Embed Size (px)
Citation preview

For peer review only
Cost-effectiveness of a repeat HIV test in pregnancy in India
Journal: BMJ Open
Manuscript ID: bmjopen-2014-006718
Article Type: Research
Date Submitted by the Author: 23-Sep-2014
Complete List of Authors: Joshi, Smita; Hirabai Cowasji Jehangir Medical Research Institute, Preventive Oncology Kulkarni, Vinay; Prayas, Gangakhedkar, Raman; National AIDS Research Institute, Mahajan, Uma; Hirabai Cowasji Jehangir Medical Research Institute, Shamra, Sushama; MIMER, Shirole, Devendra; Kamala Nehru Hospital, Chandhiok, Nomita; Indian Council of Medical Research,
<b>Primary Subject Heading</b>:
HIV/AIDS
Secondary Subject Heading: Epidemiology, HIV/AIDS, Obstetrics and gynaecology
Keywords: EPIDEMIOLOGY, HIV & AIDS < INFECTIOUS DISEASES, Public health < INFECTIOUS DISEASES
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on D
ecember 14, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006718 on 11 June 2015. D
ownloaded from

For peer review only
Page 1 of 15
Cost-effectiveness of a repeat HIV test in pregnancy in India
Joshi Smita1, Kulkarni Vinay2, Gangakhedkar Raman3, Mahajan Uma1, Sharma Sushma4,
Shirole Devendra5, Chandhiok Nomita6,
1Hirabai Cowasji Jehangir Medical Research Institute (HCJMRI), Jehangir Hospital Premises,
32, Sasoon Road, Pune 411 001, Maharashtra, India. E-Mail: [email protected]
2 Prayas Health Group, Amrita Clinic, Athwale Corner, Karve Road, Deccan Gymkhana,
Pune 411 004, India. E-Mail: [email protected]
3National AIDS Research Institute, 73, G Block, MIDS, Bhosari, Pune-411026, India.
Email: [email protected]
4 MIMER Hospital, Talegaon, Pune. Email: [email protected]
5Kamla Nehru Hospital and Pune Municipal Corporation, Pune, India (added posthumously)
6 Indian Council of Medical Research, New Delhi, India. E-mail: [email protected]
Address for correspondence:
Dr Smita Joshi
Hirabai Cowasji Jehangir Medical Research Institute, Jehangir Hospital Premises, 32
Sassoon Road, Pune-411001
Email: [email protected], Phone no: +91-9881132506
Key words: HIV, PMTCT, cost-effectiveness, HIV prevention
Word count: 2754
Page 1 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 2 of 15
Abstract:
Objective: To evaluate cost-effectiveness of second HIV test in pregnancy
Background: Current strategy of single HIV test during pregnancy in India is likely to miss
new HIV infections acquired after the first test or those HIV infections that were missed in the
first test due to a false negative HIV test.
Methods: In a cross-sectional study between August 2011 and April 2013, 9097 pregnant
women who had tested HIV negative at least three months prior and who were near term (34
weeks or beyond) or within 4 weeks of post-partum period were offered a second HIV test.
Primary and secondary outcome: Primary outcome was new (incident) HIV infections in
pregnant women who were tested HIV negative three months prior and secondary outcome
was QALYs gained by addition of second HIV test.
Results: We detected 4 new HIV infections in the second test giving an HIV incidence of
0.12 (95% 0.032-0.297) per 100 person women years (PWY). One-way sensitivity analysis
of cost and effectiveness of current strategy (of single HIV test) and proposed strategy (of
additional second HIV test during pregnancy) was performed. Current strategy of a single
HIV test is 13.5 times costlier for less QALYs gained as compared to proposed repeat HIV
testing of pregnant women who test negative during the first test. The incremental cost-
effectiveness ratio varied the most in response to change in HIV incidence and our proposed
strategy remained cost saving with different probabilities of HIV incidence.
Conclusions: Our results warrant urgent consideration of including second HIV test of all
pregnant women in the national programme.
Key Words
HIV, PMTCT, cost-effectiveness, 2nd HIV test in pregnancy
Page 2 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 3 of 15
Strengths and limitations of this study:
• Of all the biological interventions to prevent HIV transmission, PMTCT of HIV is the
most efficacious intervention.
• Current strategy of single HIV test during pregnancy in India is likely to miss new HIV
infections acquired after the first test or those HIV infections that were missed in the
first test due to a false negative HIV test.
• This is the first report describing cost-effectiveness of 2nd HIV test in pregnancy from
India.
• Current strategy of a single HIV test results in 13.5 times more cost for less QALYs
gained as compared to proposed repeat HIV testing of pregnant women who test
negative in the first test which offers 1 healthy child at USD 4.14.
• These findings will help in shaping national policies in India and other countries with
high HIV burden.
Page 3 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 4 of 15
Introduction:
Mother to child transmission of HIV (MTCT) remains the most significant route of HIV
infection among children in the developing countries. At the same time, of all the biological
interventions to prevent HIV transmission, prevention of MTCT (PMTCT) of HIV is the most
efficacious intervention. The science of PMTCT has seen transformations by leaps and
bounds and world is making strides towards the elimination of new HIV infections among
children by 2015(1) by improving coverage of HIV testing of pregnant women and provision
of effective treatment with antiretroviral treatment (ART) to reduce the risk of MTCT. The
global plan towards elimination of new HIV infections among children reported 38%
decrease in new HIV infections among children(1). Eliminating pediatric HIV infection
appears to be the most achievable goal globally. In the developed regions of the world,
MTCT transmission rates are as low as 2% due to wide coverage and provision of highly
effective anti-retroviral treatment (ART) regimen(2,3).
In India, PMTCT program is called the Prevention of Parent to Child Transmission of
HIV/AIDS (PPTCT) programme and it was initiated in 2002. Since then, there has been
sustained scale up of PPTCT programme in the country. In India, total annual births in 2009
were 26,787,000(4) and the Interagency Task Team of UNICEF on the prevention and
treatment of HIV infection in pregnant women, mothers and children estimated that of these
27 million annual pregnancies in India, 22,000 to 61,0000 occurred in HIV positive pregnant
women(5). It is estimated by National AIDS Control Organization (NACO) that 5.4% of the
new HIV infections in India are due to transmission of infection from parent to child(6). The
PPTCT program of NACO offers routine HIV testing to all pregnant mothers and as per the
current protocol women are tested only once during pregnancy(7). Therefore, pregnant
women who are in the window period at the time of the first HIV test or those who acquire
HIV after the first test do not receive interventions to prevent transmission of HIV to the
baby. Acute HIV infection is associated with very high levels of HIV-1 RNA(8,9) thus acute
maternal HIV-1 infection during pregnancy and breast-feeding is associated with higher rates
of mother-to-child transmission (MTCT) of HIV-1(10–12). The aim of eliminating MTCT of
Page 4 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 5 of 15
HIV will be accomplished only if appropriate strategies to prevent transmission are applied
for each at risk situation. The Centre for Disease Control (CDC), USA has recommended
repeat HIV testing in the third trimester for all women in jurisdictions with elevated HIV or
AIDS incidence and for women receiving health care in facilities with at least one diagnosed
HIV case per 1,000 pregnant women per year(13). Second HIV testing of pregnant women is
not yet implemented in India. In addition to the already declining HIV epidemic and other
competing health priorities, we are at the cross roads of carefully allocating available
resources for HIV prevention efforts. In order to include the second HIV test of pregnant
women in the National programme to achieve the goal of elimination of MTCT; a cost-
effectiveness analysis of the intervention could help policy makers in taking an appropriate
decision for implementation of the intervention. Therefore we conducted a study to evaluate
the utility and cost-effectiveness of an additional HIV test at or near term among pregnant
women attending antenatal clinics in Pune, Maharashtra.
Methods:
The study was approved by the Ethics Committee of Hirabai Cowasji Jehangir Medical
Research Institute (HCJMRI) and Jehangir Clinical Development Centre (JCDC). The study
was conducted at 2 Primary Health Centres (Kamshet and Talegaon in Maval Tehsil) and 3
urban sites (Maharashtra Institute of Medical Education and Research, Kamla Nehru Hospital
and Sane Guruji Hospital). The study was conducted between August 2011 and April 2013.
Monthly data regarding number of pregnant women tested for HIV (1st HIV test as per
national guidelines) and number detected with HIV (baseline HIV prevalence in pregnant
women) were collected from the NACO ART centre at the site.
In this cross sectional study, women in the late third trimester of pregnancy (beyond
34 weeks of pregnancy) with a documented HIV negative test report at least 3 months prior to
the visit, willing to sign a written informed consent form and willing to undergo a repeat HIV
test were consented and offered a second HIV test. Written informed consent included
possibility of a telephonic call or a home visit if they were confirmed to be HIV-infected so that
Page 5 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 6 of 15
PPTCT services could be offered. After signing the informed consent form, data were
collected on a structured questionnaire regarding the woman’s age, education, religion,
marital status, occupation of both partners, age at first sexual contact, husband’s risk for HIV
infection, history of any risk after the initial HIV test (history of blood transfusion, tattoo,
ear/nose piercing, injections) and obstetrical history. A rapid HIV test was performed on whole
blood sample collected by a finger prick on site. Post-test counseling was done and HIV test
report was given to the woman immediately. Women were also counseled to encourage their
partners to get themselves tested for HIV as per the national protocol and for an institutional
delivery.
If the HIV test report was positive in the rapid HIV test, a second venous sample was
immediately collected for confirmation of HIV infection and women were called after one week
for the test report. Women who were detected with HIV infection were referred appropriately
for PPTCT interventions. Recently delivered women who could not be tested for 2nd HIV test
prior to delivery (for e.g. those who delivered on admission) but had a documented negative
HIV test report at least 3 months prior to delivery were also invited to participate in the
proposed study and were tested within 4 weeks of delivery so that it could not be attributed to
HIV acquisition after delivery.
Data analysis:
Data were collected on a structured questionnaire. Data entry was done in MS Access 2007
software and analyzed using STATA 12.0 software. Standard formulae were used to
calculate 95% confidence interval (CI). TreeAge software was used for cost-effectiveness
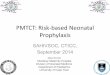
and sensitivity analysis. A decision analysis model was created to compare 2 strategies
(Figure 1): 1) current strategy of a single HIV test during pregnancy that is implemented by
NACO, and 2) proposed strategy of addition of 2nd HIV test of pregnant women after 34
weeks of pregnancy or within 4 weeks after delivery who were tested HIV negative in the first
test (in addition to current strategy of single HIV test). The model was created for 9097
women enrolled in the study to compare the proposed strategy with the current strategy. The
Page 6 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 7 of 15
model included 4 women who were HIV negative in the first test at baseline but were
detected with HIV infection after three months in the second test and had an opportunity to
prevent MTCT with the use of ART. We also compared HIV status of their babies and life
expectancy of the HIV infected baby with and without ART. Baseline values for input
parameters for decision analysis model are given in Table 1. The programme costs included
personnel, infrastructure, recurrent costs, cost of ART for PPTCT to women detected with
HIV and treatment of HIV infected baby. For the current strategy, USD 3.33 was included as
the cost of 1st HIV test (14), (15). For the proposed strategy the cost of 1st HIV test as well as
2nd HIV test (USD 0.6) was included in the model. We included the actual cost of HIV test kit
for 2nd HIV test and no additional costs were included since the existing infrastructure of
NACO at these sites can be utilized. Thus additional cost with proposed strategy included
the cost of the actual HIV test kit with confirmation of HIV infection which was INR 30 (USD
0.6) per woman for this project (in addition to the cost of 1st HIV test). The probabilities of
new HIV infections, ART for mother and HIV status of the baby at the end of 18 months
obtained from this study were used for decision analysis. We have assumed that life
expectancy of an HIV-infected child in India on ART would be at least 50% of the normal life
expectancy(16) and since the life expectancy of a healthy baby in India is 65 years(17), for
convenience we rounded the life expectancy to 30 years. Thus we included cost of ART for
an HIV infected child(18) for 30 years after birth. We assigned a QALY (quality adjusted life
years) weight of 1 for a healthy child (HIV-negative), 0.83 for HIV infected child with ART,
and 0.73 for the one without ART(19),(20). The outcome in terms of QALY, costs and
probability were entered into the TreeAge software for cost-effectiveness and sensitivity
analysis. We performed one-way sensitivity analysis to determine the effect of HIV incidence
on the cost-effectiveness of the programme.
Results:
We enrolled 9164 women in this study of whom 67 were excluded from final analysis due to
inadequate data and thus 9097 women are included in the final analysis. Majority of the
Page 7 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 8 of 15
enrolled participants (69.4%) were less than 25 years of age, 94.5% had some education
and 79% of the participants were Hindu. About 90% of them were housewives and 99.4%
were living with a husband who was earning. About 45.4% were primigravida and 99.9%
were not infected with HIV in the second HIV test. Baseline HIV prevalence in pregnant
women (HIV prevalence in pregnant women during the first HIV test) at rural sites was 0.42
and at urban sites it was 0.46 and the difference was not statistically significant [data not
shown].
We enrolled 2229 women at rural sites and 6868 women at urban sites. Two women
each were detected with new HIV infection in the second test at the rural and urban sites.
Thus HIV incidence at the urban sites was 0.8 (95% CI 0.0.21-2.0) per 1000 Person Women
Years (PWY) and it was 2.3 (95% 0.62-5.81) per 1000 PWY at rural sites. HIV incidence at
the rural sites was higher than that of urban women sites but the difference was not
statistically significant. The overall HIV incidence was 1.2 per 1000 PWY (95% CI 0.32-2.97).
Of the 9097 women included in the final analysis, 4 women were detected with HIV
infection in the 2nd HIV test as stated above. Their partners were also tested for HIV and all 4
were detected to be HIV-infected. However, none of them were aware of their HIV status. All
these 4 women were primigravida and their mean age was 27.25 (range 20-35 years). Of
these 4 women, 1 woman refused to accept the test result and absconded. One woman
defaulted on treatment for PPTCT and her baby was found to be infected with HIV at 12
months of follow- up. Two women completed ART for PPTCT and their babies remained HIV
negative at 18 months. These transmission probabilities and above mentioned costs were
used in the TreeAge software. On rollback the cost of proposed strategy i.e. addition of 2nd
HIV test in late pregnancy was USD 4.14 per 64.98 QALYs gained (equivalent to one
healthy life of an HIV un-infected child) whereas the current strategy of single HIV test during
pregnancy requires USD 55.83 per 39.09 QALYs gained. Thus the currently administered
national strategy spends 13.5 times more USD for less QALYs gained.
Page 8 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 9 of 15
Sensitivity analysis: One-way sensitivity analysis was done to determine the changes in
cost-effectiveness with different probabilities of HIV incidence and it is presented in
Table 3. The incremental cost-effectiveness ratio varied the most in response to change in
HIV incidence and our proposed strategy remained cost saving with different probabilities of
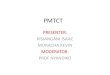
HIV incidence. Figure 2 represents cost effectiveness ratio (CER) versus HIV incidence and
CER remains almost stable at 1.4 in spite of increasing HIV incidence.
Discussion:
Our study provides an important lead to strengthen NACO’s programme for PPTCT and
addition of 2nd HIV test near term of pregnant women who were tested HIV negative in the
first HIV test done early in pregnancy was found to be cost effective. To our knowledge this
is the first study in India that has evaluated HIV incidence and cost-effectiveness of 2nd HIV
test among pregnant women. Current strategy of a single HIV test results in 13.5 times more
cost for less QALYs gained as compared to proposed repeat HIV testing of pregnant women
who test negative in the first test which offers 1 healthy child at USD 4.14. Our proposed
strategy is cost effective only with addition of HIV test kit cost and without addition of
incidental benefits of early HIV diagnosis of young women and their partners which include
early diagnosis and linkage to care and increasing chances of better treatment outcomes.
With current programme guidelines of offering lifelong ART to all pregnant and lactating
mothers irrespective of CD4 counts, this becomes even more beneficial. It is also worth
noting that we detected one woman with HIV infection on the second day of her delivery.
Thus repeat HIV testing should be offered to women in the immediate post-partum period if
the second test was not done prior to delivery or if they were never tested before.
For the second HIV test we included the actual kit cost that was paid during the study
period. Competitive costing for bulk purchase of the HIV kit under NACO’s programme for
PPTCT will lead to further cost reductions and the programme will be even more cost
effective with less USD spent for the same QALYs gained.
Page 9 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 10 of 15
During 2012, about 5.71 million pregnant women were tested for HIV in India. The
overall HIV prevalence amongst them was 0.17% while in Maharashtra it was 0.23%(21).
We observed a higher prevalence (0.45) of HIV in pregnant women at our study sites that
are located in Maharashtra for the first HIV test.
A wide variation of HIV prevalence among antenatal women has been reported
across different states in India with lowest HIV prevalence of 0.02% in Arunachal Pradesh,
Jammu and Kashmir and highest prevalence of 0.84% in Nagaland. HIV incidence among
pregnant women is likely to vary similarly across different states/ sites within India. Our
study indicates that repeat HIV testing is cost effective even with very low HIV incidence
(<0.0001) and this strategy can be implemented and would be beneficial for all the states in
India.
Although we could not ascertain whether all 4 new HIV infections were acquired after
the first test (since we did not perform detuned ELISA on the samples) and it is possible that
the first HIV test during pregnancy was a false negative test, our large study, for the first time
in India, provides some insight into the HIV incidence among pregnant women.
Considering our HIV incidence of 1.2 per 1000 PWY, a substantial number of new HIV
infected pregnant women could be detected with the proposed strategy of 2nd HIV test and
this opportunity for PMTCT should not be missed if India wishes to achieve the goal of zero
new HIV infection.
Previous study from Pune region has estimated declining HIV incidence in young
pregnant women based on estimation by exposure person-time, which was an estimate of
the average age specific duration of marriage(22). This study reported that the estimated
HIV incidence decreased from 2.2/100 PYs (95% CI: 1.6 to 3.0) in 2002-2003 to 0.73/100
PYs (95% CI: 0.5 to 1.0) in 2006(22). Our finding of HIV incidence of 0.12/ 100 PWY
indicates that since 2006, during the last 8 years there appears to be substantial decline in
new HIV infections among young pregnant women.
In our study, male partners of women newly detected with HIV were encouraged to
get tested for HIV after appropriate pre-test counselling and all 4 male partners were also
Page 10 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 11 of 15
found to be HIV infected. They were referred appropriately and this additional benefit of early
diagnosis, referral and linkage to treatment provides additional collateral benefit and addition
to cost-effectiveness of our proposed intervention. Spread of HIV among married
monogamous women from the partners with high-risk behaviour has been previously
reported(23). It is possible that increased male partner involvement, counseling and testing
of male partners at the time of first test could avert some of the transmissions to women and
consequentially to their children. In addition to CDC(13), rescreening of pregnant women in
the last trimester has been recommended by South African government(24) and has been
shown to be cost effective(19).
We conclude that re-screening of all pregnant women in the last trimester/
immediately after delivery is cost effective and our findings will help NACO in shaping the
policy for strengthening PMTCT programme.
Page 11 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 12 of 15
Acknowledgements:
This study was funded by the Indian Council of Medical Research (IRIS ID no. 2010-08370).
We thank authorities at the Pune Municipal Corporation, Sane Guruji Hospital, Kamla Nehru
Hospital, Taluka Medical Office, Maval Taluka and The District Health Officer of Pune for
allowing us to conduct this study at various study sites. We thank our staff for their tireless
efforts to complete this large study. We thank Director and other staff of HCJMRI for the
administrative and logistic support. We sincerely thank Dr Kenneth Freedberg, Professor of
Medicine at Harvard Medical School and Director of the Program in Epidemiology and
Outcomes Research at the Harvard Medical School's Division of AIDS, and Director of the
HIV Research Program in the Division of General Medicine at Massachusetts General
Hospital for his review and suggestions for the manuscript.
Contributorship statement: JS and KV designed, implemented the study, analysed data
and prepared the manuscript, GR, MU, SS, SD, CN analysed data and prepared the
manuscript.
Data sharing statement: No extra data is available.
Competing interests: None.
Page 12 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 13 of 15
References:
1. UNAIDS. Global plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive. 2011-2015. Accessed online at http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2011/20110609_jc2137_global-pla.
2. Mofenson LM. Successes and challenges in the perinatal HIV-1 epidemic in the United States as illustrated by the HIV-1 Serosurvey of childbearing women. Arch Pediatr Adolesc Med [Internet]. 2004 May [cited 2013 Jul 21];158(5):422–5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15123471
3. Mother-to-child transmission of HIV infection in the era of highly active antiretroviral therapy. European Collaborative Study. Clin Infect Dis [Internet]. 2005 Feb 1 [cited 2013 Jul 21];40(3):458–65. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15668871
4. India PMTCT Factsheet: UNICEF, accessed online at http://www.unicef.org/aids/files/IndiaFactsheet_PMTCTFactsheet_2010.pdf on 5th October 2013.
5. Factsheets on the status of national PMTCT responses in the most affected countries. The Interagency Task Team on the Prevention and Treatment of HIV Infection in Pregnant Women, Mothers and Children. [Internet]. [cited 2013 Aug 25]. Available from: http://www.emtct-iatt.org/countries/india/
6. NACO. Annual CMIS Bulletin 2008-09. NACO. Department of AIDS Control, Ministry of Health and Family Welfare, Govt of India. Accessed online at http://aidsdatahub.org/dmdocuments/NACO_Annual_CMIS_BULLETIN_2008-09.pdf on 5th October 2013.
7. National AIDS Control Organisation M of H& FWG of I. Antiretroviral Therapy Guidelines for HIV-Infected Adults and Adolescents Including Post-exposure Prophylaxis.
8. Garcia PM, Kalish LA, Pitt J, Minkoff H, Quinn TC, Burchett SK, et al. Maternal levels of plasma human immunodeficiency virus type 1 RNA and the risk of perinatal transmission. Women and Infants Transmission Study Group. N Engl J Med [Internet]. 1999 Aug 5 [cited 2013 Sep 6];341(6):394–402. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10432324
9. Lindbäck S, Karlsson AC, Mittler J, Blaxhult A, Carlsson M, Briheim G, et al. Viral dynamics in primary HIV-1 infection. Karolinska Institutet Primary HIV Infection Study Group. AIDS [Internet]. 2000 Oct 20 [cited 2013 Sep 6];14(15):2283–91. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11089616
10. Dunn DT, Newell ML, Ades AE, Peckham CS. Risk of human immunodeficiency virus type 1 transmission through breastfeeding. Lancet [Internet]. 1992 Sep 5 [cited 2013 Sep 6];340(8819):585–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/1355163
Page 13 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 14 of 15
11. Gray RH, Li X, Kigozi G, Serwadda D, Brahmbhatt H, Wabwire-Mangen F, et al. Increased risk of incident HIV during pregnancy in Rakai, Uganda: a prospective study. Lancet [Internet]. 2005 Oct 1 [cited 2013 Sep 6];366(9492):1182–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16198767
12. Cao Y, Krogstad P, Korber BT, Koup RA, Muldoon M, Macken C, et al. Maternal HIV-1 viral load and vertical transmission of infection: the Ariel Project for the prevention of HIV transmission from mother to infant. Nat Med [Internet]. 1997 May [cited 2013 Sep 6];3(5):549–52. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9142125
13. Branson BM, Handsfield HH, Lampe MA, Janssen RS, Taylor AW, Lyss SB, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep [Internet]. 2006 Sep 22 [cited 2013 Jul 21];55(RR-14):1–17; quiz CE1–4. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16988643
14. Dandona L, Kumar SP, Ramesh Y, Rao MC, Kumar AA, Marseille E, et al. Changing cost of HIV interventions in the context of scaling-up in India. AIDS [Internet]. 2008 Jul [cited 2014 Apr 17];22 Suppl 1:S43–9. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3688470&tool=pmcentrez&rendertype=abstract
15. Venkatesh KK, Becker JE, Kumarasamy N, Nakamura YM, Mayer KH, Losina E, et al. Clinical impact and cost-effectiveness of expanded voluntary HIV testing in India. PLoS One [Internet]. 2013 Jan [cited 2014 Apr 17];8(5):e64604. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3669338&tool=pmcentrez&rendertype=abstract
16. Aledort JE, Ronald A, Le Blancq SM, Ridzon R, Landay A, Rafael ME, Shea MV, Safrit J, Peeling RW, Hellmann N, Mwaba P, Holmes K WC. Reducing the burden of HIV/AIDS in infants: the contribution of improved diagnostics. Nature 2006 Nov 23;444 Suppl 119-28.
17. WHO. Global Health Observatory (GHO). Country Statistics (India). [Internet]. World Health Organization; Available from: http://www.who.int/gho/countries/ind/en/
18. WHO. Use of antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. World Health Organization; [cited 2014 Apr 17]; Available from: http://www.who.int/hiv/pub/mtct/programmatic_update2012/en/
19. Soorapanth S, Sansom S, Bulterys M, Besser M, Theron G, Fowler MG. Cost-effectiveness of HIV rescreening during late pregnancy to prevent mother-to-child HIV transmission in South Africa and other resource-limited settings. J Acquir Immune Defic Syndr [Internet]. 2006 Jun [cited 2013 Oct 6];42(2):213–21. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16639346
20. Sanders GD, Bayoumi AM, Sundaram V, Bilir SP, Neukermans CP, Rydzak CE, et al. Cost-effectiveness of screening for HIV in the era of highly active antiretroviral therapy. N Engl J Med [Internet]. 2005 Feb 10 [cited 2014 Mar 24];352(6):570–85. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15703422
21. National AIDS Control Organisation. Annual Report 2012-13. Department of AIDS Control. Ministry of Health and Family Welfare. [Internet]. [cited 2014 Apr 18]. Available from:
Page 14 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 15 of 15
http://www.naco.gov.in/NACO/Quick_Links/Publication/Annual_Report/NACO_Annual_Report/Annual_Report_2012-13/
22. Gupte N, Sastry J, Brookmeyer R, Phadke MA, Bhosale RA, Bollinger RC. Declining HIV infection rates among recently married primigravid women in Pune, India. J Acquir Immune Defic Syndr [Internet]. 2007 Aug 15 [cited 2013 Oct 6];45(5):570–3. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17577126
23. Gangakhedkar RR, Bentley ME, Divekar AD, Gadkari D, Mehendale SM, Shepherd ME, et al. Spread of HIV infection in married monogamous women in India. JAMA [Internet]. 1997 Dec 17 [cited 2014 Mar 2];278(23):2090–2. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9403424
24. PMTCT Guidelines 2013 | Health Systems Trust. The South African Antiretroviral Treatment Guidelines 2013. PMTCT Guidelines: Revised March 2013. [Internet]. [cited 2014 Apr 18]. Available from: http://www.hst.org.za/publications/pmtct-guidelines-2013
25. Newell M-L, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet [Internet]. [cited 2014 Apr 17];364(9441):1236–43. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15464184
Page 15 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Table 1: Input parameters for decision analysis model
Variable [Reference] Comment
Life expectancy in years Life expectancy of a healthy baby(17)
65
Life expectancy of an HIV positive baby with ART(16)
30
Life expectancy of an HIV positive baby without ART(25)
2
Probabilities
Probability of HIV incidence rate in pregnant women
0.0012 (95% CI 0.00032-0.00297)
Based on new HIV infections detected during second HIV test in our study
Probability of receiving ART to women detected with HIV in the second test
0.5 (95% CI 0.33-0.964)
Based on our study findings
Probability of breast feeding 1 Based on our study findings Cost (USD, 1 USD = INR 50) Cost of first HIV test(14), (15) USD 3.33
Cost of 2nd HIV test USD 0.6 (actual cost that was paid per test for the study)
Cost of ART for PMTCT(18) USD 178.75
Cost of HIV testing (HIV PCR) USD 16.0
Based on cost to Prayas’s EGPAF’s PMTCT programme
Cost of ART for HIV-infected baby(18)
USD 194.0
Quality Adjusted Life Years (QALY)
QALY of HIV un-infected baby(19),(20) 1 QALY of HIV-infected baby on ART(19), (20) 0.83 QALY of HIV positive baby without ART(19), (20) 0.73 QALY gained QALY gained* for healthy baby (HIV uninfected/ HIV negative baby)(17)
65
QALY gained for HIV positive baby on ART(20)
24.9
QALY gained for HIV positive baby without ART(20)
1.46
*QALY gained = QALY*Life expectancy
Page 16 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Table 2: Baseline HIV prevalence, enrollments at rural and urban sites and HIV
incidence in pregnant women
Rural sites Urban sites
No. of women tested for 1st HIV test 4803 13109
No detected with HIV in first HIV test 20 60
Baseline HIV prevalence (1st HIV test) 0.42 0.46
No of women enrolled for 2nd HIV test 2229 6868
No of women detected with HIV in the 2nd HIV tests 2 2
HIV incidence rate per 1000 Persons Women Years (PWY)
2.3 (95% CI 0.62-5.81)
0.8 (95% CI 0.21-2.0)
Overall HIV incidence-1000 PWY 1.2 (95% CI 0.32-2.97)
Page 17 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Table 3: One-way sensitivity analysis of cost and effectiveness of current strategy (of
single HIV test) and proposed strategy (of addition of 2nd HIV test during pregnancy)
HIV incidence Strategy Cost ( C)
Effect (E) QALY gained
C/E (USD per QALY gained)
Incr C/E (ICER)
0.0001 Proposed $4.00 64.9987 0.06158 Cost saving
Current $55.83 39.09 1.42824
0.005 Proposed $4.62 64.93406 0.07114 Cost saving
Current $55.83 39.09 1.42824
0.010 Proposed $5.24 64.86941 0.08072 Cost saving
Current $55.83 39.09 1.42824
0.015 Proposed $5.85 64.80477 0.09032 Cost saving
Current $55.83 39.09 1.42824
0.020 Proposed $6.47 64.74012 0.09994 Cost saving
Current $55.83 39.09 1.42824
0.025 Proposed $7.09 64.67548 0.10957 Cost saving
Current $55.83 39.09 1.42824
0.030 Proposed $7.70 64.61083 0.11923 Cost saving
Current $55.83 39.09 1.42824
0.035 Proposed $8.32 64.54619 0.12891 Cost saving
Current $55.83 39.09 1.42824
0.040 Proposed $8.94 64.48154 0.13861 Cost saving
Current $55.83 39.09 1.42824
0.045 Proposed $9.55 64.4169 0.14832 Cost saving
Current $55.83 39.09 1.42824
0.050 Proposed $10.17 64.35225 0.15806 Cost saving
Current $55.83 39.09 1.42824
Proposed strategy: Second (repeat) HIV test in late pregnancy
Current strategy: Second HIV test not offered
Incr Cost = Cost of proposed strategy – cost of current strategy
Incr Eff = Effect of proposed strategy – effect of current strategy
���� =(����� ����� ���� − ������ �� ����)
(�������� ����� ���� − ��������� �� ����)
Page 18 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 19 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Figure 1: Decision analysis model
Page 20 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on December 14, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006718 on 11 June 2015. Downloaded from

For peer review only
Figure 2: One-way sensitivity analysis of cost effectiveness ratio of current strategy
(of single HIV test) and proposed strategy (of additional second HIV test during
pregnancy)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
0.000 0.005 0.010 0.015 0.020 0.025 0.030 0.035 0.040 0.045 0.050
Cost/effectiveness ratio (CER)
HIV incidence
Proposed Strategy Current Strategy
Page 21 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 22 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on
Dec
embe
r 14
, 202
0 by
gue
st. P
rote
cted
by
copy
right
.ht
tp://
bmjo
pen.
bmj.c
om/
BM
J O
pen:
firs
t pub
lishe
d as
10.
1136
/bm
jope
n-20
14-0
0671
8 on
11
June
201
5. D
ownl
oade
d fr
om

For peer review only
Page 23 of 23
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on
Dec
embe
r 14
, 202
0 by
gue
st. P
rote
cted
by
copy
right
.ht
tp://
bmjo
pen.
bmj.c
om/
BM
J O
pen:
firs
t pub
lishe
d as
10.
1136
/bm
jope
n-20
14-0
0671
8 on
11
June
201
5. D
ownl
oade
d fr
om

For peer review only
Cost-effectiveness of a repeat HIV test in pregnancy in India
Journal: BMJ Open
Manuscript ID: bmjopen-2014-006718.R1
Article Type: Research
Date Submitted by the Author: 05-Mar-2015
Complete List of Authors: Joshi, Smita; Hirabai Cowasji Jehangir Medical Research Institute, Preventive Oncology Kulkarni, Vinay; Prayas, Gangakhedkar, Raman; National AIDS Research Institute, Mahajan, Uma; Hirabai Cowasji Jehangir Medical Research Institute, Shamra, Sushama; MIMER, Shirole, Devendra; Kamala Nehru Hospital, Chandhiok, Nomita; Indian Council of Medical Research,
<b>Primary Subject Heading</b>:
HIV/AIDS
Secondary Subject Heading: Epidemiology, HIV/AIDS, Obstetrics and gynaecology
Keywords: EPIDEMIOLOGY, HIV & AIDS < INFECTIOUS DISEASES, Public health < INFECTIOUS DISEASES
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on D
ecember 14, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006718 on 11 June 2015. D
ownloaded from

For peer review only
Page 1 of 18
Cost-effectiveness of a repeat HIV test in pregnancy in India
Joshi Smita1, Kulkarni Vinay2, Gangakhedkar Raman3, Mahajan Uma1, Sharma Sushma4,
Shirole Devendra5, Chandhiok Nomita6
1Hirabai Cowasji Jehangir Medical Research Institute (HCJMRI), Jehangir Hospital Premises,
32, Sasoon Road, Pune 411 001, Maharashtra, India. E-Mail: [email protected]
2 Prayas Health Group, Amrita Clinic, Athwale Corner, Karve Road, Deccan Gymkhana,
Pune 411 004, India. E-Mail: [email protected]
3National AIDS Research Institute, 73, G Block, MIDS, Bhosari, Pune-411026, India.
Email: [email protected]
4 MIMER Hospital, Talegaon, Pune. Email: [email protected]
5Kamla Nehru Hospital and Pune Municipal Corporation, Pune, India (added posthumously)
6 Indian Council of Medical Research, New Delhi, India. E-mail: [email protected]
Address for correspondence:
Dr Smita Joshi
Hirabai Cowasji Jehangir Medical Research Institute, Jehangir Hospital Premises, 32
Sassoon Road, Pune-411001
Email: [email protected], Phone no: +91-9881132506
Key words: HIV, PMTCT, cost-effectiveness, HIV prevention
Word count: 2754
Page 1 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 2 of 18
Abstract:
Objective: To evaluate cost-effectiveness of second HIV test in pregnancy.
Background: Current strategy of single HIV test during pregnancy in India can miss new
HIV infections acquired after the first test or those HIV infections that were missed in the first
test due to a false negative HIV test.
Methods: Between August 2011 and April 2013, 9097 pregnant HIV un-infected women
were offered a 2nd HIV test near term (34 weeks or beyond) or within 4 weeks of post-partum
period. A decision analysis model was used to evaluate cost-effectiveness of 2nd HIV test in
pregnant women near term.
Primary and secondary outcome:
Our key outcome measures include program cost with addition of 2nd HIV test in pregnant
women and quality-adjusted life years (QALYs) gained.
Results: We detected 4 new HIV infections in the second test. Thus HIV incidence among
pregnant women was 0.12 (95% 0.032-0.297) per 100 person women years (PWY). Current
strategy of a single HIV test is 8.2 times costlier for less QALYs gained as compared to
proposed repeat HIV testing of pregnant women who test negative during the first test.
Conclusions: Our results warrant consideration at the national level for including second
HIV test of all pregnant women in the national programme. However prior to allocation of
resources for 2nd HIV test in pregnancy, appropriate strategies will have to be planned for
improving compliance for prevention of MTCT of HIV and reducing loss-to-follow-up of those
women detected with HIV.
Key Words
HIV, PMTCT, cost-effectiveness, 2nd HIV test in pregnancy
Page 2 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 3 of 18
Strengths and limitations of this study:
• Of all the biological interventions to prevent HIV transmission, PMTCT of HIV is the
most efficacious intervention.
• Our proposed strategy of repeat HIV test in pregnancy near term is cost-effective and
strengths of our study include large sample size and demonstration of low HIV
incidence in pregnant women.
• Current strategy of a single HIV test results in 8.2 times more cost for less QALYs
gained. Our proposed strategy of repeat HIV testing of pregnant women who test
negative in the first test offers 1 healthy child with USD 6.8.
• The limitations of the study include low HIV incidence and loss-to-follow up.
Therefore prior to allocation of resources for 2nd HIV test in pregnancy, appropriate
strategies will have to be planned for minimizing such loss-to-follow-up.
Page 3 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 4 of 18
Introduction:
Mother-to-child transmission of HIV (MTCT) remains the most significant route of HIV
infection among children in the developing countries. At the same time, of all the biological
interventions to prevent HIV transmission, prevention of MTCT of HIV is the most efficacious
intervention. The global plan towards elimination of new HIV infections among children has
reported 38% decrease in new HIV infections among children(1). In the developed regions of
the world, MTCT transmission rates are as low as 2% due to wide coverage and provision of
highly effective anti-retroviral treatment (ART) regimen(2,3). Eliminating pediatric HIV
infection appears to be the most achievable goal globally.
In India, Prevention of Parent to Child Transmission of HIV/AIDS (PPTCT)
programme was initiated in 2002. Since then, there has been sustained scale up of PPTCT
programme in the country. Total annual births in 2009 in India were 26,787,000(4) and the
Interagency Task Team of UNICEF on the prevention and treatment of HIV infection in
pregnant women, mothers and children estimated that of these 27 million annual
pregnancies, 22,000 to 61,000 occurred in HIV positive pregnant women(5). It is estimated
by National AIDS Control Organization (NACO) that 5.4% of the new HIV infections in India
are due to transmission of infection from parent to child(6). The PPTCT program of NACO
offers routine HIV testing to all pregnant mothers. As per the current protocol, women are
tested for HIV only once during pregnancy(7). Therefore, pregnant women who are in the
window period at the time of the first HIV test or those who acquire HIV after the first test do
not receive interventions to prevent transmission of HIV to the baby. Acute HIV infection is
associated with very high levels of HIV-1 RNA(8,9) thus acute maternal HIV-1 infection
during pregnancy and breast-feeding is associated with higher rates of mother-to-child
transmission (MTCT) of HIV-1(10–12). The aim of eliminating MTCT of HIV will be
accomplished only if appropriate strategies to prevent transmission are applied at each step.
The Centre for Disease Control (CDC), USA has recommended repeat HIV testing in the
third trimester for all women in jurisdictions with elevated HIV incidence and for women
Page 4 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 5 of 18
receiving health care in facilities with at least one diagnosed HIV case per 1,000 pregnant
women per year(13).
Second HIV testing of pregnant women is not yet implemented in India. In addition to
the already declining HIV epidemic and other competing health priorities, we are at the cross
roads of carefully allocating available resources for HIV prevention efforts. In order to include
second HIV test of pregnant women in the national programme to achieve the goal of
elimination of MTCT; a cost-effectiveness analysis of the intervention can help policy makers
in taking an appropriate decision for implementation of the intervention. Therefore we
conducted a study to evaluate cost-effectiveness of an additional HIV test among pregnant
women attending antenatal clinics in Pune, Maharashtra.
Methods:
The study was approved by the Ethics Committee of Hirabai Cowasji Jehangir Medical
Research Institute (HCJMRI) and Jehangir Clinical Development Centre (JCDC). The study
was conducted at 2 Primary Health Centres (Kamshet and Talegaon in Maval Tehsil) and 3
urban sites (Maharashtra Institute of Medical Education and Research, Kamla Nehru
Hospital and Sane Guruji Hospital).
The study was conducted between August 2011 and April 2013. Study staff was
hired and trained prior to study initiation. Monthly data regarding number of pregnant
women tested for HIV (1st HIV test as per national guidelines) and number detected with HIV
(baseline HIV prevalence in pregnant women) were collected from the NACO ART centre at
these sites.
Potential study participants were identified based on their antenatal chart review.
Women in the late third trimester of pregnancy (beyond 34 weeks of pregnancy) with a
documented HIV negative test report at least 3 months prior to the visit, willing to sign a
written informed consent form and willing to undergo a repeat HIV test were consented and
offered a second HIV test. Written informed consent included possibility of a telephonic call
or a home visit if they were confirmed to be HIV-infected so that PPTCT services could be
Page 5 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 6 of 18
offered. After signing the informed consent form, data were collected on a structured
questionnaire regarding age, education, religion, marital status, occupation of both partners,
age at first sexual contact, husband’s risk for HIV infection, history of any risk after the initial
HIV test (history of blood transfusion, tattoo, ear/nose piercing, injections) and obstetrical
history. A rapid HIV test was performed on whole blood sample collected by a finger prick
on site. Post-test counseling was done and HIV test report was given to the woman
immediately. As per the national protocol, women were also counseled to encourage their
partners to get tested for HIV and to opt for an institutional delivery.
If the HIV test report was positive in the rapid HIV test, a second venous sample was
immediately collected for confirmation of HIV infection and women were called after one week
for the test report. Women who were detected with HIV infection, were referred appropriately
for PPTCT interventions. Recently delivered women who could not be tested for 2nd HIV test
prior to delivery (for e.g. those who delivered on admission) but had a documented negative
HIV test report at least 3 months prior to delivery were also invited to participate in the study
and were tested within 4 weeks of delivery so that it could not be attributed to HIV acquisition
after delivery.
Data analysis:
Data were collected on a structured questionnaire. Data entry was done in MS Access 2007
software and analyzed using STATA 12.0 software. Standard formulae were used to
calculate 95% confidence interval (CI). TreeAge software was used for cost-effectiveness
and sensitivity analysis. The indicator of cost-effectiveness was program cost with addition
of 2nd HIV test in pregnant women and quality-adjusted life years (QALYs) gained. A
decision analysis model was created to compare 2 strategies (Figure 1): 1) current strategy
of a single HIV test during pregnancy that is implemented by NACO, and 2) proposed
strategy with addition of 2nd HIV test of pregnant women after 34 weeks of pregnancy or
within 4 weeks after delivery who were tested HIV negative in the first test (in addition to
current strategy of single HIV test). The model was created for 9097 women enrolled in the
study to compare proposed strategy with the current strategy. The model included 4 women
Page 6 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 7 of 18
who were HIV negative in the first test at baseline but were detected with HIV infection after
three months in the second test and had an opportunity to prevent MTCT with the use of
ART. We also compared HIV status of their babies and life expectancy of the HIV infected
baby with and without ART. Baseline values for input parameters for decision analysis
model are given in Table 1. The programme costs included personnel, infrastructure,
recurrent costs, cost of ART for PPTCT to women detected with HIV and treatment of HIV
infected baby. For the current strategy, USD 3.33 was included as the cost of 1st HIV test
(14), (15). For the proposed strategy the cost of 1st HIV test as well as 2nd HIV test (USD
3.33 each) was included in the model (Figure 1). The cost of 2nd HIV test for the programme
is likely to be less than USD 3.33 as the infrastructure already exists however for
convenience, we have considered USD 3.33 for 2nd test also to account for personnel time
and cost. The probabilities of new HIV infections, ART for mother and HIV status of the baby
at the end of 18 months obtained from this study were used for decision analysis. We have
assumed that life expectancy of an HIV-infected child in India on ART would be at least 50%
of the normal life expectancy(16) and since the life expectancy of a healthy baby in India is
65 years(17), for convenience we rounded off the life expectancy to 30 years. Thus we
included cost of ART for an HIV infected child(18) for 30 years after birth. We assigned a
QALY (quality adjusted life years) weight of 1 for a healthy child (HIV-negative), 0.83 for HIV
infected child with ART, and 0.73 for the one without ART(19),(20). The outcome in terms of
QALY, costs and probability were entered into the TreeAge software for cost-effectiveness
and sensitivity analysis. We performed one-way sensitivity analysis to determine the effect of
HIV incidence on the cost-effectiveness of the programme.
Results:
We enrolled consecutive 9164 eligible women in this study of whom 67 were excluded from
final analysis due to inadequate data and thus 9097 women were included in the final
analysis. Of these 9079 women, 2229 and 6868 women were enrolled at rural and urban
sites respectively. Majority of the enrolled participants (69.4%) were less than 25 years of
Page 7 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 8 of 18
age, 94.5% had some education and 79% of the participants were Hindu. None of them
declined a second HIV test. About 90% of them were housewives and 99.4% were living
with a husband who was earning. About 45.4% were primigravida and 99.9% were not
infected with HIV in the second HIV test. Table 2 provides enrollments at rural and urban
sites, baseline HIV prevalence and HIV incidence in pregnant women. Baseline HIV
prevalence in pregnant women (HIV prevalence in pregnant women during the first HIV test)
at rural sites was 0.42 and at urban sites it was 0.46 and the difference was not statistically
significant [data not shown]. The overall HIV prevalence at baseline in pregnant women was
0.45%.
We detected 4 new HIV infections among pregnant women and thus HIV incidence
among pregnant women was 1.2 per 1000 PWY (95% CI 0.32-2.97). Two women each
were detected with new HIV infection in the second test at the rural and urban sites. HIV
incidence at the urban sites was 0.8 (95% CI 0.0.21-2.0) per 1000 Person Women Years
(PWY) and it was 2.3 (95% 0.62-5.81) per 1000 PWY at rural sites. HIV incidence at the
rural sites was higher than that of urban women sites but the difference was not statistically
significant.
Of the 9097 women included in the final analysis, 4 women were detected with HIV
infection in the 2nd HIV test as stated above. Their partners were also tested for HIV and all 4
were detected to be HIV-infected. However, none of them were aware of their HIV status. All
these 4 women were primigravida and their mean age was 27.25 (range 20-35 years). Of
these 4 women, 1 woman refused to accept the test result and absconded. One woman
defaulted on treatment for PPTCT and her baby was found to be infected with HIV at 12
months of follow- up. Two women completed ART for PPTCT and their babies remained HIV
negative at 18 months. These transmission probabilities and above mentioned costs were
used in the TreeAge software. On rollback, the cost of proposed strategy i.e. addition of 2nd
HIV test in late pregnancy was USD 6.8 per 64.98 QALYs gained (equivalent to one healthy
life of an HIV un-infected child) whereas the current strategy of single HIV test during
Page 8 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 9 of 18
pregnancy requires USD 55.83 per 39.09 QALYs gained. Thus the currently administered
national strategy spends 8.2 times more USD for less QALYs gained.
Sensitivity analysis: One-way sensitivity analysis was done to determine the changes in
cost-effectiveness with different probabilities of HIV incidence and it is presented in
Table 3. Our HIV incidence was 0.12 per 100 PWY and with different probabilities of HIV
incidence ranging from 0.01 per 100 PWY to 5.0 per 100 PWY, proposed strategy remained
cost-effective with less USD spent and more QALYs gained.
Discussion:
Our study provides an important lead to strengthen NACO’s programme for PPTCT.
Addition of 2nd HIV test near term for pregnant women who had tested HIV negative in the
first HIV test in pregnancy was found to be cost-effective. To our knowledge this is the first
study in India that has evaluated cost-effectiveness of 2nd HIV test among pregnant women.
Current strategy of a single HIV test results in 8.2 times more cost for less QALYs gained as
compared to proposed repeat HIV testing of pregnant women. Our proposed strategy offers
1 healthy child at USD 6.8. Our proposed strategy is cost-effective only with addition of the
cost of 2nd HIV test and without addition of incidental benefits of early HIV diagnosis of young
women and their partners. With current programme guidelines of offering lifelong ART to all
pregnant and lactating mothers irrespective of CD4 counts, this becomes even more
beneficial. It is also worth noting that we detected one woman with HIV infection on the
second day of her delivery. Thus repeat HIV testing should be offered to women in the
immediate post-partum period if the second test was not done prior to delivery or if they were
never tested before.
During 2012, about 5.71 million pregnant women were tested for HIV in India. The
overall HIV prevalence in India amongst them was 0.17% while in Maharashtra it was
0.23%(21). We observed higher prevalence of HIV (0.45%) in pregnant women at our study
sites. A wide variation of HIV prevalence among antenatal women has been reported across
Page 9 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 10 of 18
different states in India with lowest HIV prevalence of 0.02% in Arunachal Pradesh, Jammu
and Kashmir and highest prevalence of 0.84% in Nagaland.
Similarly, HIV incidence among pregnant women is likely to vary across different
states/ sites within India. Our study indicates that repeat HIV testing is cost-effective even
with very low HIV incidence (<0.0001) and this strategy can be implemented and would be
beneficial for all the states in India.
Although we could not ascertain whether all 4 new HIV infections were acquired after
the first test (since we did not perform detuned ELISA on the samples) and it is possible that
the first HIV test during pregnancy was a false negative test. Considering our HIV incidence
of 1.2 per 1000 PWY, a substantial number of new HIV infected pregnant women could be
detected with the proposed strategy of 2nd HIV test and this opportunity for PMTCT should
not be missed if India wishes to achieve the goal of zero new HIV infection.
An important finding of this study is the low incidence of HIV in pregnant women
which supports other studies in demonstrating a decline in the HIV epidemic in India.
Decline in adult HIV prevalence and new HIV infections are sustained in most of the states in
India including all the high prevalence states of South India and North East except for some
low prevalence states(22). A report from Pune region has reported decline in HIV incidence
in young pregnant women and the estimated HIV incidence decreased from 2.2/100 PYs
(95% CI: 1.6 to 3.0) in 2002-2003 to 0.73/100 PYs (95% CI: 0.5 to 1.0) in 2006(23). We have
previously reported 82% decline in HIV prevalence in pregnant women from 2003 to 2008 in
the same region (24). In our study, HIV incidence was 0.12/ 100 PWY and this also supports
decline in new HIV infections among young pregnant women.
In our study, male partners of women newly detected with HIV were encouraged to
get tested for HIV after appropriate pre-test counselling and all 4 male partners were also
found to be HIV infected. They were referred appropriately and this additional benefit of early
diagnosis, referral and linkage to treatment provides additional collateral benefit and addition
to cost-effectiveness of our proposed intervention. Spread of HIV among married
monogamous women from the partners with high-risk behaviour has been previously
Page 10 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 11 of 18
reported(25). It is possible that increased male partner involvement, counseling and testing
of male partners at the time of first test could avert some of the transmissions to women and
consequentially to their children.
The strengths of our study include large sample size, demonstration of incident HIV
infections in pregnant women who were tested HIV negative in the 1st HIV test in pregnancy
and cost-effectiveness of repeat testing for HIV in pregnancy in spite of low incidence of HIV.
This is probably because of substantial reduction in the cost of HIV testing as against to the
cost of life-long ART if infected with HIV. The weaknesses of the study include low HIV
incidence and loss-to-follow up. Although we detected 4 new HIV infections in pregnant
women, only 2 women completed appropriate ART for PMTCT and their babies remained
HIV un-infected at the end of 18 months. Therefore prior to allocation of resources for 2nd
HIV test in pregnancy, appropriate strategies will have to be planned for minimizing such
loss-to-follow-up.
In addition to CDC(13), rescreening of pregnant women in the last trimester has been
recommended by South African government(26). South Africa is a country with very HIV
prevalence as well as HIV incidence. The cost-effectiveness of HIV re-screening during
pregnancy in South Africa was shown to prevent a substantial number of infant HIV
infections and save costs to the health care system(19). Our findings will help NACO in
shaping the national policy for strengthening PMTCT programme.
Page 11 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 12 of 18
Acknowledgements:
This study was funded by the Indian Council of Medical Research (IRIS ID no. 2010-08370).
We thank authorities at the Pune Municipal Corporation, Sane Guruji Hospital, Kamla Nehru
Hospital, Taluka Medical Office, Maval Taluka and The District Health Officer of Pune for
allowing us to conduct this study at various study sites. We thank our staff for their tireless
efforts to complete this large study. We thank Director and other staff of HCJMRI for the
administrative and logistic support. We sincerely thank Dr Kenneth Freedberg, Professor of
Medicine at Harvard Medical School and Director of the Program in Epidemiology and
Outcomes Research at the Harvard Medical School's Division of AIDS, and Director of the
HIV Research Program in the Division of General Medicine at Massachusetts General
Hospital for his review and suggestions for the manuscript.
Contributorship statement: JS and KV designed, implemented the study, analysed data
and prepared the manuscript, GR, MU, SS, SD, CN analysed data and prepared the
manuscript. All authors have approved the final submitted version.
Data sharing statement: No additional data available.
Competing interests: None.
Page 12 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 13 of 18
Figure 1: Decision analysis model showing comparison of cost-effectiveness of proposed
strategy of repeat HIV testing of pregnant women in late pregnancy with the current strategy
of single HIV test
References:
1. UNAIDS. Global plan towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive. 2011-2015. Accessed online at http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2011/20110609_jc2137_global-pla.
2. Mofenson LM. Successes and challenges in the perinatal HIV-1 epidemic in the United States as illustrated by the HIV-1 Serosurvey of childbearing women. Arch Pediatr Adolesc Med [Internet]. 2004 May [cited 2013 Jul 21];158(5):422–5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15123471
3. Mother-to-child transmission of HIV infection in the era of highly active antiretroviral therapy. European Collaborative Study. Clin Infect Dis [Internet]. 2005 Feb 1 [cited 2013 Jul 21];40(3):458–65. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15668871
4. India PMTCT Factsheet: UNICEF, accessed online at http://www.unicef.org/aids/files/IndiaFactsheet_PMTCTFactsheet_2010.pdf on 5th October 2013.
5. Factsheets on the status of national PMTCT responses in the most affected countries. The Interagency Task Team on the Prevention and Treatment of HIV Infection in Pregnant Women, Mothers and Children. [Internet]. [cited 2013 Aug 25]. Available from: http://www.emtct-iatt.org/countries/india/
6. NACO. Annual CMIS Bulletin 2008-09. NACO. Department of AIDS Control, Ministry of Health and Family Welfare, Govt of India. Accessed online at http://aidsdatahub.org/dmdocuments/NACO_Annual_CMIS_BULLETIN_2008-09.pdf on 5th October 2013.
7. National AIDS Control Organisation M of H& FWG of I. Antiretroviral Therapy Guidelines for HIV-Infected Adults and Adolescents Including Post-exposure Prophylaxis.
8. Garcia PM, Kalish LA, Pitt J, Minkoff H, Quinn TC, Burchett SK, et al. Maternal levels of plasma human immunodeficiency virus type 1 RNA and the risk of perinatal transmission. Women and Infants Transmission Study Group. N Engl J Med [Internet]. 1999 Aug 5 [cited 2013 Sep 6];341(6):394–402. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10432324
9. Lindbäck S, Karlsson AC, Mittler J, Blaxhult A, Carlsson M, Briheim G, et al. Viral dynamics in primary HIV-1 infection. Karolinska Institutet Primary HIV Infection Study Group. AIDS [Internet]. 2000 Oct 20 [cited 2013 Sep 6];14(15):2283–91. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11089616
Page 13 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 14 of 18
10. Dunn DT, Newell ML, Ades AE, Peckham CS. Risk of human immunodeficiency virus type 1 transmission through breastfeeding. Lancet [Internet]. 1992 Sep 5 [cited 2013 Sep 6];340(8819):585–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/1355163
11. Gray RH, Li X, Kigozi G, Serwadda D, Brahmbhatt H, Wabwire-Mangen F, et al. Increased risk of incident HIV during pregnancy in Rakai, Uganda: a prospective study. Lancet [Internet]. 2005 Oct 1 [cited 2013 Sep 6];366(9492):1182–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16198767
12. Cao Y, Krogstad P, Korber BT, Koup RA, Muldoon M, Macken C, et al. Maternal HIV-1 viral load and vertical transmission of infection: the Ariel Project for the prevention of HIV transmission from mother to infant. Nat Med [Internet]. 1997 May [cited 2013 Sep 6];3(5):549–52. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9142125
13. Branson BM, Handsfield HH, Lampe MA, Janssen RS, Taylor AW, Lyss SB, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep [Internet]. 2006 Sep 22 [cited 2013 Jul 21];55(RR-14):1–17; quiz CE1–4. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16988643
14. Dandona L, Kumar SP, Ramesh Y, Rao MC, Kumar AA, Marseille E, et al. Changing cost of HIV interventions in the context of scaling-up in India. AIDS [Internet]. 2008 Jul [cited 2014 Apr 17];22 Suppl 1:S43–9. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3688470&tool=pmcentrez&rendertype=abstract
15. Venkatesh KK, Becker JE, Kumarasamy N, Nakamura YM, Mayer KH, Losina E, et al. Clinical impact and cost-effectiveness of expanded voluntary HIV testing in India. PLoS One [Internet]. 2013 Jan [cited 2014 Apr 17];8(5):e64604. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3669338&tool=pmcentrez&rendertype=abstract
16. Aledort JE, Ronald A, Le Blancq SM, Ridzon R, Landay A, Rafael ME, Shea MV, Safrit J, Peeling RW, Hellmann N, Mwaba P, Holmes K WC. Reducing the burden of HIV/AIDS in infants: the contribution of improved diagnostics. Nature 2006 Nov 23;444 Suppl 119-28.
17. WHO. Global Health Observatory (GHO). Country Statistics (India). [Internet]. World Health Organization; Available from: http://www.who.int/gho/countries/ind/en/
18. WHO. Use of antiretroviral drugs for treating pregnant women and preventing HIV infection in infants. World Health Organization; [cited 2014 Apr 17]; Available from: http://www.who.int/hiv/pub/mtct/programmatic_update2012/en/
19. Soorapanth S, Sansom S, Bulterys M, Besser M, Theron G, Fowler MG. Cost-effectiveness of HIV rescreening during late pregnancy to prevent mother-to-child HIV transmission in South Africa and other resource-limited settings. J Acquir Immune Defic Syndr [Internet]. 2006 Jun [cited 2013 Oct 6];42(2):213–21. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16639346
20. Sanders GD, Bayoumi AM, Sundaram V, Bilir SP, Neukermans CP, Rydzak CE, et al. Cost-effectiveness of screening for HIV in the era of highly active antiretroviral
Page 14 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 15 of 18
therapy. N Engl J Med [Internet]. 2005 Feb 10 [cited 2014 Mar 24];352(6):570–85. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15703422
21. National AIDS Control Organisation. Annual Report 2012-13. Department of AIDS Control. Ministry of Health and Family Welfare. [Internet]. [cited 2014 Apr 18]. Available from: http://www.naco.gov.in/NACO/Quick_Links/Publication/Annual_Report/NACO_Annual_Report/Annual_Report_2012-13/
22. 2012. A online at http://www. who. int/gho/map_gallery/en. on 18th D. WHO | Map gallery. World Health Organization; [cited 2012 Dec 18]; Available from: http://www.who.int/gho/map_gallery/en/
23. Gupte N, Sastry J, Brookmeyer R, Phadke MA, Bhosale RA, Bollinger RC. Declining HIV infection rates among recently married primigravid women in Pune, India. J Acquir Immune Defic Syndr [Internet]. 2007 Aug 15 [cited 2013 Oct 6];45(5):570–3. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17577126
24. Kulkarni V, Joshi S, Gupte N, Parchure R, Darak S, Kulkarni S. Declining HIV prevalence among women attending antenatal care in Pune, India. Trans R Soc Trop Med Hyg [Internet]. 2011 Jun [cited 2013 Oct 6];105(6):315–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21550094
25. Gangakhedkar RR, Bentley ME, Divekar AD, Gadkari D, Mehendale SM, Shepherd ME, et al. Spread of HIV infection in married monogamous women in India. JAMA [Internet]. 1997 Dec 17 [cited 2014 Mar 2];278(23):2090–2. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9403424
26. PMTCT Guidelines 2013 | Health Systems Trust. The South African Antiretroviral Treatment Guidelines 2013. PMTCT Guidelines: Revised March 2013. [Internet]. [cited 2014 Apr 18]. Available from: http://www.hst.org.za/publications/pmtct-guidelines-2013
27. Newell M-L, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet [Internet]. Jan [cited 2014 Apr 17];364(9441):1236–43. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15464184
Page 15 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 16 of 18
Table 1: Input parameters for decision analysis model
Variable [Reference] Comment
Life expectancy in years Life expectancy of a healthy baby(17)
65
Life expectancy of an HIV positive baby with ART(16)
30
Life expectancy of an HIV positive baby without ART(27)
2
Probabilities
Probability of HIV incidence rate in pregnant women
0.0012 (95% CI 0.00032-0.00297)
Based on new HIV infections detected during second HIV test in our study
Probability of receiving ART to women detected with HIV in the second test
0.5 (95% CI 0.33-0.964)
Based on our study findings
Probability of breast feeding 1 Based on our study findings Cost (USD, 1 USD = INR 50) Cost of first HIV test(14), (15) USD 3.33
Cost of 2nd HIV test(14), (15) USD 3.33
Cost of ART for PMTCT(18) USD 178.75
Cost of HIV testing (HIV PCR) USD 16.0
Based on cost to Prayas’s EGPAF’s PMTCT programme
Cost of ART for HIV-infected baby(18)
USD 194.0
Quality Adjusted Life Years (QALY)
QALY of HIV un-infected baby(19),(20) 1 QALY of HIV-infected baby on ART(19), (20) 0.83 QALY of HIV positive baby without ART(19), (20) 0.73 QALY gained QALY gained* for healthy baby (HIV uninfected/ HIV negative baby)(17)
65
QALY gained for HIV positive baby on ART(20)
24.9
QALY gained for HIV positive baby without ART(20)
1.46
*QALY gained = QALY*Life expectancy
Page 16 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 17 of 18
Table 2: Baseline HIV prevalence, enrollments at rural and urban sites and HIV
incidence in pregnant women
Rural sites Urban sites
No. of women tested for 1st HIV test 4803 13109
No detected with HIV in first HIV test 20 60
Baseline HIV prevalence (1st HIV test) 0.42 0.46
No of women enrolled for 2nd HIV test 2229 6868
No of women detected with HIV in the 2nd HIV tests 2 2
HIV incidence rate per 1000 Persons Women Years (PWY)
2.3 (95% CI 0.62-5.81)
0.8 (95% CI 0.21-2.0)
Overall HIV incidence-1000 PWY 1.2 (95% CI 0.32-2.97)
Page 17 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 18 of 18
Table 3: One-way sensitivity analysis of cost and effectiveness of current strategy (of
single HIV test) and proposed strategy (of addition of 2nd HIV test during pregnancy)
HIV incidence (PWY) Strategy Cost ( C) Effect (E)
C/E (USD per QALY gained Incr C/E (ICER)
0.0001 Proposed $6.67 65.00 0.10265 Cost saving
Current $55.83 39.09 1.42824
0.005 Proposed $7.29 64.93 0.11226 Cost saving
Current $55.83 39.09 1.42824
0.010 Proposed $7.91 64.87 0.12188 Cost saving
Current $55.83 39.09 1.42824
0.015 Proposed $8.52 64.80 0.13152 Cost saving
Current $55.83 39.09 1.42824
0.020 Proposed $9.14 64.74 0.14118 Cost saving
Current $55.83 39.09 1.42824
0.025 Proposed $9.76 64.68 0.15086 Cost saving
Current $55.83 39.09 1.42824
0.030 Proposed $10.37 64.61 0.16056 Cost saving
Current $55.83 39.09 1.42824
0.035 Proposed $10.99 64.55 0.17027 Cost saving
Current $55.83 39.09 1.42824
0.040 Proposed $11.61 64.48 0.18001 Cost saving
Current $55.83 39.09 1.42824
0.045 Proposed $12.22 64.42 0.18977 Cost saving
Current $55.83 39.09 1.42824
0.05 Proposed $12.84 64.35 0.19955 Cost saving
Current $55.83 39.09 1.42824
Page 18 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Figure 1: Decision analysis model showing comparison of cost-effectiveness of proposed strategy of repeat HIV testing of pregnant women in late pregnancy with the current strategy of single HIV test
88x30mm (300 x 300 DPI)
Page 19 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 14, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006718 on 11 June 2015. Dow
nloaded from

For peer review only
Page 20 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on
Dec
embe
r 14
, 202
0 by
gue
st. P
rote
cted
by
copy
right
.ht
tp://
bmjo
pen.
bmj.c
om/
BM
J O
pen:
firs
t pub
lishe
d as
10.
1136
/bm
jope
n-20
14-0
0671
8 on
11
June
201
5. D
ownl
oade
d fr
om

For peer review only
Page 21 of 21
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on
Dec
embe
r 14
, 202
0 by
gue
st. P
rote
cted
by
copy
right
.ht
tp://
bmjo
pen.
bmj.c
om/
BM
J O
pen:
firs
t pub
lishe
d as
10.
1136
/bm
jope
n-20
14-0
0671
8 on
11
June
201
5. D
ownl
oade
d fr
om