Embed Size (px)
Citation preview

HOW WE DO IT
Bilobed Flap for Reconstruction of Small Alar Rim Defects
NATHANIEL J. JELLINEK, MD,*†‡ AND KATHARINE B. CORDOVA, MD*‡
The authors have indicated no significant interest with commercial supporters.
The bilobed flap is a well-established recon-
structive technique for many small to medium-
sized defects on the nose.1,2 Its use in large defects
involving the ala has also been demonstrated.3 This
flap is useful in areas near facial free margins such as
the lower eyelid and alar rim. It functions as a
pushing rather than pulling flap, minimizing the
risks of ectropion and ecnasion. These particular
properties, when applied on the nose, also have the
unintended potential to “bulldoze” and depress
nasal free margins in the setting of thicker, seba-
ceous skin, oversized or incorrect flap design, or
conservatively undermined flaps.2
True alar rim defects encountered after Mohs
surgery present multiple challenges: restoration of
the external nasal valve; aesthetic considerations;
and lack of an adjacent, mobile tissue reservoir on
a free margin. Traditional reconstructive options
include full-thickness skin grafts, composite grafts,
combined cartilage and skin grafts, wedge excision,
V–Y advancement flaps, turn-down hinge flaps,
and cheek-to-nose or paramedian forehead inter-
polation flaps. Second-intention healing and full-
thickness skin grafts risk alar notching associated
with wound healing and contraction, yet for
shallower alar defects away from the free margin,
they remain a viable option.4 Composite grafts are
an attractive option and provide structure and
cosmesis yet remain a challenging and less-reliable
reconstruction with frequent necrosis or partial
take. Combined cartilage and skin grafts can
mitigate these risks. Wedge excision, perhaps the
simplest option, by definition will reduce the
aperture of the nares and external nasal valve. V–Y
advancement flaps lack a mobile pedicle, and
necrosis can occur. The authors have found this
flap to be useful more superiorly on the alar lobule
and not along the rim. Any flap or graft necrosis
can result in free margin compromise, ecnasion,
and constriction of the nasal valve. Cheek-to-nose
interpolation flaps are a reliable reconstructive
option for many of these defects, albeit at the
expense of a staged surgery, cheek scar, and
potential nasolabial fold asymmetry.
The authors present a technique used in six patients
with small defects (<1 cm) on the alar rim that were
reconstructed immediately after Mohs surgery. The
bilobed flap has several attributes that make it a
reliable reconstructive option in this location: robust
perfusion, predictable pushing movement of the flap
toward the free margin, restoration of contour over
a convexity, and limiting the repair to a single
cosmetic subunit, the ala.
Technique
Sterile surgical preparation and infiltrative anes-
thesia are performed in standard fashion. It is
*Department of Dermatology, Warren Alpert Medical School, Brown University, Providence, Rhode Island; †Divisionof Dermatology, University of Massachusetts Medical School, Worcester, Massachusetts; ‡Dermatology Professionals,Inc., East Greenwich, Rhode Island
© 2013 by the American Society for Dermatologic Surgery, Inc. � Published by Wiley Periodicals, Inc. �ISSN: 1076-0512 � Dermatol Surg 2013;39:649–652 � DOI: 10.1111/dsu.12055
649

important to assess the inherent elasticity and
inelasticity of the nasal tissue and the natural
resistance of the ala to collapse before injection of
anesthesia. If anteriorly located, the defect should
be made full thickness through dermis and muscle
although not through-and-through. The flap is
designed with a muscular pedicle. If anteriorly
located, the defect should be made full thickness
through dermis and muscle although not through-
and-through. Converting the defect from partial to
full thickness minimizes flap protuberance once
healed and minimizes tension during flap move-
ment. The flap is designed with a muscular pedicle.
The flap is usually laterally based, although larger
defects and those laterally located can be medially
based. It is designed as a Zitelli-modification
bilobed flap, with total arc of rotation of approx-
imately 90º, the tertiary defect relatively perpen-
dicular to the alar rim, and the standing cone
excised as a part of the flap design—in this instance
along the alar rim.
The standing cone is excised first, then the flap is
incised and undermined in the submuscular plane,
taking care to establish and maintain the appropriate
plane of dissection. Given the small size of the
surgical field, sharp undermining using a scalpel
blade or fine-tipped gradle or tenotomy scissors is
preferred. Undermining in the caudal-most portion
of the flap in type III nasal skin is limited because of
the anatomic turn of this skin posteriorly
toward mucosa.
Hemostasis is obtained with care to avoid elec-
trosurgery on the tissue edges and walls; such
cautery creates focal areas of necrosis and pre-
disposes to more prominent and inverted suture
lines.
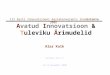
(A)
(B) (C)
(D) (E) (F) (G)
Figure 1. (A) Preoperative basal cell carcinoma located on the left ala bordering the alar rim. (B) Postoperative defect withbilobed flap designed in surgical marking pen. The standing cone is excised medially on the alar rim. The lobes are sizedequally and have a total arc of rotation of approximately 90º. (C) Immediate postoperative image. (D–G) Two-month follow-up photographs.
BILOBED FLAP FOR RECONSTRUCTION OF SMALL ALAR RIM DEFECTS
DERMATOLOGIC SURGERY650

The tertiary defect is sutured first. A single buried
suture is sufficient to set the flap into position and
relieve any tension on the free margin. One or two
more buried vertical mattress sutures are sufficient to
stabilize the flap in position and evert the skin edges.
All buried sutures are placed in muscle to muscle,
which may minimize the scar contraction that leads
to a trapdoor deformity.5 Superficial sutures finish
the repair and are usually removed at 5–7 days.
Postoperative antibiotics are frequently prescribed as
cotton-tipped applicators introduced intranasally
during the procedure in a nasal region that can be
prepared and scrubbed with antiseptic as can be
done with cutaneous surfaces.
A correctly designed flap will restore the natural
bulk and three-dimensional fullness of the ala and
curvature of the alar rim. The small but complex
suture lines, although initially conspicuous, tend to
fade significantly in the setting of appropriate
contour restoration, as demonstrated in the
images (Figures 1, S1, S2).
There are potential pitfalls of faulty flap design,
typically under- or oversizing of the flap. The former
will lead to contraction along the ala and ecnasion.
The latter can bulldoze the free margin, leading to
alar asymmetry and depression. Any tension along
the flap, particularly if the flap is undermined too
superficially, can lead to flap tip necrosis along the
free margin. Care must also be taken to avoid
internal valve constriction when suturing the tertiary
defect. This physiologic valve, located most closely
under the alar groove, can collapse from swelling
associated with flap movement. When the flap is
undermined and open, the surgeon must test the
ipsilateral nasal breathing of the patient, and then
repeat the test after the first key suture. If there is
constriction with this suture, a simple pexing suture
from the depth of the alar groove, fixed to the
sidewall periosteum, will open the valve and prevent
collapse.
This flap is more difficult to perform on patients
with soft, “floppy” alae, which tend to collapse
with minimal pressure and simplest in patients with
firm alar margins. We have not needed to use a
cartilage batten graft to buttress the alar free
margin during our series and would likely choose a
different reconstructive option if such a situation
arose. Similarly, if the defect is larger than 1 cm, it
is possible that the tissue movement would distort
the free margin. Given the stiff skin of the alae in
patients for whom this repair is indicated, subtle
alar base asymmetry may be appreciated; this
asymmetry has been subtle and not distressing to
patients.
The authors have found that the bilobed flap is a
reliable technique to reconstruct small alar rim
defects after Mohs surgery. This procedure addresses
all of the unique functional and aesthetic complex-
ities of the ala: maintenance of the nasal valve,
contour restoration, and reconstruction of the
free margin.
References
1. Zitelli JA. The bilobed flap for nasal reconstruction. Arch
Dermatol 1989;125:957–9.
2. Cook JL. A review of the bilobed flap’s design with particular
emphasis on the minimization of alar displacement. Dermatol
Surg 2000;26:354–62.
3. Cook JL. Reconstructive utility of the bilobed flap: lessons from
flap successes and failures. Dermatol Surg 2005;31:1024–33.
4. Collins SC, Dufresne RG Jr, Jellinek NJ. The bilobed
transposition flap for single-staged repair of large surgical defects
involving the nasal ala. Dermatol Surg 2008;34; discussion: 1379
–85.
5. Ricks M, Cook J. Extranasal applications of the bilobed flap.
Dermatol Surg 2005;31:941–8.
6. Neuhaus IM, Yu SS. Second-Intention Healing of Nasal Alar
Defects. Dermatol Surg 2012;38:697–702.
7. Teltzrow T, Arens A, Schwipper V. One-stage reconstruction of
nasal defects: evaluation of the use of modified auricular
composite grafts. Facial Plast Surg 2011;27:243–8.
8. Ewanowski CD, Cook J. Using cartilage and skin grafts
concurrently: an alternate route to repair. Dermatol Surg
2009;35:1809–17.
9. Asgari M, Odland P. Nasalis island pedicle flap in nasal ala
reconstruction. Dermatol Surg 2005;31:448–52.
10. Fader DJ, Baker SR, Johnson TM. The staged cheek-to-nose
interpolation flap for reconstruction of the nasal alar rim/lobule.
J Am Acad Dermatol 1997;37:614–19.
JELLINEK ET AL
39 : 4 :APRIL 2013 651

11. Nguyen TH. Staged cheek-to-nose and auricular interpolation
flaps. Dermatol Surg 2005;31:1034–45.
12. Cook JL. The undesirable influence of reconstructive procedures
on the symmetry of the nasolabial folds. Dermatol Surg
2005;31:1409–16.
13. Zitelli J. Commentary. Dermatol Surg 2008;34:1385–6.
Address correspondence and reprint requests to: NathanielJ. Jellinek, MD, 1672 South County Trail, Suite 101, EastGreenwich, RI 02818, or e-mail: [email protected]
Supplementary Material
Additional Supporting Information may be found in
the online version of this article:
Figure S1. (A–B) Preoperative photograph
demonstrating a basal cell carcinoma on the right
alar rim. (C–D) Surgical defect after two stages of
Mohs surgery, clear of tumor. (E) Laterally based
bilobed flap designed with a standing cone laterally
along the alar margin and a total arc of rotation of
approximately 90°. (F) Bilobed flap sutured into
place. (G–J) Three-month follow-up photographs
demonstrate well-camouflaged scar lines and
symmetric alar margin.
Figure S2. (A–C) Small surgical defect on the right
alar rim. (D–F) Two-month follow-up photographs
demonstrate wellcamouflaged scar lines and
preserved free alar margin.
BILOBED FLAP FOR RECONSTRUCTION OF SMALL ALAR RIM DEFECTS
DERMATOLOGIC SURGERY652