Embed Size (px)
Citation preview

11/3/2017
1
Billing, Coding, Credentialing, Contracting,
and ReimbursementBopanna B. Ballachanda, Ph.D.
Audiology ConsultantAlbuquerque, NM
Distinguished speaker
Kris R. KwolekPartner at Husch Blackwell’s Law firm
J.D., University of Texas at Austin School of Law, B.S., Texas A&M University,
Direct: 512.479.9716
PRACTICE AREAS
• Ancillary Service Providers
• Healthcare Audit Defense
• Healthcare Compliance
• Counseling and Defense
• Healthcare Fraud & Abuse
• Healthcare Insolvency &
• Bankruptcy Healthcare
• Investigations and Government
• Enforcement Healthcare
• Operations Hospitals & Health Systems
• Intellectual Property
• Life Sciences
• Life Sciences IP
• Life Sciences Licensing and Tech Transfer
• Medicaid Reimbursement
• Strategies Medicare Advantage
• Patents Physicians & Other
• Professionals Pharmacy
• Pharmacy
• Benefit Managers
• Post-Acute Care Providers
Presenter is receiving an honorarium and travel support from the Association
Presenter has no relevant non-financial relationships to disclose.
The purpose of this presentation is to inform and educate the members, the presenter does not take any responsibility for the consequences by the use of this information by any individual.
I am not a biller or coder
4
Disclaimer

11/3/2017
2
Presentation Topics• OPERATING COST: Learn how much it cost to operate a clinic
• CALCULATING FEES: Learn how to determine fees for your services
• CODING: Learn the codes that describe the services you provide.
• What is new in Medicare - MACRA
• CONTRACTING: How to establish a contracting with various payors?
• REIMBURSEMENT: How to get reimbursement
• BILLING: case studies of billing issues
• CREDENTIALING: What is credentialing?
• DENIAL AND APPEAL: How to read denial and the appeal process
• Compliance and Red Flags
Audiology is a Business
It Is More Than Just Being a Good Clinician
Is It Time To Reassess Business Practices?
• What is your profit margin for cost of goods? Cost of “doing” business?
• When was the last time you reviewed a fee schedule, the reimbursement levels, and utilization numbers for a health plan? How does it relate to the cost of doing business?
Minding the Business
• “Reimbursement” is the multi-faceted foundation for sound practice management
• Must know the “language”
• Must utilize best coding and billing practices
• Have you Negotiated good insurance contracts?
• Are your third party contracts profitable?
• Are they what was originally negotiated?• Have you re-negotiated periodically?

11/3/2017
3
Operating cost
How much does it cost to run a practice?
Any practice – Private or Funded
How to Calculate Hourly Rates
Annual Expense =Rate
Annual Contact Hours
Profit and Loss Formula
Profit or Loss : Revenue – Expenses = Profit (Loss)
Annual Expenses + Desired Profit_ = Rate/Hour
Annual Contact Hours
How to determine the number of hours
• Copy of Calculating TAA.xlsx

11/3/2017
4
Revenue-Expense at Your Clinic• Revenue (Income)
• Tests• Hearing aid sales• Therapies/Consultation• Others (Accessories)
• Expenses• Cost of goods sold• Salaries and benefits• Clinic related
• Rent• Incidentals -• Equipment (leased or loan/Interest)• Others (Travel, etc.)
A Challenge • You write the case for a 55 year old male with a bilateral symmetrical
SNHL who was fit with bilateral hearing aids with a remote microphone and coupled using custom earmolds (not domes).
• (1.comprehensive audio + 2. immittance); visit to a physician for 3.medical clearance because the patient had 4.asymmetry – SN loss and 5.unilateral tinnitus (also got an 6.ABR and 7.MRI and results were negative for 8th nerve). He came back for the 8.HAE where I did 9.unaided QuickSIN, 10.LDL’s as well as 11.unaided COSI. I also made 12.impressions to order earmolds and 13. ordered the aids (Selection). I did a 14. hearing aid fit 2 weeks later using 15. real ear measures, 16. aided LDLS for speech and pure-tone sweep RESR90) and 17.aided QuickSIN. 18.Counseled and patient 19.returned 6 weeks later to let me know he loves the aids (why wouldn’t he) and I did some fine-tuning to address some loudness and sound quality issues and he completed the 20. aided COSI.
Itemization of clinic services
• ItemizedBilling.xlsx
Reimbursement:
CODING: Learn the codes that describe the services you provide. Use these codes to communicate with health plans
Must know the “language”
BILLING; Billing the Proper Code: Learn how to bill for your services

11/3/2017
5
National Provider Identifiers (NPIs)
• The NPI is the health care provider identification system adopted by the U.S. Department of Health and Human Services as part of the implementation of HIPAA. All health care providers that are considered covered entities under HIPAA, and those who file claims electronically or use a clearinghouse to bill insurance, are required to apply for an NPI. All other health care providers are eligible to receive an NPI if they desire.
• Audiologists and speech-language pathologists can apply online for their NPI, free of charge, at: https://nppes.cms.hhs.gov/NPPES/Welcome.do
Credentialing
We encourage you to submit an application, attestation and authorization form using the Council for Affordable Quality Health Care (CAQH) Universal Credentialing DataSource application at http://www.caqh.org
CAQH CORE: Operating Rules to Drive the Business of Healthcare
• Established in 2005, CAQH CORE is a multi-stakeholder collaboration of more than 130 organizations –providers, health plans, vendors, government agencies, and standard-setting bodies – developing operating rules to simplify healthcare administrative transactions. CAQH CORE participating organizations include health plans representing more than 75% of commercially insured lives, plus Medicare and Medicaid beneficiaries.
• Operating rules support a range of existing standards to make electronic data transactions more predictable and consistent, regardless of the technology. Operating rules facilitate many high-volume transactions that involve multiple parties, such as automated banking transactions and airline ticket bookings.
• The CORE process centers on an integrated model consisting of: rule development, testing and certification, and measure tracking/outreach.
• A voluntary CORE Certification program drives value and return on investment for all trading partners by ensuring the rules are used consistently; thereby encouraging broader use of the rules. Health plans, providers, vendor/clearinghouses that create, transmit or use administrative data may become CORE-certified.
• CAQH CORE has been designated by the Secretary of the Department of Health and Human Services (HHS) as the author for federally mandated operating rules per Section 1104 of the Patient Protection and Affordable Care Act (ACA).
Credentialing, Contracting, Billing, Coding, and Reimbursement
CPT Codes – Procedural Codes
ICD-10 Codes – Diagnostic Codes
HCPCS Codes - Service Codes

11/3/2017
6
CPT Codes – Procedural CodesAudiology Diagnostic Procedures
• 92550 Tympanogram and reflex threshold measurements
• 92551 Screening, PT air only
• 92552 PT audio, threshold, air only
• 92553 Air and bone
• 92555 Speech audiometry, threshold
• 92556 Speech audiometry threshold with speech recognition
• 92557 Comp aud eval (92553 and 92556 combined)
• 92565 Stenger test, PT
• 92567 Tympanometry
• 92568 Acoustic reflex testing, threshold
• 92570 Acoustic immittance testing (tymps, ART, ARD)
• 92572 Staggered spondaic word test
• 92576 Synthetic sentence identification test
• 92577 Stenger test, speech
• 92579 Visual reinforcement audiometry
• 92582 Conditioned play audiometry
• 92585 Auditory evoked potentials, comprehensive
• 92586 Auditory evoked potentials, limited
• 92587 OAEs, limited
• 92588 OAEs, comprehensive
• 92620 Evaluation of central auditory function, with report, initial 60 min
• 92621 Each additional 15 minutes (must bill with 92620)
• 92625 Assess of tinnitus (pitch, loudness matching, masking
Hearing aid Procedure Codes• 92590 Hearing aid exam and selection, monaural
• 92591 Hearing aid exam and selection, binaural
• 92592 Hearing aid check, monaural
• 92593 Hearing aid check, binaural
• 92594 Electroacoustic eval for hearing aid, monaural
• 92595 Electroacoustic eval for hearing aid, binaural
• 92596 Ear protector attenuation measurements
• 92626 Eval of aud rehab status, first hour
• 92627 Each additional 15 minutes (must bill with 92626)
• 92630 Aud rehab, prelingual HL
• 92633 Aud rehab, postlingual HL
• 92700 Unlisted otorhinolarngological svc or procedure
• OTHER
• 69210 Cerumen removal
VESTIBULAR TESTS AND REHABILITATION
• 92540 Basic vestibular eval (92541, 92542, 92544, 92545)
• 92541 Spont nystagmus test, gaze and fixation, w/ recording
• 92542 Positional nystagmus test, min of 4 positions, w/ recording
• 92537* Caloric vest test, with recording, bilateral; bithermal (4 irrigations)
• 92538* Caloric vest test, with recording, bilateral, monothermal (2 irrigations)
• 92544 OPK nystagmus, bidirectional, foveal or peripheral stim, w/ recording
• 92545 Oscillating track test, w/ recording
• 92546 Sinusoidal vertical axis rotational testing
• 92547 Use of vertical electrodes
• 92548 Comp dynamic posturography
• 95992 Canalith Repositioning Procedure
Modifiers used with CPT codes• Common Modifiers
• 22 Increased procedural service
• 26 PC, If you only interpret 92540–92546, 92548, 92585,92587 or 92588
• 52 Reduced services
• 59 Distinct procedural service (Use for 92541, 92542, 92544 or 92545), if reporting 1–3 of these codes individually
• TC If you only perform 92540– 92546, 92548, 92585, 92587 or 92588
• Medicare Modifiers
• GA Use with a mandatory Advanced Beneficiary Notice (ABN) for a covered service
• GX Use with a voluntary ABN for a non-covered service
• GZ The provider or supplier expects a medical necessity denial; however, did not
provide an ABN to the patient
• GX & GY May be utilized for non-covered services
• GY Use for a statutorily excluded service (often used when a denial from
Medicare is necessary for a secondary payor)

11/3/2017
7
Question
• Question : CPT stands for:
• a) Clinical Practice Terminology
• b) Clinical Procedural Terminology
• c) Certified Procedural Technology
• d) Clinical Procedural Technology
Answer
• Question : CPT stands for:
• a) Clinical Practice Terminology
• b) Clinical Procedural Terminology
• c) Certified Procedural Technology
• d) Clinical Procedural Technology
Evaluation and Management Code• These are the codes physicians and non-physician practitioners (such as nurse
practitioners and physician assistants) utilize to bill for office visits. Per the CPT manual, these codes can be used by
• “qualified health professionals who are authorized to perform such services within the scope of their practice.” Please note: Most E/M code descriptions (except 99211) contain the term “physician.” As a result, use of these codes does contain some level of risk.
• Common codes to be considered by audiologists are: 99201-99203 and 99211-99213. Avoid 99204-99205 and 99214-99215 as inappropriate for audiologists as this level of code requires a high risk of morbidity and mortality (which otologic issues do not contain).
• It is important to inform the audiologists about use of evaluation and management (E&M) codes. It is important the E&M codes are within the scope of licensure law in the state of practice and the contract states that billing E&M codes are reimbursable with appropriate documentation by the third party payors. It is also important to remember that the E&M codes should be billed to all payors including Medicare (even though it is a noncovered item). As a cautionary note, do not use E&M codes for hearing aid check and visits, also do not use it when it was used by another provider (e.g., ENT or hospital setting where it was billed by others on the same day).
Pediatric Case Study

11/3/2017
8
CPT Codes used for Pediatric Assessment and follow up:
Case Example : Child 12 months old was recommended for hearing evaluation and follow up.
Hearing evaluation:
Few important things to remember while billing pediatric evaluation are:
1) Use codes that represents the procedure performed;
2) Document the child’s medical history to support the reasons for performing various tests and the codes that was used for billing.
CPT Codes used for Pediatric Assessment and follow up:
• Visual Reinforcement Audiometry: 92579: Above 6 months
• Conditioned Play Audiometry: 92582: At age three years and above
• Clinician should perform if applicable:
• Speech threshold audiometry (92555)
• Picture Audiometry (92583)
• Or Speech Audiometry Threshold with Speech Recognition (92556).
Assessment of middle ear and inner ear status:
• CPT codes associated with tests for middle ear evaluation:
• Tympanometry (92567);
• Acoustic Reflex Threshold Testing (92568); or
• Combined Tympanometry and Reflex Threshold Measurements (92550),
• Acoustic Immittance testing, which includes Tympanometry, Acoustic Reflex Threshold Testing and Acoustic Reflex Decay Testing (92570).
• If a Pediatric Audiologist performs 1,000 Hz ipsilateral acoustic reflex screening, there is no CPT code for this procedure. In this case, the Tympanometry code (92567) can be used.
Question
• CPT code 92570. - Acoustic Immittance testing:
• a)Tympanometry, Acoustic reflex threshold and reflex decay
• b)Tympanometry, ipsilateral reflex threshold and decay
• c) Pure tone threshold, acoustic reflex threshold and speech testing
• d) None of the above

11/3/2017
9
Assessment of Inner ear and lower brainstem Evaluation:• OAE screening code (92558) should be billed when an overall pass/fail
result is obtained and no additional interpretation is performed. • The OAE limited evaluation code (92587) should be used when the purpose
of the test is to evaluate hearing status. 92587 specifies that three to six OAE frequencies should be evaluated per ear.
• The OAE comprehensive evaluation code (92588) should be used when evaluating 12 or more OAE frequencies per ear.
• The Limited Auditory Evoked Potential code (92586) is generally used by Universal Newborn Hearing Screening (UNHS) programs for screening. The comprehensive Auditory Evoked Potential code (92585) should be used for all other auditory evoked response testing, including testing via air and bone conduction.
• Currently, there is not a CPT code that differentiates “threshold-search” auditory brainstem response (ABR) from “diagnostic” ABR.
Answer
• CPT code 92570. - Acoustic Immittance testing:
• a)Tympanometry, Acoustic reflex threshold and reflex decay
• b)Tympanometry, ipsilateral reflex threshold and decay
• c) Pure tone threshold, acoustic reflex threshold and speech testing
• d) None of the above
Vestibular Assessment
CPT Codes used for Vestibular Assessment and follow up:
• If the canal is impacted with cerumen (H61.20, H61.21, H61.22, H61.23), it should be removed in order to complete caloric testing (69210).
• Basic vestibular evaluation, includes spontaneous nystagmus test with eccentric gaze fixation nystagmus, with recording, positional nystagmus test, minimum of 4 positions, with recording, optokinetic nystagmus test, bidirectional foveal and peripheral stimulation, with recording, and oscillating tracking test, with recording.
• In case the clinician performed all these tests then it should be reported under one code (92540).

11/3/2017
10
• Caloric Testing: Caloric vestibular test, each irrigation with recording (92537). The caloric vestibular test with recording, bilateral; bithermal (i.e., one warm and one cool irrigation in each ear for a total of four irrigations) and 92538 (Caloric vestibular test with recording, bilateral; monothermal (i.e., one irrigation in each ear for a total of two irrigations). In the event that the clinician was not able to complete either the monothermal (92538) or bithermal (92537) and a modifier (-52) should be used to reflect reduced testing.
• Rotary Chair: Sinusoidal vertical axis rotational testing – must have rotational chair (92546). This test requires the use of a chair capable of rotating around a vertical axis. This code is NOT appropriate for substitute chairs or platforms or for VAT/VORTEQ or other active head-shake tests. Technically speaking, this is considered a ‘contact code’ which only allows for billing of one unit per date of contact or service with the patient. This is regardless of whether multiple rotary chair procedures (such as sinusoidal harmonic acclerations, step velocity, off-axis and/or visual-vestibular interaction tests) are performed or if multiple frequencies are performed. There is no allowance to bill this code for more than one date of service though there are a few payers who will pay multiple units, though inappropriately.
• Posturography Computerized dynamic posturography - Need a platform (92548). This is a single unit code for billing purposes. Technically speaking, it’s use is confined to computerized platforms (the original full descriptor states it must include SOT, MCT and EMG which is really only offered by one manufacturer, NeuroCom). The irony of this code is that it is one of the few codes that Medicare WILL pay but many private insurances do not. Typically most private insurers follow. Keep it simple and bill it as one unit and technically it should be performed using a computerized platform that is capable of SOT and MCT at minimum.
• Follow up. The follow up after vestibular and balance testing can lead to Canalith repositioning procedure(s) (eg Epley maneuver, Semont maneuver), 1 unit per day (95992).
Diagnostic CodesICD -10 for
Ear Disease and Hearing loss.
• Organized in 21 chapters. Each chapter is uniquely identified by letter.
• 1st digit—always alphabetic
• 2nd and 3rd digits—always numeric
• 4th, 5th, and 6th digits—may be letters or numbers, or may be a placeholder (x)
• There is always a decimal after the first three digits.
• First 3 digits—define the code category
• Second three digits—etiology, anatomical site, or severity
• Seventh digit—”extension” describes the encounter type (initial, subsequent, sequela) for certain conditions such as TBI
40
ICD-10-CM

11/3/2017
11
• 1 Certain infectious and parasitic diseases (A00-B99)
• 2 Neoplasms (C00-D49)
• 3 Diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism (D50-D89)
• 4 Endocrine, nutritional and metabolic diseases (E00-E89)
• 5 Mental, Behavioral and Neurodevelopmental disorders (F01-F99)
• 6 Diseases of the nervous system (G00-G99)
• 7 Diseases of the eye and adnexa (H00-H59)
• 8 Diseases of the ear and mastoid process (H60-H95)• 9 Diseases of the circulatory system (I00-I99)
• 10 Diseases of the respiratory system (J00-J99)
• 11 Diseases of the digestive system (K00-K95)
• 12 Diseases of the skin and subcutaneous tissue (L00-L99)
• 13 Diseases of the musculoskeletal system and connective tissue (M00-M99)
• 14 Diseases of the genitourinary system (N00-N99)
• 15 Pregnancy, childbirth and the puerperium (O00-O9A)
• 16 Certain conditions originating in the perinatal period (P00-P96)
• 17 Congenital malformations, deformations and chromosomal abnormalities (Q00-Q99)
• 18 Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (R00-R99)
• 19 Injury, poisoning and certain other consequences of external causes (S00-T88)
• 20 External causes of morbidity (V00-Y99)
• 21 Factors influencing health status and contact with health services (Z00-Z99)
41
ICD-10-CM TABULAR LIST of DISEASES and INJURIES
Question
• Question: ICD-10 codes belong to:
• a) American Medical Association
• b) Center for Disease Control
• c) World Health Organization
• d) Center for Medicare and Medicaid Services
Answer
• Question: ICD-10 codes belong to:
• a) American Medical Association
• b) Center for Disease Control
• c) World Health Organization
• d) Center for Medicare and Medicaid Services
• Section I. Conventions, general coding guidelines and chapter specific guidelines
• Section II. Selection of Principal Diagnosis
• Section III. Reporting Additional Diagnoses
• Section IV. Diagnostic Coding and Reporting Guidelines for Outpatient Services
• Appendix I 105 Present on Admission Reporting Guidelines
44
ICD-10-CM Official Guidelines for Coding and Reporting

11/3/2017
12
• Section I. Conventions, general coding guidelines and chapter specific guidelines
• A. Conventions for the ICD-10-CM
• 1. The Alphabetic Index and Tabular List
• 2. Format and Structure:
• The ICD-10-CM Tabular List contains categories, subcategories and codes. Characters for categories, subcategories and codes may be either a letter or a number. All categories are 3 characters. A three-character category that has no further subdivision is equivalent to a code. Subcategories are either 4 or 5 characters. Codes may be 3, 4, 5, 6 or 7 characters. That is, each level of subdivision after a category is a subcategory. The final level of subdivision is a code. Codes that have applicable 7th characters are still referred to as codes, not subcategories. A code that has an applicable 7th character is considered invalid without the 7th character.
• The ICD-10-CM uses an indented format for ease in reference.
45
ICD-10-CM Official Guidelines for Coding and Reporting • 11 Includes:
• The word 'Includes' appears immediately under certain categories to further define, or give examples of, the content of the category.
• 12 Excludes Notes
• The ICD-10-CM has two types of excludes notes. Each note has a different definition for use but they are both similar in that they indicate that codes excluded from each other are independent of each other.
• Excludes1
• A type 1 Excludes note is a pure excludes. It means 'NOT CODED HERE!' An Excludes1 note indicates that the code excluded should never be used at the same time as the code above the Excludes1 note. An Excludes1 is used when two conditions cannot occur together, such as a congenital form versus an acquired form of the same condition.
• Excludes2
• A type 2 excludes note represents 'Not included here'. An excludes2 note indicates that the condition excluded is not part of the condition it is excluded from but a patient may have both conditions at the same time. When an Excludes2 note appears under a code it is acceptable to use both the code and the excluded code together.
46
A. Conventions for the ICD-10-CM
• For bilateral conditions, the final character indicates laterality. 1 = RIGHT, 2 = LEFT, 3 = BILATERAL. Unspecified is coded as 0 or 9
• There are exceptions:• Bilateral conductive HL: H90.0
• Unilateral conductive HL: H90.11 or H90.12
• Bilateral SNHL: H90.3
• Unilateral SNHL: H90.41 or H90.42
• Bilateral mixed HL: H90.6
• Unilateral mixed HL: H90.71 or H90.72
47
13. Coding Laterality
• Every code starts with an H
• Organization:• Diseases of external ear (H60-H62)• Disorders of middle ear and mastoid (H65-H75)• Diseases of inner ear (H80-H83)• Other disorders of the ear (H90-H94)• Intraoperative and postprocedural complications and
disorders of ear and mastoid process, not elsewhere classified (H95)
• Hearing loss is organized under Other Disorders of the Ear (H90-H95)
48
Chapter 8 in ICD-10-CM

11/3/2017
13
• Conditions are not part of the coded in Chapter 8 , but the patient may have both conditions at the same time.
• Certain conditions originating in the perinatal period (P04-P96)
• Certain infectious and parasitic diseases (A00-B99)
• Complications of pregnancy, childbirth and the puerperium (O00-O99)
• Congenital malformations, deformations and chromosomal abnormalities (Q00-Q99)
49
Other Chapters for additional information
• Endocrine, nutritional and metabolic diseases (E00-E88)
• Injury, poisoning and certain other consequences of external causes (S00-T88)
• Neoplasms (C00-D49)
• Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (R00-R94)
50
Other Chapters for additional information
ICD-10 has given us the following
• Laterality (right, left, bilateral)
• New codes for unilateral and bilateral temporary threshold shift (H93.24-)
• New codes for ototoxic hearing loss (H91.0-)
• New codes for intra-operative and post-procedural complications (H95)
51
Note worthy information
• H91.8 Other specified hearing loss
• H91.8X Other specified hearing loss
• H91.8X1 Other specified hearing loss, right ear
• H91.8X2 Other specified hearing loss, left ear
• H91.8X3 Other specified hearing loss, bilateral
• H91.8X9 Other specified hearing loss, unspecified ear

11/3/2017
14
• H81.0- Ménière's disease• H81.1 Benign paroxysmal vertigo• H81.2-Vestibular neuronitis• H81.31- Aural vertigo• H81.39- Other peripheral vertigo • H81.4- Central vertigo• H81.8x- Other disorders of vestibular function• H82- Vertiginous syndromes classified elsewhere• H83.0- Labyrinthitis• H83.1- Labyrinthine fistula• H83.2x- Labyrinthine dysfunction• Final character: “1”=right, “2”=left, “3”=bilateral, “0” or
“9”= unspecified
53
How Do I Code Balance Disorders?
New Codes 2017
• H90.A11 Conductive hearing loss, unilateral, right ear with restricted hearing on the contralateral side
• H90.A12 Conductive hearing loss, unilateral, left ear with restricted hearing on the contralateral side
• H90.A2 Sensorineural hearing loss, unilateral, with restricted hearing on the contralateral side
• H90.A21 Sensorineural hearing loss, unilateral, right ear, with restricted hearing on the contralateral side
• H90.A22 Sensorineural hearing loss, unilateral, left ear, with restricted hearing on the contralateral side
• H90.A3 Mixed conductive and sensorineural hearing loss, unilateral with restricted hearing on the contralateral side
• H90.A31 Mixed conductive and sensorineural hearing loss, unilateral, right ear with restricted hearing on the contralateral side
• H90.A32 Mixed conductive and sensorineural hearing loss, unilateral, left ear with restricted hearing on the contralateral side
55
Additional Codes for Audiology Diagnosis
• Code the complication code followed by the specific effect of the complication (e.g. hearing loss).
• H95.31 Accidental puncture and laceration of the ear and mastoid process during a procedure on the ear and mastoid process
• H95.41 Postprocedural hemorrhage and hematoma of ear and mastoid process following a procedure on the ear and mastoid process
• Example: Accidental TM perforation with hearing loss
• H95.31
• H90.11 Conductive hearing loss, unilateral, right ear, with unrestricted hearing on the contralateral side
•
56
Post-procedural Complications

11/3/2017
15
• Z codes represent reasons for encounters. A corresponding procedure code must accompany a Z code if a procedure is performed. Z codes are neither diagnoses or procedures.
• Used for circumstances other than a disease:
• When a person who may or may not be sick encounters the health services for some specific purpose, such as limited care or service for a current condition, to donate an organ or tissue, immunization, or to discuss a problem which is in itself not a disease or injury.
• When some circumstance or problem is present which influences the person's health status but is not in itself a current illness or injury.
57
Supplemental Codes
• Status codes—indicate that a patient has the sequelae or residual of a past disease or condition. • Includes such things as the presence of prosthetic or mechanical
devices resulting from past treatment. • Status may affect the course of treatment and its outcome. • A status code is distinct from a history code. The history code
indicates that the patient no longer has the condition.
• There are two types of history Z codes, personal and family.• Personal history—explains a patient’s past medical condition that
no longer exists and is not receiving any treatment, but that has the potential for recurrence, and therefore may require continued monitoring.
• Family history —use when a patient has a family member(s) who has had a particular disease that causes the patient to be at higher risk of also contracting the disease.
58
Status and History Codes
• Z02 Encounter for administrative examination• Z02.0 Encounter for examination for admission to educational institution• Z02.1 Encounter for pre-employment examination• Z02.2 Encounter for examination for admission to residential institution• Z02.3 Encounter for examination for recruitment to armed forces• Z02.71 Encounter for disability determination
• Z03 Encounter for screening for other diseases and disorders• Z13.5 Encounter for screening for eye and ear disorders• Z13.850 Encounter for screening for traumatic brain injury
•
59
Supplemental Codes
• Encounter for other special examination without complaint, suspected or reported diagnosis• Z01.10 Encounter for examination of ears and hearing without abnormal findings
• Z01.110 Encounter for hearing examination following failed hearing screening. New born hearing evaluation and get paid for this diagnosis.
• Z01.118 Encounter for examination of ears and hearing with other abnormal findings
• Use additional code to identify abnormal findings
• Z01.12 Encounter for hearing conservation and treatment
•
60
Supplemental Codes

11/3/2017
16
• Z45 Encounter for adjustment and management of implanted device• Z45.320 Encounter for adjustment and management of bone
conduction device• Z45.321 Encounter for adjustment and management of cochlear
device• Z45.328 Encounter for adjustment and management of other
implanted hearing device
• Other Useful Codes• Z46.1 Encounter for fitting and adjustment of hearing aid• Z57.0 Occupational exposure to noise• Z71.2 Person consulting for explanation of examination or test
findings• Z76.5 Malingerer (Person feigning illness with obvious motivation)• Z77.122 Contact with and (suspected) exposure to noise
61
Supplemental Codes
• Z83.52 Family history of ear disorders
• Z86.69 Personal history of other diseases of the nervous system and sense organs
• Z96.20 Presence of otological and audiological implant, unspecified
• Z96.21 Cochlear implant status
• Z96.22 Myringotomy tube(s) status
• Z96.29 Presence of other otological and audiological implants
• Z97.4 Presence of external hearing-aid
62
Supplemental Codes
Coding a visit: Basics
• Code for the reason for the visit (Medicare transmittal 84)
• Code with signs and/or symptoms • Why the patient presented to your office?
• Code by patient history/Complaints (Medical Necessity)• Tinnitus• Hearing loss• Disequilibrium
• Code by findings• SNHL?• Tinnitus?• Conductive hearing loss, middle ear?
Question
• Question : Coding a finding is based on: a) Code for the reason for the visit
• b) Code with signs and/or symptoms
• c) patient history/Complaints (Medical Necessity)
• d) All of the above

11/3/2017
17
Answer
• Question: Coding a finding is based on: a) Code for the reason for the visit
• b) Code with signs and/or symptoms
• C) patient history/Complaints (Medical Necessity)
• d) All of the above
Case 1 – Presentation
• 52 Year old male patient
• Chief complaint : Difficulty in hearing speech in noise.
• Remaining case history is unremarkable
• No report of dizziness, ear ache, pain, family history of hearing loss, noise exposure or any other complications.
CPT code
• What would be the CPT code?
CPT code
• What would be the CPT code?
• 92557 - ??

11/3/2017
18
CPT code
• What would be the CPT code?
• 92557 – 52
• Some requirement of the code were not performed but interpretation was the finding will not be affected.
Question
• Question: Modifier 52 when attached with a CPT code reflects:
• a) Increased services
• b) Reduced services
• c) Services provided for children
• d) No service was provided
Answer
• Question: Modifier 52 when attached with a CPT code reflects:
• a) Increased services
• b) Reduced services
• c) Services provided for children
• d) No service was provided
Coding a visit: Basics
• Code for the reason for the visit (Medicare transmittal 84)
• Code with signs and/or symptoms • Why the patient presented to your office?
• Code by patient history/Complaints (Medical Necessity)• Tinnitus• Hearing loss• Disequilibrium
• Code by findings• SNHL?• Tinnitus?• Conductive hearing loss, middle ear?

11/3/2017
19
How do we code this patient?
• Code based on test/procedural outcome?• Normal findings
• Code based on symptoms?
• Code based on chief complaint?
• Code based on the reason for the visit? • Patient reported difficulties in hearing speech in noise.
What code to diagnose this patient?
• 1. H 90.3
Bilateral sensorineural loss?
• 2. H 90.5• Unspecified sensorineural loss?
• 3. H 9.299• Other abnormal auditory perception – Unspecified ear
• 4. Z01.10 • Encounter for examination of ears and hearing without abnormal finding
What code to diagnose this patient?
• 1. H 90.3
Bilateral sensorineural loss? NO
• 2. H 90.5• Unspecified sensorineural loss? NO
• 3. H 9.299• Other abnormal auditory perception – Unspecified ear – based on chief
complaint
• 4. Z01.10 • Encounter for examination of ears and hearing without abnormal finding. Not
get paid.
New Codes 2017
• H90.A11 Conductive hearing loss, unilateral, right ear with restricted hearing on the contralateral side
• H90.A12 Conductive hearing loss, unilateral, left ear with restricted hearing on the contralateral side
• H90.A2 Sensorineural hearing loss, unilateral, with restricted hearing on the contralateral side
• H90.A21 Sensorineural hearing loss, unilateral, right ear, with restricted hearing on the contralateral side
• H90.A22 Sensorineural hearing loss, unilateral, left ear, with restricted hearing on the contralateral side
• H90.A3 Mixed conductive and sensorineural hearing loss, unilateral with restricted hearing on the contralateral side
• H90.A31 Mixed conductive and sensorineural hearing loss, unilateral, right ear with restricted hearing on the contralateral side
• H90.A32 Mixed conductive and sensorineural hearing loss, unilateral, left ear with restricted hearing on the contralateral side

11/3/2017
20
How do we code this patient?
• H90.A22 Sensorineural hearing loss, unilateral, left ear, with restricted hearing on the contralateral side
• H90.A31 Mixed conductive and sensorineural hearing loss, unilateral, right ear with restricted hearing on the contralateral side
• http://www.audiology.org/practice/coding/ICD-10-CM
• http://www.audiology.org
• http://www.asha.org
• http://www.cdc.gov/nchs/icd/icd10cm.htm
• https://www.cms.gov/Medicare/Coding/ICD10
• http://www.cdc.gov
78
Additional References
Credentialing, Contracting, Billing, Coding, and Reimbursement
HCPCS Codes – Service Codes• S0618 Audiometry for HAE to determine the level and degree of HL
• V5008Hearing screening
• V5010Assessment for hearing aid
• V5011Fitting/orientation/checking of hearing aid
• V5014Repair/modification of a hearing aid
• V5020Conformity evaluation
• V5090Dispensing fee, unspecified hearing aid
• V5095Semi-implantable middle ear hearing prosthesis
• V5110Dispensing fee, bilateral
• V5120Binaural, body
• V5130Binaural, in the ear
• V5140Binaural, behind the ear
• V5160Dispensing fee, binaural
• V5170Hearing aid, CROS, in the ear
• V5180Hearing aid, CROS, behind the ear

11/3/2017
21
• V5200 Dispensing fee, CROS
• V5210 Hearing aid, BICROS, in the ear
• V5220 Hearing aid, BICROS, behind the ear
• V5240 Dispensing fee, BICROS
• V5241 Dispensing fee, monaural hearing aid, any type
• V5244 Hearing aid, digitally programmable analog, monaural, CIC
• V5245 Hearing aid, digitally programmable analog, monaural, ITC
• V5246 Hearing aid, digitally programmable analog, monaural, ITE
• V5247 Hearing aid, digitally programmable analog, monaural, BTE
• V5250 Hearing aid, digitally programmable analog, binaural, CIC
• V5251 Hearing aid, digitally programmable analog, binaural, ITC
• V5252 Hearing aid, digitally programmable, binaural, ITE• V5253 Hearing aid, digitally programmable, binaural, BTE• V5254 Hearing aid, digital, monaural, CIC• V5255 Hearing aid, digital, monaural, ITC• V5256 Hearing aid, digital, monaural, ITE• V5257 Hearing aid, digital, monaural, BTE• V5258 Hearing aid, digital, binaural, CIC• V5259 Hearing aid, digital, binaural, ITC• V5260 Hearing aid, digital, binaural, ITE• V5261 Hearing aid, digital, binaural, BTE• V5262 Hearing aid, disposable, any type, monaural• V5263 Hearing aid, disposable, any type, binaural
• V5264 Ear mold/insert, not disposable, any type
• V5265 Ear mold/insert, disposable, any type
• V5266 Battery for use in hearing device
• V5267 Hearing aid supplies/accessories
• V5268 Assistive listening device, telephone amplifier, any type
• V5269 Assistive listening device, alerting, any type
• V5270 Assistive listening device, television amplifier, any type
• V5271 Assistive listening device, television caption decoder
• V5272 Assistive listening device, TDD
• V5273 Assistive listening device, for use with cochlear implant
• V5274 Assistive listening device, not otherwise specified
• V5275 Ear impression, each
• V5298 Hearing aid, not otherwise classified
• V5299 Hearing service, miscellaneous
Question
• Question: HCPCS service code V5160 indicates:
• a) Dispensing fee, binaural
• b) Dispensing fee, monaural
• c) Dispensing fee assistive listening devices
• d) Dispensing fee OTC

11/3/2017
22
Answer
• Question: HCPCS service code V5160 indicates:
• a) Dispensing fee, binaural
• b) Dispensing fee, monaural
• c) Dispensing fee assistive listening devices
• d) Dispensing fee OTC
Standardized Billing Form:The CMS 1500
What is MACRA
• MACRA is the Medicare Access & CHIP Reauthorization Act also know colloquially as the ‘permanent doc fix’. Although MACRA is know for repealing the Sustainable Growth Rate (SGR) provisions that would have significantly cut physicians salaries (but was reversed every December), there are other provisions.
Medicare Prior to MACRAFee-for-service (FFS) payment system, where clinicians are paid based on volume of services, not value.
Established in 1997 to control the cost of Medicare payments to physicians
IFOverall Target Medicare Physician payment cutphysician costs expenditures across board
Each year, Congress passed temporary “doc fixes” to avert cuts (no fix in 2015 would have meant a 21% cut in Medicare payments to clinicians
The Sustainable Growth Rate (SGR)

11/3/2017
23
MACRA
• Clinicians can choose how they want to participate in the Quality Payment Program based on their practice size, specialty, location, or patient population.
• Two tracks to choose from: one or the other
Advance Alternative Payment Models (APMS)
If you decide to enroll in this program you may earn Medicare incentive payment
The Merit-based Incentive Payment System(MIPS)
You man earn performance-based payment adjustment through MIPS
PQRS
• Note: 2016 was the last program year for PQRS. PQRS transitioned to the Merit-based Incentive Payment System (MIPS) under the Quality Payment Program. The final data submission timeframe for reporting 2016 PQRS quality data to avoid the 2018 PQRS downward payment adjustment was January through March 2017. The first MIPS performance period is January through December 2017
Medicare Payment Prior to MACRA
Fee-for-service (FFS) payment system, where clinicians
are paid based on volume of services, not value.
Quality Payment Program
✓ Repeals the Sustainable Growth Rate (SGR) Formula
✓ Streamlines multiple quality reporting programs into the new
Merit-based Incentive Payment System (MIPS)
✓Provides incentive payments for participation in
Advanced Alternative Payment Models (APMs)
The Merit-based
Incentive
Payment System
(MIPS)
or Advanced
Alternative
Payment Models
(APMs)
✓ First step to a fresh start
✓ We’re listening and help is available
✓ A better, smarter Medicare for healthier people
✓ Pay for what works to create a Medicare that is enduring
✓ Health information needs to be open, flexible, and user-centric

11/3/2017
24
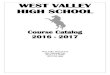
QUALITY
50%
ADVANCING CARE
INFORMATION
25%
CLINICAL PRACTICE
IMPROVEMENT
ACTIVITIES
15%
Resource Use
10%

11/3/2017
25
QUESTIONS