Embed Size (px)
Citation preview
Arch. Dis. Childh., 1965, 40, 411.
BIOCHEMICAL, PHARMACOLOGICAL,AND HISTOCHEMICAL STUDIES IN NEUROBLASTOMA
BY
P. P. ANTHONY, H. M. T. COLES, JOHN PRYSE-DAVIES, and LEONARD SINCLAIRFrom Westminster Children's Hospital and the Vincent Square Laboratories of Westminster Hospital
(RECEIVED FOR PUBLICATION FEBRUARY 3, 1965)
In recent years there has been some interest in theautonomic effects produced by neural crest tumoursand in their biochemical characteristics. Hyper-tension and diarrhoea have been reported in severalcases in which there has also been an excessiveexcretion of catecholamines, their precursors, ormetabolic products (Mason, Hart-Mercer, Millar,Strang, and Wynne, 1957; Isaacs, Medalie, andPolitzer, 1959; Voorhess and Gardner, 1961; Kaserand von Studnitz, 1961; Rosenstein and Engleman,1963; Marsden, 1963). Most investigators havesuggested that these substances have activated thesmooth muscle of arterioles or the intestine toproduce these effects. However, in other reportedcases (Wilkins, 1957; Voorhess and Gardner, 1962)there has been no evidence of excessive secretion ofadreno-medullary metabolites to account for thesemanifestations. Further, Rosenstein and Engleman(1963) and Sourkes, Denton, Murphy, Chavez, andSaint Cyr (1963) recorded cases with no symptomsreferable to autonomically innervated structures butwith significantly increased secretion of catechol-amine derivatives.
This report concerns two cases of metastasizingneuroblastoma and the investigations undertakenupon them. Both had hypertension and in one thiswas associated with diarrhoea and convulsions. Itis thought that the raised blood pressure in one casemight be associated with the excessive production ofcatecholamines by the large tumour mass. In theother patient there is no evidence to indicate that theneuroblastoma produced abnormal amounts ofcatecholamine-like substances during the period ofstudy or that these were responsible for severehypertension and intractable diarrhoea.
Methods
Urinary Excretion of Catecholamines and Metabolites.The combined and individual concentrations of noradren-aline and adrenaline were estimated in 24-hour collections
411
of urine by a fluorometric method based on that ofWeil-Malherbe and Bone (1957). 4-hydroxy-3-methoxy-mandelic acid (HMMA, formerly VMA) was determinedby the spectrophotometric method of Pisano, Crout, andAbraham (1962). The concentration of 4-hydroxy-3-methoxyphenylacetic acid (homovanillic acid, HVA) wasestimated by chromatography according to the methoddescribed by Robinson, Ratcliffe, and Smith (1959).
Storage and Treatment of Tumour Tissue. Blocks ofeach intra-abdominal tumour were removed within 20minutes of death. Tissue for biochemical, pharma-cological, and histochemical investigation was frozenimmediately to -70° C. using solid carbon dioxide andstored at this temperature until required. Some blocksused for immediate histochemical study were frozendirectly on to microtome chucks for use with a cryostat.
Extracts of tumour tissues for biochemical determina-tion of catecholamine concentrations and for pharma-cological estimation of pressor substances were preparedby homogenization at 40 C. in 5% w/v trichloracetic acidusing a Potter-Elvehjem hand homogenizer. Theextracts for pharmacological study were further washedwith diethyl ether to remove excess trichloracetic acid, asrecommended by von Euler (1956).
Other tumour blocks were fixed immediately afterremoval from the body in neutral formalin and Helly'schromate fixative; these were paraffin-embedded and usedfor histological studies and examined for chromaffin cells.
Determination of Catecholamine Concentrations inTumour Tissue. Extracts of weighed amounts of tumourtissue prepared as outlined above were investigated by thefluorimetric method used in the urine studies.
Investigation of Pressor Substances in Tumour Tissue.Washed extracts prepared as above were injected into thefemoral vein of a dog anaesthetized with pentobarbitone,and arterial blood pressure was recorded directly via acannula in the femoral artery (Dr. P. Cliffe). The effectof these extracts on the dog's blood pressure was com-pared with those obtained by injecting a standardnoradrenaline solution, trichloracetic acid extracts ofother tissues including a phaeochromocytoma, andsaline extracts of the tumour and other tissues.
copyright. on 17 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.40.212.411 on 1 A
ugust 1965. Dow
nloaded from
ANTHONY, COLES, PRYSE-DAVIES, AND SINCLAIRHistochemical Investigation of Tumour Tissue.
Chromate fixation was used in an attempt to demonstratechromaffin granules. The presence of noradrenaline wassought in 50,u cryostat sections fixed in formol calcium(Eranko, 1955). The presence of ganglioneuromatousdifferentiation was investigated by enzyme histochemicalmeans by studying non-specific esterase and cholinesteraseactivities in 15it cryostat sections, using an azo dyecoupling method and a modification of Gomori'sacetylthiocholine technique respectively (details given byPearse, 1960).As monoamine oxidase plays an important role in the
breakdown of adrenaline and noradrenaline in thetissues, the presence of this enzyme was also investigated.Employing the method of Glenner, Burtner, and Brown(1957) and 15,u cryostat sections of fresh tissue, trypta-mine hydrochloride was used as the substrate, and activitywas shown by the reduction of Nitro blue tetrazolium(Sigma Chemical Company). The specificity of thismethod was checked by using control sections pre-incubated for 30 minutes in 0 * 01 M Iproniazid (Marsilid,Roche Products) as a monoamine oxidase inhibitor.
Case ReportsCase 1. M.V., a male infant, was delivered normally
at full term on July 20, 1961, weighing 7 lb. (3,175 g.).The mother had not been ill nor had she taken any drugsduring pregnancy. The child was admitted to QueenMary's Hospital for Children, Carshalton, at the age of 1year suffering from streptococcal tonsillitis and iron-deficiency anaemia. Two months later, aged 14 months,he was readmitted with fever and a history of anorexia,vomiting, and increasing pallor. A large, irregular masswas palpable in the left upper quadrant of the abdomen.The Hb had fallen to 38 %, but no abnormal cells weredetected in the peripheral blood film.
Shortly after his transfer to Westminster Children'sHospital, when aged 15 months, he developed a unilateralconvulsion involving the right side of the face and body.This soon became generalized and continued for an hour
HMMAEXCRETION(mg./day)
200-
180-
160-
x. 140-
E 120-E
00-80
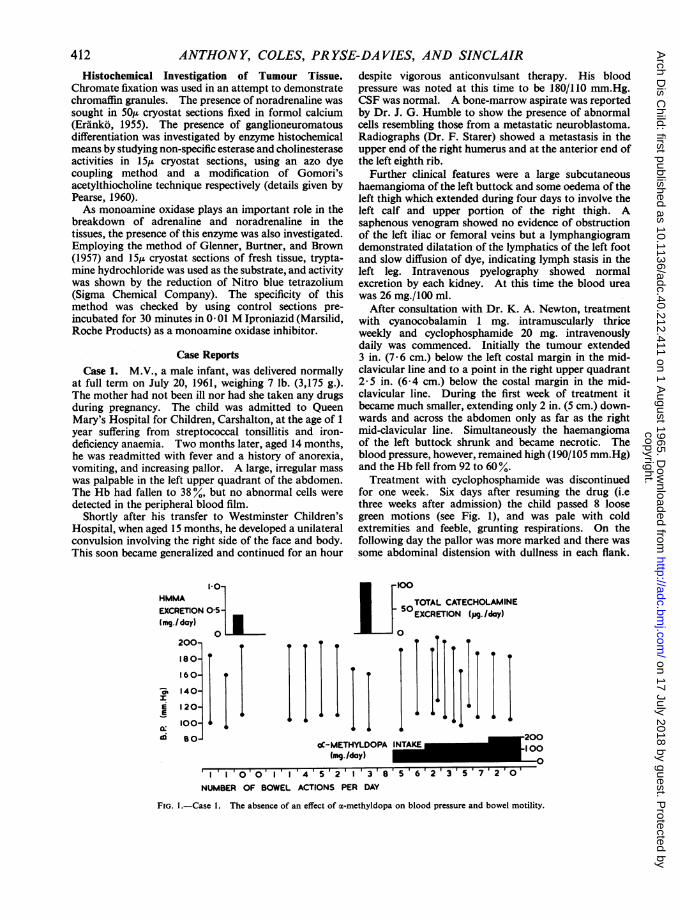
FIG. 1.-Case 1. The absence of an effect of a-methyldopa on blood pressure and bowel motility.
I
despite vigorous anticonvulsant therapy. His bloodpressure was noted at this time to be 180/110 mm.Hg.CSF was normal. A bone-marrow aspirate was reportedby Dr. J. G. Humble to show the presence of abnormalcells resembling those from a metastatic neuroblastoma.Radiographs (Dr. F. Starer) showed a metastasis in theupper end of the right humerus and at the anterior end ofthe left eighth rib.
Further clinical features were a large subcutaneoushaemangioma of the left buttock and some oedema of theleft thigh which extended during four days to involve theleft calf and upper portion of the right thigh. Asaphenous venogram showed no evidence of obstructionof the left iliac or femoral veins but a lymphangiogramdemonstrated dilatation of the lymphatics of the left footand slow diffusion of dye, indicating lymph stasis in theleft leg. Intravenous pyelography showed normalexcretion by each kidney. At this time the blood ureawas 26 mg./100 ml.
After consultation with Dr. K. A. Newton, treatmentwith cyanocobalamin 1 mg. intramuscularly thriceweekly and cyclophosphamide 20 mg. intravenouslydaily was commenced. Initially the tumour extended3 in. (7 6 cm.) below the left costal margin in the mid-clavicular line and to a point in the right upper quadrant2- 5 in. (6-4 cm.) below the costal margin in the mid-clavicular line. During the first week of treatment itbecame much smaller, extending only 2 in. (5 cm.) down-wards and across the abdomen only as far as the rightmid-clavicular line. Simultaneously the haemangiomaof the left buttock shrunk and became necrotic. Theblood pressure, however, remained high (190/105 mm.Hg)and the Hb fell from 92 to 60 %.Treatment with cyclophosphamide was discontinued
for one week. Six days after resuming the drug (i.ethree weeks after admission) the child passed 8 loosegreen motions (see Fig. 1), and was pale with coldextremities and feeble, grunting respirations. On thefollowing day the pallor was more marked and there wassome abdominal distension with dullness in each flank.
4 _200eC-METHYLDOPA 100
(mg./day)III 00 '4I'54'5'125I'23856235720'NUMBER OF BOWEL ACTIONS PER DAY
412
copyright. on 17 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.40.212.411 on 1 A
ugust 1965. Dow
nloaded from
BIOCHEMICAL STUDIES IN NEUROBLASTOMAThe Hb had fallen to 40% and he was thought to havehad a retroperitoneal haemorrhage. After transfusionwith 220 ml. fresh blood the Hb was only 48%. Afurther 170 ml. was given and the Hb rose to 74%. Afluctuant swelling now appeared at the anterior end of theleft eighth rib. This became smaller during the nextthree days and the infant's general condition seemed toimprove though the hypertension persisted.
In an attempt to reduce dopamine formation fromdopa by the tumour and possibly thereby to diminish thediarrhoea as well as to mitigate the hypertension, treat-ment with a-methyldopa at a dosage of 100 mg./day wasstarted two days after the onset of the diarrhoea (seeFig. 1). This was increased to 150 mg./day two dayslater and to 200 mg./day after a further four days. Therewas no fall in the blood pressure or decrease in thediarrhoea during the course of this therapy. On the daybefore death he was comatose and severely dehydrated.Repeated generalized convulsions could not be controlledwith phenobarbitone and paraldehyde. Within 20minutes of death (30 days from admission) necropsy wasperformed and a portion of the tumour removed forestimation of catecholamine content and pharmacologicalactivity.NECROPSY (Dr. I. M. P. Dawson). The abdomen was
protuberant and there was an area of scarring over theleft buttock. A large lobulated tumour weighingapproximately 670 g. (10% of the body weight) was foundarising from the region of the left adrenal gland, carryingthe spleen on the anterior surface, compressing the leftlobe of the liver, the upper pole of the left kidney, andsurrounding the aorta and the inferior vena cava. Thecut surface was necrotic and no adrenal tissue could beidentified. The only metastases found were in the righthumerus and in the 8th left rib near the costal cartilage.The heart was very enlarged, weighing 54 g. andshowing concentric left ventricular hypertrophy. Noother cardiovascular changes were found. The kidneysappeared normal. There was evidence of an oldretroperitoneal haemorrhage.
HIsToLoGY. No adrenal tissue could be identified forcertain. Much of the tumour was necrotic. The growththat remained consisted of loose sheets of round and ovalcells, occasionally forming recognizable rosette structureswith conspicuous fibrous and collagen framework.There was no evidence of conversion to ganglioneuroma.In sections of the kidney there were no vascular changesto suggest arterial hypertension.
Case 2. E.S. was 9 years, when in June 1963 hecomplained ofnausea and pain in the right upper quadrantof the abdomen and was admitted to the London JewishHospital under the care of Dr. S. B. Dimson. There hewas found to have an enlarged liver which was firm andpalpable three fingers breadths below the right costalmargin. The Hb was 70%. A bone-marrow biopsyshowed evidence of round cell infiltration and a needleaspirate of the liver revealed infiltration with similar cells.An intravenous pyelogram demonstrated a centrallyplaced mass in the retroperitoneum displacing the right
kidney laterally. The diagnosis at the time of transfer tothe Westminster Children's Hospital, a month after firstadmission to hospital, was of an intra-abdominalneuroblastoma with metastasis. Just before this he haddeveloped an evening fever, and his leucocyte countshowed a few myelocytes and 2 normoblasts per 100 cellscounted.On admission to Westminster Children's Hospital in
early August the liver had increased in size extending tothe umbilicus and there was a palpable mass in the leftpara-aortic area. The blood pressure was 110/65 mm.Hgand Hb 60%. The only investigations of relevance atthis time were the urinary excretion ofHMMA (3 7 mg./24 hr.) and hydroxymethyl phenylacetic acid (14 mg./24hr.). The serum lactic dehydrogenase was 5,000 unitsand the o-hydroxybutyric dehydrogenase 3,500 units(thought in retrospect to be due to tumour necrosis).
Within one week of admission his condition haddeteriorated and the Hb had fallen to 54%. He wastransfused with 1,200 ml. blood and given mustinehydrochloride 2- 0 mg. intravenously daily. Thisinduced nausea so was discontinued 2 days later andcorticotrophin gel 20 units daily was substituted. Duringthe ensuing week two estimations of 24-hour excretion ofurinary catecholamines were 665 ,ug. and 590 ,tg.,respectively. At this time he was normotensive and hisclinical condition remained unchanged. By the end ofAugust, however, he showed signs of inferior vena cavalobstruction and had collapse/consolidation of the rightlower lobe.One week later his general state was worse, with Hb of
39 %, platelet count of 600/c.mm., and 24-hour catechol-amine excretion of 155 jig. Treatment was changed toprednisone 30 mg./day and he was transfused with 600 ml.packed cells. He appeared to improve but it was notedon the following day that his blood pressure had risen to155/125 mm.Hg and his pulse rate had fallen from 100 to70 per minute. The size of the abdominal mass hadmeanwhile increased and the liver had enlarged, extend-ing to below the umbilicus.Next morning the heart rate suddenly increased to 136
and he rapidly lapsed into unconsciousness, with frothingat the mouth and incontinence of urine and faeces.There was generalized muscular hypotonia and hypore-flexia, with conjugate deviation of the eyes to the right.The CSF pressure was over 300 mm. withi a proteincontent of 40 mg./100 ml. There were 3 lymphocytesand more than 600 erythrocytes/c.mm. No abnormalcells were detected. The patient was treated withintravenous phentolamine and oral guanethidine but thehypertension and tachycardia persisted. The Hb fell to28% and he was again transfused with 1,200 ml. packedcells. He continued to deteriorate and died at the end ofSeptember, less than four months from the onset of hisillness.
NECROPSY (Dr. J. Pryse-Davies). A preliminarynecropsy was performed within 20 minutes of death inorder to remove as freshly as possible specimens of thetumour from the abdomen for storage at -70° C. Thenecropsy was completed 10 hours later.
413
copyright. on 17 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.40.212.411 on 1 A
ugust 1965. Dow
nloaded from
ANTHONY, COLES, PRYSE-DAVIES, AND SINCLAIRTABLE
COMPARISON OF CLINICAL FEATURES AND INVESTIGATIONS ON EACH PATIENT
Case I Case 2
Autonomic effectspresent .Tachycardia, hypertension,. Tachycardia, hypertensionand diarrhoea
Response to phentolamine .Fall in blood pressure No changeResponse to a-methyldopa .None
In presence of Before onset of After onset ofhypertension hypertension hypertension
Total daily urinary excretion of catecholamines (,ug.) 103 665 and 590 340 and 142Daily urinary excretion ofHMMA (mg.) .. . 04 and 2-3 - 3-7Daily urinary excretion of HVA (mg.) .. . - 14-0Concentration of catecholamines in tumour (wet weight) Nil - 3 0 ,Lg./g.Effect of tumour extract on dog blood pressure Nil _ Rise
The body was that of a wasted child with a protuberantabdomen due to a large retroperitoneal mass whichpushed the liver forwards and was closely applied to theposterior wall of the abdomen enclosing the aorta andinferior vena cava. The left kidney was not affected butthe right kidney was distorted, the pelvis being invadedbut the cortex uninvolved though stretched around thegrowth. The tumour weighed 730 g. and measured 15cm. in maximum diameter. The cut surface was reddish-pink in colour divided by some fibrous septa. Since theright adrenal gland was not identified it was presumedthat the tumour had arisen from the right adrenalmedulla or possibly from ganglionic tissue in this region.Metastases were present in the right parietal and visceralpleurae, in the pancreas, sternal, and femoral bone-marrow, in lymph nodes at the aortic arch and near theporta hepatis, in the skull at the lateral point of thegreater wing of the right sphenoid bone and also the leftparietal bone just lateral to the vertex.
HIsTOLOGY. The tumour was composed of smallround cells with scanty cytoplasm arranged in sheets butshowing a few areas of classical rosette formation.There was a fair amount of necrosis and local haemor-rhage. No evidence of hypertensive change was foundin sections of the kidneys.
InvestigationsResponse to Phentolamine. In Case 1 this was tested
measuring systolic pressures only. The baseline levelwas 220 nmm.Hg. One minute after 1 mg. of the drugintravenously it fell to 130 mm.Hg, rising again graduallyto 155 mm.Hg. The response appears to be significantby the criteria of Soffer (1954).
In Case 2 there was no response to intravenous phentol-amine 2 mg. initially, then 2 mg. hourly for 10 hours,and 3 mg. hourly for a further 5 hours. The bloodpressure remained approximately 155/125 mm.Hgthroughout.
Excretion of Adreno-medullary Metabolites. Theseare shown in the Table. In Case 1 the only complete24-hour urine collection contained 103 itg. catechol-amines. Few figures for the normal values at this age areavailable. Sourkes et al. (1963), using similar methods,give the range for combined adrenaline and noradrenaline
excretion as 3 to 115 pg./24 hr. with a daily mean of 31 ptg.The subject with the highest excretion in this series was a13-month-old boy with supraventricular tachycardia.Voorhess and Gardner (1960) give a mean figure of lessthan 15 pg./24 hr. The excretion of catecholamines wasmuch increased in Case 2. Initially they were 665, 590,and 340 pg./24 hr. and fell to 142 ,ug. terminally. Theexcretion of HMMA was within the normal range foreach patient (M. Sandler and C. R. J. Ruthven, 1964,personal communication) and that ofHVA was increasedin Case 2 (14 ,ug./24 hr.).
Response to a-Methyldopa. This agent was tried inCase 1 (see Fig. 1). The dosage was increased from100 mg. to 200 mg. over seven days. As can be seen therewas no alteration in systolic blood pressure or ameliora-tion of the diarrhoea. The drug was not used in Case 2.
Biochemical and Pharmacological Investigations ofTumour Tissues. An extract of the tumour in Case 1 wasexamined for the presence of catecholamine-like sub-stances by Mr. C. R. J. Ruthven but none could bedetected in stored material investigated 6 weeks afterdeath. A similar extract from Case 2 was examined inthe Vincent Square Laboratories of Westminster Hospitalby Mr. B. Morris using the fluorimetric method. In thisa total catecholamine concentration of 3 -0 ,ug./g. wettissue was found (2 -4 pg. noradrenaline and 0-6 ptg.adrenaline). The tumour weighed 730 g. Assuming auniform distribution in the growth the total noradrenalinecontent was thus 1,750 ,ug. and that of adrenaline 438 ztg.The effects of extracts on the blood pressure of a dog
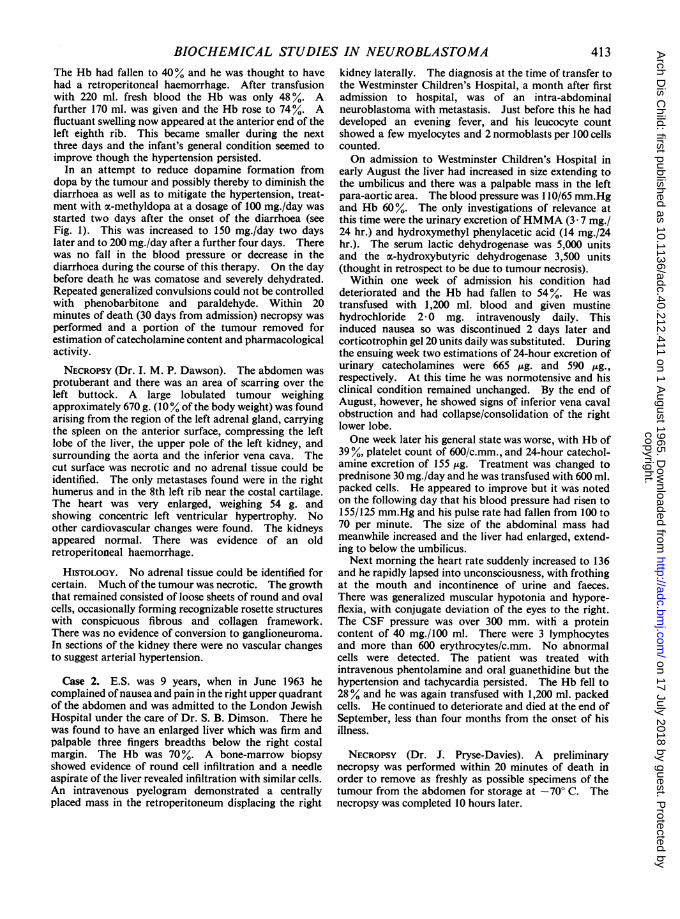
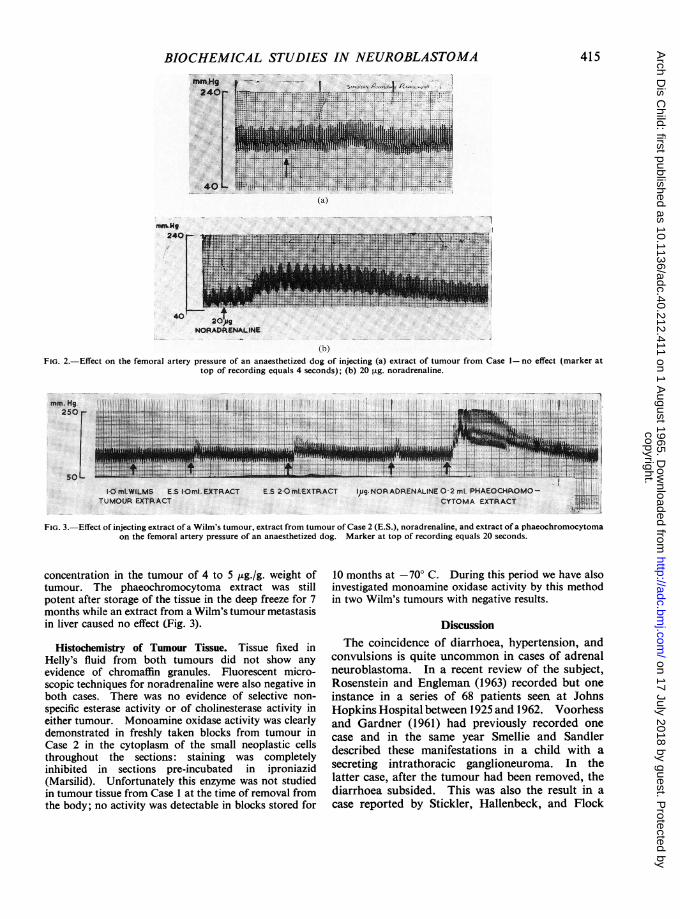
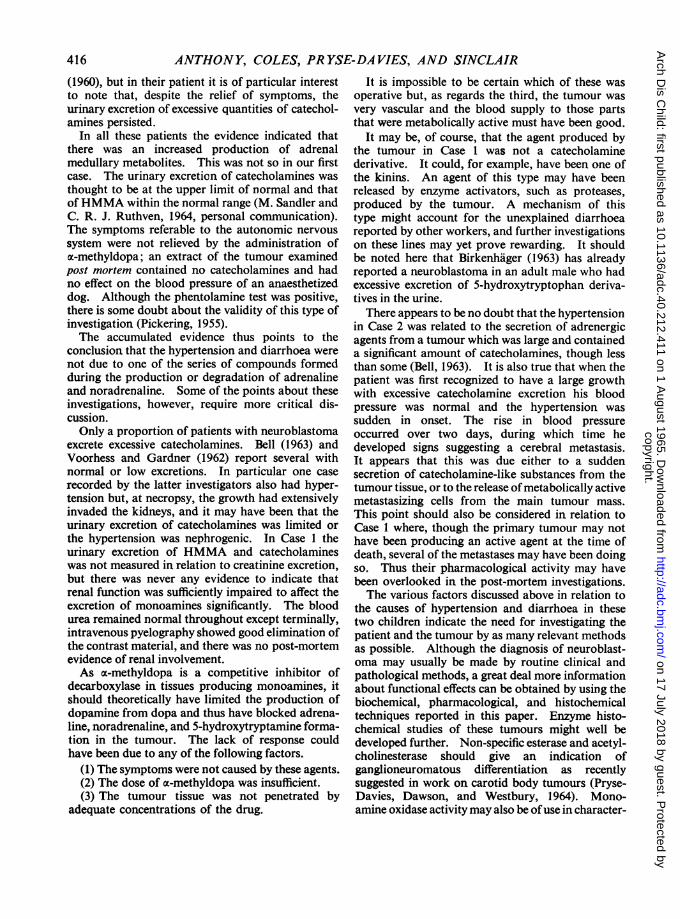
were observed in each case. The tissues from thetumours had been stored for 6 months and 6 weeks,respectively. A similar extract was made of mousekidney and a phaeochromocytoma; saline extracts of thetumour and mouse tissues were also examined. Eachextract from Case 1 caused no significant rise of bloodpressure when injected into an anaesthetized dog (Fig. 2a).The extract from the phaeochromocytoma (Fig. 3) and astandard noradrenaline solution (Fig. 2b) caused asustained rise in pressure, while the mouse kidney andsaline extracts of the tumour caused no alteration.The injection of tumour extract from Case 2 produced
a significant rise in femoral artery pressure which, bycomparison with noradrenaline standards, indicated a
414
copyright. on 17 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.40.212.411 on 1 A
ugust 1965. Dow
nloaded from
BIOCHEMICAL STUDIES IN NEUROBLASTOMA
2. '.
S..lshUg
.40
(b)FIG. 2.-Effect on the femoral artery pressure of an anaesthetized dog of injecting (a) extract of tumour from Case 1- no effect (marker at
top of recording equals 4 seconds); (b) 20 ,ug. noradrenaline.
M,LWILMS E.S IOml.EXTRACTT. R.... E.XTRA..CT
I.P. NORAOFENALtNe 0 2 ml PHAEOCHROMO-CYTOMA EXTRACT
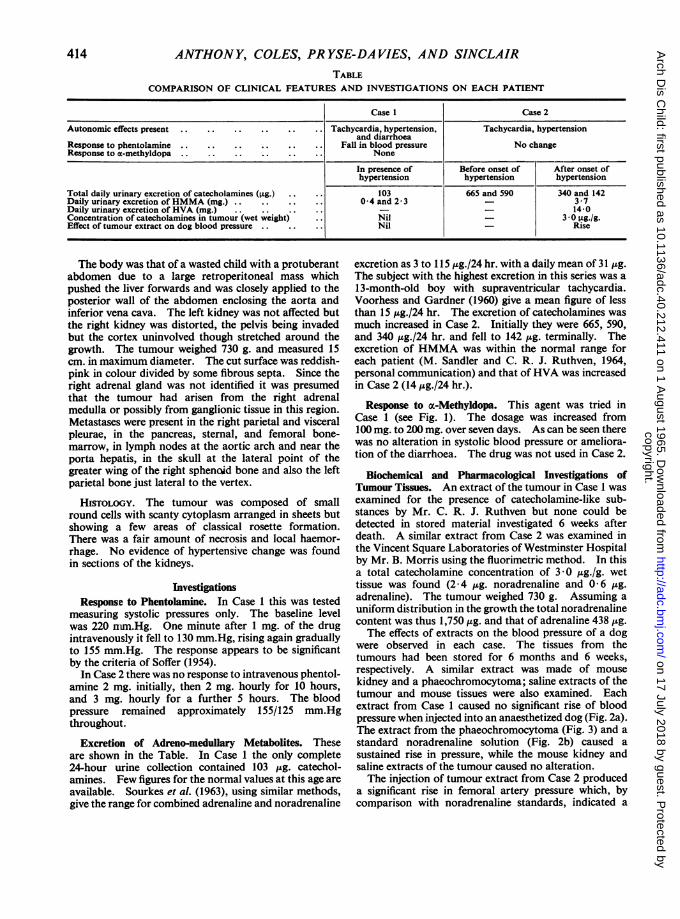
FIG. 3.-Effect of injecting extract of a Wilm's tumour, extract from tumour of Case 2 (E.S.), noradrenaline, and extract of a phaeochromocytomaon the femoral artery pressure of an anaesthetized dog. Marker at top of recording equals 20 seconds.
concentration in the tumour of 4 to 5 ,g./g. weight oftumour. The phaeochromocytoma extract was stillpotent after storage of the tissue in the deep freeze for 7months while an extract from a Wilm's tumour metastasisin liver caused no effect (Fig. 3).
Histochemistry of Tumour Tissue. Tissue fixed inHelly's fluid from both tumours did not show anyevidence of chromaffin granules. Fluorescent micro-scopic techniques for noradrenaline were also negative inboth cases. There was no evidence of selective non-specific esterase activity or of cholinesterase activity ineither tumour. Monoamine oxidase activity was clearlydemonstrated in freshly taken blocks from tumour inCase 2 in the cytoplasm of the small neoplastic cellsthroughout the sections: staining was completelyinhibited in sections pre-incubated in iproniazid(Marsilid). Unfortunately this enzyme was not studiedin tumour tissue from Case 1 at the time of removal fromthe body; no activity was detectable in blocks stored for
10 months at -70° C. During this period we have alsoinvestigated monoamine oxidase activity by this methodin two Wilm's tumours with negative results.
DiscussionThe coincidence of diarrhoea, hypertension, and
convulsions is quite uncommon in cases of adrenalneuroblastoma. In a recent review of the subject,Rosenstein and Engleman (1963) recorded but oneinstance in a series of 68 patients seen at JohnsHopkins Hospital between 1925 and 1962. Voorhessand Gardner (1961) had previously recorded onecase and in the same year Smellie and Sandlerdescribed these manifestations in a child with asecreting intrathoracic ganglioneuroma. In thelatter case, after the tumour had been removed, thediarrhoea subsided. This was also the result in acase reported by Stickler, Hallenbeck, and Flock
415
(a)
copyright. on 17 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.40.212.411 on 1 A
ugust 1965. Dow
nloaded from
ANTHONY, COLES, PR YSE-DA VIES, AND SINCLAIR
(1960), but in their patient it is of particular interestto note that, despite the relief of symptoms, theurinary excretion of excessive quantities of catechol-amines persisted.
In all these patients the evidence indicated thatthere was an increased production of adrenalmedullary metabolites. This was not so in our firstcase. The urinary excretion of catecholamines wasthought to be at the upper limit of normal and thatof HMMA within the normal range (M. Sandler andC. R. J. Ruthven, 1964, personal communication).The symptoms referable to the autonomic nervoussystem were not relieved by the administration ofoc-methyldopa; an extract of the tumour examinedpost mortem contained no catecholamines and hadno effect on the blood pressure of an anaesthetizeddog. Although the phentolamine test was positive,there is some doubt about the validity of this type ofinvestigation (Pickering, 1955).The accumulated evidence thus points to the
conclusion that the hypertension and diarrhoea werenot due to one of the series of compounds formedduring the production or degradation of adrenalineand noradrenaline. Some of the points about theseinvestigations, however, require more critical dis-cussion.Only a proportion of patients with neuroblastoma
excrete excessive catecholamines. Bell (1963) andVoorhess and Gardner (1962) report several withnormal or low excretions. In particular one caserecorded by the latter investigators also had hyper-tension but, at necropsy, the growth had extensivelyinvaded the kidneys, and it may have been that theurinary excretion of catecholamines was limited orthe hypertension was nephrogenic. In Case 1 theurinary excretion of HMMA and catecholamineswas not measured in relation to creatinine excretion,but there was never any evidence to indicate thatrenal function was sufficiently impaired to affect theexcretion of monoamines significantly. The bloodurea remained normal throughout except terminally,intravenous pyelography showed good elimination ofthe contrast material, and there was no post-mortemevidence of renal involvement.As cx-methyldopa is a competitive inhibitor of
decarboxylase in tissues producing monoamines, itshould theoretically have limited the production ofdopamine from dopa and thus have blocked adrena-line, noradrenaline, and 5-hydroxytryptamine forma-tion in the tumour. The lack of response couldhave been due to any of the following factors.
(1) The symptoms were not caused by these agents.(2) The dose of cx-methyldopa was insufficient.(3) The tumour tissue was not penetrated by
adequate concentrations of the drug.
It is impossible to be certain which of these wasoperative but, as regards the third, the tumour wasvery vascular and the blood supply to those partsthat were metabolically active must have been good.
It may be, of course, that the agent produced bythe tumour in Case 1 was not a catecholaminederivative. It could, for example, have been one ofthe kinins. An agent of this type may have beenreleased by enzyme activators, such as proteases,produced by the tumour. A mechanism of thistype might account for the unexplained diarrhoeareported by other workers, and further investigationson these lines may yet prove rewarding. It shouldbe noted here that Birkenhager (1963) has alreadyreported a neuroblastoma in an adult male who hadexcessive excretion of 5-hydroxytryptophan deriva-tives in the urine.
There appears to be no doubt that the hypertensionin Case 2 was related to the secretion of adrenergicagents from a tumour which was large and containeda significant amount of catecholamines, though lessthan some (Bell, 1963). It is also true that when thepatient was first recognized to have a large growthwith excessive catecholamine excretion his bloodpressure was normal and the hypertension wassudden in onset. The rise in blood pressureoccurred over two days, during which time hedeveloped signs suggesting a cerebral metastasis.It appears that this was due either to a suddensecretion of catecholamine-like substances from thetumour tissue, or to the release of metabolically activemetastasizing cells from the main tumour mass.This point should also be considered in relation toCase 1 where, though the primary tumour may nothave been producing an active agent at the time ofdeath, several of the metastases may have been doingso. Thus their pharmacological activity may havebeen overlooked in the post-mortem investigations.The various factors discussed above in relation to
the causes of hypertension and diarrhoea in thesetwo children indicate the need for investigating thepatient and the tumour by as many relevant methodsas possible. Although the diagnosis of neuroblast-oma may usually be made by routine clinical andpathological methods, a great deal more informationabout functional effects can be obtained by using thebiochemical, pharmacological, and histochemicaltechniques reported in this paper. Enzyme histo-chemical studies of these tumours might well bedeveloped further. Non-specific esterase and acetyl-cholinesterase should give an indication ofganglioneuromatous differentiation as recentlysuggested in work on carotid body tumours (Pryse-Davies, Dawson, and Westbury, 1964). Mono-amine oxidase activitymay also be ofuse in character-
416
copyright. on 17 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.40.212.411 on 1 A
ugust 1965. Dow
nloaded from
BIOCHEMICAL STUDIES IN NEUROBLASTOMA 417izing neuroblastoma cells, and it is interesting tospeculate on the relation between catecholamineproduction and monoamine oxidase concentrationsin such tumours.
SummaryIt has been assumed that the autonomic effects
induced by neuroblastomata are always due to theproduction of catecholamine compounds. Twocases are reported with details of biochemical,pharmacological, and histochemical investigations.In one there was hypertension, and evidence suggestedthat this was due to the release of adrenaline andnoradrenaline. In the other patient, who sufferedboth hypertension and diarrhoea, there was noevidence to indicate that the tumour was associatedwith excessive catecholamine activity, and it ispostulated that another agent, not a catecholaminederivative, may have been produced by the tumour.
We wish to thank Dr. J. G. Humble, Dr. K. A. Newton,Mr. J. C. Ruthven, Dr. Merton Sandler, and Dr. J. H.Wilkinson for their co-operation, Dr. Ian Dawson for hisconstructive criticism, Dr. Percy Cliffe and the Depart-ment of Clinical Measurement, Westminster Hospital forinvaluable help in the pharmacological work, and Dr.Peter Hansell and the Department of Medical Photo-graphy, Westminster Hospital for the preparation of thephotographs. One of us (J.P-D) was in receipt of a grantfrom the British Empire Cancer Campaign.
REFERENCESBell, M. (1963). The clinical chemistry of neuroblastomas. In
West-European Symposia on Clinical Chemistry, Vol. 2, ed.H. Varley and A. H. Gowenlock, p. 82. Elsevier, Amsterdam,London, and New York.
Birkenhager, J. C. (1963). Metastasizing neuroblastoma withexcretion of 5-hydroxyindoleacetic acid, serotonin and 5-hy-droxytryptophan. Acta med. scand., 174, 621.
Eranko, 0. (1955). Distribution of adrenaline and noradrenaline inthe adrenal medulla. Nature (Lond.), 175, 88.
Euler, U. S. von (1956). Noradrenaline: Chemistry, Physiology,Pharmacology and Clinical Aspects, 1st ed., p. 62. Thomas,Springfield, Illinois.
Glenner, G. C., Burtner, H. J., and Brown, G. W., Jr. (1957). Thehistochemical demonstration of monoamine oxidase activity bytetrazolium salts. J. Histochem. Cytochem., 5, 591.
Isaacs, H., Medalie, M., and Politzer, W. M. (1959). Noradrenaline-secreting neuroblastomata. Brit. med. J., 1, 401.
Kaser, H., and von Studnitz, W. (1961). Urine of children withsympathetic tumours. The excretion of 3-methoxy-4-hydroxy-mandelic acid. Amer. J. Dis. Child., 102, 199.
Marsden, H. B. (1963). Clinical and pathological features ofneuroblastoma. In West European Symposia on ClinicalChemistry, Vol. 2, ed. H. Varley and A. H. Gowenlock, p. 71.Elsevier, Amsterdam, London, and New York.
Mason, G. A., Hart-Mercer, J., Millar, E. J., Strang, L. B., andWynne, N. A. (1957). Adrenaline-secreting neuroblastoma in aninfant. Lancet, 2, 322.
Pearse, A. G. E. (1960). Histochemistry: Theoretical and Applied,2nd ed. Churchill, London.
Pickering, G. W. (1955). High Blood Pressure, p. 404. Churchill,London.
Pisano, J. J., Crout, J. R., and Abraham, D. (1962). Determinationof 3-methoxy-4-hydroxymandelic acid in urine. Clin. chim.Acta, 7, 285.
Pryse-Davies, J., Dawson, I. M. P., and Westbury, G. (1964). Somemorphologic, histochemical, and chemical observations onchemodectomas and the normal carotid body, including a studyof the chromaffin reaction and possible ganglion cell elements.Cancer (Philad.), 17, 185.
Robinson, R., Ratcliffe, J., and Smith, P. (1959). A screening test forphaeochromocytoma. J. clin. Path., 12, 541.
Rosenstein, B. J., and Engleman, K. (1963). Diarrhea in a child witha catecholamine-secreting ganglioneuroma: case report andreview of the literature. J. Pediat., 63, 217.
Smellie, J. M., and Sandler, M. (1961). Secreting intrathoracicganglioneuroma. Proc. roy. Soc. Med., 54, 327.
Soffer, A. (1954). Regitine and benodaine in the diagnosis ofphoechromocytoma. Med. Clin. N. Amer., 38, 375.
Sourkes, T. L., Denton, R. L., Murphy, G. F., Chavez, B., and SaintCyr, S. (1963). The excretion of dihydroxyphenylalanine,dopamine and dihydroxyphenylacetic acid in neuroblastoma.Pediatrics, 31, 660.
Stickler, G. B, Hallenbeck, G. A., and Flock, E. V. (1960). Ganglio-neuroblastoma associated with increased excretion of catecho-lamines. Amer. J. Dis. Child., 100, 634.
Voorhess, M. L., and Gardner, L. I. (1960). Catecholamine metabol-ism in neuroblastomas. Lancet, 2, 651.
-, and - (1961). Urinary excretion of norepinephrine,epinephrine and 3-methoxy-4-hydroxymandelic acid by childrenwith neuroblastoma. J. clin. Endocr., 21, 321.
-, and - (1962). Studies of catecholamine excretion bychildren with neural tumors. ibid., 22, 126.
Weil-Malherbe, H., and Bone, A. D. (1957). The estimation ofcatecholamines in urine by a chemical method. J. clin. Path., 10,138.
Wilkins, L. (1957). The Diagnosis and Treatment of EndocrineDisorders in Childhood andAdolescence, 2nd ed., p. 254. Thomas,Springfield, Illinois.
copyright. on 17 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.40.212.411 on 1 A
ugust 1965. Dow
nloaded from





























![Histochemical Studies with an Estrogen Receptor-related ... · [CANCER RESEARCH 46, 6475-6480, December 1986] Histochemical Studies with an Estrogen Receptor-related Protein in Human](https://img.pdfslide.us/doc/110x75/5eca3f17ce74ca60fc41cc79/histochemical-studies-with-an-estrogen-receptor-related-cancer-research-46.jpg)