Embed Size (px)
DESCRIPTION
Bipolar
Citation preview
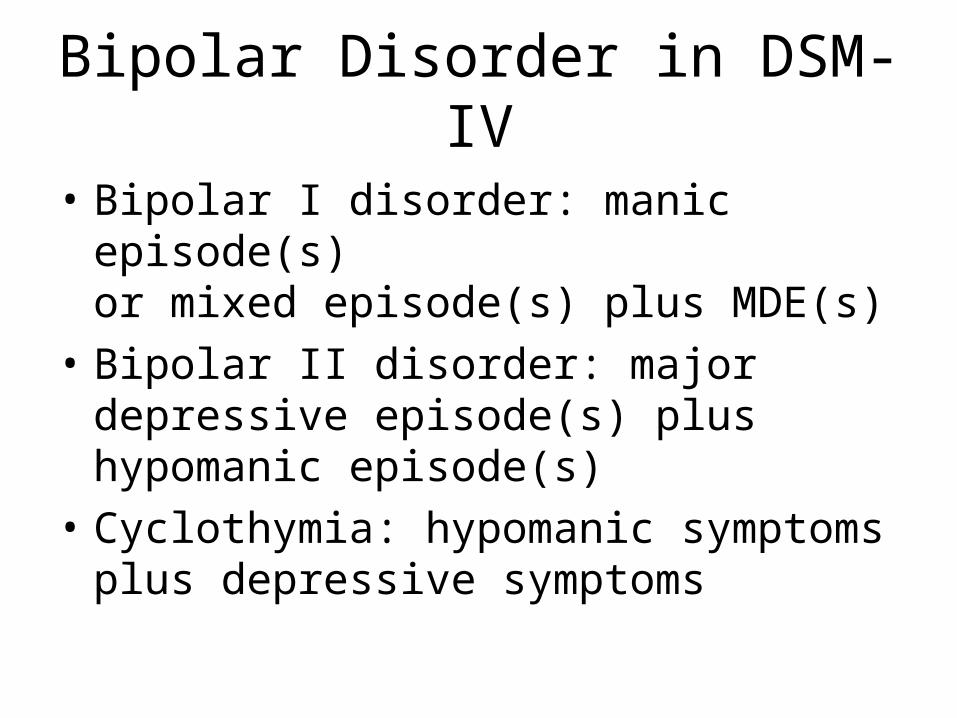
Bipolar Disorder in DSM-IV
• Bipolar I disorder: manic episode(s)or mixed episode(s) plus MDE(s)
• Bipolar II disorder: major depressive episode(s) plus hypomanic episode(s)
• Cyclothymia: hypomanic symptomsplus depressive symptoms
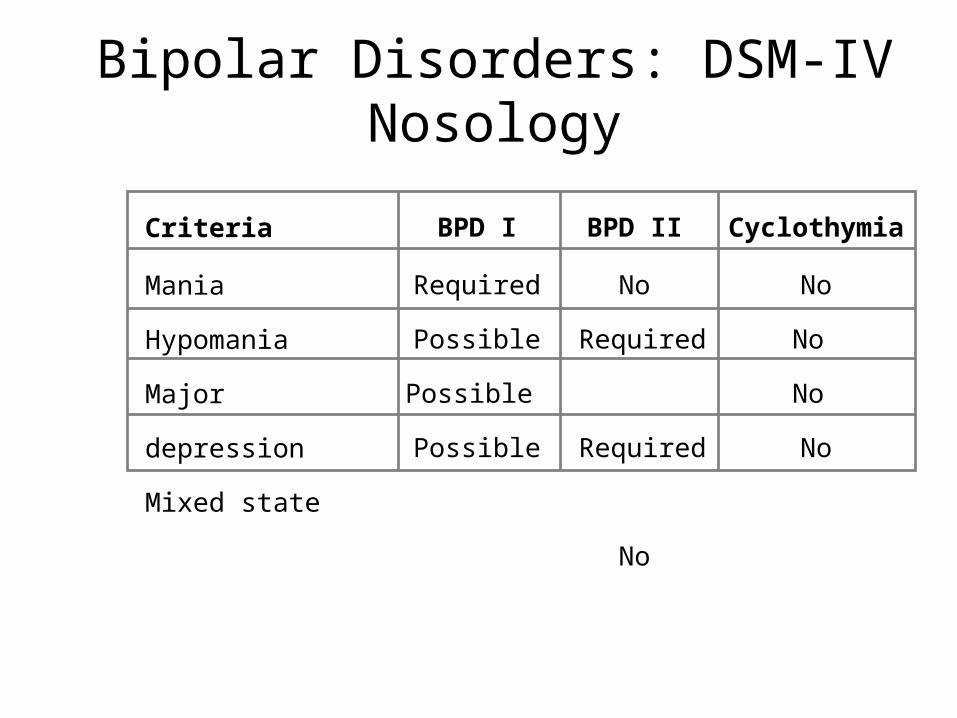
Bipolar Disorders: DSM-IV Nosology
Criteria
Mania
Hypomania
Major depression
Mixed state
BPD I
Required
Possible
Possible
Possible
BPD II
No
Required
Required
No
Cyclothymia
No
No
No
No
Manic Episode: Diagnostic Criteria
• Elevated, expansive, or irritable mood for 1 week or longer, plus 3 or more of the following– Inflated self-esteem or grandiosity– Decreased need for sleep– Pressured speech– Racing thoughts/flight of ideas– Distractibility– Psychomotor agitation/increased goal-directed activity– Excessive involvement in high-risk activities
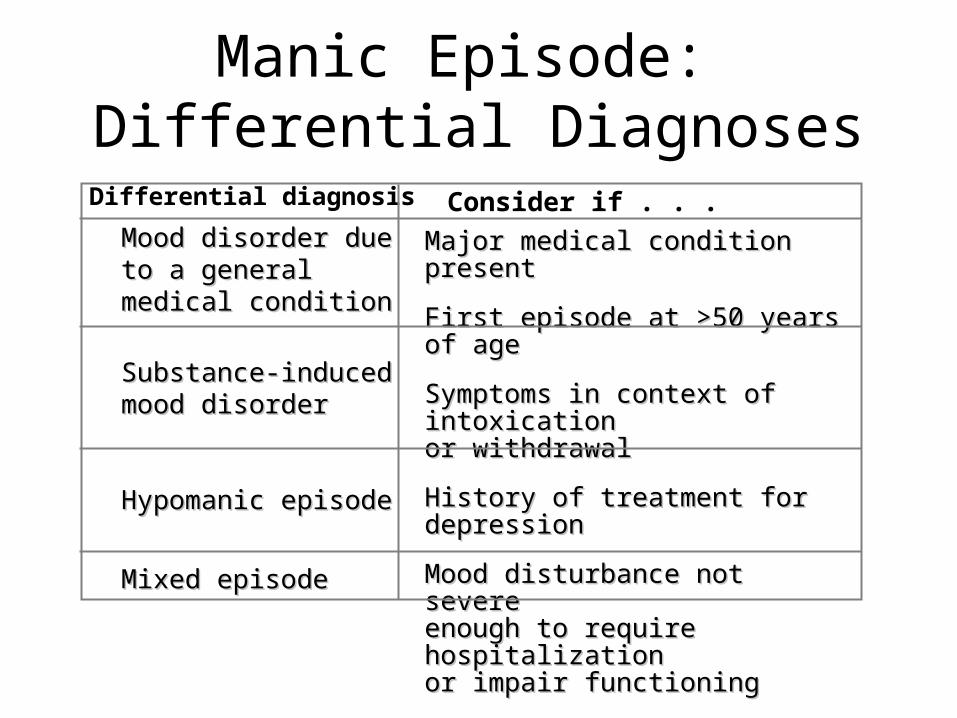
Manic Episode: Differential Diagnoses
Differential diagnosis Consider if . . . Mood disorder due to a Mood disorder due to a general medical general medical conditioncondition
Substance-inducedSubstance-inducedmood disordermood disorder
Hypomanic episodeHypomanic episode
Mixed episodeMixed episode
Major medical condition present Major medical condition present
First episode at >50 years of ageFirst episode at >50 years of age
Symptoms in context of intoxicationSymptoms in context of intoxicationor withdrawalor withdrawal
History of treatment for depressionHistory of treatment for depression
Mood disturbance not severeMood disturbance not severeenough to require hospitalizationenough to require hospitalizationor impair functioningor impair functioning
Manic episode and MDE in 1 weekManic episode and MDE in 1 week
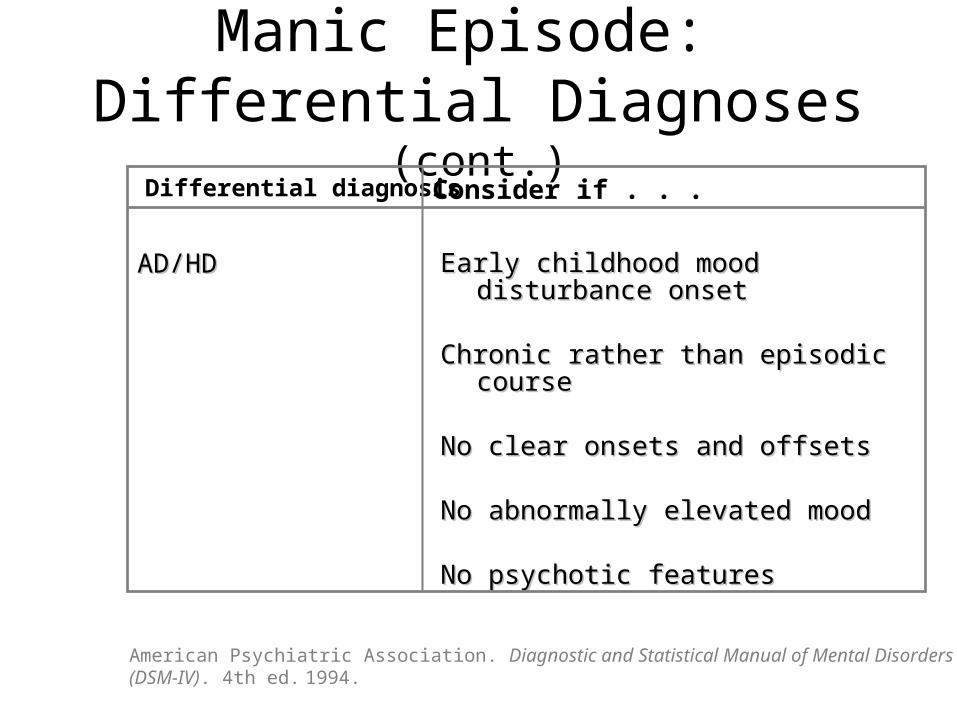
Manic Episode: Differential Diagnoses (cont.)
AD/HDAD/HD Early childhood mood disturbance onset Early childhood mood disturbance onset
Chronic rather than episodic courseChronic rather than episodic course
No clear onsets and offsets No clear onsets and offsets
No abnormally elevated moodNo abnormally elevated mood
No psychotic features No psychotic features
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). 4th ed. 1994.
Differential diagnosis Consider if . . .
• Depressed mood and/or loss of interest or pleasure 2 weeks duration
• Associated symptoms– Physical: insomnia/hypersomnia,
appetite/weight change, decreased energy, psychomotor change
– Psychological: feelings of guilt or worthlessness, poor concentration/indecisiveness, thoughts of death/suicidal intentions (SI)
Major Depressive Episode: DSM-IV Criteria
…and 4 of the following symptoms
• Physical– Sleep disorder– Appetite change– Fatigue– Psychomotor
retardation
• Psychological– Low self
esteem/guilt– Poor concentration/
indecisiveness– Thoughts of
death/SI
Mixed Episode: Diagnostic Criteria
• Criteria met for both manic episode + MDE for 1 week
• Symptoms – Are sufficient to impair functioning
or– Necessitate hospitalization
or– Are accompanied by psychotic features
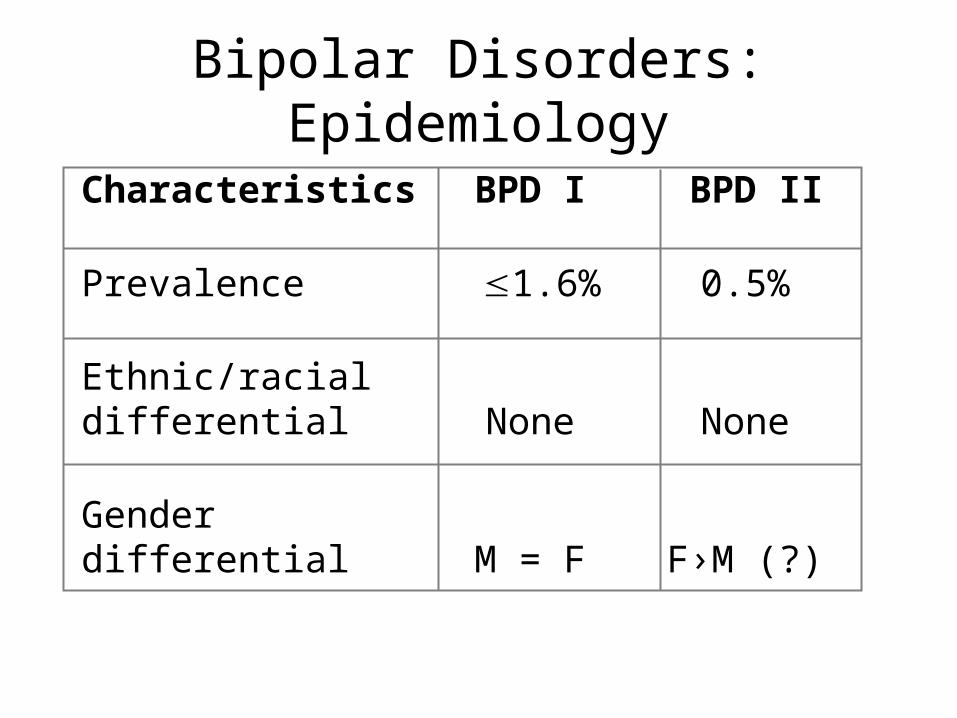
Characteristics BPD I BPD II
Prevalence 1.6% 0.5%
Ethnic/racial differential None None
Gender differential M = F F›M (?)
Bipolar Disorders: Epidemiology
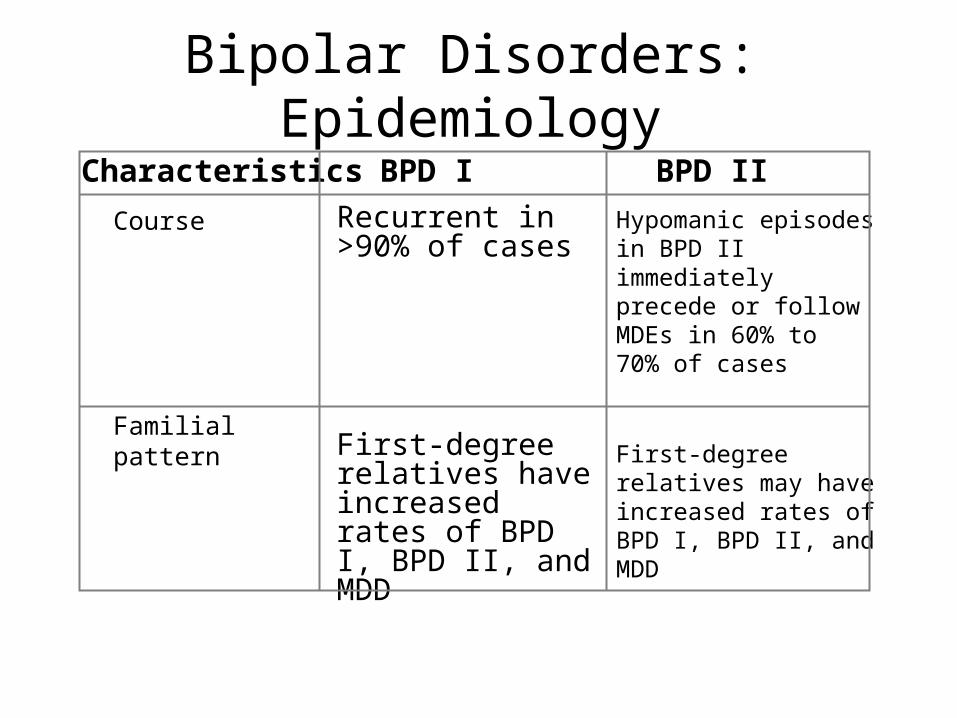
Characteristics BPD I BPD II
Bipolar Disorders: Epidemiology
Hypomanic episodes in BPD II immediately precede or follow MDEs in 60% to 70% of cases
First-degree relatives may have increased rates of BPD I, BPD II, and MDD
Recurrent in >90% of cases
First-degree relatives have increased rates of BPD I, BPD II, and MDD
Course
Familial pattern
Epidemiology
• Peak age of onset: adolescence through early 20s– Onset of first manic episode after age 40 years is
“red flag” to consider substance use or generalmedical condition
• Seasonal variation– Depression more common in spring and autumn
– Mania more common in summer
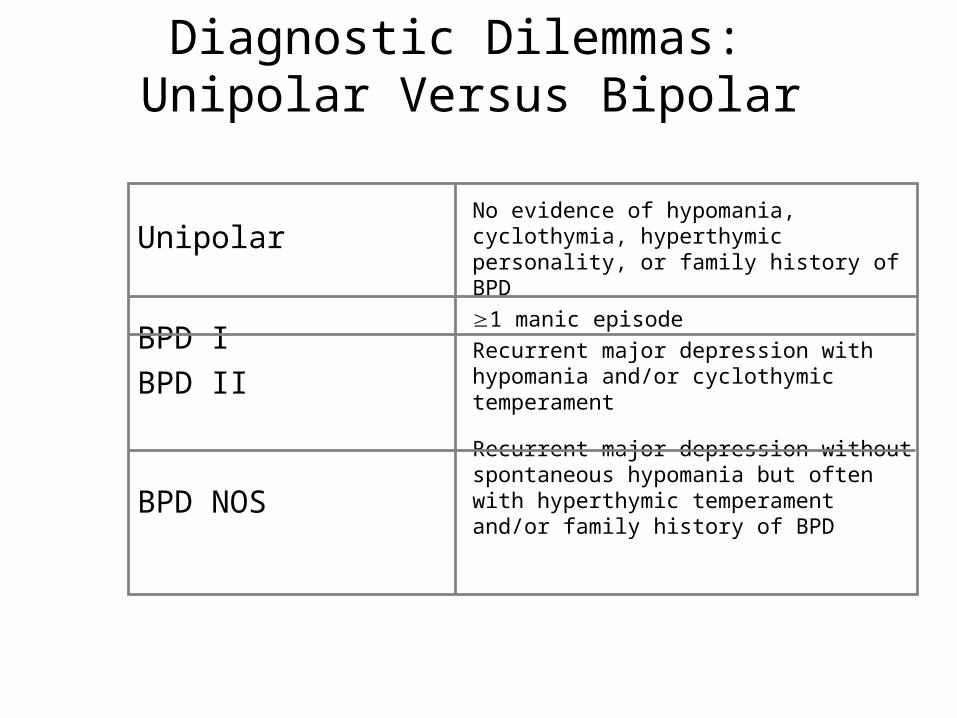
Diagnostic Dilemmas: Unipolar Versus Bipolar
No evidence of hypomania, cyclothymia, hyperthymic personality, or family history of BPD
1 manic episode
Recurrent major depression with hypomania and/or cyclothymic temperament
Recurrent major depression without spontaneous hypomania but often with hyperthymic temperament and/or family history of BPD
Unipolar
BPD I
BPD II
BPD NOS
Etiology
Heritability
• Evidence for heritability is much stronger for bipolar than for unipolar disorders
• Specific genetic association has not been consistently replicated
EVIDENCE FOR HERITABILITY OF BIPOLAR DISORDER
• Family Studies- First degree relatives are 8 to 18 times more likely to have Bipolar I
• 2 to 10 times to have MDD.
• Risk is 25% if one parent has illness, and 50% to 75% with both parents affected
FAMILY STUDIES
• The majority of individuals with bipolar disorder have a positive family history of some type of mood disorder
• About 50% of all bipolar I patients have at least one parent with a mood disorder
ADOPTION STUDIES
• Prevalence of bipolar disorder in adopted away offspring corresponds to rates in biological, but not adoptive relatives
• Twin Studies- Concordance rate in MZ twins is 33 to 90%, in DZ is 5 to 25%
Cognitive Deficits
• Working memory• Sustained attention• Abstract reasoning• Visuomotor skills• Verbal memory• Verbal fluency• Cognitive flexibility• General cognitive functioning
Potential Explanations for Cognitive Deficits
• Iatrogenic or Alcohol use
• Temporary functional changes
• Degenerative brain changes
• Permanent structural lesions
• Permanent functional alterations of neural networks underlying affect and cognition
Alcohol Use
• Alcohol use occurs in 30-50% of cases• Impairs memory and executive functioning• Gorp et al (1998)
– Compared BP only, BP + AD, Control– BP + AD > BP only for cognitive impairment– No difference between Control and BP only
• Other studies have reported cognitive deficits in non substance abusing BP patients
Iatrogenic
• Lithium – Memory and psychomotor functioning
• Valproate and Carbemazepine – Attentional deficitis
• Neuroleptics– Sustained attention– Visuomotor speed deficits
• Benzodiazapines– Memory
• Crews et al.– Performance on WCST negatively related to years of exposure
to antipsychotic drugs
Questions
• Some evidence indicates that Lithium exerts a neuroprotective effect on neuronal tissue– Are studies indicating adverse effects of lithium not
accounting for complex combinations of meds?
• Could we even study this issue empirically??– Ethics– Generalizability
Temporal Functional Deficits• Are cognitive deficits specific to depressive or manic states?
• Depression– Decreased dorsal prefrontal cortex and anterior cingulate gyrus
activation– Increased ventral prefrontal cortex activation– Reductions in left hemisphere activity
• Mania– Opposite pattern– Decreased ventral and increased dorsal activity of the prefrontal cortex– Reductions in right hemisphere activity
• Remission of depressive symptoms associated with increased blood flow to dorsolateral and medial prefrontal cortex
• Distractibility and behavioral dysregulation during mania
– Heightened left hemisphere prefontal corticol activity
• Attentional deficits accompanying depression
– Right hemisphere disturbance of dorsal prefrontal cortex, cingulate gyrus, parlimbic cortex
Summary
• Authors contend (Savitz et al, 2005) that functional disturbances have a neurodevelopmental and possibly genetic etiology that may be exacerbated by mood disturbances