Embed Size (px)
Citation preview

B L E E D I N G D I S O R D E R
น ง น ช ส ร ะ ช ย น น ท
ภ า ค ว ช า ก ม า ร เ ว ช ศ า ส ต ร

O U T L I N E S
Basic knowledge
Symptoms and signs
Investigation Treatment
B A S I C H E M O S T A S I S
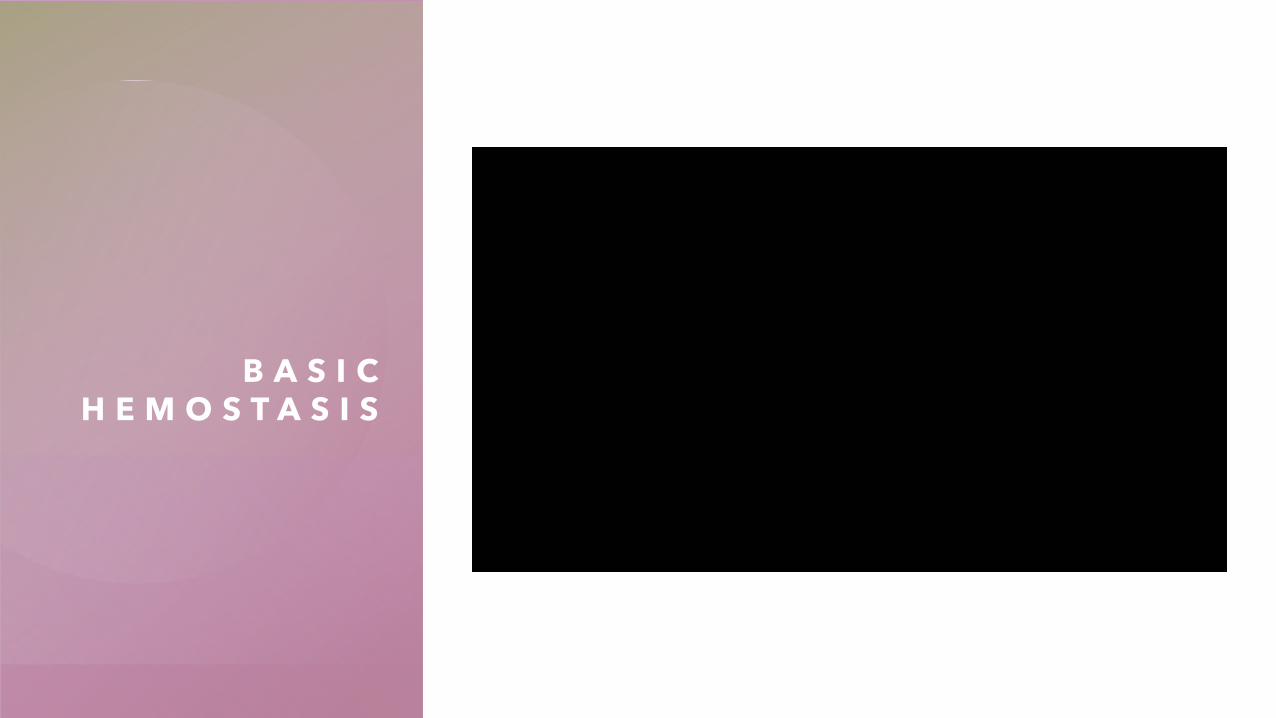
H E M O S TA S I S
TF-FVIIa
Thrombin
Fibrin
FVIII
FXIFV
FIXa
Platelet
vWF
GPIb/IX/VGPIIb/IIIa
Platelet
Platelet
Fibrin
Vascular Platelet Coagulation protein
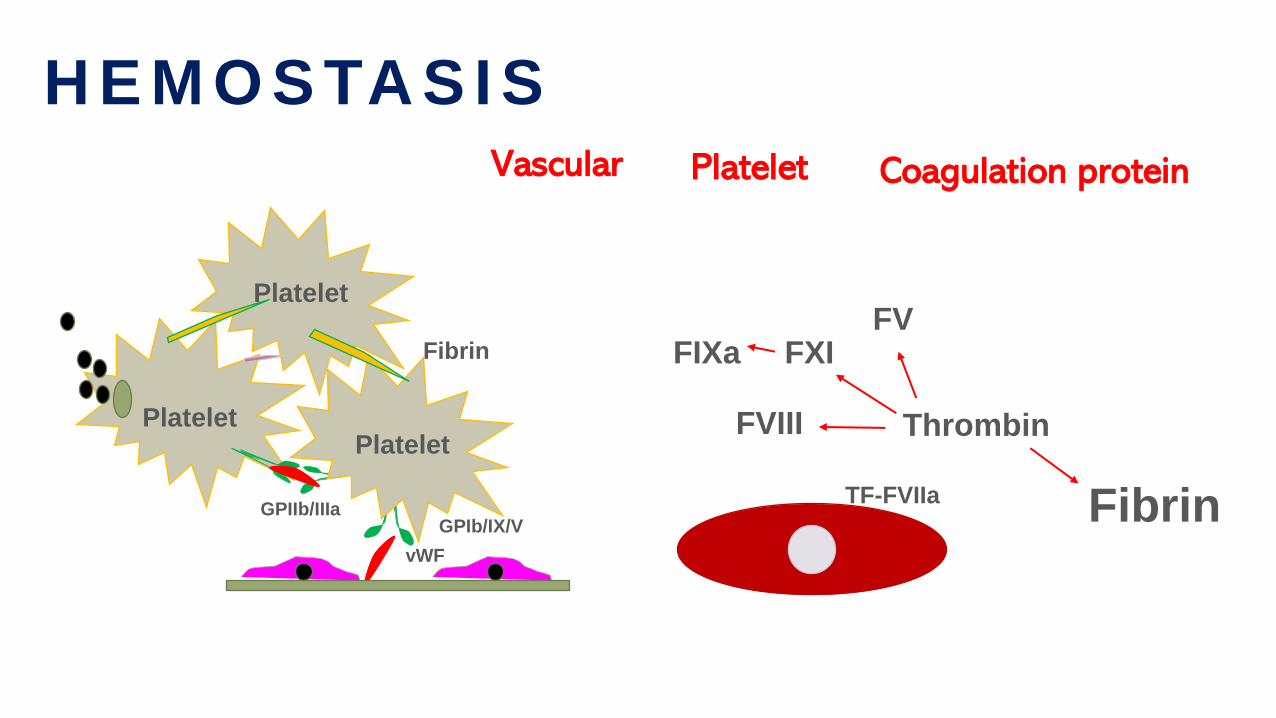
2-AntiplasminPAI-1
Plasminogen Activators
Plasminogen Activation Plasmin
Degradation
Fibrin
Degradationproducts
Fibrin strands network
-
-
H E M O S TA S I S : F I B R I N O LY S I S
D-dimer
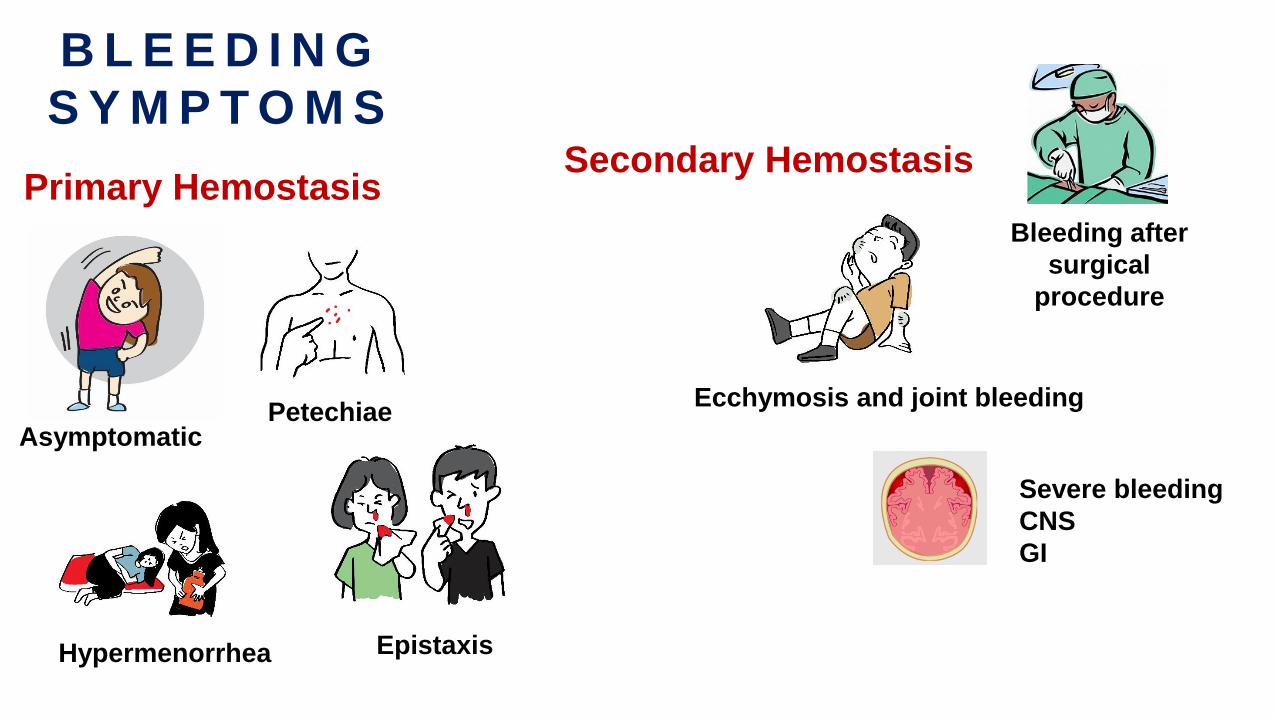
B L E E D I N G
S Y M P T O M S
Asymptomatic
Hypermenorrhea
Petechiae
Epistaxis
Ecchymosis and joint bleeding
Severe bleeding
CNS
GI
Bleeding after
surgical
procedure
Primary HemostasisSecondary Hemostasis
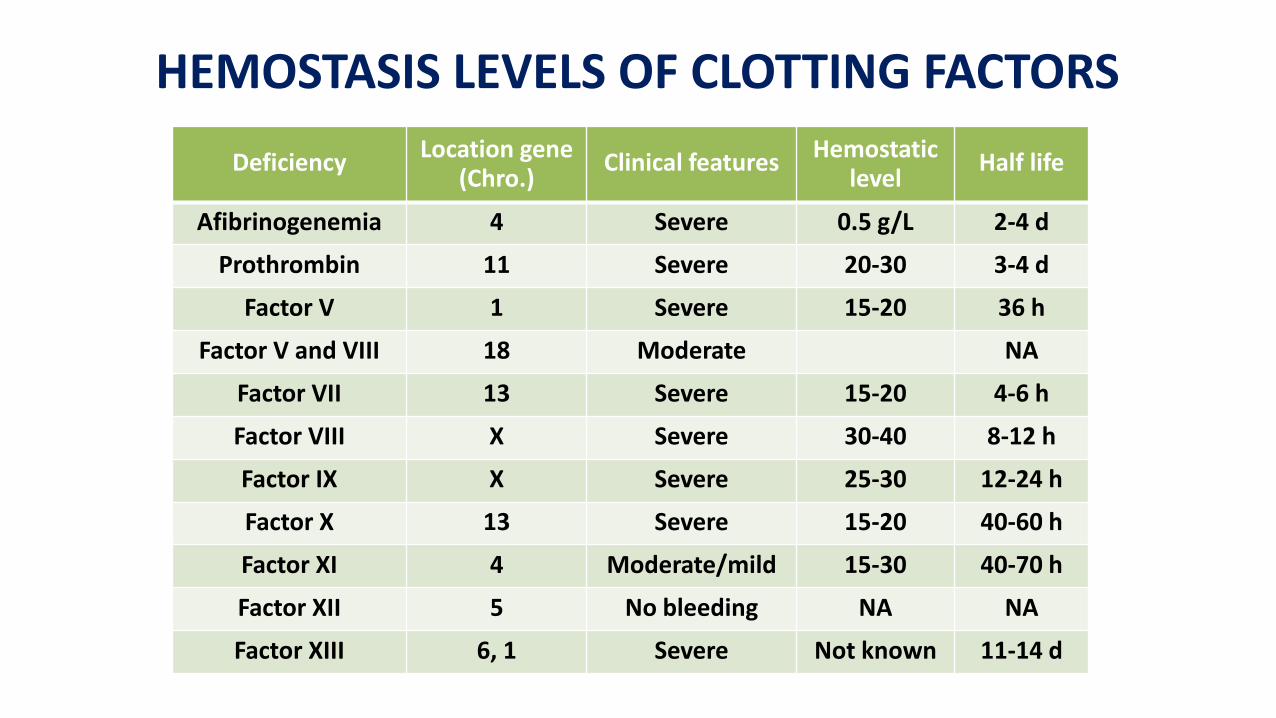
HEMOSTASIS LEVELS OF CLOTTING FACTORS
DeficiencyLocation gene
(Chro.)Clinical features
Hemostaticlevel
Half life
Afibrinogenemia 4 Severe 0.5 g/L 2-4 d
Prothrombin 11 Severe 20-30 3-4 d
Factor V 1 Severe 15-20 36 h
Factor V and VIII 18 Moderate NA
Factor VII 13 Severe 15-20 4-6 h
Factor VIII X Severe 30-40 8-12 h
Factor IX X Severe 25-30 12-24 h
Factor X 13 Severe 15-20 40-60 h
Factor XI 4 Moderate/mild 15-30 40-70 h
Factor XII 5 No bleeding NA NA
Factor XIII 6, 1 Severe Not known 11-14 d
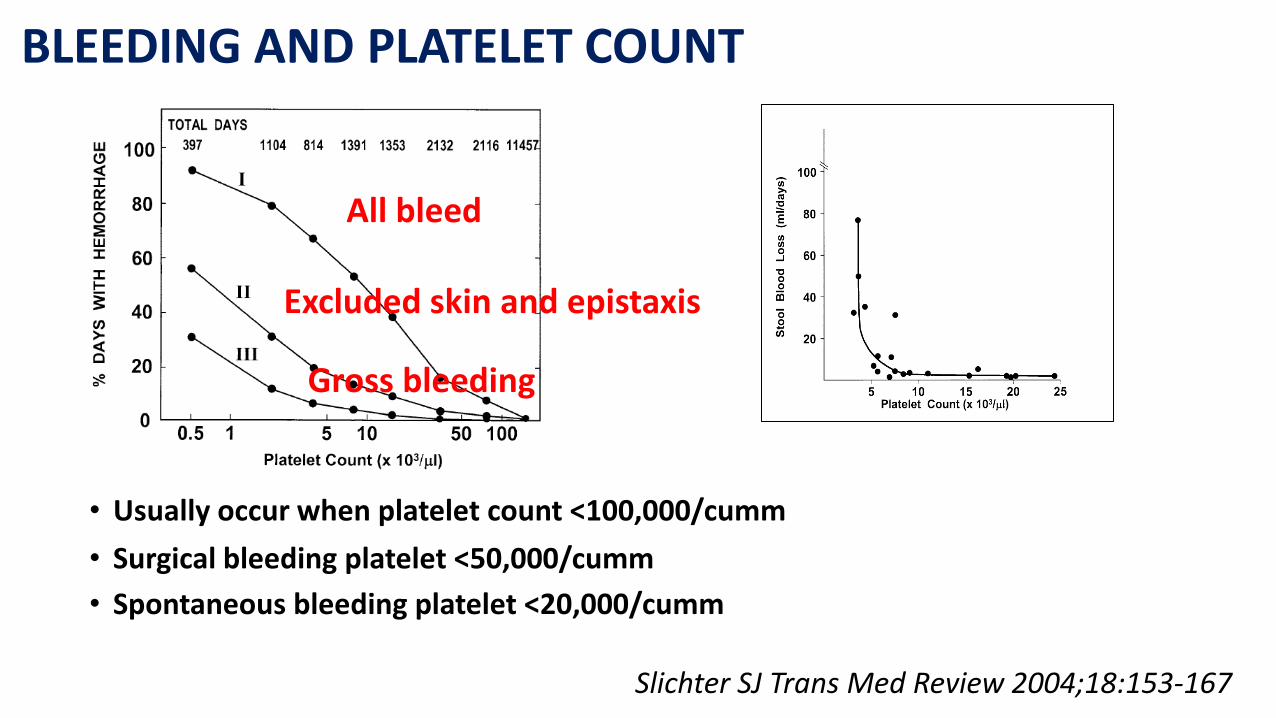
BLEEDING AND PLATELET COUNT
• Usually occur when platelet count <100,000/cumm
• Surgical bleeding platelet <50,000/cumm
• Spontaneous bleeding platelet <20,000/cumm
Slichter SJ Trans Med Review 2004;18:153-167
All bleed
Excluded skin and epistaxis
Gross bleeding
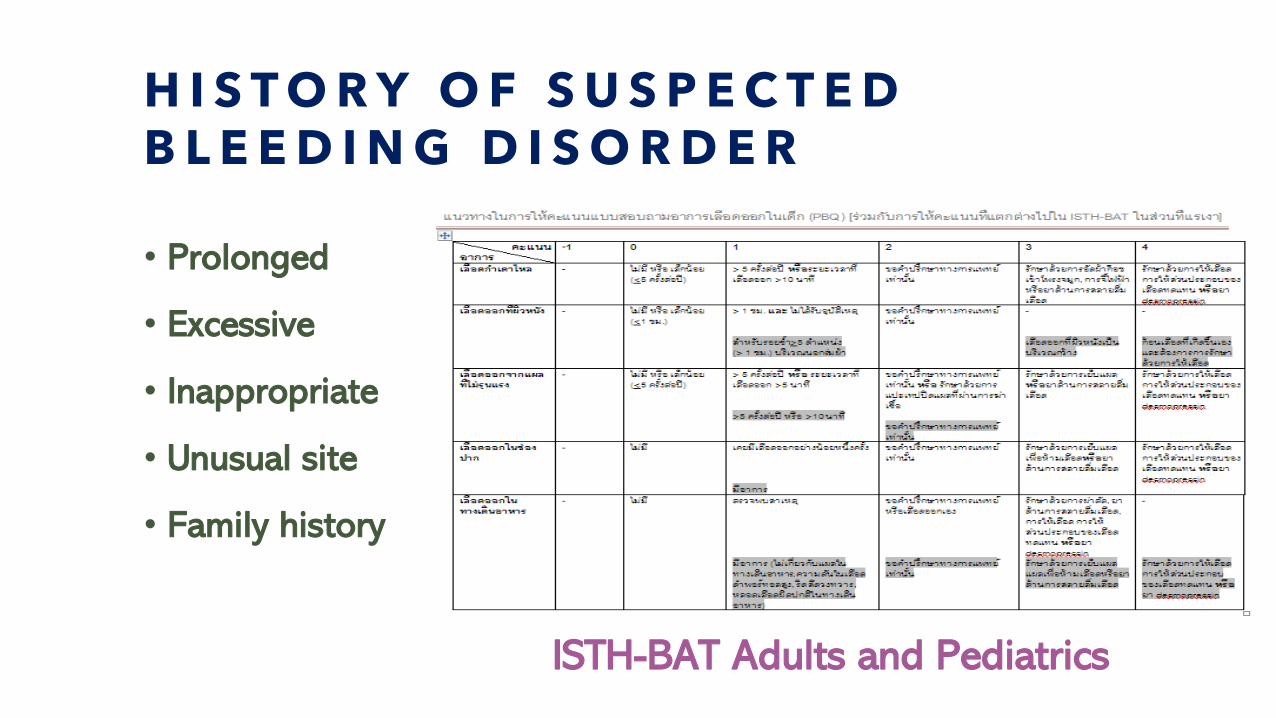
H I S T O R Y O F S U S P E C T E D B L E E D I N G D I S O R D E R
• Prolonged
• Excessive
• Inappropriate
• Unusual site
• Family history
ISTH-BAT Adults and Pediatrics
Q U E S T I O N 1
• Which of the following is the symptoms of platelet
disorder?
A. Muscle bleeding
B. Hemarthrosis
C. Large ecchymosis
D. Epistaxis
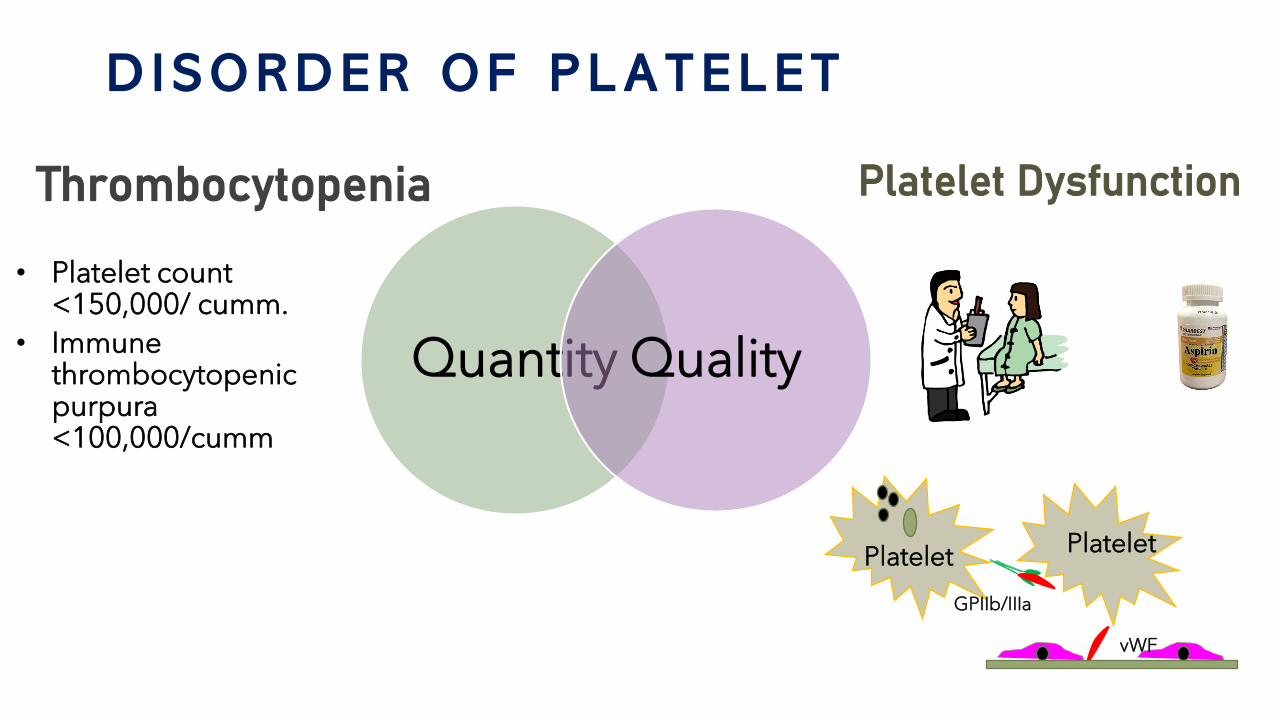
D I S O R D E R O F P L A T E L E T
Quantity Quality
• Platelet count <150,000/ cumm.
• Immune thrombocytopenic purpura <100,000/cumm
Thrombocytopenia Platelet Dysfunction
Platelet
vWF
GPIIb/IIIa
Platelet
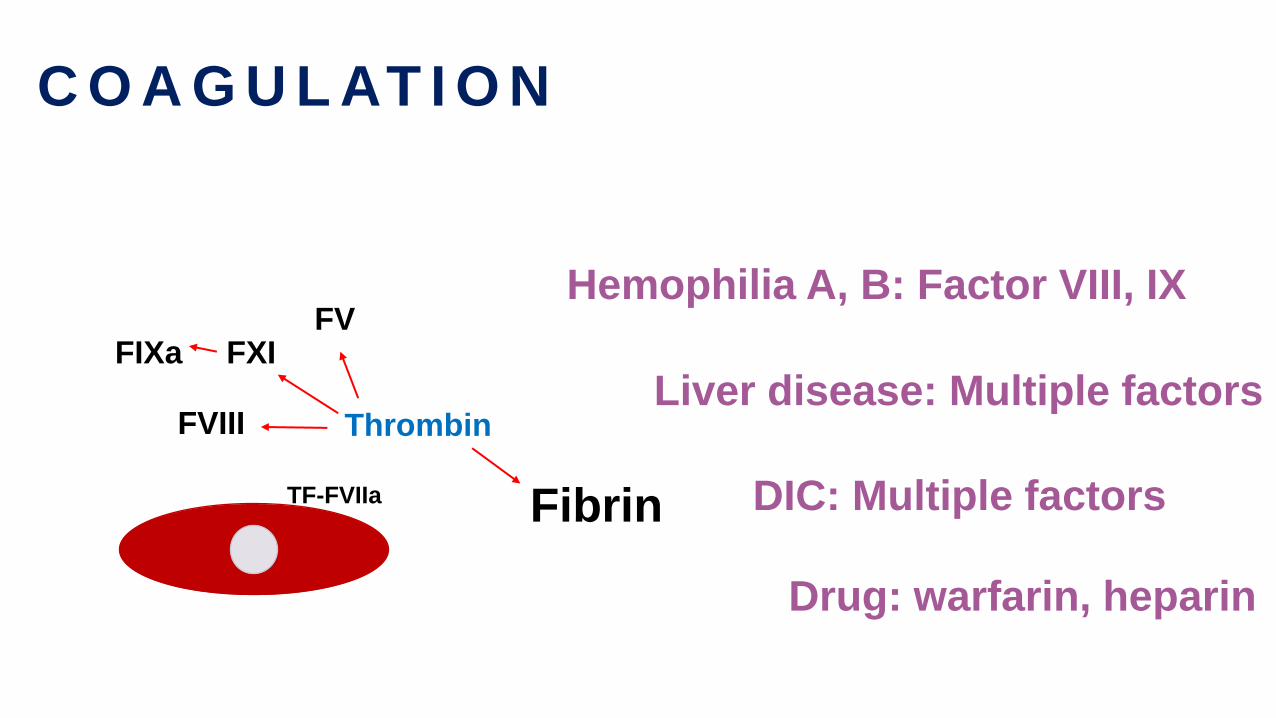
C O A G U L AT I O N
TF-FVIIa
Thrombin
Fibrin
FVIII
FXIFV
FIXa
Hemophilia A, B: Factor VIII, IX
Liver disease: Multiple factors
DIC: Multiple factors
Drug: warfarin, heparin
L A B O R A T O R Y T E S T I N H E M O S TA S I S
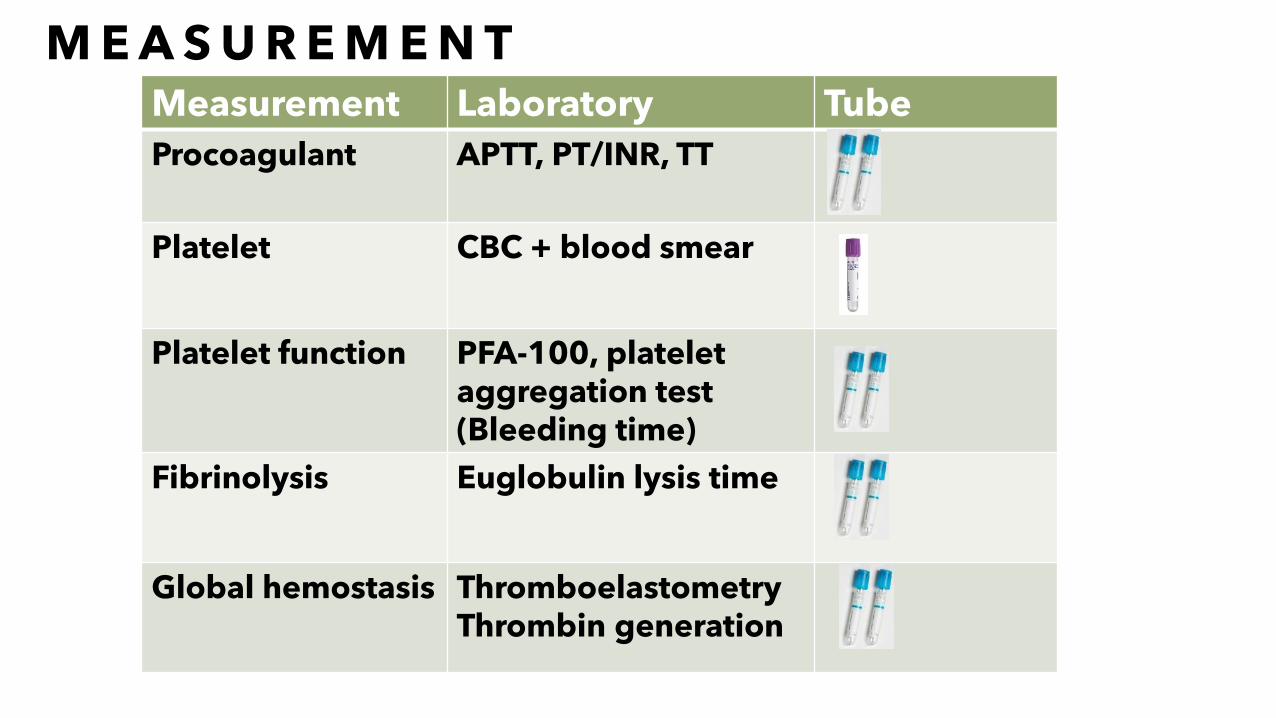
M E A S U R E M E N TMeasurement Laboratory Tube
Procoagulant APTT, PT/INR, TT
Platelet CBC + blood smear
Platelet function PFA-100, platelet aggregation test(Bleeding time)
Fibrinolysis Euglobulin lysis time
Global hemostasis ThromboelastometryThrombin generation
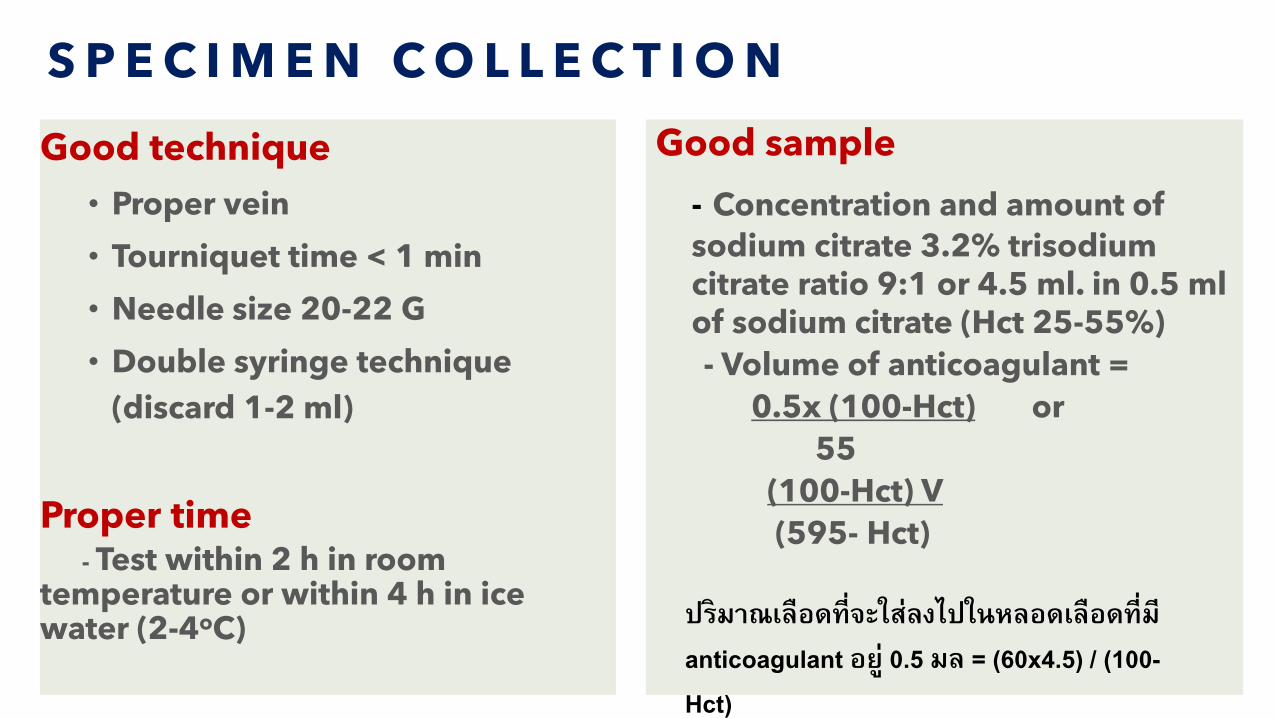
S P E C I M E N C O L L E C T I O N
Good technique
• Proper vein
• Tourniquet time < 1 min
• Needle size 20-22 G
• Double syringe technique
(discard 1-2 ml)
Proper time- Test within 2 h in room
temperature or within 4 h in ice water (2-4oC)
Good sample
- Concentration and amount of
sodium citrate 3.2% trisodiumcitrate ratio 9:1 or 4.5 ml. in 0.5 ml of sodium citrate (Hct 25-55%)
- Volume of anticoagulant =
0.5x (100-Hct) or
55
(100-Hct) V
(595- Hct)
ปรมาณเลอดทจะใสลงไปในหลอดเลอดทม anticoagulant อย 0.5 มล = (60x4.5) / (100-Hct)
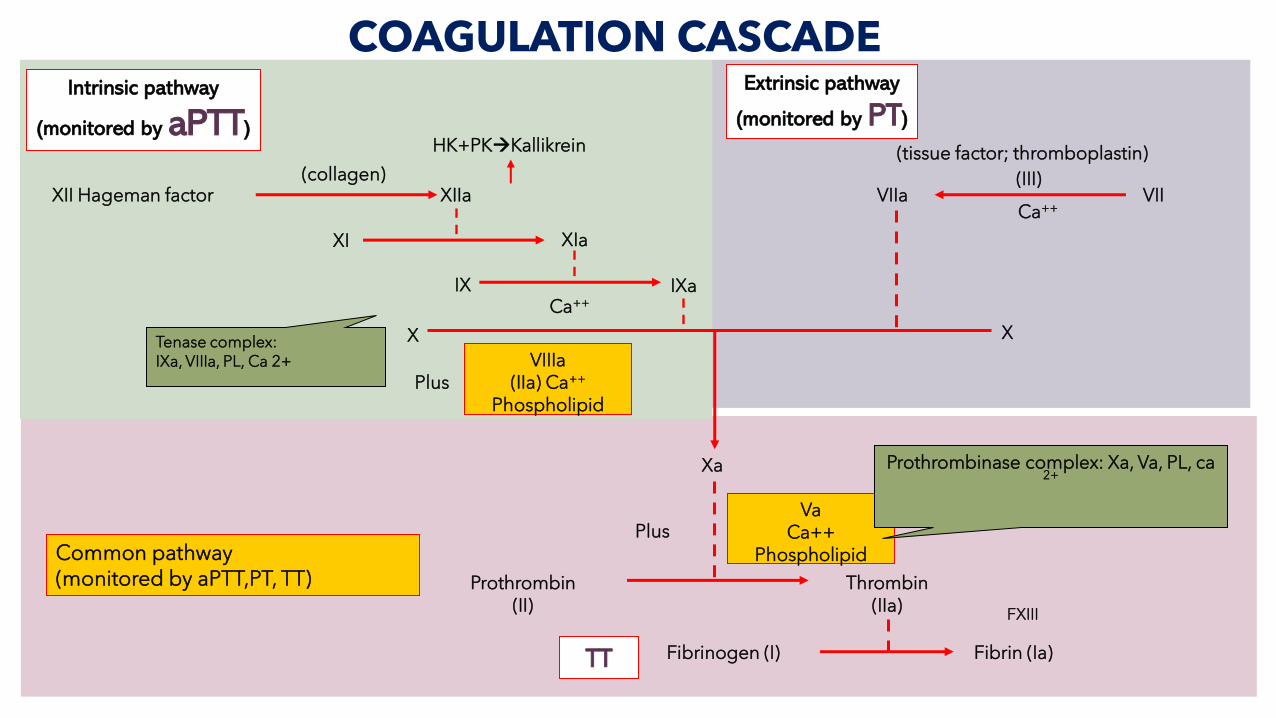
Extrinsic pathway
(monitored by PT)
(tissue factor; thromboplastin)
VIIa VII(III)
Ca++
X
Xa
VaCa++
Phospholipid
Plus
Prothrombin(II)
Thrombin(IIa)
Fibrinogen (I) Fibrin (Ia)
Common pathway(monitored by aPTT,PT, TT)
COAGULATION CASCADEIntrinsic pathway
(monitored by aPTT)
XII Hageman factor(collagen)
XIIa
XI XIa
IX IXa
X
Ca++
VIIIa(IIa) Ca++
PhospholipidPlus
FXIII
Prothrombinase complex: Xa, Va, PL, ca 2+
Tenase complex: IXa, VIIIa, PL, Ca 2+
HK+PK→Kallikrein
TT
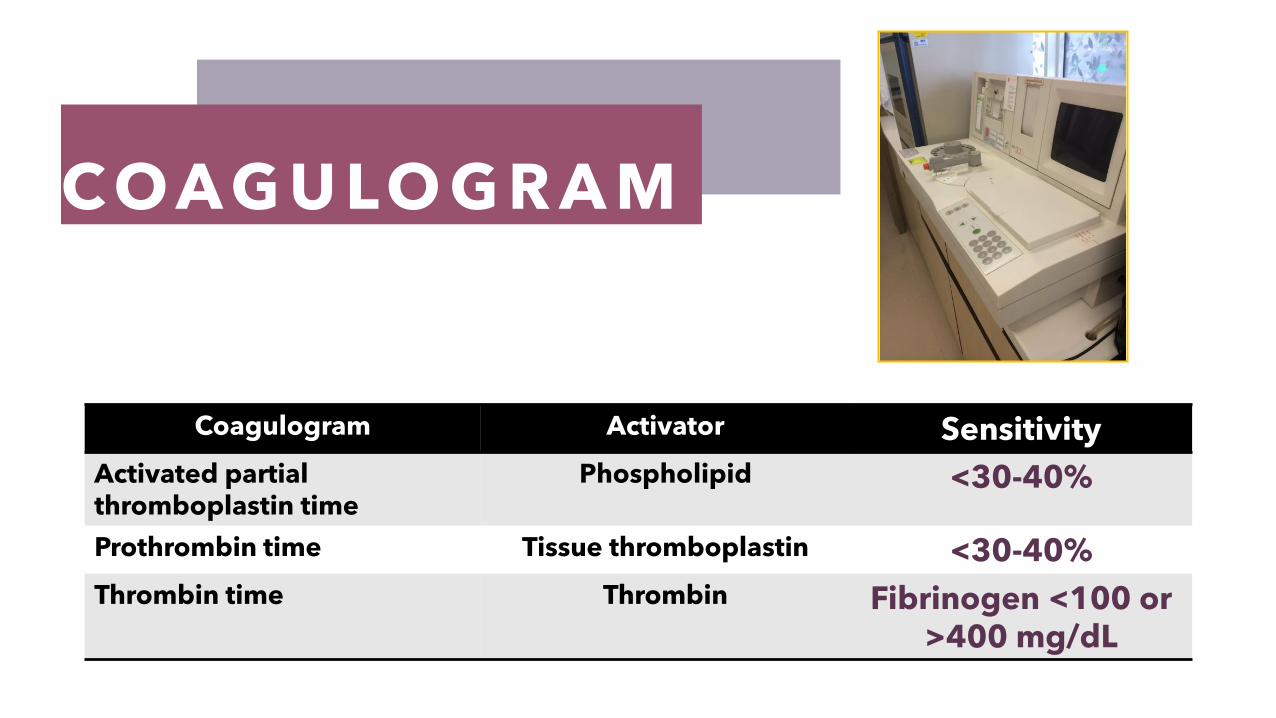
C OA G U LO G R A M
Coagulogram Activator Sensitivity
Activated partial thromboplastin time
Phospholipid <30-40%
Prothrombin time Tissue thromboplastin <30-40%
Thrombin time Thrombin Fibrinogen <100 or >400 mg/dL
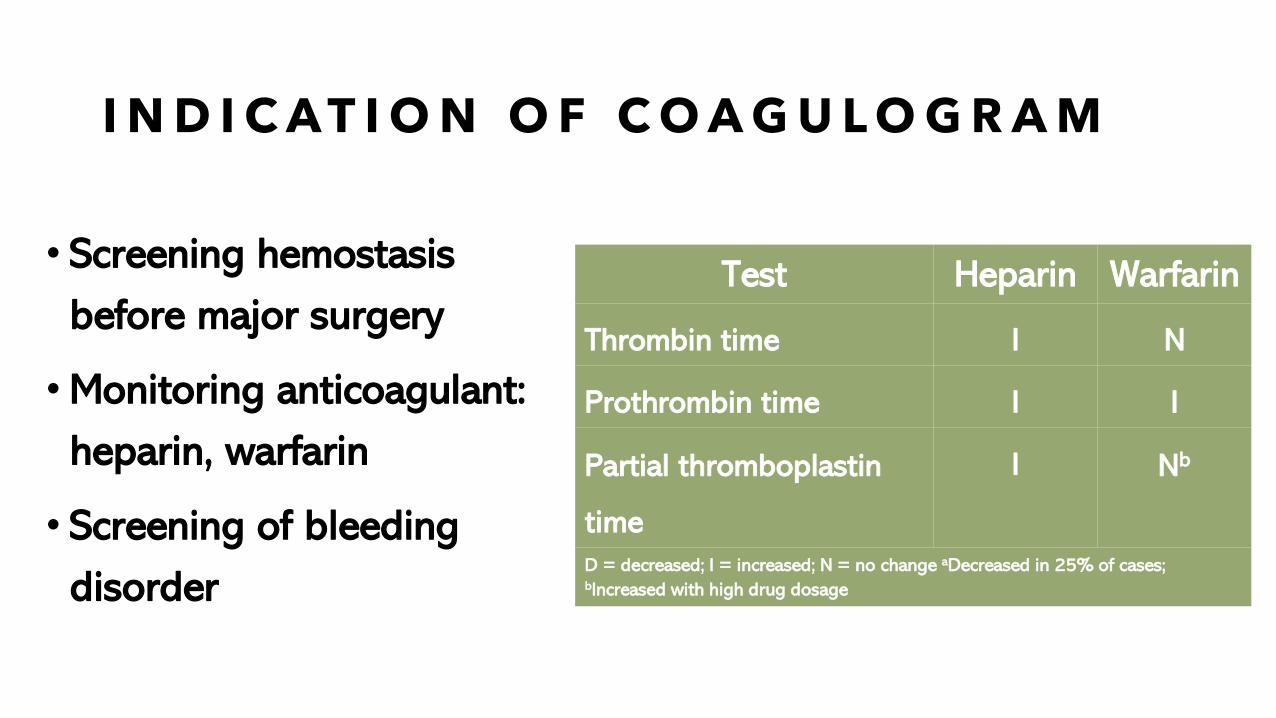
I N D I C A T I O N O F C O A G U L O G R A M
• Screening hemostasis
before major surgery
•Monitoring anticoagulant:
heparin, warfarin
• Screening of bleeding
disorder
Test Heparin Warfarin
Thrombin time I N
Prothrombin time I I
Partial thromboplastin
time
I Nb
D = decreased; I = increased; N = no change aDecreased in 25% of cases; bIncreased with high drug dosage
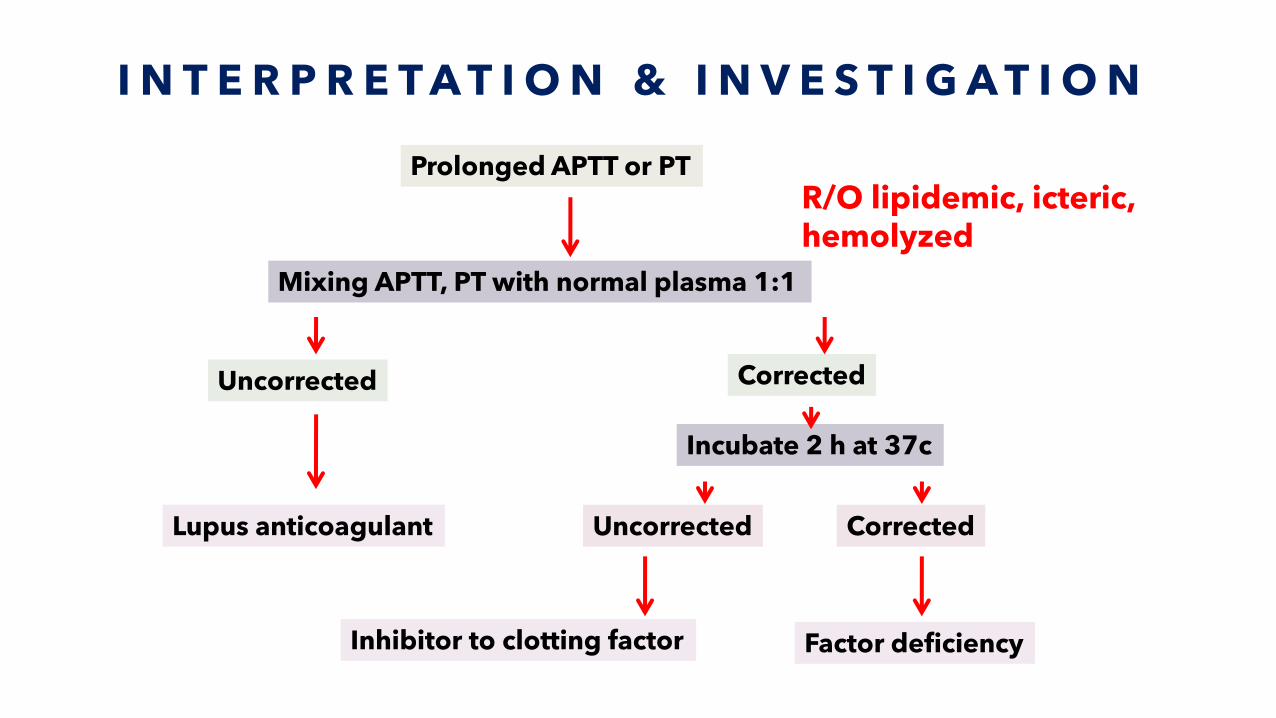
I N T E R P R E T A T I O N & I N V E S T I G A T I O N
Prolonged APTT or PT
Mixing APTT, PT with normal plasma 1:1
Uncorrected
Lupus anticoagulant
Corrected
Incubate 2 h at 37c
Uncorrected
Inhibitor to clotting factor
Corrected
Factor deficiency
R/O lipidemic, icteric, hemolyzed
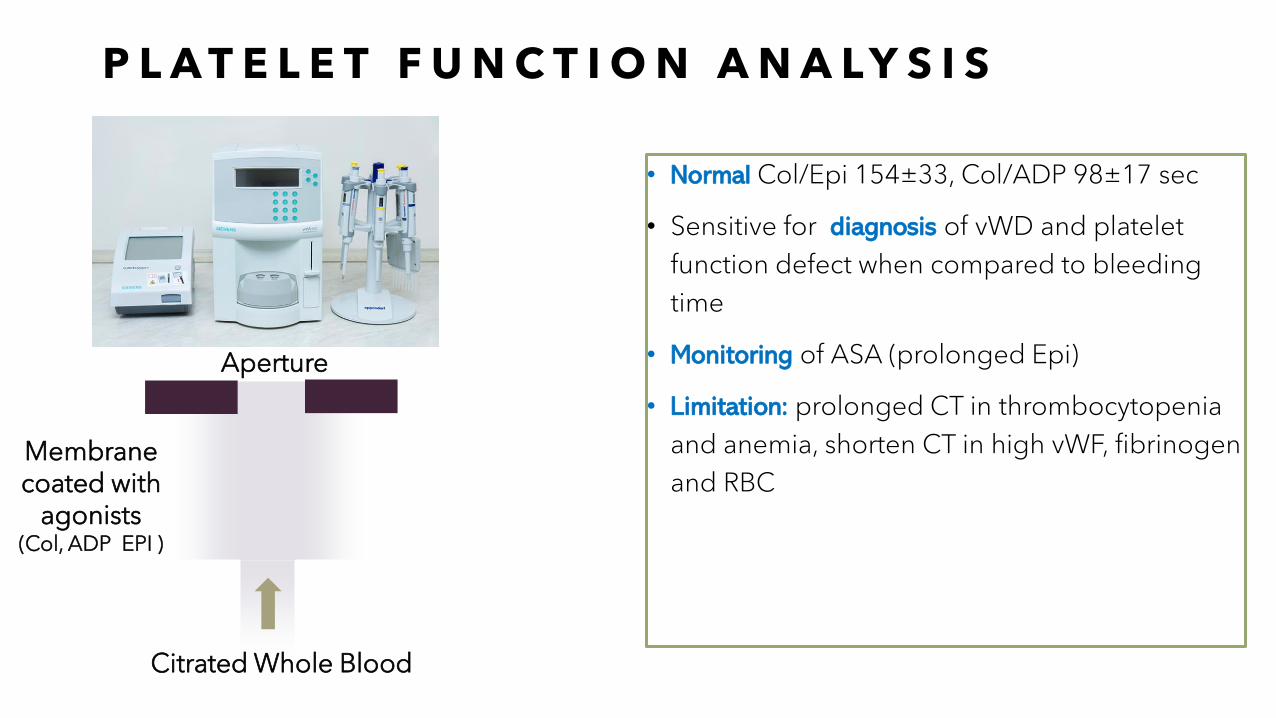
P L A T E L E T F U N C T I O N A N A L Y S I S
• Normal Col/Epi 154±33, Col/ADP 98±17 sec
• Sensitive for diagnosis of vWD and platelet
function defect when compared to bleeding
time
• Monitoring of ASA (prolonged Epi)
• Limitation: prolonged CT in thrombocytopenia
and anemia, shorten CT in high vWF, fibrinogen
and RBCMembranecoated with
agonists(Col, ADP EPI )
Citrated Whole Blood
Aperture
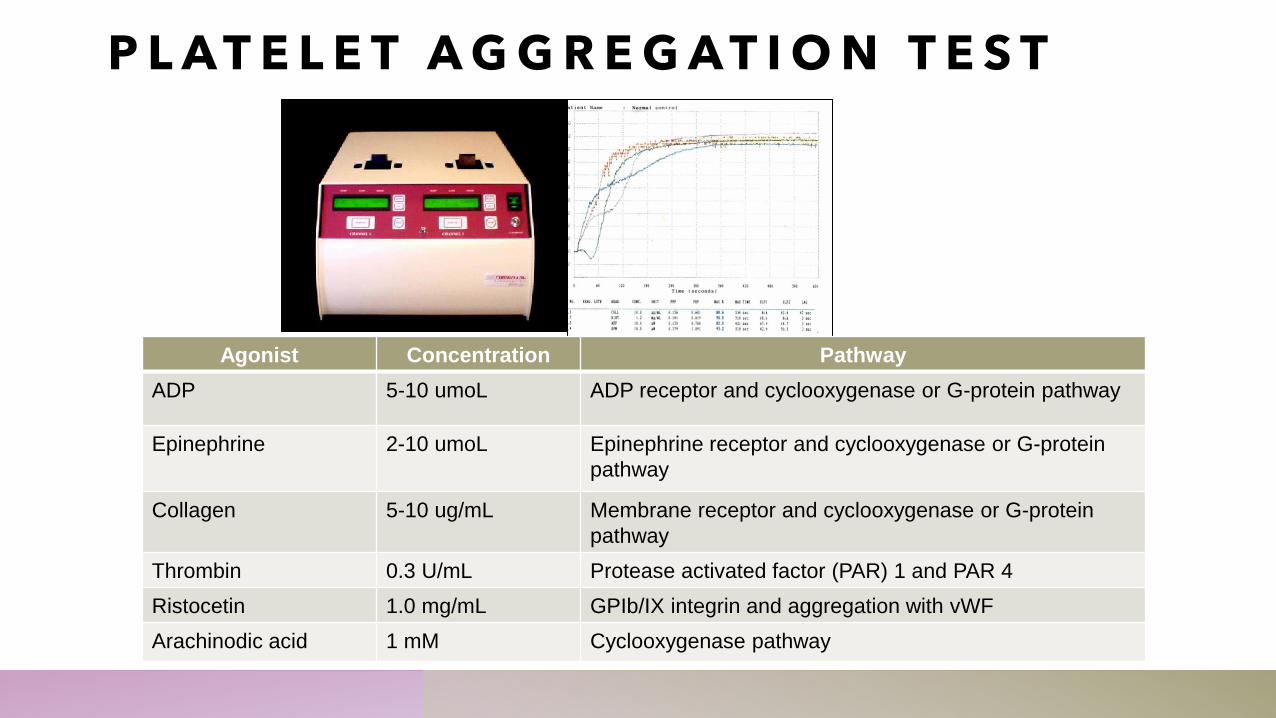
Agonist Concentration Pathway
ADP 5-10 umoL ADP receptor and cyclooxygenase or G-protein pathway
Epinephrine 2-10 umoL Epinephrine receptor and cyclooxygenase or G-protein
pathway
Collagen 5-10 ug/mL Membrane receptor and cyclooxygenase or G-protein
pathway
Thrombin 0.3 U/mL Protease activated factor (PAR) 1 and PAR 4
Ristocetin 1.0 mg/mL GPIb/IX integrin and aggregation with vWF
Arachinodic acid 1 mM Cyclooxygenase pathway
P L A T E L E T A G G R E G A T I O N T E S T
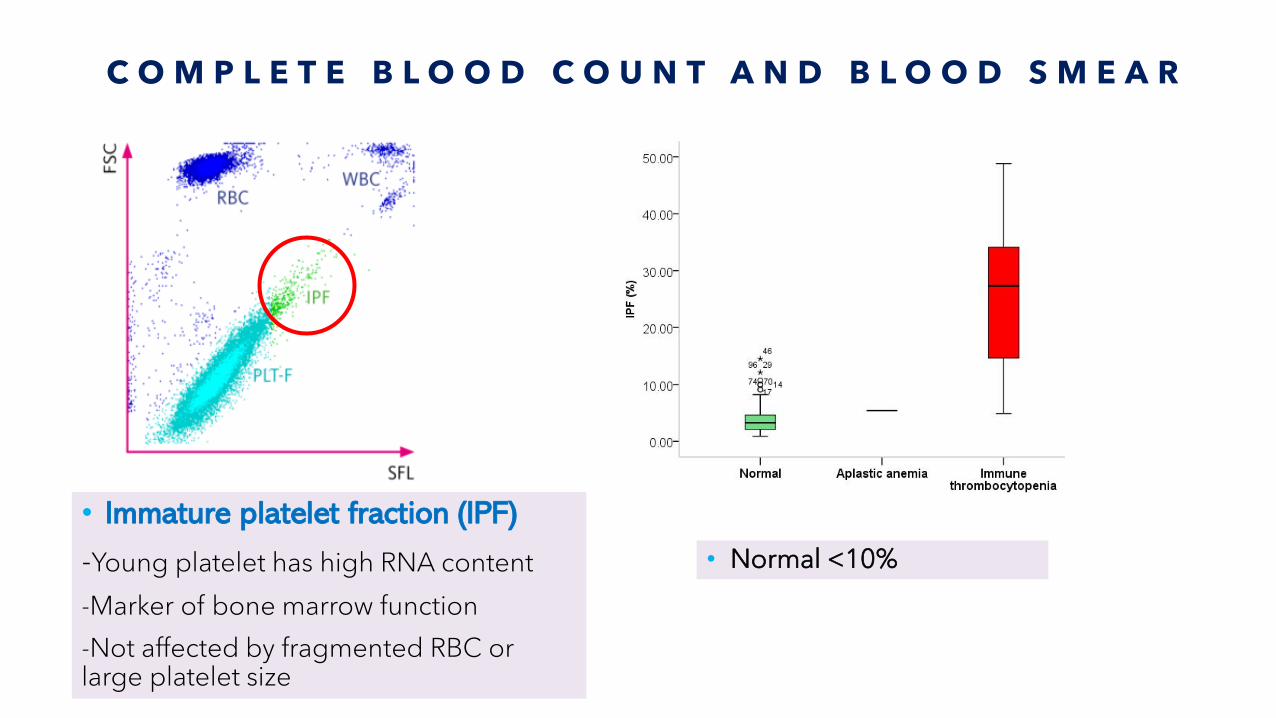
C O M P L E T E B L O O D C O U N T A N D B L O O D S M E A R
• Immature platelet fraction (IPF)
-Young platelet has high RNA content
-Marker of bone marrow function
-Not affected by fragmented RBC or large platelet size
• Normal <10%
G LO B A L H E M O S TA S I S T E S T S
-Thromboelastometry
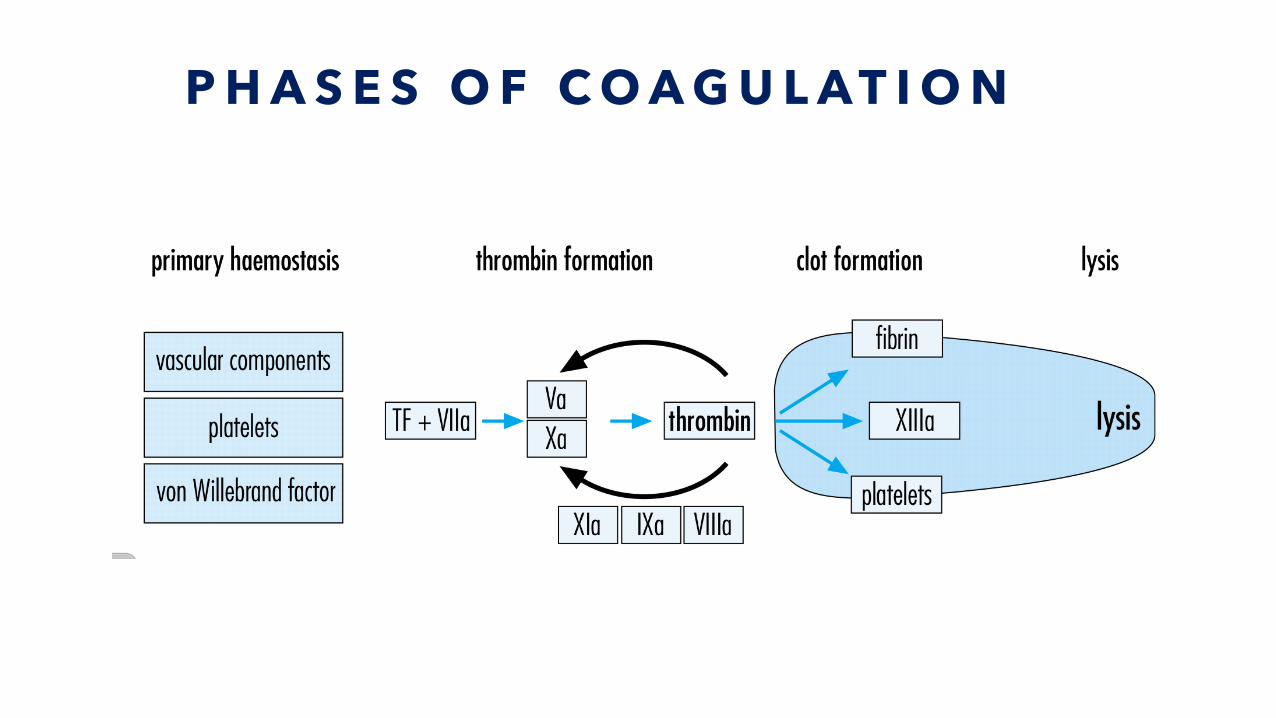
P H A S E S O F C O A G U L A T I O N
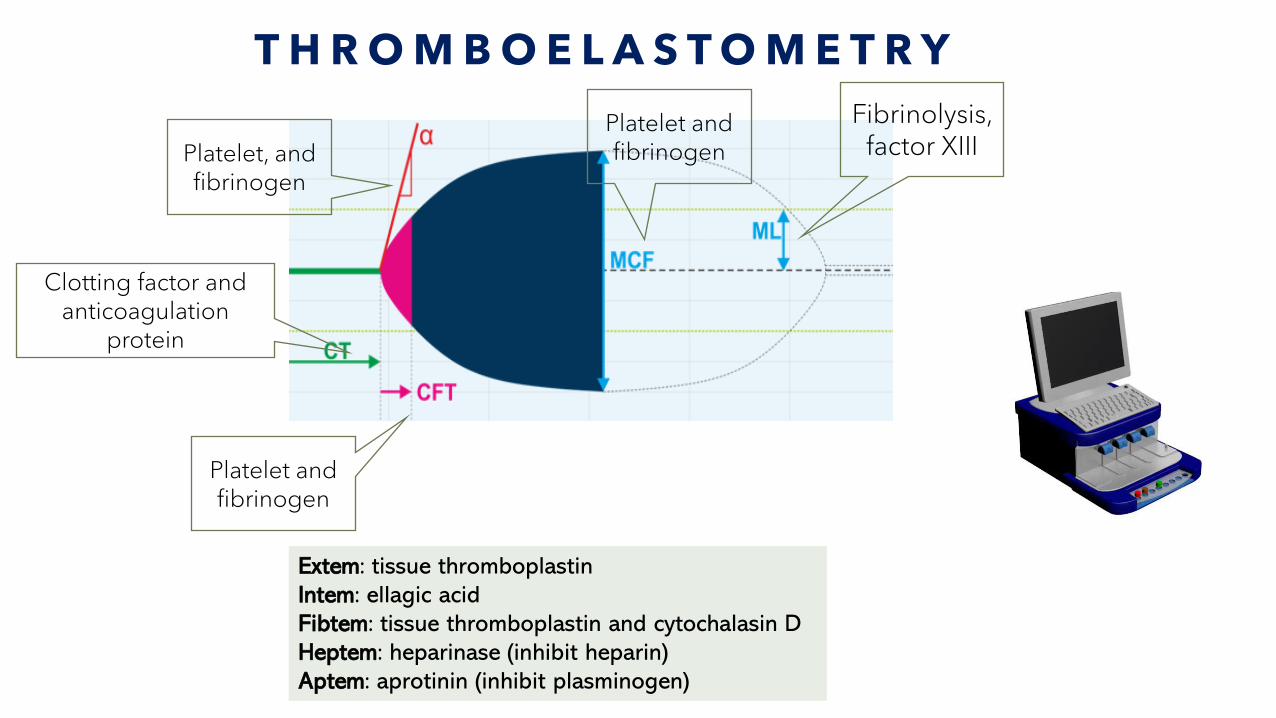
T H R O M B O E L A S T O M E T R Y
Extem: tissue thromboplastin
Intem: ellagic acid
Fibtem: tissue thromboplastin and cytochalasin D
Heptem: heparinase (inhibit heparin)
Aptem: aprotinin (inhibit plasminogen)
Clotting factor and anticoagulation
protein
Platelet and fibrinogen
Platelet, and fibrinogen
Platelet and fibrinogen
Fibrinolysis, factor XIII
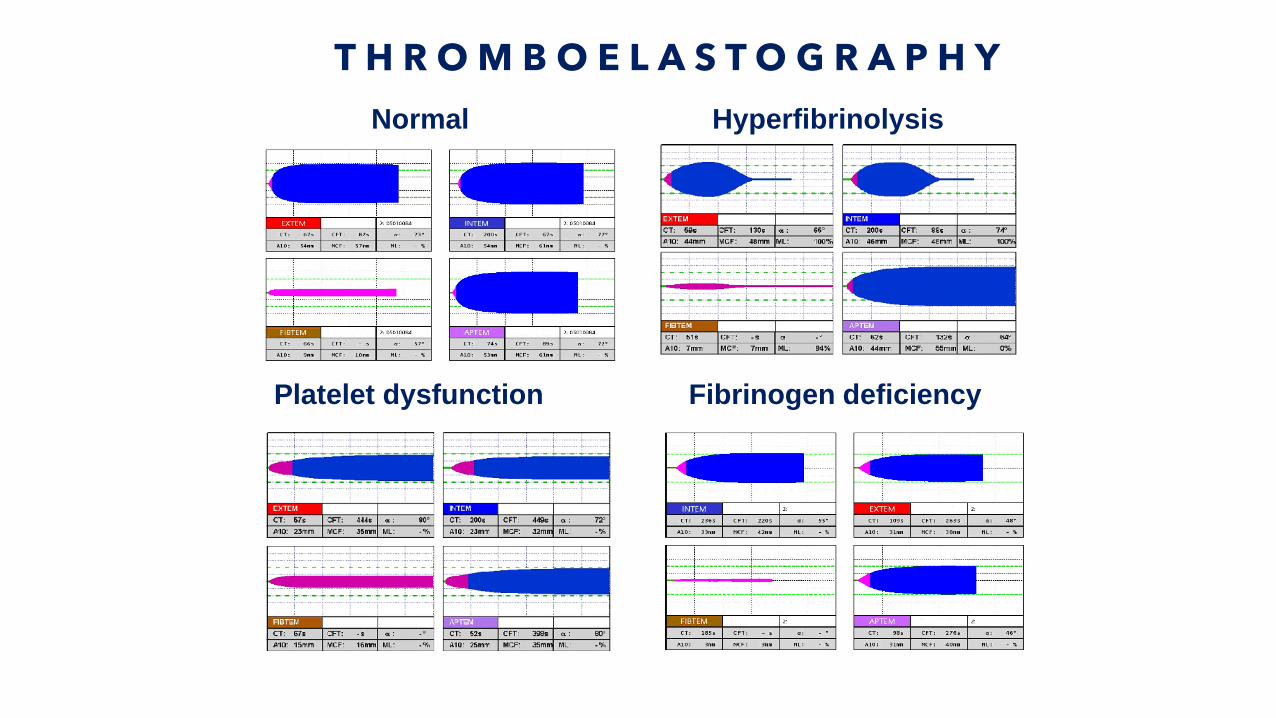
T H R O M B O E L A S T O G R A P H Y
Normal Hyperfibrinolysis
Fibrinogen deficiency Platelet dysfunction
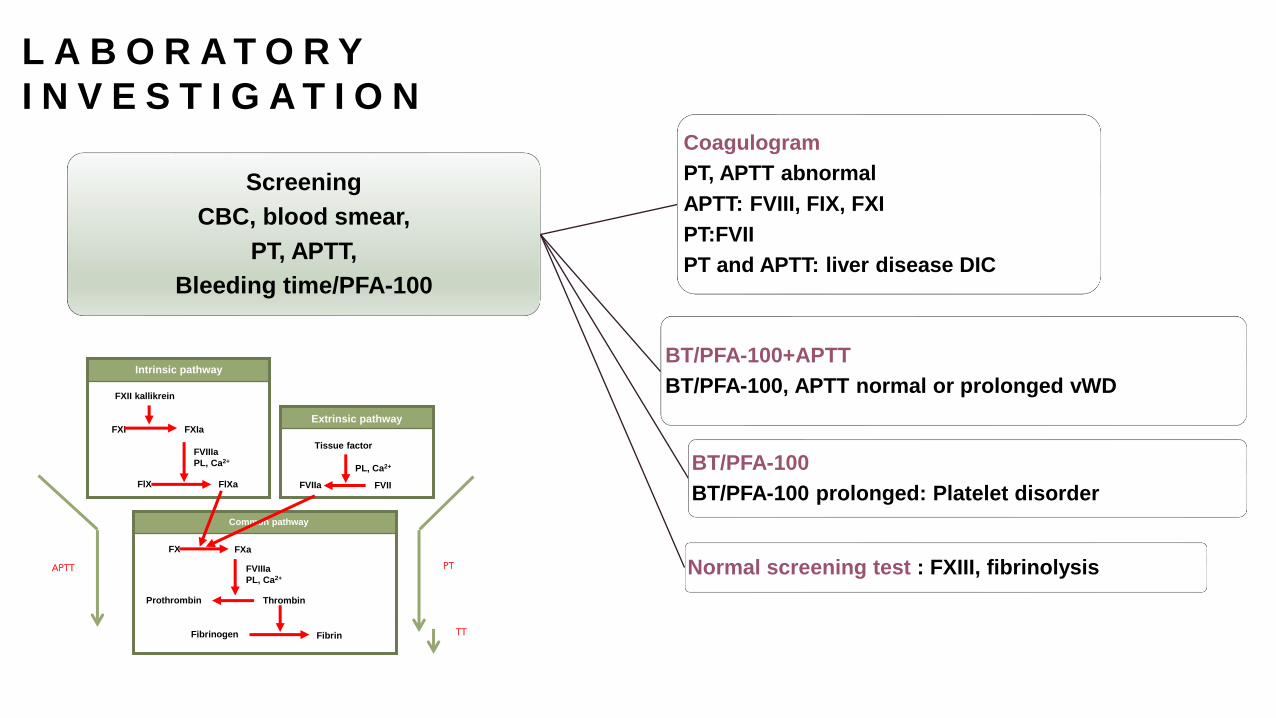
L A B O R A T O R Y
I N V E S T I G A T I O N
Screening
CBC, blood smear,
PT, APTT,
Bleeding time/PFA-100
Coagulogram
PT, APTT abnormal
APTT: FVIII, FIX, FXI
PT:FVII
PT and APTT: liver disease DIC
BT/PFA-100+APTT
BT/PFA-100, APTT normal or prolonged vWD
BT/PFA-100
BT/PFA-100 prolonged: Platelet disorder
Normal screening test : FXIII, fibrinolysis
FXII kallikrein
FXI FXIa
FVIIIa
PL, Ca2+
FlX FlXa
Intrinsic pathway
Tissue factor
PL, Ca2+
FVIIa FVII
Extrinsic pathway
FX
Prothrombin Thrombin
Common pathway
FXa
FVIIIa
PL, Ca2+
Fibrinogen Fibrin
APTT PT
TT
Q U E S T I O N 2
• Which of the following screening test is abnormal in hemophilia?
A. APTT
B. PT
C. TT
D. APTT and PT
E. APTT, PT and TT
C O M M O N P L A T E L E T D I S E A S E S
•Thrombocytopenia• Congenital
• Acquired
• Dysfunction
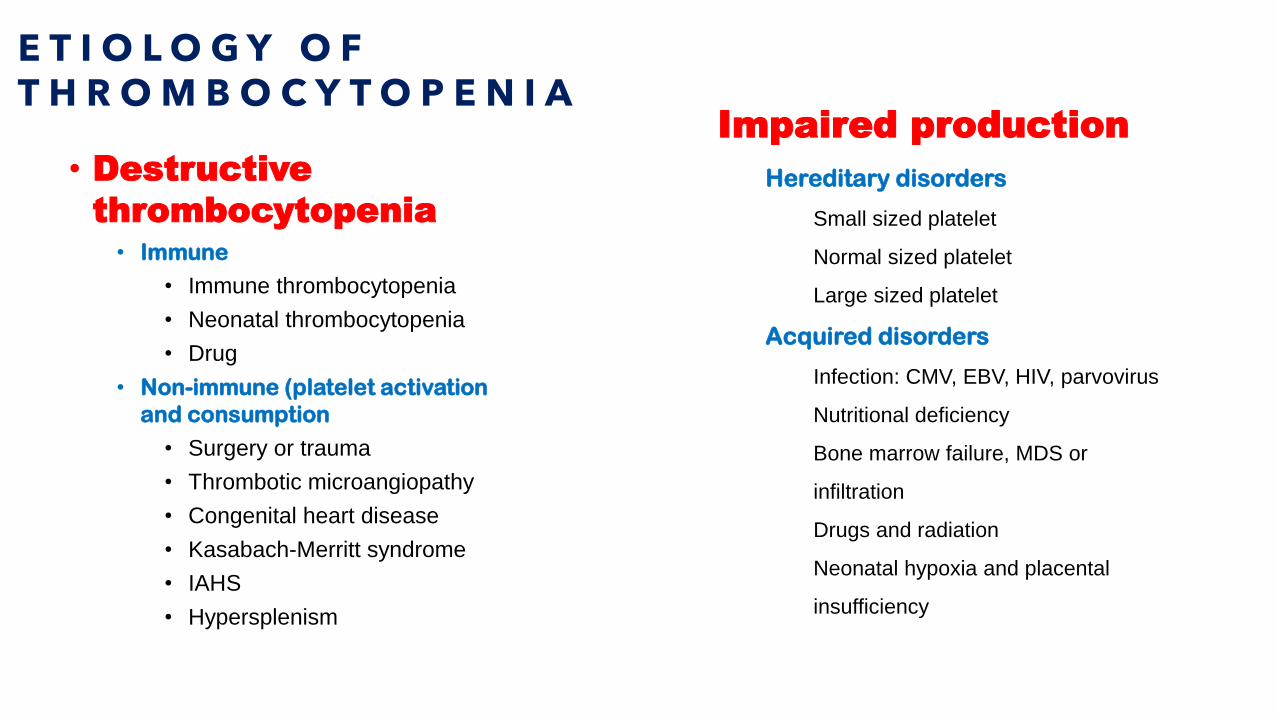
E T I O L O G Y O F T H R O M B O C Y T O P E N I A
• Destructive
thrombocytopenia• Immune
• Immune thrombocytopenia
• Neonatal thrombocytopenia
• Drug
• Non-immune (platelet activation
and consumption
• Surgery or trauma
• Thrombotic microangiopathy
• Congenital heart disease
• Kasabach-Merritt syndrome
• IAHS
• Hypersplenism
Impaired production
Hereditary disorders
Small sized platelet
Normal sized platelet
Large sized platelet
Acquired disorders
Infection: CMV, EBV, HIV, parvovirus
Nutritional deficiency
Bone marrow failure, MDS or
infiltration
Drugs and radiation
Neonatal hypoxia and placental
insufficiency
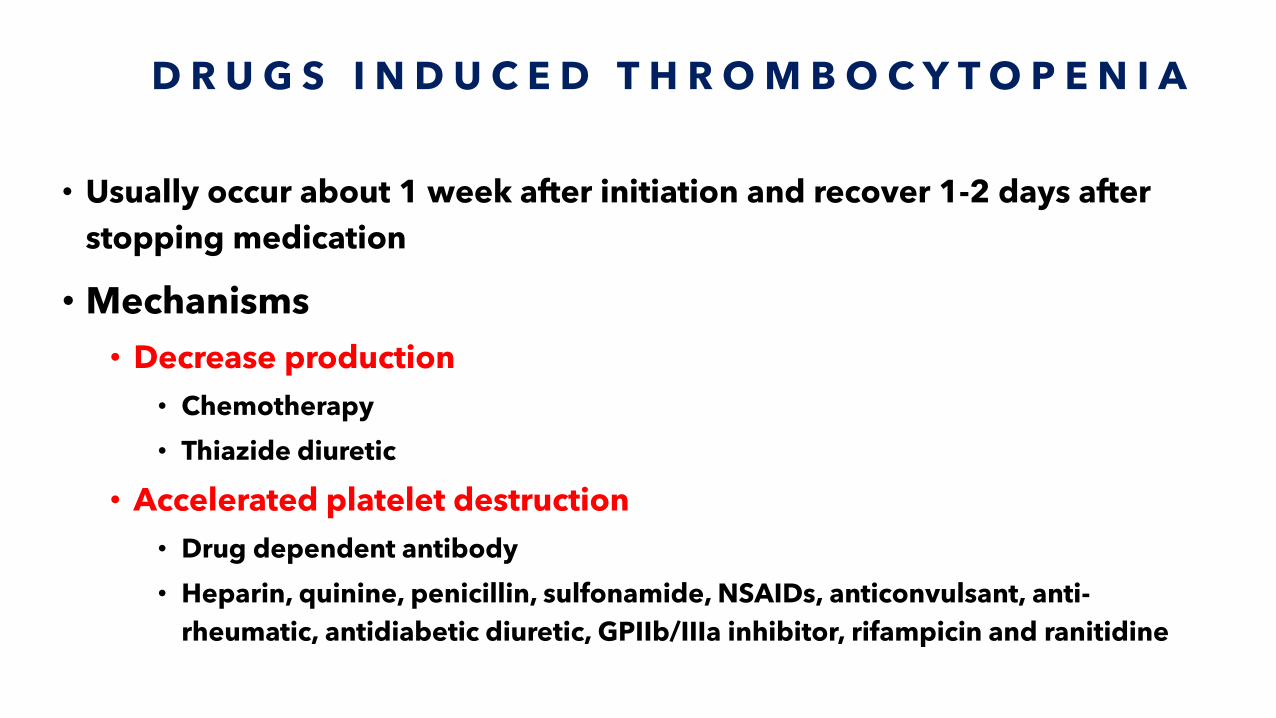
D R U G S I N D U C E D T H R O M B O C Y T O P E N I A
• Usually occur about 1 week after initiation and recover 1-2 days after
stopping medication
• Mechanisms
• Decrease production
• Chemotherapy
• Thiazide diuretic
• Accelerated platelet destruction
• Drug dependent antibody
• Heparin, quinine, penicillin, sulfonamide, NSAIDs, anticonvulsant, anti-
rheumatic, antidiabetic diuretic, GPIIb/IIIa inhibitor, rifampicin and ranitidine
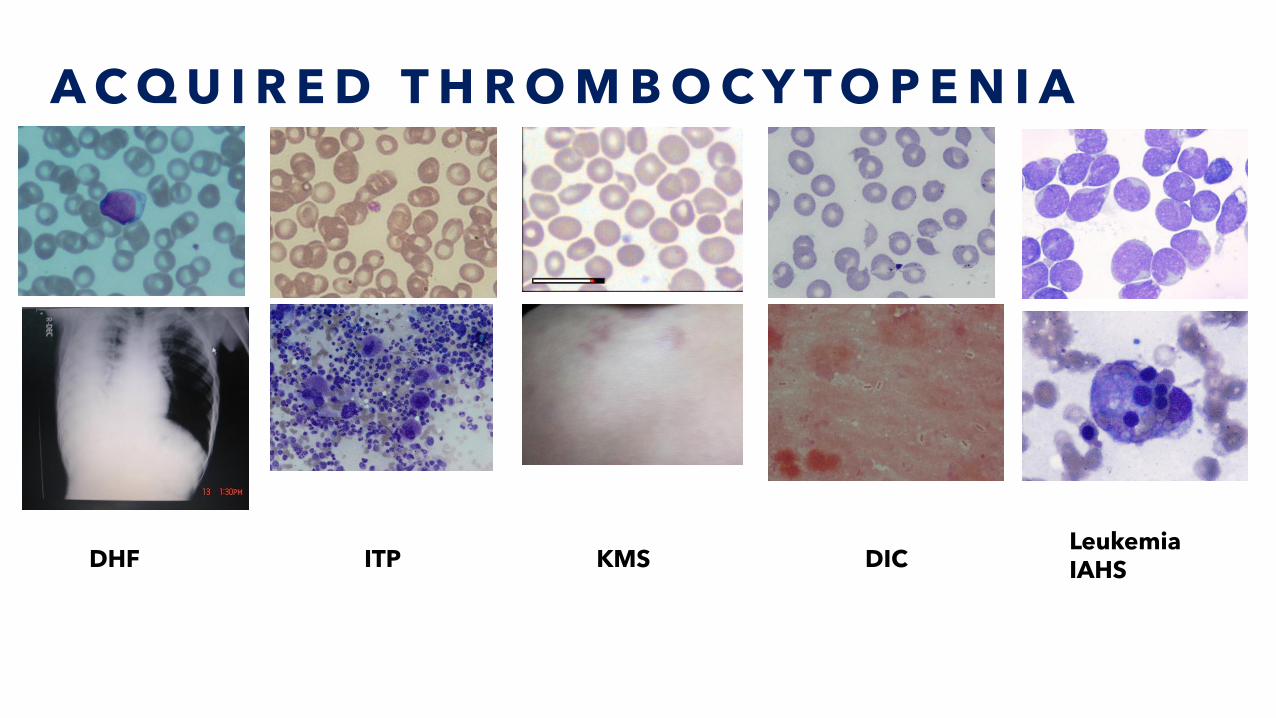
A C Q U I R E D T H R O M B O C Y T O P E N I A
DHF ITP KMS DICLeukemiaIAHS
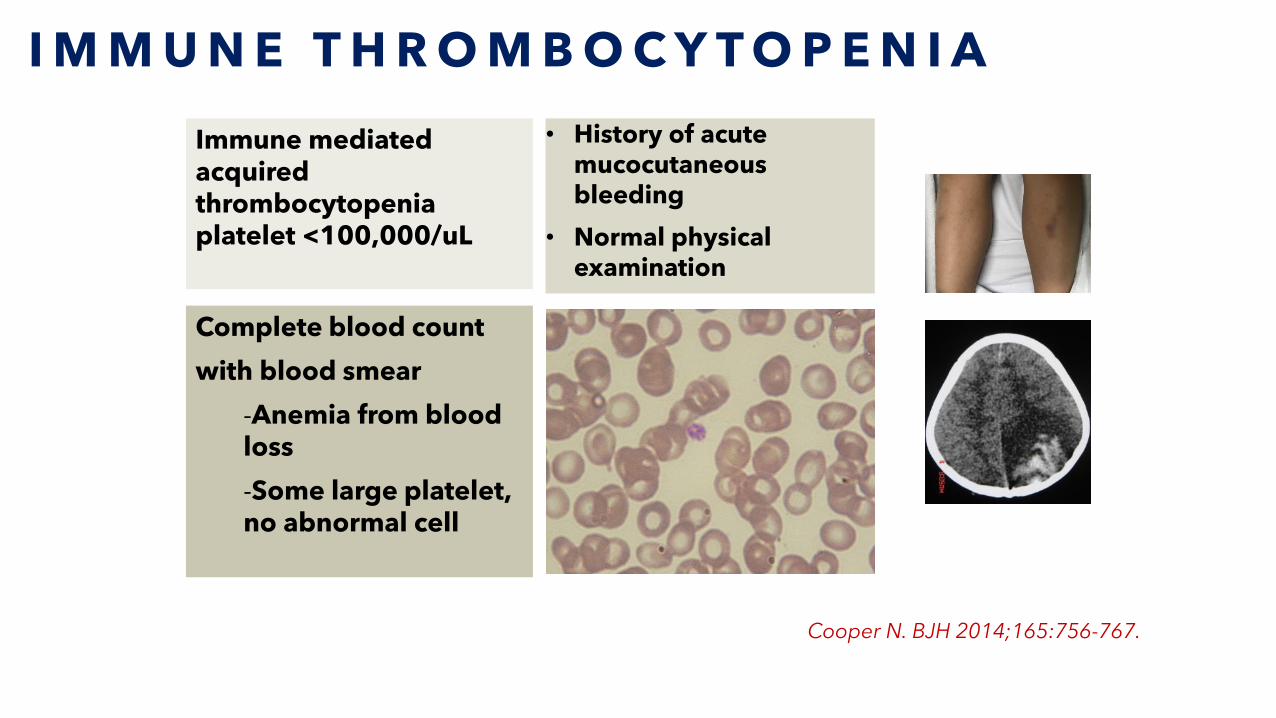
I M M U N E T H R O M B O C Y T O P E N I A
• History of acute mucocutaneous bleeding
• Normal physical examination
Cooper N. BJH 2014;165:756-767.
Immune mediated acquired thrombocytopenia platelet <100,000/uL
Complete blood count
with blood smear
-Anemia from blood loss
-Some large platelet, no abnormal cell
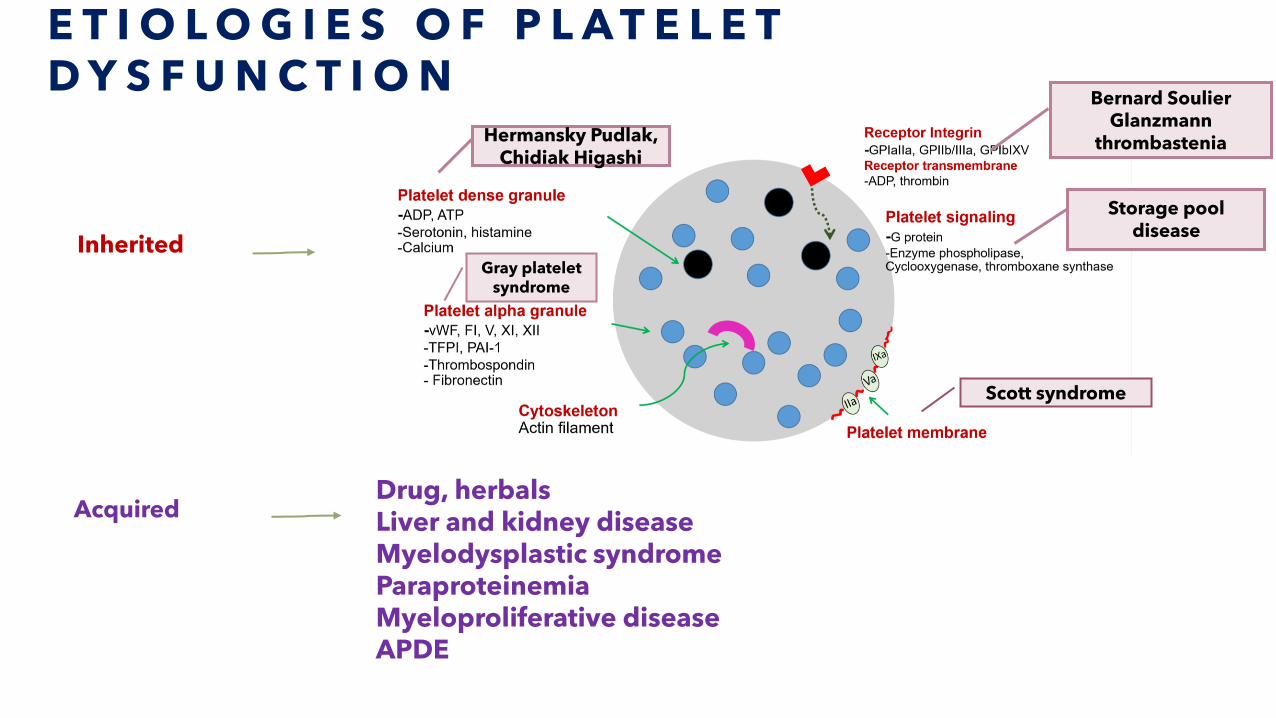
E T I O L O G I E S O F P L A T E L E T D Y S F U N C T I O N
Inherited
Acquired Drug, herbalsLiver and kidney diseaseMyelodysplastic syndromeParaproteinemiaMyeloproliferative diseaseAPDE
Hermansky Pudlak, Chidiak Higashi
Gray platelet syndrome
Scott syndrome
Bernard SoulierGlanzmann
thrombastenia
Storage pool disease
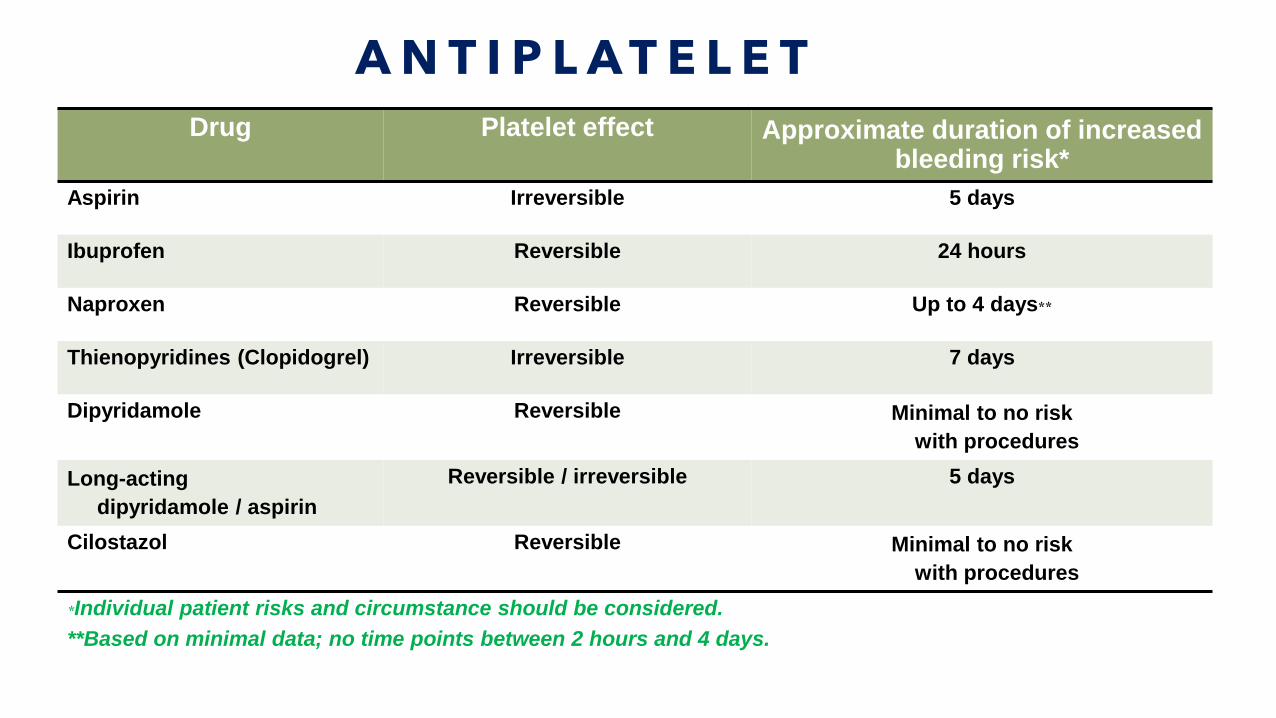
A N T I P L A T E L E T
Drug Platelet effect Approximate duration of increased bleeding risk*
Aspirin Irreversible 5 days
Ibuprofen Reversible 24 hours
Naproxen Reversible Up to 4 days**
Thienopyridines (Clopidogrel) Irreversible 7 days
Dipyridamole Reversible Minimal to no risk
with procedures
Long-acting
dipyridamole / aspirin
Reversible / irreversible 5 days
Cilostazol Reversible Minimal to no risk
with procedures
*Individual patient risks and circumstance should be considered.
**Based on minimal data; no time points between 2 hours and 4 days.
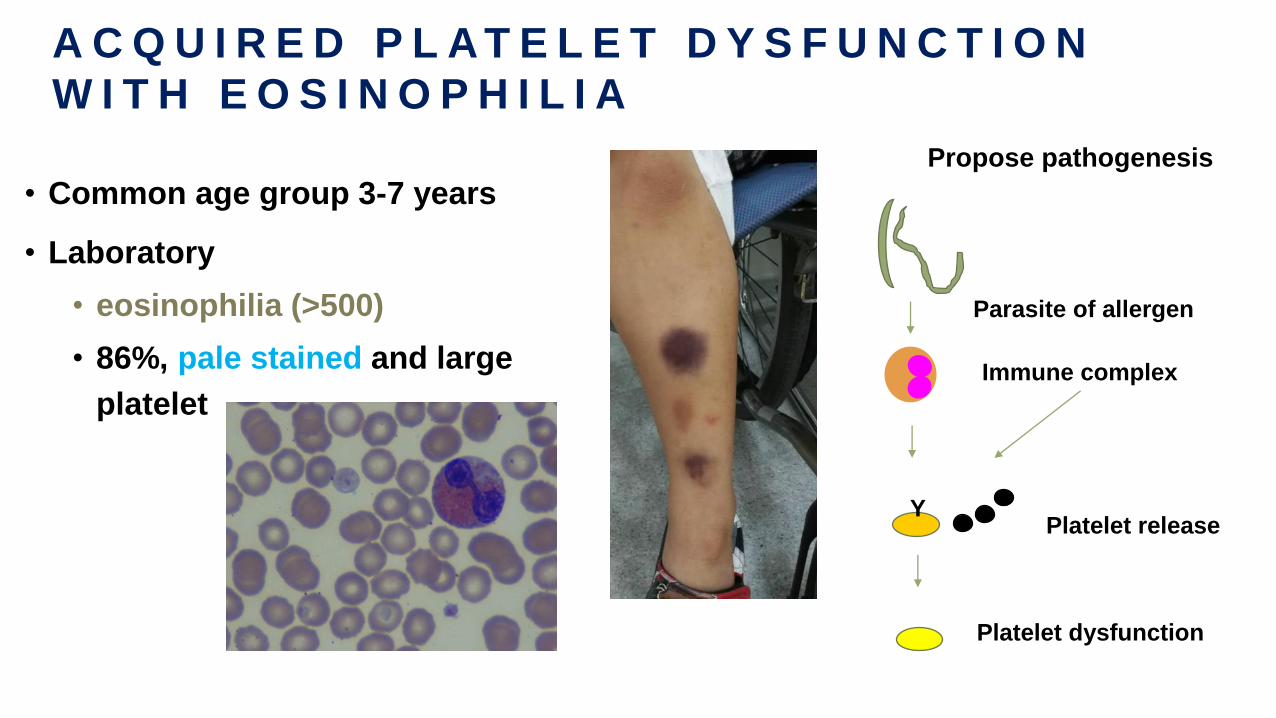
A C Q U I R E D P L A T E L E T D Y S F U N C T I O N
W I T H E O S I N O P H I L I A
• Common age group 3-7 years
• Laboratory
• eosinophilia (>500)
• 86%, pale stained and large
platelet
Parasite of allergen
Immune complex
Y
Platelet dysfunction
Platelet release
Propose pathogenesis
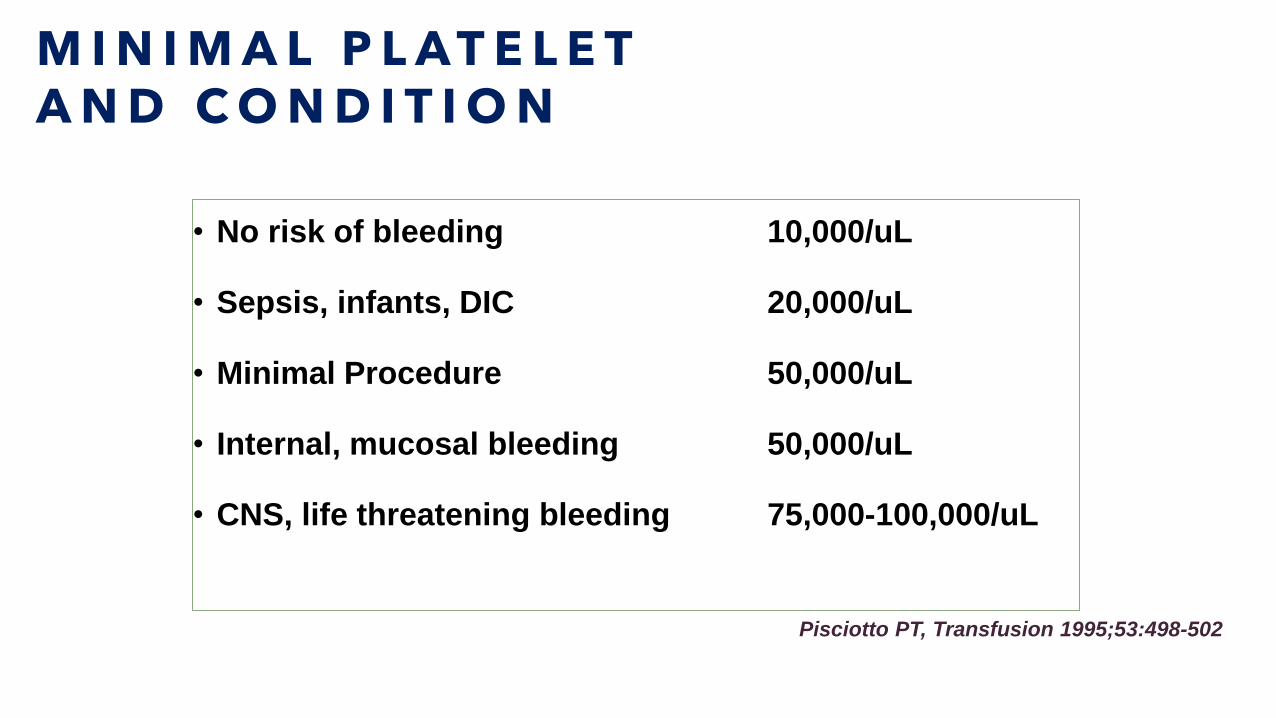
M I N I M A L P L A T E L E T A N D C O N D I T I O N
• No risk of bleeding 10,000/uL
• Sepsis, infants, DIC 20,000/uL
• Minimal Procedure 50,000/uL
• Internal, mucosal bleeding 50,000/uL
• CNS, life threatening bleeding 75,000-100,000/uL
Pisciotto PT, Transfusion 1995;53:498-502
C O M M O N C O A G U L A T I O N D I S O R D E R
• Congenital
• Most common vWD and Hemophilia
• Acquired
• Liver disease, DIC
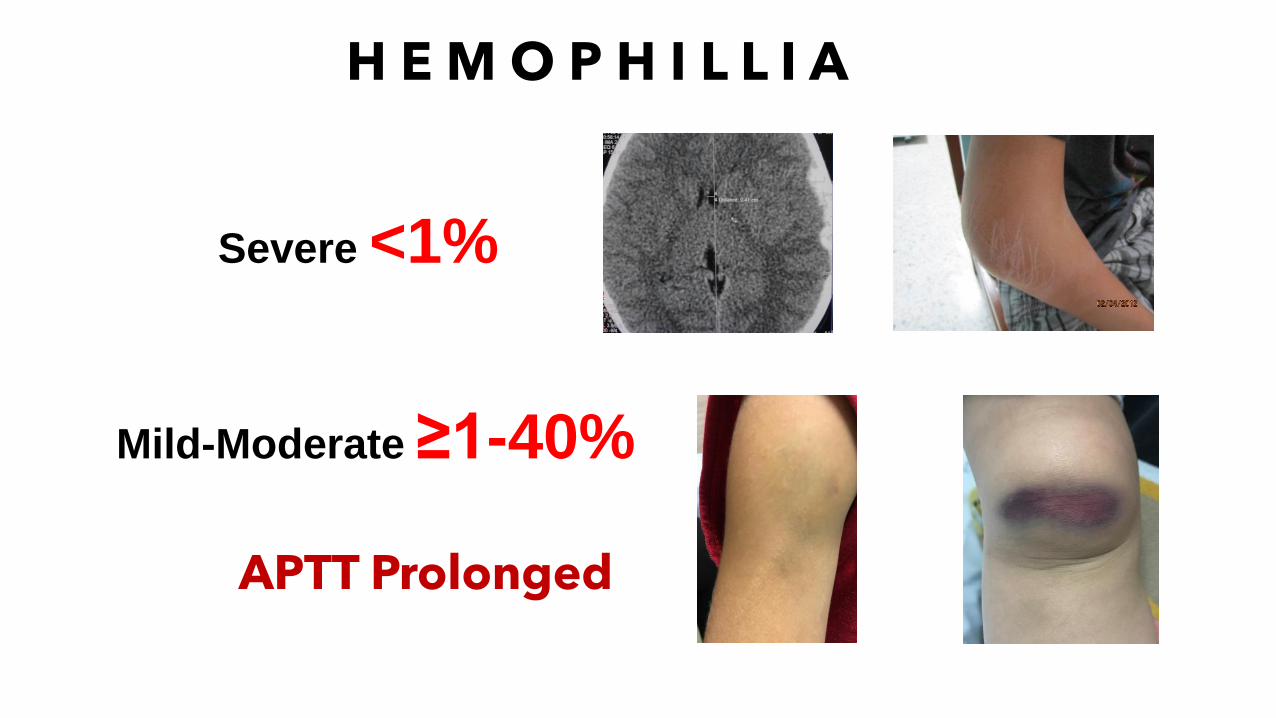
H E M O P H I L L I A
Severe <1%
Mild-Moderate ≥1-40%
APTT Prolonged
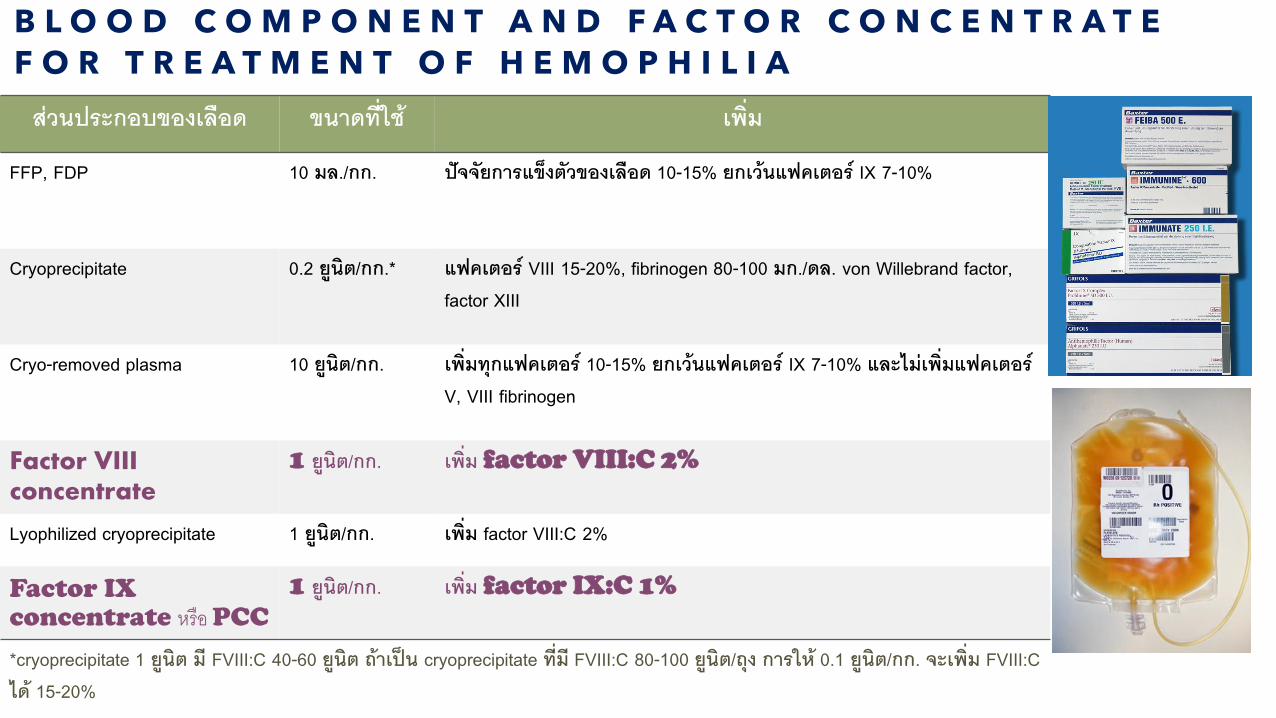
B L O O D C O M P O N E N T A N D F A C T O R C O N C E N T R A T E
F O R T R E A T M E N T O F H E M O P H I L I A
สวนประกอบของเลอด ขนาดทใช เพม
FFP, FDP 10 มล./กก. ปจจยการแขงตวของเลอด 10-15% ยกเวนแฟคเตอร IX 7-10%
Cryoprecipitate 0.2 ยนต/กก.* แฟคเตอร VIII 15-20%, fibrinogen 80-100 มก./ดล. von Willebrand factor, factor XIII
Cryo-removed plasma 10 ยนต/กก. เพมทกแฟคเตอร 10-15% ยกเวนแฟคเตอร IX 7-10% และไมเพมแฟคเตอร V, VIII fibrinogen
Factor VIII concentrate
1 ยนต/กก. เพม factor VIII:C 2%
Lyophilized cryoprecipitate 1 ยนต/กก. เพม factor VIII:C 2%
Factor IX concentrate หรอ PCC
1 ยนต/กก. เพม factor IX:C 1%
*cryoprecipitate 1 ยนต ม FVIII:C 40-60 ยนต ถาเปน cryoprecipitate ทม FVIII:C 80-100 ยนต/ถง การให 0.1 ยนต/กก. จะเพม FVIII:C ได 15-20%
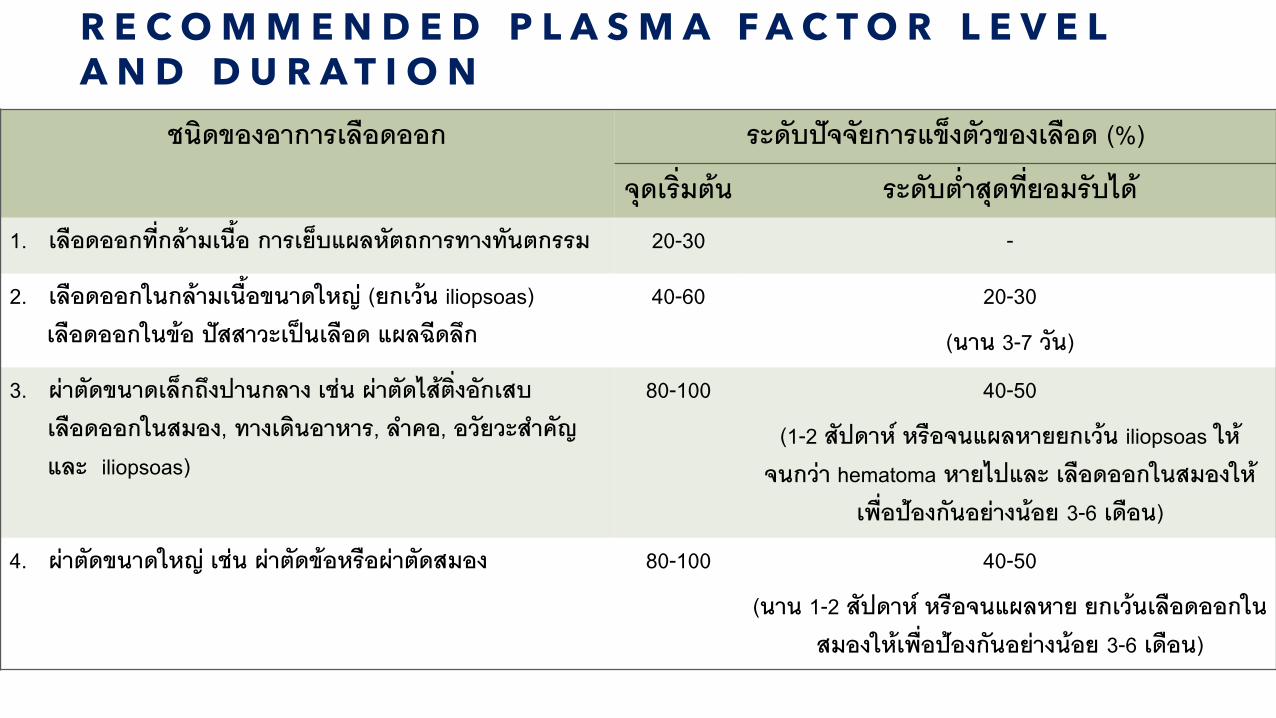
R E C O M M E N D E D P L A S M A F A C T O R L E V E L A N D D U R A T I O N
ชนดของอาการเลอดออก ระดบปจจยการแขงตวของเลอด (%)
จดเรมตน ระดบต าสดทยอมรบได1. เลอดออกทกลามเนอ การเยบแผลหตถการทางทนตกรรม 20-30 -
2. เลอดออกในกลามเนอขนาดใหญ (ยกเวน iliopsoas) เลอดออกในขอ ปสสาวะเปนเลอด แผลฉดลก
40-60 20-30
(นาน 3-7 วน)
3. ผาตดขนาดเลกถงปานกลาง เชน ผาตดไสตงอกเสบ เลอดออกในสมอง, ทางเดนอาหาร, ล าคอ, อวยวะส าคญ และ iliopsoas)
80-100 40-50
(1-2 สปดาห หรอจนแผลหายยกเวน iliopsoas ใหจนกวา hematoma หายไปและ เลอดออกในสมองให
เพอปองกนอยางนอย 3-6 เดอน)
4. ผาตดขนาดใหญ เชน ผาตดขอหรอผาตดสมอง 80-100 40-50
(นาน 1-2 สปดาห หรอจนแผลหาย ยกเวนเลอดออกในสมองใหเพอปองกนอยางนอย 3-6 เดอน)
T R E A T M E N T O F H E M O P H I L I A
ผปวยนอก หรอ หอสงเกตอาการ 150,000บาท ไมเกน 2 ครง ตอ เดอนผปวยในภาวะฉกเฉน 300,000 บาท ตอ ครง
“Early treatment to primary prophylaxis”
ลงทะเบยนในสถานพยาบาลทจดทะเบยนดแลผปวย
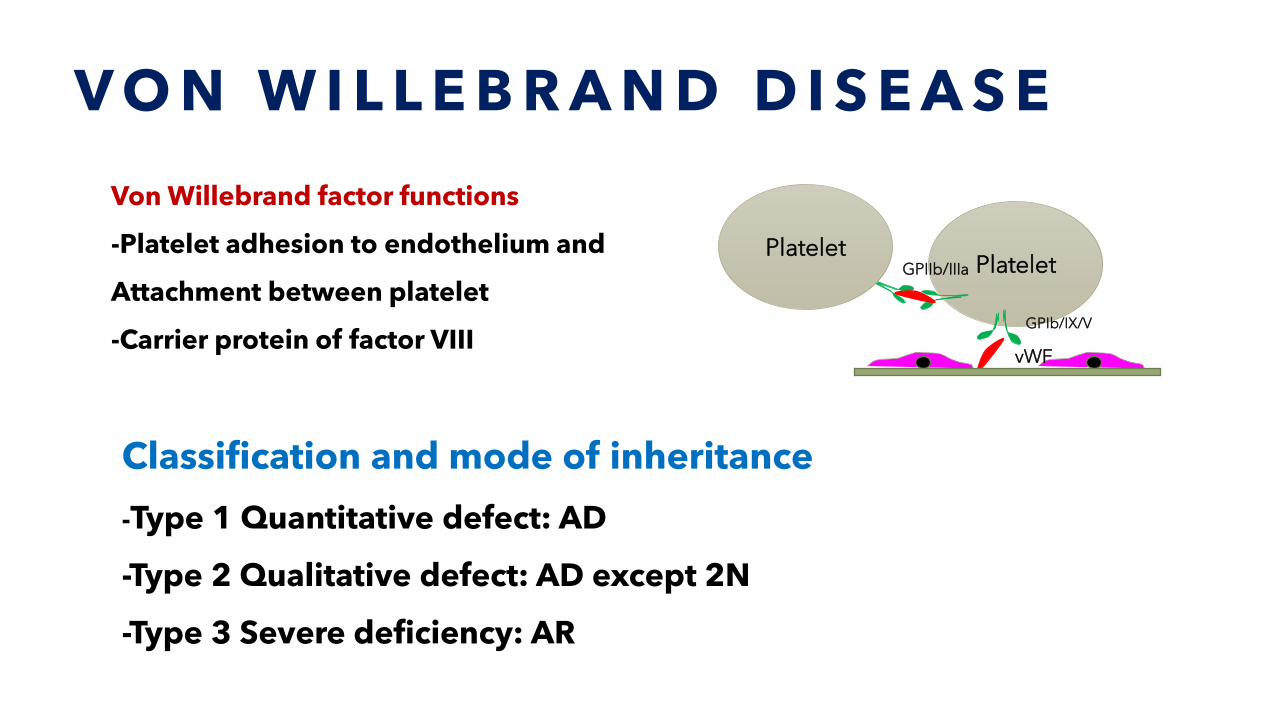
V O N W I L L E B R A N D D I S E A S E
Platelet
vWF
GPIb/IX/V
GPIIb/IIIaPlatelet
Von Willebrand factor functions
-Platelet adhesion to endothelium and
Attachment between platelet
-Carrier protein of factor VIII
Classification and mode of inheritance
-Type 1 Quantitative defect: AD
-Type 2 Qualitative defect: AD except 2N
-Type 3 Severe deficiency: AR
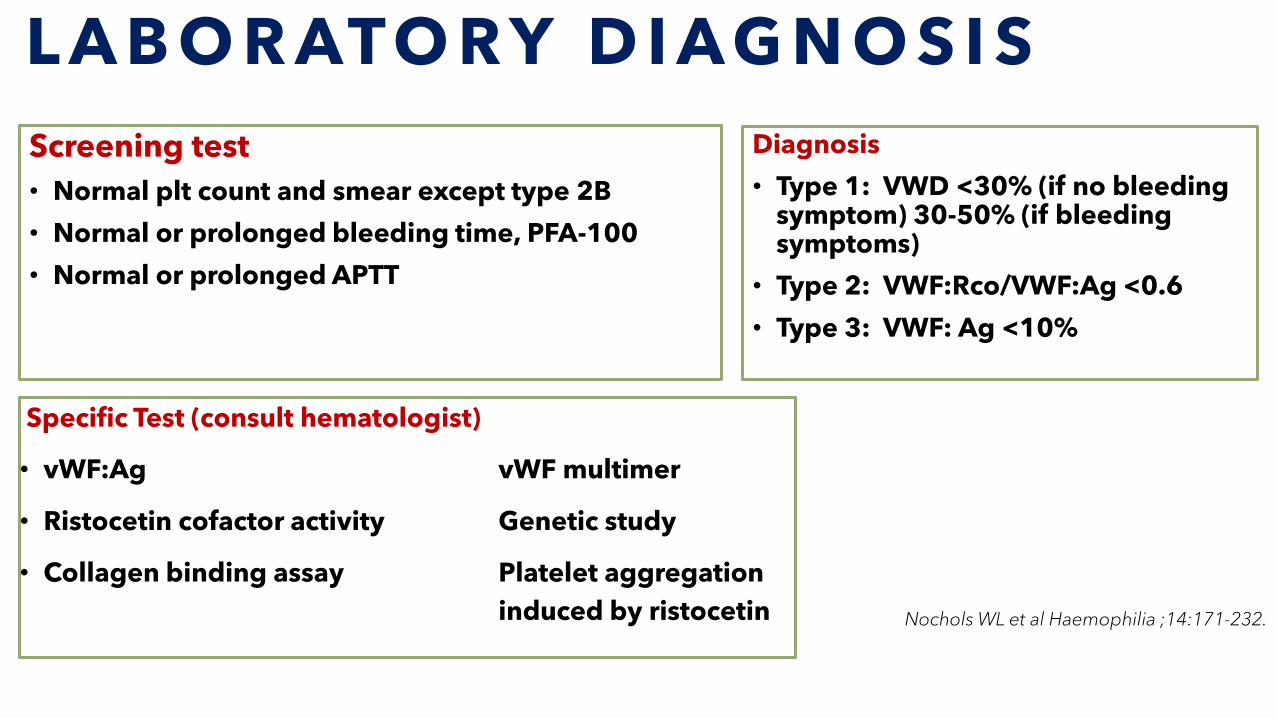
L A B O R ATO R Y D I AG N O S I S
Specific Test (consult hematologist)
• vWF:Ag vWF multimer
• Ristocetin cofactor activity Genetic study
• Collagen binding assay Platelet aggregation
induced by ristocetin
Screening test
• Normal plt count and smear except type 2B
• Normal or prolonged bleeding time, PFA-100
• Normal or prolonged APTT
Diagnosis
• Type 1: VWD <30% (if no bleeding symptom) 30-50% (if bleeding symptoms)
• Type 2: VWF:Rco/VWF:Ag <0.6
• Type 3: VWF: Ag <10%
Nochols WL et al Haemophilia ;14:171-232.
T R E A T M E N T O F V O N W I L L E B R A N D D I S E A S E
• DDAVP 0.3 mcg/kg/dose in 0.9% NSS 15 mL intravenous in
15-30 mins in VWD type 1, type 2A
• Tranxenamic acid 10 mg/kg/dose IV, 15-20 mg/kg/dose oral
q 4-6 h
• Factor VIII conc. (vWF/FVIII): Alphanate, Immunate
Mannuccio PM Engl J Med 2004;351:683-94.
S U P P O R T I V E T R E A T M E N T
• Antifibrinolytic agent
• Tranexamic acid
• 10 mg/kg/dose intravenously
• 15-20 mg/kg/dose orally
• 5% solution mouth rinse
• Desmopressin• DDAVP 0.3 mcg/kg
D I S S E M I N A T E D I N T R A V A S C U L A R C O A G U L A T I O N
Acquired syndrome,
characterized by the systemic
intravascular activation arising
from different causes, can cause
damage to the microvasculature
result in organ dysfunction
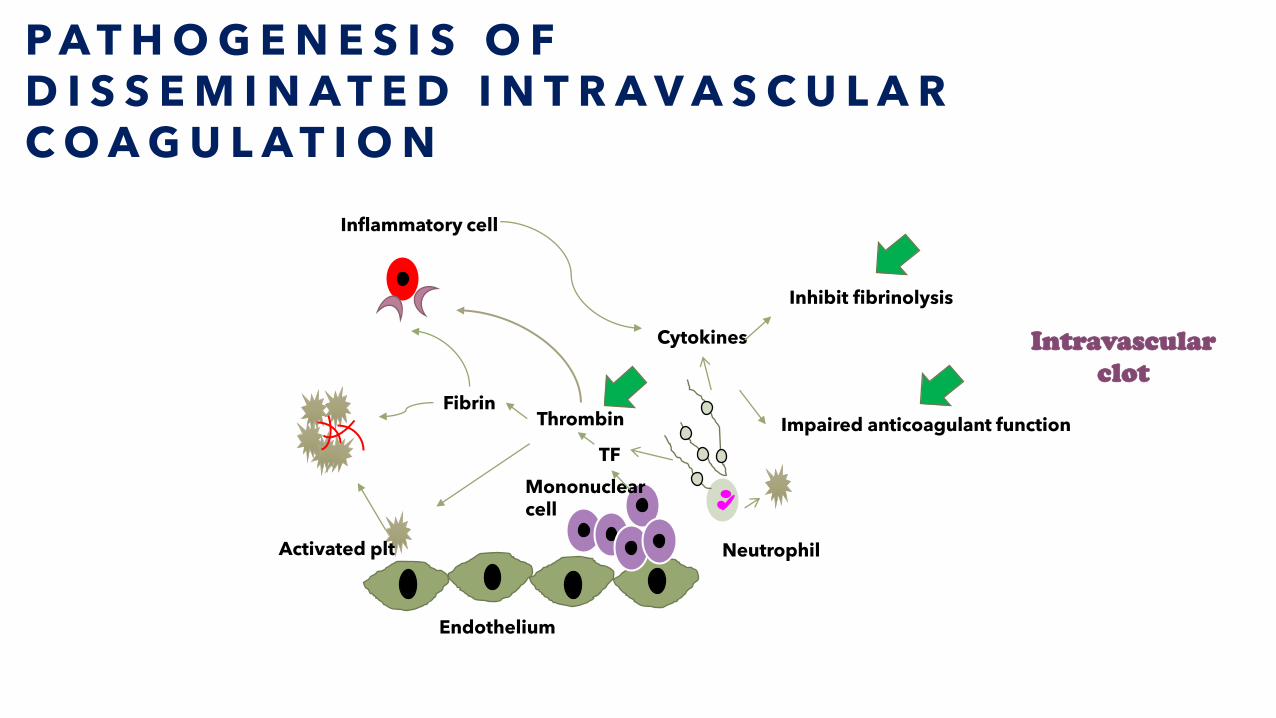
P A T H O G E N E S I S O F D I S S E M I N A T E D I N T R A V A S C U L A R C O A G U L A T I O N
Mononuclearcell
Endothelium
Activated plt
Inflammatory cell
TF
ThrombinFibrin
Cytokines
Inhibit fibrinolysis
Impaired anticoagulant function
Neutrophil
Intravascular
clot
C O N D I T I O N S A S S O C I A T E D W I T H D I S S E M I N A T E D I N T R A V A S C U L A R C O A G U L A T I O N
Sepsis and severe infection
Trauma
Organ destruction e.g. pancreatitis
Malignancy
Solid tumors
Leukemia
Obstetric
Amniotic fluid embolism
Placental abruption
Pre-eclampsia
Vascular abnormalities
Large hemangioma
Vascular aneurysm
Severe liver failure
Toxic and immunological insults
Recreational drugs
ABO transfusion incompatibility
Transplant rejection
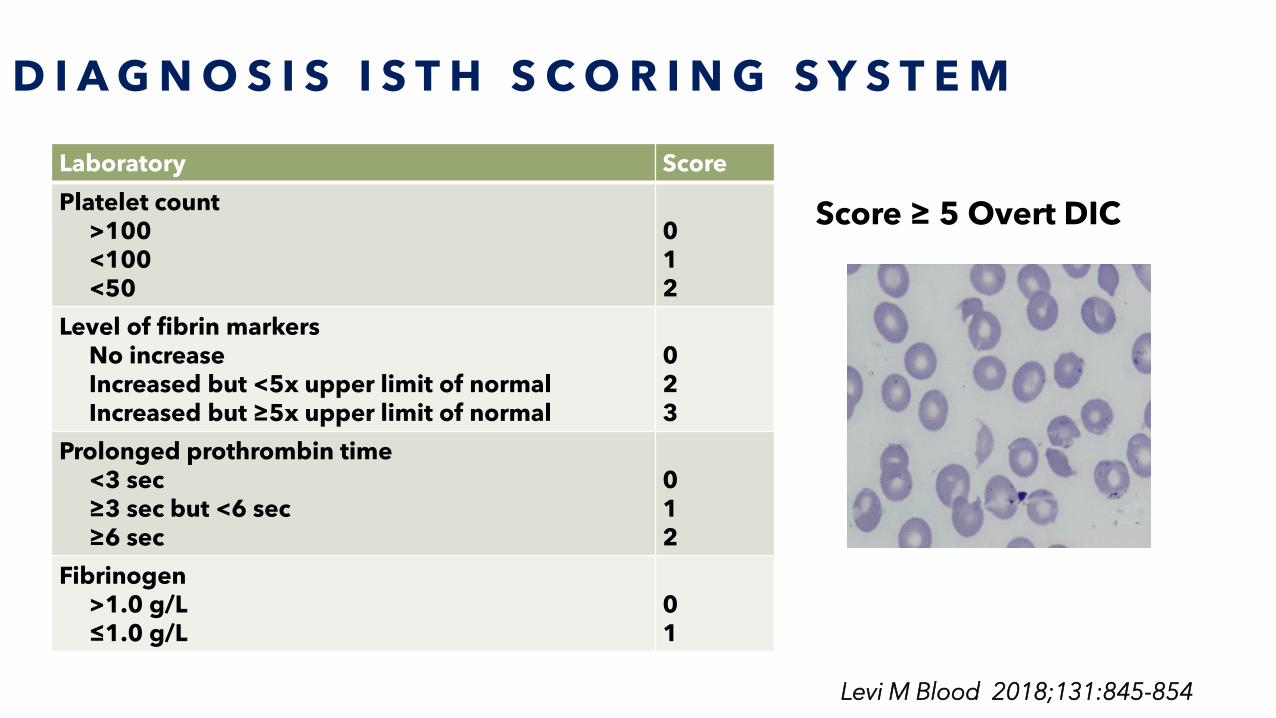
D I A G N O S I S I S T H S C O R I N G S Y S T E M
Laboratory Score
Platelet count>100<100<50
012
Level of fibrin markersNo increaseIncreased but <5x upper limit of normalIncreased but ≥5x upper limit of normal
023
Prolonged prothrombin time<3 sec≥3 sec but <6 sec≥6 sec
012
Fibrinogen >1.0 g/L≤1.0 g/L
01
Score ≥ 5 Overt DIC
Levi M Blood 2018;131:845-854
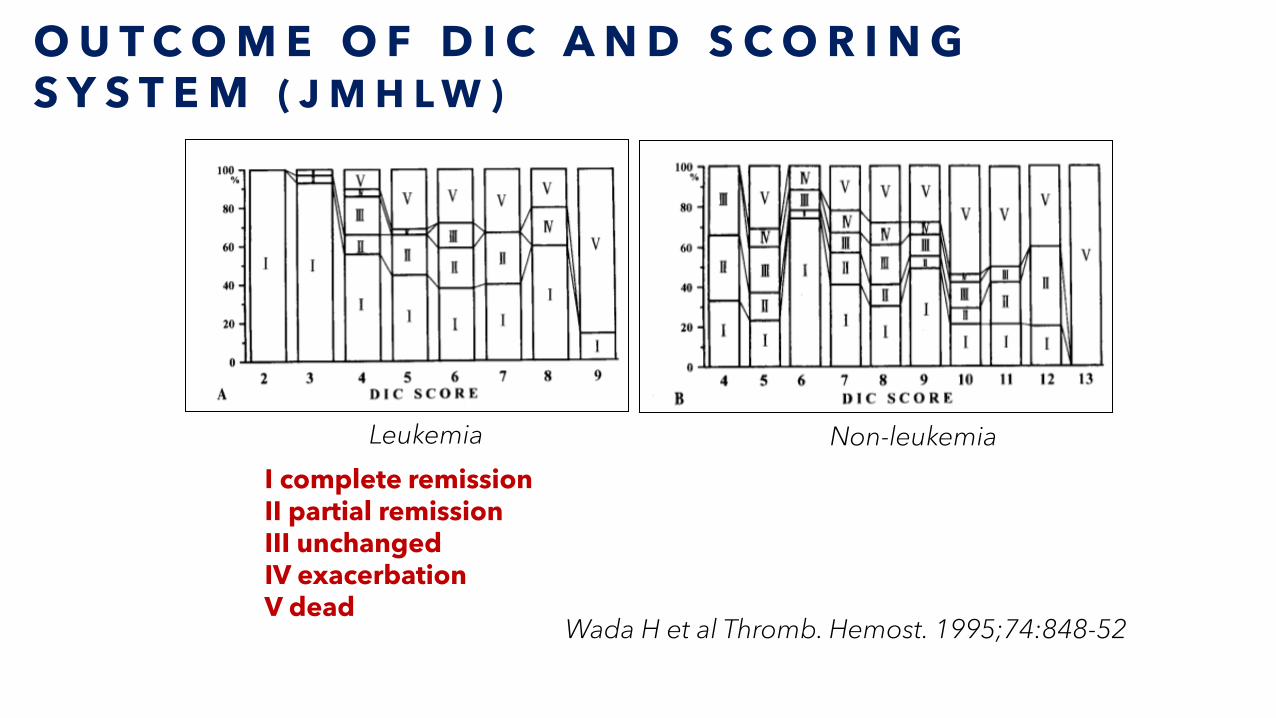
O U T C O M E O F D I C A N D S C O R I N G S Y S T E M ( J M H L W )
Wada H et al Thromb. Hemost. 1995;74:848-52
I complete remissionII partial remissionIII unchangedIV exacerbationV dead
Leukemia Non-leukemia
H E M O S T A S I S I N L I V E R D I S E A S E
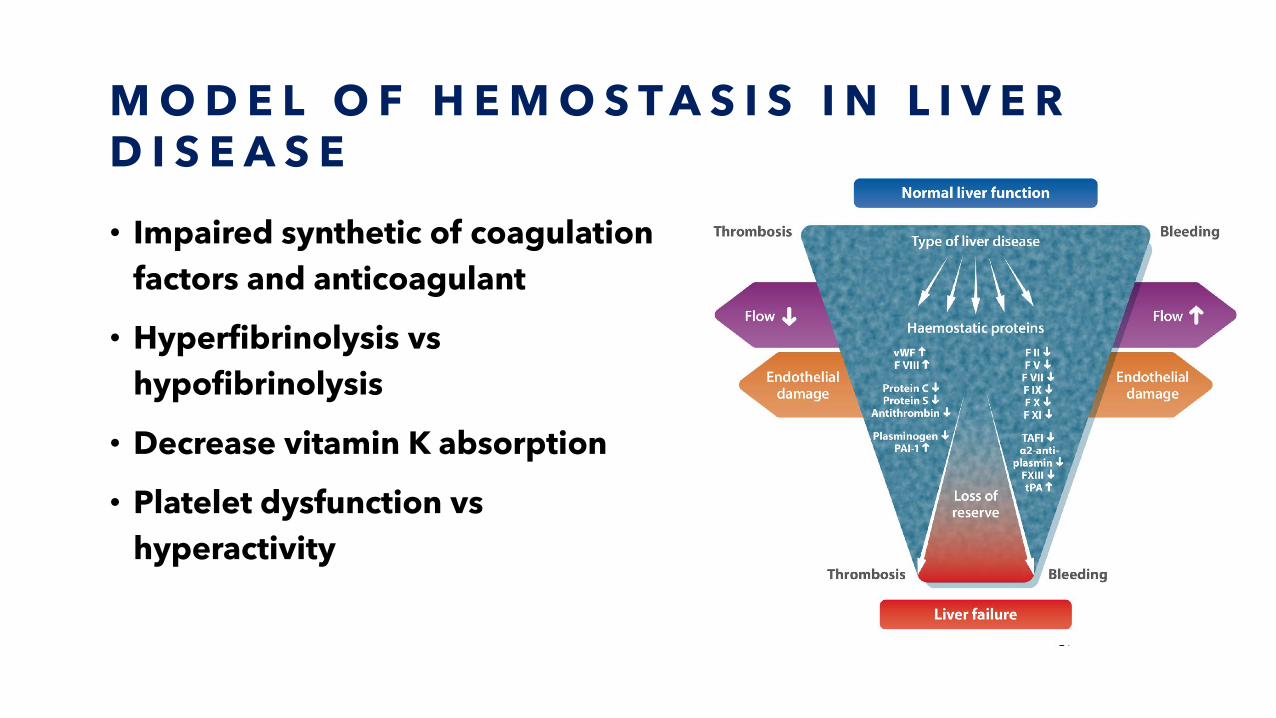
M O D E L O F H E M O S T A S I S I N L I V E R D I S E A S E
• Impaired synthetic of coagulation
factors and anticoagulant
• Hyperfibrinolysis vs
hypofibrinolysis
• Decrease vitamin K absorption
• Platelet dysfunction vs
hyperactivity
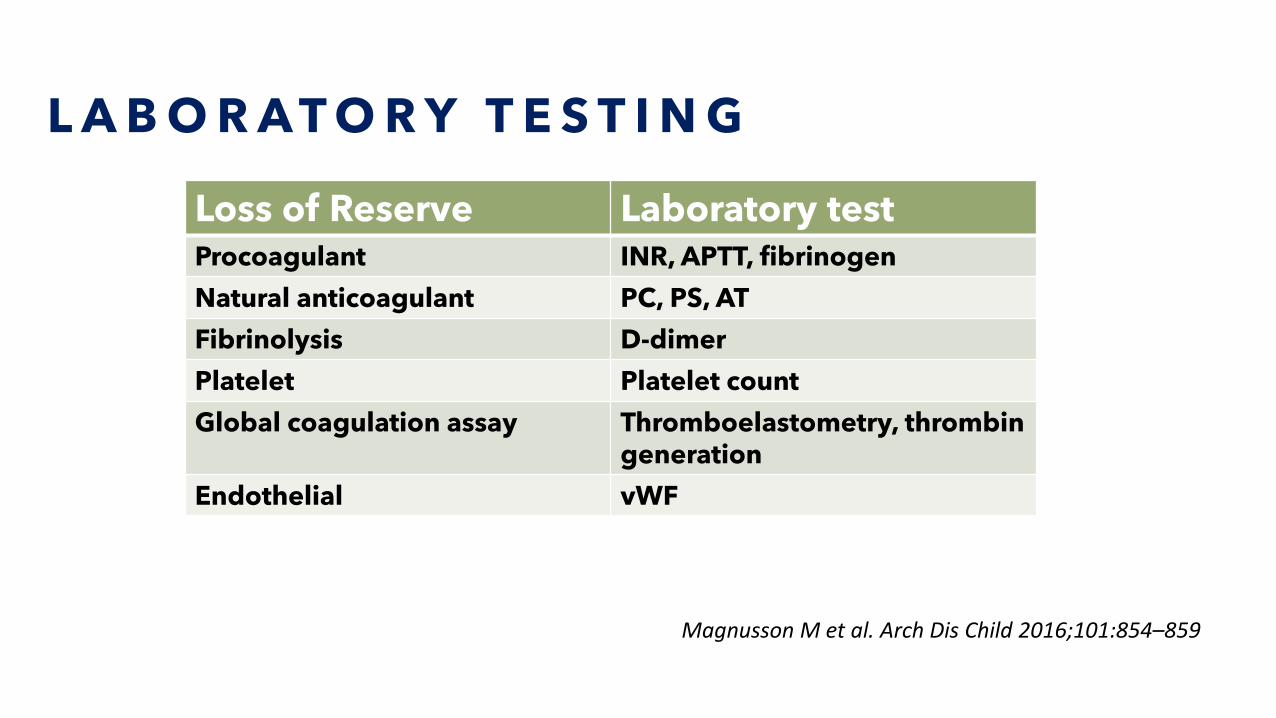
L A B O R A T O R Y T E S T I N G
Loss of Reserve Laboratory testProcoagulant INR, APTT, fibrinogen
Natural anticoagulant PC, PS, AT
Fibrinolysis D-dimer
Platelet Platelet count
Global coagulation assay Thromboelastometry, thrombin generation
Endothelial vWF
Magnusson M et al. Arch Dis Child 2016;101:854–859
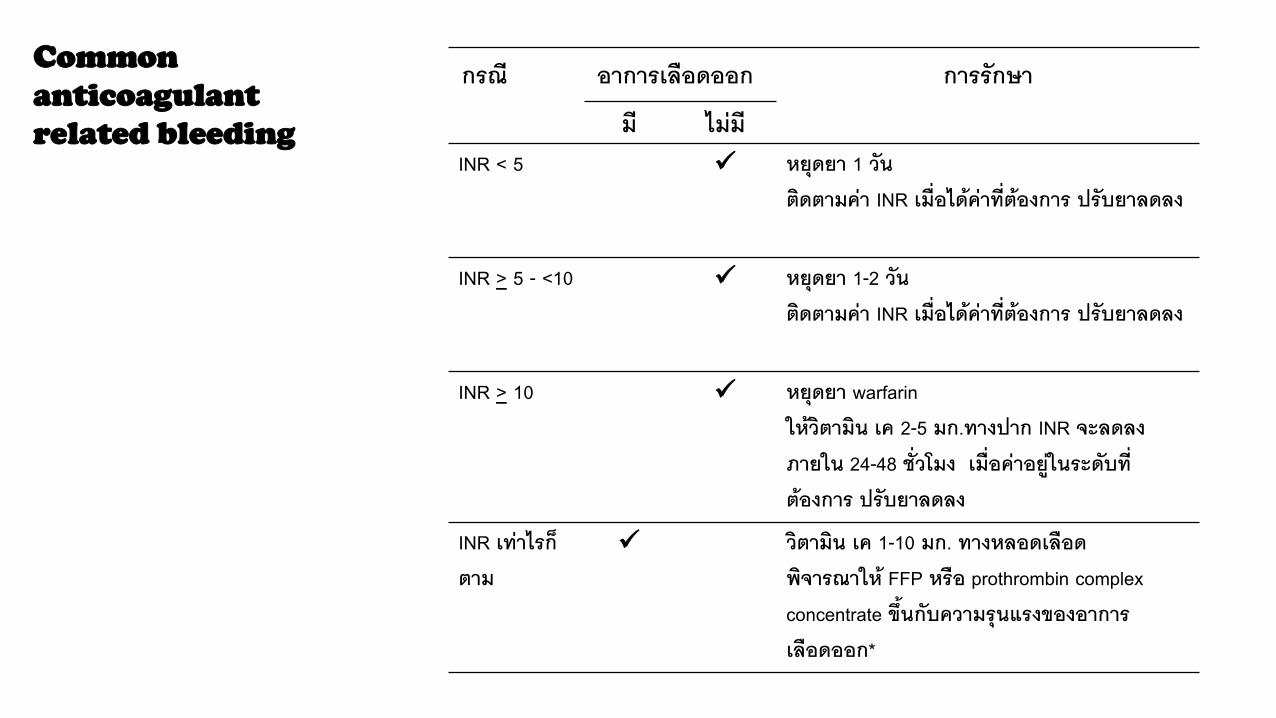
W A R F A R I N A N D
B L E E D I N G M A N A G E M E N T
กรณ อาการเลอดออก การรกษา
ม ไมมINR < 5 ✓ หยดยา 1 วน
ตดตามคา INR เมอไดคาทตองการ ปรบยาลดลง
INR > 5 - <10 ✓ หยดยา 1-2 วน ตดตามคา INR เมอไดคาทตองการ ปรบยาลดลง
INR > 10 ✓ หยดยา warfarin ใหวตามน เค 2-5 มก.ทางปาก INR จะลดลงภายใน 24-48 ชวโมง เมอคาอยในระดบทตองการ ปรบยาลดลง
INR เทาไรกตาม
✓ วตามน เค 1-10 มก. ทางหลอดเลอดพจารณาให FFP หรอ prothrombin complex concentrate ขนกบความรนแรงของอาการเลอดออก*
Common
anticoagulant
related bleeding

T R E A T M E N T O F
H E P A R I N R E L A T E D
B L E E D I N G
ระยะเวลาตงแตไดรบยา heparin ครง
สดทาย (นาท)
ขนาดยา protamine ตอ 100 ยนต ของ
heparin
(มก.)
<30 1
30-60 0.5-0.75
60-120 0.375-0.5
>120 0.25-0.375
M A S S I V E B L O O D L O S S
• Hemorrhage is a leading cause of
preventable traumatic death for patients
of all ages, accounting for 20%-40% of
all early trauma-related mortality
Nosanov L. The American Journal of Surgery 2013; 206:655-660.
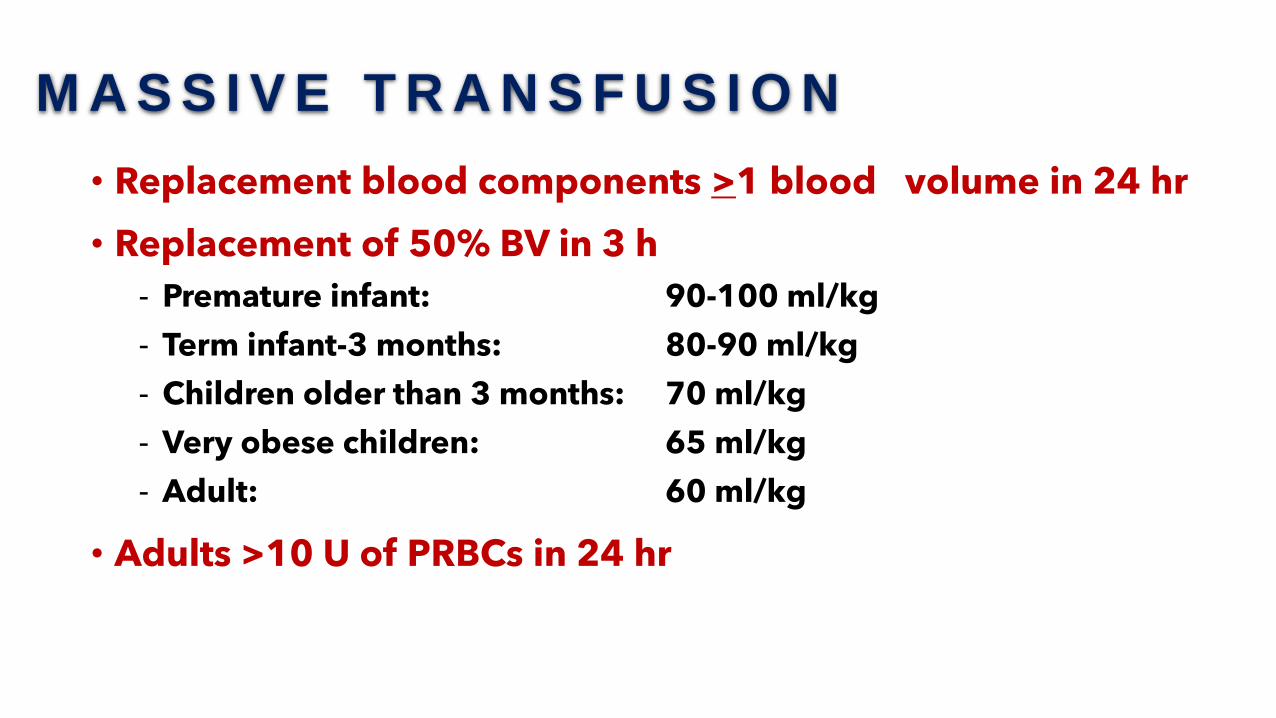
M A S S I V E T R A N S F U S I O N
• Replacement blood components >1 blood volume in 24 hr
• Replacement of 50% BV in 3 h
- Premature infant: 90-100 ml/kg
- Term infant-3 months: 80-90 ml/kg
- Children older than 3 months: 70 ml/kg
- Very obese children: 65 ml/kg
- Adult: 60 ml/kg
• Adults >10 U of PRBCs in 24 hr
C A U S E O F M A S S I V E B L E E D I N G
Trauma
Surgery
Uncontrolled bleeding
Uncontrolled bleeding
Massive Blood loss
CoagulopathyPlatelet disorderAnticoagulant, antiplatelet
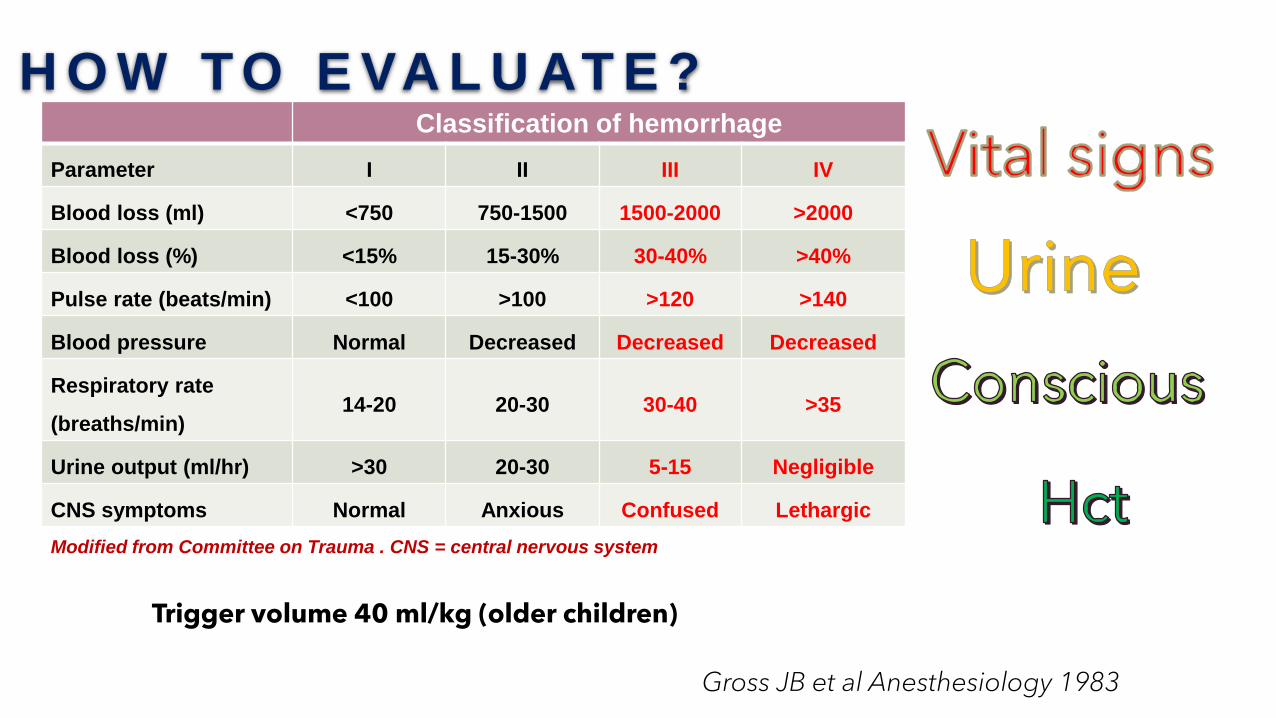
H O W T O E VA L U AT E ?Classification of hemorrhage
Parameter I II III IV
Blood loss (ml) <750 750-1500 1500-2000 >2000
Blood loss (%) <15% 15-30% 30-40% >40%
Pulse rate (beats/min) <100 >100 >120 >140
Blood pressure Normal Decreased Decreased Decreased
Respiratory rate
(breaths/min)14-20 20-30 30-40 >35
Urine output (ml/hr) >30 20-30 5-15 Negligible
CNS symptoms Normal Anxious Confused Lethargic
Modified from Committee on Trauma . CNS = central nervous system
Gross JB et al Anesthesiology 1983
Trigger volume 40 ml/kg (older children)
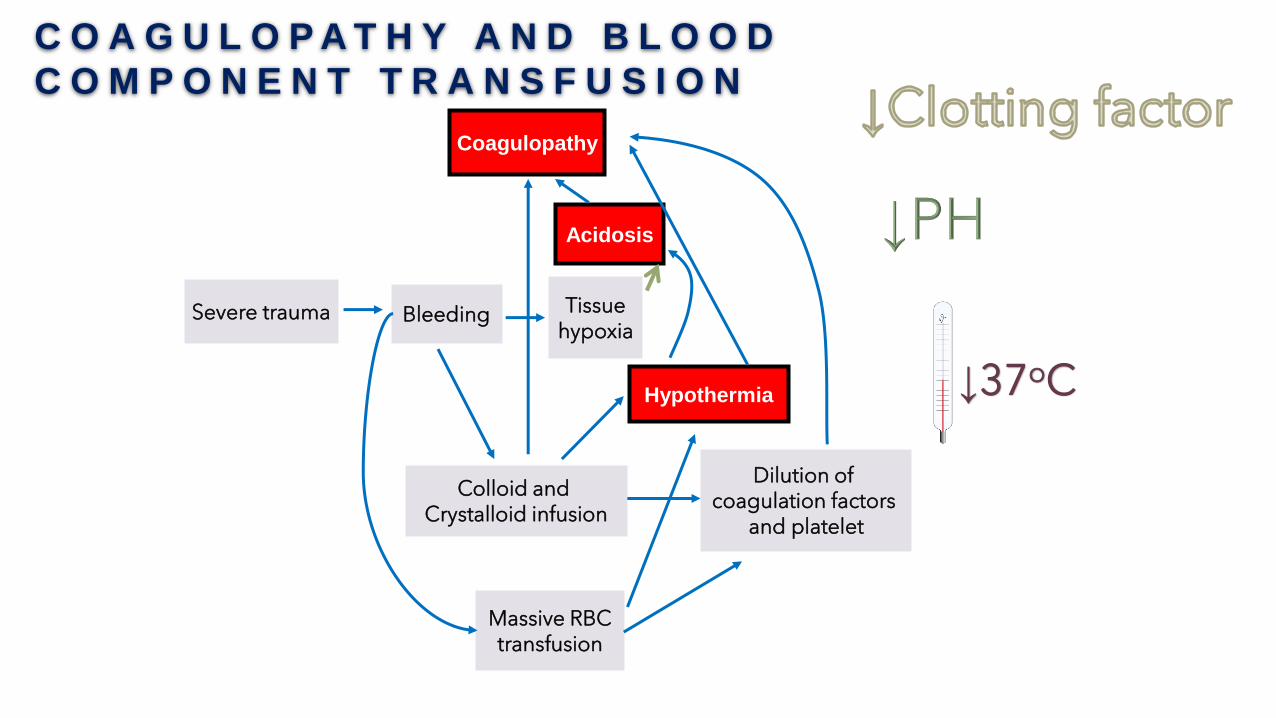
C O A G U L O P A T H Y A N D B L O O D
C O M P O N E N T T R A N S F U S I O N
Coagulopathy
Acidosis
BleedingSevere trauma Tissuehypoxia
Hypothermia
Colloid and Crystalloid infusion
Massive RBCtransfusion
Dilution of coagulation factors
and platelet
↓37oC
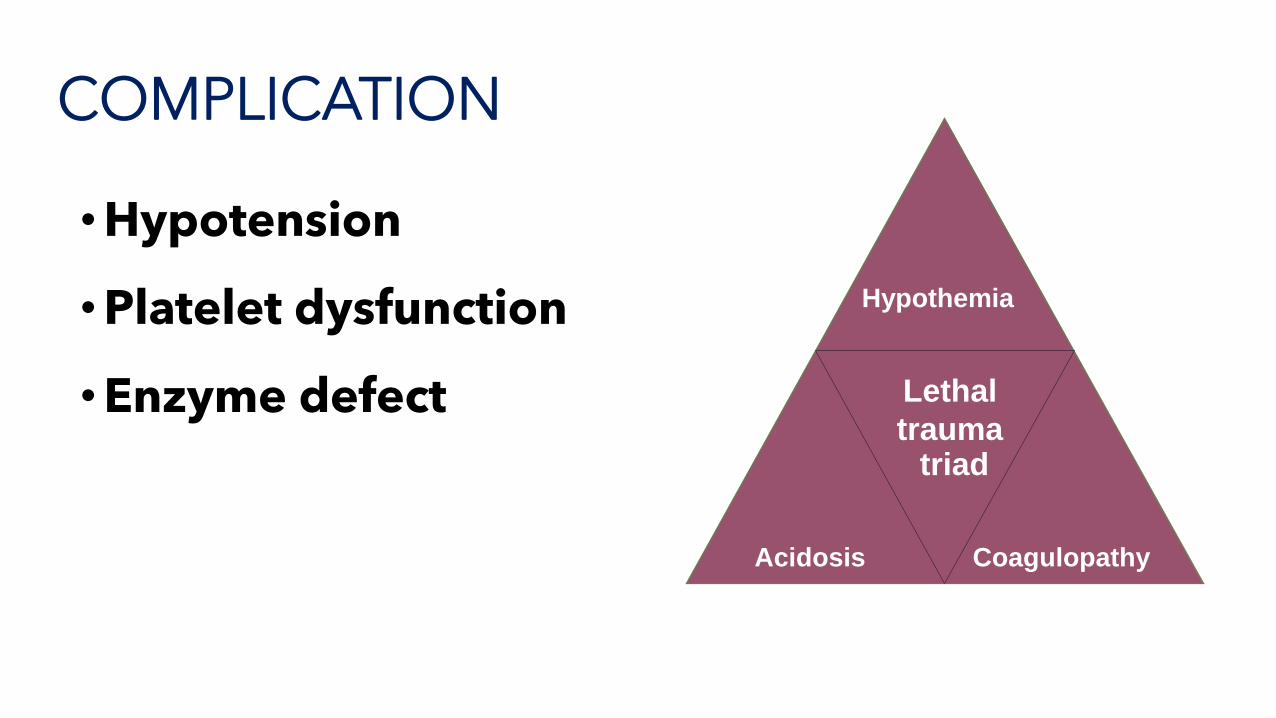
•Hypotension
•Platelet dysfunction
•Enzyme defect
Hypothemia
CoagulopathyAcidosis
Lethal
trauma triad
COMPLICATION
M A N A G E M E N T O F M A S S I V E B L E E D I N G
• Stop bleeding
• Identified site of bleeding
• Surgical or interventional management
• Restoration of coagulation
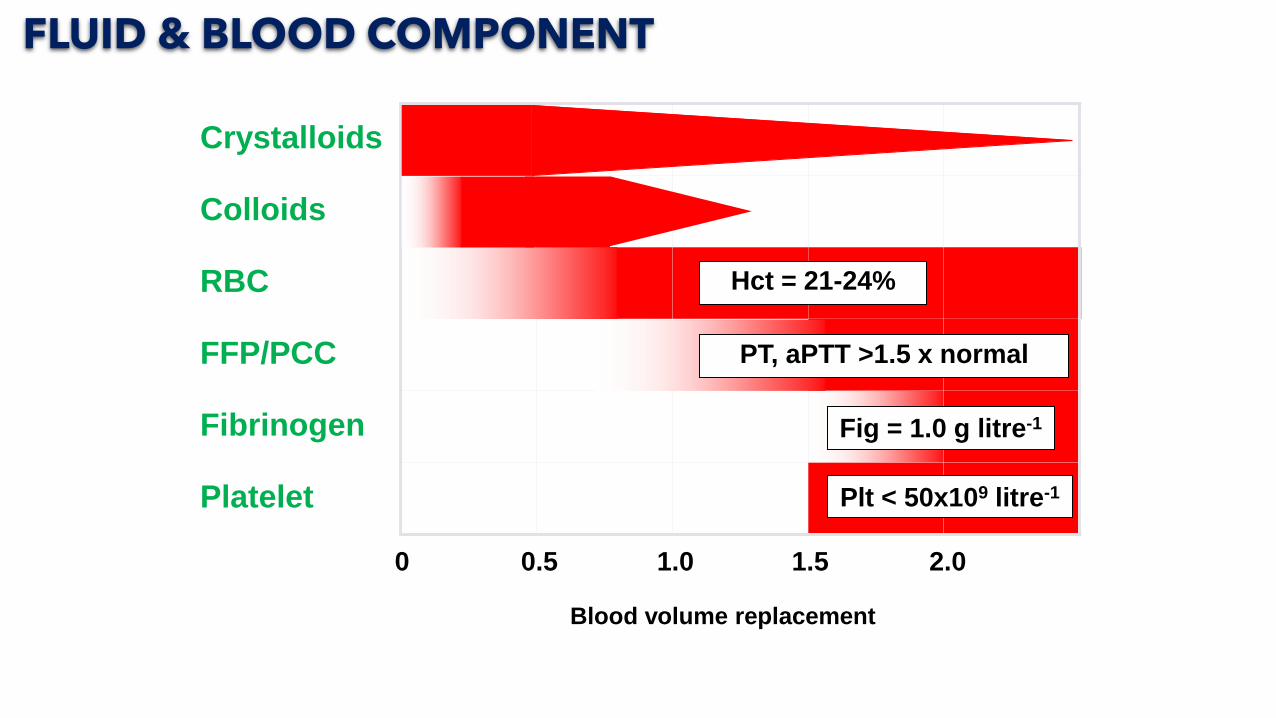
Crystalloids
Colloids
RBC
FFP/PCC
Fibrinogen
Platelet
0 0.5 1.0 1.5 2.0
Blood volume replacement
2.5
Hct = 21-24%
Fig = 1.0 g litre-1
Plt < 50x109 litre-1
PT, aPTT >1.5 x normal
FLUID & BLOOD COMPONENT
I N V E S T I G AT I O N
• Complete blood count
• Coagulogram (APTT, PT and TT)
• Fibrinogen, euglobulin clot lysis time
• Thromboelastometry
• Liver function and renal function test
• Urine examination
• Arterial blood gas
• Serum lactate, electrolyte Ca, ionized Ca and
albumin
T H R O M B O E L A S T O M E T R Y A N D G U I D A N C E O F T R A N S F U S I O N
• A systematic review or 9 randomized clinical trials, mostly
cardiac surgery in 776 adults
• Benefit: reduced bleeding, reduction of patients receiving
transfusion as a combined FFP and platelet
• No difference in mortality event rate
Wikkelsoe AJ et al Acta Anaesthesiol Scand 2011;55:1174-1189
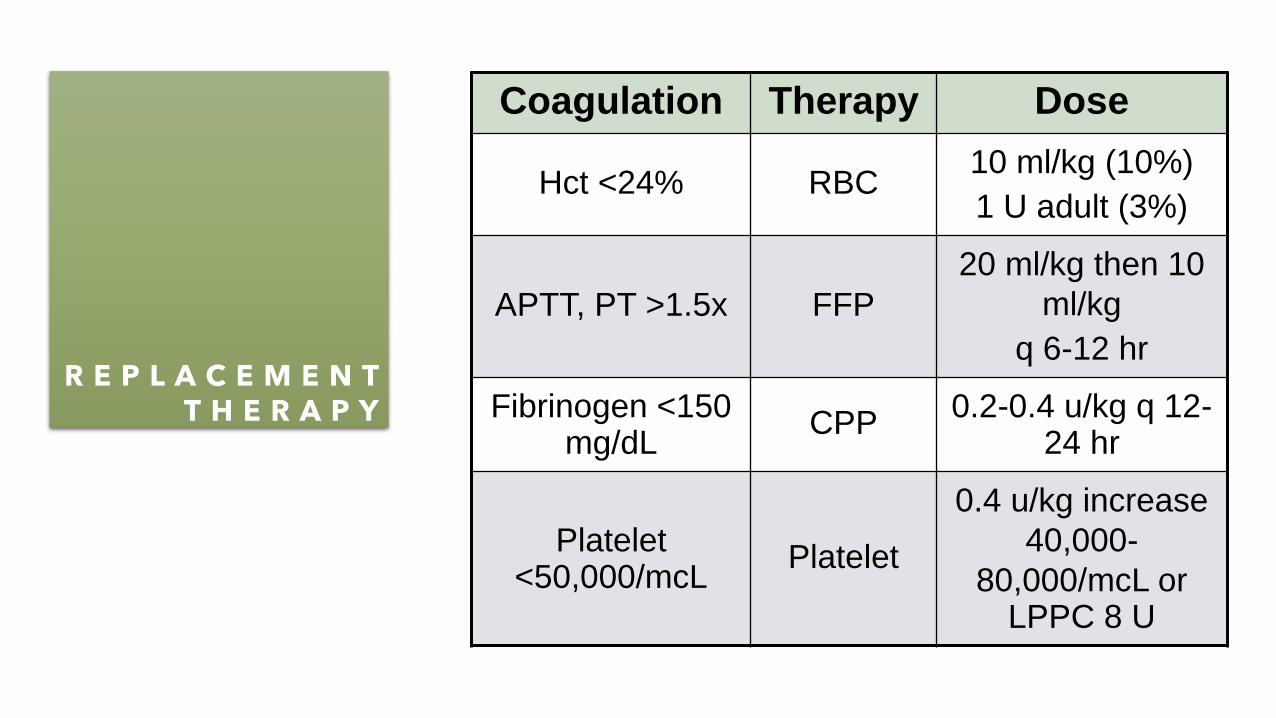
R E P L A C E M E N T T H E R A P Y
Coagulation Therapy Dose
Hct <24% RBC10 ml/kg (10%)
1 U adult (3%)
APTT, PT >1.5x FFP
20 ml/kg then 10
ml/kg
q 6-12 hr
Fibrinogen <150 mg/dL
CPP0.2-0.4 u/kg q 12-
24 hr
Platelet <50,000/mcL
Platelet
0.4 u/kg increase
40,000-
80,000/mcL or LPPC 8 U
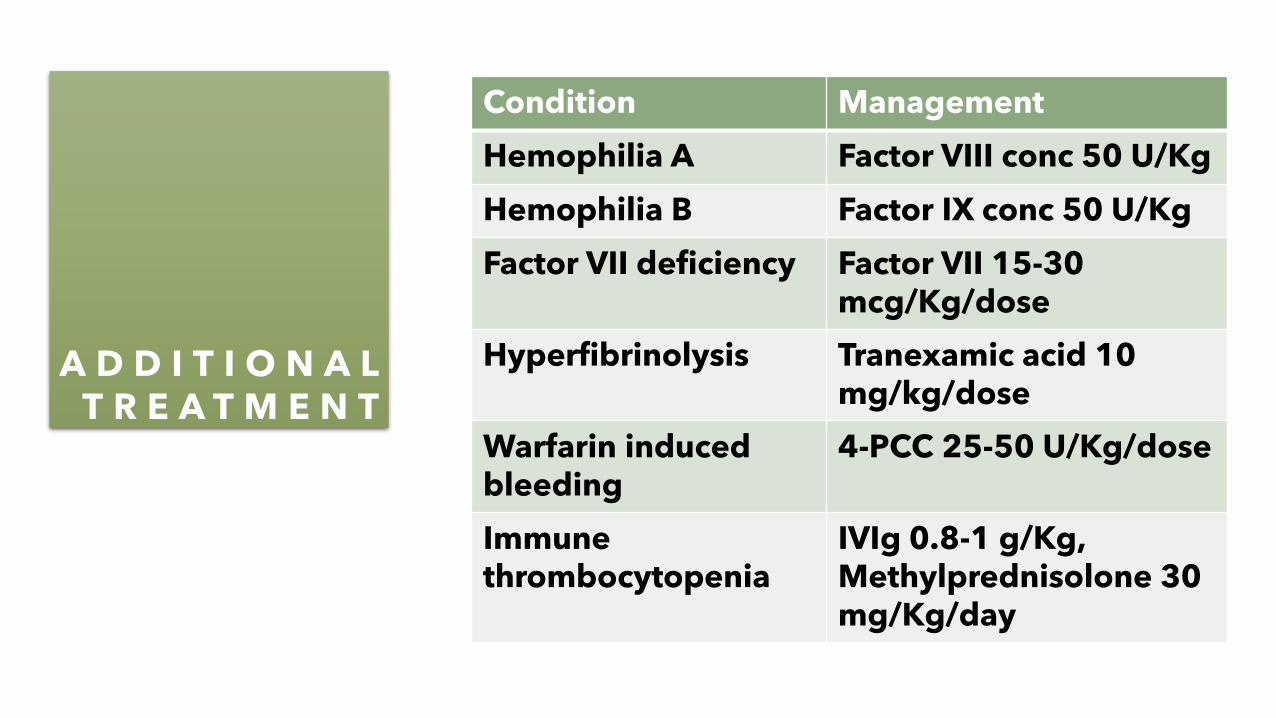
A D D I T I O N A L T R E A T M E N T
Condition Management
Hemophilia A Factor VIII conc 50 U/Kg
Hemophilia B Factor IX conc 50 U/Kg
Factor VII deficiency Factor VII 15-30 mcg/Kg/dose
Hyperfibrinolysis Tranexamic acid 10 mg/kg/dose
Warfarin induced bleeding
4-PCC 25-50 U/Kg/dose
Immune thrombocytopenia
IVIg 0.8-1 g/Kg, Methylprednisolone 30 mg/Kg/day
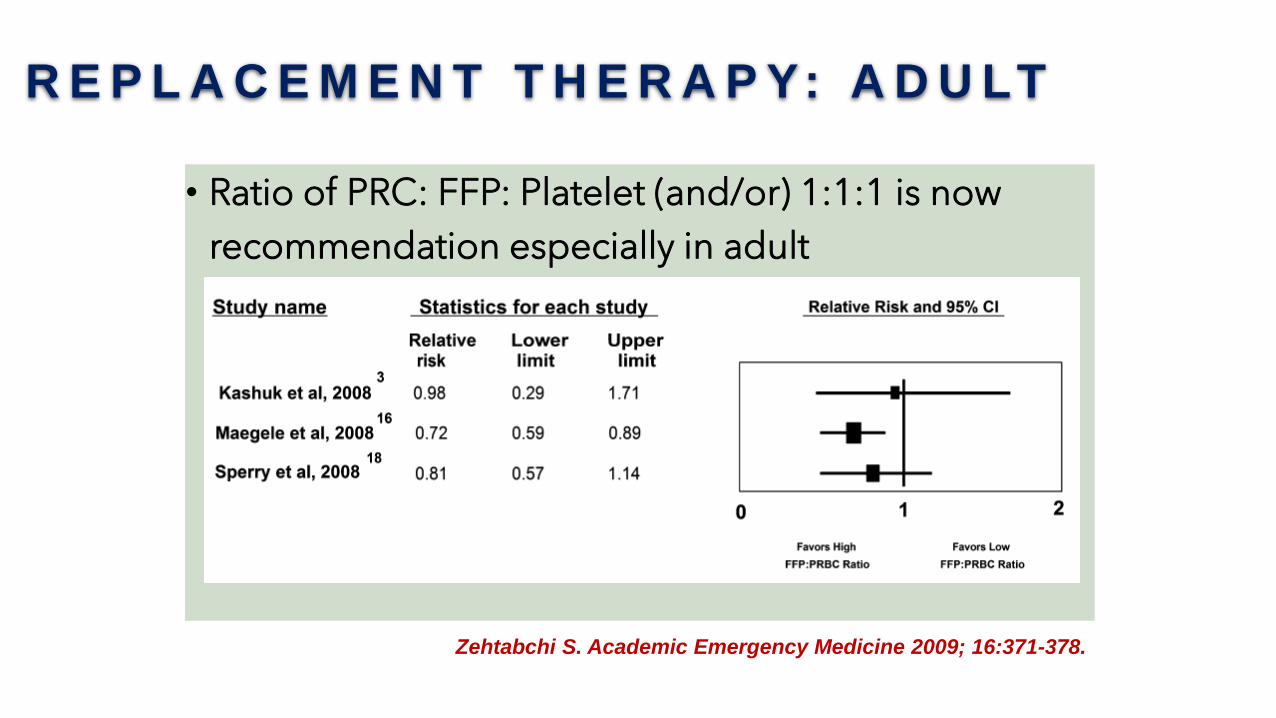
R E P L A C E M E N T T H E R A P Y: A D U LT
• Ratio of PRC: FFP: Platelet (and/or) 1:1:1 is now
recommendation especially in adult
Zehtabchi S. Academic Emergency Medicine 2009; 16:371-378.
S Y S T E M A T I C R E V I E W R E P L A C E M E N T T H E R A P Y : C H I L D R E N
• Important message
• Early use of thromboelastometry
• Ratio of transfusion (FFP:Plt:RBC) 1:1:1 or 1:1:2 did not
change the outcomes but increase FFP and plt transfusion in
lower ratio
• Ratio 1:1:1 is required when replacement is > 40 mL/Kg
• Tranexamic acid in severe trauma could reduce transfusion
requirement
Maw G Pediatr Emergency Care 2018;34:594-8
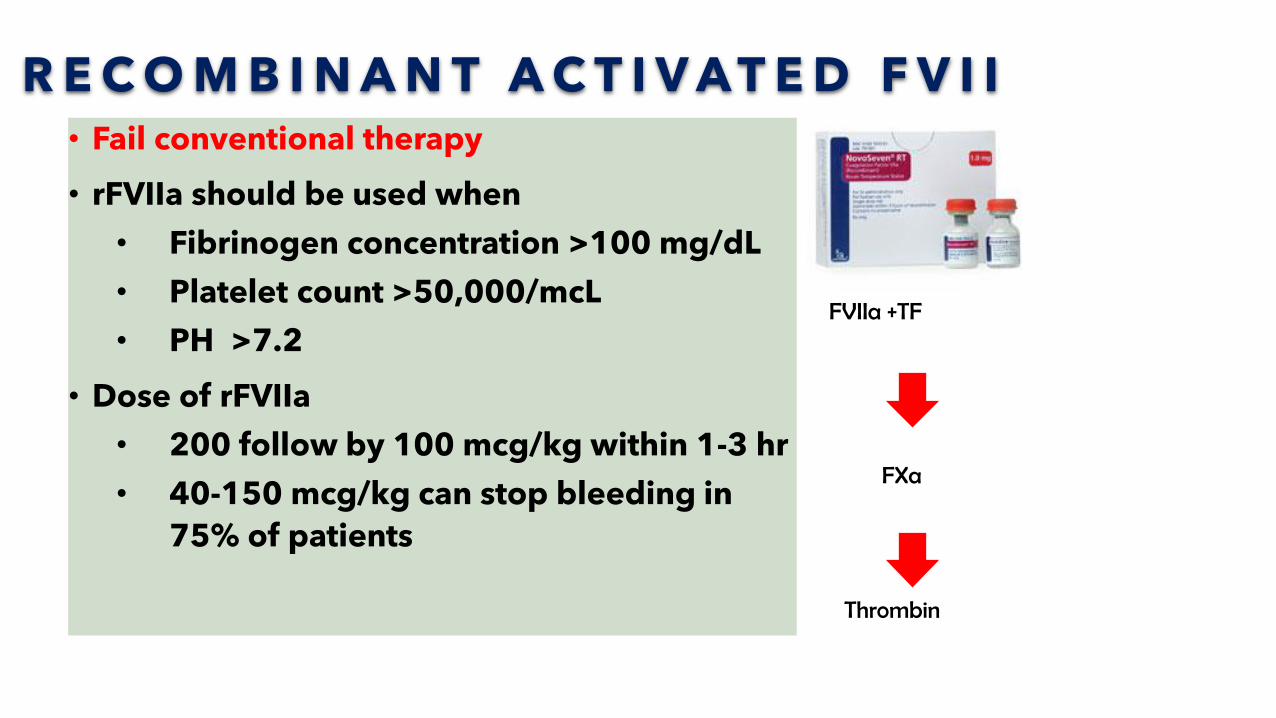
R E C O M B I N A N T A C T I V A T E D F V I I• Fail conventional therapy
• rFVIIa should be used when
• Fibrinogen concentration >100 mg/dL
• Platelet count >50,000/mcL
• PH >7.2
• Dose of rFVIIa
• 200 follow by 100 mcg/kg within 1-3 hr
• 40-150 mcg/kg can stop bleeding in
75% of patients
FVIIa +TF
FXa
Thrombin
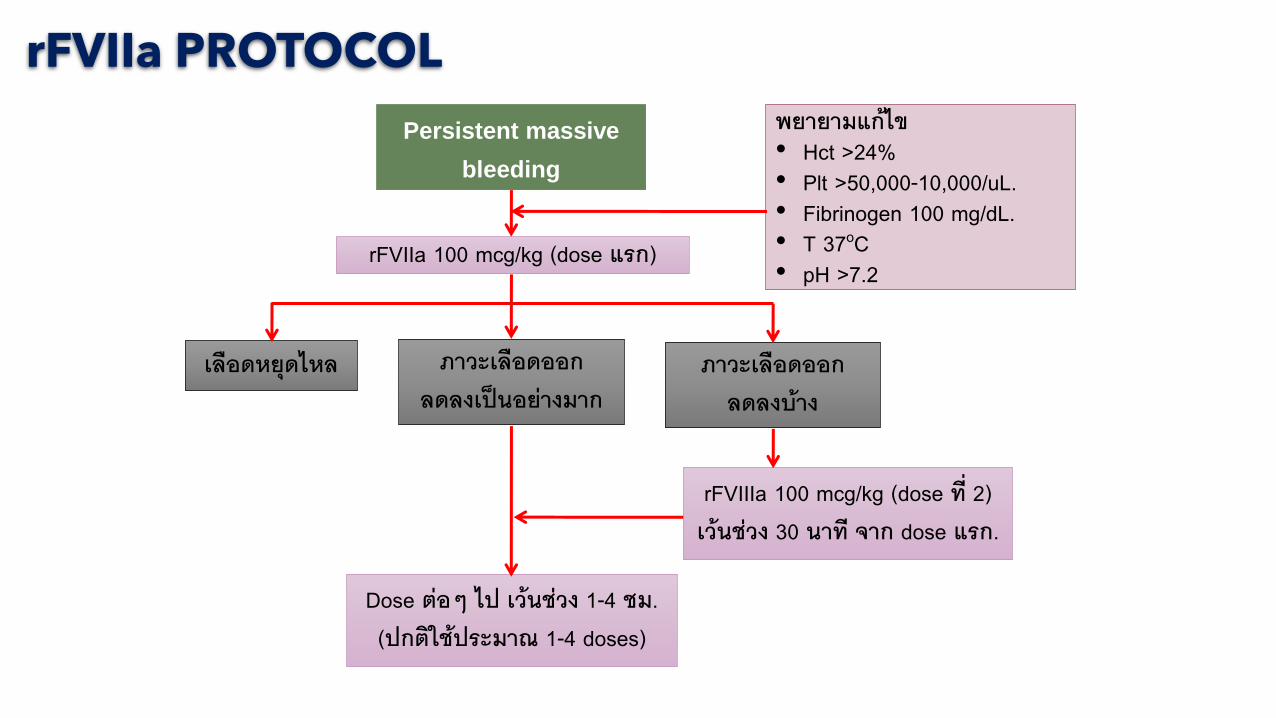
Persistent massive
bleeding
rFVIIa 100 mcg/kg (dose แรก)
เลอดหยดไหล ภาวะเลอดออกลดลงเปนอยางมาก
Dose ตอๆ ไป เวนชวง 1-4 ชม.(ปกตใชประมาณ 1-4 doses)
rFVIIIa 100 mcg/kg (dose ท 2) เวนชวง 30 นาท จาก dose แรก.
พยายามแกไข• Hct >24%• Plt >50,000-10,000/uL.• Fibrinogen 100 mg/dL.• T 37oC• pH >7.2
ภาวะเลอดออกลดลงบาง
rFVIIa PROTOCOL
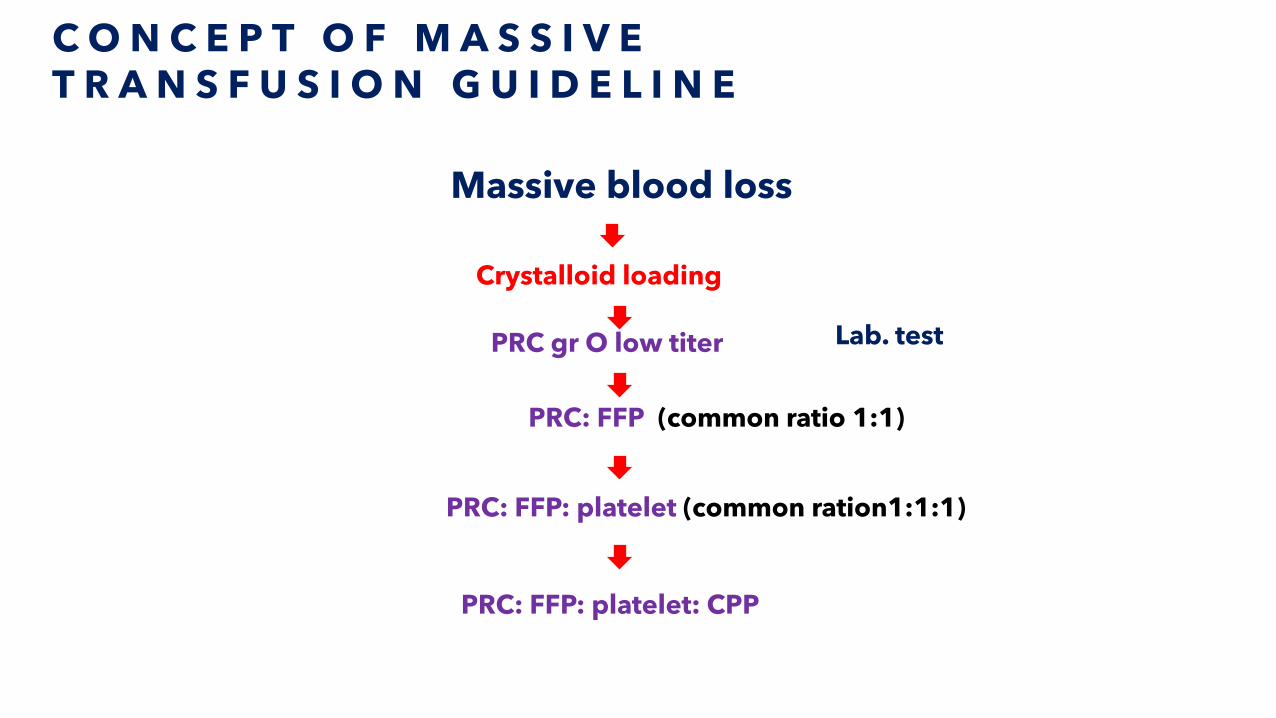
C O N C E P T O F M A S S I V E T R A N S F U S I O N G U I D E L I N E
Massive blood loss
Crystalloid loading
PRC gr O low titer
PRC: FFP (common ratio 1:1)
PRC: FFP: platelet (common ration1:1:1)
PRC: FFP: platelet: CPP
Lab. test
S U M M A R Y
• Hemostasis consists of
• Vascular, platelet, coagulation
protein
• Symptoms of suspected bleeding
disorder
• Prolonged bleeding after injury
• Excessive bleeding
• Multisystem
Common hemostasis defect
• Platelet
• Thrombocytopenia
• Dysfunction
• Coagulation
• Congenital
• Acquired
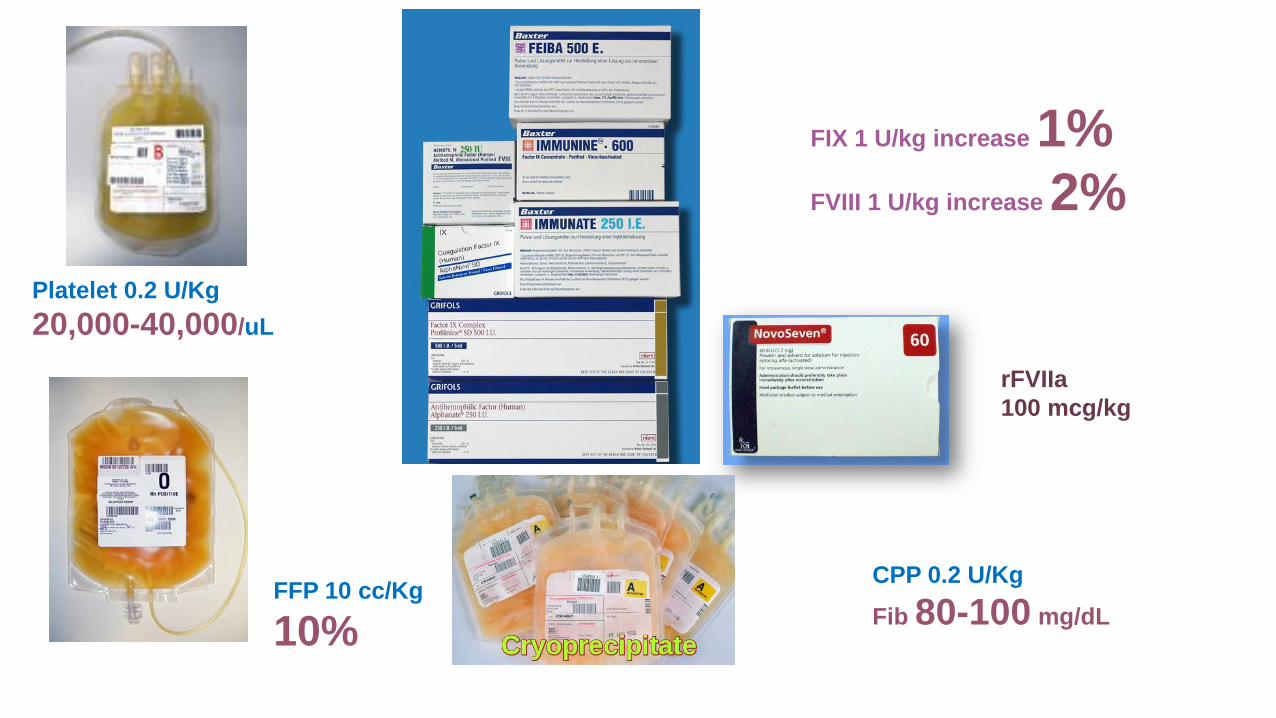
Platelet 0.2 U/Kg
20,000-40,000/uL
rFVIIa
100 mcg/kg
FIX 1 U/kg increase 1%
FVIII 1 U/kg increase 2%
FFP 10 cc/Kg
10%
CPP 0.2 U/Kg
Fib 80-100 mg/dL

THANK YOU