Embed Size (px)
Citation preview

BLOOD AND TISSUEPROTOZOONS
PLASMODIUMTRYPANASOMA
BABESIA
Doç.Dr.Hrisi BAHARDoç.Dr.Hrisi BAHAR

The Malarias:
PLASMODIUMS
Plasmodium falciparumPlasmodium vivax
Plasmodium malariaePlasmodium ovale
PLASMODIUM SPECIES CAUSES “MALARIAS”
IN HUMAN
►Plasmodium falciparum ►Plasmodium vivax ►Plasmodium malariae ►Plasmodium ovale

PLASMODIUMS
►The malaria parasite exhibits a complex life cycle involving an insect vector (mosquito) and a vertebrate host (human).
► Four Plasmodium species infect humans.
► All four species exhibit a similar life cycle with only minor variations.

PLASMODIUMS
1*The infection is initiated when sporozoites are injected with the saliva of a feeding mosquito.
Sporozoites are carried by the circulatory system to the liver and invade hepatocytes
2*The intracellular parasite undergoes an asexual replication known as exoerythrocytic schizogony within the hepatocyte

PLASMODIUMS
3*Exoerythrocytic schizogony activates the production of merozoites which are released into the bloodstream
4*Merozoites invade erythrocytes and undergo a trophic period in which the parasite enlarges
5*The early trophozoite is often referred to as 'ring form' because of its morphology.

PLASMODIUMPLASMODIUM
Plasmodium vivax Plasmodium malaria
Ring formRing form

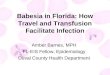
Scanning electron micrograph of Plasmodium-infected red blood cells. One cell has burst open, releasing merozoites

PLASMODIUMPLASMODIUM
► Trophozoite enlargement is accompanied by an active metabolism including the ingestion of host cytoplasm and the proteolysis of hemoglobin into amino acids.
► The end of the trophic period is manifested by multiple rounds of nuclear division without cytokinesis resulting a schizont

PLASMODIUMPLASMODIUM
► A proportion of the liver-stage parasites
from P. vivax and P. ovale go through a dormant
period instead of immediately undergoing
asexual replication
► These hypnozoites will reactivate several weeks to months (or years) after the primary infection and are responsible for relapses.

PLASMODIUMPLASMODIUM
► The merozoites from the mature schizont are released following rupture of the infected erythrocyte.
► Invasion of erythrocytes reinitiates another round of the blood-stage replicative cycle

Life cycle Life cycle
Life cycle

PLASMODIUMPLASMODIUM
► The blood stage is responsible for the pathology associated with malaria
► The intermittent fever paroxyms are due to the synchronous lysis of the infected erythrocytes

PLASMODIUMPLASMODIUM
► P.malariae exhibits a 72 hour periodicity, whereas the other three species exhibit 48 hour cycles for the fever.
►P. falciparum often exhibits a continuous fever rather than the periodic paroxyms.
P.falciparum also is responsible for more morbidity and mortality than the other species

PLASMODIUMPLASMODIUM
► This increase virulence is due in part to the higher levels of parasitemia associated with
P. falciparum infections. In addition, more complications are associated with P. falciparum because of the sequestration of the trophozoite- and schizont-infected erythrocytes in the deep tissues

PLASMODIUMPLASMODIUM
► As an alternative to the asexual replicative cycle, the parasite can differentiate into sexual forms known as macro- or microgametocytes
► The gametocytes are large parasites which fill upthe erythrocyte, but only contain one nucleus.
► Ingestionof gametocytes by the mosquito vectorinduces gametogenesis and escape from the hostErythrocyte.

PLASMODIUMPLASMODIUM
►Microgametes, formed by a process
known as exflagellation , are flagellated forms
which will fertilize the macrogamete
leading to a zygote .
► The zygote develops into a motile ookinete
which penetrates the gut epithelial cells and
develops into an oocyst

PLASMODIUMPLASMODIUM
► The oocyst undergoes multiple rounds of asexual replication resulting in the production of sporozoites .
► Rupture of the mature oocyst releases the sporozoites into the body cavity of the mosquito The sporozoites migrate to and invade the salivary glands, thus completing the life cycle.

PLASMODIUMPLASMODIUM
In summary, malaria parasites undergo three distinct asexual replicative stages
1-Exoerythrocytic schizogony
2-Blood stage schizogony
3- Sporogony

General Clinical Manifestationof “Malaria”
► Infection is characterized by acute febrile attacks (malaria paroxysms) due to blood stage (not liver stage or gametocytes)
► Manifestations and severity of the infection depend on species and host status, immunity, general health,nutritional state, genetics.

General Clinical Manifestationof “Malaria”
► Recrudescences or relapses can occur over months or years and can develop severe complications.(especially P. falciparum)


PATHOGENESIS OF PATHOGENESIS OF “MALARIA”“MALARIA”
Primary attackPrimary attack
► Infected erythrocyte rupture Infected erythrocyte rupture products of schizont, stimulate the release products of schizont, stimulate the release
of cytokines (TNF) of cytokines (TNF) paroxysm (shiver, paroxysm (shiver,
fever, sweat)fever, sweat)

PATHOGENESIS OF PATHOGENESIS OF “MALARIA“MALARIA
RelapseRelapse
► It is a recurrence that taken place after It is a recurrence that taken place after
complete initial clearing of the erythrocytic complete initial clearing of the erythrocytic
infection and implies reinvation of the infection and implies reinvation of the
blood stream by merozoites from activated blood stream by merozoites from activated
hypnozoites in liver.hypnozoites in liver.

PATHOGENESIS OF PATHOGENESIS OF “MALARIA“MALARIA
RecrudescenceRecrudescence► It is a recurrence of symptoms in a patient It is a recurrence of symptoms in a patient
whose blood stream infection has previously whose blood stream infection has previously
been at such a low level as not to be clinically been at such a low level as not to be clinically
demonstrable or cause symptoms.demonstrable or cause symptoms.

ComplicationsComplications Of “MALARİA Of “MALARİA””
► AnemiaAnemia Hemolysis of infected erythrocytesHemolysis of infected erythrocytes HypersplenismHypersplenism Autoimmunization of uninfected erythrocytes Autoimmunization of uninfected erythrocytes TNF-TNF-
► Splenomegaly:Splenomegaly:
► Malarious nephrosisMalarious nephrosis
► Cerebral malariaCerebral malaria

DiagnosisDiagnosis of “Malaria” of “Malaria”
► 1.1.Parasite; Species; DensityParasite; Species; Density
**Thin blood films (species identification)Thin blood films (species identification)
**Thick blood filmsThick blood films

DiagnosisDiagnosis of “Malaria” of “Malaria”
► 22 Immuno-diagnosisImmuno-diagnosis
**Specific antibody detectionSpecific antibody detection **Antigen detectionAntigen detection
**Specific DNA or RNA detectionSpecific DNA or RNA detection

TreatmentTreatment
1.1. Treatment by cTreatment by classes of antimalarial drugslasses of antimalarial drugs
► 1)1) Blood schizonticides (quinine; Blood schizonticides (quinine; chloroquine; artemisinin; mefloquine; chloroquine; artemisinin; mefloquine; sulfadoxin-pyrimethamine) sulfadoxin-pyrimethamine)
--Effect on erythrocytic stage, use for acute Effect on erythrocytic stage, use for acute attackattack..

TreatmentTreatment
► 2)2) Tissue schizonticides (Primaquine)Tissue schizonticides (Primaquine)
--Effect on the stages in liver (including Effect on the stages in liver (including
hypnozoite), use for prevent relapse (radical hypnozoite), use for prevent relapse (radical
cure) of cure) of P.vP.v or or P.oP.o malaria malaria

Choice of drugsChoice of drugs
11)) Treatment of vivax, malariae, ovale and Treatment of vivax, malariae, ovale and chloroquine-sensitive falciparum malaria: chloroquine-sensitive falciparum malaria: chloroquinechloroquine
2)2) Radical cure of vivax or ovale malaria: Radical cure of vivax or ovale malaria: chloroquine + primaquinechloroquine + primaquine
3)3) Treatment of chloriquine-resistant Treatment of chloriquine-resistant falciparum malaria: falciparum malaria: artemisinin or mefloquine artemisinin or mefloquine or quinineor quinine

Transmission and preventionTransmission and prevention
► Factors of transmissionFactors of transmission Suitable species of anopheles (60 Suitable species of anopheles (60
species are considered to be vectors species are considered to be vectors of malaria, major vectors in China: of malaria, major vectors in China:
A. sinensis, A. minimusA. sinensis, A. minimus))

Transmission and preventionTransmission and prevention
Prevention:Prevention:
BBreaking the human-mosquito-human cyclereaking the human-mosquito-human cycle
1)1) Control of the source of infectionControl of the source of infection by by chemotherapychemotherapy
2)2) Control of transmission routeControl of transmission route: :
residual insecticides, avoidance of infected residual insecticides, avoidance of infected mosquitoesmosquitoes

Transmission and preventionTransmission and prevention
33) Chemoproplylaxis) Chemoproplylaxis
TTaking suppressive drugs, beginning one aking suppressive drugs, beginning one
week before travel to endemic area and week before travel to endemic area and
continuing until 6 weeks after returncontinuing until 6 weeks after return
44) Malaria vaccines) Malaria vaccines

TRYPANASOMATRYPANASOMA
► Trypanosomes infect a variety of hosts Trypanosomes infect a variety of hosts and cause various diseases, including the and cause various diseases, including the fatal diseasefatal disease SLEEPING SICNESSSLEEPING SICNESS in in humans. These deadly parasites mostly humans. These deadly parasites mostly live in the blood and tissue fluids but can live in the blood and tissue fluids but can also inhabit intracellular locations in the also inhabit intracellular locations in the host's body as well. host's body as well.

““Trypanasoma”Trypanasoma”

Life cycleLife cycle
► < < Infection occurs when infected Infection occurs when infected metacyclic trypomastigotes enter the body metacyclic trypomastigotes enter the body through wound openings or mucous through wound openings or mucous membranes.membranes.
► < < The trypomatigotes enter various cells, The trypomatigotes enter various cells, differentiate into amastigotes and multiply differentiate into amastigotes and multiply intracellularly.intracellularly.

Life cycleLife cycle
► << The amastigotes differentiate into The amastigotes differentiate into trypomastigotes which are then released trypomastigotes which are then released back into the bloodstream.back into the bloodstream.
► << The life cycle is continued when a The life cycle is continued when a reduviid bug feeds on an infected person reduviid bug feeds on an infected person and ingests trypomastigotes in the blood and ingests trypomastigotes in the blood mealmeal..

Life cycle

TRYPANASOMATRYPANASOMA
► Human African Trypanosomiasis, also known as sleeping sickness, is a vector-borne parasitic disease.
► The parasites concerned are protozoa belonging to the Trypanosoma Genus.
► They are transmitted to humans by tsetse fly (Glossina Genus) bites which
have acquired their infection from human beings or from animals harbouring the human pathogenic parasites.

tsetse flytsetse fly
Glossina brevipalpisGlossina brevipalpis

TRYPANASOMATRYPANASOMA
► Sleeping sickness occurs only in sub-Sleeping sickness occurs only in sub-SaharanAfrica in regions where there are SaharanAfrica in regions where there are tsetse flies thatcan transmit the disease. tsetse flies thatcan transmit the disease.
► For reasons that are so far unexplained, For reasons that are so far unexplained, there are many regions where tsetse flies there are many regions where tsetse flies are found, but sleeping sickness is not.are found, but sleeping sickness is not.

TRYPANASOMATRYPANASOMA
► Sleeping sickness generally occurs in remote rural areas where health systems are weak or non-existent. The disease spreads in poor settings. Displacement of populations, war and poverty are important factors leading to increased transmission.
► The disease develops in areas whose size can range from a village to an entire region. Within a given area, the intensity of the disease can vary from one village to the next

TRYPANASOMATRYPANASOMA
Human African Trypanosomiasis takes two forms, depending on the parasite involved.
1.form► Trypanosoma brucei gambiense (T.b.g.) is found in
west and central Africa. This form represents more than 90% of reported cases of sleeping sickness and causes a chronic infection.
► A person can be infected for months or even years without major signs or symptoms of the disease. When symptoms do emerge, the patient is often already in an advanced disease stage when the central nervous system is affected.

TRYPANASOMATRYPANASOMA
2.Form
► Trypanosoma brucei rhodesiense (T.b.r.) is found in eastern and southern Africa. This form represents less than 10% of reported cases and causes an acute infection.
First signs and symptoms are observed after a few months or weeks. The disease develops rapidly and invades the central nervous system.

TRYPANASOMATRYPANASOMA
Another form of trypanosomiasis occurs in 15 Central and South American countries. It is known as :
American Trypanosomiasis or “Chagas disease”. The causal organism is a different species from those causing the African form of the disease.

Symptoms of Symptoms of “Sleeping Sicness”“Sleeping Sicness”
The disease is transmitted through the bite of an infected tsetse fly. At first the trypanosomes multiply in subcutaneous tissues, blood and lymph. In time, the parasites cross the blood-brain barrier to infect the central nervous system. The process can take years.

Symptoms of Symptoms of “Sleeping Sicness”“Sleeping Sicness”
► The first stage of the disease, known as a The first stage of the disease, known as a ““haemolymphatic phasehaemolymphatic phase”, entails bouts of ”, entails bouts of fever, headaches, joint pains and itching. fever, headaches, joint pains and itching.
► The second stage, known as the The second stage, known as the ““neurological phaseneurological phase”, begins when the ”, begins when the parasite crosses the blood-brain barrier parasite crosses the blood-brain barrier and invades the central nervous system .and invades the central nervous system .

Symptoms of Symptoms of “Sleeping Sicness“Sleeping Sicness
► In general this is when the signs and symptoms In general this is when the signs and symptoms of the disease appear: confusion, sensory of the disease appear: confusion, sensory disturbances and poor coordination. Disturbance disturbances and poor coordination. Disturbance of the sleep cycle, which gives the disease its of the sleep cycle, which gives the disease its name, is an important feature of the second name, is an important feature of the second stage of the disease.stage of the disease.
► Without treatment, sleeping sickness is fatalWithout treatment, sleeping sickness is fatal . .

DiagnosisDiagnosis
Diagnosis must be made as early as Diagnosis must be made as early as possible and before the neurological stage possible and before the neurological stage in order to avoid complicated, difficult and in order to avoid complicated, difficult and risky treatment procedures.risky treatment procedures.
Diagnosis follows a three-step pathway Diagnosis follows a three-step pathway
► ScreeningScreening
► Diagnostic confirmation, Diagnostic confirmation,
► Staging. Staging.

DiagnosisDiagnosis
► ► Diagnostic confirmation then relies on Diagnostic confirmation then relies on the finding of trypanosomes in the blood, the finding of trypanosomes in the blood, lymph nodes, or cerebrospinal fluid (CSF). lymph nodes, or cerebrospinal fluid (CSF). Unfortunately, it is estimated that 20 to Unfortunately, it is estimated that 20 to 30% of patients are missed by the 30% of patients are missed by the standard parasitological techniques standard parasitological techniques

TreatmentTreatment
First stage treatmentsFirst stage treatments PentamidinePentamidine: : discovered in 1941, used discovered in 1941, used
for the treatment of the first stage of for the treatment of the first stage of T.b. T.b. gambiensegambiense sleeping sickness. sleeping sickness.
SuraminSuramin: : discovered in 1921, used for the discovered in 1921, used for the treatment of the first stage of treatment of the first stage of T.b. T.b. rhodesienserhodesiense. .

TreatmentTreatment
Second stage treatmentsSecond stage treatments
Melarsoprol:Melarsoprol: discovered in 1949, it is discovered in 1949, it is used in both forms of infection.used in both forms of infection.
Eflornithine:Eflornithine: this molecule, less toxic this molecule, less toxic than melarsoprol, was registered in than melarsoprol, was registered in 1990. It is only effective against 1990. It is only effective against T.b. T.b. gambiensegambiense. .

BABESIABABESIA
► BabesiaBabesia is a protozoan parasite of the is a protozoan parasite of the blood that causes a hemolytic disease blood that causes a hemolytic disease known asknown as Babesiosis.Babesiosis.
► Babesia microtiBabesia microti andand Babesia Babesia divergensdivergens are the two species to most are the two species to most frequently infect humansfrequently infect humans

BABESIA SPBABESIA SP
► There are >100 specicies of this intracellular There are >100 specicies of this intracellular parasiteparasite. . ► Babesia microtiBabesia microti is the predominant human pathogen, is the predominant human pathogen, endemic to the Midwest.endemic to the Midwest.► 10-20% of adults are seropositive in endemic areas10-20% of adults are seropositive in endemic areas► Natural parasite reservoir is rodentsNatural parasite reservoir is rodents► Carried by the hard-bodied Carried by the hard-bodied IxodesIxodes Deer tick Deer tick. . ► Also carries agents for Lyme Disease, and Also carries agents for Lyme Disease, and EhrlichoisisEhrlichoisis. . ► Can also be transferred transplacentally and through Can also be transferred transplacentally and through blood transfusion.blood transfusion.

Babesia in erythrocytsBabesia in erythrocyts
Presence of 4 daughter merozoites in a tetrad . Never seen in malaria.

Clinical presentationClinical presentation
► Ranges from asymptomatic infection to fatal Ranges from asymptomatic infection to fatal illness (rare)illness (rare)
► No direct correlation between parasitemia and No direct correlation between parasitemia and severity. severity.
► More severe infection tends to occur in More severe infection tends to occur in immunnocompromised, elderly, and the very immunnocompromised, elderly, and the very young.young.

Clinical presentationClinical presentation
► The extreme end of the spectrum is often The extreme end of the spectrum is often described as a malaria-like infection; described as a malaria-like infection; symptoms may include malaise, chills, symptoms may include malaise, chills, mylagia, anemia, fatigue, and fever mylagia, anemia, fatigue, and fever ..
Some cases also described emesis, Some cases also described emesis,
night sweats, weight loss, and hematuria.night sweats, weight loss, and hematuria.

Life cycleLife cycle
► The trophozoite is very similar to the ring form The trophozoite is very similar to the ring form of the of the PlasmodiumPlasmodium species species
► The organism (The organism (sporozoitesporozoite) is transmitted by a ) is transmitted by a tick and enters the red cell where it undergoes tick and enters the red cell where it undergoes mitosis and the organisms (mitosis and the organisms (merozoitemerozoite) are ) are released to infect other red cells. Ticks acquire released to infect other red cells. Ticks acquire the organism during feeding on an infected the organism during feeding on an infected individual. In the tick, the organism divides individual. In the tick, the organism divides sexually in the gut and migrates into the salivary sexually in the gut and migrates into the salivary glandgland


Special Case – SplenectomySpecial Case – Splenectomy
► Illness appears suddenly, with hemoglobinuria Illness appears suddenly, with hemoglobinuria as the presenting symptom followed by jaundice as the presenting symptom followed by jaundice due to severe hemolysis. due to severe hemolysis.
► Parasitemia can reach 80% of RBCsParasitemia can reach 80% of RBCs
► Can be a medical emergency.Can be a medical emergency.
► In the most severe cases, patients develop a In the most severe cases, patients develop a shock-like picture, with renal failure and shock-like picture, with renal failure and pulmonary edema.pulmonary edema.
► Chronic disease with many relapses over Chronic disease with many relapses over months to years may occur if not treatedmonths to years may occur if not treated..

Co-InfectionCo-Infection
► It is estimated from serologic surveys that as many as It is estimated from serologic surveys that as many as 13% of Lyme disease patients in babesia-endemic areas 13% of Lyme disease patients in babesia-endemic areas are coinfected with are coinfected with B. microtiB. microti
► The initial symptoms of both babesiosis and Lyme The initial symptoms of both babesiosis and Lyme disease overlap significantly.disease overlap significantly.
► Like babesiosis, Lyme disease also presents with Like babesiosis, Lyme disease also presents with nonspecific symptoms of fever,fatigue, and other flu-like nonspecific symptoms of fever,fatigue, and other flu-like symptoms.symptoms.
► Patients coinfected with Patients coinfected with B. microtiB. microti and and B. burgdorferiB. burgdorferi experience more severe symptoms, but does not experience more severe symptoms, but does not increase the duration of Babesia parisitemia.increase the duration of Babesia parisitemia.
► Doxycycline will not kill Babesia. Doxycycline will not kill Babesia.

DiagnosisDiagnosis► Diagnosis is based on clinical suspicion and Diagnosis is based on clinical suspicion and history of exposure.history of exposure.► Thick and thin smears remain most clinically Thick and thin smears remain most clinically used .used .► Various PCR detection assays are available Various PCR detection assays are available for detection of for detection of B microticB microtic and other species. and other species.► Indirect fluorescent antibody test can also be Indirect fluorescent antibody test can also be used as a confirmatory test.used as a confirmatory test.► Can have false negatives (HIV) or false pos Can have false negatives (HIV) or false pos (autoimmune)(autoimmune)

TreatmentTreatment
► Current treatment is Quinine plus Clindamycin Current treatment is Quinine plus Clindamycin
► 72% receiving quinine and clindamycin had side effects 72% receiving quinine and clindamycin had side effects
attributed attributed to the drugs—diarrhea, tinnitus, or vertigo to the drugs—diarrhea, tinnitus, or vertigo
► 15% receiving atovaquone plus azithromycin 15% receiving atovaquone plus azithromycin experienced side effects (usually diarrhea or rash).experienced side effects (usually diarrhea or rash).
► For severe cases (asplenic) with high levels of For severe cases (asplenic) with high levels of parasitemia, RBC exchange transfusions may also be parasitemia, RBC exchange transfusions may also be necessary.necessary.