Embed Size (px)
Citation preview

1
Mary L. Bouxsein, PhD
Beth Israel Deaconess Medical CenterHarvard Medical School, Boston, MA
UCSF Osteoporosis CourseJune 2013
Beyond BMD:
Bone Quality andBone Strength
Disclosures
Consultant / advisor:Amgen, Eli Lilly, Merck
Research funding:Amgen, Merck
Outline
• Determinants of Bone Strength
• Limitations of BMD
• Beyond BMD
• Biomechanics of Fractures: Comparing applied loads to strength
Structural failure of the skeleton

2
Design of a Structure
• Consider what loads it mustsustain
• Design options– Overall geometry– Building materials– Architectural details
Determinants of Whole Bone StrengthMorphologysize (mass)shape (distribution of mass)porositymicroarchitecture
Properties of Bone Matrixmineralizationcollagenmicrodamage…others…
Bouxsein, Osteop Int, 2003
Hierarchical Structure of Bone
Cell nanometer
Matrix100’s nanometer
LamellarOsteonal
micron
µ-architecture
micron to 100’s micron
Whole Bone
millimeter andbeyond
Assessing BoneBiomechanical Properties
DISPLACEMENT
LOAD
StructuralProperties
MaterialProperties

3
Biomechanical TestingKey Properties
DISPLACEMENT
LOAD
Strength
Energy absorbed (toughness)
Stiffness
Mechanical Behavior of Common Materials
Plastic(ductile)
Glass (brittle)
Deformation (Strain)
Load(Stress)
Mechanical Behavior of Bone and Its Constituents
Bone
Collagen
Mineral
Strain
Stress
Outline
• Osteoporosis & Bone Strength
• Limitations of BMD

4
Clinical Assessment of Bone Strength
Areal BMD by DXA• Bone mineral / projected area (g/cm2)• Reflects (indirectly)
– Bone size– Mineralization
• Moderate to strong correlation withwhole bone strength (r2 = 50 - 90%)
• Strong predictor of fracture risk inuntreated women (Marshall et al, 1996) Bouxsein et al, 1999
Hip BMD T-score (SD)-3 -2 -1 0 1
0
10
20
50
60
70
80Age (yrs)
10 Y
ear F
ract
ure
Prob
abili
ty (%
)
Kanis et al, 2004
Age and BMD Are Independent Risk Factors for HipFracture
> 5-fold increase infracture probabilityfrom age 50 to 80
History of Previous Fracture is a Risk Factor for Future Fracture,Independent of BMD
0 1 2 3 4 5 6
Vert Frx
No Vert Frx
5.83.4
2.3
1.71.0
0.2
Risk of Vertebral Fractures (% / yr)
Ross et al, Ann Int Med, 1991
LowMiddleHigh
BMD Tertiles
* Based on WHO guidelines for Osteoporosis Diagnosis
Fracture risk prediction:Less than half of patients who fracture have
osteoporosis by BMD testing(ie t-scores > -2.5*)
• Only 34% of women and 21% of men suffering a non-vertebralfrx had BMD in osteoporotic range (Schuit et al, 2004; 2006)
• Only half of elderly women with incident hip frx had BMD inosteoporotic range at baseline (Wainwright et al , JCEM 2005)

5
Outline
• Osteoporosis & Bone Strength
• Limitations of BMD
• Beyond BMD
Bone Strength
MORPHOLOGYsize & shape
microarchitecture
MATRIX PROPERTIESmineralizationcollagen traits
etc…
OSTEOPOROSIS DRUGS
Bouxsein, Best Practice in Clin Rheum, 2005
BONE REMODELINGformation / resorption
Bone Strength
MORPHLOGYsize & shape
microarchitecture
MATRIX PROPERTIEStissue compositionmatrix properties
BONE REMODELINGformation / resorption
Distribution of Mass Affects MechanicalBehavior
Moment of Inertiaproportional to d4
d

6
Effect of cross-sectional geometry onlong bone strength
↑
↑↑↑
↑
↑↑
=
=
Compressive Strength
Bending Strength
===aBMD (by DXA)
Bone Strength
SIZNE & SHAPEmacroarchitecturemicroarchitecture
MATRIX PROPERITEStissue compositionmatrix properties
BONE REMODELINGformation / resorption
Age-Related Changes in Trabecular Microarchitecture
Decline in bone massand deterioration of
trabecular bonestructure both
contribute to decreasedbone strength.
Excessive Bone Resorption Weakens TrabecularArchitecture
Perforation
Stress concentration(focal weakness)
L. Mosekilde, 1998

7
Effect of Resorption Cavities on Trabecular BoneStrength
van der Linden, et al, JBMR 2001
20% decrease in bone mass
1) trabecular thinning↓
30% decrease in strength
2) add resorption cavities
↓ 50% decrease in strength
Effect of Density Reduction on Strength:Change in Trabecular Thickness vs. Number
Density Reduction (%)
Residual Strength
(%)
5 10 150
25
50
75
100
0
Silva and Gibson, Bone, 1997
TrabecularThickness
TrabecularNumber
20% reductionin strength
65% reductionin strength
Microarchitectural changes thatinfluence bone strength
Force required to cause aslender column to buckle:
• Directly proportional to– Column material– Cross-sectional geometry
• Inversely proportional to– (Length of column)2
Force
Mosekilde, Bone, 1988
L
Theoretical effect of cross-struts on bucklingstrength
Buckling Strength proportional to (Strut Length)2
# Horizontal Effective Buckling Trabeculae Length Strength
0 L S
1 1/2 L 4 x S

8
Dramatic Changes in Trabecular Architecture in EarlyPostmenopausal Women
Dufresne TE et al. Calcif Tissue Int. 2003;73:423-432.
Baseline 1 yr
(52 yr old woman, 3 yrs post-menopause)
Anti-Resorptive Tx Preserves Trabecular Architecture in EarlyPostmenopausal Women
(Placebo vs Risedronate, 5 mg/d, 1 yr)
*P<0.05 vs baseline.†P< 0.05 vs PBO.
PBO (n=12)
Trabecularnumber
Trabecularseparation
Trabecularbone volume
–3.3 *
–20.3*
–13.5 *
13.1 *
0
5
10
15
% c
hang
e fr
om b
asel
ine
SpineBMD
5
1015
20
Dufresne TE et al. Calcif Tissue Int. 2003; 73:423-432.
RIS (n=14)
2.0 *
15.2
6.4
–7.2
†
†
†
†
20 yr old 80 yr old
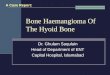
Age-related changes in femoral neck cortex andassociation with hip fracture
Those with hip fractures have:
• Preferential thinning of the inferior anterior cortex• Increased cortical porosity
Bell et al. Osteop Int, 1999; Jordan et al. Bone, 2000
Mayhew et al, Lancet 2005
Porosity is profound inthe aging femoral neck
Bousson et al, JBMR, 2004
19 elderly femalecadavers (87 ± 8 yrs)
Intracortical porosityranged from 5% to 39%

9
Cortical porosity and trabecularization of theendocortical surface with age
Zebaze et al, Lancet 2010
29 yr
67 yr
90 yr
Bone loss (mg/HA)CorticalTrabecular
Cortical bone lossincreases with age.
Prior studies have likelyunderestimated cortical
bone loss
50-64 65-79 > 80 yrs
Bone Strength
GEOMETRYmacroarchitecturemicroarchitecture
MATERIALtissue compositionmatrix properties
BONE REMODELINGformation / resorption
How is mineralization density influenced by rate ofbone turnover?
• Slow process of 2o
mineralization
• Decreased boneturnover allowsmineralization toproceed
Primarymineralization
(3 months)
Secondarymineralization
(years)
Time
Degree ofMineralization (%)
100-
50 -
0 -
Increased bone turnover with estrogen deficiencydecreases mineralization density
Meunier and Boivin,Bone, 1997

10
Relationship between mineralization andbiomechanical properties
Normal
Low(osteomalacia)
High(osteopetrosis)
Displacement
Load
Mineralization
Stiffness Strength
Toughness
Bone remodeling & microdamage
What is “damage” ?
– Repetitive loading
– No repair process– ↓ Mechanical properties
Microdamage in Bone
• Associated with decreased cortical bonestrength
• Microcracks seen in human femur & vertebra,increase with age
• Signal for remodeling & repair– in animals, microdamage increases when
remodeling is suppressed
• No demonstrated relationship with fracturerisk
Schaffler, 1995; Wenzel et al, 1996; Mashiba et al, 2001; Burr et al 1997, 2002; Arlot et al 2008
Fazzalari et al, Bone, 1998
Human femoral neck
Age-related changes in bone properties thatlead to decreased bone strength
• Decreased bone mass and BMD
• Altered geometry
• Altered architecture
– Cortical thinning– Cortical porosity– Trabecular deterioration
• Altered matrix propertiesImages from L. Mosekilde, Technology andHealth Care. 1998
young
elderly

11
Whole bone strength declinesdramatically with age
0
2000
4000
6000
8000
10000 Femoral Neck(sideways fall)
young
old
Courtney et al, J Bone Jt Surg 1995; Mosekilde L. Technology and Health Care. 1998.
Lumbar Vertebrae(compression)
Who
le B
one
Stre
ngth
(New
tons
)
0
2000
4000
6000
8000
10000
young old
Outline
• Determinants of Bone Strength
• Limitations of BMD
• Beyond BMD
• Biomechanics of Fractures: Comparing applied loads to strength
Fracture Etiology
FRACTURE?
Loads applied to the bone
Bone StrengthΦ = Applied Load
Failure Load
FRACTURE?
Loads applied to the bone
direction & magnitude
Bone strengthGeometry
MicrostructureMaterial Properties
Fall traitsProtective responsesSoft-tissue padding
Impact surface
Propensity to fall
Bending, lifting activity
Spine curvatureMuscle strength
Disc degeneration

12
Biomechanics of HipFracture
• Over 90% of hip fx’s associated with a fall
• Less than 2% of falls result in hip fracture
• Fall is necessary but not sufficient
• What is a high risk fall ?
Independent Risk Factors for Hip Fx
Factor Adjusted Odds Ratio
Fall to side 5.7 (2.3 - 14)↓ Femoral BMD 2.7 (1.6 - 4.6)*↑ Fall energy 2.8 (1.5 - 5.2)**↓ Body mass index 2.2 (1.2 - 3.8)*
* calculated for a decrease of 1 SD** calculated for an increase of 1 SD
Greenspan et al, JAMA, 1994
Estimating Loads Applied to the Hip
In young volunteers, only 2/6 wereable to break the fall
85% of impact force delivereddirectly to femur
Force ↑ by ↑ body wt
Force ↓ by ↑ thickness oftrochanteric soft tissue
Peak impact forces applied to greater trochanter:270 - 730 kg (600 - 1600 lbs)
(for 5th to 95th percentile woman)Robinovitch et al, 1991; 1997; van den Kroonenberg et al 1995, 1996
Peak impact forces applied to greater trochanter:270 - 730 kg (600 - 1600 lbs)
(for 5th to 95th percentile woman)Robinovitch et al, 1991; 1997; van den Kroonenberg et al 1995, 1996
Very high forces appliedto the hip during a
sideways fall
• Human cadavers• Human volunteers• Crash dummy• Mathematical models and
simulations

13
Femoral ‘strength’ depends on loading direction
Stance Sideways Fall
Femur is weak in atypical loading conditions
Keyak et al, J Biomechanics, 1998
0123456789
Stance Sideways Fall
Failu
re L
oad
(kN
)
P < 0.0013.4-fold lower
2318 ± 300 N7978 ± 700 N
0
2000
4000
6000
8000
10000
Fem
ur S
tren
gth
(New
tons
)
Young(age = 33)
Old(age = 74)
Courtney et al, J Bone Jt Surg 1995
Load duringsideways fall}
Femoral strength in sideways falldeclines markedly with age
Older femurs are half as strongand absorb 1/3 as much energyas young femurs
Biomechanics of Vertebral Fractures
• Difficult to study– Many do not come to clinical
attention– Slow vs. acute onset– The event that causes the fracture is
often unknown
• Poor understanding of the relationshipbetween spinal loading and vertebralfragility

14
Estimating Loads on the Spine
Biomechanical model• Simulate bending and lifting activities• Height, weight, body position
• Determine compressive forces onvertebra for different activities
Φ = Applied LoadFailure Load
Standing 51
Rise from chair 173
Stand, hold 8 kg, 230arms extended
Stand, flex trunk 30o, 146arms extendedLift 15 kg from floor 319for a 162 cm, 57 kg woman
Activity Load (% BW)
Predicted Loads on Lumbar Spine for Activitiesof Daily Living
Ratio of load to strength for L3 during activities ofdaily living
Adapted from Myers and Wilson, Spine, 1997
1.5
2.6 1.1 0.7
2.1 0.9
3.7 1.5 1.0 0.7
3.0 1.3 0.8
1.1
1.4
1.4
0.6 0.4 0.3 0.2 0.2
0.5 0.4 0.3
0.6 0.4 0.3 0.3
0.6 0.5
0.6 0.5 0.4
0.5 0.3 0.2 0.2 0.1
0.6 0.4 0.3 0.2 0.2
0.6 0.4 0.3 0.2 0.2
Get up from sitting
Lift 15 kgknees straightLift 15 kg w/deep knee bendLift 30 kgknees straightLift 30 kg w/deep knee bendOpen windoww/ 6 kg of forceOpen windoww/ 10 kg of forceTie shoessitting down
-3.5 -2.8 -2.2 -1.5 -0.8 0
Lateral Spine BMD t-score
Applied LoadBone Strength
Fracture PreventionStrategies
Reduce the Loads Applied to Bone– Decrease fall frequency / severity– Safe-landing strategies– Trochanteric padding– Avoid high risk lifting / bending activities
Maintain or Increase Bone Strength– Exercise, diet (Ca, Vit D), pharmacologic treatment

15
Summary: Factors Affecting Bone Strength andFracture Risk
Microarchitecture
Size & Shape LoadingMaterial