Embed Size (px)
Citation preview

10/12/2015
1
Biological Disc Regeneration and
Repair in the SpinePhysiology of Disc Degeneration and Biologic
Regeneration and Repair Options
Dom Coric, M.D.
Carolina Neurosurgery and Spine Associates
Chief, Department of Neurosurgery
Carolinas Medical Center
Charlotte, NC
11/21/15
DISCLOSURE
– Medtronic: Consultant
– Spine Wave: Consultant/Stock/Royalties
– Globus Medical: Consultant
– Premia Spine: Consultant
– DiscGenics: Consultant
• All disc/nucleus repair procedures are investigational.
Introduction
• Nucleus/Disc Repair Techniques:
– (I) Cellular therapy
– (II) Growth factor therapy
– (III) Gene therapy
Pfirrmann CS, Boos N, et al: Magnetic resonance imaging classification of
lumbar intervertebral disc degeneration. Spine 26:1873-78,2001
Grade 1 Grade 2 Grade 3 Grade 4 Grade 5

10/12/2015
2
IVD
Annulus Fibrosus• Outer fibrous structure with:
– (A) Fibroblast-type cells
• Scant cells
– (B) Type I collagen (abundant)
• Tensile strength.
Nucleus Pulposus• Inner gelatinous structure
– (A) Chondrocytic cells
• Proteogylcans
– (B) Type II collagen
• Compressive forces.
• Fibro-cartilaginous structure.
IVD
• NUCLEUS PULPOSUS
– 2 cells types derived from distinct embryonic
sources (maintain ECM homeostasis):
– (1) Notochord cells
• notochordal remnant
• generally disappear by age 20
– (2) Chondrocytic disc cells
• derived from axial mesoderm
– Homeostasis: balance between anabolism and
catabolism of disc cells and the ECM they
produce.
ECM• Extracellular matrix primarily consists of:
– (a) Proteoglycans
• Aggrecan and versican: largest/most common
– Hydrophilic molecules: protein stems
surrounded by highly neg-charged
glycosaminoglycan (GAG) side chains.
– Chondroitin-6-sulfate and keratin sulfate :
» 2 most abundant GAG molecules, attract and
hold pos-charged H2O molecules.
– (b) Type II collagen: scaffold
Aggrecan

10/12/2015
3
IVD• Degenerative Disc Disease
– Loss of chondrocytic nucleus pulposus cells
results in inability to produce and maintain
normal ECM.
– Annulus fibrosus
• Delamination: annular tears.
– Nucleus pulposus
• Cellular loss: depletion of extracellular matrix,
replacement with fibrocartilage.
• Dessication: progressive loss of proteoglycans/H2O.
IVD
• DEGENERATIVE DISC DISEASE (DDD)
– Progressive changes in disc composition and
function out of proportion those associated
with normal aging.
– Calcification of cartilaginous endplate
(sclerosis) limits blood/nutrient supply.
– Factors favor ECM destruction (catabolism)
over production (anabolism).
Balance Imbalance
Anabolic Catabolic
IVDDEGENERATIVE DISC DISEASE (DDD)
Proteoglycans
Hydration
Disc dessication/degeneration/ disc ht
Load on surrounding structures
Annular tears/disc dessication, loss of ht/Modic changes/HNP
PAIN Photos courtesy of Prof Rauschning MD
10/12/2015
4
Disc Repair• 3 main mechanisms:
– I. Growth factors: exogenous protein injection.
• Boost native chondrocytic cell production by up-
regulating production of anabolic ECM proteins,
down-regulate catabolic factors.
– II. Gene therapy: transfer of genetic material.
• Boost native chondrocytic cell production by
inserting genetic material to maintain/restore ECM.
– III. Cell therapy: exogenous injection of cells.
• Introduction of exogenous cells to
augment/replenish ECM.
– Stem, native disc and chondrocyte cells
Growth Factors
• (I) Direct protein (growth factor) injection.
– Growth factors: small peptide cytokines with
cell regulatory function.
– In vitro studies show exogenous application of
growth factors can positively influence ECM
synthesis by chondrocytic cells.
Growth Factors
• Up-regulate ECM proteins:
– (a) Transforming growth factor (TGF-beta)
– (b) Insulin-like growth factor 1 (IGF-1)
– (c) Epidermal growth factor (EGF)
– (d) Platelet-derived growth factor
– (e) Bone morphogenetic proteins (BMP)
• BMP-7 (OP-1), BMP-2, GDF-5
• Increase anabolic activity.

10/12/2015
5
Growth Factors
• Down-regulate inflammatory cytokines:
– (a) Interleukin (IL-1, IL-6)
– (b) Tumor necrosis factor-alpha (TNF)
– (c) Matrix metalloproteinases (MMPs)
– (d) Nitric oxide (NO)
– (e) Prostaglandin E2 (PGE2)
• Decrease catabolic activity.
Growth Factors
• Challenges
– Practical clinical use of growth factors for
nuclear repair may be limited by their short
biologic half-lives (?hours/days).
– May be especially limited in chronic
conditions, such as DDD.
– Clinical correlation: growth factors clearly
improve disc structure in in vivo animal studies,
will this correlate with pain improvement in
humans?
Gene Therapy
• (II) Transfer of genetic material (DNA or
RNA) into a target cell (i.e. chondrocytic
cells) to modulate cellular activity (i.e. up-
regulate anabolic proteins or down-regulate
catabolic proteins), potentially long-term.

10/12/2015
6
Gene Therapy
• Challenges
– Since gene therapy involves active transfer of genetic
material, generally utilizing a viral vector, there is some
inherent risk (i.e. viral mutagenicity, systemic viral
infection, immune response).
– Therefore, may be more appropriate for potentially life-
threatening disorders, especially those resulting from
single gene defects (i.e. cystic fibrosis, sickle cell dz).
– May play a more limited role in non-life threatening
disorders with multifactorial etiology (i.e. rheumatoid
arthritis, DDD).
Cell Therapy
• Notochordal cells
– Allogeneic: embryonic human NP, soon after
birth these cells diminish rapidly.
• Chondrocytes
– Autologous: mature
– Allogeneic: juvenile
• Mesenchymal stem cells
– Autologous: bone marrow/adipose
– Allogeneic: embryonic/adult/umbilical
Nucleus Repair
• Cell therapy: Advantages
– Nucleus is surrounded and contained by
annulus, preventing cell migration.
– Limited blood supply and contained space
provides immune privileged milieu.

10/12/2015
7
Nucleus Repair
• Cell therapy: Challenges
– Degenerative environment: if endplate sclerosis
limits blood supply: decrease O2, increase
lactic acid (decrease pH) leads to cell death and
decreased ECM production, then transplanted
cells are subjected to same harsh environment.
– Normal ECM production and turnover is slow
(generally measured in yrs), transplanted cells
may take months/yrs to affect change.
Nucleus Repair• Cell therapy: Mechanism
– (1) Cell harvest
– (2) Cell expansion
• Musculoskeletal cell therapies generally introduce
5-10 million cells/defect: cells are expanded by
growing in monolayer to encourage proliferation.
– (3) Add scaffold/carrier
• Hyaluronic acid, fibrin, silk, collagen
– (4) Insertion
• Ideally minimally invasive with percutaneous needle
1
Cell Therapy
Donor Cells
Cell expansion
Carrier

10/12/2015
8
CNSA Disc Repair IND Experience
• NuQu – Phase I, Phase II
– Juvenile chondrocyte nucleus repair
– Thrombin/fibrinogen carrier
– Phase I: prospective
– Phase II: prospective, randomized, placebo
• Mesoblast – Phase II, Phase III (ongoing)
– Stem cell nucleus repair
– Phase II/III: prospective, randomized, placebo
– Allogeneic mesenchymal stem cells
– Hyaluronic acid carrier
Coric D, Pettine K, Sumich A, Boltes MO: Prospective Study of Disc Repair with NuQu®
Allogeneic Chondrocytes. J Neurosurg-Spine 18:36-42, 2013
Stem Cells for DDD
• Yoshikawa et al. (2010) reported on two patients
treated with expanded iliac crest derived
mesenchymal stem cells
– Case report: 2 patients
– Autologous marrow-derived mesenchymal stem cells.
• 100,000 cells/mL
– Advanced DDD (stenosis and adjacent to fusion).
– Positive clinical results.
Yoshikawa T, Ueda Y, Miyazaki K, Koizumi M, Takakura Y: Disc regeneration therapy using
marrow mesenchymal cell transplantation: a report of two cases. Spine 35:E475-80, 2010
Stem Cells for DDD
• Orozco et al. (2011) published a pilot series of ten
patients with chronic LBP also treated with
expanded iliac crest derived mesenchymal stem
cells.
– Case series: 10 patients
– Autologous marrow-derived mesenchymal stem cells.
• 5,000,000 cells/mL
– DDD with chronic low back pain (minimum 6 months).
– Positive clinical results.
Orozco L, Soler R, Morera C, Alberca M, Sanchez A, Garcia-Sancho J:Intervertebral disc repair
by autologous mesenchymal bone marrow cells: a pilot study. Transplant 92:822-828, 2011

10/12/2015
9
Cartilage Cells for DDD
• NuQu: Juvenile cartilage cells
– Phase I: 15 pts - prospective, non-randomized.
– Phase II: 44 pts - prospective, randomized, blinded, placebo-
controlled.
• Pts with discogenic back pain secondary to
mild/moderate degenerative disc disease (DDD) L2-S1.
– Fibrin glue carrier.
Coric D, Pettine K, Sumich A, Boltes MO: Prospective Study of Disc Repair with NuQu®
Allogeneic Chondrocytes. J Neurosurg-Spine 18:36-42, 2013
Cartilage Cells for DDD
• Phase I Pilot Study
• Levels:• L3-4: 2
• L4-5: 1
• L5-S1: 12
• Injection duration: Avg=11.6 s (Range 5-32s)
• Injection amount: Avg=1.4cc (Range 1-1.6cc)
• Est # of viable cells 6.75-13.5 million cells/cc
• Indiscal press (peak): Avg=92.4 psi (Range 60-101)
Cartilage Cells for DDD
• Phase I results: CLINICAL
– Mean preoperative pain (NRS), disability (ODI) and
function (SF-36) scores improved significantly at six
months and were maintained through 2 years.
Pre-op 6 mths 2 yrs
NRS: 5.7 3.8 2.5 (p=0.0036)
ODI: 53.3 26.9 14.3 (p<0.0001)
SF-36:35.5 43.4 29.2 (p=0.0014)

10/12/2015
10
Disc Repair for DDD
• CH: Pt is 40 yo with long h/o mechanical LBP.
– 7 in, 22-gauge.
– 1.4 cc injection, 12s.
– Max press= 82 psi.
– Pt now 1 yr postop
resolution of chronic
mechanical LBP (16 mnths),
no narcotics, VAS=1.
Conclusion• Disc repair is both a minimally invasive as
well as motion preserving technique to treat
symptomatic degenerative disc disease
earlier and less invasively.
• Continued investigation into the diagnosis
and treatment of DDD is warranted.
THANK
YOU!

10/21/2015
1
Current Trials and the Status of Tissue-Engineering Strategies
Roger Härtl, MD
Professor of NeurosurgeryDirector of Spinal Surgery
Department of NeurosurgeryWeill-Cornell Medical College
New York, NYUSA
Disclosure
• Consultant
• Funding
– Synthes
– Baxter
– BrainLab
– AOSpine
– AOFoundation
– NFL
– Baxter
– Nuvasive
Biological Strategies for Disc Repair and Regeneration
• Growth Factors
• Gene therapy
• Transplantation of cells– Stem cells / Progenitor cells
• Autologous / allogeneic
– Chondrocytes• Autologous / allogeneic juvenile
• Whole disc allograft transplant
• Transplantation of disc/scaffold constructs– NP
– Composite bio-engineered discs
– High density collagen gel

10/21/2015
2
NPAF
EP
VB
Healthy Disc Degenerated Disc and Therapeutic Targets
Supply Demand
Metabolism Cells Structure
Tissue Engineered ConstructsBiomolecules Cells
bone
AFNP
EP Blood Vessel
VB
NPAFEP
DDD and Biological NP Repair
Tissue Engineering for Disc Regeneration
Biopsy
Scaffold
Cell cultivation Cell proliferation
Allograft transplant
Tissue engineered disc
Transplant
Cell transplant
Mechanical
Stimuli
Growth
Factors
Tissue developmentCell isolation
Pluripotent Stem
Cells
Progenitor Cells
Differentiated
Disc
Chondrocytes
NP AF AC
Genes
Biomaterial implantation
Early Intermediate Advanced
Viable
Cells
Structural
Damage
Biomolecular
Cell-based therapy
Engineered constructs
Therapeutic
Strategy
Degrees of
Degeneration
Stages of Disc Repair / Regeneration

10/21/2015
3
Cell implantation
Promising Animal Data:
• MSC
• Chondrocytes
• NP cells, etc.
Autologous Chondrocytes
Canine and clinical trail
Autologous cell from AF and NP
Cells expanded in culture, replanted after
12 weeks
Euro spine J, 2008
In canine
collected in
open
procedure
For clinical trial
collected during
discectomy for disc
herniation
2006, 2008
Clinical trail 24 month follow-up
- Cells were transplanted 12
weeks after discectomy
-112 patients enrolled,
patients were
randomized
- OLBPD, VAS, SF-36 scores
for follow up
- Follow up MRI
Eur Spine J 2006, 2008

10/21/2015
4
First (and last) interim analysis
• Removed cells could be expanded in culture
• Patients who received cells had greater pain reduction after discectomy at 2 years
• Discs with transplant demonstrated significant more fluid content on MRI
Before 1d 3m 12m 24m 60m
Stem Cells
• Unexpanded hematopoietic stem cells obtained from iliac crest bone marrow
• 10 patients
• 12 months
• No control
• No improvement of low back pain at 1 year
– 8 patients had surgery: Fusion, arthroplasty
2006
SPINE Volume 35, Number 11
2010
- 2. case: Instability with
spinal canal stenosis L4/L5
- Two cases
- 1. case: adjacent
segment disease after
ALIF L4/L5
LBP, numbness right lower
leg 6 years after fusion
LBP, leg pain over
several years

10/21/2015
5
MRI outcome 2 Years
PRE-OP POST-OP 2yrsPOST-OP 2yrs PRE-OP
• 10 patients with DDD
• No respond to cons. Therapy after 6months
• BMA iliac crest, expanded, 12 month outcome
• VAS and ODI
• Follow up MRI was obtained
Patients showed improvement
- No increase of disc height
- Significant increase in signal
intensity after 1 year
2011
12 month outcome

10/21/2015
6
Allogeneic Mesenchymal Progenitor Cells
• Phase 2 clinical trial
– 100 patients with moderate to severe low back pain, > 6 months, caused by early disc degeneration, single level
• Randomized to receive
– direct intra-disc injection of saline (n= 20), hyaluronic acid (HA, n=20), 6 million allogeneic MPCs in hyaluronic acid carrier (6M, n=30) or 18 million allogeneic MPCs in hyaluronic acid carrier (18M, n=30)
• Results
– Reduced low back pain and improved function
– less opioids for pain relief, greater radiographically-determined disc stability
– underwent less additional surgical and non-surgical treatment interventions
• 18 sheep
• C3/4/5 ACD
– Group 1: Absorbable cage & Gelfoam sponge only
– Group 2: Cage & Gelfoam sponge with MPCs with chondrogenic agent pentosan polysulfate (PPS)
– Group 3: Cage & Gelfoam sponge with MPCs
• MPCs in combination with PPS to produce cartilaginous tissue
• Preserve motion
• May offer an alternative to fusion
SHEEP
Allogeneic Mesenchymal Progenitor Cells& Cage
2010
Juvenile chondrocytes
10/21/2015
7
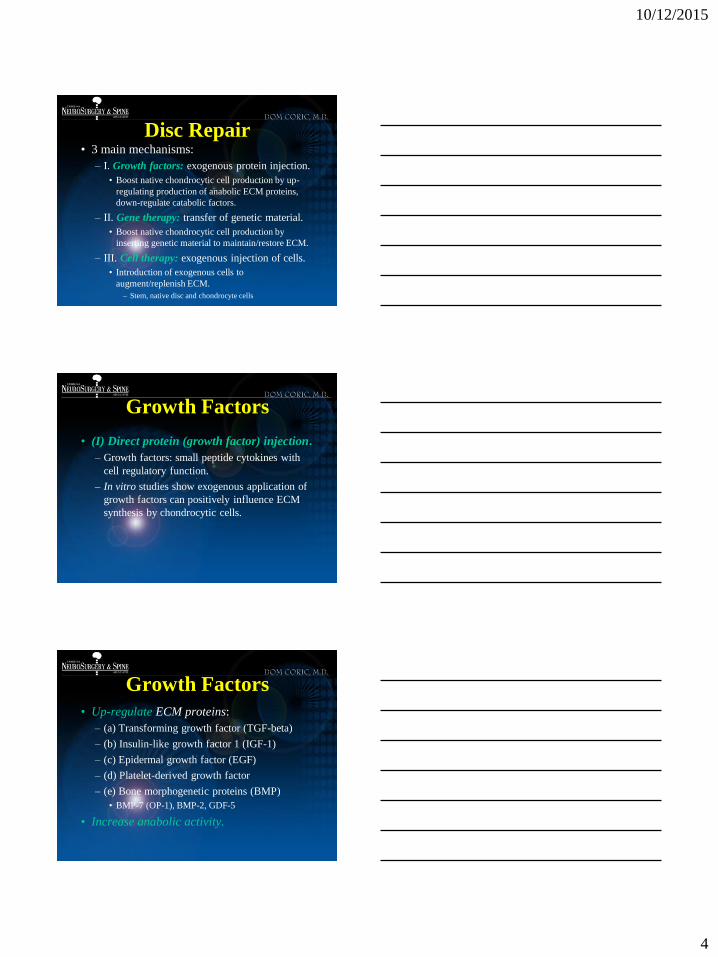
-Juvenile chondrocytes implanted into degenerated
lumbar spine of pigs
-After 12 months cells showed high GAG and
Protein content
1 Year follow up
- Cells proved viable by FISH (Y-chromosome)
analysis after 12 months
- Juvenile chondrocytes were superior according to
cell viability and GAG synthesis compared to
implanted MSC
2011
Three months
MSC
healthy
carrier
Juv. Chondr.
FISH fluorescence in
situ proves viability
In vitro juv. chondrocytes Cell injection
2013

10/21/2015
8
Clinical trial Juvenile chondrocytes
• Phase I study, 15 patients
• 12 month follow up, ODI, NRS, SF-36
• MRI follow up
60% improved,
mostly because
of reduced HIZ
Treatment for single level
lumbar spondylosis
Scores significantly
improved from baseline
No complications
20% had surgery
Patient follow (6-12 months)
Reduced HIZ after 12 months
Preop. Postop.
10/21/2015
9
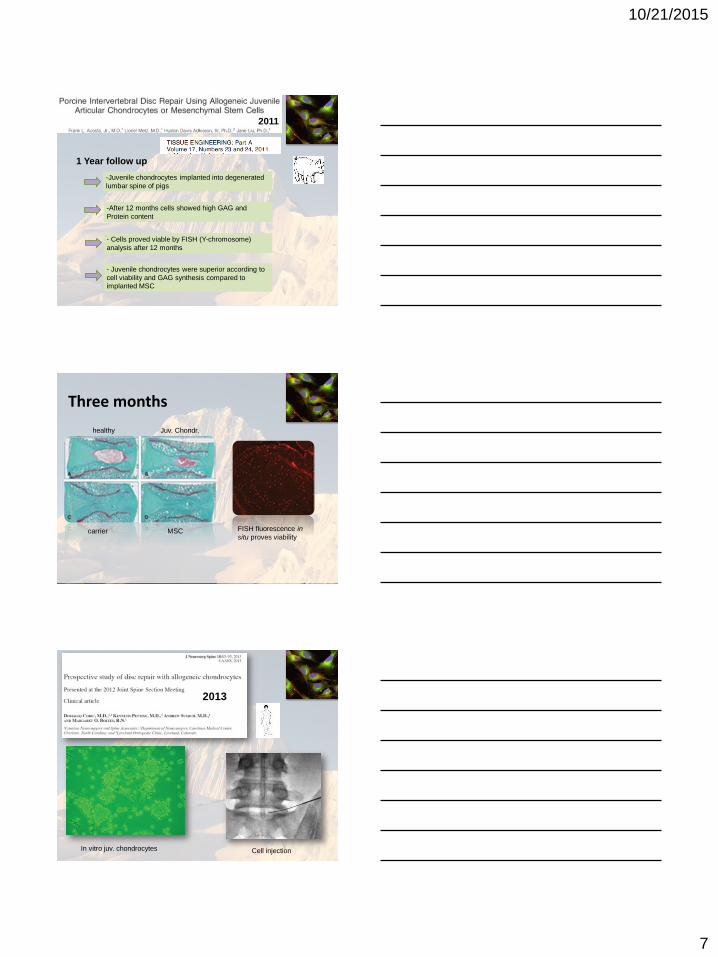
Disc Transplantation
2007
• Total disc transplant in beagle dogs
• Transplants injected and cultured with
– NP cells
– NP cells & human telomerase reverse
transcriptase (hTERT) gene-transfection
– DMEM/F12, no cells
• hTERT may upregulate and activate NP function
• NP cells or hTERT-loaded NP cells effectively resist degeneration of the allogenic transplants
• hTERT - loaded NP cells had a better antidegenerationeffect
Disc Transplantation plus NP activation with
hTERT2013
Bone Marrow Concentrate (BMC)
2015
HarvestExpansion
Concentrate BMC
MSC
Up to 2 hours
Weeks

10/21/2015
10
CFU-F; colony-forming unit-fibroblast
Percutaneous Injection
Researcher Trial Patients ControlFollow-up
(M)Outcomes Journal
Meisel HJ et al.Autologous Disc Chondrocyte
Transplantation (EuroDisc)28
Microdiscectomy alone
24ADCT with discectomy shows decreased in OPDQ than discectomy. No adverse risks
Eur Spine J 2006, 2008
Haufe SMW et al. Hematopoietic Stem Cell 10 No control 12None of the patients achieved any
improvement of their discogenic back pain after 1 year.
Stem Cells Dev. 2006
Yoshikawa T et al.Autologous Bone Marrow
Mesenchymal Cell2 No control 24
Improvements in the vacuum phenomenon as well as signal intensity of T2-weighed MRIs.
Spine 2010
Orozco L et al.Autologous Bone Marrow
Mesenchymal Cell10 No control 12
Rapid improvement of pain and disability. Disc height not recovered, but water content
elevated
Transplan-tation 2011
Coric D et al.Allogenic juvenile
chondrocytes (NuQu)15 No control 12
ODI, NRS, SF-36 improved from baseline. 89% of patients show the improvement on MRI. 20% of the patients underwent reoperation
JNS 2013
Berlemann et al. Injectable Biomimetic
Nucleus Hydrogel 14 No control 24
Significant improvement in leg and back pain after micro-discectomy
Euro Spine 2009
Ruan et al. Total Disc Replacement with
Allogeneic IVD 5
No control 60
The allograft engrafted the disc space without apparent immunoreaction; all minus
one disc preserved range of motion
Lancet 2007
Pettine et al. Injection of autologous bone
marrow concentrate cells26
No control 12
Improvement in pain scores prominently in patients with higher CFU-F concentrations. Rehydration of the discs observed (n=8)
Stem Cells 2015
Summary: Published Clinical Studies on Disc Regeneration - All cell-based -
Title of Trial Design NFU
(M)Treatment
PI/ Sponsor
Status
A Study Comparing the Safety and Effectiveness of Cartilage Cell Injected Into the Lumbar Disc as Compared to a Placebo
Double-blind, Randamized, Phase 2
44 24Allogenic juvenile
chondrocytes (NuQu) in fibrin carrier.
ISTO Technologies,
Inc.Phase II done
Safety and Preliminary Efficacy Study of Mesenchymal Precursor Cells (MPCs, Mesoblast) in Subjects With Lumbar Back Pain
Double-blind, Randomized, Phase 2
100 366 or 18 million MPCs
(Mesoblast) in a hyaluronic acid carrier
Mesoblast, Ltd.
Phase II done
Treatment of Degenerative Disc Disease With Allogenic Mesenchymal Stem Cells (MSV) (Disc_allo)
Double-blind, Randamized, Phase 1,2
24 1225 millions MSC in 2 ml
of saline
Red de Terapia Celular
Ongoing
Autologous Adipose Tissue Derived Mesenchymal Stem Cells Transplantation in Patient With Lumbar Intervertebral Disc Degeneration
Non-randamized, open label
8 6Autologous Adipose Tissue derived MSCs
K-Stemcell Co Ltd
Ongoing
Adipose Cells for Degenerative Disc DiseaseNon-randamized, open
label100 12
Adipose tissue-derived stem cells suspended in
platelet rich plasmaBioheart, Inc. Ongoing
Intradiscal rhGDF-5 (BMP14) for Early Stage Lumbar DDD
Double-blind, Randamized, Phase 1,2
38 36 rhGDF-5 DePuy Spine Ongoing
Intradiscal rhGDF-5 (BMP14) for Early Stage Lumbar DDD
Case Series10 24
Autologous NP cells from fusion, co-
cultured with bone marrow MSCs
Mochida J. et al
Ongoing
Lumbar Intradiscal PRP injectionsDouble-blind,
Randomized Controlled study
72 6 Single injection of PRP Lutz et. al,
HSS Complete
Intradiscal injection of PRP-releasate for the treatment of lumbar disc degeneration Case-Series 6 6
Injection of the soluble releasate isolated from
clotted PRP
Akedaet. al.,
Complete
Non-published ongoing or terminated clinical trials

10/21/2015
11
Tissue engineering
• Multistep process
– cartilage harvest and cell isolation
– cell growth (proprietary)
– reimplantation
Tissue Engineering in the knee; ACI/ACT Methods
Chondrocyte Transplantation (ACT)
• ACI/ACT commercialized by Genzyme (Carticel®)
• Human trials since ~1990 (reimbursed since 2002)
• Patient load of >10,000 by 2007 (4,000/yr currently)
• Revision surgery for microfracture or OATS

10/21/2015
12
NeoCart
Crawford et al. Am J Sports Med.
Crawford et al. J Bone Joint Surg Am. 2012
A phase 3 product using a patient’s own cartilage cells harvested from the non-weight-bearing cartilage surface of the patient’s femur
ACT/ACI General Results
• New tissue formation
– hyaline cartilage 40-50%
– fibrocartilage 40-50%
• “Success” rate
– 1 year 80-90%
– 2 year 70-80%
– long term 50-80%
• Significant extension of time to TKR (from 3 yr 15+ yr)
http://www.carticel.com
Ear Fabrication From Printed Molds
Photo Reconstruction 8 week culture
10/21/2015
13
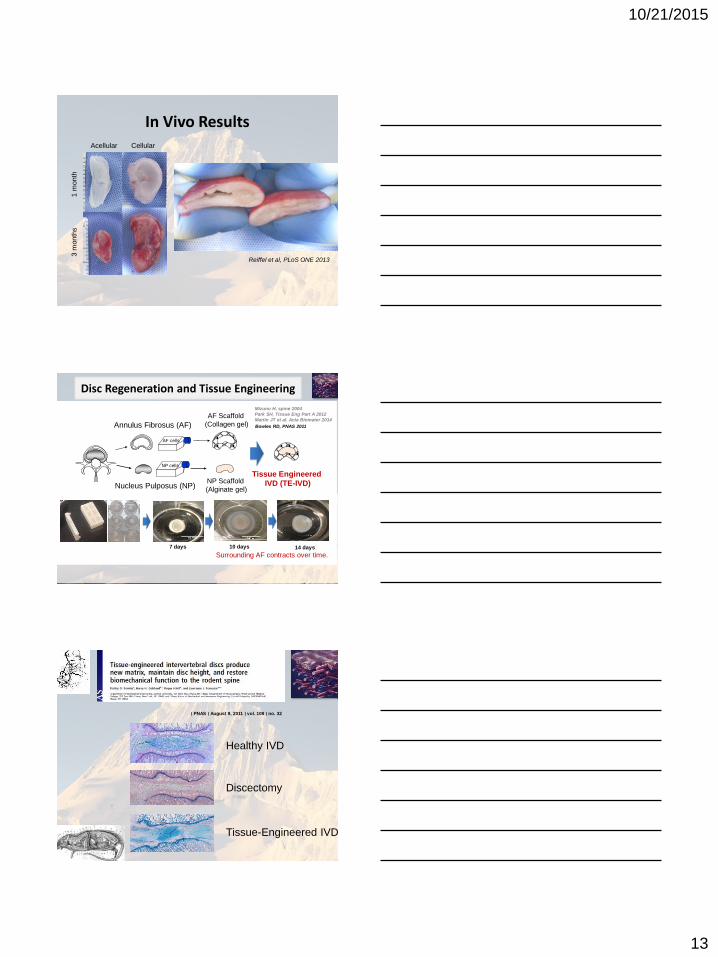
In Vivo Results
Reiffel et al, PLoS ONE 2013
1 m
onth
3 m
onth
s
Acellular Cellular
Disc Regeneration and Tissue Engineering
10 days7 days 14 days
Surrounding AF contracts over time.
AF Scaffold
(Collagen gel)
NP cells
Annulus Fibrosus (AF)
Nucleus Pulposus (NP)
AF cells
NP Scaffold
(Alginate gel)
Tissue Engineered
IVD (TE-IVD)
Bowles RD, PNAS 2011
Mizuno H, spine 2004
Park SH, Tissue Eng Part A 2012
Martin JT et al. Acta Biomater 2014
∣ PNAS ∣ August 9, 2011 ∣ vol. 108 ∣ no. 32
Healthy IVD
Discectomy
Tissue-Engineered IVD

10/21/2015
14
Qualitative MRI analysis:
Bio-engineered Disc
Post-op 1 month 4.5 month 8 month

10/21/2015
15
Experimental Protocol
・Solely discectomized discs (n=2)
・Discs implanted with TE-IVD (n=12)
Size ⇔ Voxel Count
Hydration ⇔ T2 Relaxation Time
MRI-based analysis of nucleus pulposus (NP)
Grunert P et al. ORS 2014, Spine 2014
X ray & MRI
Histological analysis
2 4 8 16 weeksDiscectomy
Post-operative Assessment
Adjacent Healthy
Discectomy
10mm 500 um
X ray T2 MRIs Safranin OT2 Mapping
16 week
16 week
TE-IVD Implantation
4 week
16 week
Histological Assessment with Safranin O staining
White and black arrows indicate NP-like and AF-like cells, respectively. VB; Vertebral Body, Bars; 100 μm
VB
VB
4-week TE-IVD 16-week TE-IVDAdjacent Disc Discectomy
VBVB
VB VB
VB
VB
NP
AF

10/21/2015
16
In Vivo Total Disc Replacement Using Tissue Engineered Disc Implant
Implanted TE-IVDs
• Maintain its position and integrated into the native tissue
• Restore disc height and physiological hydration
• Yielded disc-like tissues over 16 weeks
• Problem with surgery:
– “Hole in disc”
– Reherniation relates to size of the defect
– up to 15% experience recurrence
– Progressive degeneration
– “Sealing the hole” ??
Annular Defect Repair
Cross-linked high density collagen gel
• Stiffer collagen with increased
equilibrium modulus
• Decreased hydraulic
permeability
• Highly biocompatible,
supporting cell migration and
matrix rearrangement
(Zhang 2011, Cross 2010, Puetzer JL
2013).
Rat -Tail Needle Puncture Model
10/21/2015
17
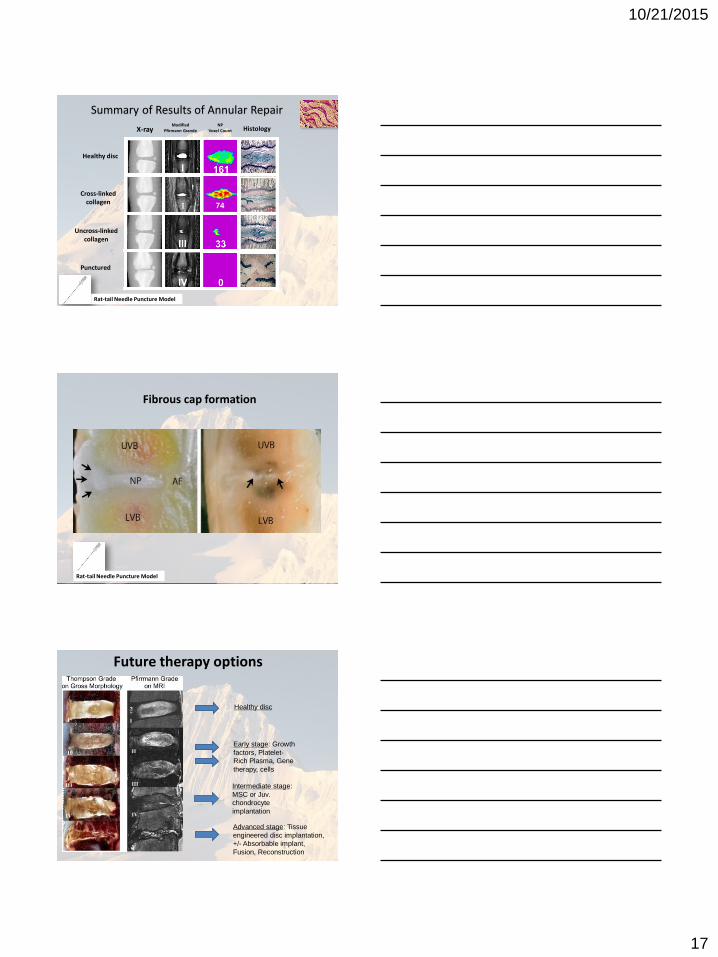
74I
Healthy disc
Uncross-linked collagen
Cross-linked collagen
Punctured
X-rayModified
Pfirmann GrandeNP
Voxel Count Histology
Summary of Results of Annular Repair
Rat-tail Needle Puncture Model
Fibrous cap formation
Rat-tail Needle Puncture Model
Future therapy options
Healthy disc
Early stage: Growth
factors, Platelet-
Rich Plasma, Gene
therapy, cells
Intermediate stage:
MSC or Juv.
chondrocyte
implantation
Advanced stage: Tissue
engineered disc implantation,
+/- Absorbable implant,
Fusion, Reconstruction
10/21/2015
18
52
Summary
– Promising initial clinical results
– Questions• Growth factors
• Gene therapy
• Cells– Type
– Indications & Timing
• Allogeneic Disc transplants
• Tissue engineering work– Total disc replacement
– Combination with structural implants / stabilization
The slides below are for reference
Tissue-Engineered Total
Disc Replacement
Tissue-engineered total disc
replacement (TE-TDR)
–Restore Motion
–Mechanical damping
– Integrate with the native tissue
–Produce a disc like extracellular matrix

10/21/2015
19
Disc Fabrication
AF Scaffold
implant
NP cells
AF cells
Annulus Fibrosus (AF)
Nucleus Pulposus (NP)
NP
Scaffold
∣ PNAS ∣ August 9, 2011 ∣ vol. 108 ∣ no. 32
Healthy IVD
Discectomy
Tissue-Engineered IVD

10/21/2015
20
Qualitative MRI analysis:
Bio-engineered Disc
Post-op 1 month 4.5 month 8 month
Beagle C3/4 biological disc at 4 weeks
500μm
Beagle MRI

10/21/2015
21
• Leading cause of disability worldwide.
• 480,000 operations per year in US for DDD.
• Conventional surgery does not treat underlying pathology (degeneration).
• Following fusion, 21.5% require reoperations (Martin BI, 2007).
Low Back Pain (LBP) &
Degenerative Disc Disease (DDD)
Fusion
Extended
Fusion
Prosthetic
TDR
Canine Postnucleotomy Disc Cells 6.0x106
cells/1ml/ Disc Disc remained viable, produced ECM,
better maintained disc heightGaney T 2003,
Hohaus C 2008
Porcine Nucleotomy Allogeneic Juvenile Chondrocytes and
MSCs
7-10 x106 / 0.5-75ml
fibrin carrier
JC outperformed MSCs in proteoglycan synthesis at 12 months
Acosta 2011
Porcine Postnucleotomy Human MSCs 0.5x106 / hydrogel carrier
Implanted human MSCs survived and differentiated into disc-like cells at 6 mos.
Henriksson HB 2009
Canine Postnucleotomy Autologous MSCs 1.0x106 /ml Stem cells
MSCs led to better disc height,MRI, and histology grading at 12 weeks
Hiyama A 2008
Canine Postnucleotomy Bone Marrow MSCs 105 , 106, 107
cells The disc treated with 106 MSCs showed
more viable cells than 105 and less apoptotic cells than 105 cells at 12
weeks.
Serigano K 2010
Table 2: Published Large Animal In vivo Studies of Cell Therapy in Disc Regeneration
Species Model Cell Type Dose Outcome Reference
Porcine Nucleotomy Cell-scaffold made of NP cells and an injectable hyaluronan-derived polymeric substitute material
Injected discs had a central NP-like region with viable chondrocytes forming matrix
Revell 2007
Canine Post-nucleotomy Autologous adipose tissue derived stem and regenerative cells in hyaluronic acid carrier
Disc produced matrix and resembled native disc in morphology at 12 months
Ganey T 2009
Canine Total discectomy Cell-allograft IVD with allograft and NP cells transduced with hTERT expressing viral vector
Addition of hTERT-loaded NP cells inducedresistance to allogenic disc degeneration
Xin H 2013
Canine Nucleotomy Cell-scaffold composite made of three-dimensional porous PLGA scaffolds and NP cells
Disc height, segmental stability, and T2-weighted MRI signal were preserved
Ruan DK 2010
Sheep Total Discectomy Absorbable interbody cage filled with mesenchymal progenitor cell and pentosan polysulfate
Production of cartilaginous tissue at 3 months Goldschlager T. Neurosurg Focus
2010.
Sheep Nucleotomy Allogenic disc cells in hydrogel containing hyaluronic acid and maleolyl-albumin.
Intrinsic repair of traumatic damage occurs in sheep discs at 6 mo.
Benz K 2012
Porcine Post-annularInjury
Autologous MSCs in either HydrogelPhotoFix (PF) or Hyaluronic Acid (HA)
Treatment group had higher T2 MRI intensities and lower degeneration.
Bendtsen 2011
Porcine Partial nucleotomy Bone marrow MSCs transduced with retrovirus encoding luciferase in albumin hydrogel
After 3 days, persistent metabolically active implanted cells in the disc
Olmor GW, 2014
Goat Post-disc injury Bone marrow stromal cells in chondroitin sulfate-based hydrogel
Significant increase in NP proteoglycan accumulation at 6 months.
Zhang Y, 2011
Sheep Post-chondroitinase-ABC injection
Human Mesenchymal Precursor cells (MPCs) suspended in hyaluronic acid
High dose injection improved histopathology scores at 3 mos., while low dose at 6 mos.
Ghosh P 2012
Table 3: Published Large Animal In vivo Studies of Tissue Engineering in Disc Regeneration
Species Model Construct Outcome Reference

10/19/2015
1
State of The Art
Hyun Bae, M.D.
Medical Director, Director of Education
Cedars Spine Center
Future of Regenerative Medicine in Spine

10/19/2015
2
Chronic Axial Lumbar Back Pain
Patient profile
•12.5M Patients annually present with chronic
(>6 months), low back pain in the United
States
•Only 20% present with evidence of an easily
imaged pathology or anatomic source of pain
•10M U.S. patients annually present with
symptoms of discogenic pain:
• Chronic axial low back pain (> 6 months)
• Referred leg pain that is less than back pain
• Mild to moderate disc generation at 1 or
more adjacent levels
• No significant instability or disc height loss
• Minimal central canal or foraminal stenosis
L2-3
L3-4
L4-5
Control
24 New Zealand White Rabbits (3.5 kg)
Special needle with a stopper to control the puncture depth at 5 mm.
Experimental group
1: Lactose injection : 10 ųl of 5% lactose
2: OP-1 injection: 100 ųg of OP-1
4 weeks after the puncture
Animal Model: Acute Disc Injury
DDD LBP
Current Models
No Symptoms
10/19/2015
3
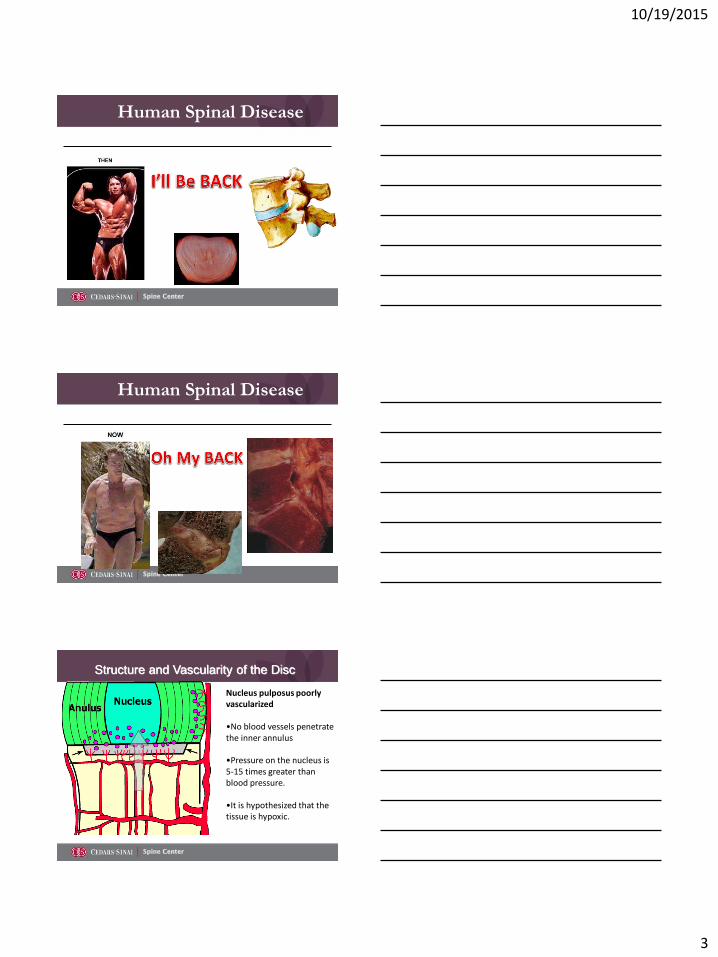
Human Spinal Disease
Human Spinal Disease
Structure and Vascularity of the Disc
Nucleus pulposus poorly vascularized
•No blood vessels penetrate the inner annulus
•Pressure on the nucleus is 5-15 times greater than blood pressure.
•It is hypothesized that the tissue is hypoxic.

10/19/2015
4
Pre-Op MRI
BSF 03-020
OP-1 rhGDF-5Pre-Op MRI
CAL 03-019
Delivery System Benefits
· Percutaneusinjection of fibrin sealant (BIOSTAT BIOLOGX®)
· Flows into and seals fissures
· Fibrin matrix
· Clinical Study
· Biostat System
· Phase III
· Internal disc disruptions (IDD) of lumbar intervertebral discs
· 15 sites, N=260
· One or two level, randomized, blinded
· First patient in February 2010
Fibrin Glue Study

10/19/2015
5
MRI L4-5 Disc Degeneration,Example pt treated with Fibrin Sealant
pre injection post injection follow-up
11-003 wdo Fibrin Sealant
Biostat Fibrin Sealant for
Intervertebral Disc Repair
Results of the Randomized Clinical Trial:
One Site Analysis
Presenter – Hyun Bae, MD
Demographics
Except for smoking status,
Demographics were similar
BioStat Saline
Number of patients 20 9
% Males 55.3 66.7
Age (years) 38.6 44.1
% Current Smokers 30% 0
% Prior Injections 80% 100%
% Prior Surgery 0 0
% Follow-up @ 12 mo 100% 100%
Study is closed
Randomized
10/19/2015
6
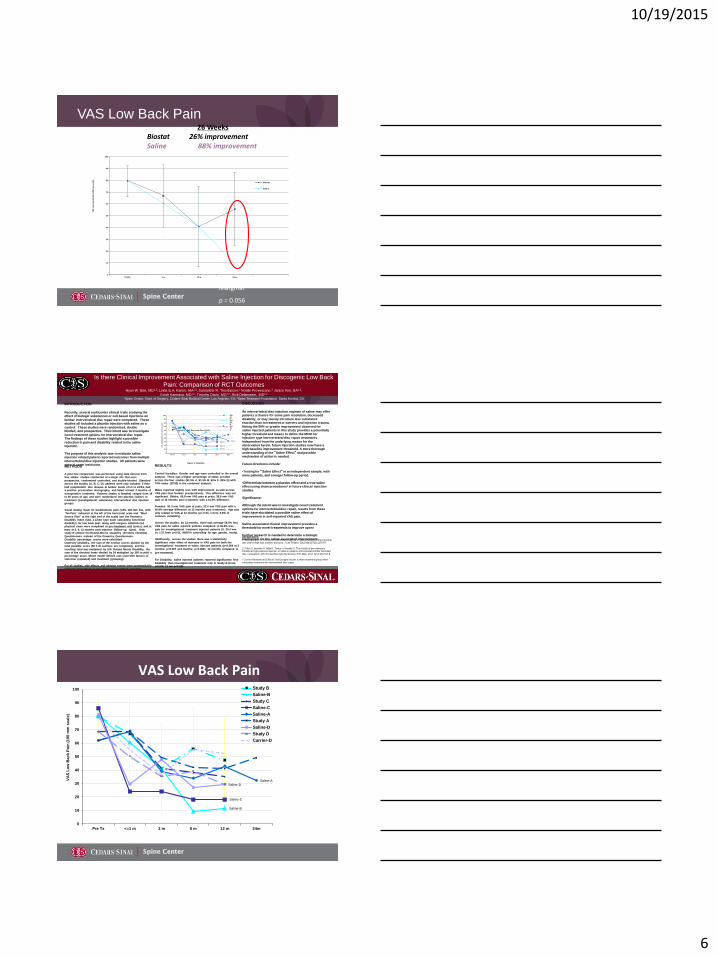
VAS Low Back Pain26 Weeks
Biostat 26% improvementSaline 88% improvement
0
10
20
30
40
50
60
70
80
90
100
PreOp 1 w 13 w 26 w
VA
S L
ow
Ba
ck
Pa
in (
10
0 m
m s
ca
le)
Biostat
Saline
Marginal
p = 0.056
INTRODUCTION
Recently, several multicenter clinical trials studying the effect of biologic substances or cell-based injections on
lumbar intervertebral disc repair were completed. These studies all included a placebo injection with saline as a
control. These studies were randomized, double blinded, and prospective. Their intent was to investigate
novel treatment options for intervertebral disc repair. The findings of these studies highlight a possible
reduction in pain and disability related to the saline injection.
The purpose of this analysis was to evaluate saline injection related patient reported outcomes from multiple
intervertebral disc injection studies. All patients were seen at same institution.METHODS
A post hoc comparison was performed using data derived from
four similar studies conducted at a single site that were
prospective, randomized controlled, and double-blinded. Standard
across the studies (A, B, C, D), patients were only included if they
had symptomatic disc disease at lumbar levels of L1 to L5/S1, had
a positive provocative discography, and failed at least 3 months of
nonoperative treatment. Patients (males & females) ranged from 18
to 65 years of age, and were randomized into placebo (saline) or
treatment (investigational substance) intervertebral disc injection
groups.
Visual Analog Scale for back/buttock pain (VAS, 100-mm line, with
‘No Pain’ indicated at the left of the horizontal scale and ‘Most
Severe Pain’ at the right end of the scale) and the Oswestry
Disability Index (ODI, a Likert type scale calculating functional
disability) for low back pain, along with surgeon administered
physical exam were completed at pre-treatment visit (pretx), and at
least at 3, 6, 12 months post injection (follow-up, 12mo). Only
study B utilized the Roland-Morris Disability (24 items checklist)
Questionnaire instead of the Oswestry Questionnaire.
Disability percentage scores were calculated:
Oswestry Disability, the sum of the section scores divided by the
total possible score (50 if all sections are completed), and the
resulting total was multiplied by 100. Roland Morris Disability, the
sum of the checked items divided by 24 multiplied by 100 to yield a
percentage score. Mixed model ANOVA was used with factors of
visit-time (repeated) and treatment (grouping).
For all studies, side effects and adverse events were systematically
collected throughout as per clinical trial standard operating
procedures at the site.
RESULTS
Control Variables: Gender and age were controlled in the overall
analysis. There was a higher percentage of males enrolled
across the four studies (61.5% A, 61.5% B, 60% C, 94% D) with
74% males (37/50) in the combined analysis.
Males reported slightly less VAS improvement as well as less
VAS pain than females preoperatively; This difference was not
significant. (Males: 66.8 mm VAS pain at pretx, 39.6 mm VAS
pain at 12 months post treatment, with a 41.5% difference.
Females: 81.3 mm VAS pain at pretx, 32.4 mm VAS pain with a
40.6% average difference at 12 months post treatment). Age was
only related to VAS at 12 months (p< 0.04, r=0.31, 9.6% of
common variability).
Across the studies, by 12 months, there was average 58.5% less
VAS pain for saline injected patients compared to 36.6% less
pain for investigational treatment injected patients (S: 20.4 mm
vs. I:37.7mm p<0.01, ANOVA controlling for age, gender, study).
Additionally, across the studies there was a statistically
significant main effect of decrease in VAS pain for both the
investigational treatment or saline injected patients (p<0.004 at 3
months; p<0.007 at 6 months; p<0.0001, 12 months compared to
pre-treatment).
For Disability, saline injected patients reported significantly less
Disability than investigational treatment only in Study B (6 mo,
p<0.04; 12 mo p<0.05).
Is there Clinical Improvement Associated with Saline Injection for Discogenic Low Back
Pain: Comparison of RCT OutcomesHyun W. Bae, MD1,2, Linda E.A. Kanim, MA1,2, Samantha R. Thordarson,1 Noelle Provenzano,1 Janice Kim, BA1,2,
Evish Kamrava, MD1,2, Timothy Davis, MD1,2, Rick Delamarter, MD1,2
1Spine Center, Dept. of Surgery, Cedars-Sinai Medical Center, Los Angeles, CA; 2Spine Research Foundation, Santa Monica, CA
REFERENCES
1: Mavrogonatou E, Kletsas D. Differential response of nucleus pulposus intervertebral disc cells to high salt, sorbitol, and urea. J Cell Physiol. 2012 Mar;227(3):1179-87.
2: Fukui S, Iwashita N, Nitta K, Tomie H, Nosaka S. The results of percutaneous intradiscal high-pressure injection of saline in patients with extruded lumbar herniated
disc: comparison with microendoscopic discectomy. Pain Med. 2012 Jun;13(6):762-8.
* Current Randomized Clinical Trial Designs include a sham treatment group when
evaluating treatments for intervertebral disc repair.
DISCUSSION
An intervertebral disc injection regimen of saline may offer patients a chance for some pain resolution, decreased
disability, or may merely introduce less substance reaction than to treatment or carriers and injection trauma.
Noting the 50% or greater improvement observed for saline injected patients in this study provides a potentially
higher threshold and means to define the MCID for injection type intervertebral disc repair treatments.
Independent from the underlying reason for the observation herein, future injection studies now have a high baseline improvement threshold. A more thorough
understanding of the “Saline Effect” and possible mechanism of action is needed.
Future directions include:
•Testing for “Saline Effect” in an independent sample, with
more patients, and a longer follow-up period.
•Differentiate between a placebo effect and a true saline effect using sham procedures* in future clinical injection
studies.
Significance:
Although the intent was to investigate novel treatment
options for intervertebral disc repair, results from these trials have elucidated a possible saline effect of
improvement in self-reported VAS pain.
Saline-associated clinical improvement provides a threshold for novel treatments to improve upon!
Further research is needed to determine a biologic
mechanism for the saline-associated improvement.
Figure 2. Disability
Figure 1. Self Reported Pain (VAS)
Saline-B
Saline-C
Saline-ASaline-D
0
10
20
30
40
50
60
70
80
90
100
Pre Tx <=1 m 3 m 6 m 12 m 24m
VAS
Lo
w B
ac
k P
ain
(1
00
mm
sc
ale
)
StudyBSaline-BStudyC
VAS Low Back Pain
Saline-B
Saline-C
Saline-A
Saline-D
0
10
20
30
40
50
60
70
80
90
100
Pre Tx <=1 m 3 m 6 m 12 m 24m
VA
S L
ow
Bac
k P
ain
(1
00
mm
sc
ale
)
Study B
Saline-B
Study C
Saline-C
Saline-A
Study A
Saline-D
Study D
Carrier-D

10/19/2015
7
Results
•Four RCT using saline as control
• 58.5% decrease in patients at 12 months
treated with saline
•36.6% decrease in pateints at 12 months
treated with investigational drug
•p<0.04
Allogeneic Stem Cell TherapyAllogeneic Stem Cells– The Future?
Stem Cell Pool
10/19/2015
8
Bioreactor Cell Processing
Commercial Viability
Cell Bank to Provide Off the Shelf Solution
24
Products ForEye Diseases
bone
cartilage
Isolated Cells
US Composition Patentgranted
Culture-expanded Cells
US Manufacturing Process Patent
granted
heart muscle
pancreas
US Bone RepairPatent granted
OrthopaedicProducts
Products ForCardiacDiseases + Diabetes
Blood vessel
MPC Highly Expandable + Non-Immunogenic
beads/magnet
bone marrow+ antibody
Global Use Patentsfiled
10/19/2015
9
25
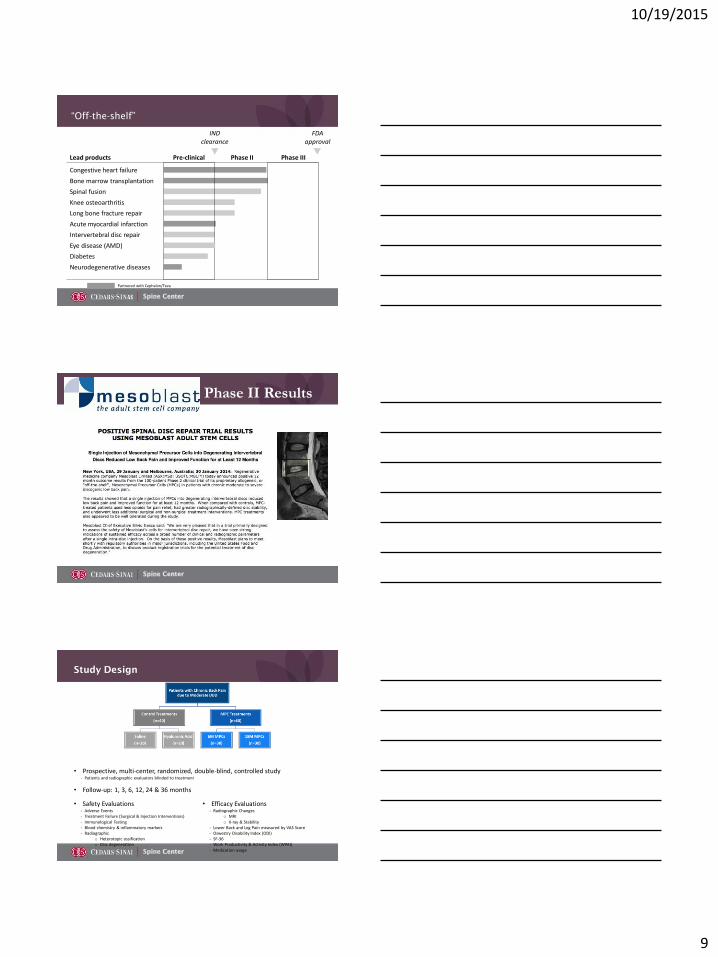
“Off-the-shelf”
Lead products
Congestive heart failure
Bone marrow transplantation
Spinal fusion
Knee osteoarthritis
Long bone fracture repair
Acute myocardial infarction
Intervertebral disc repair
Eye disease (AMD)
Diabetes
Neurodegenerative diseases
Pre-clinical Phase II Phase III
IND clearance
FDA approval
Partnered with Cephalon/Teva
Phase II Results
Study Design
• Prospective, multi-center, randomized, double-blind, controlled study- Patients and radiographic evaluators blinded to treatment
• Follow-up: 1, 3, 6, 12, 24 & 36 months
• Safety Evaluations- Adverse Events- Treatment Failure (Surgical & Injection Interventions)- Immunological Testing- Blood chemistry & inflammatory markers- Radiographic
o Heterotopic ossificationo Disc degeneration
• Efficacy Evaluations- Radiographic Changes
o MRIo X-ray & Stability
- Lower Back and Leg Pain measured by VAS Score- Oswestry Disability Index (ODI)- SF-36- Work Productivity & Activity Index (WPAI)- Medication usage
10/19/2015
10
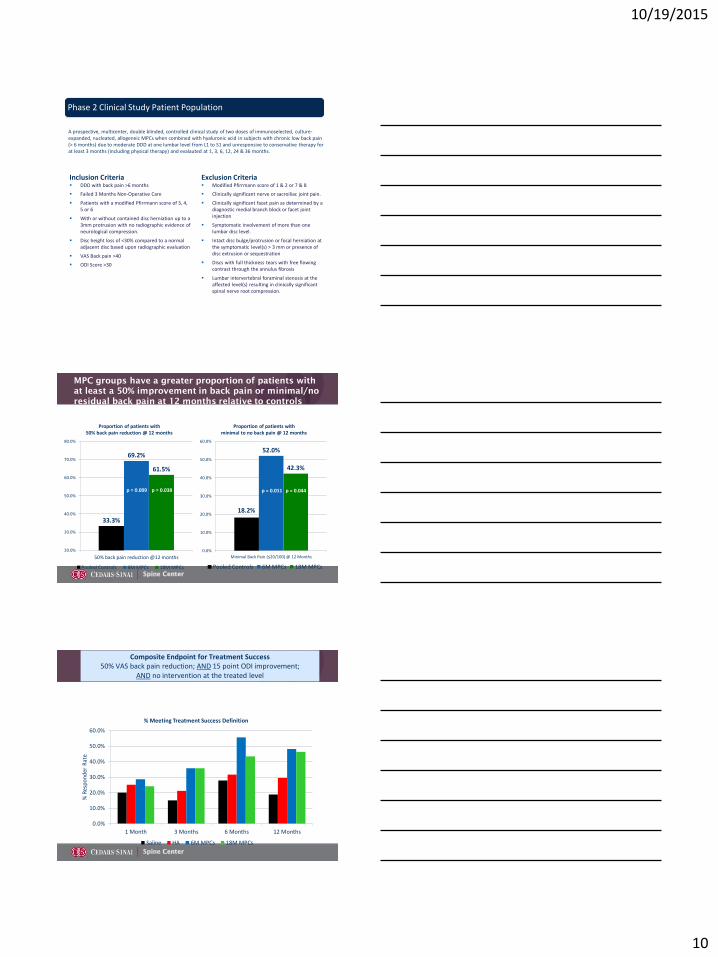
Inclusion Criteria DDD with back pain >6 months
Failed 3 Months Non-Operative Care
Patients with a modified Pfirrmann score of 3, 4, 5 or 6
With or without contained disc herniation up to a 3mm protrusion with no radiographic evidence of neurological compression.
Disc height loss of <30% compared to a normal adjacent disc based upon radiographic evaluation
VAS Back pain >40
ODI Score >30
Exclusion Criteria Modified Pfirrmann score of 1 & 2 or 7 & 8
Clinically significant nerve or sacroiliac joint pain.
Clinically significant facet pain as determined by a diagnostic medial branch block or facet joint injection
Symptomatic involvement of more than one lumbar disc level.
Intact disc bulge/protrusion or focal herniation at the symptomatic level(s) > 3 mm or presence of disc extrusion or sequestration
Discs with full thickness tears with free flowing contrast through the annulus fibrosis
Lumbar intervertebral foraminal stenosis at the affected level(s) resulting in clinically significant spinal nerve root compression.
Phase 2 Clinical Study Patient Population
A prospective, multicenter, double blinded, controlled clinical study of two doses of immunoselected, culture-expanded, nucleated, allogeneic MPCs when combined with hyaluronic acid in subjects with chronic low back pain (> 6 months) due to moderate DDD at one lumbar level from L1 to S1 and unresponsive to conservative therapy for at least 3 months (including physical therapy) and evalauted at 1, 3, 6, 12, 24 & 36 months.
MPC groups have a greater proportion of patients with
at least a 50% improvement in back pain or minimal/no
residual back pain at 12 months relative to controls
33.3%
69.2%
61.5%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
50% back pain reduction @12 months
Proportion of patients with 50% back pain reduction @ 12 months
Pooled Controls 6M MPCs 18M MPCs
p = 0.009 p = 0.038p = 0.009 p = 0.038
18.2%
52.0%
42.3%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
Minimal Back Pain (≤20/100) @ 12 Months
Proportion of patients with minimal to no back pain @ 12 months
Pooled Controls 6M MPCs 18M MPCs
p = 0.011 p = 0.044
MPCs groups show sustained treatment effect relative to controls
over 12 months
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
1 Month 3 Months 6 Months 12 Months
% R
esp
on
der
Rat
e
% Meeting Treatment Success Definition
Saline HA 6M MPCs 18M MPCs
Composite Endpoint for Treatment Success50% VAS back pain reduction; AND 15 point ODI improvement;
AND no intervention at the treated level

10/19/2015
11
MPC groups have a significantly greater proportion of patients witha 50% pain reduction with no intervention compared to saline @ 24 months
p = 0.009 p = 0.038
p = 0.024vs. saline
p = 0.020vs. saline
18.8%
60.9%
47.8%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
Pro
po
rtio
n o
f P
atie
nts
50% back pain reduction with no intervention @ 24 months
Saline 6 million MPCs 18 million MPCs
p = 0.020vs. saline
p = 0.093vs. saline
MPC groups have a significantly greater proportion of patients with clinically significant function improvement and no intervention compared to saline @ 24 months
18.8%
56.5%60.9%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
Pro
po
rtio
n o
f Pa
tien
ts
15 point ODI improvement with no intervention @ 24 months
Saline 6 million MPCs 18 million MPCs
p = 0.009 p = 0.038
p = 0.024vs. saline
p = 0.020vs. saline
p = 0.020vs. saline
p = 0.093vs. saline
Conclusion
•Allogeneic MPCs were well tolerated
•Both MPC doses showed improvement relative to controls for
pain and functional improvement and reduced interventions
•Radiographic improvement in disc motion suggests
improvement in disc structure and stability
•Over three fold increase in the number of MPC treated patients
achieving concordant pain and function treatment success at
both 6 and 12 months relative to saline controls
•Next steps: Randomized, placebo controlled phase 3 trials
comparing 6M MPCs to saline placebo
10/19/2015
12
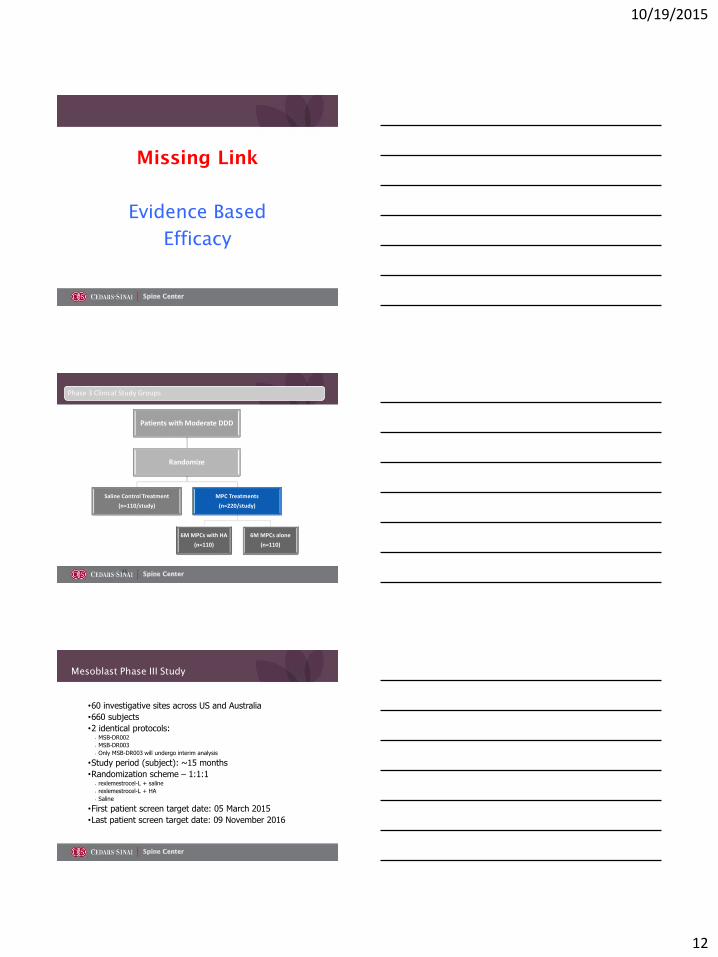
Missing Link
Evidence Based
Efficacy
35
Patients with Moderate DDD
Randomize
Saline Control Treatment
(n=110/study)
MPC Treatments
(n=220/study)
6M MPCs with HA
(n=110)
6M MPCs alone
(n=110)
Phase 3 Clinical Study Groups
Mesoblast Phase III Study
•60 investigative sites across US and Australia
•660 subjects
•2 identical protocols:• MSB-DR002
• MSB-DR003
• Only MSB-DR003 will undergo interim analysis
•Study period (subject): ~15 months
•Randomization scheme – 1:1:1• rexlemestrocel-L + saline
• rexlemestrocel-L + HA
• Saline
•First patient screen target date: 05 March 2015
•Last patient screen target date: 09 November 2016

10/19/2015
13
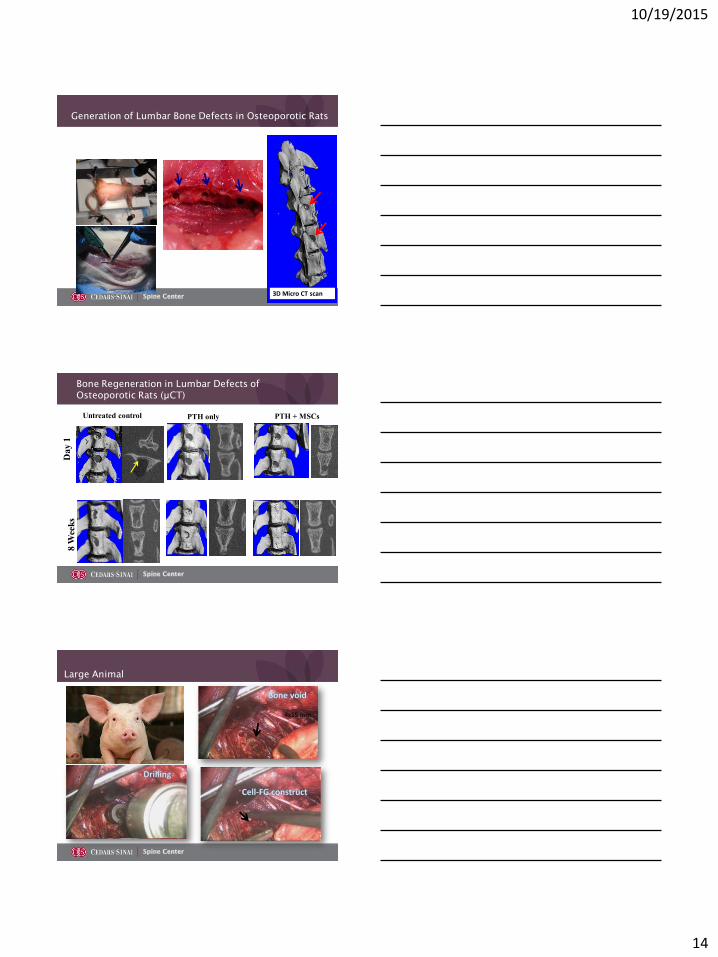
CIRM
Created by Californians in 2004 with Prop 71 to Provide 3 Billion dollars for Stem Cell Research and Clinical Applications
Gazit and Bae team awarded $7.1 million from CIRM to develop stem cell treatments for osteoporosis and segmental defects
Goal is to develop world's first biological treatment for compression fractures
Systemic Adult Stem Cell
Therapy for Osteoporosis-
Related Vertebral Compression
Fractures
•CIRM Early Translational II Award (TR2-01780)
Hyun Bae and Dan Gazit
Co PIs
Proposed therapy
MSC Injection
PTH
MSCs
Regenerated Vertebra
10/19/2015
14
Generation of Lumbar Bone Defects in Osteoporotic Rats
3D Micro CT scan
Da
y 1
Untreated control
8 W
eek
s
PTH + MSCsPTH only
Bone Regeneration in Lumbar Defects of
Osteoporotic Rats (µCT)
Large Animal
4x15 mm

10/19/2015
15
Validation of design in larger animals
THANK YOU
















![Percutaneous Endoscopic Lumbar Spine Surgery for …1.1. Lumbar Disc Herniation (LDH) Lumbar disc herniation [1][2] [3] (Figure 1(a)) is a medical condition affecting the spine in](https://img.pdfslide.us/doc/110x75/5f01e5a17e708231d4019244/percutaneous-endoscopic-lumbar-spine-surgery-for-11-lumbar-disc-herniation-ldh.jpg)