Embed Size (px)
Citation preview

Autism &
Asperger’s
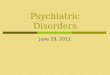
Pervasive Developmental Disorders
(PDD)
Autistic Disorder
Childhood Disintegrative Disorder
PDD-NOS
Asperger’s Disorder
Rett’s Disorder
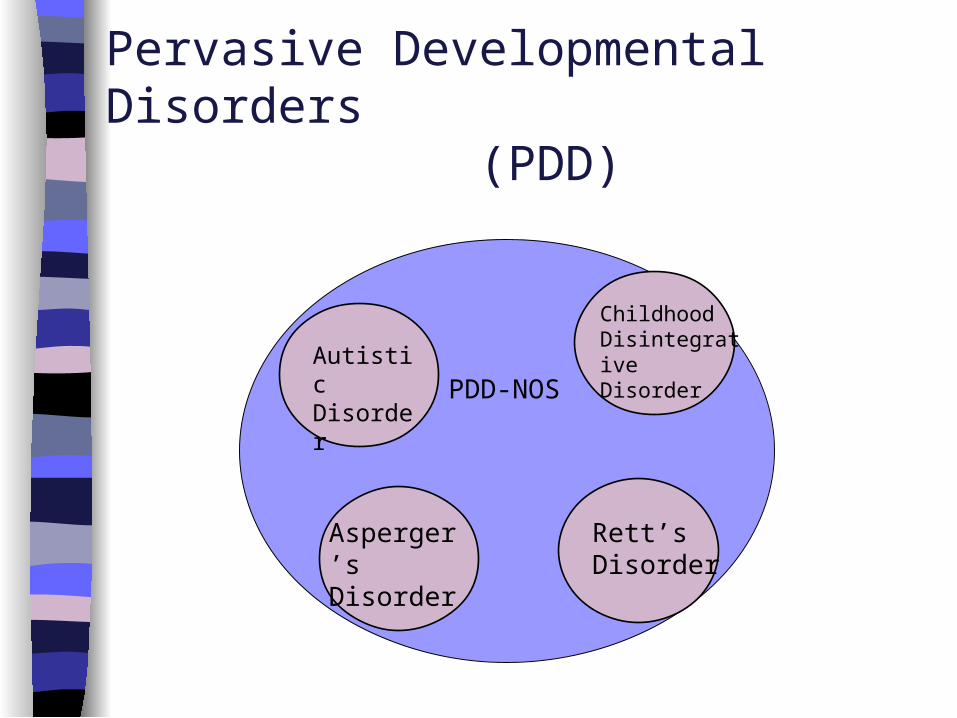
Autistic Disorder (DSM-IV)
(1) Qualitative Impairment in Reciprocal Social Interaction:
a) impaired nonverbalsb) poor peer relationshipsc) lack of spontaneous social sharingd) lack of social/emotional
reciprocity(must have 2 or more of 4)
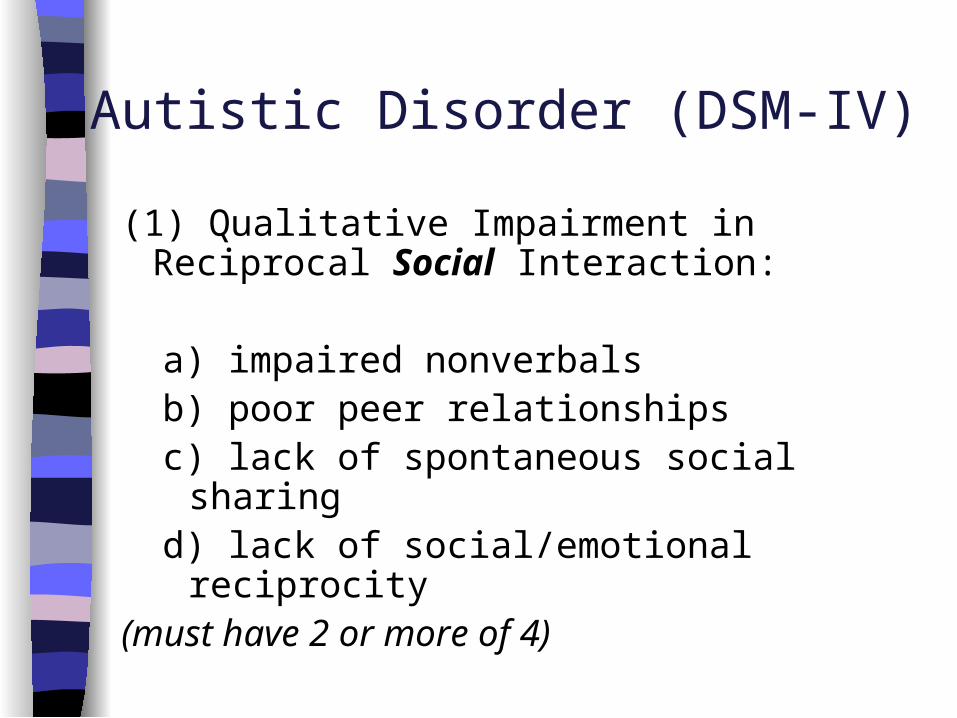
(2) Qualitative Impairment in Communication:
a) delayed/absent speech b) impaired conversational skills c) stereotyped, repetitive language d) lack of pretend and social play
(must have 1 or more of 4)
Autistic Disorder (DSM-IV)
(3) Restricted, Repetitive, & Stereotyped Patterns of Behaviour, Interests, & Activities:
a) preoccupations, narrow interestsb) adherence to routine, ritualc) stereotyped behaviourd) preoccupation with parts of objects
(must have 1 or more of 4)
Autistic Disorder (DSM-IV)
Ben Loves Trains
Ben is 2.5 and he loves trains. He is content to play with them alone for hours. Yet he doesn’t seem to really understand that they are trains. He doesn’t pretend to make them go on the track or have crashes or imagine what the cars are carrying or talk, as he plays alone. He just lines them up in the same way every time. He gets very upset if anyone rearranges his trains. Sometimes he carries a train around with him and rubs it against his chin or waves it in front of his eyes. He never brings a train to show his father, never points to the trains to show his sister. In fact, he completely ignores his sister. Ben doesn’t talk at all, rarely looks at other people and rarely smiles…
Early Behaviours in Autism:What these children often do Avoid eye contact Avoid others, appear aloof Use toys in repetitive, non-functional
ways Focus on parts of objects Tantrums/problem behaviours Odd speech (if any) Instrumental communication Autistic leading Stereotypies (e.g., flapping hands) Know familiar people
Early Behaviours in Autism:What these children often don’t do Make eye contact Imitate Pretend play Joint attention gestures (e.g., eye gaze,
pointing) Social interest and social play Use language to comment Use language for social purposes Theory of mind

Early ‘Red Flags’
no babbling 12 months no pointing, other gestures 12 months no single words 16 months no spontaneous 2-word phrases 24 months any loss of language or other skills at any
age
With younger children the absence of typical behaviour is more diagnostic than presence of atypical behaviour
Early Diagnosis
If ‘red flags’ are present, specific autism diagnostic tools are used
A diagnosis should incorporate information from various sources
A reliable & valid diagnosis can be made by age 2 by an expert clinician
Likely trend towards overdiagnosis in young delayed children and trend towards underdiagnosis in high-functioning children
Prevalence (best estimates)
Autistic Disorder 10 per 10,000
PDD-NOS 15 per 10,000 Asperger’s 2.5 per 10,000 Total 27.5 per 10,000 (1 per ~350)
Ratio 4:1 Males:Females
Is Autism Increasing? It depends…
Prevalence vs. Incidence Prevalence = % of people in the
population who have the disorder• Definitely increasing
Incidence = # of new cases per unit of time
• Debatable, no good evidence of increase
Why does is seem like autism is “increasing”?
The diagnostic criteria have broadened and changed
Much better now at early diagnosis Low functioning children can now
get a diagnosis of autism rather than just MR
At the high end of the spectrum there is more recognition of the broader phenotype
Who has autism?
No relationship to SES No relationship to immigrant status No relationship to race or ethnicity No environmental causes/clusters Some evidence of genetic
concordance
What “causes” autism? A specific cause has not been yet been identified
Current investigations specific to autism include:– birth and pregnancy problems– problems in specific areas of brain– brain chemicals (neurotransmitters)– brain infections– genetics
One single cause cannot account for everything/all subtypes of PDD
We do know that it is NOT parents
Is there a “cure”?...New & Alternative Treatments Auditory Training Sensory Integration Vitamins/Food Supplements Special Diets/Food Allergies, Sensitivities Physical Exercise Holding Therapy Deep Pressure Facilitated Communication Miller Method Irlen Lenses Patterning Gentle Teaching Swimming with Dolphins Secretin Centrifugal Therapy …
New & Alternative Treatments The problem is that most of these
treatments are not supported by any research
Many parents believe in “miracle” or “breakthrough” “cures”– Gives them hope– Feel less helpless– Danger in not accepting the child as he/she
is– Expensive

Intensive Behavioural Intervention
(IBI) “Intensive” (often 20-40 hrs/wk for 1-2
yrs.) Begin early (usually before 4) Schedule is highly structured
and predictable Program is individualized Specific teaching methods vary Include complex variety of techniques to
promote independence and generalization
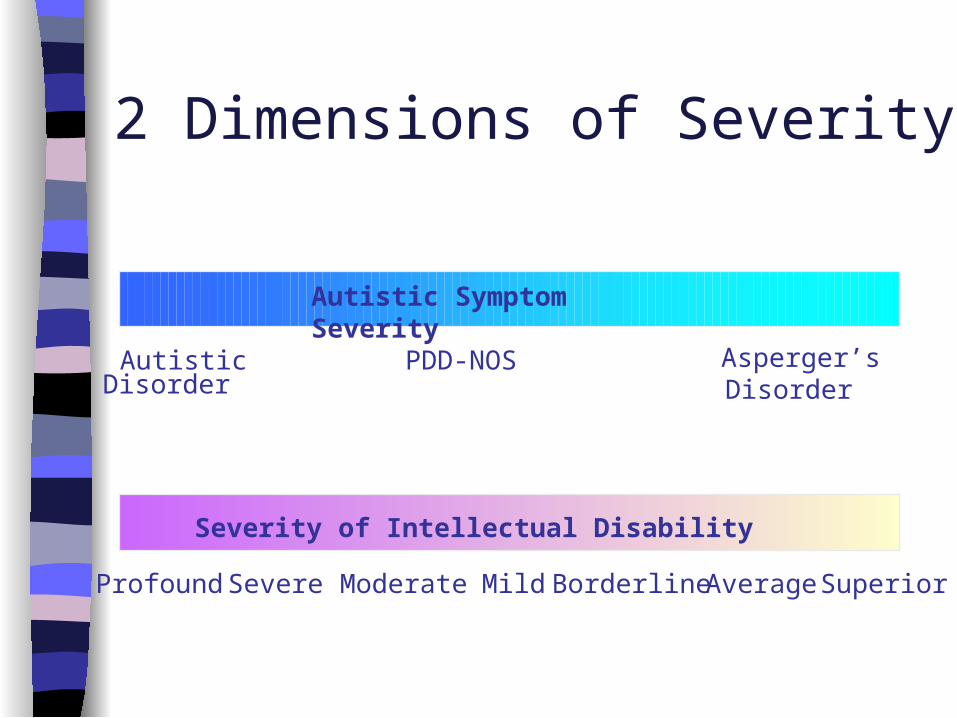
2 Dimensions of Severity
AutisticDisorder
PDD-NOS Asperger’sDisorder
Autistic Symptom Severity
Profound Severe Moderate SuperiorAverage
Severity of Intellectual Disability
Mild Borderline
Carolyn Just Wants to Be FriendsCarolyn is 12 and is great at puzzles. She can do them just as fast whether they are picture side up or upside down! She struggles with her school work, especially language arts and social studies, but is pretty good at spelling and math and has an excellent memory. She was in special education classes when she was younger, but is now in a regular class. She seems very friendly and talkative, though a bit immature. She goes up and asks questions of anyone she comes in contact with, even if they’re not interested in talking to her. She doesn’t know how to relate to other kids very well but really wants to be friends. She is enrolled in a social skills group at a local treatment agency. Her mother worries about what is in store for Carolyn as a teenager and adult…
Asperger’s Disorder (DSM-IV)
A. Qualitative Impairment in Reciprocal Social Interaction:
a) impaired nonverbalsb) poor peer relationshipsc) lack of spontaneous social
sharingd) lack of social/emotional
reciprocity(must have 2 or more of 4)

Asperger’s Disorder (DSM-IV)
B. Restricted, Repetitive, and Stereotyped Patterns of Behaviour, Interests, and Activities:
a) preoccupations, narrow interestsb) adherence to routine, ritualc) stereotyped behaviourd) preoccupation with parts of objects
(must have 1 or more of 4 criteria)
Asperger’s Disorder (DSM-IV)
C. Clinically significant impairment in social, occupational functioning
D. No clinically significant language delay
E. No clinically significant cognitive delay, adaptive behaviour
Prevalence
Prevalence ranges:– 3-4 in every 1000 children develop the full
clinical picture of AS – 2.5 per 10,000
Why is there such a range?– No consistent diagnostic criteria for AS
6:1 Male to Female ratio– Actual ratio is believed to be closer to 4:1

Other difficulties associated with Asperger’s IQ profile Communication problems affecting speech
and language– Language “oddities”:
• Hyperlexia• Literal use and understanding of language• Pragmatic difficulties• Flat prosody
Perceptual problems Motor control problems
Comorbidity ADHD Tics and Tourette Syndrome Anxiety
– Social anxiety– OCD
Conduct disorder Eating disorders Mood Disorders
– Depression (most common secondary diagnosis)
– Bipolar– Suicidal ideation
Alcohol and Drug abuse Schizophrenia & isolated psychotic episodes
Interventions for Asperger’s Not one specific empirically validated
treatment (like IBI for Autism)
Social skill groups
School interventions
Medications– often used to treat comorbid conditions– have to watch for atypical reactions to
the drugs• e.g., SSRIs, Neuroleptic, Stimulants, Anti-epileptic
drugs, Lithium

Summary Autism and Asperger’s are two of the Pervasive
Developmental Disorders Children with Autism must show impairments in
social and communication abilities as well as have behavioural concerns to receive a diagnosis
Children with Asperger’s must show impairments in their social abilities and specific behavioural concerns, but do not show language impairments like children with Autism
The prevalence of Autism/Asperger’s is increasing, although perhaps not the incidence
The “cause” of Autism/Asperger’s is still unknown There is currently no “cure” for Autism or for
Asperger’s IBI is the current intervention of choice for children
with Autism









![ADOPTED REGULATION OF THE STATE BOARD OF EDUCATION … · 2010-05-07 · disorder, [aspeger’s] asperger’s disorder, atypical autism, pervasive developmental disorder and other](https://img.pdfslide.us/doc/110x75/5fb827387372d9390e7ce909/adopted-regulation-of-the-state-board-of-education-2010-05-07-disorder-aspegeras.jpg)