Embed Size (px)
Citation preview

For peer review only
The STEMS pilot trial: A pilot cluster randomised controlled trial to investigate the addition of patient direct access to
physiotherapy to usual GP-led primary care for adults with musculoskeletal pain (ISRCTN23378642)
Journal: BMJ Open
Manuscript ID bmjopen-2016-012987
Article Type: Research
Date Submitted by the Author: 12-Jul-2016
Complete List of Authors: Bishop, Annette; Keele University, Institute for Primary Care and Health Sciences Ogollah, Reuben; Keele University, Primary Care & Health Sciences Jowett, Sue; University of Birmingham, Health Economics Unit Kigozi, Jesse; University of Birmingham Tooth, Stephanie; Keele University, Primary Care & Health Sciences Protheroe, Joanne; Institute of Primary Care and Health Sciences,, Keele University, UK, Arthritis Research UK Primary Care Centre Hay, Elaine; Arthritis Research Primary Care Centre Salisbury, Chris; University of Bristol, Centre for Academic Primary Care
Foster, Nadine; Keele University, Arthritis Research UK Primary Care Centre
<b>Primary Subject Heading</b>:
Health services research
Secondary Subject Heading: General practice / Family practice, Health services research
Keywords: Patient direct access, musculoskeletal, physiotherapy, feasibility and pilot trial, PRIMARY CARE
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 11 July 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2016-012987 on 12 M
arch 2017. Dow
nloaded from

For peer review only
1
The STEMS pilot trial: A pilot cluster randomised controlled trial to investigate the addition of
patient direct access to physiotherapy to usual GP-led primary care for adults with musculoskeletal
pain (ISRCTN23378642)
Annette Bishop - Research Institute for Primary Care & Health Sciences, Keele University, UK
Reuben O Ogollah - Research Institute for Primary Care & Health Sciences, Keele University, UK
Sue Jowett - Health Economics Unit, University of Birmingham, UK
Jesse Kigozi - Health Economics Unit, University of Birmingham, UK
Stephanie Tooth - Research Institute for Primary Care & Health Sciences, Keele University, UK
Joanne Protheroe - Research Institute for Primary Care & Health Sciences, Keele University, UK [email protected]
Elaine M Hay - Research Institute for Primary Care & Health Sciences, Keele University, UK
Chris Salisbury - Centre for Academic Primary Care, University of Bristol, UK
Nadine E Foster - Research Institute for Primary Care & Health Sciences, Keele University, UK [email protected]
and the STEMS study team
Corresponding author
Annette Bishop Research Institute for Primary Care & Health Sciences
Keele University
Keele
Staffordshire
UK
ST5 5BG
Telephone: 01782 734838
Fax: 01782 734719 Email: [email protected]
Page 1 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
2
Abstract
Introduction: Around 17% of GP consultations are for musculoskeletal conditions, which will rise as the
population ages. Patient direct access to physiotherapy provides one solution, yet adoption in the NHS has
been slow.
Setting: A pilot, pragmatic, non-inferiority, cluster randomised controlled trial (RCT) in general practice and
physiotherapy services.
Objectives: To assess the feasibility of a main RCT.
Participants: Adult patients registered in participating practices and consulting with a musculoskeletal
problem.
Interventions: 4 general practices (clusters) randomised to provide GP-led care as usual or the addition of a
patient direct access to physiotherapy pathway.
Outcomes: Process outcomes and exploratory analyses of clinical and cost outcomes.
Data collection: Participant level data were collected via questionnaires at identification, 2, 6 and 12 months
and through medical records.
Blinding: The study statistician and research nurses were blinded to practice allocation.
Results: Of 2,696 patients invited to complete study questionnaires, 978 participated (intervention group
n=425, control arm n=553) and were analysed. Participant recruitment was completed in 6 months. Follow-
up rates were 78% (6 months) and 71% (12 months). No evidence of selection bias was observed. The direct
access pathway was used by 90% of patients in intervention practices needing physiotherapy. Some increase
in referrals to physiotherapy occurred from one practice, although waiting times for physiotherapy did not
increase (28 days before, 26 days after introduction of direct access) . No safety issues were identified.
Clinical and cost outcomes were similar in both groups. Estimate of between group effect (using SF-36
PCS) at 6 months was -0.28 (95% CIs -1.35, 0.79) and at 12 months 0.12 (95% CIs -1.27, 1.51).
Conclusion: A full RCT is feasible and will provide trial evidence about the clinical and cost-effectiveness
of patient direct access to physiotherapy.
Trial registration: Current Controlled Trials ISRCTN23378642
Funding: Chartered Society of Physiotherapy Charitable Trust
Key words: Patient direct access, primary care, physiotherapy, musculoskeletal, feasibility and pilot trial
Strengths and limitations of this study
• This was a pilot randomised controlled trial (RCT) of patient direct access to physiotherapy in four
general practices and one physiotherapy service in one English town
• It provides evidence for the feasibility and safety of patient direct access to physiotherapy services
• Observed recruitment and follow-up rates can inform a future full RCT
• As a pilot RCT, analyses of clinical and cost outcomes are exploratory
Page 2 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
For peer review only
3
Background
In the UK, primary care is struggling to meet the current record demand from patients. General Practitioners
(GPs) now do an estimated 370 million consultations each year, 60 million more than five years ago.
Musculoskeletal problems account for around 17% of GP consultations1 and given the ageing population,
the demand for musculoskeletal healthcare is set to rise further.2
Patient direct access to NHS physiotherapy is one potential solution, allowing patients to refer themselves to
physiotherapy services rather than referral being initiated by the GP. Despite reported benefits from
observational research such as reduction in GP workload particularly for repeat consultations,3 improved
access for patients,4,5 and reductions in costs,
6,7 progress towards widespread provision of patient direct
access to NHS physiotherapy has been slow. A specific recommendation in the recent Primary Care
Workforce Commission is to investigate whether direct access to physiotherapy for some conditions makes
cost-effective use of NHS resources.8
The aim of the STEMS pilot trial was to assess the feasibility of a future large trial to compare the clinical
and cost-effectiveness of the addition of patient direct access to physiotherapy versus continuing with usual
GP-led care alone for adults with common musculoskeletal problems. The specific objectives of this pilot
trial comprised process objectives to assess the feasibility of a future large cluster randomised trial, and
research objectives that focused on exploratory analysis of clinical outcomes and costs.
Process objectives
i. To assess the engagement of GP practices and physiotherapy services to participate and stay in
the trial through follow-up
ii. To assess the feasibility of establishing a patient direct access to physiotherapy pathway
iii. To develop, and test approaches to market, the direct access pathway to ensure a sufficient
proportion of patients use the pathway
iv. To estimate recruitment rates in both control and intervention practices
v. To explore any evidence of selection bias in the control and intervention practices
vi. To estimate follow-up rates at each follow-up time-point
Research objectives
i. To explore changes in the proposed main trial primary outcome measure (physical health
measured using the SF36v2 Physical Component Summary)
ii. To explore changes in other outcome measures (overall perceived change, SF36v2 Mental
Component Summary, pain self-efficacy, quality of life, understanding of the condition,
experience of care, and convenience and accessibility of services)
iii. To provide an exploratory estimate of costs, both healthcare and societal costs
iv. To estimate the parameters needed for a realistic sample size calculation for a future large cluster
RCT.
v. To explore the use of Willingness to Pay (WTP) methodology to capture the strength of patient
preferences for self-referral to NHS physiotherapy. This analysis will be reported in a separate
future paper.
Page 3 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
For peer review only
4
Methods
Design and setting
STEMS was a pilot, pragmatic, two-arm parallel, non-inferiority, cluster RCT in general practice and
physiotherapy services. The methods have been described in full in the STEMS trial protocol,9 but are
briefly summarised below.
Randomisation
Four general practices were randomised using computer-generated random numbers stratified by the practice
size (small or large) in the ratio 1:1 to continue to offer GP-led care alone as usual care (n=2) or GP-led care
plus the addition of a new pathway permitting patient direct access to an existing NHS physiotherapy
service. Patients followed the care to which their practice was randomised and were recruited through
identical patient information explaining that musculoskeletal services were being evaluated using patient
self-reported clinical outcomes and medical record review. Patient direct access to physiotherapy was not
available to patients registered with control practices. The study statistician was blinded to practice
allocation.
Participants
Individual participants were eligible if they were 18 years or over and presenting to their general practice or
physiotherapy service with a musculoskeletal condition. Patients who were undergoing palliative care, had
severe learning disabilities, were housebound or in nursing home accommodation or unable to communicate
in English were not eligible to take part.
Potentially eligible participants were identified when they presented to the general practice or physiotherapy
service and were mailed a study pack including the first questionnaire. Follow-up data collection was via
participant self-completion postal questionnaires at 2, 6 and 12 months and through review of general
practice and physiotherapy records.
Setting up the patient direct access to physiotherapy pathway
Physiotherapists attended a one-day training programme to prepare them for providing care to patients who
self-refer, including topics such as prevalence and identification of red flags, serious pathology and medical
masqueraders and review of common over-the-counter and prescribed medications for musculoskeletal
pain.9 Physiotherapists also attended regular mentoring meetings with a senior physiotherapist in the
participating physiotherapy service.
The patient direct access pathway began 8 weeks prior to the start of participant recruitment to the study in
order to allow familiarisation with receiving and managing patients using the direct access pathway. All
referrals (GPs or patient self-referral) were triaged using existing physiotherapy service criteria and were
classified as urgent, routine or inappropriate for physiotherapy. In common with all referrals received in the
service, urgent cases were offered the next available appointment whereas routine cases joined the routine
physiotherapy waiting list.
In order to ensure patients were aware of the new direct access pathway, all adult registered patients at the
two intervention practices (n=8222) were individually mailed an information letter about direct access.
Posters, flyers and self-referral forms were readily available in intervention practices. Even with the offer of
Page 4 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
5
self-referral, we anticipated that some patients would continue to consult their GP or practice nurse,
therefore in the intervention practices, patients could access physiotherapy either by traditional written
referral, be recommended to self-refer (GP or nurse ‘recommended’ self-referral), or choose to self-refer to
physiotherapy without contacting their GP practice (‘true’ self-referrers).
Safety of the pathway was explored by the number of adverse events reported and by systematically
searching for diagnostic codes of a wide range of pathologies (including cancer, fractures, joint infections
and stroke) in the medical records of participants who used the direct access pathway.
Outcomes and analysis
Outcomes were collected from several sources. Anonymised process outcome data were collected from
physiotherapy service records and self-referral forms. Individual participants provided data on their
characteristics, clinical outcomes and costs through self-completed questionnaires following recruitment to
the research and at 2, 6 and 12 months. Key outcome data were sought from non-responders through
minimum data collection (MDC). The anticipated primary clinical outcome for a future full RCT is physical
health measured using the SF36v2 Physical Component Summary,10 to provide an overall assessment of
physical health. A cost-consequence analysis was undertaken to identify patient-level resource use (for their
musculsoskeletal condition), costs and Quality Adjusted Life Years (QALYs) (using EQ-5D-5L11) by trial
arm. The complete case analysis was from an NHS and healthcare perspective. To ensure transparency in
analyses, a statistical analysis plan (SAP) was developed and approved by the Trial Steering Committee
(TSC) prior to the final analysis.
Sample size
As this was a pilot trial formal sample size calculation was not carried out. The sample size was based on
the number of patients we anticipated could be recruited within six months and that was sufficiently large to
estimate the key feasibility parameters (e.g. recruitment and retention) to a sufficient degree of accuracy
(<10% in the rates). We aimed to recruit 960 participants at baseline, over a period of six months and
achieve at least 80% follow-up rate (n=768) at 6 months.
Results
A flowchart showing the flow of practices (units of randomisation) and flow of individual participants is
shown in Figure 1. As can be seen one of the control practices was considerable larger that the other
randomised practices resulting in more participants in the control arm in this pilot trial.
Insert figure 1 about here
Process results
Engagement of GP practices and the physiotherapy service
Of five GP practices approached, four participated with three full-time equivalent GPs at each of the two
intervention practices and five and two in the control practices. In the physiotherapy service four of five
Page 5 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
6
physiotherapists participated in the STEMS training programme and delivered care to patients using the
direct access pathway (NHS Agenda for Change band 7 (n=1), band 6 (n=2), and band 5 (n=1)).
Feasibility of the patient direct access pathway
Of the participants in the STEMS pilot trial (n=978), a total of 256 (26.2%) accessed physiotherapy care
during the study period, 152 (35.8%) in the intervention arm and 104 (18.8%) in the control arm. Of the 152
who accessed physiotherapy care in the intervention arm, 142 (93.4%) were self-referrals (comprising 98
(69%) ‘recommended’ and 44 (31%) ‘true’ self-referrals).
Comparisons to service level data (which may not be entirely comparable) from the same period one year
prior to start of direct access suggests one practice in the intervention arm had broadly similar rates of
patients accessing physiotherapy care, whereas the other had a substantial increase once the direct access
pathway had been introduced. However, overall waiting time in the physiotherapy service (applying to all
patients in the service), from logging of the referral to first appointment, was 28 days prior to the
introduction of direct access and 26 days during the direct access period of the trial. Of the patients using the
direct access pathway, triaging according to pre-existing service criteria classified 23% (n=159) cases as
urgent, 73% (n=507) as routine and 4% (n=25) as unsuitable for physiotherapy.
Marketing of the direct access pathway was successful. We aimed to ensure a minimum of 20% of the
physiotherapy caseload during the pilot trial, from intervention arm practices, was through direct access.
Using anonymised physiotherapy service data, of 765 patients registered at intervention practices and
accessing care for ten months following the introduction of the direct access pathway, 691 (90.3%) used the
pathway (comprising 515 (74.5%) ‘recommended’ and 176 (25.5%) ‘true’ self-referrals).
Safety of direct access
No adverse events were reported by GPs or physiotherapists during the pilot trial. Review of medical
records identified no evidence of missed serious pathology in patients who directly accessed physiotherapy.
Participant recruitment and retention
Of 2,696 participants invited to take part in the data collection, 978 (36%) participated (425 (44%) in the
intervention practices and 553 (57%) in the control practices). Recruitment was completed within six
months (June – December 2013). Response rates were as follows; 74.3% at 2 months (intervention 70.4%,
control 77.4%), 78.4% at 6 months (intervention 76.7%, control 79.8%) and 70.7% at 12 months
(intervention 69.4%, control 71.6%). Minimum data collection was included at 6 and 12 months only
resulting in higher response rates at these time-points.
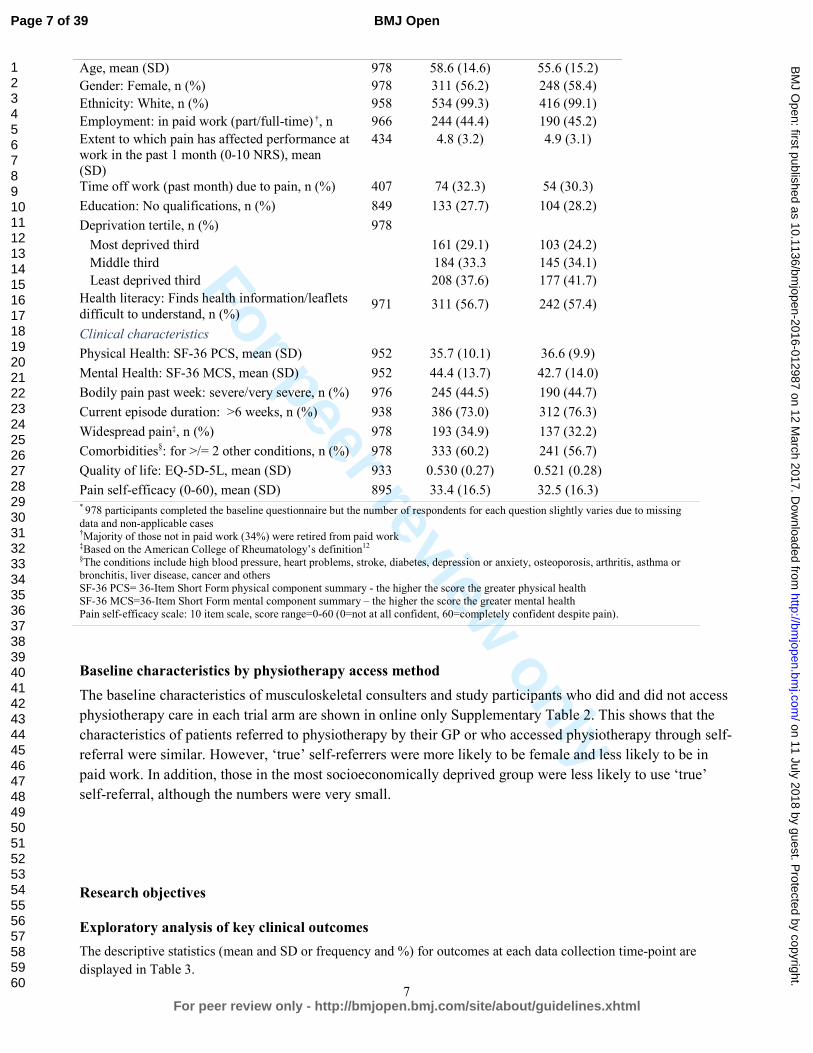
Comparability of baseline characteristics
The baseline characteristics of participants (Table 1) were comparable in the two arms of the trial and there
was no evidence of selection bias.
Table 1: Comparability of baseline characteristics
Key characteristics n* Control
n=553
Intervention
n=425
Non-clinical characteristics
Page 6 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
For peer review only
7
Age, mean (SD) 978 58.6 (14.6) 55.6 (15.2)
Gender: Female, n (%) 978 311 (56.2) 248 (58.4)
Ethnicity: White, n (%) 958 534 (99.3) 416 (99.1)
Employment: in paid work (part/full-time) †, n (%)
966 244 (44.4) 190 (45.2)
Extent to which pain has affected performance at
work in the past 1 month (0-10 NRS), mean
(SD)
434 4.8 (3.2) 4.9 (3.1)
Time off work (past month) due to pain, n (%) 407 74 (32.3) 54 (30.3)
Education: No qualifications, n (%) 849 133 (27.7) 104 (28.2)
Deprivation tertile, n (%) 978
Most deprived third 161 (29.1) 103 (24.2)
Middle third 184 (33.3 145 (34.1)
Least deprived third 208 (37.6) 177 (41.7)
Health literacy: Finds health information/leaflets
difficult to understand, n (%) 971 311 (56.7) 242 (57.4)
Clinical characteristics
Physical Health: SF-36 PCS, mean (SD) 952 35.7 (10.1) 36.6 (9.9)
Mental Health: SF-36 MCS, mean (SD) 952 44.4 (13.7) 42.7 (14.0)
Bodily pain past week: severe/very severe, n (%) 976 245 (44.5) 190 (44.7)
Current episode duration: >6 weeks, n (%) 938 386 (73.0) 312 (76.3)
Widespread pain‡, n (%) 978 193 (34.9) 137 (32.2)
Comorbidities§: for >/= 2 other conditions, n (%) 978 333 (60.2) 241 (56.7)
Quality of life: EQ-5D-5L, mean (SD) 933 0.530 (0.27) 0.521 (0.28)
Pain self-efficacy (0-60), mean (SD) 895 33.4 (16.5) 32.5 (16.3) * 978 participants completed the baseline questionnaire but the number of respondents for each question slightly varies due to missing
data and non-applicable cases †Majority of those not in paid work (34%) were retired from paid work
‡Based on the American College of Rheumatology’s definition12 §The conditions include high blood pressure, heart problems, stroke, diabetes, depression or anxiety, osteoporosis, arthritis, asthma or
bronchitis, liver disease, cancer and others
SF-36 PCS= 36-Item Short Form physical component summary - the higher the score the greater physical health
SF-36 MCS=36-Item Short Form mental component summary – the higher the score the greater mental health
Pain self-efficacy scale: 10 item scale, score range=0-60 (0=not at all confident, 60=completely confident despite pain).
Baseline characteristics by physiotherapy access method
The baseline characteristics of musculoskeletal consulters and study participants who did and did not access
physiotherapy care in each trial arm are shown in online only Supplementary Table 2. This shows that the
characteristics of patients referred to physiotherapy by their GP or who accessed physiotherapy through self-
referral were similar. However, ‘true’ self-referrers were more likely to be female and less likely to be in
paid work. In addition, those in the most socioeconomically deprived group were less likely to use ‘true’
self-referral, although the numbers were very small.
Research objectives
Exploratory analysis of key clinical outcomes
The descriptive statistics (mean and SD or frequency and %) for outcomes at each data collection time-point are
displayed in Table 3.
Page 7 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
8
Table 3: Descriptive statistics (mean and SD or frequency and %) for outcome measures at each time-point
Outcome Initial questionnaire 2 Months 6 Months 12 months
Intervention Control Intervention Control Intervention Control Intervention Control
Physical Health: SF-36 PCS, mean (SD) 36.6 (9.9) 35.7 (10.1) 38.5 (10.5) 37.5 (11.2) 38.7 (11.2) 37.9 (11.3) 39.7 (11.2) 38.7 (12.0)
Mental Health: SF-36 MCS, mean (SD) 42.7 (14.0) 44.4 (13.7) 44.7 (12.5) 45.9 (12.7) 45.2 (12.9) 46.2 (13.1) 45.3 (13.2) 45.7 (13.4)
Overall perceived change from baseline, n (%)
Completely recovered - - 4 (1.4) 8 (1.9) 13 (4.0) 28 (6.5) 21 (7.2) 30 (7.6)
Much improved - - 33 (11.2) 52 (12.3) 56 (17.2) 44 (10.1) 50 (17.2) 60 (15.3)
Somewhat improved - - 72 (24.3) 81 (19.2) 52 (15.0) 79 (18.2) 38 (13.1) 59 (15.0)
Same - - 114 (38.5) 176 (41.7) 99 (30.5) 133 (30.7) 86 (29.7) 106 (27.0)
Somewhat worse - - 59 (19.9) 89 (21.1) 80 (24.6) 120 (27.7) 67 (23.1) 113 (28.8)
Much worse - - 14 (4.7) 16 (3.8) 25 (7.7) 30 (6.9) 28 (9.7) 25 (6.4)
Pain self-efficacy (0-60), mean (SD) 32.5 (16.3) 33.4 (16.5) 37.1 (16.1) 36.8 (16.0) 36.8 (16.3) 36.0 (16.1) 38.1 (16.3) 35.5 (16.8)
Convenience of services received†, mean (SD) - - 7.2 (2.5) 7.1 (2.8) 7.4 (2.6) 7.1 (2.5) - -
Satisfaction with services received‡, mean (SD) - 6.9 (2.9) 6.8 (2.9) 7.2 (2.7) 7.0 (2.7) - - SF-36 PCS= 36-Item Short Form physical component summary – the higher the score the better the physical health
SF-36 MCS=36-Item Short Form mental component summary – the higher the score the better the mental health
Pain self-efficacy scale: 10 item scale, score range=0-60 (0=not at all confident, 60=completely confident despite pain). †0-10 Numerical Rating Scale: (0 = not at all convenient, 10 = very convenient).
‡0-10 Numerical Rating Scale: (0 = not satisfied, 10 = very satisfied).
Page 8 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2016-012987 on 12 March 2017. Downloaded from

For peer review only
9
Patients’ physical health measured using the SF-36 PCS is the anticipated primary clinical outcome for a
future main trial. Higher scores represent better physical health. Very similar scores over time in participants
in both arms of the trial were seen. The adjusted mean difference between groups and 95% confidence
interval showed estimates of effect at 2 months -0.14 (95% CI -1.02, 0.74), at 6 months -0.28 (-1.35, 0.79)
and at 12 months 0.12 (-1.27, 1.51). The lower limit of the two-sided 95% CI for intervention versus control
mean difference was greater than -2, the smallest expected standard treatment effect for the outcome (SF-36
PCS). Adjusted estimates of treatment effect are provided in the online only Supplementary Table 4.
Health economics results
EQ-5D-5L responses were available at all time-points for 493 participants (281 (51%) control arm, 212
(50%) intervention arm). Self-reported resource use data were available at all time-points for 555
participants (237 (43%) control arm, 318 (57%) intervention arm). Details of NHS and healthcare resource
use are reported in online only supplementary Table 5, with most resource use involving consultations with
GPs, physiotherapists and practice nurses. Over 12 months, on average, the control arm was associated with
slightly more GP visits, more investigations (including scans, x-rays and MRIs) and visits to some
consultants (rheumatologists and orthopaedic surgeons) and inpatient days resulting from surgeries. The
intervention arm was however associated with more physiotherapist visits.
Table 6 shows the disaggregated mean (SD) healthcare costs per patient for each treatment arm. The mean
NHS costs per patient were slightly cheaper in the intervention arm (£940 in intervention compared to £951
in the control arm), with considerable uncertainty in the estimates (95% CI of difference -340.83 to 363.27).
The proportion of participants that reported having taken time off work due to their musculoskeletal problem
was similar between the two arms of the trial over 12 months. The intervention arm was however associated
with fewer self-reported days off work and lower costs at 12 months follow-up. Productivity loss and costs
as a result of reduced productivity at work were higher in the intervention group. Mean quality of life scores
(EQ-5D-5L) scores (quality of life at baseline and follow-up and mean QALYs) are presented in Table 7.
Quality of life increased in both groups from the initial questionnaire over all follow-up time-points.
Unadjusted mean QALYs were slightly higher in the control arm however, QALYs were slightly higher in
the intervention arm once adjusted for clustering and baseline EQ-5D-5L but this difference was very small.
Overall, the results show similar outcomes and costs between the intervention and control arms of the trial.
Table 6: Costs per participant by trial arm over 12 months
Complete case analysis Control
(n=318)
£Mean (SD)
Intervention
(n=237)
£Mean (SD)
NHS
GP 106.70 (134.57) 96.97 (134.58)
Practice nurse 7.87 (33.51) 8.35 (37.93)
Physiotherapist 61.99 (165.96) 74.67 (163.36)
Orthopaedic surgeon 48.43 (114.47) 36.58 (102.54)
Rheumatologist 20.91 (87.79) 11.22 (52.17)
Acupuncturist 5.67 (50.74) 1.67 (13.63)
Chiropractor 4.28 (35.81) 1.48 (15.08)
Page 9 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
10
Occupational therapist 7.89 (51.29) 5.01 (24.62)
Other healthcare professionals 33.88 (187.28) 21.67 (117.81)
Prescriptions 55.18 (118.24) 47.15 (110.41)
Surgery 422.97 (1759.25) 404.12 (1655.21)
Inpatient costs 21.57 (230.41) 75.11 (956.32)
Investigations 109.53 (329.93) 100.77 (263.43)
Injections 44.37 (164.06) 55.22 (274.33)
Private
Physiotherapist 9.46 (55.05) 22.68 (155.41)
Orthopaedic surgeon 4.49 (34.07) 3.01 (23.74)
Rheumatologist 0 1.12 (17.27)
Acupuncturist 3.04 (30.91) 5.76 (40.60)
Chiropractor 9.13 (85.47) 6.68 (48.31)
Occupational therapist 0 0.74 (11.43)
Other healthcare professionals 3.98 (38.49) 7.63 (97.90)
Over-the-counter medicines 20.20 (52.59) 15.06 (30.06)
Work-related outcomes
Musculoskeletal-related work absence
costs
740.30 (2084.75) 539.36 (2069.43)
Complete Case
Total NHS cost, £ 951.25 (2050.88) 940.02 (2157.24)
11.22 (-340.8255 to 363.27)
Total healthcare costs*, £ 1001.56 (2068.62) 1002.72 (2230.66)
-1.15 (-360.3217 to 358.00)
*Includes costs to the NHS, private healthcare costs and over-the-counter treatment costs
Table 7: EQ-5D-5L scores and QALYs at each time point
Complete case analysis Control
(n=281)
Mean (SD)
Intervention
(n=212)
Mean (SD)
Initial questionnaire 0.565 (0.246) 0.544 (0.262)
2 months 0.600 (0.227) 0.580 (0.246)
6 months 0.602 (0.251) 0.594 (0.262)
12 months 0.615 (0.254) 0.606 (0.258)
Total 12 month QALYs
(unadjusted)
0.602 (0.225) 0.589 (0.236)
Incremental QALYs (95%
CI)
-0.012 (-0.053 to 0.028)
Total 12 month QALYs
(adjusted for clustering and
baseline EQ-5D-5L)*
0.575 0.578
EQ-5D-5L = EuroQol; QALYs = quality-adjusted life years; SD = Standard Deviation * QALYs have been adjusted for baseline differences and clustering
Page 10 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
11
Discussion
No other RCTs of direct access to physiotherapy have been conducted. This pilot RCT explored the
feasibility of a future main cluster RCT and has provided an exploratory analysis of clinical and cost
outcomes.
The results show that a future main trial is feasible and general practices and physiotherapy services are
willing to take part. The patient recruitment target was achieved rapidly within the estimated six month
recruitment period. Follow-up rates were good although the follow-up at 12-months fell below our
anticipated 80%. In a future main trial we would include small patient payments to compensate participants
for their time in completing and returning questionnaires. Cluster trials have particular challenges including
the concern about selection bias.13,14
To minimise the risk of selection bias we avoided participating
clinicians being involved in the identification and recruitment of potential participants. The baseline
characteristics of the participants showed no evidence of selection bias, which shows that our methods of
identification and recruitment are suitable for use in a future main trial. Participant recruitment and retention
through to long-term follow-up at 12 months was feasible and completed on time and to target. The likely
primary clinical outcome for a main trial is patients’ physical health assessed using the SF-36 PCS.10 This
performed well in the pilot trial and exploratory analyses of clinical outcomes showed very similar changes
in patient self-reported physical health measured in both arms of the trial. The hypotheses for a main trial
would be non-inferiority on clinical outcomes (i.e. the addition of a patient direct access pathway to usual
GP-led care would not lead to worse clinical outcomes for patients than usual GP-led care alone) but
superiority on other key outcomes (i.e. higher patient ratings of access to services, convenience and
satisfaction with services, and reduced costs). A future main cluster RCT with a primary clinical outcome of
physical health measured using the SF-36 PCS would require a sample size of approximately 12 average-
sized general practices and a minimum of 2880 individual participants.
Exploratory health economic findings show that costs and outcomes were similar between the intervention
and control arms, although there is considerable imprecision in the estimates due to the sample size in this
pilot RCT. Data collection through patient report in the questionnaires was successful and indicates that a
full economic evaluation of adding a patient direct access to physiotherapy pathway to usual GP-led primary
care versus usual GP-led primary care alone will be possible in a future main trial.
This pilot trial suggests that adding a new patient direct access pathway to an existing physiotherapy service
is feasible. We observed an increase in the number of overall referrals to physiotherapy in the intervention
arm practices compared to service level data collected in the year prior to the STEMS pilot trial, mostly
from one practice, but this did not impact on the waiting time for physiotherapy care. The level of GP
referral to physiotherapy prior to the STEMS pilot trial was very low in this one practice (32.6 referrals per
annum per 1000 registered adults compared to the other practices (59.3, 69.5 and 92.4 referrals per annum
per 1000 registered adults). An initial increase in referrals is perhaps not surprising bearing in mind the
active marketing of the direct access pathway that was undertaken. This type of marketing is unlikely to
occur outside the context of a trial but plans to support participating services will be required in a future
main trial. Whilst no robust claims can be made about safety given the pilot nature of this RCT, no adverse
events were reported. In addition, our systematic search of diagnostic codes of serious or significant
pathology in the medical records of patients who directly accessed physiotherapy found no evidence that the
direct access pathway led to missed serious pathologies. This is in keeping with a recent analysis of 12,976
patient visits to a US physical therapist student health centre over 10 years, without a physician referral that
reported no adverse events and no missed cases of serious pathology.15
Page 11 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
For peer review only
12
Non-attendance rates
We also aimed to compare patient non-attendance rates for physiotherapy before and during patient direct
access, but we were unable to achieve this as the physiotherapy service changed the definition and processes
for recording non-attendance part way through the STEMS pilot trial.
Conclusion
In line with calls for research on ways to ensure patient demand can be met in primary care, this pilot trial
shows that a future large RCT is feasible and will provide high quality evidence about the clinical and cost
effectiveness of direct access to physiotherapy for patients with musculoskeletal pain.
References
1. Jordan KP, Kadam UT, Hayward R, Young C, Croft P. Annual consultation prevalence of regional
musculoskeletal problems in primary care: an observational study. BMC Musculoskelet Disord 2010;11:144
2. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Ezzati M, Shibuya K, Salomon JA,
Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR,
Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels
DH, Basáñez MG, Baxter A, Bell ML, Benjamin EJ, et al.:Disability-adjusted life years (DALYs)for 291
diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study
2010. Lancet 2012, 380:2197-2223
3. Holdsworth LK, Webster VS, McFadyen AK. What are the costs to NHS Scotland of self-referral to
physiotherapy? Results of a national trial. Physiotherapy 2007;93(1):3-11
4. Department of Health. Self-referral pilots to musculoskeletal physiotherapy and the implications of improving access to other AHP services. Leeds. Department of Health; 2008
[www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_089516].
Accessed 01 February 2015
5. Leemrijse CJ, Swinkels ICS, Veenhof C. Direct access to physical therapy in the Netherlands: results from the
first year in community-based physical therapy. Physical Therapy 2008;88(8):936-46
6. QIPP Quality and Productivity Case Studies. Musculoskeletal Physiotherapy: patient self-referral 2012 citing Holdsworth et al 2007, costs updated in accordance with Department of Health 2011
https://www.evidence.nhs.uk/qipp. Accessed 10th January 2015
7. Mallett R, Bakker E, Burton M. Is physiotherapy self-referral with Telephone Triage Viable, Cost-effective and Beneficial to Musculoskeletal Outpatients in a Primary Care Setting? Musculoskeletal Care
2014;12(4):251-60
8. Primary Care Workforce Commission. The future of primary care. Creating teams for tomorrow. 2015
www.hee.nhs.uk
9. Bishop A, Tooth S, Protheroe J, Salisbury C, Ogollah RO, Jowett S, Hay EM, Foster NE and on behalf of the
STEMS study team. A pilot cluster randomised controlled trial to investigate the addition of direct access to
physiotherapy to usual GP-led primary care for adults with musculoskeletal pain: the STEMS pilot trial protocol (ISRCTN23378642). Pilot and Feasibility Studies 2015, 1:26 doi:10.1186/s40814-015-0020-4
10. SF-36.org: A community for measuring health outcomes using SF tools. http://www.sf-36.org/].
11. Herdman M, Gudex C, Lloyd A, Janssen MF, Kind P, Parkin D, Bonsel G, Badia X. Development and
preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research. 2011; 20(10): 1727–1736.
12. Wolfe F, Smythe H, Yunus M, et al. The American College of Rheumatology 1990 criteria for the
classification of fibromyalgia. Arthritis Rheum 1990; 33: 160–71
13. Puffer S, Torgerson D, Watson J. Evidence for risk of bias in cluster randomised trials: Review of recent trials
published in three general medical journals. BMJ 2003;327:785–789
14. Hahn S, Puffer S, Torgerson DJ, Watson J. Methodological bias in cluster randomised trials. BMC Medical
Research Methodology 2005. DOI: 10.1186/1471-2288-5-10
15. Mintken PE, Pascoe SC, Barsch AK, Cleland JA. Direct access to physical therapy services is safe in a
university student health center setting. J Allied Health. 2015;44(3):164-8
Page 12 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
13
Competing interests
The authors declare that they have no competing interests.
Funding
The STEMS pilot trial was funded by the Chartered Society of Physiotherapy Charitable Trust (SRP (11)2).
NEF and AB are funded through a National Institute of Health Research (NIHR) Research Professorship
awarded to NE Foster (NIHR-RP-011-015). NEF is an NIHR Senior Investigator. The views and opinions
expressed are those of the authors and do not necessarily reflect those of the NHS, the NIHR or the
Department of Health. The North Staffordshire Primary Care Research Consortium provided additional
funding for GP and Physiotherapy Research Facilitators to advise on the engagement and recruitment of GP
practices and physiotherapists in the STEMS pilot trial.
Authors' contributions
AB helped plan the trial, contributed to the funding application, chaired the Trial Management Group
(TMG) and led the writing of this paper. RO developed the analysis plan and performed the quantitative
analyses. SJ developed the health economic data collection and analysis plan and supervised JK who
conducted the health economic analysis. ST was responsible for trial co-ordination, supporting the TMG, the
general practices and physiotherapy service. JP provided general practice expertise and contributed to the
training of physiotherapists offering the direct access pathway. EH provided senior trials leadership,
expertise and oversight. CS helped design the trial and provided general practice expertise. NEF led the
design of the trial and the funding application, and provided senior trials leadership and oversight. All
authors contributed to this paper and approved the final version.
Acknowledgements
The STEMS trial team acknowledges the support from Keele Clinical Trials Unit, including Dr Ruth
Beardmore (Research Programme Manager) for input into research governance and gaining of regulatory
approvals, and administrators Michelle Robinson and Victoria Harper for coordinating mailings of
consenting patients and general research administrative support. We also acknowledge the NIHR Clinical
Research Network (CRN) including Ian Thomas for coordinating systems to help the participating practices
identify eligible patients and assistance in providing anonymised patient data, the research nurse team,
including Julie Young, Debbie D’Cruz, Alice Mackie, William Cole, and Sian Jones who dealt with patient
queries and conducted minimum data collection via telephone. We thank the CRN physiotherapy and GP
research facilitators, Gemma Sellors, Carol Doyle and Beth Hanson. Thanks to the Independent Advisory
Panel comprising Jill Gamlin, Sue Greenhalgh, Lesley Holdsworth and Ruth ten Hove who provided advice
on setting up patient direct access to physiotherapy and Sue Greenhalgh for her input into the
physiotherapist training. We are grateful to the general practices and physiotherapy service that participated
in this pilot trial and in particular the support of Ruth Heaton, Therapy Manager, and to the physiotherapists
who delivered care to patients.. We acknowledge Arthritis Research UK who funded early stakeholder
thinktanks to develop and design the STEMS trial. Finally we are particularly indebted to our PPIE
members, Trial Steering Committee members and all the participants who provided data.
Data sharing
No additional data available
Page 13 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
For peer review only
Figure and table legends
Figure 1: STEMS pilot trial flowchart
Online only supplementary Table 2: Baseline characteristics of participants by care pathway
Online only Supplementary Table 4: Adjusted estimates (adjusted mean difference or odds ratio) and
95% confidence intervals for the treatment effect of outcomes based on mixed effect model (linear for
continuous and logistic for binary).
Online only supplementary Table 5: Healthcare resource use by trial arm over 12 months. Results are
mean (SD) number of visits unless otherwise stated.
Page 14 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Figure 1: STEMS pilot trial flowchart
Approached to participate in the trial (n=5 GP practices)
Declined to participate (n=1 practice)
Analysed for proposed primary outcome (n=425
participants)
Intervention: 2 GP Practices (Practice sizes:
5429 & 5046)
♦ Both had patient direct access pathway
♦ 1177 patients sent initial questionnaires
Randomised (n=4 GP practices*)
Enrolment
Allocation
Follow-up
Analysis
Control: 2 GP Practices (Practice sizes: 10014 &
4460)
♦ Neither had patient direct access pathway
♦ 1519 patients sent initial questionnaires
Completed 2 months follow-up (n=299
participants (70.4% of recruited))
♦ Lost to follow-up (n=126; 29.7%) †
Completed 2 months follow-up (n= 428
participants (77.4% of recruited))
♦ Lost to follow-up (n=125; 22.6%)†
425 participants (36.1% of those invited) returned
initial questionnaires (254 & 171 participants
from each practice)
553 participants (36.4% of those invited) returned
initial questionnaires (365 & 188 participants
from each practice)
Analysed for proposed primary outcome (n= 553
participants)
Completed 6 months follow-up (n= 326
participants (76.7%))‡
♦ Lost to follow-up (n=99; 23.3%)§
Completed 6 months follow-up (n= 441
participants (79.8%))‡
♦ Lost to follow-up (n=112; 20.3%)§
Completed 12 months follow-up (n= 2
practices; 295 participants (69.4%))‡
♦ Lost to follow-up (n=130; 30.6%)¶
Completed 12 months follow-up (n=2
practices; 396 participants (71.6%))‡
♦ Lost to follow-up (n=157; 28.4%)¶
*All four randomised GP practices remained in the trial to the end
† Included 4 withdrawals, 2 from each arm ‡ The 6 and 12 months follow-up figures also include minimum data collection on key outcomes
§ Included 42 additional withdrawals, 21 from each arm
¶ Included 15 additional withdrawals, 6 from intervention and 9 from control arm
Page 15 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Online only supplementary Table 2: Baseline characteristics of participants by care pathway
Control practices
n = 553
Intervention practices
n = 425
Usual GP-led care only Usual GP-led care Direct access to physiotherapy
Key characteristics Not
referred to
physiother
apy
n =449
(81.2%)
Referred
to
physiother
apy
n=104
(18.8%)
Not referred to
physiotherapy
n = 273
(64.2%)
GP referral to
physiotherapy
n = 10
All
physiotherapy
self-referrers
n =142
Recommen
ded self-
referrers
n = 98
True self-
referrers
n = 44
Non-clinical characteristics
Age, mean (SD) 59.3 (14.8) 55.4 (13.6) 55.3 (15.6) 52.5 (8.3) 56.5 (14.7) 56.1 (13.4) 57.2 (17.3)
Gender: Female, n (%) 253 (56.4) 58 (55.8) 155 (56.7) 5 (50%) 88 (62.0) 57 (58.2) 31 (70.5)
Employment: in paid work (part/full-time), n (%) 185 (41.8) 58 (55.8) 118 (43.5) 7 (70%) 64 (46.4) 49 (51.0) 15 (35.7)
Extent to which pain has affected performance at
work in the past 1 month (0-10 NRS), mean (SD)
4.8 (3.1) 4.5 (3.4) 5.1 (3.2) 3.3 (2.3) 4.7 (2.9) 4.6 (2.6) 5 (3.8)
Education: No qualifications, n (%) 118 (30.0) 15 (17.2) 67 (28.0) 2 (28.6) 35 (28.5) 24 (28.2) 11 (29.0)
Deprivation tertile, n (%)
Most deprived third 137 (30.5) 24 (23.1) 67 (24.5) 2 (20%) 34 (23.9) 27 (27.6) 7 (15.9)
Middle third 149 (33.2) 35 (33.7) 97 (35.5) 4 (40%) 44 (31.0) 24 (24.5) 20 (45.5)
Least deprived third 163 (36.3) 45 (43.3) 109 (39.9) 4 (40%) 64 (45.1) 47 (48.0) 17 (38.6)
Health literacy: Finds health information/leaflets
difficult to understand, n (%)
256 (57.5) 55 (52.9) 162 (57.7) 7 (70%) 80 (56.7) 56 (57.7) 24 (54.6)
Clinical characteristics
Physical Health: SF-36 PCS, mean (SD) 35.2 (10.3) 38.0 (8.8) 36.6 (10.0) 38.6 (8.3) 36.5 (9.8) 37.1 (9.8) 35.1 (9.8)
Mental Health: SF-36 MCS, mean (SD) 44.2 (13.5) 45.3 (14.3) 42.5 (13.7) 40.1 (18.0) 43.2 (14.2) 43.8 (14.3) 42.0 (13.9)
Current episode duration: >6 weeks, n (%) 307 (72.2) 79 (78.2) 198 (77.7) 8 (80.0) 106 (78.5) 73 (77.7) 33 (80.5)
Comorbidities*: 2 or more other conditions, n (%) 278 (61.9) 55 (52.9) 161 (58.9) 5 (50.0) 75 (52.8) 47 (48.0) 28 (63.6)
Pain self-efficacy (0-60), mean (SD) 33.1 (16.3) 35.1 (17.3) 32.3 (16.6) 33.5 (16.2) 32.7 (15.9) 33.6 (15.4) 30.8 (17.0)
Page 16 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2016-012987 on 12 March 2017. Downloaded from

For peer review only
Satisfaction with services received
Satisfaction at 2 Months†, mean (SD) 6.6 (3.0) 7.2 (2.5) 6.9 (2.8) 5.0 (2.3) 7.0 (3.0) 6.8 (2.8) 7.5 (3.3)
Satisfaction at 6 Months†, mean (SD) 6.8 (2.8) 7.5 (2.3) 7.3 (2.7) 6.0 (2.2) 7.1 (2.7) 7.3 (2.4) 6.8 (3.1)
*The conditions include high blood pressure, heart problems, stroke, diabetes, depression or anxiety, osteoporosis, arthritis, asthma or bronchitis, liver disease, cancer and others
SF-36 PCS= 36-Item Short Form physical component summary – the higher the score the better the physical health
SF-36 MCS=36-Item Short Form mental component summary – the higher the score the better the mental health
Pain self-efficacy scale: 10 item scale, score range=0-60 (0=not at all confident, 60=completely confident despite pain). †0-10 Numerical Rating Scale: (0 = not satisfied, 10 = very satisfied).
Page 17 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2016-012987 on 12 March 2017. Downloaded from

For peer review only
Online only Supplementary Table 4: Adjusted estimates (adjusted mean difference or odds
ratio) and 95% confidence intervals for the treatment effect of outcomes based on mixed
effect model (linear for continuous and logistic for binary).
Outcomes 2 months 6 months 12 months
Intervention vs. control arm (reference
category) Estimate
(95% CI)
Estimate
(95% CI)
Estimate
(95% CI)
Physical Health: SF-36 PCS -0.14 (-1.02, 0.74) -0.28 (-1.35, 0.79) 0.12 (-1.27, 1.51)
Mental Health: SF-36 MCS 0.001 (-1.24, 1.24) 0.52 (-0.86, 1.91) 0.34 (-1.40, 2.07)
Pain self-efficacy (0-60) 0.62 (-0.68, 1.93) 2.22 (0.49, 3.96) 1.94 (-0.35, 4.24)
Overall perceived change from baseline:
completely recovered or much improved* 0.63 (0.31, 1.29) 1.37 (0.72, 2.59) 1.05 (0.56, 1.98)
Convenience of services received for pain or pain related symptoms (0-10 NRS)
0.11 (-0.56, 0.78) 0.17 (-0.34, 0.62) -
Satisfaction with the services received for pain
problem (0-10 NRS) 0.19 (-0.29, 0.67) 0.08 (-0.44, 0.60) -
Adjusted for baseline outcome measure (where applicable), age, gender, widespread pain, area deprivation and a random
effect for GP practice
Continuous outcomes estimated by linear mixed model. *Binary outcome estimated by mixed effect logistic regression; the
estimates are odds ratios and 95% CIs
Page 18 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Online only Supplementary Table 5: Healthcare resource use by trial arm over 12 months.
Results are mean (SD) number of visits unless otherwise stated.
Resource use category Control
(n=318) Intervention
(n=237)
n (%) Mean (SD) n (%) Mean (SD)
NHS
GP 218 (68%) 3.13 (3.95) 153 (64%) 2.85 (3.95)
Practice nurse 82 (26%) 0.87 (3.72) 52 (22%) 0.93 (4.21)
Physiotherapist 106 (33%) 1.93 (5.19) 96 (41%) 2.33 (5.10)
Orthopaedic surgeon 67 (21%) 0.47 (1.12) 36 (15%) 0.36 (1.01)
Rheumatologist 26 (8%) 0.16 (0.66) 12 (6%) 0.08 (0.39)
Acupuncturist 8 (3%) 0.13 (1.15) 5 (2%) 0.04 (0.31)
Chiropractor 7 (2%) 0.09 (0.81) 4 (2%) 0.03 (0.34)
Occupational therapist 15 (5%) 0.18 (1.16) 12 (5%) 0.11 (0.56)
Other healthcare professionals 29 (9%) 0.27 (1.06) 20 (8%) 0.20 (0.81)
Private
Physiotherapist 18 (6%) 0.29 (1.72) 14 (6%) 0.71 (4.86)
Orthopaedic surgeon 7 (2%) 0.04 (0.33) 4 (2%) 0.03 (0.23)
Rheumatologist 0 0.00 (-) 1 (0.5%) 0.01 (0.13)
Acupuncturist 4 (1%) 0.07 (0.70) 8 (3%) 0.13 (0.92)
Chiropractor 9 (3%) 0.21 (1.94) 5 (2%) 0.15 (1.09)
Occupational therapist 0 0.00 (-) 1 (0.5%) 0.02 (0.25)
Other healthcare professionals 6 (2%) 0.08 (0.73) 3 (1%) 0.17 (2.22)
Other resource use
Investigations (MRI, CT, X-rays,
“scan”)
124 (39%) 1.88 (8.67) 86 (36%) 0.81 (1.52)
Injections 27 (8%) 0.16 (0.56) 19 (8%) 0.19 (0.93)
Inpatient stay 29 (9%) 0.65 (3.12) 22 (9%) 0.56 (3.82)
Prescribed Medication (n, %) 255 (80%) - 185 (78%) -
‘Over the counter’ treatments (n,
%) 203 (63%) - 141 (59%)
Work-related outcomes
Time-off work due to
musculoskeletal condition 20 (18%) - 19 (19%)
Work absence days due to
musculoskeletal condition 10.28 - 8.34 -
Page 19 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Section/Topic Item No
Standard Checklist item
Extension for cluster designs
Page number
Title and abstract
1a Identification as a randomised trial in the title
Identification as a cluster randomised trial in the title
1
1b Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts)i,ii
See table 2 1
Introduction
Background and objectives
2a Scientific background and explanation of rationale
Rationale for using a cluster design
2
2b Specific objectives or hypotheses
Whether objectives pertain to the the cluster level, the individual participant level or both
2
Methods
Trial design 3a Description of trial design (such as parallel, factorial) including allocation ratio
Definition of cluster and description of how the design features apply to the clusters
3
3b Important changes to methods after trial commencement (such as eligibility criteria), with reasons
n/a
Participants 4a Eligibility criteria for participants
Eligibility criteria for clusters
3 + protocol
4b Settings and locations where the data were collected
3
Interventions 5 The interventions for each group with sufficient details to allow replication, including how and when they were actually administered
Whether interventions pertain to the cluster level, the individual participant level or both
3 + protocol
Outcomes 6a Completely defined pre-specified primary and secondary outcome measures, including how and when they were assessed
Whether outcome measures pertain to the cluster level, the individual participant level or both
n/a as pilot
Page 20 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
For peer review only
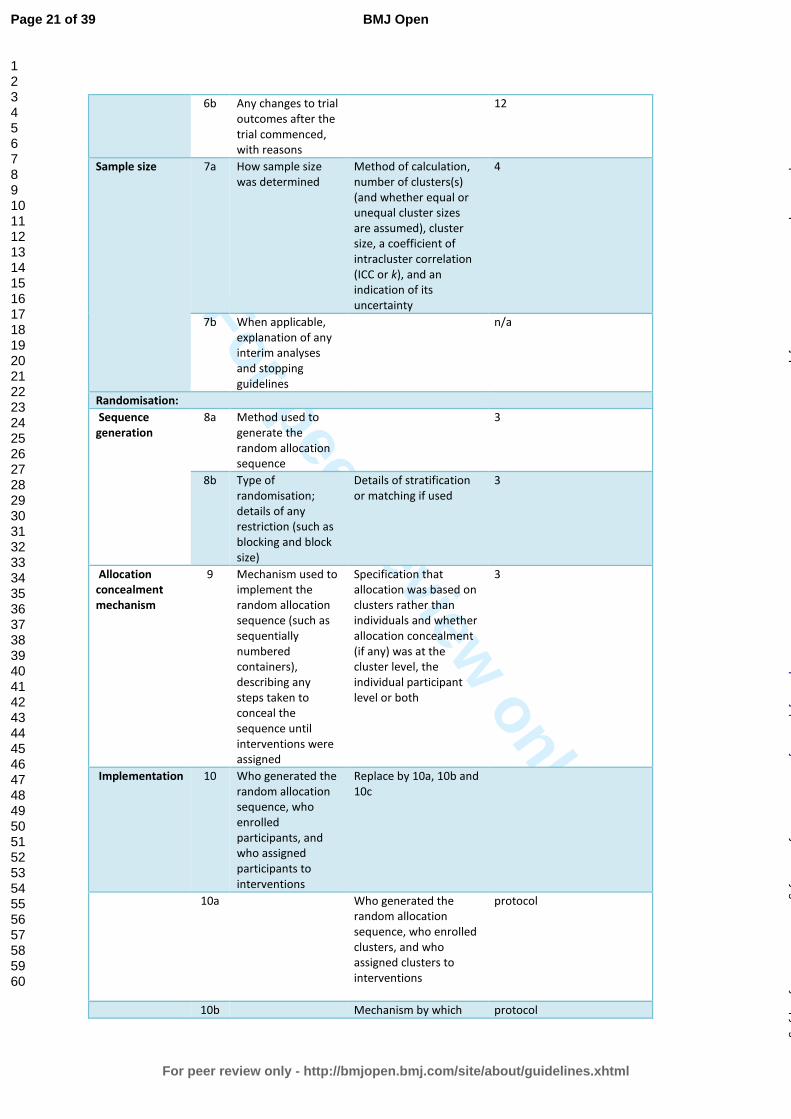
6b Any changes to trial outcomes after the trial commenced, with reasons
12
Sample size 7a How sample size was determined
Method of calculation, number of clusters(s) (and whether equal or unequal cluster sizes are assumed), cluster size, a coefficient of intracluster correlation (ICC or k), and an indication of its uncertainty
4
7b When applicable, explanation of any interim analyses and stopping guidelines
n/a
Randomisation:
Sequence generation
8a Method used to generate the random allocation sequence
3
8b Type of randomisation; details of any restriction (such as blocking and block size)
Details of stratification or matching if used
3
Allocation concealment mechanism
9 Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned
Specification that allocation was based on clusters rather than individuals and whether allocation concealment (if any) was at the cluster level, the individual participant level or both
3
Implementation
10 Who generated the random allocation sequence, who enrolled participants, and who assigned participants to interventions
Replace by 10a, 10b and 10c
10a Who generated the random allocation sequence, who enrolled clusters, and who assigned clusters to interventions
protocol
10b Mechanism by which protocol
Page 21 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
individual participants were included in clusters for the purposes of the trial (such as complete enumeration, random sampling)
10c From whom consent was sought (representatives of the cluster, or individual cluster members, or both), and whether consent was sought before or after randomisation
protocol
Blinding 11a If done, who was blinded after assignment to interventions (for example, participants, care providers, those assessing outcomes) and how
3
11b If relevant, description of the similarity of interventions
Statistical methods
12a Statistical methods used to compare groups for primary and secondary outcomes
How clustering was taken into account
protocol
12b Methods for additional analyses, such as subgroup analyses and adjusted analyses
protocol
Results
Participant flow (a diagram is strongly recommended)
13a For each group, the numbers of participants who were randomly assigned, received intended treatment, and were analysed for the primary outcome
For each group, the numbers of clusters that were randomly assigned, received intended treatment, and were analysed for the primary outcome
Figure 1
13b For each group, losses and exclusions after randomisation, together with reasons
For each group, losses and exclusions for both clusters and individual cluster members
Figure 1
Recruitment 14a Dates defining the 5
Page 22 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
periods of recruitment and follow-up
14b Why the trial ended or was stopped
n/a
Baseline data 15 A table showing baseline demographic and clinical characteristics for each group
Baseline characteristics for the individual and cluster levels as applicable for each group
Table1, page 6
Numbers analysed
16 For each group, number of participants (denominator) included in each analysis and whether the analysis was by original assigned groups
For each group, number of clusters included in each analysis
Figure 1
Outcomes and estimation
17a For each primary and secondary outcome, results for each group, and the estimated effect size and its precision (such as 95% confidence interval)
Results at the individual or cluster level as applicable and a coefficient of intracluster correlation (ICC or k) for each primary outcome
7 but as pilot exploratory
17b For binary outcomes, presentation of both absolute and relative effect sizes is recommended
Ancillary analyses
18 Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing pre-specified from exploratory
9-10
Harms 19 All important harms or unintended effects in each group (for specific guidance see CONSORT for harmsiii)
5
Discussion
Limitations 20 Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of
11
Page 23 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
analyses
Generalisability 21 Generalisability (external validity, applicability) of the trial findings
Generalisability to clusters and/or individual participants (as relevant)
n/a
Interpretation 22 Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence
11
Other information
Registration 23 Registration number and name of trial registry
1
Protocol 24 Where the full trial protocol can be accessed, if available
2 (http://pilotfeasibilitystudies. biomedcentral.com/ articles/10.1186/s40814-015-0020-4
Funding 25 Sources of funding and other support (such as supply of drugs), role of funders
12
i Hopewell S, Clarke M, Moher D, Wager E, Middleton P, Altman DG, et al. CONSORT
for reporting randomised trials in journal and conference abstracts. Lancet 2008, 371:281-283
ii Hopewell S, Clarke M, Moher D, Wager E, Middleton P, Altman DG at al (2008)
CONSORT for reporting randomized controlled trials in journal and conference abstracts: explanation and elaboration. PLoS Med 5(1): e20
iii Ioannidis JP, Evans SJ, Gotzsche PC, O'Neill RT, Altman DG, Schulz K, Moher D. Better reporting of harms in randomized trials: an extension of the CONSORT statement. Ann Intern Med 2004; 141(10):781-788.
Page 24 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
For peer review only
STUDY PROTOCOL Open Access
A pilot cluster randomised controlled trialto investigate the addition of direct accessto physiotherapy to usual GP-led primarycare for adults with musculoskeletal pain:the STEMS pilot trial protocol(ISRCTN23378642)Annette Bishop1*, Stephanie Tooth1, Joanne Protheroe1, Chris Salisbury2, Reuben O Ogollah1, Sue Jowett3,Elaine M Hay1, Nadine E Foster1 and on behalf of the STEMS study team
Abstract
Background: Musculoskeletal problems are common, accounting for up to 30 % of general practitioner (GP)consultations and are a major cause of chronic disability worldwide. Demand for health care for musculoskeletalconditions is likely to continue to rise given the ageing population and the increasing impact of these commonpainful conditions. Physiotherapists are well equipped to deliver evidence-based management for these conditions.Direct access allows patients to access physiotherapy without seeing their GP or another referring practitioner first;however, for most patients in the UK, access to National Health Service physiotherapy is controlled through GP referral.
Methods/Design: The aim of this pilot, pragmatic, cluster trial is to assess the feasibility of a future large trial tocompare the clinical and cost-effectiveness of the additional offer of direct access to physiotherapy versus continuingwith usual GP-led primary care alone for adults with common musculoskeletal problems. The pilot will focus onprocess outcomes to assess feasibility, although performance of the likely outcomes of a main trial will also beassessed. This is a two-arm parallel, cluster RCT where GP practices are the units of randomisation (the clusters), yetdata are collected from individual patients with musculoskeletal problems (the participants). A direct access service willbe set up in the participating physiotherapy service to provide the option of direct access to patients of theintervention arm practices. Inclusion criteria are broad to reflect the ‘real-world’ operation of an NHS physiotherapydirect access service for patients with musculoskeletal pain. Data collection will be through patient self-reportedquestionnaires at baseline, 2, 6 and 12 months and medical record review.
Discussion: No previous trials have been conducted into direct access to physiotherapy for patients withmusculoskeletal problems. The strengths of the STEMS pilot trial are its size, the length of follow-up, and collection ofprocess, clinical and cost outcomes to fully inform a future main trial to meet calls to provide robust trial evidence ofthe impact on clinical outcomes, work loss and costs to provide clinicians and service funders with the high quality trialdata they need to guide decisions on the best models of care.
Trial registration: The STEMS pilot trial is registered at Current Controlled Trials: ISRCTN23378642
Keywords: Physiotherapy, Direct access, Self-referral, Musculoskeletal, Cluster trial, Pilot
* Correspondence: [email protected] Institute for Primary Care & Health Sciences, Keele University,Keele, Staffordshire ST5 5BG, UKFull list of author information is available at the end of the article
© 2015 Bishop et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium,provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 DOI 10.1186/s40814-015-0020-4
Page 25 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
BackgroundMusculoskeletal problems are common and costly andincrease with age. Musculoskeletal conditions accountfor up to 30 % of general practitioner (GP) consultations[1], and yet it is estimated that only between 30–40 % ofindividuals with musculoskeletal problems consult theirGP [2–4]. The Global Burden of Disease Study showsthat musculoskeletal conditions are a major cause ofchronic disability worldwide and have increased mark-edly in the last decade [5]. Given the ageing populationand the increasing impact of these common painful con-ditions, the demand for musculoskeletal healthcare is setto rise and health care delivery systems will need to de-velop a ‘coherent policy for dealing with musculoskeletaldisorders’ [5]. Best evidence for many of these musculo-skeletal conditions recommends treatments such as ad-vice, education, exercise, manual therapy and acupuncture[1, 6, 7]. Such treatments are cost-effective [8] and arethose that professionals such as physiotherapists areequipped to deliver. Early physiotherapy intervention formusculoskeletal problems reduces sick leave and helpsprevent acute problems becoming chronic [1, 9–12].However, for most patients in the UK, access to NationalHealth Service (NHS) physiotherapy is controlled throughGP referral.Direct access to physiotherapy is a system of access in
which ‘patients are able to refer themselves to a physio-therapist directly without having to see anyone else first orwithout being told to refer themselves by a health profes-sional’ [13]. Although direct access is well established inprivate practice in the UK and in other countries includingAustralia, the Netherlands, some states within the USAand in Scotland [14–17], uptake in the NHS in Englandhas been very limited. Funders of physiotherapy servicesexpress concerns about creating excessive demand and as-sociated costs and where direct access services have beenestablished at least one in England has been stopped dueto funding being withdrawn [18].To date, evidence about direct access to physiotherapy
comes from observational studies only. These have sug-gested that direct access may reduce GP workload [19]with estimates of a 20 % reduction in multiple GP consul-tations [20]. An evaluation in the Netherlands reportedthat in the first 12 months of direct access, patients refer-ring themselves accounted for 22–28 % of all physiother-apy referrals [14, 21]. Reported patient benefits of directaccess are greater freedom of choice and improved accessto musculoskeletal care [13, 14, 19, 22], since direct accessallows the patient to opt for physiotherapy when they arein most need. There are also some suggested cost-benefits, with GP referral costing £133 an episode and anepisode of care through direct access costing £100 [23].A global review of direct access to physiotherapy has
identified professional legislation, the medical profession,
politicians and policy makers as both barriers to and fa-cilitators of direct access [24]. A European-focused re-view of direct access services concluded that clinicians,managers and service funders need high quality trialdata on both clinical and cost-effectiveness to guide de-cisions on the best models of care [25]. In addition, anindependent evaluation of the observational UK Depart-ment of Health pilots of direct access to physiotherapy[13] concluded that robust evidence of the impact onclinical outcomes, work loss and costs are lacking due toimportant flaws in observational study designs and thata randomized controlled trial (RCT) comparing areasthat do and do not offer direct access is required to pro-vide robust evidence about direct access [26].The most appropriate design for a RCT to evaluate
direct access is a non-inferiority cluster RCT that com-pares the clinical and cost-effectiveness of the additionaloffer of direct access to physiotherapy versus continuingwith usual GP-led care alone for patients with musculo-skeletal conditions in primary care. However, given thatthis involves developing a new direct access service, it isimportant to conduct feasibility and pilot work first inorder to fully inform a future main trial.
Overall aimThe overall aim of the STEMS pilot trial is to assess thefeasibility of a future large trial to compare the clinicaland cost-effectiveness of the additional offer of directaccess to physiotherapy versus continuing with usualGP-led primary care alone for adults with common mus-culoskeletal problems.
ObjectivesThe objectives of the STEMS pilot trial include bothprocess and research objectives. Analysis of the processobjectives will enable the feasibility of a larger cluster RCTto be assessed. They focus on the feasibility of workingwith general practices and physiotherapy services to de-velop and set up a direct access to physiotherapy service,the acceptability of direct access and the ability to both re-cruit and retain participants in the research evaluation.
Process objectives
1. To assess the number of practices approached andagreeing to take part (baseline) and the engagementof GP practices and physiotherapy services to stay inthe pilot trial through follow-up (12 months)
2. To develop and test approaches to market a newdirect access service in ways that ensure a sufficientproportion (at least 20 %) of patients accessphysiotherapy through self-referral to make a maintrial feasible (assessed through referral methods asphysiotherapy service)
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 2 of 15
Page 26 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
3. To assess the feasibility of establishing aphysiotherapy direct access service that can respondto demand and avoid increases in waiting times orstaffing levels (monitored throughout therecruitment period)
4. To estimate participant recruitment rates in bothcontrol and intervention practices (assessed at endof recruitment)
5. To explore any evidence of selection bias inparticipants recruited to the research evaluationfrom the control and intervention practices(assessed through participant characteristics atbaseline)
6. To estimate retention of participants in the researchevaluation at each follow-up time-point across bothcontrol and intervention practices
Research objectivesThe pilot trial will also provide a useful test of outcomedata collection methods, including key clinical out-comes, and provide information on the likely changes inthese outcomes in the control and intervention groups.Whilst a main trial will provide the definitive test of thedifference between trial groups on these clinical out-comes, the pilot has the following research objectives:
1. To investigate likely changes in the primary clinicaloutcome measure (physical health measured usingthe SF36v2 Physical Component Summary)
2. To investigate likely changes in secondary outcomemeasures (overall perceived change, mental health,pain self-efficacy, quality of life, understanding of thecondition, experience of care and convenience andaccessibility of service)
3. To provide an early estimate of the costs, bothhealthcare and societal costs, in both interventionand control groups
4. To explore the use of willingness to pay (WTP)methodology to capture the strength of patientpreferences for direct access to NHS physiotherapy
5. To confirm the parameters needed for a realisticsample size calculation for a future main cluster RCT
MethodsDesignThe design is a pilot, pragmatic, cluster RCT in generalpractice and physiotherapy services. The most appropri-ate trial design is a simple, two-arm parallel, clusterRCT where GP practices are the units of randomisation(the clusters), yet data are collected from individual pa-tients with musculoskeletal problems (the participants).This design overcomes the problem of contaminationbetween arms and the problems associated with indi-vidually consenting and randomising patients to a trial
testing service-level changes. A main trial would employ anon-inferiority design as it will be essential that the inter-vention is as least as good as usual GP-led care in terms ofpatients’ clinical outcomes (physical health measuredusing the SF36v2 Physical Component Summary).A repeated measures design will be adopted, whereby
participants will complete the questionnaires at baseline,2, 6 and 12 months. Each participant’s involvement inthe trial is for 12 months, during which time they will allhave access to usual GP-led primary care. No analysis ofclinical outcomes will be undertaken until the 12-monthfollow-up time-point.
Setting and clustersThe setting is primary care in England for adults withmusculoskeletal problems (GP practices and linked NHSphysiotherapy services). GP practices are the unit of ran-domisation, and thus, patients follow the care pathwaysto which the practice is randomised. In this pilot, RCTpractices will be stratified only on practice size, but in amain trial, practices would also ideally be stratified byindex of deprivation. Randomisation of GP practices willbe undertaken by an independent statistician. GP prac-tices will be randomised to one of two arms, either tocontinue with usual GP-led primary care for musculo-skeletal patients with the addition of the offer of a self-referral physiotherapy pathway (intervention group) orto continue with usual GP-led primary care alone (usualcare control group). Practices will be randomised accord-ing to a computer-generated random numbers stratifiedby the practice size (small or large) in the ratio 1:1. In amain study, we would plan to further stratify by practicesetting and area level deprivation (through minimisation)in order to ensure balance in key practice characteristicsin each arm of the trial.GP practices are eligible to take part if they meet the
following criteria: they are within the Vale Royal ClinicalCommissioning Group area of Cheshire and the ClinicalResearch Network (CRN); they are a group practice, cur-rently referring musculoskeletal patients to NHS physio-therapy services; they do not currently offer directaccess to physiotherapy; and they are willing to test dir-ect access. The balance between scientific considerationsand the need for consent is a known issue for cluster tri-als [27]. Informed consent for practices to participatewill be provided by the senior GP partner in each prac-tice acting as ‘guardian’ for patients in their care. Pa-tients will follow the care to which their practice israndomised with identical patient information for botharms providing general information about the study,explaining that their local musculoskeletal services arebeing evaluated using patient self-reported clinical out-comes and medical record review. Individual patientswill therefore be able to opt out of data collection.
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 3 of 15
Page 27 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
ParticipantsThe inclusion criteria have been designed to be as broadas possible to reflect the ‘real-world’ operation of an NHSphysiotherapy direct access service for patients with mus-culoskeletal pain.Inclusion criteria are all adults consulting participating
GP practices or physiotherapy services with musculoskel-etal problems (for either their first consultation for a newepisode of musculoskeletal pain or a reconsultation).Exclusion criteria are: under 18 years old at the time
of consultation; consulting with non-musculoskeletalproblems; unable to provide their own consent to theresearch evaluation; undergoing palliative care; severelearning disabilities; housebound or in nursing home ac-commodation; and unable to communicate in English(although all potential participants will be offered theopportunity to telephone a research nurse, blinded topractice allocation, for help in completing the paperwork).
Participant identification and recruitmentFollowing randomisation of GP practices, potentially eli-gible participants will be identified through one of threemethods.Method 1: Patients consulting GP practices with a
musculoskeletal problem will have a musculoskeletalRead code1 (entered by GPs or nurse practitioners) en-tered into their computerised medical record. A memberof the GP practice team, or CRN staff, will download thedetails of patients with these Read codes twice weeklychecking for exclusion criteria and then forward thesedetails to a CRN administrator. GPs will be able to ex-clude any patients they perceive as being particularlyvulnerable and unsuitable to approach for involvementin research by using a dedicated exclusion code set upfor the study.Method 2: In addition, for those GP practices rando-
mised to also offer direct access to physiotherapy, pa-tients who self-refer to physiotherapy will be identifiedwhen they forward a completed self-referral form to thephysiotherapy service or telephone the physiotherapy ad-ministrator for help in completing a form. As in method1 the details of identified patients will be forwarded to aCRN administrator.Method 3: Patients referred by GPs or practice nurses
to the physiotherapy service, but not identified inmethod 1 due to an absence of an appropriate Read codein the computerised medical records, will be identifiedfrom the physiotherapy administration database. Aphysiotherapy administrator will download the details ofall patients referred from the participating GP practicestwice weekly and forward these details to a CRN admin-istrator. Duplication checks will ensure that eligible pa-tients are not invited to take part in the research morethan once.
All eligible patients will be mailed a STEMS studypack (letter of invitation, participant information leaflet(see Additional file 1), consent form, baseline question-naire and pre-paid return envelope). Participants willnot be individually consented to randomisation, ratherparticipants in both arms of the trial will be asked togive written consent to take part in a study investigatingmusculoskeletal problems and local health services, con-sisting of the baseline and follow-up questionnaires (at2, 6 and 12 months) and to allow the research team ac-cess to their medical records to review healthcare usefor their musculoskeletal problem. Patients interested inparticipating will be offered the option of telephoning aresearch nurse, blinded to practice allocation, who willanswer any questions and support those who need it tocomplete the consent form and questionnaire over thephone. Participants who consent to participation will re-turn the completed questionnaire and consent form tothe research centre, and the research team will then haveaccess to their personal identification details. Partici-pants completing the consent form but having missingdata at baseline on the primary outcome measure (theSF36v2), such that a Physical Component Summaryscore cannot be calculated, will be contacted by telephoneto collect the missing data. At each data collection time-point (baseline, 2, 6 and 12 months), non-responderswill be mailed a postcard reminder 2 weeks after mail-ing of the trial study pack and a repeat study pack2 weeks after the reminder postcard. At 6- and 12-month follow-up, non-responders will subsequently bemailed a very brief minimum data questionnaire, con-sisting of the SF-36v2 and the single Global Assessmentof Change question only. Telephone collection of mini-mum data will be attempted for the remaining non-responders.This method of recruitment has been used successfully
in previous studies. Our processes ensure that all eligiblepatients will be identified, recruited through postal studypacks (with telephone support where needed) with iden-tical information about the evaluation study given tothose in both arms of the trial [27]. Participants’ GPs willbe notified of their consent to participate in the researchevaluation. Participating general practices will be sup-ported to assist with identification of potentially eligibleparticipants for the STEMS pilot trial through smallpractice payments to reimburse their time for screeningpatient lists. The physiotherapy service will be supportedto participate through financial reimbursement for thetime taken from service delivery for participation in thetraining programme. Participants will not receive anypayments or other incentives to take part in the STEMSpilot trial or to return baseline or follow-up question-naires. A flowchart illustrating the STEMS pilot trial isshown in Fig. 1.
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 4 of 15
Page 28 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
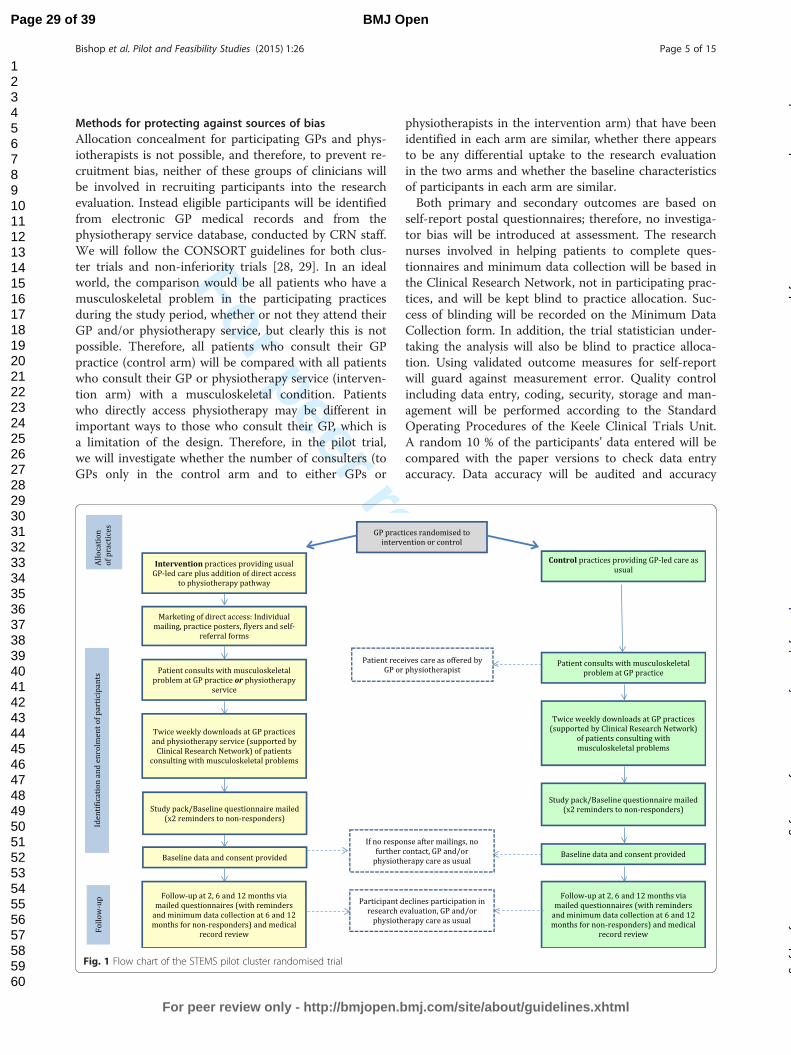
For peer review only
Methods for protecting against sources of biasAllocation concealment for participating GPs and phys-iotherapists is not possible, and therefore, to prevent re-cruitment bias, neither of these groups of clinicians willbe involved in recruiting participants into the researchevaluation. Instead eligible participants will be identifiedfrom electronic GP medical records and from thephysiotherapy service database, conducted by CRN staff.We will follow the CONSORT guidelines for both clus-ter trials and non-inferiority trials [28, 29]. In an idealworld, the comparison would be all patients who have amusculoskeletal problem in the participating practicesduring the study period, whether or not they attend theirGP and/or physiotherapy service, but clearly this is notpossible. Therefore, all patients who consult their GPpractice (control arm) will be compared with all patientswho consult their GP or physiotherapy service (interven-tion arm) with a musculoskeletal condition. Patientswho directly access physiotherapy may be different inimportant ways to those who consult their GP, which isa limitation of the design. Therefore, in the pilot trial,we will investigate whether the number of consulters (toGPs only in the control arm and to either GPs or
physiotherapists in the intervention arm) that have beenidentified in each arm are similar, whether there appearsto be any differential uptake to the research evaluationin the two arms and whether the baseline characteristicsof participants in each arm are similar.Both primary and secondary outcomes are based on
self-report postal questionnaires; therefore, no investiga-tor bias will be introduced at assessment. The researchnurses involved in helping patients to complete ques-tionnaires and minimum data collection will be based inthe Clinical Research Network, not in participating prac-tices, and will be kept blind to practice allocation. Suc-cess of blinding will be recorded on the Minimum DataCollection form. In addition, the trial statistician under-taking the analysis will also be blind to practice alloca-tion. Using validated outcome measures for self-reportwill guard against measurement error. Quality controlincluding data entry, coding, security, storage and man-agement will be performed according to the StandardOperating Procedures of the Keele Clinical Trials Unit.A random 10 % of the participants’ data entered will becompared with the paper versions to check data entryaccuracy. Data accuracy will be audited and accuracy
Fig. 1 Flow chart of the STEMS pilot cluster randomised trial
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 5 of 15
Page 29 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
rates recorded. Loss to follow-up will be minimised byimplementing standardised reminder procedures andminimal data collection for non-responders. Participantswill be free to withdraw from the research at any timewithout having to give any explanation. Where possible,we will collect information about the reasons for with-drawal. All records will be kept confidential and data setsfor each participant will be identified by the patient’s par-ticipant number. Analysis will be performed on anintention-to-treat (ITT) basis using the full set of availabledata (mixed model and multiple imputation of missingdata). Patients self-referring or being GP-referred receiveequitable treatment, for example, in the length of wait tofirst physiotherapy contact once they are logged on thephysiotherapy administration system. The physiotherapistsparticipating in the trial will provide physiotherapy care topatients from both arms of the trial (initiated from trad-itional GP referral in the control arm versus from bothtraditional GP referral and patient self-referral in the inter-vention arm). As this trial is investigating the addition ofdirect access to physiotherapy, the physiotherapy care pro-vided will be determined by clinical need and assessmentfindings and will therefore be consistent with routine prac-tice and not differ for patients in different arms of the trial.
Description of intervention and control armsControl practices: In GP practices allocated to the con-trol arm patients will continue to be managed accordingto usual GP-led care. This normally consists of a patientconsulting their GP and receiving advice and treatment(often medication but we expect around 20–25 % to bereferred to physiotherapy, or for a diagnostic test orother treatment service). For some patients, it may meanbeing triaged by a practice nurse and managed with ad-vice and/or referral to physiotherapy or other services.Usual GP-led care therefore includes all of these path-ways in participating GP practices but will not includethe offer of direct access to physiotherapy. No additionalinformation on physiotherapy services will be dissemi-nated by the research team to GP practices deliveringusual care. Regular contact with, and feedback to, thecontrol practices through CRN staff, a GP research fa-cilitator and from the PI and study team will help ensuresmooth trial operationalisation.Intervention practices: In practices allocated to the
intervention arm patients will continue to be able to ac-cess care via usual GP-led care pathways (as describedabove) in addition to direct access to physiotherapy formusculoskeletal patients. Direct access will allow adultswith musculoskeletal problems to refer themselves tothe physiotherapy service. Those opting for direct accessto physiotherapy will complete a self-referral form,which will be available at their GP practice or, wherepossible, online. The self-referral form will include
questions about ‘red flag’ symptoms, indicative of sus-pected serious pathology that would require urgent med-ical investigation, with advice to patients to contact theirGP if one or more of these symptoms are present. Sub-mitted self-referral forms will be reviewed by a seniorphysiotherapist who will identify, based on existingphysiotherapy service criteria, whether the referral is ap-propriate and whether classed as urgent or routine. Ur-gent cases will be offered the next available appointmentwhereas routine cases will join all other routine patientson a waiting list for the physiotherapy service and beseen in order of receipt of referral. In cases where the re-ferral is considered inappropriate for physiotherapymanagement, the patient will be contacted by thephysiotherapy service and signposted to the most appro-priate practitioner or service. Direct access to physio-therapy will be actively marketed in the interventionpractices to ensure that all registered patients are awareof this option [30]. This will start eight weeks prior toparticipant recruitment to the research evaluation andcontinue until patient recruitment to the trial has fin-ished. Marketing will include communications withpractice staff (clinical and administrative teams), practiceposters, rolling presentations in practice waiting areas(where possible), patient flyers and self-referral forms inpractices. In order to best ensure that all adults in thepractice become aware of the availability of direct access,an information letter and direct access flyer will bemailed to all registered adult patients at each interven-tion practice. A phased approach to the marketing of thenew service is planned, over 8 weeks, so that demandfor physiotherapy through direct access can be moni-tored. The posters, flyers and forms will clearly explainhow patients can directly access the service. The physio-therapy administrator will input patients’ data into thetrial registration database and be responsible for arran-ging face-to-face physiotherapy appointments at con-venient times and dates following prioritisation of thereferrals by senior physiotherapists in the service. Evenwith the offer of direct access, we anticipate that manypatients will opt to consult their GP as usual. Therefore,in the intervention practices, patients may consult theirpractice and be referred to physiotherapy, either bywritten referral or be recommended to access physio-therapy by GPs or nurse practitioners (GP or nurse rec-ommended self-referral) or choose to directly accessphysiotherapy without contacting their GP practice (trueself-referral). Each patient’s pathway will be recorded.
Support for physiotherapists providing the direct accessserviceAlthough physiotherapists are autonomous practitionerson qualification, additional education and developmentneeds of physiotherapists have been identified as part of
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 6 of 15
Page 30 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
the work-up of the pilot trial and a training programme isplanned to address these. The brief training programmewill include the following content: prevalence and identifi-cation of red flags, serious pathology and medical mas-queraders, review of common over-the-counter andprescribed medications for musculoskeletal pain patients,the provision of occupational/work advice to patients andinformation about the practicalities of the trial, includingdelivery of the trial protocols and identification of any ser-ious pathologies or serious adverse events. Continuingsupport of physiotherapists delivering the direct accessservice will take the form of a mentoring programme pro-vided by the lead musculoskeletal physiotherapist in theteam and another senior physiotherapist who has experi-ence of providing direct access services. The physiother-apy service leads will also agree pathways for patientsusing direct access with suspected serious pathologywho are in need of medical attention, or who may re-quire a fit note or a prescription from their GP. Approxi-mately 18 physiotherapists will participate in the trainingprogramme, half of whom will initially provide the newdirect access physiotherapy service and the remainder willbe able to provide cover as needed throughout the dur-ation of the trial, for example for holiday periods.
Outcome measuresProcess outcomes: Process outcomes will determine if afuture main trial is possible and desirable. Anonymisedprocess outcome data will be collected from GP recordsand physiotherapy administration databases and self-referral forms. Health service process outcomes includethe proportion of patients not referred to physiotherapyservices, those referred to physiotherapy and the num-ber of patients directly accessing physiotherapy in theintervention practices, proportion of ‘recommendedself-referral’ and ‘true self-referral’ in the direct accesspathway, waiting times for treatment (time from loggingof referral to first physiotherapy appointment), number ofGP and NHS physiotherapy consultations for musculo-skeletal problems and non-attended physiotherapy ap-pointments (DNA rates). Research process outcomesinclude estimation of recruitment rates, exploration of evi-dence of selection bias and follow-up rates at each time-point with differences in the control and interventionpractices explored to identify sources of bias. A summaryof the process measures is shown in Table 1.Clinical outcomes: Data collection will include the col-
lection of clinical and cost data through patient self-report questionnaires at baseline and 2, 6 and 12 monthsfollow-up. The primary clinical outcome is physicalhealth measured using the SF36v2 Physical ComponentSummary. A summary of the clinical outcomes andother measures included in each questionnaire is shownin Table 2.
Adverse eventsThe occurrence of adverse events from all interventionswill be monitored and assessed using case report forms,contact with the trial coordinator, physiotherapist report,and follow-up questionnaires. However, as the interven-tion is the introduction of a direct access pathway andthe treatments received will be the same as in usual
Table 1 STEMS pilot trial process measures
Engagement of GP practices and PT services
Physiotherapy site recruitment rate to participate in STEMS study
GP Practice recruitment rate to participate in STEMS study
Research evaluation
Recruitment rate to the research evaluation—all adults withmusculoskeletal conditions
Recruitment rate to the research evaluation—‘true self-referral’a patients
Recruitment rate to the research evaluation—‘recommendedself-referral’b patients
Retention rates to research evaluation at 2, 6 and 12 months follow-up
GP practice characteristics
Number of GPs and nurse practitioners per practice
Number of patients and number of adults registered at practice
GP consultation rates for adults with musculoskeletal conditions(before and during study)
Physiotherapy team characteristics
Number of physiotherapists working in the physiotherapy service(in total and STEMS trained)
Seniority of physiotherapists in the physiotherapy service(in total and STEMS trained)
Physiotherapy service
Physiotherapy service GP referral rate (before and during study)
Physiotherapy service ‘true self-referral’a rate
Physiotherapy service ‘recommended self-referral’b rate
Non-attendance rates at physiotherapy site for GP referrals(before and during study) and for self-referrals during study
Number of physiotherapy consultations for GP referrals, ‘true self-referral’and ‘recommended self-referral’ patients in the intervention practices
Number of self-referring patients deemed unsuitable at each stage inthe direct access pathway
Onward referral rate from physiotherapy (to GP, other services) for GPreferrals, ‘true self-referral’ and ‘recommended self-referral’
Physiotherapy waiting time (month-by-month) from 12 months prior tointroduction of direct access to end of study
Number of patient complaints about direct access at physiotherapy site
Monitoring of safety
Number of cases of missed serious pathology in patients directlyaccessing physiotherapy
Number of adverse events in GP-referred, ‘true self-referral’‘recommended self-referral’aThose who are prompted by their GP or practice nurse to accessphysiotherapy carebThose who directly access physiotherapy care without prompting by their GPor practice nurse
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 7 of 15
Page 31 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
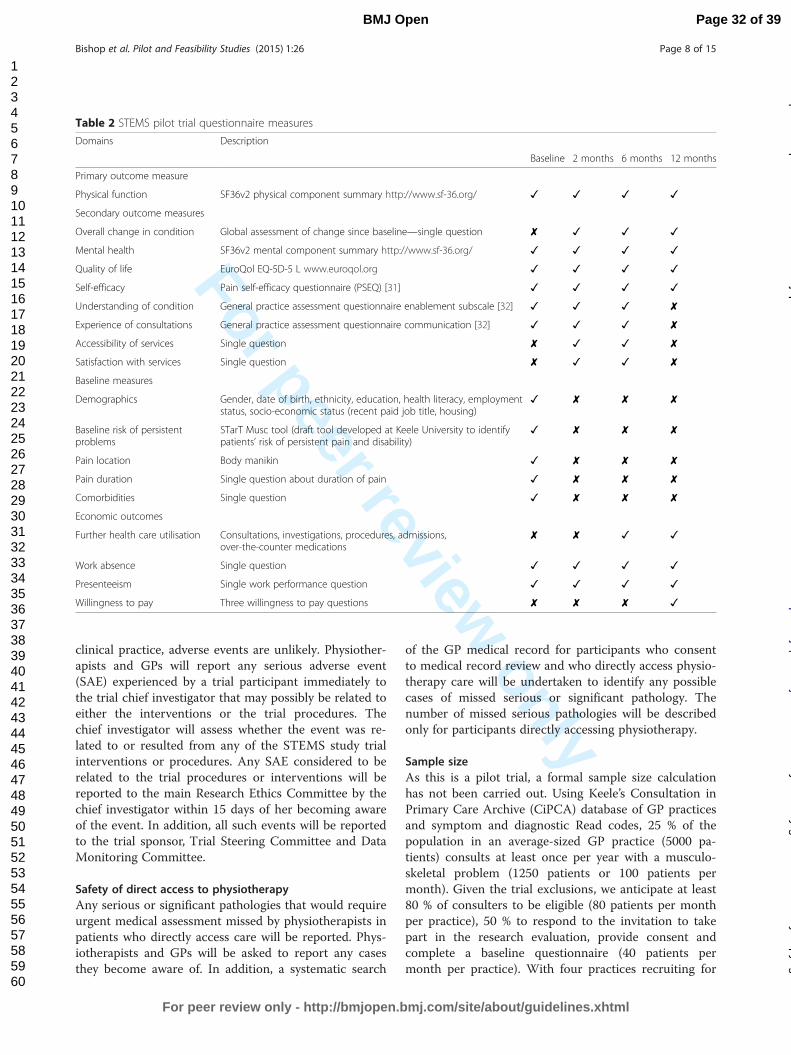
For peer review only
clinical practice, adverse events are unlikely. Physiother-apists and GPs will report any serious adverse event(SAE) experienced by a trial participant immediately tothe trial chief investigator that may possibly be related toeither the interventions or the trial procedures. Thechief investigator will assess whether the event was re-lated to or resulted from any of the STEMS study trialinterventions or procedures. Any SAE considered to berelated to the trial procedures or interventions will bereported to the main Research Ethics Committee by thechief investigator within 15 days of her becoming awareof the event. In addition, all such events will be reportedto the trial sponsor, Trial Steering Committee and DataMonitoring Committee.
Safety of direct access to physiotherapyAny serious or significant pathologies that would requireurgent medical assessment missed by physiotherapists inpatients who directly access care will be reported. Phys-iotherapists and GPs will be asked to report any casesthey become aware of. In addition, a systematic search
of the GP medical record for participants who consentto medical record review and who directly access physio-therapy care will be undertaken to identify any possiblecases of missed serious or significant pathology. Thenumber of missed serious pathologies will be describedonly for participants directly accessing physiotherapy.
Sample sizeAs this is a pilot trial, a formal sample size calculationhas not been carried out. Using Keele’s Consultation inPrimary Care Archive (CiPCA) database of GP practicesand symptom and diagnostic Read codes, 25 % of thepopulation in an average-sized GP practice (5000 pa-tients) consults at least once per year with a musculo-skeletal problem (1250 patients or 100 patients permonth). Given the trial exclusions, we anticipate at least80 % of consulters to be eligible (80 patients per monthper practice), 50 % to respond to the invitation to takepart in the research evaluation, provide consent andcomplete a baseline questionnaire (40 patients permonth per practice). With four practices recruiting for
Table 2 STEMS pilot trial questionnaire measures
Domains Description
Baseline 2 months 6 months 12 months
Primary outcome measure
Physical function SF36v2 physical component summary http://www.sf-36.org/ ✓ ✓ ✓ ✓
Secondary outcome measures
Overall change in condition Global assessment of change since baseline—single question ✘ ✓ ✓ ✓
Mental health SF36v2 mental component summary http://www.sf-36.org/ ✓ ✓ ✓ ✓
Quality of life EuroQol EQ-5D-5 L www.euroqol.org ✓ ✓ ✓ ✓
Self-efficacy Pain self-efficacy questionnaire (PSEQ) [31] ✓ ✓ ✓ ✓
Understanding of condition General practice assessment questionnaire enablement subscale [32] ✓ ✓ ✓ ✘
Experience of consultations General practice assessment questionnaire communication [32] ✓ ✓ ✓ ✘
Accessibility of services Single question ✘ ✓ ✓ ✘
Satisfaction with services Single question ✘ ✓ ✓ ✘
Baseline measures
Demographics Gender, date of birth, ethnicity, education, health literacy, employmentstatus, socio-economic status (recent paid job title, housing)
✓ ✘ ✘ ✘
Baseline risk of persistentproblems
STarT Musc tool (draft tool developed at Keele University to identifypatients’ risk of persistent pain and disability)
✓ ✘ ✘ ✘
Pain location Body manikin ✓ ✘ ✘ ✘
Pain duration Single question about duration of pain ✓ ✘ ✘ ✘
Comorbidities Single question ✓ ✘ ✘ ✘
Economic outcomes
Further health care utilisation Consultations, investigations, procedures, admissions,over-the-counter medications
✘ ✘ ✓ ✓
Work absence Single question ✓ ✓ ✓ ✓
Presenteeism Single work performance question ✓ ✓ ✓ ✓
Willingness to pay Three willingness to pay questions ✘ ✘ ✘ ✓
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 8 of 15
Page 32 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
6 months in the pilot trial, we estimate 960 participantsat baseline and 80 % follow-up (n = 768).
AnalysisSince this is a pilot trial, the analyses will focus on de-scribing the key process measures in order to decide if amain trial is feasible and desirable, in addition to finalis-ing the sample size for a future main trial.
Determine engagement of GP practices and thephysiotherapy serviceThe number of GP practices and physiotherapy servicesthat have agreed to participate in the trial will be re-corded and presented as a proportion of the number ofeligible practices approached. Information will be pre-sented that summarises GP practice characteristics (full-time equivalent of GP staff, number of patients andnumber of adults registered at practice and GP consult-ation rates for musculoskeletal patients before and dur-ing pilot trial recruitment as well as the physiotherapyteam characteristics (full-time equivalent staff and theirclinical grades).
Feasibility of study recruitment and retentionThe number of participants identified and recruitedusing each recruitment method will be reported, alongwith the number of participants followed up at eachtime-point. Withdrawals (and where possible, reasonsfor withdrawals) will be reported. A priori, we have de-fined a success criterion of 40 % of the total number ofparticipants invited to be recruited to the research evalu-ation. Whilst a retention rate of 100 % would be ideal,we will consider a rate of 70 % at 6 months follow-upsatisfactory. We will provide the point estimate of theproportion and its 95 % confidence interval (CI). Differ-ence in recruitment uptake rate and follow-up rates ateach time-point will be compared between the interven-tion and control arms.
Feasibility of direct accessAn audit of the feasibility of offering direct access willbe conducted using anonymised data. This will includereporting the number of participants who are referred tophysiotherapy by their GP, those who are ‘recommendedself-referrals’ (prompted by their GP or practice nurse torefer) and those who are ‘true self-referrals’ and the wait-ing time to the first physiotherapy appointment. Figureswill be presented month-by-month for patients usingdirect access as well as the overall totals. The proportionof patients directly accessing care (true and recom-mended self-referrals) compared to all referrals receivedat the physiotherapy site will be calculated to check thesuccess of marketing the direct access service. The aimis to ensure that a minimum of 20 % of the total
physiotherapy caseload during the pilot trial, from prac-tices randomised to the intervention arm, is through dir-ect access. In order to assess the feasibility of establishinga direct access service that can respond to demand, de-scriptive measures of the total number of referrals re-ceived from participating practices and staffing levels inthe participating physiotherapy department will be used toestablish how the physiotherapy service responds to de-mand through waiting time for first physiotherapy ap-pointment. The source by which patients, who access caredirectly, become aware of the direct access service will bepresented and compared in order to establish whichmethods (GP advised, poster, individual mailing, heardfrom a friend and other methods) are most successful inmarketing the service.
Evidence of selection biasSince this is a pilot trial with only four clusters rando-mised, it is likely that there will be some imbalance be-tween participants in each of the treatment arms on oneor more baseline characteristics. Baseline comparisonswill be carried out to detect any substantial differencesbetween participants recruited from the control andintervention arms. This will be done by scrutinising thebaseline table for any serious imbalances in observablebaseline variables and the trends of the imbalance if any.The recruitment rates will also be estimated and com-pared between the control and intervention arms. Wewill examine the size of any imbalances and decide ifthere is evidence of systematic selection bias in the typesof patients being recruited in control versus interventionarms. Any systematic imbalance in the sense that onearm is consistently favoured by the imbalances may notreflect chance alone and may suggest selection bias.
Explore generalisability of the sampleAnonymised data on key baseline characteristics (age, gen-der and index of multiple deprivation (from post-codes)) ofthose who are invited but who do not participate will becompared with those who do participate. Key baselinecharacteristics will be compared between those participantsfollowed up and those lost to follow-up at each time-point.Key characteristics of the participants recruited using eachrecruitment method will be reported. Delays in return ofquestionnaires (>35 days from initial mailing date) will alsobe compared between the two arms.
Analyses of clinical outcomesAnalyses will be conducted for the clinical outcomes, butthis will be treated as exploratory and will be mainly de-scriptive. A baseline table (descriptive statistics and fre-quencies) will compare the demographic and clinicalcharacteristics (gender, age, education, employment status,pain interference with performance at work, type of
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 9 of 15
Page 33 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
accommodation, health literacy, physical health (SF-36v2PCS) and mental health (SF-36v2 MCS), pain location,physical function, pain duration, baseline risk of persistentproblems, comorbidities, pain self-efficacy, understandingof the condition, experience of care and convenience andaccessibility of service) between the two arms. Since thebaseline assessment for the clinical characteristics will becompleted, for many patients, after their initial consult-ation about their musculoskeletal problem, there could beimplications on evaluation and interpretation of thesemeasures as they may not be ‘true baseline’ but ratherpossible ‘outcomes’ at the first time-point. All continuousvariables will be summarised using mean, standard devi-ation, median and interquartile range as appropriate. Thefrequency and percentages of observed levels will be re-ported for all categorical measures.As this is a pilot trial, no emphasis will be put on the
p values for any inferential statistical tests conducted. Amixed effect model, which allows all available data at allthe four time-points to be used and account for missingdata and clustering effect, will be used to estimate atwo-sided 95 % CI to show a credible range for the truedifference in the SF-36v2 PCS subscale between inter-vention and the control arms. The model will be ad-justed for key patient-level baseline characteristics (age,area level deprivation and widespread pain (from mani-kin data)) and a random effect for the GP practices andwill include a treatment-by-time interaction to obtainthe estimates of treatment effect (and 95% CI) at eachfollow-up visit (2, 6 and 12 months). Analyses of the sec-ondary outcomes will be performed similarly.Further analysis will descriptively compare the base-
line characteristics and key clinical outcomes betweenthe participants referred to physiotherapy in the controlpractices with participants self-referring in the inter-vention practices. We will also compare the self-referrers with those that do not self-refer within theintervention group.The pilot data will provide information on the parame-
ters needed for a realistic sample size calculation (mean,standard deviation and treatment effects of the primaryoutcome for the two arms) for a future, main clusterRCT. The intra-cluster correlation (ICC) will be calcu-lated and compared with the estimates from previouslarge primary-care-based trials. However, as we onlyhave 4 GP practices, we expect the estimated ICC to beunreliable given the likely wide confidence intervals.The non-inferiority margin will not be calculated fromthe pilot data as previous research in musculoskeletaldisorders has estimated a minimal clinically importantdifference (MCID) from 2 to 4 points for the SF-36v2Physical Component Summary (PCS) subscale whichwill be used to inform the non-inferiority margin of anyfuture main trial [33–36].
Missing outcome dataSince the primary outcome measure, physical healthmeasured using the SF-36v2 PCS involves scoring indi-vidual items, we do not expect all returned question-naires to have every item on the SF-36 completed. Basedon the recommendation in the scoring manual [33], ascale score should be calculated if a respondent answersat least 50 % of the items in a scale. Missing data will beestimated by the average score, across completed itemsin the same scale for that respondent. If more than 50 %of the items in a scale are left blank, the imputation al-gorithm identifies the scale as ‘not computable’ and sothe respondent is considered to have missing data forthe SF-36v2 component scales.In order to explore the extent and patterns of missing
outcome data, we will report the proportion of missingvalues per item, proportion of participants who completeall items on the questionnaire and the proportion of re-spondents who answer at least 50 % of the items in ascale. The proportion of missing data will also be re-ported for the other key outcomes and compared be-tween the participants from intervention and controlpractices. The characteristics of those lost to follow-upwill also be compared with those who remain in the trialthrough follow-up.
Safety of direct accessAny possible cases of missed serious or significant path-ology will be discussed within the study team. For anypatient where there is evidence to suggest the physio-therapist failed to correctly identify this pathology whenthe patient directly accessed physiotherapy care andmedical intervention was delayed will be reported.
Health economic analysisThe economic analysis will be exploratory, with the aim toinform the design of a full cost-utility analysis alongside afuture main trial. A cost-consequence analysis will be re-ported, describing all the important results relating to costsand consequences for direct access to physiotherapy andusual care arms of the trial. Results will be presented froma health service perspective and a broader societal perspec-tive taking into account patient-incurred costs and prod-uctivity losses. An exploratory willingness to pay (WTP)study [37] will also be conducted to assess the use of thismethodology to measure broader benefits of direct access.Data on costs will be sought from all participants and
from a broad perspective, taking into account healthcare,patient and societal costs. Healthcare resource used will becollected using self-completed questionnaires at 6 and12 months, with a recall period of 6 months in each. Ques-tions will ask patients to recall GP consultations, visits tohealthcare professionals, outpatient appointments, investi-gations or treatments and inpatient stays related to the
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 10 of 15
Page 34 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
index condition. Participants will be asked to distinguishbetween NHS and private practice visits. Resource usedfor the direct access pathway will be directly recorded andcosts attached, staff time (taking into account any in-creased referrals to physiotherapy), materials (posters,flyers, referral forms) and training sessions. GP medicalrecord review of all participants will provide data on rele-vant prescribed medications for all musculoskeletal prob-lems. In addition, information on costs borne by thepatient (e.g. over-the-counter medicines, devices) will becollected via the self-complete questionnaires. Productiv-ity costs will take into account both absenteeism and pres-enteeism and will utilise self-report data on employmentstatus, occupation and time off work and reduced prod-uctivity at work (presenteeism). As this is a pilot trial, thesuitability of questions for collecting cost data directlyfrom patients can be assessed, in order to ensure effectiveresource use and that cost data collection systems areestablished for a larger trial.All patients will be asked to complete the 5-level version
of the EuroQoL-5D (EQ-5D) questionnaire at baseline,6 months and 12 months in order for the quality-adjustedlife years (QALYs) over the 12-month time period to becalculated for each participant. The QALYs combine infor-mation on health-related quality of life and survival.Resource use will be multiplied by unit costs obtained
from standard sources (NHS Reference Costs, BritishNational Formulary, Unit Costs of Health and Social Care)and healthcare providers. Due to the lack of nationallyrepresentative unit cost estimates for private healthcare,this care will be costed as the NHS equivalent in the basecase. Patient reported costs for over-the-counter treat-ments will be used. Productivity costs will be calculatedusing data collected on employment status at every time-point and days off work due to their musculoskeletalproblem. For those in paid employment, information onoccupation and the nature of their employment (full timeor part time) will be requested. The average wage for eachrespondent will be identified using UK Standard Occupa-tional Classification coding and annual earnings data foreach job type. The analysis will use the human capital ap-proach, and the self-reported days of absence will bemultiplied by the respondent-specific wage rate. The hu-man capital approach assumes that the value of lost workis equal to the amount of resources an individual wouldhave been paid to do that work and values productivitylosses as a result of morbidity (or mortality) by measuringtime lost from work and multiplying this with the grosswage of the person. Responses to the EQ-5D question-naire at baseline and 6 and 12 months will be used to cal-culate QALYs for each participant using the area underthe curve method.As this is a pilot trial this will be an exploratory ana-
lysis, with the aim to inform the cost data collection and
analysis of a future main larger trial. We will test ourmethods of collecting cost data, from patient question-naires and medical record reviews and assess the com-pleteness of the data collected. A cost-consequenceanalysis will be reported, describing all the important re-sults relating to costs and consequences. Analyses willbe mainly descriptive, and all costs and outcomes will besummarised using means and 95 % confidence intervals.The data for costs are likely to have a skewed distribu-tion; therefore, the plan is to explore the nature of thedistribution of costs. If the data is not normally distrib-uted, a non-parametric comparison of means (e.g. boot-strapping) will be undertaken.The base case cost analysis will adopt a NHS and per-
sonal social services (PSS) perspective. A broader costingperspective will be considered in a sensitivity analysis, tak-ing into account NHS/PSS costs, patients’ personal ex-penditure and costs associated with work loss. Therobustness of the results will be explored using sensitivityanalysis and will explore uncertainties in the trial baseddata and any assumptions made in the base case analysis.
Nested willingness to pay analysis Exploratory workusing a willingness to pay (WTP) approach that fitswithin a cost-benefit analysis framework will also beconducted in this pilot trial. Cost-benefit analysis isideally placed for the evaluation of interventions wherethe benefits may be non-health related. The approach isone way of measuring how valuable a service is and howmuch (in monetary terms) participants would be willingto give up in order to receive it. The hypothetical natureof the question is highlighted in the information given toparticipants. The WTP study questionnaire will be sentto all participants at 12 months. The main WTP ques-tion contains presenting the participant with a range ofmonetary values in a table from £0 to £350 and asks par-ticipants what is the maximum amount of money theywould be willing to pay to have direct access to a physio-therapy service. A space is provided for them to explainthe reasons for their answer, and there are further ques-tions asking if they would use a direct access service ifavailable and their annual household income.Firstly, the pilot study will test the completion rate of
the WTP questions and whether WTP can be measuredin this context. This does not aim to obtain definitiveWTP findings but to explore the feasibility of themethod for use in a future main trial. Descriptive statis-tics for willingness to pay values will be presented inboth trial arms, including the proportion of protest zeroresponses. ‘Protest zeros’ occur when participants reporta zero WTP even though they value the service (in con-trast to reporting a zero WTP if they do not value theservice) and are usually due to refusal to engage with theWTP questions. All reasons for responses will be coded.
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 11 of 15
Page 35 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
A preliminary linear regression analysis will be undertakento explore the relationship between stated WTP and par-ticipant characteristics, using WTP values as the dependentvariable and variables such as trial arm, age, gender, healthstatus and income as independent variables.
Trial organisation and monitoringThe STEMS pilot trial is sponsored by Keele University.The day-to-day operation of the trial will be overseen by aTrial Management Group (led by AB), in line with theStandard Operating Procedures of the Keele ClinicalTrials Unit. The Trial Management Group will meetmonthly and AB will meet more frequently with the studycoordinator. The trial will be monitored by an independ-ent Trial Steering Committee (TSC) chaired by ProfessorTracey Howe, who will meet approximately twice a yeartimed to coincide with key milestones, such as approval ofthe protocol, approval of the statistical analysis plan andinterpretation of results. The TSC is made up of individ-uals with expertise in musculoskeletal research, delivery ofcare in general practice and lay members with musculo-skeletal pain. An independent Data Monitoring Commit-tee (DMC) monitors all trials conducted at the ResearchInstitute for Primary Care and Health Sciences. Havingreviewed the protocol and in view of the feasibility andpilot nature of the STEMS pilot trial, the DMC (chairedby Dr Janine Gray) proposed that monitoring of this studyremains the responsibility of the TSC. During the pilottrial period no interim analyses are planned.
DisseminationResults from the STEMS pilot study will be disseminatedthrough oral and poster presentations at conferencesalong with publications in peer review journals andother media. A report to the funder is a requirement offunding and will be submitted at the end of the study.Results will also be disseminated to participating generalpractices and the physiotherapy service through face-to-face meetings and/or electronic methods, depending onpreference. Results will be made available on the Re-search Institute’s website and dissemination to partici-pants will be coordinated in liaison with the Patient andPublic Involvement coordinator. Keele University CTUhas established data sharing arrangements to supportjoint publications and other research collaborations.
Data confidentiality and archivingThe transportation of electronic sensitive data originatingfrom NHS sources, such as contact details or medical re-cords, will be conducted in accordance with the guidelinesprovided by NHS National Information GovernanceBoard (NIGB). Data collected as part of the medical rec-ord review of consenting participants will be recorded onNHS compatible encrypted laptop computers and then
transferred to university computers. Any transfer of per-sonal information between CRN staff and GP practice orphysiotherapy service administrators will be transferredusing NHS email accounts. Paper records kept for re-search purposes will include hard copies of the completedquestionnaires with signed consent forms and case reportforms (CRFs). Consent forms will contain names and ad-dress but will be stored in a secure environment separatefrom patient data. The contact details of consenting par-ticipants will be required for mailing the follow-up ques-tionnaires for this study. These contact details will bestored on a separate database to their questionnaire re-sponses and clinical data, linked by their unique ID num-ber. All trial-related information will be stored securely atthe Research Institute for Primary Care and Health Sci-ences at Keele University. Coded identification numberswill be used to anonymise data with the data and the link-ing code stored in separate locations, under password pro-tection. Access to the data will be to the small number ofindividuals necessary for quality control, audit and ana-lysis. The final trial dataset will be accessed by the statisti-cian (RO), the trial principal investigator (AB) and chiefinvestigator (NEF). We will publish and communicate thepilot trial results regardless of the outcome of the trial.Data from the STEMS pilot trial will be archived andmade available for future, secondary analysis and datapooling purposes from the Research Institute for PrimaryCare and Health Sciences at Keele University.
Ethical review and trial registrationThe STEMS pilot trial received research ethical approvalfrom NRES Committee North West—Preston in February2013 (REC reference, 13/NW/0053), and site-specific ap-provals have been received from the appropriate local re-search and development offices. The trial is beingconducted in accordance with the ethical principles in theDeclaration of Helsinki and good practice guidelines onthe proper conduct of research. The STEMS pilot trial isregistered at Current Controlled Trials ISRCTN23378642.
Results and discussionThe STEMS pilot trial will investigate the feasibility ofa future large trial to compare the clinical and cost-effectiveness of the additional offer of direct access tophysiotherapy versus continuing with usual GP-led pri-mary care alone for adults with common musculoskel-etal problems. It is essential that changes to serviceprovision and delivery are supported by research evi-dence and arguable that research about how to improvethe delivery of health care is just as important in im-proving the health of patients with musculoskeletalconditions as the testing of new drugs or therapeuticapproaches.
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 12 of 15
Page 36 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Previous research into direct access to physiotherapyhas been limited to observational studies with the inherentlimitations of observational designs. No previous trialshave been conducted into direct access to physiotherapyfor patients with musculoskeletal problems and this pilottrial will inform a main trial to fill this evidence gap andmeet the calls to provide robust trial evidence of the im-pact on clinical outcomes, work loss and costs in a trialcomparing areas that do and do not offer direct access[26] and to provide clinicians and service commissionerswith the high quality trial data they need to guide deci-sions on the best models of care [25]. Direct access will bedeemed to be the preferred model if it is not inferior interms of patients’ physical health (on the SF-36v2PCS—the main trial primary outcome) and is associ-ated with benefits such as shorter waiting times, greatersatisfaction, improved work outcomes and greater cost-effectiveness. Direct access may prove to be more cost-effective if it reduces other health service consultationsand prescriptions, or improves quality of life or lesscost-effective if it involves additional physiotherapyconsultations with no reduction in GP consultations orprescriptions or improvements in quality of lifeThe strengths of the STEMS pilot trial are its size, the
length of follow-up and collection of process, clinical andcost outcomes to fully inform a future main trial. Inaddition, marketing of the direct access service at GPpractice level will avoid contamination between arms butwill ensure that all registered adult patients are aware ofthe direct access service. This will enable sufficient partici-pants to directly access physiotherapy care during thepilot trial to allow planned analyses. The care pathway tophysiotherapy in the intervention practices will be set upto mimic closely what would happen if direct access wereroutinely available. Although patients in the interventionarm may choose to access physiotherapy directly withoutever contacting their general practice about their muscu-loskeletal condition (true self-referrers), some patients willcontact their practice and may be advised that they canself-refer to physiotherapy (recommended self-referrers).The facility for GPs to send a written referral in the trad-itional manner also continues as this may be particularlysuitable for some patients e.g. the frail elderly or thosewith very complex problems.
Design considerations and limitationsWe acknowledge that a limitation of the trial design isrecruiting patients in the control arm from GP practicesand in the intervention arm from GP practices and thephysiotherapy service. In an ideal design, we would com-pare all patients who have a musculoskeletal problemregistered with participating practices during the studyperiod, whether or not they attend their GP and/orphysiotherapy service but clearly this is not possible.
Other trial designs were considered, but these wouldhave led to greater differences in patients recruited tothe two arms of the trial. We will therefore make consid-erable efforts to identify any evidence of selection andrecruitment bias between the arms of the pilot trial, al-though we acknowledge that patients may differ onother unknown factors.It is possible that over time, as patients become accus-
tomed to direct access, their expectations and serviceuse may change. Clinical outcomes are unlikely tochange beyond 12-month follow-ups, but costs and ben-efits may change as direct access becomes establishedwithin a community. Therefore, this pilot trial includesfollow-up to 12 months as longer follow-up would beexpensive within the context of a trial.This pilot aims to inform a main trial with a non-
inferiority design as the addition of a direct access tophysiotherapy pathway is not anticipated to be superior interms of patients’ clinical outcomes. However, a range ofsecondary outcomes is included that in a main trial willprovide important information for patients, health carepractitioners and commissioners if clinical non-inferiorityis demonstrated. Previous work suggests an effect size of0.2 to 0.6 as a minimum clinically important difference,and we would thus, anticipate specifying a difference be-tween groups of 0.2 as the threshold for the purposes ofdemonstrating non-inferiority in a main trial.
ConclusionsThis pilot cluster randomised control trial will providevaluable information to inform a future future large trialto compare the clinical and cost-effectiveness of the add-itional offer of direct access to physiotherapy versus con-tinuing with usual GP-led primary care alone for adultswith common musculoskeletal problems
Endnotes1Read codes are the standard diagnostic codes used in
general practice in the UK
Additional file
Additional file 1: STEMS Participant Information Leaflet.
AbbreviationsCI: confidence Interval; CiPCA: Consultation in primary care archive;CRN: Clinical Research Network; CSP: Chartered Society of Physiotherapy;DMC: Data Monitoring Committee; DNA: did not attend; DoH: Department ofHealth; GP: general practitioner; ICC: inter-cluster correlation; ITT: intention totreat; NHS: National Health Service; NRES: National Research Ethics Service;PCS: Physical Component Summary; PSS: personal social services;QALY: quality-adjusted life year; QIPP: quality and productivity case studies;RCT: randomized controlled trial; SAE: serious adverse event; SF36v2: shortform 36 version 2; STEMS: Stepping up the evidence for musculoskeletalservices; TSC: Trial Steering Committee; UK: United Kingdom; US: UnitedStates; WTP: willingness to pay.
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 13 of 15
Page 37 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
For peer review only
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsNEF, AB, EMH, CS, and SJ conceived of the trial, developed the trial designand secured funding. AB, JP, RO, SJ and NEF wrote the detailed protocol. ABis the trial principal investigator, leads the trial management group andproduced the first draft of this manuscript. ST is the trial coordinator andcontributed to the operational aspects of the trial in the protocol. CSprovided expertise in delivery of primary care services and trial design. EMHprovided expertise in trial methodology. RO provided statistical expertise anddeveloped the detailed statistical analysis plan for the STEMS pilot trial. SJadvised on the cost data collection and led on the analysis plan for theeconomic evaluation. All authors contributed to revisions of this manuscript,have read and approved the final manuscript and take public responsibilityfor its content.
AcknowledgementsThe STEMS trial team also includes Dr Ruth Beardmore, Ian Thomas, JulieYoung, Debbie D’Cruz, Alice Mackie, William Cole, Sian Jones, MichelleRobinson and Victoria Harper. The authors would like to thank the healthinformatics, administrative staff, research nurse team and general practiceand physiotherapy research facilitators from the Research Institute forPrimary Care and Health Sciences.
FundingThe STEMS pilot trial is funded by the Chartered Society of PhysiotherapyCharitable Trust (SRP (11)2). NR and AB are funded through an NIHRResearch Professorship for NE Foster (NIHR-RP-011-015). The views andopinions expressed are those of the authors and do not necessarily reflectthose of the NHS, the NIHR or the Department of Health. The North StaffsPrimary Care Research Consortium provided additional funding for GP andPhysiotherapy Research Facilitators to advise on the engagement andrecruitment of the GP practices and physiotherapists in the STEMS pilot trial.
Author details1Research Institute for Primary Care & Health Sciences, Keele University,Keele, Staffordshire ST5 5BG, UK. 2Centre for Academic Primary Care,University of Bristol, Bristol, UK. 3Health Economics Unit, University ofBirmingham, Birmingham, UK.
Received: 24 February 2015 Accepted: 18 June 2015
References1. Savigny P, Watson P, Underwood M. Early management of persistent
non-specific low back pain: summary of NICE guidance. BMJ. 2009;338:b1805.2. Picavet HS, Schouten JS. Musculoskeletal pain in the Netherlands: prevalences,
consequences and risk groups, the DMC3-study. Pain. 2003;102(1-2):167–78.3. Hart LG, Deyo RA, Cherkin DC. Physician office visits for low back pain.
Frequency, clinical evaluation, and treatment patterns from a U.S. nationalsurvey. Spine. 1995;20:11–9.
4. Jordan KP, Kadam UT, Hayward R, Young C, Croft P. Annual consultationprevalence of regional musculoskeletal problems in primary care: anobservational study. BMC Musculoskelet Disord. 2010;11:144.
5. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al.Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21regions, 1990–2010: a systematic analysis for the global burden of diseasestudy 2010. Lancet. 2012;380:2197–223.
6. Chou R, Qaseem A, Snow V, Casey D, Cross Jr JT, Shekelle P, et al. Diagnosisand treatment of low back pain: a joint clinical practice guideline from theAmerican College of Physicians and the American Pain Society. Ann InternMed. 2007;147(7):478–91.
7. National Collaborating Centre for Chronic Conditions. Osteoarthritis:national clinical guideline for care and management in adults. London:Royal College of Physicians; 2008.
8. Lin CW, Haas M, Maher CG, Machado LA, van Tulder MW. Cost-effectivenessof general practice care for low back pain: a systematic review. Eur Spine J.2011;20(7):1012–23.
9. Zigenfus GC, Yin J, Giang GM, Fogarty WT. Effectiveness of early physicaltherapy in the treatment of acute low back musculoskeletal disorders. JOccup Environ Med. 2000;42:35–9.
10. Wand BM, Bird C, McAuley JH, Doré CJ, Mac Dowell M, De Souza LH. Earlyintervention for the management of acute low back pain: a single-blindrandomized controlled trial of biopsychosocial education, manual therapyand exercise. Spine. 2004;29:2350–6.
11. Nordeman L, Nilsson B, Moller M, Gunnarsson R. Early access to physicaltherapy treatment for subacute low back pain in primary health care: aprospective randomized clinical trial. Clin J Pain. 2006;22:505–11.
12. Addley K, Burke C, McQuillan P. Impact of a direct access occupationalphysiotherapy treatment service. Occup Med (Lond). 2010;60(8):651–3.
13. Department of Health. Self-referral pilots to musculoskeletal physiotherapyand the implications of improving access to other AHP services. Leeds:Department of Health; 2008. http://webarchive.nationalarchives.gov.uk/20130107105354/http:/www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_116358.pdf.
14. Leemrijse CJ, Swinkels ICS, Veenhof C. Direct access to physical therapy inthe Netherlands: results from the first year in community-based physicaltherapy. Physical Therapy. 2008;88(8):936–46.
15. Galley P. Physiotherapists as first contact practitioners: new challenges andresponsibilities in Australia. Physiotherapy. 1977;63:246–8.
16. Massey BF. American Physical Therapy Association presidential address:what’s all the fuss about direct access? Phys Ther. 2002;82:1120–3.
17. Holdsworth LK, Webster VS. Direct access to physiotherapy in primary care:now and into the future? Physiotherapy. 2004;90:64–72.
18. Chartered Society of Physiotherapy Frontline magazine. Northern Irelandcancels self-referral. http://www.csp.org.uk/news/2014/12/17/northern-ireland-cancels-self-referral-physiotherapy. Accessed 01 February 2015
19. Chartered Society of Physiotherapy. Briefing paper: Self-referral tophysiotherapy services. CSP, London, UK. 2004
20. Holdsworth LK, Webster VS, McFadyen AK. What are the costs to NHSScotland of self-referral to physiotherapy? Results of a national trial.Physiotherapy. 2007;93(1):3–11.
21. Holdsworth LK, Webster VS, McFadyen AK. Are patients who referthemselves to physiotherapy different than those referred by GPs? Resultsof a national trial. Physiotherapy. 2006;92:26–33.
22. Snow BL, Shamus E, Hill C. Physical therapy as primary health care: publicperceptions. J Allied Health. 2001;30:35–8.
23. QIPP Quality and Productivity Case Studies. Musculoskeletal Physiotherapy:patient self-referral 2012 citing Holdsworth et al 2007, costs updated inaccordance with Department of Health 2011 http://www.nice.org.uk/savingsAndProductivityAndLocalPracticeResource?ci=http%3a%2f%2farms.evidence.nhs.uk%2fresources%2fQIPP%2f29492%3fniceorg%3dtrue.Accessed 10th January 2015
24. Bury TJ, Stokes EK. A global view of direct access and patient self-referral tophysical therapy: implications for the profession. Phys Ther. 2013;93:449–59.
25. Bury TJ, Stokes EK. Direct access and patient/client self-referral tophysiotherapy: a review of contemporary practice within the EuropeanUnion. Physiotherapy. 2013 Mar 25. doi:pii: S0031-9406(13)00023-0. 10.1016/j.physio.2012.12.011.
26. Salisbury C. http://ukpolicymatters.thelancet.com/self-referral-to-physiotherapy/ 201127. Eldridge S, Kerry S, Torgerson DJ. Bias in identifying and recruiting
participants in cluster randomised trials: what can be done? BMJ.2009;339:b4006. doi:10.1136/bmj.b4006.
28. Campbell MK, Piaggio G, Elbourne DR, Altman DG, CONSORT Group.CONSORT 2010 statement: extension to cluster randomised trials. BMJ.2012;345:e5661.
29. Piaggio G, Elbourne DR, Pocock SJ, Evans SJW, Altman DG, for the CONSORTGroup. Reporting of noninferiority and equivalence randomized trials.Extension of the CONSORT 2010 statement. JAMA. 2012;308(24):2594–604.
30. Francis D, Roberts I, Elbourne DR, Shakur H, Knight RC, Garcia J, et al. Marketingand clinical trials: a case study. Trials. 2007;8:37. doi:10.1186/1745-6215-8-37.
31. Nicholas MK. The pain self-efficacy questionnaire: taking pain into account.Eur J Pain. 2007;11:153–63.
32. Mead N, Bower P, Roland M. The general practice assessment questionnaire(GPAQ): development and psychometric characteristics. BMC Fam Pract.2008;9:13. doi:10.1186/1471-2296-9-13.
33. Ware JE, Kosinski M, Bjorner JB, Turner-Bowker DM, Gandek B. MaruishMEUser’s manual for the SF-36v2 Health Survey. 2nd ed. Lincoln, RI:QualityMetric Inc; 2007.
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 14 of 15
Page 38 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
For peer review only
34. Angst F, Aeschlimann A, Stucki G. Smallest detectable and minimal clinicallyimportant differences of rehabilitation intervention with their implicationsfor required sample sizes using WOMAC and SF-36 quality of lifemeasurement instruments in patients with osteoarthritis of the lowerextremities. Arthritis Care Res. 2001;45(4):384–91.
35. Kosinski M, Zhao SZ, Dedhiya S, Osterhaus JT, Ware JE Jr. Determining minimallyimportant changes in generic and disease-specific health-related quality of lifequestionnaires in clinical trials of rheumatoid arthritis. Arthritis Rheum.2000;43(7):1478–87.
36. Norman GR, Sloan JA, Wyrwich KW. Interpretation of changes in health-relatedquality of life: the remarkable universality of half a standard deviation. MedCare. 2003;41(5):582–92.
37. McIntosh E, Clarke PM, Frew EJ, Louviere JJ, editors. Applied methods ofcost-benefit analysis in health care. Oxford: Oxford University Press; 2010.
Bishop et al. Pilot and Feasibility Studies (2015) 1:26 Page 15 of 15
Page 39 of 39
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
The STEMS pilot trial: A pilot cluster randomised controlled trial to investigate the addition of patient direct access to
physiotherapy to usual GP-led primary care for adults with musculoskeletal pain
Journal: BMJ Open
Manuscript ID bmjopen-2016-012987.R1
Article Type: Research
Date Submitted by the Author: 04-Jan-2017
Complete List of Authors: Bishop, Annette; Keele University, Institute for Primary Care and Health Sciences Ogollah, Reuben; Keele University, Primary Care & Health Sciences Jowett, Sue; University of Birmingham, Health Economics Unit Kigozi, Jesse; University of Birmingham Tooth, Stephanie; Keele University, Primary Care & Health Sciences Protheroe, Joanne; Institute of Primary Care and Health Sciences,, Keele University, UK, Arthritis Research UK Primary Care Centre Hay, Elaine; Arthritis Research Primary Care Centre Salisbury, Chris; University of Bristol, Centre for Academic Primary Care
Foster, Nadine; Keele University, Arthritis Research UK Primary Care Centre
<b>Primary Subject Heading</b>:
Health services research
Secondary Subject Heading: General practice / Family practice, Health services research
Keywords: Patient direct access, musculoskeletal, physiotherapy, feasibility and pilot trial, PRIMARY CARE
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 11 July 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2016-012987 on 12 M
arch 2017. Dow
nloaded from

For peer review only
1
The STEMS pilot trial: A pilot cluster randomised controlled trial to investigate the addition of
patient direct access to physiotherapy to usual GP-led primary care for adults with musculoskeletal
pain
Annette Bishop - Research Institute for Primary Care & Health Sciences, Keele University, UK
Reuben O Ogollah - Research Institute for Primary Care & Health Sciences, Keele University, UK
Sue Jowett - Health Economics Unit, University of Birmingham, UK
Jesse Kigozi - Health Economics Unit, University of Birmingham, UK
Stephanie Tooth - Research Institute for Primary Care & Health Sciences, Keele University, UK
Joanne Protheroe - Research Institute for Primary Care & Health Sciences, Keele University, UK [email protected]
Elaine M Hay - Research Institute for Primary Care & Health Sciences, Keele University, UK
Chris Salisbury - Centre for Academic Primary Care, University of Bristol, UK
Nadine E Foster - Research Institute for Primary Care & Health Sciences, Keele University, UK [email protected]
and the STEMS study team
Corresponding author
Annette Bishop Research Institute for Primary Care & Health Sciences
Keele University
Keele
Staffordshire
UK
ST5 5BG
Telephone: 01782 734838
Fax: 01782 734719 Email: [email protected]
Trial registration: Current Controlled Trials ISRCTN23378642
Key words: Patient direct access, self-referral, physiotherapy, musculoskeletal, feasibility, pilot trial
Word count, excluding title page, abstract, references, figures and tables: 4333
Number of tables: 5 plus 3 others suggested for online only supplementary material
Page 1 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
2
Abstract
Introduction: Around 17% of GP consultations are for musculoskeletal conditions, which will rise as the
population ages. Patient direct access to physiotherapy provides one solution, yet adoption in the NHS has
been slow.
Setting: A pilot, pragmatic, non-inferiority, cluster randomised controlled trial (RCT) in general practice and
physiotherapy services in the UK.
Objectives: Investigate feasibility of a main RCT.
Participants: Adult patients registered in participating practices and consulting with a musculoskeletal
problem.
Interventions: 4 general practices (clusters) randomised to provide GP-led care as usual or the addition of a
patient direct access to physiotherapy pathway.
Outcomes: Process outcomes and exploratory analyses of clinical and cost outcomes.
Data collection: Participant level data were collected via questionnaires at identification, 2, 6 and 12 months
and through medical records.
Blinding: The study statistician and research nurses were blinded to practice allocation.
Results: Of 2,696 patients invited to complete study questionnaires, 978 participated (intervention group
n=425, control arm n=553) and were analysed. Participant recruitment was completed in 6 months. Follow-
up rates were 78% (6 months) and 71% (12 months). No evidence of selection bias was observed. The direct
access pathway was used by 90% of patients in intervention practices needing physiotherapy. Some increase
in referrals to physiotherapy occurred from one practice, although waiting times for physiotherapy did not
increase (28 days before, 26 days after introduction of direct access) . No safety issues were identified.
Clinical and cost outcomes were similar in both groups. Exploratory estimates of between group effect
(using SF-36 PCS) at 6 months was -0.28 (95% CIs -1.35, 0.79) and at 12 months 0.12 (95% CIs -1.27,
1.51).
Conclusion: A full RCT is feasible and will provide trial evidence about the clinical and cost-effectiveness
of patient direct access to physiotherapy.
Trial registration: Current Controlled Trials ISRCTN23378642
Funding: Chartered Society of Physiotherapy Charitable Trust
Key words: Patient direct access, primary care, physiotherapy, musculoskeletal, feasibility and pilot trial
Strengths and limitations of this study
• This was a pilot randomised controlled trial (RCT) of patient direct access to physiotherapy in four
general practices and one physiotherapy service in one English town
• It provides evidence for the feasibility and safety of patient direct access to physiotherapy services
• Observed recruitment and follow-up rates can inform a future full RCT
Page 2 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
3
• As a pilot RCT, analyses of clinical and cost outcomes are exploratory
Background
In the UK, primary care is struggling to meet the current record demand from patients. General Practitioners
(GPs) now do an estimated 370 million consultations each year, 60 million more than five years ago,1 which
equates to a 16% increase in workload since 2007.2 Musculoskeletal problems account for around 17% of
GP consultations3 and given the ageing population, the demand for musculoskeletal healthcare is set to rise
further.4
Patient direct access to UK National Health Service (NHS) physiotherapy is one potential solution, allowing
patients to refer themselves to physiotherapy services rather than referral being initiated by the GP. Despite
reported benefits from observational research such as reduction in GP workload particularly for repeat
consultations,5 improved access for patients,
6,7 and reductions in costs,
8,9 progress towards widespread
provision of patient direct access to NHS physiotherapy has been slow.
In the UK health care under the NHS is free at point of delivery, meaning that patients do not pay fees to see
NHS GPs, NHS physiotherapists or to access specialist NHS hospital services. However, patients can access
private health care providers but these costs must be met in full by the patient or by employer provided or
personally bought private medical insurance. Around 11% of the UK population has some private medical
insurance but many of these policies exclude many health conditions.10 The NHS is therefore the
predominant healthcare provider in the UK. Legislation has allowed patients to access physiotherapists
directly since 1977 but in the NHS services are commissioned by clinical commissioning groups, allocated
funds from the Department of Health, and patient direct access to physiotherapy is only available in some
areas of the UK. The physiotherapists involved in this pilot trial did not have advanced practice roles and so
were not able to order and interpret investigations or make referrals to hospital specialist services.
A specific recommendation in the recent Primary Care Workforce Commission is to investigate whether
direct access to physiotherapy for some conditions makes cost-effective use of NHS resources.11
The aim of the STEMS pilot trial was to assess the feasibility of a future large trial to compare the clinical
and cost-effectiveness of the addition of patient direct access to physiotherapy versus continuing with usual
GP-led care alone for adults with common musculoskeletal problems. The specific objectives of this pilot
trial comprised process objectives to assess the feasibility of a future large cluster randomised trial, and
research objectives that focused on exploratory analysis of clinical outcomes and costs.
Process objectives
i. To assess the engagement of GP practices and physiotherapy services to participate and stay in
the trial through follow-up
ii. To assess the feasibility of establishing a patient direct access to physiotherapy pathway
iii. To develop, and test approaches to marketing the direct access pathway to ensure a sufficient
proportion of patients use the pathway
iv. To estimate recruitment rates in both control and intervention practices
v. To explore any evidence of selection bias in the control and intervention practices
vi. To estimate follow-up rates at each follow-up time-point
Page 3 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
4
Research objectives
i. To explore changes in the proposed main trial primary outcome measure (physical health
measured using the SF36v2 Physical Component Summary)
ii. To explore changes in other outcome measures (overall perceived change, SF36v2 Mental
Component Summary, pain self-efficacy, quality of life, understanding of the condition,
experience of care, and convenience and accessibility of services)
iii. To provide an exploratory estimate of costs, both healthcare and societal costs
iv. To estimate the parameters needed for a realistic sample size calculation for a future large cluster
RCT.
v. To explore the use of Willingness to Pay (WTP) methodology to capture the strength of patient
preferences for self-referral to NHS physiotherapy. This analysis will be reported in a separate
future paper.
Methods
Design and setting
STEMS was a pilot, pragmatic, two-arm parallel, non-inferiority, cluster RCT in 4 general practices in one
town in Cheshire UK, referring patients to a local NHS physiotherapy service, which did not offer patient
direct access to care prior to the set-up of the STEMS trial. The methods have been described in full in the
STEMS trial protocol,12 but are summarised below.
Randomisation
General practices were randomised using computer-generated random numbers stratified by the practice size
(small or large, based on the average number of patients registered per practice at the start of the pilot trial)
in the ratio 1:1 to continue to offer GP-led care alone as usual care (n=2) or GP-led care plus the addition of
a new pathway permitting patient direct access to an existing NHS physiotherapy service. Patients followed
the care to which their practice was randomised and were recruited through identical patient information
explaining that musculoskeletal services were being evaluated using patient self-reported clinical outcomes
and medical record review. Patient direct access to physiotherapy was not available to patients registered
with control practices. The study statistician was blinded to practice allocation.
Participants
Data were collected from individual participants who were eligible if they were 18 years or over and
presenting to their general practice or physiotherapy service with a musculoskeletal condition. Patients who
were undergoing palliative care, had severe learning disabilities, were housebound or in nursing home
accommodation or unable to communicate in English were not eligible to take part.
Potentially eligible participants were identified when they presented to the general practice or physiotherapy
service and were mailed a study pack including the first questionnaire. Follow-up data collection from
consenting participants was via participant self-completion postal questionnaires at 2, 6 and 12 months and
through review of general practice and physiotherapy records.
Page 4 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
5
Setting up the patient direct access to physiotherapy pathway
Physiotherapists attended a one-day training programme to prepare them for providing care to patients who
self-refer, including topics such as prevalence and identification of red flags, physical and MSK
manifestations of underlying medical pathology and review of common over-the-counter and prescribed
medications for musculoskeletal pain.13 Physiotherapists also attended regular mentoring meetings with a
senior physiotherapist in the participating physiotherapy service.
The patient direct access pathway began 8 weeks prior to the start of participant recruitment to the study in
order to allow familiarisation with receiving and managing patients using the direct access pathway. All
referrals (GPs or patient self-referral) were triaged using existing physiotherapy service criteria and were
classified as urgent, routine or inappropriate for physiotherapy. Whether self-referring or GP referred to
physiotherapy patients received equitable treatment such as the length of wait to first appointment once
logged on the physiotherapy administration system. As this trial investigated the addition of direct access to
physiotherapy, the physiotherapy care provided was determined by clinical need and assessment findings
and was therefore consistent with routine practice and did not differ for patients in the different arms of the
trial.
In order to ensure patients were aware of the new direct access pathway, all adult registered patients at the
two intervention practices (n=8222) were individually mailed an information letter about direct access.
Posters, flyers and self-referral forms were readily available in intervention practices. Even with the offer of
self-referral, we anticipated that some patients would continue to consult their GP or practice nurse,
therefore in the intervention practices, patients could access physiotherapy either by traditional written
referral, be recommended to self-refer (GP or nurse ‘recommended’ self-referral), or choose to self-refer to
physiotherapy without contacting their GP practice (‘true’ self-referrers).
Safety of the pathway was explored by the number of adverse events reported and by systematically
searching for diagnostic codes of a wide range of pathologies (including cancer, fractures, joint infections
and stroke) in the medical records of participants who used the direct access pathway.
Outcomes and analysis
As a pilot trial the emphasis was on process outcomes to establish the feasibility for a full trial. Outcomes
were collected from several sources. Anonymised process outcome data were collected from physiotherapy
service records and self-referral forms. Individual participants provided data on their characteristics, clinical
outcomes and costs through self-completed questionnaires following recruitment to the research and at 2, 6
and 12 months. Key outcome data were sought from non-responders through minimum data collection
(MDC). A list of outcomes is provided in Table 1. To ensure transparency in analyses, a statistical analysis
plan (SAP) was developed and approved by the Trial Steering Committee (TSC) prior to the final analysis.
Since this was a pilot trial, the aim of all analyses was to decide if a main trial is feasible and desirable, in
addition to finalising the sample size for a future main trial. Descriptive summaries report the number of
participants identified and recruited, along with the number of participants followed up at each time-point.
Withdrawals (and where possible, reasons for withdrawals) are reported. Anonymised data on key baseline
characteristics (age, gender and index of multiple deprivation) of those who were invited but did not
participate are compared with those who did participate.
Page 5 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
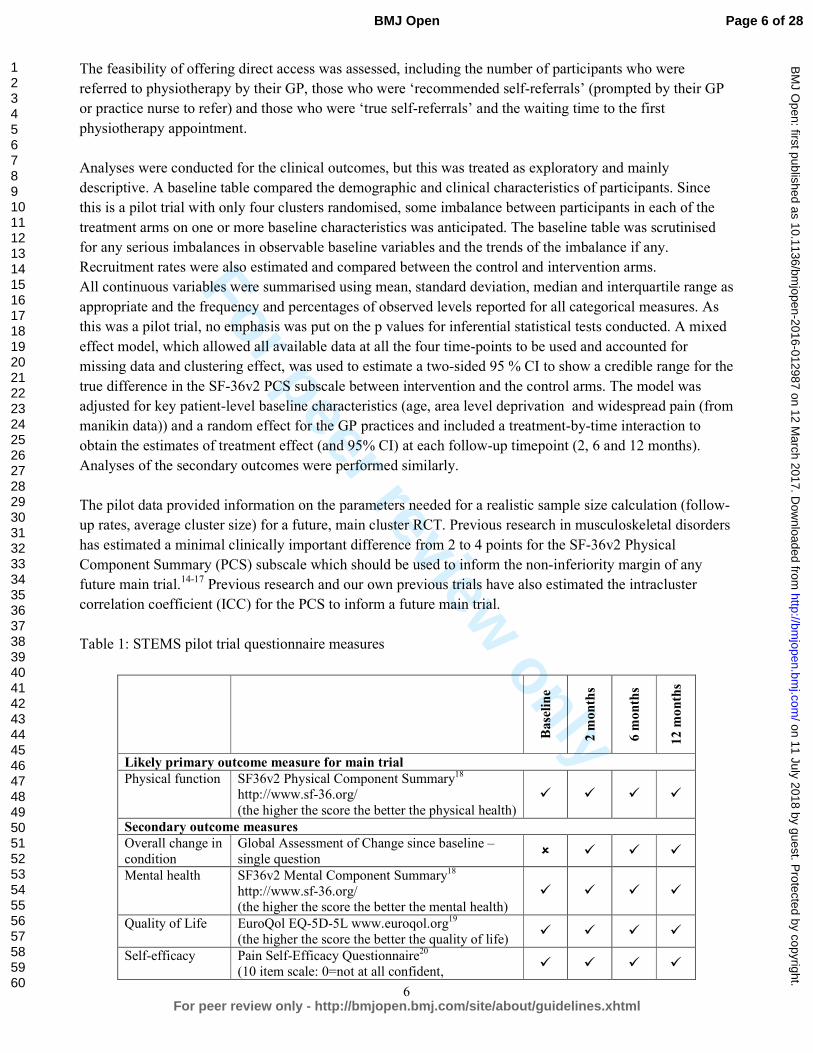
For peer review only
6
The feasibility of offering direct access was assessed, including the number of participants who were
referred to physiotherapy by their GP, those who were ‘recommended self-referrals’ (prompted by their GP
or practice nurse to refer) and those who were ‘true self-referrals’ and the waiting time to the first
physiotherapy appointment.
Analyses were conducted for the clinical outcomes, but this was treated as exploratory and mainly
descriptive. A baseline table compared the demographic and clinical characteristics of participants. Since
this is a pilot trial with only four clusters randomised, some imbalance between participants in each of the
treatment arms on one or more baseline characteristics was anticipated. The baseline table was scrutinised
for any serious imbalances in observable baseline variables and the trends of the imbalance if any.
Recruitment rates were also estimated and compared between the control and intervention arms.
All continuous variables were summarised using mean, standard deviation, median and interquartile range as
appropriate and the frequency and percentages of observed levels reported for all categorical measures. As
this was a pilot trial, no emphasis was put on the p values for inferential statistical tests conducted. A mixed
effect model, which allowed all available data at all the four time-points to be used and accounted for
missing data and clustering effect, was used to estimate a two-sided 95 % CI to show a credible range for the
true difference in the SF-36v2 PCS subscale between intervention and the control arms. The model was
adjusted for key patient-level baseline characteristics (age, area level deprivation and widespread pain (from
manikin data)) and a random effect for the GP practices and included a treatment-by-time interaction to
obtain the estimates of treatment effect (and 95% CI) at each follow-up timepoint (2, 6 and 12 months).
Analyses of the secondary outcomes were performed similarly.
The pilot data provided information on the parameters needed for a realistic sample size calculation (follow-
up rates, average cluster size) for a future, main cluster RCT. Previous research in musculoskeletal disorders
has estimated a minimal clinically important difference from 2 to 4 points for the SF-36v2 Physical
Component Summary (PCS) subscale which should be used to inform the non-inferiority margin of any
future main trial.14-17
Previous research and our own previous trials have also estimated the intracluster
correlation coefficient (ICC) for the PCS to inform a future main trial.
Table 1: STEMS pilot trial questionnaire measures
Baseline
2 months
6 months
12 months
Likely primary outcome measure for main trial Physical function SF36v2 Physical Component Summary
18
http://www.sf-36.org/
(the higher the score the better the physical health) � � � �
Secondary outcome measures Overall change in
condition
Global Assessment of Change since baseline –
single question � � � �
Mental health SF36v2 Mental Component Summary18
http://www.sf-36.org/ (the higher the score the better the mental health)
� � � �
Quality of Life EuroQol EQ-5D-5L www.euroqol.org19
(the higher the score the better the quality of life) � � � �
Self-efficacy Pain Self-Efficacy Questionnaire20
(10 item scale: 0=not at all confident, � � � �
Page 6 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
7
60=completely confident despite pain)
Understanding of
condition
General Practice Assessment Questionnaire
enablement subscale21
(very well, unsure, not very well) � � � �
Experience of
consultations
General Practice Assessment Questionnaire
communication21
(Based on 5 items represented as a percentage of
the maximum possible score 100)
� � � �
Convenience of
services
Single question
(0-10 Numerical Rating Scale: 0 = not at all
convenient, 10 = very convenient) � � � �
Satisfaction with
services
Single question
(0-10 Numerical Rating Scale: 0 = not satisfied,
10 = very satisfied) � � � �
Baseline measures
Demographics
Gender, date of birth, ethnicity, education, health
literacy, employment status, socio-economic
status (recent paid job title, housing) � � � �
Baseline risk of
persistent
problems
STarT Musc tool [draft tool developed at Keele
University to identify patients’ risk of persistent
pain and disability] � � � �
Pain location Body Manikin � � � � Pain duration Single question about duration of pain � � � � Comorbidities Single question � � � � Economic outcomes Further health care utilisation
Consultations, investigations, procedures, admissions, over-the-counter medications
� � � �
Work absence Single question (number of days) � � � � Presenteeism Single work performance question
(0-10 Numerical Rating Scale: 0 = not at all
affected, 10 = unable to do my job) � � � �
The economic analysis was exploratory, with the aim to inform the design of a full cost-utility analysis
alongside a future main trial. All patients were asked to complete the 5-level version of the EuroQoL-5D
(EQ-5D) questionnaire at baseline, 6 months and 12 months in order for the quality-adjusted life years
(QALYs) over the 12-month time period to be calculated for each participant. The QALYs combine
information on health-related quality of life and survival. A cost-consequence analysis is reported,
describing all the important results relating to costs and consequences. Analyses were mainly descriptive,
and total costs and outcomes were summarised using means and 95 % confidence intervals. The base case
cost analysis adopted a NHS and personal social services (PSS) perspective. A broader costing perspective
was considered in a sensitivity analysis, taking into account NHS/PSS costs and patients’ personal
expenditure costs. Costs associated with work loss were also reported as part of the cost-consequence
analysis.
Sample size
As this was a pilot trial formal sample size calculation was not carried out. The sample size was based on
the number of patients we anticipated could be recruited within six months and that was sufficiently large to
estimate the key feasibility parameters (e.g. recruitment and retention) to a sufficient degree of accuracy
(<10% in the rates). We aimed to recruit 960 participants at baseline, over a period of six months and
achieve at least 80% follow-up rate (n=768) at 6 months.
Page 7 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
8
Ethical approval and trial registration
The STEMS pilot trial received research ethical approval from NRES Committee North West— Preston in
February 2013 (REC reference, 13/NW/0053), The STEMS pilot trial is registered at Current Controlled
Trials ISRCTN23378642.
Results
A flowchart showing the flow of practices (units of randomisation) and flow of individual participants is
shown in Figure 1. As can be seen one of the control practices was considerable larger that the other
randomised practices resulting in more participants in the control arm in this pilot trial.
Insert figure 1 about here
Process results
Engagement of GP practices and the physiotherapy service
Of five GP practices approached, four participated with three full-time equivalent GPs at each of the two
intervention practices and five and two in the control practices. In the physiotherapy service of the
physiotherapists who undertook STEMS training programme four worked in the clinic local to the
participating general practices and delivered care to patients using the direct access pathway (NHS Agenda
for Change band 7 (n=1), band 6 (n=2), and band 5 (n=1)). Agenda for Change is the NHS Terms and
Conditions of Service and determines salary scales for NHS staff.
Feasibility of the patient direct access pathway
Of the participants in the STEMS pilot trial (n=978), a total of 256 (26.2%) accessed physiotherapy care
during the study period, 152 (35.8%) in the intervention arm and 104 (18.8%) in the control arm. Of the 152
who accessed physiotherapy care in the intervention arm, 142 (93.4%) were self-referrals (comprising 98
(69%) ‘recommended’ and 44 (31%) ‘true’ self-referrals).
Comparisons to service level data (which may not be entirely comparable, due to the introduction of new
administration software in the physiotherapy service), from the same period one year prior to start of direct
access suggests one practice in the intervention arm had broadly similar rates of patients accessing
physiotherapy care, whereas the other had a substantial increase once the direct access pathway had been
introduced. The referral rates to physiotherapy prior to the trial showed considerable variation between the 4
participating practices. The practice in which referrals increased following the introduction of patient direct
access previously referred 32.6 referrals per annum per 1000 registered adults compared to the other
practices (59.3, 69.5 and 92.4 referrals per annum per 1000 registered adults. However, the median (IQR;
Range) overall waiting time in the physiotherapy service (applying to all patients in the service, as all
patients joined one waiting list), from logging of the referral to first appointment, was 28 (13-36; 0-73) days
prior to the introduction of direct access and 26 (17-42; 0-182) days during the direct access period of the
trial. Of the patients using the direct access pathway, triaging according to pre-existing service criteria
classified 23% (n=159) cases as urgent, 73% (n=507) as routine and 4% (n=25) as unsuitable for
physiotherapy.
Marketing of the direct access pathway was successful. We aimed to ensure a minimum of 20% of the
physiotherapy caseload during the pilot trial, from intervention arm practices, was through direct access.
Page 8 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
9
Using anonymised physiotherapy service data, of 765 patients registered at intervention practices and
accessing care for ten months following the introduction of the direct access pathway, 691 (90.3%) used the
pathway (comprising 515 (74.5%) ‘recommended’ and 176 (25.5%) ‘true’ self-referrals).
Safety of direct access
No adverse events were reported by GPs or physiotherapists during the pilot trial. Review of medical
records identified no evidence of missed serious pathology in patients who directly accessed physiotherapy.
Participant recruitment and retention
Of 2,696 participants invited to take part in the data collection, 978 (36%) participated (425 (44%) in the
intervention practices and 553 (57%) in the control practices). Recruitment was completed within six
months (June – December 2013). Response rates were as follows; 74.3% at 2 months (intervention 70.4%,
control 77.4%), 78.4% at 6 months (intervention 76.7%, control 79.8%) and 70.7% at 12 months
(intervention 69.4%, control 71.6%). Minimum data collection was included at 6 and 12 months only
resulting in higher response rates at these time-points.
Comparability of baseline characteristics
The baseline characteristics of participants (Table 2) were comparable in the two arms of the trial and there
was no evidence of selection bias.
Table 2: Comparability of baseline characteristics
Key characteristics n* Control
n=553
Intervention
n=425
Non-clinical characteristics
Age, mean (SD) 978 58.6 (14.6) 55.6 (15.2)
Gender: Female, n (%) 978 311 (56.2) 248 (58.4)
Ethnicity: White, n (%) 958 534 (99.3) 416 (99.1)
Employment: in paid work (part/full-time) †, n
(%)
966 244 (44.4) 190 (45.2)
Extent to which pain has affected
performance at work in the past 1 month (0-
10 NRS), mean (SD)
434 4.8 (3.2) 4.9 (3.1)
Time off work (past month) due to pain, n
(%)
407 74 (32.3) 54 (30.3)
Education: No qualifications, n (%) 849 133 (27.7) 104 (28.2)
Deprivation tertile (Index of Multiple
Deprivation), n (%)
978
Most deprived third 161 (29.1) 103 (24.2)
Middle third 184 (33.3 145 (34.1)
Least deprived third 208 (37.6) 177 (41.7)
Health literacy: Finds health information/leaflets
difficult to understand, n (%) 971 311 (56.7) 242 (57.4)
Clinical characteristics
Physical Health: SF-36 PCS, mean (SD) 952 35.7 (10.1) 36.6 (9.9)
Mental Health: SF-36 MCS, mean (SD) 952 44.4 (13.7) 42.7 (14.0)
Page 9 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
10
Bodily pain past week: severe/very severe, n (%) 976 245 (44.5) 190 (44.7)
Current episode duration: >6 weeks, n (%) 938 386 (73.0) 312 (76.3)
Widespread pain‡, n (%) 978 193 (34.9) 137 (32.2)
Comorbidities§: for >/= 2 other conditions, n (%) 978 333 (60.2) 241 (56.7)
Quality of life: EQ-5D-5L, mean (SD) 933 0.530 (0.27) 0.521 (0.28)
Pain self-efficacy (0-60), mean (SD) 895 33.4 (16.5) 32.5 (16.3) * 978 participants completed the baseline questionnaire but the number of respondents for each question slightly varies due to missing
data and non-applicable cases †Majority of those not in paid work (34%) were retired from paid work ‡Based on the American College of Rheumatology’s definition12 §The conditions include high blood pressure, heart problems, stroke, diabetes, depression or anxiety, osteoporosis, arthritis, asthma or
bronchitis, liver disease, cancer and others
SF-36 PCS= 36-Item Short Form physical component summary - the higher the score the greater physical health
SF-36 MCS=36-Item Short Form mental component summary – the higher the score the greater mental health
Pain self-efficacy scale: 10 item scale, score range=0-60 (0=not at all confident, 60=completely confident despite pain).
Baseline characteristics by physiotherapy access method
The baseline characteristics of musculoskeletal consulters and study participants who did and did not access
physiotherapy care in each trial arm are shown in online only Supplementary Table S1. This shows that the
characteristics of patients referred to physiotherapy by their GP or who accessed physiotherapy through self-
referral were similar. However, ‘true’ self-referrers were more likely to be female and less likely to be in
paid work. In addition, those in the most socioeconomically deprived group were less likely to use ‘true’
self-referral, although the numbers were very small.
Research objectives
Exploratory analysis of key clinical outcomes
The descriptive statistics (mean and SD or frequency and %) for outcomes at each data collection time-point are
displayed in Table 3.
Page 10 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
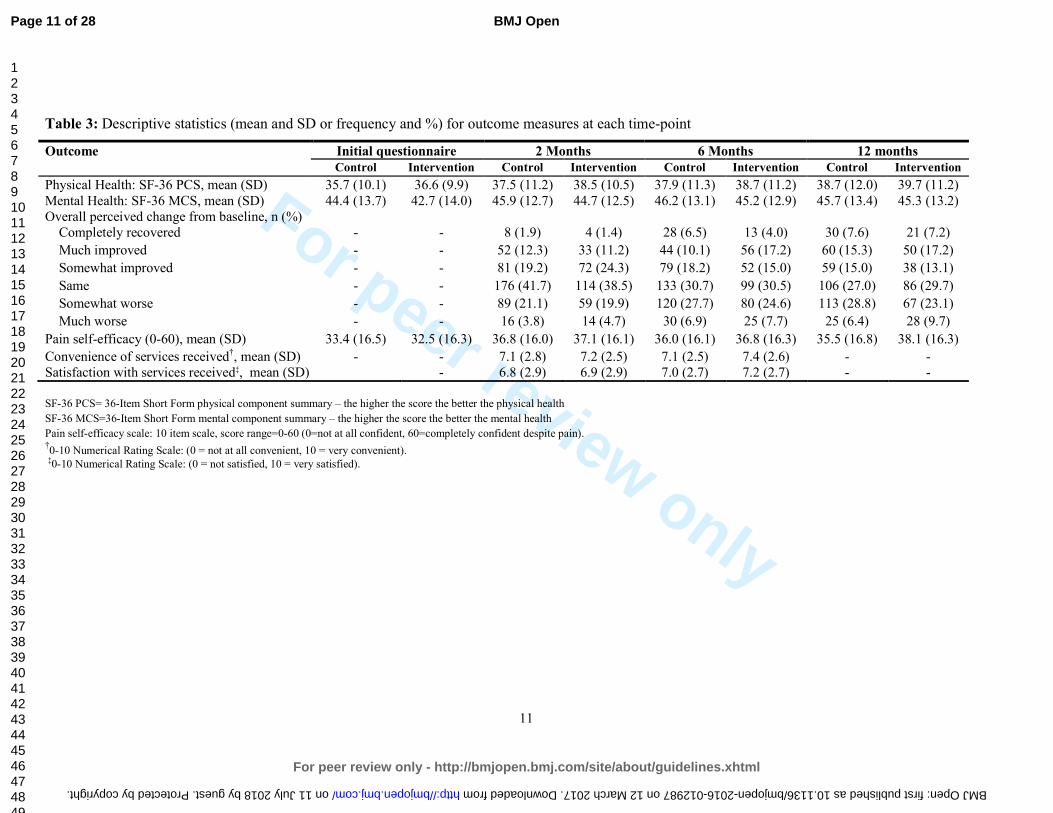
For peer review only
11
Table 3: Descriptive statistics (mean and SD or frequency and %) for outcome measures at each time-point
Outcome Initial questionnaire 2 Months 6 Months 12 months
Control Intervention Control Intervention Control Intervention Control Intervention
Physical Health: SF-36 PCS, mean (SD) 35.7 (10.1) 36.6 (9.9) 37.5 (11.2) 38.5 (10.5) 37.9 (11.3) 38.7 (11.2) 38.7 (12.0) 39.7 (11.2)
Mental Health: SF-36 MCS, mean (SD) 44.4 (13.7) 42.7 (14.0) 45.9 (12.7) 44.7 (12.5) 46.2 (13.1) 45.2 (12.9) 45.7 (13.4) 45.3 (13.2)
Overall perceived change from baseline, n (%)
Completely recovered - - 8 (1.9) 4 (1.4) 28 (6.5) 13 (4.0) 30 (7.6) 21 (7.2)
Much improved - - 52 (12.3) 33 (11.2) 44 (10.1) 56 (17.2) 60 (15.3) 50 (17.2)
Somewhat improved - - 81 (19.2) 72 (24.3) 79 (18.2) 52 (15.0) 59 (15.0) 38 (13.1)
Same - - 176 (41.7) 114 (38.5) 133 (30.7) 99 (30.5) 106 (27.0) 86 (29.7)
Somewhat worse - - 89 (21.1) 59 (19.9) 120 (27.7) 80 (24.6) 113 (28.8) 67 (23.1)
Much worse - - 16 (3.8) 14 (4.7) 30 (6.9) 25 (7.7) 25 (6.4) 28 (9.7)
Pain self-efficacy (0-60), mean (SD) 33.4 (16.5) 32.5 (16.3) 36.8 (16.0) 37.1 (16.1) 36.0 (16.1) 36.8 (16.3) 35.5 (16.8) 38.1 (16.3)
Convenience of services received†, mean (SD) - - 7.1 (2.8) 7.2 (2.5) 7.1 (2.5) 7.4 (2.6) - -
Satisfaction with services received‡, mean (SD) - 6.8 (2.9) 6.9 (2.9) 7.0 (2.7) 7.2 (2.7) - -
SF-36 PCS= 36-Item Short Form physical component summary – the higher the score the better the physical health
SF-36 MCS=36-Item Short Form mental component summary – the higher the score the better the mental health
Pain self-efficacy scale: 10 item scale, score range=0-60 (0=not at all confident, 60=completely confident despite pain). †0-10 Numerical Rating Scale: (0 = not at all convenient, 10 = very convenient).
‡0-10 Numerical Rating Scale: (0 = not satisfied, 10 = very satisfied).
Page 11 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2016-012987 on 12 March 2017. Downloaded from

For peer review only
12
Patients’ physical health measured using the SF-36 PCS is the anticipated primary clinical outcome for a
future main trial. Higher scores represent better physical health. In this exploratory analysis very similar
scores over time in participants in both arms of the trial were seen. The adjusted mean difference between
groups and 95% confidence interval showed estimates of effect at 2 months -0.14 (95% CI -1.02, 0.74), at 6
months -0.28 (-1.35, 0.79) and at 12 months 0.12 (-1.27, 1.51). The lower limit of the two-sided 95% CI for
intervention versus control mean difference was greater than -2, the smallest expected standard treatment
effect for the outcome (SF-36 PCS). Exploratory adjusted estimates of treatment effects for other outcomes
are provided in the online only Supplementary Table S2.
Health economics results
EQ-5D-5L responses were available at all time-points for 493 participants (281 (51%) control arm, 212
(50%) intervention arm). Self-reported resource use data were available at all time-points for 555
participants (237 (43%) control arm, 318 (57%) intervention arm). Details of musculoskeletal-related NHS
and healthcare resource use are reported in online only supplementary Table S3, with most resource use
involving consultations with GPs, physiotherapists and practice nurses. Over 12 months, on average, the
control arm was associated with slightly more GP visits, more investigations (including scans, x-rays and
MRIs) and visits to some consultants (rheumatologists and orthopaedic surgeons) and inpatient days
resulting from surgeries. The intervention arm was however associated with more physiotherapist visits.
Table 4 shows the disaggregated mean (SD) healthcare costs per patient for each treatment arm. The mean
NHS costs per patient were slightly cheaper in the intervention arm (£940 in intervention compared to £951
in the control arm), with considerable uncertainty in the estimates (95% CI of difference -363.27 to 340.83).
The proportion of participants that reported having taken time off work due to their musculoskeletal problem
was similar between the two arms of the trial over 12 months. The intervention arm was however associated
with fewer self-reported days off work and lower costs at 12 months follow-up. Productivity loss and costs
as a result of reduced productivity at work were higher in the intervention group. Mean quality of life scores
(EQ-5D-5L) scores (quality of life at baseline and follow-up and mean QALYs) are presented in Table 5.
Quality of life increased in both groups from the initial questionnaire over all follow-up time-points.
Unadjusted mean QALYs were slightly higher in the control arm however, QALYs were similar in both
groups arm once adjusted for clustering and baseline EQ-5D-5L score. Overall, the results show similar
outcomes and costs between the intervention and control arms of the trial.
Table 4: Costs per participant by trial arm over 12 months
Complete case analysis Control
(n=318)
£Mean (SD)
Intervention
(n=237)
£Mean (SD)
NHSa
GP 106.70 (134.57) 96.97 (134.58)
Practice nurse 7.87 (33.51) 8.35 (37.93)
Physiotherapist 61.99 (165.96) 74.67 (163.36)
Orthopaedic surgeon 48.43 (114.47) 36.58 (102.54)
Rheumatologist 20.91 (87.79) 11.22 (52.17)
Acupuncturist 5.67 (50.74) 1.67 (13.63)
Page 12 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
13
Chiropractor 4.28 (35.81) 1.48 (15.08)
Occupational therapist 7.89 (51.29) 5.01 (24.62)
Other healthcare professionals 33.88 (187.28) 21.67 (117.81)
Prescriptions 55.18 (118.24) 47.15 (110.41)
Surgery 422.97 (1759.25) 404.12 (1655.21)
Inpatient costs 21.57 (230.41) 75.11 (956.32)
Investigations 109.53 (329.93) 100.77 (263.43)
Injections 44.37 (164.06) 55.22 (274.33)
Privatea
Physiotherapist 9.46 (55.05) 22.68 (155.41)
Orthopaedic surgeon 4.49 (34.07) 3.01 (23.74)
Rheumatologist 0 1.12 (17.27)
Acupuncturist 3.04 (30.91) 5.76 (40.60)
Chiropractor 9.13 (85.47) 6.68 (48.31)
Occupational therapist 0 0.74 (11.43)
Other healthcare professionals 3.98 (38.49) 7.63 (97.90)
Over-the-counter medicines 20.20 (52.59) 15.06 (30.06)
Work-related outcomes
Musculoskeletal-related work absence
costs
740.30 (2084.75) 539.36 (2069.43)
Complete Case
Total NHS cost, £ 951.25 (2050.88) 940.02 (2157.24)
Mean difference (95% CI)b 11.22 (-363.27 to 340.82)
Total healthcare costs*, £ 1001.56 (2068.62) 1002.72 (2230.66)
Mean difference (95% CI)b -1.15 (-358.00 to 360.32)
*Includes costs to the NHS, private healthcare costs and over-the-counter treatment costs. In the UK, private healthcare costs are met in full by the patient.
a Resource use and costs were related to the respondent’s MSK condition b Difference = Intervention – control. Confidence intervals were generated using regression models for clustered data.
Table 5: EQ-5D-5L scores and QALYs at each time point
Complete case analysis Control
(n=281)
Mean (SD)
Intervention
(n=212)
Mean (SD)
Initial questionnaire 0.565 (0.246) 0.544 (0.262)
2 months 0.600 (0.227) 0.580 (0.246)
6 months 0.602 (0.251) 0.594 (0.262)
12 months 0.615 (0.254) 0.606 (0.258)
Total 12 month QALYs
(unadjusted)
0.602 (0.225) 0.589 (0.236)
Incremental QALYs (95%
CI)a
-0.012 (-0.053 to 0.028)
Total 12 month QALYs 0.575 0.578
Page 13 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
14
(adjusted for clustering and
baseline EQ-5D-5L)*
Incremental QALYs 0.003
EQ-5D-5L = EuroQol; QALYs = quality-adjusted life years; SD = Standard Deviation a Difference = Intervention – Control . Confidence intervals were generated using regression models for clustered data.
* QALYs have been adjusted for baseline differences and clustering
Discussion
No other RCTs of direct access to physiotherapy have been conducted. This pilot RCT explored the
feasibility of a future main cluster RCT and has provided an exploratory analysis of clinical and cost
outcomes.
The results show that a future main trial is feasible and general practices and physiotherapy services are
willing to take part. The patient recruitment target was achieved rapidly within the estimated six month
recruitment period. Follow-up rates were good although the follow-up at 12-months fell below our
anticipated 80%. In a future main trial we would include small patient payments to compensate participants
for their time in completing and returning questionnaires. Cluster trials have particular challenges including
the concern about selection bias.22,23
To minimise the risk of selection bias we avoided participating
clinicians being involved in the identification and recruitment of potential participants. The baseline
characteristics of the participants showed no evidence of selection bias, which shows that our methods of
identification and recruitment are suitable for use in a future main trial. We also compared the characteristics
(age gender and area level deprivation) of those who returned the questionnaires and consented to data
collection to those who did not return the questionnaires. These were comparable in terms of gender (57%
vs. 55%), but slightly different in terms of age (mean (SD) of 57 (15) vs. 49 (17) and deprivation 27% most
deprived 3rd vs. 38% for those who returned the questionnaires compared to those who did not. Participant
recruitment and retention through to long-term follow-up at 12 months was feasible and completed on time
and to target. The likely primary clinical outcome for a main trial is patients’ physical health assessed using
the SF-36 PCS.18 This performed well in the pilot trial and exploratory analyses of clinical outcomes showed
very similar changes in patient self-reported physical health measured in both arms of the trial. The
hypotheses for a main trial would be non-inferiority on clinical outcomes (i.e. the addition of a patient direct
access pathway to usual GP-led care would not lead to worse clinical outcomes for patients than usual GP-
led care alone) but superiority on other key outcomes (i.e. higher patient ratings of access to services,
convenience and satisfaction with services, and reduced costs). A future main cluster RCT with a primary
clinical outcome of physical health measured using the SF-36 PCS would require a sample size of
approximately 12 average-sized general practices and a minimum of 2880 individual participants. This is
based on a margin of non-inferiority of 2 points from previous research,14-17
a standard deviation of 10, a
power of 90% at a 2.5% one-sided significance level, in a design with three repeated measurements,24 and an
autocorrelation of 0.5. The sample size has also been inflated by 20% to allow for loss to follow-up, and a
further inflation for the design effect using an intracluster correlation coefficient (ICC) of 0.0075,25 and an
average cluster size of 240, allowing for a coefficient of variation in cluster size of 0.65.26
Exploratory health economic findings show that costs and outcomes were similar between the intervention
and control arms, although there is considerable imprecision in the estimates due to the sample size in this
pilot RCT. Data collection through patient questionnaires was successful and indicates that a full economic
evaluation of adding a patient direct access to physiotherapy pathway to usual GP-led primary care versus
usual GP-led primary care alone will be possible in a future main trial. Additional costs required to set-up
the service should also be considered in a future trial.
Page 14 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
15
This pilot trial suggests that adding a new patient direct access pathway to an existing physiotherapy service
is feasible. We observed an increase in the number of overall referrals to physiotherapy in the intervention
arm practices compared to service level data collected in the year prior to the STEMS pilot trial, mostly
from one practice, but this did not impact on the waiting time for physiotherapy care. The level of GP
referral to physiotherapy prior to the STEMS pilot trial was very low in this one practice compared to the
other practices. Pre-existing referral rates to physiotherapy have previously been highlighted as a possible
contributing factor to subsequent increases in demand following the introduction of patient direct access.27
An initial increase in referrals is perhaps not surprising bearing in mind the active marketing of the direct
access pathway that was undertaken. This type of marketing is unlikely to occur outside the context of a trial
but in a future main trial processes should be in place to support participating physiotherapy services
through availability of suitably trained staff and resources for increasing staffing levels if demand increases.
Whilst no robust claims can be made about safety given the pilot nature of this RCT, no adverse events were
reported. In addition, our systematic search of diagnostic codes of serious or significant pathology in the
medical records of patients who directly accessed physiotherapy found no evidence that the direct access
pathway led to missed serious pathologies. This is in keeping with a recent analysis of 12,976 patient visits
to a US physical therapist student health centre over 10 years, without a physician referral that reported no
adverse events and no missed cases of serious pathology.28
Non-attendance rates
We also aimed to compare patient non-attendance rates for physiotherapy before and during patient direct
access, but we were unable to achieve this as the physiotherapy service changed the definition and processes
for recording non-attendance part way through the STEMS pilot trial.
Conclusion
In line with calls for research on ways to ensure patient demand can be met in primary care, this pilot trial
shows that a future large RCT is feasible and will provide high quality evidence about the clinical and cost
effectiveness of direct access to physiotherapy for patients with musculoskeletal pain.
References
1. Roland M, Everington S. Tackling the crisis in general practice. BMJ. 2016 Feb 17;352:i942. doi:
10.1136/bmj.i942
2. Hobbs FDR, Bankhead C, Mukhtar T, Stevens S, Perera-Salazar R, Holt T, Salisbury C on behalf of
the National Institute for Health Research School for Primary Care Research. Clinical workload in
UK primary care: a retrospective analysis of 100 million consultations in England, 2007–14. Lancet
2016; 387: 2323–30 Published Online April 5, 2016 http://dx.doi.org/10.1016/ S0140-
6736(16)00620-6
3. Jordan KP, Kadam UT, Hayward R, Young C, Croft P. Annual consultation prevalence of regional
musculoskeletal problems in primary care: an observational study. BMC Musculoskelet Disord
2010;11:144
4. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Ezzati M, Shibuya K, Salomon
JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M,
Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo
S, Barrero LH, Bartels DH, Basáñez MG, Baxter A, Bell ML, Benjamin EJ, et al.:Disability-adjusted
life years (DALYs)for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for
the global burden of disease study 2010. Lancet 2012, 380:2197-2223
Page 15 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
16
5. Holdsworth LK, Webster VS, McFadyen AK. What are the costs to NHS Scotland of self-referral to
physiotherapy? Results of a national trial. Physiotherapy 2007;93(1):3-11
6. Department of Health. Self-referral pilots to musculoskeletal physiotherapy and the implications of
improving access to other AHP services. Leeds. Department of Health; 2008
[www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_089
516]. Accessed 01 February 2015
7. Leemrijse CJ, Swinkels ICS, Veenhof C. Direct access to physical therapy in the Netherlands: results
from the first year in community-based physical therapy. Physical Therapy 2008;88(8):936-46
8. QIPP Quality and Productivity Case Studies. Musculoskeletal Physiotherapy: patient self-referral
2012 citing Holdsworth et al 2007, costs updated in accordance with Department of Health 2011
https://www.evidence.nhs.uk/qipp. Accessed 10th January 2015
9. Mallett R, Bakker E, Burton M. Is physiotherapy self-referral with Telephone Triage Viable, Cost-
effective and Beneficial to Musculoskeletal Outpatients in a Primary Care Setting? Musculoskeletal
Care 2014;12(4):251-60
10. The Kings Fund. The UK Private Health Market. 2014.
https://www.kingsfund.org.uk/sites/files/kf/media/commission-appendix-uk-private-health-
market.pdf
11. Primary Care Workforce Commission. The future of primary care. Creating teams for tomorrow.
2015 www.hee.nhs.uk
12. Bishop A, Tooth S, Protheroe J, Salisbury C, Ogollah RO, Jowett S, Hay EM, Foster NE and on
behalf of the STEMS study team. A pilot cluster randomised controlled trial to investigate the
addition of direct access to physiotherapy to usual GP-led primary care for adults with
musculoskeletal pain: the STEMS pilot trial protocol (ISRCTN23378642). Pilot and Feasibility
Studies 2015, 1:26 doi:10.1186/s40814-015-0020-4
13. Ware JE, Kosinski M, Bjorner JB, Turner-Bowker DM, Gandek B. Maruish ME. User’s manual for
the SF-36v2 Health Survey. 2nd ed. Lincoln, RI:QualityMetric Inc; 2007.
14. Angst F, Aeschlimann A, Stucki G. Smallest detectable and minimal clinically important differences
of rehabilitation intervention with their implications for required sample sizes using WOMAC and
SF-36 quality of life measurement instruments in patients with osteoarthritis of the lower extremities.
Arthritis Care Res. 2001;45(4):384–91.
15. Kosinski M, Zhao SZ, Dedhiya S, Osterhaus JT, Ware JE Jr. Determining minimally important
changes in generic and disease-specific health-related quality of life questionnaires in clinical trials
of rheumatoid arthritis. Arthritis Rheum.2000;43(7):1478–87.
16. Norman GR, Sloan JA, Wyrwich KW. Interpretation of changes in health-related quality of life: the
remarkable universality of half a standard deviation. Med Care. 2003;41(5):582–92.
17. SF-36.org: A community for measuring health outcomes using SF tools. http://www.sf-36.org/].
18. Herdman M, Gudex C, Lloyd A, Janssen MF, Kind P, Parkin D, Bonsel G, Badia X. Development
and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life
Research. 2011; 20(10): 1727–1736.
19. Nicholas MK. The pain self-efficacy questionnaire: taking pain into account. Eur J Pain.
007;11:153–63
20. Mead N, Bower P, Roland M. The general practice assessment questionnaire (GPAQ): development
and psychometric characteristics. BMC Fam Pract. 2008;9:13. doi:10.1186/1471-2296-9-13.
21. Wolfe F, Smythe H, Yunus M, et al. The American College of Rheumatology 1990 criteria for the
classification of fibromyalgia. Arthritis Rheum 1990; 33: 160–71
22. Puffer S, Torgerson D, Watson J. Evidence for risk of bias in cluster randomised trials: Review of
recent trials published in three general medical journals. BMJ 2003;327:785–789
23. Hahn S, Puffer S, Torgerson DJ, Watson J. Methodological bias in cluster randomised trials. BMC
Medical Research Methodology 2005. DOI: 10.1186/1471-2288-5-10
24. Diggle PJ, Heagerty P, Liang K-Y, Zeger SL. Analysis of Longitudinal Data. 2nd Edition. Oxford
University Press, Oxford.2002
Page 16 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
For peer review only
17
25. Adams G, Gulliford MC, Ukoumunne OC, Eldridge S, Chinn S, Campbell MJ. Patterns of intra-
cluster correlation from primary care research to inform study design and analysis. J Clin Epidemiol.
2004 57(8):785-94
26. Eldridge SM, Ashby D, Kerry S. Sample size for cluster randomized trials: effect of coefficient of
variation of cluster size and analysis method. Int J Epidemiol. 2006;35(5):1292-300
27. Salisbury C. http://ukpolicymatters.thelancet.com/making-the-most-of-evaluation-to-ensure-health-
policy-reform-is-evidence-based/ 2011
28. Mintken PE, Pascoe SC, Barsch AK, Cleland JA. Direct access to physical therapy services is safe
in a university student health center setting. J Allied Health. 2015;44(3):164-8
Competing interests
The authors declare that they have no competing interests.
Funding
The STEMS pilot trial was funded by the Chartered Society of Physiotherapy Charitable Trust (SRP (11)2).
NEF and AB are funded through a National Institute of Health Research (NIHR) Research Professorship
awarded to NE Foster (NIHR-RP-011-015). NEF is an NIHR Senior Investigator. The views and opinions
expressed are those of the authors and do not necessarily reflect those of the NHS, the NIHR or the
Department of Health. The North Staffordshire Primary Care Research Consortium provided additional
funding for GP and Physiotherapy Research Facilitators to advise on the engagement and recruitment of GP
practices and physiotherapists in the STEMS pilot trial.
Authors' contributions
AB helped plan the trial, contributed to the funding application, chaired the Trial Management Group
(TMG) and led the writing of this paper. RO developed the analysis plan and performed the quantitative
analyses. SJ developed the health economic data collection and analysis plan and supervised JK who
conducted the health economic analysis. ST was responsible for trial co-ordination, supporting the TMG, the
general practices and physiotherapy service. JP provided general practice expertise and contributed to the
training of physiotherapists offering the direct access pathway. EH provided senior trials leadership,
expertise and oversight. CS helped design the trial and provided general practice expertise. NEF led the
design of the trial and the funding application, and provided senior trials leadership and oversight. All
authors contributed to this paper and approved the final version.
Acknowledgements
The STEMS trial team acknowledges the support from Keele Clinical Trials Unit, including Dr Ruth
Beardmore (Research Programme Manager) for input into research governance and gaining of regulatory
approvals, and administrators Michelle Robinson and Victoria Harper for coordinating mailings of
consenting patients and general research administrative support. We also acknowledge the NIHR Clinical
Research Network (CRN) including Ian Thomas for coordinating systems to help the participating practices
identify eligible patients and assistance in providing anonymised patient data, the research nurse team,
including Julie Young, Debbie D’Cruz, Alice Mackie, William Cole, and Sian Jones who dealt with patient
queries and conducted minimum data collection via telephone. We thank the CRN physiotherapy and GP
research facilitators, Gemma Sellors, Carol Doyle and Beth Hanson. Thanks to the Independent Advisory
Panel comprising Jill Gamlin, Sue Greenhalgh, Lesley Holdsworth and Ruth ten Hove who provided advice
on setting up patient direct access to physiotherapy and Sue Greenhalgh for her input into the
physiotherapist training. We are grateful to the general practices and physiotherapy service that participated
Page 17 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
18
in this pilot trial and in particular the support of Ruth Heaton, Therapy Manager, and to the physiotherapists
who delivered care to patients.. We acknowledge Arthritis Research UK who funded early stakeholder
thinktanks to develop and design the STEMS trial. Finally we are particularly indebted to our PPIE
members, Trial Steering Committee members and all the participants who provided data.
Data sharing
No additional data available
Figure and table legends
Figure 1: STEMS pilot trial flowchart
Table 1: STEMS pilot trial questionnaire measures
Table 2: Comparability of baseline characteristics
Table 3: Descriptive statistics (mean and SD or frequency and %) for outcome measures at each time-point
Table 4: Costs per participant by trial arm over 12 months
Table 5: EQ-5D-5L scores and QALYs at each time point
Supplementary Table S1: Baseline characteristics of participants by care pathway
Supplementary Table S2: Adjusted estimates (adjusted mean difference or odds ratio) and 95% confidence intervals
for the treatment effect of outcomes based on mixed effect model (linear for continuous and logistic for binary)
Supplementary Table S3: Healthcare resource use by trial arm over 12 months. Results are number of patients
(%) reporting each resource use type and mean (SD) number of visits/treatments per patient unless otherwise
stated
Page 18 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Figure 1: STEMS pilot trial flowchart A flowchart showing the flow o 165x233mm (300 x 300 DPI)
Page 19 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Supplementary Table S1: Baseline characteristics of participants by care pathway
Control practices
n = 553
Intervention practices
n = 425
Usual GP-led care only Usual GP-led care Direct access to physiotherapy
Key characteristics Not
referred to
physiother
apy
n =449
(81.2%)
Referred
to
physiother
apy
n=104
(18.8%)
Not referred to
physiotherapy
n = 273
(64.2%)
GP referral to
physiotherapy
n = 10
All
physiotherapy
self-referrers
n =142
Recommen
ded self-
referrers*
n = 98
True self-
referrers†
n = 44
Non-clinical characteristics
Age, mean (SD) 59.3 (14.8) 55.4 (13.6) 55.3 (15.6) 52.5 (8.3) 56.5 (14.7) 56.1 (13.4) 57.2 (17.3)
Gender: Female, n (%) 253 (56.4) 58 (55.8) 155 (56.7) 5 (50%) 88 (62.0) 57 (58.2) 31 (70.5)
Employment: in paid work (part/full-time), n (%) 185 (41.8) 58 (55.8) 118 (43.5) 7 (70%) 64 (46.4) 49 (51.0) 15 (35.7)
Extent to which pain has affected performance at
work in the past 1 month (0-10 NRS), mean (SD)
4.8 (3.1) 4.5 (3.4) 5.1 (3.2) 3.3 (2.3) 4.7 (2.9) 4.6 (2.6) 5 (3.8)
Education: No qualifications, n (%) 118 (30.0) 15 (17.2) 67 (28.0) 2 (28.6) 35 (28.5) 24 (28.2) 11 (29.0)
Deprivation tertile, n (%)
Most deprived third 137 (30.5) 24 (23.1) 67 (24.5) 2 (20%) 34 (23.9) 27 (27.6) 7 (15.9)
Middle third 149 (33.2) 35 (33.7) 97 (35.5) 4 (40%) 44 (31.0) 24 (24.5) 20 (45.5)
Least deprived third 163 (36.3) 45 (43.3) 109 (39.9) 4 (40%) 64 (45.1) 47 (48.0) 17 (38.6)
Health literacy: Finds health information/leaflets
difficult to understand, n (%)
256 (57.5) 55 (52.9) 162 (57.7) 7 (70%) 80 (56.7) 56 (57.7) 24 (54.6)
Clinical characteristics
Physical Health: SF-36 PCS, mean (SD) 35.2 (10.3) 38.0 (8.8) 36.6 (10.0) 38.6 (8.3) 36.5 (9.8) 37.1 (9.8) 35.1 (9.8)
Mental Health: SF-36 MCS, mean (SD) 44.2 (13.5) 45.3 (14.3) 42.5 (13.7) 40.1 (18.0) 43.2 (14.2) 43.8 (14.3) 42.0 (13.9)
Current episode duration: >6 weeks, n (%) 307 (72.2) 79 (78.2) 198 (77.7) 8 (80.0) 106 (78.5) 73 (77.7) 33 (80.5)
Comorbidities‡: 2 or more other conditions, n (%) 278 (61.9) 55 (52.9) 161 (58.9) 5 (50.0) 75 (52.8) 47 (48.0) 28 (63.6)
Pain self-efficacy (0-60), mean (SD) 33.1 (16.3) 35.1 (17.3) 32.3 (16.6) 33.5 (16.2) 32.7 (15.9) 33.6 (15.4) 30.8 (17.0)
Page 20 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Satisfaction with services received
Satisfaction at 2 Months§, mean (SD) 6.6 (3.0) 7.2 (2.5) 6.9 (2.8) 5.0 (2.3) 7.0 (3.0) 6.8 (2.8) 7.5 (3.3)
Satisfaction at 6 Months§, mean (SD) 6.8 (2.8) 7.5 (2.3) 7.3 (2.7) 6.0 (2.2) 7.1 (2.7) 7.3 (2.4) 6.8 (3.1)
*Recommended self-referrers are those seen by a GP or nurse ‘recommended’ to self-refer †True self referrers are those who choose to self-refer to physiotherapy without contacting their GP practice ‡The conditions include high blood pressure, heart problems, stroke, diabetes, depression or anxiety, osteoporosis, arthritis, asthma or bronchitis, liver disease, cancer and others
SF-36 PCS= 36-Item Short Form physical component summary – the higher the score the better the physical health
SF-36 MCS=36-Item Short Form mental component summary – the higher the score the better the mental health
Pain self-efficacy scale: 10 item scale, score range=0-60 (0=not at all confident, 60=completely confident despite pain). §0-10 Numerical Rating Scale: (0 = not satisfied, 10 = very satisfied).
Page 21 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Supplementary Table S2: Adjusted estimates (adjusted mean difference or odds ratio) and
95% confidence intervals for the treatment effect of outcomes based on mixed effect model
(linear for continuous and logistic for binary).
Outcomes 2 months 6 months 12 months
Intervention vs. control arm (reference
category) Estimate
(95% CI)
Estimate
(95% CI)
Estimate
(95% CI)
Physical Health: SF-36 PCS -0.14 (-1.02, 0.74) -0.28 (-1.35, 0.79) 0.12 (-1.27, 1.51)
Mental Health: SF-36 MCS 0.001 (-1.24, 1.24) 0.52 (-0.86, 1.91) 0.34 (-1.40, 2.07)
Pain self-efficacy (0-60) 0.62 (-0.68, 1.93) 2.22 (0.49, 3.96) 1.94 (-0.35, 4.24)
Overall perceived change from baseline:
completely recovered or much improved* 0.63 (0.31, 1.29) 1.37 (0.72, 2.59) 1.05 (0.56, 1.98)
Convenience of services received for pain or
pain related symptoms (0-10 NRS) 0.11 (-0.56, 0.78) 0.17 (-0.34, 0.62) -
Satisfaction with the services received for pain
problem (0-10 NRS) 0.19 (-0.29, 0.67) 0.08 (-0.44, 0.60) -
Adjusted for baseline outcome measure (where applicable), age, gender, widespread pain, area deprivation and a random
effect for GP practice
Continuous outcomes estimated by linear mixed model. *Binary outcome estimated by mixed effect logistic regression; the
estimates are odds ratios and 95% CIs
Page 22 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Supplementary Table S3: Healthcare resource use by trial arm over 12 months. Results are
number of patients (%) reporting each resource use type and mean (SD) number of
visits/treatments per patient unless otherwise stated.
Resource use category Control
(n=318) Intervention
(n=237)
n (%) Mean (SD)
a n (%) Mean (SD)
NHS
GP 218 (68%) 3.13 (3.95) 153 (64%) 2.85 (3.95)
Practice nurse 82 (26%) 0.87 (3.72) 52 (22%) 0.93 (4.21)
Physiotherapist 106 (33%) 1.93 (5.19) 96 (41%) 2.33 (5.10)
Orthopaedic surgeon 67 (21%) 0.47 (1.12) 36 (15%) 0.36 (1.01)
Rheumatologist 26 (8%) 0.16 (0.66) 12 (6%) 0.08 (0.39)
Acupuncturist 8 (3%) 0.13 (1.15) 5 (2%) 0.04 (0.31)
Chiropractor 7 (2%) 0.09 (0.81) 4 (2%) 0.03 (0.34)
Occupational therapist 15 (5%) 0.18 (1.16) 12 (5%) 0.11 (0.56)
Other healthcare professionals 29 (9%) 0.27 (1.06) 20 (8%) 0.20 (0.81)
Private
Physiotherapist 18 (6%) 0.29 (1.72) 14 (6%) 0.71 (4.86)
Orthopaedic surgeon 7 (2%) 0.04 (0.33) 4 (2%) 0.03 (0.23)
Rheumatologist 0 0.00 (-) 1 (0.5%) 0.01 (0.13)
Acupuncturist 4 (1%) 0.07 (0.70) 8 (3%) 0.13 (0.92)
Chiropractor 9 (3%) 0.21 (1.94) 5 (2%) 0.15 (1.09)
Occupational therapist 0 0.00 (-) 1 (0.5%) 0.02 (0.25)
Other healthcare professionals 6 (2%) 0.08 (0.73) 3 (1%) 0.17 (2.22)
Other resource use
Investigations (MRI, CT, X-rays,
“scan”)
124 (39%) 1.88 (8.67) 86 (36%) 0.81 (1.52)
Injections 27 (8%) 0.16 (0.56) 19 (8%) 0.19 (0.93)
Inpatient stay in days 29 (9%) 0.65 (3.12) 22 (9%) 0.56 (3.82)
Prescribed Medication (n, %) 255 (80%) - 185 (78%) -
‘Over the counter’ treatments (n,
%) 203 (63%) - 141 (59%)
Work-related outcomes
Time-off work due to
musculoskeletal condition 20 (18%) - 19 (19%)
Work absence days due to
musculoskeletal condition 10.28 - 8.34 -
a Data is based on patients reporting resource utilisation and includes resource use data from patients who returned a questionnaire at both
follow-up time points
Page 23 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
Section/Topic Item No
Standard Checklist item
Extension for cluster designs
Page number
Title and abstract
1a Identification as a randomised trial in the title
Identification as a cluster randomised trial in the title
1
1b Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts)i,ii
See table 2 1
Introduction
Background and objectives
2a Scientific background and explanation of rationale
Rationale for using a cluster design
2
2b Specific objectives or hypotheses
Whether objectives pertain to the the cluster level, the individual participant level or both
2
Methods
Trial design 3a Description of trial design (such as parallel, factorial) including allocation ratio
Definition of cluster and description of how the design features apply to the clusters
3
3b Important changes to methods after trial commencement (such as eligibility criteria), with reasons
n/a
Participants 4a Eligibility criteria for participants
Eligibility criteria for clusters
3 + protocol
4b Settings and locations where the data were collected
3
Interventions 5 The interventions for each group with sufficient details to allow replication, including how and when they were actually administered
Whether interventions pertain to the cluster level, the individual participant level or both
3 + protocol
Outcomes 6a Completely defined pre-specified primary and secondary outcome measures, including how and when they were assessed
Whether outcome measures pertain to the cluster level, the individual participant level or both
n/a as pilot
Page 24 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
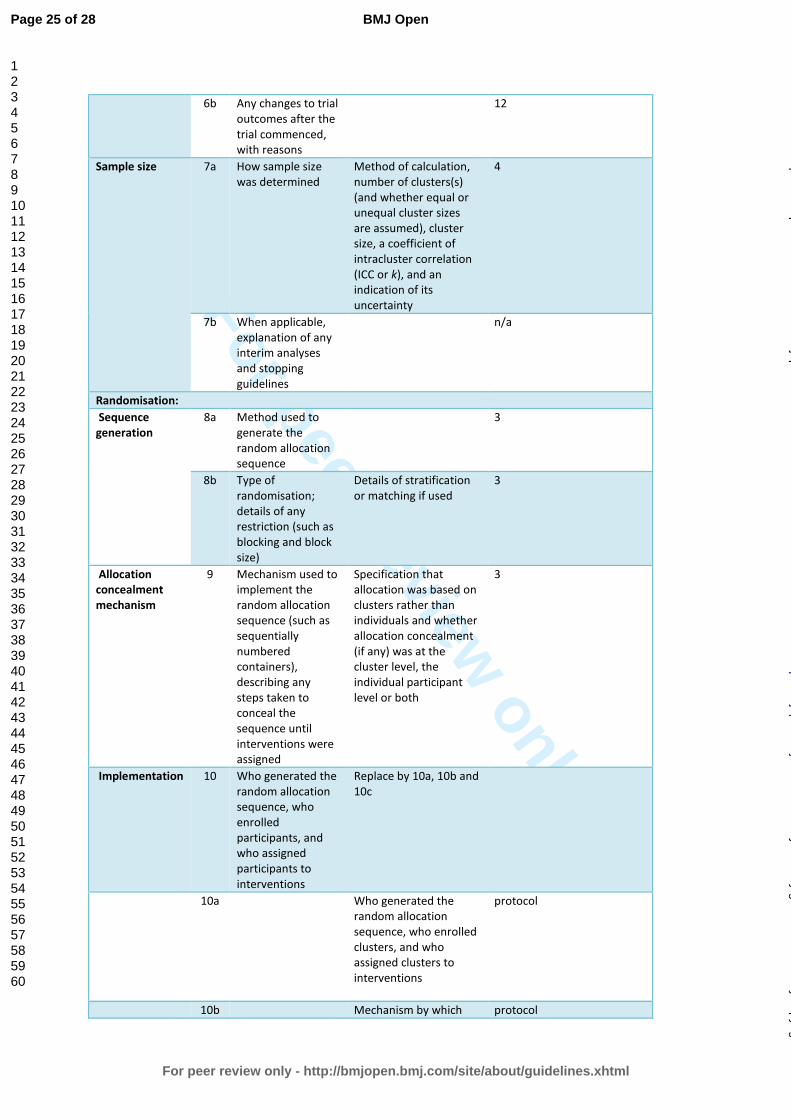
For peer review only
6b Any changes to trial outcomes after the trial commenced, with reasons
12
Sample size 7a How sample size was determined
Method of calculation, number of clusters(s) (and whether equal or unequal cluster sizes are assumed), cluster size, a coefficient of intracluster correlation (ICC or k), and an indication of its uncertainty
4
7b When applicable, explanation of any interim analyses and stopping guidelines
n/a
Randomisation:
Sequence generation
8a Method used to generate the random allocation sequence
3
8b Type of randomisation; details of any restriction (such as blocking and block size)
Details of stratification or matching if used
3
Allocation concealment mechanism
9 Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned
Specification that allocation was based on clusters rather than individuals and whether allocation concealment (if any) was at the cluster level, the individual participant level or both
3
Implementation
10 Who generated the random allocation sequence, who enrolled participants, and who assigned participants to interventions
Replace by 10a, 10b and 10c
10a Who generated the random allocation sequence, who enrolled clusters, and who assigned clusters to interventions
protocol
10b Mechanism by which protocol
Page 25 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from

For peer review only
individual participants were included in clusters for the purposes of the trial (such as complete enumeration, random sampling)
10c From whom consent was sought (representatives of the cluster, or individual cluster members, or both), and whether consent was sought before or after randomisation
protocol
Blinding 11a If done, who was blinded after assignment to interventions (for example, participants, care providers, those assessing outcomes) and how
3
11b If relevant, description of the similarity of interventions
Statistical methods
12a Statistical methods used to compare groups for primary and secondary outcomes
How clustering was taken into account
protocol
12b Methods for additional analyses, such as subgroup analyses and adjusted analyses
protocol
Results
Participant flow (a diagram is strongly recommended)
13a For each group, the numbers of participants who were randomly assigned, received intended treatment, and were analysed for the primary outcome
For each group, the numbers of clusters that were randomly assigned, received intended treatment, and were analysed for the primary outcome
Figure 1
13b For each group, losses and exclusions after randomisation, together with reasons
For each group, losses and exclusions for both clusters and individual cluster members
Figure 1
Recruitment 14a Dates defining the 5
Page 26 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
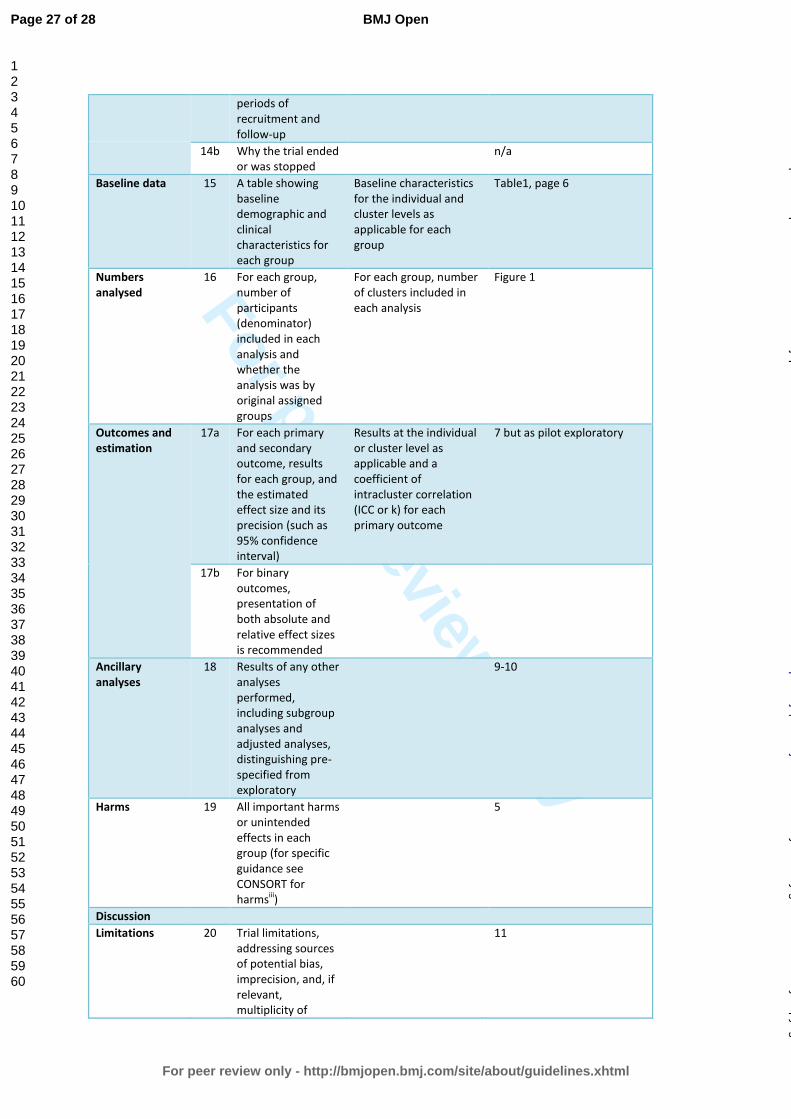
For peer review only
periods of recruitment and follow-up
14b Why the trial ended or was stopped
n/a
Baseline data 15 A table showing baseline demographic and clinical characteristics for each group
Baseline characteristics for the individual and cluster levels as applicable for each group
Table1, page 6
Numbers analysed
16 For each group, number of participants (denominator) included in each analysis and whether the analysis was by original assigned groups
For each group, number of clusters included in each analysis
Figure 1
Outcomes and estimation
17a For each primary and secondary outcome, results for each group, and the estimated effect size and its precision (such as 95% confidence interval)
Results at the individual or cluster level as applicable and a coefficient of intracluster correlation (ICC or k) for each primary outcome
7 but as pilot exploratory
17b For binary outcomes, presentation of both absolute and relative effect sizes is recommended
Ancillary analyses
18 Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing pre-specified from exploratory
9-10
Harms 19 All important harms or unintended effects in each group (for specific guidance see CONSORT for harmsiii)
5
Discussion
Limitations 20 Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of
11
Page 27 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from
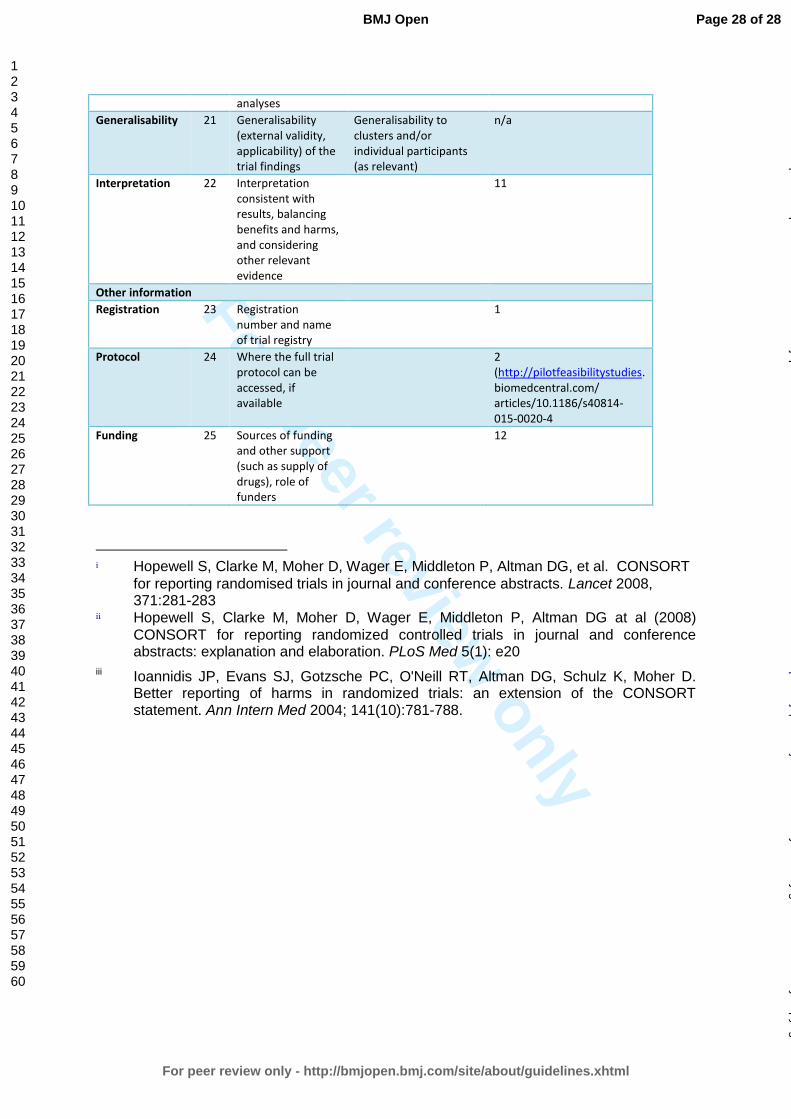
For peer review only
analyses
Generalisability 21 Generalisability (external validity, applicability) of the trial findings
Generalisability to clusters and/or individual participants (as relevant)
n/a
Interpretation 22 Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence
11
Other information
Registration 23 Registration number and name of trial registry
1
Protocol 24 Where the full trial protocol can be accessed, if available
2 (http://pilotfeasibilitystudies. biomedcentral.com/ articles/10.1186/s40814-015-0020-4
Funding 25 Sources of funding and other support (such as supply of drugs), role of funders
12
i Hopewell S, Clarke M, Moher D, Wager E, Middleton P, Altman DG, et al. CONSORT
for reporting randomised trials in journal and conference abstracts. Lancet 2008, 371:281-283
ii Hopewell S, Clarke M, Moher D, Wager E, Middleton P, Altman DG at al (2008)
CONSORT for reporting randomized controlled trials in journal and conference abstracts: explanation and elaboration. PLoS Med 5(1): e20
iii Ioannidis JP, Evans SJ, Gotzsche PC, O'Neill RT, Altman DG, Schulz K, Moher D. Better reporting of harms in randomized trials: an extension of the CONSORT statement. Ann Intern Med 2004; 141(10):781-788.
Page 28 of 28
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 11 July 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2016-012987 on 12 March 2017. D
ownloaded from