Embed Size (px)
Citation preview

ORIGINAL ARTICLE AESTHETIC
Borderline to Moderate Blepharoptosis Correction UsingRetrotarsal Tucking of Muller Muscle: Levator Aponeurosisin Asian Eyelids
Seungil Chung • Byungjoon Ahn • Wonyong Yang •
Jinsik Bum • Kiyup Kim • Sangyoon Kang
Received: 28 May 2014 / Accepted: 16 October 2014
� Springer Science+Business Media New York and International Society of Aesthetic Plastic Surgery 2014
Abstract
Background The purpose of this paper is to report the
outcome of retrotarsal tucking of Muller muscle-levator
aponeurosis for the correction of borderline to moderate
ptosis in conjunction with esthetic blepharoplasty in Asian
eyelids and to explore the relationship between the extent
of advancement and change in the eyelid position (MRD1).
Methods The medical records of 290 consecutive patients
who underwent retrotarsal tucking of Muller muscle-leva-
tor aponeurosis from February 2005 to November 2011
were reviewed. Of those, 26 patients (51 eyelids) were
statistically analyzed. The correction was performed
through an external upper blepharoplasty approach. Once
the orbital septum was opened, the Muller muscle-levator
aponeurosis was advanced and tucked under the posterior
surface of the tarsus by a single lifting suture. The average
follow-up period was 20.6 months, with a range of
3–68 months.
Results In 26 patients (51 eyelids), satisfactory results were
recorded for 49 of 51 eyelids (96.1 %). The margin reflex
distance-1 (MRD1) increased from 1.56 ± 0.70 mm pre-
operatively to 3.86 ± 0.94 mm postoperatively (p \ 0.001,
Wilcoxon signed rank test). When 6.1 mm of advancement
was implemented, an average MRD1 of 1 mm was achieved.
For 7.2 and 8.3 mm of advancement, the average MRD1
achieved was 2 and 3 mm each. A noteworthy complication,
although not included in statistical analysis, was one patient
who had developed corneal irritation caused by the con-
junctival exposure to the non-absorbable suture 3 years after
the surgery, which led the subject to have the suture removed.
Conclusion The author concludes that this procedure is
one of the most effective surgical options in correcting
borderline to moderate blepharoptosis in conjunction with
esthetic blepharoplasty. The main advantage of such a
method is that once the orbital septum is opened, Muller
muscle-levator aponeurosis is easily advanced and tucked
under the posterior surface of the tarsal plate without
extensive dissection or resection, which is less traumatic
and gives a more vertical lifting vector, thus producing
excellent cosmetic results and quick recovery.
Level of Evidence V This journal requires that authors
assign a level of evidence to each article. For a full
description of these Evidence-Based Medicine ratings,
please refer to the Table of Contents or the online
Instructions to Authors www.springer.com/00266.
Keywords Sleepy eye � Blepharoptosis correction �Muller tucking
Introduction
While performing esthetic blepharoplasty in Asians, the
levator complex must be manipulated for patients with
blepharoptosis, as well as for patients within the normal
margin reflex distance (MRD) range, but exhibit poor
folding of the double eyelid and want to obtain brighter
eyes [1–3].
E-Poster presented at the Annual Meeting of the ASAPS (The
American Society for Aesthetic Plastic Surgery) & ASERF (Aesthetic
Surgery Education and Research Foundation), New York, April
11–16, 2013.
S. Chung (&) � W. Yang � J. Bum � K. Kim � S. Kang
Department of Plastic and Reconstructive Surgery, Graduate
School of Medicine, Kyung Hee University, #1 Hoegi-dong,
Dongdaemoon-gu, Seoul 130-702, Korea
e-mail: [email protected]
B. Ahn
Secret Plastic Surgery Clinic, Seoul, Korea
123
Aesth Plast Surg
DOI 10.1007/s00266-014-0420-5

Based on the levator function, the amount of ptosis and
the surgeon’s preference, various techniques including
levator complex plication, advancement or shortening via a
percutaneous anterior or a posterior conjunctival approach
have been introduced over the years [4–10].
In recent days, the importance of the Muller muscle has
been emphasized in eyelid surgeries in light of the theory
that the Muller muscle, rather than the levator aponeurosis,
plays the primary role in the transmission of the force of
the levator muscle during eyelid lift [11–13]. By consid-
ering the functional reduction of the Muller muscle caused
by its resection, techniques such as advancement or tucking
of the Muller muscle-levator aponeurosis to the anterior
surface of the tarsal plate via limited resection or plication
have become mainstream [14–17].
However, when using the methods described above, it is
necessary that either the anatomical layers between the
Muller muscle and levator aponeurosis or conjunctiva be
dissected to form a flap, or that the Muller muscle be
separated from the tarsal plate. Thus, these methods have
disadvantages, such as the long time it takes to perform
such procedures and the difficulty of obtaining symmetry
when conducting a simultaneous esthetic double eyelid
operation. To overcome these disadvantages, it is necessary
to shorten the operation time using a less invasive and
simpler technique, which effectively reduces the intraop-
erative change of the eyelid caused by swelling or
bleeding.
To this end, the authors devised a technique that mini-
mizes dissection by avoiding the separation of the Muller
muscle from the upper margin of the tarsus, levator apo-
neurosis or conjunctiva; and this technique fixes the Muller
muscle and levator aponeurosis via posterior rather than
anterior advancement to overcome the increased possibility
of eversion of the tarsal plate [18].
Although similar techniques that advance the Muller
muscle and levator aponeurosis to the tarsal plate have
been reported, the study of retrotarsal tucking of the Muller
muscle-levator aponeurosis has not been reported yet.
Therefore, based on the past 5-year experience in the sur-
gery of borderline to moderate blepharoptosis, the out-
comes of retrotarsal tucking of the Muller muscle-levator
aponeurosis were clinically and statistically analyzed.
Materials and Methods
Subjects
This study was retrospectively conducted on 290 patients
(34 men and 256 women) who underwent retrotarsal
tucking (advancement) of the Muller muscle-levator apo-
neurosis in conjunction with esthetic blepharoplasty from
February 2005 to November 2011. Subject ages ranged
from 15 to 70 years (Mean age: 26.0 years). Of patients
who had mild to moderate blepharoptosis (amount of ptosis
B3 mm) based on the Berke method and patients who had
‘borderline blepharoptosis’ prior to treatment, those who
underwent retrotarsal tucking (advancement) of the Muller
muscle-levator aponeurosis because of the pathological
status of the levator palpebrae muscle during the treatment
were included in the study. For the preoperative plan, a
amount of ptosis using MRD, and levator function using
Berke method were measured. The levator function was
shown to be greater than 8 mm in 282 patients and modest
(5–7 mm) in 8 patients.
Methods
Of the subjects, the condition of 26 subjects (51 eyelids)
was followed up for 3 months or longer. For each of these
subjects, the MRD1 (margin reflex distance: distance
between pupil center and upper eyelid margin) of their
preoperative and postoperative digital photos was objec-
tively measured using Adobe Photoshop for statistical
analysis.
Measurement Using the Digital Photos (The Outcome
Measurements)
The subject’s MRD1, which was measured using the Berke
method before and after the surgery, varies depending on
the measurer’s experience and bias. To rule out the
aforementioned problem, the MRD1 was obtained using the
photos of the subjects who were followed up for 3 months
or longer and whose preoperative and postoperative photos
were all available. From among the digital photos of each
subject, only the front shots were used. To increase mea-
surement accuracy, these photos were uniformly magnified
and adjusted for size ratio, and then the MRD1 was mea-
sured using Adobe Photoshop CS5 Portable. The distance
from the reflex point of the pupil center to the upper eyelid
margin shown in the photos was determined as the MRD1.
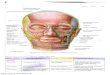
The corneal length, which is relatively constant in the eyes,
was also measured. The mean corneal length of Koreans is
known to be 11.5 mm, and the MRD1 was adjusted based
on the mean corneal length (Fig. 1) [19, 20]. In cases in
which photos were unavailable, the corresponding subject
was excluded from statistical analysis even though his/her
MRD1 was recorded in the chart.
Evaluation of the Results
The position of the upper eyelid margin in their frontal
gaze was compared with the normal range of the height of
the upper eyelid margin for bilateral blepharoptosis, and
Aesth Plast Surg
123

with the normal eyelid for unilateral blepharoptosis. When
all of the following four criteria were met, the surgery was
assessed to be successful: Postoperative MRD1 of 3–5 mm;
difference in the MRD1 between both eyes B1 mm; dif-
ference in the size and shape of the double eyelids between
the two eyes B1 mm; symmetrical size and shape of the
double eyelids. Contrarily, in case any of the four criteria
was unmet or resurgery was required, the surgery was
determined to be unsuccessful.
Anatomical & Physical Considerations: Surgical
Concept and Schematic Diagram
During eyelid lift, the levator aponeurosis is known to not
only suspend the preaponeurotic fat and lift the eyelid
margin with slight eversion, but also control the tension of
the anterior lamella, as the Muller muscle controls the
tension of the posterior lamella [11–13].
As the eyelid is lifted up while rotating around the eye, it
is most efficiently lifted up when the force is transmitted to
the tangential direction of the eye. In other words, the
corresponding direction becomes the axial direction of the
tarsal plate. In light of this, the authors believe that an
eyelid lift using the middle layer and posterior surface of
the tarsal plate is a good alternative, since it causes less
friction (Fig. 2) [18].
Surgical Technique
For surgery, double eyelid incision is performed under
local anesthesia, and a small dose of a local anesthetic
agent (2 % lidocaine containing 1:100,000 epinephrine) is
applied to minimize the stimulation of the Muller muscle.
The skin and orbicularis oculi muscle are incised, and the
anterior muscle and fat of the tarsal plate are partially
removed to expose the orbital septum. The orbital septum
is inferiorly incised, which is close to the conjoined fascia,
to expose the levator aponeurosis. The orbital fat is also
removed, if necessary. Then, factors that inhibit the eye
from opening, such as excessive skin or orbicularis oculi
muscle, preaponeurotic fat, connective tissues around the
lower transverse ligament, and lateral horn of aponeurosis
are also removed (Fig. 3).
A pore is made using an iris scissor with a sharp tip
2 mm beneath the upper margin of the tarsal plate, and then
Fig. 1 Method of real MRD1 measurement. X measured diameter of
cornea, Y measured MRD1 in Adobe Photoshop) Method to obtain the
real MRD1 value 11.5 mm: real MRD1 = X: Y real
MRD1 = 11.5 mm 9 Y/X
Fig. 2 Because the upper lid is elevated over the surface of an
eyeball, the force of elevating the upper lid is transferred most
effective when the force is redirected tangentially to an eyeball and in
parallel to the axis of tarsal plate. While lifting an eyelid, the force of
friction is proportional to the force applied to an eyeball, which needs
to be minimized. In this case, the fixation of the Muller’s muscle-
levator aponeurosis to the posterior surface of tarsal plate requires less
force of friction and force to elevate the upper lid than the fixation to
the anterior surface of it. The torque ( _s) acting on the plate relative to
the fixed point ‘O’ is a vector quality defined as _s ¼ _r � _F. The
curved arrow shows the direction of the ‘torque ( _s)’. The small arrow
on the component indicates the ‘ _r’ vector (radius), and the long arrow
indicates the ‘ _F’ vector (the force). (Left) When fixed at the anterior
surface of tarsal plate, a clockwise torque is developed. Thus, the
upper lid tends to be everted. (Center) On the other hand, when
fixated at the posterior surface, a counter-clockwise torque is
developed. (Right) This illustrates the tendencies of eversion or
inversion with fixations at either position. Consequently, eversion of
the upper lid is minimized
Aesth Plast Surg
123

the region between the levator aponeurosis and Muller
muscle is partially dissected while checking the peripheral
arterial arcade (Fig. 4a–c). After the amount of advance-
ment from the incised site was determined according to the
preoperative plan, a 6-0 nylon suture is used to simulta-
neously penetrate the levator aponeurosis and Muller
muscle medially to the midpupilary line, with caution not
to expose the conjunctiva, and then again 2 mm beneath
the upper margin of the tarsal plate toward the anterior
surface of the tarsal plate from the posterior surface
(Fig. 4d–f). The suture is then pulled out of the anterior
surface of the tarsal plate and knitted to pass through a
Fig. 3 Schematic diagram of
surgical technique. (Left)
Needle passage. 6-0 nylon
suture is placed through the
aponeurosis—Muller muscle
and full-layered tarsus from
posterior to anterior surface
followed by penetration of the
mid-lamella of the upper tarsal
border. (Right) Knot is tied after
Muller muscle-levator
aponeurosis is advanced and
tucked under the posterior
surface of the tarsal plate
Fig. 4 a–c shows the dissection
of the levator aponeurosis and
the superior portion of the tarsal
plate. Here, the Muller muscle is
not detached from the tarsus and
lower conjunctiva. By grasping
the soft tissues over the tarsal
plate upward, it is possible to
obtain the hole necessary for
needle passages. c–i Muller
muscle-levator aponeurosis is
advanced (tucked) under the
posterior surface of the tarsal
plate, while making the mattress
suture just off the medium to the
mid-pupillary line with 6-0
nylon at 2 mm inferior from the
upper margin of the tarsus
Aesth Plast Surg
123

horizontal width of 3 mm, and then pulled out of the mid-
lamella of the tarsal plate (Fig. 4g). An assistant proceeds
to lift the tarsal plate with a forceps to secure the posterior
surface of the tarsal plate, followed by transient suturing.
The height of the upper eyelid margin is then adjusted to
be positioned 1 mm beneath the upper corneal limbus at
primary gaze, and the suture is ligated (Figs. 4h, i).
If the margin of the upper eyelid appears to be unnatural
or insufficient, an additional lifting suture is medially and
laterally performed. The orbital septum of the distal region
of the sutured site and levator aponeurosis stump are
trimmed to have a proper length to form double eyelids that
are natural in appearance. After trimming, the stump and
the muscle or the dermis of the lower eyelid flap are fixed
at 5–7 sites to form the double eyelid. This is followed by
skin suturing.
Statistical Analysis
For statistical analysis, the Wilcoxon signed rank test,
Mann-Whiteney test, and Kruskal Walis tests were con-
ducted as nonparametric tests for univariate analysis. In
addition, linear regression analysis and multiple regression
analysis were also conducted. Statistical analysis was
conducted using SPSS 18.0 at a significance level of\0.05.
Results
Statistical analysis was conducted on 51 eyelids (26 sub-
jects) out of 577 eyelids (290 subjects: 34 men and 256
women). The mean age of the subjects who underwent the
statistical analysis was 25.4 ± 8.0 years, and the mean
follow-up period was 20.6 ± 19.8 months, with a range of
3–68 months. The subjects consisted of 7 men and 19
women. They had 36 eyelids of borderline blepharoptosis
and 15 eyelids of mild to moderate blepharoptosis
(B3 mm). Among the 51 eyelids, epicanthoplasty was
additionally conducted on the 20 eyelids and the surgery
outcomes were assessed by comparing preoperative and
postoperative MRD1 values (Table 1).
Among the 26 subjects (51 eyelids) who underwent the
statistical analysis, 24 eyelids (47.1 %) were assessed to be
‘excellent’ (MRD1 4.1–5.0 mm) and 25 eyelids (49.0 %)
were assessed to be ‘good’ (MRD1 3.1–4.0 mm), which
showed that the satisfactory results of good or higher levels
were observed in 49 eyelids (96.1 %) (Figs. 5, 6).
As for postoperative complications, one subject (2
cases) had under-correction and three subjects had asym-
metry, of which one case was misdiagnosed before the
surgery, but had pseudoptosis due to preoperative hyper-
tropia of the left eye.
In the data excluded from the statistics, the complica-
tions from 290 total patients were minor, with the most
common occurrence being a slight asymmetry in 16
patients (5.5 %), mostly related to under-correction (17
patients; 5.9 %).
Moreover, the cases in which corneal irritation occurred
in 7 patients (2.4 %) who were excluded from statistical
analysis. Six of these patients underwent correction as the
condition occurred in the early postoperative period. The
one remaining patient had corneal irritation caused by
conjunctival exposure of the non-absorbable suture 3 years
after the surgery, forcing the subject to have their suture
removed.
The other complication was over-correction in 2 patients
(0.7 %).
No symptoms of dry eye, exposure keratopathy, or other
complications were encountered in any patient. No contour
abnormalities, infections, hematomas, or other complica-
tions were noted.
Results of Statistical Analysis
The mean preoperative and postoperative values were
shown to be 1.56 ± 0.70 and 3.86 ± 0.94, respectively. To
test the significance of the difference between the preop-
erative and postoperative values, the Wilcoxon signed rank
test, a nonparametric paired comparison, was conducted.
As a result, the difference was shown to be statistically
significant (p \ 0.001).
Table 1 Case summary
Variables n (51)
Age (year)
10–19 10
20–29 29
30 12
Sex
Male 14
Female 37
Follow-up duration (months)
3–12 28
13–36 12
37 11
Diagnosis
Borderline ptosis 36
True ptosis 15
Additional procedure
None 31
Medial epicanthoplasty 20
Aesth Plast Surg
123

Discussion
Various surgery methods for blepharoptosis have been
reported according to levator function, degree of ptosis, or
surgeon’s experience or preference. They include a tech-
nique that advances the levator muscle-aponeurosis and
Muller muscle to the anterior surface of the tarsal plate or
shortens them by resection via an external anterior, trans-
conjunctival posterior approach, or frontalis transfer.
However, surgery for mild to moderate blepharoptosis is
still controversial [4–10, 21–26].
In the past, it was thought that the levator aponeurosis
plays a leading role in transmitting levator functions.
However, the Muller muscle is currently thought to be
more significant. Since arriving at this conclusion, more
techniques using the Muller muscle have been actively
reported [11].
Haramoto et al. reported the eyelid lift mechanism as a
dual elastic suspension system where the anterior levator
aponeurosis, which attaches to the soft tissue of the anterior
tarsal plate, indirectly suspends the tarsal plate via this soft
tissue, and the Muller muscle, which not only directly
attaches to the upper margin of the tarsal plate but also
attaches to the anterior tarsal plate via the pretarsal fascia,
directly suspends the tarsal plate [12]. In addition, the
Muller muscle, which is governed by the sympathetic
nervous system, plays a main role in 2–3 mm lift of the
eyelid, maintaining the elevated eyelid at the constant
height and making the eyelid blink naturally [9, 12, 21, 27].
Thus, the aforementioned roles of the Muller muscle sug-
gest that the Muller muscle and the levator aponeurosis
should be simultaneously advanced for maintaining long-
term stability in the conduct of blepharoptosis surgery.
The Muller muscle was first included in a blepharoptosis
surgery conducted by Fasanella-Servat, upon which a small
amount of the Muller muscle was resected. In a study
conducted by Putterman et al., 4, 6, 8, and 10 mm of the
Muller’s muscle and conjunctiva were resected for 1, 1.5,
2, and 3 mm of ptosis amount, respectively [7, 8].
As for the surgery outcome of Muller muscle-conjunc-
tiva resection, Putterman et al., and Dresner reported a
success rate of 90 and 95 %, respectively. The good sur-
gery outcomes were explained by the following mecha-
nisms. First, the shortening of the Muller’s muscle
reinforces the tensile strength of it and improves the stretch
reflex as Matsuo suggested, which results in functional
improvement as the terminal tissue of the levator muscle.
Second, the shortening of the Muller muscle causes the
plication or advancement of the anterior levator aponeu-
rosis, which results in the good transmission of the force of
the levator muscle to the tarsal plate [8, 10, 28].
However, the aforementioned methods that resect the
conjunctiva, tarsal plate, and Muller muscle via a posterior
approach through the conjunctiva are inappropriate for
Asians who undergo blepharoptosis correction in con-
junction with double eyelid operation for esthetic purposes
rather than for the correction of vision disorders. The
reason for this is that the anterior approach is more
advantageous than the posterior approach in removing
factors that restrict eyelid lift such as skin, orbicularis oculi
muscle, orbital fat, lower transverse ligament, or connec-
tive tissues around the lateral horn of levator aponeurosis,
etc. Furthermore, if more of the Muller muscle is resected,
it increases the possibility of injury to the mechanorecep-
tors or the stretch reflex, which deviates from the recent
trend in which the Muller muscle is preserved as much as
possible [14, 15].
Accordingly, in recent days, techniques using the Muller
muscle have been mainly used in mild to moderate
blepharoptosis patients. They include advancement of the
Muller muscle-levator aponeurosis composite flap; Muller
tucking that advances the Muller muscle to the anterior
surface of the tarsal plate after the separation of the Muller
muscle from the levator aponeurosis; and balanced tucking
that advances the levator aponeurosis and fixes it to the
tarsal plate, pretarsal orbicularis oculi muscle, or dermis
without tension together with Muller tucking [14–17, 25].
Generally, in the methods described above, the Muller
muscle must be dissected from the levator aponeurosis,
Fig. 5 (Left) Preoperative view of a 22-year-old male with mild
blepharoptosis. (Right) Six months postoperative photo after 8 mm of
retrotarsal advancement of the Muller muscle-levator aponeurosis on
the right side and 6 mm of advancement on the left side and
simultaneous double eyelid surgery on both sides
Fig. 6 (Left) Preoperative view of a 28-year-old male with borderline
blepharoptosis. (Right) Fourteen months after 6 mm of retrotarsal
advancement of the Muller muscle-levator aponeurosis and simulta-
neous double eyelid surgery on both sides
Aesth Plast Surg
123

conjunctiva or the tarsal plate to form a flap. As such, these
methods have disadvantages because of the significant
amount of time they require, the relatively significant
edema, and the difficulty of obtaining symmetry when
performing an esthetic double eyelid operation. Further-
more, all of these methods fix the Muller muscle and
levator aponeurosis to the anterior surface of the tarsal
plate via shortening or advancement. Thus, due to the
occurrence of clockwise torque, the possibility of eversion
of the tarsal plate increases. This tendency particularly
increases as the fixation point is lower than the upper
margin of the tarsal plate. In addition, as the eyelid is lifted
up while rotating around the eyes, it is most efficiently
lifted up when the force is transmitted to the tangential
direction of the eyes. Thus, the corresponding direction
becomes the axial direction of the tarsal plate. The authors
believe that an eyelid lift using the middle layer and pos-
terior surface of the tarsal plate can be effective as a
smaller force is transmitted to the eyeball, which causes
less friction (Fig. 2) [18].
Accordingly, the authors developed retrotarsal tucking
(advancement) of the Muller muscle-levator aponeurosis
without dissection between the Muller’s muscle and levator
aponeurosis.
Particularly, in cases of sleepy-looking eyes, exhibiting
borderline blepharoptosis or in cases which, even after
removing all factors restricting the movement of the upper
eyelids, significant drooping of the eyelids is still observed,
the authors’ technique can easily be conducted by mini-
mally dissecting the site between the levator aponeurosis
and Muller muscle. Thus, obtaining symmetry is easier due
to the minimization of edema and bleeding. This is based
on our experience that the tissue trauma or edema occurred
less using our method in comparison to the cases of pro-
cedures that were done using preexisting techniques with
extensive dissection. In general, an eyelid lift is sufficiently
performed by a single lifting suture. The eyelid margin
with the most natural arc is obtained by positioning the
suture slightly nasally rather than the mid-pupillary line
[6]. In addition, eyelid peaking is significantly observed in
the cases of the weak tarsal plate, lowered fixation point
from the upper margin of the tarsal plate, penetration of
only the partial layer of the anterior surface by the suture,
and improper interval of the transverse matrix suture. In
this study, the suture was inserted through the entire layer
of the tarsal plate, and then pulled out via the mid-lamella
of the upper margin of the tarsal plate to prevent eyelid
peaking [26, 29].
As for the outcome of surgery, the success rate was
shown to be 96.1 % in this study, which was similar to that
of the previous studies. The mean preoperative MRD1 was
1.56 ± 0.70 and the mean postoperative MRD1 was
3.86 ± 0.94 in this study. Also, the difference in the MRD1
before and after the surgery was statistically significant
(p \ 0.001). Conventionally, 4 mm of levator muscle has
been resected for 1 mm of ptosis, or methods reported by
Putterman et al. have been used [7, 8, 24]. In this study,
however, when the difference in the values measured
before and after the surgery was analyzed based on the
relationship of the values measured before and after the
surgery rather than using the regression equation and sta-
tistical analysis, the advancement of 6.1, 7.2, and 8.3 mm
was estimated to be required for improving the MRD1 of 1,
2, and 3 mm, respectively. However, with the limited
sample size, this does not carry significant meaning and
with more cases to consider, the result is thought to con-
verge to a similar value.
In the analyzed group, one subject had under-correction
and three subjects exhibited asymmetry. As under-correc-
tion occurred even though the bilateral Muller muscle-
levator aponeuroses were advanced by approximately
10 mm, other methods including levator muscle resection
should have been considered for the correction of moderate
blepharoptosis with levator function 5–7 mm. Based on
previous experience, the maximum advancement that can
be achieved by the above method was approximately
12 mm. If the advancement exceeds 12 mm, the patient
may suffer discomfort during lid movement due to the
excessive plication of the conjunctiva. If blepharoptosis
correction is insufficient via this technique, however,
levator muscle resection may be conducted anytime, and
under-correction can be resolved as it is reversible. In the
case of asymmetrical results, it may occur due to improper
preoperative design, different skin resection amount or fat
removal amount, unstable fixation between the levator
aponeurosis and dermis, intraoperative bleeding or edema,
or levator palsy caused by local esthesis. In this study,
asymmetry occurred because of insufficient correction on
one side. Although no other complications were observed,
one subject, who was excluded from statistical analysis,
had corneal irritation caused by conjunctival exposure of
the non-absorbable suture 3 years after the surgery, in
which case the subject had to have the suture removed.
Conclusion
The retrotarsal tucking (advancement) of Muller muscle-
levator aponeurosis without the separation of the Muller
muscle from the upper margin of the tarsal plate achieves
efficient eyelid lift without the eversion of the tarsal plate.
In addition, this technique has many advantages including:
less bleeding and edema due to less extensive tissue dis-
section, increased ease of obtaining bilateral symmetry
during the surgery, and the relative simplicity to perform.
Thus, this procedure is suitable for correcting borderline to
Aesth Plast Surg
123

moderate blepharoptosis in conjunction with esthetic
blepharoplasty. However, conjunctival suture erosion is
theoretically possible, so we need to prevent it by carefully
checking the suture exposure in the conjunctival side and
making the intraoperative knot toward the skin. Moreover,
because data from this procedure are only available from a
limited sample size, this novel technique clearly needs
further study to evaluate long-term safety and efficacy.
Conflict of interest The authors declare that they have no conflict
of interest.
References
1. Park SG, Lee SK, Baek RM (2006) A new interpretation of ptosis-
like eyes through the results of small-incision double-eyelid
operation. J Korean Soc Plast Reconstr Surg 33(4):449–453 Korean
2. Li J, Lin M, Zhou H, Jia R, Fan X (2011) Double-eyelid bleph-
aroplasty incorporating blepharoptosis surgery for ‘latent’ apo-
neurotic ptosis. J Plast Reconstr Aesthet Surg 64(8):993–999
3. Ha KY, Suh HW, Kim BY, Kim TY, Park SG (2010) Correlation
analysis of ocular dominance and levator palpebrae superioris
muscle function. J Korean Soc Plast Reconstr Surg 37(3):265–270
Korean
4. Jones LT, Quickert MH, Wobig JL (1975) The cure of ptosis by
aponeurotic repair. Arch Ophthalmol 93(8):629–634
5. Harris WA, Dortzbach RK (1975) Levator tuck: a simplified
blepharoptosis procedure. Ann Ophthalmol 7(6):873–878
6. Liu D (1993) Ptosis repair by single suture aponeurotic tuck. Sur-
gical technique and long-term results. Ophthalmology 100(2):
251–259
7. Putterman AM, Urist MJ (1975) Muller muscle-conjunctiva
resection. Technique for treatment of blepharoptosis. Arch
Ophthalmol 93(8):619–623
8. Putterman AM, Fett DR (1986) Muller’s muscle in the treatment
of upper eyelid ptosis: a ten-year study. Ophthalmic Surg 17(6):
354–360
9. Beard C (1985) Muller’s superior tarsal muscle: anatomy, phys-
iology, and clinical significance. Ann Plast Surg 14(4):324–333
10. Dresner SC (1991) Further modifications of the Muller’s muscle-
conjunctival resection procedure for blepharoptosis. Ophthal
Plast Reconstr Surg 7(2):114–122
11. Bang YH, Park SH, Kim JH, Cho JH, Lee CJ, Roh TS (1998) The
role of Muller’s muscle reconsidered. Plast Reconstr Surg
101(5):1200–1204
12. Haramoto U, Kubo T, Tamatani M, Hosokawa MK (2001)
Anatomic study of the insertions of the levator aponeurosis and
Muller’s muscle in oriental eyelids. Ann Plast Surg 47(5):
528–533
13. Kakizaki H, Zako M, Nakano T, Asamoto K, Miyaishi O, Iwaki
M (2005) The levator aponeurosis consists of two layers that
include smooth muscle. Ophthal Plast Reconstr Surg 21(5):
379–382
14. Baik BS, Kim TB, Hong WK, Yang WS (2005) Muller’s muscle-
levator aponeurosis advancement procedure for blepharoptosis.
J Korean Soc Plast Reconstr Surg 32(2):219–226 Korean
15. Baik BS, Suhk JH, Choi WS, Yang WS (2009) Treatment of
blepharoptosis by the advancement procedure of the muller’s
muscle-levator aponeurosis composite flap. J Korean Soc Plast
Reconstr Surg 36(2):211–220 Korean
16. Park JW, Shin HS, Park ES, Kim YB (2006) Balanced tucking of
the levator muscle and muller’s muscle in blepharoptosis.
J Korean Soc Plast Reconstr Surg 33(2):149–154 Korean
17. Park DH, Baik BS (2008) Advancement of the Muller muscle-
levator aponeurosis composite flap for correction of blepharop-
tosis. Plast Reconstr Surg 122(1):140–142
18. Halliday D et al (2005) Fundamentals of Physics, vol 7. Wiley,
New York, pp 281–282
19. Oh CH (2009) Analysis of postoperative complications in
blepharoptosis. J Korean Soc Plast Reconstr Surg 36(6):743–749
Korean
20. Bae TH (2003) A Photogrammetic study of the eyes in Korean
youths. J Korean Soc Plast Reconstr Surg 34:37–41 Korean
21. Park DH, Baik BS (1998) Cosmetic and reconstructive oculo-
plastic surgery, 1st edn. Koonja Publishing, Inc., Seoul 241
22. Lee MG, Kim HC, Minn KW (1995) Levator advancement for
correction of blepharoptosis. J Korean Soc Plast Reconstr Surg
22:1386 Korean
23. Uchida J (1962) A surgical procedure for blepharoptosis vera and
for pseudo-blepharoptosis orientalis. Br J Plast Surg 15:271–276
24. Park DH, Baik BS, Nahai F (2009) Cosmetic and reconstructive
oculoplastic surgery, 3rd edn. Koonja Publishing, Inc., Seoul,
p 149–186, 509–563
25. Yuzuriha S, Matsuo K, Kushima H (2000) An anatomical
structure which results in puffiness of the upper eyelid and a
narrow palpebral fissure in the Mongoloid eye. Br J Plast Surg
53(6):466–472
26. Meltzer MA, Elahi E, Taupeka P, Flores E (2001) A simplified
technique of ptosis repair using a single adjustable suture. Oph-
thalmology 108(10):1889–1892
27. Kuwabara T, Cogan DG, Johnson CC (1975) Structure of the
muscles of the upper eyelid. Arch Ophthalmol 93(11):1189–1197
28. Matsuo K (2002) Stretching of the Mueller muscle results in
involuntary contraction of the levator muscle. Ophthal Plast
Reconstr Surg 18(1):5–10
29. Park DH, Kim CW, Shim JS (2008) Strategies for simultaneous
double eyelid blepharoplasty in Asian patients with congenital
blepharoptosis. Aesthetic Plast Surg 32(1):66–71
Aesth Plast Surg
123















![Volunteer Management Plan and Procedures - … Plan Template.docx · Web viewU.S. Army Volunteer Management Plan and Procedures [Type the document subtitle] Tucking-Strickler, Devan](https://img.pdfslide.us/doc/110x75/5d1c12dc88c99357178c1aac/volunteer-management-plan-and-procedures-plan-templatedocx-web-viewus-army.jpg)