Embed Size (px)
Citation preview
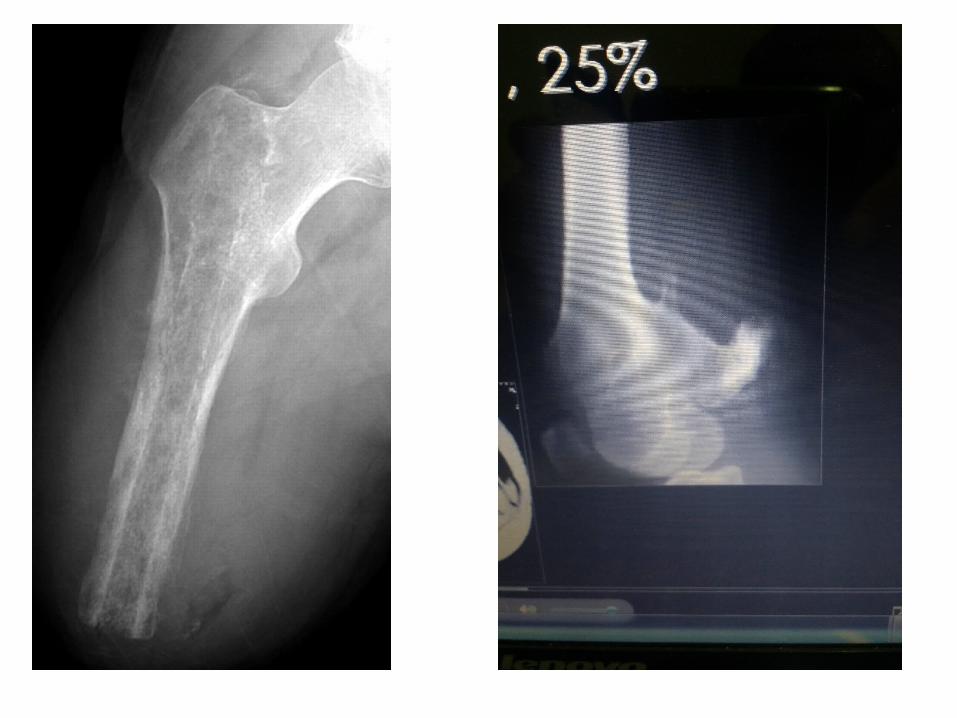
Bone tumors• Imaging modalities:
- Plain x-ray, CT, MRI, Ultrasonography, radionuclide bone scanning.
- Plain x-ray:Regional AP, Lateral, Oblique view
Chest PA, Lateral.
Can predict the nature of the lesion 70-80%.
Should never be omitted in the investigation of bone tumors.
What is the site of the lesion?
Epiphysis , metaphysis , diaphysis
You can know the lesion from the site.
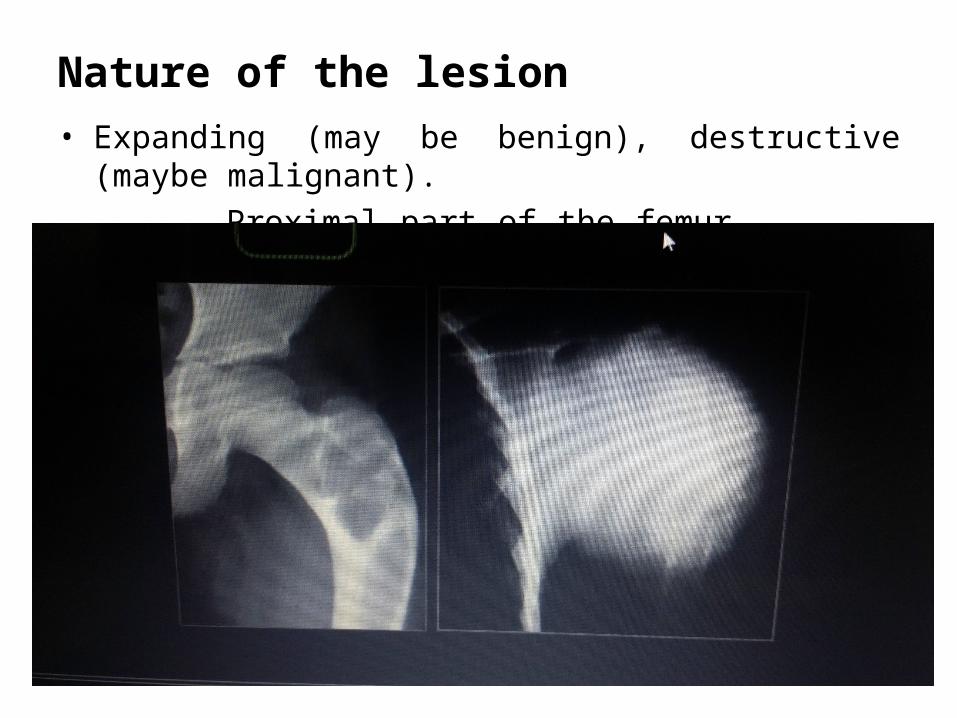
Nature of the lesion• Expanding (may be benign), destructive (maybe malignant).
Proximal part of the femur humorous

• Well defined (scelerotic, not) ill defined
Benign malignant
Margin of the lesion
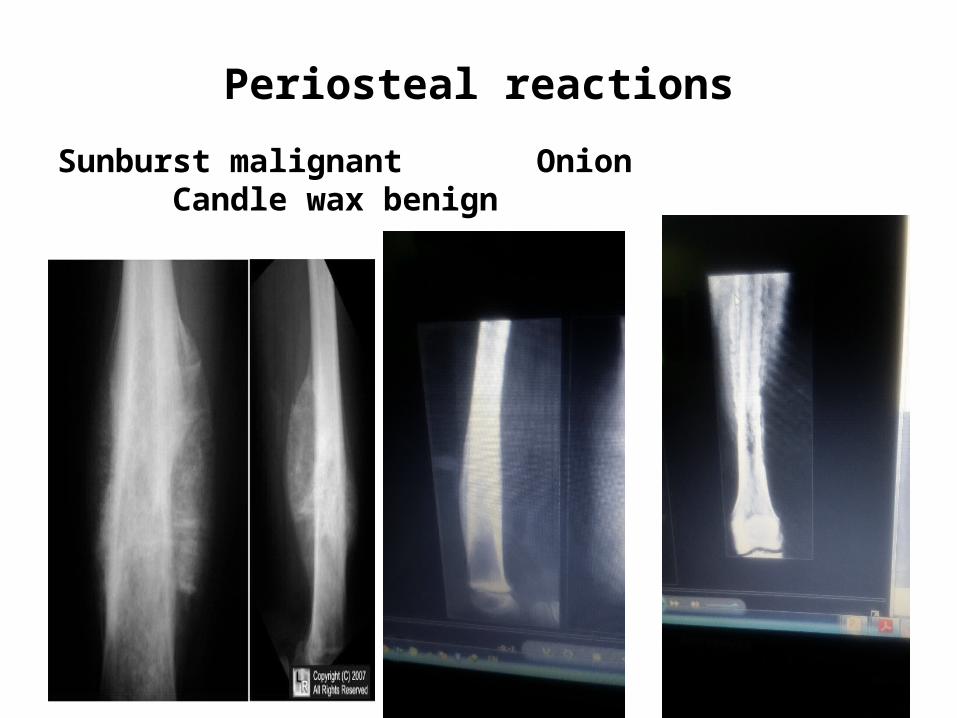
Periosteal reactions
Sunburst malignant Onion Candle wax benign
malignant
Bone tumors from the imaging point of view
Lesion with characteristic imaging features
Lesion with suggestive imaging features
Lesion with non specific imaging features
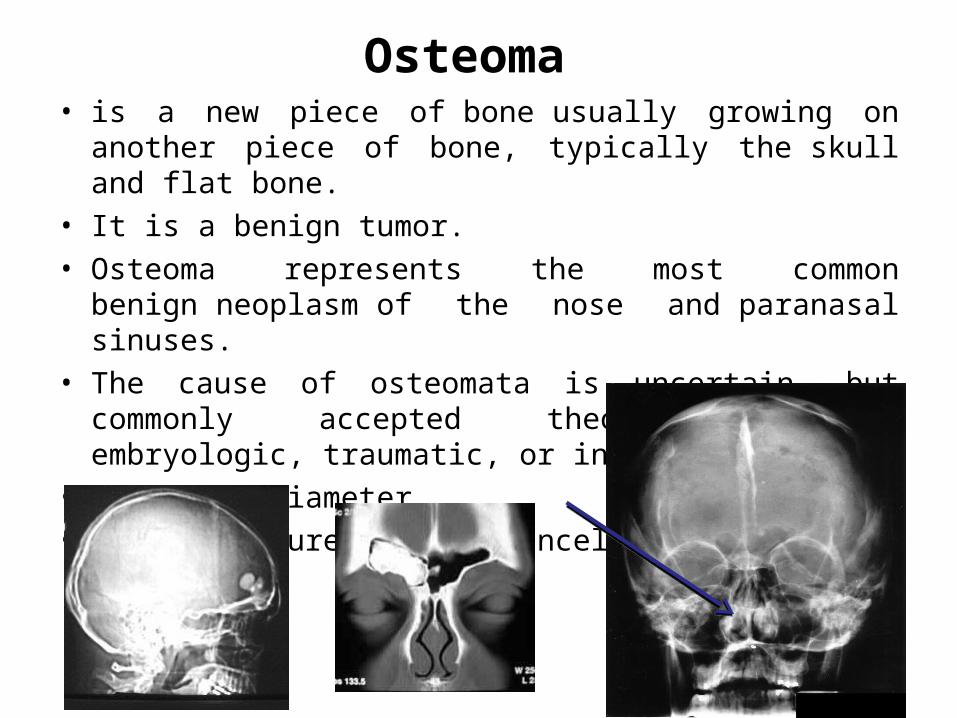
Osteoma • is a new piece of bone usually growing on another piece of
bone, typically the skull and flat bone.
• It is a benign tumor.
• Osteoma represents the most common benign neoplasm of the nose and paranasal sinuses.
• The cause of osteomata is uncertain, but commonly accepted theories propose embryologic, traumatic, or infectious causes.
• 2.5 cm in diameter.
• Bony structure with no canceleous bone
Osteoid osteoma
• is a benign bone tumor that arises from osteoblasts and was originally thought to be a smaller version of an osteoblastoma.
• Tend to be less than 1.5 cm in size. • The tumor can be in any bone in the body but are most
common in long bones, such as the femur and tibia. They account for 10 to 12 percent of all benign bone tumors. "Osteoid osteomas may occur at any age, and are most common in patients between the ages of 4 and 25 years old.
• Males are affected approximately three times more commonly than females.
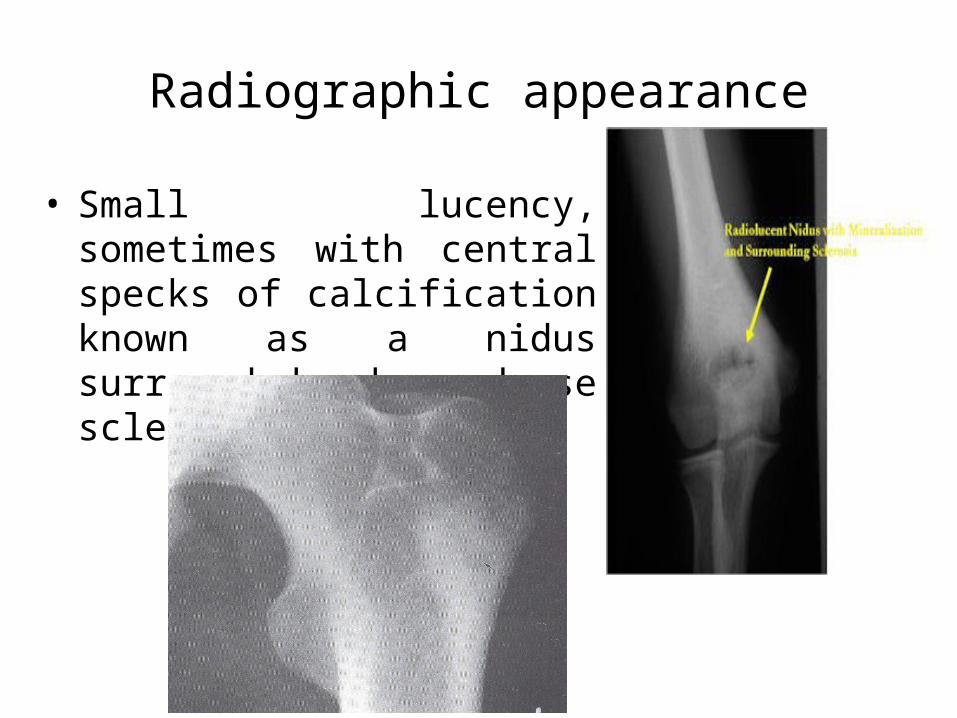
Radiographic appearance
• Small lucency, sometimes with central specks of calcification known as a nidus surrounded by dense sclerotic rim.
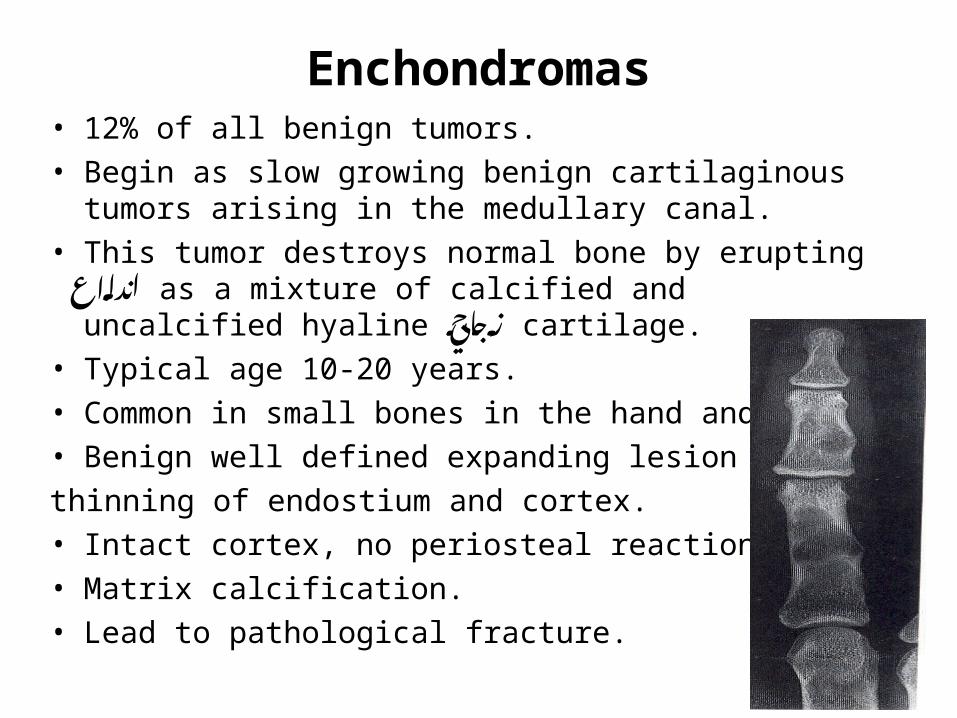
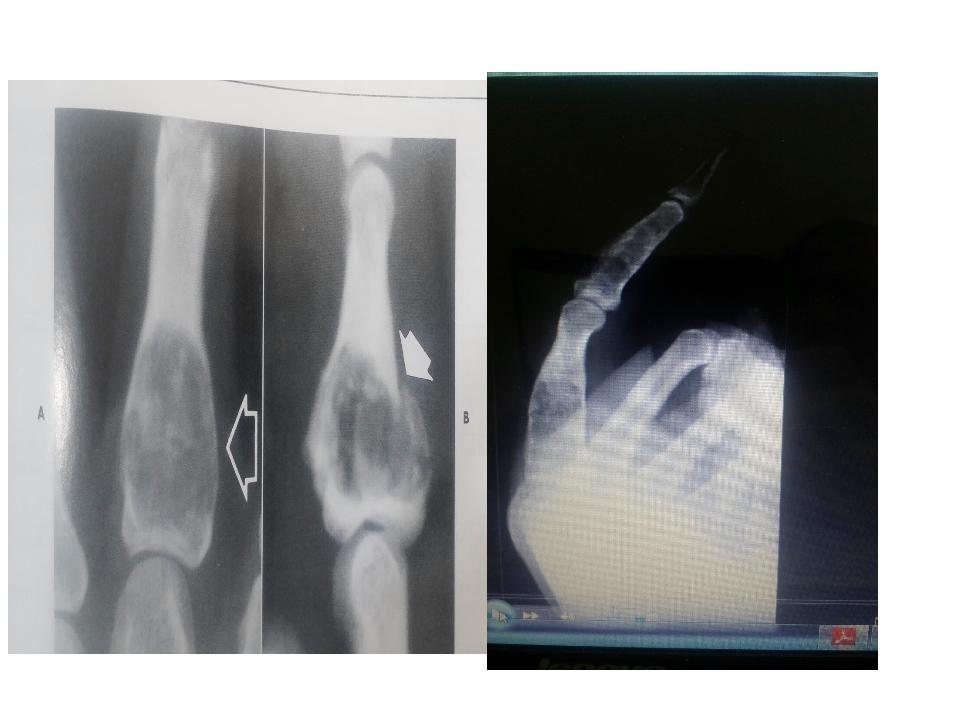
Enchondromas• 12% of all benign tumors.
• Begin as slow growing benign cartilaginous tumors arising in the medullary canal.
• This tumor destroys normal bone by erupting اندالع as a mixture of calcified and uncalcified hyaline زجاجي cartilage.
• Typical age 10-20 years.
• Common in small bones in the hand and feet.
• Benign well defined expanding lesion causing
thinning of endostium and cortex.
• Intact cortex, no periosteal reaction.
• Matrix calcification.
• Lead to pathological fracture.
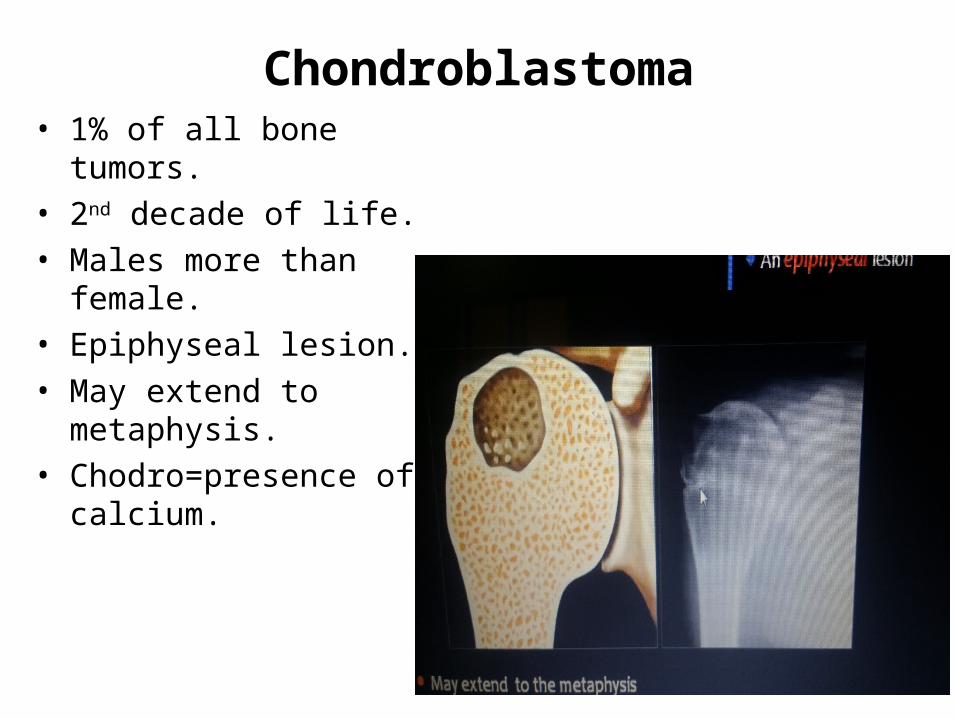
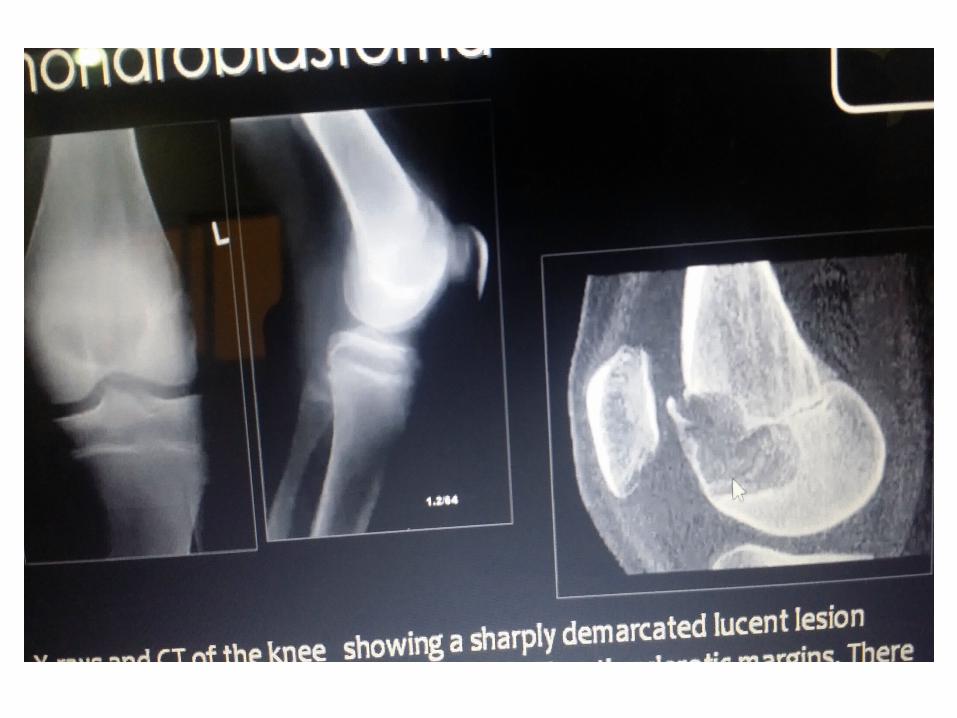
• 1% of all bone tumors.
• 2nd decade of life.
• Males more than female.
• Epiphyseal lesion.
• May extend to metaphysis.
• Chodro=presence of calcium.
Chondroblastoma
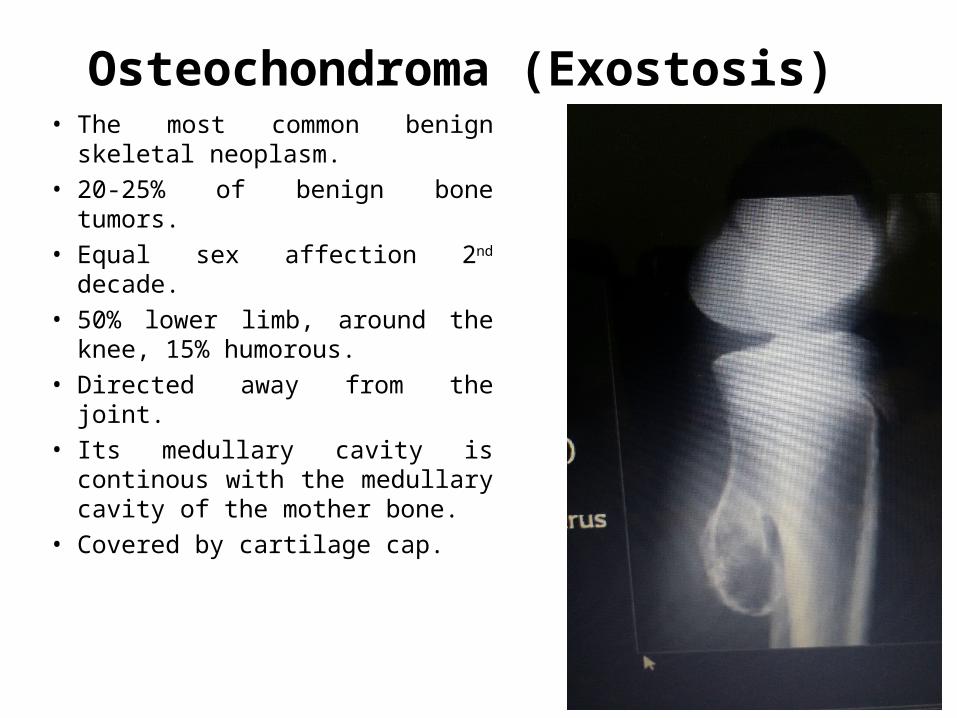
Osteochondroma (Exostosis) • The most common benign
skeletal neoplasm.
• 20-25% of benign bone tumors.
• Equal sex affection 2nd decade.
• 50% lower limb, around the knee, 15% humorous.
• Directed away from the joint.
• Its medullary cavity is continous with the medullary cavity of the mother bone.
• Covered by cartilage cap.
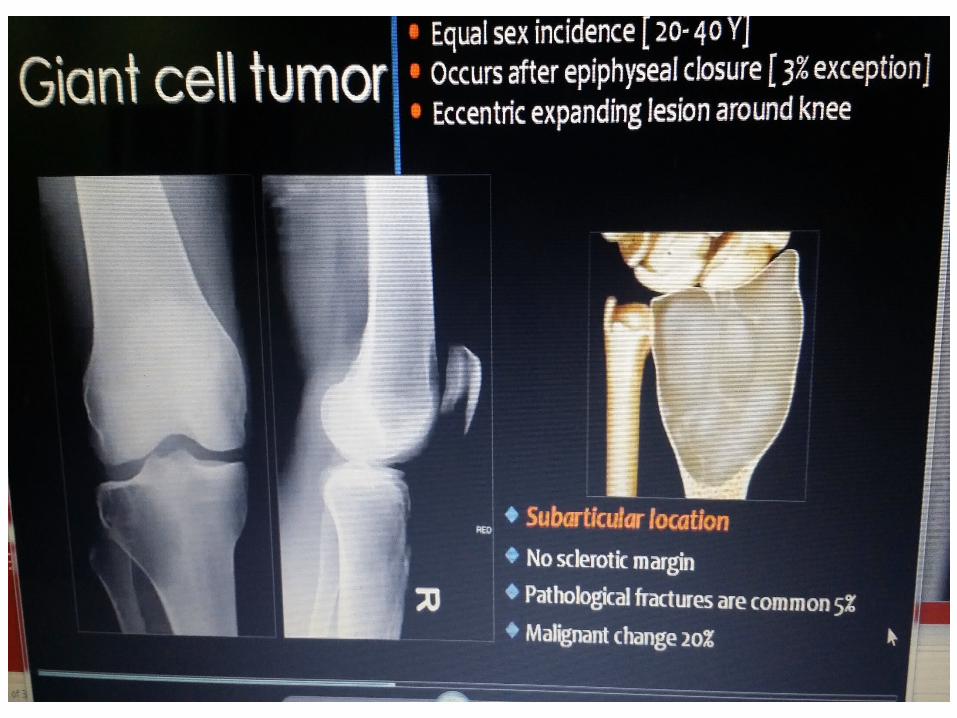
Giant Cell Tumor Locally malignant. Equal sex incidence (20-40Y). Occurs after epiphyseal closure (3% exception). Subarticular location. No sclerotic margin. Pathological fractures are common (5%). Is expanding and reaching the articular surface. Well defined.


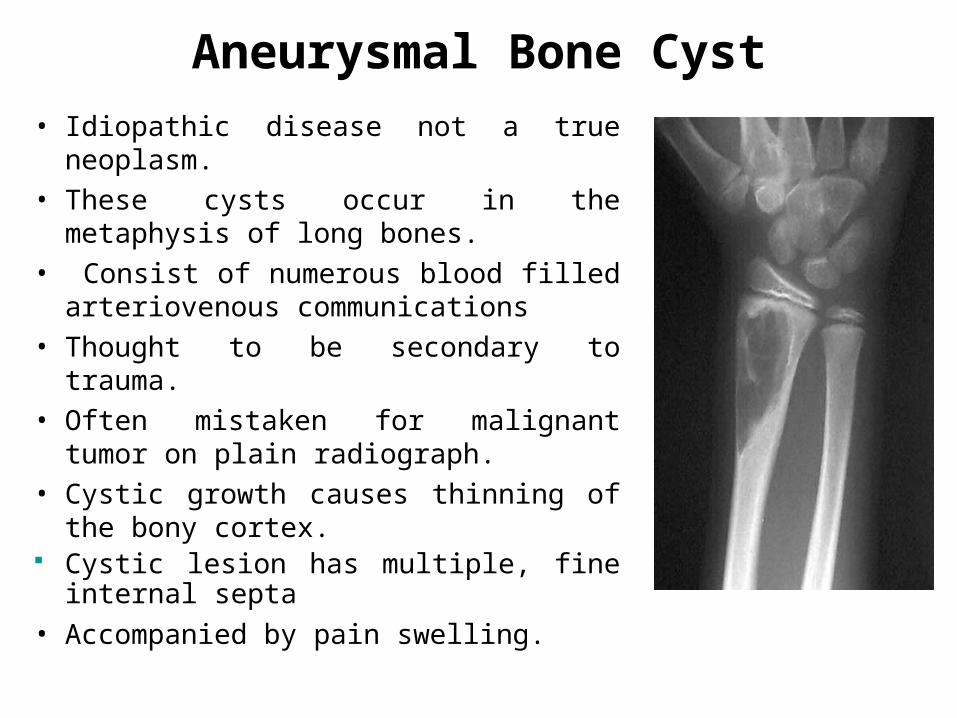
Aneurysmal Bone Cyst
• Idiopathic disease not a true neoplasm.
• These cysts occur in the metaphysis of long bones.
• Consist of numerous blood filled arteriovenous communications
• Thought to be secondary to trauma.
• Often mistaken for malignant tumor on plain radiograph.
• Cystic growth causes thinning of the bony cortex.
Cystic lesion has multiple, fine internal septa
• Accompanied by pain swelling.
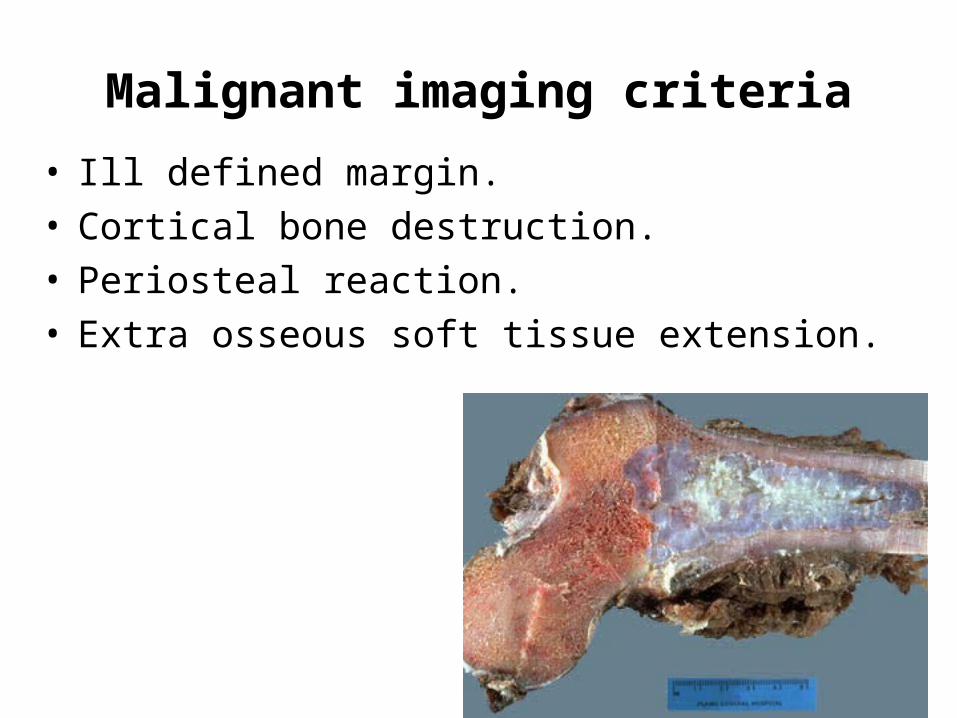
Malignant imaging criteria
• Ill defined margin.• Cortical bone destruction.• Periosteal reaction.• Extra osseous soft tissue extension.
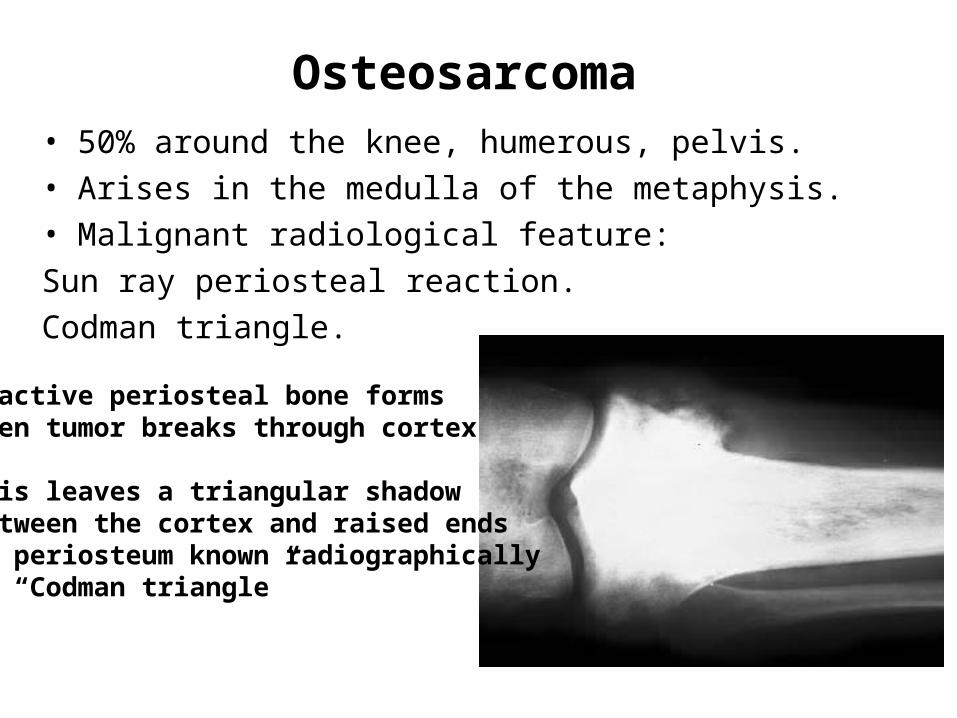
Osteosarcoma • 50% around the knee, humerous, pelvis.
• Arises in the medulla of the metaphysis.
• Malignant radiological feature:
Sun ray periosteal reaction.
Codman triangle.
Reactive periosteal bone formswhen tumor breaks through cortex
This leaves a triangular shadow between the cortex and raised endsof periosteum known radiographicallyas “Codman triangle”

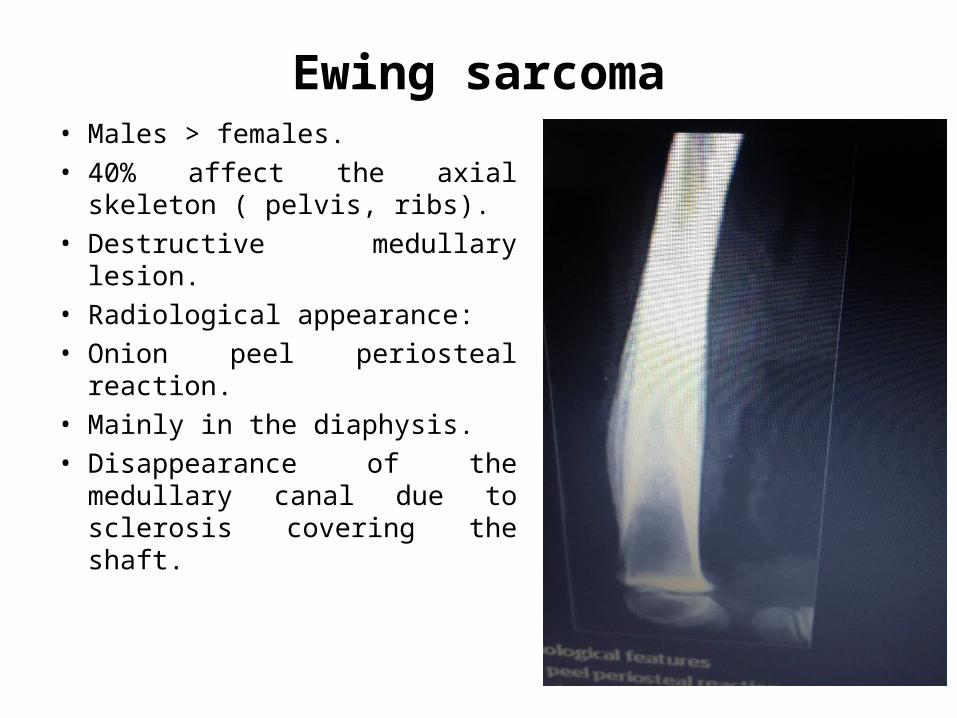
Ewing sarcoma• Males > females.
• 40% affect the axial skeleton ( pelvis, ribs).
• Destructive medullary lesion.
• Radiological appearance:
• Onion peel periosteal reaction.
• Mainly in the diaphysis.
• Disappearance of the medullary canal due to sclerosis covering the shaft.
Chondrosarcoma • Malignant tumor of cartilaginous origin.
• 10% of all malignant tumors of the skeletal system are chondrosarcomas.
• Common locations: pelvis, shoulder, and ribs.
• Men (older) > women 3 times.
• Tend to destroy the bone as they extend through the cortex into the surrounding soft tissue.
• Radiographic appearance: it shows irregular or circular radiolucencies in combinations with granular areas of calcifications.
• These tumors cause destruction and penetration of the cortex and extension of the soft tissues.
• Signs of malignancy + calcium inside the tumor = chondrosarcoma