Arimi, 2002). Together with compensation forfarmers, accreditation and financial incentives for disease free herds, this status could beachieved. However, the threat of reintroduction is ever present through the movement oflivestock (Godfroid et al., 2011).
Page 4

2.2.2 Zoonotic capacity
Brucella is one of the worlds most widespread zoonotic pathogens; it infects approxi-mately 500.000 people worldwide annually (He, 2012). Although it is the most commonbacterial zoonotic infection, it is still a regionally neglected disease (Pappas et al., 2006a).It can result in significant human morbidity, particularly in some of the endemic areas(Boschiroli et al., 2001; Corbel, 1997; OIE, 2009). Infection in man is associated withdi!erent manifestations and characteristically with recurrent febrile episodes. This ledto the description of the disease as undulant fever, Malta fever or Mediterranean fever(Corbel, 1997; Cutler et al., 2005).Brucella melitensis, B. abortus, B. suis and B. canis are pathogenic to humans, althoughinfections with B. canis are rare (Figure 2.2) (He, 2012). The majority of the humaninfections are due to B. melitensis. Brucella melitensis infection in cattle, which is lesscommon, is therefore of serious public health importance (Renukaradhya et al., 2002).In most cases, the disease is caused by consumption of contaminated non-pasteurised milkand cheese or as an accidental or occupational exposure to infected animals or carcasses,aborted fœtuses or uterine secretions (Corbel, 1997; Young, 1995). Less often, manipula-tion of live vaccine strains or virulent Brucella in the laboratory may also cause accidentalinfection (Corbel, 1997; Young, 1995). The World Health Organization (WHO) labora-tory biosafety manual classifies Brucella in risk group III and specific recommendationshave been made for the biosafety precautions to be observed with Brucella-infected ma-terials (OIE, 2009; WHO, 2006).Animal brucellosis is therefore of significant public health importance for livestock farmers,dairy workers, slaughterhouse personnel, veterinarians, and laboratory personnel (Rah-man et al., 2012a). Raw milk consumption, close intimacy with animals and low awarenesson zoonosis facilitate transmission of the disease to men (Megersa et al., 2012).Brucella melitensis, B. suis and B. abortus strains are even included on the list of etiologicagents considered to pose risk for use as bioweapons (Pappas et al., 2006b).
Figure 2.2: Transmission of Brucella to humans (Gadaga, 2013)
Page 5

Brucella infected people often su!er from a chronic, debilitating and disabling illness.Clinical symptoms are non-specific systemic signs including amongst others, fever, sweat-ing, anorexia, fatigue and headache. Given the high proportion of brucellosis cases withfever, brucellosis should be considered as a di!erential diagnosis for fevers of unknownorigin. This is especially important in malaria endemic areas where fever is often as-sumed to be malaria. Poor diagnosis and treatment may result in serious, sometimeslife-threatening, complications such as infectious endocarditis, encephalitis and spondyli-tis and testicular infection can cause sterility. The disease may progress into a morechronic form and debilitation can result from brucellosis infection because joint, muscleand back pain are common manifestations (Dean et al., 2012).Unfortunately, there is no safe, e!ective human brucellosis vaccine (He, 2012). Since in-fected animals are the reservoir, the key for eradicating the disease in men is preventionand control of animal brucellosis (Boschiroli et al., 2001).
2.2.3 Bovine Brucellosis
Bovine brucellosis is predominantly a disease of sexually mature animals (Rahman etal., 2011; 2012b). It is characteristically associated with abortion at the first gestation(“abortion storm” in naıve heifers) and is mainly caused by biovars (mainly biotype-1) ofBrucella abortus (Godfroid et al., 2010; OIE, 2009). However, both B. melitensis and B.suis in cattle are also an emerging veterinary and public health problem.Brucella melitensis is capable of colonizing the bovine udder, with consequent excretionin the milk. Cases of cross-infection with B. melitensis are reported especially where cat-tle are kept in close association with goats and/or sheep (Samaha et al., 2008). Brucellaabortus infection in sheep and B. melitensis in cattle were only reported when a source ofBrucella spp. was found in its preferential host, i.e. B. melitensis in sheep and B. abortusin cattle. This suggest that B. abortus in sheep and B. melitensis infection in cattle arespill over infections and cannot establish enzootic infections (Godfroid et al., 2011).Brucella suis is found worldwide in most areas where pigs are kept, although brucellosis isalso described in wild suidae (Godfroid et al., 2011). Brucella suis has not been reportedto cause abortion or spread to other animals, but it may occasionally cause a chronicinfection in the mammary gland of cattle with excretion of the bacteria in the milk (God-froid et al., 2011; Olsen and Hennager, 2010). In South Carolina, USA, it has recentlybeen shown that feral pigs were infected with B. abortus wildtype, S19 and RB51 vaccinestrains besides B. suis biovar 1 (Sto!regen et al., 2007). It is of special veterinary andpublic health importance because it demonstrates that pigs can act as reservoir host forB. abortus in the absence of contact with cattle for more than 25 years (Godfroid et al.,2011). An unpublished observation of B. abortus S19 in a goat in Ecuador also exemplifiesthe danger of cross-infection (Berkvens, pers.comm.).Importantly, B. melitensis and B. suis infections interfere with serological diagnosis ofB. abortus infection in cattle (Ewalt et al., 1997).
Brucella spp. is commonly transmitted to other animals by indirect or direct con-tact with infected animals or their discharges (OIE, 2009). The bacteria invade theblood stream and lymphatics upon entry into humans or animals. Here they multiplyin phagocytic cells and eventually cause septicaemia. The lifecycle contains two phases:(i) a chronic infection of phagocytic macrophage, which results in bacterial survival andreplication for prolonged periods of time and (ii) an acute infection leading to reproduc-
Page 6

tive tract pathology and abortion when the bacteria infect non-phagocytic epithelial cells(Hort et al., 2003). The outcome of infection in cattle is dependent on age, reproductiveand immunological status, natural resistance, route of infection, infectious challenge andvirulence of the infective strain (Adams, 2002). Bovine brucellosis causes great economicloss to livestock industries because it induces delayed œustrus, increased calving interval,birth of weak calves, infectious abortion, infertility and subsequent culling. Furthermore,interruption of lactation may lead to a reduction in milk yield (Roth et al., 2003).In acute infections, the bacteria are present in most major lymph nodes of the body andreplicate in large numbers in placental trophoblasts of pregnant adult females, which canresult in disruption of the integrity of the placenta. Hence, B. abortus or B. melitensiscan induce placentitis, usually resulting in abortion between the fifth and ninth month ofpregnancy (Figure 2.3)(OIE, 2009). The pregnant uterus is an immunological privilegedsite, which prevents the rejection of the fetus by modulating local immune responses.This may in turn allow Brucella spp. to replicate extensively (Neta et al., 2010). Pro-fuse excretion of the bacteria occurs in the placenta, fetal fluids and vaginal discharges,even in the absence of abortion. In addition, the mammary gland and associated lymphnodes may be infected, which can result in excretion of organisms in the milk (OIE, 2009).
Figure 2.3: Bovine placenta, containing numerous haemorrhagic cotyledons (the cen-ter for food security and public health, 2009)
Usually, infected females abort only once, although the infection may persist for theirwhole life (Godfroid et al., 2010). In non-pregnant females the disease is usually asymp-tomatic and after the first episode of Brucella induced abortion, the cow often has normalsubsequent parturitions. However, uterine and mammary infection recurs, with reducednumber of organisms in milk and uterine secretions (OIE, 2009). Animals are thereforenot always contagious; excretion only occurs at certain times (Godfroid et al., 2010).Brucellosis can cause infertility in both sexes; adult male cattle may develop orchitisand/or epididymitis. Another common manifestation of brucellosis in some tropic coun-tries is hygromas (localized swelling), usually involving leg joints (OIE, 2009).
2.2.4 Brucellosis in Bangladesh
In Bangladesh, brucellosis is endemic (Rahman et al., 2011). The disease may constitute aconsiderable impact on human and animal health as well as on socioeconomic factors andit might be a significant drawback in the development of the livestock sector (Rahman etal., 2011; 2012b). People usually live in very close proximity of their livestock and ruralincome relies largely on dairy products and livestock breeding. Eighty percent of the
Page 7

rural people in the agro-based economy of Bangladesh are directly or indirectly involvedin livestock rearing and livestock contribute to 2.73% of the total GDP. An estimated1.86 million bu!aloes, 1.1 million sheep, 33.5 million goats and 23.5 million cattle arebeing reared in Bangladesh (Rahman et al., 2011). There are abundant opportunitiesfor intermixing of species; both on grazing lands and in smallholdings of mixed livestock(Rahman et al., 2012b).Many undiagnosed cases of retained placenta, stillbirth and abortion in cattle, bu!aloes,sheep and goats are reported every year, in which Brucella might be the causal agent(Rahman et al., 2012b). The Rose Bengal Test (RBT) and Slow Agglutination Test(SAT), either alone or in series, were used in previous serological studies in Bangladesh.However, previous reported sero-prevalence using these tests were apparent prevalencesince none of these tests is considered to be a gold standard. In addition, the performanceof these tests, which is traditionally evaluated by comparison to a perfect test, has notbeen evaluated in naturally infected cattle of Bangladesh (Rahman et al., unpublished).The severity and prevalence of the disease may vary with the type of diagnostic test,geographic location, breed, husbandry and environmental factors (Amin et al., 2005).The sero-prevalence is significantly higher in animals with previous abortion reported,compared to animals with no abortion record. In addition, in females a relatively higherprevalence is found than in male cattle, sheep and goats although in the case of bu!aloes,this is the other way around (Rahman et al., 2012b). Furthermore, significant associationis reported between age and sero-prevalence of brucellosis. In cattle and bu!alo, thehighest sero-prevalence was found in the age group above 48 months of age (Rahmanet al., 2011). This may be because the bacteria can remain latent or chronic for anunspecified period of time before manifesting as clinical disease. Alternatively, the highersero-prevalence among older cows may be related to aged animals having a greater chanceof coming into contact with other animals and becoming infected (Rahman et al., 2011).Because vaccination has never been practiced in Bangladesh, sero-positivity is consideredto be due to natural infection (Amin et al., 2005).
2.3 Diagnosis of Brucella spp.
2.3.1 Diagnostic methods
In cattle, all abortions from the fifth month should be treated as suspected and investi-gated for brucellosis. Since many pathogens can cause abortion, the clinical diagnosis ofbrucellosis on the basis of abortion is equivocal (OIE, 2009). Therefore, diagnostic meth-ods, including direct and indirect tests, are essential. Direct tests involve microbiologicalanalysis or polymerase chain reaction (PCR)-based methods detecting DNA. On the otherhand, indirect tests, either applied in vitro on blood or milk or in vivo (skin test), arebased on the detection of immune responses induced by infection (Godfroid et al., 2010).Only the direct test, with isolation and identification of Brucella spp., is defined as the“gold standard” for diagnosis of brucellosis (OIE, 2009). A gold standard test, or perfecttest, is a diagnostic test with 100% sensitivity and specificity (Berkvens et al., 2006).However, the direct test is better considered to be a so-called confirmatory reference test,because in practice the sensitivity is far below 100%. Bacteriological examination of milk,colostrum, tissues, abortion material, vaginal secretions, semen or fluid collected fromarthritis or hygroma is not practicable for routine application (OIE, 2009; WHO, 2006).Brucella culture takes several days to weeks to grow (Rahman et al., 2012a).
Page 8

Furthermore, in developing countries direct diagnosis is usually di"cult to perform due tothe requirement of sophisticated laboratory facilities with high level of safety containmentand experienced personnel (Rahman, unpublished). Diagnostic methods for brucellosishave therefore primarily been based on serology. The lipopolysaccharides (LPS) on thecell surface of smooth Brucella strains produce the greatest immunological responses invarious hosts (Cutler et al., 2005).Since none of the currently available serological tests can be seen as a gold standard, itis important to know the tests characteristics of these tests (Muma et al., 2007b). Andbecause all serological tests have limitations, no single serological test is appropriate inall epidemiological situations (Nielsen et al., 2006). The use of at least two tests is recom-mended; samples that are positive in a screening test should be assessed in a confirmatorytest and/or complementary strategy (OIE, 2009).
2.3.2 Test characteristics
The sensitivity (Se) and specificity (Sp) determine the validity of a test. Serological testresults should be analysed according to the true disease status of an animal in order tobe able to estimate these test characteristics (Godfroid et al., 2010).Suppose that T+(T!) indicates a positive (negative) diagnostic test result and D+(D!)that a subject is diseased (disease-free). The number of diseased (nD+) and disease-free subjects (nD!) are known when a gold standard test, with 100% sensitivity andspecificity, is used. This is also the case in an experiment where a proportion of thesubjects are artificially infected. Table 2.1 represents testing n subjects for disease Dwith one diagnostic test T (Berkvens et al., 2006).
Table 2.1: Two-by-two contingency table
Diseased (D+) Disease-free (D!) Total
Positive test result (T+) nT+|D+ nT+|D! nT+
Negative test result (T!) nT!|D+ nT!|D! nT!
Total nD+ nD! n
where n indicates the number of subjects, T+(T!) indicates a positive (negative) test resultwith diagnostic test T and D+(D!) indicates that the subject is diseased (disease-free)
The sensitivity (Se) is defined as the probability of a positive test given that the animalis truly diseased and the specificity (Sp) as the probability of a negative test result giventhat the animal is truly disease free. Derived from Table 2.1, the following estimation ofsensitivity and specificity can be given (Berkvens et al., 2006):
Sensitivity =nT+|D+
nD+=
number of true positives
number of true positives + number of false negatives
Specificity =nT!|D!
nD!=
number of true negatives
number of true negatives + number of false positives
Page 9

In addition, the positive predictive value (PPV = the proportion of test results thatare true positive) and negative predictive value (NPV = the proportion of negative testresults that are true negative) can be derived from Table 2.1.
PPV =nT+|D+
nT+=
number of true positives
number of true positives + number of false positives
NPV =nT!|D!
nT!=
number of true negatives
number of true negatives + number of false negatives
Traditionally, some textbooks define the sensitivity and specificity as values, which areintrinsic to the diagnostic test (Rogan and Gladen, 1978; Thrusfield, 1995). These valuesare theoretical concepts determined in the population to validate the test (Berkvens et al.,2006; Greiner and Gardner, 2000). However, sensitivity parameters need to be determentin experimental conditions or with a gold standard, often on a small number of subjects,and are therefore usually quite distinct from the real-life situation. Estimation of speci-ficity parameters on the other hand is easier since these can be estimated in a population,which is known to be disease free (Berkvens et al., 2006). Moreover, it is argued that Seand Sp values are not constant and universally applicable, but vary with external factors(Saegerman et al., 2004) and others (Greiner and Gardner, 2000). Assuming constancyof test parameters over di!erent populations may grossly misestimate true prevalence.Therefore, to get an improved estimation of Se and Sp, the characteristics of the popu-lation of interest must be used when applying a test in that population (Berkvens et al.,2006; Greiner and Gardner, 2000).
In a field observation only the probability of a positive test result, i.e. the apparentprevalence, can be directly estimated as P (T+) = nT+/n. The true prevalence P (D+)can be estimated using the prevalence estimator proposed by Rogan and Gladen (1978):
P (D+) =P (T+) + Sp! 1
Se+ Sp! 1
This implies that the sensitivity and specificity must be known. However, since Se and Spare rarely know exactly, these must be estimated from data, which means we have to takeinto account the sampling variability with which the prevalence is estimated (Berkvens etal. 2006; Rogan and Gladen, 1978).
There exists a warning that Table 2.1 contains inherently little information on thetrue prevalence and the test characteristics (Berkvens et al., 2006). The data resultingfrom one or two tests in the absence of confirmatory testing by a gold standard test areinsu"cient to estimate all of the parameters (Johnson et al., 2000).
2.3.3 Serological response to Brucella
Brucella abortus, B. melitensis and B. suis comprise the most important species whichcontain O-polysacharide (OPS), which is part of the lipopolysaccharide (LPS), on theircell surface (Nielsen, 2002). These OPS containing species are diagnosed serologically
Page 10

using either smooth lipopolysacharide (sLPS) prepared by chemical extraction or a wholecell antigen. Virtually all serological tests for antibody to these bacteria utilize B. abortusantigen because common epitopes are present in B. melitensis, B. suis and B. abortus(OIE, 2009). Because sLPS is shared to a great extent by the di"rent smooth Brucellaspp., it is not possible to ascribe which Brucella spp. (B. abortus, B. melitensis or B. suis)induces the antibodies (Corbel, 1985).
Frequently, the diagnosis of brucellosis is di"cult, because the serological response incattle is influenced by several factors. These include the type of exposure, the stage ofgestation at the time of exposure, the vaccination status and the variable and long incu-bation period during which serotest results are negative (Lord et al., 1988).The antibody response to Brucella, shown in Figure 2.4, consists of an early IgM iso-type response 2-3 weeks after exposure, which may disappear after a few months. Thisrapidly induced IgM response is followed almost immediately by production of IgG. TheIgG response shows a peak around approximately 3-4 weeks post infection, persists andremains detectable over a long period of time (up to several years) (Godfroid et al., 2002;Saegerman et al., 2004). Given the kinetics of the immune responses induced after infec-tion, epidemiological information is extremely important for informing the interpretationof test results, because the time-point post infection at which sampling and testing occurshas a major impact on the results (Godfroid et al., 2010).The activity of these immunoglobulin isotypes in the di!erent serological tests and theirkinetics of appearance and disappearance might permit the distinction between acute andchronic infection. The presence of IgG alone is characteristic for chronic brucellosis, whilea combination of IgM and IgG suggests acute infection. Furthermore, to be indicativefor brucellosis, a seropositive response in a predominantly IgM detecting test has to beconfirmed within one week by a test, which mainly detects IgG (Godfroid et al., 2010).
IgG
SAT+ELISA-
SAT+ELISA+
SAT-ELISA+
SAT-ELISA-
IgMSAT cut-o!
ELISA cut-o!
Ig
time
ELISA+
SAT+
Figure 2.4: Serological response to Brucella and outcome of the Slow Agglutina-tion Test (SAT - mainly measuring IgM) and enzyme immunoassay test(ELISA - mainly measuring IgG) (Godfroid et al., 2010)
Page 11

The serological test results can be strongly influenced by the presence of false positiveserological cross-reactions (FPSR) due to other gram-negative bacteria sharing antigenicdeterminats with the Brucella O-chain. Cross-reactivity was observed between BrucellasLPS and sLPS of other bacteria such as Yersinia enterocolitica O:9, Salmonella groupN (O:30), Vibrio cholera O1, Escherichia coli O:157, some strains of Escherichia her-manni and Stenotrophomonas maltophila (Gerbier et al., 1997). Potentially, FPSR dueto Yersinia enterocolitica O:9 presents the most serious source of confusion since theimmune-dominant O-chain of sLPS of Yersinia enterocolitica serotype O:9 and Brucellaspecies are identical (Saegerman et al., 2004).Serological tests that measure IgM are not desirable as false positive results occur, sincemost cross-reacting antibody consist mainly of IgM. Therefore the main isotype for sero-logical testing is IgG1 and assays that predominantly measure IgG1 are the most useful(Nielsen., 2002).
2.3.4 Vaccination
In 1930, Buck introduced a vaccine, B. abortus S19, against bovine brucellosis. This at-tenuated (live) vaccine was useful in controlling and eliminating the disease in many areasin the world (Nielsen and Gall, 2001). Because the vaccine carries a smooth lipopolysac-charide (sLPS) with an O-polysaccharide similar to that of the wild type Brucellae, itinduces anti-O-antigen antibody in the host (He, 2012; Schurig et al., 1991).
Limitations of the vaccine are that it may induce abortion if applied during pregnancy,it may induce lesions in males and a small proportion of animals may develop subclinicalinfections and shed the vaccine. However, the major drawback of the vaccine is that S19generates immune responses interfering in diagnostic tests (Godfroid et al., 2011).Many countries use test and slaughter regimes and a strict embargo on transport andsale of infected animals to eradicate the disease. This makes it important to be able todistinguish between an animal that is vaccinated or one infected with a virulent bacteria(Boschiroli et al., 2001). Before the development of the primary binding assays, vacci-nation frequently confounded serological diagnosis, because many of the serological testscould not distinguish antibodies resulting from infection from that due to vaccination(Nielsen and Gall, 2001; Nielsen et al., 2002). This lead to allowance of higher antibodylevels and the common practice of vaccinating animals before the age of 10 months, whichresults in a reduction of antibody level before sexual maturity (Nielsen, 2002). Conjunc-tival vaccination with reduced doses before the age of 4 months avoids the serologicalinterference as well as the abortions and udder infections (Godfroid et al., 2011).To overcome the interference with diagnostic tests a (R mutant) vaccine, B. abortus RB51,derived from smooth virulent strain 2308 was developed. Because it contains no or minuteamounts of OPS on its cell surface, it induces no or a minimal anti-O-antigen serologi-cal antibody response (He, 2012; Nielsen, 2002; Schurig et al., 1991). However, it alsohas its limitations and it yields inferior protection compared to S19 and, furthermore, itis resistant to rifampicin and penicillin and thus poses a potential risk for public health(Godfroid et al., 2011; Moriyon et al., 2004). Another way was the development of the pri-mary binding assays including the fluorescence polarization assay (FPA) and competitiveenzyme immunoassays (cELISA) (Nielsen et al., 2002).
Page 12

2.3.5 Diagnostic tests
Diagnostic tests can be applied for di!erent goals: Screening or confirmation diagno-sis, prevalence studies and for surveillance purposes. The choice of a particular testingstrategy depends on the goal and the epidemiological situation in the region of interest(Godfroid et al., 2010). One of the principle requirements of a screening test is that it iseconomical, rapid and in order to ensure all true serological reactors are detected it mustbe as diagnostically sensitive as possible, but it need not to be highly specific. This meansa high number of false positive reactions may be expected. Therefore confirmatory tests,to be used on sera that reacted positively in screening tests, are recommended. They areusually more complicated but show a high level of diagnostic specificity and yet maintainan e!ective sensitivity (Nielsen, 2002; Stemshorn, 1985). Common in use tests for thediagnosis of brucellosis are shown in Table 2.2 (Nielsen, 2002):
Table 2.2: Common in use tests for the diagnosis of brucellosis
Tests Agglutination tests: Primary binding assays:
Slow agglutination (SAT) Radioimmunoassay (RIA)Acidified antigen (RBT, card , BPAT) Particle concentration fluorescence immunoassay (PCFIA)High salt Indirect enzyme-linked immunosorbent assay (iELISA)EDTA Competitive enzyme-linked immunosorbent assay (cELISA)Reducing agents (2ME, DTT) Fluorescence polarization assay (FPA)Rivanol (RIV)HeatAntiglobulin testsMilk ring test (MRT)
Tests Complement fixation tests: Precipitation tests:
Warm (CFT) Agar gel immunodi!usion test (AGID)Cold Single radial immunodi!usion test (SRD)Indirect hemolysis test (IHLT)Hemolysis in gel (HIG)
In our study we used the following serological tests; Slow Agglutination Test (SAT),Rose Bengal Test (RBT) and the indirect enzyme-linked immunosorbent assay (iELISA).These tests are therefore further discussed.
2.3.5.1 Agglutination tests
More than 100 years ago serological diagnosis of brucellosis began with a simple agglu-tination test. This test format was simple, inexpensive and could be rapid, althoughresults were subjectively scored (Nielsen, 2002). The principle of the slow agglutinationtest (SAT) is that it detects agglutinin antibodies (mainly IgM, but also IgG) againstBrucella spp.. Large antigen-antibody complexes form when antibodies are present in thesample and precipitate at the bottom of the test tube or plate (Godfroid et al., 2010).At a slightly below neutral or neutral pH, IgM isotype of antibody is the most activeagglutinin, which makes the SAT susceptible to false positive reactions by cross-reactingantibody, resulting in specificity problems (Nielsen et al., 1984). Therefore, the OIErecommends the discontinuation of this test as a diagnostic tool (OIE, 2009). A lot ofmodifications were made to destroy or inactivate IgM agglutinins. Commonly used modi-fications are acidified antigen, rivanol precipitation and the use of 2-mercaptoethanol andethylenediaminetetraacetic acid (EDTA) (Nielsen, 2002).
Page 13

2.3.5.2 Acidified antigen modifications
The rose-bengal test (RBT) (Davis, 1971) is a commonly used, inexpensive, standardizedand easy to perform agglutination test. The test uses whole cells stained with rose-bengal.The low PH used (PH 3.65) reduces non-specific reactions because it prevents some ag-glutination by IgM and encourages agglutination by IgG1 (Corbel, 1973). RBT is verysensitive and is considered as screening test. However, rarely false negative reactions occurmainly due to prozoning, which results in sensitivity limitations (OIE, 2009). Prozoningoccurs when too many antibodies are present to bind to the antigens. Since in this casefew or no antibodies bind more than one antigenic particle and no bridges are made be-tween antigens, no agglutination occurs. Consequently, the test result is false negative.Prozoning can be avoided by diluting the serum.In addition, some cross-reacting antibodies and antibodies resulting from B. abortus S19vaccination are detected by the test. Therefore it is necessary to use other test(s) for con-firmation. Nevertheless RBT appears to be adequate as a screening test to guarantee theabsence of infection in brucellosis-free herds or for detecting infected herds (OIE, 2009).
2.3.5.3 ELISA
There are two categories of enzyme-linked immunosorbent assay tests (ELISA), the com-petitive ELISA (cELISA) and the indirect ELISA (iELISA). Most iELISAs use purifiedsmooth lipopolisacharide (sLPS) as antigen but also whole cells or the O-polisacharide(OPS) are used. The iELISA is highly sensitive but lacks the capability to fully resolvethe FPSR problem and the problem of di!erentiating between antibodies resulting frominfection and S19 vaccination (OIE, 2009). The cELISA is based on specific epitopes ofthe OPS and can therefore eliminate some of the cross-reaction problems seen in iELISA.Although cELISA is shown to have higher diagnostic specificity it has a lower sensitivitythan the iELISA (Munoz et al., 2005).
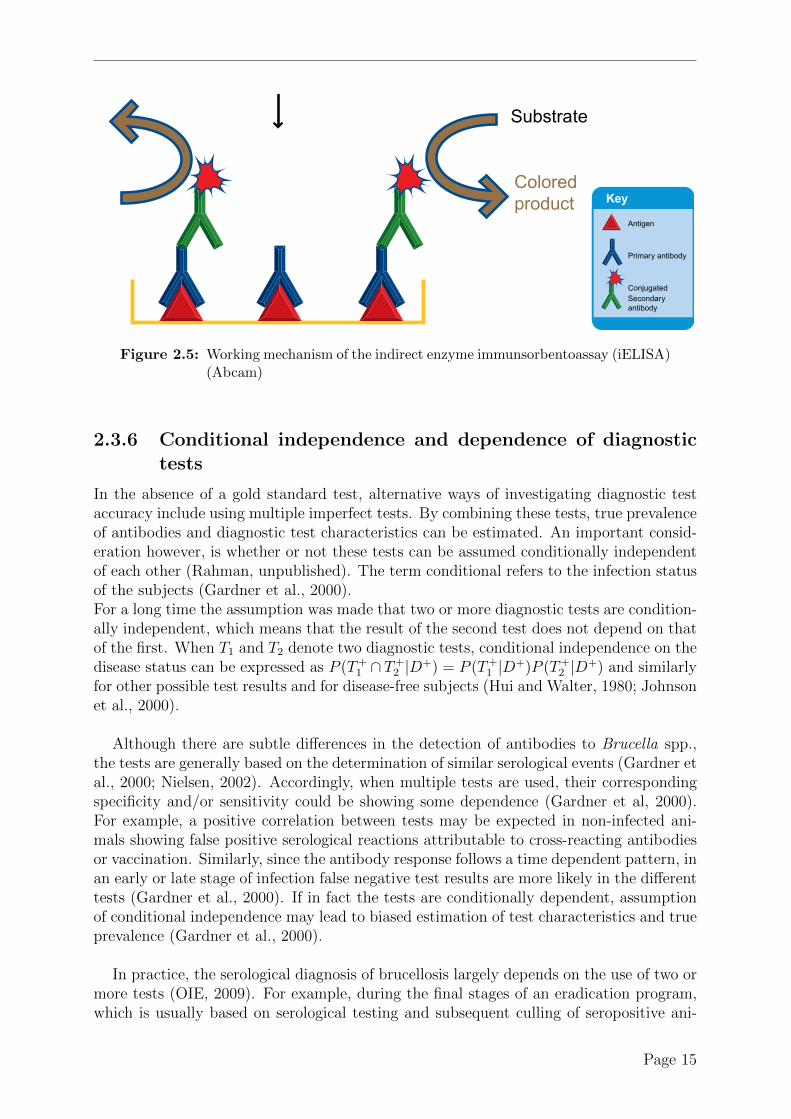
Figure 2.5 shows the working mechanism of iELISA. First, the antigens are immobilizedon a solid support. Then diluted test sera are added to the plates, and antibody-antigencomplexes are formed when antibodies (mainly IgG) against Brucella are present in thesample. An enzyme-conjugated secondary antibody detects and quantifies the primaryantibody. In the final step, a substance containing the enzyme"s substrate is added. Theoptical density (OD) of the visually detectable signal (usually a colour development),resulting from the enzymatic reaction, can be detected by spectrophotometry (Nielsen,2002; OIE, 2009). Assessment of assay performance and quality are conducted by in-cluding a negative, weak positive and strong positive control serum. Frequently, data isexpressed as reactivity percentage of the strong positive control (Nielsen, 2002).
Page 14
Key
Block with 5% serum or BSA 2 hr or overnight 4˚C
Wash plates with PBS 0.2% Tween 20 4 times
Wash plates with PBS 0.2% Tween 20 4 times
Wash plates with PBS 0.2% Tween 20 4 times
Substrate
Coloredproduct
Read absorbance on ELISA platereader and analyze results
Add conjugatedsecondary antibodyIncubate 1 - 2 hr
Enzymatic detectionFollow manufacturersrecommendations
Incubate with primary antibody2 hr RT or 4˚C overnight
Coat plate with antigen2 hr RT or 4˚C overnight
Antigen
Primary antibody
Conjugated Secondary antibody
Indirect ELISA
Key
Block with 5% serum or BSA 2 hr or overnight 4˚C
Wash plates with PBS 0.2% Tween 20 4 times
Wash plates with PBS 0.2% Tween 20 4 times
Wash plates with PBS 0.2% Tween 20 4 times
Substrate
Coloredproduct
Read absorbance on ELISA platereader and analyze results
Add conjugatedsecondary antibodyIncubate 1 - 2 hr
Enzymatic detectionFollow manufacturersrecommendations
Incubate with primary antibody2 hr RT or 4˚C overnight
Coat plate with antigen2 hr RT or 4˚C overnight
Antigen
Primary antibody
Conjugated Secondary antibody
Indirect ELISA
Figure 2.5: Working mechanism of the indirect enzyme immunsorbentoassay (iELISA)(Abcam)
2.3.6 Conditional independence and dependence of diagnostictests
In the absence of a gold standard test, alternative ways of investigating diagnostic testaccuracy include using multiple imperfect tests. By combining these tests, true prevalenceof antibodies and diagnostic test characteristics can be estimated. An important consid-eration however, is whether or not these tests can be assumed conditionally independentof each other (Rahman, unpublished). The term conditional refers to the infection statusof the subjects (Gardner et al., 2000).For a long time the assumption was made that two or more diagnostic tests are condition-ally independent, which means that the result of the second test does not depend on thatof the first. When T1 and T2 denote two diagnostic tests, conditional independence on thedisease status can be expressed as P (T+
1 " T+2 |D+) = P (T+
1 |D+)P (T+2 |D+) and similarly
for other possible test results and for disease-free subjects (Hui and Walter, 1980; Johnsonet al., 2000).
Although there are subtle di!erences in the detection of antibodies to Brucella spp.,the tests are generally based on the determination of similar serological events (Gardner etal., 2000; Nielsen, 2002). Accordingly, when multiple tests are used, their correspondingspecificity and/or sensitivity could be showing some dependence (Gardner et al, 2000).For example, a positive correlation between tests may be expected in non-infected ani-mals showing false positive serological reactions attributable to cross-reacting antibodiesor vaccination. Similarly, since the antibody response follows a time dependent pattern, inan early or late stage of infection false negative test results are more likely in the di!erenttests (Gardner et al., 2000). If in fact the tests are conditionally dependent, assumptionof conditional independence may lead to biased estimation of test characteristics and trueprevalence (Gardner et al., 2000).
In practice, the serological diagnosis of brucellosis largely depends on the use of two ormore tests (OIE, 2009). For example, during the final stages of an eradication program,which is usually based on serological testing and subsequent culling of seropositive ani-
Page 15

mals, the specificity of serological tests is of utmost importance (Godfroid et al., 2002;Muoz et al., 2005). In this case, it is usually recommended to apply at least two testsserially because this maximizes specificity and positive predictive value. However, it mayhave the risk of missing true positive cases (Mainar-Jaime et al., 2005).
When test specificities are conditionally independent of each other, the resulting ex-pected specificity of serial testing is said to be higher than the corresponding individualspecificities (Sp1 and Sp2) of each test (Dohoo et al., 2003). In this case, the expectedspecificity is expressed as Spexp = 1! (1! Sp1)(1! Sp2) (Mainar-Jaime et al., 2005).However, when the diagnostic tests show specificity dependence, the overall specificitywill be lower than if the tests are conditionally independent. In this case, the specificityis expressed by the formula Spdep = 1 ! (1 ! Sp1)(1 ! Sp2) ! !Sp. Here, !Sp is an es-timation of the specificity dependence between the two tests, which is zero when testspecificities are conditionally independent (Mainar-Jaime et al., 2005). This conditionalcovariance for specificity (!Sp) can be calculated as !Sp = p ! Sp1Sp2, where p is theobserved proportion of non-infected animals that are negative in both tests (Gardner etal., 2000). Consequently, a positive dependence in test specificity reduces the specificityof serial interpretation compared to the values obtained when conditional independence isassumed. Similarly, the sensitivity of parallel test interpretation is reduced when a posi-tive dependence in test sensitivity exists (Gardner et al., 2000; Mainar-Jaime et al., 2005).
It is the overall balance between individual specificities and specificity dependence thatmakes a combination of tests more or less appropriate for a given situation. Evidence ofdependence between tests may be obscured when the individual specificity of a test, tobe used in serial testing, is overestimated, giving a false assumption of independence be-tween tests (Mainar-Jaime et al., 2005). The evaluation of test accuracy must alwaysbe performed on representative populations of the context in which the test has to beused (Munoz et al., 2005). One should be cautious when recommending testing schemeswithout consideration of di!erent epidemiological situations.For example, in the existence of a FPSR problem, certain test combinations can result ina considerable increase in the number of false positive reactors in eradication programs(Mainar-Jaime et al., 2005). In addition, it has been argued that serial testing using pairsof specificity-correlated serological tests have lower specificity than expected when appliedto disease free populations. At a low disease prevalence (<1%), an increased proportionof non-infected animals are classified as seropositive and the positive predictive value ofthe test is closer to zero (Dohoo et al., 2003; Mainar-Jaime et al., 2005).Importantly, assuming constancy of test parameters over di!erent populations and inde-pendence of tests, may grossly misestimate true prevalence (Berkvens et al., 2006).
2.3.7 Overparametrisation
When applying h tests to each individual 2h ! 1 parameters can be estimated. However,when tests show conditional dependence 2h+1 ! 1 parameters need to be estimated. Thisincludes the true prevalence, h test sensitivities and specificities and 2h+1 ! 2h ! 2 pa-rameters representing the dependence of the tests, given the true disease status. Theparameters to be estimated under conditional independence are equal to 2h+1 (Berkvenset al., 2006). This means that in the in the case of three tests (h=3) the maximum numberof estimable parameters is 7. When the tests are conditional independent the estimable
Page 16

parameters are equal to the 7 parameters to estimate. However, when conditional de-pendence exists between the tests, 15 parameters must be estimated, which exceeds theamount that can be estimated. Because more parameters must be estimated than thedata permit, estimation of the true disease prevalence and test characteristics becomeseither impossible or extra information must be added by means of imposing constraintson the parameters. These restrictions must come from external sources (expert opinion,previous similar studies, etc.) and can be classified in two types: deterministic and prob-abilistic constraints (Berkvens et al, 2006).
Examples of deterministic constraints are assuming conditional independence or set-ting Se and/or Sp to a particular value. Assuming conditional independence of three testsresults in a reduction of the number of parameters to estimate from 15 to 7. Fixing theSp of one test, reduces the number of parameters that need to be estimated by one.Probabilistic constraints in a Bayesian approach are for example specifying a prior dis-tribution for a parameter using expert opinion (Berkvens et al., 2006). In the Bayesiancontext, the impact of probabilistic constraints is not immediately clear. However, toquantify this impact, the e!ective number of estimated parameters (pD) of the model canbe calculated (Spiegelhalter et al., 2002).
Hence, by combining the data (test results) and the external information the trueprevalence and the test characteristics can be estimated (Berkvens et al., 2006). Often,prior knowledge on sensitivity and specificity is incorporated. However, since constancyof test parameters cannot be assumed expert opinions will regularly be in conflict withthe observed data. The Bayesian framework allows making the prior distributions moredi!use (Berkvens et al, 2006).To verify whether the prior information is in conflict with the test results two measuresfor discordance can be used. The Bayesian p-value is based on a Bayesian goodness-of-fittest and the second one uses the deviance information criterion (DIC) (Berkvens et al.,2006; Spiegelhalter et al., 2002).
Page 17


3Materials and Methods
3.1 Study area
The study area includes two districts in Bangladesh (Figure 3.1); the Mymensingh districtand the Dhaka district, where the Government owned Central Cattle Breeding and DairyFarm (CCBDF) is located in Savar. These areas were chosen because they have the highestlivestock population density (> 600/km2) in Bangladesh and because the BangladeshAgricultural University (BAU), which manages the brucellosis diagnostic laboratory, islocated in Mymensingh. The areas are located between latitudes 23#31’ and 25#12’N andlongitudes 90#01’ and 90#47’E and have an average elevation of 10m above sea level.
3.2 Animal husbandry systems
The CCBDF is the largest farm in Bangladesh and supplies milk to Dhaka city. Apartfrom the production of milk its major objectives are to support the national artificialinsemination (AI) program by collecting semen from their proven bulls and to producecrossbred heifers and bulls for distribution to farmers. Sahiwal- and Holstein Friesianbreeds are mainly used for semen production. On average, this farm has been maintaininga herd of about 2500 cattle during the last 25 years. The animal management system isintensive and AI is used solely for reproduction.The cattle management system in the Mymensingh district is a small-scale dairy systemmainly practicing zero grazing with occasional semi-zero and tethering systems. Thefeeding practice is cut-and-carry in this traditional crop-based subsistence agriculturalsystem. Occasionally when there is no crop in the field, animals of separate owners grazetogether. Common supplements are wheat bran, rice polish and oil cake but their supplyto animals is low, irregular and restricted mostly to milking cows. The common breedsare indigenous and their crosses with Holstein Friesian- and Sahiwal breeds. Vaccinationagainst brucellosis has not been initiated in any livestock species of Bangladesh.
19

Figure 3.1: Map of Bangladesh showing the study areas
3.3 Sampling design
The field work was carried out between September 2007 and August 2008 by Dr. A.Rahman (Rahman, pers.comm 2013). In the Mymensingh district a cross-sectional studywas carried out to investigate the seroprevalence of bovine brucellosis. The first step ofthe sampling process was the digitisation of the map of Mymensingh district using Ar-cView Version 3.2 (Environmental Systems Research Institute, Inc. Redlands, California)because there is no livestock databank in Bangladesh. Mymensingh district consist ofseveral Upa-Zillas and 146 unions (sub Upa-Zilla). Out of these 146 unions, 28 were ran-domly selected. Subsequently, one geographical coordinate was randomly selected fromeach selected union and located by a hand held GPS reader. Livestock farmers withina 0.5 km radius of the selected point were informed about the survey (Cringoli et al.,2002). Free anthelmintics and vitamin-mineral premix were supplied to the animals toencourage livestock farmers to participate. All animals of a selected and participatingherd were sampled.In the Dhaka district blood samples were collected from the Government owned CentralCattle Breeding and Dairy Farm (CCBDF). Sampling included all breeding bulls andsystematic random samples of cows (every 10th cow).A questionnaire designed to collect animal and herd level data was administered duringblood sampling of each herd.
Page 20

3.4 Ethics and consent of farm owner
Prior to the collection of blood samples verbal and written consent of farm owners wereobtained. Farm owned animals were used just once for jugular venipuncture. The proce-dure followed established techniques and minimal restraining of the animals was needed;mainly a halter was used. Approval by the ethical committee was not needed becauseit was not an experimental research on animals. This level of intervention has no im-pact on the well-being of the animal. Jugular venipuncture is routinely performed by theveterinarians for the purpose of disease diagnosis, treatment and research.
3.5 Processing of blood samples
From each selected animal about 5-7 ml of blood was collected by jugular venipuncturewith disposable needles and Venoject tubes. The tubes were labelled and transportedto the laboratory on ice (after clotting) within 12 hours of collection. In the laboratorysamples were kept in the refrigerator (2-8#C) and one day after delivery sera were separatedby centrifuging at 6000g for 10 minutes. Each serum was divided into two tubes eachcontaining about 1-1.5ml of serum, labelled to identify the animal and stored at -20#C.One of the two tubes was used for testing and the other was preserved in a serum bank.
3.6 Serological tests
Our case definition is an animal that has been exposed to B. abortus. We attemptedto identify cases using three serological tests, which detect IgM and IgG antibodies.All blood samples were therefore tested in parallel using iELISA, SAT and RBT inthe Medicine Department laboratory of Bangladesh Agricultural University (BAU), My-mensingh, Bangladesh.
3.6.1 Indirect Enzyme-Linked Immunosorbent Assay (iELISA)
Indirect Enzyme-Linked Immunosorbent Assay (iELISA) was performed according toLimet et al. (1988) using B. abortus biotype 1 [Weybridge 99] smooth lipopolysaccha-ride (sLPS) as antigen. Six dilutions, 1/270 to 1/8640, of the positive reference serum(no. 1121) were prepared for the standard curve. Test sera were 1:50 diluted in a bu!er(pH 9.2) consisting of 0.17M sodium chloride, 0.1M glycine, 50mM ethylenediaminete-traacetic acid (EDTA), 0.1% (volume) Tween 80 and destilled water. Fifty microliter ofthe serum dilutions were added to the wells of the microtiter plate in duplicate and theplates were incubated at room temperature for 1 hour. As enzyme conjugated secondaryantibody, a Protein G-horseradish peroxidase (G-HRP) conjugate, was used to detectthe primary antibodies. To visualize the enzyme activity of the horseradish peroxidase acitrate-phosphate bu!er containing 0.4% O-phenylenediamene and 2mM H2O2 was used.A VMax®Microplate reader was used to read the optical density (OD) of the visuallydetectable signal resulting from the enzymatic reaction. Reading was done at 492 nmand 620 nm and the results (OD492 - OD620) were expressed as antibody units (IU/ml)in comparison with the dilutions of the reference serum and the corresponding standardcurve. The cut-o! value for a positive result was defined at di!erent levels; 2, 5, 7.5, 10,12.5, 15 and 20 IU/ml of test serum.
Page 21

3.6.2 Rose Bengal Test (RBT)
The Rose Bengal Test (RBT) was performed according to the standard procedure asdescribed by Alton et al. (1988). The antigen used was a concentrated suspension ofB. abortus biotype 1 [Weybridge 99] (Institute Pourquier, Montpellier, France). Antigen,test sera and control sera were brought to room temperature (22 ± 4 #C) and equal vol-umes (30 µL) of antigen and serum were mixed and rotated for 4 minutes on a glass plate.The result was considered positive when agglutination was noticeable after 4 minutes.
3.6.3 Slow Agglutination Test (SAT)
As described by Garin et al. (1985), the Slow Agglutination Test (SAT) was carriedout with ethylenediaminetetraacetic acid (EDTA). B. abortus biotype 1 [Weybridge 99](Synbiotics Europe, France) was used as antigen. In the first well of a 96-well microtitreplate 168 µL of slow seroagglutination (SAW) bu!er was added and 100 µL in the secondand the third wells. To obtain a 1/6.25 dilution, 32 µL of serum was added in the firstwell. After mixing of serum and diluent, 100 µL from the first well was transferred to thesecond well to obtain a 1/12.5 dilution. Similarly, 100 µL was transferred from the secondto the third well (dilution 1/25) and 100 µL was discarded from the third. To obtainthe serial serum dilutions of 1/12.5; 1/25 and 1/50, 100 µL of standardized SAW antigenwas added in each well. The microtitre plates were agitated and incubated for 20-24hours at 37#C. Reading of the results was done on the basis of degree of agglutinationand expressed in international units (IU). As prescribed by the OIE, any serum with anantibody titre greater than or equal to 30 IU/ml was considered positive (OIE, 2009).
3.7 Statistical analysis
To estimate the prevalence, sensitivity and specificity of the three tests, a Bayesian anal-ysis framework was used in R 2.15.2 (R Foundation and Statistical Computing, 2012) andWinBUGS 1.4 (Spiegelhalter et al., 2003).As explained in the literature review, the data resulting from multiple tests in the ab-sence of confirmatory testing by a gold standard test and without external constraintsare insu"cient to estimate all of the parameters (Johnson et al., 2000). Converting theapparent prevalence (sero-prevalence) into the true prevalence always requires one to solvea system of overparametrized equations (Bervens et al., 2006). Two types of restrictions,deterministic- and probabilistic constraints, can be imposed on the parameters to be ableto estimate the true prevalence and test characteristics. This requires the input of exter-nal (prior, independent) information (Berkvens et al., 2006).Two deterministic assumptions are regularly made in literature, namely that the testsused are conditionally independent and/or that the test characteristics are constant overpopulations (Hui and Walter, 1980). A probabilistic constraint in a Bayesian approach is,for example, specifying a prior distribution for a parameter using expert opinion (Berkvenset al., 2006). Often, test results (observed data) are combined with prior knowledge onsensitivity and specificity. However, since constancy of test parameters can not be as-sumed expert opinions will regularly be in conflict with the observed data. The Bayesianframework allows making the prior distributions more di!use (Berkvens et al., 2006).
Page 22

3.7.1 Modeling approaches
Di!erent theoretical frameworks have been developed over the years; we examined fourmodeling approaches. All models were run with a burn-in period of 10,000 iterations andestimates were based on a further 10,000 iterations using three chains.
3.7.1.1 The Hui and Walter model
Hui and Walter (1980) developed a system based on two diagnostic tests applied in twopopulations with the assumption of conditional independence between tests and constantsensitivity and specificity over the two populations. This allows estimation of the trueprevalence and test characteristics without explicit external information. Estimation ofthese parameter could be done both deterministically and probabilistically by using threetest combinations (iELISA/RBT, iELISA/SAT and RBT/SAT) in the two localities.
3.7.1.1.1 Deterministic estimation The estimation of the parameters was donein R by means of the model shown in appendix 1. The set of equations (shown be-low) used in the deterministic estimation are adapted from Hui and Walter (1980) anduse standard notation [prevalence in population i = p(D+
i ) (with i # {1, 2} for thetwo populations); sensitivity of test j = p(T+
j |D+); specificity of test j = p(T!j |D!);
{p111, p110, p101, p100, p211, p210, p201, p200} are the respective proportions p1T+1 T+
2, p1T+
1 T!2,
p1T!1 T+
2and p1T!
1 T!2in the first population and p2T+
1 T+2, p2T+
1 T!2, p2T!
1 T+2and p2T!
1 T!2in the
second population; p... represents summation]
p(D+1 ) =
1
2+
p11.(p1.1 ! p2.1) + p1.1(p11. ! p21.) + p211 ! p1112D
p(D+2 ) =
1
2+
p21.(p1.1 ! p2.1) + p2.1(p11. ! p21.) + p211 ! p1112D
p(T+1 |D+) = 1! p1.0p20. ! p10.p2.0 + p100 ! p200 +D
2(p2.1 ! p1.1)
p(T!1 |D!) = 1! p11.p2.1 ! p1.1p21. + p211 ! p111 +D
2(p2.1 ! p1.1)
p(T+2 |D+) = 1! p2.0p10. ! p20.p1.0 + p100 ! p200 +D
2(p21. ! p11.)
p(T!2 |D!) = 1! p21.p1.1 ! p2.1p11. + p211 ! p111 +D
2(p21. ! p11.)
with
D = ±!
(p11.p2.1 ! p21.p1.1 + p111 ! p211)2 ! 4(p11. ! p21.)(p111p2.1 ! p211p1.1)
3.7.1.1.2 Probabilistic estimation Estimation was done by means of the Win-BUGS model shown in appendix 2, which gives the example of the iELISA/RBT com-bination. The posterior mean and the 95% credibility interval (CI) are reported. Thegeneral equation is:
pi(tj) = pri"
j
#11!tj ! (!1)tjsej
$+ (1! pri)
"
j
#1tj ! (!1)1!tjspj
$
Page 23

with
i # {1, 2} (locality); t # {0, 1} (-ve, +ve); j # {1, 2} (test)
pr = prevalence; se = sensitivity; sp = specificity
3.7.1.2 Conditional independence
This approach uses the conditional independence hypothesis as prior information. Thevariables that need to be estimated under this assumption of conditional independenceare the prevalence and three pairs of sensitivity and specificity, which makes a total ofseven parameters per locality. The maximum number of estimable parameters is alsoseven, which means that all parameters can be estimated without additional externalinformation. In contrast to the Hui and Walter model, this approach allows for di!erentsensitivity and specificity estimates per locality. The WinBUGS code (for Mymensinghwith an iELISA cut-of of 7.5 IU/ml) to estimate this model is given in appendix 3. Theposterior mean and the 95% credibility interval (CI) are reported. The general equationis:
p(tj) = pr"
j
#11!tj ! (!1)tjsej
$+ (1! pr)
"
j
#1tj ! (!1)1!tjspj
$
with
t # {0, 1} (-ve, +ve); j # {1, 2, 3} (test)
pr = prevalence; se = sensitivity; sp = specificity
3.7.1.3 Conditional dependence
Since iELISA, RBT and SAT are based on similar biological events, namely the detectionof serum antibody response, the tests might be considered dependent on each other giventhe true disease status of subjects (Rahman, unpublished). Dependency of tests substan-tially changes the theoretical values of Se and Sp of multiple combined tests comparedwith the values expected when tests are conditionally independent (Gardner et al., 2000).Therefore, estimation procedures should adjust for these dependencies among tests (Den-dukuri and Joseph, 2001).As discussed in the literature review, the full model assuming conditional dependencehas the implicit characteristic of being overparametrized. When conditional dependenceexists between the tests, 15 parameters need to be estimated, which exceeds the amountthat can be estimated. Because more parameters must be estimated than the data permit,estimation of the true disease prevalence and test characteristics becomes either impossi-ble or external (prior) information must be added by means of imposing constraints onthe parameters (Berkvens et al., 2006).
3.7.1.3.1 Conditional dependence - Covariance scheme A first approach usescovariances to model the conditional dependence. This mathematical model, proposed byGardner et al. (2000), calculates the probabilities of the di!erent outcomes in function oftest sensitivities, specificities and covariances (as a measure of dependence). To overcomethe problem of overparametrisation it is possible to combine prior information on these
Page 24

parameters with the test results in a Bayesian manner. The WinBUGS code for the caseof Mymensingh (with iELISA cut-o! of 7.5 IU/ml) is shown in appendix 4. The modelgave rise to problems when setting up; the initial values cannot be generated, but mustbe supplied to ensure probabilities between 0 and 1. Therefore we generated and loadedthe three lists of initial values shown in appendix 4.The posterior mean and 95% credibility intervals (CI) are reported. The general equationis:
p(tI) = pr ·
%
&'
J |#J $=1
!J ·"
i
#J(i)
(
)+ (1! pr) ·
%
&'
J |#J $=1
!"J ·
"
i
$J(i)
(
)
with
I = {1, 2, 3}; $i # I ti # {0, 1} (-ve, +ve); J # P(I)
!J = covse...; !"J = covsp...; !! = !"
! = 1
#(i) =
*!(!1)ti $i # Jti · sei + (1! ti) · (1! sei) $i /# J
$(i) =
*!(!1)ti $i # J(1! ti) · spi + ti · (1! spi) $i /# J
pr = prevalence; se = sensitivity; sp = specificity
Which gives the following test result probabilities:
P (T+1 T+
2 T+3 ) = pr[!1!2!3 + !1"23 + !2"13 + !3"12 + "123]+
(1! pr)[(1! #1)(1! #2)(1! #3) + (1! #1)"!23 + (1! #2)"
!13 + (1! #3)"
!12 ! "!
123]
P (T+1 T+
2 T"3 ) = pr[!1!2(1! !3)! !1"23 ! !2"13 + (1! !3)"12 ! "123]+
(1! pr)[(1! #1)(1! #2)#3 ! (1! #1)"!23 ! (1! #2)"
!13 + #3"
!12 + "!
123]
P (T+1 T"
2 T+3 ) = pr[!1(1! !2)!3 ! !1"23 + (1! !2)"13 ! !3"12 ! "123]+
(1! pr)[(1! #1)#2(1! #3)! (1! #1)"!23 + #2"
!13 ! (1! #3)"
!12 + "!
123]
P (T+1 T"
2 T"3 ) = pr[!1(1! !2)(1! !3) + !1"23 ! (1! !2)"13 ! (1! !3)"12 + "123]+
(1! pr)[(1! #1)#2#3 + (1! #1)"!23 ! #2"
!13 ! #3"
!12 ! "!
123]
P (T"1 T+
2 T+3 ) = pr[(1! !1)!2!3 + (1! !1)"23 ! !2"13 ! !3"12 ! "123]+
(1! pr)[#1(1! #2)(1! #3) + #1"!23 ! (1! #2)"
!13 ! (1! #3)"
!12 + "!
123]
P (T"1 T+
2 T"3 ) = pr[(1! !1)!2(1! !3)! (1! !1)"23 + !2"13 ! (1! !3)"12 + "123]+
(1! pr)[#1(1! #2)#3 ! #1"!23 + (1! #2)"
!13 ! #3"
!12 ! "!
123]
P (T"1 T"
2 T+3 ) = pr[(1! !1)(1! !2)!3 ! (1! !1)"23 ! (1! !2)"13 + !3"12 + "123]+
(1! pr)[#1#2(1! #3)! #1"!23 ! #2"
!13 + (1! #3)"
!12 ! "!
123]
P (T"1 T"
2 T"3 ) = pr[(1! !1)(1! !2)(1! !3) + (1! !1)"23 + (1! !2)"13 + (1! !3)"12 ! "123]+
(1! pr)[#1#2#3 + #1"!23 + #2"
!13 + #3"
!12 + "!
123]
Page 25

with
pr = prevalence; "i = Sei, %i = Spi; &ijk = covSeiSejSek ; &"ijk = covSpiSpjSpk
3.7.1.3.2 Conditional dependence - Berkvens et al. scheme Because the co-variances cannot be related to real-life situations, the prior distributions for the covari-ances are quite di"cult to elicit from expert opinion (Berkvens et al., 2006). Therefore,Berkvens et al. (2006) proposed an alternative parametrization for the full model. Incertain cases it could be easier to elicit information on the conditional performance of onetest given the result of another test.For example, when two test are applied on the same animal, a question such as ”What isthe probability that a subject tests positively in test 2, given that it is diseased and thatis has tested positively in test 1?” could be easier to answer by experts. This approachtherefore uses the conditional probabilities shown in Table 3.1 to model the conditionaldependence.
Table 3.1: Conditional probabilities
prevalence P (D+) '1Se1 P (T+
1 |D+) '2Sp1 P(T!
1 |D!) '3P(T+
2 |D+ " T+1 ) '4
P(T+2 |D+ " T!
1 ) '5P(T!
2 |D! " T!1 ) '6
P(T!2 |D! " T+
1 ) '7P(T+
3 |D+ " T+1 " T+
2 ) '8P(T+
3 |D+ " T+1 " T!
2 ) '9P(T+
3 |D+ " T!1 " T+
2 ) '10P(T+
3 |D+ " T!1 " T!
2 ) '11P(T!
3 |D! " T!1 " T!
2 ) '12P(T!
3 |D! " T!1 " T+
2 ) '13P(T!
3 |D! " T+1 " T!
2 ) '14P(T!
3 |D! " T+1 " T+
2 ) '15
The WinBUGS code for the Mymensingh case (with iELISA cut-o! of 7.5 IU/ml) isshown in appendix 5. The posterior mean and the 95% credibility intervals (CI) arereported. The general equation for this parametrization is:
p(tI) = pr ·"
i
+
,(1! ti)! (!1)ti · p
%
&T+i
------D+
i!1.
i"=1|i>1
Tti"i"
(
)
/
0
+ (1! pr) ·"
i
+
,ti + (!1)ti · p
%
&T!i
------D!
i!1.
i"=1|i>t
Tti"i"
(
)
/
0
Page 26

with
I = {1, 2, 3}; $i, i" # I ti, ti" # {0, 1} (-ve, +ve);
D+ = true case; D! = true non-case;
T+i , T!
i = positive, negative result of test i;
pr = prevalence
Which gives the following test result probabilities:
P (T+1 T+
2 T+3 ) = '1'2'4'8 + (1! '1)(1! '3)(1! '7)(1! '15)
P (T+1 T+
2 T!3 ) = '1'2'4(1! '8) + (1! '1)(1! '3)(1! '7)'15
P (T+1 T!
2 T+3 ) = '1'2(1! '4)'9 + (1! '1)(1! '3)'7(1! '14)
P (T+1 T!
2 T!3 ) = '1'2(1! '4)(1! '9) + (1! '1)(1! '3)'7'14
P (T!1 T+
2 T+3 ) = '1(1! '2)'5'10 + (1! '1)'3(1! '6)(1! '13)
P (T!1 T+
2 T!3 ) = '1(1! '2)'5(1! '10) + (1! '1)'3(1! '6)'13
P (T!1 T!
2 T+3 ) = '1(1! '2)(1! '5)'11 + (1! '1)'3'6(1! '12)
P (T!1 T!
2 T!3 ) = '1(1! '2)(1! '5)(1! '11) + (1! '1)'3'6'12
The following relationship exists between covariance and conditional probabilities:
&ij = cov#T1, T2
--D+$=
1Ni=1 (T
i1 ! Se1) (T i
2 ! Se2)
N= p++ ! Se1 % Se2
=2P#T+2
--D+ " T+1
$! Se2
3% Se1
= (2 % (1! (2)% ((4 ! (5)
&"ij = cov
#T1, T2
--D! $ =1N
i=1 [(1! T i1)! Sp1] [(1! T i
2)! Sp2]
N= p!! ! Sp1 % Sp2
=2P#T!2
--D! " T!1
$! Sp2
3% Sp1
= (3 % (1! (3)% ((6 ! (7)
with
T i = 0, 1(!ve,+ve); p=observed proportion of (non-)infected animals that are positive(negative) in both tests
3.7.2 Meta analysis
As discussed above, when conditional dependence exists between the tests, 15 parametersneed to be estimated, which exceeds the amount that can be estimated. Due to thisoverparametrization, estimation of the true disease prevalence and test characteristicsbecomes either impossible or external (prior) information must be added by means ofimposing constraints on the parameters (Berkvens et al., 2006).
Page 27

The first two models were constrained by the assumptions that the tests used are condi-tionally independent and/or that the test characteristics are constant over populations.The constraint imposed on the conditionally dependent models (3 and 4) was the useof external (prior) information. This external (prior) information on sensitivities andspecificities was generated by means of a meta-analysis based on data from 11 di!erentpublications. The calculation of prior distributions from this information was carried outin Stata MP/12.1 (StataCorp, 2011).
The prior distributions used are in the form of beta distributions, Beta(a,b), with athe lower limit and b the upper limit. We decided not to specify the prior distributionsin a uniform syntax (dunif) with an interval from min to max because this uniform dis-tribution only samples within the 95% confidence interval. Even though this distributionyields a slightly better model fit, we did not use it because the beta distribution takesthe full scope of the distribution into account and is thus more correct. The beta distri-bution samples over the whole [0,1] range, including the 2,5% tails. For conversion of theprior distributions into beta distributions the following equation was used in R 2.15.2 (RFoundation and Statistical Computing, 2012):
m ="! 1
" + % ! 2
% ="(1!m)! 1
m+ 2
with
m = mode; " = alpha; % = beta
3.7.3 Bayesian p-value, PD and DIC
To verify whether the constraints (external prior information) are in conflict with thetest results two measures for discordance were used. The Bayesian p-value (Bayesp) isbased on a Bayesian goodness-of-fit test and the second one uses the deviance informationcriterion (DIC). The e!ective number of estimated parameters (pD) of every model iscalculated to quantify the impact of the constraints (Berkvens et al., 2006; Spiegelhalteret al., 2002).
1. The bayesian p-valueThe Bayesian p-value expresses the fit of the assumed model to the data. Werandomly generated observations (pseudo-data) using the di!erent models and werepeatedly sampled these pseudo observations. The deviance of the sampled pseudo-data (devr) with the deviance of the observed data (devo) is represented by ) =devo ! devr. When ) is a positive value, the fit of the model to the observed data isworse than the fit of the model to the pseudo-data generated under the same model(Berkvens et al., 2006).) can be calculated at each iteration based on the current sampled value of theparameter estimates 'j(j = 1, ....q) yielding a chain )1, ......)T . The posterior esti-mate of P () > 0) is called the Bayesian p-value and is elicited from the average
Page 28

1T
1Tt=1 I() > 0), whereby I(x) = 1 when x & 0 and 0 otherwise. Thus, when the
first part of ) (=deviance of observations) (almost) always exceeds the second part(=deviance sampled values) so that I() > 0) (almost) always takes the value 1, wehave a (very) poorly fitting model (Berkvens et al., 2006).First we observed the Bayesian p-value in the unconstrained model. Thereafter wemade sure this value did not significantly increase when constraints were added tothe model, which would indicate a poor fit of the prior information with the data.In all models, except for the covariance model, we used log functions to calculatedevr and devo and consequently the Bayesian p-value. In this case the Bayesianp-value tends to zero if there is a good model fit and to one if the fit is poor. Incontrast, in the covariance model we used power model functions for devr and devo,which means there is a good model fit when the Bayesian P-value is between 0.30and 0.70.
2. The e!ective number of estimable parameters (pD)Only when the pD-values are smaller or equal to 2h ! 1 there is hope that theprevalence of the disease can be estimated (Berkvens et al., 2006). When no priorconstraints are added pD typically starts with a negative value in WinBUGS. Thevalue of pD increases when more and more constraints are added until a maximumvalue is reached. We calculated these optimum values for Mymensingh and the gov-ernment farm in R. The model becomes over-specified when one increases the (wellfitting) constraints even more, resulting in a reduction of the number of parametersthat are to be estimated. This is reflected by decreasing values of pD until eventuallythe prior information is so detailed that all parameters are fully specified. At thispoint pD becomes zero (Berkvens et al., 2006).
3. Deviance Information Criterion (DIC)Also the optimum values of DIC are calculated in R. Models with a high valuefor DIC indicate a bad model; either the model (likelihood) part is badly specifiedand/or the prior distributions are not compatible with the data (Berkvens et al.,2006).
Page 29


4Results
4.1 Meta analysis
External prior information was generated by means of a meta-analysis based on data from11 di!erent publications. The data used to calculate the prior values for the di!erenttests are shown in Table 4.1, Table 4.2 and Table 4.3. The meta-analysis yielded theprior distributions shown in Table 4.4 for the respective test characteristics. The priordistributions for sensitivity and specificity were then converted into uniform distributions(Beta(1,1)) truncated on the interval [a,b], with the lower limit a and the upper limit b.These parameters are listed in Table 4.5.
Table 4.1: iELISA data for the meta-analysis
Source Se (95% CI) Sp (95% CI) tp fp fn tn Cut-o! value
Van Aert et al., 1984 (S 19) 71.4 (41.9, 91.6) 100 (99.5, 100)* 10 0 4 677 3x OD of the blankVan Aert et al., 1984 (S 2308) 70.6 (44.0, 89.7) 100 (99.5, 100)* 12 0 5 677 3x OD of the blankDohoo et al., 1986 96.6 (92.6, 98.7) 99.0 (98.3, 99.5) 168 11 6 1117 OD &0.22Dohoo et al., 1986 94.8 (90.4, 97.6) 99.5 (98.8, 99.8) 165 6 9 1122 OD &0.26Dohoo et al., 1986 94.3 (89.7, 97.2) 99.8 (99.4, 99.9) 164 2 10 1126 OD &0.30Dohoo et al., 1986 92.5 (87.5, 96.0) 99.9 (99.5, 99.9) 161 1 13 1127 OD &0.34Saegerman et al., 2004 100 (69.2, 100)* 97.1 (95.8, 98.1) 10 27 0 909 OD & 0.25 (2.5 IU/ml)Abernethy et al., 2012 67.2 (59.5, 74.4) 100 (99.9, 100)* 109 0 53 2663 "Uzal et al., 1996 98.9 (96.1, 99.9) 98.8 (96.4, 99.7) 182 3 2 240 31% of positive serumSamartino et al., 1999 98.2 (97.2, 98.9) 98.6 (97.1, 99.4) 982 7 18 493 40% of positive serum
! = 100 x (OD450 value of the sample - OD450 value of the negative control)/(mean OD450value of the positive control - OD450 value of the negative control)120%
*97.5% CI; tp = true positives; fp = false positives; fn = false negatives; tn = true negatives
31

Table 4.2: RBT data for the meta-analysis
Source Se (95% CI) Sp (95% CI) tp fp fn tn
Van Aert et al., 1984 (S 19) 35.7 (12.8, 64.9) 100 (99.5, 100)* 5 0 9 677Van Aert et al., 1984 (S 2308) 76.5 (50.1, 93.2) 100 (99.5, 100)* 13 0 4 677Abernethy et al., 2012 64.2 (56.3, 71.6) 100 (99.9, 100)* 104 0 58 2663Samartino et al., 1999 96.1 (94.7, 97.2) 97.8 (96.1, 98.9) 961 11 39 489Dajer et al., 1999 96.2 (94.1, 97.7) 68.8 (64.5, 72.9) 481 153 9 337Muma et al., 2007b 92.6 (85.4, 96.9) 80.0 (63.1, 91.6) 88 7 7 28Mainer Jaime et al., 2005 100 (98.1, 100)* 86.4 (79.1, 91.9) 189 17 0 108
*97.5% CI; tp = true positives; fp = false positives; fn = false negatives; tn = true negatives
Table 4.3: SAT data for the meta-analysis
Source Se (95% CI) Sp (95% CI) tp fp fn tn Cut-o! value
Van Aert et al., 1984 35.7 (12.8, 64.9) 100 (99.5, 100)* 4 0 10 677 30 IU/mlLord et al., 1989 100 (93.6, 100)* 100 (96.4, 100)* 56 0 0 100 100 IU/mlAbernethy et al., 2012 75.9 (68.6, 82.3) 98.6 (98.0, 98.9) 123 38 39 2624 31 IU/mlStemshorn et al., 1985 68.9 (61.2, 75.8) 99.5 (98.6, 99.8) 115 4 52 726 60 IU/ml
*97.5% CI; tp=true positives; fp=false positives; fn=false negatives; tn=true negatives
Table 4.4: Summary values of prior parameters
Sensitivity SpecificityTest mean 95% CI mean 95% CI
iELISA 93.9 86.9 - 97.2 99.8 99.1 - 99.9RBT 91.0 70.6 - 97.7 99.6 84.3 - 99.9SAT 82.6 27.8 - 98.3 99.7 97.4 - 99.9
Table 4.5: Summary values of prior beta distribution parameters
Sensitivity SpecificityTest " % " %
iELISA 85.00 6.4867 750.0 2.6544RBT 18.80 2.7583 22.6 1.0837SAT 3.45 1.5142 190.0 1.6483
4.2 Descriptive statistics
A total of 1360 cattle, of which 1020 in the Mymensingh district and 340 at the govern-ment farm, were subjected to the three serological tests. About 69% of the cattle wereindigenous and 70% female. The age ranged from 0.03 to 17 years with an average of4.1±0.09 years (mean ± standard error). The mean body weight of cattle was 126.2±3.5
Page 32

kg with a median of 80 kg. In the Mymensingh district, the herd size ranged from 1 to13 with a median of 3 animals. Only 12 herds had more than 10 animals and about 62%of the herds consisted of 1-3 cattle. From Mymensingh, 1020 sera samples were collectedand 340 from the government owned dairy farm.
The cross classified test results of the three serological tests with di!erent iELISA cut-o!s are shown in Table 4.6. With the traditionally used iELISA cut-o! of 2 IU/ml, a totalof 2 (0.2%) and 51 (15.6%) cattle were positive for all three tests and 863 (84.6%) and 217(63.8%) were negative for all three tests respectively in Mymensingh and the governmentdairy farm. The number of cattle testing positive in at least one serological test was 15.4%(95% CI: 13.2-17.8) and 36.2% (95% CI: 31.1-41.5) in Mymensingh and the governmentdairy farm respectively. In the Mymensingh district about 31.9% (116/363) of the herdswere serologically positive in at least one of the three tests. The median and range ofwithin herd prevalence in larger herds (> 10) were 19.1% and 0.0-58.3% respectively.
The apparent prevalence in Mymensingh and at the government dairy farm was 14.8%(95% CI: 12.7-17.1) and 33.5% (95% CI: 28.5-38.8) respectively based on iELISA. Based onRBT the apparent prevalence was 0.9% (0.4-1.7) and 18.2% (14.3-22.8) and SAT yieldedthe values 1.3% (0.7-2.2) and 19.7% (15.6-24.3) for Mymensingh and the Governmentfarm respectively.
Especially the high numbers of positive animals for the iELISA alone, 137 and 53 inthe Mymensingh district and at the government farm respectively, is notable. When weshifted the iELISA cut-o! to 5 IU/ml and 7.5 IU/ml this high number almost completelydisappeared in the Mymensingh area. At the government farm this number droppedconsiderably when we increased the cut-o! to 5 IU/ml but only showed low numbers froma cut-o! of 12.5 IU/ml onwards.Increasing the iELISA cut-o! resulted in lower apparent prevalences of 0.9% (0.4-1.7) and19.4% (15.3-24.0) for a 5 IU/ml cut-o! and 0.4% (0.1-1.0) and 17.6% (13.7-22.1) basedon a 7.5 IU/ml iELISA cut-o! for Mymensingh and the Government farm respectively.The latter values are comparable to the apparent prevalences found with RBT and SAT.
Table 4.6: Cross-classified test results for brucellosis in cattle in Mymensingh and thegovernment dairy farm based on iELISA, RBT and SAT with di!erentiELISA cut-o! values
iELISA cut-o!: 2 IU/ml 5 IU/ml 7.5 IU/ml 10 IU/ml 12.5 IU/ml 15 IU/ml 20 IU/ml
iELISA RBT SAT Mym Govt Mym Govt Mym Govt Govt Govt Govt Govt
1 1 1 2 51 1 47 1 45 45 44 44 401 1 0 6 3 1 2 0 2 2 2 2 21 0 1 6 7 2 6 1 6 6 5 4 41 0 0 137 53 5 11 2 7 4 2 1 10 1 1 0 8 1 12 1 14 14 15 15 190 1 0 1 0 6 1 7 1 1 1 1 10 0 1 5 1 9 2 10 2 2 3 4 40 0 0 863 217 995 259 998 263 266 268 269 269
Total 1020 340 1020 340 1020 340 340 340 340 340
iELISA = indirect Enzyme-Linked ImmunoSorbent Assay; RBT = Rose Bengal Test;SAT = Slow Agglutination Test; 1 = positive test result; 0 = negative test result;
Mym = Mymensingh; Govt = Government farm
Page 33

4.3 Calculations of the di!erent models
4.3.1 Hui and Walter Model
The Hui and Walter model uses a system based on two diagnostic tests applied in twopopulations with the assumption of conditional independence between tests and constantsensitivity and specificity over the two populations. In our case, this resulted in threetest combinations (iELISA/RBT, iELISA/SAT and RBT/SAT) in the two localities. Togive an example of the calculations used in the Hui and Walter Model, we explain thecombination of the two tests, iELISA and RBT. Table 4.7 shows the cross-classified testresults and corresponding frequencies of iELISA (with a cut-o! value of 7.5 IU/ml) andRBT. These frequencies were used as input in the deterministic Hui and Walter modelshown in appendix 1. The test results were used as input in the probabilistic Hui andWalter model shown in appendix 2.
Table 4.7: Cross-classified test results in Mymensingh and at the government dairyfarm based on iELISA (with a cut-o! value of 7.5 IU/ml) and RBT
ELISA RBT Mymensingh Govt. farmnr freq nr freq
1 1 1 0.00098 47 0.138241 0 3 0.00294 13 0.038240 1 8 0.00784 15 0.044120 0 1008 0.98824 265 0.77941
4.3.2 Independent model
As discussed before, all parameters could be estimated without additional external priorinformation in this model. In contrast to the Hui and Walter model, this approachallows for di!erent sensitivity and specificity estimates per locality. The WinBUGS code(for Mymensingh with an iELISA cut-o! of 7.5 IU/ml) for estimation of the di!erentparameters is given in appendix 3.
4.3.3 Conditional dependence - Covariance scheme
The covariance model is shown in appendix 4 for Mymensingh with a 7.5 IU/ml iELISAcut-o!. First, we ran the model without any constraints, thereafter, we included all theprior distributions generated by the meta-analysis. By varying the inclusion of priordistributions we analyzed the e!ect of the prior belief on the estimation of the prevalenceand test characteristics. Since constancy of test parameters cannot be assumed expertopinions is regularly in conflict with the observed data. Indeed, when we used all sixprior beta distributions for the sensitivities and specificities, the model fit was poor.Excluding the narrow priors for the specificity of iELISA (dbeta(750, 2.6544)) and SAT(dbeta(190,1.6483)) resulted in a better model fit.The prior distributions (elicited from the meta-analysis) used in the covariance model arelisted below; where pr represents the prevalence and se[1] - sp[1], se[2] - sp[2] and se[3] -sp[3] represent the sensitivity and specificity of iELISA, RBT and SAT respectively.
Page 34

Priorspr ' dbeta(1,1)I(0,0.5)se[1] ' dbeta(85,6.4867)se[2] ' dbeta(18.8,2.7583)se[3] ' dbeta(3.45,1.5142)sp[1] ' dbeta(1,1)sp[2] ' dbeta(22.6,1.0837)sp[3] ' dbeta(1,1)
Conditional dependence is considered significant if zero is excluded from the covariance95% credibility interval. With the majority of the iELISA cut-o!s the model showed de-pendence (at a 95% probability) between the specificities of iELISA and SAT (covarianceb13) and/or RBT and SAT (covariance b23) both in the Mymensingh district and atthe government farm. Only in Mymensingh, at an iELISA cut-o! of 5 IU/ml, the modelshowed additional dependence between the specificities of iELISA and RBT (covarianceb12). Because the sensitivities and some of the specificities showed no dependence themodel (appendix 4) could be simplified. When for example only specificity conditionaldependence existed between iELISA and SAT (covariance b13) and RBT and SAT (co-variance b23) respectively, the model could be simplified as shown in the listing below[where p[i] are the test result probabilities; p[1] = P (T+
1 T+2 T+
3 ); p[8] = P (T!1 T!
2 T!3 ); pr =
prevalence; aijk = &ijk = covSeiSejSek ; bijk = &"ijk = covSpiSpjSpk ]:
p[1] = pr*(se[1]*se[2]*se[3])+(1-pr)*((1-sp[1])*(1-sp[2])*(1-sp[3])+(1-sp[1])*b23+(1-sp[2])*b13)
p[2] = pr*(se[1]*se[2]*(1-se[3]))+(1-pr)*((1-sp[1])*(1-sp[2])*sp[3]-(1-sp[1])*b23-(1-sp[2])*b13)
p[3] = pr*(se[1]*(1-se[2])*se[3])+(1-pr)*((1-sp[1])*sp[2]*(1-sp[3])-(1-sp[1])*b23+sp[2]*b13)
p[4] = pr*(se[1]*(1-se[2])*(1-se[3]))+(1-pr)*((1-sp[1])*sp[2]*sp[3]+(1-sp[1])*b23-sp[2]*b13)
p[5] = pr*((1-se[1])*se[2]*se[3])+(1-pr)*(sp[1]*(1-sp[2])*(1-sp[3])+sp[1]*b23-(1-sp[2])*b13)
p[6] = pr*((1-se[1])*se[2]*(1-se[3]))+(1-pr)*(sp[1]*(1-sp[2])*sp[3]-sp[1]*b23+(1-sp[2])*b13)
p[7] = pr*((1-se[1])*(1-se[2])*se[3])+(1-pr)*(sp[1]*sp[2]*(1-sp[3])-sp[1]*b23-sp[2]*b13)
p[8] = pr*((1-se[1])*(1-se[2])*(1-se[3]))+(1-pr)*(sp[1]*sp[2]*sp[3]+sp[1]*b23+sp[2]*b13)
4.3.4 Conditional dependence - Berkvens et al. scheme
Because the covariance model showed no dependencies between the test sensitivities, allthree prior test sensitivity distributions could be used. This means, in terms of the pa-rameters in Table 3.1, '4 and '5 become equal, just like '8, '9, '10 and '11. Again theprior beta distributions of the iELISA- and SAT specificity were not used and remaineduniform distributions (Beta (1,1)). The specificity of RBT could be used in most cases(except in Mymengingh with iELISA 5 IU/ml cut-o!) because there was no dependencebetween the iELISA and RBT specificities and '6 and '7 thus become equal. However,due to the dependencies (discussed above) between the specificities of iELISA - SAT andRBT - SAT, '12, '13, '14 and '15 were not equal. Therefore, the only possible option for in-cluding prior beta distributions in the conditional dependence model (shown in appendix
Page 35

5) in both areas was the list below (where p[i] represent the conditional probabilities 'i).However, in Mymensingh using an iELISA cut-o! of 5 IU/ml, '6 and '7 were not equaland remained uniform distributions (Beta 1,1) because the model showed additional de-pendence between the specificities of iELISA and RBT.
Priorsp[1] ' dbeta(1,1)I(0,0.5)p[2] ' dbeta(85, 6.4867)p[3] ' dbeta(1,1)p[4] ' dbeta(18.8, 2.7583)p[5] < ! p[4]p[6] ' dbeta(22.6, 1.0837)p[7] < ! p[6]p[8] ' dbeta(3.45,1.5142)p[9] < ! p[8]p[10] < ! p[8]p[11] < ! p[8]p[12] ' dbeta(1,1)p[13] ' dbeta(1,1)p[14] ' dbeta(1,1)p[15] ' dbeta(1,1)
4.4 Overall results of the di!erent models
Table 4.8, Table 4.9 and Table 4.10 show the posterior means together with the 95%credibility intervals of the prevalence and diagnostic test characteristics of all three tests,at di!erent iELISA cut-o!s, calculated by the four di!erent models.Table 4.11 shows the estimated parameter values at the government farm using the modelbased on conditional dependence - covariance parametrisation with increasing iELISAcut-o!.
Page 36

Table 4.8: Estimated parameter values using an iELISA cut-o! at 2 units
iELISA RBT SATModel prev se sp se sp se sp
HWER,d 0.0133 0.8703 0.8617 0.6781 1.0000HWES,d 0.0122 0.8783 0.8602 0.7316 0.9954HWRS,d 0.0021 0.9207 0.9931 0.9814 0.9893HWER,p 0.0135 0.8716 0.8608 0.6809 0.9982
(0.0056 – 0.0250) (0.7820 – 0.9429) (0.8374 – 0.8826) (0.5321 – 0.8663) (0.9941 – 0.9999)HWES,p 0.0130 0.8665 0.8598 0.7267 0.9945
(0.0047 – 0.0252) (0.7679 – 0.9476) (0.8369 – 0.8816) (0.5663 – 0.9125) (0.9876 – 0.9992)HWRS,p 0.0034 0.9074 0.9926 0.9590 0.9885
(0.0006 – 0.0083) (0.8091 – 0.9842) (0.9867 – 0.9969) (0.8855 – 0.9980) (0.9811 – 0.9943)IT 0.0372 0.8669 0.8791 0.2980 0.9980 0.2832 0.9939
(0.0114 – 0.1121) (0.6142 – 0.9954) (0.8479 – 0.9395) (0.0684 – 0.6635) (0.9938 – 0.9999) (0.0714 – 0.5904) (0.9869 – 0.9989)DT1 0.0100 0.9325 0.8584 0.8628 0.9977 0.4319 0.9889
(0.0041 – 0.0186) (0.8759 – 0.9732) (0.8356 – 0.8792) (0.6849 – 0.9720) (0.9934 – 0.9999) (0.1833 – 0.7205) (0.9814 – 0.9947)DT2 0.0104 0.9307 0.8588 0.8656 0.9981 0.4140 0.9871
(0.0044 – 0.01871) (0.8720 – 0.9726) (0.8369 – 0.8796) (0.6911 – 0.9728) (0.9941 – 0.9999) (0.1681 – 0.6927) (0.9792 - 0.9934)
iELISA RBT SATModel prev se sp se sp se sp
HWER,d 0.2691 0.8703 0.8617 0.6781 1.0000HWES,d 0.2648 0.8783 0.8602 0.7316 0.9954HWRS,d 0.1920 0.9207 0.9931 0.9814 0.9893HWER,p 0.2670 0.8716 0.8608 0.6809 0.9982
(0.1969 – 0.3386) (0.7820 – 0.9429) (0.8374 – 0.8826) (0.5321 – 0.8663) (0.9941 – 0.9999)HWES,p 0.2668 0.8665 0.8598 0.7267 0.9945
(0.1981 – 0.3389) (0.7679 – 0.9476) (0.8369 – 0.8816) (0.5663 – 0.9125) (0.9876 – 0.9992)HWRS,p 0.1947 0.9074 0.9926 0.9590 0.9885
(0.1530 – 0.2400) (0.8091 – 0.9842) (0.9867 – 9969) (0.8855 – 0.9980) (0.9811 – 0.9943)IT 0.2055 0.8658 0.8010 0.8803 0.9952 0.9412 0.9928
(0.1639 – 0.2504) (0.7771 – 0.9356) (0.7512 – 8469) (0.7900 – 0.9510) (0.9826 – 0.9999) (0.8689 – 0.9878) (0.9763 – 0.9998)DT1 0.1942 0.9250 0.8015 0.8825 0.9826 0.9310 0.9790
(0.1488 – 0.2421) (0.8707 – 0.9689) (0.7526 – 0.8465) (0.8023 – 0.9455) (0.9538 – 0.9992) (0.8537 – 0.9809) (0.9480 – 0.9986)DT2 0.1864 0.9241 0.7937 0.9129 0.9831 0.9335 0.9670
(0.1412 – 0.2339) (0.8691 – 0.9679) (0.7424 – 0.8415) (0.8248 – 0.9787) (0.9547 – 0.9992) (0.8567 – 0.9845) (0.9336 – 0.9915)
(a) = Mymensingh; (b) = Government Farm; iELISA = indirect Enzyme-Linked ImmunoSorbentAssay; RBT = Rose Bengal Test; SAT = Slow Agglutination Test; prev = prevalentie; se = sensitivity;
sp = specificity; HW = Hui and Walter; E = iELISA; R = RBT; S = SAT; ,d = deterministic;
,p = probabilistic; IT = independent tests ; DT1 = dependent test - covariance parametrisation;
DT2 = dependent test - conditional parametrisation
Page 37

Table 4.9: Estimated parameter values using an iELISA cut-o! at 5 units
iELISA RBT SATModel prev se sp se sp se sp
HWER,d 0.0031 0.8123 0.9937 0.7613 0.9935HWES,d 0.0043 0.8204 0.9947 0.8201 0.9907HWRS,d 0.0021 0.9207 0.9931 0.9814 0.9893HWER,p 0.0050 0.7991 0.9931 0.7480 0.9928
(0.0009 – 0.0124) (0.6812 – 0.9011) (0.9866 –0.9980) (0.6289 – 0.8538) (0.9863 – 0.9976)HWES,p 0.0060 0.8076 0.9940 0.8071 0.9900
(0.0015 – 0.0136) (0.6926 – 0.9098) (0.9878 –0.9985) (0.6940 –0.9023) (0.9826 – 0.9958)HWRS,p 0.0034 0.9074 0.9926 0.9590 0.9885
(0.0006 – 0.0083) (0.8091 – 0.9842) (0.9867 – 0.9969) (0.8855 – 0.9980) (0.9811 – 0.9943)IT 0.0136 0.5059 0.9956 0.3854 0.9941 0.5254 0.9921
(0.0033 – 0.0347) (0.1498 – 0.9252) (0.9895 –0.9997) (0.1003 – 0.7838) (0.9878 – 0.9991) (0.1751 – 0.9153) (0.9845 – 0.9988)DT1 0.0030 0.9281 0.9916 0.8624 0.9914 0.6943 0.9866
(0.0003 – 0.0083) (0.8670 – 0.9714) (0.9844 – 0.9968) (0.6854 – 0.9717) (0.9845 – 0.9964) (0.3066 – 0.9650) (0.9785 – 0.9931)DT2 0.0027 0.9281 0.9918 0.8620 0.9907 0.6713 0.9857
(0.0001 – 0.0079) (0.8669 – 0.9715) (0.9850 – 0.9968) (0.6826 – 0.9723) (0.9838 – 0.9958) (0.2758 – 0.9613) (0.9777 – 0.9920)
iELISA RBT SATModel prev se sp se sp se sp
HWER,d 0.2330 0.8123 0.9937 0.7613 0.9935HWES,d 0.2316 0.8204 0.9947 0.8201 0.9907HWRS,d 0.1920 0.9207 0.9931 0.9814 0.9893HWER,p 0.2353 0.7991 0.9931 0.7480 0.9928
(0.1869 – 0.2881) (0.6812 – 0.9011) (0.9866 –0.9980) (0.6289 – 0.8538) (0.9863 – 0.9976)HWES,p 0.2337 0.8076 0.9940 0.8071 0.9900
(0.1858 – 0.2851) (0.6926 – 0.9098) (0.9878 –0.9985) (0.6940 –0.9023) (0.9826 – 0.9958)HWRS,p 0.1947 0.9074 0.9926 0.9590 0.9885
(0.1530 – 0.2400) (0.8091 – 0.9842) (0.9867 – 0.9969) (0.8855 – 0.9980) (0.9811 – 0.9943)IT 0.2034 0.7952 0.9567 0.8821 0.9936 0.9475 0.9923
(0.1622 – 0.2484) (0.6924 – 0.8818) (0.9292 – 0.9782) (0.7917 – 0.9508) (0.9803 – 0.9997) (0.8763 – 0.9902) (0.9765 – 0.9997)DT1 0.1804 0.9201 0.9570 0.8835 0.9695 0.9370 0.9661
(0.1370 – 0.2288) (0.8566 – 0.9677) (0.9296 – 0.9784) (0.8021 – 0.9463) (0.9385 – 0.9955) (0.8610 – 0.9851) (0.9339 – 0.9930)DT2 0.1732 0.9196 0.9493 0.9108 0.9698 0.9375 0.9556
(0.1297 – 0.2215) (0.8534 – 0.9680) (0.9171 – 0.9745) (0.8226 – 0.9778) (0.9396 – 0.9957) (0.8588 – 0.9869) (0.9205 – 0.9857)
(a) = Mymensingh; (b) = Government Farm; iELISA = indirect Enzyme-Linked ImmunoSorbentAssay; RBT = Rose Bengal Test; SAT = Slow Agglutination Test; prev = prevalentie; se = sensitivity;
sp = specificity; HW = Hui and Walter; E = iELISA; R = RBT; S = SAT; ,d = deterministic;
,p = probabilistic; IT = independent tests ; DT1 = dependent test - covariance parametrisation;
DT2 = dependent test - conditional parametrisation
Page 38

Table 4.10: Estimated parameter values using an iELISA cut-o! at 7.5 units
iELISA RBT SATModel prev se sp se sp se sp
HWER,d 0.0015 0.7834 0.9973 0.7927 0.9924HWES,d 0.0029 0.7935 0.9983 0.8562 0.9897HWRS,d 0.0021 0.9207 0.9931 0.9814 0.9893HWER,p 0.0032 0.7698 0.9966 0.7793 0.9918
(0.0003 – 0.0091) (0.6482 – 0.8780) (0.9918 –0.9995) (0.6614 – 0.8810) (0.99851 – 0.9967)HWES,p 0.0044 0.7807 0.9975 0.8441 0.9890
(0.0009 – 0.0106) (0.6606 – 0.8871) (0.9932 –0.9998) (0.7375 –0.9294) (0.9815 – 0.9949)HWRS,p 0.0034 0.9074 0.9926 0.9590 0.9885
(0.0006 – 0.0083) (0.8091 – 0.9842) (0.9867 – 0.9969) (0.8855 – 0.9980) (0.9811 – 0.9943)IT 0.0086 0.4284 0.9975 0.4355 0.9928 0.6557 0.9910
(0.0015 – 0.0257) (0.0775 – 0.9064) (0.9933 – 0.9998) (0.0869 – 0.8865) (0.9860 – 0.9981) (0.2037 – 0.9856) (0.9830 – 0.9984)DT1 0.0024 0.9282 0.9964 0.8659 0.9913 0.7399 0.9863
(0.0003 – 0.0067) (0.8676 – 0.9717) (0.9917 – 0.9993) (0.6970 – 0.9718) (0.9846 – 0.9961) (0.3589 – 0.9766) (0.9784 – 0.9926)DT2 0.0024 0.9286 0.9964 0.8656 0.9914 0.7403 0.9862
(0.0003 – 0.0067) (0.8680 – 0.9717) (0.9917 – 0.9993) (0.6940 – 0.9727) (0.9850 – 0.9961) (0.3601 – 0.9762) (0.9783 – 0.9925)
iELISA RBT SATModel prev se sp se sp se sp
HWER,d 0.2226 0.7834 0.9973 0.7927 0.9924HWES,d 0.2208 0.7935 0.9983 0.8562 0.9897HWRS,d 0.1920 0.9207 0.9931 0.9814 0.9893HWER,p 0.2247 0.7698 0.9966 0.7793 0.9918
(0.1776 – 0.2757) (0.6482 – 0.8780) (0.9918 –0.9995) (0.6614 – 0.8810) (0.9851 – 0.9967)HWES,p 0.2225 0.7807 0.9975 0.8441 0.9890
(0.1755 – 0.2726) (0.6606 – 0.8871) (0.9932 –0.9998) (0.7375 –0.9294) (0.9815 – 0.9949)HWRS,p 0.1947 0.9074 0.9926 0.9590 0.9885
(0.1530 – 0.2400) (0.8091 – 0.9842) (0.9867 – 0.9969) (0.8855 – 0.9980) (0.9811 – 0.9943)IT 0.2041 0.7655 0.9716 0.8802 0.9939 0.9465 0.9927
(0.1624 – 0.2495) (0.6591 – 0.8578) (0.9480 – 0.9885) (0.7909 – 0.9486) (0.9810 – 0.9998) (0.8759 – 0.9895) (0.9774 – 0.9997)DT1 0.1682 0.9186 0.9642 0.9047 0.9630 0.9312 0.9499
(0.1243 – 0.2189) (0.8469 – 0.9686) (0.9350 – 0.9861) (0.8111 – 0.9754) (0.9309 – 0.9951) (0.8504 – 0.9821) (0.9111 – 0.9889)DT2 0.1668 0.9208 0.9642 0.9065 0.9625 0.9346 0.9490
(0.1238 – 0.2154) (0.8529 – 0.9688) (0.9351 – 0.9859) (0.8152 – 0.9754) (0.9314 – 0.9907) (0.8528 – 0.9859) (0.9131 – 0.9799)
(a) = Mymensingh; (b) = Government Farm; iELISA = indirect Enzyme-Linked ImmunoSorbentAssay; RBT = Rose Bengal Test; SAT = Slow Agglutination Test; prev = prevalentie; se = sensitivity;
sp = specificity; HW = Hui and Walter; E = iELISA; R = RBT; S = SAT; ,d = deterministic;
,p = probabilistic; IT = independent tests ; DT1 = dependent test - covariance parametrisation;
DT2 = dependent test - conditional parametrisation
Page 39

Table 4.11: Estimated parameter values at the government farm using the model basedon conditional dependence - covariance parametrisation with increasingiELISA cut-o!
iELISA RBT SATModel prev se sp se sp se sp
DT1 (2) 0.1942 0.9250 0.8015 0.8825 0.9826 0.9310 0.9790(0.1488 – 0.2421) (0.8707 – 0.9689) (0.7526 – 0.8465) (0.8023 – 0.9455) (0.9538 – 0.9992) (0.8537 – 0.9809) (0.9480 – 0.9986)
DT1 (5) 0.1804 0.9201 0.9570 0.8835 0.9695 0.9370 0.9661(0.1370 – 0.2288) (0.8566 – 0.9677) (0.9296 – 0.9784) (0.8021 – 0.9463) (0.9385 – 0.9955) (0.8610 – 0.9851) (0.9339 – 0.9930)
DT1 (7.5) 0.1682 0.9186 0.9642 0.9047 0.9630 0.9312 0.9499(0.1243 – 0.2189) (0.8469 – 0.9686) (0.9350 – 0.9861) (0.8111 – 0.9754) (0.9309 – 0.9951) (0.8504 – 0.9821) (0.9111 – 0.9889)
DT1 (10) 0.1691 0.9192 0.9765 0.9025 0.9639 0.9307 0.9516(0.1251 – 0.2193) (0.8485 – 0.9684) (0.9498 – 0.9946) (0.8115 – 0.9737) (0.9341 – 0.9922) (0.8476 – 0.9817) (0.9151 – 0.9864)
DT1 (12.5) 0.1688 0.9201 0.9903 0.8903 0.9608 0.9326 0.9539(0.1269 – 0.2167) (0.8507 – 0.9683) (0.9746 – 0.9990) (0.8093 – 0.9517) (0.9306 – 0.9869) (0.8519 – 0.9831) (0.9217 – 0.9840)
DT1 (15) 0.1647 0.9212 0.9934 0.9038 0.9595 0.9339 0.9489(0.1238 – 0.2115) (0.8534 – 0.9691) (0.9803 – 0.9996) (0.8253 – 0.9612) (0.9293 – 0.9866) (0.8563 – 0.9831) (0.9156 – 0.9787)
DT1 (20) 0.1507 0.9233 0.9935 0.8980 0.9457 0.9284 0.9353(0.1122 – 0.1949) (0.8567 – 0.9695) (0.9806 – 0.9997) (0.8148 – 0.9583) (0.9146 – 0.9734) (0.8440 – 0.9817) (0.9016 – 0.9658)
iELISA = indirect Enzyme-Linked ImmunoSorbent Assay; RBT = Rose Bengal Test;SAT = Slow Agglutination Test; prev = prevalentie; se = sensitivity; sp = specificity;DT1 = dependent test - covariance parametrisation; (2) = iELISA cut-o! 2 IU/ml;
(5) = iELISA cut-o! 5 IU/ml; (7.5) = iELISA cut-o! 7.5 IU/ml;(10) = iELISA cut-o! 10 IU/ml; (12.5) = iELISA cut-o! 12.5 IU/ml
(15) = iELISA cut-o! 15 IU/ml; (20) = iELISA cut-o! 20 IU/ml
Page 40

5Discussion
It is traditionally assumed that the values of sensitivity and specificity, as supplied by themanufacturer of the test, apply to the population on which the test is used. In this way,the prior knowledge of the test characteristics is given so much weight that the actual dataat hand become more or less insignificant as far as these characteristics are concerned.This suggests that the prevalence can be estimated. However, these Se and Sp values areusually not constant and universally applicable and assuming constancy of test parame-ters over di!erent populations may grossly misestimate the true prevalence. Therefore,the characteristics of the population of interest must be considered. In the absence of agold standard test, an alternative way to get an improved estimation of Se, Sp and thetrue prevalence, is combining multiple imperfect test (Berkvens et al., 2006; Greiner andGardner, 2000).
An important consideration however, is whether or not these tests can be assumedconditionally independent. Since iELISA, RBT and SAT are based on similar biologicalevents, namely the detection of serum antibody response, the tests might be considereddependent on each other given the true disease status of subjects (Rahman, unpublished).Dependency of tests substantially changes the theoretical values of Se and Sp of multiplecombined tests compared with the values expected when tests are conditionally indepen-dent (Gardner et al., 2000). Therefore, estimation procedures should adjust for thesedependencies among tests (Dendukuri and Joseph, 2001). However, the full model as-suming conditional dependence has the implicit characteristic of being overparametrized.When conditional dependence exists between the tests, 15 parameters need to be esti-mated, which exceeds the amount that can be estimated. Hence, estimation of the truedisease prevalence and test characteristics becomes either impossible or external (prior)information must be added by means of imposing constraints on the parameters (Berkvenset al., 2006).Anything from genuine information acquired through high-quality data to a personalopinion can be quantified and fed as a prior belief into a model. We imposed di!erentconstraints onto the four models; ranging from the assumption of conditional indepen-dence and/or constancy of test parameters over populations to the specification of prior
41

distributions on parameters using expert opinion. This resulted in the estimations of theposterior means (and the 95% credibility intervals) of the prevalence and diagnostic testcharacteristics of all three tests at the di!erent iELISA cut-o!s shown in Table 4.8, Ta-ble 4.9, Table 4.10 and Table 4.11.
The user can monitor the e!ect of this prior belief on the results and it may be easierfor the user to appreciate the fact that the actual interpretation of the test results isconditional on the prior opinion. The e!ect of imposing deterministic and/or probabilisticconstraints is reflected in the value of pD and can thus be evaluated. DIC, pD and theBayesian p-value are useful in the process of selecting a model and evaluating the fit ofprior information (Berkvens et al., 2006). The results of the di!erent scenarios clearlyshow that the estimates of the prevalence and test characteristics depend on the modeland the expert opinion chosen and that widely varying estimates can be obtained. It isimportant to understand this and realize that the chosen model and expert opinion havegreat impact on the final estimation of the prevalence.
5.1 Comparison of Bayesian models
5.1.1 Bayesian p-value, PD and DIC
As an example, both the optimum values as well as the Bayesian p-value, DIC and pDvalues obtained from the models (with iELISA cut-o! 7.5 IU/ml) are shown in Table 5.1.When we excluded the prior information on the iELISA- and the SAT specificity weobtained the best values for these parameters. For most models the Bayesian p-value wasaround 0.4 - 0.5 indicating no particular problem and when we compared the results forDIC and pD to the optimum values obtainable in Mymensingh and the government farmwe could assume a good model fit.
Table 5.1: Summary of Bayesian p-value, pD and DIC results from the di!erent mod-els and optimum values for DIC and pD obtainable from the data
i ELISA cut-o! 7.5 IU/ml Mymensingh Government farm
Bayesp pD DIC Bayesp pD DICModel Optimum: 4.468 27.284 5.031 36.947
IT 0.4329 4.031 26.847 0.4909 5.051 36.966DT1 0.4427 4.395 27.414 0.5153 5.464 37.433DT2 0.4216 4.334 27.315 0.4807 5.258 37.023
IT = independent tests ; DT1 = dependent test - covariance parametrisation;DT2 = dependent test - conditional parametrisation; Bayesp = Bayesian p-value;
DIC = deviance information criterion; pD = The e!ective number of estimated parameters
5.1.2 Independent test model
The independent test model yielded moderate pD, DIC and Bayesian p-values but theprevalence and test-characteristic estimates are totally di!erent from other models espe-cially in the Mymensingh district. Due to these aberrant estimates we decided not to usethis model in these areas.
Page 42

5.1.3 Hui and Walter models
The Hui and Walter model is surprisingly accurate in this situation, especially wheniELISA was not included. Even though the Hui and Walter model assumes independenceof the test results, just like the independent model, it has far less aberrant estimates. TheHui and Walter model probably works because only two tests are involved and dependenceis restrained to specificity (and high specificities mean low values of covariances).To avoid mirror symmetry we constrained the prevalence to dbeta(1,1)I(0,0.5) in all mod-els, except the deterministic Hui and Walter model. Mirror symmetry yields severalpossible solutions, depending on the starting conditions. Replacing the prevalence by itsown complement, i.e. p°= 1 - p, sensitivity by the complement of specificity (se°= 1 - sp)and specificity by the complement of sensitivity (sp°= 1 - se) yields a symmetric solution.Constraining the prevalence to [0-0.5] results in convergence and identifiable estimatesfor al parameters (Berkvens et al., 2006). Strangely, in the probabilistic Hui and Waltermodel constraining the two prevalence priors did not su"ce to permit convergence. Priorconstraints had to be applied to both sensitivity and specificity of one test for convergenceto occur.
5.1.4 Dependent test models
Since iELISA, RBT and SAT are based on similar biological events, namely the detectionof serum antibody response, we suggest to work under the assumption of conditional de-pendence. Dependency of tests substantially changes the theoretical values of Se and Sp ofmultiple combined tests compared with the values expected when tests are conditionallyindependent (Gardner et al., 2000). When dependence exists between tests, the number ofparameters that have to be estimated, 15 for three tests, exceeds the the number that canbe estimated. This can be resolved through the inclusion of expert opinion (probabilisticcontrainst). Models developed on the basis of covariances and conditional probabilitiesallow formalisation of this expert opinion, whatever form it might take (Berkvens et al.,2006). We included expert opinion in the form of prior beta distributions for sensitivityand specificity as specified by the meta-analysis and we monitored the e!ect of this priorbelief on the results. However, it is argued that it is practically impossible to give reliableprior information on the sensitivity of a diagnostic test because this is often determenton a small number of subjects (Berkvens et al., 2006).
First, we ran the models without any constraints, thereafter, we included all the priordistributions generated by the meta-analysis. By varying the inclusion of prior distribu-tions we analyzed the e!ect of the prior belief on the estimation of the prevalence and testcharacteristics. Since constancy of test parameters cannot be assumed expert opinions isregularly in conflict with the observed data. When we used all the priors, the model fitwas not su"cient. Excluding the narrow priors for the specificity of iELISA (dbeta(750,2.6544)) and SAT (dbeta(190,1.6483)) resulted in a better model fit.The results of the di!erent scenarios clearly show that the estimate of the prevalenceand test characteristics depends on the model and priors chosen and that widely varyingestimates can be obtained. It is important to understand this and realise that the expertopinion has a great impact on the final estimation of the prevalence and test character-istics. We have to appreciate the fact that the actual interpretation of the test results isconditional on the prior opinion.
Page 43

Taking into account conditional dependence between the three diagnostic tests con-siderably reduces the prevalence (compared to independent tests) and generally speakingspecificities decrease and sensitivities increase (except for the sensitivity of SAT at thegovernment farm).
The model based on conditional dependence - Berkvens et al. scheme presumes de-tailed expert knowledge about conditional probabilities. To be able to provide specificinformation about the behavior of one test conditional on the result of another test, ex-perts must have practical experience with the use of di!erent combinations of tests underexperimental conditions (Berkvens et al., 2006).Unfortunately, this expertise was not available for brucellosis. Therefore, we had to elicitinformation on dependency from the covariance model. The Se and Sp from the tests thatprove to be independent in the covariance model could be used in the conditional model.Only in this case raw sensitivities and specificities could be used because '’s become equal.For example, as discussed above the sensitivity of RBT was independent of iELISA testresults in the covariance model, which means '4 and '5 become equal in the Berkvens etal. scheme. Hence, the conditional model could not be su"ciently constrained to yieldmeaningful estimates.
We suggest that the covariance model is the appropriate model for brucellosis becauseit permitted us to use all the available information. Although the covariances cannot berelated to real-life situations, the raw sensitivities and specificities available through themeta-analysis could be used in this model. However, one problem had to be overcomewhen using this model; the initial values could not be generated, but had to be suppliedto ensure probabilities between 0 and 1. Therefore, we generated and loaded the threelists shown in appendix 4.
5.2 Results of the model based on conditional depen-dence - Covariance scheme
The estimates resulting from the covariance model in both the Mymensingh area as wellas at the government farm are shown in Table 5.2.
Page 44

Table 5.2: Estimates of prevalence and diagnostic test characteristics using the modelbased on conditional dependence - covariance parametrisation with increas-ing iELISA cut-o!
iELISA RBT SATModel prev se sp se sp se sp
DT1 (2) 0.0100 0.9325 0.8584 0.8628 0.9977 0.4319 0.9889(0.0041 – 0.0186) (0.8759 – 0.9732) (0.8356 – 0.8792) (0.6849 – 0.9720) (0.9934 – 0.9999) (0.1833 – 0.7205) (0.9814 – 0.9947)
DT1 (5) 0.0030 0.9281 0.9916 0.8624 0.9914 0.6943 0.9866(0.0003 – 0.0083) (0.8670 – 0.9714) (0.9844 – 0.9968) (0.6854 – 0.9717) (0.9845 – 0.9964) (0.3066 – 0.9650) (0.9785 – 0.9931)
DT1 (7.5) 0.0024 0.9282 0.9964 0.8659 0.9913 0.7399 0.9863(0.0003 – 0.0067) (0.8676 – 0.9717) (0.9917 – 0.9993) (0.6970 – 0.9718) (0.9846 – 0.9961) (0.3589 – 0.9766) (0.9784 – 0.9926)
iELISA RBT SATModel prev se sp se sp se sp
DT1 (2) 0.1942 0.9250 0.8015 0.8825 0.9826 0.9310 0.9790(0.1488 – 0.2421) (0.8707 – 0.9689) (0.7526 – 0.8465) (0.8023 – 0.9455) (0.9538 – 0.9992) (0.8537 – 0.9809) (0.9480 – 0.9986)
DT1 (5) 0.1804 0.9201 0.9570 0.8835 0.9695 0.9370 0.9661(0.1370 – 0.2288) (0.8566 – 0.9677) (0.9296 – 0.9784) (0.8021 – 0.9463) (0.9385 – 0.9955) (0.8610 – 0.9851) (0.9339 – 0.9930)
DT1 (7.5) 0.1682 0.9186 0.9642 0.9047 0.9630 0.9312 0.9499(0.1243 – 0.2189) (0.8469 – 0.9686) (0.9350 – 0.9861) (0.8111 – 0.9754) (0.9309 – 0.9951) (0.8504 – 0.9821) (0.9111 – 0.9889)
DT1 (10) 0.1691 0.9192 0.9765 0.9025 0.9639 0.9307 0.9516(0.1251 – 0.2193) (0.8485 – 0.9684) (0.9498 – 0.9946) (0.8115 – 0.9737) (0.9341 – 0.9922) (0.8476 – 0.9817) (0.9151 – 0.9864)
DT1 (12.5) 0.1688 0.9201 0.9903 0.8903 0.9608 0.9326 0.9539(0.1269 – 0.2167) (0.8507 – 0.9683) (0.9746 – 0.9990) (0.8093 – 0.9517) (0.9306 – 0.9869) (0.8519 – 0.9831) (0.9217 – 0.9840)
DT1 (15) 0.1647 0.9212 0.9934 0.9038 0.9595 0.9339 0.9489(0.1238 – 0.2115) (0.8534 – 0.9691) (0.9803 – 0.9996) (0.8253 – 0.9612) (0.9293 – 0.9866) (0.8563 – 0.9831) (0.9156 – 0.9787)
DT1 (20) 0.1507 0.9233 0.9935 0.8980 0.9457 0.9284 0.9353(0.1122 – 0.1949) (0.8567 – 0.9695) (0.9806 – 0.9997) (0.8148 – 0.9583) (0.9146 – 0.9734) (0.8440 – 0.9817) (0.9016 – 0.9658)
(a) = Mymensingh; (b) = Government Farm; iELISA = indirect Enzyme-Linked ImmunoSorbentAssay; RBT = Rose Bengal Test; SAT = Slow Agglutination Test;
prev = prevalentie; se = sensitivity; sp = specificity;DT1 = dependent test - covariance parametrisation; (2) = ELISA cut-o! 2 IU/ml;
(5) = ELISA cut-o! 5 IU/ml; (7.5) = ELISA cut-o! 7.5 IU/ml(10) = iELISA cut-o! 10 IU/ml; (12.5) = iELISA cut-o! 12.5 IU/ml
(15) = iELISA cut-o! 15 IU/ml; (20) = iELISA cut-o! 20 IU/ml
After we converted the posterior estimates (95% credibility intervals), obtained fromthe covariance model with iELISA cut-o! 7.5 IU/ml1, into beta distributions (Table 5.3)we could plot them against the prior distributions obtained from the meta-analysis (Ta-ble 4.5). This resulted in the graphs shown in appendix 6. It is notable that all theposterior distributions are narrower than their respective prior distributions. In addition,except for the sensitivity of SAT in the government farm, the graphs show lower posteriorsensitivity values compared to the prior Se. Furthermore a di!erence is notable in thefact that the posterior Sp values seem to be narrower in the Mymensingh district, whileat the government farm the posterior Se are narrower. This might be explained by thelower prevalence in Mymensingh resulting in more negative testing animals and thus abetter update of the specificity. At the government farm this is the other way around; thehigher prevalence and the consequently higher number of positive testing animals resultin a better update of the sensitivity.
1We opted for a common cut-o! for Mymensingh and government farm for comparison’s sake
Page 45

Table 5.3: Summary values of posterior beta distribution parameters
Mymensingh Government farm
Sensitivity Specificity Sensitivity SpecificityTest " % " % " % " %
iELISA 112.784 9.6469 1416.971 6.1159 90.293 8.9125 264.827 10.7957RBT 26.030 4.8763 1284.296 12.2627 62.113 7.4376 231.752 9.8659SAT 5.846 2.7035 1283.237 18.8107 70.9110 6.1652 197.422 11.3598
5.3 Epidemiology of brucellosis
5.3.1 False positive serological cross-reactions
In both areas there might be an indication for false positive serological cross-reactions(FPSR) due to cross-reacting antibodies. The number of FPSR are generally assumedto decease with increasing iELISA cut-o! value. Table 5.2 shows the estimates resultingfrom the covariance model in both the Mymensingh area as well as at the governmentfarm and the prevalence and test characteristics at the government farm in function ofthe iELISA cut-o! are shown in Figure 5.1.The prevalence decreased with increasing iELISA cut-o!, potentially because the numberof false positive serological reactions decreased. In addition, the iELISA specificity in-creased with increasing cut-o!, while at the government farm the opposite occured withRBT and SAT. Because false positive serological reactions (FPSR) are known to drasti-cally decrease the specificity of iELISA (Saegerman et al., 2004), the increasing iELISAspecificity might be explained by the decreasing number of false positive reactors withincreasing cut-o! values. The traditional cut-o! at 2 IU/ml indeed yielded specificityestimates that were very low, indicating the potential presence of cross-reactions.On the other hand, the decreasing Sp of RBT and SAT at the government farm mightbe due to the mathematical consequence of the decreasing prevalence, which results inan increased proportion of disease free animals. Whereas the number of test-negativetruly uninfected animals remains the same, the number of test-positive truly uninfectedanimals increases and thus there is a decrease in Sp. While the FPSR are filtered outin the iELISA with increasing cut-o!, there might be some FPSR left in RBT and SAT,since nothing changed in the reading of these test.Possibly unexpected, the sensitivity of all three tests hardly changed with increasingiELISA cut-o!, except for SAT in the Mymensingh area.
At a certain iELISA cut-o!, all three tests show a low specificity at the government farmwhen we compare this to the estimates in the Mymensingh area. This might be explainedby the fact that next to the higher Brucella antibody prevalence at the government farm,the prevalence of infections with cross-reacting bacteria and their respective antibodytiters might be higher due to the usually higher susceptibility of high productive animalsto infections and a higher risk of introducing pathogens due to import of animals. Thisresults in higher FPSR prevalence and titers and consequently a lower specificity. Thisdemonstrates that the test characteristics depend on the area in which the tests are used,and constancy of test characteristics cannot be assumed. Hence, there is reason to rec-ommend using a higher iELISA cut-o! at the government farm compared to Mymensingh.
Page 46

5 10 15 20
0.15
0.17
0.19
prevalence
5 10 15 20
0.80
0.90
1.00
iELISA
5 10 15 20
0.88
0.92
0.96
RBT
5 10 15 20
0.93
0.95
0.97
iELISA cut-off
SAT
Figure 5.1: Government Farm: Estimates of prevalence and diagnostic test character-istics with increasing iELISA cut-o!with: —– = Sensitivity; —– = Specificity
Since the prevalence in the Mymensigh area is low it is also important to rememberthat a high proportion of positive serological results may be obtained even in the absenceof brucellosis infection since the serological tests are ”imperfect” tests. Even though theiELISA (sensitivity of 92.81% and specificity of 99.16%) in the Mymensigh area with aniELISA cut-o! of 5 IU/ml is highly specific, the positive predictive value (the probability
Page 47

to be a true positive) is estimated to be 24.95%. This means that 75.05% of the animalsclassified sero-positive are actually not infected. In contrast, even with a lower specificityof iELISA (sensitivity of 92.01% and specificity of 95.70%) at the government farm withan iELISA cut-o! of 5 IU/ml, this test yields an estimated 82.49% positive predictivevalue because the prevalence is higher.
5.3.2 iELISA cut-o!
Traditionally an iELISA cut-o! of around 2 IU/ml is used. In our case, this cut-o! yieldediELISA specificity estimates that were very low and showed great di!erences between My-mensingh and the government farm. As discussed above, this might be an indication forthe presence of false positive cross-reactions.Especially the high numbers of positive animals for the iELISA alone, 137 and 53 in theMymensingh district and at the government farm respectively, is notable in Table 4.6.These values caused a high total number of iELISA positive animals in comparison to thenumber of positive animals in RBT and SAT.When we plot all test results for iELISA (in IU/ml) against age (in years) we obtainfigure Figure 5.2a and Figure 5.2b. Comparison of the corrected iELISA ODs shows adramatic di!erence between Mymensingh, with very low titres, and the government farm,showing much higher titres. In the field (Mymensingh) the iELISA units hardly exceeded7.5 IU/ml, while at the government farm iELISA units were significantly higher. Becausethe iELISA units in Mymensingh are lower compared to the values at the governmentfarm, it is clear why the number of iELISA positive animals in the Mymensingh districtdrastically decreases when we change the iELISA cut-o! to 5 or 7.5 IU/ml. At the gov-ernment farm this number drops considerably when we increase the cut-o! to 5 IU/mlbut only shows low and steady numbers of iELISA positive animals from a cut-o! of 12.5IU/ml onwards.
Hence, there is reason to recommend using a higher iELISA cut-o! at the governmentfarm compared to the Mymensingh area. Because the sensitivity remains around 92% andthe specificity reaches above 99%, a cut-o! of 5 IU/ml seems the most appropriate in theMymensingh area. At the government farm, a cut-o! value of 12.5 IU/ml appears moreappropriate, because a specificity of 99% is only reached from this point onward while thesensitivity remains around 92%. To avoid the FPSR problem, we therefore suggest to usethe results obtained with an iELISA cuto! of 5 IU/ml in the Mymensingh area and 12.5IU/ml at the government farm.
5.3.3 Comparison of the brucellosis prevalence in Mymensinghand at the government farm
Now, we might assume the iELISA results between 2- and 5 IU/ml in the Mymensingharea and 2- and 12.5 IU/ml at the government farm are false positive serological reactionsdue to cross reacting antibodies. In this case, animals are negative below an iELISAcut-o! value of 2 IU/ml, false positive between 2- and 5 UI/ml and true positive above5 IU/ml in the Mymensingh area. In the same way, at the government farm animalsare assumed negative below 2 IU/ml, false positive between 2- and 12.5 IU/ml and truepositive above an iELISA cut-o! of 12.5 IU/ml. When we plot this in function of age weobtain the graphs in figure Figure 5.2c and Figure 5.2d.
Page 48

These graphs suggest that the proportion of false positive cattle is greater than the smallproportion of true positive cattle in the Mymensingh area. In addition all three iELISAstatuses (negative, false positive and true positive) hardly change with age.In contrast, at the government farm the proportion of false positive animals is lower thanthe proportion of true positive cattle. With increasing age the proportion of negative an-imals decreases while the proportion of true positive cattle increases. This might suggestwe are dealing with normal infection dynamics, since significant association is reportedbetween age and sero-prevalence of brucellosis. In cattle, the highest sero-prevalence wasfound in the age group above 48 months of age (Rahman et al., 2011). The higher sero-prevalence among older cows may be because the bacteria can remain latent or chronic foran unspecified period of time before it manifests as a clinical disease. Alternatively, thehigher sero-prevalence among older cows may be related to aged animals having a greaterchance of coming into contact with other animals and becoming infected (Rahman et al.,2011).
Most articles describe cattle seroprevalence to range between 3 and 15% in endemicareas. Factors influencing prevalence include production systems, management factors,husbandry practices, agro-ecological zones and contact with wildlife (Muma et al., 2007a).At the government farm cattle are not tested and the farm practices indiscriminate breed-ing. The import of animals to the government farm results in a higher risk of introducingpathogens. In addition, the animals at the farm are mainly high producing animals, whichare usually more susceptible to infections. Because cell-mediated immunity plays a keyrole in the protection against brucellosis (He, 2012), a less e"cient cell-mediated responsein high producing animals may result in higher bacterial counts and a consequently morepronounced humoral response. Furthermore, donor bulls, held on the farm for nationalAI service, were even found positive. Because the semen of infected bulls can be contami-nated with B. abortus, the risk of transmission via artificial insemination is not negligible.These reasons might explain the very high infection prevalence and iELISA titers.The low prevalence in the Mymensingh area might be explained by the fact that thecommon breeds are indigenous (and their crosses), which are less susceptible, that thedisease is known by cattle owners and positive animals are slaughtered. Unpublisheddata show absence of correlation between Brucella infection and abortion in this area(more than 10% of the herds had experienced abortion during the last year, Rahman,pers.comm. 2013), which means probably another causative agent is involved. This ab-sence of correlation might be explained by the low prevalence and possibly also by thefact that the disease can be asymptomatic and the bacteria can remain latent or chronicfor an unspecified period of time (Godfroid et al., 2010; Rahman et al., 2011; unpublished).
Page 49

020
4060
0 5 10 15age
elisaplot cut1cut2
(a)
020
4060
0 5 10 15 20Agyrs
elisaplot cut1cut3
(b)
0.2
.4.6
.8
0 5 10 15age
Pr(elisa3==0) Pr(elisa3==1)Pr(elisa3==2)
(c)
0.2
.4.6
.8
0 5 10 15 20Agyrs
Pr(elisa3==0) Pr(elisa3==1)Pr(elisa3==2)
(d)
Figure 5.2: iELISA units (IU/ml) and status in function of agea and b show the iELISA units (IU/ml) in function of age with: cut1 = 2 IU/ml iELISA
cut-o!; cut2 = 5 IU/ml iELISA cut-o!; cut3 = 12.5 IU/ml iELISA cut-o!.c and d show the proportion of negative, true positive and false positive animals infunction of age with: —– = negative; —– = false positive; —– = true positive
5.4 Strategy for control and eradication of brucellosis
Bovine brucellosis continues to cause great economic loss to livestock industries becauseit induces delayed œustrus, increased calving interval, birth of weak calves, infectiousabortion, infertility and subsequent culling and interruption of lactation may lead to areduction in milk yield (Roth et al., 2003). Together with its (international) trade andpublic health implications brucellosis remains of particular concern in Bangladesh. There-fore control and eradication of the disease is a goal. The choice of a control and eradicationstrategy in the regions should be made after a scenario analysis; an independent, scien-tific and collective assessment where costs and the range and magnitude of consequencesof measures or surveillance programs of all susceptible domestic livestock (and possibly)wildlife are considered. Such a risk assessment should be performed taking into accountthe particular local situation, current scientific knowledge, and uncertainties about the
Page 50

parameters (Hadorn and Stark, 2008). Futhermore, control strategies should be accept-able to communities and take into account anthropological factors (Godfroid et al., 2011).
In the countries that are o"cially brucellosis free, control has been achieved through thecombination of vaccination and test-and-slauhter programs coupled with e!ective diseasesurveillance, animal movement control and milk pasteurization (McDermott and Arimi,2002). Together with compensation for farmers, accreditation and financial incentives fordisease free herds, this status could be achieved (Godfroid et al., 2011).Eradication programs have always been long, costly and hard to carry out. In areas wherebrucellosis is endemic and favorable environmental conditions exist, proper campaign or-ganization, the decisive factor in eradication, is unlikely to be reached soon. The mostimportant di"culties in controlling and eradicating are the animal management condi-tions; indiscriminate breeding, coexistence of several livestock species etc. (Godfroid et al.,2011). In addition, test-and-slaughter regimes are di"cult to achieve because of possibleemotional attachment and limited resources to indemnify farmers (McDermott and Arimi,2002). Furthermore, the current vaccines require proficient veterinary services, which isa potential limitation (Godfroid et al., 2011). Control and eradication can therefore onlybe facilitated by a perfect brucellosis vaccine. The perfect brucellosis vaccine should: (1)be e!ective in a single dose; (2) trigger a solid and life-lasting immunity; (3) not interferewith serological diagnostic tests; (4) protect against infection by Brucella species otherthan those typical of a given host; (5) be a!ordable; (6) be innocuous regardless of thephysiological state of the animal; (7) not be shed in the environment; (8) not be virulentfor humans or carry resistance to antibiotics; and (9) be stable (Godfroid et al., 2011).Furthermore, e!ective surveillance and testing of animals at purchase, before usage inAI programs and after an abortion is important. Finally, test-and-slaughter regimes andanimal movement controls may need to be considered.
Albeit the host preferences, Brucella spp. have also been isolated from non-typical hostanimal species and a great variety of wildlife species. As a consequence, these animalsmay act as spill-over hosts (victims) or as a reservoir hosts (vectors) of Brucella spp. forhumans and other animal species (Pappas et al., 2006b).Both B. melitensis and B. suis in cattle are an emerging veterinary and public healthproblem. It is recommended to reduce opportunities for B. suis, B. melitensis and pos-sibly B. abortus to ”jump” between domestic, feral and wild suidae, ovine/caprine andbovine on one hand and humans on the other hand (Godfroid et al., 2011). B. abortusinfection in sheep and B. melitensis in cattle were only reported when a source of Bru-cella spp. was found in their respective preferential host, i.e. B. melitensis in sheep andB. abortus in cattle. This suggest that B. abortus in sheep and B. melitensis infectionin cattle are spill over infections and cannot establish enzootic infections. It is thereforeimportant to remind that any sound vaccination program in livestock should be imple-mented in reservoir hosts, not in spill-over hosts. Moreover, vaccines for all susceptibleanimals such as water bu!aloes, camels and swine are still missing (Godfroid et al., 2011).
Since the positive predictive value (PPV) of a serological test depends on the specificityand the prevalence, a lower positive predictive value occurs when an eradication programis close to its end and the prevalence drops. Hence, the PPV of tests varies according tothe progress of the eradication program. Therefore, it is important to adapt the controland eradication strategy to the epidemiological situation. The specificities of the serolog-
Page 51

ical tests become more important when the prevalence of brucellosis decreases (Godfroidet al., 2011). However, the sensitivity of the test used should remain su"ciently high toensure proper eradication.
To overcome the FPSR problem, competitive ELISA, the brucellin skin test, the in-terferon gamma (IFN-!) test and the native hapten and cytosol protein-based test mightbe considered. The iELISA is highly sensitive but lacks the capability of fully resolvingthe FPSR problem and the problem of di!erentiating between antibodies resulting frominfection and S19 vaccination (OIE, 2009). The cELISA is based on specific epitopes ofthe OPS and can therefore eliminate some of the cross-reaction problems seen in iELISA.Although cELISA is shown to have higher diagnostic specificity it usually has a lowersensitivity than the iELISA (Munoz et al., 2005).Alternative immunological tests, the brucellin skin test and the brucellosis IFN-! test,measure the cell-mediated response in bovine brucellosis, which is directed against pro-teins. The INF-! test involves stimulation of lymphocytes in whole blood with a suitableantigen resulting in INF-! production, which can be measured by a capture ELISA (God-froid et al., 2002; OIE, 2009). The brucellin skin test can be used in unvaccinated cattleand is one of the most specific tests, such that serological negative animals that react tothe brucellin skin test should be regarded as infected animals. This may aid the interpre-tation of serological reactions thought to be FPSR due to infection with cross-reactingbacteria, especially in areas with a low to non-existing brucellosis prevalence (Saegermanet al., 1999). However, the sensitivity is low, which means not all infected animals react.Therefore this test alone cannot be recommended as sole diagnostic test and should besupported by a reliable serological test. An interval of 6 weeks is generally recommendedbetween two tests in the same animal because the intradermal inoculation of brucellinmight induce a temporary anergy in the cellular immune response (OIE, 2009).Finally, precipitin tests using native hapten or Brucella cytosol proteins have also beenshown to eliminate, in most cases, FPSR of unknown origin and FPSR caused by Yersiniaenterocolitica O:9 (Munoz et al., 2005).
It seems to be relevant to find the origin of the FPSR. Since the immune-dominantO-chain of sLPS of Yersinia enterocolitica serotype O:9 and Brucella species are iden-tical, FPSR due to Yersinia enterocolitica O:9 usually presents the most serious sourceof confusion (Saegerman et al., 2004). Therefore testing of cattle for Yersinia enteroco-litica might be the first step in finding the source of FPSR. Yersinia enterocolitica arefrequently encountered in terrestrial and freshwater ecosystems and in animals, food andwater. Although the bacteria have been isolated from many vertebrate species, swineare an important reservoir of the bacteria and regularly harbour pathogenic Yersinia en-terocolitica (including O:9), which cause human infection (Kapperud, 1991). However,especially due to religious perspectives, Bangladesh has a limited number of pork con-sumers and thus a small (but increasing) pig population (Rahman et al., 2012c). Thismeans there is a possibility that other causative agents are involved.
Overall, it would be benificial to improve the diagnostic capabilities, especially sinceFPSR still interfere in serological diagnosis (Godfroid et al., 2011). Brucellosis aware-ness, comprehensive surveillance, testing with reliable tests and e"cacious vaccines areof paramount importance in order to eradicate or at least control brucellosis (Englandet al., 2004, Cutler et al., 2005). In addition, it is important to improve the brucellosis
Page 52

awareness and the surveillance in other livestock species, wildlife and humans.Because brucellosis has international-trade and public health implications, all memberstates of the OIE have an obligation of reporting. The liberalization of exchange andremoval of sanitary barriers in accordance with the World Trade Organization Agreementrequire the harmonization of the brucellosis health status among countries to eliminatethe risk of contamination through importation of live animals and animal products. It isa global responsibility to reduce opportunities for Brucella spp. to spread and to ”jump”host species at the animal/environment/human interface. Therefore, a ”One Health” ap-proach is probably needed to be successful (Godfroid et al., 2011).
Finally, whatever approach is envisaged in Bangladesh, it must not be forgotten thatlocal farmers managing local animals seem to be fully aware of the problem and in fullcontrol of it. A detailed economic analysis of additional costs and benefits must beconducted before any decisions are made to ensure that things are not made worse.
Page 53


6Conclusion
We imposed di!erent constraints onto the four di!erent models; ranging from the assump-tion of conditional independence and/or constancy of test parameters over populationsto the specification of prior distributions on parameters using expert opinion. External(prior) information (in the form of beta distributions) was generated by means of a meta-analysis based on data from 11 di!erent publications. By combining the data (test results)and the external information, the posterior means (and the 95% credibility intervals) ofthe true prevalence and diagnostic test characteristics of all three tests at the di!erentiELISA cut-o!s could be estimated. Hence, we used a new way to incorporate expertopinion in the form of prior beta distributions for sensitivities and specificities as speci-fied by the meta analysis and we monitored the e!ect of this prior belief on the results.The e!ect of imposing deterministic and/or probabilistic constraints is reflected in thevalue of DIC, pD and the Bayesian p-value, which are useful in the process of selectinga model and evaluating the fit of prior information. The results of the di!erent scenariosclearly show that the estimates of the prevalence and test characteristics depend on themodel and the expert opinion chosen and that widely varying estimates can be obtained.
Since iELISA, RBT and SAT are based on similar biological events, namely the detec-tion of serum antibody response, we suggest to work under the assumption of conditionaldependence. We suggest that the covariance model, which assumes dependence betweentests, is the appropriate model for brucellosis because it permitted us to use all the avail-able information. Although the covariances cannot be related to real-life situations, theraw sensitivities and specificities available through the meta-analysis could be used in thismodel. This is in contrast with the Berkvens et al. scheme, which could not be su"cientlyconstrained to yield meaningful estimates due to a lack of detailed expert knowledge onthe behavior of one test conditional on the result of another test (i.e. conditional proba-bilities).
The prevalence decreased and the iELISA specificity increased with increasing iELISAcut-o!. This might be an indication for false positive serological cross-reactions (FPSR)due to cross-reacting antibodies. The decreasing Sp of RBT and SAT at the government
55

farm might be due to the fact that while the FPSR are filtered out in the iELISA withincreasing cut-o!, there might be some FPSR left in RBT and SAT, since nothing changedin the reading of these test. Possibly unexpected, the sensitivity of all three tests hardlychanged with increasing iELISA cut-o!, except for SAT in the Mymensingh area.
Comparison of the corrected iELISA ODs shows a dramatic di!erence between My-mensingh, where the iELISA units hardly exceeded 7.5 IU/ml, and the government farm,showing much higher titres. In the Mymensingh area we find low prevalence and unpub-lished data show absence of correlation between Brucella infection and abortion in thisarea, which means probably another causative agent is involved. The low prevalence andtiters in the Mymensingh area might be explained by the fact that the common breeds areindigenous (and their crosses), which are less susceptible, the disease is known by cattleowners and positive animals are slaughtered.In contrast, at the government farm the prevalence and titers are high and we might bedealing with normal infection dynamics. Cattle are not tested and the farm practicesindiscriminate breeding. Donor bulls, held on the farm for national AI service, were evenfound positive. Because the semen of infected bulls can be contaminated with B. abortus,the risk of transmission via artificial insemination is not negligible. Furthermore, due tothe usually higher susceptibility of high productive animals to infections and a higherrisk of introducing pathogens due to import of animals, Brucella antibody prevalence andiELISA titers might be higher in this area compared to Mymensingh. Importantly, thisprobably also counts for infections with cross-reacting bacteria, which results in higherFPSR prevalence and titers and consequently a lower specificity. This can explain whyat a certain iELISA cut-o! all three tests show a low specificity at the government farmwhen we compare this to the estimates in the Mymensingh area. It demonstrates thatthe test characteristics depend on the area in which the tests are used, and constancy oftest characteristics cannot be assumed.Hence, there is reason to recommend using a higher iELISA cut-o! at the governmentfarm compared to the Mymensingh area. Because the sensitivity remains around 92% andthe specificity reaches above 99%, a cut-o! of 5 IU/ml seems the most appropriate in theMymensingh area. At the government farm, a cut-o! value of 12.5 IU/ml appears moreappropriate, because a specificity of 99% is only reached from this point onward whilethe sensitivity remains around 92%. To avoid the FPSR problem, we therefore suggestto use the results obtained with the covariance model at an iELISA cuto! of 5 IU/mlin the Mymensingh area and 12.5 IU/ml at the government farm. This means we mightassume the iELISA results between 2- and 5 IU/ml in the Mymensingh area and 2- and12.5 IU/ml at the government farm are false positive serological reactions due to crossreacting antibodies.
Further research is necessary to understand why we find such dramatic di!erences iniELISA titers, test characteristics and antibody prevalence between the Mymensingh areaand the government farm and to find the most appropriate iELISA cut-o! value. Overall,it would be beneficial to further investigate and improve the diagnostic capabilities, es-pecially since FPSR still interfere in serological diagnosis. In addition, further research isnecessary to find the origin of the FPSR and the absence of correlation between abortionand Brucella infection.
Page 56

References
Abcam, http://www.abcam.com
Abertnethy D.A., Menzies F.D., McCullough S.J., McDowell S.W.J., Burns K.E., WattR., Gordon A.W., Greiner M., Pfei!er D.U., 2012. Field trail of six serological tests forbovine brucellosis. The Veterinary Journal 191, 364-370
Adams L.G., 2002. The pathology of brucellosis reflects the outcome of the battle betweenthe host genome and the Brucella genome. Veterinary Microbiology 90, 553-561
Alton G., Jones L., Angus R., Verger J., 1988. Techniques for the brucellosis laboratory.1st edn. Tech. rep., Institut National de la Recherche Agronomique, Paris. Referred toin Lopez-Goni and O’Callaghan, 2012
Amin K.M.R., Rahman M.B., Rahman M.S., Han J.C., Park J.H., Chae J.S., 2005.Prevalence of Brucella antibodies in sera of cows in Bangladesh. Journal of VeterinaryScience 6(3), 223-226
Berkvens D., Speybroeck N., Praet N., Adel A., Lesa!re E., 2006. Estimating diseaseprevalence in a Bayesian framework using probabilistic constraints. Epidemiology 17,145-153
Boschiroli M.L., Foulonge V., OCallaghan D., 2001. Brucellosis: a worldwide zoono-sis. Current Opinion in Microbiology 4, 58-64
Corbel M.J., 1973. Identification of the immunoglobulin class active in the Rose Ben-gal plate test for bovine brucellosis. The Journal of Hygiene 70, 779-795. Referred to inNielsen, 2002
Corbel M.J., 1985. Recent advances in the study of Brucella antigens and their sero-logical cross reactions. Veterinary Bulletin 55, 927-942. Referred to in Megersa et al.,2012.
Corbel M.J., 1997. Brucellosis; an overview. Emerging Infectious Diseases 3, 213-221
Cringoli G., Rinaldi L., Veneziano V., Capelli G., Malone J., 2002. A cross-sectionalcoprological survey of liver flukes in cattle and sheep from an area of southern ItalianApennines. Veterinary Parasitology 108, 137-143
Cutler S.J., Whatmore A.M., Commander N.J., 2005. Brucellosis: new aspects of an
57

old disease. Journal of Applied Microbiology 98, 1270-1281
Dajer A., Luna-Martınez E., Zapata D., Villegas S., Gutierrez E., Pena G., Gurrıa F.,Nielsen K., Gall D., 1999. Evaluation of a fluorescence-polarization assay for the diagnosisof bovine brucellosis in Mexico. Preventive Veterinary Medicine 40, 67-73
Davis G., 1971. The Rose Bengal Test. Veterinary Research 88, 447-449. From Nielsen,2002
Dean A.S., Crump L., Greter H., Hattendorf J., Schelling E., Zinsstag J., 2012. Clin-ical manifestations of human brucellosis: A systematic review and meta-analysis. PLOSNeglected tropical diseases 6(12), e1929
Dendukuri N. and Joseph L., 2001. Bayesian approaches to modeling the conditionaldependence between multiple diagnostic tests. Biometrics 57, 208-217
Dohoo I., Martin W., Stryhn H., 2003. Screening and diagnostic tests. In: VeterinaryEpidemiologic Research, 85-120
Dohoo I.R., Wright P.F., Ruckerbauer G.M., Samagh B.S., Robertson F.J., Forbes L.B.,1986. A comparison of five serological tests for bovine brucellosis. Canadian Journal ofVeterinary Research 50, 485-493
England T., Kelly L., Jones R., MacMillian A., Wooldridge M., 2004. A simulationmodel of brucellosis spread in Brittish cattle under several testing regimes. PreventiveVeterinary Medicine 63, 63-73
Ewalt D.R., Payeur J.B., Rhyan J.C., Geer P.L., 1997. Brucella suis biovar 1 in nat-urally infected cattle; a bacteriological, serological and histological study. Journal ofVeterinary Diagnostic Investigation 9, 417-420
Foster G., Osterman B.S., Godfroid J., Jacques I., Cloeckaert A., 2007. Brucella cetisp.nov. and Brucella pinnipedialis sp.nov. for Brucella strains with cetaceans and sealsas their preferred hosts. International Journal of Systematic and Evolutionary Microbi-ology 57, 2688-2693
Gadaga B., 2013. A survey of brucellosis and bovine tuberculosis in humans at a wildlife/domestic animal/human interface in Zimbabwe. Research platform - Production and con-servation in partnership (RP-PCP).
Gardner I.A., Stryhn H., Lind P., Collins M.T., 2000. Conditional dependence betweentests a!ects the diagnosis and surveillance of animal diseases. Preventive VeterinaryMedicine 45, 107-122
Garin B., Trap D., Gaumont R., 1985. Assessment of EDTA seroagglutination test forthe diagnosis of bovine brucellosis. Veterinary Record 117, 444-445
Garrity G.M., 2001. Bergeys Manual of Systematic Bacteriology, second ed. Springer,
Page 58

New York, 721
Gerbier G., Garin-Bastuji B., Pouillot R., Very P., Cau C., Berr V., Dufour B., MoutouF., 1997. False positive serological reactions in bovine brucellosis: evidence of the role ofYersinia enterocolitica serotype O:9 in a field trail. Veterinary Research 28, 375-383
Godfroid J., Nielsen K., Saegerman C., 2010. Diagnosis of brucellosis in livestock andwildlife. Croatian Medical Journal 51(4), 296-305
Godfroid J., Saegerman C., Wellemans V., Walravens K., Letesson J.J., Tibor A., MacMil-lan A., Spencer S., Sanaa M., Bakker D., Pouillot R., Garin-Bastuji B., 2002. How tosubstantiate the freedom of bovine brucellosis when aspecific serological reactions emergein brucellosis test? Veterinary Microbiology 90, 461-477
Godfroid J., Scholz H.C., Barbier T., Nicolas C., Wattiau P., Fretin D., WhatmoreA.M., Cloeckaert A., Blasco J.M., Moriyon I., Saegerman C., Muma J.B., Al DahoukS., Neubauer H., Letesson J.J., 2011. Brucellosis at the animal/ecosystem/human inter-face at the beginning of the 21st century. Preventive veterinary medicine 102, 118-131
Gorvel J.P., 2008. Brucella: a Mr. “Hide” converted into Dr Jekyll. Microbes andInfection 48, 1461-1464
Greiner M., Gardner I.A., 2000. Epidemiological issues in the validation of veterinarydiagnostic tests. Preventive Veterinary Medicine 45, 3-22
Hadorn D.C., Stark K.D.C., 2008. Evaluation and optimization of surveillance systemsfor rare and emerging infectious diseases. Veterinary Research 39(6)
He Y., 2012. Analysis of Brucella pathogenesis, host immunity, and vaccine targets usingsystems biology and bioinformatics. Frontiers in cellular and infection microbiology 2, 2
Hort G.M., Weisenburger J., Borsdorf B., Peters C., Banai M., Hahn H., Jacob J., MielkeM.E.A., 2003. Delayed type of hypersensitivity-associated disruption of splenic periarte-riolar lymphatic sheats coincides with temporary loss of IFN-! production an impairederadication of bacteria in Brucella abortus-infected mice. Microbes and Infection 5, 95-106
Hui S.L., Walter S.D., 1980. Estimating the error rates of diagnostic tests. Biomet-rics 36, 167-171
Johnson W.O., Gastwirth J.L., Pearson L.M., 2000. Screening without a Gold Standard:The Hui and Walter Paradigm Revisited. American Journal of Epidemiology 153, 921-924
Kapperud G., 1991. Yersinia enterocolitica in food hygiene. International Journal ofFood Microbiology 12, 53-66
Limet J., Kerkhofs P., Wij!els R., Dekeyser P., 1988. Le diagnostic serologique de labrucellose bovine par ELISA. Annales de Medicine Veterinaire 132, 565-575
Page 59

Lopez-Goni I., O’Callaghan D., 2012. Brucella molecular microbiology and genomics.Caister Academic Press, Norfolk, UK.
Lord V.R., Rolo M.R., Cherwonogrodzky J.W., 1989. Evaluation of humoral immu-nity to Brucella spp. in cattle by use of an agar-gel immunodi!usion test containing apolysaccharide antigen. American Journal of Veterinary Research 11, 1813- 1816
Mainar-jaime R.C., Munoz P.M., de Miguel M.J., Grillo M.J., Marın C.M., MoriyonI., Blasco J.M., 2005. Specificity dependence between serological tests for diagnosingbovine brucellosis in Brucella-free farms showing false positive serological reactions dueto Yersinia enterocolitica O:9. Canadian Veterinary Journal 46, 913-916
McDermott J.J. and Arimi S.M., 2002. Brucellosis in sub-Saharan Africa: epidemiol-ogy, control and impact. Veterinary Microbiology 90, 111-134.
Megersa B., Bi!a D., Abunna F., Regassa A., Godfroid J., Skjerve E., 2012. Sero-epidemiological study of livestock brucellosis in a pastoral region. Epidemiology andInfection 140, 887-896
Moriyon I., Grillo M.J., Monreal D., Gonzalez D., Marin C., Lopez-Goni I., Mainar-JaimeR.C., Moreno E., Blasco J.M., 2004. Rough vaccines in animal brucellosis: structural andgenetic basis and present status. Veterinary Research 35, 1-38
Muma J.B., Samui K.L., Oloya J., Munyeme M., Skjerve E., 2007. Risk factors forbrucellosis in indigenous cattle reared in livestock-wildlife interface areas of Zambia. Pre-ventive Veterinary Medicine 80, 306-317
Muma J.B., Toft N., Oloya J., Lund A., Nielsen K., Samui K., Skjerve E., 2007. Evalua-tion of three serological tests for brucellosis in naturally infected cattle using latent classanalysis. Veterinary Microbiology 125, 187-192
Munoz P.M., Marn C.M., Monreal D., Gonzlez D., Garin-Bastuji B., Daz R., Mainar-Jaime R.C., Moriyn I., Blasco J.M., 2005. E"cacy of several serological tests and Anti-gens for diagnosis of bovine brucellosis in the presence of false-positive serological resultsdue to Yersinia enterocolitica O:9. Clinical and Diagnostic Laboratory Immunology 12(1),141-151
Neta A.V.C., Mol J.P.S., Xavier M.N., Paixao T.A., Lage A.P., Santos R.L., 2010. Patho-genesis of bovine brucellosis. The Veterinary Journal 184, 146-155
Nielsen K., 2002. Diagnosis of brucellosis by serology. Veterinary Microbiology 90, 447-459
Nielsen K. and Gall D., 2001. Fluorescence polarization assay for the diagnosis of brucel-losis: A review. Journal of Immunoassay and Immunochemistry 22(3), 183-201
Nielsen K., Heck F., Wagner G., Stiller J., Rosenbaum B., Pugh R., Flores E., 1984.Comparative assessment of antibody isotypes to Brucella abortus by primary and sec-ondary binding assays. Preventive Veterinary Medicine 2, 197-204. Referred to in OIE,
Page 60

2009
Nielsen K., Smith P., Yu W., Nicoletti P., Jurgersen G., Stack J., Godfroid J., 2006. Sero-logical discrimination by indirect enzyme immunoassay between the antibody response toBrucella spp. and Yersinia enterocolitica O:9 in cattle and pigs. Veterinary Immunologyand Immunopathology 109, 69-78
OIE, Manual of standards for diagnostic tests and vaccines. Bovine brucellosis. Paris:O"ce International de Epizooties (OIE), 2009
Olsen S.C., Hennager S.G., 2010. Immune responses and protection against experimentalBrucella suis biovar 1 challenge in non-vaccinated or B. abortus strain RB51-vaccinatedcattle. Clinical and Vaccine Immunology 17, 1891-1895
Osterman B., and Moriyon I., 2006. International Committee on Systematics of Prokary-otes Subcommittee in the taxonomy of Brucella, International Journal of Systematic andEvolutionary Microbiology 56, 1173-1175
Pappas G., Papadimitriou P., Akritidi N., Christou L., Tsianos E.V., 2006. The newglobal map of human brucellosis. The Lancet Infectious Diseases 6, 91-99
Pappas G., Panagopoulou P., Christou L., Akritidis N., 2006. Brucella as a biologi-cal weapon. Cellular and Molecular Life Sciences 63, 2229-2236
Rahman A.K.M., Abatih E., Saegerman C., Fretin D., Ahmed M.U., Shamsuddin M.,Praet N., Speybroeck N., Berkvens D., unpublished. Bayesian estimation of the true ex-posure prevalence, sensitivity and specificity of three serological tests for the diagnosis ofbovine brucellosis in Bangladesh.
Rahman A.K.M., Berkvens D., Fretin D., Saegerman C., Ahmed M.U., Muhammad N.,Hossain A., Abatih E., 2012. Seroprevalence and risk factors for brucellosis in high-riskgroup of individuals in Bangladesh. Foodborn Pathogens and Disease 9(3), 190-197
Rahman M.S., Faruk M.O., Her M., Kim J.Y., Kang S.I., Jung S.C., 2011. Prevalence ofbrucellosis in ruminants in Bangladesh. Veterinarni Medicina 56 (8), 379-385
Rahman M.S., Her M., Kim J.Y., Kang S.I., Lee K., Uddin M.J. Chakrabartty A., JungS.C., 2012. Brucellosis among ruminants in some districts of Bangladesh using four con-ventional serological assays. African Journal of Microbiology Research 6 (22), 4775-4781
Rahman M.S., Nuruzzaman M., Ahasan M.S., Sarker S.S., Chakrabartty A., Nahar A.,Uddin M.J., Sarker M.A.S., Akhter L., 2012. Prevalence of brucellosis in pigs: The firstreport in Bangladesh. Bangladesh Journal of Veterinary Medicine 10(1&2), 75-80
Renukaradhya G.J., Isloor S., Rajasekhar M., 2002. Epidemiology, zoonotic aspects,vaccination and control/eradication of brucellosis in India. Veterinary Microbiology 90,183-195
Page 61

Rogan W.J. and Gladen B., 1978. Estimating prevalence from the results of a screeningtest. American Journal of Epidemiology 107, 71-76
Roth F., Zinsstag J., orkhon D., Chimed-Ochir G., Hutton G., 2003. Human healthbenefits from livestock vaccination for brucellosis: Case study. Bulletin of the WorldHealth Organization 81, 867-876
Saegerman C., De Waele L., Gilson D., Godfroid J., Thiange P., Michel P., LimbourgD., Vo T.K.-O., Limet J., Leteson J.J., Berkvens D., 2004. Evaluation of the serumi-ELISA using monoclonal antibodies and protein G as peroxidase conjugate for the di-agnosis of bovine brucellosis. Veterinary Microbiology 100, 91-105
Saegerman C., Vo T.K.O., De Waele L., Gilson D., Bastin A., Dubray G., FlanaganP., Limet J.N., Letesson J.J., Godfroid J., 1999. Diagnosis of bovine brucellosis by skintest: conditions for the test and evaluation of its performance. Veterinary Record 145(8), 214-218
Samaha H., Al-Rowaily M., Khoudair R.M., Ashour H.M., 2008. Multicenter study ofbrucellosis in Egypt. Emerging Infectious Diseases 14, 1916-1918.
Samartino L., Gregoret R., Gall D., Nielsen K., 1999. Fluorescence polarization assay:Application to the diagnosis of bovine brucellosis in Argentina. Journal of Immunoassay20(3), 115-126
Scholz H.C., Hubalek Z., Sedlacek I., Vergnaud G., Tomaso H., Al Dahouk S., MelzerF., Kampfer P., Neubauer H., Cloeckaert A., Maquart M., Huber B., Busse H.J., NocklerK., 2008. Brucella microti sp.nov., isolated from the common vole Microtus arvalis. In-ternational Journal of Systematic and Evolutionarry Microbiology 58, 375-382
Scholz H.C., Nockler K., Gollner C., Bahn P., Vergnaud G., Tomaso H., Al DahoukS., Kampfer P., Cloeckaert A., Maquart M., Zygmunt M.S., Whatmore A.M., Pfe!er M.,Huber B., Busse H.J., De B.K., 2010. Brucella inopinata sp.nov., isolated from a breastimplant infection. International Journal of Systematic and Evolutionary Microbiology 60,801-808
Schurig G.G., Roop R.M., Buhrman D., Boyle S., Bagchi T., Sriranganathan N., 1991.Biological properties of RB51, a stable O-chain deficient mutant of Brucella abortus. Vet-erinary Microbiology 28, 171-188
Spiegelhalter D.J., Best N.G., Carlin B.P., van der Linde A., 2002. Bayesian measures ofmodel complexity and fit (with discussion). Journal of the Royal Statistical Society B 64,583-640.
Spiegelhalter D., Thomas A., Best N., Lunn D., 2003. WinBUGS Version 1.4 User Man-ual. MRC Biostatistics Unit, Cambridge
StataCorp, 2011. Stata: Release 12. Statistical Software. College Station, TX. Stat-aCorp LP
Page 62

Stemshorn B.W., Forbes L.B. Eaglesome M.D., Nielsen K.H, Robertson F.J., SamaghB.S., 1985. A comparison of standard serological tests for the diagnosis of bovine brucel-losis in Canada. Canadian Journal of Comparative Medicine 49, 391-394
Sto!regen W.C., Olsen S.C., Wheeler C.J., Bricker B.J., Palmer M.V., Jensen A.E.,Halling S.M., Alt D.P., 2007. Diagnostic characterization of a feral swine herd enzooti-cally infected with Brucella. Journal of Veterinary Diagnostic Investigation 19, 227-237
The center for food security and public health, Iowa state university, 2009. Bovine bru-cellosis: Brucella abortus. http://www.cfsph.iastate.edu
Thrusfield D., 1995. Veterinary Epidemiology. Oxford University Press, Oxford.
Uzal F.A., Carrasco A.E., Nielsen K., Echaide S., Cabrera R.F., 1996. An indirect ELISAusing a monoclonal anti IgG1 enzyme conjugate for the diagnosis of bovine brucellosis.Veterinary Microbiology 52, 175-180
Van Aert A., Brioen P., Dekeyser P., Uytterhaegen L., Sijens R.J., Boeye A., 1984. Acomparative study of ELISA and other methods for the detection of Brucella antibodiesin bovine sera. veretrinary Microbiology 10, 13-21
Verger J.M., Grimont F., Grimont P.A.D., Grayon M., 1985. Brucella, a monospecificgenus as shown by deoxyribonucleic acid hybridization. International Journal of System-atic Bacteriology 35, 292-295. Referred to in Lopez-Goni and O’Callaghan, 2012
World Health Organization (WHO). Brucellosis in humans and animals. Geneva, Swit-serland: WHO Press, 2006
Young E.J., 1995. An overview of human brucellosis. Clinical Infectious Diseases 21,283-289
Page 63

Appendices
64

1 Hui and Walter scheme - deterministic estimation
1 hw = function ( p111 , p110 , p101 , p100 , p211 , p210 , p201 , p200 )2 {3 ## p111 . . . p200 = FREQUENTIES4 p1ss = p111+p110+p101+p100 ; p2ss = p211+p210+p201+p2005 p111 = p111/p1ss ; p110 = p110/p1ss ; p101 = p101/p1ss ; p100 = p100/
p1ss6 p211 = p211/p2ss ; p210 = p210/p2ss ; p201 = p201/p2ss ; p200 = p200/
p2ss7 p11s = p111+p110 ; p1s1 = p111+p101 ; p10s = p101+p100 ; p1s0 = p110+
p1008 p21s = p211+p210 ; p2s1 = p211+p201 ; p20s = p201+p200 ; p2s0 = p210+
p2009 d1 = sqrt ( ( p11s!p2s1 ! p21s!p1s1 + p111 ! p211 ) ˆ2 ! 4! ( p11s!p21s )! (
p111!p2s1 ! p211!p1s1 ) )10 d2 = !d111
12 prev1a = 0.5+( p11s! ( p1s1!p2s1 )+p1s1! ( p11s!p21s )+p211!p111 )/(2!d1 )13 prev1b = 0.5+( p11s! ( p1s1!p2s1 )+p1s1! ( p11s!p21s )+p211!p111 )/(2!d2 )14 prev2a = 0.5+( p21s! ( p1s1!p2s1 )+p2s1! ( p11s!p21s )+p211!p111 )/(2!d1 )15 prev2b = 0.5+( p21s! ( p1s1!p2s1 )+p2s1! ( p11s!p21s )+p211!p111 )/(2!d2 )16 se1a = 1!(p1s0!p20s!p10s!p2s0 + p100 ! p200 + d1 )/(2! ( p2s1!p1s1 ) )17 se1b = 1!(p1s0!p20s!p10s!p2s0 + p100 ! p200 + d2 )/(2! ( p2s1!p1s1 ) )18 sp1a = 1!(p11s!p2s1 ! p1s1!p21s + p211 ! p111 + d1 )/(2! ( p2s1!p1s1 ) )19 sp1b = 1!(p11s!p2s1 ! p1s1!p21s + p211 ! p111 + d2 )/(2! ( p2s1!p1s1 ) )20 se2a = 1!(p2s0!p10s ! p20s!p1s0 + p100 ! p200 + d1 )/(2! ( p21s!p11s ) )21 se2b = 1!(p2s0!p10s ! p20s!p1s0 + p100 ! p200 + d2 )/(2! ( p21s!p11s ) )22 sp2a = 1!(p21s!p1s1 ! p2s1!p11s + p211 ! p111 + d1 )/(2! ( p21s!p11s ) )23 sp2b = 1!(p21s!p1s1 ! p2s1!p11s + p211 ! p111 + d2 )/(2! ( p21s!p11s ) )24
25 print ( ” F i r s t s o l u t i o n ” , quote=F)26 print (paste ( ”Preva lence 1 : ” , s p r i n t f ( ”\%6.4 f ” , prev1a ) ) , quote=F)27 print (paste ( ”Preva lence 2 : ” , s p r i n t f ( ”\%6.4 f ” , prev2a ) ) ,quote=F)28 print (paste ( ” S e n s i t i v i t y 1 : ” , s p r i n t f ( ”\%6.4 f ” , se1a ) ) ,quote=F)29 print (paste ( ” S p e c i f i c i t y 1 : ” , s p r i n t f ( ”\%6.4 f ” , sp1a ) ) ,quote=F)30 print (paste ( ” S e n s i t i v i t y 2 : ” , s p r i n t f ( ”\%6.4 f ” , se2a ) ) ,quote=F)31 print (paste ( ” S p e c i f i c i t y 2 : ” , s p r i n t f ( ”\%6.4 f ” , sp2a ) ) ,quote=F)32 print ( ”” ,quote=F)33 print ( ” Secondso lut ion ” ,quote=F)34 print (paste ( ”Preva lence 1 : ” , s p r i n t f ( ”\%6.4 f ” , prev1b ) ) ,quote=F)35 print (paste ( ”Preva lence 2 : ” , s p r i n t f ( ”\%6.4 f ” , prev2b ) ) ,quote=F)36 print (paste ( ” S e n s i t i v i t y 1 : ” , s p r i n t f ( ”\%6.4 f ” , se1b ) ) ,quote=F)37 print (paste ( ” S p e c i f i c i t y 1 : ” , s p r i n t f ( ”\%6.4 f ” , sp1b ) ) ,quote=F)38 print (paste ( ” S e n s i t i v i t y 2 : ” , s p r i n t f ( ”\%6.4 f ” , se2b ) ) ,quote=F)39 print (paste ( ” S p e c i f i c i t y 2 : ” , s p r i n t f ( ”\%6.4 f ” , sp2b ) ) ,quote=F)40 }
Page 65

2 Hui andWalter scheme (iELISA (cut-o! 7.5 IU/ml)and RBT) - probabilistic estimation
1 l i s t ( r1=c (1 , 3 , 8 , 1008) , n1=1020 , r2=c (47 ,13 ,15 ,265) , n2 = 340)2 Model{3 r1 [ 1 : 4 ] ˜ dmulti ( p1 [ 1 : 4 ] , n1 )4 p1 [ 1 ]<!prev [ 1 ] !se [ 1 ] !se [ 2 ] + (1!prev [ 1 ] ) !(1!sp [ 1 ] ) !(1!sp [ 2 ] )5 p1 [ 2 ]<!prev [ 1 ] !se [ 1 ] !(1!se [ 2 ] ) + (1!prev [ 1 ] ) !(1!sp [ 1 ] ) !sp [ 2 ]6 p1 [ 3 ]<!prev [ 1 ] !(1!se [ 1 ] ) !se [ 2 ] + (1!prev [ 1 ] ) !sp [ 1 ] !(1!sp [ 2 ] )7 p1 [ 4 ]<!prev [ 1 ] !(1!se [ 1 ] ) !(1!se [ 2 ] ) + (1!prev [ 1 ] ) !sp [ 1 ] !sp [ 2 ]8 r2 [ 1 : 4 ] ˜ dmulti ( p2 [ 1 : 4 ] , n2 )9 p2 [ 1 ]<!prev [ 2 ] !se [ 1 ] !se [ 2 ] + (1!prev [ 2 ] ) !(1!sp [ 1 ] ) !(1!sp [ 2 ] )
10 p2 [ 2 ]<!prev [ 2 ] !se [ 1 ] !(1!se [ 2 ] ) + (1!prev [ 2 ] ) !(1!sp [ 1 ] ) !sp [ 2 ]11 p2 [ 3 ]<!prev [ 2 ] !(1!se [ 1 ] ) !se [ 2 ] + (1!prev [ 2 ] ) !sp [ 1 ] !(1!sp [ 2 ] )12 p2 [ 4 ]<!prev [ 2 ] !(1!se [ 1 ] ) !(1!se [ 2 ] ) + (1!prev [ 2 ] ) !sp [ 1 ] !sp [ 2 ]13 prev [ 1 ] ˜dbeta ( 1 , 1 )14 prev [ 2 ] ˜dbeta ( , 1 )15 se [ 1 ] ˜dbeta ( 1 , 1 )16 sp [ 1 ] ˜dbeta ( 1 , 1 )17 se [ 2 ] ˜dbeta ( 1 , 1 ) I ( 0 . 5 , 1 )18 sp [ 2 ] ˜dbeta ( 1 , 1 ) I ( 0 . 5 , 1 )19 r3 [ 1 : 4 ] ˜dmulti ( p1 [ 1 : 4 ] , n1 )20 for ( i in 1 : 4 )21 {22 d1 [ i ] <! r1 [ i ] !log (max( r1 [ i ] , 1 )/ ( p1 [ i ] !n1 ) )23 d2 [ i ] <! r3 [ i ] !log (max( r3 [ i ] , 1 )/ ( p1 [ i ] !n1 ) )24 }25 G01 <! 2!sum( d1 [ ] )26 Gt1 <! 2!sum( d2 [ ] )27 bayesp [ 1 ] <! step (G01 ! Gt1)28 r4 [ 1 : 4 ] ˜dmulti ( p2 [ 1 : 4 ] , n2 )29 for ( i in 1 : 4 )30 {31 d3 [ i ] <! r2 [ i ] !log (max( r2 [ i ] , 1 )/ ( p2 [ i ] !n2 ) )32 d4 [ i ] <! r4 [ i ] !log (max( r4 [ i ] , 1 )/ ( p2 [ i ] !n2 ) )33 }34 G02 <! 2!sum( d3 [ ] )35 Gt2 <! 2!sum( d4 [ ] )36 bayesp [ 2 ] <! step (G02 ! Gt2)37 bayesp [ 3 ] <! step (G01 + G02 ! Gt1 ! Gt2)
Page 66

3 Conditional independance (Mymensingh - iELISAcut-o! 7.5 IU/ml)
1 l i s t ( r1=c ( 1 , 0 , 1 , 2 , 1 , 7 , 10 , 998 ) , N=1020)2 Model{3 r1 [ 1 : 8 ] ˜ dmulti (p [ 1 : 8 ] ,N)4 p [ 1 ]<!prev!se [ 1 ] !se [ 2 ] !se [ 3 ] + (1!prev )!(1!sp [ 1 ] ) !(1!sp [ 2 ] ) !(1!sp [ 3 ] )5 p [ 2 ]<!prev!se [ 1 ] !se [ 2 ] !(1!se [ 3 ] ) + (1!prev )!(1!sp [ 1 ] ) !(1!sp [ 2 ] ) !sp [ 3 ]6 p [ 3 ]<!prev!se [ 1 ] !(1!se [ 2 ] ) !se [ 3 ] + (1!prev )!(1!sp [ 1 ] ) !sp [ 2 ] !(1!sp [ 3 ] )7 p [ 4 ]<!prev!se [ 1 ] !(1!se [ 2 ] ) !(1!se [ 3 ] ) + (1!prev )!(1!sp [ 1 ] ) !sp [ 2 ] !sp [ 3 ]8 p [ 5 ]<!prev!(1!se [ 1 ] ) !se [ 2 ] !se [ 3 ] + (1!prev )!sp [ 1 ] !(1!sp [ 2 ] ) !(1!sp [ 3 ] )9 p [ 6 ]<!prev!(1!se [ 1 ] ) !se [ 2 ] !(1!se [ 3 ] ) + (1!prev )!sp [ 1 ] !(1!sp [ 2 ] ) !sp [ 3 ]
10 p [ 7 ]<!prev!(1!se [ 1 ] ) !(1!se [ 2 ] ) !se [ 3 ] + (1!prev )!sp [ 1 ] !sp [ 2 ] !(1!sp [ 3 ] )11 p [ 8 ]<!prev!(1!se [ 1 ] ) !(1!se [ 2 ] ) !(1!se [ 3 ] ) + (1!prev )!sp [ 1 ] !sp [ 2 ] !sp [ 3 ]12 prev˜dbeta ( 1 , 1 ) I ( 0 , 0 . 5 ) ## symmetry13 se [ 1 ] ˜dbeta ( 1 , 1 )14 sp [ 1 ] ˜dbeta ( 1 , 1 )15 se [ 2 ] ˜dbeta ( 1 , 1 )16 sp [ 2 ] ˜dbeta ( 1 , 1 )17 se [ 3 ] ˜dbeta ( 1 , 1 )18 sp [ 3 ] ˜dbeta ( 1 , 1 )19 r2 [ 1 : 8 ] ˜dmulti (p [ 1 : 8 ] ,N)20 for ( i in 1 : 8 )21 {22 d1 [ i ] <! r1 [ i ] !log (max( r1 [ i ] , 1 )/ (p [ i ] !N) )23 d2 [ i ] <! r2 [ i ] !log (max( r2 [ i ] , 1 )/ (p [ i ] !N) )24 }25 G0 <! 2!sum( d1 [ ] )26 Gt <! 2!sum( d2 [ ] )27 bayesp <! step (G0 ! Gt)28 }
Page 67

4 Conditional dependence - Covariance scheme(Mymensingh - iELISA cut-o! 7.5 IU/ml)
1 model2 {3 r [ 1 : 8 ] ˜ dmulti (p [ 1 : 8 ] , n )4 ## p [ 1 ] = p (111) ; p [ 8 ] = p (000) ; pr = true preva l ence ; a i j k = sigma ; b i j k
= sigmaˆprime5
6 p [ 1 ] <! pr! ( se [ 1 ] !se [ 2 ] !se [3 ]+ se [ 1 ] !a23+se [ 2 ] !a13+se [ 3 ] !a12+a123 ) + (1!pr )!((1! sp [ 1 ] ) !(1!sp [ 2 ] ) !(1!sp [ 3 ] ) +(1!sp [ 1 ] ) !b23+(1!sp [ 2 ] ) !b13+(1!sp [ 3 ] ) !b12!b123 )
7
8 p [ 2 ] <! pr! ( se [ 1 ] !se [ 2 ] !(1!se [ 3 ] )!se [ 1 ] !a23!se [ 2 ] !a13+(1!se [ 3 ] ) !a12!a123 ) +(1!pr )!((1! sp [ 1 ] ) !(1!sp [ 2 ] ) !sp [3]!(1! sp [ 1 ] ) !b23!(1!sp [ 2 ] ) !b13+sp [ 3 ] !b12
+b123 )9
10 p [ 3 ] <! pr! ( se [ 1 ] !(1!se [ 2 ] ) !se [3]! se [ 1 ] !a23+(1!se [ 2 ] ) !a13!se [ 3 ] !a12!a123 ) +(1!pr )!((1! sp [ 1 ] ) !sp [ 2 ] !(1!sp [ 3 ] )!(1!sp [ 1 ] ) !b23+sp [ 2 ] !b13!(1!sp [ 3 ] ) !b12
+b123 )11
12 p [ 4 ] <! pr! ( se [ 1 ] !(1!se [ 2 ] ) !(1!se [ 3 ] )+se [ 1 ] !a23!(1!se [ 2 ] ) !a13!(1!se [ 3 ] ) !a12+a123 ) + (1!pr )!((1! sp [ 1 ] ) !sp [ 2 ] !sp [3]+(1! sp [ 1 ] ) !b23!sp [ 2 ] !b13!sp [ 3 ] !b12!b123 )
13
14 p [ 5 ] <! pr!((1!se [ 1 ] ) !se [ 2 ] !se [3]+(1! se [ 1 ] ) !a23!se [ 2 ] !a13!se [ 3 ] !a12!a123 ) +(1!pr )! ( sp [ 1 ] !(1!sp [ 2 ] ) !(1!sp [ 3 ] )+sp [ 1 ] !b23!(1!sp [ 2 ] ) !b13!(1!sp [ 3 ] ) !b12
+b123 )15
16 p [ 6 ] <! pr!((1!se [ 1 ] ) !se [ 2 ] !(1!se [ 3 ] )!(1!se [ 1 ] ) !a23+se [ 2 ] !a13!(1!se [ 3 ] ) !a12+a123 ) + (1!pr )! ( sp [ 1 ] !(1!sp [ 2 ] ) !sp [3]! sp [ 1 ] !b23+(1!sp [ 2 ] ) !b13!sp [ 3 ] !b12!b123 )
17
18 p [ 7 ] <! pr!((1!se [ 1 ] ) !(1!se [ 2 ] ) !se [3]!(1! se [ 1 ] ) !a23!(1!se [ 2 ] ) !a13+se [ 3 ] !a12+a123 ) + (1!pr )! ( sp [ 1 ] !sp [ 2 ] !(1!sp [ 3 ] )!sp [ 1 ] !b23!sp [ 2 ] !b13+(1!sp [ 3 ] ) !b12!b123 )
19
20 p [ 8 ] <! pr!((1!se [ 1 ] ) !(1!se [ 2 ] ) !(1!se [ 3 ] ) +(1!se [ 1 ] ) !a23+(1!se [ 2 ] ) !a13+(1!se[ 3 ] ) !a12!a123 ) + (1!pr )! ( sp [ 1 ] !sp [ 2 ] !sp [3 ]+ sp [ 1 ] !b23+sp [ 2 ] !b13+sp [ 3 ] !b12+b123 )
21
22 pr ˜ dbeta ( 1 , 1 ) I ( 0 , 0 . 5 )23 se [ 1 ] ˜ dbeta ( 1 , 1 )24 se [ 2 ] ˜ dbeta ( 1 , 1 )25 se [ 3 ] ˜ dbeta ( 1 , 1 )26 sp [ 1 ] ˜ dbeta ( 1 , 1 )27 sp [ 2 ] ˜ dbeta ( 1 , 1 )28 sp [ 3 ] ˜ dbeta ( 1 , 1 )29 l l 1 <! max(!(1!se [ 1 ] ) !(1!se [ 2 ] ) , !se [ 1 ] !se [ 2 ] )30 ul1 <! min( se [ 1 ] !(1!se [ 2 ] ) ,(1! se [ 1 ] ) !se [ 2 ] )31 a12 ˜ dunif ( l l 1 , u l1 )32 l l 2 <! max(!(1!se [ 1 ] ) !(1!se [ 3 ] ) , !se [ 1 ] !se [ 3 ] )33 ul2 <! min( se [ 1 ] !(1!se [ 3 ] ) ,(1! se [ 1 ] ) !se [ 3 ] )34 a13 ˜ dunif ( l l 2 , u l2 )35 l l 3 <! max(!(1!se [ 2 ] ) !(1!se [ 3 ] ) , !se [ 2 ] !se [ 3 ] )36 ul3 <! min( se [ 2 ] !(1!se [ 3 ] ) ,(1! se [ 2 ] ) !se [ 3 ] )
Page 68

37 a23 ˜ dunif ( l l 3 , u l3 )38 l l 4 <! max(!(1!sp [ 1 ] ) !(1!sp [ 2 ] ) , !sp [ 1 ] !sp [ 2 ] )39 ul4 <! min( sp [ 1 ] !(1!sp [ 2 ] ) ,(1! sp [ 1 ] ) !sp [ 2 ] )40 b12 ˜ dunif ( l l 4 , u l4 )41 l l 5 <! max(!(1!sp [ 1 ] ) !(1!sp [ 3 ] ) , !sp [ 1 ] !sp [ 3 ] )42 ul5 <! min( sp [ 1 ] !(1!sp [ 3 ] ) ,(1! sp [ 1 ] ) !sp [ 3 ] )43 b13 ˜ dunif ( l l 5 , u l5 )44 l l 6 <! max(!(1!sp [ 2 ] ) !(1!sp [ 3 ] ) , !sp [ 2 ] !sp [ 3 ] )45 ul6 <! min( sp [ 2 ] !(1!sp [ 3 ] ) ,(1! sp [ 2 ] ) !sp [ 3 ] )46 b23 ˜ dunif ( l l 6 , u l6 )47 l l 7 1 <! !(se [ 1 ] !se [ 2 ] !se [3 ]+ se [ 1 ] !a23+se [ 2 ] !a13+se [ 3 ] !a12 )48 l l 7 2 <! !((1!se [ 1 ] ) !(1!se [ 2 ] ) !se [3]!(1! se [ 1 ] ) !a23!(1!se [ 2 ] ) !a13+se [ 3 ] !a12 )49 l l 7 3 <! !((1!se [ 1 ] ) !se [ 2 ] !(1!se [ 3 ] )!(1!se [ 1 ] ) !a23+se [ 2 ] !a13!(1!se [ 3 ] ) !a12 )50 l l 7 4 <! !(se [ 1 ] !(1!se [ 2 ] ) !(1!se [ 3 ] )+se [ 1 ] !a23!(1!se [ 2 ] ) !a13!(1!se [ 3 ] ) !a12 )51 l l 7 <! max(max( l l 7 1 , l l 7 2 ) , max( l l 7 3 , l l 7 4 ) )52 ul71 <! (1!se [ 1 ] ) !se [ 2 ] !se [3]+(1! se [ 1 ] ) !a23!se [ 2 ] !a13!se [ 3 ] !a1253 ul72 <! se [ 1 ] !(1!se [ 2 ] ) !se [3]! se [ 1 ] !a23+(1!se [ 2 ] ) !a13!se [ 3 ] !a1254 ul73 <! se [ 1 ] !se [ 2 ] !(1!se [ 3 ] )!se [ 1 ] !a23!se [ 2 ] !a13+(1!se [ 3 ] ) !a1255 ul74 <! (1!se [ 1 ] ) !(1!se [ 2 ] ) !(1!se [ 3 ] ) +(1!se [ 1 ] ) !a23+(1!se [ 2 ] ) !a13+(1!se [ 3 ] )
!a1256 ul7 <! min(min( ul71 , u l72 ) , min( ul73 , u l74 ) )57 l 1 l <! min( l l 7 , u l7 )58 u1l <! max( l l 7 , u l7 )59 a123 ˜ dunif ( l 1 l , u1 l )60 l l 8 1 <! !(sp [ 1 ] !sp [ 2 ] !sp [3 ]+ sp [ 1 ] !b23+sp [ 2 ] !b13+sp [ 3 ] !b12 )61 l l 8 2 <! !((1!sp [ 1 ] ) !(1!sp [ 2 ] ) !sp [3]!(1! sp [ 1 ] ) !b23!(1!sp [ 2 ] ) !b13+sp [ 3 ] !b12 )62 l l 8 3 <! !((1!sp [ 1 ] ) !sp [ 2 ] !(1!sp [ 3 ] )!(1!sp [ 1 ] ) !b23+sp [ 2 ] !b13!(1!sp [ 3 ] ) !b12 )63 l l 8 4 <! !(sp [ 1 ] !(1!sp [ 2 ] ) !(1!sp [ 3 ] )+sp [ 1 ] !b23!(1!sp [ 2 ] ) !b13!(1!sp [ 3 ] ) !b12 )64 l l 8 <! max(max( l l 8 1 , l l 8 2 ) , max( l l 8 3 , l l 8 4 ) )65 ul81 <! (1!sp [ 1 ] ) !sp [ 2 ] !sp [3]+(1! sp [ 1 ] ) !b23!sp [ 2 ] !b13!sp [ 3 ] !b1266 ul82 <! sp [ 1 ] !(1!sp [ 2 ] ) !sp [3]! sp [ 1 ] !b23+(1!sp [ 2 ] ) !b13!sp [ 3 ] !b1267 ul83 <! sp [ 1 ] !sp [ 2 ] !(1!sp [ 3 ] )!sp [ 1 ] !b23!sp [ 2 ] !b13+(1!sp [ 3 ] ) !b1268 ul84 <! (1!sp [ 1 ] ) !(1!sp [ 2 ] ) !(1!sp [ 3 ] ) +(1!sp [ 1 ] ) !b23+(1!sp [ 2 ] ) !b13+(1!sp [ 3 ] )
!b1269 ul8 <! min(min( ul81 , u l82 ) , min( ul83 , u l84 ) )70 l 2 l <! min( l l 8 , u l8 )71 u2l <! max( l l 8 , u l8 )72 b123 ˜ dunif ( l 2 l , u2 l )73
74 r2 [ 1 : 8 ] ˜ dmulti (p [ 1 : 8 ] , n )75 for ( i in 1 : 8 )76 {77 d [ i ] <! pow( r [ i ]!p [ i ] !n , 2 )/ (p [ i ] !n)78 d2 [ i ] <! pow( r2 [ i ]!p [ i ] !n , 2 )/ (p [ i ] !n)79 }80 bayesp <! step (sum(d [ ] ) ! sum( d2 [ ] ) )81 }82 l i s t ( r=c ( 1 , 0 , 1 , 2 , 1 , 7 , 10 , 998 ) , n=1020)83
84 l i s t ( pr=0.05 , se=c ( 0 .968 , 0 .927 , 0 .834 ) , sp=c ( 0 .994 , 0 .99 , 0 .997 ) ,a12= 0.013664 , a13= 0.010688 , a23= 0.024382 , b12= 0.00294 , b13= 0.001482, b23= 0.00147 , a123= !0.003783552 , b123= !0.000717360000000001 , r2=c
( 1 , 0 , 1 , 2 , 1 , 7 , 10 , 998 ) )85
86 l i s t ( pr=0.05 , se=c ( 0 .98 , 0 .917 , 0 .824 ) , sp=c ( 0 .974 , 0 .97 , 0 .977 ) ,a12= 0.00834000000000001 , a13= 0.00648 , a23= 0.026892 , b12= 0.01222 , b13= 0.010902 , b23= 0.01081 , a123= !0.00216432 , b123= !0.00484288 , r2=c( 1 , 0 , 1 , 2 , 1 , 7 , 10 , 998 ) )
Page 69

87
88 l i s t ( pr=0.05 , se=c ( 0 .96 , 0 .957 , 0 .854 ) , sp=c ( 0 .964 , 0 .98 , 0 .967 ) ,a12= 0.01828 , a13= 0.01416 , a23= 0.015222 , b12= 0.00928000000000001 , b13= 0.015312 , b23= 0.00934000000000001 , a123= !0.00586224 , b123=!0.00402752 , r2=c ( 1 , 0 , 1 , 2 , 1 , 7 , 10 , 998 ) )
Page 70

5 Conditional dependence - Berkvens et al. scheme(Mymensingh - iELISA cut-o! 7.5 IU/ml)
1 l i s t ( r1=c ( 1 , 0 , 1 , 2 , 1 , 7 , 10 , 998 ) , N=1020)2 Model{3 r1 [ 1 : 8 ] ˜ dmulti ( pr [ 1 : 8 ] ,N)4 pr [ 1 ]<!p [ 1 ] !p [ 2 ] !p [ 4 ] !p [8 ]+ (1!p [ 1 ] ) !(1!p [ 3 ] ) !(1!p [ 7 ] ) !(1!p [ 1 5 ] )5 pr [ 2 ]<!p [ 1 ] !p [ 2 ] !p [ 4 ] !(1!p [ 8 ] )+ (1!p [ 1 ] ) !(1!p [ 3 ] ) !(1!p [ 7 ] ) !p [ 1 5 ]6 pr [ 3 ]<!p [ 1 ] !p [ 2 ] !(1!p [ 4 ] ) !p [9 ]+ (1!p [ 1 ] ) !(1!p [ 3 ] ) !p [ 7 ] !(1!p [ 1 4 ] )7 pr [ 4 ]<!p [ 1 ] !p [ 2 ] !(1!p [ 4 ] ) !(1!p [ 9 ] ) + (1!p [ 1 ] ) !(1!p [ 3 ] ) !p [ 7 ] !p [ 1 4 ]8 pr [ 5 ]<!p [ 1 ] !(1!p [ 2 ] ) !p [ 5 ] !p [ 1 0 ] + (1!p [ 1 ] ) !p [ 3 ] !(1!p [ 6 ] ) !(1!p [ 1 3 ] )9 pr [ 6 ]<!p [ 1 ] !(1!p [ 2 ] ) !p [ 5 ] !(1!p [ 1 0 ] ) + (1!p [ 1 ] ) !p [ 3 ] !(1!p [ 6 ] ) !p [ 1 3 ]
10 pr [ 7 ]<!p [ 1 ] !(1!p [ 2 ] ) !(1!p [ 5 ] ) !p [ 1 1 ] + (1!p [ 1 ] ) !p [ 3 ] !p [ 6 ] !(1!p [ 1 2 ] )11 pr [ 8 ]<!p [ 1 ] !(1!p [ 2 ] ) !(1!p [ 5 ] ) !(1!p [ 1 1 ] ) + (1!p [ 1 ] ) !p [ 3 ] !p [ 6 ] !p [ 1 2 ]12
13 p [ 1 ] ˜dbeta ( 1 , 1 ) I ( 0 , 0 . 5 )14 p [ 2 ] ˜dbeta ( 1 , 1 )15 p [ 3 ] ˜dbeta ( 1 , 1 )16 p [ 4 ] ˜dbeta ( 1 , 1 )17 p [ 5 ] ˜dbeta ( 1 , 1 )18 p [ 6 ] ˜dbeta ( 1 , 1 )19 p [ 7 ] ˜dbeta ( 1 , 1 )20 p [ 8 ] ˜dbeta ( 1 , 1 )21 p [ 9 ] ˜dbeta ( 1 , 1 )22 p [ 1 0 ] ˜dbeta ( 1 , 1 )23 p [ 1 1 ] ˜dbeta ( 1 , 1 )24 p [ 1 2 ] ˜dbeta ( 1 , 1 )25 p [ 1 3 ] ˜dbeta ( 1 , 1 )26 p [ 1 4 ] ˜dbeta ( 1 , 1 )27 p [ 1 5 ] ˜dbeta ( 1 , 1 )28
29 prev <!p [ 1 ]30 se [ 1 ] < p [ 2 ]31 sp [ 1 ] <!p [ 3 ]32 se [ 2 ] <!p [ 2 ] !p[4]+(1!p [ 2 ] ) !p [ 5 ]33 sp [ 2 ] <!p [ 3 ] !p[6]+(1!p [ 3 ] ) !p [ 7 ]34 se [ 3 ] <!p [ 2 ] ! (p [ 4 ] !p[8]+(1!p [ 4 ] ) !p [ 9 ] ) +(1!p [ 2 ] ) ! (p [ 5 ] !p[10]+(1!p [ 5 ] ) !p [ 1 1 ] )35 sp [ 3 ] <!p [ 3 ] ! (p [ 6 ] !p[12]+(1!p [ 6 ] ) !p [ 1 3 ] )+(1!p [ 3 ] ) ! (p [ 7 ] !p[14]+(1!p [ 7 ] ) ! p
[ 1 5 ] )36 r2 [ 1 : 8 ] ˜dmulti ( pr [ 1 : 8 ] ,N)37 for ( i in 1 : 8 )38 {39 d1 [ i ] <! r1 [ i ] !log (max( r1 [ i ] , 1 )/ ( pr [ i ] !N) )40 d2 [ i ] <! r2 [ i ] !log (max( r2 [ i ] , 1 )/ ( pr [ i ] !N) )41 }42 G0 <! 2!sum( d1 [ ] )43 Gt <! 2!sum( d2 [ ] )44 bayesp <! step (G0 ! Gt)45 }
Page 71

6 Prior and posterior beta distributions
0.0 0.2 0.4 0.6 0.8 1.0
iELISA Se prior-posterior
Se
0.0 0.2 0.4 0.6 0.8 1.0
iELISA Sp prior-posterior
Sp
0.0 0.2 0.4 0.6 0.8 1.0
RBT Se prior-posterior
Se
0.0 0.2 0.4 0.6 0.8 1.0
RBT Sp prior-posterior
Sp
0.0 0.2 0.4 0.6 0.8 1.0
SAT Se prior-posterior
Se
0.0 0.2 0.4 0.6 0.8 1.0
SAT Sp prior-posterior
Sp
Prior and posterior beta distributions at Mymensinghwith: —– = prior beta distribution; —– = posterior beta distribution
Page 72

0.0 0.2 0.4 0.6 0.8 1.0
iELISA Se prior-posterior
Se
0.0 0.2 0.4 0.6 0.8 1.0
iELISA Sp prior-posterior
Sp
0.0 0.2 0.4 0.6 0.8 1.0
RBT Se prior-posterior
Se
0.0 0.2 0.4 0.6 0.8 1.0
RBT Sp prior-posterior
Sp
0.0 0.2 0.4 0.6 0.8 1.0
SAT Se prior-posterior
Se
0.0 0.2 0.4 0.6 0.8 1.0
SAT Sp prior-posterior
Sp
Prior and posterior beta distributions at the government farmwith: —– = prior beta distribution; —– = posterior beta distribution
Page 73






























