-
8/22/2019 Blood Barrier Testis
1/10
T he n e w e n g l a n d j o u r n a l o f medicine
n engl j med 363;17 nejm.org october 21, 2010 1621
original article
Expression of Follicle-Stimulating Hormone
Receptor in Tumor Blood VesselsAurelian Radu, Ph.D., Christophe
Pichon, Ph.D., Philippe Camparo, M.D.,
Martine Antoine, M.D., Yves Allory, M.D., Anne Couvelard,
M.D.,Galle Fromont, M.D., Mai Thu Vu Hai, Ph.D.,
and Nicolae Ghinea, Ph.D.
From Mount Sinai School of Medicine,
New York (A.R.); and INSERM Unit 753,Villejuif (C.P.),
Val-de-Grce Hospital, Par is(P.C.), Tenon Hospital, Paris
(M.A.),INSERM Unit 955-Eq 07, UniversitParis-Est, Crteil (Y.A.,
M.T.V.H., N.G.),Beaujon Hospital, Clichy (A.C.), and Cen-tre
Hospitalier Universitaire de Poitiers,Poitiers (G.F.) all in
France. Addressreprint requests to Dr. Ghinea at INSERMUnit 955-Eq
07, 8 rue du Gnral Sarrail,Universit Paris-Est, Crteil, France, or
[email protected].
N Engl J Med 2010;363:1621-30.Copyright 2010 Massachusetts
Medical Society.
A b s t ra c t
Background
In adult humans, the follicle-stimulating hormone (FSH) receptor
is expressed only
in the granulosa cells of the ovary and the Sertoli cells of the
testis. It is minimallyexpressed by the endothelial cells of
gonadal blood vessels.
Methods
We used immunohistochemical and immunoblotting techniques
involving four sepa-
rate FSH-receptor-specific monoclonal antibodies that recognize
different FSH re-
ceptor epitopes and in situ hybridization to detect FSH receptor
in tissue samples
from patients with a wide range of tumors. Immunoelectron
microscopy was used
to detect FSH receptor in mouse tumors.
Results
In all 1336 patients examined, FSH receptor was expressed by
endothelial cells in
tumors of all grades, including early T1 tumors. The tumors were
located in the pros-
tate, breast, colon, pancreas, urinary bladder, kidney, lung,
liver, stomach, testis, and
ovary. In specimens obtained during surgery performed to remove
tumors, the FSH
receptor was not expressed in the normal tissues located more
than 10 mm from the
tumors. The tumor lymphatic vessels did not express FSH
receptor. The endothelial
cells that expressed FSH receptor were located at the periphery
of the tumors in a
layer that was approximately 10 mm thick; this layer extended
both into and outside
of the tumor. Immunoelectron microscopy in mice with xenograft
tumors, after
perfusion with antiFSH-receptor antibodies coupled to colloidal
gold, showed that
the FSH receptor is exposed on the luminal endothelial surface
and can bind and
internalize circulating ligands.
Conclusions
FSH receptor is selectively expressed on the surface of the
blood vessels of a wide
range of tumors. (Funded by INSERM.)
The New England Journal of Medicine
Downloaded from nejm.org by SIANIPAR MANGARA on August 9, 2013.
For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights
reserved.
-
8/22/2019 Blood Barrier Testis
2/10
Th e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 363;17 nejm.org october 21, 20101622
The follicle-stimulating hormone
(FSH) receptor is a glycosylated transmem-
brane protein that binds FSH and belongs
to the family of G-protein-coupled receptors. FSH,
a key hormone in mammalian reproduction, is
produced mainly in the anterior pituitary gland,
and the target organs are the ovary and testis. In
females, FSH stimulates follicular maturation andestrogen
production through aromatization of an-
drogens.1 In males, FSH stimulates Sertoli-cell pro-
liferation in immature testes and maintains nor-
mal spermatogenesis in adults.2
In adult humans and animals, the FSH recep-
tor is known to be expressed only in the testicu-
lar Sertoli cells and the ovarian granulosa cells,3,4
and it is expressed in low levels in the endothe-
lial cells of the ovary5 and testis.6 In the testis,
the FSH receptor mediates the translocation of
FSH across the blood-testis endothelial barrier
by a process of receptor-mediated transcytosis.6We conducted a
study to assess endothelial-cell
expression of the FSH receptor in blood vessels in
a wide range of human cancers.
Methods
Tissue Specimens
Tumor specimens (see Table 1 in the Supplemen-
tary Appendix, available with the full text of this
article at NEJM.org) were obtained from 1336 pa-
tients immediately after surgery. The patients did
not receive cytotoxic agents or hormones before
surgery. The specimens were fixed in formalin
and embedded in paraffin. Five study investiga-
tors performed histologic analysis of each tumor
specimen. Gleason scores and stages for prostate
tumors were assigned according to the World
Health Organization guidelines.7 (The Gleason
score is the sum of the two most common histo-
logic patterns or grades in a prostate tumor, each
of which is graded on a scale of 1 to 5, with 5 be-
ing the most cytologically aggressive.) The other
tumor types were graded histologically accord-ing to the
standards of the American Joint Com-
mittee on Cancer.8
The protocol was approved by the institutional
review board or ethics committee at each study
site. Written informed consent was obtained at the
time of surgery from all living donors from whom
samples were obtained. Control samples consist-
ed of normal tissue that routinely accompanies
tumors removed by surgery. Donors of normal
tissue also provided written informed consent.
Antibodies
Two FSH-receptor antibodies, FSHR18 and
FSHR323, were purified from hybridomas (Amer-
ican Type Culture Collection numbers CRL-2688
and CRL-2689). Two other FSH-receptor antibodies,FSHR190 and
FSHR225, were provided by anoth-
er researcher. The antibodies were shown to be
monospecific for the FSH receptor by the follow-
ing three independent methods: immunoblotting
of cell extracts from ovarian specimens and of ly-
sates of cell cultures transfected with FSH-receptor
complementary DNA (cDNA), coimmunoprecipi-
tation of radiolabeled FSH from cells that express
the FSH receptor, and immunohistochemical de-
tection of the FSH receptor in cells known to be
targets for the FSH in human tissues (granulosa
cells in the ovary and Sertoli cells in the testis).5
In Situ Hybridization and Confocal
Microscopy
In situ hybridization was performed with the use
of a biotinylated cDNA antisense oligonucleotide
probe9 (for details, see the Supplementary Ap-
pendix).Indirect immunofluorescence confocal
microscopy was performed on paraformaldehyde-
fixed cryostat sections obtained from unfixed
frozen prostate specimens or on paraffin-embed-
ded sections. The FSH receptor was detected with
the use of the FSHR323 antibody (for details, see
the Supplementary Appendix).
Immunoprecipitation, Electrophoresis,
and Western Blotting
Frozen tissue was solubilized in TRIS buffer
(pH 7.4) containing 0.4 M sodium chloride and
1.2% Triton X-100 (for details, see the Supplemen-
tary Appendix), and the FSHR323 antibody was
added to the supernatant. The complexes were cap-
tured on protein-A Sepharose beads and analyzed
by means of sodium dodecyl sulfatepolyacryl-amide-gel
electrophoresis (SDS-PAGE), followed
by immunoblotting with the use of the FSHR18
antibody.
Immunoelectron Microscopy
Tumors were generated by injecting nude mice
with LNCaP human prostate-cancer cells (for de-
tails, see the Supplementary Appendix). The blood
The New England Journal of Medicine
Downloaded from nejm.org by SIANIPAR MANGARA on August 9, 2013.
For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights
reserved.
-
8/22/2019 Blood Barrier Testis
3/10
FSH-Receptor Expression in Tumor Blood Vessels
n engl j med 363;17 nejm.org october 21, 2010 1623
was removed by systemic perfusion, and anti-FSH-
receptor antibodies coupled to colloidal gold were
systemically introduced by means of perfusion for
20 minutes. The vasculature was washed and pro-
cessed for electron microscopy.6
Results
Expression of FSH Receptor by Endothelial
Cells in Prostate Tumors
Our initial analysis was performed in human pros-
tate tumors with the use of the antiFSH-receptor
monoclonal antibody FSHR323. Immunohisto-
chemical analysis of paraff in-embedded sections
revealed strong staining of endothelial cells in tu-
mors (Fig. 1A). The FSH-receptor-positive blood
vessels were located at the periphery of the tu-
mors, as detailed below. No staining of endothe-
lial cells was visible in normal prostate tissue
(Fig. 1B), which was located more than 10 mmoutside the tumors
in specimens obtained by total
prostatectomy. A faint FSH-receptor signal was
visible occasionally in the tumor cells (Fig. 1A).
No staining occurred when tissue sections ob-
tained from patients with prostate cancer were in-
cubated with nonimmune mouse IgG2a of the
same isotype as FSHR323 (Fig. 1A in the Supple-
mentary Appendix), or when the primary antibody
was omitted (Fig. 1B in the Supplementary Ap-
pendix). The endothelial cells were identified as
belonging to blood vessels by costaining them
with an antibody against the vascular endothelial
marker, von Willebrand factor (Fig. 1F, 1G, and
1H). The lymphatic vessels in tumors, identified
with the use of the monoclonal antibody D2-40,
did not express the FSH receptor (Fig. 1D and 1E).
The identity of the antigen recognized in tumor
endothelial cells by the FSHR323 antibody was
confirmed by immunohistochemical analysis with
two other well-characterized monoclonal anti-
bodies, FSHR190 and FSHR225, which bound epi-
topes of the FSH receptor that are different from
those recognized by FSHR3235
and revealed astaining pattern identical to that of FSHR323
(Fig. 2 in the Supplementary Appendix).
The identity of the antigen was further con-
firmed by immunoprecipitation followed by de-
tection with an independent monoclonal antibody.
Prostate-tumor extract was immunoprecipitated
with the use of the FSHR323 antibody, subjected
to SDS-PAGE, and analyzed by means of immu-
noblotting with the use of FSHR18, which rec-
ognizes an epitope that is different from that
recognized by FSHR323.5 An 87-kD band corre-
sponding to the known molecular weight of the
mature glycosylated FSH receptor5 was detected
in the prostate-cancer tissue (Fig. 2A). No FSH-
receptor signal was visible in extracts from
normal-appearing prostate tissue obtained frompatients with
prostate cancer (Fig. 2A). It is ex-
tremely improbable that a protein other than the
FSH receptor contains both epitopes recognized
by the two antibodies and has the same molecu-
lar weight as the FSH receptor. In situ hybridiza-
tion confirmed the expression of FSH-receptor
RNA in the tumor endothelial cells (Fig. 2B and
2C). Thus, all three techniques used (immuno-
histochemical analysis with the use of three in-
dependent antibodies, immunoblotting, and in
situ hybridization) identified the FSH receptor.
The same consistent expression of the FSHreceptor by the
endothelial cells of tumor blood
vessels was detected in tissue specimens ob-
tained from all 773 patients with prostate can-
cer who were evaluated, and the absence of ex-
pression was confirmed in all associated normal
tissues. The lowest Gleason score in the tumors
analyzed was 5; this score characterizes tumors
of low malignant potential. Among the 773 tu-
mors analyzed, 41% had Gleason scores of 5 or
6. The most advanced tumors analyzed had the
highest Gleason score, 10. FSH-receptorpositive
blood vessels were also detected in approximately
20% of benign prostatic hyperplasia specimens, in
vessels surrounding hyperplastic glands (Fig. 1C).
In contrast to the findings in the tumors, the FSH-
receptorpositive vessels were present throughout
the hyperplastic areas, not only at the periphery.
The anatomical location of benign prostatic hy-
perplasia differed from the sites of most prostate
tumors10 and thus, FSH-receptorbased imaging
could be used to distinguish the two conditions.
Expression of FSH Receptor by EndothelialCells in Other Cancers
and Nonmalignant
Tissues
Immunohistochemical studies similar to those
described above were performed for 10 other tu-
mor types in a total of 563 patients (for details,
see Table 1 in the Supplementary Appendix). Ap-
proximately 70% of the tumors were grade I or II,
approximately 25% were grade III, and the re-
The New England Journal of Medicine
Downloaded from nejm.org by SIANIPAR MANGARA on August 9, 2013.
For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights
reserved.
-
8/22/2019 Blood Barrier Testis
4/10
Th e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 363;17 nejm.org october 21, 20101624
A
D
F G H
E
B C
*
Blood Vessel
Blood Vessel
LymphaticVessel
LymphaticVessel
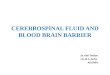
Figure 1. Expression of Follicle-Stimulating Hormone (FSH)
Receptor by Vascular Endothelial Cells in Human ProstateTumors.
Immunohistochemical analysis was performed on paraffin-embedded
sections of human prostate tissues with theuse of the
anti-FSH-receptor monoclonal antibody 323, followed by a secondary
peroxidase-coupled antibody visual-
ized with the use of the red-brown peroxidase-reaction product.
Sections were also stained with hematoxylin (Pan-els A and B). A
prostate tumor with a Gleason score of 6 showed strong staining of
vascular endothelial cells (Panel A,
arrows), whereas blood vessels of normal prostate tissue were
negative for the FSH receptor (Panel B, arrows). A
faintFSH-receptor signal was visible occasionally in the tumor
cells (Panel A, asterisk). The FSH receptor was expressed
in the blood vessels of hyperplastic tissue in 20% of samples
from patients with benign prostatic hyperplasia (Panel C,arrows).
In serial sections of tumor tissue, the blood vessels showed a
strong presence of FSH receptor (Panel D),
whereas the lymphatic vessels, identified with the use of the
monoclonal antibody D2-40 (Panel E), did not expressthe FSH
receptor. Double immunofluorescence on prostate-tumor tissue
confirmed the identity of the cells express-
ing the FSH receptor (Panels F through H). An antibody against
the vascular endothelial-cell marker von Willebrand
factor, followed by a green-labeled secondary antibody (Panel
G), overlapped with the signal from the anti FSH-receptor antibody
detected by a secondary red-labeled antibody (Panel F). Merging of
the two antibody signals with
a Nomarski image is shown in Panel H. The scale bar represents
25 m in all panels.
The New England Journal of Medicine
Downloaded from nejm.org by SIANIPAR MANGARA on August 9, 2013.
For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights
reserved.
-
8/22/2019 Blood Barrier Testis
5/10
FSH-Receptor Expression in Tumor Blood Vessels
n engl j med 363;17 nejm.org october 21, 2010 1625
maining tumors were grade IV. Examples of oth-
er types of tumors are shown in Figure 3. In each
of the tumors analyzed, without exception, we de-
tected consistent expression of the FSH receptor
by endothelial cells. As we found with the pros-
tate tumors, occasional cancer cells were also
faintly stained in breast tumors and exocrine
pancreatic tumors (data not shown).In all normal control
samples, which were ob-
tained from the same sections as the tumor sam-
ples, the endothelial cells of blood vessels were
negative for the FSH receptor (Fig. 3 in the Sup-
plementary Appendix), with the exception of a
faint FSH-receptor signal that was barely visible
in the blood vessels of testes and ovaries (Fig. 4 in
the Supplementary Appendix), which are known to
express the FSH receptor.5,6
We also analyzed nonmalignant inflammatory,
regenerative, and proliferative tissues and found
that expression of the FSH receptor is not a gen-eral feature of
such tissue responses. In samples
from patients with rheumatoid arthritis (Fig. 3B,
panel e), chronic pancreatitis (Fig. 3B, panel f),
Crohns disease, and wound healing (Fig. 5A, 5B,
and 5C in the Supplementary Appendix), no FSH-
receptor expression was detected in the endothe-
lial cells. In placental endothelial cells, high lev-
els of FSH receptor were expressed in all vessels
(Fig. 5D in the Supplementary Appendix).
Localization of FSH Receptor at Tumor
Periphery
A general characteristic of the vessels with endo-
thelial cells that expressed the FSH receptor in
prostate tumors was that they were located at
the periphery of the tumors, in shells that had a
thickness of approximately 10 mm (range, 7 to 15)
and extended a few millimeters both inside and
outside the tumor in the apparently normal tissue.
No FSH receptor-expressing vessels were detected
in the deeper areas of the tumors. Figure 4 shows
the distribution of the vessels expressing the FSH
receptor.The same shell-type distribution of endothelial
cells expressing the FSH receptor was observed in
all 11 tumor types examined, with the exception
of renal-cell carcinomas; in the latter type, in ap-
proximately 30%, the FSH receptor was expressed
uniformly in the vessels throughout the tumor,
and in approximately 40%, the FSH receptor was
expressed only at the exterior of the tumor. The
percentage of vessels expressing the FSH recep-
tor reached a maximum of 40 to 100% at the de-
marcation line between the tumor and the normal
tissue and decreased gradually to zero both to-
ward the interior and away from the tumor. The
values for both shell thickness and maximum per-
centage of FSH-receptorpositive vessels were low-
est in tumors of the exocrine pancreas and hepato-
BA
C
Molecular
Mass
Cancerou
sTiss
ue
Normal
Tiss
ue
220
97.4
87
66
46
30
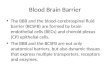
Figure 2. Immunoblotting and In Situ Hybridization Confirmation
of the
Identity of the Antigen Recognized in Tumors by the FSHR323
Antibody.
Panel A shows the results of immunoblotting to detect the
follicle-stimulat-
ing hormone (FSH) receptor. Equal amounts of Triton X-100
extracts fromcancerous and normal prostate tissues from the same
donor were immu-
noprecipitated with the FSHR323 antibody, subjected to sodium
dodecylsulfatepolyacrylamide-gel electrophoresis under reducing
conditions, and
transferred to nitrocellulose membranes. The samples were probed
withthe FSHR18 monoclonal antibody detected by ECL. FSHR18
recognized an
epitope that was different from the epitope recognized by
FSHR323. The ar-row in the column of molecular-mass markers
indicates the known size of
the mature glycosylated FSH receptor, 87 kD. The faint bands
correspond
to the mouse IgG used for immunoprecipitation. When the
experiment wasrepeated with tissues obtained from four other
patients, the results were
identical. Panels B and C show FSH-receptorpositive blood
vessels (arrows)detected by in situ hybridization. FSH-receptor
messenger RNA was revealed
with the use of a biotinylated probe detected by a
streptavidinalkaline phos-phatase conjugate, visualized by the
purple phosphatase-reaction product.
The sections were also stained with methyl green. The specimens
wereobtained from a patient with prostate cancer (Panel B) and a
patient with
clear-cell renal-cell carcinoma (Panel C). The scale bars
represent 25 m.
The New England Journal of Medicine
Downloaded from nejm.org by SIANIPAR MANGARA on August 9, 2013.
For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights
reserved.
-
8/22/2019 Blood Barrier Testis
6/10
Th e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 363;17 nejm.org october 21, 20101626
a
b
c
d
e
f
a
b
c
d
e
f
A
B
Figure3.
TumorTissuesfromO
therTypesofHumanCancersandInflam
matoryTissues.
Theperoxidase-coupledantibo
dywasvisualizedwiththeuseofthered-b
rownperoxidase-reactionproduct.Sectio
nswerealsostainedwithhematoxylin.Allarrowsshownpointto
bloodvessels.PanelAshowss
pecimensobtainedfrompatientswithbre
astcancerinsitu(a),nonsmall-celllung
cancer(b),liveradenocarcinoma(c),colo
nadenocarcinoma(d),
pancreaticadenocarcinoma(e)
,andstomachadenocarcinoma(f)(scale
bar,25m).PanelBshowsspecimensob
tainedfrompatientswithatestistumor(seminoma)(a),ovarian
cancer(b),urinarybladdercan
cer(c),andclear-cellrenal-cellcarcinoma
(d).TheFSHreceptorwasnotexpressedbytheendothelialcellsinspecimensfrom
patientswithrheuma-
toidarthritis(inthesynovialtissue)(e)andchronicpancreatitis(inthep
ancreaticparenchyma)(f)(scalebar,25
m).
The New England Journal of Medicine
Downloaded from nejm.org by SIANIPAR MANGARA on August 9, 2013.
For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights
reserved.
-
8/22/2019 Blood Barrier Testis
7/10
FSH-Receptor Expression in Tumor Blood Vessels
n engl j med 363;17 nejm.org october 21, 2010 1627
carcinomas; intermediate in tumors of the urinary
bladder, ovary, lung, and stomach; and highest
in tumors of the prostate, kidney, colon, breast,
and testis. The thickness of the shell did not ap-
pear to be related to the size of the tumor.
Exposure of FSH Receptor on the Luminal
Surface of the Tumor Epithelium
Tumor-specific endothelial receptors could be can-
didates for tumor imaging and therapy because
they may be directly accessible to intravenously
delivered agents, which may also accumulate in
the tumors after crossing the endothelial cells.
In Situ Animal Model
To assess whether endothelial FSH receptors are
accessible to intravenously delivered ligands, we
used an in situ animal model: mice that carried
LNCaP human xenograft tumors. The tumor en-
dothelial cells in these mice express the FSH re-ceptor (Fig. 6
in the Supplementary Appendix).
After perfusion of these mice for 20 minutes with
anti-FSH-receptor antibodies coupled to colloidal
gold, immunoelectron microscopy showed that in
tumors, gold particles were attached to the lumi-
nal aspect of the endothelium, on the plasma-
lemma proper (Fig. 5A), on the diaphragms of
fenestrae (Fig. 5B), and in the coated pits (Fig. 5C).
Particles were also visible in the interior of the
endothelial cells in coated vesicles (Fig. 5D), en-
docytic vesicles (Fig. 5E), and infrequently in mul-
tivesicular bodies (Fig. 5F). No tracer was detected
in the intercellular junctions of the endothelial
layer (Fig. 5G), indicating that no intercellular
transport occurred. Particles were also visible in
the lumen of channels that connect the luminal
and abluminal fronts of the endothelium and in
the subendothelial space adjacent to these struc-
tures (Fig. 7A in the Supplementary Appendix).
Accumulations of gold particles were infrequent-
ly visible in the interstitial space (Fig. 7B in the
Supplementary Appendix).
In contrast to the findings in the tumor en-dothelial cells,
extremely rare gold particles were
observed in endothelial cells of normal organs
(lung and prostate) obtained from the same ani-
mals. Most microscopical f ields did not show any
particles in the lung tissue (Fig. 5H) or the pros-
tate tissue. The most likely explanation for their
presence is that they were the few unbound par-
ticles in the blood vessels that had not been re-
moved by washing, and they were subsequently
cross-linked by glutaraldehyde to the endothelial-
cell surface. In the tumors, the gold particles were
visible on all examined endothelial cells in all
blood-vessel profiles; by contrast, in testes, the
particles were present in only approximately 10%
of the vessels, on the endothelial-cell plasma mem-
branes, and in coated pits, and at much lower
density than in the tumor blood vessels. Isolated
gold particles were also visible in rare cases in
the subendothelial space of the testes.
Discussion
We report FSH-receptor expression by endotheli-
al cells of blood vessels in a wide range of tumors
in all 1336 patients examined. Two previous stud-
ies showed immunohistochemical detection of the
FSH receptor in the tumor cells of prostate ade-
nocarcinomas.11,12 The presence of the FSH recep-
tor in the endothelial cells was not mentioned,
possibly because specimens from the peripheral
areas had not been examined. This supposition
VesselsExpressingFSH
Receptor(%)
No.ofVesselspermm2
100
75
50
25
0
50
40
30
10
20
06 4 2 0 642 8 10
Distance from Tumor Border (mm)
Tumor Normal Tissue
FSH-expressing vessels No. of vessels
Figure 4. FSH-Receptor Expression According to Vessel
Location.
The blood vessels were visualized with the use of antivon
Willebrand fac-
tor antibodies followed by Alexa-488 dye secondary antibodies,
and FSH-receptorstained vessels were visualized by the FSHR323
antibody followed
by Alexa-555 dyelabeled secondary antibodies. The vessels were
countedon 148 microscopical digital images of tumors obtained from
five patients.
Zero indicates the border of the tumor, the negative numbers
indicate theinterior of the tumor, and the positive numbers
indicate the exterior of the
tumor. The red circles and dashed line represent the percentage
of FSH-receptorexpressing vessels. The blue squares indicate the
total number
of vessels per square millimeter; the mean number was higher in
the interi-
or of the tumor than in the exterior (372 vs. 251 vessels per
square milli-meter, P
-
8/22/2019 Blood Barrier Testis
8/10
Th e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 363;17 nejm.org october 21, 20101628
cannot be verified because the antibodies are no
longer available.
The location of the FSH-receptorpositive ves-
sels in the normal tissue immediately adjacent tothe tumor is
consistent with the view that the tu-
mor cells in the invasive front attract surround-
ing blood vessels toward the tumor, and during
this process, FSH-receptor expression is activated.
Another possibility is suggested by the observa-
tion that in breast tumors in humans, endothelial
cells proliferate at the tumor periphery but not in
the interior.13 Accordingly, FSH-receptor expres-
sion by endothelial cells may be associated with
their proliferation in this particular location.
If it becomes possible to exploit FSH-receptor
expression for imaging purposes, the location of
the FSH-receptor signal at the boundary between
the tumoral and the normal tissues should makeit useful for
defining the target volume for ra-
diation therapy or surgery.
If it can be shown that intravenously adminis-
tered antibodies can detect tumor endothelial
cells, the presence of FSH receptor on the surface
of these cells in a wide range of tumors makes it
a potential target for both tumor imaging and
therapy. As shown in Figure 4 in the Supplemen-
tary Appendix, FSH-receptor density on the go-
nadal endothelial cells is much lower than that
BasalMembrane
A B C
D E F
G H
Lumen
Lumen Lumen
Lumen Lumen
PlasmaMembrane
Lumen
Lumen Lumen
Plasma Membrane
Fenestra
Fenestra
JunctionJunction
Luminal CaveolaLuminal Caveola
Coated Pit
CoatedVesicle
LuminalCaveola
Endosome
Endosome
MultivesicularBody
Figure 5. AntiFSH-Receptor Antibodies Coupled to Perfused
Colloidal Gold in the Vasculature of Tumor-Bearing Mice.
Tumors generated by the prostate-cancer line LNCaP were excised
after a 20-minute perfusion of the mice with5-nm gold particles
conjugated to FSHR323 and were processed for electron microscopy.
Ultrathin sections were
stained with uranyl acetate and lead citrate. The conjugate
particles were bound to the plasma membrane (Panel A),to the
diaphragms of fenestrae (Panel B), and to luminal coated pits
(Panel C), and they were internalized in coated
vesicles (Panel D), endosomes (Panel E), and multivesicular
bodies (Panel F). The particles did not cross the endo-thelial
layer through the junctions (Panel G). No binding was visible on
either the luminal plasma membrane or the
luminal caveolae associated with the surface of capillaries in
the lung, the first organ of the mouse that was accessi-ble by
perfusion to the FSHR323-gold particles (Panel H). Scale bars in
Panels A through F and Panel H represent
50 nm, and the scale bar in Panel G represents 100 nm.
The New England Journal of Medicine
Downloaded from nejm.org by SIANIPAR MANGARA on August 9, 2013.
For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights
reserved.
-
8/22/2019 Blood Barrier Testis
9/10
FSH-Receptor Expression in Tumor Blood Vessels
n engl j med 363;17 nejm.org october 21, 2010 1629
in tumors, and therefore, it may be possible to
find a therapeutic window so that the gonadal
vessels are not substantially affected. The Sertoli
and granulosa cells, which express high levels of
FSH receptor, could be spared if the toxic agents
targeted at the FSH receptor were delivered in a
particulate form that would not cross the blood-
gonadal endothelial barrier. The volume that canbe targeted by
FSH receptor represents a substan-
tial fraction of the volume of small tumors (e.g.,
a 3-mm-thick peripheral layer inside a tumor with
a 2-cm diameter accounts for 66% of its volume,
leaving an unstained core with a 14-mm diame-
ter). The functional relevance of the volume that
can be targeted may be even greater than its
geometric contribution because of a more in-
tense proliferation of cancer cells at the tumor
periphery.14-19
Our in situ experiments cannot be considered
to be a proof-of-principle demonstration that theFSH receptor
expressed on tumor-associated blood
vessels can be exploited clinically. We removed
the blood from the mice before perfusing gold-
labeled antibodies into vasculature. Our model
does not mimic a clinical application in humans.
The binding of FSH to FSH receptor in ovarian
granulosa cells induces an increase in hypoxia-
inducible factor 1 protein levels under normoxic
conditions, which in turn leads to up-regulation
of vascular endothelial growth factor (VEGF).20
This observation provides support for the specu-
lation that FSH-receptor expression could in-
duce VEGF and VEGF receptor 2 (VEGFR-2) signal-
ing in tumor endothelial cells and thus promote
angiogenesis. The fact that FSH and FSH-receptor
signaling is known to generate activated Gq/11
protein21 suggests yet another biologic role for
the presence of the FSH receptor in tumor en-dothelial cells.
Gq/11 has been shown to induce
VEGFR-2 signaling in human umbilical-vein
endothelial cells, even in the absence of VEGF.22
This effect may substantially enhance the prolif-
eration and migration of endothelial cells in
cancer independently of VEGF availability. For
both mechanisms, we speculate that blocking
FSH-receptor signaling could be a new antitumor
strategy.
In conclusion, we found that the FSH receptor,
which was present on the endothelial surface of
blood vessels at the periphery of a wide range oftumors, was
accessible to agents injected intra-
venously.
Supported by INSERM.Disclosure forms provided by the authors are
available with
the full text of this article at NEJM.org.We thank Sylvette
Reposo and Pascale Soyeux-Porte for excel-
lent technical assistance, Drs. Karen Leroy and Jeanne Tran
Van
Nhieu for some of the liver and colon antibodies, Dr.
HuguesLoosfelt for the FSHR190 and FSHR225 specimens, Dr.
Xavier
Decrouy for assistance with confocal microscopy, Dr.
ChristoChristov for assistance with electron microscopy, and Dr.
Fran-
cis Vachereau for the LNCaP xenografts.
References
1. Macklon NS, Fauser BC. Follicle de-velopment dur ing the
normal menstrual
cycle. Matur itas 1998;30:181-8.
2. Plant TM, Marshall GR. The function-
al signif icance of FSH in spermatogenesis
and the control of its secretion in maleprimates. Endocr Rev
2001;22:764-86.
3. Sprengel R, Braun T, Nikolics K, Sega-loff DL, Seeburg PH.
The testicular recep-
tor for follicle-stimulating hormone: struc-ture and functional
expression of cloned
cDNA. Mol Endocrinol 1990;4:525-30.
4. Simoni M, Gromoll J, Nieschlag E. Thefollicle stimulating
hormone receptor: bio-
chemistry, molecular biology, physiology,and pathophysiology.
Endocr Rev 1997;
18:739-73.
5. Vannier B, Loosfelt H, Meduri G, PichonC, Milgrom E.
Anti-human FSH receptor
monoclonal antibodies: immunochemicaland immunocytochemical
characterization
of the receptor. Biochemistry 1996;35:1358-
66.6. Vu Hai MT, Lescop P, Loosfelt H,
Ghinea N. Receptor-mediated transcytosisof follicle stimulating
hormone through
the rat testicular microvasculature. BiolCell
2004;96:133-44.
7. Eble JN, Sauter G, Epstein JI, Sester-henn IA, eds. World
Health Organization
classification of tumours: pathology andgenetics of tumours of
the urinary system
and male genital organs. Lyon, France:
IARC Press, 2004.8. Green FL, Compton CC, Fritz AG, Shah
JP, Winchester DP, eds. American JointCommittee on Cancer: AJCC
cancer stag-
ing atlas. Heidelberg, Germany: Springer-Verlag, 2006.
9. Bckers TM, Nieschlag E, Kreutz MR,
Bergmann M. Localization of follicle-stim-ulating hormone (FSH)
immunoreactivity
and hormone receptor mRNA in testicu-lar tissue of infert ile
men. Cell Tissue Res
1994;278:595-600.
10. De Marzo AM, Platz EA, Sutclif fe S, etal. Inflammation in
prostate carcinogen-
esis. Nat Rev Cancer 2007;7:256-69.
11. Mariani S, Salvatori L, Basciani S, et
al. Expression and cellular localization of
follicle-stimulating hormone receptor innormal human prostate,
benign prostatic
hyperplasia and prostate cancer. J Urol2006;175:2072-7.
12. Ben-Josef E, Yang SY, Ji TH, et al. Hor-mone-refractory
prostate cancer cells ex-
press functional follicle-stimulating hor-mone receptor (FSHR).
J Urol 1999;161:
970-6.
13. Fox SB, Gatter KC, Bicknell R, et al.
Relationship of endothelial cell prolifera-
tion to tumor vascularity in human breastcancer. Cancer Res
1993;53:4161-3.
14. Begum R, Douglas-Jones AG, MorganJM. Radial intratumoral
increase and cor-
relation of microvessels and proliferationin solid breast
carcinoma. Histopatholo-
gy 2003;43:244-53.
15. Belin JA, van Diest PJ, Baak JP. Rela-tionships between
vascularization and pro-
liferation in invasive breast cancer. J
Pathol1999;189:309-18.
16. Shoji M, Dobashi Y, Morinaga S, Jiang
SX, Kameya T. Tumor extension and cellproliferation in
adenocarcinomas of the
lung. Am J Pathol 1999;154:909-18.
17. Rodins K, Cheale M, Coleman N, Fox
SB. Minichromosome maintenance pro-
tein 2 expression in normal kidney andrenal cell carcinomas:
relationship to tu-
mor dormancy and potential clinical util-ity. Clin Cancer Res
2002;8:1075-81.
18. Fernebro J, Engellau J, Persson A, Ryd-holm A, Nilbert M.
Standardizing evalua-
The New England Journal of Medicine
Downloaded from nejm.org by SIANIPAR MANGARA on August 9, 2013.
For personal use only. No other uses without permission.
Copyright 2010 Massachusetts Medical Society. All rights
reserved.
-
8/22/2019 Blood Barrier Testis
10/10
n engl j med 363;17 nejm.org october 21, 20101630
FSH-Receptor Expression in Tumor Blood Vessels
tion of sarcoma proliferation: higher Ki-67 expression in the
tumor periphery than
the center. APMIS 2007;115:707-12.
19. Ohashi K, Nemoto T, Eishi Y, Matsu-
no A, Nakamura K, Hirokawa K. Prolifer-
ative activity and p53 protein accumula-tion correlate with
early invasive trend, and
apoptosis correlates with differentiationgrade in oesophageal
squamous cell car-
cinomas. Virchows Arch 1997;430:107-15.20. Alam H, Weck J,
Maizels E, et al. Role
of the phosphatidylinositol-3-kinase andextracellular regulated
kinase pathways
in the induction of hypoxia-inducible fac-tor (HIF)-1 activity
and the HIF-1 target
vascular endothelial growth factor in ovar-
ian granulosa cells in response to follicle-stimulating hormone.
Endocrinology 2009;
150:915-28.
21. Castro-Fernndez C, Maya-Nez G,
Mndez JP. Regulation of follicle-stimulat-ing and luteinizing
hormone receptor sig-
naling by regulator of G protein signalingproteins. Endocrine
2004;25:49-54.
22. Zeng H, Zhao D, Yang S, Datta K, Muk-hopadhyay D.
Heterotrimeric G alpha q/G
alpha 11 proteins function upstream of
vascular endothelial growth factor (VEGF)receptor-2 (KDR)
phosphorylation in vas-
cular permeability factor/VEGF signaling.J Biol Chem
2003;278:20738-45.
Copyright 2010 Massachusetts Medical Society.
The New England Journal of Medicine
Downloaded from nejm.org by SIANIPAR MANGARA on August 9, 2013.
For personal use only. No other uses without permission.