Embed Size (px)
Citation preview
For peer review only
Factors associated to develop anemia among lactating mothers in Ethiopia: A pooled data analysis from two rounds
of demographic and health surveys
Journal: BMJ Open
Manuscript ID: bmjopen-2014-006001
Article Type: Research
Date Submitted by the Author: 29-Jun-2014
Complete List of Authors: Tarekegn, Yihunie; Ethiopian Public Helth Association, Project management Biadgilign, Sibhatu Haile, Demewoz; Madawalabu University,
<b>Primary Subject Heading</b>:
Public health
Secondary Subject Heading: Nutrition and metabolism, Public health, Health policy
Keywords: NUTRITION & DIETETICS, Nutritional support < ONCOLOGY, Anaemia < HAEMATOLOGY
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on F
ebruary 16, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006001 on 14 April 2015. D
ownloaded from
For peer review only
Factors associated to develop anemia among lactating mothers in Ethiopia: A pooled data
analysis from two rounds of demographic and health surveys
Yihunie Lakew1, Sibhatu Biadgilign
2, Demewoz Haile
3*
1 Ethiopian public health association, Addis Ababa, Ethiopia
2 Independent public health consultants, Addis Ababa, Ethiopia
3 Department of Public Health, College of Medicine and Health sciences, Madawalabu
University, Ethiopia
Email address
Yihunie Lakew – [email protected]
Sibhatu Biadgilign- [email protected]
Demewoz Haile–[email protected]
*Corresponding author
Address of corresponding author
Department of Public Health
College of Medicine and Health sciences
Madawalabu University, Ethiopia
Bale Goba , p, box 302
Running title: Factors associated with anemia among lactating mothers in Ethiopia
Key words: Lactating mothers, anemia, Ethiopia,
Word count: 2143
Page 1 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Abstract
Objective: To identify factors associated with anemia among lactating mothers in Ethiopia.
Design: A cross-sectional secondary data analysis pooled from two rounds of the 2005 and 2011
Ethiopian demographic and health survey (EDHS) was used. Multivariable logistic regression
model was applied to determine the factors associated with anemia.
Population: A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047 from EDHS
2011) were included from 11 administrative states of Ethiopia.
Main outcome measures: Lactating mothers considered as anemic if hemoglobin level <12 g/dl
Results: The overall prevalence of anemia among lactating mothers was found to be 22.1%
[95% CI: (21.13-23.03)]. The prevalence in urban settings was 13.7% [95% CI: (11.35-16.05)]
and in rural areas was 23% [95% CI: (22.68-23.32)]. The multivariable statistical model showed
that lactating mothers whose husbands had attended primary and secondary education were,
respectively, 26% [adjusted odds ratio (AOR) = 0.74; 95% CI: (0.60-0.92)] and 34% [AOR=
0.66; 95% CI: (0.44-0.99)] less likely to have anemia as compared to lactating mothers whose
husbands had no education. Family planning use [AOR= 0.71; 95% CI: (0.55-0.92)], antenatal
care attendance [AOR= 0.77; 95% CI: (0.62-0.95)], engaging in work [AOR=0.78; 95% CI:
(0.63-95)] and having normal body mass index between 18.5 to 24.9 kg/m2 [AOR=0.79 (0.63-
0.98)] were found to be protective factors against developing anemia among lactating mothers.
Variables including wealth index, maternal age, maternal education, parity and religion were not
associated with anemia in lactating mothers.
Conclusion: Anemia is highly prevalent among lactating mothers, particularly in rural and
pastoralist Ethiopia. Factors including paternal education, family planning use, body mass index
(BMI), occupational status, and antenatal care attendance were strong predictors of anemia
among lactating mothers. Promoting partner education, improving BMI, scaling up family
planning and antenatal care services are recommended interventions.
Page 2 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
ARTICLE SUMMARY
Strength and Limitations
• The study attempted to identify factors associated with laboratory confirmed anemia at
the national level in lactating mothers which will potentially influence policy actions.
• The study is a secondary data analysis that missed key potential variables such as dietary
factors. Furthermore, the data has small sample size for some regions, which questions
the accuracy of prevalence estimates per region.
Key messages
• Anemia prevalence is a public health problem among lactating mothers in Ethiopia.
• There are regional disparities regarding the prevalence of anemia among lactating
mothers, with the highest rates found in pastoralist regions.
• Husband education, family planning and ANC attendance were protective factors for
developing anemia.
• Overweight and obese lactating mothers were at high risk for developing anemia.
Page 3 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Introduction
Anemia is one of the nutrition problems affecting millions in developing countries, and remains
a major challenge for human health, social and economic development1. Lactating mothers are
one of the vulnerable groups of anemia. During the period of lactation, mothers are susceptible
to anemia due to maternal iron depletion and blood loss during child birth2. Studies have shown
that the concentration of iron in breast milk is independent of maternal iron status and that the
quality of breast milk is maintained at the expense of maternal stores2 3. Postpartum anemia has
been found highest in mothers who were anemic during pregnancy4. Furthermore, lactating
mothers are highly susceptible to iron depletion if they have not had enough energy and nutrient
intake in their diets. Yet the problem of anemia in postnatal women has been relatively neglected
which is far away from previously thoughts5. Lactating mothers enter into the postnatal period
after having iron depleted through the continuum from pregnancy to childbearing 6. A study from
South Africa evidenced that there was a strong relation between iron status and depression,
stress, and cognitive functioning in poor African mothers during the postpartum period7.
In a meta-analysis of observational and intervention trials, Ross and Thomas8, found that
approximately 20% of the maternal mortality seen in sub-Saharan Africa and South Asia was
attributable to anemia that is primarily the result of iron deficiency. Ethiopia is one of the sub-
Saharan Africa countries heavily affected by anemia9.
Anemia testing was included in the two rounds of the Ethiopian demographic and health surveys
(EDHS) 10. The prevalence of anemia among lactating mothers was 29.9% in 2005 and 18.5% in
2011 9, which is considerably higher as compared with other women (23.9% in 2005 and 15% in
2011), and low as compared with pregnant mothers (30.6% in 2005 and 22% in 2011). This
prevalence of anemia in lactating mothers is one of the highest among developing countries.
However, there is a scarcity of evidence for the factors associated with anemia among lactating
mothers in Ethiopia. Therefore, this study aims to identify the factors associated with anemia
among Ethiopian lactating mothers using the pooled data of EDHS 2005 and 2011.
Page 4 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Methods
Data type and study design
This study is an in-depth analysis to identify risk factors for anemia among lactating mothers
based on secondary data of the EDHS 2005 and 2011 datasets. The EDHS was designed to
provide population and health indicators at national (urban and rural) and regional levels and
were conducted within five year intervals. Both the 2005 and 2011 EDHS samples were selected
using a stratified, two-stage cluster design. The detailed methodology is found elsewhere 9 10
.
Data Extraction
Both EDHS 2005 and 2011 data were downloaded from the Measure EDHS website in SPSS
format with permission. After understanding the detailed data coding, further data cleaning and
recoding was completed. A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047
from EDHS 2011) were included in the analysis. Based on published literature, information on a
wide-range of socio-demographic and economic variables, health service related factors and
anemia level indicators were extracted from the datasets that can potentially influence the
existence of anemia.
Measurement
In both rounds of the EDHS, haemoglobin analysis was carried out onsite using a battery-
operated portable HemoCue analyzer for all anemia samples. The raw measured values of
haemoglobin were obtained using the HemoCue instrument and adjusted for altitude and
smoking status9. All the necessary quality control measures were considered.
Data processing and statistical analysis
Both surveys were administered by the Ethiopian Central Statistics Authority (CSA). Data entry
and editing was performed using CSPro software. For this study’s analysis, the 2005 and 2011
EDHS data were pooled to achieve high power for detecting the associated factors and analyzed
using STATA 11 software. Descriptive statistics was used to show the prevalence of anemia
among lactating mothers across the regional states and city administrations of Ethiopia.
Multivariable binary logistic regression statistical analysis was carried out to determine the
Page 5 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
factors associated with anemia among lactating mothers. Both crude and adjusted odds ratios
(OR) were determined with 95% confidence interval (CI). All tests were two-sided, weighted
and a p-value <0.05 was considered statistically significant. Variables found statistically
significant at p-value <0.3 during bivariate analysis were considered for adjustment in the
multivariable logistic regression model.
Ethical statements
The data were downloaded and used after communicating the purpose of the analysis and
receiving permission from Measure DHS Organization. The original EDHS data were collected
in accordance with international and national ethical guidelines.
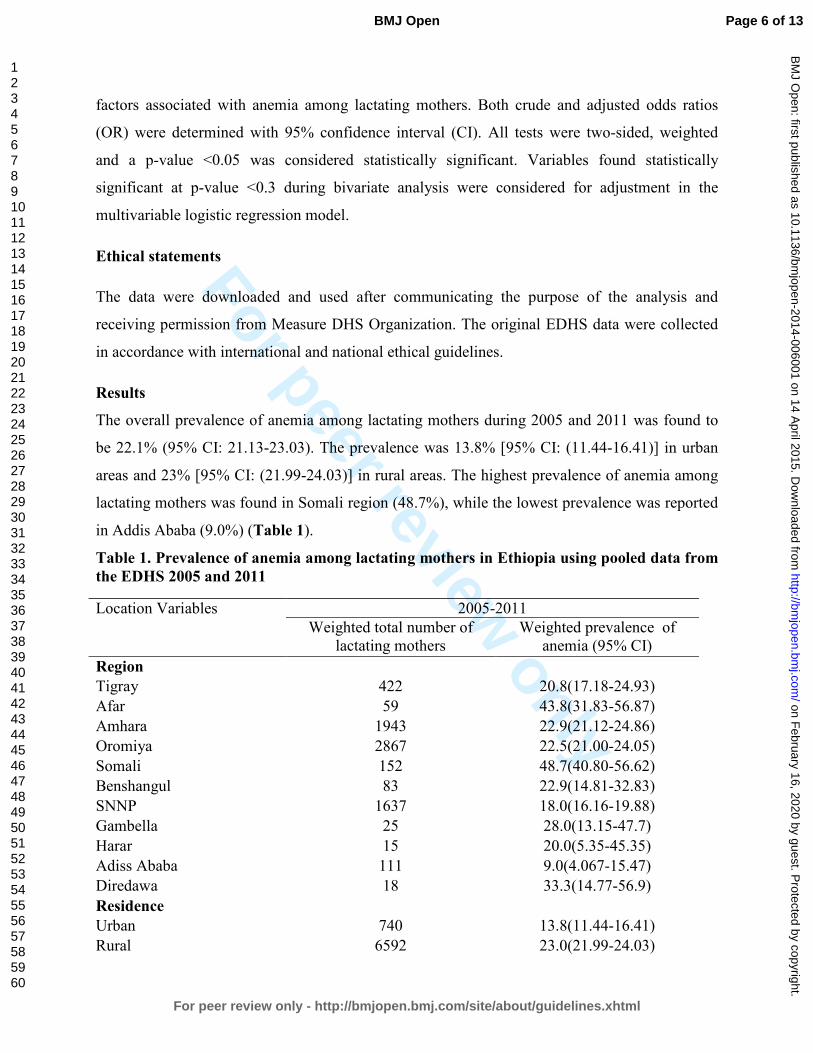
Results
The overall prevalence of anemia among lactating mothers during 2005 and 2011 was found to
be 22.1% (95% CI: 21.13-23.03). The prevalence was 13.8% [95% CI: (11.44-16.41)] in urban
areas and 23% [95% CI: (21.99-24.03)] in rural areas. The highest prevalence of anemia among
lactating mothers was found in Somali region (48.7%), while the lowest prevalence was reported
in Addis Ababa (9.0%) (Table 1).
Table 1. Prevalence of anemia among lactating mothers in Ethiopia using pooled data from
the EDHS 2005 and 2011
Location Variables
2005-2011
Weighted total number of
lactating mothers
Weighted prevalence of
anemia (95% CI)
Region
Tigray 422 20.8(17.18-24.93)
Afar 59 43.8(31.83-56.87)
Amhara 1943 22.9(21.12-24.86)
Oromiya 2867 22.5(21.00-24.05)
Somali 152 48.7(40.80-56.62)
Benshangul 83 22.9(14.81-32.83)
SNNP 1637 18.0(16.16-19.88)
Gambella 25 28.0(13.15-47.7)
Harar 15 20.0(5.35-45.35)
Adiss Ababa 111 9.0(4.067-15.47)
Diredawa 18 33.3(14.77-56.9)
Residence
Urban 740 13.8(11.44-16.41)
Rural 6592 23.0(21.99-24.03)
Page 6 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Total 7332 22.1(21.13-23.03)
In total, 12 variables for anemia were both available from the EDHS and identified as risk factors
based on literature review. Of the twelve, the factors identified as significantly associated with
anemia in the bivariate step were wealth index, place of residence, maternal education, paternal
education, maternal occupation, family planning use, maternal BMI and antenatal care
attendance. However, in the multivariable model, paternal education, maternal occupation,
family planning use, maternal BMI and antenatal care attendance remained the independent
predictors of anemia for Ethiopian lactating mothers.
Paternal educational status was found to be a predictor of anemia among lactating mothers.
Those lactating mothers who had husbands who attended primary education were at 26% lower
risk for having anemia as compared to those mothers who had husbands with no education
[AOR=0.74; 95% CI: (0.60-0.92)]. Those lactating mothers with husbands who had secondary
education had a 34% lower risk of having anemia as compared to those lactating mothers with
husbands who had no education [AOR=0.66; 95% CI: (0.44-0.99)]. Working lactating mothers
had a 22% lower risk for anemia as compared to their counter parts [AOR=0.78; 95% CI: (0.63-
95)]. Having a normal maternal BMI was found protective of anemia [AOR=0.79; 95% CI:
(0.63-0.98)]. However, lactating mothers who had BMI 25kg/m2 had a 80% higher risk of
developing anemia as compared to undernourished (defined as BMI<18.5kg/m2) lactating
mothers[AOR=1.8; 95% CI: (1.02-3.12)](Table 2).
Among maternal health service factors, family planning use and antenatal care (ANC) were the
significant predictors of anemia in lactating mothers. Lactating mothers who ever used family
planning were 29% less likely to have anemia as compared to lactating mothers who never used
family planning [AOR=0.71; 95% CI: (0.55-0.92)]. Lactating mothers who reported ANC
attendance were 23% less likely to develop anemia as compared to their counterparts
[AOR=0.77; 95% CI: (0.62-0.95)] (Table 2).
Page 7 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
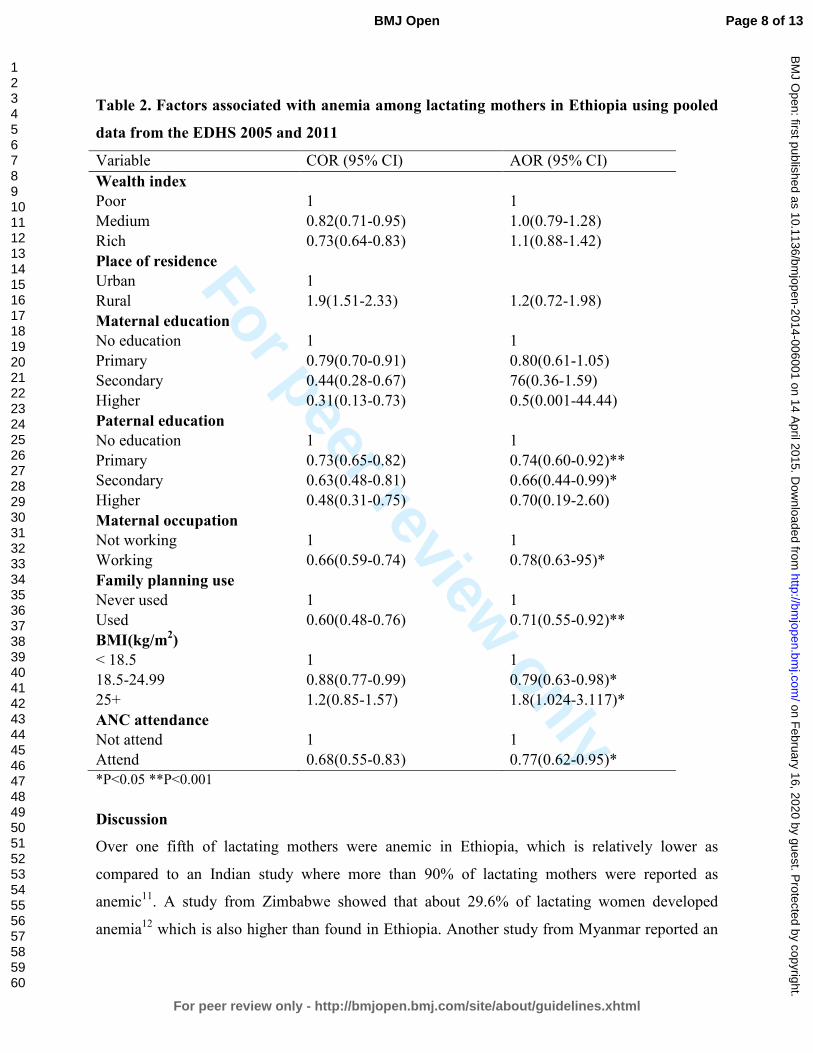
Table 2. Factors associated with anemia among lactating mothers in Ethiopia using pooled
data from the EDHS 2005 and 2011
Variable COR (95% CI) AOR (95% CI)
Wealth index
Poor 1 1
Medium 0.82(0.71-0.95) 1.0(0.79-1.28)
Rich 0.73(0.64-0.83) 1.1(0.88-1.42)
Place of residence
Urban 1
Rural 1.9(1.51-2.33) 1.2(0.72-1.98)
Maternal education
No education 1 1
Primary 0.79(0.70-0.91) 0.80(0.61-1.05)
Secondary 0.44(0.28-0.67) 76(0.36-1.59)
Higher 0.31(0.13-0.73) 0.5(0.001-44.44)
Paternal education
No education 1 1
Primary 0.73(0.65-0.82) 0.74(0.60-0.92)**
Secondary 0.63(0.48-0.81) 0.66(0.44-0.99)*
Higher 0.48(0.31-0.75) 0.70(0.19-2.60)
Maternal occupation
Not working 1 1
Working 0.66(0.59-0.74) 0.78(0.63-95)*
Family planning use
Never used 1 1
Used 0.60(0.48-0.76) 0.71(0.55-0.92)**
BMI(kg/m2)
< 18.5 1 1
18.5-24.99 0.88(0.77-0.99) 0.79(0.63-0.98)*
25+ 1.2(0.85-1.57) 1.8(1.024-3.117)*
ANC attendance
Not attend 1 1
Attend 0.68(0.55-0.83) 0.77(0.62-0.95)*
*P<0.05 **P<0.001
Discussion
Over one fifth of lactating mothers were anemic in Ethiopia, which is relatively lower as
compared to an Indian study where more than 90% of lactating mothers were reported as
anemic11. A study from Zimbabwe showed that about 29.6% of lactating women developed
anemia12 which is also higher than found in Ethiopia. Another study from Myanmar reported an
Page 8 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
anemia prevalence rate of 60.3% in lactating women, with 20.3% of lactating mothers having
severe anemia13. Although the prevalence of anemia among lactating mothers in Ethiopia was
relatively low as compared to the above studies, still it is a moderate public health problem
according to WHO classification14. Anemia during lactation has received less attention in the
Health Extension Program which is practiced in Ethiopia. Even though the health extension
package of Ethiopia has nutrition component, it has no much emphasis on prevention of anemia
among lactating mothers. The EDHS also shows that iron supplementation coverage for pregnant
mothers remained low over time, despite its known contribution for reducing the risk of
postpartum hemorrhage 9. However, the culture of care provided for lactating mothers during the
postpartum period in Ethiopia may contribute to the prevention of anemia.
Although there are common assumptions that pastoralist populations are at a lower risk for
anemia due to their dietary habits and dependence on animal food sources, this study showed that
anemia is a widespread problem in the pastoralist community. The prevalence of anemia in
lactating mothers was highest in pastoralist regions and the decrease in prevalence between 2005
and 2011 EDHS was very small. This might be associated with anemia specifically resulting
from infection, such as malaria which is prevalent in those pastoralist areas.
One of the factors determined to be associated with anemia was paternal education. Having a
husband with a higher level of education was found to be protective for anemia among lactating
mothers. Those mothers having husbands with education of primary and secondary levels were
less likely to develop anemia as compared to those with husbands who had no education.
However, maternal educational status was not statistically associated with anemia, which is
contradictory to many studies from Ethiopia as well as from abroad 13 15-17
. The absence of
association between maternal educational status and anemia versus the associate with husbands’
educational status and anemia among lactating mothers might imply that partner education is
more influential in preventing anemia. This might indicate the importance of involving husbands
in anemia prevention efforts.
Lactating mothers who are working were at lower risk of having anemia as compared to their
counter parts. This might be because working mothers are more empowered as compared to non-
Page 9 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
employed mothers. Therefore, women’s empowerment through economic interventions could
have a positive contribution toward preventing anemia.
As one strategy for preventing anemia, family planning has been used. This study also supports
the importance of family planning for reducing the risk of anemia. Those lactating mothers who
have ever used family planning (modern or traditional) had a lower risk of developing anemia as
compared to those who had never used family planning. This finding is consistent with an
Ethiopian study on the correlates of anemia among reproductive age women by Samson and his
colleague 15.
Maternal nutritional status (measured by body mass index) was found to be significantly
associated with anemia. As compared with undernourished lactating mothers (BMI<18.5kg/m2),
being in the normal BMI category (18.5-24.9kg/m2) was negatively associated with developing
anemia as expected. This finding is similar with others studies18 19
. When a mother is at risk of
deficiency for macronutrients, most likely she is also at risk also other micronutrient deficiencies
such as iron. This study found that overweight and obese lactating mothers were at an 80%
higher risk for having anemia. A study from Mexico found that being overweight did not
necessarily diminish the risk of anemia; rather diet quality was the determiner 19. A study by
Cepeda-Lopez and his colleagues explains lower iron status among obese individuals explained
by lower absorption of iron due to obesity related inflammation which affect regulation of
Hepcidin. Hepcidin levels are higher in obese individuals and are linked to subclinical
inflammation which affect iron absorption negatively 19.
ANC attendance was found to be a protective factor for anemia among lactating mothers. This is
most likely due to the fact that during ANC attendance mothers have been advised to take iron
supplements according to the Ethiopian micronutrient guideline and instructed to consume
different sources of iron rich food items20. Therefore, improving iron status during pregnancy
also helps to prevent anemia during the lactation period.
In many studies of anemia among reproductive age women, the wealth index was found to be a
statistically significant factor 13 15
. However, in this study the wealth index was not found to be a
statistically significant factor.
Conclusion
Page 10 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Anemia is a public health problem among lactating mothers in Ethiopia. There are regional
disparities regarding the prevalence of anemia, with the highest rates found in pastoralist regions.
Factors such as husband’s educational status, family planning use, BMI, maternal occupational
status and ANC attendance were identified as associated factors for anemia among lactating
mothers. Improving BMI, promotion of family planning and ANC are recommended
interventions to prevent anemia. Involvement of males in prevention of anemia should be
considered. Attention should also be given to preventing anemia among lactating mothers
through the Health Extension Package and at any health service delivery contact for lactating
mothers.
Competing interests
The authors declare that they have no competing interests.
Funding statement
This research received no specific grant from any funding agency in the public, commercial or
not-for-profit sectors'
Authors’ contributions
YL and DH conceived the idea. YL analyzed and interpreted the data and critically reviewed the
manuscript. SB assisted in critically reviewing the manuscript. DH drafted the manuscript,
assisted in the data analysis and interpretation and critically reviewed the manuscript. All authors
reviewed and approved the manuscript.
Acknowledgements
The authors acknowledge DHS Measure for granting the data freely. We are also grateful to
thank Lianna Tabar, country representative of KHI-E, for her professional language editing and
reviewing the manuscript.
Data Sharing Statement: No additional data available
References
Page 11 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
1. WHO. The world health report. Reducing risks, promoting healthy life. Geneva, World Health
Organization, 2002., 2002.
2. Whitney E, Rolfes SR. Understanding Nutrition. In: Adams P, editor. Eleventh Edition ed. United States
of America: Thomson Learning Academic Resource Center, 2008.
3. Domell V, Lonnerdal B, Dewey K, Cohen R, Hernell O. Iron zinc and copper concentrations in breast
milk are independent of maternal status. American Journal of clinical nutrition 2004;79(1):111-
15.
4. Bodnar L, Scanlon K, Freedman D, Siega–Riz A, Cogswell M. High prevalence of postpartum anaemia
amongLow income women in the United States. J. obstet. Gynecol 2001;185:4348-53.
5. Bodnar L, Scanlon K, Freedman D, Siega-Riz A, Cogswell M. High prevalence of postpartum anemia
among low-income women in the United States. Am J Obstet Gyneco 2001;185:438–43.
6. SSERUNJOGI L, SCHEUT2 F, WHYTE SR. Postnatal anaemia: neglected problems and missed
opportunities in Uganda. HEALTH POLICY AND PLANNING 2003;18(2):225-31.
7. Beard JL, Hendricks MK, Perez EM, Murray-Kolb LE, Berg A, Vernon-Feagans L, et al. Maternal Iron
Deficiency Anemia Affects Postpartum Emotions and Cognition. Journal of Nutrition
2005;135:267–72.
8. Ross J, homas E. Iron deficiency anemia and maternal mortality. PROFILES 3 working notes series no.
3. Academy for Education Development, Washington D.C., 1996.
9. CentralStatisticalAgency(CSA) EM. Demographic and Health Survey 2011. Addis Ababa, Ethiopia and
Calverton, Maryland, USA: CSA and ORC Macro., 2011.
10. Central Statistical Agency(CSA). Demographic and Health Survey 2005. Addis Ababa, Ethiopia and
Calverton, Maryland, USA: CSA and ORC Macro, 2005.
11. Agarwal KN, Agarwal DK, Sharma A, Sharma K, Prasad K, Kalita MC, et al. Prevalence of anaemia in
pregnant & lactating women in India. Indian J Med Res 2006;124:173-84.
12. Sikosana PL, Bhebhe S, Katuli S. A prevalence survey of iron deficiency and iron deficiency anaemia in
pregnant and lactating women, adult males and pre-school children in Zimbabwe. Cent Afr J
Med 1998;44(12):297-305.
13. Zhao A, Zhang Y, Li B, Wang P, Li J, Xue Y, et al. Prevalence of Anemia and Its Risk Factors Among
Lactating Mothers in Myanmar. Am J Trop Med Hyg 2014;doi: 10.4269/ajtmh.13-0660.
14. WHO. Worldwide prevalence of anaemia 1993-2005 : WHO global database on anaemia / Edited by
Bruno de Benoist, Erin McLean, Ines Egli and Mary Cogswell.
, 2008.
15. Gebremedhin S, Enquselassie F. Correlates of anemia among women of reproductive age in Ethiopia:
Evidence from Ethiopian DHS 2005. Ethiopian Journal of Health Development 2011;25(1):22-30.
16. Haidar J. Prevalence of Anaemia, Deficiencies of Iron and Folic Acid and Their Determinants in
Ethiopian Women. J HEALTH POPUL NUTR 2010;28(4):359-68.
17. Okwu GN. Studies on the predisposing factors of iron deficiency anaemia among lactating women in
Owerri, Nigeria International Research Journal of Biochemistry and Bioinformatics
2011;1(11):304-09.
18. Eckhardt CL, Torheim LE, Monterrubio E, Barquera S, Ruel M. Overweight and Obese Women Remain
at Risk for Anemia in Countries Undergoing the Nutrition Transition. THe FASEB Journal
2006;20:A986-A87.
19. Cepeda-Lopez A, Aeberli I, Zimmermann M. Does obesity increase risk for iron deficiency? A review
of the literature and the potential mechanisms. Int J Vitam Nutr Res 2010;80(4-5):263-70.
20. FMOH. NATIONAL GUIDELINE FOR CONTROL AND PREVENTION OF MICRONUTRIENT DEFICIENCIES,
2004.
Page 12 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Page 13 of 13
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Anemia prevalence and associated factors among lactating mothers in Ethiopia: Evidence from the 2005 and 2011
demographic and health surveys
Journal: BMJ Open
Manuscript ID: bmjopen-2014-006001.R1
Article Type: Research
Date Submitted by the Author: 29-Nov-2014
Complete List of Authors: Tarekegn, Yihunie; Ethiopian Public Helth Association, Project management Biadgilign, Sibhatu; 2 Independent public health consultants, Addis Ababa, Ethiopia,
Haile, Demewoz; Madawalabu University,
<b>Primary Subject Heading</b>:
Public health
Secondary Subject Heading: Nutrition and metabolism, Public health, Health policy
Keywords: Anaemia < HAEMATOLOGY, NUTRITION & DIETETICS, Nutritional support < ONCOLOGY
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on F
ebruary 16, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006001 on 14 April 2015. D
ownloaded from

For peer review only
Anemia prevalence and associated factors among lactating mothers in Ethiopia: Evidence from the
2005 and 2011 demographic and health surveys
Yihunie Lakew1, Sibhatu Biadgilign
2, Demewoz Haile
3*
1 Ethiopian public health association, Addis Ababa, Ethiopia
2 Independent public health consultants, Addis Ababa, Ethiopia
3 Department of Public Health, College of Medicine and Health sciences, Madawalabu
University, Ethiopia
Email address
Yihunie Lakew – [email protected]
Sibhatu Biadgilign- [email protected]
Demewoz Haile–[email protected]
*Corresponding author
Address of corresponding author
Department of Public Health
College of Medicine and Health sciences
Madawalabu University, Ethiopia
Bale Goba , p, box 302
Running title: Factors associated with anemia among lactating mothers in Ethiopia
Key words: Lactating mothers, anemia, Ethiopia,
Word count: 2388
Page 1 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Abstract
Objective: To identify factors associated with anemia among lactating mothers in Ethiopia.
Design: A cross-sectional secondary data analysis pooled from two rounds of the 2005 and 2011
Ethiopian demographic and health survey (EDHS) was used. Multivariable logistic regression
model was applied to determine the factors associated with anemia.
Population: A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047 from EDHS
2011) were included from 11 administrative states of Ethiopia.
Main outcome measures: Lactating mothers considered as anemic if hemoglobin level <12
gram per deciliter.
Results: The overall prevalence of anemia among lactating mothers was found to be 22.1%
[95% CI: (21.13-23.03)]. The highest prevalence was 48.7% [95% CI: (40.80-56.62)] found in
Ethiopian Somali region, followed by 43.8% [95% CI: (31.83-56.87)] in Afar region. The
multivariable statistical model showed that lactating mothers who had husbands who had
attended primary education [AOR=0.79; 95% CI: (0.68-0.91)], who were currently working
[AOR=0.71; 95% CI: (0.63-0.80)], had normal maternal body mass index (BMI) from 18.5kg/m2
to 24.99kg/m2 [AOR=0.78; 95% CI: (0.68-0.89)], were in the middle wealth quintile
[AOR=0.83; 95% CI: (0.71-0.98)] and rich wealth quintile [AOR=0.83; 95% CI: (0.70-0.98)],
reported ever use of family planning [AOR=0.68; 95% CI: (0.57-0.80)], were attending antenatal
care (ANC) for indexed pregnancy four times or more [AOR=0.73; 95% CI: (0.59-0.91)],
experienced time variation between two surveys [AOR=0.73; 95%CI: (0.64-0.85)] and who
breastfed for two years [AOR=0.76; 95% CI: (0.66-0.87)] were found to be associated with
anemia
Conclusion: Anemia is highly prevalent among lactating mothers, particularly among pastoralist
communities of Ethiopian Somali and Afar. Promoting partner education, improving maternal
nutritional status, creating behaviour change among lactating mothers to use family planning and
attend ANC services at health facilities are recommended interventions to reduce the prevalence
of anemia among lactating mothers in Ethiopia..
Page 2 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
ARTICLE SUMMARY
Strength and Limitations
• The study attempted to identify factors associated with laboratory confirmed anemia in
lactating mothers at the national level. The study findings can be used to inform policy
and program actions. Some regions from which data was collected had small sample
size. So that it should be interpreted in caution. .
Key messages
• Anemia prevalence is a public health problem among lactating mothers in Ethiopia, with
the highest prevalence found in pastoralist regions of Ethiopian Somali and Afar
• A statistically significant reduction of anemia prevalence in lactating mothers was
observed from 2005 to 2011.
• Being in middle and rich wealth quintiles, two years of breastfeeding, currently working,
normal body mass index, husbands’ primary education, ever use of family planning and
antenatal care attendance for four or more visits were factors found to be associated with
anemia.
Page 3 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Introduction
Anemia is a serious nutrition problem affecting millions in developing countries, and remains a
major challenge for human health, social and economic development1. Lactating mothers are one
of the vulnerable groups of anemia. During the period of lactation, mothers are susceptible to
anemia due to maternal iron depletion and blood loss during child birth2. Studies have shown that
though breast milk is not a good source of iron, the concentration of iron in breast milk is
independent of maternal iron status. This showed that the quality of breast milk is maintained at
the expense of maternal stores2 3
.
Postpartum anemia has been found highest in mothers who were anemic during pregnancy4.
Furthermore, lactating mothers are highly susceptible to iron depletion if they have not had
enough energy and nutrient intake in their diets.. Lactating mothers begin the postnatal period
after having iron depleted through the continuum from pregnancy to childbearing 5. A study from
South Africa showed that iron status was associated with depression, stress, and cognitive
functioning in poor African mothers during the postpartum period6. In a meta-analysis of
observational and intervention trials, Ross and Thomas, found that approximately 20% of the
maternal mortality seen in sub-Saharan Africa and South Asia was attributable to anemia that
was primarily the result of iron deficiency 7.
Ethiopia is one of the countries in sub-Saharan Africa affected by anemia and it contributes to
high rates of maternal, infant and child mortality globally8 9
. In Ethiopia, the maternal mortality
ratio was 676 maternal deaths per 100,000 live births for the seven-year period preceding the
2011 EDHS survey. This rate is one of the highest in the world. The infant mortality rate was 59
per 1,000 live births and the under-five mortality rate was 88 per 1,000 live births10
.
. Anemia testing was included in the two rounds of the Ethiopian Demographic and Health
Surveys (EDHS)10 11
. The prevalence of anemia in lactating mothers was 29.9% in 2005 and
18.5% in 201110
. It was 30.6% in 2005 and 22% in 2011 among pregnant women and it was
23.9% in 2005 and 15% in 2011 among women neither non-pregnant nor lactating. This shows
that a relatively higher prevalence of anemia was found among Ethiopian pregnant and lactating
mothers.
Page 4 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Anemia testing was included in the two rounds of the Ethiopian demographic and health surveys
(EDHS)10
,11
. The prevalence of anemia in lactating mothers was 29.9% in 2005 and 18.5% in
2011 12
. It was 30.6% in 2005 and 22% in 2011 among pregnant women and it was 23.9% in
2005 and 15% in 2011 among women neither non-pregnant nor lactating. This shows that a
relatively higher prevalence of anemia was found among Ethiopian pregnant and lactating
mothers. However, little information is available regarding socio-economic factors associated
with anemia among lactating mothers. This study aimed to identify factors associated with
anemia among lactating mothers in Ethiopia using the pooled data of EDHS 2005 and 2011.This
study aimed to identify factors associated with anemia among lactating mothers in Ethiopia using
the pooled data of EDHS 2005 and 2011.
Methods
Data type and study design
This study is an in-depth analysis to identify factors associated with anemia among lactating
mothers based on secondary data of the EDHS 2005 and 2011 datasets. The EDHS was designed
to provide population and health indicators at national and regional levels. It is conducted every
five year. Both the 2005 and 2011 EDHS samples were selected using a stratified, two-stage
cluster design. The detailed methodology is found elsewhere 11 12
.
Data Extraction
Both EDHS 2005 and 2011 data were downloaded with permission from the Measure DHS
website in SPSS format. After reviewing the detailed data coding, further data cleaning and
recoding was completed. A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047
from EDHS 2011) were included in the analysis. Based on published literature, information on a
wide-range of socio-demographic and economic variables, health service related factors and
anemia level indicators were extracted.
Page 5 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Measurement
In both rounds of the EDHS, haemoglobin analysis was carried out onsite using a battery-
operated portable HemoCue analyzer for all anemia samples. The raw measured values of
haemoglobin were obtained using the HemoCue instrument and adjusted for altitude and
smoking status12
. All the necessary quality control measures were considered9.
Data processing and statistical analysis
Both surveys were administered by the Ethiopian Central Statistics Authority (CSA). Data entry
and editing was performed using CSPro software. For this study’s analysis, the 2005 and 2011
EDHS data were pooled to achieve high power for detecting the associated factors and analyzed
using STATA 11 software. Anemia was re-categorized as anemic and non-anemic from prior
classifications in levels (no, mild, moderate, severe). The background variables were selected
based on literature review and data availability from the two rounds of EDHS. The chosen
variables were region, residence, wealth index, occupation, BMI, duration of breastfeeding,
respondent’s education, husband’s education, family planning use, ANC use, iron
supplementation during pregnancy, time variation between two surveys, marital status, age and
parity.
Descriptive statistics were used to show the prevalence of anemia among lactating mothers
varying by background characteristics. Binary and multivariable logistic regression statistical
analysis were carried out to determine the factors associated with anemia among lactating
mothers. Variables found statistically significant at p-value <0.25 during bivariate analysis were
analyzed in the multivariable logistic regression model13
. This p-value cut off point prevented
removing variables that would potentially have an effect during multivariable analysis. Both
crude and adjusted odds ratios (OR) were reported with 95% confidence interval (CI). Variables
at p-value <0.05 were considered statistically significant in the multivariable logistic regression
model.
Ethical statements
Page 6 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
The data were downloaded and used after communicating the purpose of the analysis and
receiving permission from Measure DHS Organization. The original EDHS data were collected
in accordance with international and national ethical guidelines.
Results
Prevalence of anemia in lactating mothers by background characteristics:
.
The overall prevalence of anemia among lactating mothers during 2005 to 2011 was found to be
22.1% (95% CI: 21.13-23.03). The prevalence of anemia for the years 2005 and 2011 was 29.9%
[95% CI: (28.04-31.79)] and 18.5% [95% CI: 17.45-19.60)], respectively. The prevalence was
13.8% [95% CI: (11.44-16.41)] in urban areas and 23% [95% CI: (21.99-24.03)] in rural areas.
In the period 2005 to 2011, the highest prevalence of anemia among lactating mothers was
48.7% [95%CI: (40.80-56.62)] found in Ethiopian Somali region, while the lowest prevalence
was 9.0% [95%CI: (4.07-15.47)] reported in Addis Ababa. In the period 2005 to 2011, the
prevalence of anemia in lactating mothers was consistently higher among those in the poor
wealth index group, not currently working, with BMI greater or equal to 25 kg/m2, one year
duration of breastfeeding, never educated, never used ANC, never used family planning services,
no iron supplement during pregnancy, and with higher parity. A significant reduction in the
prevalence of anemia among lactating mothers was observed in all background variables from
2005 to 2011(Table 1). Figure 1 shows the classification of anemia in terms of its detailed
parameter.
In the bivariate step of our analysis, age and marital status were not statistically significant in the
data from both individual surveys and pooled data with the cutoff point of p<0.25. The variable
associated with anemia for the 2005 data was BMI, whereas for the 2011 data the variables were
working status, wealth index, ever use of family planning, ANC attendance four times and above
for indexed pregnancy, husband’s education, maternal BMI and duration of breastfeeding.
In the final multivariable model using pooled data, the independent predictors of anemia for
Ethiopian lactating mothers were currently working, wealth index, ever use of family planning,
ANC attendance four times and above for indexed pregnancy, husband’s education, maternal
BMI, time variation in the two surveys, and durations of breastfeeding remained..
Page 7 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Paternal educational status was found to be a predictor of anemia among lactating mothers.
Those lactating mothers who had husbands who attended primary education were at 21% less
likely to have anemia as compared to those mothers who had husbands with no education
[AOR=0.79; 95% CI: (0.68-0.91)].The odd of being anemic in working lactating mothers was
29% less as compared to their counter parts [AOR=0.71; 95% CI: (0.63-0.80)].Those lactating
mothers having a normal maternal BMI (18.5kg/m2-24.99kg/m
2) were 22% less likely to be
anemic as compared to lactating mother with low BMI (<18.5kg/m2) [AOR=0.78; 95% CI:
(0.68-0.89)].Similarly, lactating women who are categorized in middle [AOR=0.83; 95% CI:
(0.71-0.98)] and rich wealth quintiles [AOR=0.83; 95% CI: (0.70-0.98)] were each 17% less
likely to have anemia as compared to lactating women in poorer quintiles.
Among reproductive characteristics, family planning use and antenatal care (ANC) were the
significant factors associated with anemia in lactating mothers. Lactating mothers who ever used
family planning were 32% less likely to have anemia as compared to lactating mothers who
never used family planning [AOR=0.68; 95% CI: (0.57- 0.80)]. Lactating mothers who reported
ANC attendance four times or more for indexed pregnancy were 27% less likely to have anemia
as compared to mothers who never attended ANC [AOR=0.73; 95% CI: (0.59-0.91)]. Those
lactating mothers who breastfed for two years were 24% less likely to have anemia as compared
to lactating women who breastfed for one year [AOR=0.76; 95% CI: (0.66-0.87)] (Table 2).
Page 8 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Discussion
Over one fifth of lactating mothers were anemic in Ethiopia, which is lower as compared to other
developing countries. For example, more than 90% of lactating mothers have been reported as
having anemia in India 14
and 29.6% of lactating mothers in Zimbabwe developed anemia15
.
Another study from Myanmar reported an anemia prevalence rate of 60.3% in lactating women,
with 20.3% of lactating mothers having severe anemia16
. Although the prevalence of anemia
among lactating mothers in Ethiopia was relatively low as compared to these studies, it remains a
public health problem according to WHO classification17
. The relatively better prevalence of
anemia in Ethiopia among lactating mothers may be due to the cultural norms of providing
nutritional care to lactating mothers during the postpartum period. During the post-partum
period, lactating mothers are encouraged to rest for 3 to 6 months and to eat a variety of foods
including from animal sources, even during religious fasting periods. Iron supplementation
coverage in Ethiopia remained low among pregnant mothers10
, despite its known contribution for
reducing the risk of postpartum hemorrhage 12
. Post-partum hemorrhage was also found to be
one of the risk factors for anemia during the period of lactation18
. This study showed that anemia
is a widespread problem in the pastoralist communities of Ethiopian Somali and Afar. The
prevalence of anemia in lactating mothers was higher in the pastoralist regions and showed slow
decline in these regions from 2005 to 2011. This could be due to the fact that pastoralist
communities are heavily dependent on animal milk as a source of daily food, with poor iron
bioavailability19 20
. The other reason could be due to low utilization of family planning and
antenatal care services in pastoralist areas10
.
One of the factors determined to be associated with anemia was paternal education. Having a
husband with a higher level of education was found to be associated with less odd of having
anemia among lactating mothers. Those mothers having husbands with primary level education
were less likely to have anemia as compared to those with husbands who had no education.
However, maternal educational status was not statistically associated with anemia, which is
contradictory to many studies from Ethiopia as well as from abroad 16 21-23
. This might be one
important motivator to involve husbands in anemia prevention efforts.
Page 9 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Working lactating mothers had lower odd of having anemia as compared to their counter parts.
This might be because working mothers were earning money as compared to non-working
mothers and the extra income enabled access to purchase more food items, including animal
sources (meat, poultry, fish etc), and increase dietary diversity. Studies have shown that income
growth improves diet diversity which in turn improves micronutrient intake, including iron 24 25
.
Similarly, the lactating mothers in the lower wealth groups had greater odds of anemia as
compared to lactating mothers in the higher wealth quintiles. In many other studies of anemia
among reproductive age women, the wealth index was found to be a statistically significant
factor 16 21
. Other studies have also shown that women of low socio-economic status are at risk
for iron deficiency anemia (IDA) in late pregnancy and in the postpartum period26 27
. Therefore,
women’s empowerment through economic interventions and working status could have a
positive contribution towards preventing anemia.
This study also supports the importance of family planning for reducing the risk of anemia.
Those lactating mothers who have ever used family planning (modern or traditional) had a lower
odd of having anemia as compared to those who had never used family planning. This finding is
consistent with studies from Ethiopia and Timor-Leste which showed that use of family planning
was associated with lower odd of having anemia.21 28
.21
.
Maternal nutritional status (measured by body mass index) was found to be significantly
associated with anemia. As compared with undernourished lactating mothers (BMI<18.5kg/m2),
being in the normal BMI category (18.5-24.9kg/m2) was associated with a lower odd of having
anemia. This finding is similar with others studies29 30
. When a mother is at risk of deficiency for
macronutrients, most likely she is also at risk also other micronutrient deficiencies such as
iron31
..
ANC attendance was found to be associated with anemia among lactating mothers. This is most
likely due to the fact that during ANC attendance mothers have been advised to take iron
supplements according to the Ethiopian micronutrient guideline and instructed to consume
different sources of iron rich food items32
. Therefore, improving iron status during pregnancy
also helps to prevent anemia during the lactation period.
Page 10 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Anemia is a public health problem among lactating mothers in Ethiopia. There are regional
disparities regarding the prevalence of anemia, with the highest prevalence found in pastoralist
regions of Ethiopian Somali and Afar. Promoting partner education, improving maternal
nutritional status, creating behavior change among lactating mothers to use family planning and
attend antenatal care services at health facilities are recommended interventions to reduce the
prevalence of anemia among lactating women in Ethiopia.
Conclusion
Anemia is a public health problem among lactating mothers in Ethiopia. There are regional
disparities regarding the prevalence of anemia, with the highest found in pastoralist regions of
Ethiopian Somali and Afar. Promoting partner education, improving maternal nutritional status,
creating behavior change among lactating mothers to use family planning and attend antenatal
care services at health facilities are recommended interventions to reduce the prevalence of
anemia among lactating women in Ethiopia.
Competing interests
The authors declare that they have no competing interests.
Funding statement
This research received no specific grant from any funding agency in the public, commercial or
not-for-profit sectors'
Authors’ contributions
YL and DH conceived the idea. YL analyzed and interpreted the data and critically reviewed the
manuscript. SB assisted in critically reviewing the manuscript. DH drafted the manuscript,
assisted in the data analysis and interpretation and critically reviewed the manuscript. All authors
reviewed and approved the manuscript.
Page 11 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Acknowledgements
The authors acknowledge DHS Measure for granting the data freely. We are also grateful to
thank Lianna Tabar, country representative of KHI-E, for her professional language editing and
reviewing the manuscript.
References
1. WHO. The world health report. Reducing risks, promoting healthy life. Geneva, World Health
Organization, 2002., 2002.
2. Whitney E, Rolfes SR. Understanding Nutrition. In: Adams P, editor. Eleventh Edition ed. United States
of America: Thomson Learning Academic Resource Center, 2008.
3. Domell V, Lonnerdal B, Dewey K, Cohen R, Hernell O. Iron zinc and copper concentrations in breast
milk are independent of maternal status. American Journal of clinical nutrition 2004;79(1):111-
15.
4. Bodnar L, Scanlon K, Freedman D, Siega–Riz A, Cogswell M. High prevalence of postpartum anaemia
amongLow income women in the United States. Journal of obstetrics and Gynecology
2001;185:4348-53.
5. Sserunjogi L, Scheut F, Whyte SR. Postnatal anaemia: neglected problems and missed opportunities in
Uganda. HEALTH POLICY AND PLANNING 2003;18(2):225-31.
6. Beard JL, Hendricks MK, Perez EM, Murray-Kolb LE, Berg A, Vernon-Feagans L, et al. Maternal Iron
Deficiency Anemia Affects Postpartum Emotions and Cognition. Journal of Nutrition
2005;135:267–72.
7. Ross J, homas E. Iron deficiency anemia and maternal mortality. PROFILES 3 working notes series no.
3. Academy for Education Development, Washington D.C., 1996.
8. Brabin BJ, Hakimin M, Pelletier D. An Analysis of Anemia and Pregnancy-Related Maternal Mortality.
The Journal of Nutrition 2001;131:604S-15S.
9. Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, Lozano R, et al. A systematic analysis of
global anemia burden from 1990 to 2010. Blood 2014;123(5).
10. Central Statistical Agency (CSA) Ethiopia. Demographic and Health Survey 2011. Addis Ababa,
Ethiopia and Calverton, Maryland, USA: CSA and ORC Macro. 2011.
11. Central Statistical Agency(CSA). Demographic and Health Survey 2005. Addis Ababa, Ethiopia and
Calverton, Maryland, USA: CSA and ORC Macro, 2005.
12. CentralStatisticalAgency(CSA) EM. Demographic and Health Survey 2011. Addis Ababa, Ethiopia and
Calverton, Maryland, USA: CSA and ORC Macro., 2011.
13. Peter C, Jack V. Automated variable selection methods for logistic regression produced unstable
models for predicting acute myocardial infarction mortality. Journal of Clinical Epidemiology
2004;57:1138-46.
14. Agarwal KN, Agarwal DK, Sharma A, Sharma K, Prasad K, Kalita MC, et al. Prevalence of anaemia in
pregnant & lactating women in India. Indian J Med Res 2006;124:173-84.
15. Sikosana PL, Bhebhe S, Katuli S. A prevalence survey of iron deficiency and iron deficiency anaemia in
pregnant and lactating women, adult males and pre-school children in Zimbabwe. Cent Afr J
Med 1998;44(12):297-305.
16. Zhao A, Zhang Y, Li B, Wang P, Li J, Xue Y, et al. Prevalence of Anemia and Its Risk Factors Among
Lactating Mothers in Myanmar. Am J Trop Med Hyg 2014;doi: 10.4269/ajtmh.13-0660.
Page 12 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
17. WHO. Worldwide prevalence of anaemia 1993-2005 : WHO global database on anaemia / Edited by
Bruno de Benoist, Erin McLean, Ines Egli and Mary Cogswell.
, 2008.
18. World Health Organization (WHO). Recommendations for the Prevention of Postpartum
Haemorrhage (summary of results from a WHO technical consultation, October 2006) Geneva:
WHO 2007.
19. Kibangou I, Bouhallab S, Henry G, Bureau F, Allouche S, Blais A, et al. Milk proteins and iron
absorption: contrasting effects of different caseinophosphopeptides. Pediatrics Research 2005
58(4):731-34.
20. Belachew T. Human Nutrition lecture note series for Health sciences students: JImma Univesity
2005:pp 229.
21. Gebremedhin S, Enquselassie F. Correlates of anemia among women of reproductive age in Ethiopia:
Evidence from Ethiopian DHS 2005. Ethiopian Journal of Health Development 2011;25(1):22-30.
22. Haidar J. Prevalence of Anaemia, Deficiencies of Iron and Folic Acid and Their Determinants in
Ethiopian Women. Journal of Health Population Nutrition 2010;28(4):359-68.
23. Okwu GN. Studies on the predisposing factors of iron deficiency anaemia among lactating women in
Owerri, Nigeria International Research Journal of Biochemistry and Bioinformatics
2011;1(11):304-09.
24. Taruvinga A, Muchenje V, Mushunje A. Determinants of rural household dietary diversity: The case
of Amatole and Nyandeni districts, South Africa International Journal of Development and
Sustainability 2013;2 (4).
25. Doan D. Does income growth improve diet diversity in China?Selected Paper prepared for
presentation at the 58 the AARES Annual Conference, Port Macquarie, New South Wales, 4-7
February 2014 2014.
26. Bodnar L, Cogswell M, Scanlon K. Low income postpartum women are at risk of iron deficiency.
Journal of Nutrition 2002;132:2298–302.
27. Sadeghian M, Fatourechi A, Lesanpezeshki M, Ahmadnezhad E. Prevalence of Anemia and Correlated
Factorsin the Reproductive Age Women in Rural Areas of Tabas. Journal of Family and
Reproductive Health 2013;7(3):143.
28. Lovermail AA, Hartman M, Chia KS, Heymann DL. Demographic and Spatial Predictors of Anemia in
Women of Reproductive Age in Timor-Leste: Implications for Health Program Prioritization. PLoS
ONE 2013;9(3):e91252.
29. Eckhardt CL, Torheim LE, Monterrubio E, Barquera S, Ruel M. Overweight and Obese Women Remain
at Risk for Anemia in Countries Undergoing the Nutrition Transition. THe FASEB Journal
2006;20:A986-A87.
30. Cepeda-Lopez A, Aeberli I, Zimmermann M. Does obesity increase risk for iron deficiency? A review
of the literature and the potential mechanisms. Int J Vitam Nutr Res 2010;80(4-5):263-70.
31. Blumfield M, Hure A, MacDonald-Wicks L, Smith R, Simpson S, Raubenheimer D, et al. The
association between the macronutrient content of maternal diet and the adequacy of
micronutrients during pregnancy in the Women and Their Children’s Health (WATCH) study.
Nutrients 2012;4(12):1958-76.
32. FMOH. NATIONAL GUIDELINE FOR CONTROL AND PREVENTION OF MICRONUTRIENT DEFICIENCIES,
2004.
Page 13 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
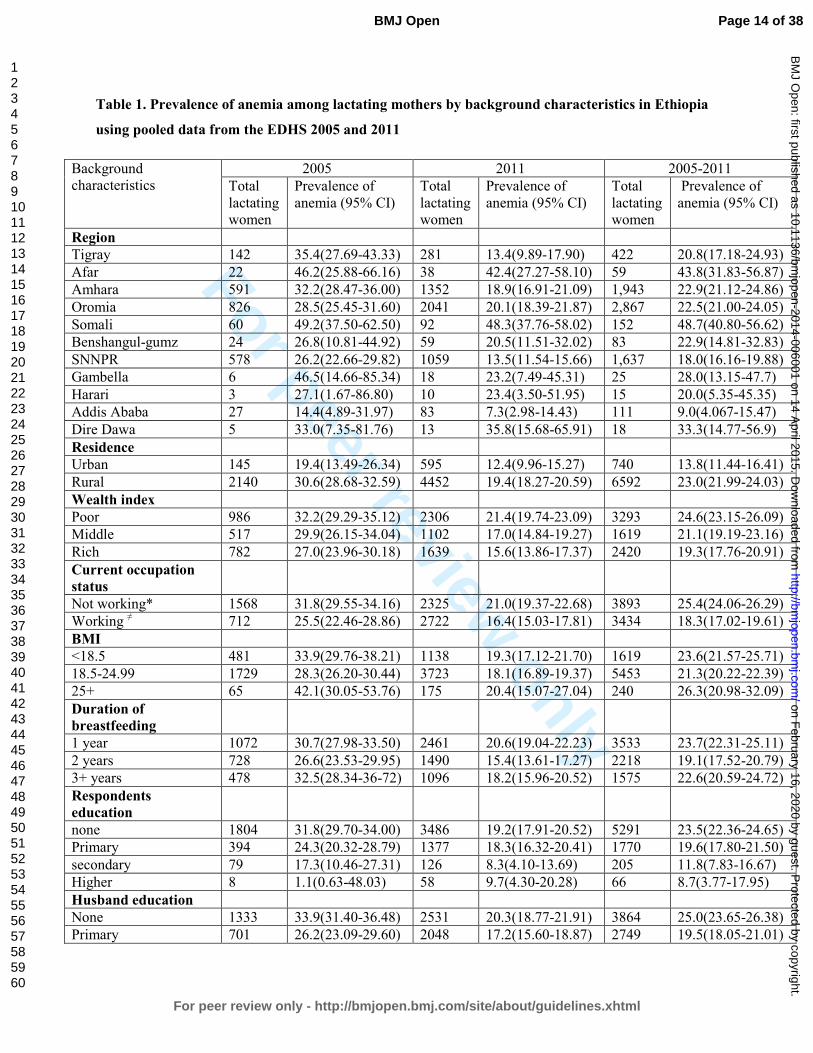
Table 1. Prevalence of anemia among lactating mothers by background characteristics in Ethiopia
using pooled data from the EDHS 2005 and 2011
Background
characteristics
2005 2011 2005-2011
Total
lactating
women
Prevalence of
anemia (95% CI)
Total
lactating
women
Prevalence of
anemia (95% CI)
Total
lactating
women
Prevalence of
anemia (95% CI)
Region
Tigray 142 35.4(27.69-43.33) 281 13.4(9.89-17.90) 422 20.8(17.18-24.93)
Afar 22 46.2(25.88-66.16) 38 42.4(27.27-58.10) 59 43.8(31.83-56.87)
Amhara 591 32.2(28.47-36.00) 1352 18.9(16.91-21.09) 1,943 22.9(21.12-24.86)
Oromia 826 28.5(25.45-31.60) 2041 20.1(18.39-21.87) 2,867 22.5(21.00-24.05)
Somali 60 49.2(37.50-62.50) 92 48.3(37.76-58.02) 152 48.7(40.80-56.62)
Benshangul-gumz 24 26.8(10.81-44.92) 59 20.5(11.51-32.02) 83 22.9(14.81-32.83)
SNNPR 578 26.2(22.66-29.82) 1059 13.5(11.54-15.66) 1,637 18.0(16.16-19.88)
Gambella 6 46.5(14.66-85.34) 18 23.2(7.49-45.31) 25 28.0(13.15-47.7)
Harari 3 27.1(1.67-86.80) 10 23.4(3.50-51.95) 15 20.0(5.35-45.35)
Addis Ababa 27 14.4(4.89-31.97) 83 7.3(2.98-14.43) 111 9.0(4.067-15.47)
Dire Dawa 5 33.0(7.35-81.76) 13 35.8(15.68-65.91) 18 33.3(14.77-56.9)
Residence
Urban 145 19.4(13.49-26.34) 595 12.4(9.96-15.27) 740 13.8(11.44-16.41)
Rural 2140 30.6(28.68-32.59) 4452 19.4(18.27-20.59) 6592 23.0(21.99-24.03)
Wealth index
Poor 986 32.2(29.29-35.12) 2306 21.4(19.74-23.09) 3293 24.6(23.15-26.09)
Middle 517 29.9(26.15-34.04) 1102 17.0(14.84-19.27) 1619 21.1(19.19-23.16)
Rich 782 27.0(23.96-30.18) 1639 15.6(13.86-17.37) 2420 19.3(17.76-20.91)
Current occupation
status
Not working* 1568 31.8(29.55-34.16) 2325 21.0(19.37-22.68) 3893 25.4(24.06-26.29)
Working ≠ 712 25.5(22.46-28.86) 2722 16.4(15.03-17.81) 3434 18.3(17.02-19.61)
BMI
<18.5 481 33.9(29.76-38.21) 1138 19.3(17.12-21.70) 1619 23.6(21.57-25.71)
18.5-24.99 1729 28.3(26.20-30.44) 3723 18.1(16.89-19.37) 5453 21.3(20.22-22.39)
25+ 65 42.1(30.05-53.76) 175 20.4(15.07-27.04) 240 26.3(20.98-32.09)
Duration of
breastfeeding
1 year 1072 30.7(27.98-33.50) 2461 20.6(19.04-22.23) 3533 23.7(22.31-25.11)
2 years 728 26.6(23.53-29.95) 1490 15.4(13.61-17.27) 2218 19.1(17.52-20.79)
3+ years 478 32.5(28.34-36-72) 1096 18.2(15.96-20.52) 1575 22.6(20.59-24.72)
Respondents
education
none 1804 31.8(29.70-34.00) 3486 19.2(17.91-20.52) 5291 23.5(22.36-24.65)
Primary 394 24.3(20.32-28.79) 1377 18.3(16.32-20.41) 1770 19.6(17.80-21.50)
secondary 79 17.3(10.46-27.31) 126 8.3(4.10-13.69) 205 11.8(7.83-16.67)
Higher 8 1.1(0.63-48.03) 58 9.7(4.30-20.28) 66 8.7(3.77-17.95)
Husband education
None 1333 33.9(31.40-36.48) 2531 20.3(18.77-21.91) 3864 25.0(23.65-26.38)
Primary 701 26.2(23.09-29.60) 2048 17.2(15.60-18.87) 2749 19.5(18.05-21.01)
Page 14 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Secondary 199 20.7(15.41-26.64) 238 14.3(10.26-19.17) 437 17.2(13.84-20.92)
Higher 23 14.8(3.43-31.53) 147 13.7(8.75-19.88) 170 13.8(8.99-19.30)
Family planning
Never use 1775 32.1(29.97-34.31) 2889 21.2(19.72-22.70) 4663 25.4(24.16-26.66)
Ever use 15 16.4(2.30-37.52) 2158 14.9(13.46-16.47) 2173 14.9(13.46.16.45)
ANC use
Never 1636 32.0(29.80-34.32) 2977 20.4(18.97-21-87) 4613 24.5(23.27-25.75)
1-3 386 27.7(23.43-32.35) 1208 18.4(16.27-20.64) 1594 20.6(18.65-22.62)
4+ 260 18.9(14.44-23.95) 845 12.6(10.44-14.91) 1105 14.1(12.16-16.27)
Iron supplement
during pregnancy
No 2046 30.1(28.15-32.12) 4196 18.8(17.64-20.01) 6242 22.5(21.47-23.54)
Yes 236 27.1(21.74-33.06) 840 16.9(14.48-19.55) 1076 19.2(16.97-21.68)
Parity
1-4 1293 28.9(26.50-31.44) 3111 18.1(16.77-19.48) 4404 21.3(20.11-22.53)
5-9 903 30.5(27.52-33.52) 1739 19.6(17.79-21.53) 2642 23.3(21.73-24.96)
10+ 89 37.1(27.53-47.46) 197 17.0(12.02-12.46) 287 23.2(18.72-28.50)
Total 2285 29.9(28.04-31.79) 5047 18.5(17.45-19.60) 7332 22.1(21.13-23.03) ANC-Antenatal Care, BMI-Body Mass Index, *those mothers who currently work to earn money, ≠ those mothers
who do not currently engage in any type of formal work to earn money.
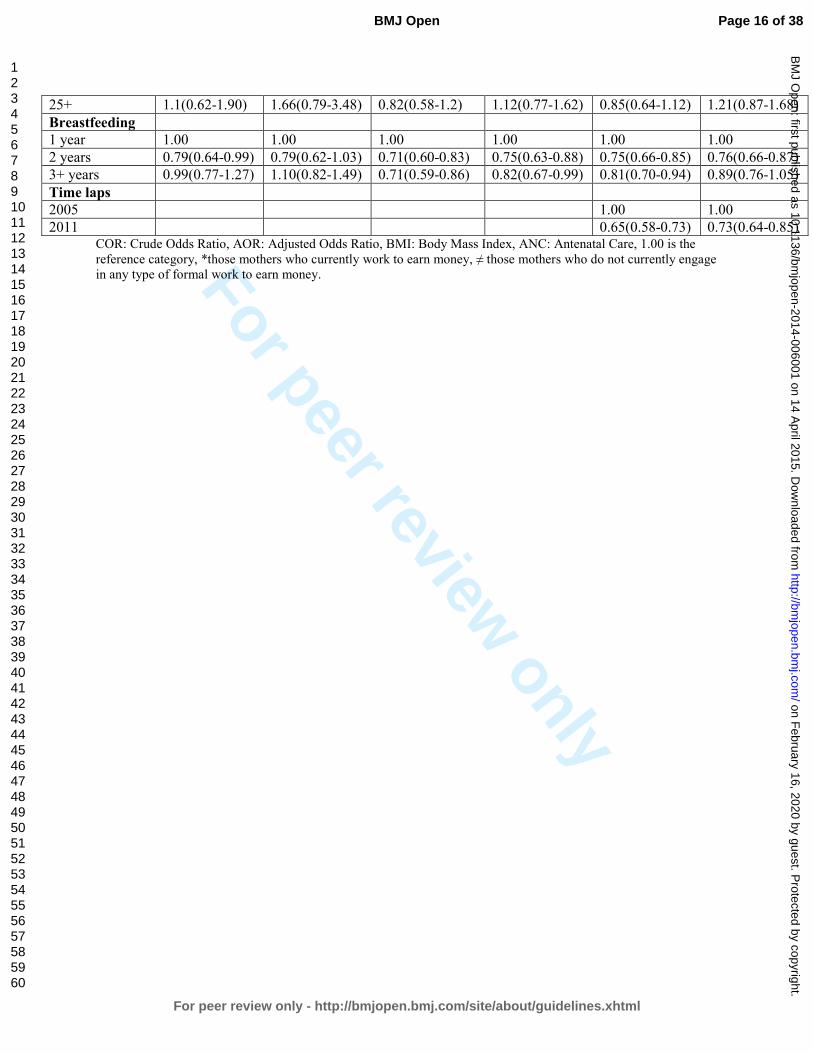
Table 12. Factors associated with anemia among lactating mothers in Ethiopia using pooled
data from the EDHS 2005 and 2011 Variables 2005 2011 2005-2011
COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI
Occupation
Not working* 1.00 1.00 1.00 1.00 1.00 1.00
Working≠ 0.82(0.66-1.00) 0.83(0.64-1.06) 0.62(0.54- 0.71) 0.68(0.58-0.78) 0.64(0.57-0.72) 0.71(0.63-0.80)
Wealth index
Poor 1.00 1.00 1.00 1.00 1.00 1.00
Middle 0.71(0.54-0.92) 0.82(0.61-1.10) 0.74(0.61- 0.89) 0.85(0.69-1.04) 0.74(0.64-0.87) 0.83(0.71-0.98)
Rich 0.66(0.53-0.82) 0.91(0.68-1.22) 0.62(0.52-0.72) 0.80(0.65-0.97) 0.65(0.57-0.73) 0.83(0.70-0.98)
FP use
Never used 1.00 1.00 1.00 1.00 1.00 1.00
Ever used 0.37(0.11-1.28) 0.51(0.14-1.91) 0.54(0.46-0.63) 0.69(0.58-0.82) 0.48(0.41-0.55) 0.68(0.57-0.80)
ANC attended
Never 1.00 1.00 1.00 1.00 1.00 1.00
1-3 0.78(0.59-1.03) 0.94(0.66-1.33) 0.78(0.59-1.00) 1.00(0.83-1.2) 0.81(0.71-0.94) 0.99(0.84-1.16)
4+ 0.55(0.41-0.74) 0.82(0.53-1.28) 0.55(0.41-0.74) 0.71(0.55-0.92) 0.52(0.44-0.61) 0.73(0.59-0.91)
Husband
education
None 1.00 1.00 1.00 1.00 1.00 1.00
Primary 0.77(0.61-0.96) 0.77(0.58-1.01) 0.69(0.59-0.80) 0.80(0.67-0.94) 0.69(0.61-0.78) 0.79(0.68-0.91)
Secondary 0.55(0.39-0.77) 0.83(0.50-1.38) 0.64(0.48-0.87) 0.81(0.58-1.14) 0.62(0.49-0.77) 0.83(0.62-1.09)
Higher 0.58(0.26-1.30) 0.50(0.73-3.40) 0.72(0.49-1.0) 0.96(0.61-1.52) 0.64(0.46-0.90) 0.94(0.61-1.45)
BMI*
<18.5 1.00 1.00 1.00 1.00 1.00 1.00
18.5-24.99 0.74(0.59-0.92) 0.76(0.59-0.99) 0.74(0.64-0.86) 0.79(0.68-0.93) 0.76(0.67-0.86) 0.78(0.68-0.89)
Page 15 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
25+ 1.1(0.62-1.90) 1.66(0.79-3.48) 0.82(0.58-1.2) 1.12(0.77-1.62) 0.85(0.64-1.12) 1.21(0.87-1.68)
Breastfeeding
1 year 1.00 1.00 1.00 1.00 1.00 1.00
2 years 0.79(0.64-0.99) 0.79(0.62-1.03) 0.71(0.60-0.83) 0.75(0.63-0.88) 0.75(0.66-0.85) 0.76(0.66-0.87)
3+ years 0.99(0.77-1.27) 1.10(0.82-1.49) 0.71(0.59-0.86) 0.82(0.67-0.99) 0.81(0.70-0.94) 0.89(0.76-1.05)
Time laps
2005 1.00 1.00
2011 0.65(0.58-0.73) 0.73(0.64-0.85) COR: Crude Odds Ratio, AOR: Adjusted Odds Ratio, BMI: Body Mass Index, ANC: Antenatal Care, 1.00 is the
reference category, *those mothers who currently work to earn money, ≠ those mothers who do not currently engage
in any type of formal work to earn money.
Page 16 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Factors associated to develop anemia among lactating mothers in Ethiopia: A pooled data
analysis from two rounds of demographic and health surveys
Anemia prevalence and associated factors among lactating mothers in Ethiopia: Evidence from the
2005 and 2011 demographic and health surveys
Yihunie Lakew1, Sibhatu Biadgilign2, Demewoz Haile3*
1 Ethiopian public health association, Addis Ababa, Ethiopia
2 Independent public health consultants, Addis Ababa, Ethiopia
3 Department of Public Health, College of Medicine and Health sciences, Madawalabu
University, Ethiopia
Email address
Yihunie Lakew – [email protected]
Sibhatu Biadgilign- [email protected]
Demewoz Haile–[email protected]
*Corresponding author
Address of corresponding author
Department of Public Health
College of Medicine and Health sciences
Madawalabu University, Ethiopia
Bale Goba , p, box 302
Running title: Factors associated with anemia among lactating mothers in Ethiopia
Formatted: Not Highlight
Page 17 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Key words: Lactating mothers, anemia, Ethiopia,
Word count: 23882143
Abstract
Objective: To identify factors associated with anemia among lactating mothers in Ethiopia.
Design: A cross-sectional secondary data analysis pooled from two rounds of the 2005 and 2011
Ethiopian demographic and health survey (EDHS) was used. Multivariable logistic regression
model was applied to determine the factors associated with anemia.
Population: A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047 from EDHS
2011) were included from 11 administrative states of Ethiopia.
Main outcome measures: Lactating mothers considered as anemic if hemoglobin level <12
gram per deciliter.g/dl
Results: The overall prevalence of anemia among lactating mothers was found to be 22.1%
[95% CI: (21.13-23.03)]. The highest prevalence was 48.7% [95% CI: (40.80-56.62)] found in
Ethiopian Somali region, followed by 43.8% [95% CI: (31.83-56.87)] in Afar region. The
prevalence in urban settings was 13.7% [95% CI: (11.35-16.05)] and in rural areas was 23%
[95% CI: (22.68-23.32)]. The multivariable statistical model showed that lactating mothers who
had husbands who attended primary education mothers whose husbands had attended primary
and secondary education were, respectively, 26% [AOR=0.79; 95% CI: (0.68-0.91)], adjusted
odds ratio (AOR) = 0.74; 95% CI: (0.60-0.92)] who were currently working [AOR=0.71; 95%
CI: (0.63-0.80)], had normal maternal body mass index (BMI) from 18.5kg/m2 to 24.99kg/m
2
[AOR=0.78; 95% CI: (0.68-0.89)], were in the middle wealth quintile [AOR=0.83; 95% CI:
(0.71-0.98)] and rich wealth quintile [AOR=0.83; 95% CI: (0.70-0.98)], reported ever use of
family planning [AOR=0.68; 95% CI: (0.57-0.80)], were attending antenatal care (ANC) for
indexed pregnancy four times or more [AOR=0.73; 95% CI: (0.59-0.91)], experienced time
variation between two surveys [AOR=0.73; 95%CI: (0.64-0.85)] and who breastfed for two
years [AOR=0.76; 95% CI: (0.66-0.87)] were found to be associated with anemia
Conclusion: Anemia is highly prevalent among lactating mothers, particularly among pastoralist
communities of Ethiopian Somali and Afar.in rural and pastoralist Ethiopia. Factors including
paternal education, family planning use, body mass index (BMI), occupational status, and
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Page 18 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
antenatal care attendance were strong predictors of anemia among lactating mothers. Promoting
partner education, improving maternal nutritional status, creating behaviour change among
lactating mothers to use family planning and attend ANC services at health facilities are
recommended interventions to reduce the prevalence of anemia among lactating mothers in
Ethiopia.Promoting partner education, improving BMI, scaling up family planning and antenatal
care services are recommended interventions.
ARTICLE SUMMARY
Strength and Limitations
• The study attempted to identify factors associated with laboratory confirmed anemia in
lactating mothers at the national level. The study findings can be used to inform policy
and program actions.
• Some regions from which data was collected had, the data has small sample size. So that
it should be interpreted in caution. for some regions, which questions the accuracy of
prevalence estimates per region.
Key messages
• Anemia prevalence is a public health problem among lactating mothers in Ethiopia, .with
the highest prevalence found in pastoralist regions of Ethiopian Somali and Afar
• There are regional disparities regarding the prevalence of anemia among lactating
mothers, with the highest rates found in pastoralist regions.
• A statistically significant reduction of anemia prevalence in lactating mothers was
observed from 2005 to 2011.
• Being in middle and rich wealth quintiles, two years of breastfeeding, currently working,
normal body mass index, husbands’ primary education, ever use of family planning and
antenatal care attendance for four or more visits were factors found to be associated with
anemia.
• Husband education, family planning and ANC attendance were protective factors for
developing anemia.
Formatted: Not Highlight
Formatted: Space After: 0 pt
Formatted: Not Highlight
Formatted: Font: Times New Roman, 12 pt,
Font color: Black
Formatted: Not Highlight
Formatted: Font: Times New Roman
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: No bullets or numbering
Page 19 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
• Overweight and obese lactating mothers were at high risk for developing anemia.
Page 20 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Introduction
Anemia is a serious nutrition problem affecting millions in Anemia is one of the nutrition
problems affecting millions in developing countries, and remains a major challenge for human
health, social and economic development1. Lactating mothers are one of the vulnerable groups of
anemia. During the period of lactation, mothers are susceptible to anemia due to maternal iron
depletion and blood loss during child birth2. Studies have shown that though breast milk is not a
good source of iron, the concentration of iron in breast milk is independent of maternal iron
status. This showed that the quality of breast milk is maintained at the expense of maternal
stores2 3. Studies have shown that the concentration of iron in breast milk is independent of
maternal iron status and that the quality of breast milk is maintained at the expense of maternal
stores2 3
.
Postpartum anemia has been found highest in mothers who were anemic during pregnancy4.
Furthermore, lactating mothers are highly susceptible to iron depletion if they have not had
enough energy and nutrient intake in their diets. Yet the problem of anemia in postnatal women
has been relatively neglected which is far away from previously thoughts8. Lactating mothers
enter begin into the postnatal period after having iron depleted through the continuum from
pregnancy to childbearing 5. A study from South Africa evidenced showed that iron status was
associated with there was a strong relation between iron status and depression, stress, and
cognitive functioning in poor African mothers during the postpartum period6. In a meta-analysis
of observational and intervention trials, Ross and Thomas6, found that approximately 20% of the
maternal mortality seen in sub-Saharan Africa and South Asia was attributable to anemia that is
was primarily the result of iron deficiency 7.. Ethiopia is one of the sub-Saharan Africa countries
heavily affected by anemia8
Ethiopia is one of the countries in sub-Saharan Africa affected by anemia and it contributes to
high rates of maternal, infant and child mortality globally8 9. In Ethiopia, the maternal mortality
ratio was 676 maternal deaths per 100,000 live births for the seven-year period preceding the
2011 EDHS survey. This rate is one of the highest in the world. The infant mortality rate was 59
per 1,000 live births and the under-five mortality rate was 88 per 1,000 live births10
.
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Page 21 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
. Anemia testing was included in the two rounds of the Ethiopian Demographic and Health
Surveys (EDHS)1011
. The prevalence of anemia in lactating mothers was 29.9% in 2005 and
18.5% in 201110
. It was 30.6% in 2005 and 22% in 2011 among pregnant women and it was
23.9% in 2005 and 15% in 2011 among women neither non-pregnant nor lactating. This shows
that a relatively higher prevalence of anemia was found among Ethiopian pregnant and lactating
mothers.
Anemia testing was included in the two rounds of the Ethiopian demographic and health surveys
(EDHS)10,11. The prevalence of anemia among in lactating mothers was 29.9% in 2005 and
18.5% in 2011 12
. It was 30.6% in 2005 and 22% in 2011 among pregnant women and it was
23.9% in 2005 and 15% in 2011 among women neither non-pregnant nor lactating. This shows
that a relatively higher prevalence of anemia was found among Ethiopian pregnant and lactating
mothers., which is considerably higher as compared with other women (23.9% in 2005 and 15%
in 2011), and low as compared with pregnant mothers (30.6% in 2005 and 22% in 2011). This
prevalence of anemia in lactating mothers is one of the highest among developing countries.
However, little information is available regarding socio-economic factors associated with anemia
among lactating mothers. This study aimed to identify factors associated with anemia among
lactating mothers in Ethiopia using the pooled data of EDHS 2005 and 2011.However, there is a
scarcity of evidence for the factors associated with anemia among lactating mothers in Ethiopia.
Therefore, tThis study aimsed to identify the factors associated with anemia among Ethiopian
lactating mothers in Ethiopia using the pooled data of EDHS 2005 and 2011.
Methods
Data type and study design
This study is an in-depth analysis to identify risk factors associated for with anemia among
lactating mothers based on secondary data of the EDHS 2005 and 2011 datasets. The EDHS was
designed to provide population and health indicators at national (urban and rural) and regional
levels. It is and were conducted within every five year intervals. Both the 2005 and 2011 EDHS
samples were selected using a stratified, two-stage cluster design. The detailed methodology is
found elsewhere 11 12.
Data Extraction
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Font: 12 pt
Formatted: Not Highlight
Page 22 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Both EDHS 2005 and 2011 data were downloaded with permission from the Measure EDHS
website in SPSS format with permission. After reviewing understanding the detailed data coding,
further data cleaning and recoding was completed. A total of 7,332 lactating mothers (2,285 from
EDHS 2005 and 5,047 from EDHS 2011) were included in the analysis. Based on published
literature, information on a wide-range of socio-demographic and economic variables, health
service related factors and anemia level indicators were extracted.
Measurement
In both rounds of the EDHS, haemoglobin analysis was carried out onsite using a battery-
operated portable HemoCue analyzer for all anemia samples. The raw measured values of
haemoglobin were obtained using the HemoCue instrument and adjusted for altitude and
smoking status12
. All the necessary quality control measures were considered9..
Data processing and statistical analysis
Both surveys were administered by the Ethiopian Central Statistics Authority (CSA). Data entry
and editing was performed using CSPro software. For this study’s analysis, the 2005 and 2011
EDHS data were pooled to achieve high power for detecting the associated factors and analyzed
using STATA 11 software. Anemia was re-categorized as anemic and non-anemic from prior
classifications in levels (no, mild, moderate, severe). The background variables were selected
based on literature review and data availability from the two rounds of EDHS. The chosen
variables were region, residence, wealth index, occupation, BMI, duration of breastfeeding,
respondent’s education, husband’s education, family planning use, ANC use, iron
supplementation during pregnancy, time variation between two surveys, marital status, age and
parity.
Descriptive statistics was were used to show the prevalence of anemia among lactating mothers
varying by background characteristics.across the regional states and city administrations of
Ethiopia. Binary and multivariable Multivariable binary logistic regression statistical analysis
was were carried out to determine the factors associated with anemia among lactating mothers.
Variables found statistically significant at p-value <0.25 during bivariate analysis were analyzed
in the multivariable logistic regression model13. This p-value cut off point prevented removing
variables that would potentially have an effect during multivariable analysis. Both crude and
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Page 23 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
adjusted odds ratios (OR) were determined reported with 95% confidence interval (CI). All tests
were two-sided, weighted and a p-value <0.05 was considered statistically significant. Variables
at p-value <0.05 were considered statistically significant found statistically significant at p-value
<0.3 during bivariate analysis were considered for adjustment in the multivariable logistic
regression model.
Ethical statements
The data were downloaded and used after communicating the purpose of the analysis and
receiving permission from Measure DHS Organization. The original EDHS data were collected
in accordance with international and national ethical guidelines.
Results
Prevalence of anemia in lactating mothers by background characteristics:
The overall prevalence of anemia among lactating mothers during 2005 and to 2011 was found
to be 22.1% (95% CI: 21.13-23.03). The prevalence of anemia for the years 2005 and 2011 was
29.9% [95% CI: (28.04-31.79)] and 18.5% [95% CI: 17.45-19.60)], respectively. The prevalence
was 13.8% [95% CI: (11.44-16.41)] in urban areas and 23% [95% CI: (21.99-24.03)] in rural
areas. In the period 2005 to 2011, the highest prevalence of anemia among lactating mothers was
48.7% [95%CI: (40.80-56.62)] found in Ethiopian Somali region, while the lowest prevalence
was 9.0% [95%CI: (4.07-15.47)] reported in Addis Ababa. . The highest prevalence of anemia
among lactating mothers was found in Somali region (48.7%), while the lowest prevalence was
reported in Addis Ababa (9.0%) In the period 2005 to 2011, the prevalence of anemia in lactating
mothers was consistently higher among those in the poor wealth index group, not currently
working, with BMI greater or equal to 25 kg/m2, one year duration of breastfeeding, never
educated, never used ANC, never used family planning services, no iron supplement during
pregnancy, and with higher parity. A significant reduction in the prevalence of anemia among
lactating mothers was observed in all background variables from 2005 to 2011 (Table 1). Figure
1 shows the classification of anemia in terms of its detailed parameter.
Table 1. Prevalence of anemia among lactating mothers in Ethiopia using pooled data from
the EDHS 2005 and 2011
Location Variables 2005-2011
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Tab stops: Not at 0.58"
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Font: Bold
Page 24 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Weighted total number of
lactating mothers
Weighted prevalence of
anemia (95% CI)
Region
Tigray 422 20.8(17.18-24.93)
Afar 59 43.8(31.83-56.87)
Amhara 1943 22.9(21.12-24.86)
Oromiya 2867 22.5(21.00-24.05)
Somali 152 48.7(40.80-56.62)
Benshangul 83 22.9(14.81-32.83)
SNNP 1637 18.0(16.16-19.88)
Gambella 25 28.0(13.15-47.7)
Harar 15 20.0(5.35-45.35)
Adiss Ababa 111 9.0(4.067-15.47)
Diredawa 18 33.3(14.77-56.9)
Residence
Urban 740 13.8(11.44-16.41)
Rural 6592 23.0(21.99-24.03)
Total 7332 22.1(21.13-23.03)
In the bivariate step of our analysis, age and marital status were not statistically significant in the
data from both individual surveys and pooled data with the cutoff point of p<0.25. The variable
associated with anemia for the 2005 data was BMI, whereas for the 2011 data the variables were
working status, wealth index, ever use of family planning, ANC attendance four times and above
for indexed pregnancy, husband’s education, maternal BMI and duration of breastfeeding.
In total, 12 variables for anemia were both available from the EDHS and identified as risk factors
based on literature review. Of the twelve, the factors identified as significantly associated with
anemia in the bivariate step were wealth index, place of residence, maternal education, paternal
education, maternal occupation, family planning use, maternal BMI and antenatal care
attendance. In the final multivariable model using pooled data, the independent predictors of
anemia for Ethiopian lactating mothers were currently working, wealth index, ever use of family
planning, ANC attendance four times and above for indexed pregnancy, husband’s education,
maternal BMI, time variation in the two surveys, and durations of breastfeeding
remained.However, in the multivariable model, paternal education, maternal occupation, family
planning use, maternal BMI and antenatal care attendance remained the independent predictors
of anemia for Ethiopian lactating mothers.
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Page 25 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Paternal educational status was found to be a predictor of anemia among lactating mothers.
Those lactating mothers who had husbands who attended primary education were at 216% lower
less risk likely to for haveing anemia as compared to those mothers who had husbands with no
education [AOR=0.79; 95% CI: (0.68-0.91)].[AOR=0.74; 95% CI: (0.60-0.92)]. Those lactating
mothers with husbands who had secondary education had a 34% lower risk of having anemia as
compared to those lactating mothers with husbands who had no education [AOR=0.66; 95% CI:
(0.44-0.99)]. The odd of being anemic in Wworking lactating mothers had awas 292% lower less
risk for anemia as compared to their counter parts [AOR=0.71; 95% CI: (0.63-
0.80)].[AOR=0.78; 95% CI: (0.63-95)]. Those lactating mothers Hhaving a normal maternal
BMI (18.5kg/m2-24.99kg/m
2) were 22% less likely to be anemic as compared to lactating
mother with low BMI (<18.5kg/m2) [AOR=0.78; 95% CI: (0.68-0.89)].was found protective of
anemia [AOR=0.79; 95% CI: (0.63-0.98)]. However, lactating mothers who had BMI 25kg/m2
had a 80% higher risk of developing anemia as compared to undernourished (defined as
BMI<18.5kg/m2) lactating mothers[AOR=1.8; 95% CI: (1.02-3.12)](Table 2). Similarly,
lactating women who are categorized in middle [AOR=0.83; 95% CI: (0.71-0.98)] and rich
wealth quintiles [AOR=0.83; 95% CI: (0.70-0.98)] were each 17% less likely to have anemia as
compared to lactating women in poorer quintiles.
Among reproductive maternal characteristicshealth service factors, family planning use and
antenatal care (ANC) were the significant predictors factors associated withof anemia in lactating
mothers. Lactating mothers who ever used family planning were 2932% less likely to have
anemia as compared to lactating mothers who never used family planning [AOR=0.68; 95% CI:
(0.57- 0.80)].[AOR=0.71; 95% CI: (0.55-0.92)]. Lactating mothers who reported ANC
attendance four times or more for indexed pregnancy were 273% less likely to develop have
anemia as compared to mothers who never attended ANC [AOR=0.73; 95% CI: (0.59-0.91)].
their counterparts [AOR=0.77; 95% CI: (0.62-0.95)] Those lactating mothers who breastfed for
two years were 24% less likely to have anemia as compared to lactating women who breastfed
for one year [AOR=0.76; 95% CI: (0.66-0.87)] (Table 2).
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Page 26 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
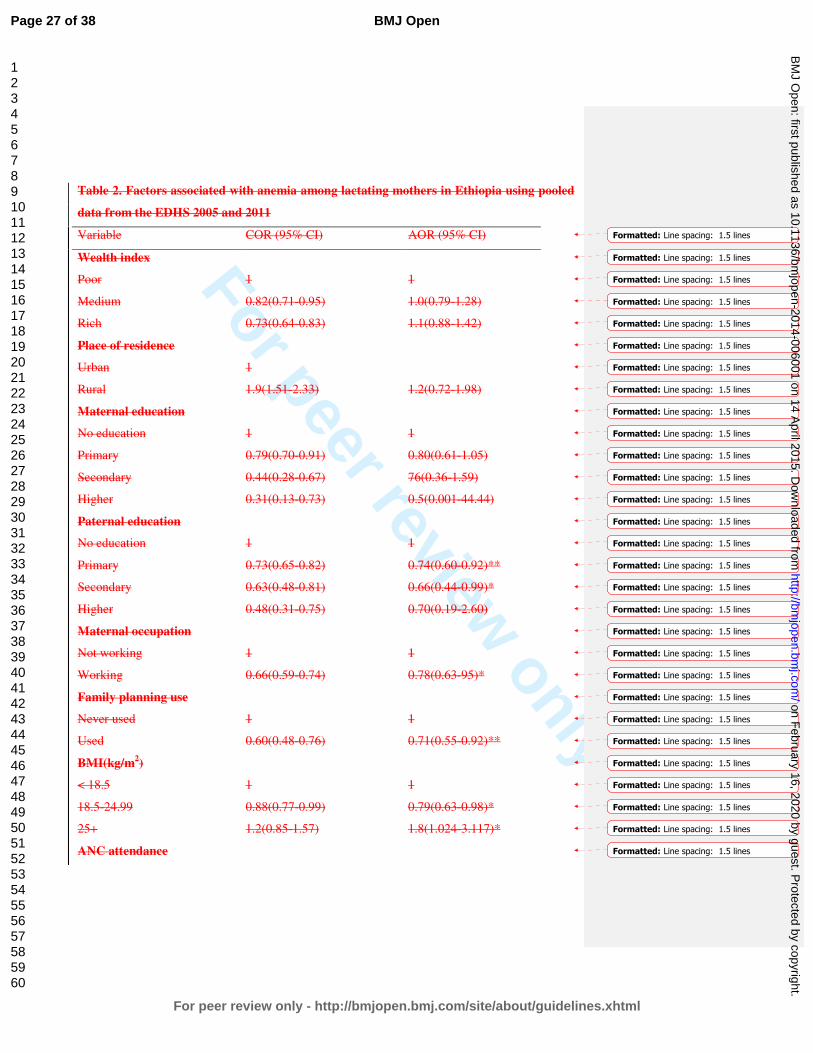
For peer review only
Table 2. Factors associated with anemia among lactating mothers in Ethiopia using pooled
data from the EDHS 2005 and 2011
Variable COR (95% CI) AOR (95% CI)
Wealth index
Poor 1 1
Medium 0.82(0.71-0.95) 1.0(0.79-1.28)
Rich 0.73(0.64-0.83) 1.1(0.88-1.42)
Place of residence
Urban 1
Rural 1.9(1.51-2.33) 1.2(0.72-1.98)
Maternal education
No education 1 1
Primary 0.79(0.70-0.91) 0.80(0.61-1.05)
Secondary 0.44(0.28-0.67) 76(0.36-1.59)
Higher 0.31(0.13-0.73) 0.5(0.001-44.44)
Paternal education
No education 1 1
Primary 0.73(0.65-0.82) 0.74(0.60-0.92)**
Secondary 0.63(0.48-0.81) 0.66(0.44-0.99)*
Higher 0.48(0.31-0.75) 0.70(0.19-2.60)
Maternal occupation
Not working 1 1
Working 0.66(0.59-0.74) 0.78(0.63-95)*
Family planning use
Never used 1 1
Used 0.60(0.48-0.76) 0.71(0.55-0.92)**
BMI(kg/m2)
< 18.5 1 1
18.5-24.99 0.88(0.77-0.99) 0.79(0.63-0.98)*
25+ 1.2(0.85-1.57) 1.8(1.024-3.117)*
ANC attendance
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Page 27 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Not attend 1 1
Attend 0.68(0.55-0.83) 0.77(0.62-0.95)*
*P<0.05 **P<0.001
Discussion
Over one fifth of lactating mothers were anemic in Ethiopia, which is relatively lower as
compared to other developing countries. For example, an Indian study where more than 90% of
lactating mothers have been reported as having anemia in India were reported as anemic14
and .
A study from Zimbabwe showed that about 29.6% of lactating women mothers in Zimbabwe
developed anemia15 which is also higher than found in Ethiopia.
Another study from Myanmar reported an anemia prevalence rate of 60.3% in lactating women,
with 20.3% of lactating mothers having severe anemia16
. Although the prevalence of anemia
among lactating mothers in Ethiopia was relatively low as compared to the above studiesthese
studies, still it remains a is a moderate public health problem according to WHO classification17
.
The relatively better prevalence of anemia in Ethiopia among lactating mothers may be due to
the cultural norms of providing nutritional care to lactating mothers during the postpartum
period. During the post-partum period, lactating mothers are encouraged to rest for 3 to 6 months
and to eat a variety of foods including from animal sources, even during religious fasting
periods.Anemia during lactation has received less attention in the Health Extension Program
which is practiced in Ethiopia. Even though the health extension package of Ethiopia has
nutrition component, it has no much emphasis on prevention of anemia among lactating mothers.
Iron supplementation coverage in Ethiopia remained low among pregnant mothers10
The EDHS
also shows that iron supplementation coverage for pregnant mothers remained low over time,
despite its known contribution for reducing the risk of postpartum hemorrhage 12
. Post-partum
hemorrhage was also found to be one of the risk factors for anemia during the period of
lactation18
. However, the culture of care provided for lactating mothers during the postpartum
period in Ethiopia may contribute to the prevention of anemia.
Although there are common assumptions that pastoralist populations are at a lower risk for
anemia due to their dietary habits and dependence on animal food sources, tThis study showed
that anemia is a widespread problem in the pastoralist communities of Ethiopian Somali and
Afar. The prevalence of anemia in lactating mothers was higherst in the pastoralist regions and
Formatted: Line spacing: 1.5 lines
Formatted: Line spacing: 1.5 lines
Formatted: Space After: 0 pt
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Font: Times New Roman, 12 pt,
Font color: Black
Page 28 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
showed slow decline in these regions from 2005 to 2011. the decrease in prevalence between
2005 and 2011 EDHS was very small. This could be due to the fact that pastoralist communities
are heavily dependent on animal milk as a source of daily food, with poor iron bioavailability19
20. The other reason could be due to low utilization of family planning and antenatal care services
in pastoralist areas10
.
This might be associated with anemia specifically resulting from infection, such as malaria
which is prevalent in those pastoralist areas.
One of the factors determined to be associated with anemia was paternal education. Having a
husband with a higher level of education was found to be protective associated with less odd of
having for anemia among lactating mothers. Those mothers having husbands with education of
primary and secondary levels education were less likely to develop have anemia as compared to
those with husbands who had no education. However, maternal educational status was not
statistically associated with anemia, which is contradictory to many studies from Ethiopia as well
as from abroad 16 21-23
. The absence of association between maternal educational status and
anemia versus the associate with husbands’ educational status and anemia among lactating
mothers might imply that partner education is more influential in preventing anemia. This might
indicate be the one importantce motivator to of involveing husbands in anemia prevention
efforts.
Working Llactating mothers who are working were athad lower risk odd of having anemia as
compared to their counter parts. This might be because working mothers are were earning money
as compared to non-working mothers and the extra income enabled access to purchase more food
items, including animal sources (meat, poultry, fish etc), and increase dietary diversity. Studies
have shown that income growth improves diet diversity which in turn improves micronutrient
intake, including iron 24 25. Similarly, the lactating mothers in the lower wealth groups had
greater odds of anemia as compared to lactating mothers in the higher wealth quintiles. In many
other studies of anemia among reproductive age women, the wealth index was found to be a
statistically significant factor 16 21
. Other studies have also shown that women of low socio-
economic status are at risk for iron deficiency anemia (IDA) in late pregnancy and in the
postpartum period26 27
. Therefore, women’s empowerment through economic interventions and
working status could have a positive contribution towards preventing anemia.
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Font: Times New Roman, 12 pt
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Page 29 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
more empowered as compared to non-employed mothers. Therefore, women’s empowerment
through economic interventions could have a positive contribution toward preventing anemia.
As one strategy for preventing anemia, family planning has been used. This study also supports
the importance of family planning for reducing the risk of anemia. Those lactating mothers who
have ever used family planning (modern or traditional) had a lower risk odd of developing
having anemia as compared to those who had never used family planning. This finding is
consistent with studies from Ethiopia and Timor-Leste which showed that use of family planning
was associated with lower odd of having anemia.21 28.an Ethiopian study on the correlates of
anemia among reproductive age women by Samson and his colleague 21
.
Maternal nutritional status (measured by body mass index) was found to be significantly
associated with anemia. As compared with undernourished lactating mothers (BMI<18.5kg/m2),
being in the normal BMI category (18.5-24.9kg/m2) was negatively associated with a lower odd
of developing having anemia as expected. This finding is similar with others studies29 30
. When a
mother is at risk of deficiency for macronutrients, most likely she is also at risk also other
micronutrient deficiencies such as iron31
. This study found that overweight and obese lactating
mothers were at an 80% higher risk for having anemia. A study from Mexico found that being
overweight did not necessarily diminish the risk of anemia; rather diet quality was the determiner
28. A study by Cepeda-Lopez and his colleagues explains lower iron status among obese
individuals explained by lower absorption of iron due to obesity related inflammation which
affect regulation of Hepcidin. Hepcidin levels are higher in obese individuals and are linked to
subclinical inflammation which affect iron absorption negatively 28.
ANC attendance was found to be a protective associated factor with for anemia among lactating
mothers. This is most likely due to the fact that during ANC attendance mothers have been
advised to take iron supplements according to the Ethiopian micronutrient guideline and
instructed to consume different sources of iron rich food items32. Therefore, improving iron
status during pregnancy also helps to prevent anemia during the lactation period.
In many studies of anemia among reproductive age women, the wealth index was found to be a
statistically significant factor 13 19. However, in this study the wealth index was not found to be a
statistically significant factor.
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Formatted: Not Highlight
Page 30 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Anemia is a public health problem among lactating mothers in Ethiopia. There are regional
disparities regarding the prevalence of anemia, with the highest prevalence found in pastoralist
regions of Ethiopian Somali and Afar. Promoting partner education, improving maternal
nutritional status, creating behavior change among lactating mothers to use family planning and
attend antenatal care services at health facilities are recommended interventions to reduce the
prevalence of anemia among lactating women in Ethiopia.
Conclusion
Anemia is a public health problem among lactating mothers in Ethiopia. There are regional
disparities regarding the prevalence of anemia, with the highest rates found in pastoralist regions
of Ethiopian Somail and Afar.. Promoting partner education, improving maternal nutritional
status, creating behavior change among lactating mothers to use family planning and attend
antenatal care services at health facilities are recommended interventions to reduce the
prevalence of anemia among lactating women in Ethiopia. Factors such as husband’s educational
status, family planning use, BMI, maternal occupational status and ANC attendance were
identified as associated factors for anemia among lactating mothers. Improving BMI, promotion
of family planning and ANC are recommended interventions to prevent anemia. Involvement of
males in prevention of anemia should be considered. Attention should also be given to
preventing anemia among lactating mothers through the Health Extension Package and at any
health service delivery contact for lactating mothers.
Competing interests
The authors declare that they have no competing interests.
Funding statement
This research received no specific grant from any funding agency in the public, commercial or
not-for-profit sectors'
Authors’ contributions
YL and DH conceived the idea. YL analyzed and interpreted the data and critically reviewed the
manuscript. SB assisted in critically reviewing the manuscript. DH drafted the manuscript,
Page 31 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
assisted in the data analysis and interpretation and critically reviewed the manuscript. All authors
reviewed and approved the manuscript.
Acknowledgements
The authors acknowledge DHS Measure for granting the data freely. We are also grateful to
thank Lianna Tabar, country representative of KHI-E, for her professional language editing and
reviewing the manuscript.
References
1. WHO. The world health report. Reducing risks, promoting healthy life. Geneva, World Health
Organization, 2002., 2002.
2. Whitney E, Rolfes SR. Understanding Nutrition. In: Adams P, editor. Eleventh Edition ed. United States
of America: Thomson Learning Academic Resource Center, 2008.
3. Domell V, Lonnerdal B, Dewey K, Cohen R, Hernell O. Iron zinc and copper concentrations in breast
milk are independent of maternal status. American Journal of clinical nutrition 2004;79(1):111-
15.
4. Bodnar L, Scanlon K, Freedman D, Siega–Riz A, Cogswell M. High prevalence of postpartum anaemia
amongLow income women in the United States. J. obstet. Gynecol 2001;185:4348-53.
5. SSERUNJOGI L, SCHEUT2 F, WHYTE SR. Postnatal anaemia: neglected problems and missed
opportunities in Uganda. HEALTH POLICY AND PLANNING 2003;18(2):225-31.
6. Beard JL, Hendricks MK, Perez EM, Murray-Kolb LE, Berg A, Vernon-Feagans L, et al. Maternal Iron
Deficiency Anemia Affects Postpartum Emotions and Cognition. Journal of Nutrition
2005;135:267–72.
7. Ross J, homas E. Iron deficiency anemia and maternal mortality. PROFILES 3 working notes series no.
3. Academy for Education Development, Washington D.C., 1996.
8. Brabin BJ, Hakimin M, Pelletier D. An Analysis of Anemia and Pregnancy-Related Maternal Mortality.
The Journal of Nutrition 2001;131:604S-15S.
9. Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, Lozano R, et al. A systematic analysis of
global anemia burden from 1990 to 2010. Blood 2014;123(5).
10. Central Statistical Agency (CSA) Ethiopia. Demographic and Health Survey 2011. Addis Ababa,
Ethiopia and Calverton, Maryland, USA: CSA and ORC Macro. 2011.
11. Central Statistical Agency(CSA). Demographic and Health Survey 2005. Addis Ababa, Ethiopia and
Calverton, Maryland, USA: CSA and ORC Macro, 2005.
12. CentralStatisticalAgency(CSA) EM. Demographic and Health Survey 2011. Addis Ababa, Ethiopia and
Calverton, Maryland, USA: CSA and ORC Macro., 2011.
13. Peter C, Jack V. Automated variable selection methods for logistic regression produced unstable
models for predicting acute myocardial infarction mortality. Journal of Clinical Epidemiology
2004;57:1138-46.
14. Agarwal KN, Agarwal DK, Sharma A, Sharma K, Prasad K, Kalita MC, et al. Prevalence of anaemia in
pregnant & lactating women in India. Indian J Med Res 2006;124:173-84.
Page 32 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
15. Sikosana PL, Bhebhe S, Katuli S. A prevalence survey of iron deficiency and iron deficiency anaemia in
pregnant and lactating women, adult males and pre-school children in Zimbabwe. Cent Afr J
Med 1998;44(12):297-305.
16. Zhao A, Zhang Y, Li B, Wang P, Li J, Xue Y, et al. Prevalence of Anemia and Its Risk Factors Among
Lactating Mothers in Myanmar. Am J Trop Med Hyg 2014;doi: 10.4269/ajtmh.13-0660.
17. WHO. Worldwide prevalence of anaemia 1993-2005 : WHO global database on anaemia / Edited by
Bruno de Benoist, Erin McLean, Ines Egli and Mary Cogswell.
, 2008.
18. World Health Organization (WHO). Recommendations for the Prevention of Postpartum
Haemorrhage (summary of results from a WHO technical consultation, October 2006) Geneva:
WHO 2007.
19. Kibangou I, Bouhallab S, Henry G, Bureau F, Allouche S, Blais A, et al. Milk proteins and iron
absorption: contrasting effects of different caseinophosphopeptides. Pediatrics Research 2005
58(4):731-34.
20. Belachew T. Human Nutrition lecture note series for Health sciences students: JImma Univesity
2005:pp 229.
21. Gebremedhin S, Enquselassie F. Correlates of anemia among women of reproductive age in Ethiopia:
Evidence from Ethiopian DHS 2005. Ethiopian Journal of Health Development 2011;25(1):22-30.
22. Haidar J. Prevalence of Anaemia, Deficiencies of Iron and Folic Acid and Their Determinants in
Ethiopian Women. J HEALTH POPUL NUTR 2010;28(4):359-68.
23. Okwu GN. Studies on the predisposing factors of iron deficiency anaemia among lactating women in
Owerri, Nigeria International Research Journal of Biochemistry and Bioinformatics
2011;1(11):304-09.
24. Taruvinga A, Muchenje V, Mushunje A. Determinants of rural household dietary diversity: The case
of Amatole and Nyandeni districts, South Africa International Journal of Development and
Sustainability 2013;2 (4).
25. Doan D. Does income growth improve diet diversity in China?Selected Paper prepared for
presentation at the 58 the AARES Annual Conference, Port Macquarie, New South Wales, 4-7
February 2014 2014.
26. Bodnar L, Cogswell M, Scanlon K. Low income postpartum women are at risk of iron deficiency.
Journal of Nutrition 2002;132:2298–302.
27. Sadeghian M, Fatourechi A, Lesanpezeshki M, Ahmadnezhad E. Prevalence of Anemia and Correlated
Factorsin the Reproductive Age Women in Rural Areas of Tabas. Journal of Family and
Reproductive Health 2013;7(3):143.
28. Lovermail AA, Hartman M, Chia KS, Heymann DL. Demographic and Spatial Predictors of Anemia in
Women of Reproductive Age in Timor-Leste: Implications for Health Program Prioritization. PLoS
ONE 2013;9(3):e91252.
29. Eckhardt CL, Torheim LE, Monterrubio E, Barquera S, Ruel M. Overweight and Obese Women Remain
at Risk for Anemia in Countries Undergoing the Nutrition Transition. THe FASEB Journal
2006;20:A986-A87.
30. Cepeda-Lopez A, Aeberli I, Zimmermann M. Does obesity increase risk for iron deficiency? A review
of the literature and the potential mechanisms. Int J Vitam Nutr Res 2010;80(4-5):263-70.
31. Blumfield M, Hure A, MacDonald-Wicks L, Smith R, Simpson S, Raubenheimer D, et al. The
association between the macronutrient content of maternal diet and the adequacy of
micronutrients during pregnancy in the Women and Their Children’s Health (WATCH) study.
Nutrients 2012;4(12):1958-76.
Page 33 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
32. FMOH. NATIONAL GUIDELINE FOR CONTROL AND PREVENTION OF MICRONUTRIENT DEFICIENCIES,
2004.
Page 34 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
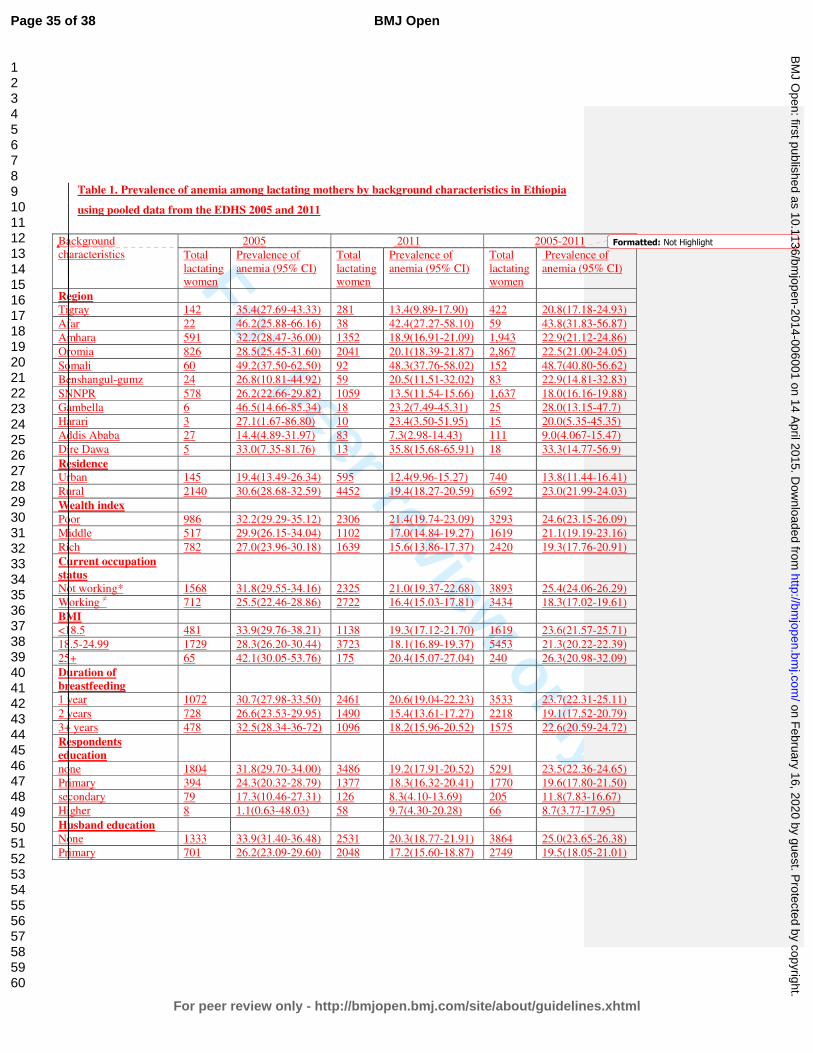
For peer review only
Table 1. Prevalence of anemia among lactating mothers by background characteristics in Ethiopia
using pooled data from the EDHS 2005 and 2011
Background
characteristics
2005 2011 2005-2011
Total
lactating women
Prevalence of
anemia (95% CI)
Total
lactating women
Prevalence of
anemia (95% CI)
Total
lactating women
Prevalence of
anemia (95% CI)
Region
Tigray 142 35.4(27.69-43.33) 281 13.4(9.89-17.90) 422 20.8(17.18-24.93)
Afar 22 46.2(25.88-66.16) 38 42.4(27.27-58.10) 59 43.8(31.83-56.87)
Amhara 591 32.2(28.47-36.00) 1352 18.9(16.91-21.09) 1,943 22.9(21.12-24.86)
Oromia 826 28.5(25.45-31.60) 2041 20.1(18.39-21.87) 2,867 22.5(21.00-24.05)
Somali 60 49.2(37.50-62.50) 92 48.3(37.76-58.02) 152 48.7(40.80-56.62)
Benshangul-gumz 24 26.8(10.81-44.92) 59 20.5(11.51-32.02) 83 22.9(14.81-32.83)
SNNPR 578 26.2(22.66-29.82) 1059 13.5(11.54-15.66) 1,637 18.0(16.16-19.88)
Gambella 6 46.5(14.66-85.34) 18 23.2(7.49-45.31) 25 28.0(13.15-47.7)
Harari 3 27.1(1.67-86.80) 10 23.4(3.50-51.95) 15 20.0(5.35-45.35)
Addis Ababa 27 14.4(4.89-31.97) 83 7.3(2.98-14.43) 111 9.0(4.067-15.47)
Dire Dawa 5 33.0(7.35-81.76) 13 35.8(15.68-65.91) 18 33.3(14.77-56.9)
Residence
Urban 145 19.4(13.49-26.34) 595 12.4(9.96-15.27) 740 13.8(11.44-16.41)
Rural 2140 30.6(28.68-32.59) 4452 19.4(18.27-20.59) 6592 23.0(21.99-24.03)
Wealth index
Poor 986 32.2(29.29-35.12) 2306 21.4(19.74-23.09) 3293 24.6(23.15-26.09)
Middle 517 29.9(26.15-34.04) 1102 17.0(14.84-19.27) 1619 21.1(19.19-23.16)
Rich 782 27.0(23.96-30.18) 1639 15.6(13.86-17.37) 2420 19.3(17.76-20.91)
Current occupation
status
Not working* 1568 31.8(29.55-34.16) 2325 21.0(19.37-22.68) 3893 25.4(24.06-26.29)
Working ≠ 712 25.5(22.46-28.86) 2722 16.4(15.03-17.81) 3434 18.3(17.02-19.61)
BMI
<18.5 481 33.9(29.76-38.21) 1138 19.3(17.12-21.70) 1619 23.6(21.57-25.71)
18.5-24.99 1729 28.3(26.20-30.44) 3723 18.1(16.89-19.37) 5453 21.3(20.22-22.39)
25+ 65 42.1(30.05-53.76) 175 20.4(15.07-27.04) 240 26.3(20.98-32.09)
Duration of
breastfeeding
1 year 1072 30.7(27.98-33.50) 2461 20.6(19.04-22.23) 3533 23.7(22.31-25.11)
2 years 728 26.6(23.53-29.95) 1490 15.4(13.61-17.27) 2218 19.1(17.52-20.79)
3+ years 478 32.5(28.34-36-72) 1096 18.2(15.96-20.52) 1575 22.6(20.59-24.72)
Respondents
education
none 1804 31.8(29.70-34.00) 3486 19.2(17.91-20.52) 5291 23.5(22.36-24.65)
Primary 394 24.3(20.32-28.79) 1377 18.3(16.32-20.41) 1770 19.6(17.80-21.50)
secondary 79 17.3(10.46-27.31) 126 8.3(4.10-13.69) 205 11.8(7.83-16.67)
Higher 8 1.1(0.63-48.03) 58 9.7(4.30-20.28) 66 8.7(3.77-17.95)
Husband education
None 1333 33.9(31.40-36.48) 2531 20.3(18.77-21.91) 3864 25.0(23.65-26.38)
Primary 701 26.2(23.09-29.60) 2048 17.2(15.60-18.87) 2749 19.5(18.05-21.01)
Formatted: Not Highlight
Page 35 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Secondary 199 20.7(15.41-26.64) 238 14.3(10.26-19.17) 437 17.2(13.84-20.92)
Higher 23 14.8(3.43-31.53) 147 13.7(8.75-19.88) 170 13.8(8.99-19.30)
Family planning
Never use 1775 32.1(29.97-34.31) 2889 21.2(19.72-22.70) 4663 25.4(24.16-26.66)
Ever use 15 16.4(2.30-37.52) 2158 14.9(13.46-16.47) 2173 14.9(13.46.16.45)
ANC use
Never 1636 32.0(29.80-34.32) 2977 20.4(18.97-21-87) 4613 24.5(23.27-25.75)
1-3 386 27.7(23.43-32.35) 1208 18.4(16.27-20.64) 1594 20.6(18.65-22.62)
4+ 260 18.9(14.44-23.95) 845 12.6(10.44-14.91) 1105 14.1(12.16-16.27)
Iron supplement
during pregnancy
No 2046 30.1(28.15-32.12) 4196 18.8(17.64-20.01) 6242 22.5(21.47-23.54)
Yes 236 27.1(21.74-33.06) 840 16.9(14.48-19.55) 1076 19.2(16.97-21.68)
Parity
1-4 1293 28.9(26.50-31.44) 3111 18.1(16.77-19.48) 4404 21.3(20.11-22.53)
5-9 903 30.5(27.52-33.52) 1739 19.6(17.79-21.53) 2642 23.3(21.73-24.96)
10+ 89 37.1(27.53-47.46) 197 17.0(12.02-12.46) 287 23.2(18.72-28.50)
Total 2285 29.9(28.04-31.79) 5047 18.5(17.45-19.60) 7332 22.1(21.13-23.03) ANC-Antenatal Care, BMI-Body Mass Index, *those mothers who currently work to earn money, ≠ those mothers
who do not currently engage in any type of formal work to earn money.
Table 12. Factors associated with anemia among lactating mothers in Ethiopia using pooled
data from the EDHS 2005 and 2011 Variables 2005 2011 2005-2011
COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI
Occupation
Not working* 1.00 1.00 1.00 1.00 1.00 1.00
Working≠ 0.82(0.66-1.00) 0.83(0.64-1.06) 0.62(0.54- 0.71) 0.68(0.58-0.78) 0.64(0.57-0.72) 0.71(0.63-0.80)
Wealth index
Poor 1.00 1.00 1.00 1.00 1.00 1.00
Middle 0.71(0.54-0.92) 0.82(0.61-1.10) 0.74(0.61- 0.89) 0.85(0.69-1.04) 0.74(0.64-0.87) 0.83(0.71-0.98)
Rich 0.66(0.53-0.82) 0.91(0.68-1.22) 0.62(0.52-0.72) 0.80(0.65-0.97) 0.65(0.57-0.73) 0.83(0.70-0.98)
FP use
Never used 1.00 1.00 1.00 1.00 1.00 1.00
Ever used 0.37(0.11-1.28) 0.51(0.14-1.91) 0.54(0.46-0.63) 0.69(0.58-0.82) 0.48(0.41-0.55) 0.68(0.57-0.80)
ANC attended
Never 1.00 1.00 1.00 1.00 1.00 1.00
1-3 0.78(0.59-1.03) 0.94(0.66-1.33) 0.78(0.59-1.00) 1.00(0.83-1.2) 0.81(0.71-0.94) 0.99(0.84-1.16)
4+ 0.55(0.41-0.74) 0.82(0.53-1.28) 0.55(0.41-0.74) 0.71(0.55-0.92) 0.52(0.44-0.61) 0.73(0.59-0.91)
Husband
education
None 1.00 1.00 1.00 1.00 1.00 1.00
Primary 0.77(0.61-0.96) 0.77(0.58-1.01) 0.69(0.59-0.80) 0.80(0.67-0.94) 0.69(0.61-0.78) 0.79(0.68-0.91)
Secondary 0.55(0.39-0.77) 0.83(0.50-1.38) 0.64(0.48-0.87) 0.81(0.58-1.14) 0.62(0.49-0.77) 0.83(0.62-1.09)
Higher 0.58(0.26-1.30) 0.50(0.73-3.40) 0.72(0.49-1.0) 0.96(0.61-1.52) 0.64(0.46-0.90) 0.94(0.61-1.45)
BMI*
<18.5 1.00 1.00 1.00 1.00 1.00 1.00
18.5-24.99 0.74(0.59-0.92) 0.76(0.59-0.99) 0.74(0.64-0.86) 0.79(0.68-0.93) 0.76(0.67-0.86) 0.78(0.68-0.89)
Field Code Changed
Formatted: Not Highlight
Page 36 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
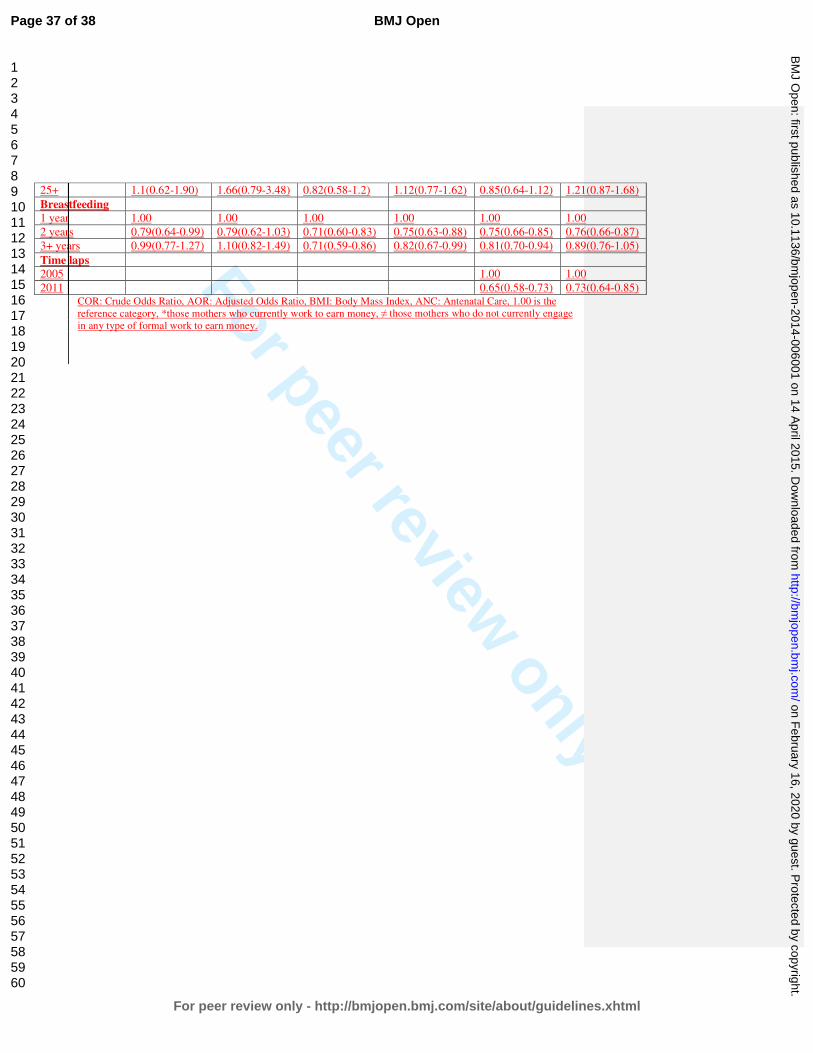
For peer review only
25+ 1.1(0.62-1.90) 1.66(0.79-3.48) 0.82(0.58-1.2) 1.12(0.77-1.62) 0.85(0.64-1.12) 1.21(0.87-1.68)
Breastfeeding
1 year 1.00 1.00 1.00 1.00 1.00 1.00
2 years 0.79(0.64-0.99) 0.79(0.62-1.03) 0.71(0.60-0.83) 0.75(0.63-0.88) 0.75(0.66-0.85) 0.76(0.66-0.87)
3+ years 0.99(0.77-1.27) 1.10(0.82-1.49) 0.71(0.59-0.86) 0.82(0.67-0.99) 0.81(0.70-0.94) 0.89(0.76-1.05)
Time laps
2005 1.00 1.00
2011 0.65(0.58-0.73) 0.73(0.64-0.85) COR: Crude Odds Ratio, AOR: Adjusted Odds Ratio, BMI: Body Mass Index, ANC: Antenatal Care, 1.00 is the
reference category, *those mothers who currently work to earn money, ≠ those mothers who do not currently engage
in any type of formal work to earn money.
Page 37 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
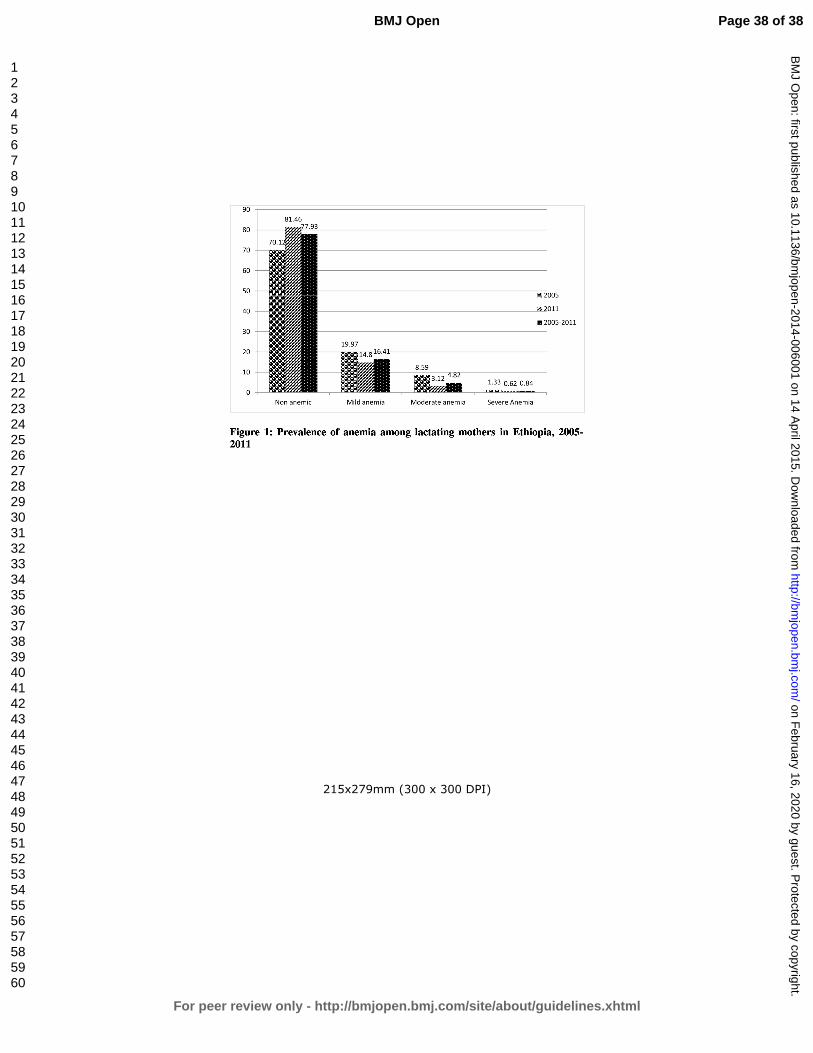
For peer review only
215x279mm (300 x 300 DPI)
Page 38 of 38
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Anemia prevalence and associated factors among lactating mothers in Ethiopia: Evidence from the 2005 and 2011
demographic and health surveys
Journal: BMJ Open
Manuscript ID: bmjopen-2014-006001.R2
Article Type: Research
Date Submitted by the Author: 27-Dec-2014
Complete List of Authors: Tarekegn, Yihunie; Ethiopian Public Helth Association, Project management Biadgilign, Sibhatu; Independent public health consultants, Addis Ababa, Ethiopia,
Haile, Demewoz; Madawalabu University,
<b>Primary Subject Heading</b>:
Public health
Secondary Subject Heading: Nutrition and metabolism, Public health, Health policy
Keywords: Anaemia < HAEMATOLOGY, NUTRITION & DIETETICS, Nutritional support < ONCOLOGY
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on F
ebruary 16, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006001 on 14 April 2015. D
ownloaded from
For peer review only
Anemia prevalence and associated factors among lactating mothers in Ethiopia: Evidence
from the 2005 and 2011 demographic and health surveys
Yihunie Lakew1, Sibhatu Biadgilign
2, Demewoz Haile
3*
1 Ethiopian Public Health Association, Addis Ababa, Ethiopia
2 Independent Public Health Consultant, Addis Ababa, Ethiopia
3 Department of Public Health, College of Medicine and Health sciences, Madawalabu
University, Ethiopia
Email address
Yihunie Lakew – [email protected]
Sibhatu Biadgilign- [email protected]
Demewoz Haile–[email protected]
*Corresponding author
Address of corresponding author
Department of Public Health
College of Medicine and Health sciences
Madawalabu University, Ethiopia
Bale Goba, P.O.Box 302
Running title: Factors associated with anemia among lactating mothers in Ethiopia
Key words: Lactating mothers, anemia, Ethiopia,
Word count: 2388
Page 1 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Abstract
Objective: To identify factors associated with anemia among lactating mothers in Ethiopia.
Design: A cross-sectional secondary data analysis pooled from two rounds of the 2005 and 2011
Ethiopian demographic and health survey (EDHS) was used. Multivariable logistic regression
model was applied to determine the factors associated with anemia.
Population: A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047 from EDHS
2011) were included from 11 administrative states of Ethiopia.
Main outcome measures: Lactating mothers considered as anemic if hemoglobin level <12
gram per deciliter.
Results: The overall prevalence of anemia among lactating mothers was 22.1% [95% CI: (21.13-
23.03)]. The highest prevalence was 48.7% [95% CI: (40.80-56.62)] found in Somali region,
followed by 43.8% [95% CI: (31.83-56.87)] in Afar region. The multivariable statistical model
showed that lactating mothers who had husbands attended primary education [AOR=0.79; 95%
CI: (0.68-0.91)], had been working in the last 12 months preceding the survey [AOR=0.71; 95%
CI: (0.63-0.80)],, had normal maternal body mass index (BMI) from 18.5kg/m2 to 24.99kg/m
2
[AOR=0.78; 95% CI: (0.68-0.89)], middle wealth index [AOR=0.83; 95% CI: (0.71-0.98)] and
rich wealth index [AOR=0.83; 95% CI: (0.70-0.98)], ever use of family planning [AOR=0.68;
95% CI: (0.57-0.80)], attending antenatal care (ANC) for indexed pregnancy four times or more
[AOR=0.73; 95% CI: (0.59-0.91)], experienced time variation between two surveys [AOR=0.73;
95%CI: (0.64-0.85)] and who breastfed for two years [AOR=0.76; 95% CI: (0.66-0.87)] were
associated with lower odd of being anemic.
Conclusion: Anemia is highly prevalent among lactating mothers, particularly among pastoralist
communities of Somali and Afar. Promoting partner education, improving maternal nutritional
status, creating behavioral change to use family planning and ANC services at health facilities
are recommended interventions to reduce the prevalence of anemia among lactating mothers in
Ethiopia.
Page 2 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
ARTICLE SUMMARY
Article focus
• Anemia is a serious nutritional problem, primarily affecting women of reproductive age
and children, and remains a major challenge in developing countries. In Ethiopia, more
than 20% of women in the reproductive age are anemic.
• Lactating mothers are among vulnerable groups with little information regarding social
determinants of anemia.
Key messages
• Anemia is a public health problem among lactating mothers in Ethiopia, with the highest
prevalence found in pastoralist regions of Somali and Afar.
• A statistically significant reduction of anemia prevalence among lactating mothers was
observed from 2005 to 2011.
• Being in middle and rich wealth quintiles, breastfeeding for two years, currently working,
normal body mass index, husbands’ primary education, ever use of family planning and
antenatal care attendance for four or more visits were factors associated with lower odds
of having anemia.
Strength and Limitations
• The study attempted to identify factors associated with laboratory confirmed anemia
among lactating mothers at the national level. The study findings can be used to inform
policy and program actions.
• Some regions from which data was collected had small sample size. So that it should be
interpreted in caution. This study also shares the limitation of cross-sectional design
which makes difficult to demonstrate cause and effect relationships.
Page 3 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Introduction
Anemia is a serious nutrition problem affecting millions in developing countries, and remains a
major challenge for human health, social and economic development1. Lactating mothers are
among vulnerable groups of anemia. During the period of lactation, mothers are susceptible to
anemia due to maternal iron depletion and blood loss during childbirth2. Studies have shown that
though breast milk is not a good source of iron, the concentration of iron in breast milk is
independent of maternal iron status. This showed that the quality of breast milk is maintained at
the expense of maternal stores2 3.
Postpartum anemia has been found highest in mothers who were anemic during pregnancy4.
Furthermore, lactating mothers are highly susceptible to iron depletion if they have not had
enough energy and nutrient intake in their diets. Lactating mothers begin the postnatal period
after having iron depleted through the continuum from pregnancy to childbearing 5. A study from
South Africa showed that iron status was associated with depression, stress, and cognitive
functioning in poor African mothers during the postpartum period6. In a meta-analysis of
observational and intervention trials, Ross and Thomas, found that approximately 20% of the
maternal mortality seen in sub-Saharan Africa and South Asia was attributable to anemia that
was primarily the result of iron deficiency7.
Ethiopia is one of the countries in sub-Saharan Africa affected by anemia and it contributes to
high rates of maternal, infant and child mortality globally8 9
. In Ethiopia, the maternal mortality
ratio was 676 maternal deaths per 100,000 live births10which is one of the highest in the world.
The country has considerably high infant and under 5 mortality rates that account for 59 and 88
deaths per 1000 live births, respectively 10.
Anemia testing was included in the two rounds of the Ethiopian demographic and health surveys
(EDHS). The prevalence of anemia among lactating mothers was 29.9% in 2005 and 18.5% in
201110,11. It was 30.6% in 2005 and 22% in 2011 among pregnant women and 23.9% in 2005
and 15% in 2011 among women neither non-pregnant nor lactating. This shows that a relatively
higher prevalence of anemia was found among Ethiopian pregnant and lactating mothers.
However, little information is available regarding socio-economic factors associated with anemia
Page 4 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
among lactating mothers. This study aimed to identify factors associated with anemia among
lactating mothers in Ethiopia using the pooled data of EDHS 2005 and 2011.
Methods
Data type and study design
This study is an in-depth analysis to identify factors associated with anemia among lactating
mothers based on cross-sectional secondary data of the EDHS 2005 and 2011 datasets. Both the
2005 and 2011 EDHS samples were selected using a stratified, two-stage cluster sampling
design. All women age 15-49 who were usual residents or who slept in the selected households
the night before the survey were eligible. The EDHS data include a women’s questionnaire that
measures socio-demographic characteristics of the mothers, information on reproductive health
and service use behaviours, as well as HIV and anemia test. The tool was pretested and translated
in to three local languages - Amharic, Oromifa and Tigregna. The EDHS was designed to
provide population and health indicators at national and regional levels. The survey is conducted
in every five years. The detailed methodology is found elsewhere10 11
.
Data Extraction
Both EDHS 2005 and 2011 data were downloaded with permission from the Measure DHS
website in SPSS format. After reviewing the detailed data coding, further data cleaning and
recoding was completed. A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047
from EDHS 2011) were included in the analysis. Based on published literature, information on a
wide-range of socio-demographic and economic variables, health service related factors and
anemia level indicators were extracted. The chosen variables were region, residence, wealth
index, occupation, BMI, duration of breastfeeding, respondent’s education, husband’s education,
family planning use, iron tablet supplementation during pregnancy, time variation between two
surveys, marital status, age, parity and antenatal care attendance.
Measurement of variables
In both rounds of the EDHS, haemoglobin analysis was carried out onsite using a battery-
operated portable HemoCue analyzer for all anemia samples. The raw measured values of
haemoglobin were obtained using the HemoCue instrument and adjusted for altitude and
Page 5 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
smoking status10. Lactating mothers considered as anemic if hemoglobin level <12 gram per
deciliter. Haemoglobin (Hb) level of anemia was measured in g/dl, operationalised as a
categorical variable by predefined cut-off points for mild, moderate and severe anemia
recommended by the WHO for women above age 15 years. For this analysis, anemia was re-
categorized as anemic and non-anemic from prior classifications in levels (no, mild, moderate,
severe). Antenatal care (ANC) attendance referred to when women get services during
pregnancy according to the WHO recommendation of at least four ANC visits for low-risk
pregnant women. The frequency of the ANC visit is measured by asking the respondent to recall
how many times she had attended for the indexed child. Occupational status was defined as non-
working and working which comprises of professional/technical/managerial, clerical, sales and
services, skilled manual, unskilled manual and agriculture classifications. BMI (kg/m2) was
categorized using standard WHO classification into underweight <18.5 kg/m2, normal 18.5–24.9
kg/m2, overweight 25.0+. Parity, defined as the number of children ever born, was categorised as
1-4, 5-9 and 10+. The wealth index constructed from household assets and characteristics
available in both surveys to categorise individuals into wealth quintiles (poorest, poorer, middle,
rich and richest) was used. However, to make it more sensible and understandable, wealth index
was re-categorized into three groups (poor, middle and rich) to give more meaningful
interpretations and suite for recommendations.
Statistical analysis
For this study, the 2005 and 2011 EDHS data were pooled to achieve high power for detecting
the associated factors. Weighted proportions and odds ratios are presented to compromise
sampling probabilities. Sample weights were applied in order to compensate for the unequal
probability of selection between the strata that has been geographically defined as well as for
non-responses. A detailed explanation of the weighting procedure can be found in the EDHS
methodology report10. We used “svy” in STATA version 11 to weight the survey data and do the
analyses.
Descriptive statistics were used to show the prevalence of anemia among lactating mothers
varying by background characteristics. Binary and multivariable logistic regression statistical
analysis was carried out to determine the factors associated with anemia among lactating
mothers. Variables found statistically significant at p-value <0.25 during bivariate analysis were
Page 6 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
analyzed in the multivariable logistic regression model12. This p-value cut off point prevented
removing variables that would potentially have an effect during multivariable analysis. Both
crude and adjusted odds ratios (OR) were reported with 95% confidence interval (CI). Variables
at p-value <0.05 were considered statistically significant in the multivariable logistic regression
model.
Ethical statements
The data were downloaded and used after communicating the purpose of the analysis and
receiving permission from Measure DHS Organization. The original EDHS data were collected
in accordance with international and national ethical guidelines.
Results
Majority of respondents (86%) were from rural. Nearly 60% of lactating mothers were Christian
followers followed by 38% of Muslims. The mean age of respondents was 28.4 with SD 6.8. The
overall prevalence of anemia among lactating mothers during 2005 to 2011 was found to be
22.1% (95% CI: 21.13-23.03). The prevalence of anemia for the years 2005 and 2011 was 29.9%
[95% CI: (28.04-31.79)] and 18.5% [95% CI: 17.45-19.60)], respectively. The prevalence was
13.8% [95% CI: (11.44-16.41)] in urban areas and 23% [95% CI: (21.99-24.03)] in rural areas.
In the period 2005 to 2011, the highest prevalence of anemia among lactating mothers was
48.7% [95%CI: (40.80-56.62)] found in Somali region, while the lowest prevalence was 9.0%
[95%CI: (4.07-15.47)] reported in Addis Ababa. In the period 2005 to 2011, the prevalence of
anemia in lactating mothers was consistently higher among those in the poor wealth index group,
not currently working, with BMI greater or equal to 25 kg/m2, one year duration of
breastfeeding, never educated, never used ANC, never used family planning services, no iron
tablet supplement during pregnancy, and with higher parity. A significant reduction in the
prevalence of anemia among lactating mothers was observed in all background variables from
2005 to 2011(Table 1). Figure 1 shows the classification of anemia in terms of its detailed
parameter.
In the bivariate step of our analysis, age and marital status were not statistically significant in the
data from both individual surveys and pooled data with the cut-off point p<0.25. The variable
Page 7 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
associated with lower odd of being anemic for the 2005 data was normal BMI, whereas for the
2011 data the variables were working status, wealth index, use of family planning, ANC
attendance for indexed pregnancy, husband’s education, maternal BMI and duration of
breastfeeding.
In the final multivariable model using pooled data, variables which significantly associated with
anemia for lactating mothers were working status, wealth index, use of family planning, ANC
attendance for indexed pregnancy, husband’s education, maternal BMI, time variation in the two
surveys, and durations of breastfeeding.
Paternal educational status was found to be a predictor of anemia among lactating mothers.
Those lactating mothers who had husbands who attended primary education were at 21% less
likely to have anemia as compared to those mothers who had husbands with no education
[AOR=0.79; 95% CI: (0.68-0.91)]. The odd of being anemic in working lactating mothers was
29% less as compared to their counter parts [AOR=0.71; 95% CI: (0.63-0.80)]. Those lactating
mothers having a normal maternal BMI (18.5kg/m2-24.99kg/m
2) were 22% less likely to be
anemic as compared to lactating mother with low BMI (<18.5kg/m2) [AOR=0.78; 95% CI:
(0.68-0.89)]. Similarly, lactating women who are categorized in middle [AOR=0.83; 95% CI:
(0.71-0.98)] and rich wealth index [AOR=0.83; 95% CI: (0.70-0.98)] were each 17% less likely
to have anemia as compared to lactating women in poorer wealth index.
Among reproductive characteristics, family planning use and antenatal care (ANC) were the
significant factors associated with anemia in lactating mothers. Lactating mothers who ever used
family planning were 32% less likely to have anemia as compared to lactating mothers who
never used family planning [AOR=0.68; 95% CI: (0.57- 0.80)]. Lactating mothers who reported
ANC attendance four times or more for indexed pregnancy were 27% less likely to have anemia
as compared to mothers who never attended ANC [AOR=0.73; 95% CI: (0.59-0.91)]. Those
lactating mothers who breastfed for two years were 24% less likely to have anemia as compared
to lactating women who breastfed for one year [AOR=0.76; 95% CI: (0.66-0.87)] (Table 2).
Page 8 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Discussion
Over one fifth of lactating mothers were anemic in Ethiopia, which is lower as compared to other
developing countries. For example, 66.0% of lactating mothers have been reported as having
anemia in India13 and 43.8 % of lactating mothers in Kenya had a hemoglobin level <12 g/dl
14.
Another study from Myanmar reported an anemia prevalence rate of 60.3% in lactating women,
with 20.3% of lactating mothers having severe anemia15. Although the prevalence of anemia
among lactating mothers in Ethiopia was relatively low as compared to these studies, it remains a
public health problem according to WHO classification16. The relatively better prevalence of
anemia in Ethiopia among lactating mothers may be due to the cultural norms of providing
nutritional care to lactating mothers during the postpartum period. During the postpartum period,
lactating mothers are encouraged to rest for 3 to 6 months and to eat a variety of foods including
animal sources, even during religious fasting periods. Iron supplementation coverage in Ethiopia
remained low among pregnant mothers10, despite its known contribution for reducing the risk of
postpartum hemorrhage17. Postpartum hemorrhage was also found to be one of the risk factors
for anemia during the period of lactation17.
This study showed that anemia is a widespread problem in the pastoralist communities of Somali
and Afar. The prevalence of anemia in lactating mothers was higher in the pastoralist regions and
showed slow decline in these regions from 2005 to 2011. This could be due to the fact that
pastoralist communities are heavily dependent on animal milk as a source of daily food, with
poor iron bioavailability18 19
. The other reason could be due to low utilization of family planning
and antenatal care services in pastoralist areas10.
One of the factors determined to be associated with anemia was paternal education. Having a
husband with a higher level of education was found to be associated with less odd of having
anemia among lactating mothers. This could be due to the fact that those educated husbands
might support their wives to use modern health services20 21
like family planning, ANC, postnatal
care which in turn reduce the odd of having anemia as well advised to eat a diversified diet.
However, maternal educational status was not statistically associated with anemia, which is
contradictory to many studies from Ethiopia and abroad15 22-24
. This might be one important
motivator to involve husbands in anemia prevention efforts.
Page 9 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Lactating mothers who had been working in the last 12 months preceding the survey had lower
odd of having anemia as compared to their counter parts. This might be due to working mothers
were earning money as compared to non-working mothers and the extra income enabled them to
access and purchase more food items, including animal sources (meat, poultry, fish etc), and
increase dietary diversity. Studies have shown that income growth improves diet diversity which
in turn improves micronutrient intake, including iron25 26
. Similarly, lactating mothers in the
lower wealth groups had greater odds of anemia as compared to lactating mothers in the higher
wealth index. In many other studies, anemia among reproductive age women, the wealth index
was found to be a statistically significant factor15 22
. Other studies have also shown that women
of low socio-economic status are at risk for iron deficiency anemia (IDA) in late pregnancy and
in the postpartum period27 28
. Therefore, women’s empowerment through economic interventions
and working status could have a positive contribution towards preventing anemia.
This study also supports the importance of family planning for reducing the risk of anemia.
Those lactating mothers who have ever used family planning (modern or traditional) had a lower
odd of having anemia as compared to those who had never used family planning. This finding is
consistent with studies from Ethiopia and Timor-Leste which showed that use of family planning
was associated with lower odd of having anemia22 29
.
Maternal nutritional status (as measured by body mass index) was found to be significantly
associated with anemia. As compared with undernourished lactating mothers (BMI<18.5kg/m2),
being in the normal BMI category (18.5-24.9kg/m2) was associated with a lower odd of having
anemia. This finding is consistent with a study from Ethiopia and Thailand22 30
. When a mother
is at risk of deficiency for macronutrients, most likely she is also at risk of other micronutrient
deficiencies such as iron31.
ANC attendance was found to be associated with less odd of having anemia among lactating
mothers. This is most likely due to the fact that during ANC attendance mothers have been
advised to take iron supplements according to the Ethiopian micronutrient guideline and
instructed to consume different sources of iron rich food items32. Therefore, improving iron
status during pregnancy also helps to prevent anemia during the lactation period.
Page 10 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Those mothers who breastfed for 2 years had lower odd of having anemia as compared to
mothers who breastfed for 1 year. This could be due to the effect of breastfeeding on maternal
depletion. Because those mothers who breastfeed younger children have high burden of
breastfeeding as compared to the older one. A study by Samson and his colleagues also found
that breastfeeding increases risk of anemia significantly.
One of the strength of this study is to use laboratory confirmed anemia data at the national level.
Therefore, the study findings can be used to inform policy and program actions. However, the
study has caveats that some regions had small sample size, which questions the accuracy of
prevalence estimates per region, so that it should be interpreted in caution. The study did not
determine the presence of soil transmitted helminthes (STH) infection as it is associated with
anemia. This study also shares the limitation of cross-sectional study design which makes
difficult to demonstrate cause and effect relationships.
Conclusion
Anemia is a public health problem among lactating mothers in Ethiopia. There are regional
disparities regarding the prevalence of anemia, with the highest found in pastoralist regions of
Somali and Afar. Promoting partner education, improving maternal nutritional status, creating
behavioral change to use family planning and attend ANC services at health facilities are
recommended interventions to reduce the prevalence of anemia among lactating women in
Ethiopia.
Competing interests
The authors declare that they have no competing interests.
Funding statement
This research received no specific grant from any funding agency in the public, commercial or
not-for-profit sectors'
Authors’ contributions
YL and DH conceived the idea. YL analyzed and interpreted the data and critically reviewed the
manuscript. SB assisted in data interpretation and critically reviewed the manuscript. DH drafted
Page 11 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
the manuscript, assisted in the data analysis and interpretation and critically reviewed the
manuscript. All authors reviewed and approved the manuscript.
Acknowledgements
The authors acknowledge DHS Measure for granting the data freely. We are also grateful to
thank Lianna Tabar, country representative of KHI-E, for her professional language editing and
reviewing the manuscript.
References
1. WHO. The world health report. Reducing risks, promoting healthy life. Geneva, World Health
Organization. 2002.
2. Whitney E, Rolfes SR. Understanding Nutrition. In: Adams P, editor. Eleventh Edition ed. United States
of America: Thomson Learning Academic Resource Center, 2008.
3. Domell V, Lonnerdal B, Dewey K, Cohen R, Hernell O. Iron zinc and copper concentrations in breast
milk are independent of maternal status. American Journal of clinical nutrition 2004;79(1):111-
15.
4. Bodnar L, Scanlon K, Freedman D, Siega–Riz A, Cogswell M. High prevalence of postpartum anaemia
among Low income women in the United States. Journal of obstetrics and Gynecology
2001;185:4348-53.
5. Sserunjogi L, Scheut F, Whyte SR. Postnatal anaemia: neglected problems and missed opportunities in
Uganda. Health Policy and Planning 2003;18(2):225-31.
6. Beard JL, Hendricks MK, Perez EM, Murray-Kolb LE, Berg A, Vernon-Feagans L, et al. Maternal Iron
Deficiency Anemia Affects Postpartum Emotions and Cognition. Journal of Nutrition
2005;135:267–72.
7. Ross J, Thomas E. Iron deficiency anemia and maternal mortality. PROFILES 3 working notes series no.
3. Academy for Education Development, Washington D.C., 1996.
8. Brabin BJ, Hakimin M, Pelletier D. An Analysis of Anemia and Pregnancy-Related Maternal Mortality.
The Journal of Nutrition 2001;131:604S-15S.
9. Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, Lozano R, et al. A systematic analysis of
global anemia burden from 1990 to 2010. Blood 2014;123(5).
10. Central Statistical Agency (CSA) Ethiopia. Demographic and Health Survey 2011. Addis Ababa,
Ethiopia and Calverton, Maryland, USA: CSA and ORC Macro. 2011.
11. Central Statistical Agency(CSA). Demographic and Health Survey 2005. Addis Ababa, Ethiopia and
Calverton, Maryland, USA: CSA and ORC Macro, 2005.
12. Peter C, Jack V. Automated variable selection methods for logistic regression produced unstable
models for predicting acute myocardial infarction mortality. Journal of Clinical Epidemiology
2004;57:1138-46.
13. Singh AB, Kandpal SD, Chandra R, Srivastava VK, Negi KS. Anemia amongst pregnant and lactating
women in district Dehradun. Indian Journal of Preventive and Social Medicine 2009;40(1):20-21.
14. Ettyanga GA, Oloob WDvMLA, Saris WHM. Serum Retinol, Iron Status and Body Composition of
Lactating Women in Nandi, Kenya. Annals of Nutrition and Metabolism 2003;47:276-83.
Page 12 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
15. Zhao A, Zhang Y, Li B, Wang P, Li J, Xue Y, et al. Prevalence of Anemia and Its Risk Factors Among
Lactating Mothers in Myanmar. The American Journal of Tropical Medicine and Hygiene
2014;doi: 10.4269/ajtmh.13-0660.
16. WHO. Worldwide prevalence of anaemia 1993-2005 : WHO global database on anaemia / Edited by
Bruno de Benoist, Erin McLean, Ines Egli and Mary Cogswell, 2008.
17. WHO. Recommendations for the Prevention of Postpartum Haemorrhage (summary of results from
a WHO technical consultation, October 2006).Geneva, World Health Organization 2007.
18. Kibangou I, Bouhallab S, Henry G, Bureau F, Allouche S, Blais A, et al. Milk proteins and iron
absorption: contrasting effects of different caseinophosphopeptides. Pediatrics Research 2005
58(4):731-34.
19. Belachew T. Human Nutrition lecture note series for Health sciences students: Jimma Univesity
2005:pp 229.
20. Kassa M, Abajobir AA, Gedefaw M. Level of male involvement and associated factors in family
planning services utilization among married men in Debremarkos town,Northwest Ethiopia.
BMC International Health and Human Rights 2014;14:33.
21. Khanal V, Lee AH, Cruz JLNBd, Karkee4 R. Factors associated with non-utilisation of health service for
childbirth in Timor-Leste: evidence from the 2009-2010 Demographic and Health Survey. BMC
International Health and Human Rights 2014;14:14.
22. Gebremedhin S, Enquselassie F. Correlates of anemia among women of reproductive age in Ethiopia:
Evidence from Ethiopian DHS 2005. Ethiopian Journal of Health Development 2011;25(1):22-30.
23. Haidar J. Prevalence of Anaemia, Deficiencies of Iron and Folic Acid and Their Determinants in
Ethiopian Women. Journal of Health Population Nutrition 2010;28(4):359-68.
24. Okwu GN. Studies on the predisposing factors of iron deficiency anaemia among lactating women in
Owerri, Nigeria. International Research Journal of Biochemistry and Bioinformatics
2011;1(11):304-09.
25. Taruvinga A, Muchenje V, Mushunje A. Determinants of rural household dietary diversity: The case
of Amatole and Nyandeni districts, South Africa. International Journal of Development and
Sustainability 2013;2 (4).
26. Doan D. Does income growth improve diet diversity in China?Selected Paper prepared for
presentation at the 58 the AARES Annual Conference, Port Macquarie, New South Wales, 4-7
February 2014
27. Bodnar L, Cogswell M, Scanlon K. Low income postpartum women are at risk of iron deficiency.
Journal of Nutrition 2002;132:2298–302.
28. Sadeghian M, Fatourechi A, Lesanpezeshki M, Ahmadnezhad E. Prevalence of Anemia and Correlated
Factors in the Reproductive Age Women in Rural Areas of Tabas. Journal of Family and
Reproductive Health 2013;7(3):143.
29. Lovermail AA, Hartman M, Chia KS, Heymann DL. Demographic and Spatial Predictors of Anemia in
Women of Reproductive Age in Timor-Leste: Implications for Health Program Prioritization. PLoS
ONE 2013;9(3):e91252.
30. Liabsuetrakul T, for Southern Soil-transmitted Helminths and Maternal Health Working Group. Is
International or Asian Criteria-based Body Mass Index Associated with Maternal Anaemia, Low
Birthweight, and Preterm Births among Thai Population?—An Observational Study. Journal of
Health Population Nutrition 2011;29(3):218-28.
31. Blumfield M, Hure A, MacDonald-Wicks L, Smith R, Simpson S, Raubenheimer D, et al. The
association between the macronutrient content of maternal diet and the adequacy of
micronutrients during pregnancy in the Women and Their Children’s Health (WATCH) study.
Nutrients 2012;4(12):1958-76.
Page 13 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
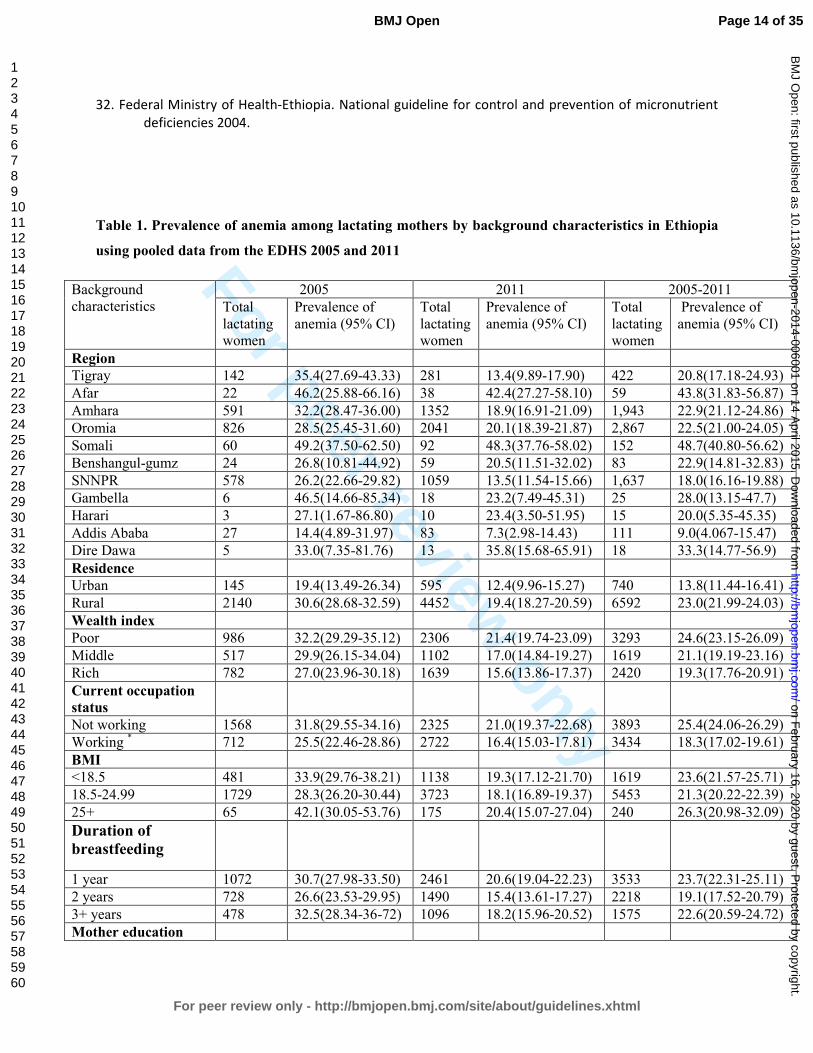
For peer review only
32. Federal Ministry of Health-Ethiopia. National guideline for control and prevention of micronutrient
deficiencies 2004.
Table 1. Prevalence of anemia among lactating mothers by background characteristics in Ethiopia
using pooled data from the EDHS 2005 and 2011
Background
characteristics
2005 2011 2005-2011
Total
lactating
women
Prevalence of
anemia (95% CI)
Total
lactating
women
Prevalence of
anemia (95% CI)
Total
lactating
women
Prevalence of
anemia (95% CI)
Region
Tigray 142 35.4(27.69-43.33) 281 13.4(9.89-17.90) 422 20.8(17.18-24.93)
Afar 22 46.2(25.88-66.16) 38 42.4(27.27-58.10) 59 43.8(31.83-56.87)
Amhara 591 32.2(28.47-36.00) 1352 18.9(16.91-21.09) 1,943 22.9(21.12-24.86)
Oromia 826 28.5(25.45-31.60) 2041 20.1(18.39-21.87) 2,867 22.5(21.00-24.05)
Somali 60 49.2(37.50-62.50) 92 48.3(37.76-58.02) 152 48.7(40.80-56.62)
Benshangul-gumz 24 26.8(10.81-44.92) 59 20.5(11.51-32.02) 83 22.9(14.81-32.83)
SNNPR 578 26.2(22.66-29.82) 1059 13.5(11.54-15.66) 1,637 18.0(16.16-19.88)
Gambella 6 46.5(14.66-85.34) 18 23.2(7.49-45.31) 25 28.0(13.15-47.7)
Harari 3 27.1(1.67-86.80) 10 23.4(3.50-51.95) 15 20.0(5.35-45.35)
Addis Ababa 27 14.4(4.89-31.97) 83 7.3(2.98-14.43) 111 9.0(4.067-15.47)
Dire Dawa 5 33.0(7.35-81.76) 13 35.8(15.68-65.91) 18 33.3(14.77-56.9)
Residence
Urban 145 19.4(13.49-26.34) 595 12.4(9.96-15.27) 740 13.8(11.44-16.41)
Rural 2140 30.6(28.68-32.59) 4452 19.4(18.27-20.59) 6592 23.0(21.99-24.03)
Wealth index
Poor 986 32.2(29.29-35.12) 2306 21.4(19.74-23.09) 3293 24.6(23.15-26.09)
Middle 517 29.9(26.15-34.04) 1102 17.0(14.84-19.27) 1619 21.1(19.19-23.16)
Rich 782 27.0(23.96-30.18) 1639 15.6(13.86-17.37) 2420 19.3(17.76-20.91)
Current occupation
status
Not working 1568 31.8(29.55-34.16) 2325 21.0(19.37-22.68) 3893 25.4(24.06-26.29)
Working * 712 25.5(22.46-28.86) 2722 16.4(15.03-17.81) 3434 18.3(17.02-19.61)
BMI
<18.5 481 33.9(29.76-38.21) 1138 19.3(17.12-21.70) 1619 23.6(21.57-25.71)
18.5-24.99 1729 28.3(26.20-30.44) 3723 18.1(16.89-19.37) 5453 21.3(20.22-22.39)
25+ 65 42.1(30.05-53.76) 175 20.4(15.07-27.04) 240 26.3(20.98-32.09)
Duration of
breastfeeding
1 year 1072 30.7(27.98-33.50) 2461 20.6(19.04-22.23) 3533 23.7(22.31-25.11)
2 years 728 26.6(23.53-29.95) 1490 15.4(13.61-17.27) 2218 19.1(17.52-20.79)
3+ years 478 32.5(28.34-36-72) 1096 18.2(15.96-20.52) 1575 22.6(20.59-24.72)
Mother education
Page 14 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
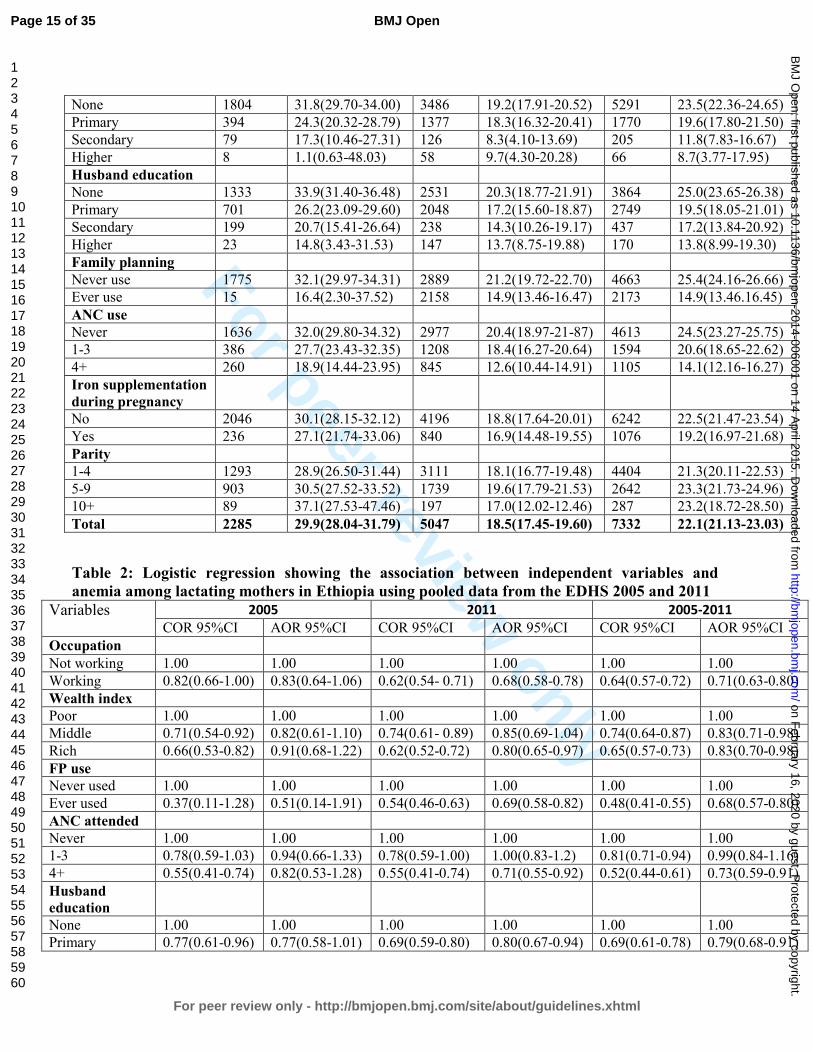
For peer review only
None 1804 31.8(29.70-34.00) 3486 19.2(17.91-20.52) 5291 23.5(22.36-24.65)
Primary 394 24.3(20.32-28.79) 1377 18.3(16.32-20.41) 1770 19.6(17.80-21.50)
Secondary 79 17.3(10.46-27.31) 126 8.3(4.10-13.69) 205 11.8(7.83-16.67)
Higher 8 1.1(0.63-48.03) 58 9.7(4.30-20.28) 66 8.7(3.77-17.95)
Husband education
None 1333 33.9(31.40-36.48) 2531 20.3(18.77-21.91) 3864 25.0(23.65-26.38)
Primary 701 26.2(23.09-29.60) 2048 17.2(15.60-18.87) 2749 19.5(18.05-21.01)
Secondary 199 20.7(15.41-26.64) 238 14.3(10.26-19.17) 437 17.2(13.84-20.92)
Higher 23 14.8(3.43-31.53) 147 13.7(8.75-19.88) 170 13.8(8.99-19.30)
Family planning
Never use 1775 32.1(29.97-34.31) 2889 21.2(19.72-22.70) 4663 25.4(24.16-26.66)
Ever use 15 16.4(2.30-37.52) 2158 14.9(13.46-16.47) 2173 14.9(13.46.16.45)
ANC use
Never 1636 32.0(29.80-34.32) 2977 20.4(18.97-21-87) 4613 24.5(23.27-25.75)
1-3 386 27.7(23.43-32.35) 1208 18.4(16.27-20.64) 1594 20.6(18.65-22.62)
4+ 260 18.9(14.44-23.95) 845 12.6(10.44-14.91) 1105 14.1(12.16-16.27)
Iron supplementation
during pregnancy
No 2046 30.1(28.15-32.12) 4196 18.8(17.64-20.01) 6242 22.5(21.47-23.54)
Yes 236 27.1(21.74-33.06) 840 16.9(14.48-19.55) 1076 19.2(16.97-21.68)
Parity
1-4 1293 28.9(26.50-31.44) 3111 18.1(16.77-19.48) 4404 21.3(20.11-22.53)
5-9 903 30.5(27.52-33.52) 1739 19.6(17.79-21.53) 2642 23.3(21.73-24.96)
10+ 89 37.1(27.53-47.46) 197 17.0(12.02-12.46) 287 23.2(18.72-28.50)
Total 2285 29.9(28.04-31.79) 5047 18.5(17.45-19.60) 7332 22.1(21.13-23.03)
Table 2: Logistic regression showing the association between independent variables and
anemia among lactating mothers in Ethiopia using pooled data from the EDHS 2005 and 2011
Variables 2005 2011 2005-2011
COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI
Occupation
Not working 1.00 1.00 1.00 1.00 1.00 1.00
Working 0.82(0.66-1.00) 0.83(0.64-1.06) 0.62(0.54- 0.71) 0.68(0.58-0.78) 0.64(0.57-0.72) 0.71(0.63-0.80)
Wealth index
Poor 1.00 1.00 1.00 1.00 1.00 1.00
Middle 0.71(0.54-0.92) 0.82(0.61-1.10) 0.74(0.61- 0.89) 0.85(0.69-1.04) 0.74(0.64-0.87) 0.83(0.71-0.98)
Rich 0.66(0.53-0.82) 0.91(0.68-1.22) 0.62(0.52-0.72) 0.80(0.65-0.97) 0.65(0.57-0.73) 0.83(0.70-0.98)
FP use
Never used 1.00 1.00 1.00 1.00 1.00 1.00
Ever used 0.37(0.11-1.28) 0.51(0.14-1.91) 0.54(0.46-0.63) 0.69(0.58-0.82) 0.48(0.41-0.55) 0.68(0.57-0.80)
ANC attended
Never 1.00 1.00 1.00 1.00 1.00 1.00
1-3 0.78(0.59-1.03) 0.94(0.66-1.33) 0.78(0.59-1.00) 1.00(0.83-1.2) 0.81(0.71-0.94) 0.99(0.84-1.16)
4+ 0.55(0.41-0.74) 0.82(0.53-1.28) 0.55(0.41-0.74) 0.71(0.55-0.92) 0.52(0.44-0.61) 0.73(0.59-0.91)
Husband
education
None 1.00 1.00 1.00 1.00 1.00 1.00
Primary 0.77(0.61-0.96) 0.77(0.58-1.01) 0.69(0.59-0.80) 0.80(0.67-0.94) 0.69(0.61-0.78) 0.79(0.68-0.91)
Page 15 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Secondary 0.55(0.39-0.77) 0.83(0.50-1.38) 0.64(0.48-0.87) 0.81(0.58-1.14) 0.62(0.49-0.77) 0.83(0.62-1.09)
Higher 0.58(0.26-1.30) 0.50(0.73-3.40) 0.72(0.49-1.0) 0.96(0.61-1.52) 0.64(0.46-0.90) 0.94(0.61-1.45)
BMI
<18.5 1.00 1.00 1.00 1.00 1.00 1.00
18.5-24.99 0.74(0.59-0.92) 0.76(0.59-0.99) 0.74(0.64-0.86) 0.79(0.68-0.93) 0.76(0.67-0.86) 0.78(0.68-0.89)
25+ 1.1(0.62-1.90) 1.66(0.79-3.48) 0.82(0.58-1.2) 1.12(0.77-1.62) 0.85(0.64-1.12) 1.21(0.87-1.68)
Duration of
breastfeeding
1 year 1.00 1.00 1.00 1.00 1.00 1.00
2 years 0.79(0.64-0.99) 0.79(0.62-1.03) 0.71(0.60-0.83) 0.75(0.63-0.88) 0.75(0.66-0.85) 0.76(0.66-0.87)
3+ years 0.99(0.77-1.27) 1.10(0.82-1.49) 0.71(0.59-0.86) 0.82(0.67-0.99) 0.81(0.70-0.94) 0.89(0.76-1.05)
Time laps
2005 1.00 1.00
2011 0.65(0.58-0.73) 0.73(0.64-0.85) COR: Crude Odds Ratio, AOR: Adjusted Odds Ratio, 1.00 is the reference category
Page 16 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Anemia prevalence and associated factors among lactating mothers in Ethiopia: Evidence
from the 2005 and 2011 demographic and health surveys
Yihunie Lakew1, Sibhatu Biadgilign
2, Demewoz Haile
3*
1 Ethiopian Ppublic Hhealth Aassociation, Addis Ababa, Ethiopia
2 Independent Ppublic Hhealth Cconsultants, Addis Ababa, Ethiopia
3 Department of Public Health, College of Medicine and Health sciences, Madawalabu
University, Ethiopia
Email address
Yihunie Lakew – [email protected]
Sibhatu Biadgilign- [email protected]
Demewoz Haile–[email protected]
*Corresponding author
Address of corresponding author
Department of Public Health
College of Medicine and Health sciences
Madawalabu University, Ethiopia
Bale Goba , P.O.Box 302
Running title: Factors associated with anemia among lactating mothers in Ethiopia
Key words: Lactating mothers, anemia, Ethiopia,
Word count: 2388
Page 17 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Abstract
Objective: To identify factors associated with anemia among lactating mothers in Ethiopia.
Design: A cross-sectional secondary data analysis pooled from two rounds of the 2005 and 2011
Ethiopian demographic and health survey (EDHS) was used. Multivariable logistic regression
model was applied to determine the factors associated with anemia.
Population: A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047 from EDHS
2011) were included from 11 administrative states of Ethiopia.
Main outcome measures: Lactating mothers considered as anemic if hemoglobin level <12
gram per deciliter.
Results: The overall prevalence of anemia among lactating mothers was found to be 22.1%
[95% CI: (21.13-23.03)]. The highest prevalence was 48.7% [95% CI: (40.80-56.62)] found in
Somali region, followed by 43.8% [95% CI: (31.83-56.87)] in Afar region. The multivariable
statistical model showed that lactating mothers who had husbands attended primary education
[AOR=0.79; 95% CI: (0.68-0.91)], had been working in the last 12 months preceding the survey
[AOR=0.71; 95% CI: (0.63-0.80)],who were currently working [AOR=0.71; 95% CI: (0.63-
0.80)], had normal maternal body mass index (BMI) from 18.5kg/m2 to 24.99kg/m
2 [AOR=0.78;
95% CI: (0.68-0.89)], middle wealth quintile index [AOR=0.83; 95% CI: (0.71-0.98)] and rich
wealth quintile index [AOR=0.83; 95% CI: (0.70-0.98)], ever use of family planning
[AOR=0.68; 95% CI: (0.57-0.80)], attending antenatal care (ANC) for indexed pregnancy four
times or more [AOR=0.73; 95% CI: (0.59-0.91)], experienced time variation between two
surveys [AOR=0.73; 95%CI: (0.64-0.85)] and who breastfed for two years [AOR=0.76; 95% CI:
(0.66-0.87)] were associated with lower odd of being anemic.
Conclusion: Anemia is highly prevalent among lactating mothers, particularly among pastoralist
communities of Somali and Afar. Promoting partner education, improving maternal nutritional
status, creating behavioral change to use family planning and ANC services at health facilities
are recommended interventions to reduce the prevalence of anemia among lactating mothers in
Ethiopia.
Formatted: Font: Font color: Auto
Page 18 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
ARTICLE SUMMARY
Article focus
• Anemia is a serious nutritional problem, primarily affecting women of reproductive age
and children, and remains a major challenge in developing countries. In Ethiopia, more
than 20% of women in the reproductive age are anemic.
• Lactating mothers are among vulnerable groups with little information regarding social
determinants of anemia.
Key messages
• Anemia prevalence is a public health problem among lactating mothers in Ethiopia, with
the highest prevalence found in pastoralist regions of Somali and Afar
• A statistically significant reduction of anemia prevalence amongin lactating mothers was
observed from 2005 to 2011.
• Being in middle and rich wealth quintiles, breastfeeding for two years, currently working,
normal body mass index, husbands’ primary education, ever use of family planning and
antenatal care attendance for four or more visits were factors associated with lower odds
of anemia.
Strength and Limitations
• The study attempted to identify factors associated with laboratory confirmed anemia
among lactating mothers at the national level. The study findings can be used to inform
policy and program actions.
• Some regions from which data was collected had small sample size. So that it should be
interpreted in caution. This study also shares the limitation of cross-sectional design which
makes difficult to demonstrate cause and effect relationships.
Page 19 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Introduction
Anemia is a serious nutrition problem affecting millions in developing countries, and remains a
major challenge for human health, social and economic development1. Lactating mothers are one
amongof the vulnerable groups of anemia. During the period of lactation, mothers are
susceptible to anemia due to maternal iron depletion and blood loss during child birth2. Studies
have shown that though breast milk is not a good source of iron, the concentration of iron in
breast milk is independent of maternal iron status. This showed that the quality of breast milk is
maintained at the expense of maternal stores2 3.
Postpartum anemia has been found highest in mothers who were anemic during pregnancy4.
Furthermore, lactating mothers are highly susceptible to iron depletion if they have not had
enough energy and nutrient intake in their diets. Lactating mothers begin the postnatal period
after having iron depleted through the continuum from pregnancy to childbearing 5. A study from
South Africa showed that iron status was associated with depression, stress, and cognitive
functioning in poor African mothers during the postpartum period6. In a meta-analysis of
observational and intervention trials, Ross and Thomas, found that approximately 20% of the
maternal mortality seen in sub-Saharan Africa and South Asia was attributable to anemia that
was primarily the result of iron deficiency7.
Ethiopia is one of the countries in sub-Saharan Africa affected by anemia and it contributes to
high rates of maternal, infant and child mortality globally8 9
. In Ethiopia, the maternal mortality
ratio was 676 maternal deaths per 100,000 live births10
. for the seven-year period preceding the
2011 EDHS survey. This rate which is one of the highest in the world. The country has
considerably high infant and under 5 mortality rates that account for 59 and 88 deaths per 1000
live births, respectively The infant mortality rate was 59 per 1,000 live births and the under-five
mortality rate was 88 per 1,000 live births10
.
. Anemia testing was included in the two rounds of the Ethiopian Demographic and Health
Surveys (EDHS)10 11. The prevalence of anemia in lactating mothers was 29.9% in 2005 and
18.5% in 201110. It was 30.6% in 2005 and 22% in 2011 among pregnant women and it was
23.9% in 2005 and 15% in 2011 among women neither non-pregnant nor lactating. This shows
that a relatively higher prevalence of anemia was found among Ethiopian pregnant and lactating
mothers.
Page 20 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Anemia testing was included in the two rounds of the Ethiopian demographic and health surveys
(EDHS). The prevalence of anemia amongin lactating mothers was 29.9% in 2005 and 18.5% in
201110
,11
. The prevalence of anemia in lactating mothers was 29.9% in 2005 and 18.5% in 2011
1012. It was 30.6% in 2005 and 22% in 2011 among pregnant women and 23.9% in 2005 and 15%
in 2011 among women neither non-pregnant nor lactating. This shows that a relatively higher
prevalence of anemia was found among Ethiopian pregnant and lactating mothers. However,
little information is available regarding socio-economic factors associated with anemia among
lactating mothers. This study aimed to identify factors associated with anemia among lactating
mothers in Ethiopia using the pooled data of EDHS 2005 and 2011.
Methods
Data type and study design
This study is an in-depth analysis to identify factors associated with anemia among lactating
mothers based on cross-sectional secondary data of the EDHS 2005 and 2011 datasets. Both the
2005 and 2011 EDHS samples were selected using a stratified, two-stage cluster sampling
design. All women age 15-49 who were usual residents or who slept in the selected households
the night before the survey were eligible. The EDHS data include a women’s questionnaire that
measures socio-demographic characteristics of the mothers, information on reproductive health
and service use behaviours, as well as HIV and anemia test. The tool was pretested and translated
in to three local languages - Amharic, Oromeifa and Tigregna. The EDHS was designed to
provide population and health indicators at national and regional levels. The survey It is
conducted in every five years. Both the 2005 and 2011 EDHS samples were selected using a
stratified, two-stage cluster sampling design. The detailed methodology is found elsewhere10 11
.
Data Extraction
Both EDHS 2005 and 2011 data were downloaded with permission from the Measure DHS
website in SPSS format. After reviewing the detailed data coding, further data cleaning and
recoding was completed. A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047
from EDHS 2011) were included in the analysis. Based on published literature, information on a
wide-range of socio-demographic and economic variables, health service related factors and
anemia level indicators were extracted. The chosen variables were region, residence, wealth
Page 21 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
index, occupation, BMI, duration of breastfeeding, respondent’s education, husband’s education,
family planning use, iron tablet supplementation during pregnancy, time variation between two
surveys, marital status, age, parity and antenatal care attendance.
Measurement of variables
In both rounds of the EDHS, haemoglobin analysis was carried out onsite using a battery-
operated portable HemoCue analyzer for all anemia samples. The raw measured values of
haemoglobin were obtained using the HemoCue instrument and adjusted for altitude and
smoking status10
. All the necessary quality control measures were considered9. Height and
weight measurements were carried out for the respondents. Weight measurements were obtained
using lightweight, SECA mother-infant scales with a digital screen, designed and manufactured.
under the guidance of UNICEF. Height measurements were carried out using a measuring board.
Lactating mothers considered as anemic if hemoglobin level <12 gram per deciliter.
Haemoglobin (Hb) level of anemia was measured in g/dl, operationalised as a categorical
variable by predefined cut-off points for mild, moderate and severe anemia recommended by the
WHO for women above age 15 years. For this analysis, anemia was re-categorized as anemic
and non-anemic from prior classifications in levels (no, mild, moderate, severe). Antenatal care
(ANC) attendance referreds to when women get services during pregnancy according to the
WHO recommendation of at least four ANC visits for low-risk pregnant women. The frequency
of the ANC visit is measured by asking the respondent to recall how many times she had
attended for the indexed child. Occupational status wasis defined as non-working and working
which comprises of professional/technical/managerial, clerical, sales and services, skilled
manual, unskilled manual and agriculture classifications. BMI (kg/m2) was categorised using
standard WHO classification into underweight <18.5 kg/m2, normal 18.5–24.9 kg/m2,
overweight 25.0+. Parity, defined as the number of children ever born, was categorised as 1-4, 5-
9 and 10+. The wealth index constructed from household assets and characteristics available in
both surveys to categorize individuals into wealth quintiles (poorest, poorer, middle, rich,
richest) was used. However, to make it more sensible and understandable, wealth index was re-
categorized into three groups (poor, middle and rich) to give more meaningful interpretations and
suite for recommendations.
Formatted: Underline, Font color: Red
Page 22 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Data processing and sStatistical analysis
Both surveys were administered by the Ethiopian Central Statistics Authority (CSA). Data entry
and editing was performed using CSPro software. For this study, the 2005 and 2011 EDHS data
were pooled to achieve high power for detecting the associated factors and analyzed using
STATA 11 software. Weighted proportions and odds ratios are presented to compromise
sampling probabilities. Sample weights were applied in order to compensate for the unequal
probability of selection between the strata that has been geographically defined as well as for
non-responses. A detailed explanation of the weighting procedure can be found in the EDHS
methodology report10
. We used “svy” in STATA version 11 to weight the survey data and do the
analyses. Anemia was re-categorized as anemic and non-anemic from prior classifications in
levels (no, mild, moderate, severe). The background variables were selected based on literature
review and data availability from the two rounds of EDHS. The chosen variables were region,
residence, wealth index, occupation, BMI, duration of breastfeeding, respondent’s education,
husband’s education, family planning use, iron tablet supplementation during pregnancy, time
variation between two surveys, marital status, age, parity and antenatal care attendance.
Descriptive statistics were used to show the prevalence of anemia among lactating mothers
varying by background characteristics. Binary and multivariable logistic regression statistical
analysis was carried out to determine the factors associated with anemia among lactating
mothers. Variables found statistically significant at p-value <0.25 during bivariate analysis were
analyzed in the multivariable logistic regression model12
. This p-value cut off point prevented
removing variables that would potentially have an effect during multivariable analysis. Both
crude and adjusted odds ratios (OR) were reported with 95% confidence interval (CI). Variables
at p-value <0.05 were considered statistically significant in the multivariable logistic regression
model.
Ethical statements
The data were downloaded and used after communicating the purpose of the analysis and
receiving permission from Measure DHS Organization. The original EDHS data were collected
in accordance with international and national ethical guidelines.
Page 23 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Results
Majority of respondents (86%) were from rural. Nearly 60% of lactating mothers were Christian
followers followed by 38% of Muslims. The mean age of respondents was 28.4 with SD 6.8. The
overall prevalence of anemia among lactating mothers during 2005 to 2011 was found to be
22.1% (95% CI: 21.13-23.03). The prevalence of anemia for the years 2005 and 2011 was 29.9%
[95% CI: (28.04-31.79)] and 18.5% [95% CI: 17.45-19.60)], respectively. The prevalence was
13.8% [95% CI: (11.44-16.41)] in urban areas and 23% [95% CI: (21.99-24.03)] in rural areas.
In the period 2005 to 2011, the highest prevalence of anemia among lactating mothers was
48.7% [95%CI: (40.80-56.62)] found in Somali region, while the lowest prevalence was 9.0%
[95%CI: (4.07-15.47)] reported in Addis Ababa. In the period 2005 to 2011, the prevalence of
anemia in lactating mothers was consistently higher among those in the poor wealth index group,
not currently working, with BMI greater or equal to 25 kg/m2, one year duration of
breastfeeding, never educated, never used ANC, never used family planning services, no iron
tablet supplement during pregnancy, and with higher parity. A significant reduction in the
prevalence of anemia among lactating mothers was observed in all background variables from
2005 to 2011(Table 1). Figure 1 shows the classification of anemia in terms of its detailed
parameter.
In the bivariate step of our analysis, age and marital status were not statistically significant in the
data from both individual surveys and pooled data with the cut-off point of p<0.25. The variable
associated with lower odd of being anemic for the 2005 data was normal BMI, whereas for the
2011 data the variables were working status, wealth index, use of family planning, ANC
attendance for indexed pregnancy, husband’s education, maternal BMI and duration of
breastfeeding.
The variable associated with anemia for the 2005 data was BMI, whereas for the 2011 data the
variables were working status, wealth index, ever use of family planning, ANC attendance four
times and above for indexed pregnancy, husband’s education, maternal BMI and duration of
breastfeeding.
In the final multivariable model using pooled data, variables which significantly associated with
anemia for lactating mothers were working status, wealth index, use of family planning, ANC
Page 24 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
attendance for indexed pregnancy, husband’s education, maternal BMI, time variation in the two
surveys, and durations of breastfeeding.
In the final multivariable model using pooled data, the independent predictors of anemia for
Ethiopian lactating mothers were currently working, wealth index, ever use of family planning,
ANC attendance four times and above for indexed pregnancy, husband’s education, maternal
BMI, time variation in the two surveys, and durations of breastfeeding remained.
Paternal educational status was found to be a predictor of anemia among lactating mothers.
Those lactating mothers who had husbands who attended primary education were at 21% less
likely to have anemia as compared to those mothers who had husbands with no education
[AOR=0.79; 95% CI: (0.68-0.91)]. The odd of being anemic in working lactating mothers was
29% less as compared to their counter parts [AOR=0.71; 95% CI: (0.63-0.80)]. Those lactating
mothers having a normal maternal BMI (18.5kg/m2-24.99kg/m2) were 22% less likely to be
anemic as compared to lactating mother with low BMI (<18.5kg/m2) [AOR=0.78; 95% CI:
(0.68-0.89)]. Similarly, lactating women who are categorized in middle [AOR=0.83; 95% CI:
(0.71-0.98)] and rich wealth quintiles index [AOR=0.83; 95% CI: (0.70-0.98)] were each 17%
less likely to have anemia as compared to lactating women in poorer wealth quintilesindex.
Among reproductive characteristics, family planning use and antenatal care (ANC) were the
significant factors associated with anemia in lactating mothers. Lactating mothers who ever used
family planning were 32% less likely to have anemia as compared to lactating mothers who
never used family planning [AOR=0.68; 95% CI: (0.57- 0.80)]. Lactating mothers who reported
ANC attendance four times or more for indexed pregnancy were 27% less likely to have anemia
as compared to mothers who never attended ANC [AOR=0.73; 95% CI: (0.59-0.91)]. Those
lactating mothers who breastfed for two years were 24% less likely to have anemia as compared
to lactating women who breastfed for one year [AOR=0.76; 95% CI: (0.66-0.87)] (Table 2).
Page 25 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Discussion
Over one fifth of lactating mothers were anemic in Ethiopia, which is lower as compared to other
developing countries. For example, more than 66.090% of lactating mothers have been reported
as having anemia in India13 14 and 43.8 29.6% of lactating mothers in Zimbabwe Kenya had a
hemoglobin level <12 g/dl14
developed anemia15
. Another study from Myanmar reported an
anemia prevalence rate of 60.3% in lactating women, with 20.3% of lactating mothers having
severe anemia15
. Although the prevalence of anemia among lactating mothers in Ethiopia was
relatively low as compared to these studies, it remains a public health problem according to
WHO classification16. The relatively better prevalence of anemia in Ethiopia among lactating
mothers may be due to the cultural norms of providing nutritional care to lactating mothers
during the postpartum period. During the postpartum period, lactating mothers are encouraged to
rest for 3 to 6 months and to eat a variety of foods including animal sources, even during
religious fasting periods. Iron supplementation coverage in Ethiopia remained low among
pregnant mothers10
, despite its known contribution for reducing the risk of postpartum
hemorrhage17
10
. Postpartum hemorrhage was also found to be one of the risk factors for anemia
during the period of lactation17
.
This study showed that anemia is a widespread problem in the pastoralist communities of Somali
and Afar. The prevalence of anemia in lactating mothers was higher in the pastoralist regions and
showed slow decline in these regions from 2005 to 2011. This could be due to the fact that
pastoralist communities are heavily dependent on animal milk as a source of daily food, with
poor iron bioavailability18 19
. The other reason could be due to low utilization of family planning
and antenatal care services in pastoralist areas10.
One of the factors determined to be associated with anemia was paternal education. Having a
husband with a higher level of education was found to be associated with less odd of having
anemia among lactating mothers. This could be due to the fact that those educated husbands
might support their wives to use modern health services20 21 like family planning, ANC, postnatal
care which in turn reduce the odd of having anemia as well advised to eat a diversified diet.
However, maternal educational status was not statistically associated with anemia, which is
contradictory to many studies from Ethiopia and abroad15 22-24
. This might be one important
motivator to involve husbands in anemia prevention efforts.
Formatted: Not Highlight
Page 26 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Lactating mothers who had been working in the last 12 months preceding the surveyWorking
lactating mothers had lower odd of having anemia as compared to their counter parts. This might
be due to working mothers were earning money as compared to non-working mothers and the
extra income enabled them to access and purchase more food items, including animal sources
(meat, poultry, fish etc), and increase dietary diversity. Studies have shown that income growth
improves diet diversity which in turn improves micronutrient intake, including iron25 26
.
Similarly, lactating mothers in the lower wealth groups had greater odds of anemia as compared
to lactating mothers in the higher wealth quintilesindex. In many other studies, anemia among
reproductive age women, the wealth index was found to be a statistically significant factor15 22.
Other studies have also shown that women of low socio-economic status are at risk for iron
deficiency anemia (IDA) in late pregnancy and in the postpartum period27 28
. Therefore, women’s
empowerment through economic interventions and working status could have a positive
contribution towards preventing anemia.
This study also supports the importance of family planning for reducing the risk of anemia.
Those lactating mothers who have ever used family planning (modern or traditional) had a lower
odd of having anemia as compared to those who had never used family planning. This finding is
consistent with studies from Ethiopia and Timor-Leste which showed that use of family planning
was associated with lower odd of having anemia22 29.
Maternal nutritional status (as measured by body mass index) was found to be significantly
associated with anemia. As compared with undernourished lactating mothers (BMI<18.5kg/m2),
being in the normal BMI category (18.5-24.9kg/m2) was associated with a lower odd of having
anemia. This finding is similar consistent with a study from Ethiopia and Thailand22 30
. When a
mother is at risk of deficiency for macronutrients, most likely she is also at risk of other
micronutrient deficiencies such as iron31
.
ANC attendance was found to be associated with less odd of having anemia among lactating
mothers. This is most likely due to the fact that during ANC attendance mothers have been
advised to take iron supplements according to the Ethiopian micronutrient guideline and
instructed to consume different sources of iron rich food items32
. Therefore, improving iron
status during pregnancy also helps to prevent anemia during the lactation period.
Page 27 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Those mothers who breastfed for 2 years had lower odd of having anemia as compared to
mothers who breastfed for 1 year. This could be due to the effect of breastfeeding on maternal
depletion. Because those mothers who breastfeed younger children have high burden of
breastfeeding as compared to the older one. A study by Samson and his colleagues also found
that breastfeeding increases risk of anemia significantly22
.
One of the strength of this study is that it has to use large sample size with laboratory confirmed
anemia data at the national level. Therefore, the study findings can be used to inform policy and
program actions. However, the study has caveats that some regions had small sample size, which
questions the accuracy of prevalence estimates per region, so that it should be interpreted in
caution. The study did not determine the presence of soil transmitted helminthes (STH) infection
as it is associated with anemia. This study also shares the limitation of cross-sectional study
design which makes difficult to see demonstratethe cause and effect relationships.
Conclusion
Anemia is a public health problem among lactating mothers in Ethiopia. There are regional
disparities regarding the prevalence of anemia, with the highest found in pastoralist regions of
Somali and Afar. Promoting partner education, improving maternal nutritional status, creating
behavioral change to use family planning and attend ANC services at health facilities are
recommended interventions to reduce the prevalence of anemia among lactating women in
Ethiopia.
Competing interests
The authors declare that they have no competing interests.
Funding statement
This research received no specific grant from any funding agency in the public, commercial or
not-for-profit sectors'
Authors’ contributions
YL and DH conceived the idea. YL analyzed and interpreted the data and critically reviewed the
manuscript. SB assisted in data interpretation and critically reviewed the manuscript. DH drafted
Page 28 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
the manuscript, assisted in the data analysis and interpretation and critically reviewed the
manuscript. All authors reviewed and approved the manuscript.
Acknowledgements
The authors acknowledge DHS Measure for granting the data freely. We are also grateful to
thank Lianna Tabar, country representative of KHI-E, for her professional language editing and
reviewing the manuscript.
References
1. WHO. The world health report. Reducing risks, promoting healthy life. Geneva, World Health
Organization. 2002.
2. Whitney E, Rolfes SR. Understanding Nutrition. In: Adams P, editor. Eleventh Edition ed. United States
of America: Thomson Learning Academic Resource Center, 2008.
3. Domell V, Lonnerdal B, Dewey K, Cohen R, Hernell O. Iron zinc and copper concentrations in breast
milk are independent of maternal status. American Journal of clinical nutrition 2004;79(1):111-
15.
4. Bodnar L, Scanlon K, Freedman D, Siega–Riz A, Cogswell M. High prevalence of postpartum anaemia
among Low income women in the United States. Journal of obstetrics and Gynecology
2001;185:4348-53.
5. Sserunjogi L, Scheut F, Whyte SR. Postnatal anaemia: neglected problems and missed opportunities in
Uganda. Health Policy and Planning 2003;18(2):225-31.
6. Beard JL, Hendricks MK, Perez EM, Murray-Kolb LE, Berg A, Vernon-Feagans L, et al. Maternal Iron
Deficiency Anemia Affects Postpartum Emotions and Cognition. Journal of Nutrition
2005;135:267–72.
7. Ross J, Thomas E. Iron deficiency anemia and maternal mortality. PROFILES 3 working notes series no.
3. Academy for Education Development, Washington D.C., 1996.
8. Brabin BJ, Hakimin M, Pelletier D. An Analysis of Anemia and Pregnancy-Related Maternal Mortality.
The Journal of Nutrition 2001;131:604S-15S.
9. Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, Lozano R, et al. A systematic analysis of
global anemia burden from 1990 to 2010. Blood 2014;123(5).
10. Central Statistical Agency (CSA) Ethiopia. Demographic and Health Survey 2011. Addis Ababa,
Ethiopia and Calverton, Maryland, USA: CSA and ORC Macro. 2011.
11. Central Statistical Agency(CSA). Demographic and Health Survey 2005. Addis Ababa, Ethiopia and
Calverton, Maryland, USA: CSA and ORC Macro, 2005.
12. Peter C, Jack V. Automated variable selection methods for logistic regression produced unstable
models for predicting acute myocardial infarction mortality. Journal of Clinical Epidemiology
2004;57:1138-46.
13. Singh AB, Kandpal SD, Chandra R, Srivastava VK, Negi KS. Anemia amongst pregnant and lactating
women in district Dehradun. Indian Journal of Preventive and Social Medicine 2009;40(1):20-21.
14. Ettyanga GA, Oloob WDvMLA, Saris WHM. Serum Retinol, Iron Status and Body Composition of
Lactating Women in Nandi, Kenya. Annals of Nutrition and Metabolism 2003;47:276-83.
Page 29 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
15. Zhao A, Zhang Y, Li B, Wang P, Li J, Xue Y, et al. Prevalence of Anemia and Its Risk Factors Among
Lactating Mothers in Myanmar. The American Journal of Tropical Medicine and Hygiene
2014;doi: 10.4269/ajtmh.13-0660.
16. WHO. Worldwide prevalence of anaemia 1993-2005 : WHO global database on anaemia / Edited by
Bruno de Benoist, Erin McLean, Ines Egli and Mary Cogswell, 2008.
17. WHO. Recommendations for the Prevention of Postpartum Haemorrhage (summary of results from
a WHO technical consultation, October 2006).Geneva, World Health Organization 2007.
18. Kibangou I, Bouhallab S, Henry G, Bureau F, Allouche S, Blais A, et al. Milk proteins and iron
absorption: contrasting effects of different caseinophosphopeptides. Pediatrics Research 2005
58(4):731-34.
19. Belachew T. Human Nutrition lecture note series for Health sciences students: Jimma Univesity
2005:pp 229.
20. Khanal V, Lee AH, Cruz JLNBd, Karkee R. Factors associated with non-utilisation of health service for
childbirth in Timor-Leste: evidence from the 2009-2010 Demographic and Health Survey. BMC
International Health and Human Rights 2014;14:14.
21. Kassa M, Abajobir AA, Gedefaw M. Level of male involvement and associated factors in family
planning services utilization among married men in Debremarkos town,Northwest Ethiopia.
BMC International Health and Human Rights 2014;14:33.
22. Gebremedhin S, Enquselassie F. Correlates of anemia among women of reproductive age in Ethiopia:
Evidence from Ethiopian DHS 2005. Ethiopian Journal of Health Development 2011;25(1):22-30.
23. Haidar J. Prevalence of Anaemia, Deficiencies of Iron and Folic Acid and Their Determinants in
Ethiopian Women. Journal of Health Population Nutrition 2010;28(4):359-68.
24. Okwu GN. Studies on the predisposing factors of iron deficiency anaemia among lactating women in
Owerri, Nigeria. International Research Journal of Biochemistry and Bioinformatics
2011;1(11):304-09.
25. Taruvinga A, Muchenje V, Mushunje A. Determinants of rural household dietary diversity: The case
of Amatole and Nyandeni districts, South Africa. International Journal of Development and
Sustainability 2013;2 (4).
26. Doan D. Does income growth improve diet diversity in China?Selected Paper prepared for
presentation at the 58 the AARES Annual Conference, Port Macquarie, New South Wales, 4-7
February 2014
27. Bodnar L, Cogswell M, Scanlon K. Low income postpartum women are at risk of iron deficiency.
Journal of Nutrition 2002;132:2298–302.
28. Sadeghian M, Fatourechi A, Lesanpezeshki M, Ahmadnezhad E. Prevalence of Anemia and Correlated
Factors in the Reproductive Age Women in Rural Areas of Tabas. Journal of Family and
Reproductive Health 2013;7(3):143.
29. Lovermail AA, Hartman M, Chia KS, Heymann DL. Demographic and Spatial Predictors of Anemia in
Women of Reproductive Age in Timor-Leste: Implications for Health Program Prioritization. PLoS
ONE 2013;9(3):e91252.
30. Liabsuetrakul T, for Southern Soil-transmitted Helminths and Maternal Health Working Group. Is
International or Asian Criteria-based Body Mass Index Associated with Maternal Anaemia, Low
Birthweight, and Preterm Births among Thai Population?—An Observational Study. Journal of
Health Population Nutrition 2011;29(3):218-28.
31. Blumfield M, Hure A, MacDonald-Wicks L, Smith R, Simpson S, Raubenheimer D, et al. The
association between the macronutrient content of maternal diet and the adequacy of
micronutrients during pregnancy in the Women and Their Children’s Health (WATCH) study.
Nutrients 2012;4(12):1958-76.
Page 30 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
32. Federal Ministry of Health-Ethiopia. National guideline for control and prevention of micronutrient
deficiencies 2004.
Page 31 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
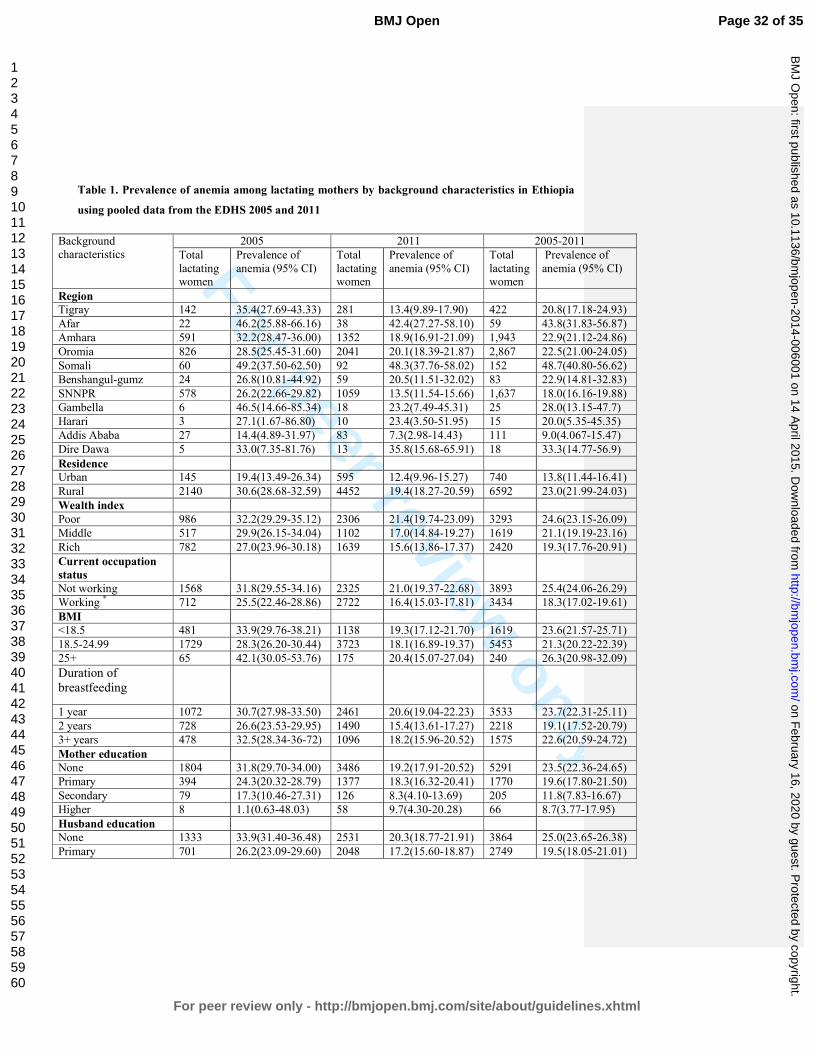
For peer review only
Table 1. Prevalence of anemia among lactating mothers by background characteristics in Ethiopia
using pooled data from the EDHS 2005 and 2011
Background
characteristics
2005 2011 2005-2011
Total
lactating women
Prevalence of
anemia (95% CI)
Total
lactating women
Prevalence of
anemia (95% CI)
Total
lactating women
Prevalence of
anemia (95% CI)
Region
Tigray 142 35.4(27.69-43.33) 281 13.4(9.89-17.90) 422 20.8(17.18-24.93)
Afar 22 46.2(25.88-66.16) 38 42.4(27.27-58.10) 59 43.8(31.83-56.87)
Amhara 591 32.2(28.47-36.00) 1352 18.9(16.91-21.09) 1,943 22.9(21.12-24.86)
Oromia 826 28.5(25.45-31.60) 2041 20.1(18.39-21.87) 2,867 22.5(21.00-24.05)
Somali 60 49.2(37.50-62.50) 92 48.3(37.76-58.02) 152 48.7(40.80-56.62)
Benshangul-gumz 24 26.8(10.81-44.92) 59 20.5(11.51-32.02) 83 22.9(14.81-32.83)
SNNPR 578 26.2(22.66-29.82) 1059 13.5(11.54-15.66) 1,637 18.0(16.16-19.88)
Gambella 6 46.5(14.66-85.34) 18 23.2(7.49-45.31) 25 28.0(13.15-47.7)
Harari 3 27.1(1.67-86.80) 10 23.4(3.50-51.95) 15 20.0(5.35-45.35)
Addis Ababa 27 14.4(4.89-31.97) 83 7.3(2.98-14.43) 111 9.0(4.067-15.47)
Dire Dawa 5 33.0(7.35-81.76) 13 35.8(15.68-65.91) 18 33.3(14.77-56.9)
Residence
Urban 145 19.4(13.49-26.34) 595 12.4(9.96-15.27) 740 13.8(11.44-16.41)
Rural 2140 30.6(28.68-32.59) 4452 19.4(18.27-20.59) 6592 23.0(21.99-24.03)
Wealth index
Poor 986 32.2(29.29-35.12) 2306 21.4(19.74-23.09) 3293 24.6(23.15-26.09)
Middle 517 29.9(26.15-34.04) 1102 17.0(14.84-19.27) 1619 21.1(19.19-23.16)
Rich 782 27.0(23.96-30.18) 1639 15.6(13.86-17.37) 2420 19.3(17.76-20.91)
Current occupation
status
Not working 1568 31.8(29.55-34.16) 2325 21.0(19.37-22.68) 3893 25.4(24.06-26.29)
Working * 712 25.5(22.46-28.86) 2722 16.4(15.03-17.81) 3434 18.3(17.02-19.61)
BMI
<18.5 481 33.9(29.76-38.21) 1138 19.3(17.12-21.70) 1619 23.6(21.57-25.71)
18.5-24.99 1729 28.3(26.20-30.44) 3723 18.1(16.89-19.37) 5453 21.3(20.22-22.39)
25+ 65 42.1(30.05-53.76) 175 20.4(15.07-27.04) 240 26.3(20.98-32.09)
Duration of
breastfeeding
1 year 1072 30.7(27.98-33.50) 2461 20.6(19.04-22.23) 3533 23.7(22.31-25.11)
2 years 728 26.6(23.53-29.95) 1490 15.4(13.61-17.27) 2218 19.1(17.52-20.79)
3+ years 478 32.5(28.34-36-72) 1096 18.2(15.96-20.52) 1575 22.6(20.59-24.72)
Mother education
None 1804 31.8(29.70-34.00) 3486 19.2(17.91-20.52) 5291 23.5(22.36-24.65)
Primary 394 24.3(20.32-28.79) 1377 18.3(16.32-20.41) 1770 19.6(17.80-21.50)
Secondary 79 17.3(10.46-27.31) 126 8.3(4.10-13.69) 205 11.8(7.83-16.67)
Higher 8 1.1(0.63-48.03) 58 9.7(4.30-20.28) 66 8.7(3.77-17.95)
Husband education
None 1333 33.9(31.40-36.48) 2531 20.3(18.77-21.91) 3864 25.0(23.65-26.38)
Primary 701 26.2(23.09-29.60) 2048 17.2(15.60-18.87) 2749 19.5(18.05-21.01)
Page 32 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Secondary 199 20.7(15.41-26.64) 238 14.3(10.26-19.17) 437 17.2(13.84-20.92)
Higher 23 14.8(3.43-31.53) 147 13.7(8.75-19.88) 170 13.8(8.99-19.30)
Family planning
Never use 1775 32.1(29.97-34.31) 2889 21.2(19.72-22.70) 4663 25.4(24.16-26.66)
Ever use 15 16.4(2.30-37.52) 2158 14.9(13.46-16.47) 2173 14.9(13.46.16.45)
ANC use
Never 1636 32.0(29.80-34.32) 2977 20.4(18.97-21-87) 4613 24.5(23.27-25.75)
1-3 386 27.7(23.43-32.35) 1208 18.4(16.27-20.64) 1594 20.6(18.65-22.62)
4+ 260 18.9(14.44-23.95) 845 12.6(10.44-14.91) 1105 14.1(12.16-16.27)
Iron supplementation
during pregnancy
No 2046 30.1(28.15-32.12) 4196 18.8(17.64-20.01) 6242 22.5(21.47-23.54)
Yes 236 27.1(21.74-33.06) 840 16.9(14.48-19.55) 1076 19.2(16.97-21.68)
Parity
1-4 1293 28.9(26.50-31.44) 3111 18.1(16.77-19.48) 4404 21.3(20.11-22.53)
5-9 903 30.5(27.52-33.52) 1739 19.6(17.79-21.53) 2642 23.3(21.73-24.96)
10+ 89 37.1(27.53-47.46) 197 17.0(12.02-12.46) 287 23.2(18.72-28.50)
Total 2285 29.9(28.04-31.79) 5047 18.5(17.45-19.60) 7332 22.1(21.13-23.03) ANC-Antenatal Care, BMI-Body Mass Index, *those mothers who currently work to earn money, ≠ those mothers
who do not currently engage in any type of formal work to earn money.*working includes
professional/technical/managerial, Clerical, Sales and Services, Skilled manual, Unskilled manual and Agriculture.
Table 2. Factors associated with anemia among lactating mothers in Ethiopia using pooled
data from the EDHS 2005 and 2011 Table 2: Logistic regression showing the association
between independent variables and anemia among lactating mothers in Ethiopia using pooled
data from the EDHS 2005 and 2011
Variables 2005 2011 2005-2011
COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI
Occupation
Not working* 1.00 1.00 1.00 1.00 1.00 1.00
Working*≠
0.82(0.66-1.00) 0.83(0.64-1.06) 0.62(0.54- 0.71) 0.68(0.58-0.78) 0.64(0.57-0.72) 0.71(0.63-0.80)
Wealth index
Poor 1.00 1.00 1.00 1.00 1.00 1.00
Middle 0.71(0.54-0.92) 0.82(0.61-1.10) 0.74(0.61- 0.89) 0.85(0.69-1.04) 0.74(0.64-0.87) 0.83(0.71-0.98)
Rich 0.66(0.53-0.82) 0.91(0.68-1.22) 0.62(0.52-0.72) 0.80(0.65-0.97) 0.65(0.57-0.73) 0.83(0.70-0.98)
FP use
Never used 1.00 1.00 1.00 1.00 1.00 1.00
Ever used 0.37(0.11-1.28) 0.51(0.14-1.91) 0.54(0.46-0.63) 0.69(0.58-0.82) 0.48(0.41-0.55) 0.68(0.57-0.80)
ANC attended
Never 1.00 1.00 1.00 1.00 1.00 1.00
1-3 0.78(0.59-1.03) 0.94(0.66-1.33) 0.78(0.59-1.00) 1.00(0.83-1.2) 0.81(0.71-0.94) 0.99(0.84-1.16)
4+ 0.55(0.41-0.74) 0.82(0.53-1.28) 0.55(0.41-0.74) 0.71(0.55-0.92) 0.52(0.44-0.61) 0.73(0.59-0.91)
Husband
education
None 1.00 1.00 1.00 1.00 1.00 1.00
Primary 0.77(0.61-0.96) 0.77(0.58-1.01) 0.69(0.59-0.80) 0.80(0.67-0.94) 0.69(0.61-0.78) 0.79(0.68-0.91)
Secondary 0.55(0.39-0.77) 0.83(0.50-1.38) 0.64(0.48-0.87) 0.81(0.58-1.14) 0.62(0.49-0.77) 0.83(0.62-1.09)
Page 33 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Higher 0.58(0.26-1.30) 0.50(0.73-3.40) 0.72(0.49-1.0) 0.96(0.61-1.52) 0.64(0.46-0.90) 0.94(0.61-1.45)
BMI
<18.5 1.00 1.00 1.00 1.00 1.00 1.00
18.5-24.99 0.74(0.59-0.92) 0.76(0.59-0.99) 0.74(0.64-0.86) 0.79(0.68-0.93) 0.76(0.67-0.86) 0.78(0.68-0.89)
25+ 1.1(0.62-1.90) 1.66(0.79-3.48) 0.82(0.58-1.2) 1.12(0.77-1.62) 0.85(0.64-1.12) 1.21(0.87-1.68)
Duration of
breastfeeding
1 year 1.00 1.00 1.00 1.00 1.00 1.00
2 years 0.79(0.64-0.99) 0.79(0.62-1.03) 0.71(0.60-0.83) 0.75(0.63-0.88) 0.75(0.66-0.85) 0.76(0.66-0.87)
3+ years 0.99(0.77-1.27) 1.10(0.82-1.49) 0.71(0.59-0.86) 0.82(0.67-0.99) 0.81(0.70-0.94) 0.89(0.76-1.05)
Time laps
2005 1.00 1.00
2011 0.65(0.58-0.73) 0.73(0.64-0.85) COR: Crude Odds Ratio, AOR: Adjusted Odds Ratio, BMI: Body Mass Index, ANC: Antenatal Care, 1.00 is the
reference category, *those mothers who currently work to earn money, ≠ those mothers who do not currently engage
in any type of formal work to earn money.* *working includes professional/technical/managerial, Clerical, Sales
and Services, Skilled manual, Unskilled manual and Agriculture.
Page 34 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
215x279mm (300 x 300 DPI)
Page 35 of 35
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Anemia prevalence and associated factors among lactating mothers in Ethiopia: Evidence from the 2005 and 2011
demographic and health surveys
Journal: BMJ Open
Manuscript ID: bmjopen-2014-006001.R3
Article Type: Research
Date Submitted by the Author: 20-Jan-2015
Complete List of Authors: Tarekegn, Yihunie; Ethiopian Public Helth Association, Project management Biadgilign, Sibhatu; Independent public health consultants, Addis Ababa, Ethiopia,
Haile, Demewoz; Madawalabu University,
<b>Primary Subject Heading</b>:
Public health
Secondary Subject Heading: Nutrition and metabolism, Public health, Health policy
Keywords: Anaemia < HAEMATOLOGY, NUTRITION & DIETETICS, Nutritional support < ONCOLOGY
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on F
ebruary 16, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006001 on 14 April 2015. D
ownloaded from

For peer review only
Anemia prevalence and associated factors among lactating mothers in Ethiopia: Evidence
from the 2005 and 2011 demographic and health surveys
Yihunie Lakew1, Sibhatu Biadgilign
2, Demewoz Haile
3*
1 Ethiopian Public Health Association, Addis Ababa, Ethiopia
2 Independent Public Health Consultant, Addis Ababa, Ethiopia
3 Department of Public Health, College of Medicine and Health sciences, Madawalabu
University, Ethiopia
Email address
Yihunie Lakew – [email protected]
Sibhatu Biadgilign- [email protected]
Demewoz Haile–[email protected]
*Corresponding author
Address of corresponding author
Department of Public Health
College of Medicine and Health sciences
Madawalabu University, Ethiopia
Bale Goba, P.O.Box 302
Running title: Factors associated with anemia among lactating mothers in Ethiopia
Key words: Lactating mothers, anemia, Ethiopia,
Word count: 2388
Page 1 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Abstract
Objective: To identify factors associated with anemia among lactating mothers in Ethiopia.
Design: A cross-sectional secondary data analysis pooled from two rounds of the 2005 and 2011
Ethiopian demographic and health survey (EDHS) was used. Multivariable logistic regression
model was applied to determine the factors associated with anemia.
Population: A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047 from EDHS
2011) were included from 11 administrative states of Ethiopia.
Main outcome measures: Lactating mothers considered as anemic if hemoglobin level <12
gram per deciliter.
Results: The overall prevalence of anemia among lactating mothers was 22.1% [95% CI: (21.13-
23.03)]. The highest prevalence was 48.7% [95% CI: (40.80-56.62)] found in Somali region,
followed by 43.8% [95% CI: (31.83-56.87)] in Afar region. The multivariable statistical model
showed that lactating mothers who had husbands attended primary education [AOR=0.79; 95%
CI: (0.68-0.91)], had been working in the last 12 months preceding the survey [AOR=0.71; 95%
CI: (0.63-0.80)],, had normal maternal body mass index (BMI) from 18.5kg/m2 to 24.99kg/m
2
[AOR=0.78; 95% CI: (0.68-0.89)], middle wealth quintile [AOR=0.83; 95% CI: (0.71-0.98)] and
rich wealth quintile [AOR=0.83; 95% CI: (0.70-0.98)], ever use of family planning [AOR=0.68;
95% CI: (0.57-0.80)], attending antenatal care (ANC) for indexed pregnancy four times or more
[AOR=0.73; 95% CI: (0.59-0.91)], experienced time variation between two surveys [AOR=0.73;
95%CI: (0.64-0.85)] and who breastfed for two years [AOR=0.76; 95% CI: (0.66-0.87)] were
factors associated with anemia.
Conclusion: Anemia is highly prevalent among lactating mothers, particularly among pastoralist
communities of Somali and Afar. Promoting partner education, improving maternal nutritional
status, creating behavioral change to use family planning and ANC services at health facilities
are recommended interventions to reduce the prevalence of anemia among lactating mothers in
Ethiopia.
Page 2 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
ARTICLE SUMMARY
Article focus
• Anemia is a serious nutritional problem, primarily affecting women of reproductive age
and children, and remains a major challenge in developing countries. In Ethiopia, more
than 20% of women in the reproductive age are anemic.
• Lactating mothers are among vulnerable groups with little information regarding social
determinants of anemia.
Key messages
• Anemia is a public health problem among lactating mothers in Ethiopia, with the highest
prevalence found in pastoralist regions of Somali and Afar.
• A statistically significant reduction of anemia prevalence among lactating mothers was
observed from 2005 to 2011.
• Being in middle and rich wealth quintiles, breastfeeding for two years, currently working,
normal body mass index, husbands’ primary education, ever use of family planning and
antenatal care attendance for four or more visits were factors associated with lower odds
of anemia.
Strength and Limitations
• The study attempted to identify factors associated with laboratory confirmed anemia
among lactating mothers at the national level. The study findings can be used to inform
policy and program actions.
• Some regions from which data was collected had small sample size. So that it should be
interpreted in caution. This study also shares the limitation of cross-sectional design
which makes difficult to demonstrate cause and effect relationships.
Page 3 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Introduction
Anemia is a serious nutrition problem affecting millions in developing countries, and remains a
major challenge for human health, social and economic development1. Lactating mothers are
among vulnerable groups of anemia. During the period of lactation, mothers are susceptible to
anemia due to maternal iron depletion and blood loss during childbirth2. Studies have shown that
though breast milk is not a good source of iron, the concentration of iron in breast milk is
independent of maternal iron status. This showed that the quality of breast milk is maintained at
the expense of maternal stores2 3.
Postpartum anemia has been found highest in mothers who were anemic during pregnancy4.
Furthermore, lactating mothers are highly susceptible to iron depletion if they have not had
enough energy and nutrient intake in their diets. Lactating mothers begin the postnatal period
after having iron depleted through the continuum from pregnancy to childbearing 5. A study from
South Africa showed that iron status was associated with depression, stress, and cognitive
functioning in poor African mothers during the postpartum period6. In a meta-analysis of
observational and intervention trials, Ross and Thomas, found that approximately 20% of the
maternal mortality seen in sub-Saharan Africa and South Asia was attributable to anemia that
was primarily the result of iron deficiency7.
Ethiopia is one of the countries in sub-Saharan Africa affected by anemia and it contributes to
high rates of maternal, infant and child mortality globally8 9
. In Ethiopia, the maternal mortality
ratio was 676 maternal deaths per 100,000 live births10
which is one of the highest in the world.
The country has considerably high infant and under 5 mortality rates that account for 59 and 88
deaths per 1000 live births, respectively 10.
Anemia testing was included in the two rounds of the Ethiopian demographic and health surveys
(EDHS). The prevalence of anemia among lactating mothers was 29.9% in 2005 and 18.5% in
201110,11. It was 30.6% in 2005 and 22% in 2011 among pregnant women and 23.9% in 2005
and 15% in 2011 among women neither non-pregnant nor lactating. This shows that a relatively
higher prevalence of anemia was found among Ethiopian pregnant and lactating mothers.
However, little information is available regarding socio-economic factors associated with anemia
Page 4 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
among lactating mothers. This study aimed to identify factors associated with anemia among
lactating mothers in Ethiopia using the pooled data of EDHS 2005 and 2011.
Methods
Data type and study design
This study is an in-depth analysis to identify factors associated with anemia among lactating
mothers based on cross-sectional secondary data of the EDHS 2005 and 2011 datasets. Both the
2005 and 2011 EDHS samples were selected using a stratified, two-stage cluster sampling
design. All women age 15-49 who were usual residents or who slept in the selected households
the night before the survey were eligible. The EDHS data include a women’s questionnaire that
measures socio-demographic characteristics of the mothers, information on reproductive health
and service use behaviours, as well as HIV and anemia test. The tool was pretested and translated
in to three local languages - Amharic, Oromefa and Tigregna. The EDHS was designed to
provide population and health indicators at national and regional levels. The survey is conducted
in every five years. The detailed methodology is found elsewhere10 11
.
Data Extraction
Both EDHS 2005 and 2011 data were downloaded with permission from the Measure DHS
website in SPSS format. After reviewing the detailed data coding, further data recoding was
completed. A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047 from EDHS
2011) were included in the analysis. Based on published literature, information on a wide-range
of socio-demographic and economic variables, health service related factors and anemia level
indicators were extracted. The chosen variables were region, residence, wealth index, occupation,
BMI, duration of breastfeeding, respondent’s education, husband’s education, family planning
use, iron tablet supplementation during pregnancy, time variation between two surveys, marital
status, age, parity and antenatal care attendance.
Measurement of variables
In both rounds of the EDHS, haemoglobin analysis was carried out onsite using a battery-
operated portable HemoCue analyzer for all anemia samples. The raw measured values of
haemoglobin were obtained using the HemoCue instrument and adjusted for altitude and
Page 5 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
smoking status10. Lactating mothers considered as anemic if hemoglobin level <12 gram per
deciliter. Haemoglobin (Hb) level of anemia was measured in g/dl, operationalised as a
categorical variable by predefined cut-off points for mild, moderate and severe anemia
recommended by the WHO for women above age 15 years. For this analysis, anemia was we re-
categorized anemia level as anemic and non-anemic from prior classifications in levels (no, mild,
moderate, severe) due to very small number of cases in the categories of severe and mild anemia
in all datasets of pooled and individual surveys.
Antenatal care (ANC) attendance referred to when women get services during pregnancy
according to the WHO recommendation of at least four ANC visits for low-risk pregnant
women. The frequency of the ANC visit is measured by asking the respondent to recall how
many times she had attended for the indexed child. Occupational status was defined as non-
working and working which comprises of professional/technical/managerial, clerical, sales and
services, skilled manual, unskilled manual and agriculture classifications. BMI (kg/m2) was
categorised using standard WHO classification into underweight <18.5 kg/m2, normal 18.5–24.9
kg/m2, overweight 25.0 kg/m
2 and above. Parity, defined as the number of children ever born,
was categorised as 1-4, 5-9 and 10+. The wealth index constructed from household assets and
characteristics available in both surveys to categorise individuals into wealth quintiles (poorest,
poorer, middle, rich and richest) was used. For the present analysis, the wealth index was re-
categorizedcollapsed into three groups (poor, middle and rich) to give a meaningful and practical
sub-population categories for designing program interventions in the general community.
Statistical analysis
For this study, the 2005 and 2011 EDHS data were pooled to achieve high power for detecting
the associated factors. Weighted proportions and odds ratios are presented to compromise
sampling probabilities. Sample weights were applied in order to compensate for the unequal
probability of selection between the strata that has been geographically defined as well as for
non-responses. A detailed explanation of the weighting procedure can be found in the EDHS
methodology report10. We used “svy” in STATA version 11 to weight the survey data and do the
analyses.
Formatted: Not Highlight
Formatted: Not Highlight
Page 6 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Descriptive statistics were used to show the prevalence of anemia among lactating mothers
varying by background characteristics. Binary and multivariable logistic regression statistical
analysis was carried out to determine the factors associated with anemia among lactating
mothers. Variables found statistically significant at p-value <0.25 during bivariate analysis were
analyzed in the multivariable logistic regression model12. This p-value cut off point prevented
removing variables that would potentially have an effect during multivariable analysis. Both
crude and adjusted odds ratios (OR) were reported with 95% confidence interval (CI). Variables
at p-value <0.05 were considered statistically significant in the multivariable logistic regression
model.
Ethical statements
The data were downloaded and used after communicating the purpose of the analysis and
receiving permission from Measure DHS Organization. The original EDHS data were collected
in accordance with international and national ethical guidelines.
Results
Majority of respondents (86%) were from rural. Nearly 60% of lactating mothers were Christian
followers followed by 38% of Muslims. The mean age of respondents was 28.4 with SD 6.8. The
overall prevalence of anemia among lactating mothers during 2005 to 2011 was found to be
22.1% (95% CI: 21.13-23.03). The prevalence of anemia for the years 2005 and 2011 was 29.9%
[95% CI: (28.04-31.79)] and 18.5% [95% CI: 17.45-19.60)], respectively. The prevalence was
13.8% [95% CI: (11.44-16.41)] in urban areas and 23% [95% CI: (21.99-24.03)] in rural areas.
In the period 2005 to 2011, the highest prevalence of anemia among lactating mothers was
48.7% [95%CI: (40.80-56.62)] found in Somali region, while the lowest prevalence was 9.0%
[95%CI: (4.07-15.47)] reported in Addis Ababa. In the period 2005 to 2011, the prevalence of
anemia in lactating mothers was consistently higher among those in the poor wealth index group,
not currently working, with BMI greater or equal to 25 kg/m2, one year duration of
breastfeeding, never educated, never used ANC, never used family planning services, no iron
tablet supplement during pregnancy, and with higher parity. A significant reduction in the
prevalence of anemia among lactating mothers was observed in all background variables from
2005 to 2011(Table 1). Figure 1 shows the classification of anemia in terms of its detailed
parameter.
Page 7 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
In the bivariate step of our analysis, age and marital status were not statistically significant in the
data from both individual surveys and pooled data with the cut-off point p<0.25. The variable
associated with anemia for the 2005 data was BMI, whereas for the 2011 data the variables were
working status, wealth index, ever use of family planning, ANC attendance four times and above
for indexed pregnancy, husband’s education, maternal BMI and duration of breastfeeding.
In the final multivariable model using pooled data, the independent predictors of anemia for
Ethiopian lactating mothers were currently working, wealth index, ever use of family planning,
ANC attendance four times and above for indexed pregnancy, husband’s education, maternal
BMI, time variation in the two surveys, and durations of breastfeeding.
Paternal educational status was found to be a predictor of anemia among lactating mothers.
Those lactating mothers who had husbands who attended primary education were at 21% less
likely to have anemia as compared to those mothers who had husbands with no education
[AOR=0.79; 95% CI: (0.68-0.91)].The odd of being anemic in working lactating mothers was
29% less as compared to their counter parts [AOR=0.71; 95% CI: (0.63-0.80)]. Those lactating
mothers having a normal maternal BMI (18.5kg/m2-24.99kg/m
2) were 22% less likely to be
anemic as compared to lactating mother with low BMI (<18.5kg/m2) [AOR=0.78; 95% CI:
(0.68-0.89)]. Similarly, lactating women who are categorized in middle [AOR=0.83; 95% CI:
(0.71-0.98)] and rich wealth quintiles [AOR=0.83; 95% CI: (0.70-0.98)] were each 17% less
likely to have anemia as compared to lactating women in poorer quintiles.
Among reproductive characteristics, family planning use and antenatal care (ANC) were the
significant factors associated with anemia in lactating mothers. Lactating mothers who ever used
family planning were 32% less likely to have anemia as compared to lactating mothers who
never used family planning [AOR=0.68; 95% CI: (0.57- 0.80)]. Lactating mothers who reported
ANC attendance four times or more for indexed pregnancy were 27% less likely to have anemia
as compared to mothers who never attended ANC [AOR=0.73; 95% CI: (0.59-0.91)]. Those
lactating mothers who breastfed for two years were 24% less likely to have anemia as compared
to lactating women who breastfed for one year [AOR=0.76; 95% CI: (0.66-0.87)] (Table 2).
Page 8 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Discussion
Over one fifth of lactating mothers were anemic in Ethiopia, which is lower as compared to other
developing countries. For example, 66.0% of lactating mothers have been reported as having
anemia in India13 and 43.8 % of lactating mothers in Kenya had a hemoglobin level <12 g/dl14.
Another study from Myanmar reported an anemia prevalence rate of 60.3% in lactating women,
with 20.3% of lactating mothers having severe anemia15. Although the prevalence of anemia
among lactating mothers in Ethiopia was relatively low as compared to these studies, it remains a
public health problem according to WHO classification16. The relatively better prevalence of
anemia in Ethiopia among lactating mothers may be due to the cultural norms of providing
nutritional care to lactating mothers during the postpartum period. During the postpartum period,
lactating mothers are encouraged to rest for 3 to 6 months and to eat a variety of foods including
animal sources, even during religious fasting periods. Iron supplementation coverage in Ethiopia
remained low among pregnant mothers10, despite its known contribution for reducing the risk of
postpartum hemorrhage17 Postpartum hemorrhage was also found to be one of the risk factors for
anemia during the period of lactation17.
This study showed that anemia is a widespread problem in the pastoralist communities of Somali
and Afar. The prevalence of anemia in lactating mothers was higher in the pastoralist regions and
showed slow decline in these regions from 2005 to 2011. This could be due to the fact that
pastoralist communities are heavily dependent on animal milk as a source of daily food, with
poor iron bioavailability18 19
. The other reason could be due to low utilization of family planning
and antenatal care services in pastoralist areas10.
One of the factors determined to be associated with anemia was paternal education. Having a
husband with a higher level of education was found to be associated with less odd of having
anemia among lactating mothers. This could be due to the fact that those educated husbands
might support their wives to use modern health services like family planning, ANC, postnatal
care which in turn reduce the odd of having anemia as well advised to eat a diversified diet.
However, maternal educational status was not statistically associated with anemia, which is
contradictory to many studies from Ethiopia and abroad15 20-22
. This might be one important
motivator to involve husbands in anemia prevention efforts.
Page 9 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Lactating mothers who had been working in the last 12 months preceding the survey had lower
odd of having anemia as compared to their counter parts. This might be due to working mothers
were earning money as compared to non-working mothers and the extra income enabled them to
access and purchase more food items, including animal sources (meat, poultry, fish etc), and
increase dietary diversity. Studies have shown that income growth improves diet diversity which
in turn improves micronutrient intake, including iron23 24
. Similarly, lactating mothers in the
lower wealth groups had greater odds of anemia as compared to lactating mothers in the higher
wealth quintiles. In many other studies, anemia among reproductive age women, the wealth
index was found to be a statistically significant factor15 20. Other studies have also shown that
women of low socio-economic status are at risk for iron deficiency anemia (IDA) in late
pregnancy and in the postpartum period25 26
. Therefore, women’s empowerment through
economic interventions and working status could have a positive contribution towards preventing
anemia.
This study also supports the importance of family planning for reducing the risk of anemia.
Those lactating mothers who have ever used family planning (modern or traditional) had a lower
odd of having anemia as compared to those who had never used family planning. This finding is
consistent with studies from Ethiopia and Timor-Leste which showed that use of family planning
was associated with lower odd of having anemia20 27.
Maternal nutritional status (as measured by body mass index) was found to be significantly
associated with anemia. As compared with undernourished lactating mothers (BMI<18.5kg/m2),
being in the normal BMI category (18.5-24.9kg/m2) was associated with a lower odd of having
anemia. This finding is consistent with a study from Ethiopia and Thailand20 28
. When a mother
is at risk of deficiency for macronutrients, most likely she is also at risk of other micronutrient
deficiencies such as iron29.
ANC attendance was found to be associated with less odd of having anemia among lactating
mothers. This is most likely due to the fact that during ANC attendance mothers have been
advised to take iron supplements according to the Ethiopian micronutrient guideline and
instructed to consume different sources of iron rich food items30. Therefore, improving iron
status during pregnancy also helps to prevent anemia during the lactation period.
Page 10 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Those mothers who breastfed for 2 years had lower odd of having anemia as compared to
mothers who breastfed for 1 year. This could be due to the effect of breastfeeding on maternal
depletion. Because those mothers who breastfeed younger children have high burden of
breastfeeding as compared to the older one. A study by Samson and his colleagues also found
that breastfeeding increases risk of anemia significantly20.
One of the strength of this study is to use laboratory confirmed anemia data at the national level.
Therefore, the study findings can be used to inform policy and program actions. However, the
study has caveats that some regions had small sample size, which questions the accuracy of
prevalence estimates per region, so that it should be interpreted in caution. The study did not
determine the presence of soil transmitted helminthes (STH) infection as it is associated with
anemia. This study also shares the limitation of cross-sectional study design which makes
difficult to demonstrate cause and effect relationships.
Conclusion
Anemia is a public health problem among lactating mothers in Ethiopia. There are regional
disparities regarding the prevalence of anemia, with the highest found in pastoralist regions of
Somali and Afar. Promoting partner education, improving maternal nutritional status, creating
behavioral change to use family planning and attend ANC services at health facilities are
recommended interventions to reduce the prevalence of anemia among lactating women in
Ethiopia.
Competing interests
The authors declare that they have no competing interests.
Funding statement
This research received no specific grant from any funding agency in the public, commercial or
not-for-profit sectors'
Authors’ contributions
YL and DH conceptualized the research idea. YL analyzed and interpreted the data and critically
reviewed the manuscript. SB assisted in data interpretation and critically reviewed the
Page 11 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
manuscript. DH drafted the manuscript, assisted in the data analysis and interpretation and
critically reviewed the manuscript. All authors reviewed and approved the manuscript.
Acknowledgements
The authors acknowledge DHS Measure for granting the data freely. We are also grateful to
thank Lianna Tabar, country representative of KHI-E, for her professional language editing and
reviewing the manuscript.
References
1. WHO. The world health report. Reducing risks, promoting healthy life. Geneva, World Health
Organization. 2002.
2. Whitney E, Rolfes SR. Understanding Nutrition. In: Adams P, editor. Eleventh Edition ed. United States
of America: Thomson Learning Academic Resource Center, 2008.
3. Domell V, Lonnerdal B, Dewey K, Cohen R, Hernell O. Iron zinc and copper concentrations in breast
milk are independent of maternal status. American Journal of clinical nutrition 2004;79(1):111-
15.
4. Bodnar L, Scanlon K, Freedman D, Siega–Riz A, Cogswell M. High prevalence of postpartum anaemia
among Low income women in the United States. Journal of obstetrics and Gynecology
2001;185:4348-53.
5. Sserunjogi L, Scheut F, Whyte SR. Postnatal anaemia: neglected problems and missed opportunities in
Uganda. Health Policy and Planning 2003;18(2):225-31.
6. Beard JL, Hendricks MK, Perez EM, Murray-Kolb LE, Berg A, Vernon-Feagans L, et al. Maternal Iron
Deficiency Anemia Affects Postpartum Emotions and Cognition. Journal of Nutrition
2005;135:267–72.
7. Ross J, Thomas E. Iron deficiency anemia and maternal mortality. PROFILES 3 working notes series no.
3. Academy for Education Development, Washington D.C., 1996.
8. Brabin BJ, Hakimin M, Pelletier D. An Analysis of Anemia and Pregnancy-Related Maternal Mortality.
The Journal of Nutrition 2001;131:604S-15S.
9. Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, Lozano R, et al. A systematic analysis of
global anemia burden from 1990 to 2010. Blood 2014;123(5).
10. Central Statistical Agency (CSA) Ethiopia. Demographic and Health Survey 2011. Addis Ababa,
Ethiopia and Calverton, Maryland, USA: CSA and ORC Macro. 2011.
11. Central Statistical Agency(CSA). Demographic and Health Survey 2005. Addis Ababa, Ethiopia and
Calverton, Maryland, USA: CSA and ORC Macro, 2005.
12. Peter C, Jack V. Automated variable selection methods for logistic regression produced unstable
models for predicting acute myocardial infarction mortality. Journal of Clinical Epidemiology
2004;57:1138-46.
13. Singh AB, Kandpal SD, Chandra R, Srivastava VK, Negi KS. Anemia amongst pregnant and lactating
women in district Dehradun. Indian Journal of Preventive and Social Medicine 2009;40(1):20-21.
14. Ettyanga GA, Oloob WDvMLA, Saris WHM. Serum Retinol, Iron Status and Body Composition of
Lactating Women in Nandi, Kenya. Annals of Nutrition and Metabolism 2003;47:276-83.
Page 12 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
15. Zhao A, Zhang Y, Li B, Wang P, Li J, Xue Y, et al. Prevalence of Anemia and Its Risk Factors Among
Lactating Mothers in Myanmar. The American Journal of Tropical Medicine and Hygiene
2014;doi: 10.4269/ajtmh.13-0660.
16. WHO. Worldwide prevalence of anaemia 1993-2005 : WHO global database on anaemia / Edited by
Bruno de Benoist, Erin McLean, Ines Egli and Mary Cogswell, 2008.
17. WHO. Recommendations for the Prevention of Postpartum Haemorrhage (summary of results from
a WHO technical consultation, October 2006).Geneva, World Health Organization 2007.
18. Kibangou I, Bouhallab S, Henry G, Bureau F, Allouche S, Blais A, et al. Milk proteins and iron
absorption: contrasting effects of different caseinophosphopeptides. Pediatrics Research 2005
58(4):731-34.
19. Belachew T. Human Nutrition lecture note series for Health sciences students: Jimma Univesity
2005:pp 229.
20. Gebremedhin S, Enquselassie F. Correlates of anemia among women of reproductive age in Ethiopia:
Evidence from Ethiopian DHS 2005. Ethiopian Journal of Health Development 2011;25(1):22-30.
21. Haidar J. Prevalence of Anaemia, Deficiencies of Iron and Folic Acid and Their Determinants in
Ethiopian Women. Journal of Health Population Nutrition 2010;28(4):359-68.
22. Okwu GN. Studies on the predisposing factors of iron deficiency anaemia among lactating women in
Owerri, Nigeria. International Research Journal of Biochemistry and Bioinformatics
2011;1(11):304-09.
23. Taruvinga A, Muchenje V, Mushunje A. Determinants of rural household dietary diversity: The case
of Amatole and Nyandeni districts, South Africa. International Journal of Development and
Sustainability 2013;2 (4).
24. Doan D. Does income growth improve diet diversity in China?Selected Paper prepared for
presentation at the 58 the AARES Annual Conference, Port Macquarie, New South Wales, 4-7
February 2014
25. Bodnar L, Cogswell M, Scanlon K. Low income postpartum women are at risk of iron deficiency.
Journal of Nutrition 2002;132:2298–302.
26. Sadeghian M, Fatourechi A, Lesanpezeshki M, Ahmadnezhad E. Prevalence of Anemia and Correlated
Factors in the Reproductive Age Women in Rural Areas of Tabas. Journal of Family and
Reproductive Health 2013;7(3):143.
27. Lovermail AA, Hartman M, Chia KS, Heymann DL. Demographic and Spatial Predictors of Anemia in
Women of Reproductive Age in Timor-Leste: Implications for Health Program Prioritization. PLoS
ONE 2013;9(3):e91252.
28. Liabsuetrakul T, for Southern Soil-transmitted Helminths and Maternal Health Working Group. Is
International or Asian Criteria-based Body Mass Index Associated with Maternal Anaemia, Low
Birthweight, and Preterm Births among Thai Population?—An Observational Study. Journal of
Health Population Nutrition 2011;29(3):218-28.
29. Blumfield M, Hure A, MacDonald-Wicks L, Smith R, Simpson S, Raubenheimer D, et al. The
association between the macronutrient content of maternal diet and the adequacy of
micronutrients during pregnancy in the Women and Their Children’s Health (WATCH) study.
Nutrients 2012;4(12):1958-76.
30. Federal Ministry of Health-Ethiopia. National guideline for control and prevention of micronutrient
deficiencies 2004.
Page 13 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Table 1. Prevalence of anemia among lactating mothers by background characteristics in Ethiopia
using pooled data from the EDHS 2005 and 2011
Background
characteristics
2005 2011 2005-2011
Total
lactating women
Prevalence of
anemia (95% CI)
Total
lactating women
Prevalence of
anemia (95% CI)
Total
lactating women
Prevalence of
anemia (95% CI)
Region
Tigray 142 35.4(27.69-43.33) 281 13.4(9.89-17.90) 422 20.8(17.18-24.93)
Afar 22 46.2(25.88-66.16) 38 42.4(27.27-58.10) 59 43.8(31.83-56.87)
Amhara 591 32.2(28.47-36.00) 1352 18.9(16.91-21.09) 1,943 22.9(21.12-24.86)
Oromia 826 28.5(25.45-31.60) 2041 20.1(18.39-21.87) 2,867 22.5(21.00-24.05)
Somali 60 49.2(37.50-62.50) 92 48.3(37.76-58.02) 152 48.7(40.80-56.62)
Benshangul-gumz 24 26.8(10.81-44.92) 59 20.5(11.51-32.02) 83 22.9(14.81-32.83)
SNNPR 578 26.2(22.66-29.82) 1059 13.5(11.54-15.66) 1,637 18.0(16.16-19.88)
Gambella 6 46.5(14.66-85.34) 18 23.2(7.49-45.31) 25 28.0(13.15-47.7)
Harari 3 27.1(1.67-86.80) 10 23.4(3.50-51.95) 15 20.0(5.35-45.35)
Addis Ababa 27 14.4(4.89-31.97) 83 7.3(2.98-14.43) 111 9.0(4.067-15.47)
Dire Dawa 5 33.0(7.35-81.76) 13 35.8(15.68-65.91) 18 33.3(14.77-56.9)
Residence
Urban 145 19.4(13.49-26.34) 595 12.4(9.96-15.27) 740 13.8(11.44-16.41)
Rural 2140 30.6(28.68-32.59) 4452 19.4(18.27-20.59) 6592 23.0(21.99-24.03)
Wealth index
Poor 986 32.2(29.29-35.12) 2306 21.4(19.74-23.09) 3293 24.6(23.15-26.09)
Middle 517 29.9(26.15-34.04) 1102 17.0(14.84-19.27) 1619 21.1(19.19-23.16)
Rich 782 27.0(23.96-30.18) 1639 15.6(13.86-17.37) 2420 19.3(17.76-20.91)
Current occupation
status
Not working 1568 31.8(29.55-34.16) 2325 21.0(19.37-22.68) 3893 25.4(24.06-26.29)
Working * 712 25.5(22.46-28.86) 2722 16.4(15.03-17.81) 3434 18.3(17.02-19.61)
BMI
<18.5 481 33.9(29.76-38.21) 1138 19.3(17.12-21.70) 1619 23.6(21.57-25.71)
18.5-24.99 1729 28.3(26.20-30.44) 3723 18.1(16.89-19.37) 5453 21.3(20.22-22.39)
25+ 65 42.1(30.05-53.76) 175 20.4(15.07-27.04) 240 26.3(20.98-32.09)
Duration of
breastfeeding
1 year 1072 30.7(27.98-33.50) 2461 20.6(19.04-22.23) 3533 23.7(22.31-25.11)
2 years 728 26.6(23.53-29.95) 1490 15.4(13.61-17.27) 2218 19.1(17.52-20.79)
3+ years 478 32.5(28.34-36-72) 1096 18.2(15.96-20.52) 1575 22.6(20.59-24.72)
Mother education
None 1804 31.8(29.70-34.00) 3486 19.2(17.91-20.52) 5291 23.5(22.36-24.65)
Primary 394 24.3(20.32-28.79) 1377 18.3(16.32-20.41) 1770 19.6(17.80-21.50)
Secondary 79 17.3(10.46-27.31) 126 8.3(4.10-13.69) 205 11.8(7.83-16.67)
Higher 8 1.1(0.63-48.03) 58 9.7(4.30-20.28) 66 8.7(3.77-17.95)
Husband education
None 1333 33.9(31.40-36.48) 2531 20.3(18.77-21.91) 3864 25.0(23.65-26.38)
Primary 701 26.2(23.09-29.60) 2048 17.2(15.60-18.87) 2749 19.5(18.05-21.01)
Page 14 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
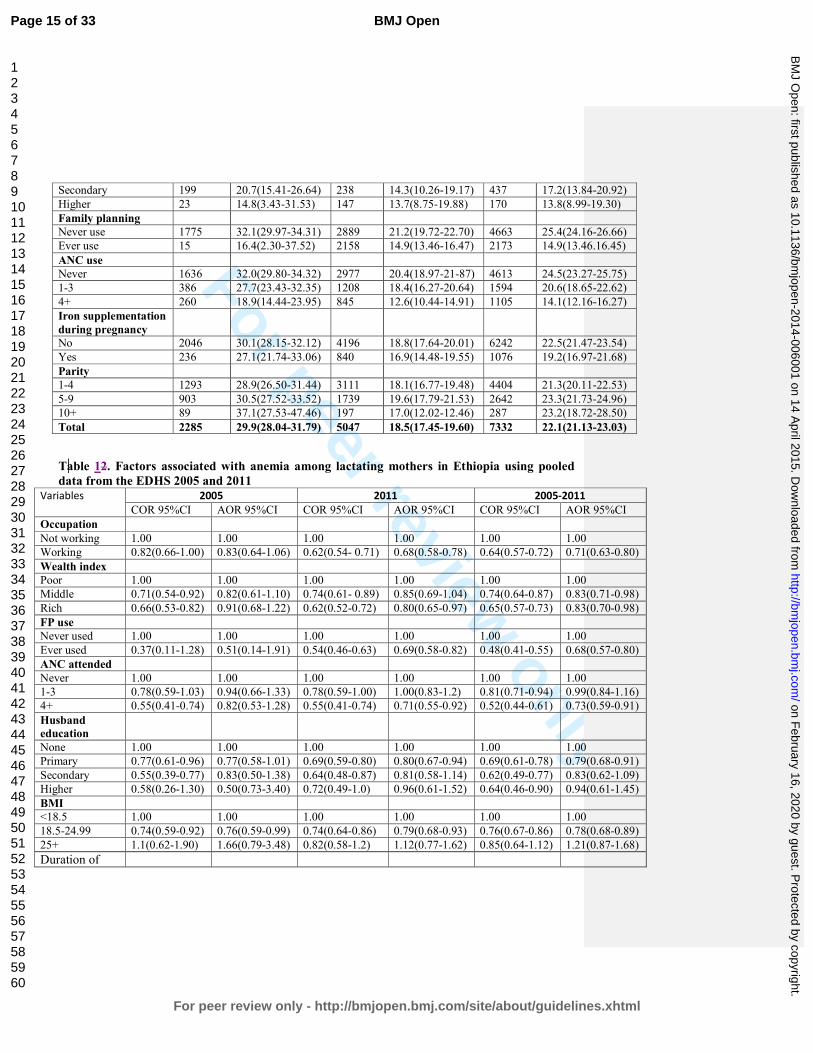
For peer review only
Secondary 199 20.7(15.41-26.64) 238 14.3(10.26-19.17) 437 17.2(13.84-20.92)
Higher 23 14.8(3.43-31.53) 147 13.7(8.75-19.88) 170 13.8(8.99-19.30)
Family planning
Never use 1775 32.1(29.97-34.31) 2889 21.2(19.72-22.70) 4663 25.4(24.16-26.66)
Ever use 15 16.4(2.30-37.52) 2158 14.9(13.46-16.47) 2173 14.9(13.46.16.45)
ANC use
Never 1636 32.0(29.80-34.32) 2977 20.4(18.97-21-87) 4613 24.5(23.27-25.75)
1-3 386 27.7(23.43-32.35) 1208 18.4(16.27-20.64) 1594 20.6(18.65-22.62)
4+ 260 18.9(14.44-23.95) 845 12.6(10.44-14.91) 1105 14.1(12.16-16.27)
Iron supplementation
during pregnancy
No 2046 30.1(28.15-32.12) 4196 18.8(17.64-20.01) 6242 22.5(21.47-23.54)
Yes 236 27.1(21.74-33.06) 840 16.9(14.48-19.55) 1076 19.2(16.97-21.68)
Parity
1-4 1293 28.9(26.50-31.44) 3111 18.1(16.77-19.48) 4404 21.3(20.11-22.53)
5-9 903 30.5(27.52-33.52) 1739 19.6(17.79-21.53) 2642 23.3(21.73-24.96)
10+ 89 37.1(27.53-47.46) 197 17.0(12.02-12.46) 287 23.2(18.72-28.50)
Total 2285 29.9(28.04-31.79) 5047 18.5(17.45-19.60) 7332 22.1(21.13-23.03)
Table 12. Factors associated with anemia among lactating mothers in Ethiopia using pooled
data from the EDHS 2005 and 2011 Variables 2005 2011 2005-2011
COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI
Occupation
Not working 1.00 1.00 1.00 1.00 1.00 1.00
Working 0.82(0.66-1.00) 0.83(0.64-1.06) 0.62(0.54- 0.71) 0.68(0.58-0.78) 0.64(0.57-0.72) 0.71(0.63-0.80)
Wealth index
Poor 1.00 1.00 1.00 1.00 1.00 1.00
Middle 0.71(0.54-0.92) 0.82(0.61-1.10) 0.74(0.61- 0.89) 0.85(0.69-1.04) 0.74(0.64-0.87) 0.83(0.71-0.98)
Rich 0.66(0.53-0.82) 0.91(0.68-1.22) 0.62(0.52-0.72) 0.80(0.65-0.97) 0.65(0.57-0.73) 0.83(0.70-0.98)
FP use
Never used 1.00 1.00 1.00 1.00 1.00 1.00
Ever used 0.37(0.11-1.28) 0.51(0.14-1.91) 0.54(0.46-0.63) 0.69(0.58-0.82) 0.48(0.41-0.55) 0.68(0.57-0.80)
ANC attended
Never 1.00 1.00 1.00 1.00 1.00 1.00
1-3 0.78(0.59-1.03) 0.94(0.66-1.33) 0.78(0.59-1.00) 1.00(0.83-1.2) 0.81(0.71-0.94) 0.99(0.84-1.16)
4+ 0.55(0.41-0.74) 0.82(0.53-1.28) 0.55(0.41-0.74) 0.71(0.55-0.92) 0.52(0.44-0.61) 0.73(0.59-0.91)
Husband
education
None 1.00 1.00 1.00 1.00 1.00 1.00
Primary 0.77(0.61-0.96) 0.77(0.58-1.01) 0.69(0.59-0.80) 0.80(0.67-0.94) 0.69(0.61-0.78) 0.79(0.68-0.91)
Secondary 0.55(0.39-0.77) 0.83(0.50-1.38) 0.64(0.48-0.87) 0.81(0.58-1.14) 0.62(0.49-0.77) 0.83(0.62-1.09)
Higher 0.58(0.26-1.30) 0.50(0.73-3.40) 0.72(0.49-1.0) 0.96(0.61-1.52) 0.64(0.46-0.90) 0.94(0.61-1.45)
BMI
<18.5 1.00 1.00 1.00 1.00 1.00 1.00
18.5-24.99 0.74(0.59-0.92) 0.76(0.59-0.99) 0.74(0.64-0.86) 0.79(0.68-0.93) 0.76(0.67-0.86) 0.78(0.68-0.89)
25+ 1.1(0.62-1.90) 1.66(0.79-3.48) 0.82(0.58-1.2) 1.12(0.77-1.62) 0.85(0.64-1.12) 1.21(0.87-1.68)
Duration of
Page 15 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
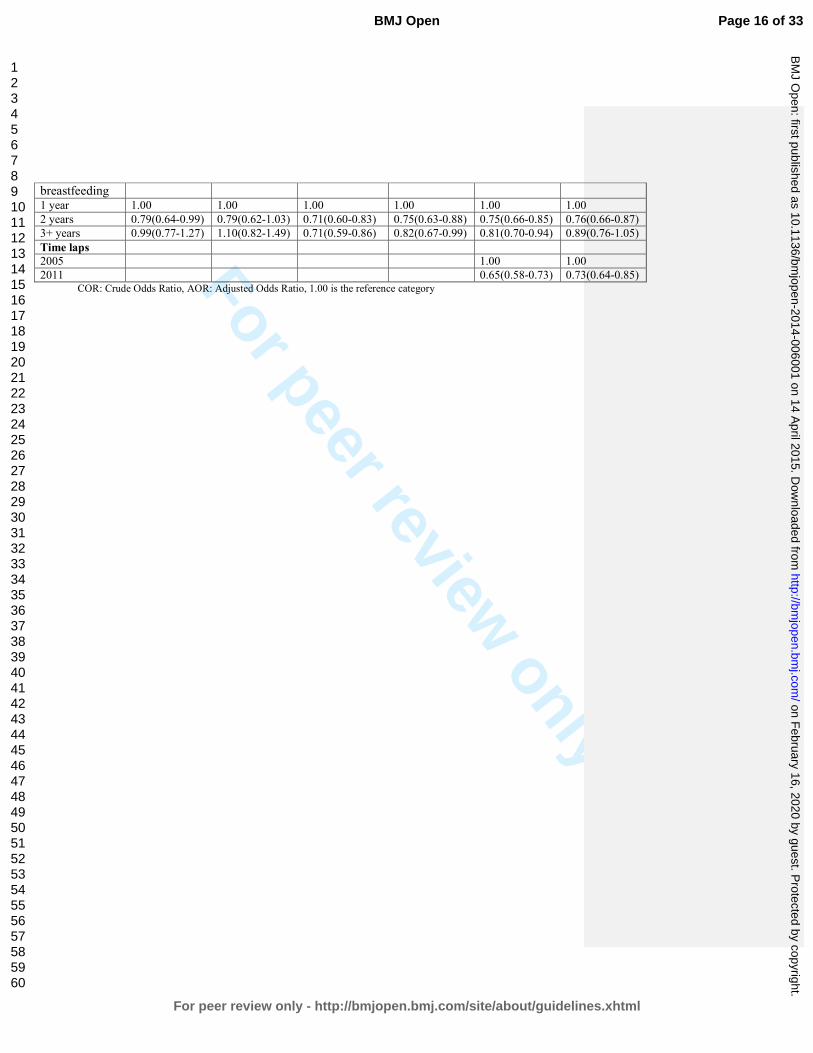
For peer review only
breastfeeding 1 year 1.00 1.00 1.00 1.00 1.00 1.00
2 years 0.79(0.64-0.99) 0.79(0.62-1.03) 0.71(0.60-0.83) 0.75(0.63-0.88) 0.75(0.66-0.85) 0.76(0.66-0.87)
3+ years 0.99(0.77-1.27) 1.10(0.82-1.49) 0.71(0.59-0.86) 0.82(0.67-0.99) 0.81(0.70-0.94) 0.89(0.76-1.05)
Time laps
2005 1.00 1.00
2011 0.65(0.58-0.73) 0.73(0.64-0.85) COR: Crude Odds Ratio, AOR: Adjusted Odds Ratio, 1.00 is the reference category
Page 16 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Anemia prevalence and associated factors among lactating mothers in Ethiopia: Evidence
from the 2005 and 2011 demographic and health surveys
Yihunie Lakew1, Sibhatu Biadgilign
2, Demewoz Haile
3*
1 Ethiopian Public Health Association, Addis Ababa, Ethiopia
2 Independent Public Health Consultant, Addis Ababa, Ethiopia
3 Department of Public Health, College of Medicine and Health sciences, Madawalabu
University, Ethiopia
Email address
Yihunie Lakew – [email protected]
Sibhatu Biadgilign- [email protected]
Demewoz Haile–[email protected]
*Corresponding author
Address of corresponding author
Department of Public Health
College of Medicine and Health sciences
Madawalabu University, Ethiopia
Bale Goba, P.O.Box 302
Running title: Factors associated with anemia among lactating mothers in Ethiopia
Key words: Lactating mothers, anemia, Ethiopia,
Word count: 2388
Page 17 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
Abstract
Objective: To identify factors associated with anemia among lactating mothers in Ethiopia.
Design: A cross-sectional secondary data analysis pooled from two rounds of the 2005 and 2011
Ethiopian demographic and health survey (EDHS) was used. Multivariable logistic regression
model was applied to determine the factors associated with anemia.
Population: A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047 from EDHS
2011) were included from 11 administrative states of Ethiopia.
Main outcome measures: Lactating mothers considered as anemic if hemoglobin level <12
gram per deciliter.
Results: The overall prevalence of anemia among lactating mothers was 22.1% [95% CI: (21.13-
23.03)]. The highest prevalence was 48.7% [95% CI: (40.80-56.62)] found in Somali region,
followed by 43.8% [95% CI: (31.83-56.87)] in Afar region. The multivariable statistical model
showed that lactating mothers who had husbands attended primary education [AOR=0.79; 95%
CI: (0.68-0.91)], had been working in the last 12 months preceding the survey [AOR=0.71; 95%
CI: (0.63-0.80)],, had normal maternal body mass index (BMI) from 18.5kg/m2 to 24.99kg/m
2
[AOR=0.78; 95% CI: (0.68-0.89)], middle wealth quintile [AOR=0.83; 95% CI: (0.71-0.98)] and
rich wealth quintile [AOR=0.83; 95% CI: (0.70-0.98)], ever use of family planning [AOR=0.68;
95% CI: (0.57-0.80)], attending antenatal care (ANC) for indexed pregnancy four times or more
[AOR=0.73; 95% CI: (0.59-0.91)], experienced time variation between two surveys [AOR=0.73;
95%CI: (0.64-0.85)] and who breastfed for two years [AOR=0.76; 95% CI: (0.66-0.87)] were
factors associated with anemia.
Conclusion: Anemia is highly prevalent among lactating mothers, particularly among pastoralist
communities of Somali and Afar. Promoting partner education, improving maternal nutritional
status, creating behavioral change to use family planning and ANC services at health facilities
are recommended interventions to reduce the prevalence of anemia among lactating mothers in
Ethiopia.
Page 18 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
ARTICLE SUMMARY
Article focus
• Anemia is a serious nutritional problem, primarily affecting women of reproductive age
and children, and remains a major challenge in developing countries. In Ethiopia, more
than 20% of women in the reproductive age are anemic.
• Lactating mothers are among vulnerable groups with little information regarding social
determinants of anemia.
Key messages
• Anemia is a public health problem among lactating mothers in Ethiopia, with the highest
prevalence found in pastoralist regions of Somali and Afar.
• A statistically significant reduction of anemia prevalence among lactating mothers was
observed from 2005 to 2011.
• Being in middle and rich wealth quintiles, breastfeeding for two years, currently working,
normal body mass index, husbands’ primary education, ever use of family planning and
antenatal care attendance for four or more visits were factors associated with lower odds
of anemia.
Strength and Limitations
• The study attempted to identify factors associated with laboratory confirmed anemia
among lactating mothers at the national level. The study findings can be used to inform
policy and program actions.
• Some regions from which data was collected had small sample size. So that it should be
interpreted in caution. This study also shares the limitation of cross-sectional design
which makes difficult to demonstrate cause and effect relationships.
Page 19 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Introduction
Anemia is a serious nutrition problem affecting millions in developing countries, and remains a
major challenge for human health, social and economic development1. Lactating mothers are
among vulnerable groups of anemia. During the period of lactation, mothers are susceptible to
anemia due to maternal iron depletion and blood loss during childbirth2. Studies have shown that
though breast milk is not a good source of iron, the concentration of iron in breast milk is
independent of maternal iron status. This showed that the quality of breast milk is maintained at
the expense of maternal stores2 3.
Postpartum anemia has been found highest in mothers who were anemic during pregnancy4.
Furthermore, lactating mothers are highly susceptible to iron depletion if they have not had
enough energy and nutrient intake in their diets. Lactating mothers begin the postnatal period
after having iron depleted through the continuum from pregnancy to childbearing 5. A study from
South Africa showed that iron status was associated with depression, stress, and cognitive
functioning in poor African mothers during the postpartum period6. In a meta-analysis of
observational and intervention trials, Ross and Thomas, found that approximately 20% of the
maternal mortality seen in sub-Saharan Africa and South Asia was attributable to anemia that
was primarily the result of iron deficiency7.
Ethiopia is one of the countries in sub-Saharan Africa affected by anemia and it contributes to
high rates of maternal, infant and child mortality globally8 9
. In Ethiopia, the maternal mortality
ratio was 676 maternal deaths per 100,000 live births10
which is one of the highest in the world.
The country has considerably high infant and under 5 mortality rates that account for 59 and 88
deaths per 1000 live births, respectively 10.
Anemia testing was included in the two rounds of the Ethiopian demographic and health surveys
(EDHS). The prevalence of anemia among lactating mothers was 29.9% in 2005 and 18.5% in
201110,11. It was 30.6% in 2005 and 22% in 2011 among pregnant women and 23.9% in 2005
and 15% in 2011 among women neither non-pregnant nor lactating. This shows that a relatively
higher prevalence of anemia was found among Ethiopian pregnant and lactating mothers.
However, little information is available regarding socio-economic factors associated with anemia
Page 20 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
among lactating mothers. This study aimed to identify factors associated with anemia among
lactating mothers in Ethiopia using the pooled data of EDHS 2005 and 2011.
Methods
Data type and study design
This study is an in-depth analysis to identify factors associated with anemia among lactating
mothers based on cross-sectional secondary data of the EDHS 2005 and 2011 datasets. Both the
2005 and 2011 EDHS samples were selected using a stratified, two-stage cluster sampling
design. All women age 15-49 who were usual residents or who slept in the selected households
the night before the survey were eligible. The EDHS data include a women’s questionnaire that
measures socio-demographic characteristics of the mothers, information on reproductive health
and service use behaviours, as well as HIV and anemia test. The tool was pretested and translated
in to three local languages - Amharic, Oromefa and Tigregna. The EDHS was designed to
provide population and health indicators at national and regional levels. The survey is conducted
in every five years. The detailed methodology is found elsewhere10 11
.
Data Extraction
Both EDHS 2005 and 2011 data were downloaded with permission from the Measure DHS
website in SPSS format. After reviewing the detailed data coding, further data recoding was
completed. A total of 7,332 lactating mothers (2,285 from EDHS 2005 and 5,047 from EDHS
2011) were included in the analysis. Based on published literature, information on a wide-range
of socio-demographic and economic variables, health service related factors and anemia level
indicators were extracted. The chosen variables were region, residence, wealth index, occupation,
BMI, duration of breastfeeding, respondent’s education, husband’s education, family planning
use, iron tablet supplementation during pregnancy, time variation between two surveys, marital
status, age, parity and antenatal care attendance.
Measurement of variables
In both rounds of the EDHS, haemoglobin analysis was carried out onsite using a battery-
operated portable HemoCue analyzer for all anemia samples. The raw measured values of
haemoglobin were obtained using the HemoCue instrument and adjusted for altitude and
Page 21 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
For peer review only
smoking status10. Lactating mothers considered as anemic if hemoglobin level <12 gram per
deciliter. Haemoglobin (Hb) level of anemia was measured in g/dl, operationalised as a
categorical variable by predefined cut-off points for mild, moderate and severe anemia
recommended by the WHO for women above age 15 years. For this analysis, we re-categorized
anemia level as anemic and non-anemic from prior classifications in levels (no, mild, moderate,
severe) due to very small number of cases in the categories of severe and mild anemia in all
datasets of pooled and individual surveys.
Antenatal care (ANC) attendance referred to when women get services during pregnancy
according to the WHO recommendation of at least four ANC visits for low-risk pregnant
women. The frequency of the ANC visit is measured by asking the respondent to recall how
many times she had attended for the indexed child. Occupational status was defined as non-
working and working which comprises of professional/technical/managerial, clerical, sales and
services, skilled manual, unskilled manual and agriculture classifications. BMI (kg/m2) was
categorised using standard WHO classification into underweight <18.5 kg/m2, normal 18.5–24.9
kg/m2, overweight 25.0 kg/m
2 and above. Parity, defined as the number of children ever born,
was categorised as 1-4, 5-9 and 10+. The wealth index constructed from household assets and
characteristics available in both surveys to categorise individuals into wealth quintiles (poorest,
poorer, middle, rich and richest) was used. For the present analysis, the wealth index was
collapsed into three groups (poor, middle and rich) to give a meaningful and practical sub-
population categories for designing program interventions in the general community.
Statistical analysis
For this study, the 2005 and 2011 EDHS data were pooled to achieve high power for detecting
the associated factors. Weighted proportions and odds ratios are presented to compromise
sampling probabilities. Sample weights were applied in order to compensate for the unequal
probability of selection between the strata that has been geographically defined as well as for
non-responses. A detailed explanation of the weighting procedure can be found in the EDHS
methodology report10. We used “svy” in STATA version 11 to weight the survey data and do the
analyses.
Formatted: Not Highlight
Formatted: Not Highlight
Page 22 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Descriptive statistics were used to show the prevalence of anemia among lactating mothers
varying by background characteristics. Binary and multivariable logistic regression statistical
analysis was carried out to determine the factors associated with anemia among lactating
mothers. Variables found statistically significant at p-value <0.25 during bivariate analysis were
analyzed in the multivariable logistic regression model12. This p-value cut off point prevented
removing variables that would potentially have an effect during multivariable analysis. Both
crude and adjusted odds ratios (OR) were reported with 95% confidence interval (CI). Variables
at p-value <0.05 were considered statistically significant in the multivariable logistic regression
model.
Ethical statements
The data were downloaded and used after communicating the purpose of the analysis and
receiving permission from Measure DHS Organization. The original EDHS data were collected
in accordance with international and national ethical guidelines.
Results
Majority of respondents (86%) were from rural. Nearly 60% of lactating mothers were Christian
followers followed by 38% of Muslims. The mean age of respondents was 28.4 with SD 6.8. The
overall prevalence of anemia among lactating mothers during 2005 to 2011 was found to be
22.1% (95% CI: 21.13-23.03). The prevalence of anemia for the years 2005 and 2011 was 29.9%
[95% CI: (28.04-31.79)] and 18.5% [95% CI: 17.45-19.60)], respectively. The prevalence was
13.8% [95% CI: (11.44-16.41)] in urban areas and 23% [95% CI: (21.99-24.03)] in rural areas.
In the period 2005 to 2011, the highest prevalence of anemia among lactating mothers was
48.7% [95%CI: (40.80-56.62)] found in Somali region, while the lowest prevalence was 9.0%
[95%CI: (4.07-15.47)] reported in Addis Ababa. In the period 2005 to 2011, the prevalence of
anemia in lactating mothers was consistently higher among those in the poor wealth index group,
not currently working, with BMI greater or equal to 25 kg/m2, one year duration of
breastfeeding, never educated, never used ANC, never used family planning services, no iron
tablet supplement during pregnancy, and with higher parity. A significant reduction in the
prevalence of anemia among lactating mothers was observed in all background variables from
2005 to 2011(Table 1). Figure 1 shows the classification of anemia in terms of its detailed
parameter.
Page 23 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
In the bivariate step of our analysis, age and marital status were not statistically significant in the
data from both individual surveys and pooled data with the cut-off point p<0.25. The variable
associated with anemia for the 2005 data was BMI, whereas for the 2011 data the variables were
working status, wealth index, ever use of family planning, ANC attendance four times and above
for indexed pregnancy, husband’s education, maternal BMI and duration of breastfeeding.
In the final multivariable model using pooled data, the independent predictors of anemia for
Ethiopian lactating mothers were currently working, wealth index, ever use of family planning,
ANC attendance four times and above for indexed pregnancy, husband’s education, maternal
BMI, time variation in the two surveys, and durations of breastfeeding.
Paternal educational status was found to be a predictor of anemia among lactating mothers.
Those lactating mothers who had husbands who attended primary education were at 21% less
likely to have anemia as compared to those mothers who had husbands with no education
[AOR=0.79; 95% CI: (0.68-0.91)].The odd of being anemic in working lactating mothers was
29% less as compared to their counter parts [AOR=0.71; 95% CI: (0.63-0.80)]. Those lactating
mothers having a normal maternal BMI (18.5kg/m2-24.99kg/m
2) were 22% less likely to be
anemic as compared to lactating mother with low BMI (<18.5kg/m2) [AOR=0.78; 95% CI:
(0.68-0.89)]. Similarly, lactating women who are categorized in middle [AOR=0.83; 95% CI:
(0.71-0.98)] and rich wealth quintiles [AOR=0.83; 95% CI: (0.70-0.98)] were each 17% less
likely to have anemia as compared to lactating women in poorer quintiles.
Among reproductive characteristics, family planning use and antenatal care (ANC) were the
significant factors associated with anemia in lactating mothers. Lactating mothers who ever used
family planning were 32% less likely to have anemia as compared to lactating mothers who
never used family planning [AOR=0.68; 95% CI: (0.57- 0.80)]. Lactating mothers who reported
ANC attendance four times or more for indexed pregnancy were 27% less likely to have anemia
as compared to mothers who never attended ANC [AOR=0.73; 95% CI: (0.59-0.91)]. Those
lactating mothers who breastfed for two years were 24% less likely to have anemia as compared
to lactating women who breastfed for one year [AOR=0.76; 95% CI: (0.66-0.87)] (Table 2).
Page 24 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Discussion
Over one fifth of lactating mothers were anemic in Ethiopia, which is lower as compared to other
developing countries. For example, 66.0% of lactating mothers have been reported as having
anemia in India13 and 43.8 % of lactating mothers in Kenya had a hemoglobin level <12 g/dl14.
Another study from Myanmar reported an anemia prevalence rate of 60.3% in lactating women,
with 20.3% of lactating mothers having severe anemia15. Although the prevalence of anemia
among lactating mothers in Ethiopia was relatively low as compared to these studies, it remains a
public health problem according to WHO classification16. The relatively better prevalence of
anemia in Ethiopia among lactating mothers may be due to the cultural norms of providing
nutritional care to lactating mothers during the postpartum period. During the postpartum period,
lactating mothers are encouraged to rest for 3 to 6 months and to eat a variety of foods including
animal sources, even during religious fasting periods. Iron supplementation coverage in Ethiopia
remained low among pregnant mothers10, despite its known contribution for reducing the risk of
postpartum hemorrhage17 Postpartum hemorrhage was also found to be one of the risk factors for
anemia during the period of lactation17.
This study showed that anemia is a widespread problem in the pastoralist communities of Somali
and Afar. The prevalence of anemia in lactating mothers was higher in the pastoralist regions and
showed slow decline in these regions from 2005 to 2011. This could be due to the fact that
pastoralist communities are heavily dependent on animal milk as a source of daily food, with
poor iron bioavailability18 19
. The other reason could be due to low utilization of family planning
and antenatal care services in pastoralist areas10.
One of the factors determined to be associated with anemia was paternal education. Having a
husband with a higher level of education was found to be associated with less odd of having
anemia among lactating mothers. This could be due to the fact that those educated husbands
might support their wives to use modern health services like family planning, ANC, postnatal
care which in turn reduce the odd of having anemia as well advised to eat a diversified diet.
However, maternal educational status was not statistically associated with anemia, which is
contradictory to many studies from Ethiopia and abroad15 20-22
. This might be one important
motivator to involve husbands in anemia prevention efforts.
Page 25 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Lactating mothers who had been working in the last 12 months preceding the survey had lower
odd of having anemia as compared to their counter parts. This might be due to working mothers
were earning money as compared to non-working mothers and the extra income enabled them to
access and purchase more food items, including animal sources (meat, poultry, fish etc), and
increase dietary diversity. Studies have shown that income growth improves diet diversity which
in turn improves micronutrient intake, including iron23 24
. Similarly, lactating mothers in the
lower wealth groups had greater odds of anemia as compared to lactating mothers in the higher
wealth quintiles. In many other studies, anemia among reproductive age women, the wealth
index was found to be a statistically significant factor15 20. Other studies have also shown that
women of low socio-economic status are at risk for iron deficiency anemia (IDA) in late
pregnancy and in the postpartum period25 26
. Therefore, women’s empowerment through
economic interventions and working status could have a positive contribution towards preventing
anemia.
This study also supports the importance of family planning for reducing the risk of anemia.
Those lactating mothers who have ever used family planning (modern or traditional) had a lower
odd of having anemia as compared to those who had never used family planning. This finding is
consistent with studies from Ethiopia and Timor-Leste which showed that use of family planning
was associated with lower odd of having anemia20 27.
Maternal nutritional status (as measured by body mass index) was found to be significantly
associated with anemia. As compared with undernourished lactating mothers (BMI<18.5kg/m2),
being in the normal BMI category (18.5-24.9kg/m2) was associated with a lower odd of having
anemia. This finding is consistent with a study from Ethiopia and Thailand20 28
. When a mother
is at risk of deficiency for macronutrients, most likely she is also at risk of other micronutrient
deficiencies such as iron29.
ANC attendance was found to be associated with less odd of having anemia among lactating
mothers. This is most likely due to the fact that during ANC attendance mothers have been
advised to take iron supplements according to the Ethiopian micronutrient guideline and
instructed to consume different sources of iron rich food items30. Therefore, improving iron
status during pregnancy also helps to prevent anemia during the lactation period.
Page 26 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
Those mothers who breastfed for 2 years had lower odd of having anemia as compared to
mothers who breastfed for 1 year. This could be due to the effect of breastfeeding on maternal
depletion. Because those mothers who breastfeed younger children have high burden of
breastfeeding as compared to the older one. A study by Samson and his colleagues also found
that breastfeeding increases risk of anemia significantly20.
One of the strength of this study is to use laboratory confirmed anemia data at the national level.
Therefore, the study findings can be used to inform policy and program actions. However, the
study has caveats that some regions had small sample size, which questions the accuracy of
prevalence estimates per region, so that it should be interpreted in caution. The study did not
determine the presence of soil transmitted helminthes (STH) infection as it is associated with
anemia. This study also shares the limitation of cross-sectional study design which makes
difficult to demonstrate cause and effect relationships.
Conclusion
Anemia is a public health problem among lactating mothers in Ethiopia. There are regional
disparities regarding the prevalence of anemia, with the highest found in pastoralist regions of
Somali and Afar. Promoting partner education, improving maternal nutritional status, creating
behavioral change to use family planning and attend ANC services at health facilities are
recommended interventions to reduce the prevalence of anemia among lactating women in
Ethiopia.
Competing interests
The authors declare that they have no competing interests.
Funding statement
This research received no specific grant from any funding agency in the public, commercial or
not-for-profit sectors'
Authors’ contributions
YL and DH conceptualized the research idea. YL analyzed and interpreted the data and critically
reviewed the manuscript. SB assisted in data interpretation and critically reviewed the
Page 27 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
manuscript. DH drafted the manuscript, assisted in the data analysis and interpretation and
critically reviewed the manuscript. All authors reviewed and approved the manuscript.
Acknowledgements
The authors acknowledge DHS Measure for granting the data freely. We are also grateful to
thank Lianna Tabar, country representative of KHI-E, for her professional language editing and
reviewing the manuscript.
References
1. WHO. The world health report. Reducing risks, promoting healthy life. Geneva, World Health
Organization. 2002.
2. Whitney E, Rolfes SR. Understanding Nutrition. In: Adams P, editor. Eleventh Edition ed. United States
of America: Thomson Learning Academic Resource Center, 2008.
3. Domell V, Lonnerdal B, Dewey K, Cohen R, Hernell O. Iron zinc and copper concentrations in breast
milk are independent of maternal status. American Journal of clinical nutrition 2004;79(1):111-
15.
4. Bodnar L, Scanlon K, Freedman D, Siega–Riz A, Cogswell M. High prevalence of postpartum anaemia
among Low income women in the United States. Journal of obstetrics and Gynecology
2001;185:4348-53.
5. Sserunjogi L, Scheut F, Whyte SR. Postnatal anaemia: neglected problems and missed opportunities in
Uganda. Health Policy and Planning 2003;18(2):225-31.
6. Beard JL, Hendricks MK, Perez EM, Murray-Kolb LE, Berg A, Vernon-Feagans L, et al. Maternal Iron
Deficiency Anemia Affects Postpartum Emotions and Cognition. Journal of Nutrition
2005;135:267–72.
7. Ross J, Thomas E. Iron deficiency anemia and maternal mortality. PROFILES 3 working notes series no.
3. Academy for Education Development, Washington D.C., 1996.
8. Brabin BJ, Hakimin M, Pelletier D. An Analysis of Anemia and Pregnancy-Related Maternal Mortality.
The Journal of Nutrition 2001;131:604S-15S.
9. Kassebaum NJ, Jasrasaria R, Naghavi M, Wulf SK, Johns N, Lozano R, et al. A systematic analysis of
global anemia burden from 1990 to 2010. Blood 2014;123(5).
10. Central Statistical Agency (CSA) Ethiopia. Demographic and Health Survey 2011. Addis Ababa,
Ethiopia and Calverton, Maryland, USA: CSA and ORC Macro. 2011.
11. Central Statistical Agency(CSA). Demographic and Health Survey 2005. Addis Ababa, Ethiopia and
Calverton, Maryland, USA: CSA and ORC Macro, 2005.
12. Peter C, Jack V. Automated variable selection methods for logistic regression produced unstable
models for predicting acute myocardial infarction mortality. Journal of Clinical Epidemiology
2004;57:1138-46.
13. Singh AB, Kandpal SD, Chandra R, Srivastava VK, Negi KS. Anemia amongst pregnant and lactating
women in district Dehradun. Indian Journal of Preventive and Social Medicine 2009;40(1):20-21.
14. Ettyanga GA, Oloob WDvMLA, Saris WHM. Serum Retinol, Iron Status and Body Composition of
Lactating Women in Nandi, Kenya. Annals of Nutrition and Metabolism 2003;47:276-83.
Page 28 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
15. Zhao A, Zhang Y, Li B, Wang P, Li J, Xue Y, et al. Prevalence of Anemia and Its Risk Factors Among
Lactating Mothers in Myanmar. The American Journal of Tropical Medicine and Hygiene
2014;doi: 10.4269/ajtmh.13-0660.
16. WHO. Worldwide prevalence of anaemia 1993-2005 : WHO global database on anaemia / Edited by
Bruno de Benoist, Erin McLean, Ines Egli and Mary Cogswell, 2008.
17. WHO. Recommendations for the Prevention of Postpartum Haemorrhage (summary of results from
a WHO technical consultation, October 2006).Geneva, World Health Organization 2007.
18. Kibangou I, Bouhallab S, Henry G, Bureau F, Allouche S, Blais A, et al. Milk proteins and iron
absorption: contrasting effects of different caseinophosphopeptides. Pediatrics Research 2005
58(4):731-34.
19. Belachew T. Human Nutrition lecture note series for Health sciences students: Jimma Univesity
2005:pp 229.
20. Gebremedhin S, Enquselassie F. Correlates of anemia among women of reproductive age in Ethiopia:
Evidence from Ethiopian DHS 2005. Ethiopian Journal of Health Development 2011;25(1):22-30.
21. Haidar J. Prevalence of Anaemia, Deficiencies of Iron and Folic Acid and Their Determinants in
Ethiopian Women. Journal of Health Population Nutrition 2010;28(4):359-68.
22. Okwu GN. Studies on the predisposing factors of iron deficiency anaemia among lactating women in
Owerri, Nigeria. International Research Journal of Biochemistry and Bioinformatics
2011;1(11):304-09.
23. Taruvinga A, Muchenje V, Mushunje A. Determinants of rural household dietary diversity: The case
of Amatole and Nyandeni districts, South Africa. International Journal of Development and
Sustainability 2013;2 (4).
24. Doan D. Does income growth improve diet diversity in China?Selected Paper prepared for
presentation at the 58 the AARES Annual Conference, Port Macquarie, New South Wales, 4-7
February 2014
25. Bodnar L, Cogswell M, Scanlon K. Low income postpartum women are at risk of iron deficiency.
Journal of Nutrition 2002;132:2298–302.
26. Sadeghian M, Fatourechi A, Lesanpezeshki M, Ahmadnezhad E. Prevalence of Anemia and Correlated
Factors in the Reproductive Age Women in Rural Areas of Tabas. Journal of Family and
Reproductive Health 2013;7(3):143.
27. Lovermail AA, Hartman M, Chia KS, Heymann DL. Demographic and Spatial Predictors of Anemia in
Women of Reproductive Age in Timor-Leste: Implications for Health Program Prioritization. PLoS
ONE 2013;9(3):e91252.
28. Liabsuetrakul T, for Southern Soil-transmitted Helminths and Maternal Health Working Group. Is
International or Asian Criteria-based Body Mass Index Associated with Maternal Anaemia, Low
Birthweight, and Preterm Births among Thai Population?—An Observational Study. Journal of
Health Population Nutrition 2011;29(3):218-28.
29. Blumfield M, Hure A, MacDonald-Wicks L, Smith R, Simpson S, Raubenheimer D, et al. The
association between the macronutrient content of maternal diet and the adequacy of
micronutrients during pregnancy in the Women and Their Children’s Health (WATCH) study.
Nutrients 2012;4(12):1958-76.
30. Federal Ministry of Health-Ethiopia. National guideline for control and prevention of micronutrient
deficiencies 2004.
Page 29 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
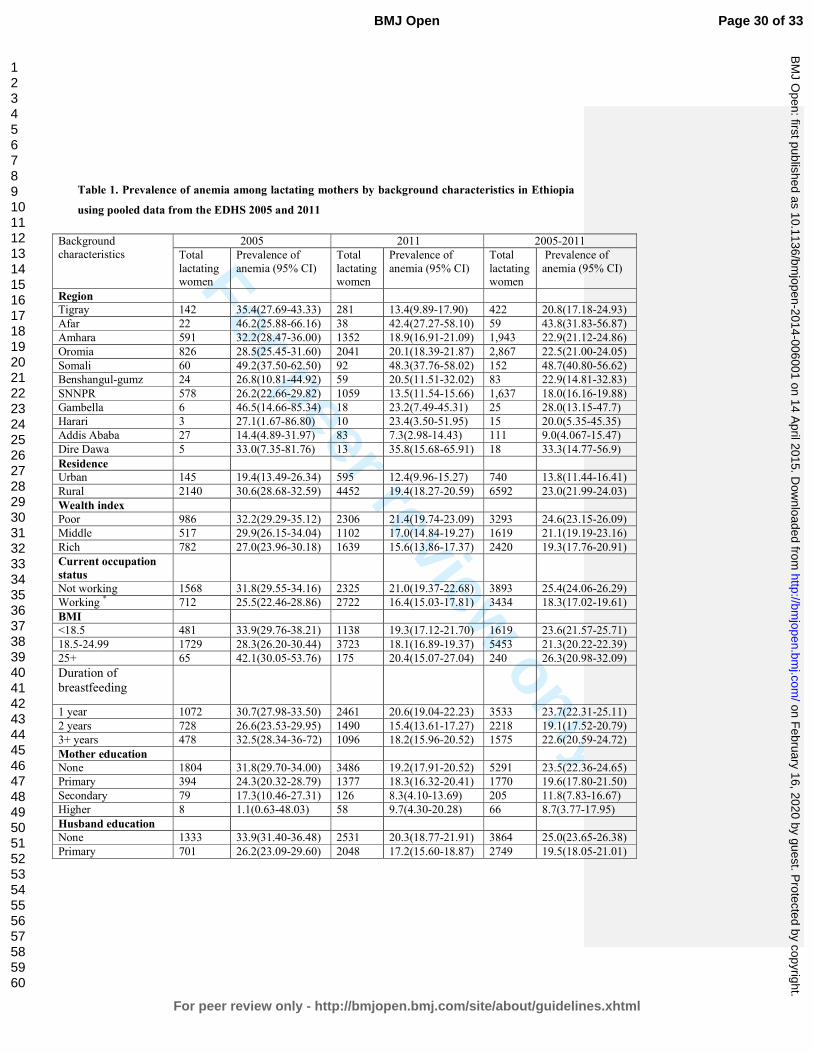
For peer review only
Table 1. Prevalence of anemia among lactating mothers by background characteristics in Ethiopia
using pooled data from the EDHS 2005 and 2011
Background
characteristics
2005 2011 2005-2011
Total
lactating women
Prevalence of
anemia (95% CI)
Total
lactating women
Prevalence of
anemia (95% CI)
Total
lactating women
Prevalence of
anemia (95% CI)
Region
Tigray 142 35.4(27.69-43.33) 281 13.4(9.89-17.90) 422 20.8(17.18-24.93)
Afar 22 46.2(25.88-66.16) 38 42.4(27.27-58.10) 59 43.8(31.83-56.87)
Amhara 591 32.2(28.47-36.00) 1352 18.9(16.91-21.09) 1,943 22.9(21.12-24.86)
Oromia 826 28.5(25.45-31.60) 2041 20.1(18.39-21.87) 2,867 22.5(21.00-24.05)
Somali 60 49.2(37.50-62.50) 92 48.3(37.76-58.02) 152 48.7(40.80-56.62)
Benshangul-gumz 24 26.8(10.81-44.92) 59 20.5(11.51-32.02) 83 22.9(14.81-32.83)
SNNPR 578 26.2(22.66-29.82) 1059 13.5(11.54-15.66) 1,637 18.0(16.16-19.88)
Gambella 6 46.5(14.66-85.34) 18 23.2(7.49-45.31) 25 28.0(13.15-47.7)
Harari 3 27.1(1.67-86.80) 10 23.4(3.50-51.95) 15 20.0(5.35-45.35)
Addis Ababa 27 14.4(4.89-31.97) 83 7.3(2.98-14.43) 111 9.0(4.067-15.47)
Dire Dawa 5 33.0(7.35-81.76) 13 35.8(15.68-65.91) 18 33.3(14.77-56.9)
Residence
Urban 145 19.4(13.49-26.34) 595 12.4(9.96-15.27) 740 13.8(11.44-16.41)
Rural 2140 30.6(28.68-32.59) 4452 19.4(18.27-20.59) 6592 23.0(21.99-24.03)
Wealth index
Poor 986 32.2(29.29-35.12) 2306 21.4(19.74-23.09) 3293 24.6(23.15-26.09)
Middle 517 29.9(26.15-34.04) 1102 17.0(14.84-19.27) 1619 21.1(19.19-23.16)
Rich 782 27.0(23.96-30.18) 1639 15.6(13.86-17.37) 2420 19.3(17.76-20.91)
Current occupation
status
Not working 1568 31.8(29.55-34.16) 2325 21.0(19.37-22.68) 3893 25.4(24.06-26.29)
Working * 712 25.5(22.46-28.86) 2722 16.4(15.03-17.81) 3434 18.3(17.02-19.61)
BMI
<18.5 481 33.9(29.76-38.21) 1138 19.3(17.12-21.70) 1619 23.6(21.57-25.71)
18.5-24.99 1729 28.3(26.20-30.44) 3723 18.1(16.89-19.37) 5453 21.3(20.22-22.39)
25+ 65 42.1(30.05-53.76) 175 20.4(15.07-27.04) 240 26.3(20.98-32.09)
Duration of
breastfeeding
1 year 1072 30.7(27.98-33.50) 2461 20.6(19.04-22.23) 3533 23.7(22.31-25.11)
2 years 728 26.6(23.53-29.95) 1490 15.4(13.61-17.27) 2218 19.1(17.52-20.79)
3+ years 478 32.5(28.34-36-72) 1096 18.2(15.96-20.52) 1575 22.6(20.59-24.72)
Mother education
None 1804 31.8(29.70-34.00) 3486 19.2(17.91-20.52) 5291 23.5(22.36-24.65)
Primary 394 24.3(20.32-28.79) 1377 18.3(16.32-20.41) 1770 19.6(17.80-21.50)
Secondary 79 17.3(10.46-27.31) 126 8.3(4.10-13.69) 205 11.8(7.83-16.67)
Higher 8 1.1(0.63-48.03) 58 9.7(4.30-20.28) 66 8.7(3.77-17.95)
Husband education
None 1333 33.9(31.40-36.48) 2531 20.3(18.77-21.91) 3864 25.0(23.65-26.38)
Primary 701 26.2(23.09-29.60) 2048 17.2(15.60-18.87) 2749 19.5(18.05-21.01)
Page 30 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
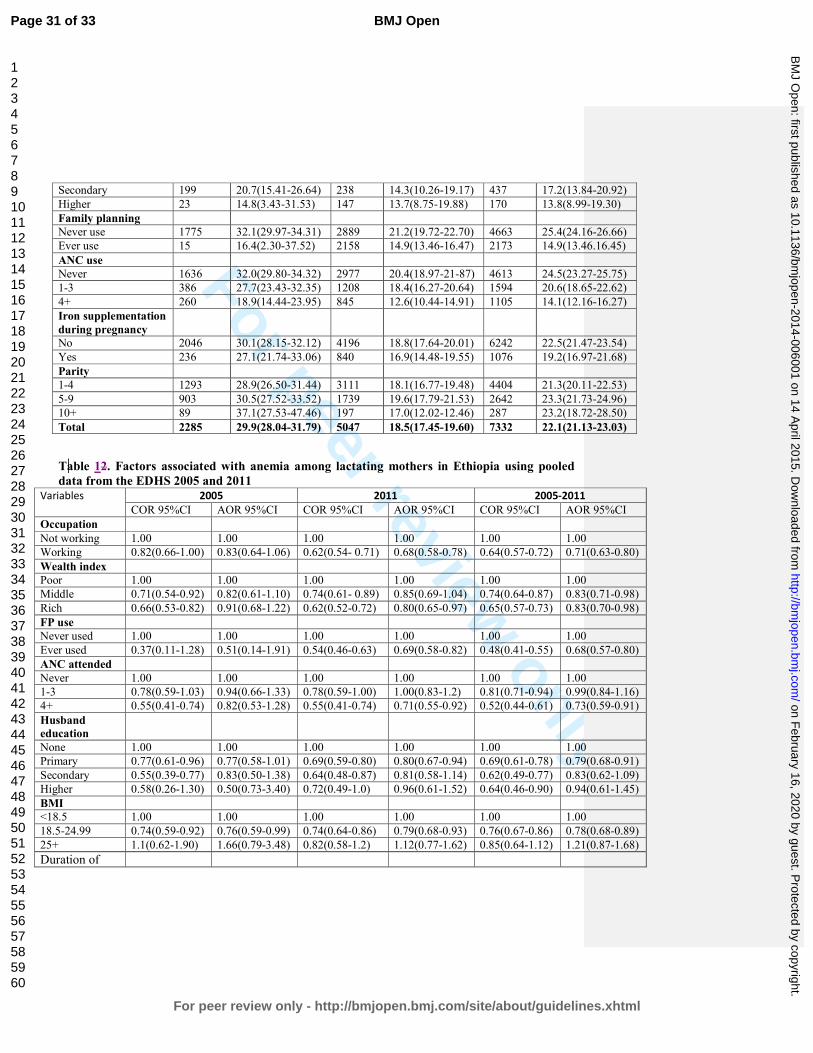
For peer review only
Secondary 199 20.7(15.41-26.64) 238 14.3(10.26-19.17) 437 17.2(13.84-20.92)
Higher 23 14.8(3.43-31.53) 147 13.7(8.75-19.88) 170 13.8(8.99-19.30)
Family planning
Never use 1775 32.1(29.97-34.31) 2889 21.2(19.72-22.70) 4663 25.4(24.16-26.66)
Ever use 15 16.4(2.30-37.52) 2158 14.9(13.46-16.47) 2173 14.9(13.46.16.45)
ANC use
Never 1636 32.0(29.80-34.32) 2977 20.4(18.97-21-87) 4613 24.5(23.27-25.75)
1-3 386 27.7(23.43-32.35) 1208 18.4(16.27-20.64) 1594 20.6(18.65-22.62)
4+ 260 18.9(14.44-23.95) 845 12.6(10.44-14.91) 1105 14.1(12.16-16.27)
Iron supplementation
during pregnancy
No 2046 30.1(28.15-32.12) 4196 18.8(17.64-20.01) 6242 22.5(21.47-23.54)
Yes 236 27.1(21.74-33.06) 840 16.9(14.48-19.55) 1076 19.2(16.97-21.68)
Parity
1-4 1293 28.9(26.50-31.44) 3111 18.1(16.77-19.48) 4404 21.3(20.11-22.53)
5-9 903 30.5(27.52-33.52) 1739 19.6(17.79-21.53) 2642 23.3(21.73-24.96)
10+ 89 37.1(27.53-47.46) 197 17.0(12.02-12.46) 287 23.2(18.72-28.50)
Total 2285 29.9(28.04-31.79) 5047 18.5(17.45-19.60) 7332 22.1(21.13-23.03)
Table 12. Factors associated with anemia among lactating mothers in Ethiopia using pooled
data from the EDHS 2005 and 2011 Variables 2005 2011 2005-2011
COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI COR 95%CI AOR 95%CI
Occupation
Not working 1.00 1.00 1.00 1.00 1.00 1.00
Working 0.82(0.66-1.00) 0.83(0.64-1.06) 0.62(0.54- 0.71) 0.68(0.58-0.78) 0.64(0.57-0.72) 0.71(0.63-0.80)
Wealth index
Poor 1.00 1.00 1.00 1.00 1.00 1.00
Middle 0.71(0.54-0.92) 0.82(0.61-1.10) 0.74(0.61- 0.89) 0.85(0.69-1.04) 0.74(0.64-0.87) 0.83(0.71-0.98)
Rich 0.66(0.53-0.82) 0.91(0.68-1.22) 0.62(0.52-0.72) 0.80(0.65-0.97) 0.65(0.57-0.73) 0.83(0.70-0.98)
FP use
Never used 1.00 1.00 1.00 1.00 1.00 1.00
Ever used 0.37(0.11-1.28) 0.51(0.14-1.91) 0.54(0.46-0.63) 0.69(0.58-0.82) 0.48(0.41-0.55) 0.68(0.57-0.80)
ANC attended
Never 1.00 1.00 1.00 1.00 1.00 1.00
1-3 0.78(0.59-1.03) 0.94(0.66-1.33) 0.78(0.59-1.00) 1.00(0.83-1.2) 0.81(0.71-0.94) 0.99(0.84-1.16)
4+ 0.55(0.41-0.74) 0.82(0.53-1.28) 0.55(0.41-0.74) 0.71(0.55-0.92) 0.52(0.44-0.61) 0.73(0.59-0.91)
Husband
education
None 1.00 1.00 1.00 1.00 1.00 1.00
Primary 0.77(0.61-0.96) 0.77(0.58-1.01) 0.69(0.59-0.80) 0.80(0.67-0.94) 0.69(0.61-0.78) 0.79(0.68-0.91)
Secondary 0.55(0.39-0.77) 0.83(0.50-1.38) 0.64(0.48-0.87) 0.81(0.58-1.14) 0.62(0.49-0.77) 0.83(0.62-1.09)
Higher 0.58(0.26-1.30) 0.50(0.73-3.40) 0.72(0.49-1.0) 0.96(0.61-1.52) 0.64(0.46-0.90) 0.94(0.61-1.45)
BMI
<18.5 1.00 1.00 1.00 1.00 1.00 1.00
18.5-24.99 0.74(0.59-0.92) 0.76(0.59-0.99) 0.74(0.64-0.86) 0.79(0.68-0.93) 0.76(0.67-0.86) 0.78(0.68-0.89)
25+ 1.1(0.62-1.90) 1.66(0.79-3.48) 0.82(0.58-1.2) 1.12(0.77-1.62) 0.85(0.64-1.12) 1.21(0.87-1.68)
Duration of
Page 31 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from

For peer review only
breastfeeding 1 year 1.00 1.00 1.00 1.00 1.00 1.00
2 years 0.79(0.64-0.99) 0.79(0.62-1.03) 0.71(0.60-0.83) 0.75(0.63-0.88) 0.75(0.66-0.85) 0.76(0.66-0.87)
3+ years 0.99(0.77-1.27) 1.10(0.82-1.49) 0.71(0.59-0.86) 0.82(0.67-0.99) 0.81(0.70-0.94) 0.89(0.76-1.05)
Time laps
2005 1.00 1.00
2011 0.65(0.58-0.73) 0.73(0.64-0.85) COR: Crude Odds Ratio, AOR: Adjusted Odds Ratio, 1.00 is the reference category
Page 32 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from
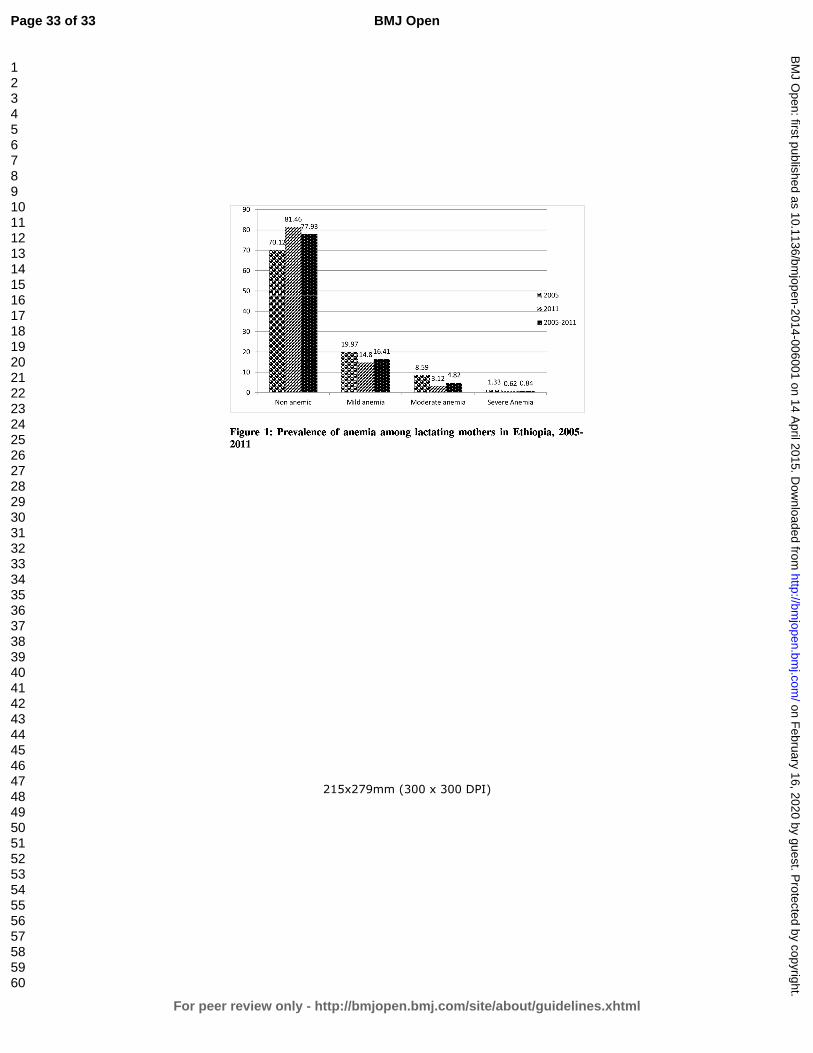
For peer review only
215x279mm (300 x 300 DPI)
Page 33 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on February 16, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006001 on 14 A
pril 2015. Dow
nloaded from























![DIET Management for Lactating Women Auto Saved]](https://img.pdfslide.us/doc/110x75/577d33ba1a28ab3a6b8b90a9/diet-management-for-lactating-women-auto-saved.jpg)