Embed Size (px)
Citation preview
BoomeritisArthritis of the hip and knee joint
Hardy Singh, M.D.

Welcome….
Hardy Singh, M.D.
3404 Wake Forest Road
Suite 201
Raleigh, NC 27609
(919) 256-1511
www.seortho.net
Background…
Hardy Singh, M.D.
Medical School, Punjab, India
Orthopaedic Training, India
Research, Duke University Medical Center
Residency Duke University Medical Center
6 month Fellowship, Joint replacement
Joint Efforts
• Putting the spring back in your steps….
• Or..
• Charting your course to a more normal lifestyle….
Choosing an orthopaedic surgeon…
• How are orthopaedic surgeons trained?
• What is Board Certification?
• What is a fellowship?
Topics..
• Arthritis
• Joint Anatomy
• Treatment options
The Arthritis Foundation
“Half of Americans diagnosed with arthritis don’t think anything can
be done to help them.”
The Arthritis Foundation
• Arthritis is the number one cause of disability in the U.S.*
• Over 16 million adults say that arthritis limits their usual activities in some way.*
• 8.2 million working aged U.S. adults (about 1 in 20) report work limitations due to arthritis or joint symptoms.
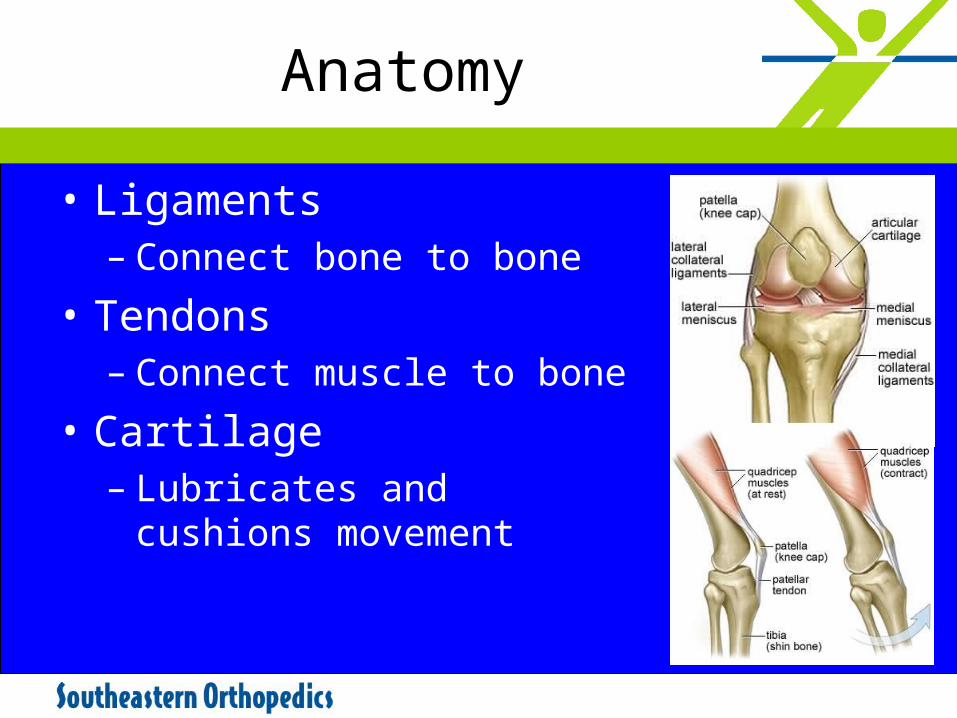
Anatomy
• Ligaments– Connect bone to bone
• Tendons– Connect muscle to bone
• Cartilage– Lubricates and cushions
movement
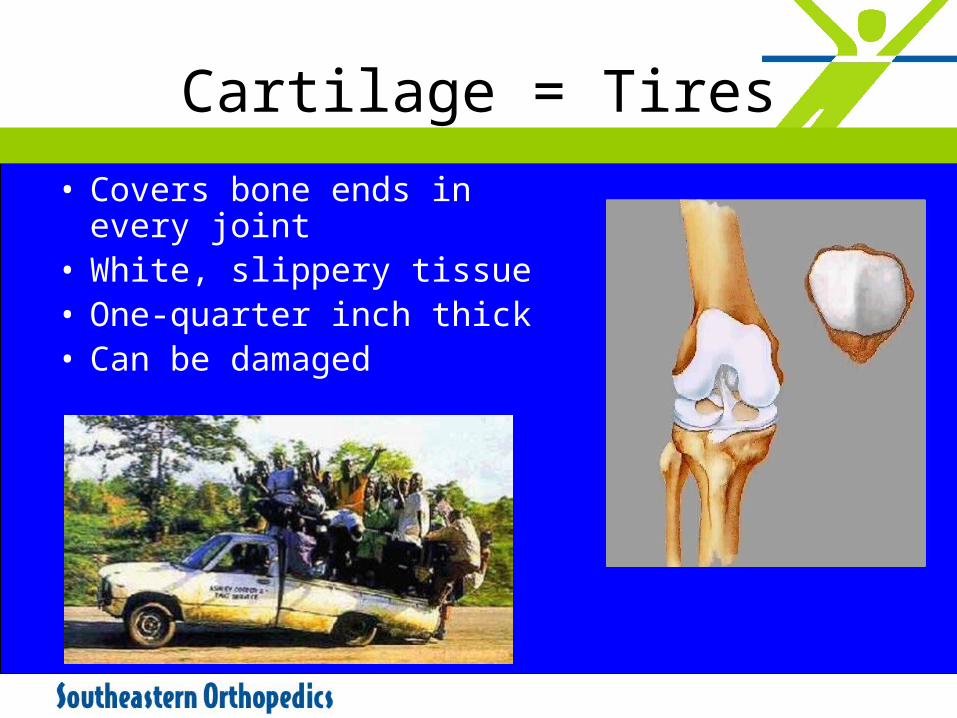
Cartilage = Tires
• Covers bone ends in every joint
• White, slippery tissue• One-quarter inch thick• Can be damaged
What is Arthritis..?
• Defined as inflammation of the joint • More than 100 different types • Affects 43 million Americans each year• Pain, swelling, and loss of motion• Most common cause of disability in US—
1 in 6 affected• Two primary types
– Osteoarthritis– Rheumatoid arthritis
• Source—Centers for Disease Control and Prevention
Rheumatoid Arthritis
• Inflammatory arthritis
• Often affects many joints at once
• Can occur at any age, even children
• Excess synovial fluid
Osteoarthritis
• Most common type of arthritis
• 23 million Americans affected annually*
• Degenerative disease affecting joint cartilage
– “wear and tear”
• May result from overuse or injury
• Knees, hips, back and hands most often affected
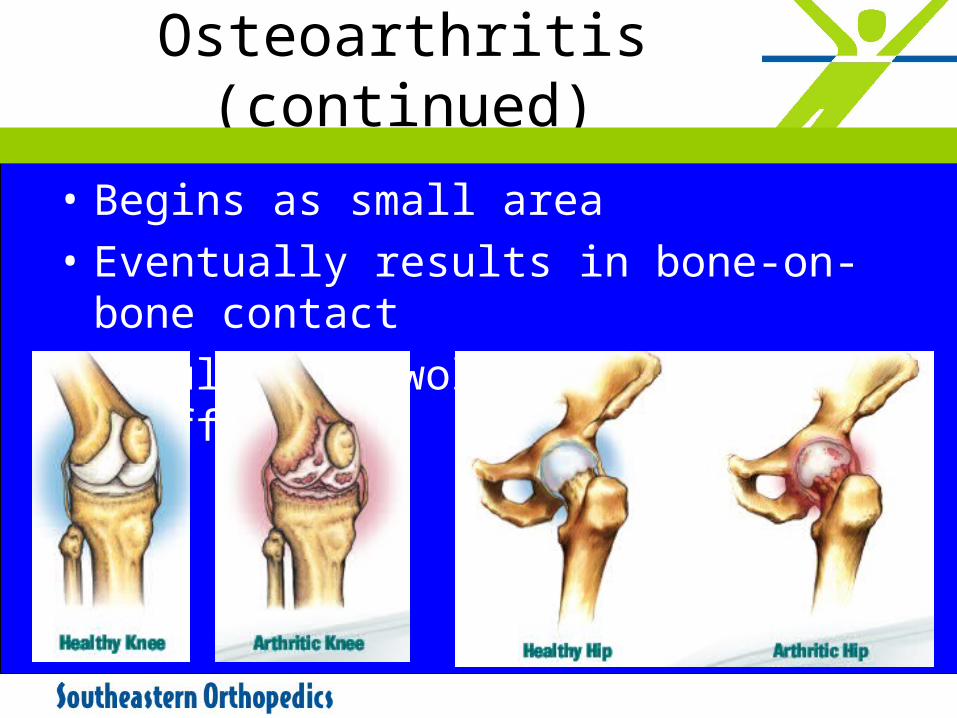
Osteoarthritis (continued)
• Begins as small area
• Eventually results in bone-on-bone contact
• Results in swollen, painful and stiff joints
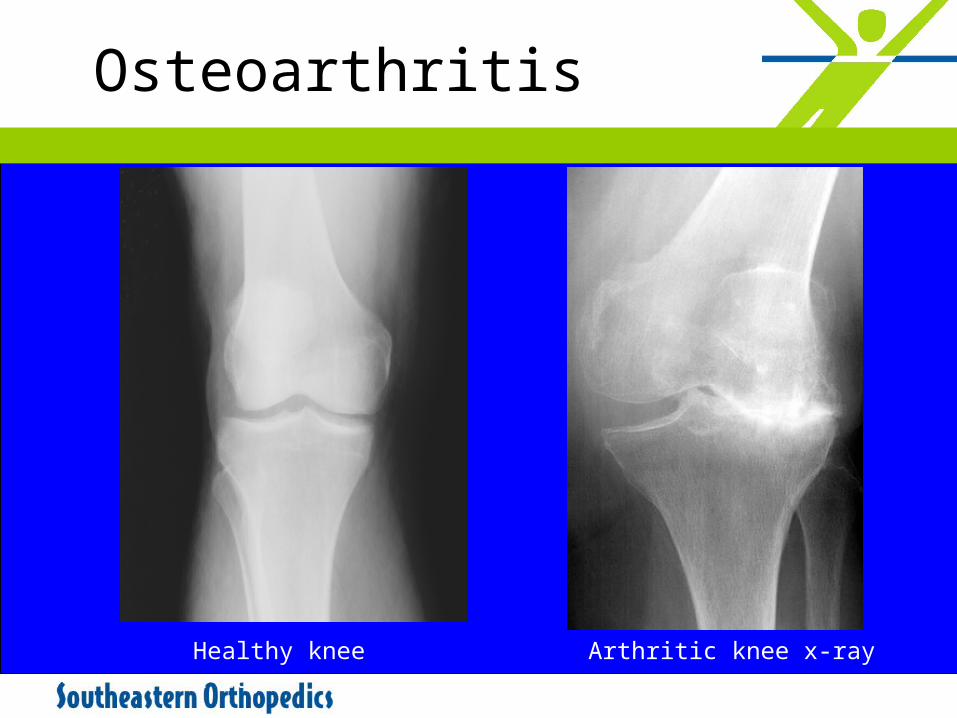
Osteoarthritis
Healthy knee x-ray Arthritic knee x-ray
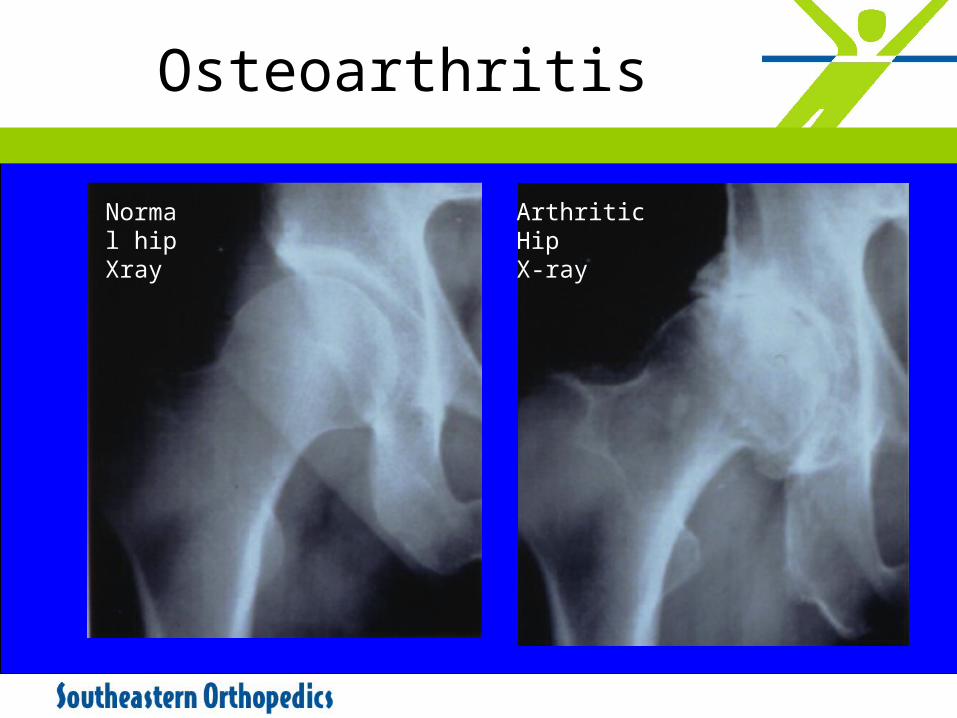
Osteoarthritis
Normal hip Xray
Arthritic HipX-ray

Symptoms of Arthritis
• Joints warm to the touch• Joints swelling• Joint pain and immobility• Joint stiffness• Joint weakness (buckling)• Decreased activity• Impaired lifestyle • Joint deformities
Osteoarthritis vs. Normal Aging
• Osteoarthritis causes changes in the bone below cartilage
• Osteoarthritis occurs primarily in weight-bearing joints
• With osteoarthritis, the water content increases early in the disease process
Exercise Nourishes Cartilage
• Extremely beneficial.• Keeps bones strong.• Keeps joints limber.• Strengthens muscles.
– Good muscle tone decreases stress to the articular surface of the joint.
• Helps prolong life of joints.
Types of Exercise
• Walking• Swimming• Bicycling• Water aerobics• Work with physical
therapist.• Posture
– Lift correctly– Rest– ADL’s
Modifying Activities of Daily Living
• Posture
• Lift correctly
• Rest
Weight Control(Being Overweight…)
• Places extra stress on your joints1
– 3 pounds of pressure for every 1 pound of body weight
– 150 pound person can place up to 450 pounds of pressure across each joint
• Accelerates rate of cartilage destruction2
• Makes it harder to exercise properly before and after surgery2.
• Harrington, I. J. (1976): A bioengineering analysis of force actions at the knee in normal and pathological gait. Biomed. Eng., 11:167–172.
• Felson, D. T.: “Weight and osteoarthritis.” J. Reumatol, 43: 7–9, 1995.

Too much to handle..
Ice….is nice
• Decreases local circulation
• Decreases swelling• Acts as a local anti-
inflammatory• Decreases pain• Improves exercise
tolerance
Heat… is nice
• Increases local circulation
• Promotes relaxation
• Helps muscles and joints stretch
• Decreases joint and muscle aches
Braces and Self-Help Devices
• Back/Hip/Knee– Abdominal supports to reduce stress
on the back– Long-handled reachers and grabbers
to reduce bending– Sock sliders
• Knee– Bracing the knee reduces painful
instability– Unloader braces are special knee
braces to reduce stress on the knee joint.
Orthotics
• Properly fitting footwear is essential to align legs
• Heel wedges or orthotics help align the legs, relieving pressure on knees
• Rubber shoe inserts may reduce some of the impact loading that your knees or hips experience.
• Canes (in opposite hand).• Walkers
Glucosamine/Chondroitin sulfate
• Building block of cartilage• May be useful in strengthening
cartilage, preventing breakdown.• Can be extracted from shells of
crabs and shrimp• Not a cure. Does not rebuild
cartilage.• May help with keeping cartilage
spongy.• Some anti-inflammatory properties.
Vitamins/ Minerals
• Some studies indicate higher incidence of arthritis in people with low Vitamin C and D intake
• Too much calcium does not cause arthritis– Too little calcium can cause osteoporosis
• Arthritis patients should take vitamins regularly
Medications/NSAID’s
• Acetaminophen, Aspirin, Naproxen, Ibuprofen, Celebrex.
• Host of NSAID’s (as needed best)
• Effective in reducing swelling
• Stomach and blood side-effects.
• Topical Creams: Capsaicin, zostrix (from red peppers)– Helps block pain.
Hyaluronate
• Naturally occurring substance in cartilage
• Relieves pain
• Restores function
• Provides lubrication to cartilage
• Relief may last from 6 to12 months.
• Hyalgan, Supartz, Synvisc, etc..
• Few side effects..pseudosepsis
Wang CT, Lin J, Chang CJ, Lin YT, Hou SM. Therapeutic effects of hyaluronic acid on osteoarthritis of the knee. A meta-analysis of randomized controlled trials. J Bone Joint Surg Am. 2004; 86:538-545
Cortisone
• Naturally Occurring Hormone.
• Anti-inflammatory
• Short term pain relief
• Reduce swelling
• Relief is variable
• Long-term use may injure cartilage.
Leopold SS, Redd BB, Warme WJ, Wehrle PA, Pettis PD, Shott S. Corticosteroid compared with hyaluronic acid injections for the treatment of osteoarthritis of the knee. A prospective, randomized trial. J Bone Joint Surg Am. 2003; 85:1197-1203.
Is Surgery for You?
• This should be a cooperative one between you, your family, your family physician and your orthopaedic surgeon.
The Orthopaedic Evaluation
• Medical history including:– Previous injuries and
surgeries– Current medications – Lifestyle issues and
demands
• Physical examination• X-rays• Occasionally blood
tests, MRI or bone scan
Surgery
Chondroplasty, RF ablation
OATS, microfracture
Carticel
Osteotomies
Partial joint replacement
Orthoglide spacer
Total joint replacement
Arthroscopy
• Controversial for Degenerative knee• Mechanical symptoms= success.
– Relieves pain from torn meniscus, Loose bodies, pathologic plica, osteophytes, notch stenosis
• Severity of arthritis= failure• Less successful with malalignment/ Gait
issues.• Arthroscopy=sham for arthritis.
Osteotomy
“Minimally Invasive” Surgery
• Traditional joint replacement surgery is performed through an 8 - 10 inch incision
• Some patients may qualify for a “minimal” incision, only 4 inches to 6 inches long
• Your surgeon will select the best approach for your unique situation.
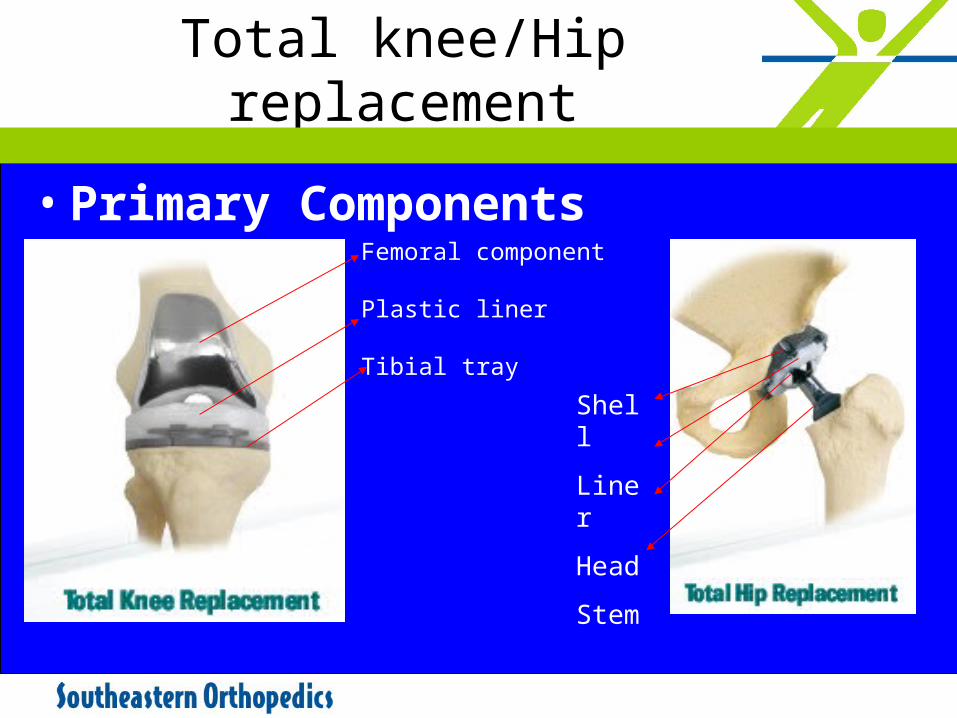
Total knee/Hip replacement
• Primary Components
Shell
Liner
Head
Stem
Femoral component
Plastic liner
Tibial tray
Preparing for Total Joint Replacement
• Donate some of your own blood
• Stop taking certain drugs before surgery
• Begin exercises to speed your recovery after surgery
• Plan for home therapy and rehabilitation after surgery
Total joint replacementRealistic expectations
90 percent of individuals who undergo total joint replacement experience a dramatic reduction of pain and a significant improvement in the ability to perform common activities of daily living.
• Survivorship:– 90%@10 yrs– 80%@15 yrs– 75%@20 yrs.
Possible Complications
• Most are successfully treatable
• Types of possible complications: – Loosening– Infection– Wear– Blood clots– Dislocation– Nerve Injury
The Recovery Process
• Use your "new" joint shortly after your operation
• Begin walking shortly after surgery
• Initially, you will walk with a walker, crutches or a cane.

Home Planning
• Safety bars
• Secure handrails
• Stable chair
• Toilet seat riser
• Remove all loose carpets and cords
• Same floor living space
The Recovery Process
• There will be temporary pain in the replaced joint
• The muscles are weak from inactivity
• The tissues are healing
• Pain will end in a few weeks or months
A few weeks later..
New Implant- FDA approved 2006
• ORTHOGLIDE
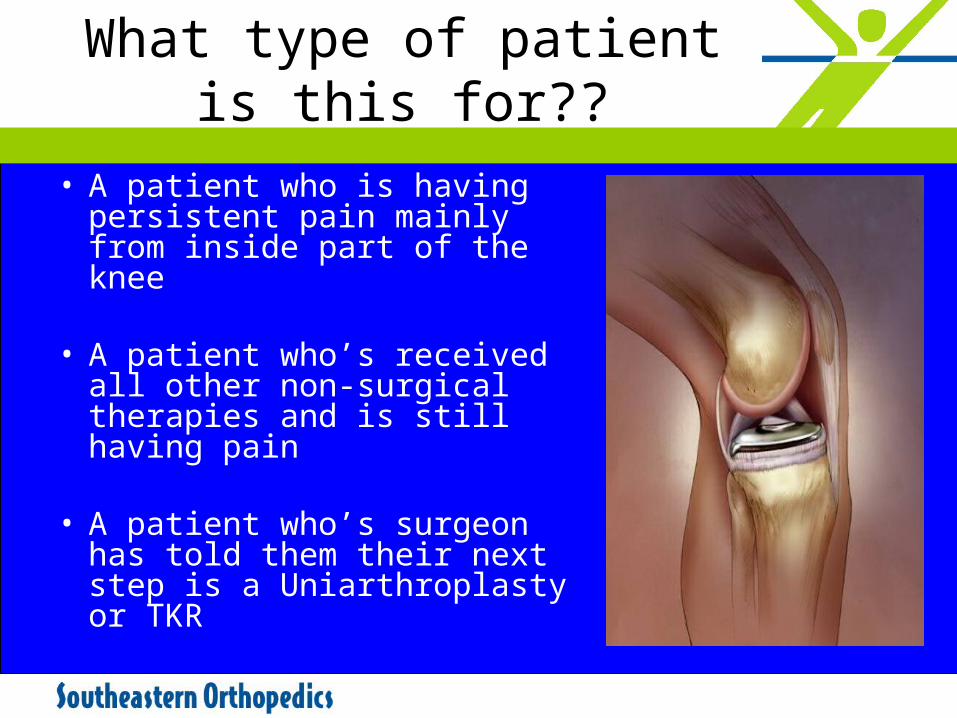
What type of patient is this for??
• A patient who is having persistent pain mainly from inside part of the knee
• A patient who’s received all
other non-surgical therapies and is still having pain
• A patient who’s surgeon has told them their next step is a Uniarthroplasty or TKR
How it works
• Reduces the forces placed on the painful middle part of the knee by redistributing them to the other less painful half
• Increase the contact area of the moving parts in the knee, thus reducing painful point forces
• Decrease the bone-on-bone friction by providing a smooth glide path for the femur to move on
The OrthoGlide Advantages…
• Provides pain relief without compromising the knee anatomy• No bone cuts
• 2-3 inches long, combined with arthroscopy• Total procedure time: 45-60 min.• Does not “Burn any Bridges”
• Easy conversion to other surgical options (i.e. Uni, TKR)
• Home next day, no Physical Therapy• Weight bearing as tolerated.
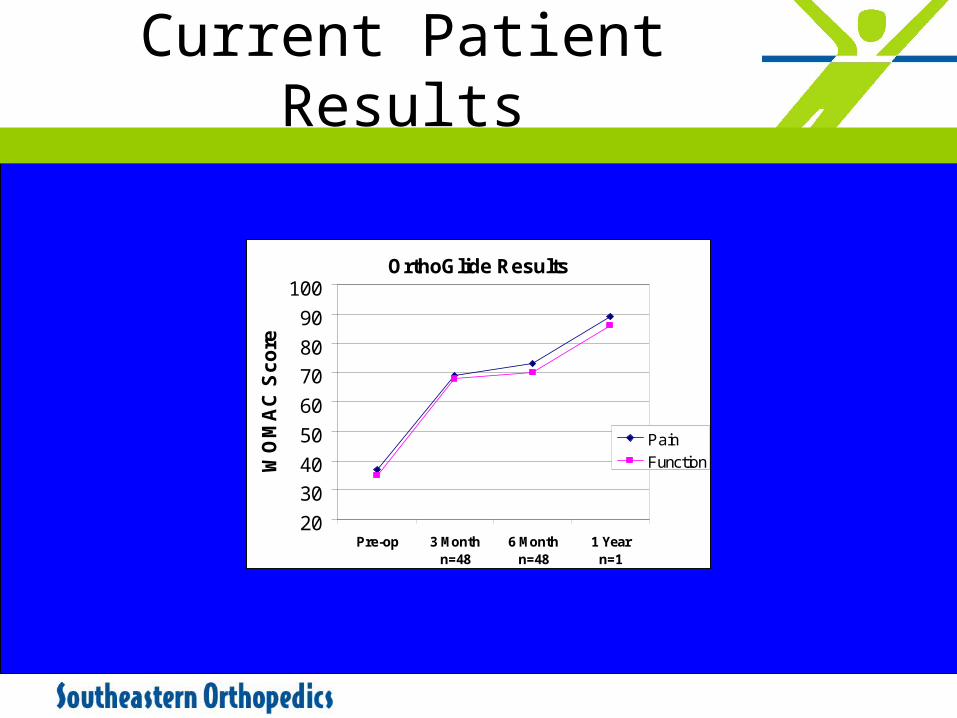
Current Patient Results
OrthoGlide Results
20
30
40
50
60
70
80
90
100
Pre-op 3 Monthn=48
6 Monthn=48
1 Yearn=1
WO
MA
C S
co
re
Pain
Function
Future of arthritis
• By the year 2030, an estimated one quarter of the projected total adult population, or 64.9 million adults aged 18 years and older, will have doctor-diagnosed arthritis, compared to the 42.7 million adults in 2002.*
• These estimates may be conservative as they do not account for current trends in obesity.
Closing
• Education of various options
• We can/must successfully treat arthritis
• Surgery is a last resort
• Returning patients to activity and employment is critical
• We must work together.
Future
• Identifying high risk patients.
• Genetic basis
• Disease prevention through– Health– Lifestyle &– Disease modifications.
Thank you
Hardy Singh, M.D.