Embed Size (px)
Citation preview

*Corresponding author email: [email protected] Group
Symbiosis www.symbiosisonline.org www.symbiosisonlinepublishing.com
Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of
LiteraturesGetinet Ayano*
Research and Training Department, Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia
SOJ Psychology Open AccessReview article
unipolar disorder by including manic states. No matter how many times a patient is depressed; only one manic/hypomanic episode is required to diagnose bipolar rather than unipolar disorder. Bipolar disorder is further characterized as type I or type II. Type I is diagnosed when at least one manic episode is identified. Usually recurrent depression also occurs, but in 5 to 10 percent of cases there are no diagnosable major depressive episodes, although almost always there will be minor depressive episodes. Bipolar disorder type II requires the absence of even one manic episode, and instead the occurrence of at least one hypomanic episode and at least one major depressive episode. The critical difference between mania and hypomania, in current DSM-V nosology, is that mania requires significant social and occupational dysfunction, while in hypomania significant social and occupational dysfunction needs to be excluded. Durational criteria are less strict for hypomania (a minimum of 4 days) than for mania (a minimum of 1 week) [1].
Bipolar disorder is common and disabling [2]. The hallmark of the disorder is mood elevation (mania or hypomania) [1]. Patients with bipolar I disorder have episodes of mania and nearly always experience major depressive episodes. Patients with bipolar II disorder suffer both hypomanic episodes and major depressive episodes.
It is one of the most severe of the psychiatric disorders. Bipolar disorder is among the most disabling and economically catastrophic medical disorders, ranked by the World Health Organization as one of the common illnesses contributing to the global burden of disease [3].
It carries a lifetime risk of around 2.6–7.8%, and its early onset and tendency to chronicity mean that its prevalence is relatively high. The social and economic impact of the illness is enormous, and its impact on sufferers and their families can be devastating [4, 5].
Bipolar disorder is a clinical diagnosis. It must be differentiated from other psychiatric and medical illnesses, as well as from disorders such as heavy metal toxicity, adverse effects of drugs, and vitamin deficiencies [1].
Received: September 30, 2016; Accepted: December 16, 2016; Published: December 28, 2016
*Corresponding author: Getinet Ayano, chief psychiatry professional and mhGap coordinator at Research and Training Department, Amanuel Mental Special-
ized Hospital, Addis Ababa, PO box: 1971 Ethiopia, Tel:+251927172968; E-mail: [email protected]
BackgroundBipolar disorder is characterized by manic or hypomanic
states: the patient is either depressed, euthymic (normal in mood), or hypomanic/manic. Bipolar disorder differs from
AbstractBipolar affective disorder, or manic depressive Illness (MDI), is
a common, severe, and persistent Mental illness. This condition is a serious lifelong struggle and challenge. Bipolar affective disorder is characterized by periods of deep, prolonged, and profound depression that alternate with periods of an excessively elevated or irritable mood known as mania. Only one manic/hypomanic episode is required to diagnose bipolar rather than unipolar disorder. Bipolar disorder is further characterized as type I or type II. Type I is diagnosed when at least one manic episode is identified.
Bipolar disorder occurs in approximately 1 percent of the population. Bipolar II disorder and Bipolar disorder not otherwise specified (NOS) account for another 2.5 percent of the population. Bipolar disorder is almost always recurrent and can be associated with severe illness-related Morbidity and increased medical mortality. About 10 to 20 percent of patients with bipolar disorder die of their illness by suicide.
Bipolar disorder is equally prevalent in men and women. It has an early age onset. The most common age of onset of bipolar disorder is 1721 years. It is a highly disabling illness, and in fact a study.
Bipolar disorder is caused by bio psychosocial influences including genetic, perinatal, neuroanatomic, neurochemical and other biologic abnormalities. In addition psychological and socio environmental factors are associated with a greater risk of bipolar disorders. The role of genes in the susceptibility to mood disorders has long been supported by family, twin, and adoption studies. That mood disorders run in families is a common observation of patients and clinicians. However, genes clearly only contribute a predisposition that must interact with environmental factors in order to cause disease.
Treatment of bipolar disorders requires an integration of medical, psychological, and psychosocial inputs.
Keywords: Bipolar; Mania; Hypomania; Cyclothymia; Mood Stabilizers; Psychotherapy;

Page 2 of 8Citation: Ayano G (2016) Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures. SOJ Psychol 3(1): 1-8.
Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures
Copyright: © 2016 Ayano
Treatment of bipolar disorders requires an integration of medical, psychological, and psychosocial inputs. The bulk of care occurs in an outpatient setting and is best carried out by a multidisciplinary team. Psychosocial rehabilitation is an essential part of treatment [1].
Etiology of bipolar disordersResearch has identified several factors that contribute to the
risk of developing bipolar disorders. Bipolar disorder is a disease caused by biopsychosocial influences including genetic, perinatal, neuroanatomic, neurochemical and other biologic abnormalities. In addition psychological and socio environmental factors are associated with a greater risk of bipolar disorders [6, 7, 8].
Genetic factors
Different studies indicated that bipolar disorders have high genetic transmission risks. Some of evidences for genetic transmission of bipolar disorders are:
Family Studies: Studies indicate that bipolar disorders run in families. First degree relatives of people with bipolar I disorder are approximately 7 times more likely to develop bipolar I disorder than the general population. Remarkably, offspring of a parent with bipolar disorder have a 50% chance of having another major psychiatric disorder. One longitudinal study found that sub threshold manic or hypomanic episodes were a diagnostic risk factor for the development of subsequent manic, mixed, or hypomanic episodes in the offspring of parents with bipolar disorder. In fact, unipolar disorder is typically the most common form of mood disorder in families of bipolar probands. However, the rate of bipolar disorder is only slightly elevated in the families of unipolar probands. This familial overlap suggests some degree of common genetic underpinnings between these two forms of mood disorder [6].
Twin Studies: Twins who are reared together share the same environment, but monozygotic (MZ) twins share all their genes, while Dizy Gotic (DZ) twins share on average only 50 percent. Twin studies compare the concordance rates in MZ and DZ twins. The concordance rate refers to the proportion of co-twins who are also affected or to the proportion of twin pairs where both twins are affected. Twin studies demonstrate a concordance of 3390% for bipolar I disorder in identical twins. As identical twins share 100% of their DNA, these studies also show that environmental factors are involved, and there is no guarantee that a person will develop bipolar disorder, even if they carry susceptibility genes [7, 8].
Adoption Studies: Adoption studies provide an alternative approach to separating genetic and environmental factors in familial transmission. Adoption studies have been conducted using a variety of experimental designs, but the most common is the adoptee as proband strategy. In this approach, probands are identified who have a mood disorder and were adopted at birth. Through this event, nature is separated from nurture. The rates of psychiatric illness are then determined in both the biological and adoptive parents. Numerous adoption studies prove that a common environment is not the only factor that makes bipolar
disorder occur in families. Children whose biologic parents have either bipolar I disorder or a major depressive disorder remain at increased risk of developing an affective disorder, even if they are reared in a home with adopted parents who are not affected [7,8].
Linkage Studies: Numerous linkage studies of bipolar disorder have implicated many different chromosomal regions. Bipolar disorder, especially bipolar type I (BPI) disorder, has a major genetic component, with the involvement of the ANK3, CACNA1C, and CLOCK genes [9, 15]. The evidence indicating a genetic role in bipolar disorder takes several forms.
Pregnancy and Birth Complications (Perinatal factors)
An association between obstetric complications, structural brain abnormality and early onset schizophrenia has been reported in a number of investigations [16, 17] and reviewed recently [12]. Although broadly defined or apparently unrelated, obstetric complications may share a common pathophysiology, namely foetal hypoxia [18]. Studies have demonstrated that patients with bipolar disorder have increased rates of obstetric complications and this was associated with an early illness onset [19]. By contrast, little research has been carried out into the relationship between obstetric complications and age of onset of bipolar affective disorder. However, increased risks of perinatal birth complications have also been reported in bipolar disorder [20-25]. The significance of such findings in the causation of bipolar disorder is still unclear; Scott’s review and metanalysis of literature [24] failed to find a significant association between obstetric complications and bipolar disorder.
Neurotransmitters (Biochemical factors)
Multiple biochemical pathways likely contribute to bipolar disorder, which is why detecting one particular abnormality is difficult. A number of neurotransmitters have been linked to this disorder, largely based on patients’ responses to psychoactive agents as in the following examples. The blood pressure drug reserpine, which depletes catecholamines from nerve terminals, was noted incidentally to cause depression. This led to the catecholamine hypothesis, which holds that an increase in epinephrine and nor epinephrine causes mania and a decrease in epinephrine and nor epinephrine causes depression. Drugs used to treat depression and drugs of abuse (e.g., cocaine) that increase levels of monoamines, including serotonin, nor epinephrine, or dopamine, can all potentially trigger mania, implicating all of these neurotransmitters in its etiology. Other agents that exacerbate mania include L-dopa, which implicates dopamine and serotoninre uptake inhibitors, which in turn implicate serotonin. Evidence is mounting of the contribution of glutamate to both bipolar disorder and major depression. A postmortem study of the frontal lobes of individuals with these disorders revealed that the glutamate levels were increased [26].
Recent life events and bipolar disorder (Environmental factors)
Overall, studies of life events have found that bipolar individuals experience increased stressful events prior to first onset and recurrences of mood episodes. Moreover,

Page 3 of 8Citation: Ayano G (2016) Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures. SOJ Psychol 3(1): 1-8.
Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures
Copyright: © 2016 Ayano
most studies have found that negative life events precede the manic/hypomanic as well as the depressive episodes of bipolar individuals. Numerous studies indicate that from 20% to 66% of bipolar patients experienced at least one stressful event rated as independent of their behavior in the 1–3month period prior to onset of a mood episode . In additions psychosocial stressors are the major causes of relapse in bipolar patients [27, 28].
EpidemiologyGlobal prevalence of Bipolar disorder
Bipolar disorder was equated with classic manic depressive (i.e., bipolar I) disorder, and the lifetime prevalence of bipolar disorder was found to be approximately 1%. However, if the diagnosis of bipolar II disorder (major depression with hypomania, but not with mania) is much higher lifetime prevalence rates of the broadly defined bipolar disorders, up to at least 5%, were reported. The recent results of the National Co morbidity Survey Replication has shown that the lifetime prevalence estimates were Studies also indicate differences in lifetime prevalence estimates for bipolar disorder type I (BPI) (1.0%), bipolar disorder type II (BPII) (1.1%), and sub threshold bipolar disorders (2.44.7%)[29].
Socio demographic factors
The gender ratio in bipolar disorder (all subtypes combined) is approximately 1:1. However, among bipolar II patients and in special subpopulations (mixed/dysphoric mania, mixed depressive episode, winter depression, bipolar depression with atypical clinical features, and rapid cycling bipolar disorder), women are overrepresented. Looking at the depression–mania continuum as a whole spectrum, there is a clear trend: The higher the depressive component, the higher the proportion of women. Consequently, in the rare cases of unipolar mania (manic episode without any major or minor depression), men are markedly overrepresented. The gender differences in lifetime prevalence rates are more marked than in 1year and current prevalence rates, which may be attributable—at least in part—to the stronger male tendency to forget previous episodes and deny emotionally negative events [30].
Diagnosing of bipolar disorders (Current Diagnostic Criteria- DSM-5)
Seven bipolar disorder categories are included in DSMV: bipolar I disorder, bipolar II disorder, cyclothymic disorder, substance/medication induced bipolar and related disorder, bipolar and related disorder due to another medical condition, other specified bipolar and related disorder, and unspecified bipolar and related disorder [1].
Bipolar I disorder
The bipolar I disorder criteria represent the modern understanding of the classic manic depressive disorder or affective psychosis described in the nineteenth century, differing from that classic description only to the extent that neither psychosis nor the lifetime experience of a major depressive episode is a requirement. However, the vast majority of individuals whose
symptoms meet the criteria for a fully syndromal manic episode also experience major depressive episodes during the course of their lives (table 1).
Bipolar II disorder
Bipolar II disorder, requiring the lifetime experience of at least one episode of major depression and at least one hypomanie episode, is no longer thought to be a “milder” condition than bipolar I disorder, largely because of the amount of time individuals with this condition spend in depression and because the instability of mood experienced by individuals with bipolar II disorder is typically accompanied by serious impairment in work and social functioning (table 2.)
Cyclothymic disorder
The diagnosis of cyclothymic disorder is given to adults who experience at least 2 years (for children, a full year) of both hypomanie and depressive periods without ever fulfilling the criteria for an episode of mania, hypomania, or major depression (table 3).
Management of bipolar disordersAlthough mood stabilizers are the mainstay of the treatment
for bipolar disorders, research has found that psychosocial interventions, including psychotherapy, can augment the clinical improvement. Just as pharmacological agents are used to treat presumed chemical imbalances, no pharmacological strategies must treat no biological issues. The complexity of bipolar disorders usually renders any single therapeutic approach inadequate to deal with the multifaceted disorder. Psychosocial modalities should be integrated into the drug treatment regimen and should support it. Patients with bipolar disorders benefit more from the combined use of mood stabilizers and psychosocial treatment than from either treatment used alone [36].
Pharmacological managements
A number of medications are used to treat bipolar disorder [31, 39] including:
• Mood stabilizers
• Anti-psychotics
• Anti-depressants
• Anti-anxiety medications
Most people with bipolar I or bipolar II will need mood stabilizers to control their manic or Hypomanic episodes. Commonly used moods stabilizers include:
• Tegretol (carbamazepine)
• Depakote (divalproex sodium., valproic acid)
• Lamictal (lamotrigine)
• Lithobid (lithium)
Antipsychotic drugs may also be used to control episodes of depression or mania, especially when delusions or hallucinations

Page 4 of 8Citation: Ayano G (2016) Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures. SOJ Psychol 3(1): 1-8.
Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures
Copyright: © 2016 Ayano
Table 1: DSM-V Diagnostic Criteria for bipolar I disorderDSM-V Diagnostic Criteria for bipolar I disorderFor a diagnosis of bipolar I disorder, it is necessary to meet the following criteria for a manic episode. The manic episode may have been preceded by and may be followed by hypomanic or major depressive episodes.Manic EpisodeA. A distinct period of abnormally and persistently elevated, expansive, or irritable mood and abnormally and persistently increased goal directed activity or energy, lasting at least 1 Week and present most of the day, nearly every day (or any duration if hospitalization is necessary).B. During the period of mood disturbance and increased energy or activity, three (or more) of the following symptoms (four if the mood is only irritable) are present to a significant degree and represent a noticeable change from usual behavior:1. Inflated self esteem or grandiosity.2. Decreased need for sleep (e.g., feels rested after only 3 hours of sleep).3. More talkative than usual or pressure to keep talking.4. Flight of ideas or subjective experience that thoughts are racing.5. Distractibility (i.e., attention too easily drawn to unimportant or irrelevant external stimuli), as reported or observed.6. Increase in goal directed activity (either socially, at work or school, or sexually) or psychomotor agitation (i.e., purposeless non goal directed activity).7. Excessive involvement in activities that have a high potential for painful consequence (e.g., engaging in unrestrained buying sprees, sexual indiscretions, or foolish business investments).C. The mood disturbance is sufficiently severe to cause marked impairment in social or occupational functioning or to necessitate hospitalization to prevent harm to self or others, or there are psychotic features.D. The episode is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication, other treatment) or to another medical condition.Note: A full manic episode that emerges during antidepressant treatment (e.g., medication, electroconvulsive therapy) but persists at a fully syndromal level beyond the physiological effect of that treatment is sufficient evidence for a manic episode and, therefore, a bipolar I diagnosis.Major Depressive EpisodeA. Five (or more) of the following symptoms have been present during the same 2 week period and represent a change from previous functioning; at least one of the symptoms is either(1) Depressed mood or (2) loss of interest or pleasure.Note: Do not include symptoms that are clearly attributable to another medical condition.1. Depressed mood most of the day, nearly every day, as indicated by either subjective report (e.g., feels sad, empty, or hopeless) or observation made by others (e.g., appears tearful). Note: In children and adolescents, can be irritable mood.2. Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day (as indicated by either subjective account or observation).3. Significant weight loss when not dieting or weight gain (e.g., a change of more than5% of body weight in a month), or decrease or increase in appetite nearly every day. Note: In children, consider failure to make expected weight gain.4. Insomnia or hypersomnia nearly every day.5. Psychomotor agitation or retardation nearly every day (observable by others; not merely subjective feelings of restlessness or being slowed down).6. Fatigue or loss of energy nearly every day.7. Feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day (not merely self reproach or guilt about being sick).8. Diminished ability to think or concentrate, or indecisiveness, nearly every day (either by subjective account or as observed by others).9. Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.B. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.C. The episode is not attributable to the physiological effects of a substance or another medical condition.Note: Criteria A constitute a major depressive episode. Major depressive episodes are common in bipolar I disorder but are not required for the diagnosis of bipolar I disorder.Note: Responses to a significant loss (e.g., bereavement, financial ruin, losses from va natural disaster, a serious medical illness or disability) may include the feelings of intense sadness, rumination about the loss, insomnia, poor appetite, and weight loss noted in Criterion A, which may resemble a depressive episode. Although such symptoms may be understandable or considered appropriate to the loss, the presence of a major depressive episode in addition to the normal response to a significant loss should also be carefully considered. This decision inevitably requires the exercise of clinical judgment based on the individual’s history and the cultural norms for the expression of distress in the context of loss.Bipolar I DisorderA. Criteria have been met for at least one manic episode (Criteria AD under “Manic Episode” above).B. The occurrence of the manic and major depressive episode(s) is not better explained by schizoaffective disorder, schizophrenia, schizophreniform disorder, delusional disorder, or other specified or unspecified schizophrenia spectrum and other psychotic disorder.
are occurring. Examples of drugs in this class include:
• Abilify (aripiprazole)
• Saphris (asenapine)
• Symbyax (olanzapine and fluoxetine)
Page 5 of 8Citation: Ayano G (2016) Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures. SOJ Psychol 3(1): 1-8.
Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures
Copyright: © 2016 Ayano
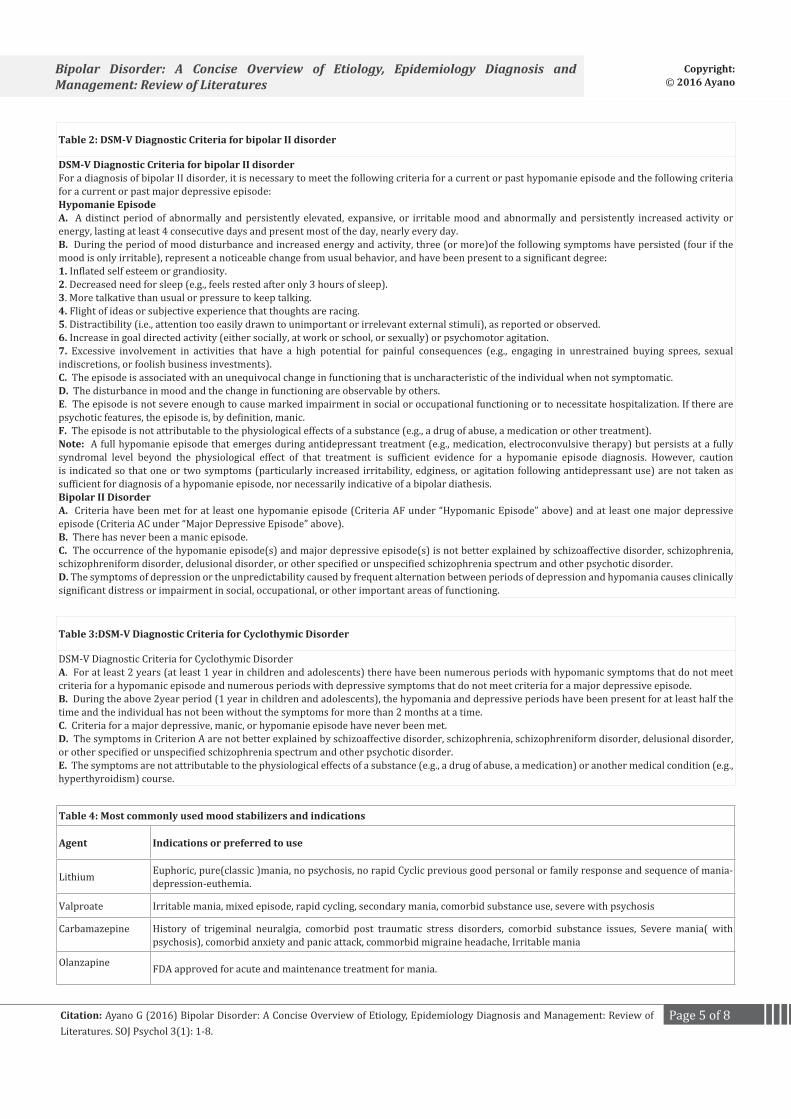
Table 2: DSM-V Diagnostic Criteria for bipolar II disorder
DSM-V Diagnostic Criteria for bipolar II disorderFor a diagnosis of bipolar II disorder, it is necessary to meet the following criteria for a current or past hypomanie episode and the following criteria for a current or past major depressive episode:Hypomanie EpisodeA. A distinct period of abnormally and persistently elevated, expansive, or irritable mood and abnormally and persistently increased activity or energy, lasting at least 4 consecutive days and present most of the day, nearly every day.B. During the period of mood disturbance and increased energy and activity, three (or more)of the following symptoms have persisted (four if the mood is only irritable), represent a noticeable change from usual behavior, and have been present to a significant degree:1. Inflated self esteem or grandiosity.2. Decreased need for sleep (e.g., feels rested after only 3 hours of sleep).3. More talkative than usual or pressure to keep talking.4. Flight of ideas or subjective experience that thoughts are racing.5. Distractibility (i.e., attention too easily drawn to unimportant or irrelevant external stimuli), as reported or observed.6. Increase in goal directed activity (either socially, at work or school, or sexually) or psychomotor agitation.7. Excessive involvement in activities that have a high potential for painful consequences (e.g., engaging in unrestrained buying sprees, sexual indiscretions, or foolish business investments).C. The episode is associated with an unequivocal change in functioning that is uncharacteristic of the individual when not symptomatic.D. The disturbance in mood and the change in functioning are observable by others.E. The episode is not severe enough to cause marked impairment in social or occupational functioning or to necessitate hospitalization. If there are psychotic features, the episode is, by definition, manic.F. The episode is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication or other treatment).Note: A full hypomanie episode that emerges during antidepressant treatment (e.g., medication, electroconvulsive therapy) but persists at a fully syndromal level beyond the physiological effect of that treatment is sufficient evidence for a hypomanie episode diagnosis. However, caution is indicated so that one or two symptoms (particularly increased irritability, edginess, or agitation following antidepressant use) are not taken as sufficient for diagnosis of a hypomanie episode, nor necessarily indicative of a bipolar diathesis.Bipolar II DisorderA. Criteria have been met for at least one hypomanie episode (Criteria AF under “Hypomanic Episode” above) and at least one major depressive episode (Criteria AC under “Major Depressive Episode” above).B. There has never been a manic episode.C. The occurrence of the hypomanie episode(s) and major depressive episode(s) is not better explained by schizoaffective disorder, schizophrenia, schizophreniform disorder, delusional disorder, or other specified or unspecified schizophrenia spectrum and other psychotic disorder.D. The symptoms of depression or the unpredictability caused by frequent alternation between periods of depression and hypomania causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Table 3:DSM-V Diagnostic Criteria for Cyclothymic Disorder
DSM-V Diagnostic Criteria for Cyclothymic DisorderA. For at least 2 years (at least 1 year in children and adolescents) there have been numerous periods with hypomanic symptoms that do not meet criteria for a hypomanic episode and numerous periods with depressive symptoms that do not meet criteria for a major depressive episode.B. During the above 2year period (1 year in children and adolescents), the hypomania and depressive periods have been present for at least half the time and the individual has not been without the symptoms for more than 2 months at a time.C. Criteria for a major depressive, manic, or hypomanie episode have never been met.D. The symptoms in Criterion A are not better explained by schizoaffective disorder, schizophrenia, schizophreniform disorder, delusional disorder, or other specified or unspecified schizophrenia spectrum and other psychotic disorder.E. The symptoms are not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition (e.g., hyperthyroidism) course.
Table 4: Most commonly used mood stabilizers and indications
Agent Indications or preferred to use
Lithium Euphoric, pure(classic )mania, no psychosis, no rapid Cyclic previous good personal or family response and sequence of mania-depression-euthemia.
Valproate Irritable mania, mixed episode, rapid cycling, secondary mania, comorbid substance use, severe with psychosis
Carbamazepine History of trigeminal neuralgia, comorbid post traumatic stress disorders, comorbid substance issues, Severe mania( with psychosis), comorbid anxiety and panic attack, commorbid migraine headache, Irritable mania
Olanzapine FDA approved for acute and maintenance treatment for mania.

Page 6 of 8Citation: Ayano G (2016) Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures. SOJ Psychol 3(1): 1-8.
Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures
Copyright: © 2016 Ayano
• Latuda (lurasidone)
• Zyprexa (olanzapine)
• Seroquel (quetiapine)
• Risperdal (risperidone)
• Geodon (ziprasidone)
An antidepressant may also be used to manage depressive episodes, in conjunction with a mood stabilizer or an antipsychotic.
Finally, Benzodiazepines Diazepam, Lorazepam, Clonazepam or another type of anti anxiety medication may be used.
Psychosocial interventions
Psycho education and more formal psychotherapy can improve outcome when used in conjunction with maintenance pharmacotherapy. Adjunctive psychosocial therapies should be considered early in the course of illness to improve medication adherence, identify prodromes of relapse, decrease residual symptoms (particularly depressive) and suicidal behavior, and help move patients towards a comprehensive functional recovery [40–46]. For bipolar disorders Psychological and social (psychosocial) interventions are important in addition to continuing on medication. These may include:
Psycho education: Psycho educational interventions include any discrete programme involving interaction between an information provider and service users or their careers which has the primary aims of offering information about the condition and the provision of support and management strategies. Complex psycho education was defined as any group programme involving an explicitly described educational interaction between the information provider and the patient/carer as the prime focus of the intervention [47, 48]. Patients/carers should be provided with information, support and different management strategies, including: illness awareness, treatment compliance, early detection of prodromal symptoms and relapse, lifestyle regularity.
Cognitive behavioral therapy (CBT): A structured and collaborative therapeutic approach, CBT is a discrete psychological intervention which aims to make explicit connections between thinking, emotions, physiology and behavior with respect to current or past problems, primarily through behavioral experiments and guided discovery. CBT seeks to achieve systemic change through the reevaluation of perceptions, beliefs or reasoning thought to cause and maintain psychological problems. The aim is to help the individual normalize and make sense of their psychotic experiences, and to reduce the associated distress and impact on functioning. Targeted outcomes include symptom reduction, relapse reduction, enhancement of social functioning, development of insight, amelioration of distress, and the promotion of recovery [49, 50].
Family intervention: Family intervention is a discrete psychological intervention with a specific supportive, educational or treatment function which involves problem solving/crisis
management and/or intervention with the identified service user. Family intervention for individuals diagnosed with bipolar disorder has developed out of the consistent finding that the emotional environment within a family was an effective predictor of relapse. In this context, ‘family’ includes people who have a significant emotional connection to the individual, such as parents, siblings and partners. Different models of family intervention aim to help families cope with their relative’s problems more effectively, provide support and education for the family, reduce levels of distress, improve the ways in which the family communicates and negotiates problems, and try to prevent relapse by the service user [51]. Family sessions with a specific supportive or treatment function based on systemic, cognitive behavioral or psychoanalytic principles, which must contain at least one of the following psycho educational intervention, problem solving/crisis management work and intervention with the identified patient.
Interpersonal and social rhythm therapy (IPSRT): Interpersonal and social rhythm therapy (IPSRT) was defined as discrete, time limited, structured psychological intervention derived from an interpersonal model of affective disorders [52, 53]. It focuses on:
• Working collaboratively with the therapist to identify the effects of key problematic areas related to interpersonal conflicts, role transitions, grief and loss, and social skills, and their effects on current symptoms, feelings states and/or problems
• Seeking to reduce symptoms by learning to cope with or resolve these interpersonal problem areas
Seeking to improve the regularity of daily life in order to minimize relapse.
References1. American Psychiatric Association. Diagnostic and Statistical Manual
of Mental Disorders, Fifth Edition (DSM-5). Arlington. 2013. Doi:10.1176/appi.books.9780890425596.
2. Merikangas KR, Jin R, He JP, Kessler RC, Lee S, Sampson NA, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry 2011;68(3):241-251. doi:10.1001/archgenpsychiatry.2011.12.
3. Bowden C, Singh V. Long-term management of bipolar disorder. Available at http://www.medscape.com/viewprogram/2686
4. Judd LL, Akiskal HS. The prevalence and disability of bipolar spectrum disorders in the U.S. population: Reanalysis of the ECA database taking into account sub threshold cases. J Affect Disord. 2003;73(1-2):123-131
5. Merikangas KR, Akiskal HS, Angst J, Greenberg PE, Hirschfeld RM, Petukhova M, et al. Lifetime and 12month prevalence of bipolar spectrum disorder in the National Comorbidity Survey replication. Arch Gen Psychiatry. 2007;64(5):543-552. DOI:10.1001/archpsyc.64.5.543.
6. Axelson D, Goldstein B, Goldstein T, Monk K, Yu H, Hickey MB, et al. Diagnostic Precursors to Bipolar Disorder in Offspring of Parents With Bipolar Disorder: A Longitudinal Study. Am J Psychiatry. 2015;172(7):638-646. doi:10.1176/appi.ajp.2014.14010035.
Page 7 of 8Citation: Ayano G (2016) Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures. SOJ Psychol 3(1): 1-8.
Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures
Copyright: © 2016 Ayano
7. Frey BN, Andreazza AC, Houenou J, Jamain S, Goldstein BI, Frye MA, et al. Biomarkers in bipolar disorder: a positional paper from the International Society for Bipolar Disorders Biomarkers Task Force. Aust N Z J Psychiatry. 2013;47(4):32132. doi:10.1177/0004867413478217.
8. The Columbia Bipolar Genetic Study. Bipolar disorder and genetics. Available at http://bipolar.hs.columbia.edu/disgenet.htm. Accessed: March 13, 2013.
9. Ferreira MA, O’Donovan MC, Meng YA, Jones IR, Ruderfer DM, Jones L, et al. Collaborative Genome wide association analysis supports a role for ANK3 and CACNA1C in bipolar disorder. NatGenet. 2008;40(9):1056-1058. doi:10.1038/ng.209.
10. Sklar P, Ripke S, Scott LJ, Andreassen OA, Cichon S, Craddock N, et al. Large scale genome wide association analysis of bipolar disorder identifies a new susceptibility locus near ODZ4. Nat Genet. 2011;43(10):977-983. doi:10.1038/ng.943.
11. Baum AE, Akula N, Cabanero M, Cardona I, Corona W, Klemens B, et al. A genome wide association study implicates diacylglycerol kinase eta (DGKH) and several other genes in the etiology of bipolar disorder. Mol Psychiatry. 2008;13(2):197-207. DOI:10.1038/sj.mp.4002012.
12. Burton PR, Clayton DG, Cardon LR, Craddock N, Deloukas P, Duncanson A, et al. Genome wide association study of 14,000 cases of seven common diseases and 3,000 Shared controls. Nature. 2007;447(7145):661-678.
13. Sklar P, Smoller JW, Fan J, Ferreira MA, Perlis RH, Chambert K, et al. Whole genome association study of bipolar disorder. Mol Psychiatry. 2008;13(6):558-569. doi:10.1038/sj.mp.4002151.
14. Roybal K, Theobold D, Graham A, DiNieri JA, Russo SJ, Krishnan V, et al. Mania like behavior induced by disruption of CLOCK. Proc Natl Acad Sci U S A. 2007;104(15):6406-6411. DOI:10.1073/pnas.0609625104.
15. Schaefer, Catherine Ann. Multiethnic genome wide association study of bipolar disorder. Kaiser Foundation Research Institute, Oakland, CA, United States.
16. Owen MJ, Lewis SW, Murray RM. Obstetric complications and schizophrenia: a computed tomographic study. Psychol Med. 1988;18:331-339.
17. DeLisi LE, Hoff AL, Schwartz JE. Brain morphology in first episode schizophrenic like psychotic patients: a quantitative magnetic resonance imaging study. Biol Psychiatry 1991;29(2):159-175. Doi:10.1016/0006-3223(91)90044-M.
18. Scott J, McNeill Y, Cavanagh J, Mary Cannon, Robin Murray. Exposure to obstetric complications and subsequent development of bipolar disorder: systematic review. Br J Psychiatry 2006;189(1):3-11. DOI:10.1192/bjp.bp.105.010579.
19. Geddes JR, Verdoux H, Takei N, Lawrie SM, Bovet P, Eagles JM, et al. Schizophrenia and complications of pregnancy and labour: an individual patient data meta analysis. Schizophr Bull. 1999;25:413-423.
20. O’Callaghan E, Gibson T, Colohan HA, Buckley P, Walshe DG, Larkin C, et al. Risk of schizophrenia in adults born after obstetric complications and their association with early onset of illness: a controlled study. BMJ. 1992;305(6864):1256-1259.
21. Dalen P. Family history, the electroencephalogram and perinatal factors in manic conditions. Acta Psychiatr Scand 1965;41(4):527-563.
22. Lewis SW, Murray RM. Obstetric complications, neuro developmental
deviance, and risk of schizophrenia. J Psychiatr Res. 1987;21(4):413-421.
23. Done JD, Johnstone CE, Frith CD, Golding J, Shepherd PM, Crow TJ. Complications of pregnancy and delivery in relation to psychosis in adult life: data from the British perinatal mortality survey sample. BMJ. 1991;302(6792):1576-1580.
24. Dennis K, Deborah A, Yurgelun-Todd, Deborah LL, David Medoff, CM Lajonchere, et al. Obstetric complications in patients with bipolar disorder and their siblings. Psychiatry Res. 1993;48:4756. Doi:10.1016/0165-1781(93)90112-T.
25. Guth C, Jones P, Murray R. Familial psychiatric illness and obstetric complications in early onset affective disorder: a case control study. Br J Psychiatry 1993;163:492-498.
26. Hashimoto K, Sawa A, Iyo M. Increased levels of glutamate in brains from patients with mood disorders. Biol Psychiatry. 2007. 62(11):13106. DOI:10.1016/j.biopsych.2007.03.017.
27. Ambelas A. Life events and mania: A special relationship. British Journal of Psychiatry. 1987;150(2):235-240. DOI:10.1192/bjp.150.2.235.
28. Clancy J, Crowe R, Winokur G, Morrison J. The Iowa 500: Precipitating factors in schizophrenia and primary affective disorder. Comprehensive Psychiatry. 1973;14(3):197-202. Doi:10.1016/S0010-440X(73)80012-4.
29. Calabrese JR. Overview of patient care issues and treatment in bipolar spectrum and bipolar II disorder. J Clin Psychiatry. 2008 ;69(6):e18.
30. Diflorio A, Jones I. Is sex important? Gender differences in bipolar disorder. Int Rev Psychiatry. 2010;22(5):437-452. DOI:10.3109/09540261.2010.514601.
31. Yatham L. Newer anticonvulsants in the treatment ofbipolar disorder. J Clin Psychiatry 2004;65 (Suppl. 10):28–35.
32. Yatham LN. Acute and maintenance treatment of bipolarmania: the role of atypical antipsychotics. Bipolar Disord. 2003;5(Suppl. 2):7-19.
33. Parikh S, Kusumakar V, Haslam D, Matte R, Sharma V, Yatham LN. Psycho social interventions as an adjunct to pharmacotherapy in bipolardisorder. Can J Psychiatry 1997;42(Suppl. 2):74S–78S.
34. Scott J, Gutierrez MJ. The current status of psychological treatments in bipolar disorders: a systematic review of relapse prevention. Bipolar Disord. 2004;6(6):498-503. DOI:10.1111/j.1399-5618.2004.00153.x.
35. Suppes T, Dennehy E, Swann A, Bowden CL, Calabrese JR, Hirschfeld RM, et al. Report of the Texas Consensus Conference Panel on medication treatment of bipolar disorder 2000. J Clin Psychiatry. 2002;63(4):288-299.
36. Vivek Kusumakar, Lakshmi N Yatham. The treatment of bipolar disorder: review of the literature, guidelines, and options. Can J Psychiatry. 1997;42 (Suppl. 2):67S–100S.
37. Australian and New Zealand clinical practice guidelines for the treatment of bipolar disorder. Aust N Z J Psychiatry. 2004;38:280-305. DOI:10.1111/j.1440-1614.2004.01356.x.
38. Goodwin G, Haddad PM, Ferrier IN, Aronson JK, Barnes T, Cipriani A, et al. Evidence based guidelines for treating bipolar disorder: recommendations from the British Association for Psychopharmacology. J Psycho pharmacol. 2016;30(6): 495-553. doi:10.1177/0269881116636545.
39. Licht R, Vestergaard P, Kessing L, Larsen J, Thomsen P. Psychopharmacological treatment with lithium and antiepileptic

Page 8 of 8Citation: Ayano G (2016) Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures. SOJ Psychol 3(1): 1-8.
Bipolar Disorder: A Concise Overview of Etiology, Epidemiology Diagnosis and Management: Review of Literatures
Copyright: © 2016 Ayano
drugs: suggested guidelines from the Danish Psychiatric Association and the Child and Adolescent Psychiatric Association in Denmark. Acta PsychiatrScand Suppl. 2003;419: 1-22
40. Zaretsky A. Targeted psychosocial interventions for bipolar disorder. Bipolar Disord. 2003;5:80–87.
41. Gonzalez-Pinto A, Gonzalez C, Enjuto S, Fernandez de Corres B, Lopez P, Palomo J, et al. Psycho education and cognitive behavioral therapy in bipolar disorder: an update. Acta Psychiatr Scand. 2004;109:83–90.
42. Jones S. Psychotherapy of bipolar disorder: a review. J Affect Disord 2004; 80(2-3):101–114. DOI:10.1016/S0165-0327(03)00111-3.
43. Yatham L, Kusumakar V, Parikh S, David RS Haslam, Raymond Matte, Verinder Sharma, et al. Bipolar depression: treatment options. Can J Psychiatry. 1997;42(Suppl. 2):87S–91S.
44. Colom F, Vieta E, Reinares M Martínez-Arán A, Torrent C, Goikolea JM, et al. Psychoeducation efficacy in bipolar disorders: beyond compliance enhancement. J Clin Psychiatry. 2003;64:1101-1105.
45. Swartz H, Frank E. Psychotherapy for bipolar depression: a phasespecific treatment strategy? Bipolar Disord. 2001;3:11-22. DOI:10.1034/j.1399-5618.2001.030102.x
46. Rucci P, Frank E, Kostelnik B, Fagiolini A, Mallinger AG, Swartz HA, et al. Suicide attempts in patients with bipolar I disorder during acute and maintenance phases of intensive treatment with pharmacotherapy and adjunctive psychotherapy. Am J Psychiatry. 2002;159:1160–1164. DOI:10.1176/appi.ajp.159.7.1160.
47. Colom F, Vieta E, Martinez Aran A, Reinares M, Goikolea JM, Benabarre
A, et al. A randomized trial on the efficacy of group psycho education in the prophylaxis of recurrences in bipolar patients whose disease is in remission. Archives of General Psychiatry. 2003;60(4):402-407. DOI:10.1001/archpsyc.60.4.402.
48. Colom F, Vieta E, Reinares M, Martínez-Arán A, Torrent C, Goikolea JM, et al. Psycho education efficacy in bipolar disorders: beyond compliance enhancement. Journal of Clinical Psychiatry. 2003;64(9):1101-1105.
49. Lam D, Bright J, Jones S et al. Cognitive therapy for bipolar illness: a pilot study of relapse prevention. Cognit Ther Res. 2000;24(5):503-520. DOI:10.1023/A:1005557911051.
50. Lam DH, Watkins ER, Hayward P, Bright J, Wright K, Kerr N, et al. A randomized controlled study of cognitive therapy for relapse prevention for bipolar affective disorder: outcome of the first year. Arch Gen Psychiatry. 2003;60:145-152.
51. Miklowitz DJ, George EL, Richards JA, Simoneau TL, Suddath RL. A randomized study of family focused Psycho education and pharmacotherapy in the outpatient management of bipolar disorder. Archives of General Psychiatry. 2003;60:904–912. DOI:10.1001/archpsyc.60.9.904.
52. Frank E. Interpersonal and social rhythm therapy prevents depressive symptomatology in bipolar I patients. Bipolar Disorders. 1999;Suppl 1:13.
53. Frank E, Kupfer DJ, Thase ME, Mallinger AG, Swartz HA, Fagiolini AM, et al. Two year outcomes forinter personal and social rhythm therapy in individuals with bipolar I disorder. Archives of General Psychiatry. 2005;62:996–1004. DOI:10.1001/archpsyc.62.9.996.