Embed Size (px)
DESCRIPTION
Papers from the Trust Board Meeting held Thursday 30th April 2015
Citation preview
Surrey and Sussex Healthcare NHS Trust
Board Papers
April 2015
Trust Board Meeting – IN PUBLIC
Thursday 30th April 2015 - 10:00 to 12:30
AD77, Trust Headquarters, East Surrey Hospital, Canada Avenue, Redhill, RH1 5RH
AGENDA
1
10:00
GENERAL BUSINESS 1.1 Welcome and apologies for absence 1.2 Declarations of Interests & Annual Declaration of
Interests Report – For Assurance 1.3 Minutes of the last meeting held on 26th March 2015 - For approval 1.4 Action tracker 1.5 Chairman’s Report
For assurance
1.6 Chief Executive’s Report For assurance
1.7 Board Assurance Framework & Significant Risk Register – For Assurance
A McCarthy A McCarthy/ G Francis-Musanu A McCarthy A McCarthy A McCarthy M Wilson G Francis- Musanu
Verbal
1.2_Annual Board Declaration of Interes
1.3_Minutes in Public 26.3.15.pdf
1.4_ACTION TRACKER - TB.pdf
Verbal
1.6_CEO Report.pdf
1.7_BAF & SRR report.pdf
1.7a_SRR April 2015.pdf
2
10:30
SAFETY, QUALITY AND PATIENT EXPERIENCE 2.1 Patient Story
For discussion & Assurance
2.2 Clinical Presentation - PROMS For discussion & Assurance 2.3 Chief Nurse & Medical Director’s Report
For assurance
2.4 Safety & Quality Committee Update For assurance
D Holden D Holden D Holden/ F Allsop R Shaw
2.1_Patient Story Executive Summary.p
2.2_Front Cover - Clinical Presentation o
2.2_Clinical Presentation - PROMS
2.3_CN MD Report.pdf
2.3_Appendix 1 - Staff Template.pdf
2.3_Appendix 2 - Research Recruitmen
2.3_Appendix 3 - Research Recruitmen
2.4_SQC Chair Update.pdf
3
11:15
OPERATIONAL PERFORMANCE 3.1 Integrated Performance Report (M12)
For assurance
3.2.1 Operational & Quality Key Performance Indicators
3.2.2 Workforce Key Performance Indicators 3.2.3 Finance Key Performance Indicators
P Bostock D Holden/ F Allsop F Allsop P Simpson
3.1_UPDATED Integrated Performan
3.2 Finance & Workforce Committee Update
For assurance
3.3 Charitable Funds Committee Update
R Durban Y Robbins
3.3_Charitable Funds Update.pdf
4
11:55
RISK, REGULATORY AND STRATEGY ITEMS 4.1 Care Quality Commission Action Plan Update For assurance 4.2 Quarterly Serious Incidents Report For assurance 4.3 Annual Board & Sub-Committee Attendance Report For assurance 4.4 Annual Plan – Q4 Update For assurance 4.5 Board Governance Self Certification For Approval
S Jenkins F Allsop G Francis-Musanu S Jenkins G Francis- Musanu
4.1_CQC Action Plan Update.pdf
4.2_Serious Incident Report.pdf
4.3_Annual Review of Board Sub-Commit
4.4_Annual Operating Plan Updat
4.4a_UPDATED Operating Business Pl
4.5_Trust Board Self Certification.pdf
5
12:25
OTHER ITEMS 5.1 Minutes from Board Committees
to receive & note 5.1.1 Finance and Workforce Committee
5.1.2 Safety & Quality Committee 5.1.3 Charitable Funds Committee
5.2 ANY OTHER BUSINESS 5.3 QUESTIONS FROM THE PUBLIC
Questions from members of the public may be submitted to the Chairman in advance of the meeting by emailing them to [email protected]
5.4 DATE OF NEXT MEETING
28th May 2015 at 10.00am
All A McCarthy A McCarthy
5.1.2_SQC Minutes 5-3-15 final.pdf
5.1.3_Charitable Funds - Minutes 24 No
TRUST BOARD IN PUBLIC
Date: 30th April 2015 Agenda Item: 1.2
REPORT TITLE: BOARD ANNUAL DECLARATION OF INTERESTS
EXECUTIVE SPONSOR: Gillian Francis-Musanu Director of Corporate Affairs
REPORT AUTHOR (s): Gillian Francis-Musanu Director of Corporate Affairs
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date) N/A
Action Required:
Approval ( ) Discussion ( ) Assurance (√)
Purpose of Report:
To provide assurance to the Board on its statutory and regulatory requirements.
Summary of key issues
Under the Standing Orders of the Corporate Governance Manual, all staff including Board members have a statutory obligation to declare external interests relating to their own or that of their partner which are relevant and material to the Trust.
This report is the current annual declaration of interests by the Board at April 2015.
Recommendation:
The board is asked to receive the report.
Relationship to Trust Strategic Objectives & Assurance Framework:
SO1: Safe -Deliver safe services and be in the top 20% against our peers SO2: Effective - Deliver effective and sustainable clinical services within the local health economy SO3: Caring – Ensure patients are cared for and feel cared about SO4: Responsive – Become the secondary care provider and employer of choice our catchment population SO5: Well led: Become an employer of choice and deliver financial and clinical sustainability around a clinical leadership model
Corporate Impact Assessment:
Legal and regulatory impact Each member of the Board has a statutory obligation of declare external interests
Financial impact A requirement of Trust Standing Orders
Patient Experience/Engagement N/A
Risk & Performance Management None identified in the report
NHS Constitution/Equality & This report will be available on the Trust
2An Associated University Hospital of Brighton and Sussex Medical School
Diversity/Communication website and is subject to Freedom of Information requests.
Attachment:
BOARD MEMBERS’ REGISTER OF INTERESTS April 2015
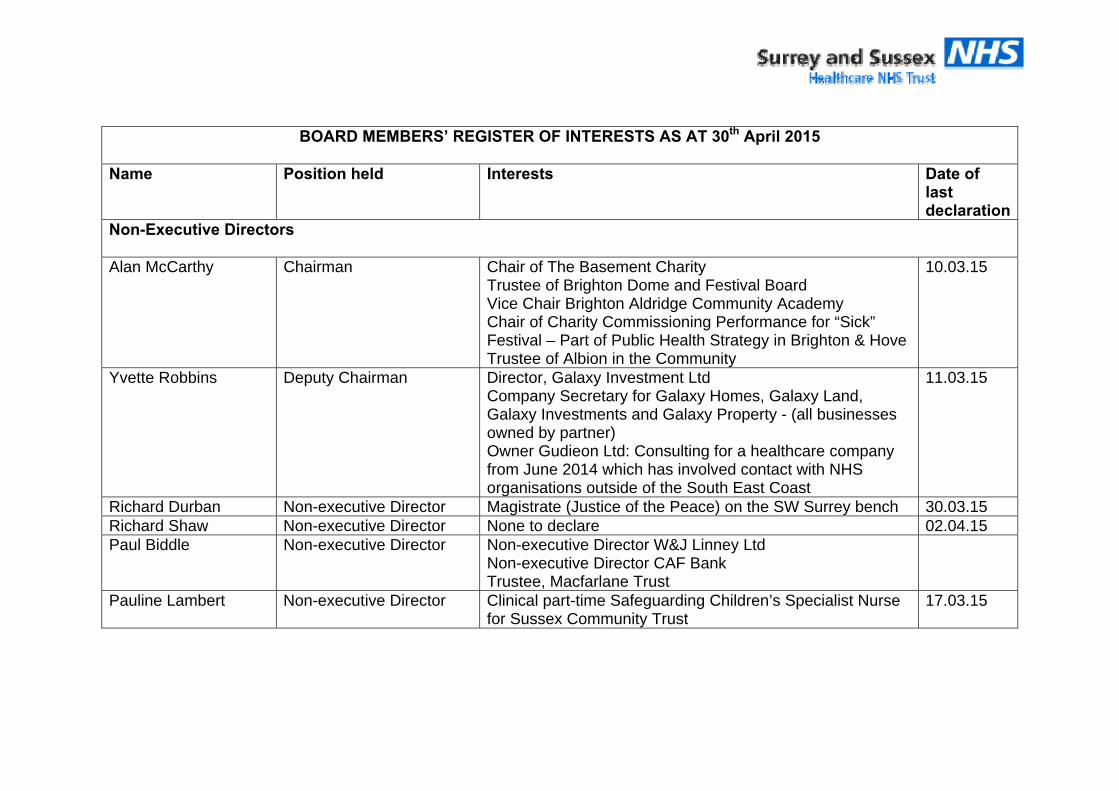
BOARD MEMBERS’ REGISTER OF INTERESTS AS AT 30th April 2015
Name Position held Interests Date of
last declaration
Non-Executive Directors Alan McCarthy Chairman Chair of The Basement Charity
Trustee of Brighton Dome and Festival Board Vice Chair Brighton Aldridge Community Academy Chair of Charity Commissioning Performance for “Sick” Festival – Part of Public Health Strategy in Brighton & Hove Trustee of Albion in the Community
10.03.15
Yvette Robbins Deputy Chairman Director, Galaxy Investment Ltd Company Secretary for Galaxy Homes, Galaxy Land, Galaxy Investments and Galaxy Property - (all businesses owned by partner) Owner Gudieon Ltd: Consulting for a healthcare company from June 2014 which has involved contact with NHS organisations outside of the South East Coast
11.03.15
Richard Durban Non-executive Director Magistrate (Justice of the Peace) on the SW Surrey bench 30.03.15 Richard Shaw Non-executive Director None to declare 02.04.15 Paul Biddle Non-executive Director Non-executive Director W&J Linney Ltd
Non-executive Director CAF Bank Trustee, Macfarlane Trust
Pauline Lambert Non-executive Director Clinical part-time Safeguarding Children’s Specialist Nurse for Sussex Community Trust
17.03.15
4 An Associated University Hospital of Brighton and Sussex Medical School
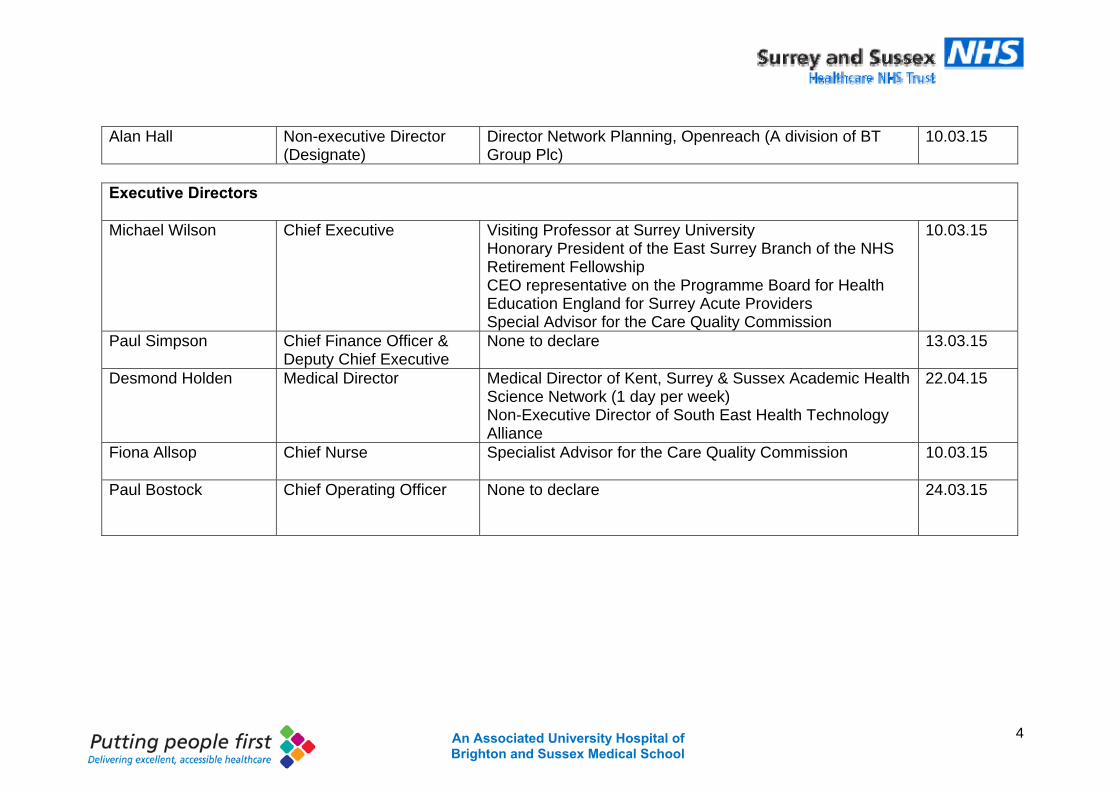
Alan Hall Non-executive Director
(Designate) Director Network Planning, Openreach (A division of BT Group Plc)
10.03.15
Executive Directors Michael Wilson Chief Executive Visiting Professor at Surrey University
Honorary President of the East Surrey Branch of the NHS Retirement Fellowship CEO representative on the Programme Board for Health Education England for Surrey Acute Providers Special Advisor for the Care Quality Commission
10.03.15
Paul Simpson Chief Finance Officer & Deputy Chief Executive
None to declare 13.03.15
Desmond Holden Medical Director Medical Director of Kent, Surrey & Sussex Academic Health Science Network (1 day per week) Non-Executive Director of South East Health Technology Alliance
22.04.15
Fiona Allsop
Chief Nurse Specialist Advisor for the Care Quality Commission 10.03.15
Paul Bostock
Chief Operating Officer None to declare 24.03.15
Page 1 of 12
Minutes of Trust Board meeting held in Public Thursday 26th March 2015 from 10:00 to 12:30
Room 7/8, PGEC East Surrey Hospital
Present
(AM) Alan McCarthy Chairman (MW) Michael Wilson Chief Executive (PS) Paul Simpson Chief Finance Officer / Deputy Chief Executive (PBo) Paul Bostock Chief Operating Officer (DH) Des Holden Medical Director (FA) Fiona Allsop Chief Nurse (SB) Sally Britain Deputy Chief Nurse (PBi) Paul Biddle Non-Executive Director (RD) Richard Durban (Non-Executive Director) (RS) Richard Shaw Non-Executive Director (AH) Alan Hall Non-Executive Director In Attendance
(GFM) Gillian Francis-Musanu Director of Corporate Affairs (JM) Janet Miller Deputy Director of HR (SMB) Sacha Beeby Notes
1. General Business
1.1 Welcome and Apologies for absence The Chairman opened the meeting by welcoming Trust Board members, staff and members of the public. Apologies for absence were noted from Pauline Lambert (Non-Executive Director) and Yvette Robbins (Deputy Chair).
1.2 Declarations of Interest The Chairman asked whether any of the Board members had any declarations of interest; none were recorded.
1.3 Minutes of the last meeting – 26th February 2015 The minutes of the meeting held on the 26th February 2015 were approved as a true and accurate record.
1.4 Action Tracker The outstanding actions were updated and closed. FA agreed to present a paper to the Trust Board in April to describe a comparison of the current and aspirational position in terms of nursing staff ratios (1:7 during the day, 1:10 during the night). This comparison will better clarify the gap. Staff survey due to be discussed by the Board at today’s meeting (Agenda Item 4.4).
Page 2 of 12
1.5 Chairman’s Report for Assurance The Chairman reflected on some of the key issues which were addressed at a recently attended NHS Providers conference also attended by representatives of the Care Quality Commission (CQC), Monitor and NHS England. Local activity pressures were clearly replicated throughout the country, with a shortfall of approximately 15000 nurses and a 46% increase in the use of agency staff. A significant deficit for the health system is expected, with a clear message from Monitor that activity plans for both NHS Trusts and CCGs must be realistic. The CQC were able to demonstrate a clear correlation between leadership and quality through the evidence of their inspections programme of NHS Trusts to date. It noted that there was an unacceptable variation in quality. The CQC are now considering a programme to inspect care pathways, although it is unclear how this would be quality-rated. PS further explained that the growth in activity for 2014/15 had increased, with a significant difference between CCG activity contract plans and actual activity. PBi reflected that the CCGs are unable to set a realistic budget perhaps because funding does not support them to do so. The Board noted the Chairman’s verbal report for assurance.
1.6 Chief Executives report for Assurance The board received and noted the Chief Executive’s report in advance of the meeting. MW presented the report and highlighted the following; A report on the independent investigation into maternity and neonatal services at Morecambe Bay was published in March following a review of serious incidents within the maternity services which included the deaths of mothers and babies. The report makes 44 recommendations; 26 of which for the wider health system. As part of the wider NHS, SaSH has committed to review the report and take stock of the recommendations to ensure that all relevant lessons are learnt from this report. The government have introduced a requirement for providers to display CQC inspection ratings in order to improve transparency in the quality and safety of care provided to its patients throughout the Trust. SaSH currently displays the appropriate rating on its website and will ensure these are displayed once the posters have been made available from the CQC. This provides an opportunity for the Trust to also demonstrate what it has done in response to recommendations made within specific areas of the Trust (e.g. Outpatients department). The Trust has now been formally recommended by the Trust Development Authority to progress to the Monitor assessment phase of its journey to Foundation Trust status. The Trust will then be invited to a formal Board-to-Board with Monitor in June, with further challenge of the Executive Team in July and potential authorisation as a FT in August. This is great news for the Trust.
Page 3 of 12
The national ‘Breaking the Cycle’ initiative to rapidly improve patient flow will be implemented by the Trust over the course of one week, starting Tuesday 7th April 2015. The whole organisation and its health and social care partners will focus on improving the emergency care pathway and potential lessons learnt from this exercise will be shared with the Board in April. MW highlighted some of the key changes to be implemented during that week; All patients will be reviewed twice daily by a consultant and all wards will have a dedicated team of juniors to carry out tasks arising from the ward round in a timely manner. DH added that this approach to ward rounds has evidenced improved patient flow and patient outcome and will allow the Trust to challenge and test that assumption. All wards will have a Nurse in Charge attending the ward round and a liaison officer to help teams chase and resolve any delays. In response to a question, MW confirmed that the recent industrial action in relation to pay had resulted in an agreed settlement by Government. The Trust maintains a good relationship with its Trade Unions and very few members of staff chose to take action at that time. The Board duly noted and took assurance from the report.
1.7 Board Assurance Framework and Significant Risk Register for Approval and Assurance GFM introduced the BAF and SRR for discussion and approval by the Board. GFM highlighted that the BAF currently presents 19 risks, 3 of which are recorded as key strategic risks and red rated. The Board was asked to consider the proposals to reduce both the financial risk relating to divisional overspend (5.A.2) and the strategic risk for IT (5.F) to a risk rating of 12 as well as the closure of the strategic risk relating to clinical leadership (5.B). PS corrected: recommendation to reduce risk 5.A.2 to a risk rating of 10 (S5 x L2 = 10). RD added that the Finance & Workforce Committee had considered and therefore made the recommendation to reduce the strategic risk relating to IT as the organisation matures and demonstrates that it is better able to recognise the benefits available from well embedded IT systems. PBi added that the Audit & Assurance Committee asks the Board to accept that a number of financial risks will carry forward to 2015/16 as it considers any new risks relevant for that year. AH noted that such risks should be considered by the Finance & Workforce Committee and Safety & Quality Committee prior to recommendation to the Board. GFM further highlighted that the Executive Committee had considered and agreed that the strategic risk relating to an outbreak of viral gastroenteritis should remain, recognising that the organisation has recently closed a number of wards due to small outbreaks. A new risk relating to the cancellation of clinics has been agreed by the
Page 4 of 12
Executive Committee and will be evidenced on the SRR in April. Action: Executive Committee to consider whether risks relating to sickness absence and temporary staffing should be replicated within the BAF. Any recommendations should be made to the Board in April. The Board resolved to approve the recommendation to close risk 5.B (reducing the BAF to 18 risks) and the reduction of risks 5.A.2 and 5.F. The board duly approved the report.
2. Safety, Quality and Patient Experience 2.1 Clinical Presentation – Haematology Service for discussion
Dr Eirini Thanopoulou (Acute Oncology Service Lead) and Dr Emma O’Donovan (Haematology Consultant) presented some of the key developments within the Acute Oncology Service as a result of a national recommendation following the National Confidentiality Enquiry into Patient Outcome & Death 2008. A recent audit (‘1 Hour to Antibiotics’) will result in changes made to the Neutropenic Sepsis Protocol to improve prevention and management of neutropenic sepsis in cancer patients. A revision to the pathway will be piloted after Easter when all suspected Neutropenia patients presenting to the Emergency Department will be immediately treated with antibiotic within 60 minutes of arrival, whilst further test results are awaited. MW requested that Julian Webb, Chief of Patient Safety was fully engaged with any changes to the pathway and guidance for treatment and assessment. The Board recommended future updates to the Safety & Quality Committee and took assurance from the presentation.
2.2 Chief Nurse and Medical Director’s Report for Assurance The board received and noted the report in advance of the meeting. FA presented the first half of the joint report focusing on the safer staffing report for February 2015 which indicates that the Trust has delivered the planned versus actual staffing levels for inpatient areas and the maternity unit. The Board noted a variation in the availability of nursing assistants during the day which has been appropriately managed by Matrons. FA highlighted that the Trust score for total staffing compliance during February was 96.1%, despite challenges to deliver the plan due to Half Term holiday and increased activity. The Family and Friends Test (FFT) scores for inpatients and the Emergency Department continued to perform well during February. In order to be inclusive for those harder to reach patients (including patients with Dementia, learning disabilities and children aged 5-16), a range of cards for the Your Care Matters survey have been designed and disseminated in collaboration with relevant staff. The organisation is currently considering any implications and requirements of the Trust following the introduction of the Care Certificate which will regulate training of Healthcare Assistants to demonstrate skills, knowledge and behaviours to ensure compassionate and high quality care and support is
Page 5 of 12
provided. DH continued to report that the Trust has appointed Dr Ben Upton as Clinical Chief Information Officer, with a deputy to support him in the roll out of our Health Informatics strategy. Dr Julian Webb has also been appointed as Clinical Chief of Patient Safety and will lead on projects designed to improve safety and learning across the organisation. Dr Webb will remain clinical lead for ED. DH further reported that two members of staff had been identified with skin infection related to PVL-MRSA, a multi-resistant organism. As a consequence, all staff and patients were screened and no further cases were identified. A deep clean operation was commissioned and normal patient flow has resumed. The Board further noted changes to the Trust’s divisional structure which will come into effect from 1st April 2015. Responsibilities which fall within the Clinical Support Services (CSS) division will be amalgamated with the Cancer, Medical, Surgical and WaCH divisions. Action: PBo to circulate further details of the revised divisional structure to all Trust Board members (including Non-Executive Directors). The Board duly noted and took assurance from the report.
2.3 15 Step Challenge Update Report for Assurance The board received and noted the report in advance of the meeting. Lynn Sanders (Corporate Matron) and FA presented the report which outlines the activity to date in relation to the 15 Step Challenge, including completed improvement actions. This monthly programme consists of a small team made up of Non-Executive Directors, clinical and non-clinical staff as well as patient representatives and volunteers. The team provides a selection of viewpoints on how each visited ward felt from a patient or visitor perspective. Themes around the recommended improvements from the 15 Steps activities include; Signage; storage of equipment; information for patients for medical conditions; information for patients and visitors about feedback; minor maintenance and cleaning issues; general decorations of area. The Chairman noted some inconsistency in reporting, which was accepted. However, the programme is not intended to be formulaic. PS proposed that the written templates clearly state this and that all contributors should be mindful of what could be misinterpreted by the media and staff. FA added that progress against recommendations and actions should be formally managed within a ward review structure – this is an aspiration of the Chief Nurse. The Board accepted that the current structure of the programme provided greater exposure and visibility to the Board and agreed that the Ward Accreditation Scheme should continue to be the driver of performance improvement.
Page 6 of 12
The Board duly noted and took assurance from the report.
2.4 Safety & Quality Committee Update for Assurance The board received and noted the report in advance of the meeting. The report summarised some of the key discussion points of the last committee meeting held on 5th March 2015. RS highlighted that the committee had been positively assured by some of the improvements made within both the Children’s and Adult’s Safeguarding teams for the Trust.
The committee’s Chairman will be writing to the Chairman of the Surrey Safeguarding Board to raise concerns that there appears to be an increasing incidence of child sexual exploitation within the local area. The Chairman will ask for assurance that the Trust is doing all it can to support the safeguarding systems in Surrey and Sussex. AM challenged what the evidence of this increasing incidence was; an informal impression provided a prompt to raise the question and challenge the Safeguarding Board in this respect. It was noted that the Trusts safeguarding policy was well embedded within the organisation and supported by an efficient team. The Trust is currently represented on the Safeguarding Board. The committee received a presentation on the Fractured Neck of Femur (FNOF) pathway which demonstrated an improving trajectory and significant reduction in the number of falls in hospital resulting in FNOF. It was noted that the key issue remains the ability to discharge patients, with an average length of stay slightly higher than average. The Woman & Children’s Health (WACH) division presented their audit plans and recent outcomes. The Committee requested a further report which should summarise the number of audits which provide positive assurance and the steps taken against those which have been negative. The board duly noted the report for assurance.
3. Operational Performance
3.1 Integrated Performance Report (M11) for Assurance
The board received the Integrated Performance report in advance of the meeting. PBo summarised the Trust’s operational performance during February 2015, noting a difficult month in terms of emergency activity levels. In February, 91% of patients were admitted or discharged within 4 hours with no 12 hour trolley wait breaches and strong performance against cancer standards. Delivery of the ED 4 hour standard remains a challenge across the country and despite the under-performance at the Trust we remain one of the best performing Trusts in the country.
Page 7 of 12
In light of the on-going operational pressures, the following risks have been added to the Significant Risk Register;
ED Access Standard – failure to maintain the emergency department standard due to lack of capacity in the health system to manage winter pressures
Patient Admitted to the Right Bed First Time – if the trust does not maintain and improve the ability to allocate the right bed first time, there is an increased risk of reduced quality of care
Incomplete pathways RTT standards were achieved at aggregate level (94%) whilst the admitted and non-admitted standard was not achieved. Non achievement of the standard is part of a national drive to reduce the 18-week backlog however, it is expected that the Trust will deliver the standard in April. Limiting the number of in-patients in order to reduce the risk of cancellation has been supported by an increase in day cases. The Trust reported six new cases of C.Diff during February, taking the total to 23 YTD against a trajectory of 27 YTD and 23 cases for the same period last year. RS noted that this was the highest increase in month; DH confirmed that despite good antibiotic prescribing, a single ward remains on increased surveillance after testing positive from patient stools. The 2015/16 C.Diff target has been reduced to 15, which will prove a significant challenge and does not recognise the increasing capacity and size of the hospital over recent years. Adult bed occupancy remains higher than plan due to increased activity and is one of the items covered within the collaborative CQC action plan. The Trust continues to monitor ward nursing on a daily basis and is assured that adequate staffing is in place. It also continues to monitor temporary staffing usage on a weekly basis. Staff turnover remains static at 15.7% in February. HR Business Partners within divisions continue to support actions to improve recruitment and retention with a significant focus on nursing. Sickness absence increased marginally to 4.4%. RD noted that the current position needed to be accurately reflected. PS reported that the forecast year end position is now a £2.5m deficit. The previous accrual in respect of the marginal rate dispute has been removed as the arbitration process will not complete in this financial year and there are no mechanisms to secure additional income. The risk to this position has been estimated at £0.7m. A dispute with East Surrey CCG also remains a risk. The year to date position was a £2.9m deficit in month 11. The year to date income continues however to include the two tranches of winter resilience funding and divisional spend remains above budget due to the levels of emergency activity within the Trust (but it is within expected tolerance). The Cost Improvement Plan year to date target is £9.8m and at month 11 this has been achieved. The underlying position at the end of February is £5.6m deficit, reflecting the non-recurrent elements in the year to date position. The forecast year end underlying position remains £5.2m.
Page 8 of 12
The cash balance at the end of February was £3.8m, below the planned position due to the delay in receiving contract payments from CCGs. The cash position is becoming more challenging as there are delays in agreeing income figures and significant financial challenges from CCGs and as a result, an application for temporary borrowing was made. However, PS noted that the Trust is not using as much of this as it anticipated. The capital forecast spend remains £19.3m and the liquidity position has corrected to its underlying position with the timing of capital expenditure, the removal of the income accrual and other balance sheet movements. PS further updated the board on the £2.4m dispute with East Surrey CCG which remains unresolved. The Board duly noted and took assurance from the report.
3.2 2015/16 Capital and Revenue Budget for Approval The Board received and noted the report in advance of the meeting. PS presented the paper which confirms the interim revenue budget for 2015/16 and the final capital budget for 2015/16 for approval. Planning has been very difficult both locally and nationally and the process has been challenging for both the Trust and CCGs. The revenue budget, which has been discussed by the Finance & Workforce Committee and is recommended for Board approval, is interim due to slippage of the national timetable for contract negotiations and delayed publication of the prices for the ‘Enhanced Tariff Option’ (ETO). Since the writing of the report, actual tariff prices linked to the ETO have been received. The Trust also expects to be in a position to agree contracts with Crawley, Horsham and Mid-Sussex CCGs imminently. The contract will describe how the Trust and its CCG will respond to changes in activity levels against the contract. Both budgets presented are consistent with the current Long Term Financial Model submitted to Monitor. The revenue budget proposes a surplus of £1.6m and includes a cost improvement plan of £8.2m. The capital budget proposes investment of £17.0m. The Board resolved to approve the 2015/16 Revenue and capital budgets.
3.3 Finance & Workforce Committee Update for Assurance The Board received and noted the update in advance of the meeting RD highlighted some of the key points of discussion from the FWC meeting held on 24th March 2015. The committee received an update on the proposed Monitor assessment timetable. Monitor are scheduled to begin their assessment of the Trust for
Page 9 of 12
Foundation Trust status on 7th April 2015. The month 11 finance, workforce & organisational development, capital and IT reports were presented and discussed by the committee. The committee has requested additional reports in relation to sickness and appraisals due to insufficient assurances gained in respect of actions to address these issues. The committee will receive the Internal Control Framework in advance of the Audit & Assurance Committee, which will seek assurance. The committee noted that an IT road map will be presented in May, highlighting the implementation of future IT projects. The Board duly noted the report for assurance.
3.4 Audit & Assurance Committee Update for Assurance PBi highlighted some of the key points of discussion from the AAC meeting held on 17th March 2015. The committee reviewed the draft BAF and discussed emerging risks to be considered for the following year. Requests were made for specific updates to financial risks to reflect end of year position and requested that workforce related risks reflected those recorded on the SRR. The Internal Audit draft end of year opinion based on 2014/15 activity provided significant assurance of internal control systems, noting that issues relating to NICE Guidance Compliance and project management reviews had now been addressed. A review of the Trust’s risk management systems demonstrated improvement and provided positive assurance, with continued progress in the improvement of systems and compliance with the policy. The draft Annual Governance Statement was presented for early review and also provided significant assurance. The Board duly noted the report for assurance.
4. Risk, Regulatory and Strategy Items
4.1 CQC Improvement Action Plan for Assurance The Board received and noted the report and action plan in advance of the meeting. Sue Jenkins, Director of Strategy presented the CQC Action Plan which was developed following a visit by the Chief Inspector of Hospitals in May 2014 and in response to their findings in relation to service improvement. The board receives a monthly update on progress against the action plan. With Outpatient capacity budgeted to increase, work is underway to review and where necessary create additional capacity in terms of clinic availability, staff and rooms. On site opportunities for additional rooms are being discussed with Guys & St Thomas’ and use of space in the Remeo Centre. Further
Page 10 of 12
considerations are also being made to make better use of Crawley and Horsham hospitals. The Board noted a progress report from East Surrey and Crawley, Horsham & Mid Sussex CCGs on how their plans will achieve the jointly agreed CQC actions. An update on progress against the system-wide quality summit actions for CCGs, Healthwatch, the General Medical Council and Health Overview & Scrutiny Committee was summarised within the report. The Board agreed that an update and status report following the roll out of Digital Dictate I.T should be presented to the Finance & Workforce Committee for assurance purposes. The Board duly noted and took assurance from the report.
4.2 Remuneration Committee Annual Report for Assurance The board received and noted the report in advance of the meeting. AM presented the report outlining the work of the Nomination and Remuneration committee throughout the year. The report summarises the purpose of the committee, the frequency of meetings and areas for improvement including work undertaken in 2014/15. AM highlighted that the committee had identified areas for improvement to the Committee’s function, including better preparation and advance circulation of meeting papers where applicable, formal minutes to be kept for all meetings and the business of the Committee to be set out in the table demonstrated by Appendix 1. AM added that consideration would need to be made regarding the future role of the Committee and its structure, assuming Foundation Trust status and recognising the introduction of the Council of Governors. Action: GFM to prepare a draft plan demonstrating the revised structure of the Committee as an FT, for discussion by the Board. The board resolved to approve the report.
4.3 Mutual Pathfinder Programme – Feasibility Study for Approval The board received and noted the report in advance of the meeting. Jonathan Knight, a representative of Bolt Partners presented the findings of the Feasibility Study, following the exploration of the suitability of a mutual model for SaSH. The study’s overall conclusion is that a move towards greater mutualisation would be an excellent cultural fit for the Trust. As a governance structure, it has the ability to embed at a constitutional level the values and behaviours that the Trust is seeking to encourage. This would provide a resilient basis for staff engagement with less dependence upon the priorities of the current board, and look to start to build similar engagement with the community.
Page 11 of 12
The Trust would not be able to develop this model at the present time due to current policy guidance and legislative frameworks however, if these contraints were removed it is recommended that SaSH continue with its exploration of a mutual approach as this has been well-received by staff in early engagement sessions. The model has some flexibilities and advantages over the standard FT model that may benefit Trust. The outcome of the draft report will be submitted to the Cabinet Committee as an output of the Mutual Pathfinder Programme. All political parties have shown an interest in the Mutual model. However, it is unknown how the new government will pursue this. Notably, improved staff and community engagement would be a full benefit to the Trust, however significant risk and consultancy fees accompany this. Emphasis should be placed on accountability of ownership by staff, rather than financial benefit. The Board duly approved the submission of the report to the Cabinet Committee.
4.4 National Staff Survey Report for Assurance The Board received and noted the report in advance of the meeting. Janet Miller, Deputy Director of HR presented a summary of results from the latest national staff survey and was pleased to report significant improvement in the reported staff engagement and satisfaction in the workplace JM further highlighted that the response rate for the Trust was 56%, which is in the highest 20% when compared against other Acute Trusts. Immediate actions have been identified and will provide focus for further improvement and learning. RD recognised a common theme amongst Trusts in relation to staff appraisals which was perhaps reflective of recent activity levels and the added pressure this has placed on staff. The newly launched appraisal process should demonstrate better quality of the appraisal itself and provide a framework for Managers to follow. PS noted his concerns at responses made in relation to bullying. JM gave assurance that detailed discussions have taken place with the Emergency Department, the most affected area of concern in this respect, and conflict resolution training has been offered. This is truly reflective of staff feeling better empowered and enabled to report such incidents. MW further added that the Trust has been in discussions with the Police Commissioner for Surrey to address some of the issues arising from mental health patients and how both organisations can better work together in response to the violent and aggressive behaviour of patients towards staff. The Board duly noted and took assurance from the report.
5. Other Items
5.1 Minutes of Board Committees to receive and note
5.1.1 Finance and Workforce
Page 12 of 12
The minutes of the committee were noted with no questions raised.
5.1.2 Safety & Quality Committees to receive and note The minutes of the committee were noted with no questions raised.
5.1.3 Audit & Assurance Committees to receive and note The minutes of the committee were noted with no questions raised
5.2 Any Other Business No further business was discussed by the Board.
5.3 Questions from the Public There were no questions raised from members of the public.
5.4 Date of the next meeting Thursday 30th April 2015 at 10.00am in Room AD77, Post Graduate Education Centre, East Surrey Hospital
Note: This is a public document and therefore will be placed into the public domain via the Trust’s website in the interests of openness and transparency under Freedom of Information Act 2000 legislation. These minutes were approved as a true and accurate record. Alan McCarthy Chairman: Date:
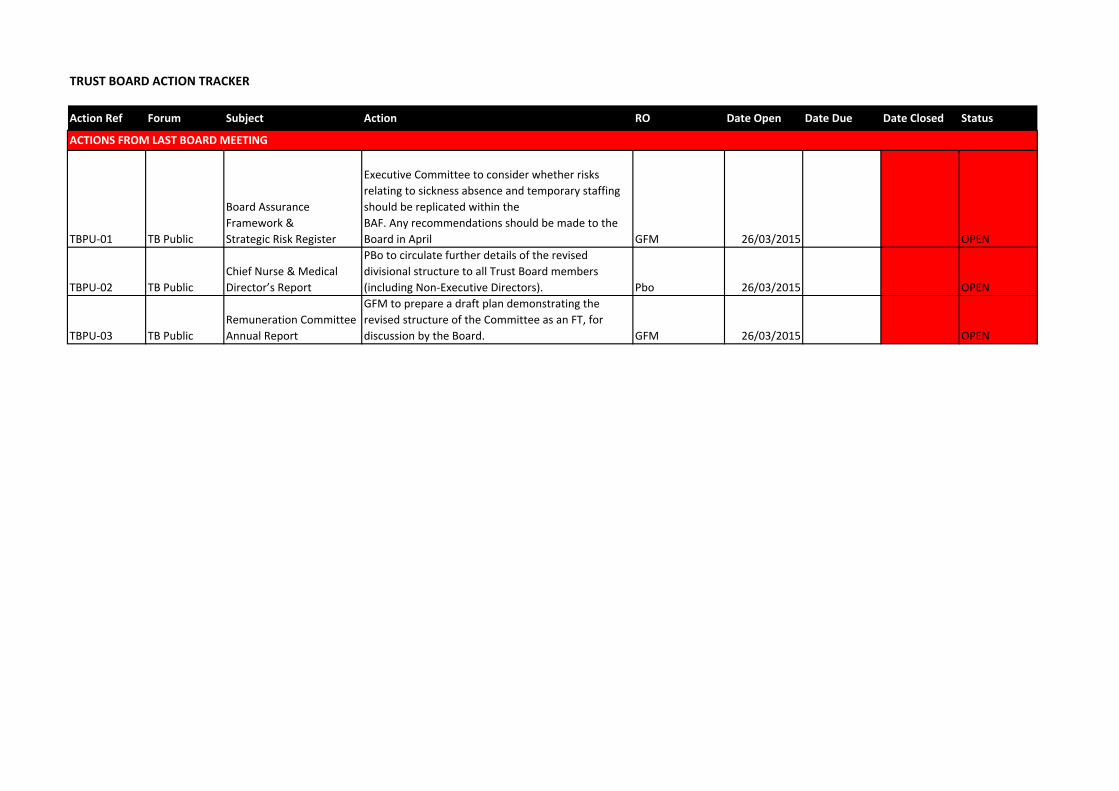
TRUST BOARD ACTION TRACKER
Action Ref Forum Subject Action RO Date Open Date Due Date Closed Status
TBPU‐01 TB Public
Board Assurance Framework & Strategic Risk Register
Executive Committee to consider whether risks relating to sickness absence and temporary staffing should be replicated within theBAF. Any recommendations should be made to the Board in April GFM 26/03/2015 OPEN
TBPU‐02 TB PublicChief Nurse & Medical Director’s Report
PBo to circulate further details of the revised divisional structure to all Trust Board members (including Non‐Executive Directors). Pbo 26/03/2015 OPEN
TBPU‐03 TB PublicRemuneration Committee Annual Report
GFM to prepare a draft plan demonstrating the revised structure of the Committee as an FT, for discussion by the Board. GFM 26/03/2015 OPEN
ACTIONS FROM LAST BOARD MEETING
TRUST BOARD IN PUBLIC
Date: 30th April 2015 Agenda Item: 1.6
REPORT TITLE: CHIEF EXECUTIVE’S REPORT
EXECUTIVE SPONSOR: Michael Wilson Chief Executive
REPORT AUTHOR (s): Gillian Francis-Musanu Director of Corporate Affairs
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date) N/A
Action Required:
Approval ( ) Discussion (√) Assurance (√)
Purpose of Report:
To ensure the Board are aware of current and new requirements from a national and local perspective and to discuss any impact on the Trusts strategic direction.
Summary of key issues
National Issues: The Health and Social Care (Safety and Quality) Act 2015 received Royal Assent.
Local Issues: Monitor Assessment Phase Appointment of New Clinical Chair for East Surrey Clinical Commissioning Group Clinical Research Surrey Choices Employability Award Successful Funding Bid for Mouth Care Matters Radio Redhill Forthcoming Events
Recommendation:
The Board is asked to note the report and consider any impacts on the trusts strategic direction.
Relationship to Trust Strategic Objectives & Assurance Framework:
SO5: Well led: Become an employer of choice and deliver financial and clinical sustainability around a clinical leadership model
Corporate Impact Assessment:
Legal and regulatory impact Ensures the Board are aware of current and new requirements.
Financial impact N/A
Patient Experience/Engagement Highlights national requirements in place to improve patient experience.
Risk & Performance Management Identifies possible future strategic risks which the Board should consider
NHS Constitution/Equality & Diversity/Communication
Includes where relevant an update on the NHS Constitution and compliance with Equality

2
Legislation
Attachment:
3
TRUST BOARD REPORT – 30th April 2015 CHIEF EXECUTIVE’S REPORT 1. National Issues
1.1 The Health and Social Care (Safety and Quality) Act 2015 received Royal Assent.
Among the measures introduced by the Act is a duty on health and adult social care providers to share information about a person’s care with other health and care professionals. This means that doctors and other professionals providing a person’s care and treatment will have the information they need so they can treat patients more effectively.
Relevant health and adult social care bodies will also be required to use a consistent identifier - the NHS Number - when processing and/or sharing information about an individual for their direct care. This will enable better connection of health and care records as people move between services, so relevant information is shared, meaning safer and better aligned care.
The Bill also makes provision about the safety of health and social care services in England including removing individuals convicted of certain offences from the registers kept by the regulatory bodies for health and social care professions and puts in place the requirements for the Professional Standards Authority for Health and Social Care to take steps in relation to Directors fitness to practise in a health or social care profession. 2. Local Issues 2.1 Monitor Assessment Phase The Board will be aware that following approval from the TDA Board the Trust is now in the formal Monitor Assessment Phase. A series of individual meetings have been held with Board members, Executive & Divisional teams as well as subject specific meetings. The date for the formal Monitor Board to Board has been confirmed as on 1st June 2015. Elections to the Council of Governors begins in May with completion of the process and the declaration of results expected on 3rd July 2015. 2.2 Appointment of New Chair for East Surrey Clinical Commissioning Group Dr Elango Vijaykumar has recently been appointed as the new Clinical Chair of East Surrey Clinical Commissioning Group. Dr Vijaykumar has served as a GP member on the CCG’s Governing Body and has co-chaired the Practices Commissioning Committee since the CCG began in April 2013. 2.3 Clinical Research
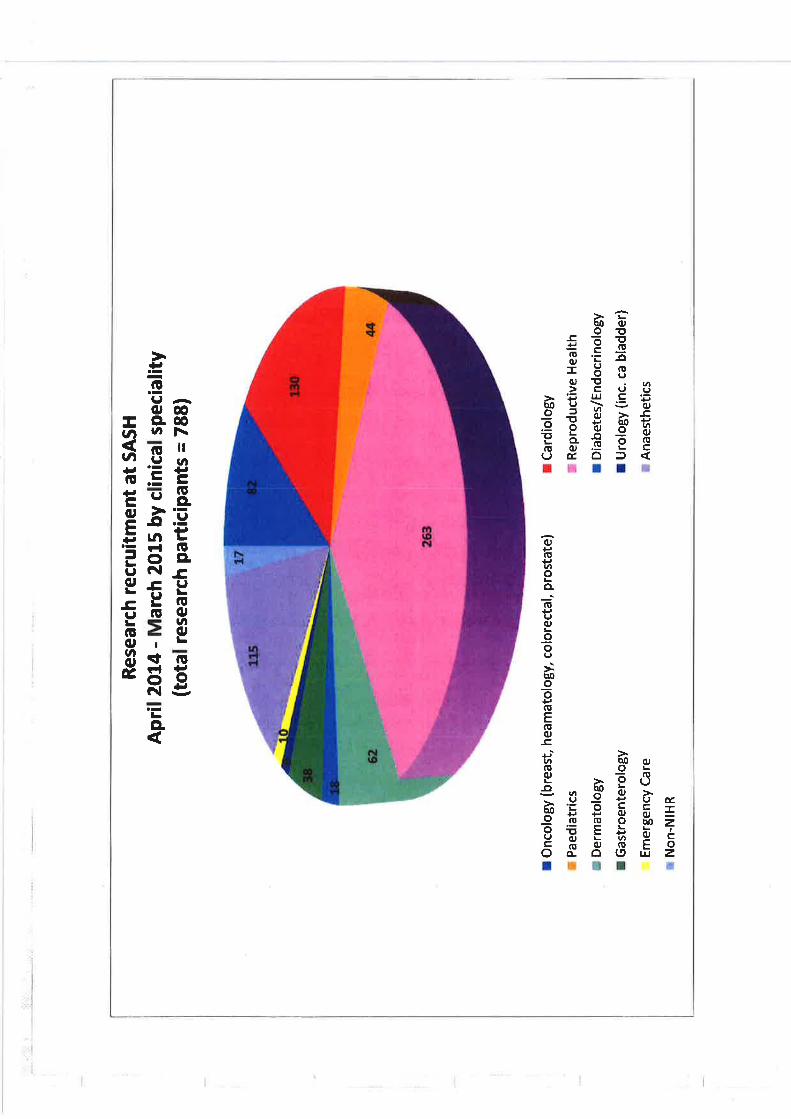
It is encouraging that the Trust is seeing a continued increase in the number of clinical staff within our Trust actively engaged in clinical research as a means of improving care and outcomes for our patients. In the last year, our research teams have opened up 26 new clinical research studies for patients to participate in and we are now supporting the care of patients in 45 different research studies and recruiting patients into 12 national and international pharmaceutical company sponsored research studies. This enthusiasm
4
and success gives SASH a strong clinical representation and role in supporting the improvement in patient care not just locally but nationally and internationally.
2.4 Surrey Choices Employability Award The Trust has won a first place award in the ‘Pulling it all together’ category of the Surrey Choice ‘Employability – Making a Difference’ Awards at an awards ceremony held on 16 April. We have a long history of working with the Surrey Choices Employability service to support people with a disability to find employment. The award recognised our flexible, creative and supportive approach in maximising employment opportunities to people with disabilities. Gavin Jackson, one of our post room assistants at East Surrey Hospital won the award for Outstanding Achievement. It is a credit to colleagues across the organisation that we are able to provide this support and it is a privilege to see the impact and important contribution that this makes. 2.5 Successful Funding Bid for Mouth Care Matters
The Trust has been successful in being awarded funding by Health Education England for our Mouth Care Matters initiative being led by the SASH dental team. The award will fund an additional four dental nurse practitioners who will work across the hospital to support and provide extra training for our nursing and ward teams as they care for our patients. Evidence shows that improving the oral health of the people we care for, especially older patients will also have a positive impact on their general health and well-being. 2.6 Radio Redhill As part of their 40th birthday celebrations I took part in an interview on Radio Redhill to update them on our Foundation Trust journey and other exciting plans we have coming up. Radio Redhill which is based at East Surrey Hospital, broadcasts a daily schedule of interviews and music 24 hours a day for our patients and their visitors along with national a local news. Run by a dedicated team of volunteers, Radio Redhill is an important member of our community. 2.7 Forthcoming Events: 14 May – Hot topic: Anaesthetics and Critical Care 15 May – East Surrey Macmillan Cancer Care Centre “turf cutting ceremony” 21 May – Marie Curie Partnership launch for End of Life discharge liaison co-ordinators – event hosted by SASH with partner Marie Curie and supported by St Catherine’s’ Hospice
3. Recommendation
The Board is asked to note the report and consider any impacts on the trusts strategic direction.
Michael Wilson Chief Executive April 2015
TRUST BOARD IN PUBLIC
Date: 30th April 2015 Agenda Item: 1.7
REPORT TITLE: Board Assurance Framework & Significant Risk Register
EXECUTIVE SPONSOR: Gillian Francis-Musanu Director of Corporate Affairs
REPORT AUTHOR (s): Colin Pink Corporate Governance Manager
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date)
Board Seminar 26th February 2015 Executive Committee for Quality & Risk 22.4.15
Action Required:
Approval (√) Discussion (√) Assurance (√)
Purpose of Report:
The Board Assurance Framework highlights potential risks to the Trust’s strategic objectives and mitigating actions and the implementation of its programme of objectives for year one of the five year plan. The Significant Risk Register (SRR) details all risks on the Trust risk register system that are recorded as significant and the links to the Board Assurance Framework.
Summary of key issues
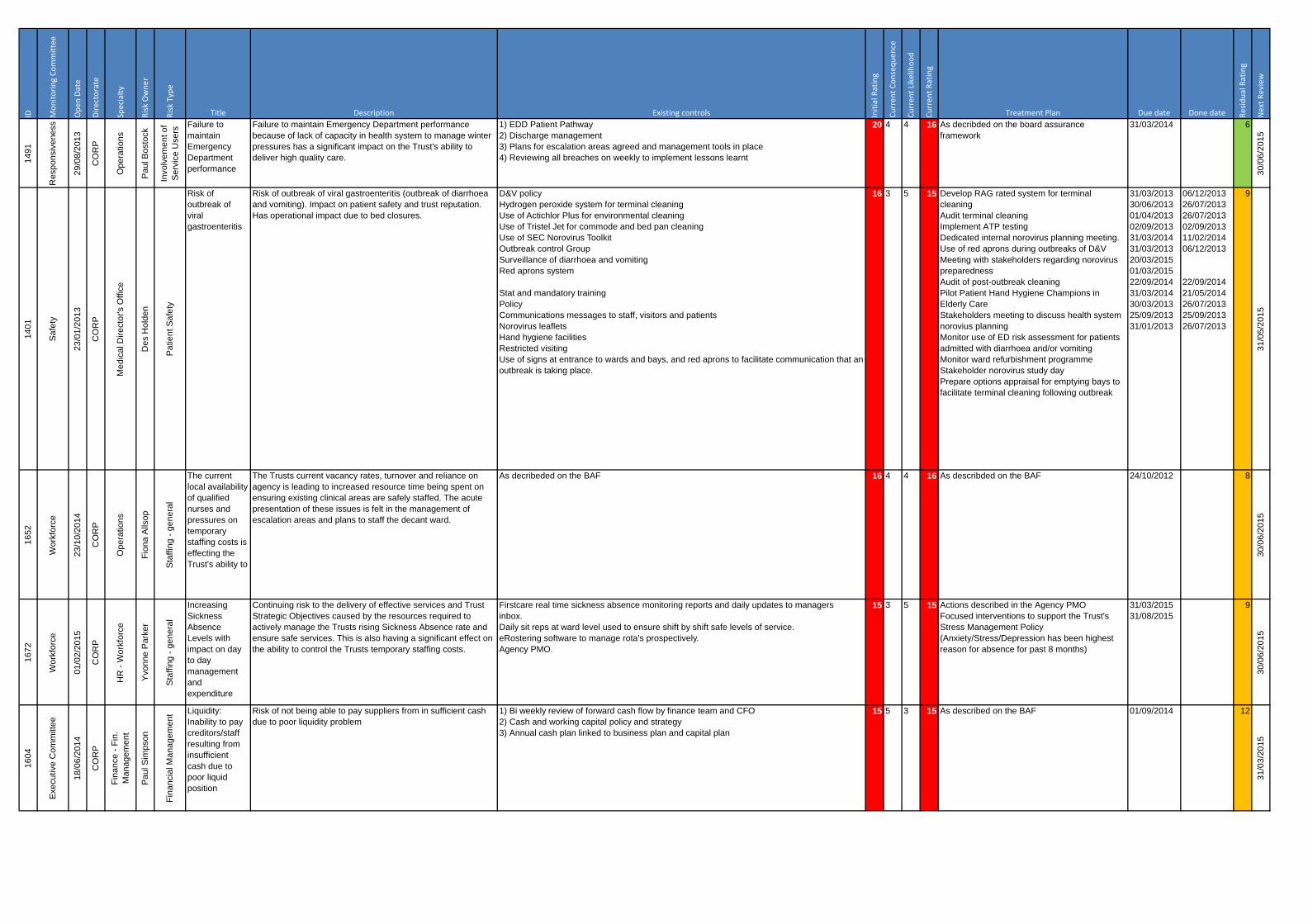
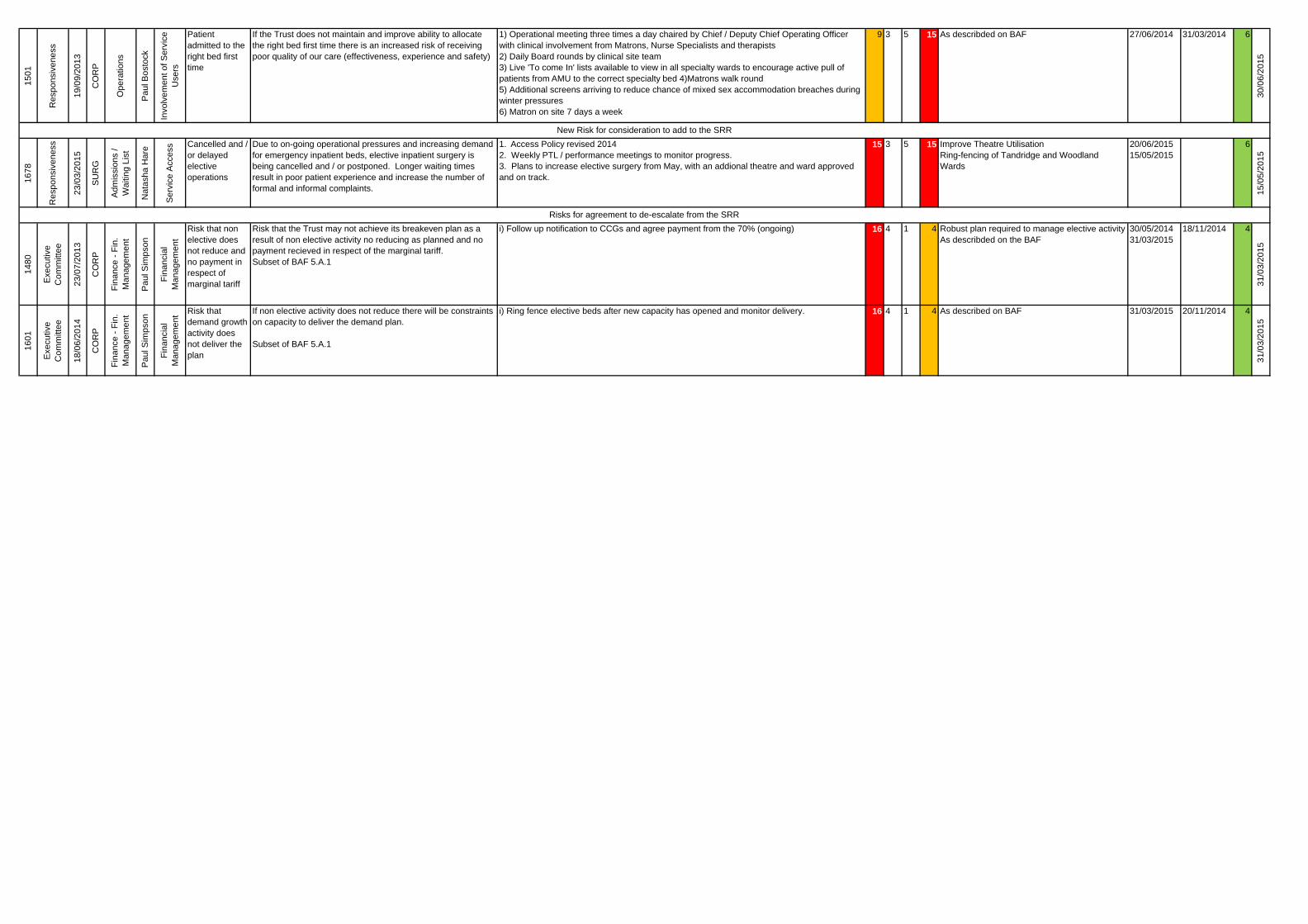
The report provides an overview of the process for developing the 2015/16 BAF. There are 8 significant risks recorded on the Trust risk register with the proposal to include one escalated risk to the significant risk register. Specifically the risks related to cancelled and / or delayed elective operations (1678). The Executive Committee for Quality and Risk is also proposing to de-escalate the following two risks; 1480: Risk that non elective does not reduce and no payment in respect of marginal
tariff 1601: Risk that demand growth activity does not deliver the plan
Recommendation:
The Board is asked to note and gain assurance from the process for the development of the 2015/16 BAF; and discuss and approve the proposals to:
include the escalated risk to the SRR de-escalate two risks from the SRR
Relationship to Trust Strategic Objectives & Assurance Framework:
SO1: Safe -Deliver safe services and be in the top 20% against our peers SO2: Effective - Deliver effective and sustainable clinical services within the local health economy SO3: Caring – Ensure patients are cared for and feel cared about SO4: Responsive – Become the secondary care provider and employer of choice our catchment population SO5: Well led - Become an employer of choice and deliver financial and clinical sustainability around a clinical leadership model
2An Associated University Hospital of Brighton and Sussex Medical School
Corporate Impact Assessment:
Legal and regulatory impact The report is a requirement for all NHS organisations.
Financial impact This is included in the report
Patient Experience/Engagement Patient experience and engagement is one of the Trusts strategic objectives.
Risk & Performance Management These are highlighted throughout the report.
NHS Constitution/Equality & Diversity/Communication
Discussed throughout the report
Attachment: Significant Risk Register – April 2015
3An Associated University Hospital of Brighton and Sussex Medical School
TRUST BOARD REPORT – 30th April 2015 Process for review and development of 2015/16 Board Assurance Framework and Significant Risk Register 1. Introduction The Board has reviewed the strategic objectives and key priorities in order to ensure that the Board Assurance Framework (BAF) continues to reflect the key risks to the Trust’s strategic objectives. 2. Process for developing 2015/16 BAF In order to facilitate this process the Director of Corporate Affairs, Chief Nurse and Corporate Governance Manager prepared a summary review of the 2014/15 BAF and strategic priorities. The purpose of this review was to propose new risks for the BAF and or changes that could be made to make the existing document more focussed on key issues. At the Board Seminar at the end of February 2015 a review was undertaken of the current risk appetite and suggestions made for how the detail could be updated to better reflect the current and future strategic position for 2015/16. In addition, each element of the BAF was reviewed and proposals were made to either; retain, close or merge current risks, update risk descriptions and or add new risks. The Executive Team have been reviewing and updating a draft 2015/16 BAF which has been circulated to the Board for review and comment. Once all comments and feedback have been received the draft BAF will be updated and reviewed by the Executive Committee and presented to the May Audit and Assurance committee such that it can review the process for developing the 15/16 BAF and the risk appetite prior to presentation at the public Board in May 2015 for approval. 3. Significant Risk Register On the 22nd April the Executive Committee for Quality and Risk (ECQR) reviewed and agreed the content of the Significant Risk Register (SRR). There are 8 risks on the Trust significant risk register. Each is in date and has mitigating actions to reduce the level of risk to an acceptable level. Following previous discussion at the Board, ECQR is proposing to include one escalated risk to the significant risk register. Specifically the risks related to cancelled and / or delayed elective operations (1678). ECQR is also proposing to de-escalate the following two risks; 1480: Risk that non elective does not reduce and no payment in respect of marginal tariff. – Income settlements have been agreed with clinical commissioning groups excluding the MRET therefore this risk is no longer applicable. 1601: Risk that demand growth activity does not deliver the plan. - The Trust has delivered its financial forecast for the year and the risks identified did not transpire.
4An Associated University Hospital of Brighton and Sussex Medical School
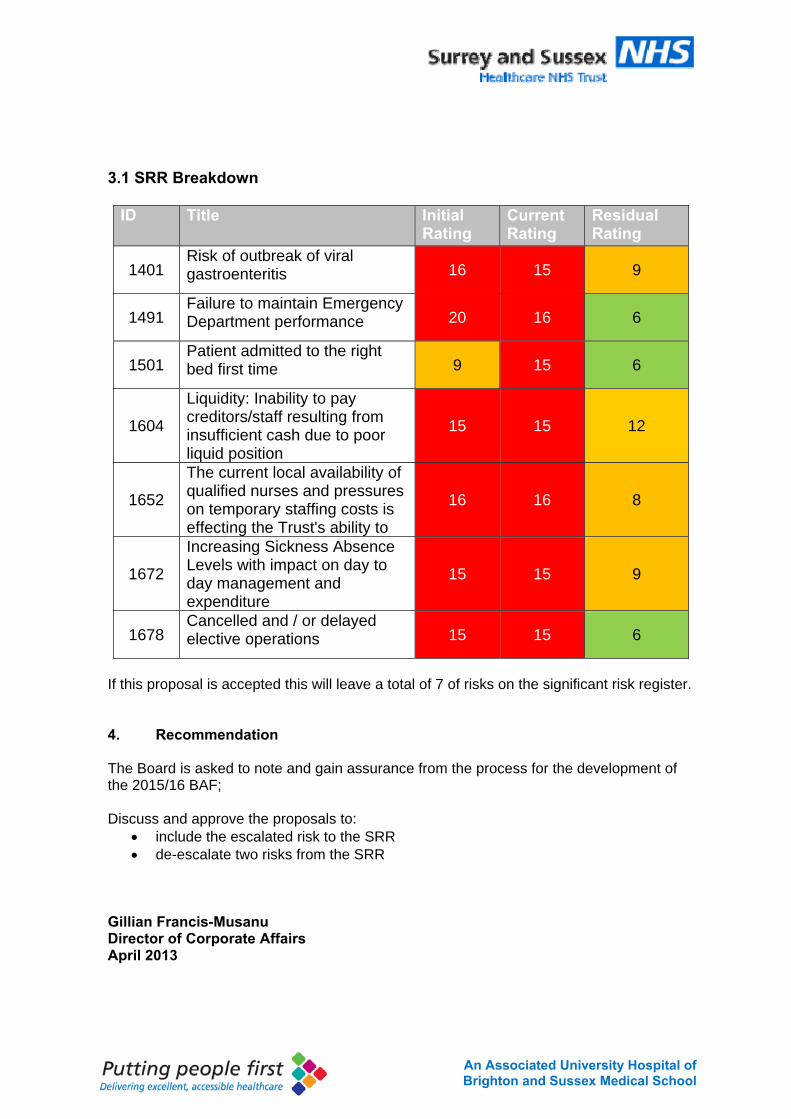
3.1 SRR Breakdown
ID Title Initial Rating
Current Rating
Residual Rating
1401 Risk of outbreak of viral gastroenteritis 16 15 9
1491 Failure to maintain Emergency Department performance 20 16 6
1501 Patient admitted to the right bed first time 9 15 6
1604
Liquidity: Inability to pay creditors/staff resulting from insufficient cash due to poor liquid position
15 15 12
1652
The current local availability of qualified nurses and pressures on temporary staffing costs is effecting the Trust's ability to
16 16 8
1672
Increasing Sickness Absence Levels with impact on day to day management and expenditure
15 15 9
1678 Cancelled and / or delayed elective operations 15 15 6
If this proposal is accepted this will leave a total of 7 of risks on the significant risk register. 4. Recommendation The Board is asked to note and gain assurance from the process for the development of the 2015/16 BAF; Discuss and approve the proposals to:
include the escalated risk to the SRR de-escalate two risks from the SRR
Gillian Francis-Musanu Director of Corporate Affairs April 2013
ID Mon
itorin
g Co
mmittee
Ope
n Da
te
Directorate
Specialty
Risk Owne
r
Risk Type
Title Description Existing controls Initial Rating
Curren
t Con
sequ
ence
Curren
t Likelihoo
d
Curren
t Rating
Treatment Plan Due date Done date Resid
ual Rating
Next R
eview
1491
Res
pons
iven
ess
29/0
8/20
13
CO
RP
Ope
ratio
ns
Pau
l Bos
tock
Invo
lvem
ent o
f S
ervi
ce U
sers
Failure to maintain Emergency Department performance
Failure to maintain Emergency Department performance because of lack of capacity in health system to manage winter pressures has a significant impact on the Trust's ability to deliver high quality care.
1) EDD Patient Pathway 2) Discharge management
3) Plans for escalation areas agreed and management tools in place4) Reviewing all breaches on weekly to implement lessons learnt
20 4 4 16 As decribded on the board assurance framework
31/03/2014 6
30/0
6/20
15
1401
Safe
ty
23/0
1/20
13
CO
RP
Med
ical
Dire
ctor
's O
ffice
Des
Hol
den
Patie
nt S
afet
y
Risk of outbreak of viral gastroenteritis
Risk of outbreak of viral gastroenteritis (outbreak of diarrhoea and vomiting). Impact on patient safety and trust reputation. Has operational impact due to bed closures.
D&V policy Hydrogen peroxide system for terminal cleaning Use of Actichlor Plus for environmental cleaning
Use of Tristel Jet for commode and bed pan cleaning Use of SEC Norovirus Toolkit
Outbreak control Group Surveillance of diarrhoea and vomiting
Red aprons system
Stat and mandatory training Policy
Communications messages to staff, visitors and patients Norovirus leaflets
Hand hygiene facilities Restricted visiting
Use of signs at entrance to wards and bays, and red aprons to facilitate communication that an outbreak is taking place.
16 3 5 15 Develop RAG rated system for terminal cleaning Audit terminal cleaning Implement ATP testing Dedicated internal norovirus planning meeting. Use of red aprons during outbreaks of D&VMeeting with stakeholders regarding norovirus preparedness Audit of post-outbreak cleaning Pilot Patient Hand Hygiene Champions in Elderly CareStakeholders meeting to discuss health system norovius planningMonitor use of ED risk assessment for patients admitted with diarrhoea and/or vomitingMonitor ward refurbishment programme Stakeholder norovirus study day Prepare options appraisal for emptying bays to facilitate terminal cleaning following outbreak
31/03/201330/06/201301/04/201302/09/201331/03/201431/03/201320/03/201501/03/201522/09/201431/03/201430/03/201325/09/201331/01/2013
06/12/201326/07/201326/07/201302/09/201311/02/201406/12/2013
22/09/201421/05/201426/07/201325/09/201326/07/2013
9
31/0
5/20
15
1652
Wor
kfor
ce
23/1
0/20
14
CO
RP
Ope
ratio
ns
Fion
a A
llsop
Sta
ffing
- ge
nera
l
The current local availability of qualified nurses and pressures on temporary staffing costs is effecting the Trust's ability to
The Trusts current vacancy rates, turnover and reliance on agency is leading to increased resource time being spent on ensuring existing clinical areas are safely staffed. The acute presentation of these issues is felt in the management of escalation areas and plans to staff the decant ward.
As decribeded on the BAF 16 4 4 16 As describded on the BAF 24/10/2012 8
30/0
6/20
15
1672
Wor
kfor
ce
01/0
2/20
15
CO
RP
HR
- W
orkf
orce
Yvo
nne
Par
ker
Sta
ffing
- ge
nera
l
Increasing Sickness Absence Levels with impact on day to day management and expenditure
Continuing risk to the delivery of effective services and Trust Strategic Objectives caused by the resources required to actively manage the Trusts rising Sickness Absence rate and ensure safe services. This is also having a significant effect on the ability to control the Trusts temporary staffing costs.
Firstcare real time sickness absence monitoring reports and daily updates to managers inbox.
Daily sit reps at ward level used to ensure shift by shift safe levels of service. eRostering software to manage rota's prospectively.
Agency PMO.
15 3 5 15 Actions described in the Agency PMOFocused interventions to support the Trust's Stress Management Policy (Anxiety/Stress/Depression has been highest reason for absence for past 8 months)
31/03/201531/08/2015
9
30/0
6/20
15
1604
Exe
cutiv
e C
omm
ittee
18/0
6/20
14
CO
RP
Fina
nce
- Fin
. M
anag
emen
t
Pau
l Sim
pson
Fina
ncia
l Man
agem
ent Liquidity:
Inability to pay creditors/staff resulting from insufficient cash due to poor liquid position
Risk of not being able to pay suppliers from in sufficient cash due to poor liquidity problem
1) Bi weekly review of forward cash flow by finance team and CFO 2) Cash and working capital policy and strategy
3) Annual cash plan linked to business plan and capital plan
15 5 3 15 As described on the BAF 01/09/2014 12
31/0
3/20
15
1501
Res
pons
iven
ess
19/0
9/20
13
CO
RP
Ope
ratio
ns
Pau
l Bos
tock
Invo
lvem
ent o
f Ser
vice
U
sers
Patient admitted to the right bed first time
If the Trust does not maintain and improve ability to allocate the right bed first time there is an increased risk of receiving poor quality of our care (effectiveness, experience and safety)
1) Operational meeting three times a day chaired by Chief / Deputy Chief Operating Officer with clinical involvement from Matrons, Nurse Specialists and therapists
2) Daily Board rounds by clinical site team 3) Live 'To come In' lists available to view in all specialty wards to encourage active pull of
patients from AMU to the correct specialty bed 4)Matrons walk round5) Additional screens arriving to reduce chance of mixed sex accommodation breaches during
winter pressures 6) Matron on site 7 days a week
9 3 5 15 As describded on BAF 27/06/2014 31/03/2014 6
30/0
6/20
15
1678
Res
pons
iven
ess
23/0
3/20
15
SU
RG
Adm
issi
ons
/ W
aitin
g Li
st
Nat
asha
Har
e
Ser
vice
Acc
ess Cancelled and /
or delayed elective operations
Due to on-going operational pressures and increasing demand for emergency inpatient beds, elective inpatient surgery is being cancelled and / or postponed. Longer waiting times result in poor patient experience and increase the number of formal and informal complaints.
1. Access Policy revised 2014 2. Weekly PTL / performance meetings to monitor progress.
3. Plans to increase elective surgery from May, with an addional theatre and ward approved and on track.
15 3 5 15 Improve Theatre UtilisationRing-fencing of Tandridge and Woodland Wards
20/06/201515/05/2015
6
15/0
5/20
15
1480
Exe
cutiv
e C
omm
ittee
23/0
7/20
13
CO
RP
Fina
nce
- Fin
. M
anag
emen
t
Pau
l Sim
pson
Fina
ncia
l M
anag
emen
t
Risk that non elective does not reduce and no payment in respect of marginal tariff
Risk that the Trust may not achieve its breakeven plan as a result of non elective activity no reducing as planned and no
payment recieved in respect of the marginal tariff.Subset of BAF 5.A.1
i) Follow up notification to CCGs and agree payment from the 70% (ongoing) 16 4 1 4 Robust plan required to manage elective activityAs describded on the BAF
30/05/201431/03/2015
18/11/2014 4
31/0
3/20
15
1601
Exe
cutiv
e C
omm
ittee
18/0
6/20
14
CO
RP
Fina
nce
- Fin
. M
anag
emen
t
Pau
l Sim
pson
Fina
ncia
l M
anag
emen
t Risk that demand growth activity does not deliver the plan
If non elective activity does not reduce there will be constraints on capacity to deliver the demand plan.
Subset of BAF 5.A.1
i) Ring fence elective beds after new capacity has opened and monitor delivery. 16 4 1 4 As described on BAF 31/03/2015 20/11/2014 4
31/0
3/20
15
New Risk for consideration to add to the SRR
Risks for agreement to de-escalate from the SRR
TRUST BOARD IN PUBLIC
Date: 30.4.15 Agenda Item: 2.1
REPORT TITLE:
Patient Story: Inadequate patient care and inadequate management of the subsequent complaint process. Changes made to improve as a result
EXECUTIVE SPONSOR: Dr Des Holden Fiona Allsop Medical Director Chief Nurse
REPORT AUTHOR (s): Des Holden and Fiona Allsop
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date) N/A
Action Required:
Discussion (√)
Purpose of Report:
The care that patients and their families receive when things do not go well should be of high quality and we should do our best to make amends and to learn as quickly as possible afterwards. The story presented here, from care in 2012, did not meet these aims and the complaint process that the patient’s family has been through has led to the Parliamentary Health Service Ombudsman (PHSO) partially upholding their complaint against the trust. The story demonstrates where we got both the care and the management of the complaint wrong, and what we have changed as a consequence.
Summary of key issues
Issues to be discussed fall under two main headings 1. The care the patient and his family received during the last weeks of life, while an in-
patient on separate occasions 2. The inadequate management and resolution of the complaints about care that were
made at the time and subsequently. Actions taken 1. We have acknowledged and apologised for failings in communication with the patient
and his family, and between wards and teams within SaSH. 2. We have made changes to the expectation of review for patients whose stay in our
wards is prolonged following a decision to discharge and for patients whose admission to an in-patient bed is characterised by prolonged care within the ED.
3. We are moving towards an electronic patient record, but the pace of this change will be relatively slow. For this reason we are changing the format of printed notes with the expectation that all staff write consecutively in a single medical record.
The PHSO stated (paragraph 4) that while aspects of the patient’s care were adequate, other aspects of the medical care including communication and record keeping were inadequate and fell far short of applicable standards. The PHSO goes on to say that they found evidence of maladministration of the patient’s daughter’s complaint and that the service failure and maladministration led to distress for the patient and his family. For this reason the complaint was partly upheld. The PHSO has been sent a significant volume of supporting evidence that we have changed our processes and therefore the risk of repetition. We have also apologised to
2An Associated University Hospital of Brighton and Sussex Medical School
the family for all failings and copied this to the PHSO. The suggested financial penalty (£500) has also been paid. Since April 2012 15 cases have gone to the PHSO. Of these three have been upheld and one has been partially upheld. Both of these percentages are low.
Recommendation:
The Trust Board should discuss the patient story in terms both of the clinical care and of the handling of the complaint, having seen the external reviews and the PHSO report, to ensure it is satisfied that lessons have been learned since this patient’s episodes of care ended.
Relationship to Trust Strategic Objectives & Assurance Framework:
SO1: Safe -Deliver safe services and be in the top 20% against our peers SO2: Effective - Deliver effective and sustainable clinical services within the local health economy SO3: Caring – Ensure patients are cared for and feel cared about
Corporate Impact Assessment:
Legal and regulatory impact Relevant to regulation
Financial impact minor
Patient Experience/Engagement Poor experience for patient and family
Risk & Performance Management Relevant particularly in relation to patient discharges and use of discharge lounge
NHS Constitution/Equality & Diversity/Communication
Included in the report
Attachment:
3An Associated University Hospital of Brighton and Sussex Medical School
TRUST BOARD REPORT – 30th April 2015 Patient Story An 88 year old man was admitted through the ED in March 2012. Although he had been thought possibly to have experienced a stroke, the working diagnosis made in the ED was of heart failure caused by a poorly functioning left ventricle, and a rhythm disturbance of the heart beat (atrial fibrillation). The patient was admitted first to AMU and then subsequently to Tilgate ward. He received various medications to reduce the work of his heart and improve his breathing and treat the rhythm disturbance. After about 13 days he suffered an acute deterioration with chest pain and slurred or difficult speech. This was thought to have been a heart attack although there was some initial confusion about this diagnosis and how it was communicated. He received further investigation and physiotherapy input and was discharged after just over a month of in-patient care. The patient was re-admitted approximately 9 weeks later with further breathing difficulties. The presumed diagnosis was of chest infection and investigations suggested that this was likely, on top of a degree of heart failure and a small pleural effusion. The patient was admitted to the acute medical unit and was commenced on therapy and after 48hours was thought to be recovered to his normal state. The decision to discharge him was taken on the morning ward round. The patient was later transferred to the discharge lounge to await his departure (wait for medications, discharge summary, etc.). In this particular patient story the patient was with us for many hours before leaving. During that period of time, having been regarded as discharged, no further observations were performed. On reaching home the patient was again significantly more breathless, such that his family called an ambulance and the patient came back to the ED that night. Although the department was not especially busy, the family’s perceptions, borne out by the medical notes, are that there was a delay of more than 4 hours between being seen by the ED nurses and being transferred to AMU, despite the patient having early warning scores that should have prompted earlier medical review. Again, it was the family’s perception that there was poor communication within ED and between teams with no one taking responsibility for doing and acting on observations. The patient was subsequently transferred to Tandridge ward after assessment on AMU, and after discussions with the family over the next few days was commenced on the Liverpool care pathway and died one week after admission. The family were strong advocates for the patient and the PHSO report indexes many examples of where they reported poor communication between health care professionals and between these groups and themselves. At their first being open meeting, having raised their concerns formally, they expected to meet with the then chief nurse and representatives from governance and from the divisions. They did not meet with an exec and the two follow up meetings were with different staff and the then acting up deputy chief of nursing. Their fourth being open meeting included the CEO and the chief nurse. Two external reports were commissioned by these directors, one into the handling of complaints (which was critical of the trust) and one into the clinical care (which was not critical). A fifth meeting involving CEO, Chief Nurse and MD was held but again failed to address satisfactorily the level of reflection on what had happened and the level of evidence required that things had improved. The family took their complaint to the PHSO at this point. The PHSO reviewed the care and the management of the family’s concerns with the help of additional external independent experts and has concluded by partially
4An Associated University Hospital of Brighton and Sussex Medical School
upholding the complaint. We have apologized unreservedly for all care failings and have changed many of our processes and expectations to reduce the chance of other patients and families experiencing these problems. What we have done As a result of the complaint and recommendations from the PHSO we have undertaken numerous improvements since 2012 which include
1. Revised the policy for patient observations in adults 2. Undertaken training in the recognition and management of deteriorating patients
including a revised national early warning score 3. Revised the policy for pressure ulcer prevention and management 4. Introduced comfort rounds and patient well-being standards 5. Implemented care plans for the last days of life 6. Introduced multidisciplinary ward and board rounds to improve clinical
communication 7. Moving towards the use of integrated patient notes 8. Reviewed and revised complaints management process, including staffing,
process to raise concerns, customer care training 9. Improved governance and accountability structures at ward, divisional, executive
and board level Des Holden Fiona Allsop Medical Director Chief Nurse April 2015
Presentation Title 36pt Arial BoldSub heading 24pt Arial
Patient Reported Outcome Measures (PROMs)
Presentation by:
Dr Kofi Nimako, Consultant Chest PhysicianDr Thayalan Kandiah, Consultant in Paediatric Dentistry
An Associated University Hospital ofBrighton and Sussex Medical School
What are PROMs ?
• Standardised validated instruments used to measure a patient’s perception of their:- Health - Functional status- QoL- Outcomes – “are my symptoms better?”
Why consider PROMs ?
• Patient centred approach to:
- Improving quality of care and QoL
A new approach to PROMs
• Incorporating into routine clinical practice• Driven by clinicians• Used to improve patient care
- Diagnosis- Communication- Treatment response- Disease monitoring
Implementation
• Utilisation of your care matters
• Retrospective completion of questionnaire
• Pilot – 3 month- Tilgate and Tandridge - Dental and Maxillofacial out-patients
• Outcomes- Rates of patient participation
Results
• N = 102
• 50% participation
Slide 6
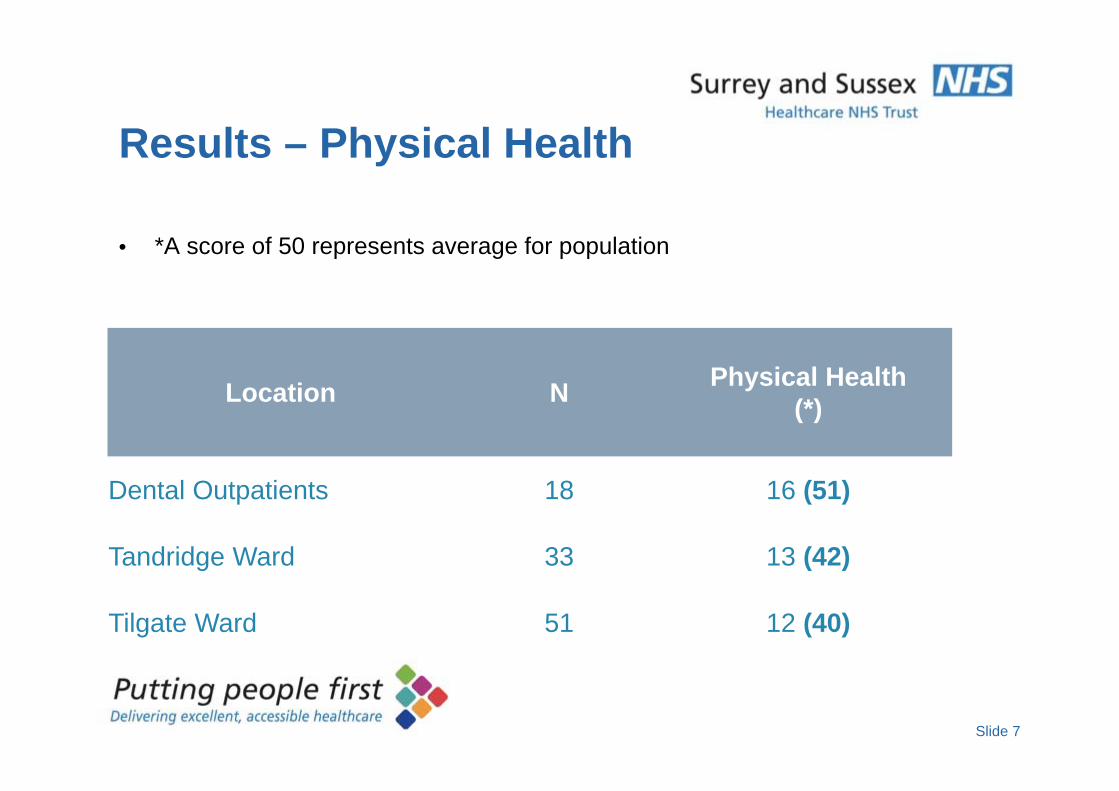
Results – Physical Health
• *A score of 50 represents average for population
Location N Physical Health(*)
Dental Outpatients 18 16 (51)
Tandridge Ward 33 13 (42)
Tilgate Ward 51 12 (40)
Slide 7
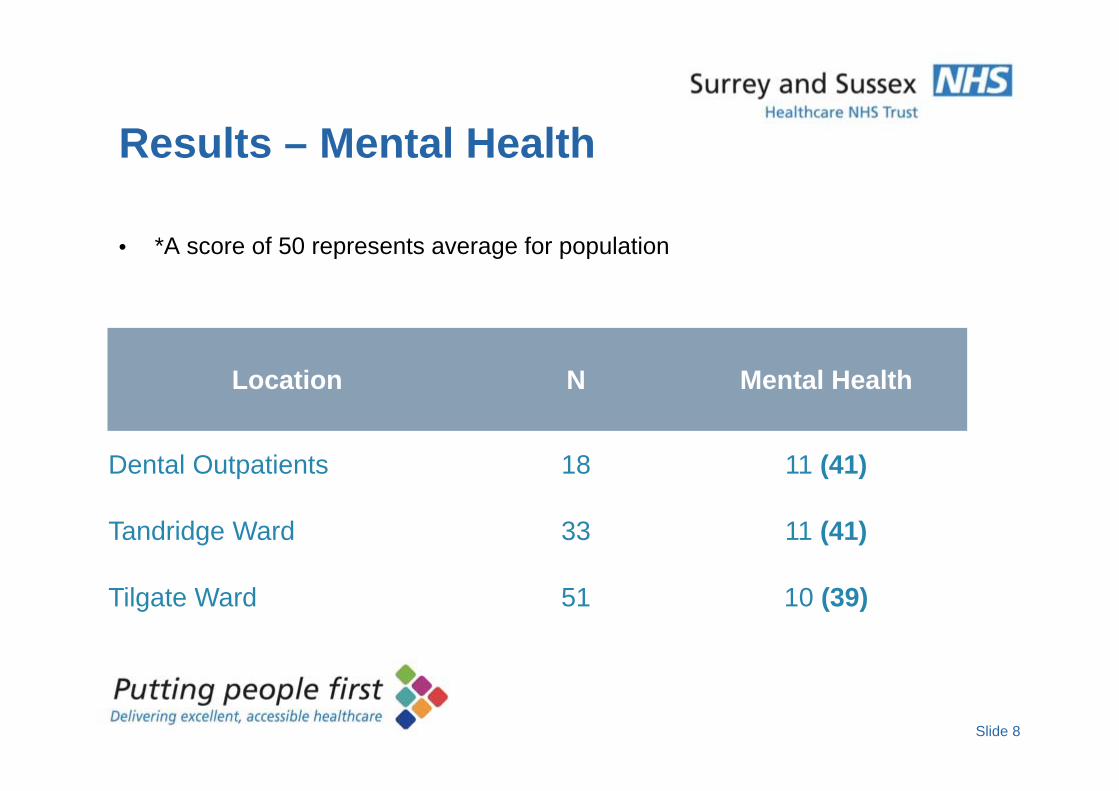
Results – Mental Health
• *A score of 50 represents average for population
Location N Mental Health
Dental Outpatients 18 11 (41)
Tandridge Ward 33 11 (41)
Tilgate Ward 51 10 (39)
Slide 8
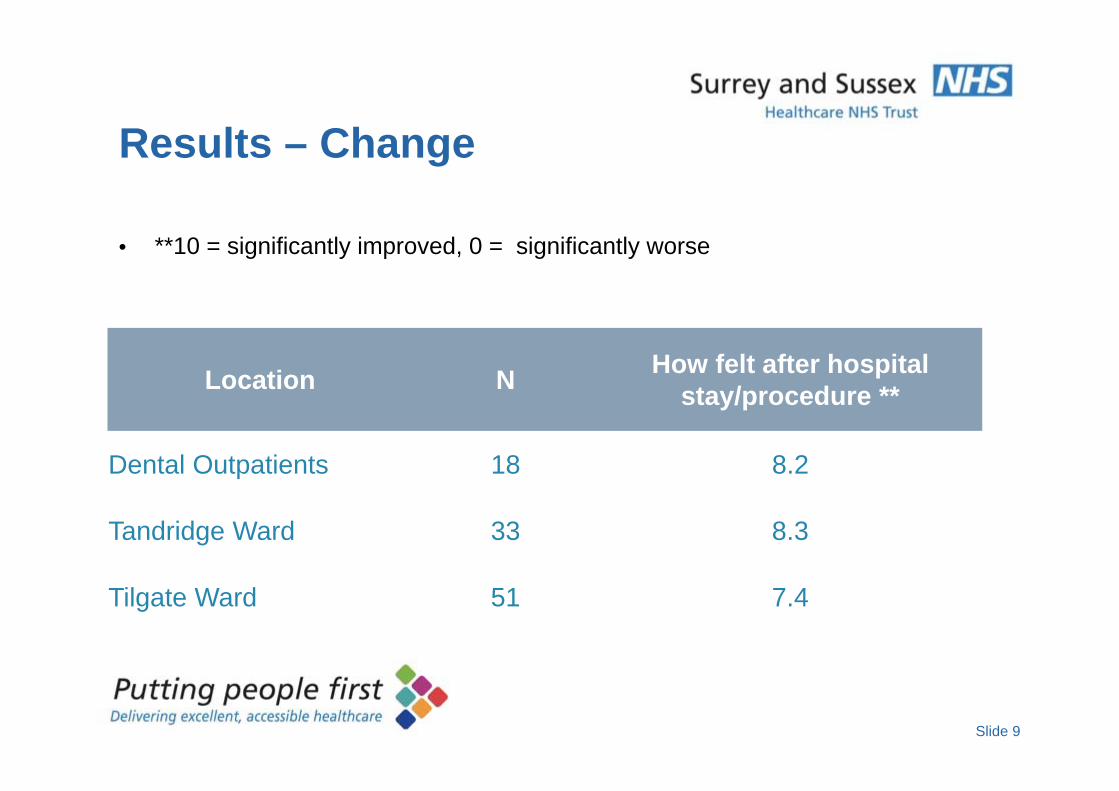
Results – Change
• **10 = significantly improved, 0 = significantly worse
Location N How felt after hospital stay/procedure **
Dental Outpatients 18 8.2
Tandridge Ward 33 8.3
Tilgate Ward 51 7.4
Slide 9
Conclusion
• Collection of PROMs data is essential to improve quality of care
• Feasible
• Good participation from patients
• Early results promising
Challenges
• Developing the results interface – currently not ideal
• Roll out to other departments
Slide 11
TRUST BOARD IN PUBLIC
Date: 30th April 2015 Agenda Item: 2.2
REPORT TITLE: New developments in patient reported outcome measures (PROMs)
EXECUTIVE SPONSOR: Dr Des Holden Medical Director
REPORT AUTHOR (s): Dr Kofi Nimako & Dr Thayalan Kandiah
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date)
Action Required:
Approval Discussion Assurance (√)
Purpose of Report:
To inform the Board of a new focus and new tools for the assessment of patient reported outcomes.
Summary of key issues
For care to be effective we would expect patients to be improved by the care or treatment they receive. Health care systems have developed a number of KPIs that lend themselves to comparison between providers (length of stay, readmission, mortality). However, the generation of KPIs whereby patients can rate themselves on how a given treatment has improved their quality of life, with a small number of exceptions reported in our quality account (e.g. hernia and varicose vein surgery) has lagged behind nationally. Both the authors of this report undertook MD theses prior to appointment at SaSH, developing PROMs in lung cancer and dental patients respectively. This presentation offers the Board an opportunity to hear how their work is being taken forward on our wards and set this in context of the national landscape.
Recommendation:
To note the new work being developed.
Relationship to Trust Strategic Objectives & Assurance Framework:
SO2: Effective - Deliver effective and sustainable clinical services within the local health economy SO3: Caring – Ensure patients are cared for and feel cared about SO4: Responsive – Become the secondary care provider and employer of choice our catchment population
Corporate Impact Assessment:
Legal and regulatory impact Likely interest to regulators
2An Associated University Hospital of Brighton and Sussex Medical School
Financial impact Nil adverse
Patient Experience/Engagement positive
Risk & Performance Management The work may enable comparison between wards and teams
NHS Constitution/Equality & Diversity/Communication
The presentation will be available on the Trust website.
Attachment:
PROMS presentation
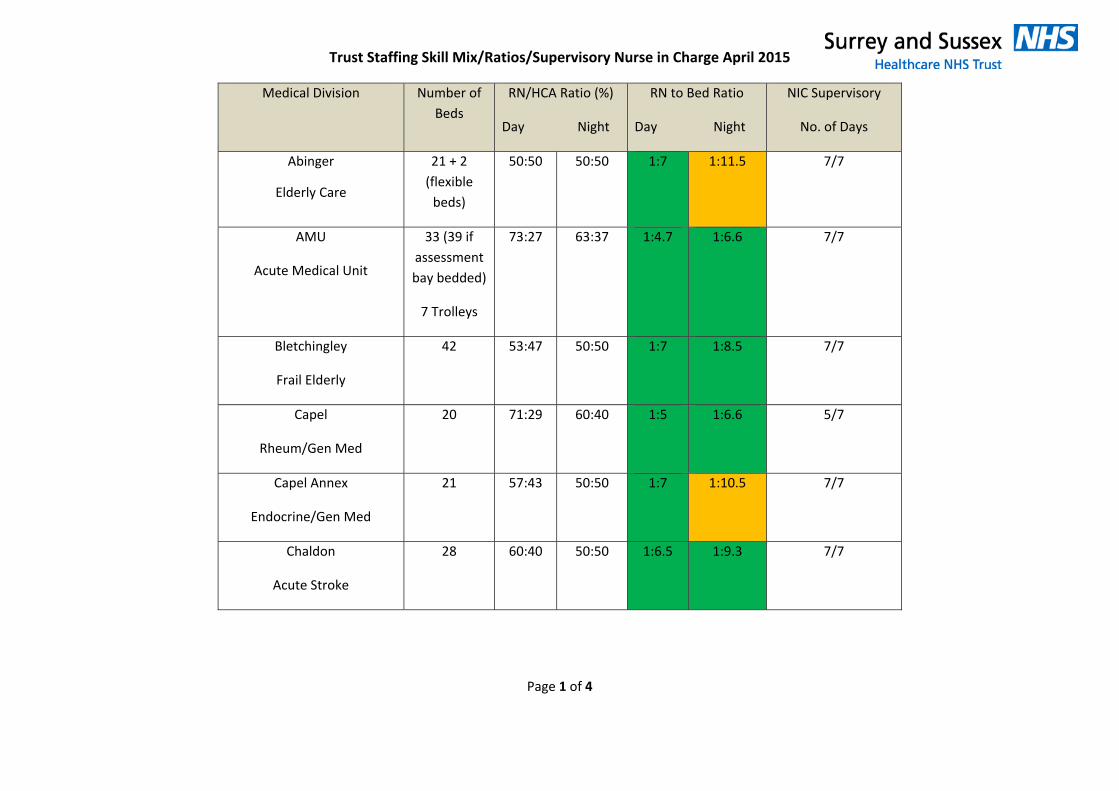
Trust Staffing Skill Mix/Ratios/Supervisory Nurse in Charge April 2015
Page 1 of 4
Medical Division Number of Beds
RN/HCA Ratio (%)
Day Night
RN to Bed Ratio
Day Night
NIC Supervisory
No. of Days
Abinger
Elderly Care
21 + 2 (flexible beds)
50:50 50:50 1:7 1:11.5 7/7
AMU
Acute Medical Unit
33 (39 if assessment bay bedded)
7 Trolleys
73:27 63:37 1:4.7 1:6.6 7/7
Bletchingley
Frail Elderly
42 53:47 50:50 1:7 1:8.5 7/7
Capel
Rheum/Gen Med
20 71:29 60:40 1:5 1:6.6 5/7
Capel Annex
Endocrine/Gen Med
21 57:43 50:50 1:7 1:10.5 7/7
Chaldon
Acute Stroke
28 60:40 50:50 1:6.5 1:9.3 7/7
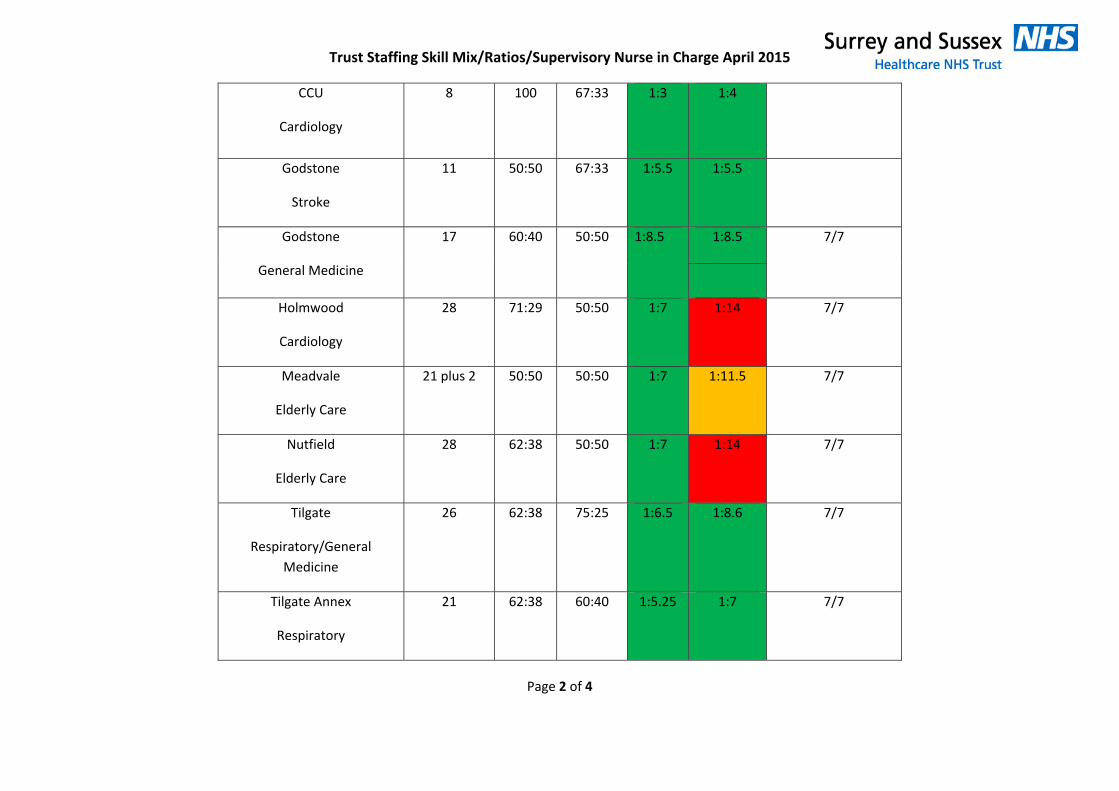
Trust Staffing Skill Mix/Ratios/Supervisory Nurse in Charge April 2015
Page 2 of 4
CCU
Cardiology
8 100 67:33 1:3 1:4
Godstone
Stroke
11 50:50 67:33 1:5.5 1:5.5
Godstone
General Medicine
17 60:40 50:50 1:8.5 1:8.5 7/7
Holmwood
Cardiology
28 71:29 50:50 1:7 1:14 7/7
Meadvale
Elderly Care
21 plus 2 50:50 50:50 1:7 1:11.5 7/7
Nutfield
Elderly Care
28 62:38 50:50 1:7 1:14 7/7
Tilgate
Respiratory/General Medicine
26 62:38 75:25 1:6.5 1:8.6 7/7
Tilgate Annex
Respiratory
21 62:38 60:40 1:5.25 1:7 7/7
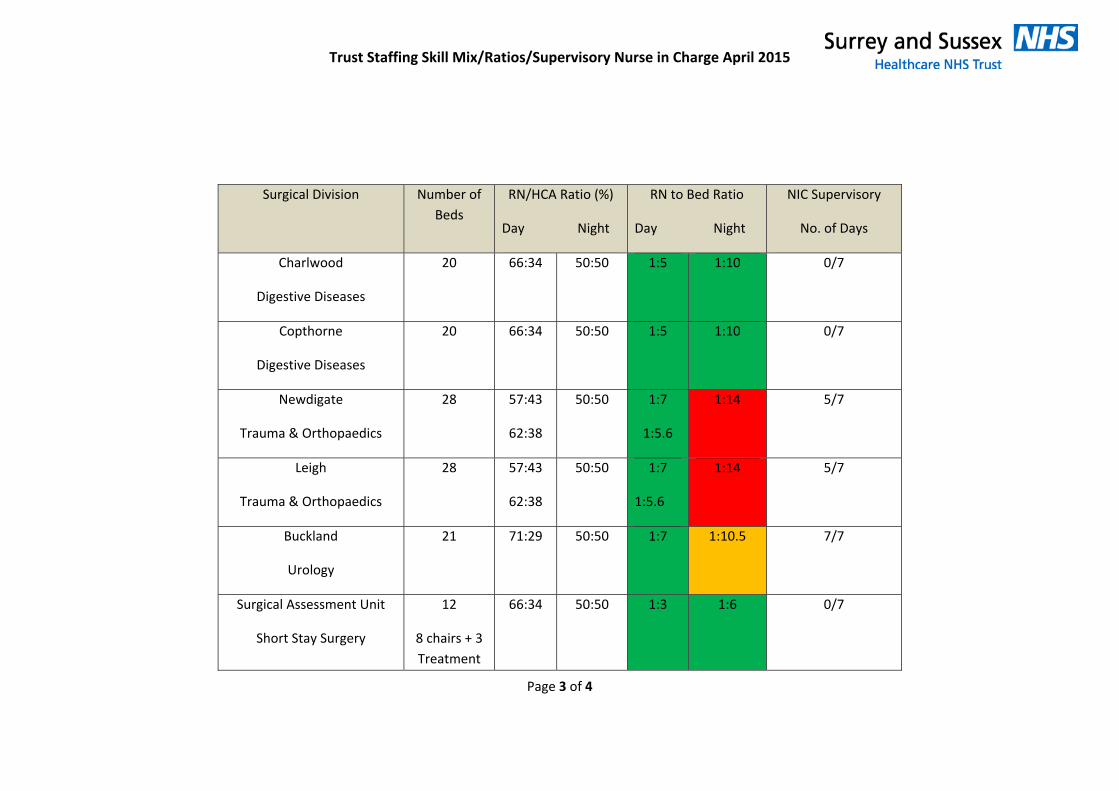
Trust Staffing Skill Mix/Ratios/Supervisory Nurse in Charge April 2015
Page 3 of 4
Surgical Division Number of Beds
RN/HCA Ratio (%)
Day Night
RN to Bed Ratio
Day Night
NIC Supervisory
No. of Days
Charlwood
Digestive Diseases
20 66:34 50:50 1:5 1:10 0/7
Copthorne
Digestive Diseases
20 66:34 50:50 1:5 1:10 0/7
Newdigate
Trauma & Orthopaedics
28 57:43
62:38
50:50 1:7
1:5.6
1:14 5/7
Leigh
Trauma & Orthopaedics
28 57:43
62:38
50:50 1:7
1:5.6
1:14 5/7
Buckland
Urology
21 71:29 50:50 1:7 1:10.5 7/7
Surgical Assessment Unit
Short Stay Surgery
12
8 chairs + 3 Treatment
66:34 50:50 1:3 1:6 0/7
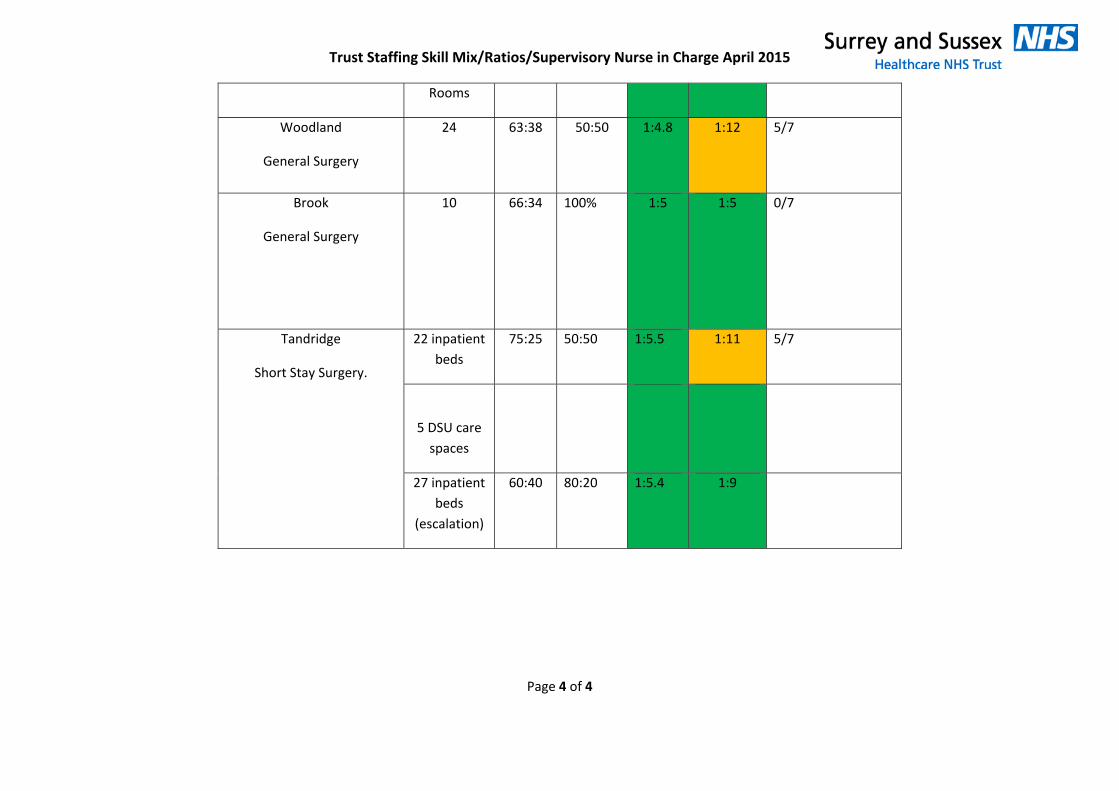
Trust Staffing Skill Mix/Ratios/Supervisory Nurse in Charge April 2015
Page 4 of 4
Rooms
Woodland
General Surgery
24 63:38 50:50 1:4.8 1:12 5/7
Brook
General Surgery
10 66:34 100% 1:5 1:5 0/7
Tandridge
Short Stay Surgery.
22 inpatient beds
75:25 50:50 1:5.5 1:11 5/7
5 DSU care spaces
27 inpatient beds
(escalation)
60:40 80:20 1:5.4 1:9
TRUST BOARD IN PUBLIC
Date: 30 April 2015 Agenda Item: 2.3
REPORT TITLE: Chief Nurse & Medical Director Report
EXECUTIVE SPONSOR: Fiona Allsop, Chief Nurse Des Holden, Medical Director
REPORT AUTHOR (s): Fiona Allsop, Chief Nurse Des Holden, Medical Director
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date) N/A
Action Required:
Approval () Discussion (√) Assurance (√)
Purpose of Report:
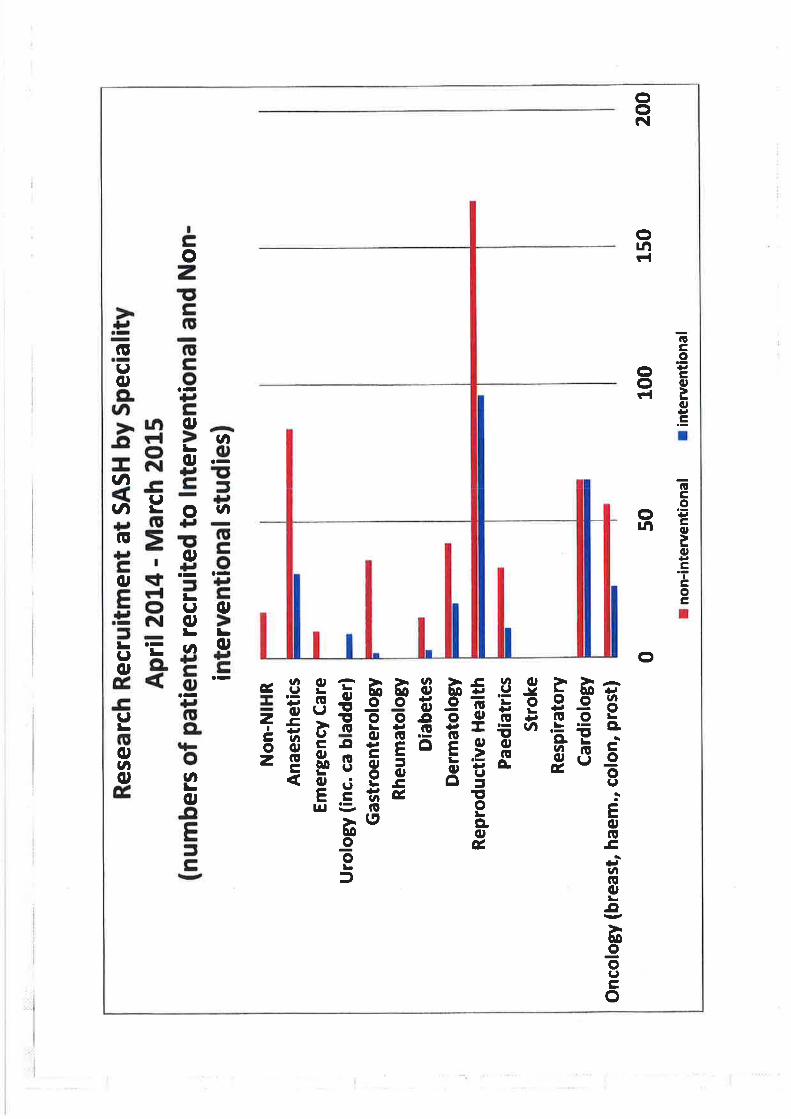
To provide an update on continuing work in relation to safe and quality focussed patient care that sits outside the operational performance reports including monthly Safer Staffing information and exception reports.
Summary of key issues
The Safer Staffing report (March 2015 data) indicates that the Trust has delivered the planned versus actual staffing levels in the inpatient areas and maternity unit against existing template. The Board will note that there has been some variation in the availability of nursing assistants during the day which has been managed by the matrons but overall the actual number of nurses on duty has matched in planned demand.
The review of ward establishments against plan in relation to Safer Staffing template to be introduced by September 2015. The Trust had prioritised the six wards for establishment increases to meet the agreed night ratio. Two wards have increased the ratio, there is a plan to increase a further two in May with the remaining two wards to meet target by September 2015.
An update on the Sign up to Safety Campaign including noting that the Trust was not successful in the bid for support funding to implement this campaign and work will continue as part of business as usual.
In 2014-15 the trust reports the highest number of patients ever recruited into NIHR adopted studies.
We report the successful appointment to the consultant grade of 3 acute physicians, two cardiologists, and a gastro-intestinal medicine consultant with a special interest in nutrition.
Recommendation:
To note the report.
Relationship to Trust Strategic Objectives & Assurance Framework:
SO1: Safe -Deliver safe services and be in the top 20% against our peers SO2: Effective - Deliver effective and sustainable clinical services within the local health economy SO3: Caring – Ensure patients are cared for and feel cared about SO4: Responsive – Become the secondary care provider and employer of choice our
2An Associated University Hospital of Brighton and Sussex Medical School
catchment population SO5: Well led: Become an employer of choice and deliver financial and clinical sustainability around a clinical leadership model
Corporate Impact Assessment:
Legal and regulatory impact Yes
Financial impact Yes
Patient Experience/Engagement Yes
Risk & Performance Management Yes
NHS Constitution/Equality & Diversity/Communication
Yes
Attachment:
See below – embedded in relevant section
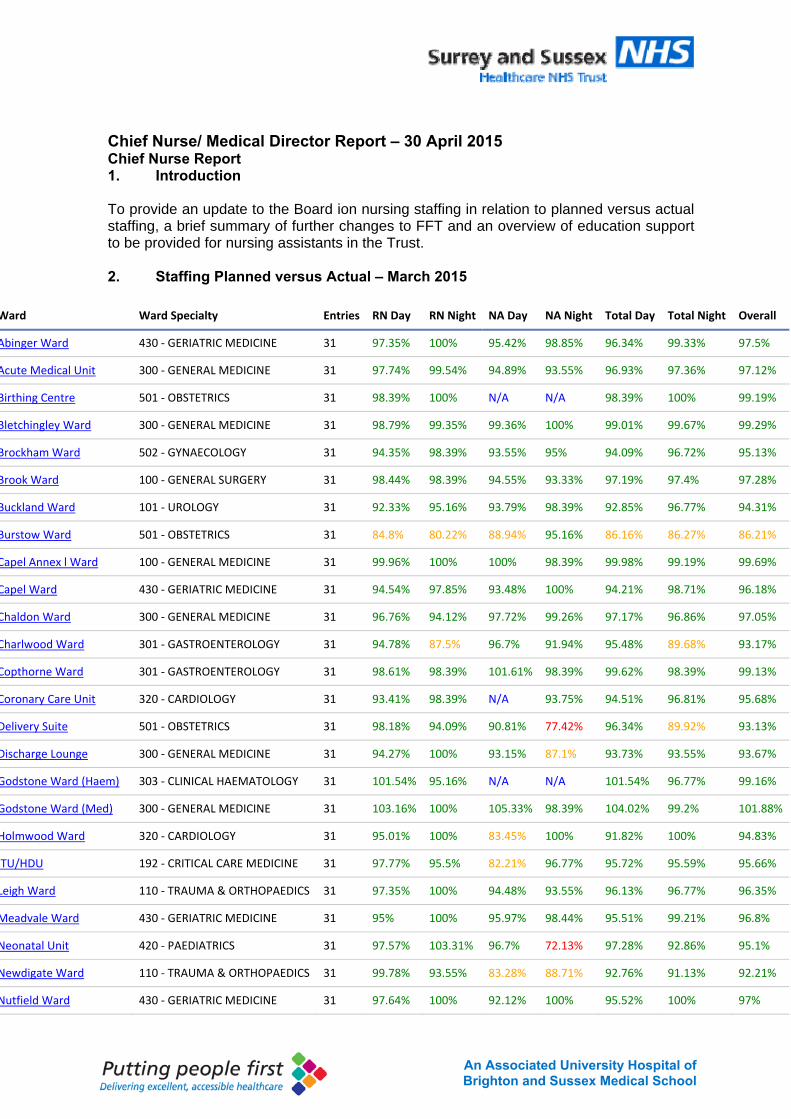
3An Associated University Hospital of Brighton and Sussex Medical School
Chief Nurse/ Medical Director Report – 30 April 2015 Chief Nurse Report 1. Introduction To provide an update to the Board ion nursing staffing in relation to planned versus actual staffing, a brief summary of further changes to FFT and an overview of education support to be provided for nursing assistants in the Trust. 2. Staffing Planned versus Actual – March 2015
Ward Ward Specialty Entries RN Day RN Night NA Day NA Night Total Day Total Night Overall
Abinger Ward 430 ‐ GERIATRIC MEDICINE 31 97.35% 100% 95.42% 98.85% 96.34% 99.33% 97.5%
Acute Medical Unit 300 ‐ GENERAL MEDICINE 31 97.74% 99.54% 94.89% 93.55% 96.93% 97.36% 97.12%
Birthing Centre 501 ‐ OBSTETRICS 31 98.39% 100% N/A N/A 98.39% 100% 99.19%
Bletchingley Ward 300 ‐ GENERAL MEDICINE 31 98.79% 99.35% 99.36% 100% 99.01% 99.67% 99.29%
Brockham Ward 502 ‐ GYNAECOLOGY 31 94.35% 98.39% 93.55% 95% 94.09% 96.72% 95.13%
Brook Ward 100 ‐ GENERAL SURGERY 31 98.44% 98.39% 94.55% 93.33% 97.19% 97.4% 97.28%
Buckland Ward 101 ‐ UROLOGY 31 92.33% 95.16% 93.79% 98.39% 92.85% 96.77% 94.31%
Burstow Ward 501 ‐ OBSTETRICS 31 84.8% 80.22% 88.94% 95.16% 86.16% 86.27% 86.21%
Capel Annex l Ward 100 ‐ GENERAL MEDICINE 31 99.96% 100% 100% 98.39% 99.98% 99.19% 99.69%
Capel Ward 430 ‐ GERIATRIC MEDICINE 31 94.54% 97.85% 93.48% 100% 94.21% 98.71% 96.18%
Chaldon Ward 300 ‐ GENERAL MEDICINE 31 96.76% 94.12% 97.72% 99.26% 97.17% 96.86% 97.05%
Charlwood Ward 301 ‐ GASTROENTEROLOGY 31 94.78% 87.5% 96.7% 91.94% 95.48% 89.68% 93.17%
Copthorne Ward 301 ‐ GASTROENTEROLOGY 31 98.61% 98.39% 101.61% 98.39% 99.62% 98.39% 99.13%
Coronary Care Unit 320 ‐ CARDIOLOGY 31 93.41% 98.39% N/A 93.75% 94.51% 96.81% 95.68%
Delivery Suite 501 ‐ OBSTETRICS 31 98.18% 94.09% 90.81% 77.42% 96.34% 89.92% 93.13%
Discharge Lounge 300 ‐ GENERAL MEDICINE 31 94.27% 100% 93.15% 87.1% 93.73% 93.55% 93.67%
Godstone Ward (Haem) 303 ‐ CLINICAL HAEMATOLOGY 31 101.54% 95.16% N/A N/A 101.54% 96.77% 99.16%
Godstone Ward (Med) 300 ‐ GENERAL MEDICINE 31 103.16% 100% 105.33% 98.39% 104.02% 99.2% 101.88%
Holmwood Ward 320 ‐ CARDIOLOGY 31 95.01% 100% 83.45% 100% 91.82% 100% 94.83%
TU/HDU 192 ‐ CRITICAL CARE MEDICINE 31 97.77% 95.5% 82.21% 96.77% 95.72% 95.59% 95.66%
Leigh Ward 110 ‐ TRAUMA & ORTHOPAEDICS 31 97.35% 100% 94.48% 93.55% 96.13% 96.77% 96.35%
Meadvale Ward 430 ‐ GERIATRIC MEDICINE 31 95% 100% 95.97% 98.44% 95.51% 99.21% 96.8%
Neonatal Unit 420 ‐ PAEDIATRICS 31 97.57% 103.31% 96.7% 72.13% 97.28% 92.86% 95.1%
Newdigate Ward 110 ‐ TRAUMA & ORTHOPAEDICS 31 99.78% 93.55% 83.28% 88.71% 92.76% 91.13% 92.21%
Nutfield Ward 430 ‐ GERIATRIC MEDICINE 31 97.64% 100% 92.12% 100% 95.52% 100% 97%
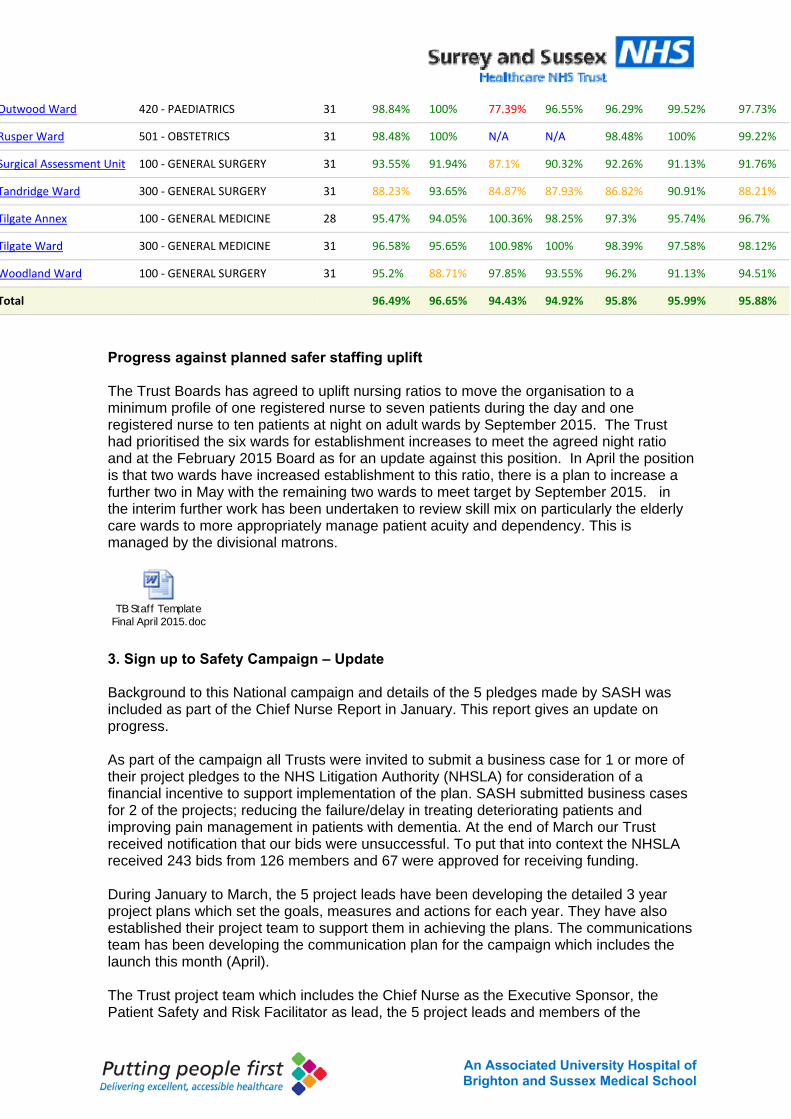
4An Associated University Hospital of Brighton and Sussex Medical School
Outwood Ward 420 ‐ PAEDIATRICS 31 98.84% 100% 77.39% 96.55% 96.29% 99.52% 97.73%
Rusper Ward 501 ‐ OBSTETRICS 31 98.48% 100% N/A N/A 98.48% 100% 99.22%
Surgical Assessment Unit 100 ‐ GENERAL SURGERY 31 93.55% 91.94% 87.1% 90.32% 92.26% 91.13% 91.76%
Tandridge Ward 300 ‐ GENERAL SURGERY 31 88.23% 93.65% 84.87% 87.93% 86.82% 90.91% 88.21%
Tilgate Annex 100 ‐ GENERAL MEDICINE 28 95.47% 94.05% 100.36% 98.25% 97.3% 95.74% 96.7%
Tilgate Ward 300 ‐ GENERAL MEDICINE 31 96.58% 95.65% 100.98% 100% 98.39% 97.58% 98.12%
Woodland Ward 100 ‐ GENERAL SURGERY 31 95.2% 88.71% 97.85% 93.55% 96.2% 91.13% 94.51%
Total 96.49% 96.65% 94.43% 94.92% 95.8% 95.99% 95.88%
Progress against planned safer staffing uplift The Trust Boards has agreed to uplift nursing ratios to move the organisation to a minimum profile of one registered nurse to seven patients during the day and one registered nurse to ten patients at night on adult wards by September 2015. The Trust had prioritised the six wards for establishment increases to meet the agreed night ratio and at the February 2015 Board as for an update against this position. In April the position is that two wards have increased establishment to this ratio, there is a plan to increase a further two in May with the remaining two wards to meet target by September 2015. in the interim further work has been undertaken to review skill mix on particularly the elderly care wards to more appropriately manage patient acuity and dependency. This is managed by the divisional matrons.
TB Staff Template Final April 2015.doc 3. Sign up to Safety Campaign – Update Background to this National campaign and details of the 5 pledges made by SASH was included as part of the Chief Nurse Report in January. This report gives an update on progress. As part of the campaign all Trusts were invited to submit a business case for 1 or more of their project pledges to the NHS Litigation Authority (NHSLA) for consideration of a financial incentive to support implementation of the plan. SASH submitted business cases for 2 of the projects; reducing the failure/delay in treating deteriorating patients and improving pain management in patients with dementia. At the end of March our Trust received notification that our bids were unsuccessful. To put that into context the NHSLA received 243 bids from 126 members and 67 were approved for receiving funding. During January to March, the 5 project leads have been developing the detailed 3 year project plans which set the goals, measures and actions for each year. They have also established their project team to support them in achieving the plans. The communications team has been developing the communication plan for the campaign which includes the launch this month (April). The Trust project team which includes the Chief Nurse as the Executive Sponsor, the Patient Safety and Risk Facilitator as lead, the 5 project leads and members of the
5An Associated University Hospital of Brighton and Sussex Medical School
communication team, will continue to meet in order to oversee the progress of the plans. Through receipt of quarterly exception reports from the 5 project leads, the Executive Committee for Quality and Risk will monitor the Safety Improvement Plan and provide assurance to the Trust Board via the Safety and Quality Committee (SQC). Professor Jane Reid, Regional Lead for the South from the NHS England campaign team has offered to attend the Trust. A date for her to speak at SQC is being confirmed. 4. R&D performance 726 patients were recruited in to research studies approved by the NIHR in 2014-15, making this the most successful year ever. In the last year, our research teams have opened up 26 new clinical research studies for patients to participate in and we are now supporting the care of patients in 45 different research studies and recruiting patients into 12 national and international pharmaceutical company sponsored research studies. We embarked on 8 commercially funded studies. Of these one met its recruitment target, three are still open and are recruiting but are yet to meet target, and four closed (patients being followed up) but less than target number of patients were recruited. The figures below show the proportion of studies in different clinical specialities, and the split between interventional and observational studies by patient recruitment.
Research Recruitment 1.pdf
Research Recruitment 2.pdf
5. Consultant recruitment In the last month we have appointed three consultants in acute medicine (Drs Martin Dachsel, Padmini Sastry and Radha Selvaratnam, and a consultant gastroenterologist with a special interest in nutrition, Dr Jonathan Nolan. Between submitting this paper and presenting it at April trust Board there will be a further appointments panel where it is hoped we will make job offers to two cardiologists, one with an interest in coronary intervention and the one with an interest in electrophysiology and devices to correct rhythm disturbance. All these posts are new rather than replacement but enable either increased demand to be met, or our increased patients being cared for by acute physicians, strengthening in addition our 7 day service. 6. Pharmacy update At the service deep dive the team once again reported full pharmacy recruitment. The service change that enables patients receiving chemotherapy to collect their medications from local branches of Boots chemists has begun. So far there have been more than 20 patients who have taken advantage of local collection and there have been no reported problems. Informal feedback through Boots is that the service is very popular with patients. We will formally audit the service after three months. 3. Recommendation To note the report
6An Associated University Hospital of Brighton and Sussex Medical School
Fiona Allsop Des Holden Chief Nurse Medical Director April 2015
TRUST BOARD IN PUBLIC
Date: 30th April 2015 Agenda Item: 2.4
REPORT TITLE: Safety & Quality Committee Update
NON-EXECUTIVE SPONSOR: Richard Shaw Chair Safety & Quality Committee
REPORT AUTHOR (s): Richard Shaw Chair Safety & Quality Committee
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date) n/a
Action Required:
Approval () Discussion ( ) Assurance ()
Purpose of Report: To provide an update of the activities of the safety and quality committee. Summary of key issues The report provides a summary of the key agenda items which were discussed at the Safety and Quality Committee in April 2015.
Recommendation:
The Board is asked to note the report for assurance.
Relationship to Trust Strategic Objectives & Assurance Framework:
SO1: Safe -Deliver safe services and be in the top 20% against our peers SO2: Effective - Deliver effective and sustainable clinical services within the local health economy SO3: Caring – Ensure patients are cared for and feel cared about Corporate Impact Assessment:
Legal and regulatory impact Compliance with CQC, MHRA and Audit Commission
Financial impact Serious incidents often become claims
Patient Experience/Engagement Patient Experience & Engagement is an essential
Risk & Performance Management Reporting, investigation and learning from serious incidents informs risk management
NHS Constitution/Equality & Diversity/Communication Included in the report
Attachment: N/A
Trust Board Report – 30th April 2015 Safety and Quality Committee Chair’s Report 1. Introduction
The Safety and Quality Committee met on 2nd April 2015. It considered its standing agenda items; the report from January’s ECQRM and CQRM meeting and the SQC Dashboard and Quality Report. 2. Action Log: Discharge Planning and Mortality data accuracy The committee had sought further assurance on the safety of night-time discharges following evidence that suggested some discharges had taken place late at night. An audit carried out over a five month period provided good assurance of safety, with all patients medically fit for discharge and discharged safely with good evidence of discharge planning. The main reason for later discharge was the provision of patient transport often affected by late afternoon ward rounds. Actions are now being put in place to achieve earlier discharge. The Committee had also sought further assurance on the accuracy of recording the date of death in Cerner. An audit carried out following concerns raised at an earlier committee showed a 23% inaccuracy rate, normally by one day and mainly at weekends. Corrections are now being made and the data resubmitted. Closer checks on data accuracy will be made in future, and breaking down the data by ward will enable more focused training and management oversight. Assurance was also taken from the role of Clinical Effectiveness Committee in reviewing mortality data and the Dr Foster report monthly. 3. Data Quality Strategy The Committee approved a final version of the Data Quality Strategy that had been revised and improved following discussion at the Trust Board. The strategy sets out context, principles and structures for providing data quality assurance. It also contains priorities for improvement and an action plan for achieving them. The Committee was assured that the Trust had the necessary expertise to deliver the strategy, although the adequacy of the scale of expertise will be kept under review. SQC will receive quarterly reports on the delivery of the strategy. 4. Quality Report and Dashboard
In discussion of the Quality Report, the Committee focused on two new sections that helpfully describe patient Length of Stay and Theatre Productivity. The length of stay data benchmarked the Trust’s performance against 30 other organisations of a similar size and case mix and will enable monitoring of the improvements the Trust needs to make. The data is available at consultant level and has been shared with the Divisions so that an improvement plan can be formulated. The data on theatres, split between Crawley and ESH, showed that productivity and patient experience are two key areas for improvement. This can be achieved by starting lists on time, booking lists appropriately and treating all patients who are booked that day. The Trust is aiming for 80% list utilisation (allowing for turnaround time). This compares to a current level of 51%, which may have been adversely affected by the extensive building work in theatres.
5. ED National Survey
The Committee is monitoring the results of national surveys of specific services, and received a report on the findings of the recent survey of the Emergency Department. This showed a positive change in performance as a result of an increased focus on quality of care and sustained improvements in establishment. It also showed some areas for further improvement, including communication of waiting times, pain control and waiting times. Actions are being put in place and will be monitored through the Patient Experience Committee. 6. Infection Control Following a concern raised at its previous meeting that staff may not be adequately aware of bio-hazard alerts on Cerner, the committee explored the nature of the risk and potential solutions, especially in relation to babies. Alerts are flagged on Cerner and all staff are trained in how to use them, but there are risks associated with “alert-fatigue” and the volume of information provided. Work is being undertaken to develop the pathology system to include an alert, and also to amend the Cerner system at the earliest opportunity so as to give more prominence to bio-hazard alerts. The issue will also be drawn to the attention of the Infection Control Committee. The Trust’s infection control regime has seen a zero incidence of MRSA over the last 12 months, a declining incidence of C-Diff and effective management of Norovirus. The Committee received a report and action plan which aims to reduce further the incidence of hospital acquired infections in 2015/15. Last year saw 24 cases of C-Diff. Further analysis of each of the cases found that there were issues of anti-biotical stewardship in 4 cases and 3 cases would be considered cross infections. The programme for 2015/16 has been adapted to incorporate the lessons learnt from each of these cases, and includes even more attention to detail and an emphasis on learning. The revised target for the Trust in the year 2015/16 is a maximum of 15 cases, which will be challenging to achieve. 7. Clinical Audit The Committee received a report setting out good evidence of learning from the clinical audit programme and actions to improve the completion rate, enhance learning from complaints and incidents, and give assurance to SQC. Divisional audit plans will be managed through the Clinical Effectiveness Committee and the minutes of the Governance Meetings containing details of audit action plans will be reviewed at ECQRM. There will be a smaller programme of work for 2015/16 with the explicit agreement that if an audit is added to the programme then it will be completed and an output will be produced. The programme will be focused on how we learn, and how we make changes following incidents and complaints in order to deliver a safer service. The national requirements will be handled centrally in order to free up the Divisions to concentrate on the work that will improve their services. SQC will review the 2015/16 audit programme at its June meeting. The next meeting of the Committee is on 7th May. 8. Recommendation The Board is asked to note the report for assurance. Richard Shaw Non-Executive Director April 2015
An Associated University Hospital of
Brighton and Sussex Medical School 1
Integrated Performance Report
M12 – March 2015
Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer)
An Associated University Hospital of
Brighton and Sussex Medical School
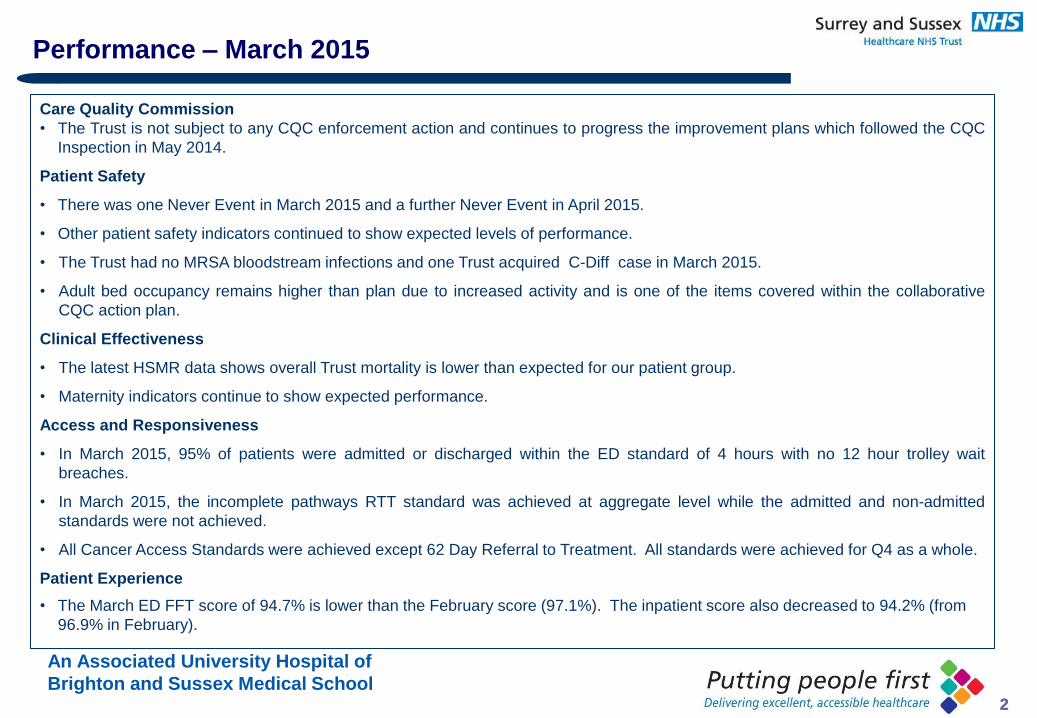
An Associated University Hospital of
Brighton and Sussex Medical School 2 2
Care Quality Commission
• The Trust is not subject to any CQC enforcement action and continues to progress the improvement plans which followed the CQC
Inspection in May 2014.
Patient Safety
• There was one Never Event in March 2015 and a further Never Event in April 2015.
• Other patient safety indicators continued to show expected levels of performance.
• The Trust had no MRSA bloodstream infections and one Trust acquired C-Diff case in March 2015.
• Adult bed occupancy remains higher than plan due to increased activity and is one of the items covered within the collaborative
CQC action plan.
Clinical Effectiveness
• The latest HSMR data shows overall Trust mortality is lower than expected for our patient group.
• Maternity indicators continue to show expected performance.
Access and Responsiveness
• In March 2015, 95% of patients were admitted or discharged within the ED standard of 4 hours with no 12 hour trolley wait
breaches.
• In March 2015, the incomplete pathways RTT standard was achieved at aggregate level while the admitted and non-admitted
standards were not achieved.
• All Cancer Access Standards were achieved except 62 Day Referral to Treatment. All standards were achieved for Q4 as a whole.
Patient Experience
• The March ED FFT score of 94.7% is lower than the February score (97.1%). The inpatient score also decreased to 94.2% (from
96.9% in February).
Performance – March 2015
An Associated University Hospital of
Brighton and Sussex Medical School 3 3
Action: The Board are asked to note and accept this report
Legal: What are the legal
considerations & implications
linked to this item? Please name
relevant Act
Patient safety: Legal actions from unintentional harm to patients would normally be covered by negligence, an area of English tort
(civil) law, providing the remedy of compensation. Case law is extensive. Criminal action could be pursued if investigation judged
intentional harm and remedies will vary according to severity.
Staff safety: The Health and Safety at Work Act etc 1974 may apply in respect of employee health and safety or non clinical risk
to patients (usually reported under the Reporting of Injuries Diseases and Dangerous Occurrences Regulations (RIDDOR) 1995)
Regulation: What aspect of
regulation applies and what are
the outcome implications? This
applies to any regulatory body.
The Care Quality Commission (CQC) regulates patient safety and quality of care and the CQC register and therefore license
care services under the Health and Social Care Act 2009 and associated regulations. The health and safety executive regulates
compliance with health and safety law. A raft of other regulators deal with safety of medicines, medical devices and other
aspects.
Workforce
• The Trust continues to monitor ward nursing (numbers and skill mix) on a daily basis and is assured that adequate staffing is in place.
Ward staffing levels are now published on the Trust’s external website at ward level. The Trust is also continuing to monitor temporary
staffing usage on a weekly basis
Finance
• The Trust has improved slightly on its forecast year position reported last month with a £2.4m year end deficit (subject to audit
review). All figures remain provisional until the external audit review is concluded.
Key Risks
• Quality – The Significant Risk Register for the Trust includes six quality risks in relation to “Right bed first time”, ED Access standards,
Outbreak of viral gastroenteritis, Local availability of qualified nurses and Increasing sickness absence levels and Cancelled and / or
delayed elective operations.
Performance – March 2015
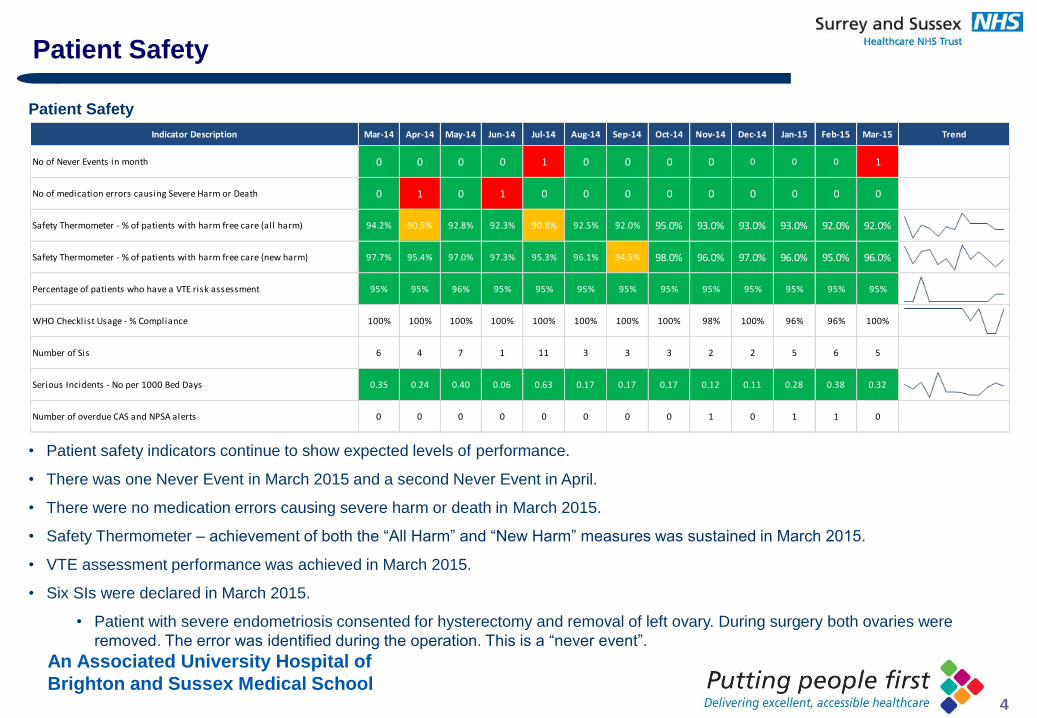
An Associated University Hospital of
Brighton and Sussex Medical School 4
Patient Safety
• Patient safety indicators continue to show expected levels of performance.
• There was one Never Event in March 2015 and a second Never Event in April.
• There were no medication errors causing severe harm or death in March 2015.
• Safety Thermometer – achievement of both the “All Harm” and “New Harm” measures was sustained in March 2015.
• VTE assessment performance was achieved in March 2015.
• Six SIs were declared in March 2015.
• Patient with severe endometriosis consented for hysterectomy and removal of left ovary. During surgery both ovaries were
removed. The error was identified during the operation. This is a “never event”.
Patient Safety
Indicator Description Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Trend
No of Never Events in month 0 0 0 0 1 0 0 0 0 0 0 0 1
No of medication errors causing Severe Harm or Death 0 1 0 1 0 0 0 0 0 0 0 0 0
Safety Thermometer - % of patients with harm free care (all harm) 94.2% 90.5% 92.8% 92.3% 90.8% 92.5% 92.0% 95.0% 93.0% 93.0% 93.0% 92.0% 92.0%
Safety Thermometer - % of patients with harm free care (new harm) 97.7% 95.4% 97.0% 97.3% 95.3% 96.1% 94.5% 98.0% 96.0% 97.0% 96.0% 95.0% 96.0%
Percentage of patients who have a VTE risk assessment 95% 95% 96% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
WHO Checklist Usage - % Compliance 100% 100% 100% 100% 100% 100% 100% 100% 98% 100% 96% 96% 100%
Number of Sis 6 4 7 1 11 3 3 3 2 2 5 6 5
Serious Incidents - No per 1000 Bed Days 0.35 0.24 0.40 0.06 0.63 0.17 0.17 0.17 0.12 0.11 0.28 0.38 0.32
Number of overdue CAS and NPSA alerts 0 0 0 0 0 0 0 0 1 0 1 1 0
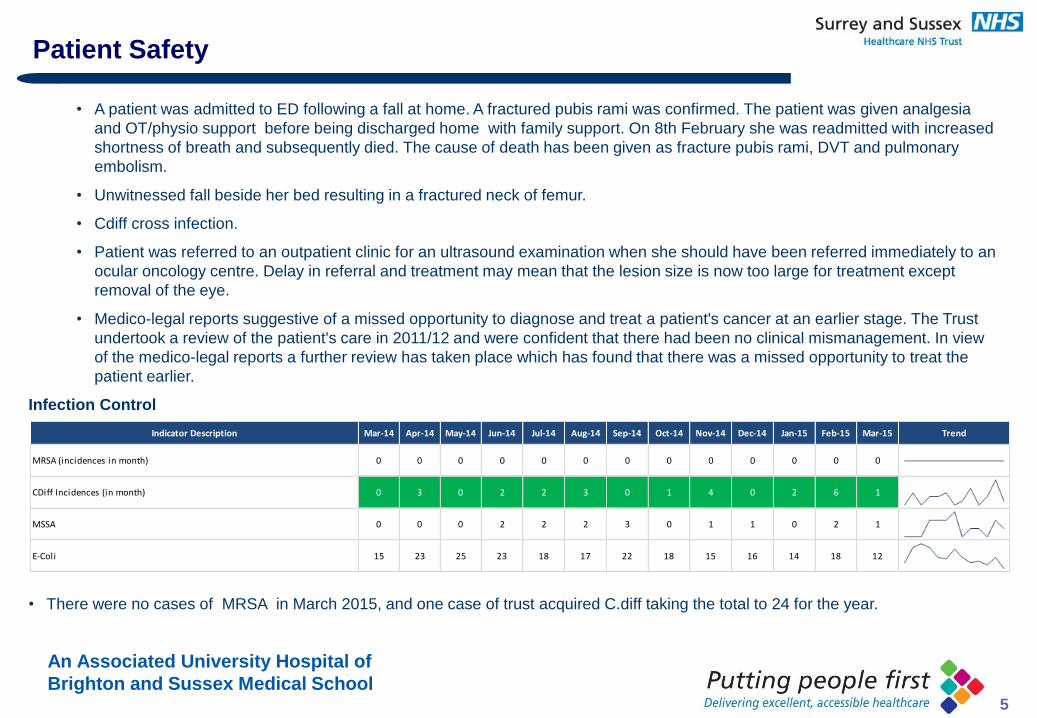
An Associated University Hospital of
Brighton and Sussex Medical School 5
• A patient was admitted to ED following a fall at home. A fractured pubis rami was confirmed. The patient was given analgesia
and OT/physio support before being discharged home with family support. On 8th February she was readmitted with increased
shortness of breath and subsequently died. The cause of death has been given as fracture pubis rami, DVT and pulmonary
embolism.
• Unwitnessed fall beside her bed resulting in a fractured neck of femur.
• Cdiff cross infection.
• Patient was referred to an outpatient clinic for an ultrasound examination when she should have been referred immediately to an
ocular oncology centre. Delay in referral and treatment may mean that the lesion size is now too large for treatment except
removal of the eye.
• Medico-legal reports suggestive of a missed opportunity to diagnose and treat a patient's cancer at an earlier stage. The Trust
undertook a review of the patient's care in 2011/12 and were confident that there had been no clinical mismanagement. In view
of the medico-legal reports a further review has taken place which has found that there was a missed opportunity to treat the
patient earlier.
Infection Control
• There were no cases of MRSA in March 2015, and one case of trust acquired C.diff taking the total to 24 for the year.
Patient Safety
Indicator Description Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Trend
MRSA (incidences in month) 0 0 0 0 0 0 0 0 0 0 0 0 0
CDiff Incidences (in month) 0 3 0 2 2 3 0 1 4 0 2 6 1
MSSA 0 0 0 2 2 2 3 0 1 1 0 2 1
E-Coli 15 23 25 23 18 17 22 18 15 16 14 18 12
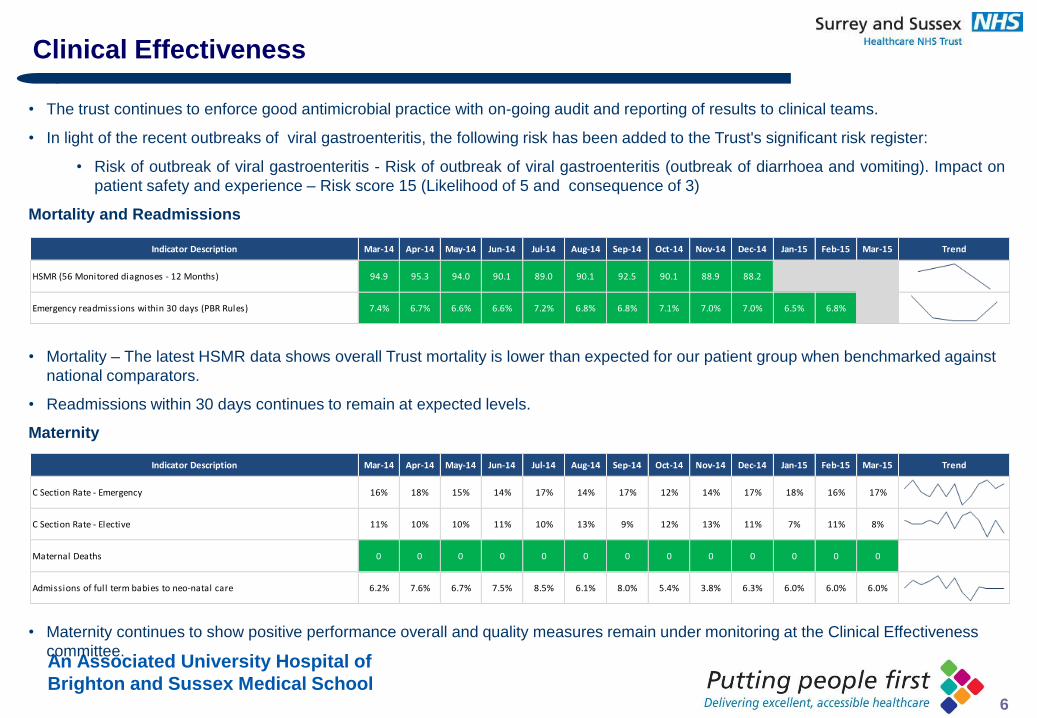
An Associated University Hospital of
Brighton and Sussex Medical School 6
• The trust continues to enforce good antimicrobial practice with on-going audit and reporting of results to clinical teams.
• In light of the recent outbreaks of viral gastroenteritis, the following risk has been added to the Trust's significant risk register:
• Risk of outbreak of viral gastroenteritis - Risk of outbreak of viral gastroenteritis (outbreak of diarrhoea and vomiting). Impact on
patient safety and experience – Risk score 15 (Likelihood of 5 and consequence of 3)
Mortality and Readmissions
• Mortality – The latest HSMR data shows overall Trust mortality is lower than expected for our patient group when benchmarked against
national comparators.
• Readmissions within 30 days continues to remain at expected levels.
Maternity
• Maternity continues to show positive performance overall and quality measures remain under monitoring at the Clinical Effectiveness
committee.
Clinical Effectiveness
Indicator Description Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Trend
HSMR (56 Monitored diagnoses - 12 Months) 94.9 95.3 94.0 90.1 89.0 90.1 92.5 90.1 88.9 88.2
Emergency readmissions within 30 days (PBR Rules) 7.4% 6.7% 6.6% 6.6% 7.2% 6.8% 6.8% 7.1% 7.0% 7.0% 6.5% 6.8%
Indicator Description Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Trend
C Section Rate - Emergency 16% 18% 15% 14% 17% 14% 17% 12% 14% 17% 18% 16% 17%
C Section Rate - Elective 11% 10% 10% 11% 10% 13% 9% 12% 13% 11% 7% 11% 8%
Maternal Deaths 0 0 0 0 0 0 0 0 0 0 0 0 0
Admissions of full term babies to neo-natal care 6.2% 7.6% 6.7% 7.5% 8.5% 6.1% 8.0% 5.4% 3.8% 6.3% 6.0% 6.0% 6.0%
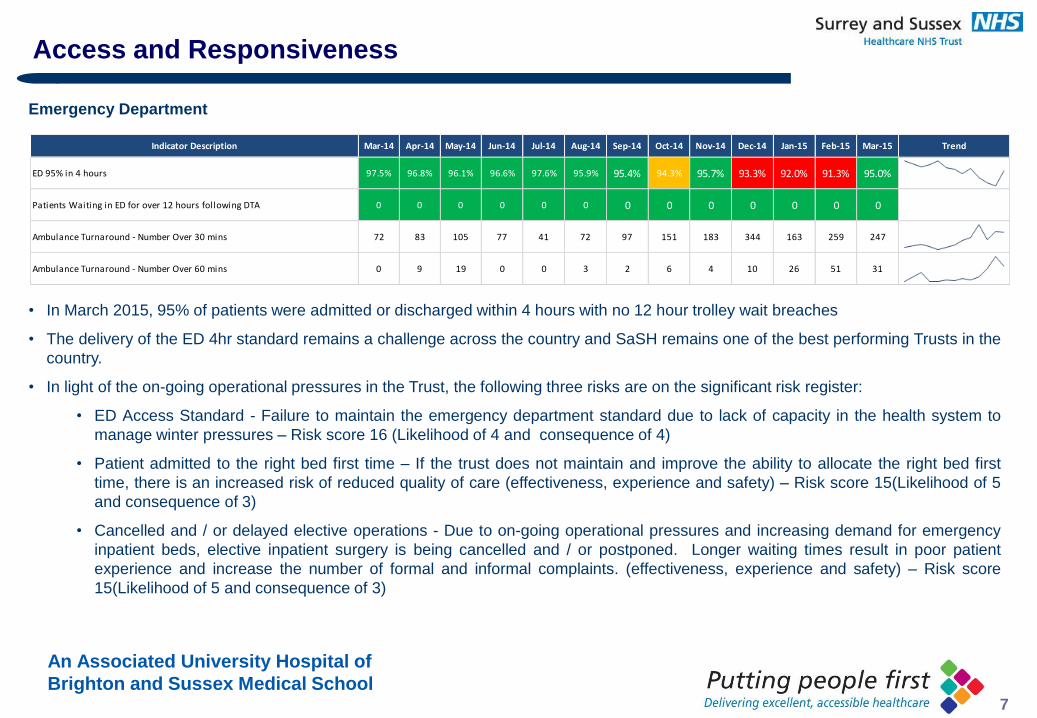
An Associated University Hospital of
Brighton and Sussex Medical School 7
Emergency Department
• In March 2015, 95% of patients were admitted or discharged within 4 hours with no 12 hour trolley wait breaches
• The delivery of the ED 4hr standard remains a challenge across the country and SaSH remains one of the best performing Trusts in the
country.
• In light of the on-going operational pressures in the Trust, the following three risks are on the significant risk register:
• ED Access Standard - Failure to maintain the emergency department standard due to lack of capacity in the health system to
manage winter pressures – Risk score 16 (Likelihood of 4 and consequence of 4)
• Patient admitted to the right bed first time – If the trust does not maintain and improve the ability to allocate the right bed first
time, there is an increased risk of reduced quality of care (effectiveness, experience and safety) – Risk score 15(Likelihood of 5
and consequence of 3)
• Cancelled and / or delayed elective operations - Due to on-going operational pressures and increasing demand for emergency
inpatient beds, elective inpatient surgery is being cancelled and / or postponed. Longer waiting times result in poor patient
experience and increase the number of formal and informal complaints. (effectiveness, experience and safety) – Risk score
15(Likelihood of 5 and consequence of 3)
Access and Responsiveness
Indicator Description Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Trend
ED 95% in 4 hours 97.5% 96.8% 96.1% 96.6% 97.6% 95.9% 95.4% 94.3% 95.7% 93.3% 92.0% 91.3% 95.0%
Patients Waiting in ED for over 12 hours following DTA 0 0 0 0 0 0 0 0 0 0 0 0 0
Ambulance Turnaround - Number Over 30 mins 72 83 105 77 41 72 97 151 183 344 163 259 247
Ambulance Turnaround - Number Over 60 mins 0 9 19 0 0 3 2 6 4 10 26 51 31
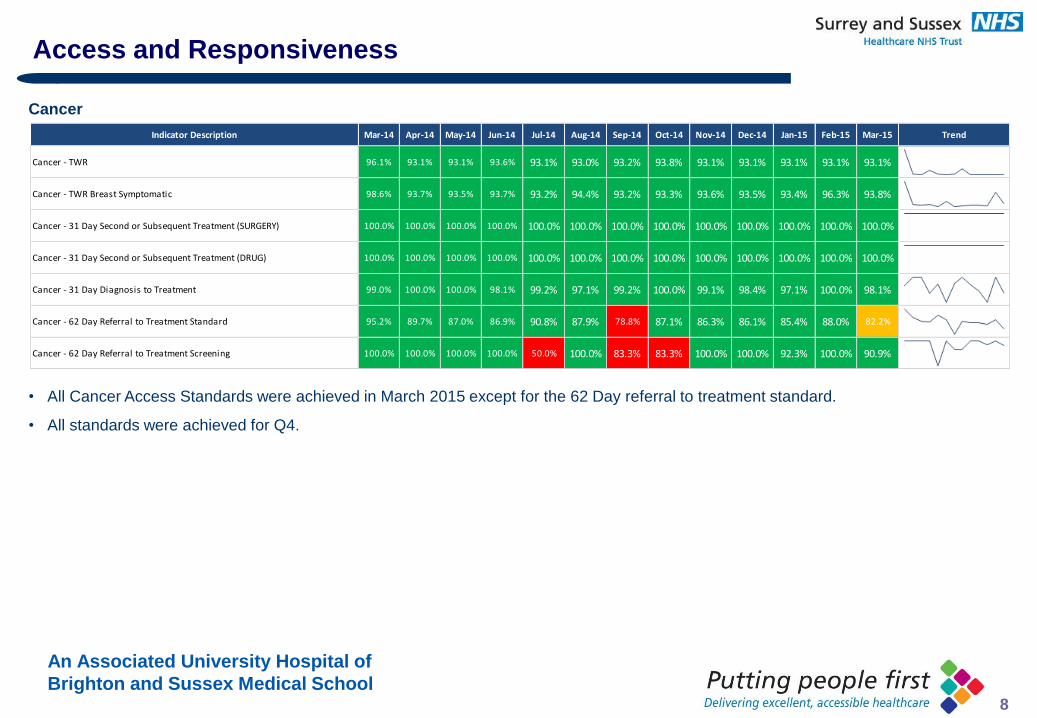
An Associated University Hospital of
Brighton and Sussex Medical School 8
Cancer
• All Cancer Access Standards were achieved in March 2015 except for the 62 Day referral to treatment standard.
• All standards were achieved for Q4.
Access and Responsiveness
Indicator Description Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Trend
Cancer - TWR 96.1% 93.1% 93.1% 93.6% 93.1% 93.0% 93.2% 93.8% 93.1% 93.1% 93.1% 93.1% 93.1%
Cancer - TWR Breast Symptomatic 98.6% 93.7% 93.5% 93.7% 93.2% 94.4% 93.2% 93.3% 93.6% 93.5% 93.4% 96.3% 93.8%
Cancer - 31 Day Second or Subsequent Treatment (SURGERY) 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
Cancer - 31 Day Second or Subsequent Treatment (DRUG) 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
Cancer - 31 Day Diagnosis to Treatment 99.0% 100.0% 100.0% 98.1% 99.2% 97.1% 99.2% 100.0% 99.1% 98.4% 97.1% 100.0% 98.1%
Cancer - 62 Day Referral to Treatment Standard 95.2% 89.7% 87.0% 86.9% 90.8% 87.9% 78.8% 87.1% 86.3% 86.1% 85.4% 88.0% 82.2%
Cancer - 62 Day Referral to Treatment Screening 100.0% 100.0% 100.0% 100.0% 50.0% 100.0% 83.3% 83.3% 100.0% 100.0% 92.3% 100.0% 90.9%
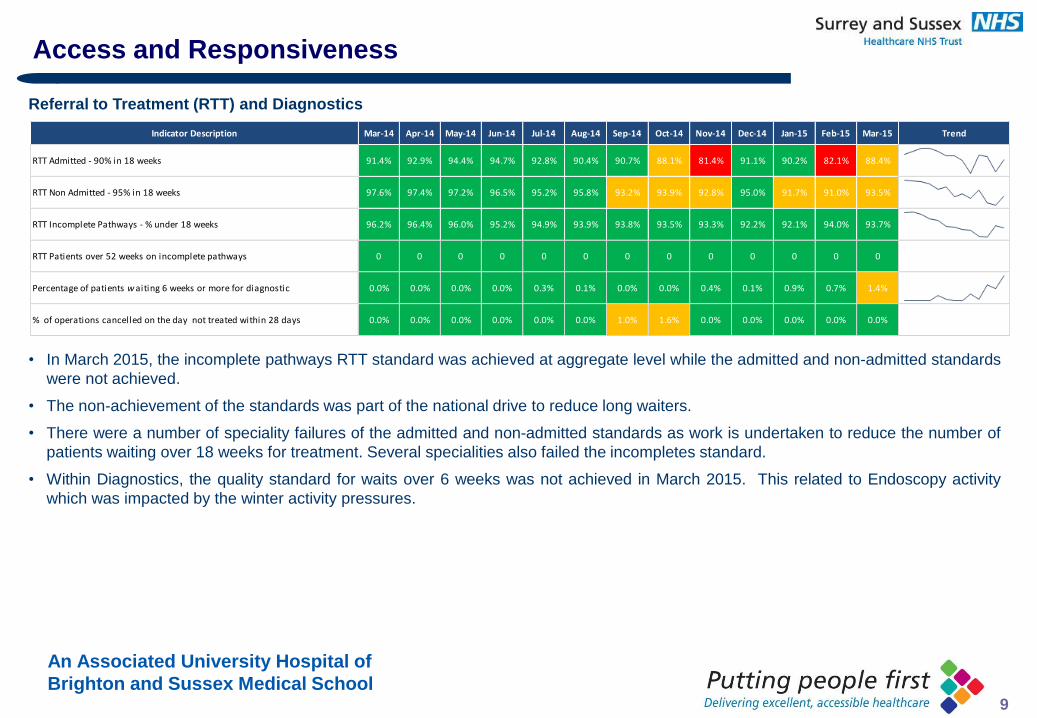
An Associated University Hospital of
Brighton and Sussex Medical School 9
Referral to Treatment (RTT) and Diagnostics
• In March 2015, the incomplete pathways RTT standard was achieved at aggregate level while the admitted and non-admitted standards
were not achieved.
• The non-achievement of the standards was part of the national drive to reduce long waiters.
• There were a number of speciality failures of the admitted and non-admitted standards as work is undertaken to reduce the number of
patients waiting over 18 weeks for treatment. Several specialities also failed the incompletes standard.
• Within Diagnostics, the quality standard for waits over 6 weeks was not achieved in March 2015. This related to Endoscopy activity
which was impacted by the winter activity pressures.
Access and Responsiveness
Indicator Description Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Trend
RTT Admitted - 90% in 18 weeks 91.4% 92.9% 94.4% 94.7% 92.8% 90.4% 90.7% 88.1% 81.4% 91.1% 90.2% 82.1% 88.4%
RTT Non Admitted - 95% in 18 weeks 97.6% 97.4% 97.2% 96.5% 95.2% 95.8% 93.2% 93.9% 92.8% 95.0% 91.7% 91.0% 93.5%
RTT Incomplete Pathways - % under 18 weeks 96.2% 96.4% 96.0% 95.2% 94.9% 93.9% 93.8% 93.5% 93.3% 92.2% 92.1% 94.0% 93.7%
RTT Patients over 52 weeks on incomplete pathways 0 0 0 0 0 0 0 0 0 0 0 0 0
Percentage of patients waiting 6 weeks or more for diagnostic 0.0% 0.0% 0.0% 0.0% 0.3% 0.1% 0.0% 0.0% 0.4% 0.1% 0.9% 0.7% 1.4%
% of operations cancelled on the day not treated within 28 days 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 1.0% 1.6% 0.0% 0.0% 0.0% 0.0% 0.0%
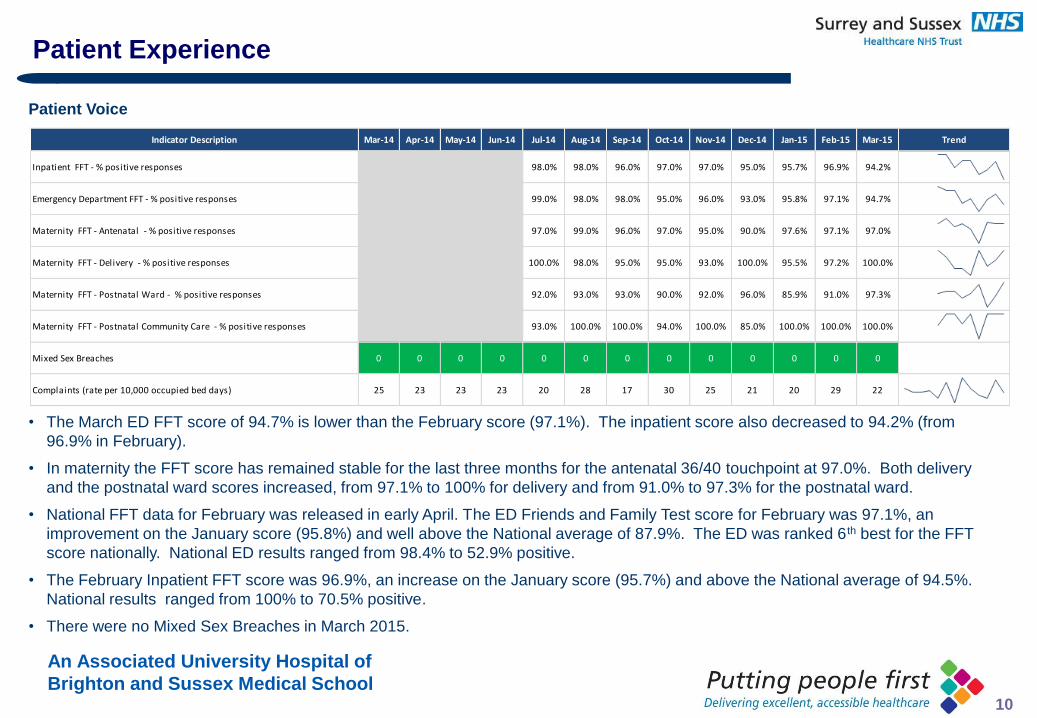
An Associated University Hospital of
Brighton and Sussex Medical School 10
Patient Voice
• The March ED FFT score of 94.7% is lower than the February score (97.1%). The inpatient score also decreased to 94.2% (from
96.9% in February).
• In maternity the FFT score has remained stable for the last three months for the antenatal 36/40 touchpoint at 97.0%. Both delivery
and the postnatal ward scores increased, from 97.1% to 100% for delivery and from 91.0% to 97.3% for the postnatal ward.
• National FFT data for February was released in early April. The ED Friends and Family Test score for February was 97.1%, an
improvement on the January score (95.8%) and well above the National average of 87.9%. The ED was ranked 6 th best for the FFT
score nationally. National ED results ranged from 98.4% to 52.9% positive.
• The February Inpatient FFT score was 96.9%, an increase on the January score (95.7%) and above the National average of 94.5%.
National results ranged from 100% to 70.5% positive.
• There were no Mixed Sex Breaches in March 2015.
Patient Experience
Indicator Description Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Trend
Inpatient FFT - % positive responses 98.0% 98.0% 96.0% 97.0% 97.0% 95.0% 95.7% 96.9% 94.2%
Emergency Department FFT - % positive responses 99.0% 98.0% 98.0% 95.0% 96.0% 93.0% 95.8% 97.1% 94.7%
Maternity FFT - Antenatal - % positive responses 97.0% 99.0% 96.0% 97.0% 95.0% 90.0% 97.6% 97.1% 97.0%
Maternity FFT - Delivery - % positive responses 100.0% 98.0% 95.0% 95.0% 93.0% 100.0% 95.5% 97.2% 100.0%
Maternity FFT - Postnatal Ward - % positive responses 92.0% 93.0% 93.0% 90.0% 92.0% 96.0% 85.9% 91.0% 97.3%
Maternity FFT - Postnatal Community Care - % positive responses 93.0% 100.0% 100.0% 94.0% 100.0% 85.0% 100.0% 100.0% 100.0%
Mixed Sex Breaches 0 0 0 0 0 0 0 0 0 0 0 0 0
Complaints (rate per 10,000 occupied bed days) 25 23 23 23 20 28 17 30 25 21 20 29 22
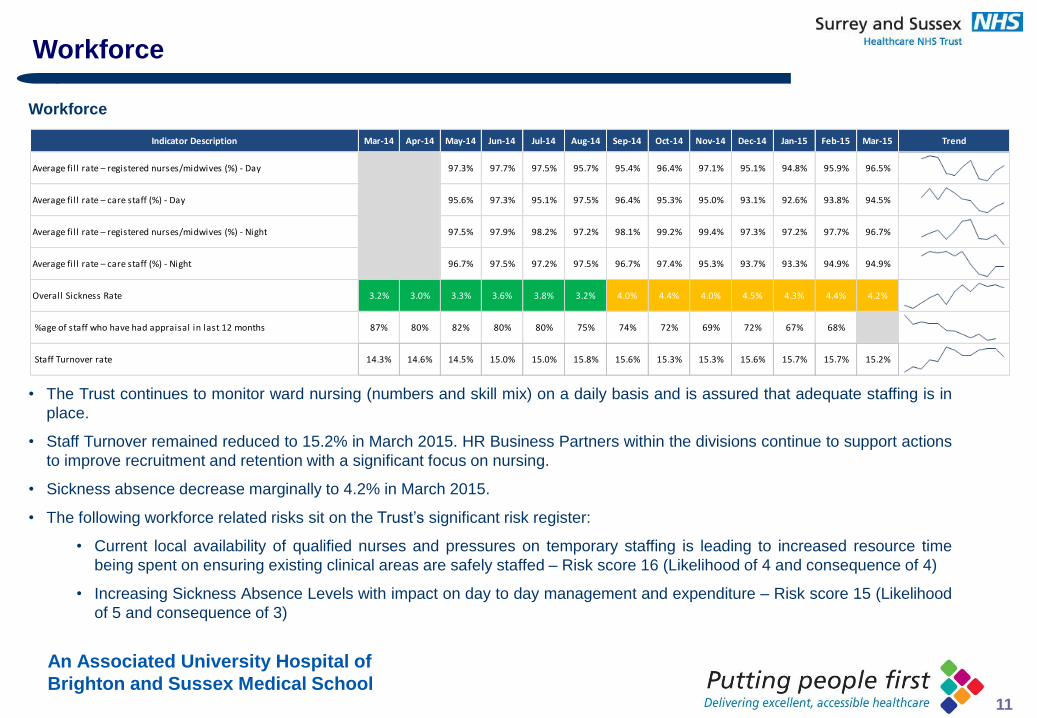
An Associated University Hospital of
Brighton and Sussex Medical School 11
Workforce
• The Trust continues to monitor ward nursing (numbers and skill mix) on a daily basis and is assured that adequate staffing is in
place.
• Staff Turnover remained reduced to 15.2% in March 2015. HR Business Partners within the divisions continue to support actions
to improve recruitment and retention with a significant focus on nursing.
• Sickness absence decrease marginally to 4.2% in March 2015.
• The following workforce related risks sit on the Trust’s significant risk register:
• Current local availability of qualified nurses and pressures on temporary staffing is leading to increased resource time
being spent on ensuring existing clinical areas are safely staffed – Risk score 16 (Likelihood of 4 and consequence of 4)
• Increasing Sickness Absence Levels with impact on day to day management and expenditure – Risk score 15 (Likelihood
of 5 and consequence of 3)
Workforce
Indicator Description Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Trend
Average fi l l rate – registered nurses/midwives (%) - Day 97.3% 97.7% 97.5% 95.7% 95.4% 96.4% 97.1% 95.1% 94.8% 95.9% 96.5%
Average fi l l rate – care staff (%) - Day 95.6% 97.3% 95.1% 97.5% 96.4% 95.3% 95.0% 93.1% 92.6% 93.8% 94.5%
Average fi l l rate – registered nurses/midwives (%) - Night 97.5% 97.9% 98.2% 97.2% 98.1% 99.2% 99.4% 97.3% 97.2% 97.7% 96.7%
Average fi l l rate – care staff (%) - Night 96.7% 97.5% 97.2% 97.5% 96.7% 97.4% 95.3% 93.7% 93.3% 94.9% 94.9%
Overall Sickness Rate 3.2% 3.0% 3.3% 3.6% 3.8% 3.2% 4.0% 4.4% 4.0% 4.5% 4.3% 4.4% 4.2%
%age of staff who have had appraisal in last 12 months 87% 80% 82% 80% 80% 75% 74% 72% 69% 72% 67% 68%
Staff Turnover rate 14.3% 14.6% 14.5% 15.0% 15.0% 15.8% 15.6% 15.3% 15.3% 15.6% 15.7% 15.7% 15.2%
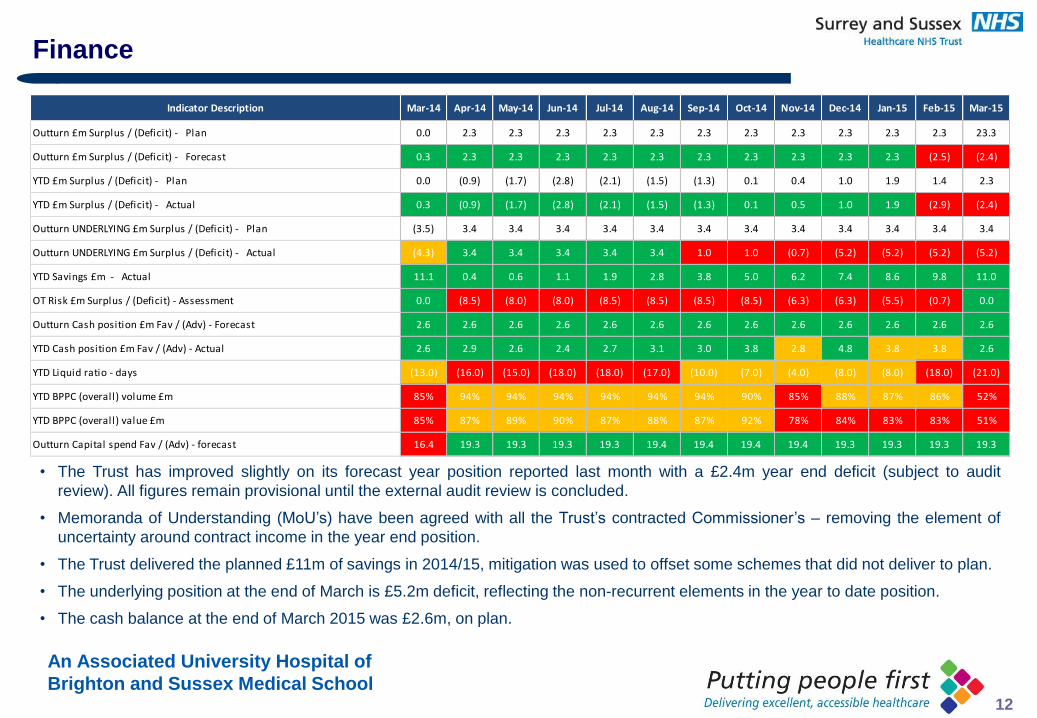
An Associated University Hospital of
Brighton and Sussex Medical School 12
Finance
• The Trust has improved slightly on its forecast year position reported last month with a £2.4m year end deficit (subject to audit
review). All figures remain provisional until the external audit review is concluded.
• Memoranda of Understanding (MoU’s) have been agreed with all the Trust’s contracted Commissioner’s – removing the element of
uncertainty around contract income in the year end position.
• The Trust delivered the planned £11m of savings in 2014/15, mitigation was used to offset some schemes that did not deliver to plan.
• The underlying position at the end of March is £5.2m deficit, reflecting the non-recurrent elements in the year to date position.
• The cash balance at the end of March 2015 was £2.6m, on plan.
Indicator Description Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Outturn £m Surplus / (Deficit) - Plan 0.0 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 23.3
Outturn £m Surplus / (Deficit) - Forecast 0.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 2.3 (2.5) (2.4)
YTD £m Surplus / (Deficit) - Plan 0.0 (0.9) (1.7) (2.8) (2.1) (1.5) (1.3) 0.1 0.4 1.0 1.9 1.4 2.3
YTD £m Surplus / (Deficit) - Actual 0.3 (0.9) (1.7) (2.8) (2.1) (1.5) (1.3) 0.1 0.5 1.0 1.9 (2.9) (2.4)
Outturn UNDERLYING £m Surplus / (Deficit) - Plan (3.5) 3.4 3.4 3.4 3.4 3.4 3.4 3.4 3.4 3.4 3.4 3.4 3.4
Outturn UNDERLYING £m Surplus / (Deficit) - Actual (4.3) 3.4 3.4 3.4 3.4 3.4 1.0 1.0 (0.7) (5.2) (5.2) (5.2) (5.2)
YTD Savings £m - Actual 11.1 0.4 0.6 1.1 1.9 2.8 3.8 5.0 6.2 7.4 8.6 9.8 11.0
OT Risk £m Surplus / (Deficit) - Assessment 0.0 (8.5) (8.0) (8.0) (8.5) (8.5) (8.5) (8.5) (6.3) (6.3) (5.5) (0.7) 0.0
Outturn Cash position £m Fav / (Adv) - Forecast 2.6 2.6 2.6 2.6 2.6 2.6 2.6 2.6 2.6 2.6 2.6 2.6 2.6
YTD Cash position £m Fav / (Adv) - Actual 2.6 2.9 2.6 2.4 2.7 3.1 3.0 3.8 2.8 4.8 3.8 3.8 2.6
YTD Liquid ratio - days (13.0) (16.0) (15.0) (18.0) (18.0) (17.0) (10.0) (7.0) (4.0) (8.0) (8.0) (18.0) (21.0)
YTD BPPC (overall) volume £m 85% 94% 94% 94% 94% 94% 94% 90% 85% 88% 87% 86% 52%
YTD BPPC (overall) value £m 85% 87% 89% 90% 87% 88% 87% 92% 78% 84% 83% 83% 51%
Outturn Capital spend Fav / (Adv) - forecast 16.4 19.3 19.3 19.3 19.3 19.4 19.4 19.4 19.4 19.3 19.3 19.3 19.3
An Associated University Hospital of
Brighton and Sussex Medical School 13
Finance
• The capital spend in 2014/15 was £19.3m, meeting the Capital Resource Limit.
• The Trust ends the year with M12 recording the 2nd highest number of ED attendances all year, a marginal rate emergency tariff
deduction of £7.2m and elective income £2.4m below plan. In month there is increased overspending in Divisions, most marked in
Medicine, and additional costs funded by the 3rd tranche of RTT resilience funding. Elective day cases, however, showed a marked
increase in month.
TRUST BOARD IN PUBLIC
Date:30 April 2015 Agenda Item: 3.3
REPORT TITLE: Charitable Funds Committee Chair Update
EXECUTIVE SPONSOR: Paul Simpson (Chief Finance Officer)
REPORT AUTHOR: Yvette Robbins (Non-Executive Director and Committee Chair)
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date) No – Board Update
Action Required:
Approval () Discussion () Assurance (√)
Summary of Key Issues
This report briefs the Board on the key issues discussed at the meeting of the committee on 5 March 2015.
Key points were:
Fund raising update;
Finance review including spending plans;
Review of Terms of Reference.
Savile Action Plan - Refresh
Relationship to Trust Strategic Objectives & Assurance Framework:
SO3: Caring – Ensure patients are cared for and feel cared about
Corporate Impact Assessment:
Legal and regulatory implications
The Charity is registered with the Charity Commission in accordance with the Charities Act 1993, registered number 1054072.
Charitable funds received by the Charity are accepted, held and administered as funds and property held on trust for purposes relating to the health service in accordance with the National Health Service Act 1977, the National Health Service and Community Care Act 1990, the National Health Service Act 2009. These funds are held on trust by the corporate body. The fund is audited by the Trust’s External Auditor (Grant Thornton UK LLP)
2An Associated University Hospital of Brighton and Sussex Medical School
Financial implications The report provides assurance about the financial management of the charitable fund.
Patient Experience/Engagement A deliberate positive impact from the use of the fund to support patient experience.
Risk & Performance Management
The committee, and this report, provides assurance about risk management relevant to the fund.
NHS Constitution/Equality & Diversity/Communication
Attachments:
Report paper
3An Associated University Hospital of Brighton and Sussex Medical School
Charitable Funds Committee Chair Update – 30th April 2015 Trust Board Report The Charitable Funds Committee met on 5 March.
Fund Raising
The Committee was advised that following Bernard Graham’s departure from the Trust in December 2014 there had not been a Fund Raising Co-ordinator in place; as an interim measure Katrina Swanston is currently fulfilling this post.
The SASH Charity was launched on 12 December 2014 and has secured in excess of 200 hits on the website, a presence on social media and is in progress with numerous partnerships; SASH Charity boxes are also in place throughout the hospital.
The individual wards are currently raising specific funds under their own banner and there are concerns regarding the legitimacy of this when £0.6m is held in individual small funds which is not being spent; a pooling of the funds will be considered once the legalities and practicalities of this is checked within the framework of The Charity Commission.
It was suggested that the staff were not always aware that there were funds available for expenditure and how to apply and therefore Communications will review how to make staff more aware of the existence of funds in their areas.
There was also concern regarding lack of clarity on the purpose of the fund raising and how the funds would be expended; it was agreed that this is a CFC decision; however it was open to review and additions of new themes & causes; going forward all subsequent fund raising will take place under the SASH Charity banner to ensure a single identity.
All new funds raised will go into a single fund although future individual donations made to specific wards or causes will remain unchanged and this will not contravene the rules around restricted and unrestricted funds where donors are specific about the use of their donations.
It was also agreed that the SASH Charity would continue to focus on Elderly care for 2015.
Finance, Policy & Savile Action Plan
The current fund balance totalled £0.6m, the Divisions are aware but the funds are not being expended; the expenditure plans from the individual fund holders are almost complete and the Committee agreed that unspent monies will be transferred to the general fund; however a balance approach and caution were advocated on the wording of the directive to avoid inappropriate expenditure.
The Committee was assured that there are systems in place regarding expenditure; finance check all expenditure requests against the individual “Purpose of the Fund” and furthermore spends over £2k are authorised by the Charitable Funds Committee (delegated authority to YR & PS).
It was agreed that where significant staff training costs are involved, in the event that the staff leave the Trust employment within 1 year costs are to be reimbursed to CFC, a policy will be drafted.
The Committee members were asked to review the Savile Action Plan Refresh report and raise any queries with the Chief Nurse.
Yvette Robbins Chair of Charitable Funds Committee 30 April 2015
[END]
TRUST BOARD IN PUBLIC
Date: 30 April 2015 Agenda Item: 4.1
REPORT TITLE: CQC Improvement Action Plan
EXECUTIVE SPONSOR: Sue Jenkins Director of Strategy
REPORT AUTHOR (s): Sue Jenkins Director of Strategy
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date) Executive Committee
Action Required:
Approval () Discussion () Assurance (√)
Purpose of Report:
This report provides the Board with assurance that the recommendations made following the CQC visit in May 2014 are being addressed.
Summary of key issues
The Chief Inspector of Hospitals visited the Trust in May 2014. The Trust was rated as “good” for all domains. In terms of the 8 core services that were reviewed the Trust received a “good” rating for all services apart from Outpatients services which were rated as “requires improvement”. This report includes a summary of the initial recommendations that were made in the report and how the Trust has responded to them. Progress against the detailed action plan that has previously been reported to the Board is also included. This report provides a summary of progress to date which confirm that all of the four main work streams are rated as green or blue. Progress against the “should do” recommendations from the CQC report will continue to be reported quarterly. The system wide updates following the quality summit are also included in this report for completeness.
Recommendation:
The Board is asked to consider this report and ensure that it provides assurance around delivery of the CQC improvement plan.
Relationship to Trust Strategic Objectives & Assurance Framework:
SO1: Safe -Deliver safe services and be in the top 20% against our peers SO2: Effective - Deliver effective and sustainable clinical services within the local health economy
2An Associated University Hospital of Brighton and Sussex Medical School
SO3: Caring – Ensure patients are cared for and feel cared about SO4: Responsive – Become the secondary care provider and employer of choice our catchment population SO5: Well led: Become an employer of choice and deliver financial and clinical sustainability around a clinical leadership model
Corporate Impact Assessment:
Legal and regulatory implications Compliance with CQC recommendations and delivery of action plan to address areas highlighted is essential
Financial implications Capital and revenue implications will be addressed through separate business cases
Patient Experience/Engagement Feedback from patients regarding their experience in outpatients is a key part of this action plan
Risk & Performance Management A monthly steering group is in place to ensure delivery of the plan
NHS Constitution/Equality & Diversity/Communication
N/A
Attachment:
CQC Improvement action plan – April 2015
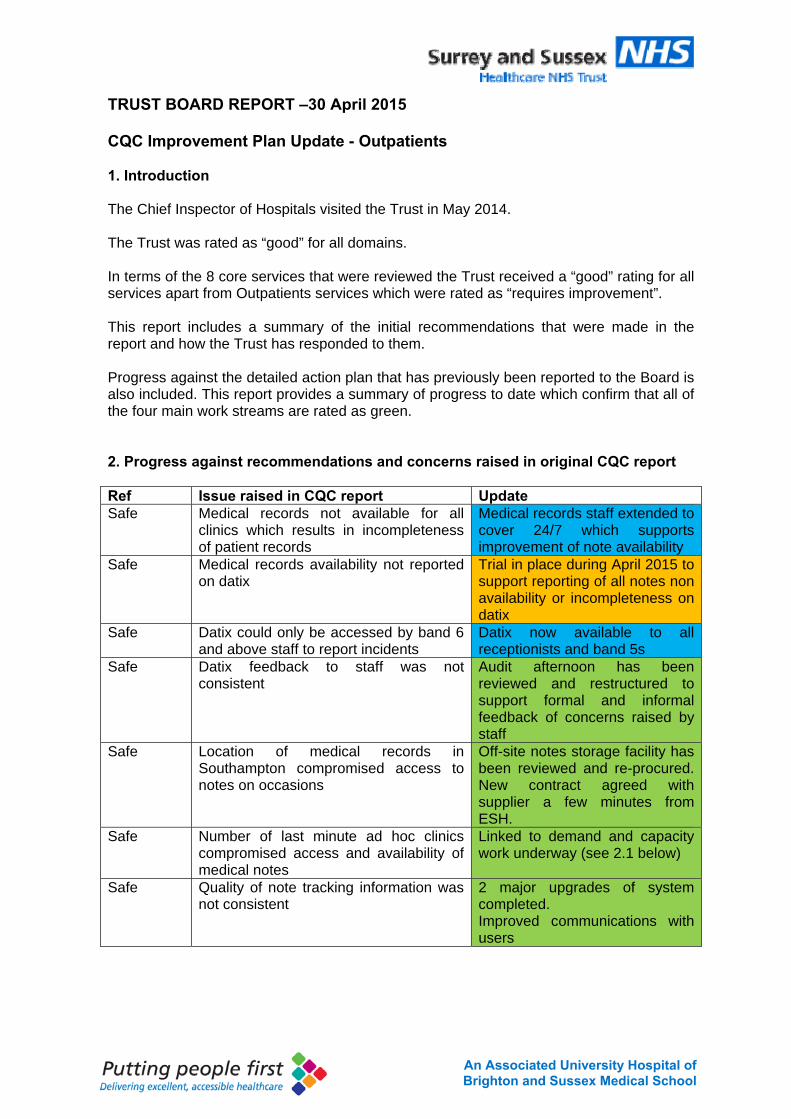
3An Associated University Hospital of Brighton and Sussex Medical School
TRUST BOARD REPORT –30 April 2015 CQC Improvement Plan Update - Outpatients 1. Introduction The Chief Inspector of Hospitals visited the Trust in May 2014. The Trust was rated as “good” for all domains. In terms of the 8 core services that were reviewed the Trust received a “good” rating for all services apart from Outpatients services which were rated as “requires improvement”. This report includes a summary of the initial recommendations that were made in the report and how the Trust has responded to them. Progress against the detailed action plan that has previously been reported to the Board is also included. This report provides a summary of progress to date which confirm that all of the four main work streams are rated as green. 2. Progress against recommendations and concerns raised in original CQC report Ref Issue raised in CQC report Update Safe Medical records not available for all
clinics which results in incompleteness of patient records
Medical records staff extended to cover 24/7 which supports improvement of note availability
Safe Medical records availability not reported on datix
Trial in place during April 2015 to support reporting of all notes non availability or incompleteness on datix
Safe Datix could only be accessed by band 6 and above staff to report incidents
Datix now available to all receptionists and band 5s
Safe Datix feedback to staff was not consistent
Audit afternoon has been reviewed and restructured to support formal and informal feedback of concerns raised by staff
Safe Location of medical records in Southampton compromised access to notes on occasions
Off-site notes storage facility has been reviewed and re-procured. New contract agreed with supplier a few minutes from ESH.
Safe Number of last minute ad hoc clinics compromised access and availability of medical notes
Linked to demand and capacity work underway (see 2.1 below)
Safe Quality of note tracking information was not consistent
2 major upgrades of system completed. Improved communications with users
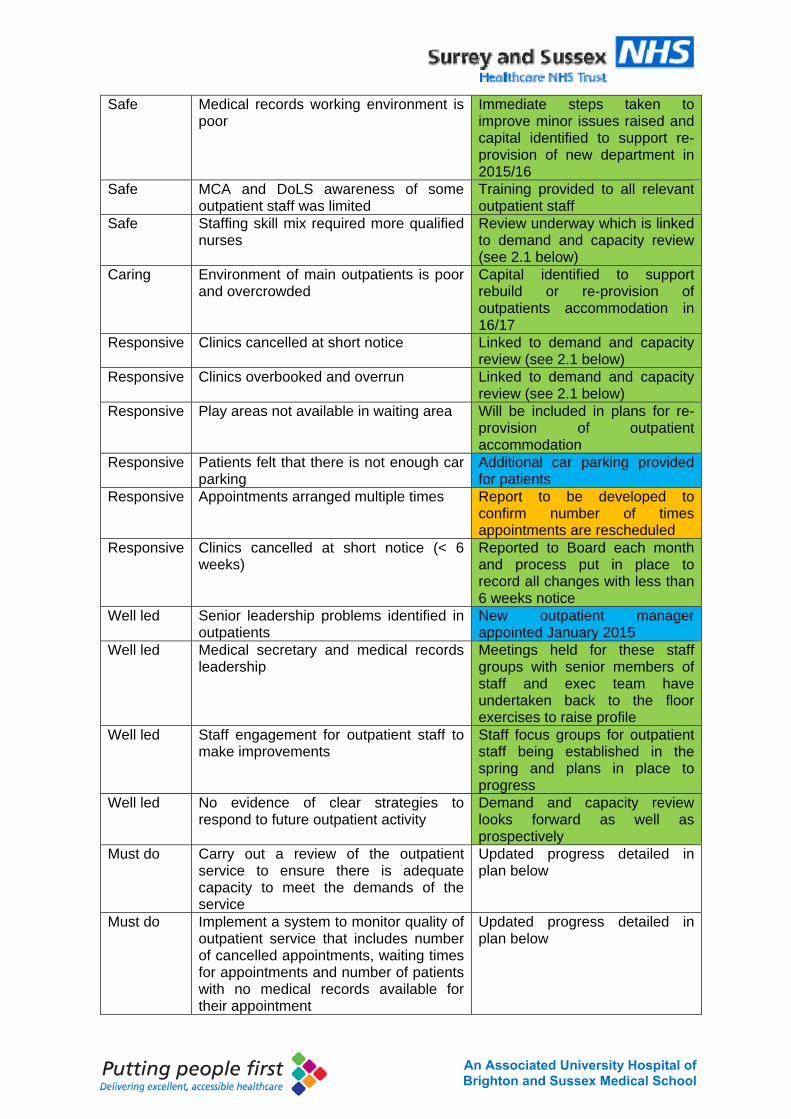
4An Associated University Hospital of Brighton and Sussex Medical School
Safe Medical records working environment is poor
Immediate steps taken to improve minor issues raised and capital identified to support re-provision of new department in 2015/16
Safe MCA and DoLS awareness of some outpatient staff was limited
Training provided to all relevant outpatient staff
Safe Staffing skill mix required more qualified nurses
Review underway which is linked to demand and capacity review (see 2.1 below)
Caring Environment of main outpatients is poor and overcrowded
Capital identified to support rebuild or re-provision of outpatients accommodation in 16/17
Responsive Clinics cancelled at short notice Linked to demand and capacity review (see 2.1 below)
Responsive Clinics overbooked and overrun Linked to demand and capacity review (see 2.1 below)
Responsive Play areas not available in waiting area Will be included in plans for re-provision of outpatient accommodation
Responsive Patients felt that there is not enough car parking
Additional car parking provided for patients
Responsive Appointments arranged multiple times Report to be developed to confirm number of times appointments are rescheduled
Responsive Clinics cancelled at short notice (< 6 weeks)
Reported to Board each month and process put in place to record all changes with less than 6 weeks notice
Well led Senior leadership problems identified in outpatients
New outpatient manager appointed January 2015
Well led Medical secretary and medical records leadership
Meetings held for these staff groups with senior members of staff and exec team have undertaken back to the floor exercises to raise profile
Well led Staff engagement for outpatient staff to make improvements
Staff focus groups for outpatient staff being established in the spring and plans in place to progress
Well led No evidence of clear strategies to respond to future outpatient activity
Demand and capacity review looks forward as well as prospectively
Must do Carry out a review of the outpatient service to ensure there is adequate capacity to meet the demands of the service
Updated progress detailed in plan below
Must do Implement a system to monitor quality of outpatient service that includes number of cancelled appointments, waiting times for appointments and number of patients with no medical records available for their appointment
Updated progress detailed in plan below
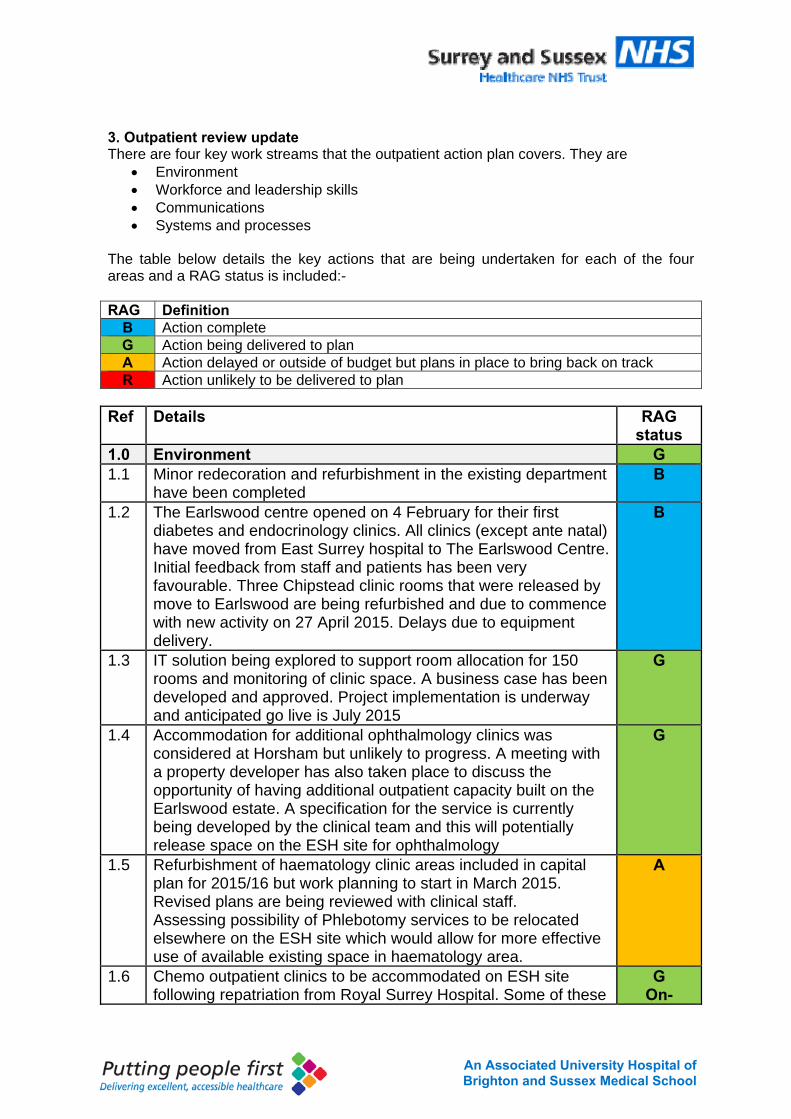
5An Associated University Hospital of Brighton and Sussex Medical School
3. Outpatient review update There are four key work streams that the outpatient action plan covers. They are
Environment Workforce and leadership skills Communications Systems and processes
The table below details the key actions that are being undertaken for each of the four areas and a RAG status is included:- RAG Definition
B Action complete G Action being delivered to plan A Action delayed or outside of budget but plans in place to bring back on track R Action unlikely to be delivered to plan
Ref Details RAG
status 1.0 Environment G 1.1 Minor redecoration and refurbishment in the existing department
have been completed B
1.2 The Earlswood centre opened on 4 February for their first diabetes and endocrinology clinics. All clinics (except ante natal) have moved from East Surrey hospital to The Earlswood Centre. Initial feedback from staff and patients has been very favourable. Three Chipstead clinic rooms that were released by move to Earlswood are being refurbished and due to commence with new activity on 27 April 2015. Delays due to equipment delivery.
B
1.3 IT solution being explored to support room allocation for 150 rooms and monitoring of clinic space. A business case has been developed and approved. Project implementation is underway and anticipated go live is July 2015
G
1.4 Accommodation for additional ophthalmology clinics was considered at Horsham but unlikely to progress. A meeting with a property developer has also taken place to discuss the opportunity of having additional outpatient capacity built on the Earlswood estate. A specification for the service is currently being developed by the clinical team and this will potentially release space on the ESH site for ophthalmology
G
1.5 Refurbishment of haematology clinic areas included in capital plan for 2015/16 but work planning to start in March 2015. Revised plans are being reviewed with clinical staff. Assessing possibility of Phlebotomy services to be relocated elsewhere on the ESH site which would allow for more effective use of available existing space in haematology area.
A
1.6 Chemo outpatient clinics to be accommodated on ESH site following repatriation from Royal Surrey Hospital. Some of these
G On-
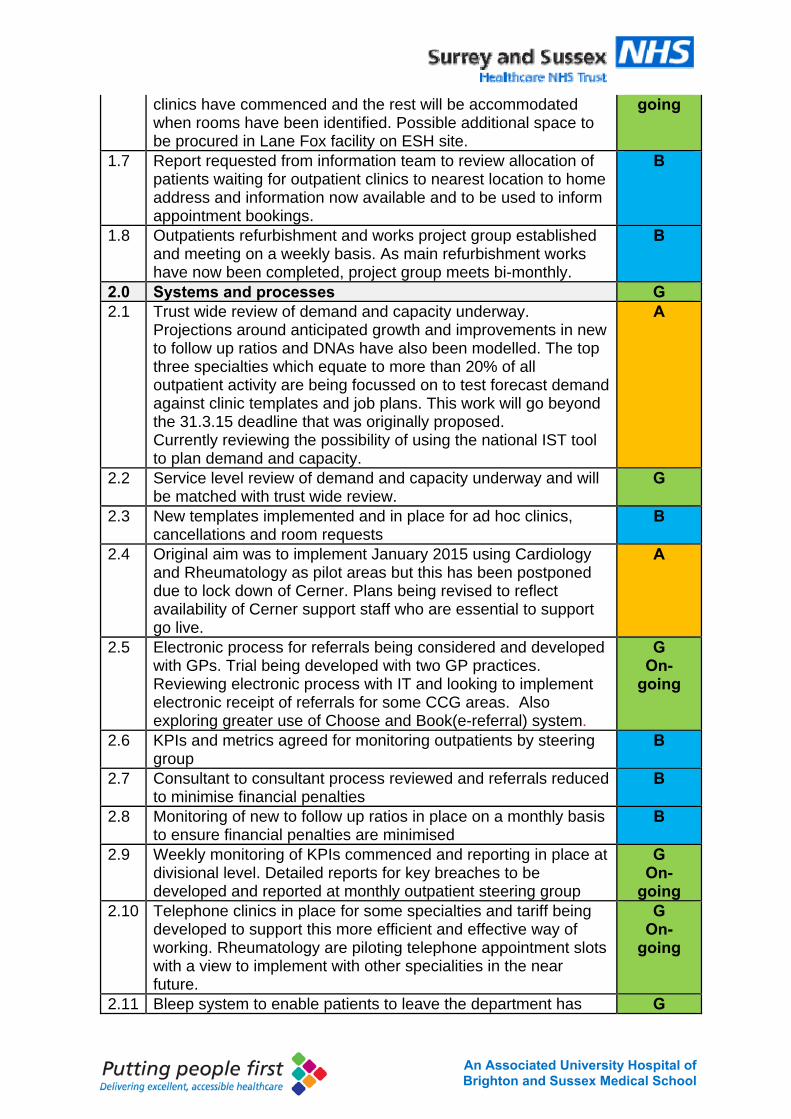
6An Associated University Hospital of Brighton and Sussex Medical School
clinics have commenced and the rest will be accommodated when rooms have been identified. Possible additional space to be procured in Lane Fox facility on ESH site.
going
1.7 Report requested from information team to review allocation of patients waiting for outpatient clinics to nearest location to home address and information now available and to be used to inform appointment bookings.
B
1.8 Outpatients refurbishment and works project group established and meeting on a weekly basis. As main refurbishment works have now been completed, project group meets bi-monthly.
B
2.0 Systems and processes G 2.1 Trust wide review of demand and capacity underway.
Projections around anticipated growth and improvements in new to follow up ratios and DNAs have also been modelled. The top three specialties which equate to more than 20% of all outpatient activity are being focussed on to test forecast demand against clinic templates and job plans. This work will go beyond the 31.3.15 deadline that was originally proposed. Currently reviewing the possibility of using the national IST tool to plan demand and capacity.
A
2.2 Service level review of demand and capacity underway and will be matched with trust wide review.
G
2.3 New templates implemented and in place for ad hoc clinics, cancellations and room requests
B
2.4 Original aim was to implement January 2015 using Cardiology and Rheumatology as pilot areas but this has been postponed due to lock down of Cerner. Plans being revised to reflect availability of Cerner support staff who are essential to support go live.
A
2.5 Electronic process for referrals being considered and developed with GPs. Trial being developed with two GP practices. Reviewing electronic process with IT and looking to implement electronic receipt of referrals for some CCG areas. Also exploring greater use of Choose and Book(e-referral) system.
G On-
going
2.6 KPIs and metrics agreed for monitoring outpatients by steering group
B
2.7 Consultant to consultant process reviewed and referrals reduced to minimise financial penalties
B
2.8 Monitoring of new to follow up ratios in place on a monthly basis to ensure financial penalties are minimised
B
2.9 Weekly monitoring of KPIs commenced and reporting in place at divisional level. Detailed reports for key breaches to be developed and reported at monthly outpatient steering group
G On-
going 2.10 Telephone clinics in place for some specialties and tariff being
developed to support this more efficient and effective way of working. Rheumatology are piloting telephone appointment slots with a view to implement with other specialities in the near future.
G On-
going
2.11 Bleep system to enable patients to leave the department has G
7An Associated University Hospital of Brighton and Sussex Medical School
been explored with other trusts who have system in place. Not considered viable as patients too concerned that they will lose their appointment slot. Self-check kiosk option being considered as an alternative and pilot being explored with potential supplier and a case to support the trial was considered and supported by CHIG in January 2015. Proof of concept being developed for go live in August. Capital confirmed
2.12 Outpatient booking office call answering currently at 98%. G On-
going 3.0 Workforce and leadership B 3.1 Interviews for Outpatient Service Manager completed and offer
made to strong candidate who commenced at beginning of January 2015. Interim management arrangements in place.
B
3.2 Skill mix review of outpatient services continually underway and reviewed each time vacancies arise.
B
3.3 Single line management of all outpatient staff considered and agreed not to progress at this point
B
3.4 Outpatient steering group and weekly operational groups all in place
B
3.5 Back to the floor session by Director of Strategy undertaken in outpatients department
B
3.6 Programme to extend skills of nurses being developed and to be worked up in more detail following appointment of new service manager
G On-
going 4.0 Communications G 4.1 Lead clinician and members of outpatient team have met with a
number of GP practices and CCG governance committee to consider views on referrals from GP perspective. This is key to improve working relationships between the Trust and primary care.
G On-
going
4.2 Lead clinician meeting with clinicians on a 121 basis to gain views and feedback on outpatient services
G On-
going 4.3 Outpatient services to be included on agenda item for all
consultants meeting – Mid September B
4.4 Outpatient nurse lead to meet with patient experience forum G On-
going 4.5 Outpatient focus group for patients planned for 2 December and
157 members interested in outpatients have been invited. Focus groups completed with 14 participants and feedback has informed an action plan which is monitored by monthly outpatient steering group.
B
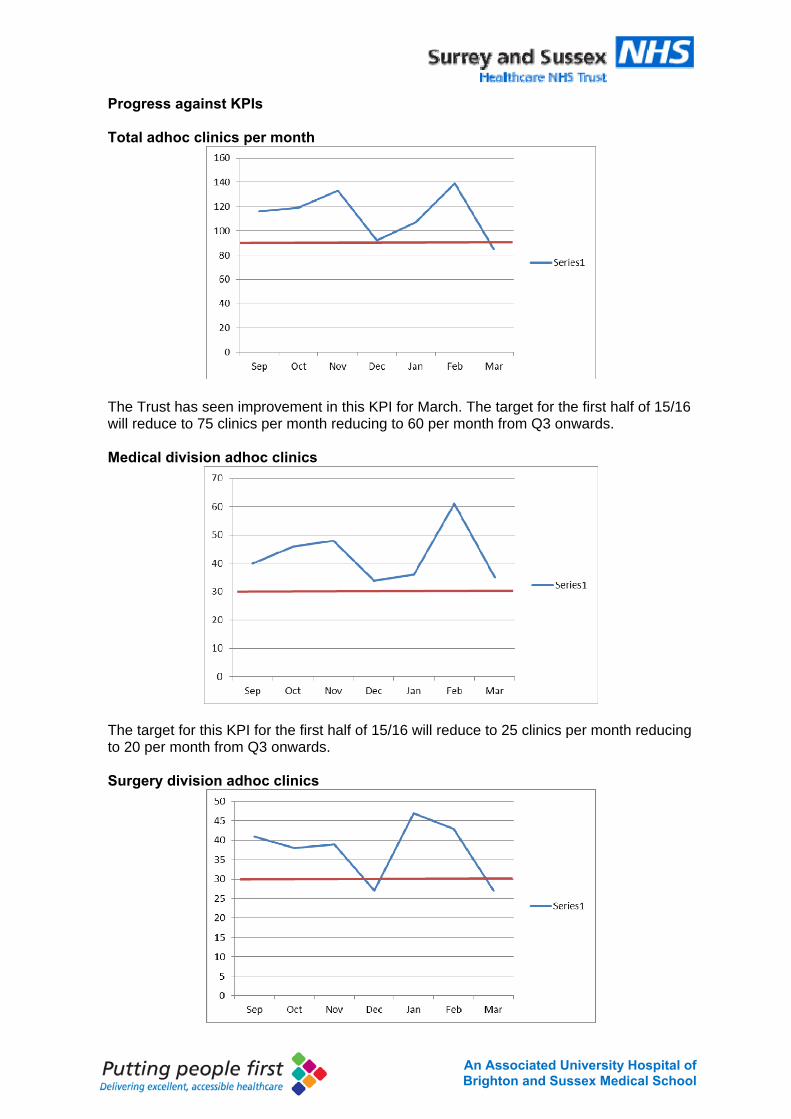
8An Associated University Hospital of Brighton and Sussex Medical School
Progress against KPIs Total adhoc clinics per month
The Trust has seen improvement in this KPI for March. The target for the first half of 15/16 will reduce to 75 clinics per month reducing to 60 per month from Q3 onwards. Medical division adhoc clinics
The target for this KPI for the first half of 15/16 will reduce to 25 clinics per month reducing to 20 per month from Q3 onwards. Surgery division adhoc clinics
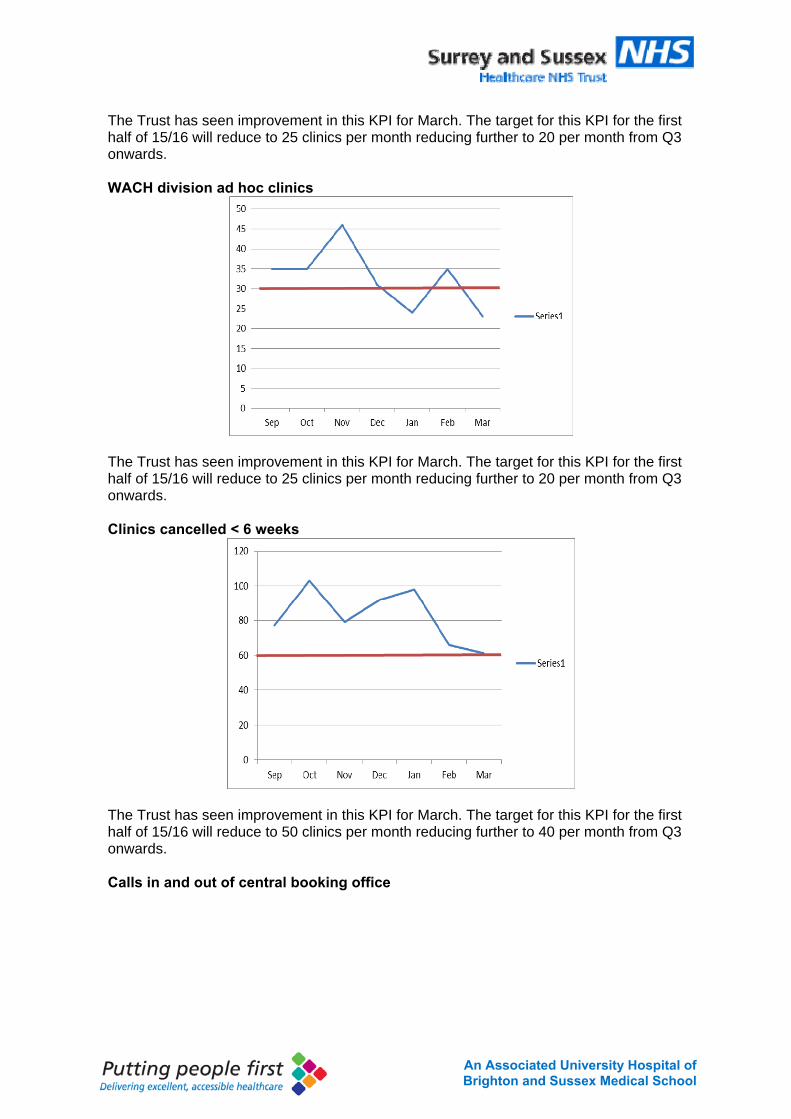
9An Associated University Hospital of Brighton and Sussex Medical School
The Trust has seen improvement in this KPI for March. The target for this KPI for the first half of 15/16 will reduce to 25 clinics per month reducing further to 20 per month from Q3 onwards. WACH division ad hoc clinics
The Trust has seen improvement in this KPI for March. The target for this KPI for the first half of 15/16 will reduce to 25 clinics per month reducing further to 20 per month from Q3 onwards. Clinics cancelled < 6 weeks
The Trust has seen improvement in this KPI for March. The target for this KPI for the first half of 15/16 will reduce to 50 clinics per month reducing further to 40 per month from Q3 onwards. Calls in and out of central booking office
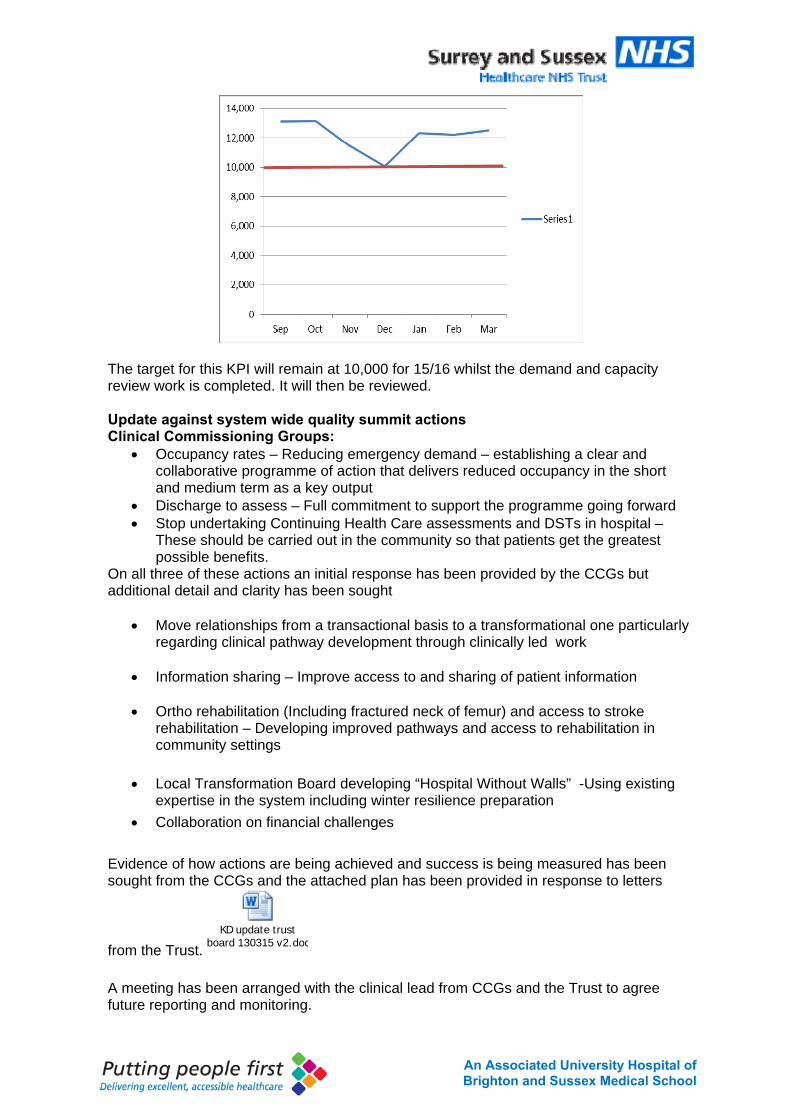
10An Associated University Hospital of Brighton and Sussex Medical School
The target for this KPI will remain at 10,000 for 15/16 whilst the demand and capacity review work is completed. It will then be reviewed. Update against system wide quality summit actions Clinical Commissioning Groups:
Occupancy rates – Reducing emergency demand – establishing a clear and collaborative programme of action that delivers reduced occupancy in the short and medium term as a key output
Discharge to assess – Full commitment to support the programme going forward Stop undertaking Continuing Health Care assessments and DSTs in hospital –
These should be carried out in the community so that patients get the greatest possible benefits.
On all three of these actions an initial response has been provided by the CCGs but additional detail and clarity has been sought
Move relationships from a transactional basis to a transformational one particularly regarding clinical pathway development through clinically led work
Information sharing – Improve access to and sharing of patient information
Ortho rehabilitation (Including fractured neck of femur) and access to stroke
rehabilitation – Developing improved pathways and access to rehabilitation in community settings
Local Transformation Board developing “Hospital Without Walls” -Using existing
expertise in the system including winter resilience preparation Collaboration on financial challenges
Evidence of how actions are being achieved and success is being measured has been sought from the CCGs and the attached plan has been provided in response to letters
from the Trust. KD update trust
board 130315 v2.doc A meeting has been arranged with the clinical lead from CCGs and the Trust to agree future reporting and monitoring.
11An Associated University Hospital of Brighton and Sussex Medical School
Healthwatch
Continue to be a critical friend Encourage Surrey & Sussex to share templates and paperwork (e.g. Continuing
Health Care Assessments) Our Chief Nurse and Deputy Chief Nurse have met with Healthwatch members from both West Sussex and Surrey and have agreed to meet them together on a quarterly basis to discuss soft intelligence they have received about the Trust. They have also agreed to consider how representatives from Healthwatch can contribute to relevant work stream within the organisation to increase the patient voice. In addition the Trust has agreed to promote the face of Healthwatch within the organisation to facilitate better knowledge and understanding by patients. Healthwatch were also updated on the recent PLACE visits. General Medical Council
Share lessons from the Surrey & Sussex Healthcare NHS Trust locally and nationally
The GMC public relevant reports on their website sharing findings and best practice on a national basis Health Overview & Scrutiny Committee
Continue to bring organisations together and provide challenge Encourage proactive work with CCGs, GPs & healthcare providers to find solutions
for appropriate use of healthcare services Provide a means of promoting the users and the public to use health services
appropriately Provide an opportunity for planning and dialogue with health and social care on demographic changes and access to health services for children and young people
The Trust has had recent experience of the West Sussex HASC calling all providers to account for how services had been delivered across the winter months. They have been instrumental in facilitating the agreement of plans which have included a commitment to increasing the social service support being provided on the hospital site Recommendation The Board is asked to consider this report and ensure that it provides assurance around delivery of the CQC improvement plan. Sue Jenkins Director of Strategy April 2015
TRUST BOARD IN PUBLIC
Date: 30th April 2015 Agenda Item: 4.2
REPORT TITLE: Serious Incident Report
EXECUTIVE SPONSOR: Fiona Allsop Chief Nurse
REPORT AUTHOR (s): Katharine Horner Patient Safety & Risk Lead Rado Dobransky Datix Administrator
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date) n/a
Action Required:
Approval () Discussion () Assurance ()
Purpose of Report: To provide an update on the position of the Trust with regard to serious incidents. Summary of key issues This paper provides the Board with a report on the serious incidents declared in quarter 3 and an update on progress with known safety themes arising from serious incidents.
Recommendation:
The Trust Board are asked to discuss the report and take assurance regarding the management of SIs and the on-going work to improve Trust Wide sharing of lessons learned and actions resulting from completed SI investigations.
Relationship to Trust Strategic Objectives & Assurance Framework:
SO1: Safe -Deliver safe services and be in the top 20% against our peers SO2: Effective - Deliver effective and sustainable clinical services within the local health economy SO3: Caring – Ensure patients are cared for and feel cared about Corporate Impact Assessment:
Legal and regulatory impact Compliance with CQC, MHRA and Audit Commission
Financial impact Serious incidents often become claims
Patient Experience/Engagement Included in the report
Risk & Performance Management Reporting, investigation and learning from serious incidents informs risk management
NHS Constitution/Equality & Diversity/Communication N/A
Attachment: N/A
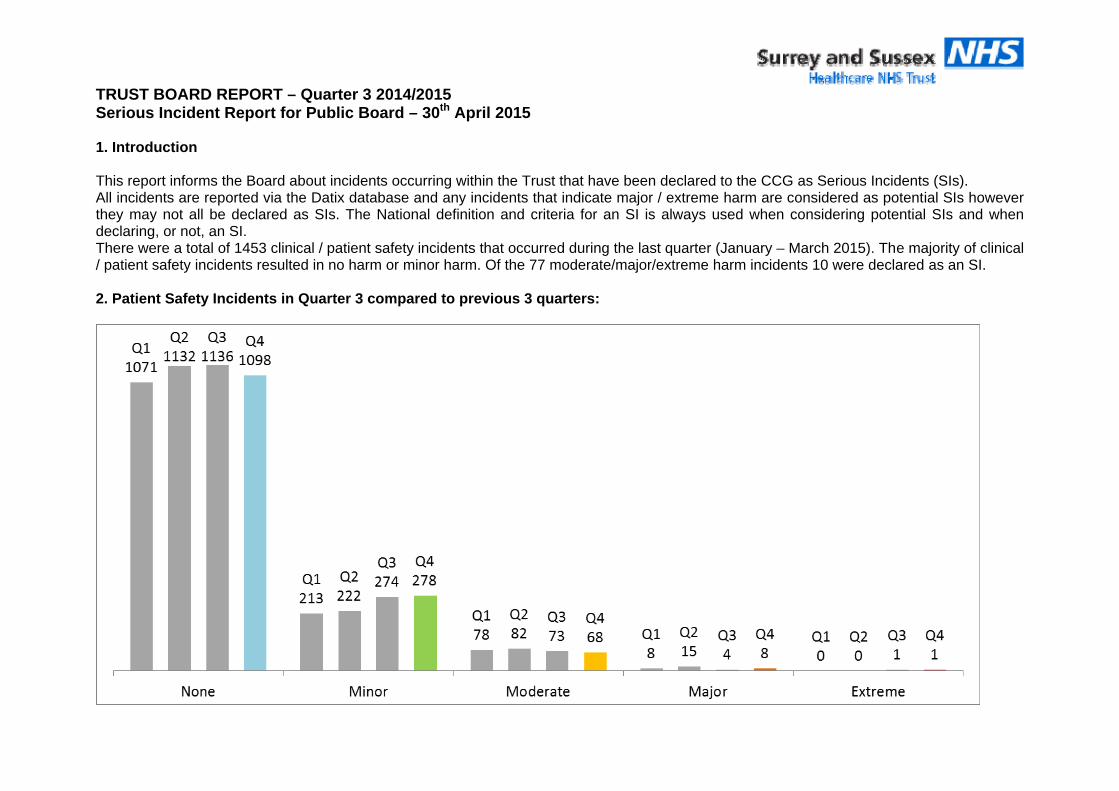
TRUST BOARD REPORT – Quarter 3 2014/2015 Serious Incident Report for Public Board – 30th April 2015 1. Introduction This report informs the Board about incidents occurring within the Trust that have been declared to the CCG as Serious Incidents (SIs). All incidents are reported via the Datix database and any incidents that indicate major / extreme harm are considered as potential SIs however they may not all be declared as SIs. The National definition and criteria for an SI is always used when considering potential SIs and when declaring, or not, an SI. There were a total of 1453 clinical / patient safety incidents that occurred during the last quarter (January – March 2015). The majority of clinical / patient safety incidents resulted in no harm or minor harm. Of the 77 moderate/major/extreme harm incidents 10 were declared as an SI. 2. Patient Safety Incidents in Quarter 3 compared to previous 3 quarters:
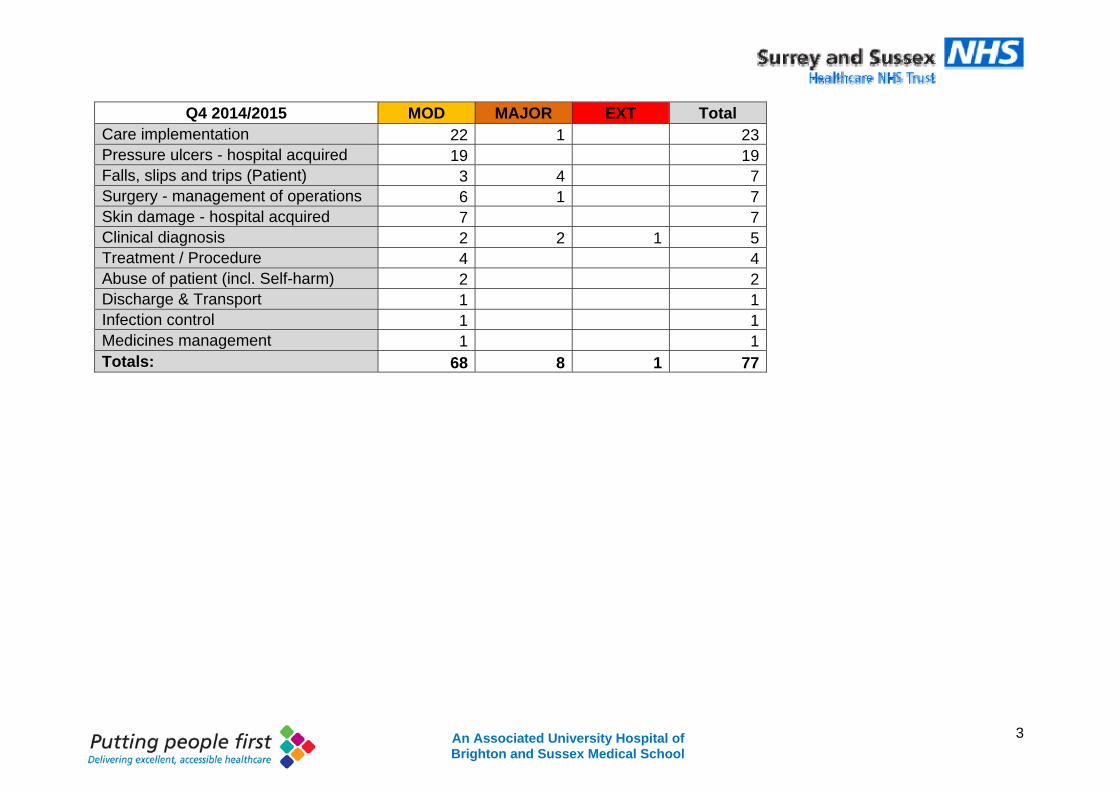
3 An Associated University Hospital of Brighton and Sussex Medical School
Q4 2014/2015 MOD MAJOR EXT Total
Care implementation 22 1 23Pressure ulcers - hospital acquired 19 19Falls, slips and trips (Patient) 3 4 7Surgery - management of operations 6 1 7Skin damage - hospital acquired 7 7Clinical diagnosis 2 2 1 5Treatment / Procedure 4 4Abuse of patient (incl. Self-harm) 2 2Discharge & Transport 1 1Infection control 1 1Medicines management 1 1Totals: 68 8 1 77
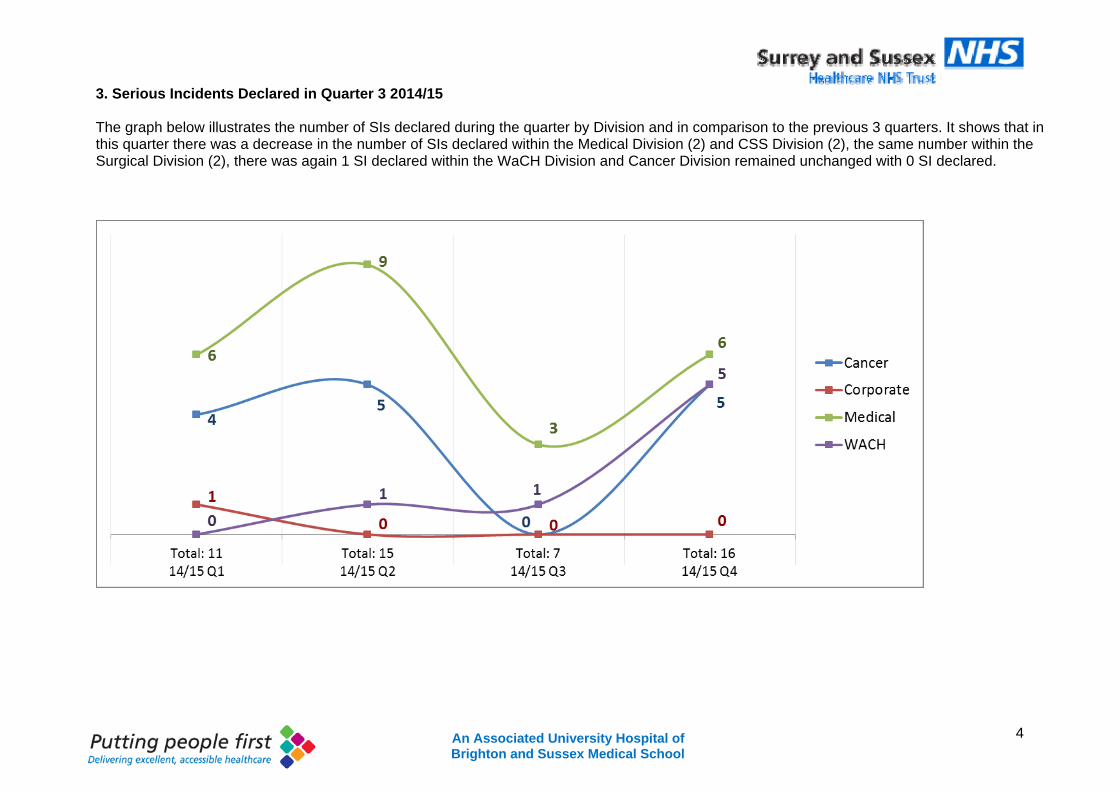
4 An Associated University Hospital of Brighton and Sussex Medical School
3. Serious Incidents Declared in Quarter 3 2014/15 The graph below illustrates the number of SIs declared during the quarter by Division and in comparison to the previous 3 quarters. It shows that in this quarter there was a decrease in the number of SIs declared within the Medical Division (2) and CSS Division (2), the same number within the Surgical Division (2), there was again 1 SI declared within the WaCH Division and Cancer Division remained unchanged with 0 SI declared.
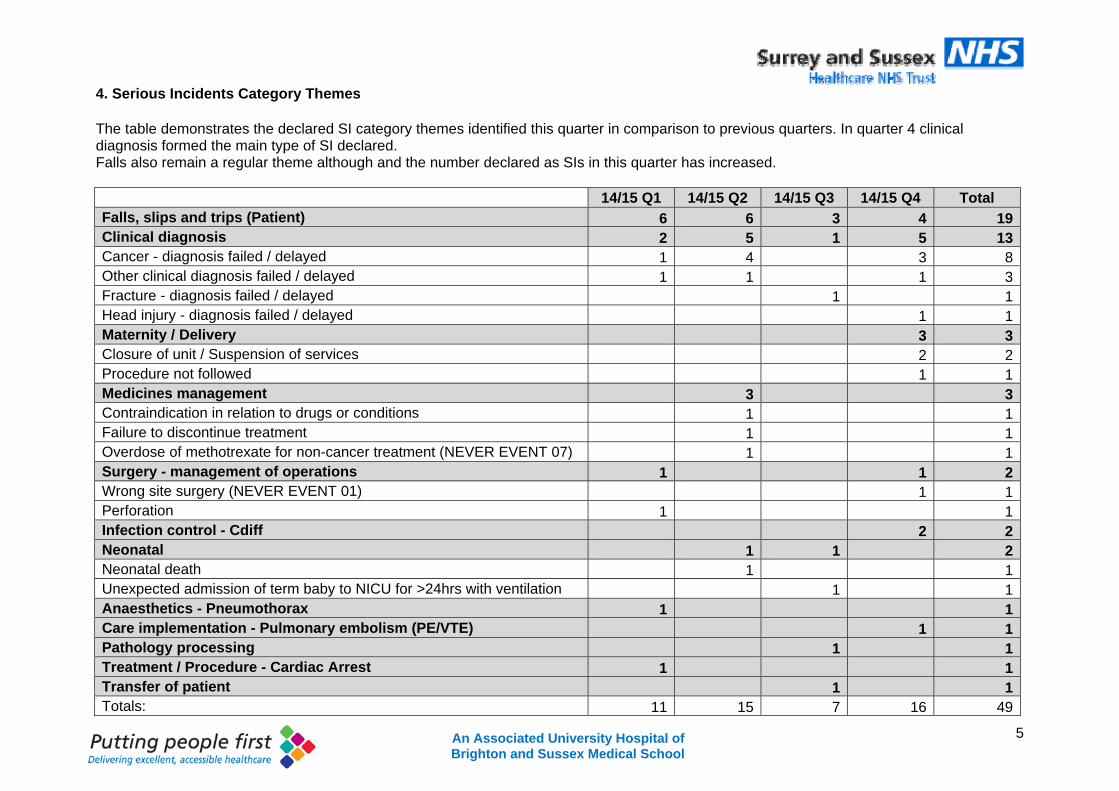
5 An Associated University Hospital of Brighton and Sussex Medical School
4. Serious Incidents Category Themes The table demonstrates the declared SI category themes identified this quarter in comparison to previous quarters. In quarter 4 clinical diagnosis formed the main type of SI declared. Falls also remain a regular theme although and the number declared as SIs in this quarter has increased. 14/15 Q1 14/15 Q2 14/15 Q3 14/15 Q4 Total Falls, slips and trips (Patient) 6 6 3 4 19 Clinical diagnosis 2 5 1 5 13 Cancer - diagnosis failed / delayed 1 4 3 8 Other clinical diagnosis failed / delayed 1 1 1 3 Fracture - diagnosis failed / delayed 1 1 Head injury - diagnosis failed / delayed 1 1 Maternity / Delivery 3 3 Closure of unit / Suspension of services 2 2 Procedure not followed 1 1 Medicines management 3 3 Contraindication in relation to drugs or conditions 1 1 Failure to discontinue treatment 1 1 Overdose of methotrexate for non-cancer treatment (NEVER EVENT 07) 1 1 Surgery - management of operations 1 1 2 Wrong site surgery (NEVER EVENT 01) 1 1 Perforation 1 1 Infection control - Cdiff 2 2 Neonatal 1 1 2 Neonatal death 1 1 Unexpected admission of term baby to NICU for >24hrs with ventilation 1 1 Anaesthetics - Pneumothorax 1 1 Care implementation - Pulmonary embolism (PE/VTE) 1 1 Pathology processing 1 1 Treatment / Procedure - Cardiac Arrest 1 1 Transfer of patient 1 1 Totals: 11 15 7 16 49
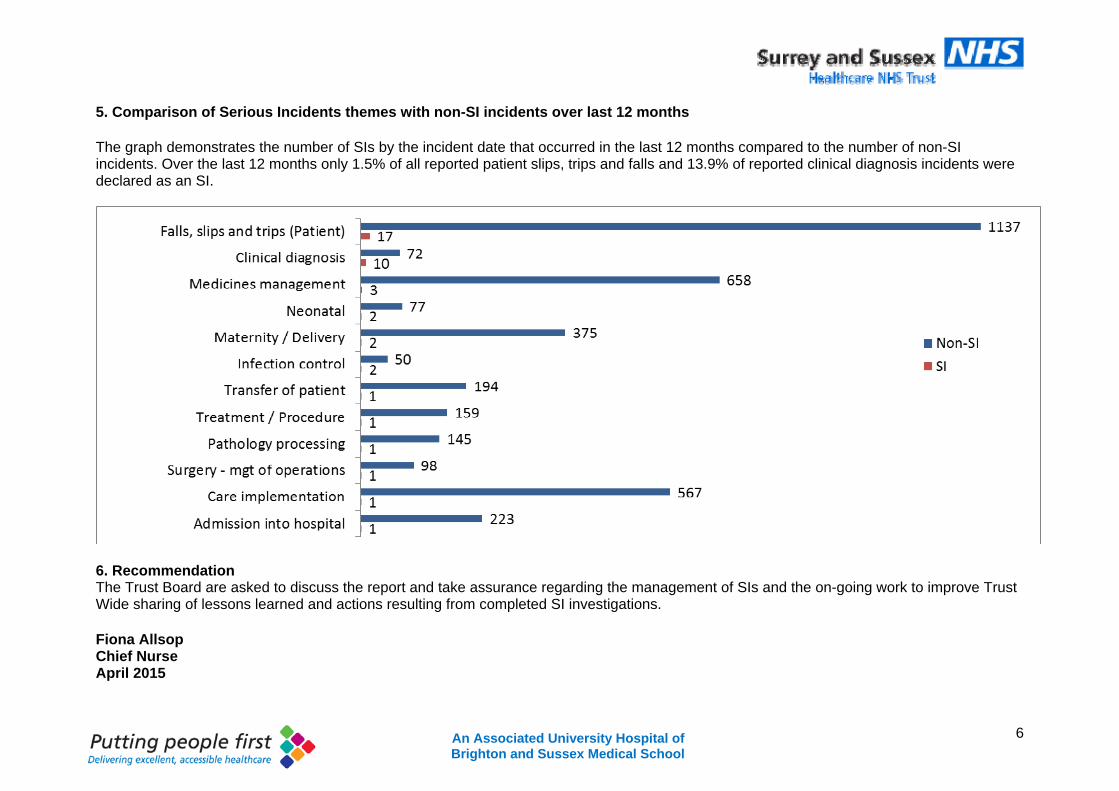
6 An Associated University Hospital of Brighton and Sussex Medical School
5. Comparison of Serious Incidents themes with non-SI incidents over last 12 months The graph demonstrates the number of SIs by the incident date that occurred in the last 12 months compared to the number of non-SI incidents. Over the last 12 months only 1.5% of all reported patient slips, trips and falls and 13.9% of reported clinical diagnosis incidents were declared as an SI.
6. Recommendation The Trust Board are asked to discuss the report and take assurance regarding the management of SIs and the on-going work to improve Trust Wide sharing of lessons learned and actions resulting from completed SI investigations. Fiona Allsop Chief Nurse April 2015
1An Associated University Hospital of Brighton and Sussex Medical School
TRUST BOARD IN PUBLIC
Date: 30th April 2015 Agenda Item: 4.3
REPORT TITLE: Annual Board and Sub-Committee Attendance for 2014/15
EXECUTIVE SPONSOR: Gillian Francis-Musanu Director of Corporate Affairs
REPORT AUTHOR (s): Gillian Francis-Musanu Director of Corporate Affairs
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date)
N/A
Action Required:
Approval () Discussion (√) Assurance (√)
Purpose of Report:
As part of the requirements for the Board Governance Assurance Framework and a mark of good governance this report gives an overview of attendance at all Board and Board sub-committee meetings for the past 12 months.
Summary of key issues
Analysis of records shows a range of 100% as the highest with 36% (due to clinical commitment) as the lowest overall rate of annual attendance.
Recommendation:
The Board is asked to note the analysis of annual attendance at the Board and sub-committees for April 2014 – March 2015.
Relationship to Trust Strategic Objectives & Assurance Framework:
SO5: Well led: Become an employer of choice and deliver financial and clinical sustainability around a clinical leadership model
Corporate Impact Assessment:
Legal and regulatory impact Best practice governance standards.
Financial impact N/A
Patient Experience/Engagement N/A
Risk & Performance Management Governance standards for high performing organisations.
NHS Constitution/Equality & Diversity/Communication
N/A
Attachment:
Appendix 1 – 6 Analysis of Board and sub-committee attendance
2An Associated University Hospital of Brighton and Sussex Medical School
TRUST BOARD REPORT – 30th April 2015 ANNUAL REVIEW OF BOARD AND SUB-COMMITTEE ATTENDANCE 1. Introduction 1.1 This report provides the Board with an annual review of attendance at Trust Board
and its Sub-Committee meetings during the last 12 months. Good meeting attendance gives the Board assurance that there is consistency and integrity of the work of its committees.
1.2 Regular meeting attendance is considered a hallmark of the conscientious director and is an important and essential element of good governance. Members who do not attend a high proportion of meetings can disrupt the flow of governance and the continuity of teamwork on the board and its sub-committees.
1.3 One of the most powerful practices for Board members is to evaluate the quality of their Board operations. This can be done in a variety of ways for example, at the end of each meeting or on a quarterly basis. At a minimum Boards are required to undertake an annual review of its performance.
1.4 As part of the Board Development programme and the Board Governance Framework (BGAF) the Board has undertaken a process of self assessment of its effectiveness in a number of key areas and has taken action to address those areas deemed to require improvement and development.
Board composition and commitment Board evaluation, development and learning Board insight and foresight Board engagement and involvement The impact of the Board using case studies
1.5 As part of the requirement for evaluation, development and learning, this report gives an overview of attendance at all Board and sub-committee meetings for the past 12 months.
2.0 Analysis of Committee Attendance
2.1 Appendices one to six list the meetings of the Board and its sub-committees and the attendance of members from April 2014 to March 2015.
Trust Board Safety and Quality Committee Audit and Assurance Committee Finance and Workforce Committee Charitable Funds Committee Nominations & Remuneration Committee
2.2 Attendance throughout the year has been recorded by the committee administrator and relates to membership of that committee as determined by the terms of reference. Each member has attracted a mean attendance score for annual attendance.
3An Associated University Hospital of Brighton and Sussex Medical School
2.3 Overall the scores range from 100% as the highest attendance to 36% (due to clinical commitments) as the lowest attendance. Due notice has been taken of members who have left the organisation and those who have been appointed within the last 12 months. It should be noted that in the majority of instances a deputy would have represented an executive director or clinical chief in their absence.
2.4 It is widely recognised in best practice guidance on good governance that overall annual attendance for individuals at meetings should be in the region of 80% – 100%.
3. Recommendation
3.1 The Board is asked to note the analysis of annual attendance at the Board and sub-committees for April 2014 – March 2015.
Gillian Francis-Musanu Director of Corporate Affairs April 2015
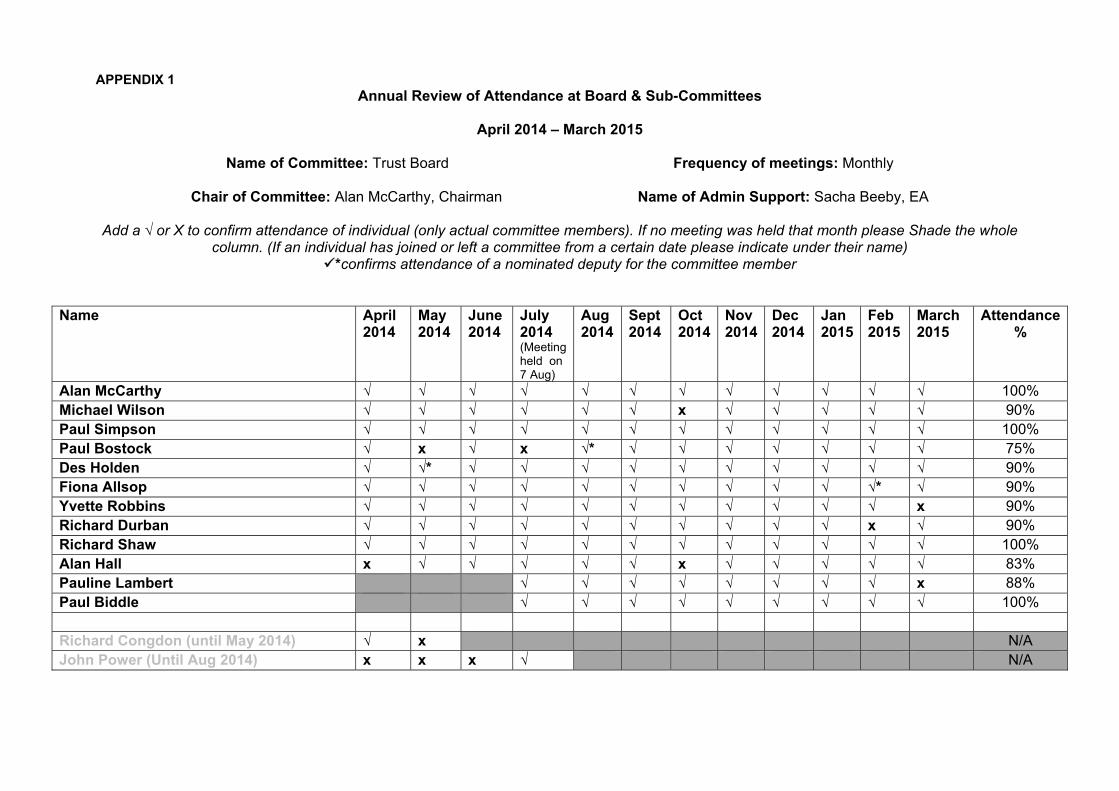
APPENDIX 1 Annual Review of Attendance at Board & Sub-Committees
April 2014 – March 2015
Name of Committee: Trust Board Frequency of meetings: Monthly
Chair of Committee: Alan McCarthy, Chairman Name of Admin Support: Sacha Beeby, EA
Add a √ or X to confirm attendance of individual (only actual committee members). If no meeting was held that month please Shade the whole
column. (If an individual has joined or left a committee from a certain date please indicate under their name) *confirms attendance of a nominated deputy for the committee member
Name April 2014
May 2014
June 2014
July 2014 (Meeting held on 7 Aug)
Aug 2014
Sept 2014
Oct 2014
Nov 2014
Dec 2014
Jan 2015
Feb 2015
March 2015
Attendance %
Alan McCarthy √ √ √ √ √ √ √ √ √ √ √ √ 100% Michael Wilson √ √ √ √ √ √ x √ √ √ √ √ 90% Paul Simpson √ √ √ √ √ √ √ √ √ √ √ √ 100% Paul Bostock √ x √ x √* √ √ √ √ √ √ √ 75% Des Holden √ √* √ √ √ √ √ √ √ √ √ √ 90% Fiona Allsop √ √ √ √ √ √ √ √ √ √ √* √ 90% Yvette Robbins √ √ √ √ √ √ √ √ √ √ √ x 90% Richard Durban √ √ √ √ √ √ √ √ √ √ x √ 90% Richard Shaw √ √ √ √ √ √ √ √ √ √ √ √ 100% Alan Hall x √ √ √ √ √ x √ √ √ √ √ 83% Pauline Lambert √ √ √ √ √ √ √ √ x 88% Paul Biddle √ √ √ √ √ √ √ √ √ 100% Richard Congdon (until May 2014) √ x N/A John Power (Until Aug 2014) x x x √ N/A
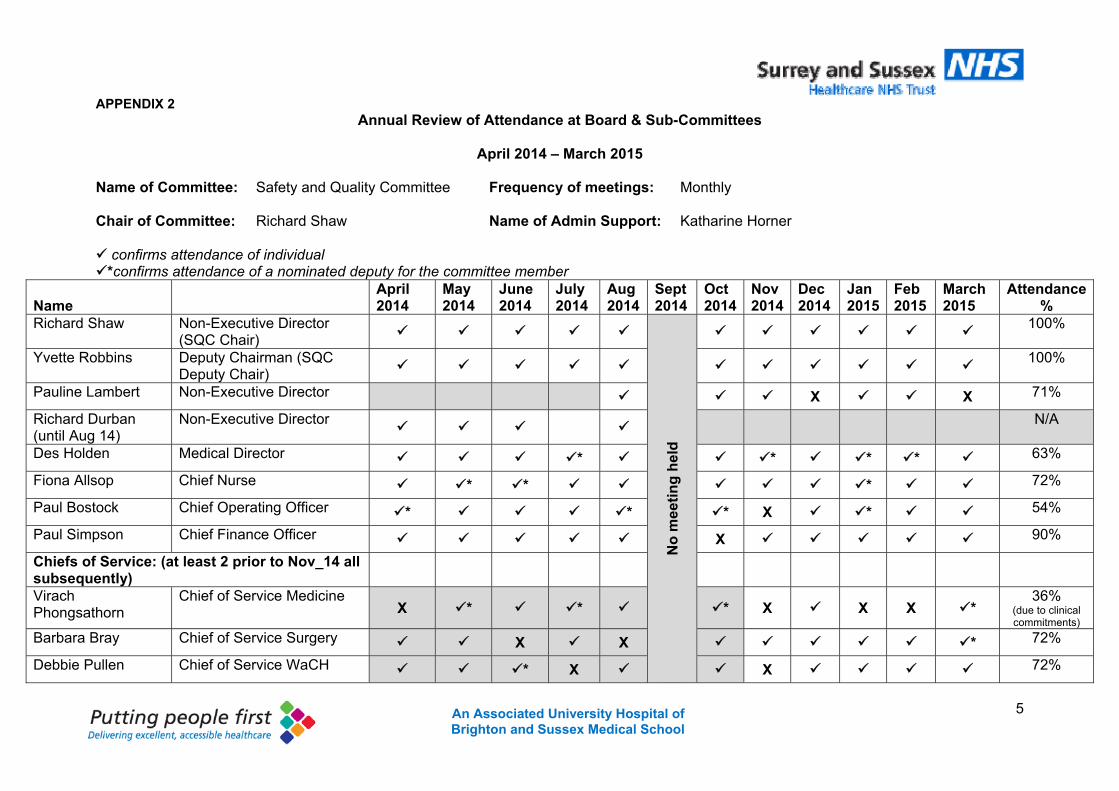
5 An Associated University Hospital of Brighton and Sussex Medical School
APPENDIX 2 Annual Review of Attendance at Board & Sub-Committees
April 2014 – March 2015
Name of Committee: Safety and Quality Committee Frequency of meetings: Monthly
Chair of Committee: Richard Shaw Name of Admin Support: Katharine Horner confirms attendance of individual *confirms attendance of a nominated deputy for the committee member
Name
April 2014
May 2014
June 2014
July 2014
Aug 2014
Sept 2014
Oct 2014
Nov 2014
Dec 2014
Jan 2015
Feb 2015
March 2015
Attendance %
Richard Shaw Non-Executive Director (SQC Chair)
No
mee
tin
g h
eld
100%
Yvette Robbins Deputy Chairman (SQC Deputy Chair)
100%
Pauline Lambert Non-Executive Director X X 71%
Richard Durban (until Aug 14)
Non-Executive Director
N/A
Des Holden Medical Director * * * * 63%
Fiona Allsop Chief Nurse * * * 72%
Paul Bostock Chief Operating Officer * * * X * 54%
Paul Simpson Chief Finance Officer X 90%
Chiefs of Service: (at least 2 prior to Nov_14 all subsequently)
Virach Phongsathorn
Chief of Service Medicine X * * * X X X *
36% (due to clinical commitments)
Barbara Bray Chief of Service Surgery X X * 72%
Debbie Pullen Chief of Service WaCH * X X 72%
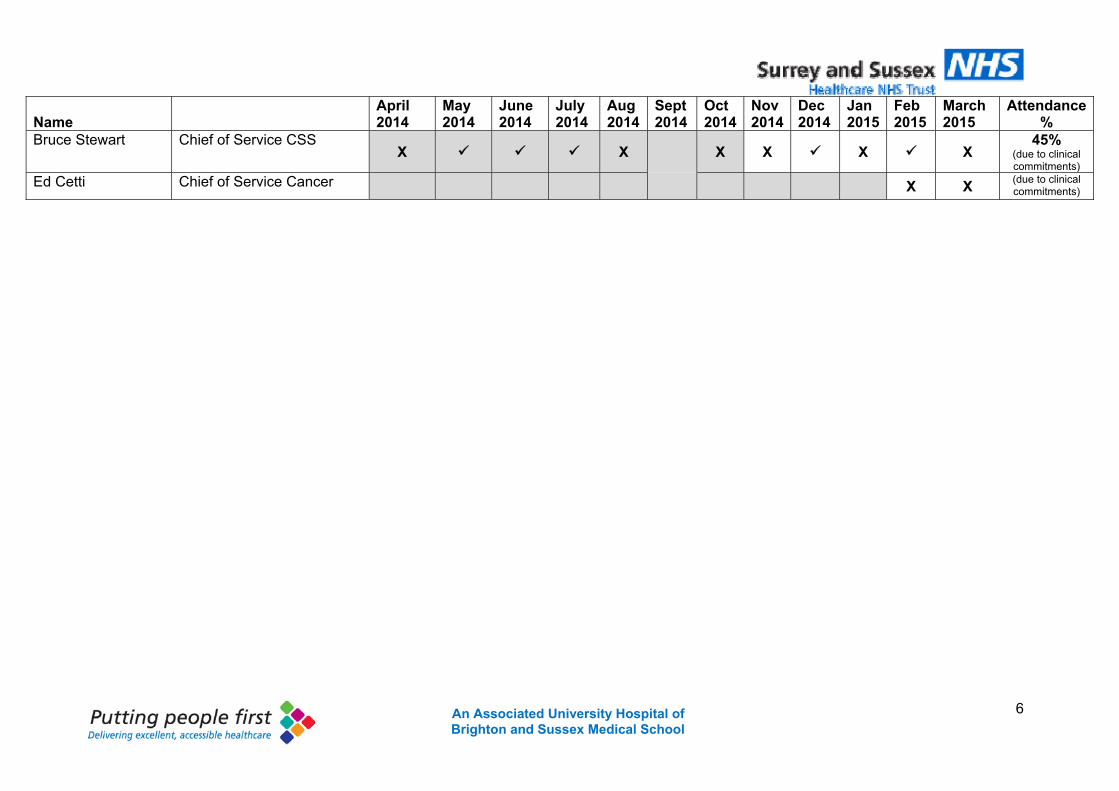
6 An Associated University Hospital of Brighton and Sussex Medical School
Name
April 2014
May 2014
June 2014
July 2014
Aug 2014
Sept 2014
Oct 2014
Nov 2014
Dec 2014
Jan 2015
Feb 2015
March 2015
Attendance %
Bruce Stewart Chief of Service CSS X X X X X X
45% (due to clinical commitments)
Ed Cetti Chief of Service Cancer X X (due to clinical commitments)
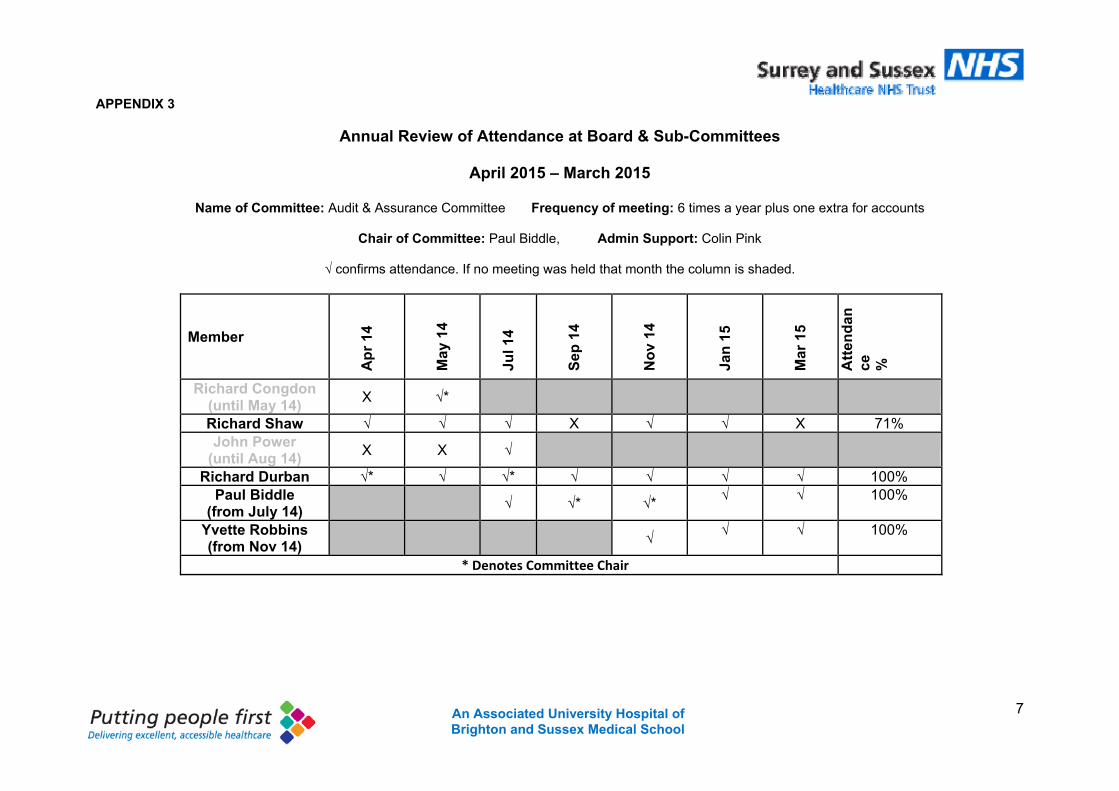
7 An Associated University Hospital of Brighton and Sussex Medical School
APPENDIX 3
Annual Review of Attendance at Board & Sub-Committees
April 2015 – March 2015
Name of Committee: Audit & Assurance Committee Frequency of meeting: 6 times a year plus one extra for accounts
Chair of Committee: Paul Biddle, Admin Support: Colin Pink
√ confirms attendance. If no meeting was held that month the column is shaded.
Member
Ap
r 14
May
14
Jul 1
4
Sep
14
No
v 14
Jan
15
Mar
15
Att
end
ance
%
Richard Congdon (until May 14)
X √*
Richard Shaw √ √ √ X √ √ X 71% John Power
(until Aug 14) X X √
Richard Durban √* √ √* √ √ √ √ 100% Paul Biddle
(from July 14) √ √* √*
√ √ 100%
Yvette Robbins (from Nov 14)
√ √ √ 100%
* Denotes Committee Chair
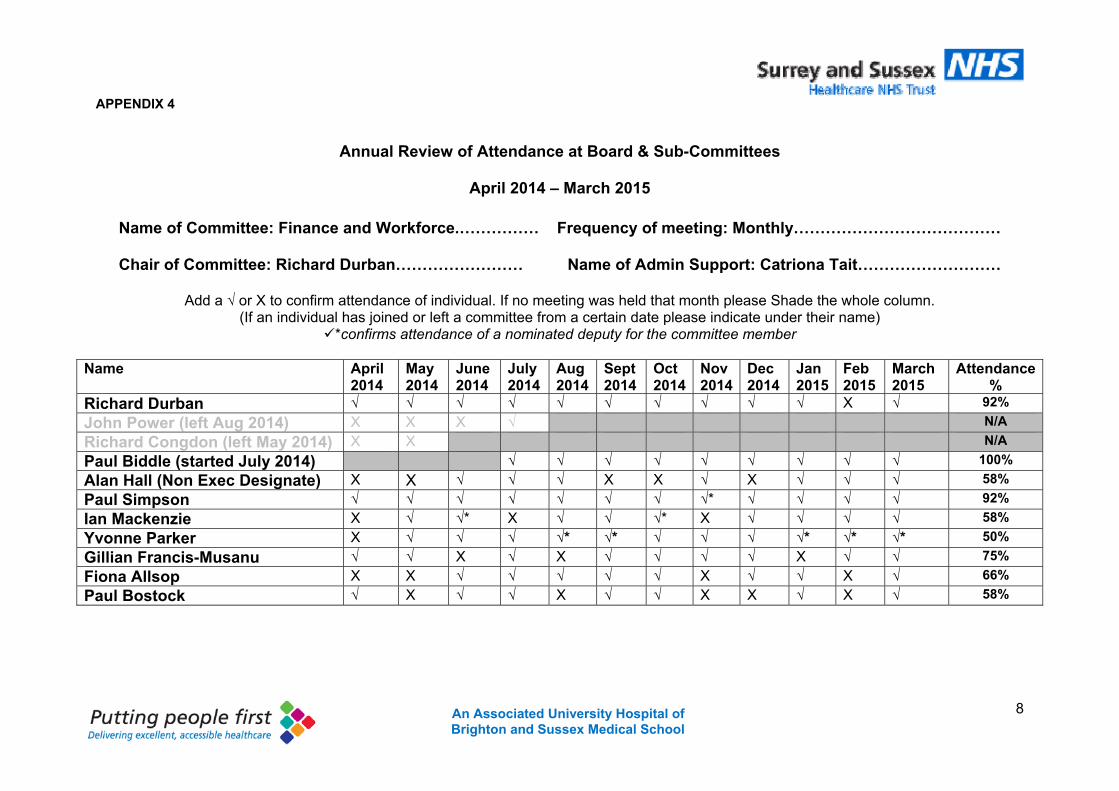
8 An Associated University Hospital of Brighton and Sussex Medical School
APPENDIX 4
Annual Review of Attendance at Board & Sub-Committees
April 2014 – March 2015
Name of Committee: Finance and Workforce.…………… Frequency of meeting: Monthly…………………………………
Chair of Committee: Richard Durban…………………… Name of Admin Support: Catriona Tait………………………
Add a √ or X to confirm attendance of individual. If no meeting was held that month please Shade the whole column.
(If an individual has joined or left a committee from a certain date please indicate under their name) *confirms attendance of a nominated deputy for the committee member
Name April
2014 May 2014
June 2014
July 2014
Aug 2014
Sept 2014
Oct 2014
Nov 2014
Dec 2014
Jan 2015
Feb 2015
March 2015
Attendance %
Richard Durban √ √ √ √ √ √ √ √ √ √ X √ 92%
John Power (left Aug 2014) X X X √ N/A
Richard Congdon (left May 2014) X X N/A
Paul Biddle (started July 2014) √ √ √ √ √ √ √ √ √ 100%
Alan Hall (Non Exec Designate) X X √ √ √ X X √ X √ √ √ 58%
Paul Simpson √ √ √ √ √ √ √ √* √ √ √ √ 92%
Ian Mackenzie X √ √* X √ √ √* X √ √ √ √ 58%
Yvonne Parker X √ √ √ √* √* √ √ √ √* √* √* 50%
Gillian Francis-Musanu √ √ X √ X √ √ √ √ X √ √ 75%
Fiona Allsop X X √ √ √ √ √ X √ √ X √ 66%
Paul Bostock √ X √ √ X √ √ X X √ X √ 58%
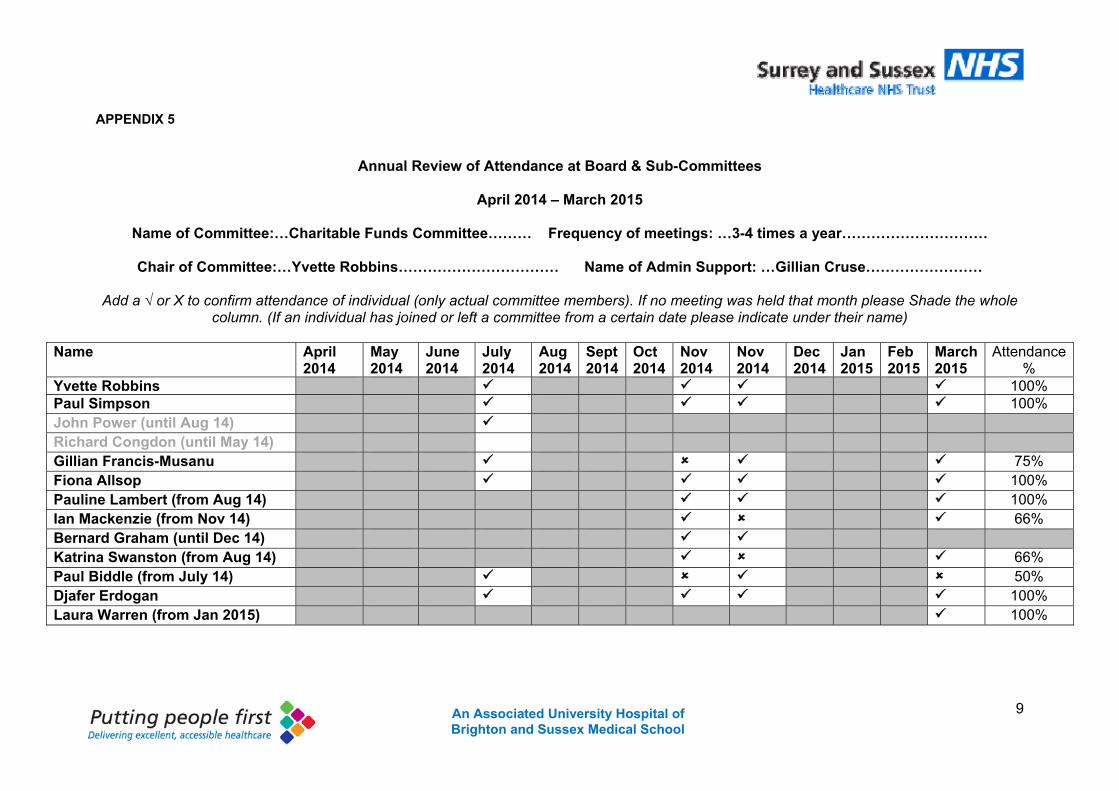
9 An Associated University Hospital of Brighton and Sussex Medical School
APPENDIX 5
Annual Review of Attendance at Board & Sub-Committees
April 2014 – March 2015
Name of Committee:…Charitable Funds Committee……… Frequency of meetings: …3-4 times a year…………………………
Chair of Committee:…Yvette Robbins…………………………… Name of Admin Support: …Gillian Cruse……………………
Add a √ or X to confirm attendance of individual (only actual committee members). If no meeting was held that month please Shade the whole column. (If an individual has joined or left a committee from a certain date please indicate under their name)
Name April
2014 May 2014
June 2014
July 2014
Aug 2014
Sept 2014
Oct 2014
Nov 2014
Nov 2014
Dec 2014
Jan 2015
Feb 2015
March2015
Attendance %
Yvette Robbins 100% Paul Simpson 100% John Power (until Aug 14) Richard Congdon (until May 14) Gillian Francis-Musanu 75% Fiona Allsop 100% Pauline Lambert (from Aug 14) 100% Ian Mackenzie (from Nov 14) 66% Bernard Graham (until Dec 14) Katrina Swanston (from Aug 14) 66% Paul Biddle (from July 14) 50% Djafer Erdogan 100% Laura Warren (from Jan 2015) 100%
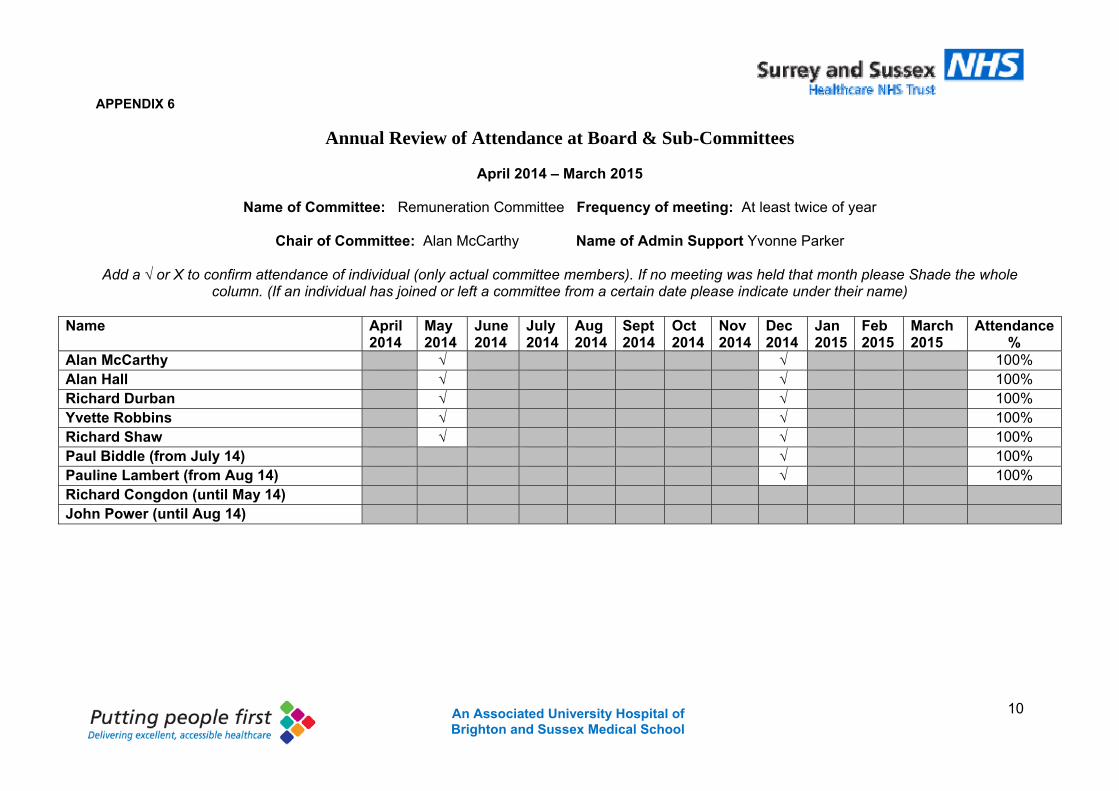
10 An Associated University Hospital of Brighton and Sussex Medical School
APPENDIX 6
Annual Review of Attendance at Board & Sub-Committees
April 2014 – March 2015
Name of Committee: Remuneration Committee Frequency of meeting: At least twice of year
Chair of Committee: Alan McCarthy Name of Admin Support Yvonne Parker
Add a √ or X to confirm attendance of individual (only actual committee members). If no meeting was held that month please Shade the whole column. (If an individual has joined or left a committee from a certain date please indicate under their name)
Name April
2014 May 2014
June 2014
July 2014
Aug 2014
Sept 2014
Oct 2014
Nov 2014
Dec 2014
Jan 2015
Feb 2015
March 2015
Attendance %
Alan McCarthy √ √ 100% Alan Hall √ √ 100% Richard Durban √ √ 100% Yvette Robbins √ √ 100% Richard Shaw √ √ 100% Paul Biddle (from July 14) √ 100% Pauline Lambert (from Aug 14) √ 100% Richard Congdon (until May 14) John Power (until Aug 14)
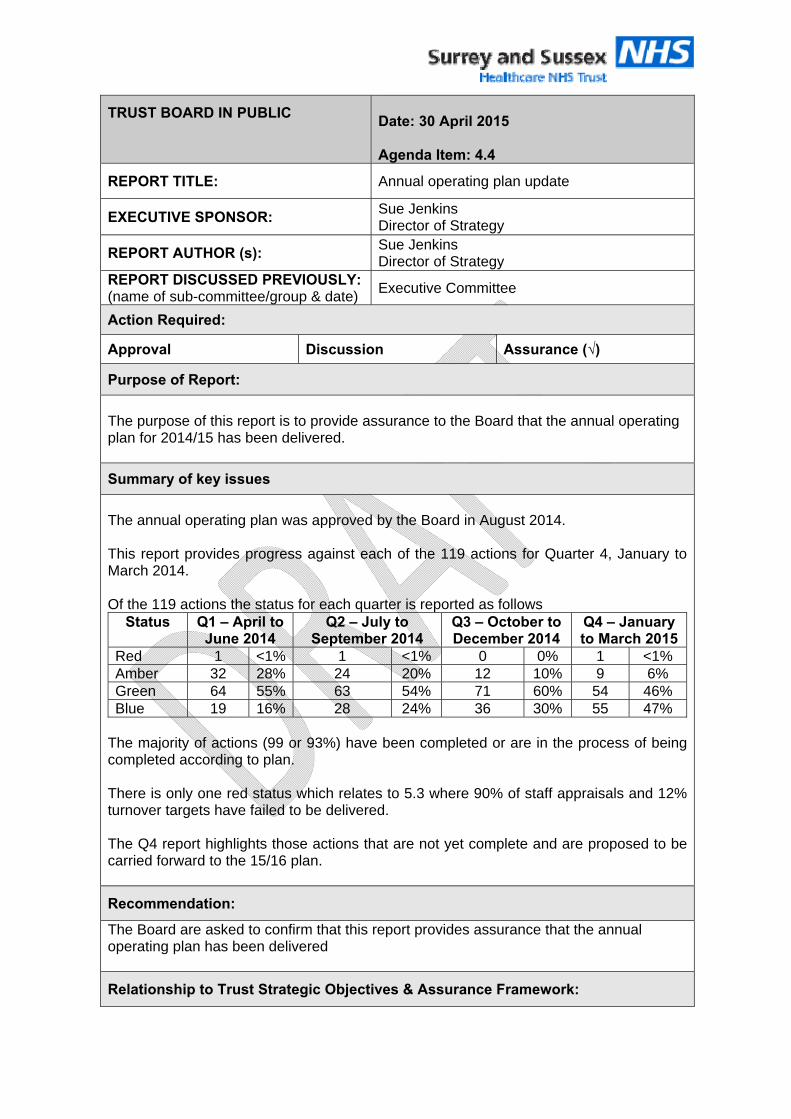
TRUST BOARD IN PUBLIC
Date: 30 April 2015 Agenda Item: 4.4
REPORT TITLE: Annual operating plan update
EXECUTIVE SPONSOR: Sue Jenkins Director of Strategy
REPORT AUTHOR (s): Sue Jenkins Director of Strategy
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date) Executive Committee
Action Required:
Approval Discussion Assurance (√)
Purpose of Report:
The purpose of this report is to provide assurance to the Board that the annual operating plan for 2014/15 has been delivered.
Summary of key issues
The annual operating plan was approved by the Board in August 2014. This report provides progress against each of the 119 actions for Quarter 4, January to March 2014. Of the 119 actions the status for each quarter is reported as follows
Status Q1 – April to June 2014
Q2 – July to September 2014
Q3 – October to December 2014
Q4 – January to March 2015
Red 1 <1% 1 <1% 0 0% 1 <1% Amber 32 28% 24 20% 12 10% 9 6% Green 64 55% 63 54% 71 60% 54 46% Blue 19 16% 28 24% 36 30% 55 47%
The majority of actions (99 or 93%) have been completed or are in the process of being completed according to plan. There is only one red status which relates to 5.3 where 90% of staff appraisals and 12% turnover targets have failed to be delivered. The Q4 report highlights those actions that are not yet complete and are proposed to be carried forward to the 15/16 plan.
Recommendation:
The Board are asked to confirm that this report provides assurance that the annual operating plan has been delivered
Relationship to Trust Strategic Objectives & Assurance Framework:
2An Associated University Hospital of Brighton and Sussex Medical School
SO1: Safe -Deliver safe services and be in the top 20% against our peers SO2: Effective - Deliver effective and sustainable clinical services within the local health economy SO3: Caring – Ensure patients are cared for and feel cared about SO4: Responsive – Become the secondary care provider and employer of choice our catchment population SO5: Well led: Become an employer of choice and deliver financial and clinical sustainability around a clinical leadership model
Corporate Impact Assessment:
Legal and regulatory impact The annual operating demonstrates delivery of key actions to support the strategic objectives
Financial impact Business cases will be developed for any significant resource developments.
Patient Experience/Engagement The annual plan includes a number of objectives linking to patient experience and engagement
Risk & Performance Management Delivery of the annual operating plan is monitored by the executive Committee and reported to the Trust Board
NHS Constitution/Equality & Diversity/Communication
The annual plan demonstrates delivery of the organisations strategic objectives
Attachment:
Annual operating plan Q4 update
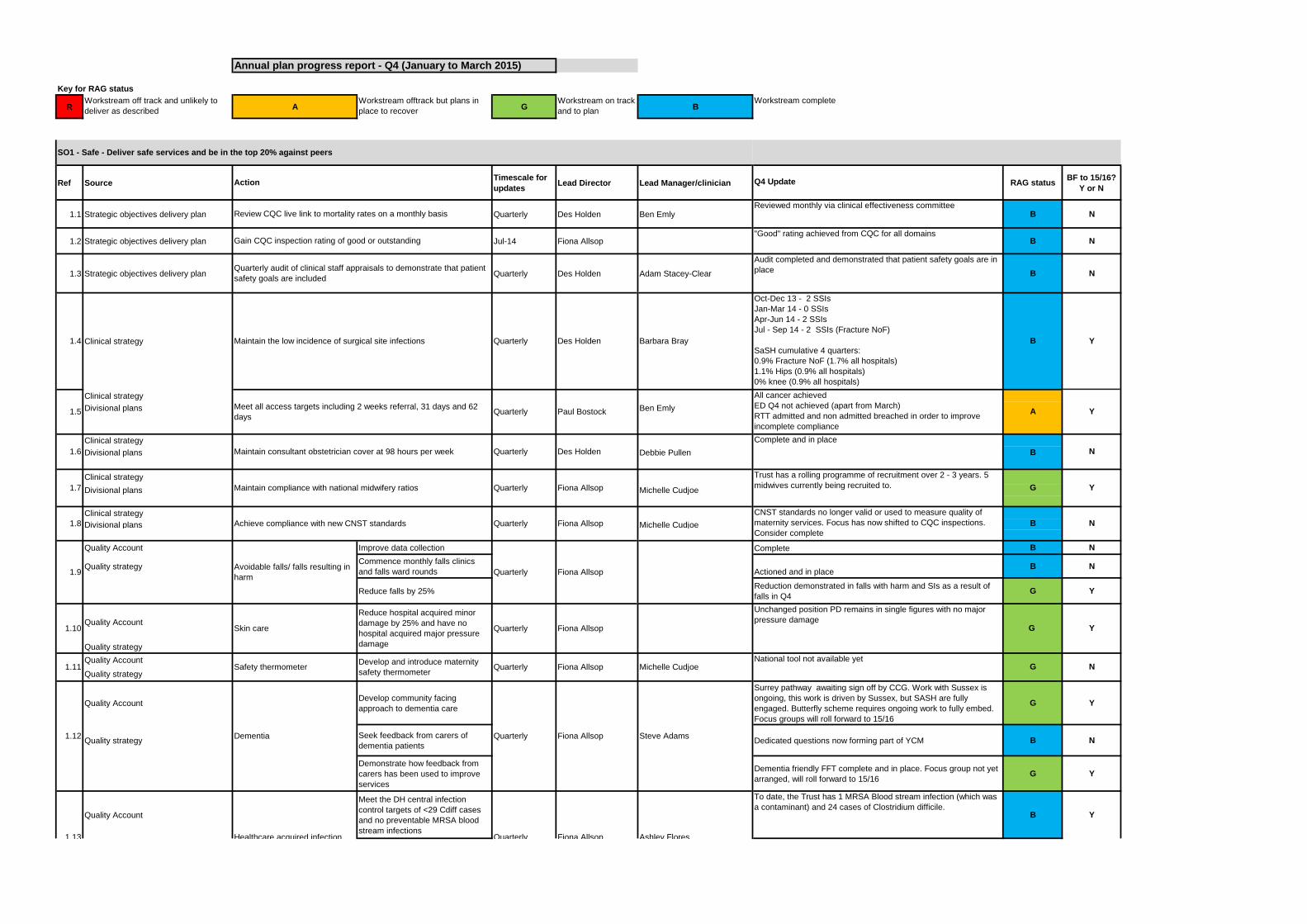
Annual plan progress report - Q4 (January to March 2015)
Key for RAG status
RWorkstream off track and unlikely to
deliver as describedA
Workstream offtrack but plans in
place to recoverG
Workstream on track
and to planB
Workstream complete
Ref SourceTimescale for
updatesLead Director Lead Manager/clinician Q4 Update RAG status
BF to 15/16?
Y or N
1.1 Strategic objectives delivery plan Quarterly Des Holden Ben EmlyReviewed monthly via clinical effectiveness committee
B N
1.2 Strategic objectives delivery plan Jul-14 Fiona Allsop"Good" rating achieved from CQC for all domains
B N
1.3 Strategic objectives delivery plan Quarterly Des Holden Adam Stacey-Clear
Audit completed and demonstrated that patient safety goals are in
place B N
Clinical strategy Y
Divisional plansClinical strategy
Divisional plans Ben Emly
Clinical strategy
Divisional plans Debbie Pullen B
Clinical strategy
Divisional plans Michelle Cudjoe
Clinical strategy
Divisional plans Michelle Cudjoe
Quality Account Improve data collection Complete B N
Quality strategyCommence monthly falls clinics
and falls ward rounds Actioned and in placeB N
Reduce falls by 25%Reduction demonstrated in falls with harm and SIs as a result of
falls in Q4G Y
Quality Account
Quality strategy
Quality Account
Quality strategy
Quality AccountDevelop community facing
approach to dementia care
Surrey pathway awaiting sign off by CCG. Work with Sussex is
ongoing, this work is driven by Sussex, but SASH are fully
engaged. Butterfly scheme requires ongoing work to fully embed.
Focus groups will roll forward to 15/16
G Y
Quality strategySeek feedback from carers of
dementia patientsDedicated questions now forming part of YCM B N
Demonstrate how feedback from
carers has been used to improve
services
Dementia friendly FFT complete and in place. Focus group not yet
arranged, will roll forward to 15/16G Y
Quality Account
Meet the DH central infection
control targets of <29 Cdiff cases
and no preventable MRSA blood
stream infections
To date, the Trust has 1 MRSA Blood stream infection (which was
a contaminant) and 24 cases of Clostridium difficile. B Y
G
Oct-Dec 13 - 2 SSIs
Jan-Mar 14 - 0 SSIs
Apr-Jun 14 - 2 SSIs
Jul - Sep 14 - 2 SSIs (Fracture NoF)
SaSH cumulative 4 quarters:
0.9% Fracture NoF (1.7% all hospitals)
1.1% Hips (0.9% all hospitals)
0% knee (0.9% all hospitals)
Trust has a rolling programme of recruitment over 2 - 3 years. 5
midwives currently being recruited to.
National tool not available yet
All cancer achieved
ED Q4 not achieved (apart from March)
RTT admitted and non admitted breached in order to improve
incomplete compliance
Complete and in place
CNST standards no longer valid or used to measure quality of
maternity services. Focus has now shifted to CQC inspections.
Consider complete
1.5Meet all access targets including 2 weeks referral, 31 days and 62
daysQuarterly Paul Bostock
1.6 Maintain consultant obstetrician cover at 98 hours per week Quarterly Des Holden
1.7 Maintain compliance with national midwifery ratios Quarterly Fiona Allsop
1.8 Achieve compliance with new CNST standards Quarterly Fiona Allsop
1.9Avoidable falls/ falls resulting in
harmQuarterly Fiona Allsop
1.10 Skin care
Reduce hospital acquired minor
damage by 25% and have no
hospital acquired major pressure
damage
Quarterly Fiona Allsop
1.11 Safety thermometerDevelop and introduce maternity
safety thermometerQuarterly Fiona Allsop Michelle Cudjoe
1.12 Dementia Quarterly Fiona Allsop Steve Adams
1.13 Healthcare acquired infection Quarterly Fiona Allsop Ashley Flores
B
G
SO1 - Safe - Deliver safe services and be in the top 20% against peers
Action
1.4 Maintain the low incidence of surgical site infections
Gain CQC inspection rating of good or outstanding
G
Review CQC live link to mortality rates on a monthly basis
Unchanged position PD remains in single figures with no major
pressure damage
Quarterly audit of clinical staff appraisals to demonstrate that patient
safety goals are included
Quarterly BBarbara BrayDes Holden
A Y
N
Y
N
Y
N
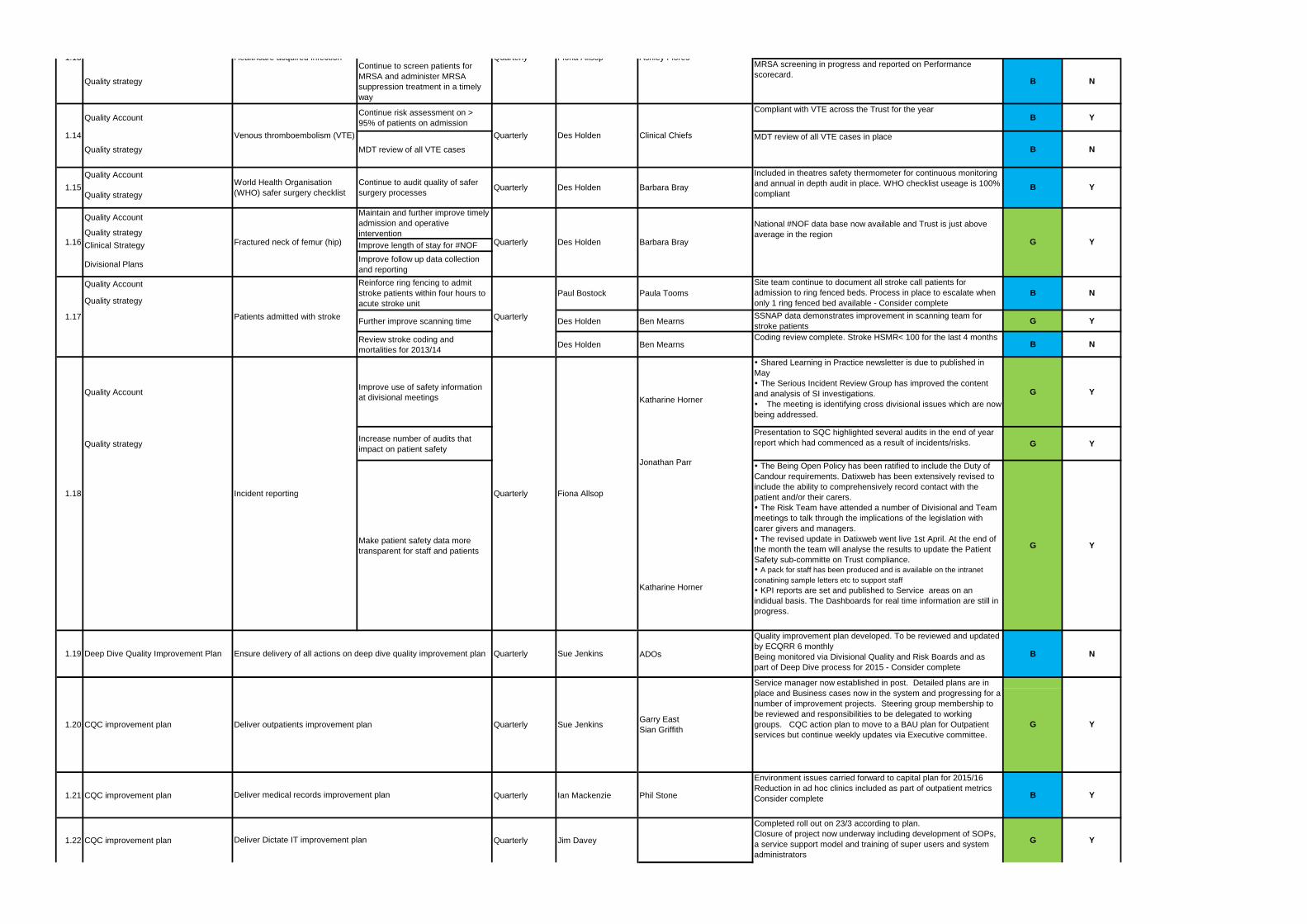
Quality strategy
Continue to screen patients for
MRSA and administer MRSA
suppression treatment in a timely
way
MRSA screening in progress and reported on Performance
scorecard. B N
Quality AccountContinue risk assessment on >
95% of patients on admission
Compliant with VTE across the Trust for the yearB Y
Quality strategy MDT review of all VTE cases
MDT review of all VTE cases in place
B N
Quality Account
Quality strategy
Quality Account
Quality strategy
Clinical Strategy Improve length of stay for #NOF
Divisional PlansImprove follow up data collection
and reporting
Quality Account
Quality strategy
Further improve scanning time Des Holden Ben MearnsSSNAP data demonstrates improvement in scanning team for
stroke patientsG Y
Review stroke coding and
mortalities for 2013/14Des Holden Ben Mearns
Coding review complete. Stroke HSMR< 100 for the last 4 monthsB N
Quality AccountImprove use of safety information
at divisional meetings
Shared Learning in Practice newsletter is due to published in
May
The Serious Incident Review Group has improved the content
and analysis of SI investigations.
The meeting is identifying cross divisional issues which are now
being addressed.
G Y
Quality strategyIncrease number of audits that
impact on patient safety
Presentation to SQC highlighted several audits in the end of year
report which had commenced as a result of incidents/risks. G Y
Make patient safety data more
transparent for staff and patients
The Being Open Policy has been ratified to include the Duty of
Candour requirements. Datixweb has been extensively revised to
include the ability to comprehensively record contact with the
patient and/or their carers.
The Risk Team have attended a number of Divisional and Team
meetings to talk through the implications of the legislation with
carer givers and managers.
The revised update in Datixweb went live 1st April. At the end of
the month the team will analyse the results to update the Patient
Safety sub-committe on Trust compliance.
A pack for staff has been produced and is available on the intranet
conatining sample letters etc to support staff
KPI reports are set and published to Service areas on an
indidual basis. The Dashboards for real time information are still in
progress.
G Y
ADOs
Quality improvement plan developed. To be reviewed and updated
by ECQRR 6 monthly
Being monitored via Divisional Quality and Risk Boards and as
part of Deep Dive process for 2015 - Consider complete
B N
1.21 CQC improvement plan Quarterly Ian Mackenzie Phil Stone
Environment issues carried forward to capital plan for 2015/16
Reduction in ad hoc clinics included as part of outpatient metrics
Consider complete B Y
1.22 CQC improvement plan Quarterly Jim Davey
Completed roll out on 23/3 according to plan.
Closure of project now underway including development of SOPs,
a service support model and training of super users and system
administrators
G Y
Included in theatres safety thermometer for continuous monitoring
and annual in depth audit in place. WHO checklist useage is 100%
compliant
National #NOF data base now available and Trust is just above
average in the region
Service manager now established in post. Detailed plans are in
place and Business cases now in the system and progressing for a
number of improvement projects. Steering group membership to
be reviewed and responsibilities to be delegated to working
groups. CQC action plan to move to a BAU plan for Outpatient
services but continue weekly updates via Executive committee.
Barbara Bray
Garry East
Sian Griffith
Clinical Chiefs
Fiona Allsop
Paul Bostock Paula Tooms
Quarterly
Sue Jenkins
Katharine Horner
Jonathan Parr
Katharine Horner
Deliver medical records improvement plan
Deliver Dictate IT improvement plan
1.13 Healthcare acquired infection Quarterly Fiona Allsop Ashley Flores
1.14 Venous thromboembolism (VTE) Quarterly Des Holden
1.15World Health Organisation
(WHO) safer surgery checklist
Continue to audit quality of safer
surgery processesQuarterly Des Holden
1.17 Patients admitted with stroke
Reinforce ring fencing to admit
stroke patients within four hours to
acute stroke unit
Quarterly
1.18
1.16 Fractured neck of femur (hip)
Maintain and further improve timely
admission and operative
interventionQuarterly
Incident reporting
1.19 Deep Dive Quality Improvement Plan Ensure delivery of all actions on deep dive quality improvement plan Quarterly Sue Jenkins
1.20 CQC improvement plan Deliver outpatients improvement plan Quarterly
B
Site team continue to document all stroke call patients for
admission to ring fenced beds. Process in place to escalate when
only 1 ring fenced bed available - Consider complete
Barbara Bray
Des Holden
B
G
G
N
Y
Y
Y
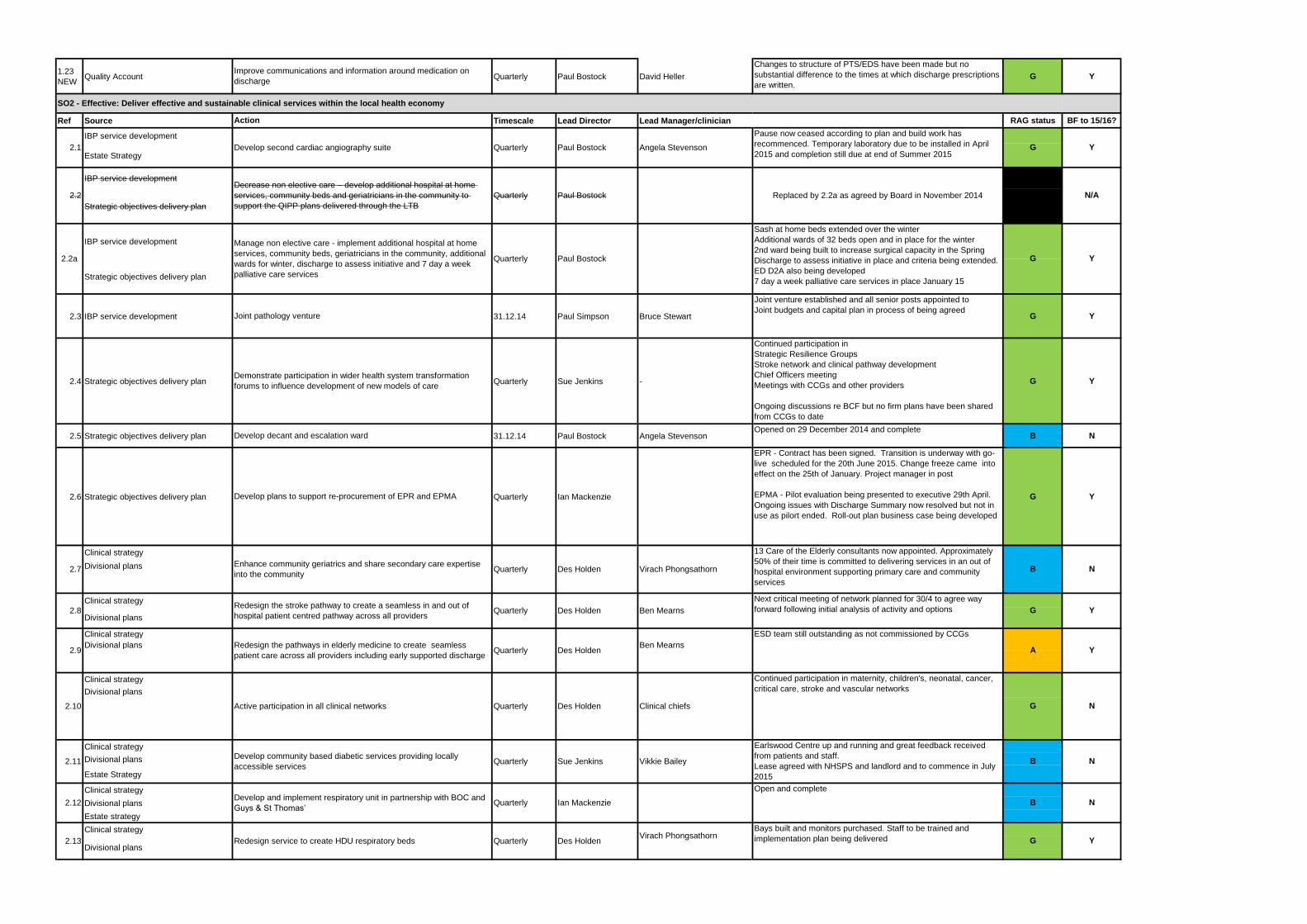
1.23
NEWQuality Account Quarterly Paul Bostock David Heller
Changes to structure of PTS/EDS have been made but no
substantial difference to the times at which discharge prescriptions
are written.G Y
Ref Source Timescale Lead Director Lead Manager/clinician RAG status BF to 15/16?
IBP service development
Estate Strategy
IBP service development
Strategic objectives delivery plan
IBP service development
Strategic objectives delivery plan
2.3 IBP service development 31.12.14 Paul Simpson Bruce Stewart
Joint venture established and all senior posts appointed to
Joint budgets and capital plan in process of being agreedG Y
2.4 Strategic objectives delivery plan Quarterly Sue Jenkins -
Continued participation in
Strategic Resilience Groups
Stroke network and clinical pathway development
Chief Officers meeting
Meetings with CCGs and other providers
Ongoing discussions re BCF but no firm plans have been shared
from CCGs to date
G Y
2.5 Strategic objectives delivery plan 31.12.14 Paul Bostock Angela StevensonOpened on 29 December 2014 and complete
B N
2.6 Strategic objectives delivery plan Quarterly Ian Mackenzie
EPR - Contract has been signed. Transition is underway with go-
live scheduled for the 20th June 2015. Change freeze came into
effect on the 25th of January. Project manager in post
EPMA - Pilot evaluation being presented to executive 29th April.
Ongoing issues with Discharge Summary now resolved but not in
use as pilort ended. Roll-out plan business case being developed
G Y
Clinical strategy
Divisional plans
Clinical strategy
Clinical strategy
Divisional plans Ben Mearns
Clinical strategy
Divisional plans
Clinical strategy
Divisional plans
Estate Strategy
Clinical strategy
Divisional plans
Estate strategy
Clinical strategy
Replaced by 2.2a as agreed by Board in November 2014
Continued participation in maternity, children's, neonatal, cancer,
critical care, stroke and vascular networks
Bays built and monitors purchased. Staff to be trained and
implementation plan being delivered
Next critical meeting of network planned for 30/4 to agree way
forward following initial analysis of activity and options
ESD team still outstanding as not commissioned by CCGs
Earlswood Centre up and running and great feedback received
from patients and staff.
Lease agreed with NHSPS and landlord and to commence in July
2015
Pause now ceased according to plan and build work has
recommenced. Temporary laboratory due to be installed in April
2015 and completion still due at end of Summer 2015
2.2a
Manage non elective care - implement additional hospital at home
services, community beds, geriatricians in the community, additional
wards for winter, discharge to assess initiative and 7 day a week
palliative care services
Quarterly Paul Bostock
Ben Mearns
Sue Jenkins
Sash at home beds extended over the winter
Additional wards of 32 beds open and in place for the winter
2nd ward being built to increase surgical capacity in the Spring
Discharge to assess initiative in place and criteria being extended.
ED D2A also being developed
7 day a week palliative care services in place January 15
G
Divisional plans
Develop plans to support re-procurement of EPR and EPMA
G
Joint pathology venture
Demonstrate participation in wider health system transformation
forums to influence development of new models of care
A
Develop decant and escalation ward
Improve communications and information around medication on
discharge
Action
Virach Phongsathorn
Clinical chiefs
Develop community based diabetic services providing locally
accessible services
Virach PhongsathornQuarterly Des Holden
Ian Mackenzie
Quarterly Vikkie Bailey2.11
2.12Develop and implement respiratory unit in partnership with BOC and
Guys & St Thomas’Quarterly
2.13 Redesign service to create HDU respiratory beds
Angela Stevenson2.1 Develop second cardiac angiography suite Quarterly Paul Bostock
2.2
Decrease non elective care – develop additional hospital at home
services, community beds and geriatricians in the community to
support the QIPP plans delivered through the LTB
Quarterly Paul Bostock
2.7Enhance community geriatrics and share secondary care expertise
into the communityQuarterly Des Holden
2.8Redesign the stroke pathway to create a seamless in and out of
hospital patient centred pathway across all providersQuarterly Des Holden
Divisional plans
2.9Redesign the pathways in elderly medicine to create seamless
patient care across all providers including early supported discharge Quarterly Des Holden
2.10 Active participation in all clinical networks Quarterly Des Holden
SO2 - Effective: Deliver effective and sustainable clinical services within the local health economy
B
G
B
R
G
Open and complete
G
Y
N
N
Y
13 Care of the Elderly consultants now appointed. Approximately
50% of their time is committed to delivering services in an out of
hospital environment supporting primary care and community
services
B
N
N
Y
N/A
Y
Y
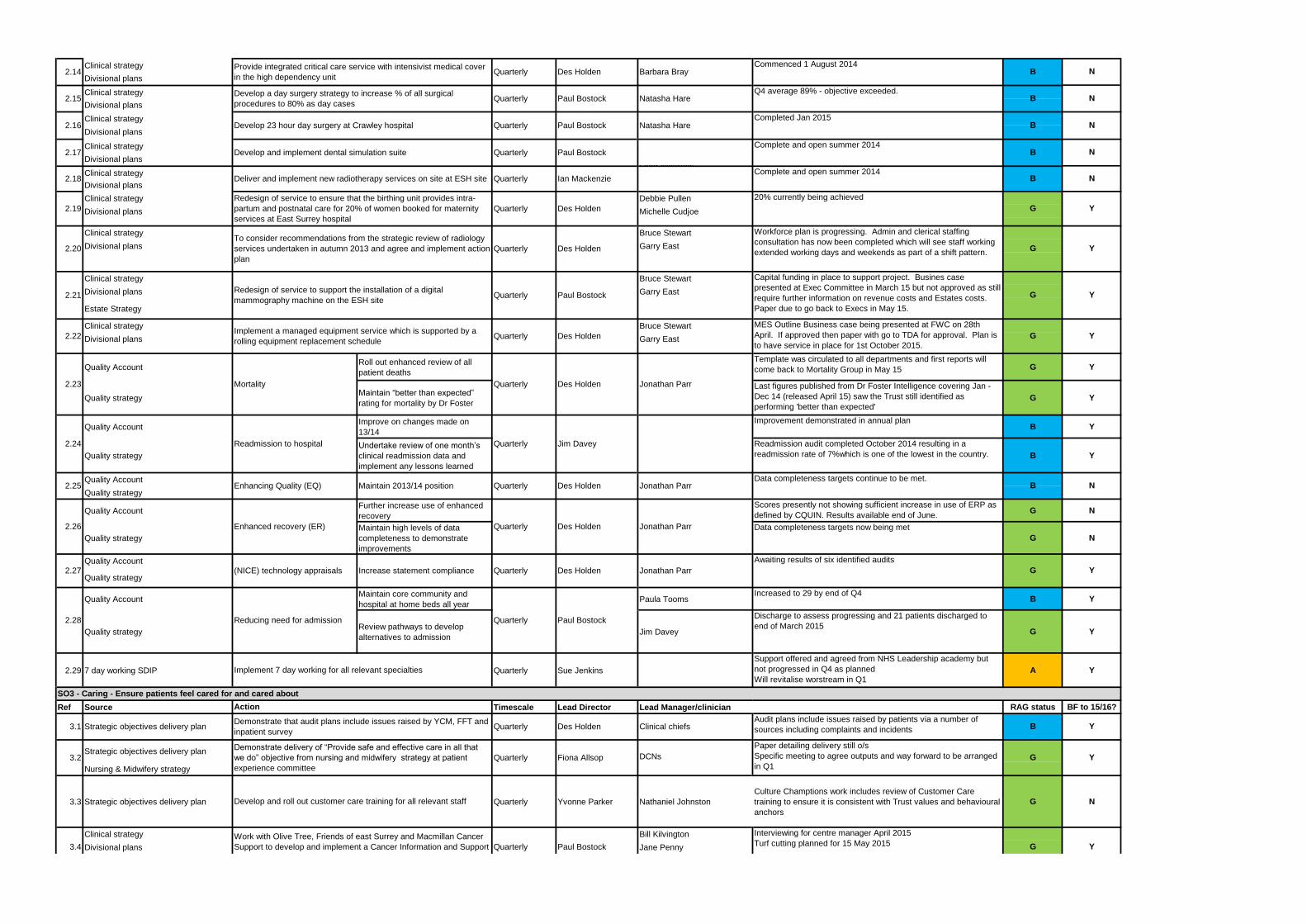
Clinical strategy
Clinical strategy
Clinical strategy
Clinical strategy
Lead clinicians NClinical strategy
Clinical strategy Debbie Pullen
Divisional plans Michelle Cudjoe
Clinical strategy Bruce Stewart
Divisional plans Garry East
Clinical strategy Bruce Stewart
Divisional plans Garry East
Estate Strategy
Clinical strategy Bruce Stewart
Divisional plans Garry East
Quality AccountRoll out enhanced review of all
patient deaths
Template was circulated to all departments and first reports will
come back to Mortality Group in May 15 G Y
Quality strategyMaintain “better than expected”
rating for mortality by Dr Foster
Last figures published from Dr Foster Intelligence covering Jan -
Dec 14 (released April 15) saw the Trust still identified as
performing 'better than expected'G Y
Quality AccountImprove on changes made on
13/14
Improvement demonstrated in annual planB Y
Quality strategy
Undertake review of one month’s
clinical readmission data and
implement any lessons learned
Readmission audit completed October 2014 resulting in a
readmission rate of 7%which is one of the lowest in the country. B Y
Quality Account Data completeness targets continue to be met.
Quality strategy
Quality AccountFurther increase use of enhanced
recovery
Scores presently not showing sufficient increase in use of ERP as
defined by CQUIN. Results available end of June.G N
Quality strategy
Maintain high levels of data
completeness to demonstrate
improvements
Data completeness targets now being met
G N
Quality Account Awaiting results of six identified audits
Quality strategy
Quality AccountMaintain core community and
hospital at home beds all yearPaula Tooms
Increased to 29 by end of Q4B Y
Quality strategyReview pathways to develop
alternatives to admissionJim Davey
Discharge to assess progressing and 21 patients discharged to
end of March 2015G Y
2.29 7 day working SDIP Quarterly Sue Jenkins
Support offered and agreed from NHS Leadership academy but
not progressed in Q4 as planned
Will revitalise worstream in Q1A Y
Ref Source Timescale Lead Director Lead Manager/clinician RAG status BF to 15/16?
Strategic objectives delivery planDCNs
Nursing & Midwifery strategy
3.3 Strategic objectives delivery plan Quarterly Yvonne Parker Nathaniel Johnston
Culture Champtions work includes review of Customer Care
training to ensure it is consistent with Trust values and behavioural
anchors
G N
Clinical strategy Bill Kilvington
Divisional plans Jane Penny
G
Paul Bostock
Jonathan Parr
Complete and open summer 2014
20% currently being achieved
MES Outline Business case being presented at FWC on 28th
April. If approved then paper with go to TDA for approval. Plan is
to have service in place for 1st October 2015.
Workforce plan is progressing. Admin and clerical staffing
consultation has now been completed which will see staff working
extended working days and weekends as part of a shift pattern.
Interviewing for centre manager April 2015
Turf cutting planned for 15 May 2015
Audit plans include issues raised by patients via a number of
sources including complaints and incidents
Complete and open summer 2014
Capital funding in place to support project. Busines case
presented at Exec Committee in March 15 but not approved as still
require further information on revenue costs and Estates costs.
Paper due to go back to Execs in May 15.
Divisional plansNatasha Hare
B
Barbara Bray
Natasha Hare
Des Holden
Clinical chiefs
Des Holden
Des Holden
B
Jim Davey
Des Holden Jonathan Parr
Quarterly Paul Bostock G
2.14Provide integrated critical care service with intensivist medical cover
in the high dependency unitQuarterly Des Holden
2.15Develop a day surgery strategy to increase % of all surgical
procedures to 80% as day cases Quarterly Paul Bostock
Divisional plans
2.16 Develop 23 hour day surgery at Crawley hospital Quarterly Paul Bostock
Divisional plans
2.17 Develop and implement dental simulation suite Quarterly Paul Bostock
2.18 Deliver and implement new radiotherapy services on site at ESH site Quarterly Ian Mackenzie
Divisional plans
Divisional plans
2.19
Redesign of service to ensure that the birthing unit provides intra-
partum and postnatal care for 20% of women booked for maternity
services at East Surrey hospital
Quarterly Des Holden
2.20
To consider recommendations from the strategic review of radiology
services undertaken in autumn 2013 and agree and implement action
plan
Quarterly
2.21Redesign of service to support the installation of a digital
mammography machine on the ESH siteQuarterly Paul Bostock
2.22Implement a managed equipment service which is supported by a
rolling equipment replacement scheduleQuarterly Des Holden
2.23 Mortality Quarterly
2.24 Readmission to hospital Quarterly
2.25 Enhancing Quality (EQ) Maintain 2013/14 position Quarterly Des Holden
Jonathan Parr
Jonathan Parr
2.26 Enhanced recovery (ER) Quarterly
Implement 7 day working for all relevant specialties
Action
2.27 (NICE) technology appraisals Increase statement compliance Quarterly
2.28 Reducing need for admission Quarterly
SO3 - Caring - Ensure patients feel cared for and cared about
3.1 Strategic objectives delivery planDemonstrate that audit plans include issues raised by YCM, FFT and
inpatient surveyQuarterly Des Holden
3.2
Demonstrate delivery of “Provide safe and effective care in all that
we do” objective from nursing and midwifery strategy at patient
experience committee
Quarterly Fiona Allsop
Develop and roll out customer care training for all relevant staff
3.4
Work with Olive Tree, Friends of east Surrey and Macmillan Cancer
Support to develop and implement a Cancer Information and Support
Centre at East Surrey Hospital
B
B
G
G
G
Paper detailing delivery still o/s
Specific meeting to agree outputs and way forward to be arranged
in Q1
G
G
Y
Y
Y
Y
N
Y
Y
Y
Y
N
N
N
N
N
Q4 average 89% - objective exceeded.
Commenced 1 August 2014
Completed Jan 2015
B
B
B
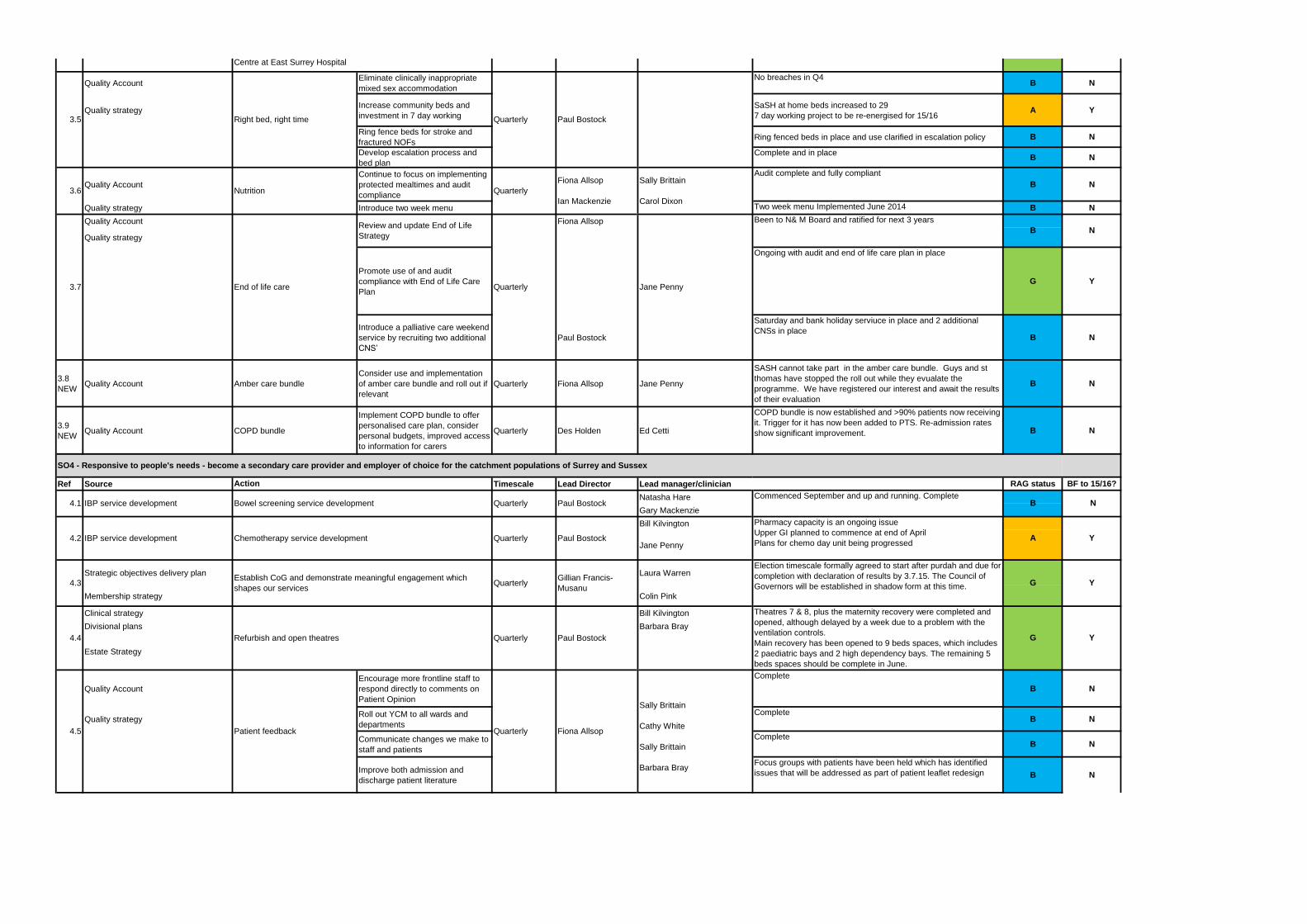
Quality AccountEliminate clinically inappropriate
mixed sex accommodation
No breaches in Q4B N
Quality strategyIncrease community beds and
investment in 7 day working
SaSH at home beds increased to 29
7 day working project to be re-energised for 15/16A Y
Ring fence beds for stroke and
fractured NOFsRing fenced beds in place and use clarified in escalation policy B N
Develop escalation process and
bed plan
Complete and in placeB N
Quality Account
Continue to focus on implementing
protected mealtimes and audit
compliance
Audit complete and fully compliant
B N
Quality strategy Introduce two week menu Two week menu Implemented June 2014 B N
Quality Account Fiona Allsop
Quality strategy
Promote use of and audit
compliance with End of Life Care
Plan
Ongoing with audit and end of life care plan in place
G Y
Introduce a palliative care weekend
service by recruiting two additional
CNS’
Paul Bostock
Saturday and bank holiday serviuce in place and 2 additional
CNSs in placeB N
3.8
NEWQuality Account Amber care bundle
Consider use and implementation
of amber care bundle and roll out if
relevant
Quarterly Fiona Allsop Jane Penny
SASH cannot take part in the amber care bundle. Guys and st
thomas have stopped the roll out while they evualate the
programme. We have registered our interest and await the results
of their evaluation
B N
3.9
NEWQuality Account COPD bundle
Implement COPD bundle to offer
personalised care plan, consider
personal budgets, improved access
to information for carers
Quarterly Des Holden Ed Cetti
COPD bundle is now established and >90% patients now receiving
it. Trigger for it has now been added to PTS. Re-admission rates
show significant improvement. B N
Ref Source Timescale Lead Director Lead manager/clinician RAG status BF to 15/16?
Natasha Hare
Gary Mackenzie
Bill Kilvington
Jane Penny
Strategic objectives delivery plan Laura Warren
Membership strategy Colin Pink
Clinical strategy Bill Kilvington
Divisional plans Barbara Bray
Estate Strategy
Quality Account
Encourage more frontline staff to
respond directly to comments on
Patient Opinion
Complete
B N
Quality strategyRoll out YCM to all wards and
departments
CompleteB N
Communicate changes we make to
staff and patients
CompleteB N
Improve both admission and
discharge patient literature
Focus groups with patients have been held which has identified
issues that will be addressed as part of patient leaflet redesign B N
G
SO4 - Responsive to people's needs - become a secondary care provider and employer of choice for the catchment populations of Surrey and Sussex
Been to N& M Board and ratified for next 3 years
Commenced September and up and running. Complete
Interviewing for centre manager April 2015
Turf cutting planned for 15 May 2015
Paul Bostock
Paul Bostock
G
Quarterly Paul Bostock
3.5 Right bed, right time Quarterly
G
Theatres 7 & 8, plus the maternity recovery were completed and
opened, although delayed by a week due to a problem with the
ventilation controls.
Main recovery has been opened to 9 beds spaces, which includes
2 paediatric bays and 2 high dependency bays. The remaining 5
beds spaces should be complete in June.
New Theatres 5 & 6 will be handed over on the 24th April to be
Sally Brittain
Cathy White
Sally Brittain
Barbara Bray
Election timescale formally agreed to start after purdah and due for
completion with declaration of results by 3.7.15. The Council of
Governors will be established in shadow form at this time.
3.6 Nutrition Quarterly
Fiona Allsop
Ian Mackenzie
Sally Brittain
Carol Dixon
3.4
Work with Olive Tree, Friends of east Surrey and Macmillan Cancer
Support to develop and implement a Cancer Information and Support
Centre at East Surrey Hospital
3.7 End of life care
Review and update End of Life
Strategy
Quarterly Jane Penny
Action
4.1 IBP service development
4.3Establish CoG and demonstrate meaningful engagement which
shapes our servicesQuarterly
4.2
Bowel screening service development Quarterly
IBP service development Chemotherapy service development
4.4 Refurbish and open theatres Quarterly Paul Bostock
Quarterly Paul Bostock
Gillian Francis-
Musanu
4.5 Patient feedback Quarterly Fiona Allsop
A
B
B
Pharmacy capacity is an ongoing issue
Upper GI planned to commence at end of April
Plans for chemo day unit being progressed
Y
Y
Y
N
N
Y
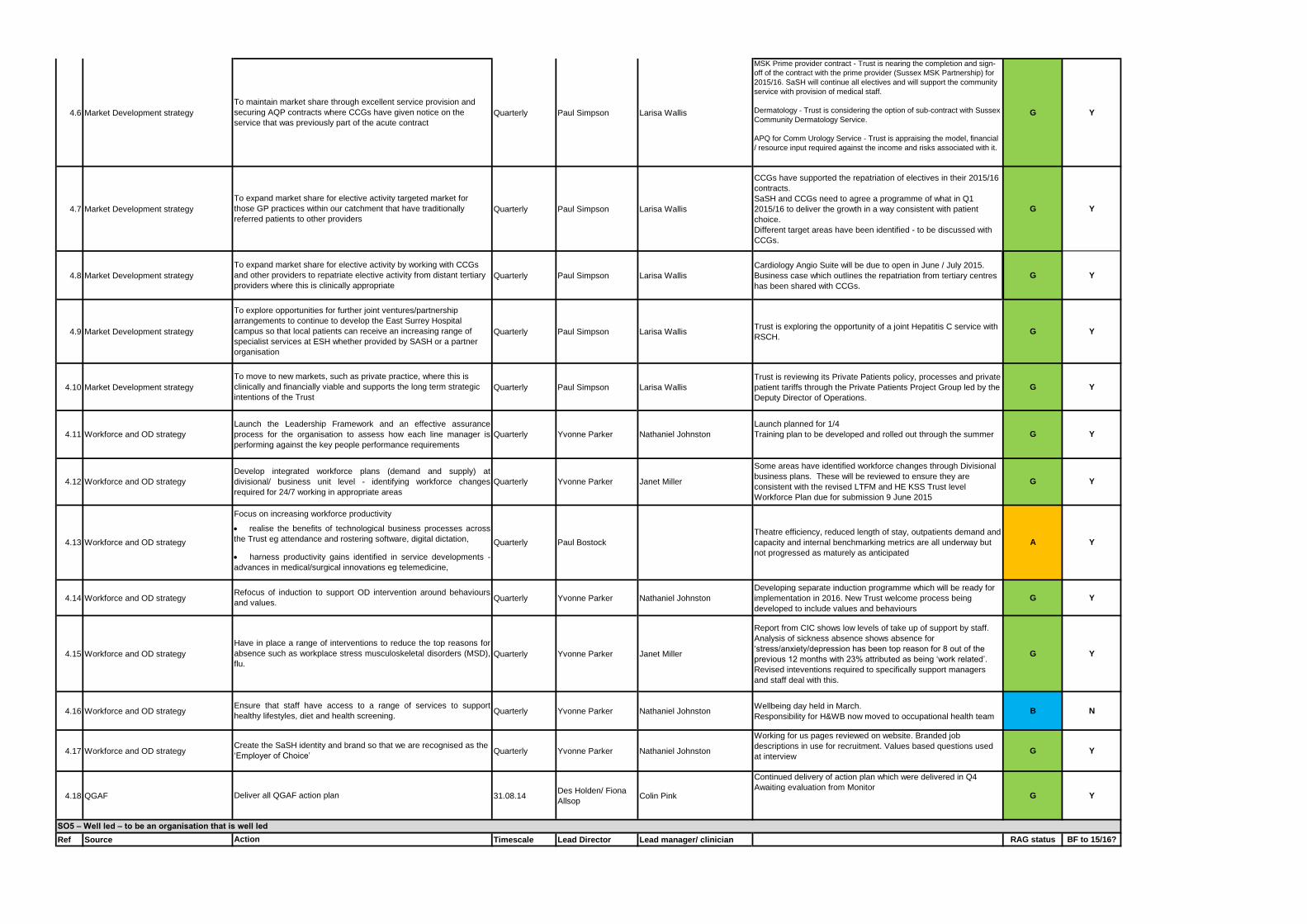
4.6 Market Development strategy Quarterly Paul Simpson Larisa Wallis
MSK Prime provider contract - Trust is nearing the completion and sign-
off of the contract with the prime provider (Sussex MSK Partnership) for
2015/16. SaSH will continue all electives and will support the community
service with provision of medical staff.
Dermatology - Trust is considering the option of sub-contract with Sussex
Community Dermatology Service.
APQ for Comm Urology Service - Trust is appraising the model, financial
/ resource input required against the income and risks associated with it.
G Y
4.7 Market Development strategy Quarterly Paul Simpson Larisa Wallis
CCGs have supported the repatriation of electives in their 2015/16
contracts.
SaSH and CCGs need to agree a programme of what in Q1
2015/16 to deliver the growth in a way consistent with patient
choice.
Different target areas have been identified - to be discussed with
CCGs.
G Y
4.8 Market Development strategy Quarterly Paul Simpson Larisa Wallis
Cardiology Angio Suite will be due to open in June / July 2015.
Business case which outlines the repatriation from tertiary centres
has been shared with CCGs.
G Y
4.9 Market Development strategy Quarterly Paul Simpson Larisa WallisTrust is exploring the opportunity of a joint Hepatitis C service with
RSCH.G Y
4.10 Market Development strategy Quarterly Paul Simpson Larisa Wallis
Trust is reviewing its Private Patients policy, processes and private
patient tariffs through the Private Patients Project Group led by the
Deputy Director of Operations.
G Y
4.14 Workforce and OD strategy Quarterly Yvonne Parker Nathaniel Johnston
Developing separate induction programme which will be ready for
implementation in 2016. New Trust welcome process being
developed to include values and behaviours
G Y
4.15 Workforce and OD strategy Quarterly Yvonne Parker Janet Miller
Report from CIC shows low levels of take up of support by staff.
Analysis of sickness absence shows absence for
‘stress/anxiety/depression has been top reason for 8 out of the
previous 12 months with 23% attributed as being ‘work related’.
Revised inteventions required to specifically support managers
and staff deal with this.
G Y
4.16 Workforce and OD strategy Quarterly Yvonne Parker Nathaniel JohnstonWellbeing day held in March.
Responsibility for H&WB now moved to occupational health teamB N
4.17 Workforce and OD strategy Quarterly Yvonne Parker Nathaniel Johnston
Working for us pages reviewed on website. Branded job
descriptions in use for recruitment. Values based questions used
at interview G Y
4.18 QGAF 31.08.14Des Holden/ Fiona
AllsopColin Pink
Continued delivery of action plan which were delivered in Q4
Awaiting evaluation from MonitorG Y
Ref Source Timescale Lead Director Lead manager/ clinician RAG status BF to 15/16?
Janet Miller
Nathaniel Johnston
A
G
G
Some areas have identified workforce changes through Divisional
business plans. These will be reviewed to ensure they are
consistent with the revised LTFM and HE KSS Trust level
Workforce Plan due for submission 9 June 2015
Theatre efficiency, reduced length of stay, outpatients demand and
capacity and internal benchmarking metrics are all underway but
not progressed as maturely as anticipated
Launch planned for 1/4
Training plan to be developed and rolled out through the summer
To maintain market share through excellent service provision and
securing AQP contracts where CCGs have given notice on the
service that was previously part of the acute contract
To expand market share for elective activity targeted market for
those GP practices within our catchment that have traditionally
referred patients to other providers
To expand market share for elective activity by working with CCGs
and other providers to repatriate elective activity from distant tertiary
providers where this is clinically appropriate
To explore opportunities for further joint ventures/partnership
arrangements to continue to develop the East Surrey Hospital
campus so that local patients can receive an increasing range of
specialist services at ESH whether provided by SASH or a partner
organisation
To move to new markets, such as private practice, where this is
clinically and financially viable and supports the long term strategic
intentions of the Trust
4.11 Workforce and OD strategy
Launch the Leadership Framework and an effective assurance
process for the organisation to assess how each line manager is
performing against the key people performance requirements
Yvonne Parker
4.12 Workforce and OD strategy
Develop integrated workforce plans (demand and supply) at
divisional/ business unit level - identifying workforce changes
required for 24/7 working in appropriate areas
Quarterly Yvonne Parker
Workforce and OD strategy
Focus on increasing workforce productivity
realise the benefits of technological business processes across
the Trust eg attendance and rostering software, digital dictation,
harness productivity gains identified in service developments -
advances in medical/surgical innovations eg telemedicine,
Quarterly
Quarterly
Deliver all QGAF action plan
Action
SO5 – Well led – to be an organisation that is well led
Paul Bostock
Refocus of induction to support OD intervention around behaviours
and values.
Have in place a range of interventions to reduce the top reasons for
absence such as workplace stress musculoskeletal disorders (MSD),
flu.
Ensure that staff have access to a range of services to support
healthy lifestyles, diet and health screening.
Create the SaSH identity and brand so that we are recognised as the
‘Employer of Choice’
4.13 Y
Y
Y
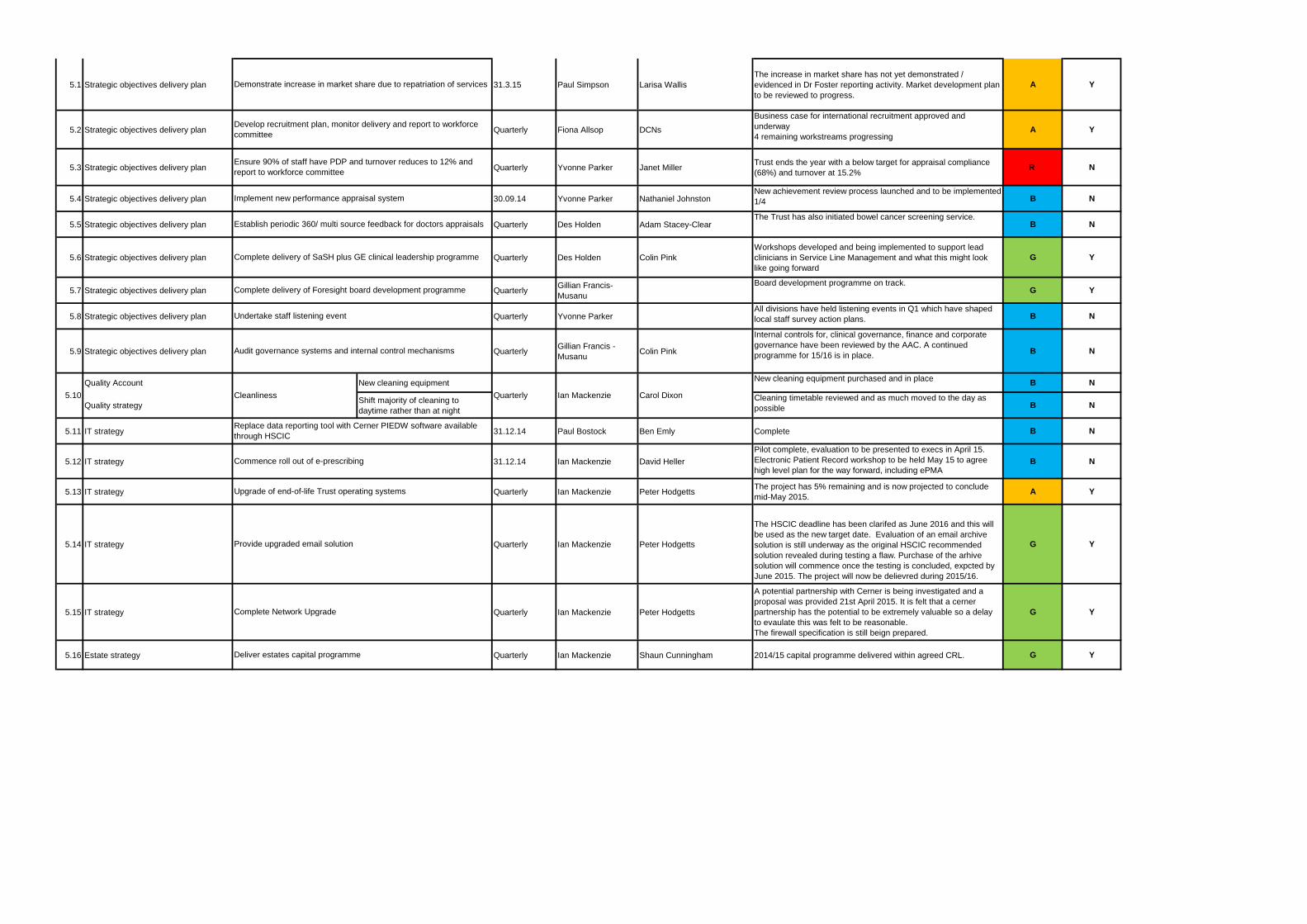
5.1 Strategic objectives delivery plan 31.3.15 Paul Simpson Larisa Wallis
The increase in market share has not yet demonstrated /
evidenced in Dr Foster reporting activity. Market development plan
to be reviewed to progress.
A Y
5.2 Strategic objectives delivery plan Quarterly Fiona Allsop DCNs
Business case for international recruitment approved and
underway
4 remaining workstreams progressingA Y
5.3 Strategic objectives delivery plan Quarterly Yvonne Parker Janet MillerTrust ends the year with a below target for appraisal compliance
(68%) and turnover at 15.2%R N
5.4 Strategic objectives delivery plan 30.09.14 Yvonne Parker Nathaniel JohnstonNew achievement review process launched and to be implemented
1/4 B N
5.5 Strategic objectives delivery plan Quarterly Des Holden Adam Stacey-ClearThe Trust has also initiated bowel cancer screening service.
B N
5.6 Strategic objectives delivery plan Quarterly Des Holden Colin Pink
Workshops developed and being implemented to support lead
clinicians in Service Line Management and what this might look
like going forward
G Y
5.7 Strategic objectives delivery plan QuarterlyGillian Francis-
Musanu
Board development programme on track.G Y
5.8 Strategic objectives delivery plan Quarterly Yvonne ParkerAll divisions have held listening events in Q1 which have shaped
local staff survey action plans. B N
5.9 Strategic objectives delivery plan QuarterlyGillian Francis -
MusanuColin Pink
Internal controls for, clinical governance, finance and corporate
governance have been reviewed by the AAC. A continued
programme for 15/16 is in place. B N
Quality Account New cleaning equipment New cleaning equipment purchased and in place
B N
Quality strategyShift majority of cleaning to
daytime rather than at night
Cleaning timetable reviewed and as much moved to the day as
possible B N
5.11 IT strategy 31.12.14 Paul Bostock Ben Emly Complete B N
5.12 IT strategy 31.12.14 Ian Mackenzie David Heller
Pilot complete, evaluation to be presented to execs in April 15.
Electronic Patient Record workshop to be held May 15 to agree
high level plan for the way forward, including ePMAB N
5.13 IT strategy Quarterly Ian Mackenzie Peter HodgettsThe project has 5% remaining and is now projected to conclude
mid-May 2015.A Y
5.14 IT strategy Quarterly Ian Mackenzie Peter Hodgetts
The HSCIC deadline has been clarifed as June 2016 and this will
be used as the new target date. Evaluation of an email archive
solution is still underway as the original HSCIC recommended
solution revealed during testing a flaw. Purchase of the arhive
solution will commence once the testing is concluded, expcted by
June 2015. The project will now be delievred during 2015/16.
G Y
5.15 IT strategy Quarterly Ian Mackenzie Peter Hodgetts
A potential partnership with Cerner is being investigated and a
proposal was provided 21st April 2015. It is felt that a cerner
partnership has the potential to be extremely valuable so a delay
to evaulate this was felt to be reasonable.
The firewall specification is still beign prepared.
G Y
5.16 Estate strategy Quarterly Ian Mackenzie Shaun Cunningham 2014/15 capital programme delivered within agreed CRL. G Y
5.10 Cleanliness
Demonstrate increase in market share due to repatriation of services
Develop recruitment plan, monitor delivery and report to workforce
committee
Ensure 90% of staff have PDP and turnover reduces to 12% and
report to workforce committee
Implement new performance appraisal system
Establish periodic 360/ multi source feedback for doctors appraisals
Deliver estates capital programme
Quarterly Ian Mackenzie Carol Dixon
Replace data reporting tool with Cerner PIEDW software available
through HSCIC
Commence roll out of e-prescribing
Upgrade of end-of-life Trust operating systems
Provide upgraded email solution
Undertake staff listening event
Complete Network Upgrade
Audit governance systems and internal control mechanisms
Complete delivery of SaSH plus GE clinical leadership programme
Complete delivery of Foresight board development programme
TRUST BOARD IN PUBLIC
Date: 30th April 2015 Agenda Item: 4.5
REPORT TITLE: BOARD GOVERNANCE SELF- CERTIFICATION
EXECUTIVE SPONSOR: Gillian Francis-Musanu Director of Corporate Affairs
REPORT AUTHOR (s): Gillian Francis-Musanu Director of Corporate Affairs
REPORT DISCUSSED PREVIOUSLY: (name of sub-committee/group & date) N/A
Action Required:
Approval (√) Discussion (√) Assurance (√)
Purpose of Report:
As part of the Monitor assessment process and in accordance with the application process for foundation trust status, the Board of Directors is required to certify compliance with risk and performance management.
Summary of key issues
Monitor’s assessment process ensures financially sustainable, well-governed NHS foundation trusts with responsible management are established. As part of this process trusts are required to provide certification that the Trust has the organisational capacity to deliver the business plan and that plans are in place to ensure ongoing compliance with the conditions of the Provider Licence. This paper outlines Monitor’s requirements for self-certification and the evidence in place to support the Boards self-certification of compliance. In addition compliance with the Monitor Provider Licence has also been assessed
Recommendation:
Board is asked to support the signing of the Board Statement and certification.
Relationship to Trust Strategic Objectives & Assurance Framework:
SO1: Safe -Deliver safe services and be in the top 20% against our peers SO2: Effective - Deliver effective and sustainable clinical services within the local health economy SO3: Caring – Ensure patients are cared for and feel cared about SO4: Responsive – Become the secondary care provider and employer of choice our catchment population SO5: Well led: Become an employer of choice and deliver financial and clinical sustainability around a clinical leadership model
Corporate Impact Assessment:
Legal and regulatory impact A requirement of the Foundation Trust application process
2
Financial impact This is included in the report
Patient Experience/Engagement N/A
Risk & Performance Management These elements are included in the report
NHS Constitution/Equality & Diversity/Communication
This report will be accessible on the Trust website
Attachment:
Appendix 1 – Board Statements Appendix 2 – Assessment of Monitor Provider Licence Appendix 3 – Monitor Risk Assessment of Joint Ventures & AHSC Appendix 4 – Monitor Access targets and outcomes framework
3
TRUST BOARD REPORT – 30th APRIL 2015 BOARD GOVERNANCE SELF CERTIFICATION STATEMENTS 1. Introduction Monitor’s assessment process ensures financially sustainable, well-governed NHS foundation trusts with responsible management are established. As part of this process trusts are required to provide certification that the Trust has the organisational capacity to deliver the business plan and that plans are in place to ensure ongoing compliance with the conditions of the Provider Licence. This paper outlines Monitor’s requirements for self-certification and the evidence in place to support this and also compliance with the Provider Licence. 2. Monitor Board Statements & Self Certification Requirements iMonitor’s Applying for NHS foundation trusts status – A guide for applicants (Oct 2013) as defined below: 2.1 Section 5.3.2.2 – Does the trust board believe that the trust has the
organisational capacity to deliver the business plan? This includes: • Is the trust board confident that the senior management has the capability and
experience necessary to deliver the strategy? • Is a selection process in place to ensure that non-executive directors have the
appropriate experience and skills? • Are adequate management structures in place to deliver the strategy? • Are the necessary management processes in place to deliver the strategy? • Performance management, risk management and planning processes 2.2 Section 5.3.2.3 – How is the applicant performing against the quality
performance threshold? This includes: • CQC registration status and CQC’s judgement of compliance • NHS TDA threshold • Governance Risk Rating • How the board is assured that it has action plans in place to meet existing targets and
registration requirements The self-certification wording is defined within Appendix B12 of the guide for applicants. Appendix 1 of this paper provides for each of the 14 required statements the level of compliance and the key supporting evidence. Appendix 2 defines compliance with the Provider Licence. The Trust is compliant with all statements and is not at risk of non-compliance regarding the Provider Licence. Monitor also require a letter from the Chair confirming that the whole Trust Board has confidence in the arrangements it has in place for each of these areas accompanied by the relevant Board paper and minutes. These will be prepared following Board approval of the attached statements.
4
3. Other Monitor Self-Certification Requirements Quality Governance A Board statement in the form of a letter from the Chair supported by the whole Trust Board together with a detailed board memorandum which describes quality governance arrangements in the Trust was submitted to Monitor on 27th March 2015. Financial Viability A Board statement on working capital and financial reporting procedures with a supporting board memorandum is due for submission following HDD assessment has been undertaken by an independent accountancy firm. 4. Recommendation Following review and discussion, the Board is asked to support the signing of the Board Statement and self-certification. Gillian Francis-Musanu Director of Corporate Affairs & Company Secretary April 2015
Appendix 1 – BOARD STATEMENTS
Defined by Appendix B12 – Monitor Applying for NHS Foundation Trust Status For each statement the Board is asked to confirm the following: Board Statement Level of
Compliance Narrative & Evidence to Support Statement
1 The board is satisfied that plans in place are sufficient to ensure ongoing compliance with the Care Quality Commission’s registration requirements.
Compliant Unconditional CQC Registration “Good” Rating in all five domains following Chief Inspector of
Hospitals (CIH) Inspection in May 2014 with End of Life Care rated as “Outstanding”.
Out Patient Services was rated as “requires improvement” and the Board receives monthly progress reports on the improvement plan with a significant number of actions rated as complete
Functioning of executive sub-committees and associated systems reporting through Executive Committee for Quality and Risk (ECQR) through to the Safety & Quality Committee and up to the Board
ECQR developing a system for monitoring new CQC Fundamental Standards of Care
CQC Intelligent Monitoring at band 6 SQC’s role in monitoring and assurance on quality and safety
Evidence: CIH Report, CQC Improvement Plan reports, Board agendas and minutes, CQC Intelligent Monitoring report, SQC terms of reference, ECQR minutes, sub-committee minutes and reports
2 The board is satisfied that processes and procedures are in place to ensure all health care professionals providing care on behalf of the trust have met the relevant registration and revalidation
Compliant Professional registration is checked at offer of employment and upon commencement
On-going registration assurance process in place through HR Responsible Officer for Revalidation reports to the Board on
compliance with medical practitioner revalidation and the
6
requirements.
Annual Organisational Audit (AOA) submission to NHS England in place with 98% consultant appraisal rate.
Evidence: HR Employment checks, NHE submissions, Board agenda, reports and minutes
3 Issues and concerns raised by external audit and external assessment groups (including reports for NHS Litigation Authority assessments) have been addressed and resolved. Where any issues or concerns are outstanding, the board is confident that there are appropriate action plans in place to address the issues in a timely manner.
Compliant Trust Board & Safety & Quality Committee (SQC) review of CQC improvement plan
Role of Audit & Assurance Committee (AAC) in monitoring outcomes and actions following external audit reports
Role of the SQC in monitoring and seeking assurance on the outcome of CQC and any NHSLA inspections, implementation of improvement plans and cross-organisational learning
Deep Dive process and reporting of actions to SQC. AAC’s role in systematic review of systems of internal control Evidence: Maternity CNST Level 2, SQC papers and minutes, Deep Dive progress reports, board reports and minutes.
4 All recommendations to the board from the audit committee are implemented in a timely and robust manner and to the satisfaction of the body concerned.
Compliant Strengthened monitoring of all internal audits with provision of assurance and escalation of on-going risk to the AAC
Monthly internal audit (IA) tracker Reports from AAC Chair to the Board which include actions
taken on behalf of the Board Evidence: Audit Committee and Board minutes and papers, Head of Internal Audit Annual Opinion, IA audit monthly tracker
5 The necessary planning, performance management and risk management processes are in place to deliver the
Compliant Role of the Executive Committee for Quality & Risk (ECQR) and its sub-committees specifically the Access & Responsiveness Committee reports directly to SQC to ensure quality and
7
integrated business plan, including but not restricted to: a. obtaining and disseminating accurate, comprehensive, timely and up-to-date information for board and committee decision-making;
b. the timely and effective scrutiny and oversight by the board of the trust’s operations;
c. effective financial decision making, management and control; and
d. taking appropriate account of quality of care considerations.
performance information is reviewed by the Board has been defined, targets set, reporting lines established and assurance on action to improve quality
integrated Quality and Performance Report reported to the Trust Board monthly
Board Assurance Framework & Risk Appetite reporting to the Board and sub-committees
Strengthened processes for the development, approval and monitoring of Cost Improvement Plans (CIPs) which is reviewed by the Finance and Workforce Committee and reported to the Board on a monthly basis. Monitoring is also undertaken by the Executive Committee
Financial decision making and management control is scrutinised and reviewed by the Finance & Workforce Committee and Financial reporting to the Audit & Assurance Committee
Implementation of the Board Assurance Framework which is reviewed by the Executive Committee, the role of the AAC and approved by the Board
Executive Committee which co-ordinates the development of the Trust and Division IBPs, Directorate Annual Business Plans and enabling strategies
Trusts Strategic objectives Evidence: IPQR, Strategic objectives, strategic intent, review of the IBP, FWC agenda and minutes, CIP reports to the Board and FWC, SQC papers & minutes, ECQR papers and minutes, ECQR & sub-committee structure, BAF, Risk Appetite, SRR, ECQR sub-committee reports, Quality Account 2013/14
6 An annual governance statement is in place, and the trust is compliant with the risk management and assurance
Compliant Annual Governance Statement (AGS) included and signed off as part of the Annual Accounts in June 2014, current AGS in draft for 14/15
8
framework requirements that support the statement pursuant to the most up-to-date guidance from HM Treasury (www.hm-treasury.gov.uk).
Head of Internal Audit Opinion provided significant assurance AGS included in the Trust’s Annual Report
Evidence: Audit Committee Chair reports, AAC minutes, Annual Report, AGS submission to the TDA
7 The board is satisfied that plans in place are sufficient to ensure: ongoing compliance with all existing access and outcomes metrics (after the application of thresholds) as set out in Appendix A of the Risk assessment framework; and all known access and outcomes metrics going forwards
Compliant • The Trust has met and continues to meet access and outcomes metrics
• Board reviews performance on access and outcome metrics on a monthly basis through the Integrated Performance Report
• The Access and Responsiveness sub-committee and the Clinical Effectiveness Committee provide governance over delivery with discussion and weekly reporting to the Executive Committee
• Performance is also reported to the SQC Evidence: Monthly Integrated Performance Reports, Access and responsiveness monthly reports, Clinical Effectiveness monthly reports, SQC minutes and reports
8 The trust has achieved a minimum of Level 2 performance against the requirements of the Information Governance Toolkit.
Compliant Information Governance Toolkit (IGT) score 72% for 2014/15 Level 2 achieved with some criteria at Level 3 Evidence: • Safety & Quality Committee minutes and papers, IGT submission
9 The board has in place a register of interests, ensuring that there are no material conflicts of interest in the board of directors; that all board positions are filled, or plans are in place to ensure any board vacancies are filled
Compliant • Board Register of Interests refreshed annually • Declarations of Interest is a standing Board agenda item • Two non-executive vacancies filled during 2014/15 • No current vacancies on the Board Evidence: Board Annual Register of Interests
9
10 The board is satisfied that all executive and non-executive directors have the appropriate qualifications, experience and skills to discharge their functions effectively, including setting strategy, monitoring and managing performance and risks, and ensuring management capacity and capability.
Compliant • Job descriptions as defined in Appendix B16 of Monitor’s Guide for Applicants for the Chair, Chief Executive and Director of Finance defining the skills and experience required are in place
• Chief Executive & Executive Directors have regular management meetings and appraisals at least annually
• Job descriptions as defined in Appendix B16 of Monitor’s Guide for Applicants for non-executive directors (NEDs) defining the skills and experience required are in place
• Assessment against NHS TDA Non Executive Team skills template informed NED recruitment
• NEDs have regular performance reviews with the Chair • Board Development Programme • Board Governance Assurance Framework & Memorandum,
Deloitte BGAF report and Board Action Plan Evidence: BGAF external report, BGAF Action Plan, CEO, Chair, CFO Job Descriptions, Board profiles, Diversity of skills on the Board, Board skills audit
11 The selection process and training programmes in place ensure that the non-executive directors have appropriate experience and skills.
Compliant • Job descriptions as defined in Appendix B16 of Monitor’s Guide for Applicants for non-executive directors defining the skills and experience required are in place
• The recruitment process for two non-executive directors (NEDs) in 2014/15 demonstrate consideration was given to the skills and experience required reflecting the composition of Board and its sub-committee’s
• Induction programme for newly appointed NEDs • Board review of quality and escalation framework • Board development programme Evidence: NED induction programme, NED job descriptions, Board review of quality & escalation framework, board skills audit, Board
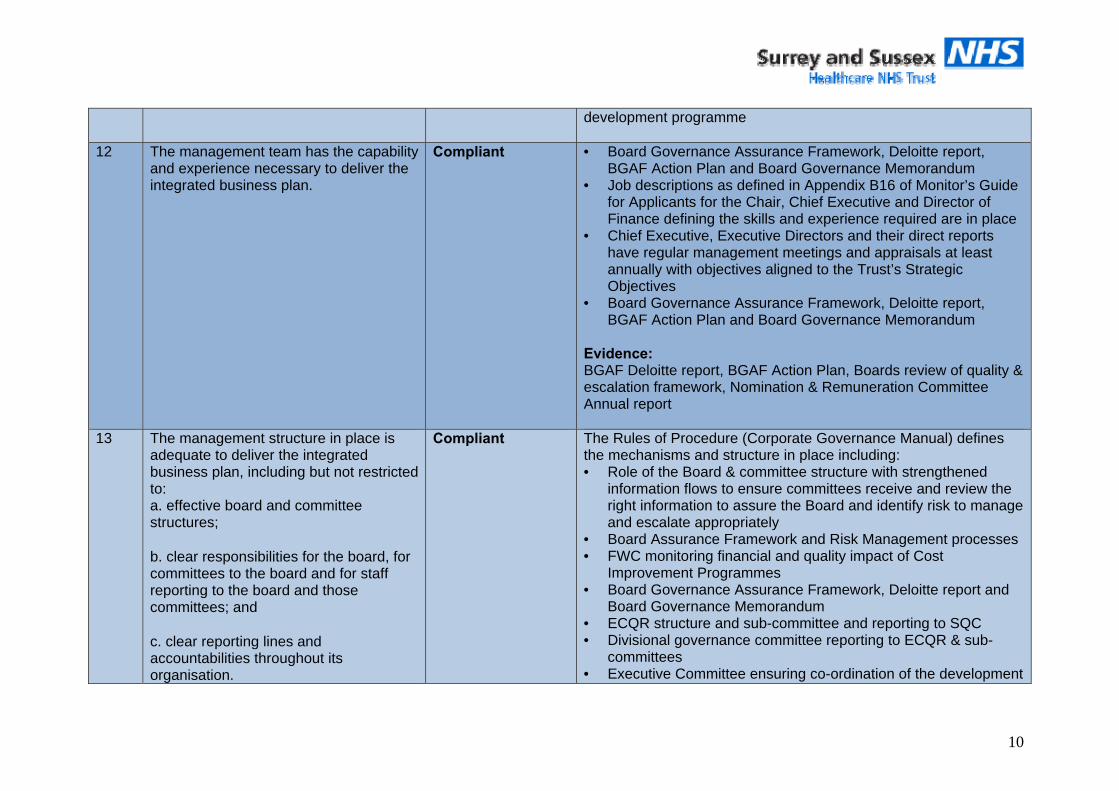
10
development programme
12 The management team has the capability and experience necessary to deliver the integrated business plan.
Compliant • Board Governance Assurance Framework, Deloitte report, BGAF Action Plan and Board Governance Memorandum
• Job descriptions as defined in Appendix B16 of Monitor’s Guide for Applicants for the Chair, Chief Executive and Director of Finance defining the skills and experience required are in place
• Chief Executive, Executive Directors and their direct reports have regular management meetings and appraisals at least annually with objectives aligned to the Trust’s Strategic Objectives
• Board Governance Assurance Framework, Deloitte report, BGAF Action Plan and Board Governance Memorandum
Evidence: BGAF Deloitte report, BGAF Action Plan, Boards review of quality & escalation framework, Nomination & Remuneration Committee Annual report
13 The management structure in place is adequate to deliver the integrated business plan, including but not restricted to: a. effective board and committee structures;
b. clear responsibilities for the board, for committees to the board and for staff reporting to the board and those committees; and
c. clear reporting lines and accountabilities throughout its organisation.
Compliant The Rules of Procedure (Corporate Governance Manual) defines the mechanisms and structure in place including: • Role of the Board & committee structure with strengthened
information flows to ensure committees receive and review the right information to assure the Board and identify risk to manage and escalate appropriately
• Board Assurance Framework and Risk Management processes • FWC monitoring financial and quality impact of Cost
Improvement Programmes • Board Governance Assurance Framework, Deloitte report and
Board Governance Memorandum • ECQR structure and sub-committee and reporting to SQC • Divisional governance committee reporting to ECQR & sub-
committees • Executive Committee ensuring co-ordination of the development
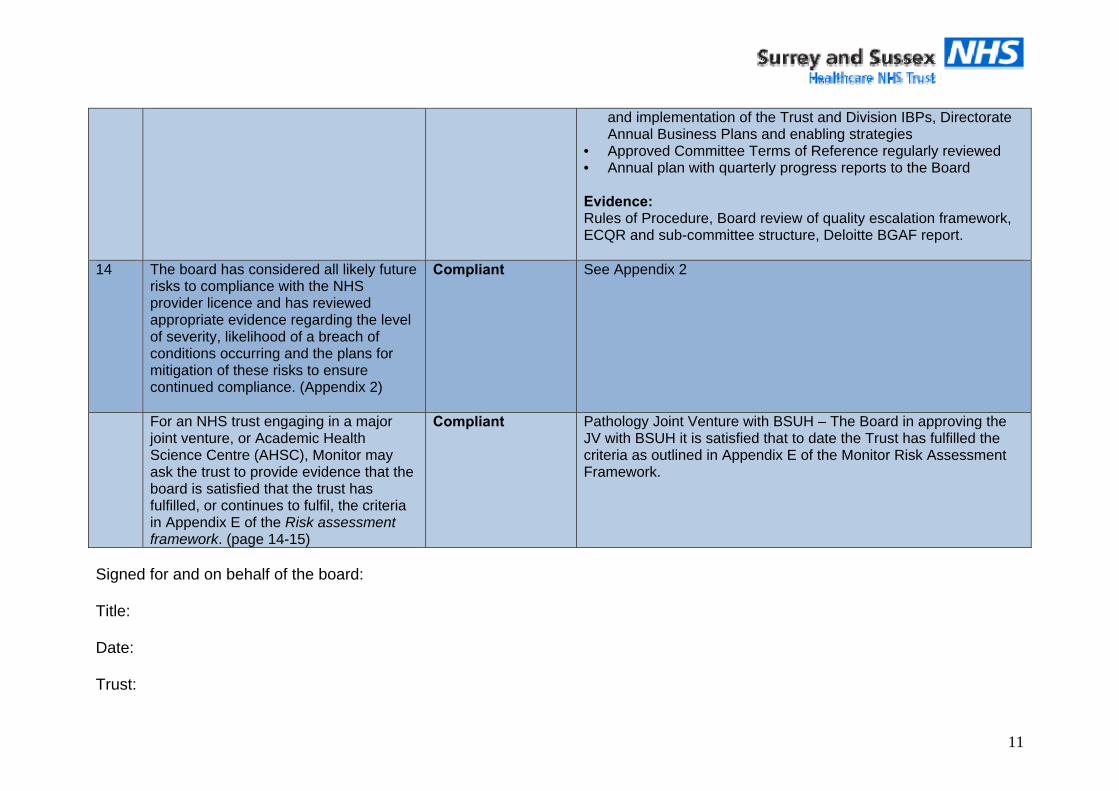
11
and implementation of the Trust and Division IBPs, Directorate Annual Business Plans and enabling strategies
• Approved Committee Terms of Reference regularly reviewed • Annual plan with quarterly progress reports to the Board Evidence: Rules of Procedure, Board review of quality escalation framework, ECQR and sub-committee structure, Deloitte BGAF report.
14 The board has considered all likely future risks to compliance with the NHS provider licence and has reviewed appropriate evidence regarding the level of severity, likelihood of a breach of conditions occurring and the plans for mitigation of these risks to ensure continued compliance. (Appendix 2)
Compliant See Appendix 2
For an NHS trust engaging in a major joint venture, or Academic Health Science Centre (AHSC), Monitor may ask the trust to provide evidence that the board is satisfied that the trust has fulfilled, or continues to fulfil, the criteria in Appendix E of the Risk assessment framework. (page 14-15)
Compliant Pathology Joint Venture with BSUH – The Board in approving the JV with BSUH it is satisfied that to date the Trust has fulfilled the criteria as outlined in Appendix E of the Monitor Risk Assessment Framework.
Signed for and on behalf of the board: Title: Date: Trust:
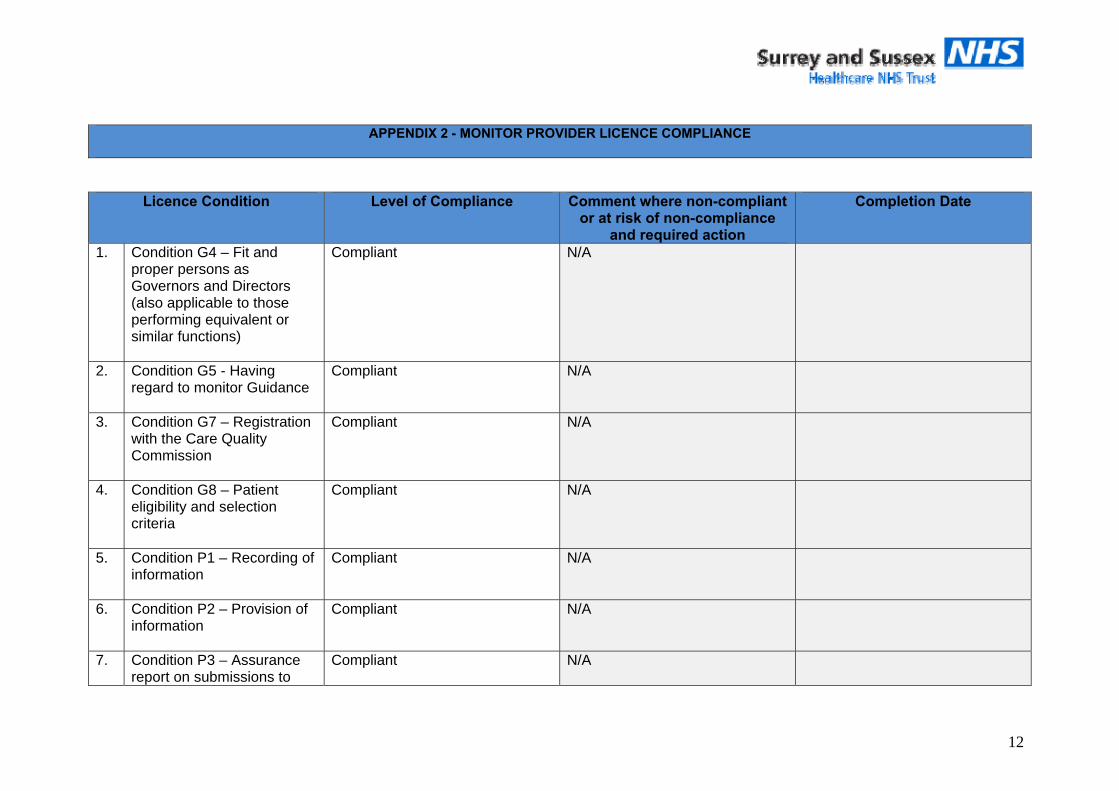
12
APPENDIX 2 - MONITOR PROVIDER LICENCE COMPLIANCE
Licence Condition Level of Compliance Comment where non-compliant or at risk of non-compliance
and required action
Completion Date
1. Condition G4 – Fit and proper persons as Governors and Directors (also applicable to those performing equivalent or similar functions)
Compliant N/A
2. Condition G5 - Having regard to monitor Guidance
Compliant N/A
3. Condition G7 – Registration with the Care Quality Commission
Compliant N/A
4. Condition G8 – Patient eligibility and selection criteria
Compliant N/A
5. Condition P1 – Recording of information
Compliant N/A
6. Condition P2 – Provision of information
Compliant N/A
7. Condition P3 – Assurance report on submissions to
Compliant N/A
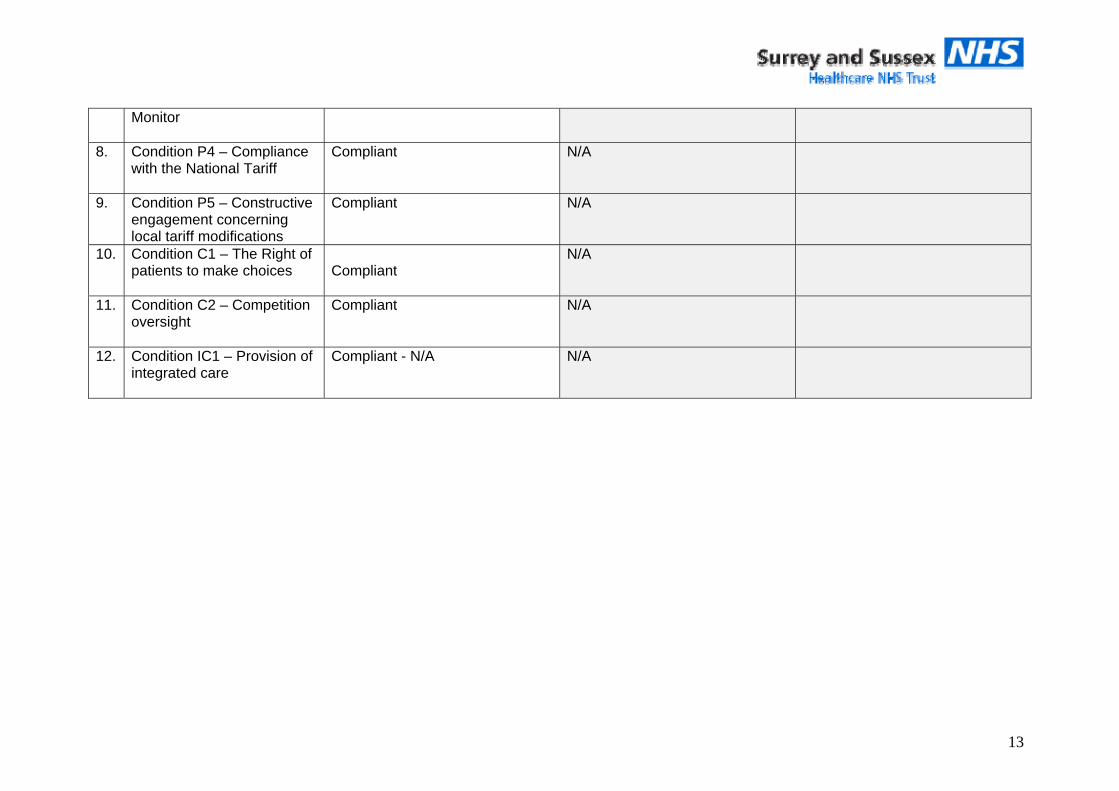
13
Monitor
8. Condition P4 – Compliance with the National Tariff
Compliant N/A
9. Condition P5 – Constructive engagement concerning local tariff modifications
Compliant
N/A
10. Condition C1 – The Right of patients to make choices
Compliant
N/A
11. Condition C2 – Competition oversight
Compliant N/A
12. Condition IC1 – Provision of integrated care
Compliant - N/A N/A
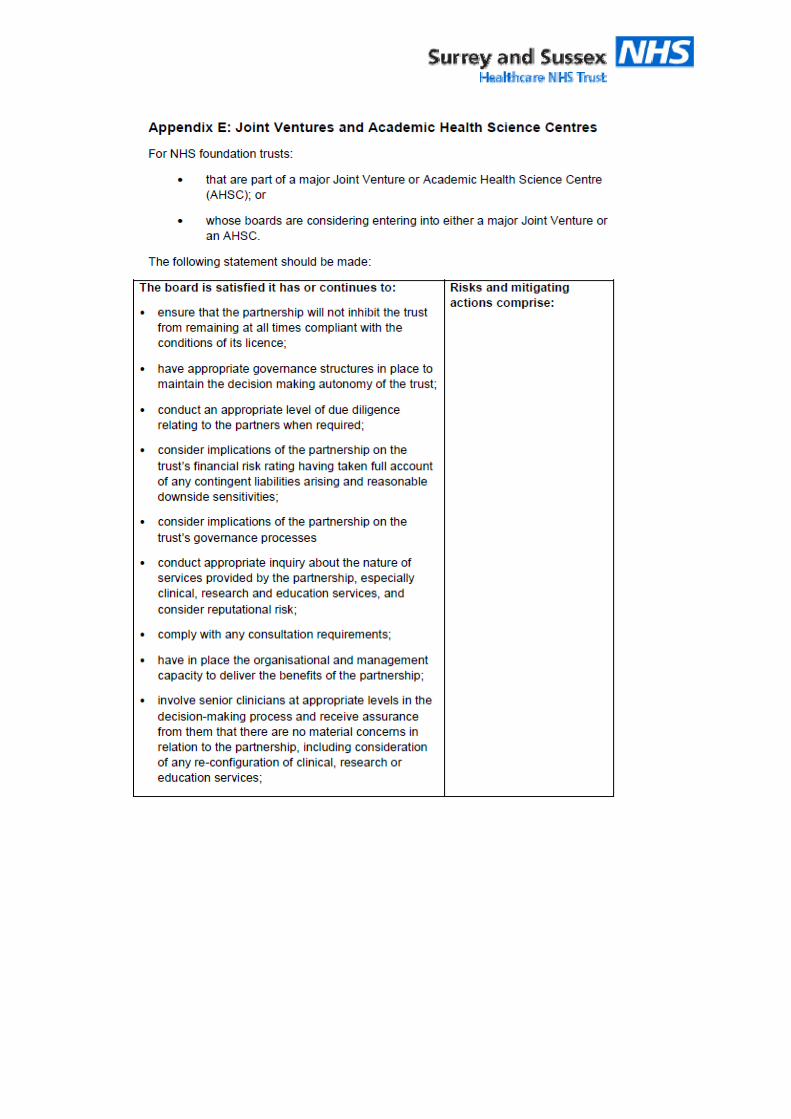
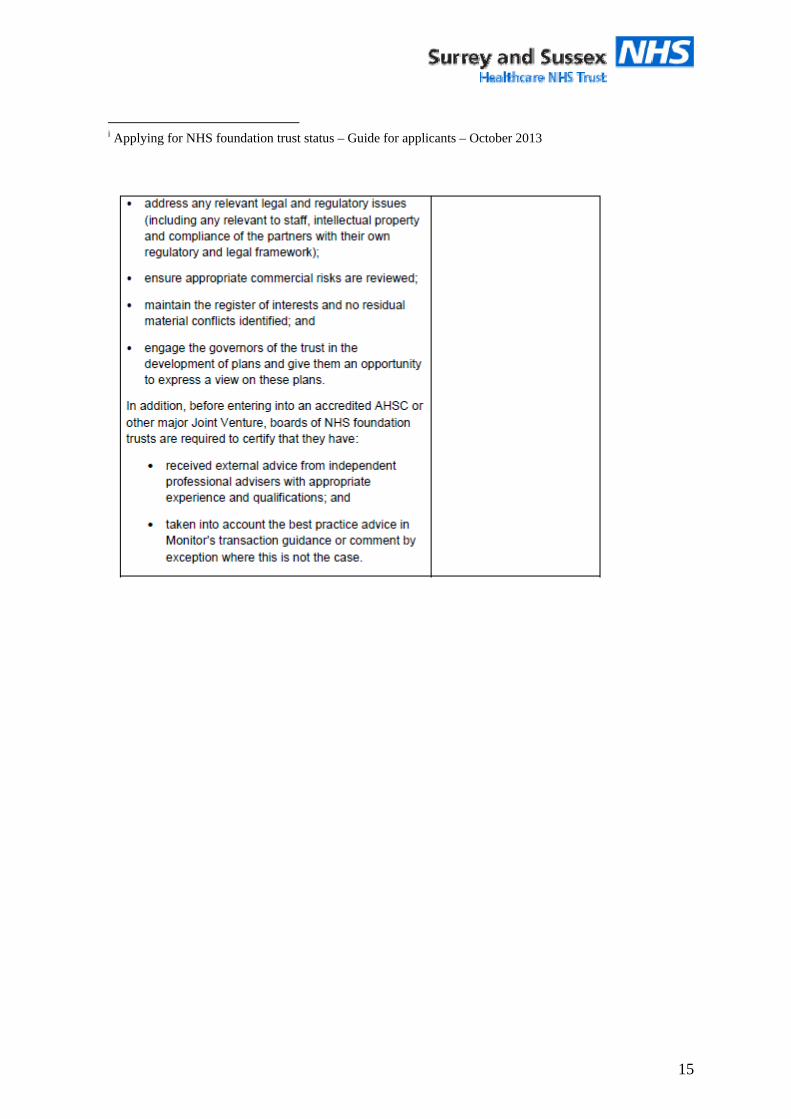
15
i Applying for NHS foundation trust status – Guide for applicants – October 2013
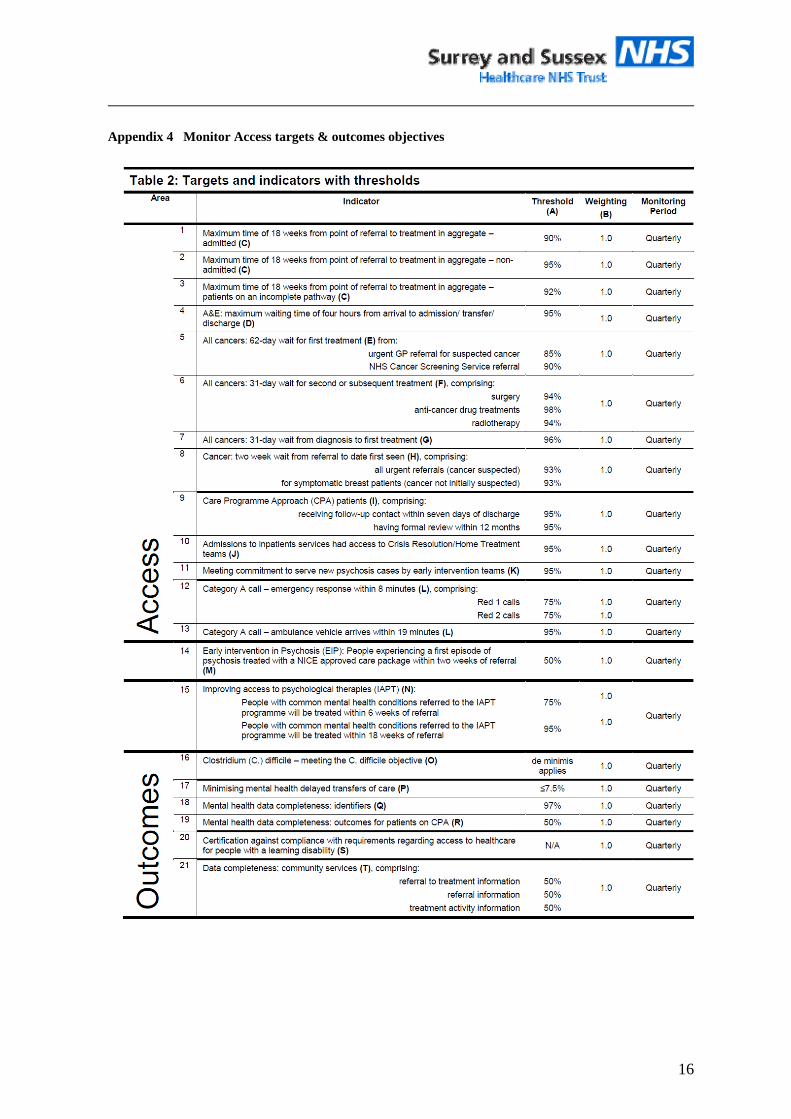
16
Appendix 4 Monitor Access targets & outcomes objectives
SQC Minutes 5th February 2015
Page 1 of 10
Safety & Quality Committee
Thursday 5th March 2015 14.00 - 16.00 AD77 Trust Headquarters, East Surrey Hospital
Minutes of Meeting
Present: Richard Shaw RS Non-Executive Director (Chair) Yvette Robbins YR Deputy Chair, Non-Executive Director Pauline Lambert PL Non-Executive Director Paul Simpson PS Chief Financial Officer Paul Bostock PB Chief Operating Officer
Fiona Allsop FA Chief Nurse Barbara Bray BB Chief of Surgery Bruce Stewart BS Chief of CSS Debbie Pullen DP Chief of WACH Jonathan Parr JP Clinical Governance Compliance
Manager Katharine Horner KH Patient Safety & Risk Lead Ben Emly BE Head of Performance
Ashley Flores AF Lead Nurse & Deputy DIPC Michele Cudjoe MC Michelle Cudjoe Denise Newman DN Denise Newman Apologies
Des Holden, Michael Wilson, Virach Phongsathorn, Karen Devanny, Victoria Daley, Colin Pink, Ed Cetti
Action 1 GENERAL BUSINESS
1.1. Chair welcomed everyone to the meeting and apologies were noted.
1.2. Minutes of the previous meeting RS asked for an amendment to page 5: Take assurance from the actions being taken to manage a difficult set of pressures but was concerned that that a higher risk was falling on the hospital trust as a result. Otherwise the January meeting minutes where agreed as an accurate record.
KH
1.3. Actions from previous meeting were discussed as follows C/F 2nd October 2014
• On the agenda
C/F 4th December 2014
• PB reported that an audit had been conducted for CQUIN on patients
SQC Minutes 5th February 2015
Page 2 of 10
discharged between 18:00 and 07:00 on 4 elderly care wards and 2 orthopaedic wards over 2 quarters. The conclusion was that very few patients were discharged after 20:00 and even fewer after 22:00. The audit has been sent to the CCG for their view. PB offered to bring the audit results and the CCG view back to a future SQC. RS made the point that SQC would be looking for assurance that there was appropriate provision made for each of the patients discharged within these hours. BE added that Q4 would be audited to see if any improvements had been made. Audit to be reported at the March meeting.
• All other items due March 2015 C/F 8th January 2015
• A&E survey has been deferred to the March meeting because it needs to go to Patient Experience Committee first.
• PS had raised the question as to whether there was reliable data on falls per 1,000 bed days going back 5 years to get a better trend analysis to assess whether the recent changes made have impacted the numbers. FA made the point that it needs to be falls with harm. BE explained that the bed data is reliable back to 2012. FA suggested looking at 2011/12, 2012/13 and 2013/14, total falls and falls with harm.
• RS suggested that the improvements made to Capel (old Godstone patients) be built into the next Falls report, for the June meeting.
PB
FA BE FA
COMMITTEE BUSINESS
1.2.1 Highlights from Executive Committee for Quality, Risk YR referred to page 5 section 2.3c (Patient Opinion results for WACH) asked what was being done to address the adverse comments that had been posted by dissatisfied patients. MC explained that the Division will endeavor to identify the each of the women concerned, make contact and offer a meeting to resolve any outstanding issues that the women may have with the care that they received. MC has met with two of the women and established contact with a third. She acknowledged that they have not then updated Patient Opinion which she accepted is important from the point of view of reassuring future patients. The issues raised relate to environment and attitude of staff. The environment for some women has not been ideal due to capacity issues, leading to issues of privacy and dignity. With regard to attitude, MC sent out a letter before Christmas to all staff to reinforce Trust values, and is picking up a number of issues with individual members of staff. MC will request access to Patient Opinion from the Communications department. FA reported that a meeting has been set up with Communications to increase the number members of staff who have access to the system and assess whether any training is required. Action: FA to report back in April on the action being taken.
FA
SQC Minutes 5th February 2015
Page 3 of 10
2.3b RS asked about the post Christmas performance review. PB reported that the meeting had taken place. The meeting looked at the impact of the pressures on the Trust as a whole and then each of the Divisions reported on their own experiences. An assessment has been made of what might be done differently in the future. The feedback will be formalised in a report to the Board and this will include the impact of cancellations. RS asked that the data includes the impact on the ability of the Trust to get stroke patients a bed within 4 hours and the fractured neck of femur pathway. DP reported the pressures that paediatrics had faced which, it was acknowledged, doesn’t always receive the same attention as the adult pathway. This caused problems in flow, safety, quality, potential breaches in ED, extra registrars for a month, to provide senior input, which is a cost pressure, and pressure on intensive care beds. P4 2.1 - YR asked for confirmation on the report of the Virginia Mason project, which essentially established a Virginia Mason “way” through standardized processes and reduction of variation. This had caused some staff at Virginia Mason Hospital to leave. PB asked for clarification on 3.1 VTE risk assessments. BE explained that CDU do not use the primary system that the rest of the Trust uses to capture the data. The Trust is required to report the aggregate performance, the target is 95%. The performance is varied and relies on validation. JP reported that the Thrombosis Committee reformed 3 months ago and is reviewing this. They will report to the Clinical Effectiveness Committee.
1.2.2 Highlights from CQRM The last meeting was held on 20th January. PS reported back to the CCGs on the A&E issues faced by the Trust over Christmas to provide assurance. The update from the CCGs on the CQC action plan was brief; VD had written to the Trust Board (as discussed at Trust Board). Surrey provided an update on RAPSID the “discharge to assess” project group which is chaired by the Trust. PS also reported to the CCGs that the Trust is now classified within the SNAP audit as a category B Trust. He informed them that the two items which are preventing the Trust from achieving level A status is timely access to the ward (because of emergency demand) and the lack of early supported discharge, particularly on the Surrey side. Nothing has been escalated from that meeting to the Single Performance Conversation. At the single performance conversation the Chief Officers discussed the marginal rate emergency tariff and early supported discharge for stroke. The Trust had agreed to provide information to cost the stroke pathway, to demonstrate the cost of the service. The costings were compared with the tariff and on an average basis the tariff does not cover the cost. The Trust declined to share
SQC Minutes 5th February 2015
Page 4 of 10
this information with the CCGs at this point because work on this appears to have taken a different direction - East Surrey CCG has written to the Trust to advise that they will stop purchasing community beds and will stop early supported discharge for stroke, trauma and orthopedics (for financial reasons). The Trust will review this position and continues working with Sussex CCGs on their work around the stroke pathway. .
1.3 Quality Summit update from CCG
2 QUALITY PERFORMANCE
2.1 Quality Report PL commented on the excellent quality of the report. PB reported that the A&E target has been delivered for the last 3 weeks, the Trust is in the top 20% nationally. The expectation is that the standard will be delivered this week, but the Trust remains vulnerable to spikes in activity which takes time to recover from. PB feels that the Trust will struggle to meet the target for the quarter because the first week was so bad. YR commented on the Patient Experience report which she felt to be very hospital centric focusing on the FFT figures. Patient Opinion and Your Care Matters is not included, needs to be more patient centric. FA agreed and explained that it had already been identified that there needed to be some PALS and Complaints information within the report. The FFT information is included to inform the board because there is income associated with the targets. FA provided assurance that triangulation of data does take place in the sub-committees. ED patient survey will come to SQC next month. PL asked whether organ donation information could be captured somewhere. JP replied that this information is reported to the Clinical Effectiveness Committee.
2.2 SQC Dashboard PS noted the number of reds around crude mortality and that this has been discussed at the Clinical Effectiveness Group. There has been an increase in deaths this year 7,000 more than the same period last year. The HSMR figure is not available yet but will adjust for seasonal variation.
SQC Minutes 5th February 2015
Page 5 of 10
2.3 Update on the impact of the Cabinet Committee initiative on delayed discharges This was announced at the Trust Board in January 2015. PB explained that there are two ways in which delayed transfers are measured. There are those patients who are “officially” delayed, all aspects of funding has been agreed and yet they are still within the Trust. These numbers are relatively low. There are also patients who are medically fit for discharge (MFFD). These are patients who may not have finished the absolute process of having social services funding agreed but there is no medical reason for them to be in an acute hospital bed. MW has lobbied hard nationally to get this cohort of patients recognised nationally. Twenty-five hospitals have been identified as having patient flow issues which relate to high numbers of MFFD patients. SASH has now been added to the list as number 26 because of the high number of MFFD patients. As of yesterday there were 113 MFFD patients within the Trust, which is a high proportion of the 550 beds within the Trust. The cabinet office has now instructed the Health Economies around the 26 hospitals to reduce the number by 50% by the end of February. The target for SASH is a reduction to 56 MFFD patients by 28th February. The target sits with the CCG but the Trust will support them. PB reported that there is an increased level of activity which is already resulting in an improvement in the number of long stay patients. The average time that a patient stays within the Trust with the status of MFFD is now 15 days; PB reported that this was 20 days 7 days ago. The numbers reduction has not yet happened. There has been a national drive to procure more private sector residential and nursing home capacity. The context is that additional beds are being procured in private nursing homes however there is a funding shortfall; social care funding equates to £600pw, continuing care funding is £800pw, however self-funding is £1,200pw, which makes self-funders the more attractive option. For the private sector to make beds available they will require a “top up”. PB confirmed that Sussex have committed to find another 10 beds, it is not currently clear what Surry’s plan is, but PB reported that there is an positive will to find long term solutions to the problem. PB confirmed that there are three types of patients within this cohort; those who are looking for a permanent placement; those for whom this is respite care or who need rehab who will eventually go home and finally those who are waiting for a package of care to be set up or equipment installed or adaptions made to their homes. PS confirmed that this initiative has been discussed at the Chief Officers meeting who have agreed to support and maintain the target. PB will give a verbal update at the next meeting and progress will be recorded in the performance report.
1:18 2.4 Update on the progress of the CQUIN programme
SQC Minutes 5th February 2015
Page 6 of 10
JP presented a summary table of the current position. He reported that the CCGs and CSUs were happy and have signed off the progress to date. JP took the opportunity to highlight a number of initiatives which have resulted in improvements in care for patients: • Steve Adams, the Dementia Nurse Specialist has successfully trained
1,000 members of staff.
• EOL training team 40/50 staff have been through that training programme
• COPD now have a self management plan in place which is reducing the number of admissions.
RS noted the good progress that has been with CQUINs. PS noted that the CCGs have not yet agreed the CQUINs for 15/16, there will be different CQUINs from NHS England, Surrey, Sussex and the MSK contract.
3 PATIENT EXPERIENCE
4 SAFETY
4.1 Update from Execs regarding evaluation of the impact of localised ward rounds The issue identified at a previous SQC meeting was that if a patient was moved from the ward specialising in the condition for which they had been admitted, for example cardiology, to a gastro ward, they would be reviewed and managed by a gastroenterologist. The question is whether this is the best model of care. This has not yet been evaluated at Execs; however PB explained that it is proposed that job planning within Medicine will change to manage ward rounds on a seven day basis. PB agreed that the admitting to patients to the correct ward first time is still a problem that needs to be solved, it is expected that the additional ward capacity will facilitate this. Action: PB will get an update from Medicine for the next meeting.
PB
4.2 Infection control update AF presented her report. There have been 0 cases MRSA against a target of 0. There have been 18 Trust acquired cases of CDiff, 3 where antibiotic prescribing has not been in line with Trust Policy and only 2 cases of cross infection; this has been declared an SI. So only 5 cases which would be classed as a “lapse in care”, which is where a failure to follow policy has resulted in the infection. The CCGs are able to fine £10,000 per lapse in care over the trajectory. This is also at the discretion of the CCG. The CCGs have not yet established a consistent approach to applying fines where a lapse of care has been identified, nor what evidence will be required. The Trust has a trajectory of 15 for 2015/16 (14/15 was
SQC Minutes 5th February 2015
Page 7 of 10
29); the trajectories vary across the region. The Trust will need to be very clear when each case is investigated that every aspect of care has been appropriate and record the evidence. 3 recent ward closures due to Norovirus; Nutfield, Chaldon and Meadvale, in Q3. The proximity of bed spaces as a result of escalation in Meadvale and the high occupancy putting pressure on the ability to clean may have contributed to this. The infection control team undertook a snapshot audit of side rooms in use in January; they found 34 patients with an infection control issue, 30 of which were successfully isolated in single rooms as per policy. Three MRSAs were being nursed together in a bay; the final patient (group A strep) was being nursed in HDU. There were 37 patients with a biohazard alert on Cerner (patient has ESBL, CDiff or MRSA) which the staff were not aware of. There is a need to increase staff awareness of the biohazard alert and to ask ED administrators to make the admitting wards aware of the alert where it exists. YR asked whether it was an IT fix or a process issue (stickers). BS felt that this was an action for the Cerner user group to take forward. BS also made the point that there aren’t enough side rooms to isolate all the patients with a biohazard alert and that a traffic light system has to be applied. AF will report back to SQC on
• the biohazard alert options with ED
• the management of CDiff
BS drew the committee’s attention to the excellent orthopaedic infection rates which is a real turnaround. RS also congratulated the Infection Control team on the zero MRSA BSI rate.
4.3 Incident report FA presented the incident report. The data shows an increasing trend in reporting across the Trust, particularly from medical staff, of no harm or near miss incidents. But the incidence of falls with harm remains similar. There has been an increase in patients who have fallen from bed, stretcher or trolley and a significant increase in delayed/inadequate care. However, the numbers are small and all these incidents are low harm. FA gave assurance that there is nothing of particular concern. There is an improvement in the timeliness of reporting to the NPSA. Serious incidents are down on Q2 which is encouraging. FA confirmed that the Trust is still dealing with a backlog of falls SI’s. There are 41 SI’s open with the CCGs. 9 are within date, 14 have been submitted to
SQC Minutes 5th February 2015
Page 8 of 10
the CCG for closure, 14 have breached but the Trust is in dialogue with the CCGs about completion dates. YR asked whether the increase in some of the subcategories is due to the pressure that the Trust has been under. It was agreed that it is difficult to know. FA asked the committee to take assurance from the fact that the Trust had not seen an increase in incidents with harm. The data is a snapshot in time and a number of these incidents will be reviewed and the severity amended. BS felt that a system under pressure would expect the majors and extremes to go up and that it is reassuring that even though staff are under pressure they are still taking the time to report incidents. The increase in no harm and near misses would indicate that this is improved reporting and a better understanding of safety. Action: To include in the next quarterly report: • Variation between reporting severity and assessed severity
• Review the profile of incident severity over 2 years.
FA
4.4 Update on Patient Safety Committee Task and Finish Group DN updated the committee on the work of the Task and Finish Group which had been commissioned by the PSC to look at under-reporting culture within the Trust. In November 44 members of staff (including domestics, porters, Bands 2-7 and some SHOs) were asked a number of set questions around incident reporting. There was a lack of robust knowledge of the incidents that require a Datix report; they aligned their reporting to KPI’s such as falls, medicines management and pressure damage. Despite that, all of the staff were able to articulate what a near miss was. Staff were not aware of a trigger list or guidance of what to report within their areas. The T&F identified a big emphasis on the lack of time to complete Datixweb. 63% had a problem accessing Datix or had a problem with the complexity of the form. The majority of staff confirmed that they had received training and education in risk management at induction but that the training was very specific to general incident reporting and all felt that specialty specific training would be beneficial. There was a lack of awareness of the total process and a perception that the responsibility for managing incident resolution lies with the Ward Manager and senior managers. It was clear that the Trust could improve the feedback mechanisms to reporters. DP reported that only a third of managers are feeding back to their staff. 60% of staff have limited or no access to e-mails. One ward had a clear process for feeding back incidents at handover and also had information on team notice boards.
SQC Minutes 5th February 2015
Page 9 of 10
DN reported that the different structures within departments makes a single solution difficult, she suggested champions within each area. MC reinforced the benefit of trigger lists. FA suggested that the recommendations are discussed with the Division risk leads. There are a number of work streams currently looking at aspects of this; the patient safety collaborative and the Virginia Mason project, so this needs to be planned carefully. The committee commended DN for the work she has done on this subject. Action: FA to give a verbal update in two months time.
FA
5 QUALITY
5.1 NICE compliance update Internal audit are satisfied with progress on actions, a report has gone to AAC regarding this. NICE compliance is now on the agenda of each Divisional Meeting, clinicians are aware of what is being assessed within their Divisions and ensuring that baseline assessments are being filled out for all clinical guidelines. The process of reviewing the 46 guidelines where the Trust was partially compliant or non-compliant started in July 2014. Nine of the first ten to be reviewed were updated, six of the guidelines were updated in October and in January the next ten to be reviewed were identified, so the Trust now has an up to date position on three-quarters of the guidelines. All the responses came through the clinical effectiveness committee and the actions that are required to move the Trust to full compliance In December the Divisions were asked to consider the NICE Quality Standards, Medicine has responded and believe that they can make progress on two; COPD and lung cancer. JP confirmed that progress is being made and stronger systems to manage compliance are in place. PS asked whether Internal Audit should be invited to review the progress that has been made, JP agreed that this would be a good idea. Action: JP to make contact with Internal Audit to arrange a review.
JP
6 ANY OTHER BUSINESS BS provided an update from AF on the financial sanctions that can be applied in the event of CDiff as follows:
SQC Minutes 5th February 2015
Page 10 of 10
2015/16 the financial sanction that can be applied to each CDI within
an acute setting will remain £10k. For each case where the provider
assessment indicates that the acquisition is not linked to a provider lapse in care, the coordinating commissioner will determine whether they accept this argument and inform the provider accordingly. If it accepts that there has been no lapse then the case should not count towards the total number of CDI cases on which any sanction will be based. This decision is for the coordinating commissioner to make at its discretion and is not subject to change through contract dispute resolution procedures. For example a single provider may have a target of 25 cases for 2015/16, it may report 30 actual cases in total, but its subsequent assessment may conclude that only 20 of the 30 cases were linked with lapses of care by the provider. In this situation and at its discretion the commissioner may choose to use the second number (20) as the basis for whether any contractual sanction may be applied. If it does so, as this number falls below 25, no sanction will apply. BS confirmed that the sanction will only be applied for cases in excess of the target for the organisation. YR asked why the Trust had abandoned Symbiotics. FA responded to confirm that Symbiotics had been a real time tool for ward based teams to look at their safety information. The organisation did not buy enough modules do this comprehensively. The system only allowed users to see one month at a time so comparisons could not be made. Web access was not good. The company was not felt to be responsive. The Trusts that are using Symbiotics well have had to purchase 20-30 modules; the Trust did not have a plan to do that. There are other mechanisms for collecting the same data and the Trust is in the process of designing a ward based at a glance safety scorecard that pulls from existing data sources that will allow Ward Managers to look at information real time. Symbiotics cost £30k for 8 modules; additional modules were not felt to be cost effective. There will be a trial in March using February data.
DATE OF NEXT MEETING 5th March 2015 14.00 – 16.00 AD77
ExtraordinaryCharitableFundsCommittee–notesof24Nov2014meeting Page1
CHARITABLE FUNDS COMMITTEE
24 November 2014
16.00 – 17.15 AD65 Attendees: Yvette Robbins YR Chair of Charitable Funds
Deputy Chairman / Non Executive Director Pauline Lambert PL Non Executive Director Paul Simpson PS Chief Finance Officer Paul Biddle PB Non-Executive Director (via teleconference) Fiona Allsop FA Chief Nurse Gillian Francis-Musanu GFM Director of Corporate Affairs Djafer Erdogan DE Head of Financial Accounts Helena Usman HU Charitable Funds Accountant Bernard Graham BG Charitable Funds fundraiser In attendance: Gillian Cruse GC Note taking
Who Status
1. Apologies for absence Yvette welcomed members to the extraordinary meeting. Apologies received from Ian Mackenzie and Katrina Swanston.
2
2.1
Fund Raising GFM and BG presented a report to the CFC with key messages for communicating the fundraising strategy for the re-launched SaSH charity. This gave a comprehensive overview of the approach for describing the SaSH Charity and the key messages for each stakeholder group. The report also showed the different logo options that had been designed and presented for final approval. Key messages Following discussion, YR identified a number of examples of charitable funds including medical research which were mainly self-financing. FA confirmed that it was very important to be explicit around what the money was to be spent on. If “Research” indicated it must be clearly outlined what the purpose is. FA felt that the wording should be amended to “Health Research” rather than “Medical Research”. This was agreed. PS requested wording around specific posts being funded to be made clearer. Concern that any initial costs funded by the CFC would then come back to SaSH funding. FA confirmed that funds had been given to pump-prime positions but once funded initially would create cost pressure to divisions in the future. As part of the process the CFC must gain evidence that the post is required. PL requested that wording be changed to “enhancing patient care”. Also change wording from “lend a hand” to “offering time”. FA requested removal of word “medical” to read …providing specialist training...
BG
BG
BG
ExtraordinaryCharitableFundsCommittee–notesof24Nov2014meeting Page2
2.2
2.3
2.4
2.5 2.6 2.7
CSR to be written in full (Corporate Social Responsibility) for clarity. Local Community Some suggestions were made regarding partnering with SaSH charity as a good opportunities to review partnerships as SaSH as an organisation could share opportunities with partners with other external organisations e.g. ½ day training. The Committee also discussed the possibility of hosting an evening outlining SaSH specialities to local businesses. Companies do encourage their staff to promote local and national charities and therefore the corporate angle is well worth pursuing, this could also tie up with local schools. Overall it was felt that the key messages read well and were well articulated and much clearer than in the past. Committee were happy in principal with the key messages subject to wording changes above. Staff The key messages for staff would be discussed at the Executive Committee and at Senior Leaders meetings and messages going to all staff. Executive support would be important for on-going success. Remove word “fitness” to read “fulfil your goal….” In relation to partnerships with other organisations, PS stressed the need for common sense in outlining clear governance rules. Rules must be strong within the strategy and the NHS brand must be safeguarded. The Charitable Funds Committee Approved the Fundraising Strategy and the communications key messages paper. Redhill Football club BG advised CFC that Redhill Football Club have already made a commitment that they wished to be our partner for the 3 year period 2015-18. A Memorandum of Understanding (MOU) guidance required for them to work with SaSH as their charity of the year. Again clear guidance required to protect NHS brand must be ensured. LOGO 5 concepts had been presented to a range of individuals internally and externally including members of the Executive Committee. Concept number 2 was the preferred option indicating many hands. It was agreed that bolder colours were required to give a stronger enhanced logo. Different colours could be used for different occasions. The Committee formally approved the logo. Launch
Launch set for 11/12. Details of the agenda would be circulated for feedback and for potential ideas prior to the launch.
YR and MW to make short presentations. FT/Stakeholders and staff would be invited. Prior to the 11/12 pledges of what people can do are required.
BG
BG
KT/BG
BG
ExtraordinaryCharitableFundsCommittee–notesof24Nov2014meeting Page3
2.8
Any potential business contacts to be passed to BG.
All
3 Any Other Business
3.1
Draft Work Plan 14-15 YP presented the Workplan for information outlining standing agenda items for future meetings. Standing item to be added to agenda for all meetings: Fund raising and strategy plus key actions
GC
3.2
3.3
Terms of Reference 14-15 Members - Head of Communications to be added as official member of committee. Page 5 - Item 3 Investments and fund raising Core duties Change wording to : To improve strategy, monitor implementation and functionality of the fund-raising operational group. Operational Committee report is signed off by Executive Committee and Charitable Funds directly by Trust Board. Need to be specific around sign off within strategy. All requests for high level expenditure will need to be approved by the MD, Chief Nurse and Executives. (Executive approval required for big items via Charitable Funds). This is a different process from the existing one. PS believed that current processes for approval are tight. Under compliance, add extra bullet point to say that “Executive Committee will recommend priorities for purpose of fund-raising”. Income generation to be included under section 3 “Investments & Fund raising)”. There was no other business.
DE
GFM
DE
DE
4
4.1
Proposed date of next meeting Next meeting 4/3/15 but earlier meeting can be arranged if required. Charitable Funds Committee meets 3-4 times per year. 3 March 2015 09.00 – 10.30 in AD65