Embed Size (px)
Citation preview

3/27/2016
1
Blood Vessels
Cardiovascular System
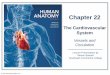
Blood Vessels
• Delivery system of dynamic structures
• Closed system
– Arteries
• Carry blood away from the heart
– Capillaries
• Contact tissue cells and directly serve cellular needs
– Veins
• Carry blood toward the heart
Figure 19.2
Large veins(capacitancevessels)
Largelymphaticvessels
Arteriovenousanastomosis
Lymphaticcapillary
Postcapillaryvenule
Sinusoid
Metarteriole
Terminal arteriole
Arterioles(resistance vessels)
Muscular arteries(distributingvessels)
Elastic arteries(conductingvessels)
Small veins(capacitancevessels)
Lymphnode
Capillaries(exchange vessels)
Precapillary sphincterThoroughfarechannel
Lymphaticsystem
Venous system Arterial system
Heart
Figure 19.20
Azygos
system
Venous
drainage
Arterial
blood
Thoracic
aorta
Inferior
vena
cava
Abdominal
aorta
Inferior
vena
cava
Superior
vena cava
Common
carotid arteries
to head and
subclavian
arteries to
upper limbs
Aortic
arch
Aorta
RA
RV LV
LA
Capillary beds of
head and
upper limbs
Capillary beds of
mediastinal structures
and thorax walls
Diaphragm
Capillary beds of
digestive viscera,
spleen, pancreas,
kidneys
Capillary beds of gonads,
pelvis, and lower limbs
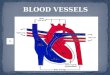
Blood Vessel Structure
• Tissue layers
– Tunica intima
– Tunica media
– Tunica externa
Tunica
intima
Tunica
media
Tunica
externa
ValveValve
Endothelial
Cell
Figure 19.1b
Tunica media(smooth muscle andelastic fibers)
Tunica externa
(collagen fibers)
Lumen
Artery
Lumen
Vein
Internal elastic lamina
External elastic lamina
Valve
(b)
Endothelial cellsBasement membrane
Capillary
network
Capillary
Tunica intima
• Endothelium• Subendothelial layer

3/27/2016
2
Blood Vessel Structure Blood Vessel Structure
Vasa vasorum nourishes outer layers of large vessels
Figure 19.21b
Internal carotid artery
Common carotid arteries
Subclavian artery
Subclavian artery
Aortic arch
Ascending aorta
Coronary artery
Thoracic aorta (abovediaphragm)
Renal artery
Superficial palmar arch
Radial artery
Ulnar artery
Internal iliac artery
Deep palmar arch
Vertebral artery
Brachiocephalic trunk
Axillary artery
Brachial artery
Abdominal aorta
Superior mesenteric artery
Gonadal artery
Common iliac artery
External iliac artery
Digital arteries
Femoral arteryPopliteal arteryAnterior tibial arteryPosterior tibial artery
Arcuate artery(b) Illustration, anterior
view
Inferior mesenteric artery
Celiac trunk
External carotid artery
Arteries of the head and trunk
Arteries that supply the upper limb
Arteries that supply the lower limb
Arteries
• Transport blood from left ventricle to body
tissues
– High pressure
• Three groups
– Elastic (conducting)
– Muscular (distributing)
– Arterioles (resistance)
Table 19.1 (1 of 2)
Arteries
• Elastic arteries
– Near the heart
• Aorta and major branches
– Conducting arteries
• Conduct blood from the heart to medium-sized arteries
– Large and thick-walled
– Large lumen = low resistance
– Highly elastic
• Expand during systole & recoil during diastole

3/27/2016
3
Arteries
• Muscular arteries
– Distributing arteries
• Distal to elastic arteries
• Deliver blood to body organs
– Thick tunica media with more smooth muscle
– Active in vasoconstriction
– Examples
• Radial, femoral, brachial
Arteries
• Resistance arteries
– Smallest arterial vessels (arterioles)
• Lead to capillary beds
• Control valves to capillary beds
– Site of most vasodilation and vasoconstriction
ArterioleVenule
Metarteriole
Capillaries
• Exchange vessels
• Exceedingly thin walls – just a tunica intima
• Capillary beds
– Microcirculation
between arterioles
and venules
Capillaries
• Two types
1. Continuous
• Open junctions between adjacent endothelial cells
• Most common
• In skin & muscles
2. Fenestrated
• Pores = permeable
• Intestines, endocrine organs, kidneys
Capillaries Capillaries
• Precapillary sphincters
– Cuff of smooth muscle fibers
– Acts as a valve to control blood flow into the
capillary
– Responds to local chemical conditions
– Vasomotor nerves (sympathetic)

3/27/2016
4
Figure 19.4
(a) Sphincters open—blood flows through true capillaries.
(b) Sphincters closed—blood flows through metarteriole
thoroughfare channel and bypasses true capillaries.
Precapillary
sphincters Metarteriole
Vascular shunt
Terminal arteriole Postcapillary venule
Terminal arteriole Postcapillary venule
Thoroughfare channel
True capillaries
Capillaries
• Tissue capillary bed may be flooded with blood
or nearly completely empty
• Examples: GI tract after a meal; skeletal muscle
during exercise
Continuous Capillaries
• Abundant in the skin and muscles
– Tight junctions connect endothelial cells
– Intercellular clefts
allow the passage of
fluids and small
solutes
Continuous Capillaries
• Continuous capillaries of the brain
– Tight junctions are complete, forming the blood-
brain barrier
– Carrier-mediated transport
Figure 19.3a
Red blood
cell in lumen
Intercellular
cleft
Endothelial
cell
Endothelial
nucleus
Tight junction Pinocytotic
vesicles
Pericyte
Basement
membrane
(a) Continuous capillary. Least permeable, and
most common (e.g., skin, muscle).
Figure 19.3b
Red blood
cell in lumen
Intercellular
cleft
Fenestrations
(pores)
Endothelial
cell
Endothelialnucleus
Basement membrane
Tight junction
Pinocytotic
vesicles
(b) Fenestrated capillary. Large fenestrations
(pores) increase permeability. Occurs in special
locations (e.g., kidney, small intestine).

3/27/2016
5
Figure 19.3c
Nucleus of
endothelial
cell
Red blood
cell in lumen
Endothelial
cell
Tight junction
Incomplete
basement
membrane
Large
intercellular
cleft
(c) Sinusoidal capillary. Most permeable. Occurs in
special locations (e.g., liver, bone marrow, spleen).
This is not in the Study Guide, just FYI
Capillaries
• Functions
– Exchange area for blood and interstitial fluid
compartment
– Diffusion
• O2 and nutrients from the blood to tissues
• CO2 and metabolic wastes from tissues to the blood
Veins
• Functions
– Collect blood from capillary beds
– “drain” organs and tissues of blood
• Become larger as they come closer to the heart
Figure 19.26b
Renal vein
Splenic vein
Basilic vein
Brachial vein
Cephalic vein
Dural venous sinuses
External jugular vein
Vertebral vein
Internal jugular vein
Superior vena cava
Right and left
brachiocephalic veins
Axillary vein
Great cardiac vein
Hepatic veins
Hepatic portal vein
Superior mesenteric
vein
Inferior vena cava
Ulnar vein
Radial vein
Common iliac vein
External iliac vein
Internal iliac vein
Digital veins
Femoral vein
Great saphenous vein
Popliteal vein
Posterior tibial vein
Anterior tibial vein
Small saphenous vein
Dorsal venous arch
(b) Illustration, anterior
view. The vessels of the
pulmonary circulation
are not shown. Dorsal metatarsal veins
Inferior mesenteric vein
Median cubital vein
Subclavian vein
Veins of the head and trunk Veins that drain
the upper limb
Veins that drain
the lower limb
Copyright © 2010 Pearson Education, Inc.
Venules
• Formed when capillary beds unite
• Very porous
– Allow fluids and WBC’s into tissues

3/27/2016
6
Figure 19.5
Heart 8%
Capillaries 5%
Systemic arteries
and arterioles 15%
Pulmonary blood
vessels 12%
Systemic veins
and venules 60%
Veins
• Thinner walls, larger lumens than arteries
• Blood pressure is lower than in arteries
• Thin tunica media and a thick tunica externa
• Capacitance vessels (blood reservoirs)
– Contain up to 60% of the blood supply
Blood Vessel Matching
1. Pump
2. Resistance vessels, site of most vasodilation and vasoconstriction
3. Exchange sites
4. Pressure reservoirs, conducting vessels
5. Blood reservoirs
6. Distributing vessels
a. Veins
b. Arterioles
c. Capillaries
d. Heart
e. Elastic arteries
f. Muscular arteries
Venous Blood Pressure
• Low pressure
– Due to cumulative effects of peripheral resistance
• Working against gravity
– Valves
– Skeletal muscle action
– Thoracic pressure changes
Venous Valves
Figure 19.7
Valve (open)
Contracted
skeletal
muscle
Valve (closed)
Vein
Direction of
blood flow

3/27/2016
7
Varicose Veins
• Incompetent valves
– Pregnancy
– Obesity
– Long periods of standing
– Hemorrhoids
Blood Flow
• Blood flow is involved in
– O2 delivery
– Removal of wastes
– Gas exchange (lungs)
– Absorption of nutrients (digestive tract)
– Urine formation (kidneys)
• Perfusion– Rate of blood flow per given volume of tissue
• Blood flow (F)– Volume of blood flowing through a vessel, an organ, or tissue
in a given period• Measured as ml/min• Varies widely through individual organs
– Based on needs
Blood Flow Blood Flow
• F= Δ P
R
o F = Blood flow
o ΔP = Difference in pressure between two points
o R = Resistance
Blood Flow
� F= Δ P
R
• Relationship between blood flow, blood pressure, and resistance
– If ∆P increases, blood flow speeds up
– If R increases, blood flow decreases
• R is more important in influencing local blood flow
– Changed by altering blood vessel diameter
Blood Pressure
• Blood pressure (BP)
– Force per unit area exerted on the wall blood vessel by the blood
– Expressed as the height of a column of mercury (mmHg)
– P = H x D
• P = pressure
• H = height of column
• D = density of material in the column

3/27/2016
8
Blood Pressure
• Factors influencing blood pressure
– Cardiac output (CO)
– Peripheral resistance (PR)
– Blood volume
Blood Pressure
• Systolic pressure
– Pressure exerted during ventricular contraction
– Top number
• Diastolic pressure
– Lowest level of arterial pressure
– Bottom number
• Average value = 120/80
• Pulse pressure
– Difference between systolic and diastolic pressure
Figure 19.6
Systolic pressure
Mean pressure
Diastolic
pressure
Blood Pressure
• Basic concepts
– The pumping action of the heart generates blood
flow
– Pressure results when flow is opposed by resistance
• Systemic pressure
– Highest in the aorta
– Declines throughout the pathway
– Is close to 0 mmHg in the right atrium
• The steepest drop occurs in arterioles
Arterial Blood Pressure
• Reflects two factors of the arteries close to the
heart
– Elasticity
– Volume of blood forced into them at any time
• Blood pressure near the heart is pulsatile
Arterial Blood Pressure
� Mean arterial blood pressure (MABP)
�Pressure that propels blood to tissues
�Represents average blood pressure
MABP = diastolic pressure + 1/3 pulse pressure
Pulse pressure and MABP both decline
with increasing distance from the heart

3/27/2016
9
Hypertension
• “Silent Killer”
– Resting systolic >140 mmHg and/or diastolic >90 mmHg
• Causes
– Loss of flexibility in vessel walls
• Results
– Heart failure
– Renal failure
– Stroke
– Increased risk of aneurysm
Capillary Blood Pressure
• Not pulsatile
• Low capillary pressure is desirable
– High BP would rupture fragile, thin-walled capillaries
– Most are very permeable, so low pressure forces
filtrate into interstitial spaces
Peripheral Resistance
• The opposition to blood flow exerted by vessel walls– The result of friction
• Influenced by 3 factors– Blood viscosity
– Blood vessel length
– Blood vessel radius
Peripheral Resistance
• Viscosity = a fluid’s resistance to flow
• Blood viscosity influenced by…
– Albumin
– Erythrocytes
Peripheral Resistance
• Vessel length
– The farther fluid travels = more cumulative friction
Peripheral Resistance
• Vessel radius
– Most significant factor
– Vasoconstriction and vasodilation
– Flow is proportional to fourth power of radius
• Alteration of radius profoundly affects blood flow

3/27/2016
10
Poiseuille’s Law
• Formula representing the factors influencing flow
F = ΔPπr4
8 nL
F= flow
ΔP = pressure gradient
r4 = vessel radius
n = viscosity
L = vessel length
Poiseuille’s Law
• Blood flow is directly proportional to pressure
gradient and vessel radius
F = ΔPπr4
8 nL
Poiseuille’s Law
• Blood flow is inversely proportional to vessel
length and blood viscosity
F = ΔPπr4
8 nL
Regulation of Peripheral Resistance
• Local control
– Arterioles vary diameters = autoregulation
• A response to the chemical composition of the blood
– Faster flow = faster removal of wastes
Regulation of Peripheral Resistance
� Local controlLocalized hypoxia
Metabolites (CO2, lactic acid, adenosine)
Acidic pH
Inhibit smooth muscle
Vasodilation
Increased blood flow
Regulation of Peripheral Resistance
• Local control
– Precapillary sphincters
• Respond to local stimuli and vasoactive hormones
– Endothelial cells & platelets
• Vasodilators
– NO, prostacyclin
• Vasoconstrictors
– Endothelians, seratonin, thromboxane A2

3/27/2016
11
Figure 19.15
Metabolic
controls
pH Sympathetic
αααα Receptors
ββββ ReceptorsEpinephrine,
norepinephrine
Angiotensin II
Antidiuretic
hormone (ADH)
Atrial
natriuretic
peptide (ANP)
Dilates
Constricts
Prostaglandins
Adenosine
Nitric oxide
Endothelins
Stretch
O2
CO2
K+
Amounts of:
Amounts of:
Nerves
Hormones
Myogenic
controls
Intrinsic mechanisms(autoregulation)
• Distribute blood flow to individual
organs and tissues as needed
Extrinsic mechanisms
• Maintain mean arterial pressure (MAP)
• Redistribute blood during exercise and
thermoregulation
Peripheral Resistance
• Example of autoregulation
– Blood flow to skeletal muscles
• During muscle activity, blood flow increases in direct
proportion to the metabolic activity
• Blood flow can increase 10× or more during physical activity
Figure 19.13
Brain
Heart
Skeletal
muscles
Skin
Kidney
Abdomen
Other
Total blood flow during strenuous
exercise 17,500 ml/min
Total blood
flow at rest
5800 ml/min
Peripheral Resistance
• Neural control
– Directed by ANS via sympathetic innervation
• Vascular smooth muscle lacks parasympathetic input
Peripheral Resistance
� Neural control
�Vasomotor center in medulla = primary control center
�Integrates input from 3 ANS reflex circuits
�Baroreflex
�Chemoreflex
�Ischemic reflex
Peripheral Resistance
• Baroreflex
– Baroreceptors (pressure receptors) in
• Carotid sinuses
• Aortic arch
– Example: Blood pressure increases
• Inhibitory signals are sent to the
vasomotor center
• Stimulatory signals are sent to
the cardioinhibitory center (which acts
through which nerve?)

3/27/2016
12
Baroreceptors
in carotid sinuses
and aortic arch
are stimulated.
Impulses from baroreceptors
stimulate cardioinhibitory center
and inhibit vasomotor
center.
Rate of
vasomotor impulses
allows vasodilation,
causing R
Sympathetic
impulses to heart
cause HR,
contractility, and
CO.
Stimulus:
Blood pressure
(arterial blood
pressure rises above
normal range).
3
2
1
Homeostasis: Blood pressure in normal range
4b
5
4a
CO and R
return blood
pressure to
homeostatic range.
Baroreceptors
in carotid sinuses
and aortic arch
are inhibited.
Impulses from baroreceptors stimulate
cardioacceleratory center and stimulate vasomotor center.
Vasomotor
fibers stimulate
vasoconstriction,
causing R
Sympathetic
impulses to heart
cause HR,
contractility, and
CO.
5
4a
4b
3
2
CO and R
return blood pressure
to homeostatic range.
Peripheral Resistance
• Chemoreflex
– Excitatory or inhibitory signals to vasomotor
center
– Chemorecetors detect low blood pH, O2 levels
and high CO2 levels
– Chemoreceptors are located in the
• Carotid bifurcation
• Aortic arch
• Large arteries of the neck
Peripheral Resistance
• Medullary Ischemic Reflex
– Triggered by low perfusion of the medulla
Hypoxia and hypercapnia (high blood CO2) of the brain
Vasoconstriction in extremities
Blood flow directed to head and upper body
Peripheral Resistance
• Hormonal controls
– Angiotensin II
• Generated by kidney release of renin
• Causes vasoconstriction
– Atrial natriuretic peptide/factor
• Causes blood volume and blood pressure to decline
• Causes generalized vasodilation
Peripheral Resistance
• Hormonal controls cont.
– Antidiuretic hormone (ADH, vasopressin)
• Causes intense vasoconstriction in cases of extremely low
BP
– Epinephrine
• Causes generalized vasoconstriction and increases cardiac
output
Figure 19.11
Activity ofmuscularpump andrespiratory
pump
Release
of ANP
Fluid loss from
hemorrhage,
excessive
sweating
Crisis stressors:
exercise, trauma,
body
temperature
Bloodborne
chemicals:
epinephrine,
NE, ADH,
angiotensin II;
ANP release
Body size
Conservation
of Na+ and
water by kidney
Blood volume
Blood pressure
Blood pH, O2,
CO2
Dehydration,
high hematocrit
Blood
volume
Baroreceptors Chemoreceptors
Venous
returnActivation of vasomotor and cardiac
acceleration centers in brain stem
Heart
rate
Stroke
volume
Diameter of
blood vessels
Cardiac output
Initial stimulus
Result
Physiological response
Mean systemic arterial blood pressure
Blood
viscosity
Peripheral resistance
Blood vessel
length

3/27/2016
13
Fluid Shifts Between Capillaries and
Tissue
• Capillaries allow plasma and solutes to pass into interstitial space �
interstitial or extracellular fluid (ECF)
– Facilitates exchange of resources & wastes between
cells & plasma
– Dynamic equilibrium
– Imbalances?
– Exceptions?
Figure 19.2
Large veins(capacitancevessels)
Largelymphaticvessels
Arteriovenousanastomosis
Lymphaticcapillary
Postcapillaryvenule
Sinusoid
Metarteriole
Terminal arteriole
Arterioles(resistance vessels)
Muscular arteries(distributingvessels)
Elastic arteries(conductingvessels)
Small veins(capacitancevessels)
Lymphnode
Capillaries(exchange vessels)
Precapillary sphincterThoroughfarechannel
Lymphaticsystem
Venous system Arterial system
Heart
Regulation of ECF Movement
• Hydrostatic and osmotic pressure
– Hydrostatic “pushes” and osmotic “sucks”
– 4 types
Capillary hydrostatic pressure
Interstitial osmotic pressure
Interstitial hydrostatic pressure
Capillary osmotic pressure
Move water out of
the vascular system
Move water into
the vascular system
Figure 19.17
HP = hydrostatic pressure• Due to fluid pressing against a wall
• “Pushes”
• In capillary (HPc)• Pushes fluid out of capillary
• 35 mm Hg at arterial end and
17 mm Hg at venous end of
capillary in this example
• In interstitial fluid (HPif)• Pushes fluid into capillary
• 0 mm Hg in this example
OP = osmotic pressure• Due to presence of nondiffusiblesolutes (e.g., plasma proteins)• “Sucks”• In capillary (OPc)
• Pulls fluid into capillary• 26 mm Hg in this example
• In interstitial fluid (OPif)• Pulls fluid out of capillary• 1 mm Hg in this example
Arteriole
Capillary
Interstitial fluid
Net HP—Net OP
(35—0)—(26—1)
Net HP—Net OP
(17—0)—(26—1)
Venule
NFP (net filtration pressure)is 10 mm Hg; fluid moves out
NFP is ~8 mm Hg;fluid moves in
Net
HP
35
mm
Net
OP
25
mm
Net
HP
17
mm
Net
OP
25
mm
Regulation of ECF Movement
• Hydrostatic
– Capillary hydrostatic pressure (HPc)
• Capillary blood pressure
• Tends to force fluids through the capillary walls
• Is greater at the arterial end (35 mm Hg) of a bed than at the venous end (17 mm Hg)
– Interstitial hydrostatic pressure (HPif)
• Pressure of fluid within intercellular spaces
• Constantly enters lymphatic drainage
• Averages 0 mmHg
Regulation of ECF Movement
• Osmotic
– Interstitial fluid osmotic pressure (OPif)
• The osmotic pressure force created by interstitial solutes
• Low (~1 mm Hg), due to low protein content
– Capillary colloid osmotic pressure (OPc)
• Created by non-diffusible plasma proteins, which draw
water toward themselves
• ~26 mm Hg

3/27/2016
14
Regulation of ECF Movement
• The movement of fluid between the
extracellular compartments is driven by a
pressure gradient
– Most influenced by capillary hydrostatic pressure
Regulation of ECF Movement
• Net Filtration Pressure (NFP)
– Comprises all the forces acting on a capillary bed
NFP = (HPc - HPif) - (Opc - OPif)
Regulation of ECF Movement
• Arterial NFP– Arterial end of a capillary bed = hydrostatic forces
dominate• Fluid moves out
• NFP = (35-0) – (26-1) = 10 mm Hg
• Venous NFP– Venous end of a capillary bed = osmotic forces dominate
• Fluid moves in
• NFP = (17-0) – (26-1) = -8 mm Hg
• Excess fluid– Returned to the blood via the lymphatic system
Figure 19.17
HP = hydrostatic pressure
• Due to fluid pressing against a wall• “Pushes”• In capillary (HPc)
• Pushes fluid out of capillary• 35 mm Hg at arterial end and
17 mm Hg at venous end ofcapillary in this example
• In interstitial fluid (HPif)• Pushes fluid into capillary• 0 mm Hg in this example
OP = osmotic pressure• Due to presence of nondiffusiblesolutes (e.g., plasma proteins)• “Sucks”• In capillary (OPc)
• Pulls fluid into capillary• 26 mm Hg in this example
• In interstitial fluid (OPif)• Pulls fluid out of capillary• 1 mm Hg in this example
Arteriole
Capillary
Interstitial fluid
Net HP—Net OP
(35—0)—(26—1)
Net HP—Net OP
(17—0)—(26—1)
Venule
NFP (net filtration pressure)is 10 mm Hg; fluid moves out
NFP is -8 mm Hg;fluid moves in
NetHP35mm
NetOP25mm
NetHP17mm
NetOP25mm
Filtration=fluid moves out
Reabsorption=fluid moves in
Figure 19.2
Large veins(capacitancevessels)
Largelymphaticvessels
Arteriovenousanastomosis
Lymphaticcapillary
Postcapillaryvenule
Sinusoid
Metarteriole
Terminal arteriole
Arterioles(resistance vessels)
Muscular arteries(distributingvessels)
Elastic arteries(conductingvessels)
Small veins(capacitancevessels)
Lymphnode
Capillaries(exchange vessels)
Precapillary sphincterThoroughfarechannel
Lymphaticsystem
Venous system Arterial system
Heart Edema
• Occurs when filtration greatly exceeds
reabsorption
– Abnormal increase in interstitial fluid volume

3/27/2016
15
Venous Blood Pressure
• Changes little during the cardiac cycle
• Low pressure due to cumulative effects of
peripheral resistance
• Central venous pressure
– Pressure at the point where vena cava enter heart
– Average = 4.6 mm Hg
Venous Return
• Venous hydrostatic pressure relatively low
• Returning blood to heart requires adaptations
Mechanisms of Venous Return
1. Thoracic pump
• Pressure changes created during breathing move blood toward the heart by squeezing abdominal veins as thoracic veins expand
2. Cardiac Suction
• During atrial systole, movement of AV valves enlarges atria = lower pressure = increasing pressure gradient between vena cava
3. Muscular pump
• Contraction of skeletal muscles “milk” blood toward the heart and valves prevent backflow
4. Gravity
• Helps with return of blood from superior regions
21_09
Mechanisms of Venous Return
• Circulatory shock
– Definition = CO is insufficient to meet the metabolic demands of the tissues
– Cardiogenic shock
• Heart’s ability to pump blood is impaired
– Other types of shock
• Due to low venous return (LVR)
– Hypovolemic shock
– Vascular shock
» Neurogenic shock
» Septic shock
» Anaphylactic shock
Types and Causes of LVR Shock
1. Hypovolemic shock
– Most common form of shock
– Result of blood loss
• Direct losses: hemorrhage, trauma, burns, bleeding ulcers
• Indirect losses: fluids other than blood lost
– Burns and dehydration

3/27/2016
16
Types and Causes of LVR Shock
2. Vascular shock
– Body retains normal blood volume but blood accumulates in extremities
a) Neurogenic shock
• Usually follows spinal cord trauma � widespread vasodilation
b) Septic shock
• Bacterial endotoxin simulates vasodilation
c) Anaphylactic shock
• Following allergic reaction
• Sudden release of histamine � massive vasodilation and permeability changes
Figure 19.18
Signs and symptoms
Acute bleeding (or other events that cause
blood volume loss) leads to:
1. Inadequate tissue perfusionresulting in ↓ O2 and nutrients to cells
2. Anaerobic metabolism by cells, so lactic
acid accumulates3. Movement of interstitial fluid into blood,
so tissues dehydrate
Initial stimulus
Result
Physiological response
Chemoreceptors activated(by ↓ in blood pH)
Baroreceptor firing reduced(by ↓ blood volume and pressure)
Hypothalamus activated(by ↓ pH and ↓ blood pressure)
Major effect Minor effect
Brain
Activation of
respiratory centers
Cardioacceleratory and
vasomotor centers activatedSympathetic nervous
system activated
ADH
released
Neurons
depressedby ↓ pH
Intense vasoconstriction
(only heart and brain spared)↑Heart rate Central
nervous systemdepressed
Adrenalcortex
Kidney
Renin released
↓ Renal blood flow
Aldosterone
released
Kidneys retain
salt and water
Angiotensin II
produced in blood
Water
retention
↓ Urine output↑ Rate and
depth ofbreathing
Tachycardia,
weak, threadypulse
Skin becomes
cold, clammy,and cyanotic
Thirst Restlessness
(early sign)
Coma
(late sign)
CO2 blown
off; bloodpH rises
Blood pressure maintained;
if fluid volume continues todecrease, BP ultimately
drops. ↓ BP is a late sign.
Pathways of Blood Circulation
• Complete circuits begin and end at heart
• A double pump with 2 pathways
– Pulmonary circulation
– Systemic circulation
Systemic Circulation
• Carries oxygen rich blood to all parts of the body
• Subdivisions
– Coronary circulation
• Supplies myocardium
– Hepatic-portal circulation
• Directs blood from spleen, stomach, pancreas, gallbladder, and intestines to the liver via portal vein
– Organs of digestion and recycling – materials are substantially metabolized in the liver before reaching general circulation
– Jaundice
• Portal systems
– 2 capillary beds
Copyright © 2010 Pearson Education, Inc.
(c) The hepatic portal circulation.
Hepatic veins
Liver
Spleen
Gastric veins
Inferior vena cava
Inferior vena cava(not part of hepaticportal system)
Splenic vein
Right gastroepiploicvein
Inferiormesenteric vein
Superiormesenteric vein
Large intestine
Hepatic portal vein
Small intestine
Rectum
Pulmonary Circulation
• Carries oxygen poor blood from heart to
alveolar surface of lungs and oxygen rich blood
back to the heart

3/27/2016
17
Fetal Circulation
• Oxygen and nutrients obtained from maternal
blood
– Respiratory and digestive systems not yet functional
– Blood oxygenated in placenta
• Attached to uterine wall by cotyledons (contain placental
villi)
• Waste carried from fetus by umbilical arteries
– Extensions of the internal iliac arteries
• Nutrient rich blood enters fetal circulation by umbilical
vein
Fetal Circulation
• Ductus venosus
– Continuation of the umbilical
vein under liver
– Drains into inferior vena cava
– Allows blood to bypass the liver
– Functionally closes minutes
after birth
– Structurally closes in term
infants in 3-7 days
Fetal Circulation
• Foramen ovale
– Opening between right and left atria � bypasses fetal
lungs
– Blood routed to aorta
Fetal Circulation
• Foramen ovale
– First breath after birth decreases pulmonary pressure
– Left atrial pressure exceeds right and forces foramen
ovale closed
– May remain open
• Patent foramen ovale or ASD
• “Hole in the heart”
• May be surgically closed
Fetal Circulation
• Ductus arteriosis
– Connects pulmonary artery with descending thoracic
aorta
– Also aids in bypassing lungs
Fetal Circulation
• Ductus arteriosis
– Failure to close at birth = patent ductus arteriosis
– Leads to pulmonary hypertension
and congestive heart failure
– NSAIDs are administered to
force closure
• Why NSAIDs MUST be
avoided in late pregnancy

3/27/2016
18
Figure 28.14a
Aortic archFetusSuperior vena cava
Ductus arteriosus
Ligamentum arteriosum
Lung
Pulmonary artery
Pulmonary veinsHeart
Foramen ovale
Fossa ovalis
LiverDuctus venosus
Ligamentum venosum
Ligamentum teres
Umbilical vein
Inferior vena cava
Hepatic portal vein
UmbilicusAbdominal aorta
Common iliac artery
Umbilical arteries
Medial umbilical ligaments
Urinary bladder
Umbilical cord
(a)
Placenta
High oxygenation
Moderate oxygenation
Low oxygenation
Very low oxygenation
Placenta
Umbilical vein
Ductus venosus
Inferior vena cava
Right atrium
Right ventricle
Pulmonary artery
Fetal Circulation
Left atrium
Aorta
Internal
iliac arteries
Umbilical
arteries
Placenta
Foramen ovale
Ductus arteriosis
Hypertension
• “Silent Killer”
– Produces few symptoms
• Major cause of heart failure, stroke & kidney
failure
• Resting systolic above?
• Resting diastolic above?
Blood Pressure Level (mmHg)
Category Systolic Diastolic
Normal < 120 and < 80
Prehypertension 120-139 or 80-89
High Blood Pressure
Stage 1 Hypertension
140–159 or 90–99
Stage 2 Hypertension
160 or 100
Categories for Blood Pressure
Levels in Adults
(Ages 18 Years and Older)
Hypertension
• Arteries are stretched
– Tears endothelium = exposes muscle = focal point
for atherosclerosis = worsens hypertension
• Remember atherosclerosis?
– Emboli may lodge in narrowed vessel
– Clots may form on roughened endothelium
– Long-standing belief that high lipid, high cholesterol
diets contribute are being called into question
Renal Hypertension
• Blood flow to kidneys is reduced
– Leads to thickening of arterioles � respond as
though BP were reduced � Angiotensin II produced
� aldosterone released
• Increases blood volume and BP
– Worsens existing hypertension �kidney failure may
result

3/27/2016
19
Hypertension
• Primary hypertension– 90% of hypertensive conditions
– Cause unknown
– Contributing factors include • Genetics
• Obesity» Adipose tissue extensively vascularized
» 10 miles per pound!!
» Means increased peripheral vascular resistance
• Smoking» Nicotine = coronary vasoconstrictor
• Diet» Salt = water retention � higher blood volume
» Mineral deficiencies (Mg, K, Ca)
Hypertension
• Secondary hypertension
– 10% of cases
– Due to identifiable disorders
• Kidney disease
• Atherosclerosis
• Endocrine disorders
– Hyperthyroidism
– Cushing’s disease
– Polycythemia
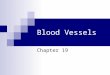
• Deep venous thrombosis (DVT)
• Affects mainly the veins in the lower leg and the thigh
• It involves the formation of a clot (thrombus) in the larger veins of the area
This picture shows a red and swollen thigh and leg caused by a
blood clot (thrombus) in the deep veins in the groin
which prevents normal return of blood from the leg to the heart.
• Can be caused by any condition that restricts venous return in the lower
extremities
• Cause in 1/3 of cases is unknown