Embed Size (px)
DESCRIPTION
Binder document
Citation preview

State of the Art Review of Tools for Assessment of Pain in Nonverbal Older Adults.
Project Overview
Updated by: Keela Herr, RN, PHD, FAAN; Heide Bursch, RN, MSN; Brianne Black, RN, The University of Iowa. Specific Aims of the Project Assessment of pain is a critical component of a comprehensive approach to pain management in all populations. Such information guides the selection of interventions and is necessary to monitor the effectiveness of treatment and to communicate care planning across health providers and care settings. Assessing pain in older adults who are unable to verbally report pain, however, is a significant challenge to health care providers. Clinicians continue to search for a clinically usable tool to adopt in their organizations. Whereas in general, self-report of pain is the gold standard for pain assessment, in this population other approaches, such as observational and surrogate report, are necessary. With increasing attention to finding an effective means for recognition and evaluation of pain in this vulnerable population, a number of researchers and clinicians have developed tools in an attempt to address this concern. As more precise and accurate methods for interpreting the expression of pain in persons with cognitive impairment are being developed, there is a need for critical evaluation of the existing tools in order to provide readily available information for best practice to those responsible for the quality of life of this vulnerable population and to provide a framework for ongoing research. The specific aims of this project were to 1) identify and evaluate existing tools for assessment of pain in nonverbal elders, 2) to prepare and make readily available evaluations of each tool which include evaluation of conceptualization, subject/setting, reliability and validity, and administration/scoring, along with a summary of strengths and weaknesses. The update was aimed at a review of research conducted after an earlier tool critique completed in 2004 by Herr, Decker and Bjoro, both in adding evidence to existing tools as well as in reviewing new tools to assess pain in non-verbal older adults. Tools evaluated in the initial review included: • The Abbey Pain Scale (Abbey) (Abbey, J., et al., 2004) • The Assessment of Discomfort in Dementia (ADD) Protocol, (Kovach, C.R., et al., (1999) • Checklist of Nonverbal Pain Indicators (CNPI), (Feldt, K., 1996) • The Discomfort Scale-Dementia of the Alzheimer’s Type (DS-DAT), (Hurley, A., et al., 1992) • The Doloplus 2, (Wary, B. and the Doloplus Group, 2001) • The Face, Legs, Activity, Cry and Consolability Pain Assessment Tool (the FLACC), (Merkel, S.I., et al., 1997) • Nursing Assistant-Administered Instrument to Assess Pain in Demented Individuals (NOPPAIN), (Snow, A.L., et al., 2001) • The Pain Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC), (Fuchs-Lacelle, S.K., et al., 2004)

• Pain Assessment for the Dementing Elderly (PADE), (Villaneuva, M.R., et al., 2003) • The Pain Assessment in Advanced Dementia (PAINAD) Scale, (Warden, V., et al., 2003) New tools added in the updated review in 2008 include: • Certified Nurse Assistant Pain Assessment Tool (CPAT), (Cervo, F., Raggi, R., Bright-
Long, L., Wright, W., Rows, et al., 2007) • Discomfort Behavior Scale (DBS), (Stevenson, K., 2006) • Disability Distress Assessment Tool(Dis DAT), (Regnard, C., Mathews, D., Gibson, L.,
Clarke, C., 2007) • Elderly Pain Caring Assessment 2 (EPCA-2), (Morello, R., Jean, A., Alix, M., Sellin-
Peres, D., Fermanian, J., 2007) • Mobilization-Observation-Behavior-Intensity-Dementia Pain Scale (MOBID),
(Husebo, B.S., Strand, I., Moe-Nilssen, R., Husebo, S.B., Snow, A,L., Ljunggren, A.E., 2007)
• Pain Assessment in Noncommunicative Elderly Persons (PAINE), (Cohen-Mansfield, J., 2006)
• Pain Behaviors for Osteoarthritis Instrument for Cognitively Impaired Elders (PBOICIE), (Tsai, P., Beck, C., Richards, K., Phillips, L., Roberson, P., Evans, J., 2008).
Two of the initially reviewed tools were not followed up with further application or research in non-verbal older adults: ADD and FLACC. In addition to tools strictly directed at assessing pain in non-verbal adults, the update continues to include discomfort and distress tools: DBS and Dis DAT . Clinicians are interested in distinguishing these different constructs and, while presenting behaviors may be similar, clearly treatment and interventions may differ. The documents included in this website are: General Information folder including:
0. Project overview 1. Criteria for Evaluation of Pain Assessment Tools 2. Comparison Grid of Pain Assessment Tools Rated on Evaluation Criteria 3. Comparison of Tool Items with the AGS 2002 Persistent Pain Guidelines 4. Review References
Individual Folder for each tool containing 5. In-depth evaluation of each tool, including contact information of tool developers 6. Brief summary evaluation of each tool 7. Copy of each tool for which permission was obtained to post
Because the science is continually evolving in the evaluation of existing tools and in response to the development of new tools, this site was updated July 2008 to provide the most current data on existing tools available for clinicians and researchers to consider for use in their settings. It is hoped that there will be further updates in the future as research and practice developments bring us closer to recommendations for best tools in clinical and research settings.

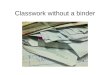
Comparison Grid of Pain Assessment Tools for Non-verbal Older Adults Rated on Evaluation Criteria Conceptualization Subjects &
Setting Administration,
Scoring, Feasibility
Reliability Validity Sum of Scores
Abbey 1 1 1 1 1 5 *ADD Protocol 2 2 2 1 2 9 CNPI 2 2 2 2 2 10 CPAT 1 1 1 0 1 4 DBS/MDS 2 2 0 1 2 7 Dis DAT 1 1 1 0 1 4 DS-DAT 2 2 1 2 2 9 Doloplus 2 2 2 2 2 2 10 EPCA-2 2 2 1 2 2 9 FLACC 0 1 0 1 1 3 MOBID 2 1 1 1 1 6 NOPPAIN 2 2 2 2 2 10 PACSLAC 2 2 2 2 2 10 PADE 1 2 2 1 2 8 PAINAD 2 3 3 3 2 13 PAINE 2 2 1 2 1 8 PBOICIE 1 1 0 1 1 4 *ADD Protocol is not included as an assessment tool, but as a protocol for validating presence of pain. Key to categories for evaluation
Conceptualization is a composite score based on purpose, conceptual basis, item generation and content validity. Reliability: a composite score including internal consistency reliability, interrater reliability and test-retest reliability. Validity: a composite score including criterion related and/or construct validity.

Key to rating
3= Available evidence is strong 2= Available evidence supports need for further testing 1= Available evidence is insufficient and/or tool revisions are needed 0= Evidence is absent
Full name of tools
• Abbey: The Abbey Pain Scale (Abbey, J., et al., 2004) • ADD: The Assessment of Discomfort in Dementia Protocol, (Kovach, C.R., et al., 1999) • CNPI: Checklist of Nonverbal Pain Indicators, (Feldt, K., 1996) • CPAT: Certified Nurse Assistant Pain Assessment Tool, (Cervo, F. A. et al., 2007) • DBS/MDS: Discomfort Behavior Scale, (Stevenson, K. M. et al., 2006). • Dis DAT: Disability Distress Assessment Tool, (Regnard, C. et al., 2007). • Doloplus 2: The Doloplus 2, (Wary, B. and the Doloplus Group, 2001) • DS-DAT: The Discomfort Scale-Dementia of the Alzheimer’s Type, (Hurley, A., et al., 1992) • FLACC: The Face, Legs, Activity, Cry and Consolability Pain Assessment Tool, (Merkel, S.I., et al., 1997) • EPCA-2: Elderly Pain Caring Assessment 2 (Morello, R. et al., 2007) • MOBID: Mobilization-Observation-Behavior-Intensity-Dementia Pain Scale (Husebo, B. S. et al., 2007). • NOPPAIN: Nursing Assistant-Administered Instrument to Assess Pain in Demented Individuals, (Snow, A.L., et al., 2001) • PACSLAC: The Pain Assessment Checklist for Seniors with Limited Ability to Communicate, (Fuchs-Lacelle, S.K., et al., 2004) • PADE: Pain Assessment for the Dementing Elderly, (Villaneuva, M.R., et al., 2003) • PAINAD: The Pain Assessment in Advanced Dementia Scale, (Warden, V., et al., 2003) • PAINE: Pain Assessment in Noncommunicative Elderly Persons (Cohen-Mansfield, J., 2006). • PBOICIE: Pain Behaviors for Osteoarthritis Instrument for Cognitively Impaired Elders (Tsai, P. F. et al., 2008).

Completed 04/04 Revised 06/08
1
The Abbey Pain Scale (The Abbey) Brief The Abbey Pain Scale (The Abbey) is an Australian tool developed to measure severity of pain in people with late-stage dementia that was efficient, effective and able to be used by a variety of care staff. Although there is no presentation of the conceptual basis for the tool, it is apparent that this informant-based tool attempts to measure “acute pain”, “chronic pain” and “acute on chronic,” in the same tool. The tool includes six items: vocalization, facial expression, change in body language, behavioral change, physiological change, and physical change. Each item is leveled on a four point scale for severity of the behavior (Absent: 0; Mild: 1; Moderate: 2; Severe: 3) with total score ranging from 0 to 18. The total score is then interpreted as severity of pain: No pain: 0-2; Mild: 3-7; Moderate: 8-13; Severe: 14+. The rater is asked to indicate which type of pain the older adult has: chronic, acute or acute on chronic. Preliminary studies give no evidence that informants can reliably rate these levels of pain using this tool. There are a few limited instructions on the tool schema. Instructions for using the Abbey Pain Scale are presented on a poster. Nurses are asked to use the tool when pain is suspected. It is not specifically designed to be a part or routine daily assessment. The tool apparently takes one minute to score, although there are no data to support this. A follow-up study does not provide any further supportive information on the feasibility, administration or clinical utility of the Abbey. With only 50% of care providers reporting that the scale was good to judge or observe pain indicators, little additional support is provided. In study 1, the tool was evaluated in 24 Australian long term care facilities with a sample of 61 older adults with late-stage for a total of 236 pain episodes. Assessment of presence and degree of cognitive impairment and pain in study subjects was not standardized. Age and gender distribution are appropriate but there is no mention of ethnic/racial diversity in either study. Study 2 was conducted in 17 Belgian nursing homes with 185 caregivers and 157 residents. The tool has not been tested in the United States. Using 5 subjects per tool item as a minimum requirement for this review, a minimum sample size of 60 subjects (12 items x 5 subjects) and 30 subjects (6 items x 5 subjects) in stage 1 and stage II respectively would be needed. Thus, with 52 subjects in stage I this sample is not sufficient for regression analysis; however, with 61 subjects in stage II the sample is sufficient for tool evaluation. No additional tool item evaluation study was conducted in Study 2. Reliability • Internal consistency reliabilities for pre- and post intervention are acceptable but it is
unclear what data were used in the analysis (e.g. pain episode, resident or mean score).
• Interrater reliability between two staff members pre and post intervention was low particularly for post intervention evaluation.
• No test-retest reliability is available. Study 2 did not add further information on reliability of the tool. Reliability, therefore, has not been adequately established based on available information.

Completed 04/04 Revised 06/08
2
Validity • Concurrent validity of the scale was evaluated against the holistic impression of pain
as assessed by the nurse: Gamma: 0.586 (p<.001). • Predictive validity was assessed by change in mean pain score pre-intervention: 9.02
(± .48), post intervention: 4.21 (± .41). A paired t-test was statistically significant (p<0.001). However, it is unclear what unit of analysis was used for examining pre-post score changes (e.g. pain episode, resident or mean score).
Summary Clinicians considering this tool need to be aware of conceptual issues. There is conceptual blurring between acute and chronic pain with no discussion in the paper on distinguishing characteristics of the pain types. Moreover, there is blurring between pain behaviors and pain etiology. Although the tool does include at least one cue from each of the 6 categories of non-verbal pain behavior indicators from the AGS Guideline on Persistent Pain in Older Adults, the inclusion of physiological indicators is not supported in the literature on chronic pain. Thus, an individual with chronic pain being scored on this tool may lose 3 points towards the overall severity score. Moreover, the ability of health care providers to determine severity of pain from behavioral indicators has not been established. Tool reliability is equivocal with current data available. Validity testing based on nurse judgment of pain severity is not substantiated in the literature, particularly, as in this case, without evidence supporting the expertise of the raters. Thus tool revision and additional testing in controlled circumstances are recommended before using this tool in clinical practice.
Source of evidence Abbey, J.A., Piller, N., DeBellis, A, Esterman, A., Parker, D., Giles, L. & Lowcay, B.
(2004). The Abbey Pain Scale. A 1-minute numerical indicator for people with late-stage dementia. International Journal of Palliative Nursing, 10(1), 6-13.
Van Iersel, T., Timmerman, D. & Mullie, A. (2006). Introduction of a pain scale for
palliative care patients with cognitive impairment. International Journal of Palliative Nursing, 12(2), 54-59.
Contact information: Jennifer Abbey, RN, PhD, FRCNA P.O. Box 703, Bribie Island Queensland 4507 Australia E-mail: [email protected] Summary completed by: K. Herr, S. Decker, K. Bjoro, University of Iowa (2004) Updated by K. Herr, H. Bursch and B. Black, University of Iowa (2008)
Contact information: [email protected]

Completed 04/04 Revised 06/08
1
Tool: The Abbey Pain Scale Tool developer: Abbey, J.A., DeBellis, A, Piller, N., Esterman, A., Parker, D., Giles, L. & Lowcay, B. Country of origin: Australia Reviewed: 04/04 Revised: 06/08 Conceptualization Panel rating: 1 Revised: 1 Purpose The stated purpose was to develop a pain scale for people with late-stage
dementia that was efficient, effective and able to be used by a variety of care staff. The Abbey Pain Scale is an informant-based tool.
Conceptual basis There is no discussion or presentation of the conceptual basis for the tool. The tool attempts to measure severity of “acute pain”, “chronic pain” and “acute on chronic.” Yet a clear discussion of the conceptual basis for the tool is absent.
Item Generation Tool items • Vocalization • Facial expression • Change in body language • Behavioral change • Physiological change • Physical change Each item is leveled on a four point scale for severity (Absent: 0; Mild: 1; Moderate: 2; Severe 3). Individual item scores are summed to arrive at a total score ranging from 0-18. The total score is interpreted as follows: No pain: 0-2; Mild: 3-7; Moderate: 8-13; Severe: 14+. Item generation process Phase I: A draft of the scale was based on: • Literature review • A Delphi study by geriatric and pain experts • Focus group of practitioners. Phase II: A prototype of the tool consisting of 12 items was generated in which each of the 6 items listed above was measured on both a dichotomous scale and an ordinal scale. Regression analysis was used to determine which of the twelve items were most predictive of the de facto gold standard (nurses’ holistic impression of pain severity). Twelve items predicted 42% of the variability on the holistic pain question. Items measuring pain severity were more powerful predictors of holistic pain than presence/absence of pain. Thus, items rated as present/absent were deleted. Six severity items were retained accounting for 41% of the variability in the scores.
Content Validity The draft scale was reviewed by gerontological and pain experts through a Delphi study before being tested clinically and also by discussion with practitioners using focus group debate.
-Panel Commentary There is conceptual blurring between acute and chronic pain. There is no discussion in the paper on characteristics of the one type of pain in

Completed 04/04 Revised 06/08
2
relationship to the other or the overlap (e.g. physiologic changes vs. behavioral change). There is conceptual blurring between pain behaviors and pain etiology, (e.g. presence of skin tears or arthritis), both elements of the rating scale. Development of the tool is based on the assumption that caregivers can reliably rate the intensity of pain in elders, although the interpretation of pain severity has not been substantiated in the research on pain in elders with dementia. Nurses’ holistic impression of pain severity was used as the gold standard. However, this assumption is not supported by current literature, which indicates that caregivers can detect presence of pain, but not severity or intensity. Therefore, using “the gold standard of caregiver’s report of pain intensity” in regression analysis to derive tool items is a limitation. Little information is available on the Delphi study: who the experts were, what items were presented in the Delphi and the results. Also, almost no information is available on the focus group: who were the participants, and their expertise (educational and clinical background and relevance to elders with dementia and pain). Comprehensiveness and clarity of items The tool includes at least one cue from each of the 6 categories of non-verbal pain behaviors in the AGS Persistent Pain Guidelines. Facial expression, Verbalizations/vocalizations, Body language and to some extent Changes in activity patterns or routines, Mental status changes and Changes in interpersonal interactions. However, inclusion of physiological indicators may compromise the overall tool scoring of chronic pain. The rationale for including pain etiology items in a tool for assessing pain that totals overall severity of behaviors in non-verbal elders is not clear. The tool is intended to measure acute pain, chronic pain and acute on chronic pain. However, it is unclear how the tool could differentiate pain types. Moreover, the tool has not been formally evaluated for content validity.
Subjects Panel rating: 1 Revised: 1 Subjects Study 1 (Abbey et al., 2004)
The tool development and testing took place in 24 aged care residential facilities in four Australian states: South Australia, New South Wales, Queensland and Victoria. Inclusion criteria: Residents with late-stage dementia as confirmed by a senior registered nurse and who were perceived by facility staff as experiencing pain during the project. Staff observations were made by 61 staff who completed the pain scale: 45 registered nurses and 7 enrolled nurses. In the initial stage of tool testing, data were available for 52 residents for a

Completed 04/04 Revised 06/08
3
total of 770 pain episodes (non-independent scores). In stage II of tool testing, data were available for 61 residents for a total of 236 pain episodes. Age: 83 years (median), Range: 60-97 years. Gender: Female: 66%, Male 34%. Study 2 (van Iersel, et al., 2006) 17 nursing homes in Belgium 185 care providers 157 patients unable to express pain verbally (no measure of cognitive impairment) Gender: 78% female; 22% male Age: mean 85 years (range 22-100)
-Panel Commentary Focus on long term care setting is clearly identified. However, the initial study was carried out at 24 sites with 61 staff members with varied skill level completing observations. This allows for wide variation and consequently potential for measurement error. A standard assessment approach to document presence of dementia or level of cognitive impairment is not included in either study. Relying on senior nurses’ confirmation of dementia allows inconsistent assessment across study sites. The study subjects in Study 1 are limited to those who were identified by the staff as having pain. It is not known whether pain assessment was carried out on a regular basis. Patients with atypical presentation of pain may not have been identified for participation in the study. Study 2 did not provide any information on how patients were determined to have pain or not. Age and gender distribution are appropriate but there is no mention of ethnic/racial diversity in either study. Study 1 represents Australian residents and Study 2 represents Belgian residents. The tool has not been evaluated in the United States. Using 5 subjects per tool item as a minimum requirement for this review, a minimum sample size of 60 subjects (12 items x 5 subjects) and 30 subjects (6 items x 5 subjects) in stage 1 and stage II respectively would be needed. Thus, with 52 subjects in stage I this sample is not sufficient for regression analysis; however, with 61 subjects in stage II the sample is sufficient for tool evaluation. No additional tool item evaluation study was conducted in Study 2.
Administration, Scoring, Feasibility Panel rating: 1 Revised: 1 Administration, Scoring, Feasibility
Instructions for using the Abbey Pain Scale are presented on a poster. Nurses are asked to use the tool when pain is suspected. Prompts depicted on the poster include “These people have dementia.” “Are they in pain?” “If they can’t tell you, use the one-minute Abbey Pain Scale.” There are a few limited instructions on the tool schema. Scoring prodecure is described above. The rater is asked to indicate what type of pain the subject has: acute, chronic or acute on chronic.

Completed 04/04 Revised 06/08
4
There are qualitative reports that the tool took less than one minute to complete. Study 2 (van Iersel et al., 2006) No specific information on clinical utility or feasibility is provided, but it appears that the tool was readily used by the care providers in these nursing homes. 56% of care providers judged indicators on the Abbey as good indicators of pain, while 21% disagreed and 24% felt it was not easy to administer.
-Panel Commentary Method of administration and scoring is not adequately described. • Nurses are asked to use the tool when pain is suspected. It is unclear what
triggers the pain assessment. A lack of systematic pain assessment may result in non-detection of pain. Systematic pain assessment may have been more appropriate in a tool development study. This gives rise to the issue of scheduled pain assessment vs. prn assessment.
• Scoring procedures are unclear. There are no instructions on what constitutes the different severity levels for each item.
• There is no justification for the total severity scoring system or its interpretation.
• There is no indication as to how the rater arrives at “type of pain” or how this impacts treatment decisions.
Clinical utility • Time: The tool developers report the tool takes less than one minute to
score. However, no data are provided. • Skill needed: The tool developers do not specify skill level needed. All
nursing personnel are referred to as “staff.” It is unclear if there are any limitations to the scope of practice of those using the tool.
Clinical utility has not been formally studied. Tool developers report the tool takes less than one minute to score. However, no data are provided. The tool developers do not specify skill level needed. All nursing personnel are referred to as “staff.” It is unclear if there are any limitations to the scope of practice of those using the tool. Study 2 does not provide any further supportive information on the feasibility, administration or clinical utility of the Abbey. With only 50% of care providers reporting that the scale was good to judge or observe pain indicators, little additional support is provided.
Reliability Panel rating: 1 Revised: 1 Internal consistency Study 1 (Abbey et al., 2004)
Internal consistency was assessed in stage II of tool testing. Data were available for 61 residents for a total of 236 pain episodes (see sample characteristics above). Internal consistency reliability reported: Pre-intervention: α =.74 and post-intervention: α =.74. Study 2 (van Iersel et al., 2006) No reliability information provided.
Interrater reliability Study 1 (Abbey et al., 2004) Interrater reliability was assessed in stage II of the testing. Residents (n=18) were assessed by two staff members. Characteristics of the wider sample of subjects are provided above.

Completed 04/04 Revised 06/08
5
Assessed by intra-class correlation coefficient:
Pre intervention: ICC=0.63 (p=0.02) Post-intervention: ICC=0.44 (p=0.12).
Study 2 (van Iersel et al., 2006) No reliability information provided.
Test-retest reliability No test retest or intrarater reliability is reported in either Study 1 or 2. -Panel commentary Internal consistency
Although the tool has an acceptable level of internal consistency, it is unclear what data were used for analysis, eg. patients, mean pain score, pain episodes. Interrater reliability Staff qualifications are not specified. Intraclass correlation is an appropriate test for interrater reliability. However, the reliabilities are low, particularly for post intervention evaluation. Test-retest reliability No test-retest or intrarater reliability is available. Thus, tool reliability has not been adequately established based on available information.
Validity: Criterion or construct Panel rating: 1 Revised: 1 Construct validity/ Criterion related validity
Study 1 (Abbey et al., 2004) Validity testing was conducted in stage II of testing. Sample included 61 residents (see sample characteristics above) with a total of 236 pain episodes. The number and types of intervention varied from patient to patient. However, the most common intervention was analgesics, followed by repositioning. Staff (n=61) completed the pain scale: 45 (74%) were registered nurses and 7 (12%) were enrolled nurses. Concurrent validity The pre-intervention pain score was associated with the holistic impression of pain as assessed by the nurse. The holistic impression was rated on a scale of 1=no pain, 2=mild, 3=discomforting, 4=distressing or 5=severe.
Results: Gamma: 0.586 (p<.001). Predictive validity Change in pain score before and after intervention: Average pain score (n=61):
Pre-intervention (n=61): 9.02 (± 3.75) Post-intervention (n=61): 4.21 (± 3.20) Paired t-test: showed the reduction to be highly statistically significant (p<0.001).
Study 2 (van Iersel et al., 2006) The purpose of this study was to determine provider feedback on the items in the Abbey and their usefulness in detecting pain. Outcomes represent only provider perceptions of the scale.

Completed 04/04 Revised 06/08
6
On average, 56% of care providers considered the observed categories of the Abbey good, and 52% considered them to be easy to observe indicators of pain. Best indicators for which over 80-% agreed were facial expression, vocalization and body language. Physiological changes in Abbey were not considered a good indicator (80%).
-Panel commentary Concurrent validity The holistic impression of pain as assessed by the nurse was used as a gold standard. However, the expertise or competence to assess pain in persons with dementia is not reported. There is no indication as to whether the Abbey Pain Scale scores and the holistic impression of pain are independent measures or assessed by the same nurse, which would impact data validity. Validity data is based on 61 different staff using the tool which presents bias for evaluation and interpretation. Gamma is an appropriate measure of association for measures at ordinal level or higher. Gamma varies between -1 and 1. The results in this study indicate that the two measures are moderately positively associated. Predictive validity Variability in interventions and their effectiveness limits ability to make conclusions regarding change in pain. However, because data reported are in the expected direction regarding change in pain score, future testing in controlled circumstances is warranted. Study 2 provides care provider perceptions of indicator usefulness but does not provide any method of judging validity of those assessments and does not contribute to psychometric evaluation of the Abbey.
Summary of panel evaluation of pain assessment tool The Abbey Pain Scale includes key behaviors representative of the scope of behavioral pain indicators in persons with dementia. However, the tool also includes items such as physiological changes and pain etiologies, which are not behavioral pain indicators and are not conceptually congruent with the intent of the tool. Moreover, the ability of health care providers to determine severity of pain from behavioral indicators has not been established. The subject sample is appropriate, however validation in minority samples and use of a standard assessment of cognitive impairment are needed. Scoring procedures and training to use the tool are not clear, nor is qualification of those individuals providing the gold standard. Tool reliability is not supported with current data available. Validity testing based on nurse judgment of pain severity is not substantiated in the literature, particularly without evidence supporting the expertise of the raters. Tool revision and additional testing in controlled circumstances are recommended. Source of evidence Abbey, J.A., Piller, N., DeBellis, A, Esterman, A., Parker, D., Giles, L. & Lowcay, B. (2004). The Abbey
Pain Scale. A 1-minute numerical indicator for people with late-stage dementia. International Journal of Palliative Nursing, 10(1), 6-13.
Van Iersel, T., Timmerman, D. & Mullie, A. (2006). Introduction of a pain scale for palliative care patients
with cognitive impairment. International Journal of Palliative Nursing, 12(2), 54-59. Key to panel rating 3= Available evidence is strong 2= Available evidence supports need for further testing 1= Available evidence is insufficient and/or tool revisions are needed 0= Evidence is absent

Completed 04/04 Revised 06/08
7
Contact address for tool developer: Jennifer Abbey, RN, PhD, FRCNA P.O. Box 703, Bribie Island Queensland 4507 Australia E-mail: [email protected] Evaluation completed by: K. Herr, S. Decker, K. Bjoro, University of Iowa. Contact information: [email protected] Revision 6/08 by: K. Herr, B. Black, H. Bursch, The University of Iowa Contact information: [email protected]


Completed 04/04 Revised 06/08
1
Doloplus 2 Brief The Doloplus 2 is a French tool developed for the multidimensional assessment of pain in non-verbal elders. The tool consists of three subscales and a total of 10 items: Somatic reactions (5 items), Psychomotor reactions (2 items) and Psychosocial reactions (3 items). Each item is leveled with four behavioral descriptions representing increasing severity of pain rated from 0 to 3. Individual item scores are summed to arrive at a total score ranging from 0 to 30 points. Five points is the threshold indicating pain. However, as the tool developers point out, pain can not be ruled out if the older adult has less than five points. The Doloplus 2 is based on sound assumptions of multidimensionality of pain in elders with pain that are supported in the literature on pain in elders with dementia. The tool is comprehensive covering 5 of 6 pain behavior categories in the AGS Persistent Pain Guideline. While there is emerging evidence that observation or informant-based pain assessment tools can track change in degrees of pain for individual residents, current literature does not support the hypothesis that such tools can reliably differentiate between mild, moderate, and severe pain, or rate pain severity on a scale from 0-10. As with any observational tool, a small number of behaviors observed increases its specificity, but limits sensitivity in that it may not detect pain in persons presenting with less obvious behaviors. Method of administration and scoring procedures are clearly described. Follow-up studies indicated that it took an average of 10 (6 to 12) minutes to administer the Doloplus-2. The tool is intended for use by health and social care providers as well as family of the elder. However, training requirements for reliable use of the tool by these different groups are not reported. It must be noted that in one study nurses in the clinical setting identified the tool as the least preferred method of pain assessment when compared to other similar observational tools. There is preliminary work with a shortened version of the Doloplus 2. Nurses in clinical practice wishing to use this tool may find several items in the the English translation unclear. Several items seem foreign when compared to the words and expressions most commonly used in English literature on pain in dementia. The English version appears to need refinement. Although the French version of the Doloplus 2 has been tested in diverse populations and settings including long term care, geriatric clinics and palliative care in France and Switzerland (see report of reliability and validity below), dementia sessment was not standardized and there are currently no reports of testing of the English version of the Doloplus 2. Reliability • Internal consistency was tested in a pooled sample of 501 elders from centers
participating in the Doloplus Group. Average age of subjects was 82.5 (±8) range 55-96; 173 males and 337 females. Cronbach alpha was 0.82. Zwakhalen reported internal consistency of 0.58-0.80. Pautex found that internal consistency was lower in residents with dementia (r=0.67) than in residents who were cognitively intact (r=0.84). Internal consistency scores were lowest for the items expression (r=0.82) and mobility (r=0.82). Internal consistency was slightly lower for the shortened

Completed 04/04 Revised 06/08
2
version or the Doloplus-2 (Cronbach alpha=0.71) than the complete version (Cronbach alpha 0.85).
• Interrater reliability was reported but may not have been statistically significant in two samples at palliative care hospitals in France.
• Test-retest reliability was evaluated in a pooled sample of 83 patients from divergent settings and was found to be good but not statistically significant. Pautex found strong test-retest reliability on subsamples of 20 residents from the same hospital units who had the same characteristics and stable chronic pain.
Validity • Convergent validity was established between the Doloplus 2 and a VAS in a mixed
sample of 143 elders from various geriatric or palliative care units in France and Switzerland (p< 0.001).
• Sensitivity was tested at 11 centers in a pooled sample of 183 elders, 73 males and 110 females, average age 80.7 years (±8.6), range 65-101 years. D0: 10.6 (±5.3); D1: 7.5 (±4.4); D7: 4.9 (±4.2) (information from web site).
• Following testing, Pautex shortened the Doloplus 2 to include only the items which were significantly associated with VAS scores. This version was also compared with the VAS. The revised version contained 3-items of the somatic dimension and two of the psychosocial dimension.
• There has been a considerable amount of evidence supporting the validity of the Doloplus-2 in subsequent studies. However, all of the studies have been in foreign populations and further validation needs to be done in English. The surprisingly high correlation between the Doloplus-2 and self report rating scales as reported in Study 3 are inconsistent with the finding in the literature. Most studies report correlations of approximately .30 between observational tools and self-report assessments.
Summary The Doloplus 2 is a comprehensive tool for assessing pain in nonverbal elders. The tool addresses many key indicators noted in the literature and AGS Guidelines. Via their website information the tool developers report extensive testing in Europe. However, information in English is limited and available reports do not provide sufficient detail on which to base sound judgment of the tool evaluation. Translation issues are evident and further study or description regarding the use of Doloplus 2 in English-speaking populations is needed.
Sources of evidence Doloplus-2 website: http://www.Doloplus-2.com Holen, J., Saltvedt, I., Fayers, P., Bjornnes, M., Stenseth, G., Hval, B., et al (2005). The
Norwegian Doloplus-2, a tool for behavioral pain assessment: translation and pilot validation in nursing home residents with cognitive impairment. Palliative Medicine, 19, 411-7.
Lefebvre-Chapiro, S. & the Doloplus-2 group. (2001). The Doloplus-2 scale – evaluating
pain in the elderly. European Journal of Palliative Care, 8(5), 191-194.

Completed 04/04 Revised 06/08
3
Pautex, S. Michon, A., Guedira, M. Emond, H., Le Lous, P., Samaras, D. et al (2006). Pain in severe dementia: Self-assessment or observational scale? JAGS, 54, 1040- 1045.
Pautex, S., Herrmann, F., Michon, A., Giannakopoulos, P., Gold, G. (2007).
Psychometric properties of the doloplus-2 observational pain scale and comparison to self-assessment in hospitalized elderly. Clinical Journal of Pain, 23(9), 774-9.
Zwakhalen, S., Hamers, J., & Berger, M. (2006). The psychometric quality and clinical
usefulness of three pain assessment tools for elderly people with dementia. Pain, 126, 210-220.
Contact information: Dr. Bernard Wary Service Regional de Soins Palliatifs CHR Meta-Thionville-BP 60327 57126 Thionville Cedex France E-mail [email protected] The tool is available free of charge from the official Doloplus 2 website: http://www.doloplus.com/versiongb/rubautres/intro.htm Contact e-mail address found at official Doloplus-2 website: [email protected] (Dr. Bernard Wary, personal communication, July 2008) This summary was completed by: K. Herr, S. Decker, K. Bjoro, University of Iowa (2004). Updated by: K. Herr, H. Bursch and B. Black, The University of Iowa (2008). Contact information: [email protected]

Completed 06/08 1
Tool: Doloplus-2 Tool developer: Wary, B. and The Doloplus-2 Group Country of origin: France Reviewed: 04/04 Revised: 06/08 Conceptualization Panel rating: 1 Revised: 2 Purpose The Doloplus-2 is an observational pain assessment tool developed for the
multidimensional assessment of pain in non-verbal elders who experience chronic pain.
Conceptual basis Doloplus-2 was based on Doloplus developed by Wary et al (1993). Pain is multidimensional with somatic, psychomotor and psychosocial dimensions. Within these domains observations are made of patient behaviors that could potentially reveal pain. This tool bases evaluation on changes in the elder’s behavior. The individual trajectory of the elder is emphasized. The tool attempts to measure pain severity.
Item Generation Study 1(Lefebvre-Chapiro, 2001) There are three subscales with a total of 10 items: • Somatic reactions (5 items)
Somatic complaints Protective body postures adopted at rest Protection of sore areas Expression Sleep pattern
• Psychomotor reactions (2 items) Washing and/or dressing Mobility
• Psychosocial reactions (3 items) Communication Social life Behavioral problems
Each of the ten behavioral items is leveled with four descriptions of behaviors rated on a four point scale from 0 to 3 representing increasing severity of pain. Individual item scores are summed to arrive at a total score, which ranges from 0 to 30 points. Five points is the threshold stated as indicating pain.
Item generation process Doloplus-2 was developed by Wary et al., (1993) based on The Douleur Enfant (Gustave Roussy), a scale for young children and was adapted for use in older adults. Doloplus-2 was developed by the Doloplus-2 Group. Study 5 ( Pautex 2007) Following testing, the Doloplus-2 was shortened to include only the items which were significantly associated with VAS scores. This version was also compared with the VAS. The revised version contained 3-items of the somatic dimension and two of the psychosocial dimension.

Completed 06/08 2
Somatic Dimensions: • Somatic complaints • Protective body posture adopted at rest • Protection of sore areas
Psychosocial Dimensions • Social Interactions • Behavior
Content Validity Very little information on the tool development is available in English. It is not known if the tool was reviewed by an external panel of content experts in the field of pain in elders with dementia.
-Panel Commentary The purpose of the tool is clearly expressed and appropriate. The tool is based on sound assumptions of multidimensionality of pain in elders with pain that are supported in the literature on pain in elders with dementia. While there is emerging evidence that observation or informant-based pain assessment tools can track change in degrees of pain for individual residents, current literature does not support the hypothesis that such tools can reliably differentiate between mild, moderate, and severe pain, or rate pain severity on a scale from 0-10. As with any observational tool, a small number of behaviors observed increases its specificity, but limits sensitivity in that it may not detect pain in persons presenting with less obvious behaviors. The tool covers 5 of 6 pain behavior categories in the AGS Persistent Pain Guidelines: Facial expression, verbalizations/ vocalizations, body language, changes in activity patterns or routines, changes in interpersonal interactions. However, the category mental status change is not addressed. Several items are unclear in the English translation of the Doloplus-2 and seem foreign when compared to the words and expressions most commonly used in English literature on pain in dementia (eg “repetitive reactive behavior “vs “agitation or aggression”; “resists all persuasion” vs. “resistance to care”. “Protection of sore areas” is commonly referred to as “guarding” in English and “expression” is more commonly referred to as “facial expression”. This indicates that the English translation needs further refinement. Although the French version may have face validity, this has not been established for the English translation. It is unclear whether the lack of clarity in items is solely due to the translation or whether this lack of clarity is also present in the original French version. No description of the item generation process is available in English for the original Doloplus or for Doloplus-2.
Subjects Panel rating: 2 Revised: 2 Subjects Study 1(Lefebvre-Chapiro, 2001)
Many tests have been conducted at various sites in France and Switzerland. Internal consistency was tested in a pooled sample of 510 elders from all centers participating in the Doloplus-2 Group. Average age of subjects was 82.5 (± 8.0), range 66-96 years, with 173 males and 337 females. Inter-observer reliability was tested in two separate samples at palliative care hospitals at Metz-Thionville and Marseille respectively. The Metz-Thionville

Completed 06/08 3
study included 43 residents with an average age of 73.5 (± 7.21) with 28 males and 15 females. The Marseille study included 41 residents with average age 82 (±8.3) with 9 males and 32 females. Test–retest reliability was evaluated in a mixed sample of 83 residents with 16 males and 67 females. Average age was 82.5 (± 8.0), range 66-96 years with short, medium and long stay hospitalization as well as palliative care. Data from these divergent settings were pooled. Convergent validity was evaluated in various geriatric centers or palliative care units in France and Switzerland in a mixed sample of 143 elders, 44 males and 99 females with an average age of 80.7 years (± 8.8), range 65-101. Sensitivity was tested at 11 centers. The sample included 183 elders with an average age of 80.7 (± 8.6), range of 65-101, 73 males and 110 females. Study 2 ( Holen et al, 2005) Location: a nursing home in Trondheim, Norway Subjects: 59 nursing home residents with a ICD-10 diagnosis of dementia Age: The authors states that there was a “median age of 82 with a range of
39” Dementia: MMSE median of 9 (Q1=3, Q3=18) and 88% of the residents had
a score < 24. Three residents did not complete the MMSE because they were aggressive and/or refused to answer.
Diversity: unspecified minorities (14%) Pain:. The presence of pain was based on information in the medical record,
information from the nurse responsible for the patient or the patient’s primary contact, information from the patient when possible, and a clinical examination. Patient’s pain was scored using the NRS-11 (0-10 likert scale). Four residents received a score of 4 or greater, 28 residents received a score from 1-3, and 25 residents did not show signs of pain.
Staff: The Doloplus-2 was completed by the patient’s nurse who collaborated with the research assistant.
Study 3 (Pautex et al 2006 ) Location: in departments of geriatrics or psychiatry Subjects: 129 French speaking hospitalized residents who met the DSM-FIV criteria for dementia with a MMSE less than 11 and a Clinical Dementia Rating of 3 or greater. Age: 83.7±6.8 Gender: 40 men, 89 women Cognitive Status:
• Dementia - Alzheimer’s disease 50 (39%) - Mixed Dementia 44 (34%) - Vascular Dementia 21 (16%) - Other causes 14 (11%)
• MMSE 6.8±3.0 Pain: 57 (44%) reported experiencing pain Staff: Nursing staff in charge of the patient completed the Doloplus-2 Study 4 (Zwakhalen 2006) Location: nursing home and psycho-geriatric wards in the Netherlands

Completed 06/08 4
Subjects: 144 nursing home residents including 128 demented residents and 16 somatically ill nursing home residents Gender: demented residents (28 )21.9% men, (100) 78.1% women;
somatically ill residents 5 men, 11 women Age: mean age dementia residents 82.4 (6.8), somatically ill 78.1(10.6)
• Dementia: MDS Cognitive Performance Scale • Severe : 61(47.7%) • Moderate: 36(28.1%) • Mild: 28(21.9%) • Unknown: 3 (2.3%)
Pain: Based on information derived from the MDS. 25% of the psycho-geriatric patient experienced pain on a daily basis and 17.2% experience pain less frequently than daily. Of these residents that experienced pain, 14.1% had mild pain, 22.7% had moderate pain, and 5.5% experienced unbearable pain at times.
Staff: 12 nurses from three nursing homes in the Netherlands. Study 5 (Pautex 2007) Location: Geneva University Geriatric Hospital and Department of Psychiatry Subjects: 289 French speaking residents with a DSMIV diagnosis of dementia and 49 French speaking residents without a DSMIV diagnosis of dementia, but a MMSE of > 25. Gender: 133 women, 47 men Age: 83.7 ± 6.5 Cognitive Status:
• Diagnoses of Dementia (n=52, 39%) - Mixed Dementia (n=45, 34%) - VascularDementia (n=26, 20%), other causes (n=7, 5%)
• MMSE 18.0 ± 7.7 Pain: For those residents who reported experiencing pain its intensity as
measured by the VAS (10 point scale) was 4.0 (3.0) and by the 30-point observational rating scale was 4.0 (7.0). 49% of the residents reported that they experienced pain in response to a direct pain question.
Staff: Doloplus-2 was completed by the nurse in charge of the patient, after discussing the patient with 1 or 2 team members who had contact with the patient as well.
-Panel Commentary The French version of the tool has been tested in diverse populations and settings including long term care, geriatric clinics and palliative care in France and Switzerland. There is no mention of possible cross cultural issues. Only one of the five studies presented above included ethnic groups in the sample for tool evaluation. It is not mentioned how the tool developers controlled for variability between sites. Age distribution is appropriate. There is gender imbalance, but this is expected for the population. Using 5 subjects per tool item as the minimum requirement for this review, a minimum sample size of 50 subjects (10 items x 5 subjects) would be needed. Thus, with the exception of the sample that was used in study one for evaluation of inter-observer reliability the sample sizes listed above are sufficient for tool evaluation. In study 2 it is noted that only 4 residents in the sample actually presented with a pain score greater than 4 on a 10-point likert scale. Currently there is available literature written in English on the Doloplus-2; however the tool has only been tested in non-English populations. Although the evaluation of the tool in European samples is strong, there is a need to

Completed 06/08 5
complete more work with the Doloplus-2 in North American populations. Administration, Scoring, Feasibility Panel rating: 2 Revised: 2 Administration, Scoring, Feasibility
Study 1(Lefebvre-Chapiro, 2001): Scoring of items (see under “item generation” above). Individual trajectory of pain is emphasized. The score is viewed as individual and is not intended for comparison between residents. Change in the score over time is important. If there is doubt about the presence of pain, a therapeutic test is recommended. Instructions for administration of the tool have been developed. According to tool developers the tool takes at most a few minutes to administer. The tool is recommended for health-care, social care or home use. Scoring by several caregivers is recommended. Also family and other persons are encouraged to contribute. Study 4 ( Zwakhalen 2006) To assess the clinical usefulness of three scales (Doloplus-2, PACSLAC, and PAINAD) nurses were asked which scale they considered most useful and which scale they preferred after having used all of the scales for all of the participants. The nurses rated the tools using a 0-10 scale. 75% of the nurses preferred the PACSLAC to measure pain in elderly residents with dementia. The lowest usefulness scores were reported for Doloplus-2 (mean 5.6; SD 2.2). Nursing comments regarding Doloplus-2 include:” the scale provides a more general view, a clear manual is provided, and the scale is difficult to score and interpret.” Study 5 (Pautex 2007) One nurse from each unit was trained to use the Doloplus-2 and had the responsibility to train and supervise the other nurses for at least 1 hour. Administration of the Doloplus-2 took an average of 10 (6 to 12) minutes. In this study, it was possible to complete the Doloplus-2 for 180 residents, but the item for sleep pattern was not completed in three residents.
-Panel Commentary Method of administration is clearly described and scoring procedures are clearly described. Interpretation of tool score is unclear. It is not clear how the score of 5 to indicate pain was determined. The instructions indicate that if an item is inappropriate it is not scored. However, it is not noted how the overall score of the tool is affected when some items are not scored. Follow-up studies indicated that it took an average of 10 (6 to 12) minutes to administer the Doloplus-2. The tool developers have intended that the tool may be used by health care providers, personnel in social care as well as family of the elder, but training requirements to assure reliable results are not reported .It is important to note nurse comments identifying the Doloplus-2 as the least preferred tool for clinical use.
Reliability

Completed 06/08 6
Panel rating: 2 Revised: 2 Internal consistency Study 1(Lefebvre-Chapiro, 2001):
Internal consistency (See sample description under “subjects” above.) Cronbach alpha coefficient = 0.82 If any one of 10 items is eliminated, Cronbach alpha falls below 0.82. Study 4 ( Zwakhalen 2006) Internal consistency Cronbach alpha scores ranged from .58 to .80 Internal Consistency (Cronbach’s alpha) of the Pain Assessment Scales At Rest During Movement Doloplus-2 0.75(89) 0.74(26) Somatic Dimension 0.7 0.63 Psychomotor Dimension 0.8 0.77 Psychosocial Dimension 0.63 0.58 The pool of nurses that offered verbal critiques for the tools commented that “it is questionable whether all items of the Doloplus-2 are relevant to detect pain.” Study 5 (Pautex 2007) Internal consistency was lower in residents with dementia (r=0.67) than in residents who were cognitively intact (r=0.84). Internal consistency scores were lowest for the items expression (r=0.82) and mobility (r=0.82). Internal consistency was slightly lower for the shortened version or the Doloplus-2 (Cronbach alpha=0.71) than the complete version (Cronbach alpha 0.85).
Interrater reliability Study 1(Lefebvre-Chapiro, 2001): Interobserver reliability was tested in two separate studies at palliative care hospitals at Thionville and Marseille respectively: For both studies the paired sample t-test was used to analyze the data. Thionville (See sample description under “subjects” above.) Scorer A: Total average score 11.4/30 (± 5) Scorer B: Total average score 10.9/30 (± 4.8) Marseille (See sample description under “subjects” above.) Scorer A: Total average score 17.3/30 (± 4.9) Scorer B: Total average score 17.1/30 (± 4.6).
Test-retest reliability Study 1(Lefebvre-Chapiro, 2001): Test-retest reliability is reported. (See sample description under “subjects” above.) Pain scores were measured at 2 times at 4 hour intervals. T-test was conducted: T1: average score: 9.33/30 (±5.17) T2 (+ 4h): average score: 9.36/30 (±5.47) Student’s t-test was not statistically significant.

Completed 06/08 7
Study 5 (Pautex 2007) Test-retest evaluation was completed on subsamples of 20 residents from the same hospital units who had the same characteristics and stable chronic pain. The first Doloplus-2 was completed on a given day and then the second Doloplus-2 was completed one day after the first one. The interclass correlation coefficient between the first and second assessment was 0.96.
-Panel commentary For study 1, little information is available about the sample that was used to arrive at the results for internal consistency, especially as relates to cognitive status of residents. There is also no information provided regarding raters of the residents for this study. However, the Cronbach alpha coefficient is appropriate for the data and the correlation coefficient is strong. Subsequent studies provide support of internal consistency with good correlations. In the sample used to test inter-rater reliability, no information on the cognitive status of the residents or a description for the raters is provided. Here, the data do not appear to be analyzed by subject. Average scores and t-tests do not adequately assess interrater reliability of the tool. Data from two raters independently and simultaneously assessing one subject would be considered appropriate. No correlation coefficient is provided. Subsequent studies do no contribute to inter-rater reliability. In study 1, scores from the same subject measured at two different times were measured. The interval of 4 hours was appropriate if no intervention occurred. Average scores were calculated and Student´s t-test was conducted. However, data on the t-test were not reported. Moreover, correlation would have been more appropriate. Information on how the test-retest was conducted is limited. No information is provided as to whether subjects received any pain treatment between measurements. There is also no information on the qualifications of the raters. Data were pooled from various settings. There is no report on how the tool developers controlled for variability across settings. The subsequent study that contributed to test-retest shows a strong interclass correlation coefficient of .96. The repeat test for test-retest evaluation was completed on the following day, which is a fairly short time frame for retesting. However, there is also a concern for receiving stable pain measures if test-retest is completed following a longer time frame. There is still a need for data from English speaking populations.
Validity: Criterion or construct Panel rating: 1 Revised: 2 Construct validity/ Criterion related validity
Convergent validity Study 1(Lefebvre-Chapiro, 2001): (See sample description under “subjects” above.) Doloplus-2 and VAS scores were compared. VAS scores varied from 0 to 10 with an average score of 5.46 (± 2.27). The convergent validity of the VAS and Doloplus-2 scale was significant (p<0.001). Sensitivity: (See sample description under “subjects” above.) D0: 10.6 (± 5.3); D1: 7.5 (± 4.4); D7: 4.9 (± 4.2). Study 3 (Pautex et al 2006) Each patient was given the Verbal Rating Scale (VRS), the Faces Pain Scale

Completed 06/08 8
(FPS), and the Horizontal Visual Analog Scale (HVAS). Residents were asked to position a sliding marker to indicate the level of pain they were currently experiencing. Residents were considered to have demonstrated comprehension of the scale if on both occasions they were able to explain its use and could correctly indicate which position corresponded to no pain at all and which position corresponded to the most severe pain. On each occasion the explanations were repeated up to three times before subjects were considered unable to comprehend a scale. On the same day the nursing staff in charge of the patient completed the Doloplus-2. The Doloplus-2 correlated only moderately with self-assessment ratings (r=0.26 to 0.63, P<.001) in residents reporting pain. For residents reporting pain using the VRS, HVAS, and FPS, the median pain intensity scores (interquartile range) were 3.0(2.0), 3.0(3.0), and 2.0(2.0) respectively. Using the Doloplus-2 to measure pain the median pain intensity (interquartile range) was 9.0(5.0). The observational rating scale tended to underestimate severity when compared with all three self-assessment scales. Correlation between Different Scales:
Spearman rho First Assessment Second Assessment
VRS HVAS FPS VRS HVAS FPS Doloplus-2 0.47 0.25 0.36 0.63 0.24 0.48 Study 4 (Zwakhalen 2006) To examine construct validity of the Doloplus-2, pain vs. non-pain groups were created based on information about “no pain” versus “daily pain” derived from the MDS scale. The mean total scores for the “daily pain” group were 9.8(6.0) and the “no pain” group had a mean of 5.1(3.9). The Doloplus-2 was then compared to the following pain assessment tools: VAS, VRS, PACSLAC, and PAINAD. Low scores were found for the Doloplus-2 as compared to the other pain assessment tools which had correlations scores ranging from 0.69 to 0.89. Pearson Correlation Between Scales
DOLOPLUS-2 VAS rater 1 0.29 VRS 0.36 VAS nurse 0.33 PACSLAC 0.29 PAINAD 0.34 Study 5( Pautex 2007) Convergent Validity was evaluated between the VAS and the Doloplus-2. Residents were considered to have understood the VAS if on two occasions they were able to explain its use and could clearly explain which position on a sliding vertical marker represented no pain and the most severe pain. Following the self assessments the nurse that was in charge of the patient completed the Doloplus-2. The Spearman’s coefficient was equal to 0.46 for the correlation between the Doloplus-2 and the VAS. The correlation was higher for residents without

Completed 06/08 9
dementia, 0.68 vs. 0.38 in residents with dementia. Half of the included residents reported no pain so a sub- analysis that included only residents who reported pain was performed. The results showed a significant correlation between Doloplus-2 and VAS (Spearman coefficient=0.36, p=0.000). In a multiple linear regression model Doloplus-2 predicted 41% of the variability of pain intensity measured by the VAS. Doloplus-2 predicted 69% of the VAS score in residents without dementia and 36% in residents with dementia. The somatic dimension explained 36% of the variability and the psychosocial dimension explained 5% of the variability, but psychomotor dimension barely contributed. The intensity of pain measured by the VAS was mainly associated with the somatic dimension of Doloplus-2 in particular the items: somatic complaints, protective body postures, and protection of sore areas. Two items of the psychosocial reaction were also statistically significant (p < 0.05): social interaction and behavior. These items were then used to develop a shortened version of the Doloplus-2 to compare with the VAS. The correlation between the intensity of pain measured by the VAS and the score of the shortened version of the Doloplus-2 was 0.48. Here the correlation was also better in residents without dementia (0.71 vs. 0.39 in residents with dementia). Criterion Validity Study 2 (Holen et al, 2005) Pain ratings by experts using the NRS-11 were set as the standard for criterion validity. A regression analysis was performed to evaluate how well the Doloplus-2 could predict the expert’s scores using two methods: regression analyses of each item’s isolated explanation value of the expert score and step wise regression analysis to explore the consecutive contribution of the different Doloplus-2 items. The experts rated 25 residents as pain free. Among these 6 had a Doloplus-2 score of 0 and 19 had <5 leaving five false positives with scores of 5 and 6. (Of the 59 cases the Doloplus-2 made false positives on 10 occasions). A regression analysis was performed to explore how well the Doloplus-2 could explain the experts’ pain scores. The unstandardized residuals had a SD=1.02. The Doloplus-2 explained 62% of the variance of the pain distribution in this population. Stepwise regression analysis demonstrated that facial expressions explained 48% of the variance of the expert score alone. Facial expressions, protective body postures adopted at rest, somatic complaints, and communication explained 68% of the total variability in the experts’ scores in the study population. For 85% of the assessments, the Doloplus-2 score multiplied by 0.25 beta corresponded to the expert score ± 1 unit on the NRS scale.
-Panel commentary There has been a considerable amount of evidence supporting the validity of the Doloplus-2 in subsequent studies. However, all of the studies have been in foreign populations and further validation needs to be done in English. The surprisingly high correlation between the Doloplus-2 and self report rating scales as reported in Study 3 are inconsistent with the finding in the literature. Most studies report correlations of approximately .30 between observational tools and self-report assessments. Use of the VAS by elders with dementia as a gold standard for comparison is questionable. If the VAS is used by the caregiver, question also remains

Completed 06/08 10
regarding ability/accuracy of health care provider judgments of severity in this population.
Summary of panel evaluation of pain assessment tool The Doloplus-2 is a comprehensive tool for assessing pain in nonverbal elders. The tool addresses many key indicators noted in the literature and AGS Guidelines. The tool is conceptually supported. Via their website information the tool developers report extensive testing in Europe. High correlations are reported between the Doloplus-2 and self-report assessment tools and the correlations that are reported are significantly higher than typically shown in the literature. Internal consistency has been adequate with good correlation values. The validity of the tool is supported in subsequent studies. It must be noted that in one study nurses in the clinical setting identified the tool as the least preferred method of pain assessment when compared to other similar observational tools. However, information in English is limited and available reports do not provide sufficient detail on which to base sound judgment of the tool evaluation. Translation issues are evident and further study or description regarding the use of Doloplus-2 in English-speaking populations is needed. Sources of evidence Doloplus-2 website: http://www.Doloplus-2.com Holen, J., Saltvedt, I., Fayers, P., Bjornnes, M., Stenseth, G., Hval, B., et al (2005). The Norwegian
Doloplus-2, a tool for behavioral pain assessment: translation and pilot validation in nursing home residents with cognitive impairment. Palliative Medicine, 19, 411-7.
Lefebvre-Chapiro, S. & the Doloplus-2 group. (2001). The Doloplus-2 scale – evaluating pain in the elderly. European Journal of Palliative Care, 8(5), 191-194.
Pautex, S. Michon, A., Guedira, M. Emond, H., Le Lous, P., Samaras, D. et al (2006). Pain in severe dementia: Self-assessment or observational scale? JAGS, 54, 1040- 1045.
Pautex, S., Herrmann, F., Michon, A., Giannakopoulos, P., Gold, G. (2007). Psychometric properties of the doloplus-2 observational pain scale and comparison to self-assessment in hospitalized elderly. Clinical Journal of Pain, 23(9), 774-9.
Zwakhalen, S., Hamers, J., & Berger, M. (2006). The psychometric quality and clinical usefulness of three pain assessment tools for elderly people with dementia. Pain, 126, 210-220.
Key to panel rating 3= Available evidence is strong 2= Available evidence supports need for further testing 1= Available evidence is insufficient and/or tool revisions are needed 0= Evidence is absent Contact Information for tool developer: Dr. Bernard Wary Service Regional de Soins Palliatifs CHR Meta-Thionville-BP 60327 57126 Thionville Cedex France E-mail [email protected] Official Doloplus-2 website: http://www.doloplus.com/versiongb/rubautres/intro.htm Contact e-mail address found at official Doloplus-2 website: [email protected] Evaluation 04/04 by: K. Herr, S. Decker, K. Bjoro, University of Iowa. Contact information: [email protected] Revision 06/08 by: K. Herr, B. Black, H. Bursch, The University of Iowa

COPYRIGHT
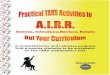
DOLOPLUS-2 SCALE BEHAVIOURAL PAIN ASSESSMENT IN THE ELDERLY
Behavioural RecordsNAME : Christian Name : Unit :
1• Somatic complaints
2• Protective body posturesadopted at rest
3• Protection ofsore areas
4• Expression
5• Sleep pattern
6• washing &/or dressing
7• Mobility
8• Communication
9• Social life
10• Problems ofbehaviour
SCORE
DATES
SOMATIC REACTIONS
PSYCHOMOTOR REACTIONS
PSYCHOSOCIAL REACTIONS
• no complaints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• complaints expressed upon inquiry only . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• occasionnal involuntary complaints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• continuous involontary complaints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• no protective body posture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• the patient occasionally avoids certain positions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• protective postures continuously and effectively sought . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• protective postures continuously sought, without success . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• no protective action taken . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• protective actions attempted without interfering against any investigation or nursing . . . . . . . . . . . . . . 1 1 1 1• protective actions against any investigation or nursing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• protective actions taken at rest, even when not approached . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• usual expression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• expression showing pain when approached . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• expression showing pain even without being approached . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• permanent and unusually blank look (voiceless,staring, looking blank) . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• normal sleep . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• difficult to go to sleep . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• frequent waking (restlessness) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• insomnia affecting waking times . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• usual abilities unaffected . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• usual abilities slightly affected (careful but thorough) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• usual abilities highly impaired, washing &/or dressing is laborious and incomplete . . . . . . . . . . . . . . 2 2 2 2• washing &/or dressing rendered impossible as the patient resists any attempt . . . . . . . . . . . . . . . . . . 3 3 3 3
• usual abilities & activities remain unaffected . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• usual activities are reduced (the patient avoids certain movements and reduces his/her walking distance) . 1 1 1 1• usual activities and abilities reduced (even with help, the patient cuts down on his/her movements) . . . . 2 2 2 2• any movement is impossible, the patient resists all persuasion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• unchanged . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• heightened (the patient demands attention in an unusual manner) . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• lessened (the patient cuts him/herself off) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• absence or refusal of any form of communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• participates normally in every activity (meals, entertainment, therapy workshop) . . . . . . . . . . . . . . . . . 0 0 0 0• participates in activities when asked to do so only . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• sometimes refuses to participate in any activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• refuses to participate in anything . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3
• normal behaviour . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 0 0 0• problems of repetitive reactive behaviour . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1 1 1• problems of permanent reactive behaviour . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 2 2• permanent behaviour problems (without any external stimulus) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3 3 3

Somatic complaintsThe patients expresses pain by word, gesture, cries, tears or moans.
Protective body postures adopted at restUnusual body positions intended to avoid or relieve pain.
Protection of sore areasThe patient protects one or several areas of his/her body by a defensive attitude or gestures.
ExpressionThe facial expression appears to express pain (grimaces, drawn, atonic) as does the gaze (fixedgaze, empty gaze, absent, tears).
InvestigationAny investigation whatsoever (approach of a caregiver, mobilization, care procedure, etc.).
Washing/dressingPain assessment during washing and/or dressing, alone or with assistance.
MobilityEvaluation of pain in movement: change of position, transfer, walking alone or with assistance.
CommunicationVerbal or non-verbal.
Social lifeMeals, events, activities, therapeutic workshops, visits, etc.
Problems of behaviourAggressiveness, agitation, confusion, indifference, lapsing, regression, asking for euthanasia, etc.
DOLOPLUS-2 SCALE : LEXICON

1 • Scale use requires learningAs is the case with any new instrument, it is judicious to test it before circulating it. Scale scoring timedecreases with experience (at most a few minutes). Where possible, it is of value to appoint a referenceperson in a given care structure.
2 • Pluridisciplinary team scoringIrrespective of the health-care, social-care or home structure, scoring by several caregivers is preferable(physician, nurse, nursing assistant, etc.). At home, the family and other persons can contribute using a liaison notebook, telephone or even a bedside meeting. The scale should be included in the 'care' or 'liaison notebook' file.
3 • Do not score if the item is inappropriateIt is not necessary to have a response for all the items on the scale, particularly given an unknown patienton whom one does not yet have all the data, particularly at psychosocial level. Similarly, in the event ofcoma, scoring will be mainly based on the somatic items.
4 • Compile score kineticsRe-assessment should be twice daily until the pain is sedated, then at longer intervals, depending on thesituation. Compile score kinetics and show the kinetics on the care chart (like temperature or blood pressure).The scale will thus become an essential argument in the management of the symptom and in treatment initiation.
5 • Do not compare scores on different patientsPain is a subjective and personal sensation and emotion. It is therefore of no value to compare scoresbetween patients. Only the time course of the scores in a given patient is of interest.
6 • If in doubt, do not hesitate to conduct a test treatment with an appropriate analgesicIt is now accepted that a score greater than or equal to 5/30 is a sign of pain. However, for borderlinescores, the patient should be given the benefit of the doubt. If the patient's behavior changes followinganalgesic administration, pain is indeed involved.
7 • The scale scores pain and not depression, dependence or cognitive functionsNumerous instruments are available for each situation. It is of primary importance to understand that thescale is used to detect changes in behavior related to potential pain.Thus, for items 6 and 7, we are not evaluating dependence or independence but pain.
8 • Do not use the DOLOPLUS 2 scale systematicallyWhen the elderly patient is communicative and cooperative, it is logical to use the self-assessment instruments.When pain is patent, it is more urgent to relieve it than to assess it ... However, if there is the slightestdoubt, hetero-assessment will avoid underestimation.
DOLOPLUS-2 SCALE : INSTRUCTIONS FOR USE

Completed 04/04 Revised 06/08
1
The Non-Communicative Patient’s Pain Assessment Instrument (NOPPAIN) Brief The Non-Communicative Patient’s Pain Assessment Instrument (NOPPAIN) is a nursing assistant-administered instrument for assessing pain behaviors in patients with dementia. This tool focuses on observation of specific pain behaviors while doing common care tasks. Pain is assessed at rest and with movement. The tool has four main sections: 1) care conditions under which pain behaviors are observed such as bathing, dressing, transfers; 2) six items about presence/absence of pain behaviors (pain words, pain noises, pain faces, bracing, rubbing and restlessness), 3) pain behavior intensity ratings using a six point Likert scale; 4) a pain thermometer for rating overall pain intensity. The method of administration for using the NOPPAIN is described; however, scoring procedures are unclear. Moreover, no criteria are provided for establishing low-high intensity of pain behavior. Interpretation of tool score is unclear and there is no indication on how to proceed once rating of individual items is completed. The tool requires little time to complete following a period of observation consistent with time to complete care activities. NOPPAIN derives a level of pain intensity from the presence and intensity of behaviors observed. The tool developers called it a pain screening tool because diagnosis or analysis of observation is not within the scope of NA practice. NAs are asked to perform behavioral observation and rate intensity of behaviors prior to formulation of a global pain score in each patient. The basis for assessment of intensity of behaviors is not reported neither is the process of how NAs translate the NSR of behavior intensity into a VDS of pain intensity.
The tool was clearly developed for use by nursing assistants. Thus, scope of practice for nursing assistants in screening for pain must be considered. It is unclear what investment in training of nursing assistants is needed to assure accuracy in tool completion. Horgas (2007) tested the reliability and validity of the NOPPAIN when used as assessment instrument by nurses; she demonstrated that accuracy of administration might be improved with training. The NOPPAIN has been evaluated in two studies: Study 1 involved research NAs who viewed videos of an actress portraying an individual with severe dementia receiving care from a NA. The NAs were mainly African-American, female, on average 37 years of age with high school diploma/GED and nearly 10 years of experience. In study 2 The NOPPAIN was evaluated in 4 Houston nursing homes and a VA nursing home unit and involved severely demented residents; the sample was predominantly female and culturally diverse. The nursing assistants were mainly female African-American, average age 37 years with 50% holding a high school education.
The tool is complex and large sample sizes would be needed to establish internal consistency for all items. Using 5 subjects per tool item as a minimum requirement for this review, a minimum sample size of 35 subjects (7 items x 5 subjects) would be needed to test the six pain behaviors, their intensities and the global pain score on the pain thermometer. Study 2 (unpublished) and study 3 involving real patients met the minimum sample size requirement. More studies are needed beyond the laboratory setting and involving more diverse patient populations.

Completed 04/04 Revised 06/08
2
Reliability • Internal consistency. No report of internal consistency is currently available. • Interrrater reliability was evaluated in study 2 (see above) using videotapes of NAs
performing morning care tasks with residents with dementia. Twenty six videos were shown to 6 untrained NAs and to 6 NAs who received one hour of training on use of the NOPPAIN. IRR’s were moderate to strong for all tool items and improved with one hour of training. Horgas found interrater reliability for presence of the 6 behaviors to be good. Average interrater reliability for pain intensity was very good.
• Test-retest reliability was evaluated in study 2 with a subset of untrained NAs. Results indicate low to moderate test retest reliability at both 2 and 24 hours. Only the Pain thermometer was stronger at 2 hours than 24 hours. In the Horgas study, each student rater re-scored 10% of the videos 1 week later: average κ of 0.7 and 0.86 for presence of pain. ICC >0.67 for pain intensity ratings (missing intra-rater consistency for pain words and rubbing).
Validity • Construct validity was evaluated in study 1 using standard videotaped patient
scenarios representing a continuum of pain intensity levels using an actor to portray a bed-bound patient with severe dementia receiving care from a NA. NAs watched and rated videos using the NOPPAIN assessment process and completed global pain rating for each video. NAs global pain rating on the NOPPAIN and pain levels portrayed in the videos resulted in weighted Kappa=0.87. NAs identified videos showing the most pain from each of 15 pairs. The parameter estimates conformed to expected responses, although borderline. The lowest intensity pain condition had the smallest parameter, with parameter size increasing with each subsequent level of the pain response scale. All pain level comparisons were 82-10% correct.
• Construct validity was evaluated in study 2 comparing NOPPAIN ratings by untrained NAs to physician NOPPAIN ratings and physician pain classification (pain/no pain) using sensitivity/specificity. For the Pain Activity Summary Score sensitivity and specificity was moderate to strong. For the Pain Behaviors Summary Score sensitivity was strong, however specificity scores were low suggesting the tool may classify patients as having pain when they are not. Moreover caution is warranted due to low levels of pain in the sample that limits evaluation of tool ability to detect pain in those with higher pain levels.
• Horgas compared nurse-ratings of pain intensity with videotaped behaviors of real patients believed to be in pain. Videos were coded extensively using the Keefe and Block Pain Behavior Measurement System. This additional standard for comparison adds to claims for convergent validity of the NOPPAIN even outside the laboratory setting.
• Horgas found strong correlations between NOPPAIN and self-reported VDS and NRS in the cognitively intact population only. This underscores the need for behavioral assessment in this population.
• The concern remains that the tool only captures typical pain behaviors and while raters consistently identify intensity as portrayed in an enacted sequence there is no validation that patients will present with this sequence as expression of intensity. A

Completed 04/04 Revised 06/08
3
final concern is that, while caregivers can identify pain in video, they may actually under-detect pain within the caregiving context itself.
Summary
The NOPPAIN was developed for the purpose of nursing assistant’s screening for pain in older adults with dementia. The tool has limited comprehensiveness with behaviors addressing only obvious and not subtle cues or changes indicated in the literature. However, preliminary testing has established that the screening tool is reliable and has preliminary validity, thus may be useful when combined with a more comprehensive screen for other indicators. Use of proxy report for pain severity in a nonverbal population has not been supported in the literature and this aspect of the tool should be evaluated in clinical samples. The tool has been tested in a racially/ethnically diverse sample, although further study is warranted. The tool appears to be clinically useful given the ability of nursing assistants to use and the limited time required for completion. Further psychometric testing is encouraged, including consideration of items to tap nursing assistant’s knowledge of baseline behavior and recognition of subtle changes that might reflect presence of pain. Because assessment activities are outside the scope of nursing assistant practice, it will be important to determine if the expectations of the tool for NA’s are actually screening activity. The tool was used successfully by senior nursing students in the laboratory setting rating real patient videos.
Sources of evidence
Snow , A.L., Hovanec, L., Passano, J., Brandt, J. (2001). Development of a pain assessment instrument for use with severely demented patients. Poster session presented at the Annual Meeting of the American Psychological Association. Washington, DC.
Snow, A. L., Weber, J. B., O'Malley, K. J., Cody, M., Beck, C., Bruera, E., et al. (2004).
NOPPAIN: A nursing assistant-administered pain assessment instrument for use in dementia. Dementia and Geriatric Cognitive Disorders, 17(3), 240-246.
Snow, A.L.,Cody, M., Beck, C., Bruera, E., O’Malley, K.J. Aston, C., El-Issa, L., Kunik, M.E.
Nursing assistants as pain screeners for nursing home residents with severe dementia: In vivo validation of the NOPPAIN. (draft article, 2004).
Horgas, A. L., Nichols, A. L., Schapson, C. A., & Vietes, K. (2007). Assessing pain in persons with dementia: Relationships among the non-communicative patient's pain assessment instrument, self-report, and behavioral observations. Pain Management Nursing: Official Journal of the American Society of Pain Management Nurses, 8(2), 77-85.
Contact information for tool developer: Lynn Snow, PhD E-mail: [email protected] Critique completed by: K. Herr, S. Decker, K. Bjoro, University of Iowa (2004). Updated by : K. Herr, H. Bursch and B. Black, The University of Iowa (2008).
Contact information: [email protected]

Completed 04/04 Revised 06/08
1
Tool: Nursing Assistant-Administered Instrument to Assess Pain in Demented Individuals (NOPPAIN) Tool developer: Snow, A.L., Weber, J.B., O’Malley, Cody, M., Beck, C., Bruera, E., Ashton, C., Kunik, M.E. Country of origin: USA Reviewed: 04/04 Revised: 06/08 Conceptualization Panel rating: 2 Revised: 2 Purpose The Non-Communicative Patient’s Pain Assessment Instrument (NOPPAIN)
is a nursing assistant-administered instrument for observing and rating pain behaviors in patients with dementia.
Conceptual basis No definition of pain or identification of the conceptual basis for the tool is provided. There is recognition that verbal assessment of pain in patients with dementia Alzheimer type (DAT) is problematic. This tool focuses on observation of specific pain behaviors while doing common care tasks, such as bathing, dressing and transfers. Pain is assessed at rest and with movement. NOPPAIN derives a level of pain intensity from the presence and intensity of behaviors observed. The tool developers called it a pain screening tool because diagnosis or analysis of observation is not within the scope of NA practice. NAs are asked to perform behavioral observation and rate intensity of behaviors prior to formulation of a global pain score in each patient. Horgas (2007) tested the reliability and validity of the NOPPAIN when used as assessment instrument by nurses.
Item Generation The tool was developed by consultation with a panel of 10 clinical and research experts in pain assessment in dementia, nursing home research and psychometrics that advised about item and instrument format issues. Little information is provided about the actual items that were generated in this process. However, the resulting items appear to reflect those on the Checklist of Nonverbal Pain Indicators (Feldt, 1998). The basis for assessment of intensity of behaviors is not reported neither is the process of how NAs translate the NSR of behavior intensity into a VDS of pain intensity. Nursing assistants’ global assessment of pain is based on the tool developer’s assumption that caregivers can reliably rate the intensity of pain in elders. Tool items The tool has four main sections: In the first section questions are asked about the caregiving situation (what tasks were performed and whether pain was observed). Two simple questions allow the patient to self-report about pain and hurt. In the second section the nursing assistant is presented with 6 pain behaviors with graphic illustrations: • Pain words • Pain noises • Pain faces • Rubbing

Completed 04/04 Revised 06/08
2
• Bracing • Restlessness For each of these items the nursing assistant is asked 1) if the behavior was observed (yes/no) and 2) to rate the intensity of the particular behavior on a 5 point numeric rating scale (NSR) with anchors 0=lowest possible intensity, 5=highest possible intensity. Section three allows the NA to mark the location of pain on a body schematic. In section four the nursing assistant is asked to rate the patient’s global pain intensity on that day on a verbal descriptor scale (VDS) in the shape of a pain thermometer with 6 verbal pain descriptors from “no pain” to “pain is almost unbearable.”
Content Validity The NOPPAIN is based on review of the literature and was developed in consultation with a multidisciplinary panel of experts not involved in the study. Content validity was established in study 1 (Snow, 2004) where nursing assistants identified NOPPAIN behaviors in a standardized actor-patient video and were able to distinguish levels of pain based on enacted behaviors by comparing 2 different videos/pain levels at a time. Study 3 (Horgas, 2007) This study compares nurse-ratings of pain intensity with videotaped behaviors of real patients believed to be in pain. Videos were coded extensively using the Keefe and Block Pain Behavior Measurement System. This additional standard for comparison adds to claims for convergent validity of the NOPPAIN.
-Panel Commentary The tool covers 3 of 6 pain behavior categories in the AGS Persistent Pain Guidelines: Facial expression, Verbalizations/ vocalizations and Body language. More subtle pain behaviors in the AGS Guidelines are not addressed: Changes in activity patterns or routines, Mental status changes, Changes in interpersonal interactions. Thus, the tool has limited comprehensiveness which may limit the likelihood of detecting pain, particularly in patients who do not present with obvious pain behaviors. One justification for involving nursing assistants in pain screening is that they may observe subtle behaviors. However, the NOPPAIN only addresses typical pain behaviors. While the unique “knowledge” that the nursing assistant may contribute to pain screening is not specifically incorporated into the tool it is unknown how such unique knowledge influences formulation of the final global pain score assigned by the NA in each patient. The nursing assistant is expected to rate the intensity of a particular behavior on a 6 point scale. However, there is little indication as to what will be observed to differentiate levels of intensity. Beyond recognizing presence/absence of pain-related behaviors by caregivers, the current literature presents conflicting information about reliability and validity of caregivers’ proxy assessment of pain severity in elders with dementia who are experiencing pain. There is a conceptual leap in inferring not only the presence but also the intensity of pain from pain behaviors. While there is emerging evidence that observation or informant-based pain assessment tools can track change in degrees of pain for individual patients, current literature does not support the hypothesis that such tools can reliably differentiate between arbitrary categories on a VDS or even escalating levels on an NSR. More testing is needed to support any population-based normed correlation between intensity of pain behaviors and

Completed 04/04 Revised 06/08
3
intensity of pain. Use of standardized patient behavior for pain assessment and rating in cognitively impaired older patients is debatable. The addition of behavior coded real patient videos as gold standard in study 2 adds strength to the contention that nurses recognize pain behaviors and can identify levels of pain in individual patients.
Subjects Panel rating: 3 Revised: 2 Subjects Study 1 (Snow, 2004)
Characteristics of nursing assistants (N=21): Gender: Female: 86%, Male: 14% Average age: 37 years (±11.50), Range: 21-60 years. Racial/ethnic composition: Caucasian: 5%, African-American: 76%, Hispanic: 10%, Asian: 7%. Education background: High school diploma/GED: 71% Experience: average 9.8 years, range 3 mos. – 30 years All NAs were hired from the same temporary employment agency.
Study 2 (Snow 2004, unpublished) Setting: Four Houston nursing homes and a VA nursing home unit Characteristics of residents (n=83):
Age of subjects: Average 83.17 years (±8.79) Range 50-100 years Gender: Female: 70%, Male: 30% Average MDS-Cognition Subscale: 5.46 (±2.86) Racial/ethnic diversity: Caucasian: 68%, African-American: 12%,
Hispanic: 11%, Other: 9% Most common pain related diagnoses were arthritis (41%), “pain” (39%),
osteoporosis (28%) and fractures (28%). Characteristics of nursing assistants (N=20):
Gender: Female: 86%, Male: 14% Average age: 37 years (±10.50), Range: 21-60 years. Racial/ethnic composition: Caucasian: 4%, African-American: 81%,
Hispanic: 7%, Asian: 7%. Education background: High school diploma/GED: 59% All NAs were hired from the same temporary employment agency.
Study 3 (Horgas, 2007) 40 Subjects were randomly selected from a volunteer sample of 128 participants from a variety of institutional and community settings.
Mean age: 83 Gender: predominantly female Diversity: not stated Cognitive impairment: 20 subjects were cognitively intact (MMSE 24-30)
and 20 were impaired (MMSE 10-23). Subjects were English-speaking, able to stand up from a chair, with Dx of osteoarthritis in lower body and not visually or hearing impaired. All had previously completed pain interviews and videotaped activity protocol data from the parent study (parent study is not cited).
Characteristics of raters: 2 senior honors nursing students
-Panel Commentary There is a clearly identified focus on the longterm care setting. Gender balance in the NA samples of the first two studies reflects general distribution in this population. Both NA samples are racially/ ethnically

Completed 04/04 Revised 06/08
4
diverse. Patient subjects in the unpublished study 2 are severely cognitively impaired as measured with standard dementia assessment tool (MMSE). Study 3 sample is only 50% cognitively impaired and less diverse. Sample size (N=40) is adequate but has some missing observations. The tool is complex and large sample sizes would be needed to establish internal consistency for all items. Using 5 subjects per tool item as a minimum requirement for this review, a minimum sample size of 35 subjects (7 items x 5 subjects) would be needed to test the six pain behaviors, their intensities and the global pain score on the pain thermometer. Study 2 (unpublished) and study 3 involving real patients meet the minimum sample size requirement. More studies are needed beyond the laboratory setting and involving more diverse patient populations.
Administration, Scoring, Feasibility Panel rating: 2 Revised: 2 Administration, Scoring, Feasibility
The tool has four main sections (for specification see “Item Generation” section above). It was designed to require minimal training for proper use. Instructions on the form indicate that the NA should complete the form following at least 5 minutes of daily care activities while observing for pain behaviors. The form is to be completed immediately following care activities. In a feasibility study, administration of the NOPPAIN took nursing assistants less than 30 seconds after an average of 8.71 minutes (±3.70, range 3-15 minutes) involved in care activity and observing the patient prior to completion. Study 3 concluded that nurse raters were able to easily, reliably and validly rate pain behavior presence and intensity after a “short” training session using CD-ROM.
-Panel Commentary The method of administration is described but scoring procedures are unclear. No criteria are provided for establishing low-high intensity of pain behavior. NAs only rate behaviors associated with activities performed. There are no directions as to how missing activities influence the global pain score. There is concern about NA rating of severity of the resident’s pain (on the pain thermometer) given inaccuracies of surrogate reporting. Study 3 (Horgas, 2007) demonstrated that accuracy of administration might be improved with training. Interpretation of the tool score is unclear. There is no indication on how to proceed once rating of individual items is completed. Findings for clinical utility are promising: The tool requires little time to complete following a period of observation consistent with time to complete care activities. The tool was clearly developed for use by nursing assistants. Scope of practice for nursing assistants in screening for pain must be considered.
Reliability Panel rating: 2 Revised: 2 Internal consistency Internal consistency of the tool has not been established.

Completed 04/04 Revised 06/08
5
Interrater reliability Study 2 (Snow, 2004 unpublished) Interrater reliability was conducted in a subsample of NAs (See characteristics of nursing assistants under subjects above). Interrater reliability was evaluated using 78 videotapes of NAs performing morning care tasks (e.g. cleaning, dressing, transferring, and toileting) with residents with dementia. Twenty-six videos were randomly chosen and shown in random order to a group of 6 NAs who had not participated in either the video development or training session on use of the NOPPAIN. To evaluate the effect of brief training on interrater reliability, a group of 6 NAs, independent from those who participated in the above activities, received one hour of training on how to complete the NOPPAIN. Interrater reliabilities (mean percent agreement) for each main item on the NOPPAIN for untrained and trained raters ranged as follows: Untrained raters Trained raters Was the activity done?* .79 - .94 .78 - .94 Pain during activity? .66 - .87 .66 - .92 Was Pain Behavior Present? .59 - .87 .69 - .99 Pain Behavior Intensity .68 - .92 .77 - .99 Pain Thermometer .85 .97 (* Activities include: lying down, turned, transferred, sitting, dressing, eating, standing, walking, bathing) Study 3 (Horgas, 2007) The PI and 2 undergraduate honors nursing students reviewed a brief standardized CD-based training program, i.e. they viewed enacted levels of pain as developed by the authors of NOPPAIN (see construct validity for study 1). Raters also practiced NOPPAIN scoring until they reached 90% agreement with the author. Nursing students then independently scored forty 10-minute videotapes which depicted the standardized activity protocol to elicit pain behaviors based on the work of Keefe and colleagues (see pain behaviors listed in item generation). Behaviors were presented in random sequence to minimize order effects.
Across the 6 behaviors, Kappa coefficients ranged from 0.72-1.0 for presence of the behavior (M=0.88). Raters agreed in a range of κ 0.72-1.0 on pain intensity (M=0.91).
Test-retest reliability Study 2 (Snow 2004, unpublished) This study was conducted with a subset of untrained nursing assistants (see under subjects above) with no previous contact with residents while providing morning care to residents. The procedure was repeated 2 hours later (n=42) and 24 hours later (n=34). Reliabilities reported were: 2 hours 24 hours Was Pain Behavior Present? .22 - .68a .27 - .67a Pain Behavior Intensity .25 - .68s .14 - .66s Pain Thermometer .60 s .39 s
a = phi correlations s=spearman correlation Study 3 (Horgas, 2007) Each student rater re-scored 10% of the videos 1 week later:
average κ of 0.7 and 0.86 for presence of pain

Completed 04/04 Revised 06/08
6
ICC =>0.67 for pain intensity ratings (missing intra-rater consistency for pain words and rubbing).
-Panel commentary Internal consistency needs to be established yet.
Interrater reliabilities were moderate to strong for all tool items. The reliabilities for observing presence of pain behaviors and pain behavior intensity improved with one hour of training. Test-retest reliability was low to moderate at both 2 and 24 hours. Only the Pain Thermometer was stronger at 2 hours than 24 hours (study 2). Test-retest/intrarater consistency over time in study 3 (Horgas, 2007) was good to very good.
Validity: Criterion or construct Panel rating: 2 Revised: 2 Construct validity/ Criterion related validity
Construct validity (study 1, Snow 2004) Standard videotaped patient scenarios representing a continuum of pain intensity levels were developed using an actor to portray a bed-bound patient with severe dementia receiving personal care from a nursing assistant. NAs watched and rated each video using the NOPPAIN assessment process. NAs completed the global pain rating for each video and were asked to identify the video showing the most pain from each of 15 pairs. NAs global pain rating on the NOPPAIN and pain levels portrayed in the videos resulted in weighted Kappa=0.87 (SE: 0.2, 95% CI: 0.82-0.91). For paired comparisons (Bradley-Terry model of paired comparisons), the parameter estimates conformed to expected responses, although borderline (Deviance GFI=18.14(10), p=0.0527, non-significance indicates a good fit). The lowest intensity pain condition had the smallest parameter, with parameter size increasing with each subsequent level of the pain response scale. Lack of agreement was mainly due to confusion between “mild pain” and “moderate pain,” which was shown by 65% of the raters. All pain level comparisons were 82-100% correct. Construct validity (study 2, Snow 2004, unpublished) Construct validity was evaluated by comparing nursing assistant NOPPAIN ratings to a physician gold standard. The gold standard for pain presence was consensus of two palliative care physicians on NOPPAIN scores and dichotomous pain classification. According to physician consensus classifications, 15 of 75 (20%) of patients were in pain. All 15 were classified by physician consensus as having mild pain on the pain thermometer; on the 0-10 pain scale, 8 (11%) were classified as having pain of level 1, 6 (8%) had pain at level 2 and 1 (1%) had pain at level 3. Pain behaviors were observed most often during transferring, turning, dressing. Of the pain behaviors: bracing, pain faces and pain noises were observed most often (in 67-73% of those classified as in pain), pain words (33%) and restlessness (13%) less often, while rubbing was not observed.

Completed 04/04 Revised 06/08
7
NOPPAIN Validity Indices using sensitivity/specificity were as follows:
Untrained rater validity: Physician ratings and NA ratings NA NOPPAIN NA NOPPAIN and and Physician Physician Pain NOPPAIN Classification (Pain/No pain)
Pain Activity Summary Score .73/.86 .67/.88 Pain Behaviors Summary Score .90/.45 .93/.43 Study 3 (Horgas, 2007) Convergent validity: Correlation analyses were conducted to examine the relationship between self-reported pain and NOPPAIN scores.
Correlation of NOPPAIN NRS and self-report NRS r = 0.39 (p<0.01) Correlation of NOPPAIN VDS and self-report VDS r = 0.31(p<0.05)
These correlations were twice as strong when figured separately for cognitively intact patients and not significant for the cognitively impaired sample. NOPPAIN scores were also compared to behavioral rating scores from detailed observational coding available for videos from the parent study. In the cognitively impaired sample correlations were very strong for all pain behaviors except bracing which was not observed In the cognitively intact sample, pain words and rubbing were not observed and there was no correlation with pain noises.
Total number of pain behaviors observed: r =/> 0.63 in the total group as well as in cognitively intact and impaired groups (p< 0.001).
-Panel commentary Preliminary evidence of tool validity is presented; however, additional study in clinical settings with larger samples and actual non-research caregivers is needed. The judgment of pain severity in persons with dementia by caregivers has not been substantiated in prior literature; however preliminary work on this tool using a standardized video approach suggests additional study in this area is warranted with clinical samples. The low specificity scores on the pain behavior items suggest the tool may classify patients as having pain when they are not. A caution is warranted regarding the low levels of pain in the sample that limits evaluation of tool ability to detect pain in those with higher pain levels. The poor correlation between NOPPAIN and self- report among cognitively impaired patients underscores the need for behavioral assessment in this population. The high correlation between detailed behavior coding and NOPPAIN scores strongly supports construct and criterion validity of the test outside the laboratory setting. The concern remains that the tool only captures typical pain behaviors and while raters consistently identify intensity as portrayed in an enacted sequence there is no validation that patients will present with this sequence as expression of intensity. A final concern is that, while caregivers can identify pain in video, they may actually under-detect pain within the caregiving context itself.
Summary of panel evaluation of pain assessment tool The NOPPAIN was developed for the purpose of nursing assistant’s screening for pain in older adults with dementia. The tool has limited comprehensiveness with behaviors addressing only obvious and not subtle cues or changes indicated in the literature. However, preliminary testing has established that the screening

Completed 04/04 Revised 06/08
8
tool is reliable and has preliminary validity, thus may be useful when combined with a more comprehensive screen for other indicators. One follow-up study supplied support for convergent validity of proxy report with detailed behavioral coding in patient video and this aspect of the tool should be evaluated further in clinical samples. The tool has been tested in a racially/ethnically diverse sample, although further study is warranted. The tool appears to be clinically useful given the ability of nursing assistants to use and the limited time required for completion. Because assessment activities are outside the scope of nursing assistant practice, it will be important to determine if the expectations of the tool for NA’s are actually screening activity. The tool was used successfully by senior nursing students in the laboratory setting rating real patient videos. Sources of evidence Snow , A.L., Hovanec, L., Passano, J., Brandt, J. (2001). Development of a pain assessment instrument for
use with severely demented patients. Poster session presented at the Annual Meeting of the American Psychological Association. Washington, DC.
Snow, A. L., Weber, J. B., O'Malley, K. J., Cody, M., Beck, C., Bruera, E., et al. (2004). NOPPAIN: A
nursing assistant-administered pain assessment instrument for use in dementia. Dementia and Geriatric Cognitive Disorders, 17(3), 240-246.
Snow, A.L.,Cody, M., Beck, C., Bruera, E., O’Malley, K.J. Aston, C., El-Issa, L., Kunik, M.E. Nursing
assistants as pain screeners for nursing home residents with severe dementia: In vivo validation of the NOPPAIN. (draft article, 2004).
Horgas, A. L., Nichols, A. L., Schapson, C. A., & Vietes, K. (2007). Assessing pain in persons with dementia: Relationships among the non-communicative patient's pain assessment instrument, self-report, and behavioral observations. Pain Management Nursing : Official Journal of the American Society of Pain Management Nurses, 8(2), 77-85.
Key to panel rating 3= Available evidence is strong 2= Available evidence supports need for further testing 1= Available evidence is insufficient and/or tool revisions are needed 0= Evidence is absent Contact address for tool developer Lynn Snow, PhD Houston Center for Quality of Care and Utilizations Studies Veterans Affairs Medical Center 2002 Holcombe Boulevard 142 Houston, Texas 77030 E-mail: [email protected] Evaluation completed by: K. Herr, S. Decker, K. Bjoro, University of Iowa. Revision 06/08 by:: K. Herr, H. Bursch, B. Black Contact information: [email protected]



Completed 04/04 Revised 06/08
1
The Pain Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC) Brief The Pain Assessment Scale for Seniors with Severe Dementia (PACSLAC) developed by a Canadian team, is a tool for the familiar caregiver to observe and assess both common and subtle pain behaviors. The tool is a checklist with four subscales and a total of 60 items: Facial expressions (13 items), Activity/body movements (20 items), Social/personality/mood (12 items) and Physiological indicators/eating and sleeping changes/vocal behaviors (15 items). Each item is scored on a present/absent dichotomous scale. Subscale scores are summed to arrive at a total score ranging from 0 to 60. However, no interpretation of the total score is currently available. Simple instructions on how to administer and score the tool are clearly described on the tool form. Preliminary cut-offs for determining pain presence are determined for the PACSLAC. Although the original PACSLAC includes 60 items, the tool requires a limited amount of time to administer, indicating that the tool is potentially useful in everyday clinical practice. Testing of the PACSLAC-D (Dutch Language), the shorter 24 item scale, suggests the tool is user friendly requiring a short time for training (30 minutes), has an established cut-off to facilitate score interpretation, and can be completed in a few minutes. Preliminary evidence of clinical utility and normative data for scoring is provided, although further validation with larger and more diverse is needed. The PACSLAC was tested in a sample of 40 RN/resident dyads in which the nurse recalled a resident that had been under his/her care for at least six months and who experienced pain. Nurses were 44 years on average with an average of 19 years experience. The 40 corresponding residents were 85 years on average, 30 females/10 males, 33 had a diagnosis of dementia and 34 had a diagnosis associated with pain. Follow-up studies evaluated the PACSLAC and PACSLAC D (Dutch language) prospectively in NH settings with samples of patients with dementia. Methods for evaluating cognitive status are appropriate and indicate severe impairment in most studies. Age and gender representation is appropriate. There is no information in any of the studies regarding racial/ethnic diversity, except testing in Canadians and Dutch. Using a minimum requirement of 5 subjects per item for the purposes of this review, the sample sizes for testing the PACSLAC and the PACSLAC-D (Dutch Language) are small. Additionally, few subjects in the existing studies had moderate or severe pain impacting evaluation of the tool usefulness across the full range of scoring. Additional evaluation in larger English-speaking samples with increased diversity are needed. Reliability • Internal consistency was good based on four remembered events: two painful events,
one distressing (but not pain-related) and one calm event. The methodology of using remembered events is appropriate in preliminary stages of tool development, but is subject to recall bias. Follow-up studies 3 and 4 were able to duplicate good internal consistencies for both total PACSLAC and PACSLAC D scales.
• Studies 3, 5 and 6 found generally high interrater reliabilities for both versions, total scales and sub scales.

Completed 04/04 Revised 06/08
2
• Study 3 had strong intrarater reliability between bedside and video scorings but the time interval is not specified.
• Additional testing in diverse samples, including those with greater range of pain severity, is recommended.
Validity • Discriminant validity was evaluated based on retrospective recall of painful events by
the nurse for four events as indicated above. The total PACSLAC score was able to discriminate among painful, calm, and non-pain related distress events (p<.001). Subscales: Facial expressions, Activity/rocking movement and Physiological indicators/eating and sleeping changes/vocal behaviors discriminated among painful, distressing and calm events (p<.001) and subscale Social/personality/mood discriminated between pain and calm events but not between pain and the distress events.
• Criterion related validity was moderate using Global Pain Intensity Ratings of the nurses’ perception of the patient’s pain as the “gold standard.”
• Zwakhalen translated the PACSLAC into Dutch and used principal component analysis with Oblimin rotation to reduce the 60-item tool into a shortened version with only 24 items. The reduced version of the scale strongly correlated with the long 60-item version of the scale with Pearson’s r of 0.945. It is important to note that the PACSLAC-D (Dutch Language) does not contain items that require prior knowledge of the patient and thus is a direct observation tool only. Both the PACSLAC and PACSLAC-D (Dutch Language) have been validated in Dutch. Further study of the PACSLAC is warranted to determine if frequency of item use and a similar factor structure and reduction holds up in English and other languages and populations.
• Further evaluation in studies 2, 3 and 5 provide support for congruent and discriminant validity of the PACSLAC, as well as preliminary support for cut-off points and sensitivity and specificity of the shorter PACSLAC-D (Dutch Language). Additional study in larger samples, with samples experiencing greater pain severity, and to evaluate tool sensitivity are needed.
Summary The PACSLAC is a potentially clinically useful behavior checklist that appears simple to use for assessing and monitoring changes in persons with dementia and diverse presentations of pain-related behavior. The tool is comprehensive and addresses pertinent indicators noted in the literature and AGS Guideline. Prospective evaluation has added to the tool’s reliability and validity, as well as factor analysis to determine the most efficient and useful indicator set for clinical use. However, the revised PACSLAC-D (Dutch Language) no longer contains items that are based on knowledge of the patient and this may under-recognize pain in patients who demonstrate less obvious indicators such as changes in activity or behavior. Because of this major revision in the tool, the PACSLAC and PACSLAC-D (Dutch Language) psychometric evaluations should be considered independently. Preliminary normative data and cut-offs are provided but require further validation in larger, more diverse samples. Additional factor analysis in English-speaking samples, other diverse samples, and in patients with increased levels of pain severity is needed, as is determination of tool sensitivity in detecting treatment effects.

Completed 04/04 Revised 06/08
3
Source of Evidence
Fuchs-Lacelle, S. & Hadjistavropoulos, T. (2004). Development and preliminary validation of the Pain Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC). Pain Management Nursing, 5(2).
Fuchs-Lacelle, S.& Hadjistavropoulos, T. (2005). A checklist for pain assessment in LTC.
PACSLAC: Pain Assessment Checklist for Seniors with Limited Ability to Communicate. Canadian Nursing Home, 16(4), 4-7.
Zwakhalen, S., Hamers, J. & Berger, M. (2006). The psychometric quality and clinical
usefulness of three pain assessment tools for elderly people dementia. Pain, 126(1-3), 210-220.
Zwakhalen, S., Hamers, J. & Berger, M. (2007). Improving the clinical usefulness of a behavioral
pain scale for older people with dementia. Journal of Advanced Nursing, 58(5), 493-502. Zwakhalen, S., Koopmans, R., Geels, P., Berger, M. & Hamers, J. (2008) The prevalence of pain
in nursing home residents with dementia measured using an observational pain scale. European Journal of Pain, xx, xxxx. (in press).
Fuchs-Lacelle, S., Hadjistavropolous, T. & Lix, L. (in press). Pain assessment as intervention: A
study of older adults with severe dementia. Clinical Journal of Pain, xx ,xxx. (in press) The authors recommend additional articles pertaining to a French language version of the PACSLAC (Dr. Thomas Hadjistavropoulos, personal communication, July 2008): Aubin, M., Verreault, R., Savoie, M., LeMay, S., Hadjistavropoulos, T., Fillion, L., Beaulieu, M.,
Viens, C., Bergeron, R., Vézina, L., Misson, L. & Fuchs-Lacelle, S. (2008). Validité et utilité clinique d'une grille d'observation (PACSLAC-F) pour évaluer la douleur chez des aînés atteints de démence vivant en milieu de soins de longue durée. Canadian Journal on Aging/La revue canadienne du vieillissement, 27, 45-55. [DISCUSSION OF PACLAC-F)
Aubin, M., Giguère, A., Hadjistavropoulos, T. & Verreault, R. (2007). Evaluation systématique
des instruments pour mesurer la douleur chez les personnes âgées ayant des capacités réduites à communiquer. Pain Research and Management, 12, 195-203. [Systematic review, using a grid of the PACSLAC in comparison to all other tools that we could find]
Contact information for PACSLAC: Thomas Hadjistavropoulos, PhD Email: [email protected] Contact information for PACSLAC-D (Dutch language version): Sandra Zwakhalen, PhD Email: [email protected] This summary was completed by: K. Herr, S. Decker, K. Bjoro, University of Iowa (2004). Updated by: K. Herr, H. Bursch and B. Black, The University of Iowa (2008).
Contact information: [email protected]

Reviewed: 04/04 Revised: 06/08
1
Tool: The Pain Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC) Tool developer: Fuchs-Lacelle, S.K. & Hadjistavropoulos, T. Country of origin: Canada Reviewed: 04/04 Revised: 06/08 Conceptualization Panel rating: 2 Revised: 2 Purpose The PACSLAC is a caregiver-administered pain assessment checklist using
direct observation and familiar caregiver information for the assessment of pain in elders with limited ability to communicate.
Conceptual basis A unified conceptual basis for the tool is not evident; However, the tool does tap pain behaviors from all 6 domains of the AGS Persistent Pain Guidelines. The authors acknowledge the limitations of rating behaviors as to pain intensity in a population with diverse presentations and thus pain indicators are measured on a dichotomous present/absent scale.
Item Generation Tool items There are four subscales with a total of 60 items: • Facial expressions (13 items) • Activity/body movements (20 items) • Social/personality/mood (12 items) • Physiological indicators/Eating and sleeping changes/Vocal behaviors
(15 items). Each item is scored on a dichotomous scale by checking off those pain behaviors that are observed. The number of checks on each subscale are added together and recorded and then these sums are added together for a total score. Phase I: Item generation Items were generated through serial interviews with experienced professional caregivers of seniors with severe dementia (see sample characteristics below). Interviews were recorded, transcribed. Transcribed material was then reviewed by two researchers who each independently developed an initial set of non-overlapping behaviors. The original total of 71 behaviors was collapsed to 65, which was used to develop the PACSLAC. A second coder independently used the list of 71 pain behaviors to review a random sample of 15 transcribed interviews. Agreement between the two coders on total number of instances each coder endorsed each behavior on the list resulted in correlation of 0.94 (p<.01). The behaviors were then grouped conceptually by the authors. Phase II: Item analysis and assessment of internal consistency A preliminary tool with 7 subscales with a total of 65 pain behaviors was used by a separate sample of 40 professional caregivers (see sample characteristics below) who reported on pain experiences of remembered patients with severe dementia. The number of subscale was reduced to four in order to improve internal consistency: Facial expressions, Activity/body movements, Social/personality/mood and Physiological indicators/Eating and sleeping changes/Vocal behaviors. Moreover, two items of the 65 items were deleted.

Reviewed: 04/04 Revised: 06/08
2
Phase III: Preliminary validation of the PACSLAC An additional three items were deleted following phase III. The final tool has 60 items on 4 subscales (see sample characteristics and results of validation study below).
Content Validity Phase II – Assessment of Usefulness The professional caregivers also rated PACSLAC items for usefulness on a numeric rating scale (Usefulness Scale) anchored by 0 (not useful) and 10 (very useful) to indicate how useful that specific behavior was for deciding whether pain was present. All items except one were rated as being useful in identifying pain as indicated by a score of at least “5”. Study 3 (Zwakhalen, Hamers & Berger, 2006) The study evaluated the validity of a Dutch-translated version of the PACSLAC and demonstrated reliability and validity in this language. Study 4 (Zwakhalen, Hamers, & Berger, 2007) Because 28 of 60 PACSLAC items were not used for over 90% of study participants in Study 3, item reduction was attempted. Using observation of patients for two minutes while receiving an influenza vaccination (T2) and during a patient-specific pain moment (e.g. care activities, washing or mobilization) (T3), item reduction techniques were used to refine the PACSLAC. This study used a translated (Dutch) version of the PACSLAC and the observer had no prior knowledge of the patient. Pain intensity was rated on a VAS. VAS and PACSLAC scoring were performed in random order within a time interval of less than three weeks. Principal components analysis with Oblimin rotation used to determine factor structure with re-examination of matrix following any item deletions to validate final scale and subscales. 35 items were discarded based on low IC and MSA values. Additional items were deleted based on low factor loadings. The final revised tool represented three components explaining 45.7% of variance with 24 items called PACSLAC-D (Dutch Language). Alpha for total scale with 24 items=0.86 at T2 and 0.82 at T3. Cronbach’s alpha for three subscales were high, ranging from 0.72 to 0.82. The reduced version of the scale was correlated with the long 60-item version of the scale with Pearson’s r of 0.945. It is important to note that the PACSLAC-D (Dutch Language) dos not contain items that require prior knowledge of the patient and thus is a direct observation tool only.
-Panel Commentary The tool covers all 6 pain behavior categories in the AGS Persistent Pain Guidelines. However, the subscales appear to be conceptually based (derived by the authors), rather than based on factor analysis. A strength of the PACSLAC is the broad nature of indicators that allows for recognition of pain in those with idiosyncratic or less obvious pain behaviors. The subscale “Physiological indicators/Eating and sleeping changes/Vocal behaviors” includes seven indicators that conceptually represent vocalization/verbalization; two represent change in activity pattern and three may represent change in mental status. Because of the large number of diverse indicators on this subscale, refinement may be needed. Because the PACSLAC is a broad list with potential pain indicators for acute and/or persistent pain and is not scored to represent severity of persistent pain, inclusion of physiological indicators appears appropriate. The items are dichotomous and scored as present/absent. The tool does not

Reviewed: 04/04 Revised: 06/08
3
attempt to measure pain severity, which is appropriate for older adults with dementia who are not able to communicate their pain verbally. The PACSLAC was assessed for content validity by an independent review process involving professional caregivers as experts and was assessed as being clinically useful for assessing pain in elders with severe dementia. A shortened version has been developed in Dutch called PACSLAC-D (Dutch Language) with 24 items derived through factor analytic procedures based on a small sample and based on an acute pain episode (with small sample experiencing situation-based pain). This shortened tool has preliminary reliability and validity, although additional testing with other types of more chronic pain and larger samples is needed. Both the PACSLAC and PACSLAC-D (Dutch Language) have been validated in Dutch. Further study of the PACSLAC is warranted to determine if frequency of item use and a similar factor structure and reduction holds up in English and other languages and populations. It should be noted that the PACSLAC is an informant-based tool requiring knowledge of the patient’s baseline behaviors as opposed to the PACSLAC-D (Dutch Language) which is strictly an observation-based tool. Given the fact that there are 60 items in the PACSLAC it has been suggested that the very few items requiring prior knowledge of the patient could be left blank. More testing is needed to see how this would affect reliability of the PACSLAC.
Subjects Panel rating: 1 Revised: 2 Subjects Study 1 (Fuchs-Lacelle & Hadjistavropoulos, 2004)
Stage I 28 primary caregivers of elders 65 years of age or older living in long term care due to serious limitations in their ability to communicate. The primary caregivers were registered nurses, licensed practical nurses and special care aides Stage II 40 RN/Resident Dyads 40 Registered nurses and registered psychiatric nurses who worked in long term care facilities with older adults with cognitive impairments that limited their ability to communicate. None of these caregivers had participated in phase I. Nurse characteristics: Average age: 49 years (±10.2) Experience as a nurse: 21.4 years (±13.0) Experience with patients reported on: 3.6 years (±2.8) 40 patients Average age: 83.2 years (±7.8) Gender: 11 males, 29 females Dementia severity: Present Functioning Questionnaire (PFQ): Average score: 44.6, (±5.3), indicating severe dementia. The subjects were “remembered patients” under the care of the nurse. Stage III 40 RN/Resident Dyads 40 nurses: Average age: 44 years Average years experience as a nurse: 19 years 40 patients:

Reviewed: 04/04 Revised: 06/08
4
Average age: 85 years Gender: 10 males, 30 females 33 patients with a diagnosis of dementia. 34 patients had a diagnosis associated with pain. Present Functioning Questionnaire (PFQ): Average score: 41, (±3.3). The subjects were “remembered patients” under the care of the nurse for at least six months and who experienced pain. Study 2 (Fuchs-Lacelle & Hadjistavropoulos, 2005) 50 nurses
Age: No information Gender: 70% female, 30% male
Patients (no information on number of patients assessed) Cognitive status: Present Functioning Questionnaire (PFQ) average score 37
(±5.7) indicating serious cognitive impairment. Study 3 (Zwakhalen, Hamers & Berger, 2006) 144 nursing home residents, with 128 dementia, 12 psychogeriatric patients. Age: mean 82.4 (SD-6.8), range 60-98 years Gender:78.1% female, 21.9% male Cognitive Status for dementia patients: MDS-CPS 47.7% severely impaired
(n-61), 28.1% moderately impaired (n-36), 21.9% mildly impaired (n=28) Diagnosis: 32% Alzheimer’s Disease; 18.8% vascular dementia, 9.4% other and 39.8% unknown.
Pain: based on MDS, 25% of psycho-geriatric patients experienced pain on daily basis; 42.2% of residents reported frequent pain (14.1% mild, 22.7% moderate, 5.5% unbearable).
16 somatically ill (control group for pain intensity scores) Age: 78.1 (SD 10.6) years Gender: 11 female, 5 male Nurses (n=12) Age: mean 34.3 (SD-9.6) years Gender: 10 female, 2 male Study 4 (Zwakhalen, Hamers, & Berger, 2007) 128 nursing home residents with dementia Age: mean 82.4 (SD-6.8), range 60-98 years Gender: 78.1% female; 21.9% male Cognitive status: same sample of dementia patients as in study 3. Study 5 (Zwakhalen,, Koopmans, Geels, Berger & Hamers, 2008) 117 residents from 3 Dutch nursing homes Age: mean 82.8 (SD=6.1), range 60-97 Gender:80% female, 20% male Cognitive status: MMSE mean score 5.7 (SD=6.8) suggesting severe impairment Study 6 (Fuchs-Lacelle, Hadjistavropoulos, & Lix, in press) 21 units within 12 long-term care facilities 181 patients randomly assigned to experimental (E) or control group (C) Age: mean 84.89 (SD=6.54) experimental and 8/39 (SD=7.00) control group Gender: E: 70.8% female; 29.2% male C: 88.1% female; 11.9% male

Reviewed: 04/04 Revised: 06/08
5
Cognitive Status: PFQ E=38.99 (SD=7.8) C=38.86 (SD=7.2) Caregivers/Nurses 61 RNs, LPNs and NAs Age: E= mean 44.1 (SD=11.4) C= mean 46.0 (SD=9.88) Gender: E: 100% female; 0 male C: 96.5% female; 3.5% male
-Panel Commentary The use of remembered patients may be appropriate for preliminary instrument testing. However, recall bias on the part of the nurses represents a threat to the validity of this study. The PACSLAC has been evaluated prospectively in NH settings with sample of patients with dementia. Methods for evaluating cognitive status are appropriate and indicate severe impairment in most studies. Age and gender representation is appropriate. There is no information in any of the studies regarding racial/ethnic diversity, except testing in Canadians and Dutch. Using a minimum requirement of 5 subjects per item for the purposes of this review, the sample sizes for testing the PACSLAC and the PACSLAC-D (Dutch Language) are small. Additionally, few subjects in the existing studies had moderate or severe pain impacting evaluation of the tool usefulness across the full range of scoring. Additional evaluation in larger English-speaking samples with increased diversity are needed.
Administration, Scoring, Feasibility Panel rating: 2 Revised: 2 Administration, Scoring, Feasibility
There are four subscales with a total of 60 items. Each item is scored on a dichotomous scale with one check for each item identified. Subscale scores are summed to arrive at a total score. It took most nurses less than five minutes to complete the PACSLAC. Study 2 (Fuchs-Lacelle & Hadjistavropoulos, 2005) Nurses completed the PACSLAC prospectively while working with the patient over an 8-hour shift, observing intermittently. No information on time to complete, perceptions of use, or feasibility reported. Study 3 (Zwakhalen, Hamers & Berger, 2006) Nurses’ rated clinical usefulness(on a 10-point scale) showing 75% preferring the PACSLAC to measure pain in elderly patients with dementia. Mean usefulness score for PACSLAC (7.0; SD 0.5) compared to the PAINAD 5.89 (SD 1.7). PACSLAC was reported to be user-friendly and not time-consuming by the participating nurses. Once used to the scale, they could assess patients within a few minutes. Study 5 (Zwakhalen., Koopmans, Geels, Berger & Hamers, 2008) 10 raters from 3 NHs received a short instruction session on use of the PACSLAC-D (Dutch Language) (30 minutes) and observed residents once for five randomly selected minutes during personal morning care (e.g. washing, showering). No raters had prior in-depth knowledge of the NH residents. Validity and reliability established suggest the tool is readily used with minimal training. Cut-offs for pain were established for the PACSLAC-D (Dutch Language) with 4 out of 24 considered to indicate presence of pain. With this cut-off, the scale sensitivity was 0.96 and specificity was 0.90. Procedure to establish cut-off included linear transformation using other observational scales with

Reviewed: 04/04 Revised: 06/08
6
known cut-offs, verification of cut-off with empirical data and determining sensitivity and specificity with sample of the study. Study 6 (Fuchs-Lacelle, Hadjistavropoulos & Lix, in press) The study provides data regarding the impact of PACSLAC use on patient outcomes. Regular use of the PACSLAC improved pain management practices over time as reflected in increased usage of PRN analgesic medications and a decrease in observable behaviors as pain interventions increased. Nurses who used the PACSLAC reported decreased distress and burnout over time. Also preliminary normative data suggest that scores greater than 12 (out of 60) represent high levels of pain for patients in LTCF. Scores between 0-5 are indicative of usual pain.
-Panel Commentary Simple instructions on how to administer and score the tool are provided on the tool form. Scoring procedures are clear, and preliminary cut-offs for determining pain presence are determined for the PACSLAC. Although the original PACSLAC includes 60 items, the tool requires a limited amount of time to administer, indicating that the tool is potentially useful in everyday clinical practice. Testing of the PACSLAC-D (Dutch Language), the shorter 24 item scale, suggests the tool is user friendly requiring a short time for training (30 minutes), has an established cut-off to facilitate score interpretation, and can be completed in a few minutes. Preliminary evidence of clinical utility and normative data for scoring is provided, although further validation with larger and more diverse is needed.
Reliability Panel rating: 1 Revised: 2 Internal consistency Study 1 (Fuchs-Lacelle & Hadjistavropoulos, 2004)
Stage II In phase II of tool development the PACSLAC observations were made by professional caregivers (see sample characteristics above). Following deletion of two items phase II and subscale revisions the following subscale internal consistency reliabilities were reported: Total tool (63 items): α=.92 Subscales: • Facial Reactions: α=.80 • Social/Personality/Mood: α=.82 • Activity/Body Movement: α=.84 • Physiological indicators/ Eating and sleeping changes/ Vocal behaviors α=.74 Stage III Internal consistency was conducted in a sample of 40 RN/Resident dyads (see sample specifications above). The 40 RNs rated 40 residents on the PACSLAC retrospectively based on four remembered events: two painful events, one distressing (but not pain-related) and one calm event. Internal consistency based on average for the two pain events was α=.85. Internal consistency for subscales: • Facial Reactions: α=.56 • Social/Personality/Mood: α=.85 • Activity/Body Movement: α=.55 • Physiological indicators/ Eating and sleeping changes/ Vocal behaviors α=.59

Reviewed: 04/04 Revised: 06/08
7
Study 3 (Zwakhalen, Hamers & Berger, 2006) Internal consistencies reported for Dutch PACSLAC across rating by nurses and rater at T and, T3. Ranges for Cronbach’s alpha’s were as follows: Total scale: 0.80-0.84 Facial Expressions subscale: 0.57-0.73 Activity/Body Movement subscale: 0.40-0.57 Social/Personality subscale: 0.65-0.76 Physiological/Eating/Sleeping changes/Vocal behaviors: 0.20-0.43 Study 4 (Zwakhalen, Hamers, & Berger, 2007) Internal consistency evaluated for the revised 24-item PACSLAC-D (Dutch Language). Alpha for total scale with 24 items=0.86 at T2 and 0.82 at T3. Cronbach’s alpha for three subscales were high, ranging from 0.72 to 0.82.
Interrater reliability Study 3 (Zwakhalen, Hamers & Berger, 2006) ICCs between rater 1 and the nurses for the PACSLAC Total scale r’s 0.93-0.96; subscales 0.77 to 0.95. The correlations could be lower depending on the pair of raters compared. Study 4 (Zwakhalen, Hamers, & Berger, 2007) No interrater reliability reported for the PACSLAC-D (Dutch Language) (24 item scale) Study 5 (Zwakhalen., Koopmans, Geels, Berger & Hamers, 2008) Fifteen residents were assessed by two raters simultaneously during morning care. ICC for total scale= 0.89; Facial expressions= -.89, Resistance/Defense=0.76, Social-Emotional aspects/mood= 0.56 Study 6 (Fuchs-Lacelle, Hadjistavropoulos & Lix, in press) Interrater reliability established between two independent, trained RA observers. Kappa coefficient=0.61, degree of agreement=0.97
Test-retest reliability Study 3 (Zwakhalen, Hamers & Berger, 2006) Intrarater reliability assessed by comparing scores on PACSLAC allocated by rater 1 at bedside with those rescored for the same time based on video recordings (n=29, no time interval given between testing points). Cronbach’s alpha=0.86 overall with subscale r’s from 0.72 to 0.92
-Panel commentary The PACSLAC has good internal consistency, interrater reliability and intrarater reliability. The PACSLAC-D (Dutch Language) also has good reliability estimates established in preliminary testing. Additional testing in diverse samples, including those with greater range of pain severity, is recommended.
Validity: Criterion or construct Panel rating: 2 Revised: 2 Construct validity/ Criterion related validity
Study 1 (Fuchs-Lacelle & Hadjistavropoulos, 2004) Discriminant validity Discriminant validity was based on retrospective recall of painful events by the nurse, two pain events with very clear cause, one distressing (but not pain-related) event, one calm event (no signs of distress). Results: Pain Event I > Distress Event (p< .001) Pain Event I > Calm Event (p<.001) Pain Event II > Distress Event (p<.001)

Reviewed: 04/04 Revised: 06/08
8
Pain Event II > Calm Event (p<.001) Distress Event > Calm Event (p<.001). Conclusion: The total PACSLAC score is able to discriminate among painful, calm, and non-pain related distress events F (3,117) = 108.1 (p<.001). Subscales: Facial Expressions, Activity/Rocking Movement and Physiological indicators/Eating and sleeping changes/Vocal behaviors discriminated as follows: Pain > Distress > Calm (p<.001). Subscale Social/Personality/Mood discriminated between pain and calm events but not between pain and the distress events. Three additional items were deleted during this phase because they occurred with greater frequency during calm events. Criterion related validity In Study 1, Global Pain Intensity Ratings of the nurses’ perception of the patients pain and PACSLAC total scores were moderately correlated: PE1: r=.39 (p<.05) PE2: r=.54 (p<.001). Study 2 (Fuchs-Lacelle & Hadjistavropoulos, 2005) This report compared nursing observations of patients without known pain to earlier retrospective ratings of pain events and distress event. MANOVA used to compare four subscale scores from observations after a nursing shift with the two Pain Events and the Distress Event.
• Total scores for both the Pain Events were significantly higher than for the total scores based on observation (of patients with no known pain problems) during a nursing work shift (t(80) > 4.0, p. < 0.001).
• All subscales were significantly higher for Pain Event I than for the subscale scores obtained after a nursing shift (F(80) > 9.46, p < 0.05).
• Subscale scores for Activity/Body Movements, Social/Personality/Mood and Other were higher for Pain Event II than for nursing shift (F(80) > 9.43, p > .05).
• Total scores and the Activity/Body Movements and other subscale scores did not differ between the pain assessment completed after a nursing shift and the assessment based on the Distress Event.
Study 3 (Zwakhalen, Hamers & Berger, 2006) Pain and non-pain groups (based on self-report on VRS) were identified and PACSLAC ability to detect increasing pain with increased behaviors was evaluated. Construct validity confirmed with upward trend in scores comparing mean PACSLAC scores at rest (2.6), at injection, T1 (5.5) and at pain inducing moment T2 (9.6). Congruent validity also established between the PACSLAC and PAINAD (r=0.85). Low correlations noted between the PACLSLAC and DOLOPLUS-2 (r=0.29 ) suggesting these two tools are not measuring the same construct. Study 5 (Zwakhalen., Koopmans, Geels, Berger & Hamers, 2008) Using data from Study 4, cut-offs for determining pain presence were identified and used in a prospective evaluation of pain prevalence in nursing

Reviewed: 04/04 Revised: 06/08
9
homes. The findings are consistent with other studies but use an observational tool for determining pain presence. The cut-off was verified using data from Study 3 to establish sensitivity and specificity of the tool. PACSLAC-D (Dutch Language) sensitivity is 0.96 and specificity is 0.90 based on a > 4 score.
-Panel commentary Retrospective recall of patients and their pain-related conditions in initial testing carries potential for bias but further testing supports tool validity. Further evaluation provides support for congruent and discriminant validity of the PACSLAC, as well as preliminary support for sensitivity and specificity of the shorter PACSLAC-D (Dutch Language). Additional study in larger samples, with samples experiencing greater pain severity, and to evaluate tool sensitivity are needed.
Summary of panel evaluation of pain assessment tool The PACSLAC is a potentially clinically useful behavior checklist that appears simple to use for assessing and monitoring changes in persons with dementia and diverse presentations of pain-related behavior. The tool is comprehensive and addresses pertinent indicators noted in the literature and AGS Guideline. Prospective evaluation has added to the tool’s reliability and validity, as well as factor analysis to determine the most efficient and useful indicator set for clinical use (PACSLAC-D (Dutch Language)). However, the revised PACSLAC-D (Dutch Language) no longer contains items that are based on knowledge of the patient and this may under-recognize pain in patients who demonstrate less obvious indicators such as changes in activity or behavior. Because of this major revision in the tool, the PACSLAC and PACSLAC-D (Dutch Language) psychometric evaluations should be considered independently. Preliminary normative data and cut-offs are provided but require further validation in larger, more diverse samples. Additional factor analysis in English-speaking samples, other diverse samples, and in patients with increased levels of pain severity is needed, as is determination of tool sensitivity in detecting treatment effects. Source of evidence Fuchs-Lacelle, S. & Hadjistavropoulos, T. (2004). Development and preliminary validation of the Pain
Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC). Pain Management Nursing, 5(2).
Fuchs-Lacelle, S.& Hadjistavropoulos, T. (2005). A checklist for pain assessment in LTC. PACSLAC:
Pain Assessment Checklist for Seniors with Limited Ability to Communicate. Canadian Nursing Home, 16(4), 4-7.
Zwakhalen, S., Hamers, J. & Berger, M. (2006). The psychometric quality and clinical usefulness of three
pain assessment tools for elderly people dementia. Pain, 126(1-3), 210-220. Zwakhalen, S., Hamers, J. & Berger, M. (2007). Improving the clinical usefulness of a behavioral pain
scale for older people with dementia. Journal of Advanced Nursing, 58(5), 493-502. Zwakhalen, S., Koopmans, R., Geels, P., Berger, M. & Hamers, J. (2008) The prevalence of pain in
nursing home residents with dementia measured using an observational pain scale. European Journal of Pain, xx, xxxx. (in press).
Fuchs-Lacelle, S., Hadjistavropolous, T. & Lix, L. (in press). Pain assessment as intervention: A study of
older adults with severe dementia. Clinical Journal of Pain, xx ,xxx. (in press) Key to panel rating 3= Available evidence is strong 2= Available evidence supports need for further testing 1= Available evidence is insufficient and/or tool revisions are needed 0= Evidence is absent

Reviewed: 04/04 Revised: 06/08
10
Contact address for PACSLAC: The PACSLAC is copyrighted by Shannon Fuchs-Lacelle and Thomas Hadjistavropoulos and may not be reproduced without permission. For permission to reproduce the PACSLAC please contact Thomas Hadjistavropoulos, PhD [email protected] Contact address for PACSLAC-D (Dutch Language): Sandra Zwakhalen, PhD Email: [email protected] Evaluation completed by: K. Herr, S. Decker, K. Bjoro, The University of Iowa. Revision 06/08 by: K. Herr, H. Bursch, B. Black, The University of Iowa Contact information: [email protected]

Indicate with a checkmark, which of the items on the
PACSLAC occurred during the period of interest.
Scoring the sub-scales is derived by counting the
checkmarks in each column. To generate a total pain
sum all sub-scale totals.
Facial Expression
Present
Grimacing
Sad look
Tighter Face
Dirty Look
Change in Eyes (Squinting, dull, bright, increased eye movements)
Frowning
Pain Expression
Grim Face
Clenching Teeth
Wincing
Open Mouth
Creasing Forehead
Screwing Up Nose
Activity/Body Movement
Present
Fidgeting
Pulling Away
Flinching
Restless
Pacing
Wandering
Trying to Leave
Refusing to Move
Thrashing
Decreased Activity
Refusing Medications
Moving Slow
Impulsive Behaviours (Repeat Movements)
Uncooperative/Resistance to care
Guarding Sore Area
Touching/Holding Sore Area
Limping
Clenching Fist
Going into Fetal Position
Stiff/Rigid
Social/Personality/Mood
Present
Physical Aggression (e.g. pushing people and/or objects, scratching others, hitting others, striking, kicking).
Verbal Aggression
Not Wanting to be Touched
Not Allowing People Near
Angry/Mad
Throwing Things
Increased Confusion
Anxious
Upset
Agitated
Cranky/Irritable
Frustrated
Other (Physiological changes/Eating
Sleeping Changes/Vocal Behaviors)
Present
Pale Face
Flushed, Red Face
Teary Eyed
Sweating
Shaking/Trembling
Cold Clammy
Changes in Sleep Routine (Please circle 1 or 2) 1) Decreased Sleep ------------------------------------ 2) Increased Sleep During the Day
Changes in Appetite (Please circle 1 or 2) 1) Decreased Appetite
----------------------------------- 2) Increased Appetite
Screaming/Yelling
Calling Out (i.e. for help)
Crying
A Specific Sound of Vocalization For pain “ow,” “ouch”
Moaning and groaning
Mumbling
Grunting
Total Checklist Score
Pain Assessment Checklist for Seniors with Limited Ability to Communicate
(PACSLAC)

The PACSLAC may not be reproduced or translated without permission. For permission to reproduce
the PACSLAC contact the copyright holders ([email protected]).
THE DEVELOPERS OF THE PACSLAC SPECIFICALLY DISCLAIM ANY AND ALL LIABILITY ARISING DIRECTLY OR INDIRECTLY FOR USE OR APPLICATION OF THE PACSLAC. USE OF THE PACSLAC MAY NOT BE APPROPRIATE FOR SOME PATIENTS AND THE PACSLAC IS NOT A SUBSTITUTE FOR A THOROUGH ASSESSMENT OF THE PATIENT BY A QUALIFIED HEALTH PROFESSIONAL.
References
Fuchs-Lacelle, S. & Hadjistavropoulos, T. (2004). Development and preliminary validation of the pain
assessment checklist for seniors with limited ability to communicate (PACSLAC). Pain Management
Nursing, 5(1), 37-49.

Completed 04/04 Revised 06/08
1
The Pain Assessment in Advanced Dementia Scale (PAINAD) Brief The Pain Assessment in Advanced Dementia (PAINAD) Scale was developed to provide a clinically relevant and easy to use pain assessment tool for individuals with advanced dementia. The tool is an adaptation of the DS-DAT and the FLACC and includes five items: Breathing, Negative vocalization, Facial expression, Body language, and Consolability. Each item is leveled on a three point scale (0-2) for severity.
The tool covers only 3 of 6 categories of non-verbal pain behaviors in the AGS Persistent Pain Guidelines: facial expression, verbalizations/vocalizations and body language. Although these are the most common pain indicators, the more subtle pain indicators such as changes in activity patterns or routines, mental status changes and changes in interpersonal interactions are not included. The tool is based on the assumption that caregivers can reliably rate the intensity of elders’ pain, an assumption for which there is conflicting evidence in current literature. Subsequent studies have demonstrated that the tool can detect presence of pain and appears to identify higher and lower levels of pain in an individual. It may not detect pain in patients that demonstrate pain with behaviors other than those included in the tool.
Method of administration is described and a guide with definitions of items is provided. Scoring procedures are clearly described, although no guide to interpretation of the tool score is provided. Subjects in the pilot study were observed for 5 minutes, but a clear recommendation for length of observation is not provided. The tool appears simple to understand and appears to be easy to use with limited training. Subsequent studies have demonstrated strong clinical utility with administration possible within 1-3 minutes, limited training required (minimum of 15 minutes to 2 hours), and reported ease of use by raters. Initial testing of the PAINAD was conducted in two studies both conducted in long term care VA Dementia special care units. Study 1 sample involved 19 severely demented veterans, all male Caucasians, with an average age of 78.1 years (±5), range 66-85 years. Study 2 was a QI study which involved charts of 25 patients. However, no demographic data or disease characteristics were available. Thus, limited sample size and demographic details of subjects limit generalizability of study results.
The PAINAD has received considerable attention internationally and 7 additional studies have been conducted that provide additional psychometric data on this tool. The PAINAD was translated and tested in Singapore, Belgium, Italy, Netherlands, and Germany, as well as two studies in the US. The majority of additional study has been conducted in NHs, however testing has also occurred in an acute care hospital and geriatric rehabilitation center. These studies have added data with female subjects, a gap in the development studies. There is still limited data on individuals from different races, although cultural variation has been tested across countries. All studies have included individuals with dementia. Age of subjects across studies is appropriate with mean age of samples ranging from 78 to 88 years. Reliability. • Internal consistency was evaluated based on a pooled sample of study 1 and study 2.
Cronbachs alpha from three situations ranged from .50 to .65, which is moderate

Completed 04/04 Revised 06/08
2
given a new tool with only 5 items. Moreover, the approach of combining research and QI data to establish reliability is not methodologically sound. Follow-up studies have demonstrated good internal consistency with correlations ranging from 0.69 to 0.85. However, the item of breathing is low.
• Interrater reliability is reported for 19 subjects with pairs of simultaneous observations by two independent raters. Pearson’s correlation coefficient: during pleasant activity: r=.97 and during unpleasant activity: r=.82. Interrater reliability reports across 5 studies indicate strong reliability. Pearson’s r ranges from 0.75 to 0.97 with most reports over 0.80.
• Test-retest reliability in three follow-up studies is strong with r’s ranging from 0.88 to 0.90.
Validity • Factor structure analysis for combined PAINAD data: 1 factor=50.1% variance
(eigenvalue 2.51), 1 minor factor explained 20.6% (eigenvalue 1.03). Further study of the PAINAD provides support for construct validity. A single factor was again isolated with greater distribution of pain. However, the number of patients with behaviors reflecting the high end of the scale scoring is still small.
• PAINAD was compared to the Pain VAS, DS-DAT, Discomfort VAS. Correlation coefficients at rest were r=.75, r=.76, r=.76, respectively. PAINAD was compared to the Pain-VAS during presumed pleasant conditions: r=.87-.95 and during presumed unpleasant conditions: r=.82-.91. Further study of the PAINAD provides support for good concurrent validity with across tool correlations ranging from 0.65 to 095 with the exception of comparison of the PAINAD to self report of pain (0.30).
• Discriminant validity of the PAINAD was established in study 1 with subjects (n=19) observed during a pleasant activity, during rest or time of no activity, during caregiving that might be unpleasant with mean scores: 1.0±1.3, 1.3±1.3 and 3.1±1.7 respectively.
• Using QI data it was demonstrated that the PAINAD was able to capture pain and change in pain. Average PAINAD scores prior to prn medication (6.7±1.8) and 30 minutes after pain medication (1.8±2.2) were significant (t24=9.6, p<.001).
• Further study of the PAINAD provides some support for construct, predictive, concurrent and discriminant validity. The most recent study that examines tool sensitivity in detecting change from treatment raises questions regarding the tools ability to do so with persons with severe dementia. Further study is needed.
• Although studies have raised concern regarding the items of breathing and consolability, authors urge maintaining the current items structure to allow international comparisons. Because removal of items did not demonstrate improved internal consistency, this recommendation seems supportable.
Summary
The PAINAD was developed as a shorter, easier observation tool for assessing pain in nonverbal elders. The tool items included are not comprehensive, but subsequent studies have provided data suggesting the tool does detect pain and changing levels of behavior (not pain) intensity. Because of the small number of items that are used to detect pain, the ability of the PAINAD to detect pain in those with less obvious changes

Completed 04/04 Revised 06/08
3
in behavior (e.g. mental status changes, aggressive behavior, changes in activities) may still be compromised.
Although clinicians desire to have a tool that provides a 1-10 score similar to the 1-10 NRS commonly used as the gold standard in verbal patients, the soundness of establishing a rating scale with pain severity scoring of behaviors has not been substantiated in the literature. Completed studies suggest the tool could be used to show higher and lower levels of pain, but there is no data to attach level of pain severity to the number obtained with the tool.
Tool reliability is good for interrater reliability, but internal consistency is only moderate and stability has not been demonstrated. Tool has good reliability in all areas.
Some conceptual and methodological issues have been identified with the development and testing of the PAINAD. However, the positive findings in detection of changes in pain behavior following intervention in the QI study reported suggests additional study in controlled circumstances is warranted. Follow-up studies have continued to document ability to detect pain and differentiate pain and no pain groups. However, further study of tool sensitivity to detect change in behavior in response to treatment is needed.
Source of evidence Warden, V., Hurley, A.C., Volicer, L. (2003). Development and psychometric evaluation
of the Pain Assessment in Advanced Dementia (PAINAD) Scale. Journal of the American Medical Directors, Jan/Feb, 9-15.
Lane, P., Kuntupis, M., MacDonald, S., McCarthy, P., Panke, J., Warden, V., Volicer, L.
(2003). A pain assessment tool for people with advanced Alzheimer’s and other progressive dementias. Home Healthcare Nurse, 21(1), 32-37.
Costardi, D., Rozzini, L., Costanzi, C., Ghianda, D., Franzoni, S., Padovani, A. &
Trabucchi, M. (2006). The Italian version of the pain assessment in advanced dementia (PAINAD) scale. Archives of Gerontology and Geriatrics, 44(2), 175-180.
DeWaters, T., Faut-Callahan, M., McCann, J. J., Paice, J. A., Fogg, L., Hollinger-Smith,
L., et al. (2008). Comparison of self-reported pain and the PAINAD scale in hospitalized cognitively impaired and intact older adults after hip fracture surgery. Orthopaedic Nursing / National Association of Orthopaedic Nurses, 27(1), 21-28.
Hutchison, R., Tucker, W., Kim, S. & Gilder, R. (2006). Evaluation of a behavioral
assessment tool for the individual unable to self-report pain. American Journal of Hospice and Palliative Medicine, 23(4), 328-331.
Leong, I., Chong, M. & Gibson, S. (2006). The use of a self-reported pain measure, a
nurse-reported pain measure and the PAINAD in nursing home residents with moderate and severe dementia: a validation study. Age and Ageing, 35, 252-256.

Completed 04/04 Revised 06/08
4
Schuler, M., Becker, S., Kaspar, R., Nikolaus, T., Kruse, A. & Basler, H. (2007).
Psychometric properties of the German “Pain Assesssment in Advanced Dementia” (PAINAD-G) in Nursing Home residents. American Medical Directors Association, July, 388-395.
Van Iersel, T., Timmerman, D. & Mullie, A. (2006). Introduction of a pain scale for
palliative care patients with cognitive impairment. International Study of Palliative Nursing, 12(2), 54-59.
Zwakhalen, S., Hamers, I. & Berger, M. (2006). The psychometric quality and clinical
usefulness of three pain assessment tools for elderly people with dementia. Pain, 126, 210-220.
Cohen-Mansfield, J. & Lipson, S. (2008). The utility of pain assessment for analgesic
use in persons with dementia. Pain, 134(1-2), 16-23. Contact information: Victoria Warden, RN GRECC (182B) E. N. Rogers Memorial Veterans Hospital, 200 Springs Road, Bedford, MA 01730. E-mail: [email protected]. This summary was completed by: K. Herr, S. Decker, K. Bjoro, University of Iowa (2004). Revised by: K. Herr, H. Bursch and B. Black, The University of Iowa (2008).
Contact information: [email protected]

Reviewed 04/04 Revised 06/08
1
Tool: The Assessment in Advanced Dementia (PAINAD) Tool developer: Warden V., Hurley, A.C., Volicer, L. Country of origin: USA Reviewed: 04/04 Revised: 06/08 Conceptualization Panel rating: 1 Revised: 2 Purpose The Pain Assessment in Advanced Dementia (PAINAD) Scale was developed
to provide a clinically relevant and easy to use observational pain assessment tool for individuals with advanced dementia. The aim of the tool developers was to “develop a tool for measuring pain in non-communicative individuals that would be simple to administer and had a score from 0 to 10.”
Conceptual basis Pain is the concept being measured. The tool attempts to measure pain severity.
Item Generation Tool items • Breathing • Negative vocalization • Facial expression • Body language • Consolability Each item is leveled on a three point scale for severity using behavioral descriptors. Item generation PAINAD is based on selected items from the DS-DAT and the FLACC. The FLACC was developed for measuring postoperative pain in young children. The article provides a review of literature and existing pain tools. However, little information on item generation is available.
Content Validity The content validity of the PAINAD was not established by independent content experts. However, subsequent evaluation studies have demonstrated that the tool measures pain behavior.
-Panel Commentary The measurement of pain severity has not been substantiated in the research on pain in elders with dementia. Although establishing a 0-10 point scale to represent pain severity may be clinically desirable, the validity of determining level of pain severity in a population of non-verbal elders with diverse presentations of possible pain related behaviors has not been established. The tool covers 3 of 6 categories of non-verbal pain behaviors in the AGS Persistent Pain Guidelines: Facial expression, verbalizations/vocalizations and body language. Three items not addressed are: Changes in activity patterns or routines, Mental status changes, Changes in interpersonal interactions. The FLACC indicators have not been demonstrated appropriate for elders with dementia and the tool item generation is narrow in focus. With only 5 items used to assess pain, the most salient indicators should be included to ensure greatest likelihood of detecting pain. Of the five pain-related behavior categories in the PAINAD, two are not most salient (breathing and consolability), potentially minimizing the likelihood of detecting pain. However, subsequent studies have demonstrated that the tool can detect

Reviewed 04/04 Revised 06/08
2
presence of pain. Scoring of the breathing indicator seems unrelated to pain severity. Breathing does not seem to be a key indicator of pain. However, the tool developers argue that one of the known areas believed to cause negative feelings for persons with dementia is the aversive symptoms associated with intercurrent respiratory infections and that pneumonia is a the proximal cause of death for many demented persons. Thus, they included the breathing item. We perceive consolablity as a response to an intervention, not a behavioral manifestation of pain. However, the relationship between consolability and pain may be an area for future research in this population. The validity for the scoring of items according to pain severity or separation of behaviors within each major category is not established, (eg. Breathing is scored: Normal=0, Occasional labored breathing/Short period of hyperventilation =1, Noisy labored breathing/Long period of hyperventilation/Cheyne-Stokes respirations=2). However the tool appears to identify higher and lower levels of pain in an individual. Although the PAINAD does not adequately sample the content area of behavioral indicators for pain in elders with dementia who are unable to communicate, studies have demonstrated that the tool measures pain. It may not detect pain in patients that demonstrate pain with behaviors other than those included in the tool.
Subjects Panel rating: 1 Revised: 3 Subjects Study 1 (Warden et al., 2003)
Long term care VA Dementia Special Care Unit (96 patient unit). Subjects: 19 veterans, all Caucasian Average age: 78.1 years (±5), Range 66-85 years Gender: Female: 0, Male: 100% The subjects had dementia for 8.7 years on average (±4.7), Range 1-20. Length of time in residence: 16.5 months average (±13.5), Range 1-50 months. MMSE: 2.8 ±4.5, Range 0-16. Bedford Alzheimer Nursing Severity Subscale: average 16.4 ±4.4, Range 9-23. Study 2 Lane et al., 2003) QI study – charts of 25 patients were used. No demographic data or disease characteristics are available for these subjects. Study 3 (Costardi et al., 2006) Geriatric Evaluation and Rehabilitation Unit, Northern Italy (n=1) Subjects: 20 with chronic pain and dementia Average age: 82 (SD=5.9) years; Range: 73-93 years Gender: Female 80% Male: 20% MMSE: 16.4 + 3.8, range 10-22 Study 4 (Hutchison et al., 2006) Acute care hospital, US (n=1) Subjects: 53 control and 27 PAINAD with acute postop pain

Reviewed 04/04 Revised 06/08
3
Average Age: 85.2 control and 88 PAINAD Gender: 85% female in control and 78% female in PAINAD MMSE: control: 0% with less than 25 in control and 100% diagnosed dementia PAINAD group: 23.6% with MMSE less than 25 and 76.4% diagnosed dementia Study 5 (Leong et al., 2006) Nursing Home in Singapore (n=1) Subjects: 88 with moderate and severe dementia Average Age: 79.6 (SD=8.3) Gender: 61.4% female; 38.6% male MMSE: Not reported Study 6 (van Iersel et al., 2006) Palliative care patients in NH setting (n=17) Patients who could not express pain Subjects: 157 patients Average Age: 85 years; range 22-100 Gender: 78% female; 22% male MMSE: Not reported Study 7 (Zwakhalen et al., 2006) Nursing Homes in Netherlands (n=3) Subjects: 128 patients with dementia; both acute and chronic pain Average Age: 82.4 (SD=6.8) years; range 60-96 Gender: 78.1% female; 21.9% male MMSE: Not reported; Cognitive Performance Scale: 21.9% mild, 28.1% moderate, 47.7% severe Study 8 (Schuler et al., 2007) Nursing Homes in Germany (n=8) Subjects: 99 residents with dementia Average Age: 84.9 (SD=7.5) Gender: 80% female; 20% male MMSE: Mean 12.1 (SD=9.7) Study 9 (Cohen-Mansfield & Lipson, 2008) Nursing homes in US (n=4) Subjects: 121 with dementia Average Age: 88 (range 59-101) Gender: 81.8% female MMSE: Mean 6.3 (range 0-20) Study 10 (DeWaters et al., 2008) Orthopedic unit in US hospital (n=1) Subjects: 25 verbal older persons, includes 13 cognitively intact and 12 cognitively impaired persons Average age: 81.24 (range 65-95) Gender: 84% female MMSE: 20.52 (range 9-30) plus diagnosis of dementia or confusion
-Panel Commentary The PAINAD has received considerable attention internationally and 7 additional studies have been conducted that provide additional psychometric data on this tool. The PAINAD was translated and tested in Singapore, Belgium, Italy, Netherlands, and Germany, as well as two studies in the US. The majority of additional study has been conducted in NHs, however testing

Reviewed 04/04 Revised 06/08
4
has also occurred in acute care hospitals and geriatric rehabilitation center. These studies have added data with female subjects, a gap in the development studies. There is still limited data on individuals from different races, although cultural variation has been tested across countries. All studies have included individuals with dementia. Age of subjects across studies is appropriate with mean age of samples ranging from 78 to 88 years.
Administration, Scoring, Feasibility Panel rating: 2 Revised: 3 Administration, Scoring, Feasibility
In the pilot test, subjects were observed for 5 minutes prior to scoring. Definitions for each item are provided. The scoring system is based on a 3 point scale: 0, 1, 2. Total scores range from 0 to 10 points, a maximum of 2 points per category. The tool developers report that because they wanted the 10 point scale, they determined that there would be a 3 point rating option for each item, and that in general, 0=none, 1=small or some or occasionally, and 2=large or a more intense negative behavior making that item operational. Specific definitions for each behavior are provided. No interpretation of the score is provided. A two hour training program was developed including video training tapes. Study 3 (Costardi et al., 2006) Comment easily administered with appropriate training Study 4 (Hutchison et al., 2006) Raters received 15 minute in-service instruction. Clinicians reported easy to administer, requiring less than 1 minute of time. Study 5 (Leong et al., 2006) No comments provided. Study 6 (van Iersel et al., 2006) Care providers (n=17): 80% agreed or had no opinion (20% disagreed) that the PAINAD was a good measure to judge pain and 76% agreed or had no opinion that PAINAD was easy to use (28% disagreed). Breathing and consolability indicators were less good indicators (<60%) Study 7 (Zwakhalen et al., 2006) On scale of 0-10 for clinical usefulness, nurses (12 nurses in 3 NHs) rated the PAINAD 5.89 (SD 1.7). 75% preferred the PACSLAC. The PAINAD was considered user-friendly and not time-consuming by participating nurses requiring a few minutes to assess. Study 8 (Schuler et al., 2007) Used a 2 minute period to observe routine nursing activities and complete rating. No comments regarding nurse perceptions/rating of usability. Study 9 (Cohen-Mansfield & Lipson, 2008) Used a 5 minute observation period. No comments regarding nurse perceptions/ratings of usability. Study 10 (DeWaters et al., 2008) No comments re. clinical feasibility
-Panel Commentary Method of administration is described and a guide with definitions of items is provided.

Reviewed 04/04 Revised 06/08
5
Scoring procedures are clearly described. No guide to interpretation of tool score is provided. The tool developers argue that clinicians are familiar with a 0-10 scale and that it is assumed that 0 means no observed pain and 10 means a high level of observed pain that should be treated. However, this assumes that judging severity of pain represented by behavioral presentation in non-verbal elders is valid—which has not been substantiated in the literature. Subsequent studies have demonstrated strong clinical utility with administration possible within 1-3 minutes, limited training required (minimum of 15 minutes to 2 hours), and reported ease of use by raters.
Reliability Panel rating: 1 Revised: 3 Internal consistency Study 1 & 2 (Warden et al, 2003; Lane et al., 2003)
Internal consistency was evaluated based on data from a sample of 19 veterans and QI data from 25 residents. (For sample characteristics see subjects above). Raters were 4 professional nurses with experience on dementia special care units and a master’s level social work intern. Three observations of subjects for 5 minutes were made under different conditions as indicated below. To achieve 10 participants per item, the research and QI data were pooled and examined for internal consistency. Observation 1: During rest or no activity: Cronbach’s alpha=.50 Observation 2: Pleasant activity: movement could lead to pain: Cronbach’s alpha=.59, .63 Observation 3: Potentially unpleasant caregiving activity (eg. Transfers, bathing, toileting) Cronbach’s alpha=.50, .67. Additional data on internal consistency has been reported by 3 studies. Study 3 (Costardi et al., 2006) Internal consistency=0.74 Study 7 (Zwakhalen et al., 2006) Cronbach’s alpha 0.69-0.74; Breathing scored consistently low -.51 to .12 Study 8 (Schuler et al., 2007) Cronbach’s alpha= 0.85 Study 10 (DeWaters et al., 2008) Cronbach’s alpha for combined group 0.852 Cronbach’s alpha for cognitively intact group =0.846 Cronbach’s alpha for cognitively impaired group =0.847
Interrater reliability Study 1 (Warden et al., 2003) Interrater reliability is reported for 19 subjects by pairs of simultaneous observations by two independent raters. Pearson’s correlation coefficient: • During pleasant activity r=.97 • During unpleasant activity r=.82.
Additional data on inter-rater reliability has been reported by 4 studies Study 3 (Costardi et al., 2006) Two raters same day=0.87 (p=.001)

Reviewed 04/04 Revised 06/08
6
Study 7 (Zwakhalen et al., 2006) Inter-rater reliabilities reported: 0.75 (rest), 0.85 (after flu vaccine) and 0.81 (patient-specific moment of potential pain). Agreement less strong at rest than during potential painful activity. Study 8 (Schuler et al., 2007) Two nurses morning and evening assessments: reliability= 0.80 (p=.001) Study 9 (Cohen-Mansfield & Lipson, 2008) Inter-rater agreement across three RAs: ICC=0.92 Study 10 (DeWaters et al., 2008) Interrater reliability between 2 master’s prepared nurse RAs for ten video vignette ratings: ICC= 0.98
Test-retest reliability No test-retest reliability is reported. Data on test-retest and/or intra-rater reliability reported in 3 studies. Study 3 (Costardi et al., 2006) One expert rater at baseline and after 15 days=0.88 (p=.045) Study 7 (Zwakhalen et al., 2006) Intra-rater reliability=0.89; comparing rating in person with rating on video Study 8 (Schuler et al., 2007) One nurses morning and evening assessments; r=0.90 (p<.001)
-Panel commentary Internal consistency Follow-up studies have demonstrated good internal consistency with correlations ranging from 0.69 to 0.85. However, the item of breathing is low. Interrater reliability Interrater reliability reports across 5 studies indicate strong reliability. Pearson’s r ranges from 0.75 to 0.97 with most reports over 0.80 and strong ICCs. Test-retest reliability Three studies report strong test-retest reliability with r’s ranging from 0.88 to 0.90.
Validity: Criterion or construct Panel rating: 2 Revised: 2 Construct validity/ Criterion related validity
Construct validity Factor structure analysis for combined PAINAD data for study 1 and study 2 1 factor = 50.1% variance (eigenvalue 2.51), 1 minor factor (breathing alone) explained another 20.6% (eigenvalue 1.03). QI data: one factor solution: 61% variance (eigenvalue 3.05). Concurrent validity The PAINAD was compared to the DS-DAT with VAS components included. Concurrent validity was reported based on associations from observations of pain and discomfort at rest. PAINAD & Pain VAS: r=.75, p<.001 PAINAD & DS-DAT: r=.76, p<.001 PAINAD & DS-VAS: r=.76, p<.001

Reviewed 04/04 Revised 06/08
7
Concurrent validity was reported based on associations from observations of pain during 1) presumed pleasant conditions for 18 veterans and 2) presumed unpleasant conditions for 19 veterans (p=.001 for all correlations). 1) Presumed pleasant conditions (n=18) PAINAD (1) & Pain-VAS (1) r=.92 PAINAD (1) & Pain-VAS (2) r=.89 Pain-VAS (1) & PAINAD (2) r=.93 PAINAD (2) & Pain-VAS (2) r=.95 2) Presumed unpleasant conditions (n=19) PAINAD (1) & Pain VAS (1) r=.82 PAINAD (1) & Pain VAS (2) r=.90 Pain-VAS (1) & PAINAD (2) r=.90 PAINAD (2) & Pain-VAS (2) r=.91 Discriminant validity Study 1 (For sample characteristics see subjects above.) Subjects (n=19) were observed 3 times to establish expected pain with significant outcomes (F1,17 = 10.93, P<0.001) Mean score 1. During rest or time of no activity: 1.3±1.3 2. During a pleasant activity: 1.0±1.3 3. During caregiving that might be unpleasant: 3.1±1.7 Study 2 (For sample characteristics see subjects above.) Change in PAINAD before and after administration of prn medications was reported based on quality improvement data from chart audit of 25 DAT residents. The PAINAD was administered prior to prn medication and 30 minutes after pain medication with significant results (T(24)=9.6, p<.001): Prior to prn medication 30 minutes after medication 6.7± 1.8 1.8 ± 2.2 Study 3 (Costardi et al., 2006) Concurrent: PAINAD compared with VDS (0.65, p=0.008) Study 4 (Hutchison et al., 2006) Predictive: Compared PME in PAINAD assessed group and control group. Significantly higher PME in PAINAD group (11.25mg) compared to control group ( 5.75mg) (p<.01). Total of unknown pain intensity lower in PAINAD group (15%) versus control group (68%) (p<0.01) Study 5 (Leong et al., 2006) Concurrent: PAINAD compared with Nurses Report r=0.842 (p<.001) PAINAD compared with Patient Self-Report r=0.304 (p<.005) Discriminant: PAINAD and Cornell Depression r=0.292 (P<.005) PAINAD and Abbreviated Mental Test r=-0.198 Few residents had severe pain; strongest relationship with nurse reported pain. Weak relationship between patients report and PAINAD. Demonstrated ordinal nature of PAINAD categorizing 0-1 as no pain; 2-3 as mild pain; 4 > as moderate and severe pain. The categorization correlated strongly with Nurses Rating of Pain (kappa 0.85, p=.001). However, because nurses made both judgments, potential for bias exists. Good discriminant validity.

Reviewed 04/04 Revised 06/08
8
Study 6 (van Iersel et al., 2006) Construct: 185 care providers report on perceptions of measure of pain. 80% agreed that three indicators were most valuable in measuring pain: facial expression, vocalization and body language. Breathing and consolability less good indicators (<60% agreement). Study 7 (Zwakhalen et al., 2006) Predictivet: Pain versus non-pain groups. Evaluated at rest (T1)1, after flu vaccination (T2) and after potentially painful activity (T3). Consistent upward trend of mean total score on PAINAD during three times as expected. Concurrent: PAINAD compared with VAS rater=0.89 PAINAD compared with VAS nurse=0.81 PAINAD compared with VRS (patient)=0.81 PAINAD compared with PACSLAC=0.85 Study 8 (Schuler et al., 2007) Construct: Demonstrated one factor structure accounting for 63.5% variance in morning assessment and 62.4% in evening assessment Predictive: Compared ratings for patients judged to have pain compared to those judged to be free of pain. All categories of scale (except consolability) rated higher in residents with pain than without. Pain intensity rated by nurses did not correlate with the occurrence of pain behaviors. PAINAD-G did not allow prediction of pain intensity. Discriminant: No significant correlations between PAINAD-G and observational measures aimed at nonpain behaviors (apathy, neuropsychiatric) Study 9 (Cohen-Mansfield & Lipson, 2008) Sensitivity: Compared ability of PAINAD (and other tools) to detect pain and change in pain resulting from treatment intervention. In treatment group of 63, 36 completed treatment to achieve no pain, 27 refused treatment by family or physician. A comparison group of 58 without pain used Determination of pain compared across tools noting that this was made by PAINAD in only 5%. Higher rates found in informant based tools (e.g. PADE, PAINE). PAINAD was not strong in detecting treatment effects. Study 10 (DeWaters et al., 2008) Concurrent validity/Pearson’s r of PAINAD with NRS
For all observations (50): 0.834 (p= .01) Unlikely pain (at rest) (25): 0.639 (p= .01) Likely pain (with movement) (25): 0.764 (p=.01) Cognitively intact (26): 0.735 (p<.001) Cognitively impaired (24): 0.915 (p<.001)
Discriminant validity/Wilcoxon signed rank test between likely and unlikely pain events For all observations: z=4.086
-Panel commentary Construct validity Data from studies 1 and 2 were combined to conduct the factor analysis. Although a single factor was isolated contributing a moderate amount of variance, the pain scores were not normally distributed with many scores clustering around 0, especially during a pleasant condition or 30 minutes after pain medication. This limits evaluation of scale effectiveness in those with higher levels of pain-related behaviors. Further study of the PAINAD provides support for construct validity. A single factor was again isolated with greater distribution of pain. However, the

Reviewed 04/04 Revised 06/08
9
number of patients with behaviors reflecting the high end of the scale scoring is still small. Concurrent validity Correlations among the pain tools are strong. However, lack of independent raters for scoring of the pain tools and the associated VAS’s potentially impacts the level of associations. Further study of the PAINAD provides support for good concurrent validity with across tool correlations ranging from 0.65 to 095 with the exception of comparison of the PAINAD to self report of pain (0.30). Discriminant validity Study 1 results show differences in expected outcome, although scores are compressed at the lower end of the scale and further study is needed. The results of study 2 (QI study) appear to capture pain and change in pain. However, limited information on subjects, variability of raters/assessors, control over chart audit data limits conclusions that can be reached for initial tool development and suggest the need for more controlled study. Further study of the PAINAD provides some support for construct, predictive, concurrent and discriminant validity. The most recent study that examines tool sensitivity in detecting change from treatment raises questions regarding the tools ability to do so with persons with severe dementia. Further study is needed. Although studies have raised concern regarding the items of breathing and consolability, authors urge maintaining the current items structure to allow international comparisons. Because removal of items did not demonstrate improved internal consistency, this recommendation seems supportable.
Summary of panel evaluation of pain assessment tool The PAINAD was developed as a shorter, easier observation tool for assessing pain in nonverbal elders. The tool items included are not comprehensive, but subsequent studies have provided data suggesting the tool does detect pain and changing levels of behavior (not pain) intensity. Because of the small number of items that are used to detect pain, the ability of the PAINAD to detect pain in those with less obvious changes in behavior (e.g. mental status changes, aggressive behavior, changes in activities) may still be compromised. Although clinicians desire to have a tool that provides a 1-10 score similar to the 1-10 NRS commonly used as the gold standard in verbal patients, the soundness of establishing a rating scale with pain severity scoring of behaviors has not been substantiated in the literature. Completed studies suggest the tool could be used to show higher and lower levels of pain, but there is no data to attach level of pain severity to the number obtained with the tool. Tool reliability is good for interrater reliability, but internal consistency is only moderate and stability has not been demonstrated. Tool has good reliability in all areas. Some conceptual and methodological issues have been identified with the development and testing of the PAINAD. However, the positive findings in detection of changes in pain behavior following intervention in the QI study reported suggests additional study in controlled circumstances is warranted. Follow-up studies have continued to document ability to detect pain and differentiate pain and no pain groups. Follow-up studies must be differentiated according to degree of dementia in the sample population, whether they study acute or chronic pain and the setting of care. Further study of tool sensitivity to detect change in behavior in response to treatment is needed.

Reviewed 04/04 Revised 06/08
10
Source of evidence Warden, V., Hurley, A.C., Volicer, L. (2003). Development and psychometric evaluation of the Pain
Assessment in Advanced Dementia (PAINAD) Scale. Journal of the American Medical Directors, Jan/Feb, 9-15.
Lane, P., Kuntupis, M., MacDonald, S., McCarthy, P., Panke, J., Warden, V., Volicer, L. (2003). A pain
assessment tool for people with advanced Alzheimer’s and other progressive dementias. Home Healthcare Nurse, 21(1), 32-37.
DeWaters, T., Faut-Callahan, M., McCann, J. J., Paice, J. A., Fogg, L., Hollinger-Smith, L., et al. (2008).
Comparison of self-reported pain and the PAINAD scale in hospitalized cognitively impaired and intact older adults after hip fracture surgery. Orthopaedic Nursing / National Association of Orthopaedic Nurses, 27(1), 21-28.
Costardi, D., Rozzini, L., Costanzi, C., Ghianda, D., Franzoni, S., Padovani, A. & Trabucchi, M. (2006).
The Italian version of the pain assessment in advanced dementia (PAINAD) scale. Archives of Gerontology and Geriatrics, 44(2), 175-180.
Hutchison, R., Tucker, W., Kim, S. & Gilder, R. (2006). Evaluation of a behavioral assessment tool for the
individual unable to self-report pain. American Journal of Hospice and Palliative Medicine, 23(4), 328-331.
Leong, I., Chong, M. & Gibson, S. (2006). The use of a self-reported pain measure, a nurse-reported pain
measure and the PAINAD in nursing home residents with moderate and severe dementia: a validation study. Age and Ageing, 35, 252-256.
Schuler, M., Becker, S., Kaspar, R., Nikolaus, T., Kruse, A. & Basler, H. (2007). Psychometric properties
of the German “Pain Assesssment in Advanced Dementia” (PAINAD-G) in Nursing Home residents. American Medical Directors Association, July, 388-395.
Van Iersel, T., Timmerman, D. & Mullie, A. (2006). Introduction of a pain scale for palliative care patients
with cognitive impairment. International Study of Palliative Nursing, 12(2), 54-59. Zwakhalen, S., Hamers, I. & Berger, M. (2006). The psychometric quality and clinical usefulness of three
pain assessment tools for elderly people with dementia. Pain, 126, 210-220. Cohen-Mansfield, J. & Lipson, S. (2008). The utility of pain assessment for analgesic use in persons with
dementia. Pain, 134(1-2), 16-23. Key to panel rating 3= Available evidence is strong 2= Available evidence supports need for further testing 1= Available evidence is insufficient and/or tool revisions are needed 0= Evidence is absent Contact address for tool developer: Victoria Warden, RN GRECC (182B) E. N. Rogers Memorial Veterans Hospital, 200 Springs Road, Bedford, MA 01730. E-mail: [email protected]. Evaluation completed by: K. Herr, S. Decker, K. Bjoro, University of Iowa.

Reviewed 04/04 Revised 06/08
11
Revision completed 06/08 by: K. Herr, H. Bursch, B. Black, The University of Iowa
Contact information: [email protected]





![Appendixes978-1-4615-1329... · 2017. 8. 28. · [BINDER 87] Binder, K.: Applications of the Monte Carlo Method in Statistical Physics. Springer, Berlin 1987. [BINDER 92] Binder,](https://img.pdfslide.us/doc/110x75/61482dc2cee6357ef9252f77/appendixes-978-1-4615-1329-2017-8-28-binder-87-binder-k-applications.jpg)