Embed Size (px)
Citation preview

Gut, 1988, 29, 378-384
Bone histomorphometry and structure incorticosteroid treated chronic active hepatitisA J STELLON, A WEBB, AND J E COMPSTON
From the Liver Unit, King's College Hospital, London, andThe Department of Histopathology, St Thomas' Hospital, London
SUMMARY Transiliac biopsies from 34 female patients with corticosteroid treated chronic activehepatitis have been examined to determine the contributions made by decreased bone formation andincreased bone resorption to bone loss associated with this condition and to determine the structuralbasis of the bone loss. Mean wall thickness was significantly reduced when compared with controlvalues (p<0.001) as was the bone formation rate at tissue (p<O.OO5) and basic multicellular unit(p<0005) level. The osteoid maturation period and the bone formation period were significantlyprolonged (p<0-02 and 0.05). The total resorption surfaces were significantly increased (p<0.02)but the mean interstitial bone thickness was normal. The mean trabecular plate thickness wassignificantly reduced (p<0.005). These findings indicate that decreased bone formation plays amajor role in bone loss associated with corticosteroid treated chronic active hepatitis and that thestructural basis of bone loss is trabecular thinning.
Reduced trabecular and cortical bone mass haverecently been reported in patients with autoimmunechronic active hepatitis (CAH) on maintenancecorticosteroids.12 Corticosteroids are known to in-duce bone loss, probably as a result both of directinhibition of bone formation and an increase inparathyroid hormone mediated bone resorptionsecondary to calcium malabsorption;`8 non-steroidtreated chronic liver disease is also associated with anincreased prevalence of osteoporosis.'3 Detailedbone histomorphometric studies in patients withchronic cholestatic or alcoholic liver disease haveshown that reduced bone formation plays a majorrole in bone loss, although increased resorption mayalso contribute;"'6 in addition, the mechanism ofbone loss in chronic cholestatic liver disease at themicroanatomic level appears to be trabecular thin-ning rather than erosion through and removal ofwhole trabecular elements. 5 The pathophysiology ofbone loss associated with steroid treated CAH has
Address for correspondence: Dr J E Compston, Department of Pathology,University of Wales College of Medicine, Cardiff, CF4 4XN.
Received for publication 24 September 1987.
not been reported. In this study we have examinedthe changes in bone histomorphometry and micro-anatomic structure in iliac crest biopsies from 34female patients with CAH receiving longterm corti-costeroid therapy.
Methods
PATIENTSThe 34 female patients, aged 20-66 years (19 post-menopausal), fulfilled internationally agreed criteriafor autoimmune CAH. 7 Twenty two of the 34patients had biopsy proven cirrhosis, documented inone or more biopsies, over a period of one to 12years. At the time of study all patients were inbiochemical and histological remission as defined bya serum aspartate transaminase (SGOT) level of lessthan 40 IU/l and a liver biopsy appearance of chronicpersistent hepatitis or an inactive cirrhosis withoutpiecemeal necrosis. All patients had received pred-nisolone for a minimum period of one year (median3-6 years; range 1-12) and were maintained on dosesof 5 mg/day in two patients, 7-5 mg/day (8), 10 mg/day (23), and 12-5 mg/day (1). Thirty one patients inaddition were receiving azathioprine 50-100 mg/day.
378
on June 20, 2022 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.29.3.378 on 1 March 1988. D
ownloaded from

Bone disease in chronic active hepatitis
Table 1 Clinical details ofpatients and controls
Chronic activeControls hepatitis(30) (34) p Value
Age 46.7 (14.9) 45 (15.6) NSPre-/postmenopausal 15/15 15/19Years since menopause 11.6 (9.2) 7.4 (4.6) NS
Results are expressed as mean (SD).
Two patients were on thyroxine replacement therapyfor myxoedema and thyroid function tests at the timeof study were normal. No patient had receivedprevious vitamin D or calcium supplementation andno patient had clinical evidence of steatorrhoea.Informed consent was obtained in all patients and thestudy was approved by the local Ethical Committee.Three patients at the time of study suffered lower
lumbar back pain and one patient generalised achesin all her limbs. Two patients had sustained fractures(wrist one, and humerus one) before corticosteroidtherapy and lateral radiographs of the thoracolumbarspine had revealed one patient with a wedgedvertebra.
Control data were obtained from 30 healthywomen (15 postmenopausal) aged 20-69 years, withno biochemical or radiological evidence of metabolicbone disease, who underwent an iliac crest biopsy atthe same time as a minor surgical procedure wasbeing carried out under general anaesthetic.'8 Thecontrols were comparable with the patients withrespect to mean age and years since menopause(Table 1). Quantitative analysis of both the CAH andhealthy control biopsies was carried out by one of us(AS) to exclude interobserver variation. Sectionswere coded so that the observer was unaware ofwhether they had been obtained from control orpatient biopsies.
BIOCHEMISTRYSerum concentrations of calcium, alkaline phos-phatase, albumin and urinary calcium and creatinineconcentrations were measured by standard methods.Serum calcium concentrations were corrected for theserum albumin concentration.'9 Serum 25-hydroxy-vitamin D concentrations were measured by a com-petitive protein binding assay after extraction andchromatography. Serum immunoreactive para-thyroid hormone (iPTH) levels were measured by anN-terminal immunoradiometric assay using an anti-body raised in sheep to synthetic 1-34 PTH peptide.2"
BONE HISTOLOGYFull thickness transiliac biopsies were obtained, witha modified Bordier trephine of 8 mm internal dia-
meter, 2 cm below and behind the anterior superioriliac spine. Two contiguous specimens were obtainedwhenever possible and were fixed in 10% phosphatebuffered formalin (pH 7) and embedded in methyl-methacrylate. Non-consecutive 8 ,um sections werecut with a Jung K microtome and stained withhaematoxylin and eosin (H&E), solochrome cyaninR or by the von Kossa technique using a van Giesencounterstain; 15 [sm unstained sections were alsoprepared for fluorescence microscopy.
All volumes were measured by point counting andall surfaces quantified using a Zeiss integrating eye-piece, containing 25 points and 5 parallel lines. Thedistance between two fluorescent labels and allthickness measurements were made using an eye-piece micrometer. One division on the eyepiecegraticule was equivalent to 1-40 ,tm at 400x magni-fication.
The following static parameters were quantified:
Total trabecular bone volume (TBV; %)The total trabecular bone volume, mineralised andunmineralised, expressed as a percentage of the totalmedullary volume including bone and marrowspaces. A minimum of 100 fields from four or morevon Kossa stained sections were examined at 100xmagnification.
Relative osteoid surface (OS; %)The percentage of total trabecular bone surfacecovered by osteoid. A minimum of 100 fields or fouror more von Kossa stained sections were examined at100x magnification.
Specific surface of trabecular bone (S,; mm2/mm3)The number of square millimetres of trabecular bonesurface lying in a typical cubic millimetre of wholetrabecular bone tissue.2`
Surface to volume ratio (SIV; mm2/mm3)This is the amount of trabecular surface existing onthe typical cubic millimetre of trabecular bone.2'
Mean trabecular plate thickness (MTPT; ,um)This is an indirect measurement of the mean thick-ness of trabeculae and was derived as follows:
MTPT 200022S/V
Mean trabecular plate separation (MTPS; jim)This is an index of the distance between trabecularplates and is calculated as follows:
MTPS = MTPT1TBV-1
379
on June 20, 2022 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.29.3.378 on 1 March 1988. D
ownloaded from

Stellon, Webb, and Compston
M ea~.MeMn wallthicknessNormal
0D 0E i
CAH
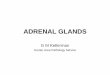
0 0~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~Fig. 1 Schematic representation oftrabecular bone remodelling in normal steady state circumstances and in corticosteroidtreated CAH. (a) shows a length ofa trabecula ofbone. Bone resorption by osteoclasts produces a resorption cavity (b) alongthe mineralised trabecular bone surface. Bone resorption is then followed by boneformation in which the previously erodedcavity isfilled in by osteoid whichfinally mineralises to produce bone (c). The mean thickness ofthe completed unit, whichrepresents the amount ofboneformed, is known as the mean wall thickness. In CAH the amount ofbone resorbed is normalbut the amount ofbone subsequentlyformed is reduced leading to net bone loss at each individual bone remodelling unit.
Mean trabecular plate density (MTPD;/mm)This provides an index of trabecular plate numberand is calculated as follows:
TBV (%) x 1022MTPD =
MTPT
Cortical thickness (CT; mm)This is the mean of the thickness of both inner andouter cortical plates. Measurements were done at 10equidistant points along each cortical plate perpen-dicular to its outer surface and the mean of thesevalues obtained.
Mean osteoid seam width (MOSW; Rm)This is the mean of four approximately equallyspaced measurements in each osteoid covered sur-face in one or two von Kossa stained sections yieldinga minimum of 80 readings. The osteoid seams weremeasured at x400 magnification.
Mean wall thickness (MWT; Rm)This represents the thickness of the completed bonestructural unit,23 (Figs 1, 2). Measurements weremade at x 400 magnification under polarised light, onsections stained with solochrome cyanin R. Fourequidistant measurements were made per packet anda minimum of 25 packets was measured from eachbiopsy from four or more sections.
Mean interstitial bone thickness (MIBT; Rm)This represents the mean thickness of the trabecularbone lying between two completed bone structuralunits in the trabeculae (Fig. 2) and is calculated asfollows:
MIBT = MTPT - (2 x MWT)24
Total resorption surfaces (TRS; %)The percentage of total trabecular bone surfaceshowing resorption cavities with or without osteo-clasts was measured in two H and E sections underpolarised light.2'
Dynamic parametersAll patients received the following tetracycline label-ling regimen of demeclocycline: 300 mg bd for twodays, followed after an interval of 12 days by 300 mgbd for four days. The bone biopsy was then takenthree to five days after the last dose. All fluorescencemicroscopy was done on unstained sections usingblue light (365 nm).
The following parameters were measured:
Mineral appositional rate (MAR,; sm/day)This is the mean of four equidistant measurementsmade along each double label in two or more sectionsat 400x magnification. A minimum of 60 readings
380
on June 20, 2022 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.29.3.378 on 1 March 1988. D
ownloaded from

Bone disease in chronic active hepatitis
-_ Bone formation at BMU levelt (BFR (BMU); Rm7/ [tm2/day)
The average amount of new mineralised bone madeMTPT per day per micrometer of osteoid covered surface,
calculated as follows:
BFR (BMU) = BFR (tissue)OS x 102
MIBT
;~~~TCAH MTPT
Fig. 2 Schematic diagram ofpart ofa trabecula to illustratethe mechanism ofbone loss and its effect on bone structure incorticosteroid treated CAH. The mean trabecularplatethickness is determined by the mean wall thickness (MWT)and the mean interstitial bone thickness (MIB T), therelationship between these three being expressed asMTPT= (2 xMWT) -MIB T. The mean wall thicknessrepresents the amount ofboneformedper remodelling cycleand the mean interstitial bone thickness is indirectlyproportioned to the depth ofthe initial resorption cavity. Incorticosteroid treated CAH boneformation is reduced,leading to a decreased mean wall thickness but resorptiondepth is normal (Fig. 1), so that the mean interstitial bonethickness is unchanged. The decrease in mean wall thicknessresults in a reduction in the mean trabecular plate thickness.
were obtained and the mineral appositional rate wascalculated as follows:
MARt(uncorrectedfor obliquity)
=Mean separation between labels
Time interval between the middleof the two labelling dose regimens
(days)
Total labelled surfaces (TLS; %)The length of single and double tetracycline labelledsurfaces expressed as a decimal fraction of the totaltrabecular bone surface. These were measured ontwo unstained sections at a magnification of x 100.
Bone formation at tissue level(BFR (tissue); Rm7/tm2/day)
The amount of new bone mineralised per micrometerof trabecular bone surface area per day calculated as
follows:
BFR (tissue) (DL + SL) x MARt21100
Bone formation period (a; days)The time taken for the formation of a complete bonepacket, calculated as follows:
MWT2'
BFR (BMU)
Mineralisation lag time (MLT)This is defined as the average lag time betweenapposition of collagen and initiation of mineral-isation of osteoid, and is calculated as follows:
MLT (days) = mB swBFR (BMU)
STATISTICAL ANALYSISA two-tailed Student's t test forcarried out on all data analysed.
unpaired data was
Results
The results of biochemical measurements are shownin Table 2. Serum calcium was decreased in twopatients both of whom were premenopausal. Serum25-hydroxyvitamin D concentrations were normal inall but three patients in whom subnormal levels (lessthan 12 nm/litre) were found. Two premenopausalpatients had raised iPTH levels. The mean fastingurinary calcium creatinine ratio was not significantlydifferent from controls despite six patients (five
Table 2 Biochemical data in patients
Chronic active Normalhepatitis range
Corrected serum calcium (mmol/l) 2-32 (0-08) 2-2 - 2-6Serum 25-hydroxyvitamin D (nmol/l) 49-9 (27) 12- 80Serum immunoreactive parathyroid 85.1 (82.6) <219hormone (pmol/l)
Fasting urinary calcium/creatinine 0-10 (0-09) 0-065 (0.05)ratio (mmol/mol)
Results are expressed as mean (SD); Conversion from SI totraditional units; serum calcium 1 mmol/l=4 mg/100 ml; serum25-hydroxyvitamin D 2.5 nmol/l=1 ng/ml; serum immunoreactiveparathyroid hormone 243 pmol/l=1 ng/ml; fasting urinary calcium/creatinine ratio 1 mmol/l calcium=4 mg/100 ml, 1 Rmol/l creatine=0-0113 mg/100 ml.
Normal
4MWT
MIBT
MT Iv 1%, 1
_.p
381
on June 20, 2022 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.29.3.378 on 1 March 1988. D
ownloaded from

Stellon, Webb, and Compston
Table 3 Static histomorphometric data in the patients andcontrols
CAH Controls(34) (30) p Value
Total trabecular bone 19 1 (4.6) 23.5 (5.8) <0(005volume (%)
Cortical thickness (mm) 1.09 (0.29) 1.30 (0.30) <0.005Mean trabecular plate 95.4 (19.7) 114 5 (25.9) <0 005
thickness (rm)Mean trabecular plate 2.02 (0.32) 208 (0.44) NS
density (/mm)Mean trabecular plate 414 (112) 390 (117) NS
separation (tm)Mean interstitial bone 21(15.5) 21(28) NS
thickness (tm)Osteoid surface (%) 12.0 (8.2) 12.3 (7.0) NSMean osteoid seam width 8 41 (2.02) 8-59 (2.36) NS
([tm)Mean wall thickness (tm) 37-3 (6.0) 47.0 (7.5) <0 001Total resorption surfaces 2 54 (1.24) 1.88 (0.69) <0 02(0)
Results are expressed as mean (SD).
postmenopausal) having raised ratios of greater than0- 16 mmol/mol.The mean trabecular bone volume was signific-
antly lower in the CAH patients (Table 3) whencompared with the control group (p<0-005). Al-together 14% patients had a trabecular bone volumevalue within the vertebral fracture threshold range of11(3)% .23 When compared with controls a statisticallysignificant decrease in mean trabecular plate thick-ness (p<0.005) but not mean trabecular plate densityor separation was found in the patients. No signific-ant differences in osteoid surface, mean osteoid seamwidth or mean interstitial bone thickness were detec-ted when compared with controls whereas the meanwall thickness was significantly decreased in thepatients (p<0.001). Total resorption surfaces weresignificantly higher in the patients when comparedwith controls (p<002) and 24% of patients hadincreased resorption surfaces (>2SD above mean ofage and sex-matched controls). Cortical plate thick-ness was decreased when compared with controls(p<0005).DYNAMIC HISTOMORPHOMETRIC INDICES(Table 4)Calculation of the mineral appositional rate andother dynamically derived parameters were not pos-sible in four patients because only single tetracyclinelabels were detectable. When compared with thecontrols the mineral appositional rate was signific-antly decreased although only one patient had asubnormal (>2SD) value. Total labelled surfaceswere significantly decreased in the patients
0 f0XC~
Fig. 3 Illustration ofthe two possible structuralmechanisms oftrabecular bone loss at a microanatomic level.In (a) trabecular thinning occurs, resulting in reduced bonevolume with preservation ofthe normal trabeculararchitecture. In thisform ofbone loss, the mean trabecularplate thickness is reduced but mean trabecular plate densityand separation remain unchanged. In (b), bone loss occursby erosion through and removal oftrabecular elements,leading to disruption and loss ofconnectivity ofthe normaltrabecularstructure. In this case the mean trabecularplatethickness is unchanged but mean trabecularplate densitydecreases and mean trabecularplate separation increases.In corticosteroid treated CAH mechanism (a) provides thestructural basisfor bone loss.
(p<0.005) when compared with controls as werethe bone formation rate at tissue level (p<0005) andBMU level (p<0 005). The osteoid maturationperiod (p<0.02) and bone formation period(p<005) were significantly prolonged when com-pared with the controls.When patients were separated into those with and
without cirrhosis, although age and mean daily doseof prednisolone and azathioprine were comparable inboth groups, no statistically significant difference wasfound between the two groups with respect to any ofthe histological parameters measured.Weak correlations were only found between main-
tenance dose of prednisolone and total resorptionsurfaces (r=0.4; p<005) and dose duration of corti-costeroid therapy and trabecular bone volume(r=-0.39; p<0.05) and cortical plate thickness(r=-0.36; p<0.05).
Discussion
Our results confirm previous reports2 of cortical andtrabecular osteoporosis in patients with corti-costeroid treated chronic active hepatitis and show
382
on June 20, 2022 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.29.3.378 on 1 March 1988. D
ownloaded from

Bone disease in chronic active hepatitis
Table 4 Dynamic histomorphometric data in the patientsand controls
CAH Controls p Value
Mineral appositional rate 0-68 (0.08) 0-74 (0.12) <0-05(>tm/day)
Total labelled surfaces (%) 6-91 (4.00) 12-9 (9.1) <0-005Bone formation rate - tissue 0-048 (0.030) 0-098 (0.063) <0-005
level ([&m31m2/day)Bone formation rate - BMU 0.45 (0.33) 0-99 (0.78) <0 005
level ( tm3/[m2/day)Bone formation period 129 (122) 70-6 (43.6) <0-05
(days)Mineralisation lag time 28-9 (31.0) 13-7 (8.4) <0-02
(days)
Results are expressed as mean (SD).
that reduced bone formation is a major contributoryfactor. The reduction in trabecular bone volume mayhave been underestimated as the decreased corticalplate thickness also observed probably resulted fromendosteal resorption, creating new trabeculae whichwould have been included in the area for quantifica-tion of trabecular bone volume. Nevertheless, 14%of the patients studied had a value for trabecularbone volume within the vertebral fracture thresholdrange of 11(3)%.23At a microanatomic level, trabecular bone loss
may be caused by either a thinning of the trabeculae,with preservation of trabecular architecture, or byerosion through and removal of trabeculae, thusreducing trabecular interconnectedness, or to a com-bination of both (Fig. 3). This study shows that thestructural basis for bone loss in corticosteroid treatedCAH is trabecular thinning rather than erosionthrough and removal of trabecular plates. Thus themean value for mean trabecular plate thickness wassignificantly reduced in the patient group without anysignificant accompanying change in mean trabecularplate separation and density, indicating preservationof the trabecular structural pattern. This pattern ofbone loss is similar to that observed in patients withprimary biliary cirrhosis'5 and jejunoileal bypass26and may be associated with a lower fracture riskthan bone loss involving loss of trabecular plates andreduced interconnectedness of trabeculae.27Mean wall thickness was significantly lower in the
patient group, indicating reduced bone formation.Further evidence of low bone formation comes fromthe finding of a reduced bone formation rate at tissueand cellular level and the presence of only singletetracycline labelling in four patients. Although themean osteoid seam width was normal in the patients,this, in association with a decreased mineralisationrate and prolonged osteoid maturation period indi-cates a reduced osteoblastic appositional rate and
decreased matrix synthesis, as under conditions ofnormal matrix synthesis delayed mineralisationwould result in an increased osteoid seam width.Because the bone formation period was increased inthe patients, it seems likely that impaired function ofosteoblasts rather than a reduction in lifespan wasresponsible for the impairment of matrix synthesisand mineralisation.The mean total resorption surface was significantly
higher in patients than in controls, although onlysmall rises were seen. Measurement of total resorp-tion surface, however, does not indicate resorptionrate and values may be raised as a result of reducedbone formation leading to incomplete filling ofnormal resorption cavities. The biochemical indica-tors of bone resorption measured in this study,namely serum iPTH and urinary calcium/creatinineratio were similar in patients and controls, althoughtwo patients had raised iPTH concentrations andurinary calcium creatinine ratios were increased infive patients. The most compelling evidence against acontribution by increased bone resorption to thebone loss seen comes from the measurements ofmean interstitial bone thickness, which reflect theamount of bone at the BMU level which has under-gone resorption in the past (Fig. 2), values for meaninterstitial bone thickness in the patient group beingextremely similar to those of controls. This differsfrom the finding that, in patients with primary biliarycirrhosis, values for mean interstitial bone thicknesswere significantly decreased, indicating that resorp-tion had been increased in the past.'5The relative contributions made by liver disease
and corticosteroid therapy to the bone loss seencannot be assessed in a study of this kind. Mostpatients in this study were also receiving azathio-prine; however, no effect of this drug on boneremodelling has been reported. The decreased boneformation and increase in total resorption surfacesobserved in the present study are compatible withchanges reported in corticosteroid induced bone lossin patients with normal liver function,35828 as well asin non-steroid treated patients with chronic liverdisease." 4 The evidence for increased activation ofremodelling sites, however, reported in some studiesof corticosteroid osteoporosis, with an increase notonly in total resorption surface but also in osteoidsurface4 21 and tetracycline labelled surfaces28 was notencountered in the present study. The observationthat spinal trabecular bone mineral content, mea-sured by quantitative computed tomography is lowerin patients with steroid treated CAH than in thosewith other forms of chronic liver disease29 providesindirect evidence that corticosteroid therapy mayexacerbate the bone loss associated with chronic liverdisease. The demonstration that bone loss associated
383
on June 20, 2022 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.29.3.378 on 1 March 1988. D
ownloaded from

384 Stellon, Webb, and Compston
with steroid treated CAH is predominantly a result ofdecreased bone formation suggests that the role ofagents which increase bone formation - for example,sodium fluoride, should be evaluated in thesepatients.
The authors thank Advisory Services (Clinical andGeneral), Roba Pharmaceuticals Limited and theSpecial Trustees, St Thomas' Hospital for generalfinancial support. We thank Dr Roger Williams forallowing us to study his patients.
References
1 Kato, Y, Epstein 0, Dick R, Sherlock S. Radiologicalpatterns of cortical bone modelling in women withchronic liver disease. Clin Radiol 1982; 33: 313-7.
2 Stellon AJ, Davies A, Compston JE, Williams R. Boneloss in autoimmune chronic active hepatitis on mainten-ance corticosteroid therapy. Gastroenterology 1985; 89:1078-83.
3 Gallagher JC, Aaron J, Horsman A, Wilkinson R,Nordin BEC. Corticosteroid osteoporosis. Clin Endo-crinol 1973; 2: 355-68.
4 Hahn TJ. Corticosteroid-induced osteopenia. Arch In-tern Med 1978; 138: 882-5.
5 Hahn TJ, Halstead LR, Teitelbaum SL, Hahn BH.Altered mineral metabolism in glucocorticoid-inducedosteopenia. J Clin Invest 1979; 64: 655-65.
6 Adinoff AD, Hollister JR. Steroid-induced fracturesand bone loss in patients with asthma. N Engl J Med1983; 5: 265-8.
7 Rickers H, Deding A, Christiansen C, Rodbro P.Mineral loss in cortical and trabecular bone during highdose prednisone treatment. Calcif Tissue Int 1984; 36:269-73.
8 Bressot C, Meunier PJ, Chapuy MC, Lejeune E,Edouard C, Darby AJ. Histomorphometric profile,pathophysiology and reversibility of corticosteroid-induced osteoporosis. Metab Bone Dis Rel Res 1979; 1:303-11.
9 Matloff DS, Kaplan MM, Neer RM, Goldberg MJ,Bitman W, Wolfe HJ. Osteoporosis in primary biliarycirrhosis: effects of 25-hydroxy-vitamin D3 treatment.Gastroenterology 1982; 83: 97-102.
10 Herlong HF, Recker RR, Maddrey WC. Bone diseasein primary biliary cirrhosis: histologic features andresponse to 25-hydroxyvitamin D. Gastroenterology1982; 83: 103-8.
11 Stellon AJ, Davies A, Compston JE, Williams R.Osteoporosis in cholestatic liver disease. Q J Med 1985;57: 783-90.
12 Hodgson SF, Dickson ER, Wahner HW, Johnson KA,Mann KG, Riggs BL. Bone loss and reduced osteoblastfunction in primary biliary cirrhosis. Ann Intern Med1985; 103: 855-60.
13 Bikle DD, Genant HK, Cann C, Recker RR, HalloranBP, Strewler GJ. Bone disease in alcohol abuse. AnnIntern Med 1985; 103: 42-8.
14 Cuthbert JA, Pak CYC, Zerwekh JE, Glass KD,
Coombes B. Bone disease in primary biliary cirrhosis:increased bone resorption and turnover in the absenceof osteoporosis or osteomalacia. Hepatology 1984; 4:1-8.
15 Stellon AJ, Webb A, Compston JE, Williams R. Lowbone turnover state in primary biliary cirrhosis. Hepa-tology 1987; 7: 137-42.
16 Mobarhan SA, Russell RM, Recker RR, Posner DB,Iber FL, Miller P. Metabolic bone disease in alcoholiccirrhosis: a comparison of the effect of vitamin DI, 25-hydroxyvitamin D, or supportive treatment. Hepatology1984; 4: 266-73.
17 Review by an International Group. Acute and chronichepatitis revisited. Lancet 1977; ii: 914-9.
18 Vedi S, Compston JE, Webb A, Tighe JR. Histomor-phometric analysis of bone biopsies from the iliac crestof normal British subjects. Metab Bone Dis Rel Res1982; 4: 231-6.
19 Payne RB, Little AJ, Williams RB, Milner JR. Inter-pretation of serum calcium in patients with abnormalserum proteins. Br Med J 1973; 4: 643-6.
20 Addison GM, Hales CN, Woodhead JS, O'RiordanJLH. Immunoradiometric assay of parathyroid hor-mone. J Endocrinol 1971; 49: 521-30.
21 Frost HM. A method of analysis of trabecular bonedynamics. In: Meunier PJ, ed. Bone histomorphometry.Second International Workshop. Toulouse, France:Societe de la Nouvelle Imprimerie Fournie, 1977:445-76.
22 Parfitt AM, Mathews CHE, Villanueva AR,Kleerekoper M, Frame B, Rao DS. Relationshipsbetween surface, volume, and thickness of iliactrabecular bone in ageing and osteoporosis. J Clin Invest1983; 72: 1396-409.
23 Meunier PJ, Courpron P, Edouard C, et al. Bonehistomorphometry in osteoporosis. In: Barzel VS, ed.Osteoporosis II. New York: Grune and Stratton, 1979:27-47.
24 Courpron P, Lepine P, Arlot M, et al. Mechanismsunderlying the reduction with age of the mean wallthickness of trabecular basic structure unit (BSU) inhuman iliac bone. In: Jee WSS, Parfitt AM, eds. Bonehistomorphometry. Third International Workshop.Paris, France: Societe Nouvelle de PublicationsMedicales et Dentaires, 1981: 323-9.
25 Vedi S, Tighe JR, Compston JE. Measurement of totalresorption surface in iliac crest trabecular bone in man.Metab Bone Dis Rel Res 1984; 5: 275-80.
26 Parfitt AM, Podenphant J, Villanueva AR, Frame B.Metabolic bone disease with and without osteomalaciaafter intestinal bypass surgery: a bone histomorpho-metric study. Bone 1985; 6: 211-20.
27 Kleerekoper M, Villanueva AR, Stanciu J, Rao DS,Parfitt AM. The role of three dimensional trabecularmicrostructure in the pathogenesis of vertebral com-pression fractures. Calcif Tissue Int 1985; 37: 594-7.
28 Dempster DW, Arlot MA, Meunier PJ. Mean wallthickness and formation periods of trabecular bonepackets in corticosteroid-induced osteoporosis. CalcifTissue Int 1983; 35: 410-7.
29 Rose JDR, Crawley EO, Evans WD, et al. Osteoporosisin chronic liver disease. Bone 1987; 8: 53.
on June 20, 2022 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.29.3.378 on 1 March 1988. D
ownloaded from