Embed Size (px)
Citation preview

Bile Duct Injury during cholecystectomyBile Duct Injury during cholecystectomy
Catherine HUBERTCatherine HUBERTJeanJean--FranFranççois GIGOTois GIGOTBenoBenoîît NAVEZt NAVEZ Division of HepatoDivision of Hepato--BiliaryBiliary--Pancreatic Pancreatic SurgerySurgery
Department of Abdominal Surgery and Department of Abdominal Surgery and TransplantationTransplantation
Strasbourg, IRCAD, October 2010
TOPICSTOPICS
Bile DuctBile Duct Injury during Lap CholeInjury during Lap Chole
1.1. Prevalence, mechanisms, prevention and diagnosisPrevalence, mechanisms, prevention and diagnosis
2. Treatment strategies:2. Treatment strategies:a.a. primary surgical repairprimary surgical repairb.b. postoperative biliary fistulapostoperative biliary fistulac.c. biliary peritonitisbiliary peritonitisd.d. biliary stricturebiliary stricture

Multicenter Belgian SurveysMulticenter Belgian Surveys
VereeckenVereecken 1992 3244 LC all t1992 3244 LC all type 0.50 %ype 0.50 %
GigotGigot < 1997 9959 LC < 1997 9959 LC all type 0.50 %all type 0.50 %
VandesandeVandesande 1997 10.595 LC all ty1997 10.595 LC all typepe 0.37 %0.37 %
11.628 11.628 all type all type 0.58 %all type all type 0.58 %
VandesandeVandesande 2000 14.715 LC all t2000 14.715 LC all typeype 0.31 %0.31 %
16.915 16.915 all type all type 0.54 %all type all type 0.54 %
Navez Navez 2004 1089 LC 2004 1089 LC acute cholecystitis 1 %acute cholecystitis 1 %
Authors Period Patients type of Authors Period Patients type of clinical BDI rateclinical BDI rateprocedure presentationprocedure presentation
X 2X 2
Local risk factors of BDI
THETHE RISK FACTORSRISK FACTORS for BDI during LAP. for BDI during LAP. CHOLE are CHOLE are MULTIFACTORIALMULTIFACTORIAL
1.1. factors inherent to the laparoscopic approachfactors inherent to the laparoscopic approach2. inadequate training of the surgeon2. inadequate training of the surgeon3. local risk factors3. local risk factors4.4. Technical factorsTechnical factors

loss of depth perceptionloss of manual palpation surgeon's dependance to the equipment limited field easily obscured by bile or
blood (loss of vision)blind manipulation of instruments.
1.RISK FACTORS 1.RISK FACTORS INHERENTINHERENT TO THE TO THE LAPAROSCOPIC APPROACHLAPAROSCOPIC APPROACH
0
5
10
15
20
25
50 100 150 200 250 300 350 400 450
Nb ofNb ofBDIBDI
!GIGOT, Surg Endosc 1997, 11 : 1171GIGOT, Surg Endosc 1997, 11 : 1171--11781178
absentabsent presentpresent
< 50 cases :< 50 cases : 55 %55 % 4545 %%
> 50 cases :> 50 cases : 24 %24 % 76 %76 %
SURGEON EXPERIENCE and LOCAL RISK FACTORS LOCAL RISK FACTORS **
SurgeonSurgeon’’s experience (Nb of LC)s experience (Nb of LC)
•• anonymous survey on 9959 LCanonymous survey on 9959 LC•• 65 patients with BDI (0.5 %)65 patients with BDI (0.5 %)
p = 0.03p = 0.03

misidentification of cystic ductmisidentification of cystic duct : : the the «« classicalclassical »» injuryinjury
‐with CBD duct during IOC 6 %during dissection 35 % 43 %43 %
‐with cystic artery 1.5 %
Laparoscopic belgian survey
cystic duct avulsion cystic duct avulsion CBD tenting CBD tenting Clipping during urgent hClipping during urgent haaemostasis emostasis
DIFFICULT 3. LOCAL RISK FACTORSAND BILE DUCT INJURIES
3 acute or severe chronic inflammation !!! (65 %)(65 %)
33 large ilarge impacted stone in the Hartman mpacted stone in the Hartman ppouchouch (16 %)(16 %)
33 MIRIZZI syndromeMIRIZZI syndrome +/+/-- biliobilio--biliary fistula (4%)biliary fistula (4%)
33 Morbid obesityMorbid obesity
33 Anatomical anomaliesAnatomical anomalies
complete cholangiogram!complete cholangiogram!

You can perform a You can perform a Subtotal cholecystectomySubtotal cholecystectomy
leave a piece of leave a piece of gallbladdergallbladder wallwall on on the the Calot triangle and at the level of Calot triangle and at the level of the Hartman Pouchthe Hartman Pouch
In SEVERE CHOLECYSTITIS with anomalous RHD
* lateral injury : 48%* lateral injury : 48%
* complete* completetranssection : 32%transsection : 32%
* resection : 10%* resection : 10%* thermal : * thermal : 11%11%
SEVERITYSEVERITY SITE ( BISMUTH classif. )SITE ( BISMUTH classif. )
* * type I : 51%type I : 51%* type II : 28%* type II : 28%
* type III : 9%* type III : 9%* type IV : 3%* type IV : 3%* type V : 9%* type V : 9%
52%52% 21%21%
GIGOT, Surg Endosc 1997; 11: 1171GIGOT, Surg Endosc 1997; 11: 1171
BDI during LC

CLINICAL PRESENTATIONCLINICAL PRESENTATION
•• peroperative detection (29) :peroperative detection (29) :
•• external biliary leak (8):external biliary leak (8): 12%12%•• biliary peritonitis :biliary peritonitis :
-- localized (biloma) (3): 6%localized (biloma) (3): 6%-- diffuse (19) :diffuse (19) : 29 % !!!29 % !!!
•• biliary stricture :biliary stricture :-- early (3):early (3): 4.5%4.5%-- late (3) :late (3) : 4.5%4.5%
65 patientsBDI during LC : the Belgian Registry
51 %51 %
44.544.5%%
* IMMEDIATE REPAIR :* IMMEDIATE REPAIR : * small caliber of non dilated ducts* small caliber of non dilated ducts(during the 1st op) * but absence of local inflammatio(during the 1st op) * but absence of local inflammation n
* EARLY REPAIR : * non dilated ducts !!!* EARLY REPAIR : * non dilated ducts !!!(<2months) * local inflammation* local inflammation
* sepsis and poor patients* sepsis and poor patients conditioncondition
* LATE REPAIR : * optimized conditions* LATE REPAIR : * optimized conditions(>2 months) (>2 months) * presence of ductal dilatation with fibrotic tissues* presence of ductal dilatation with fibrotic tissues
Bile Duct Injury during Lap.Chole..TIMING of REPAIRTIMING of REPAIR

1.Early1.Early REPAIR ofREPAIR of BDI BDI
THERMAL INJURYTHERMAL INJURY In 1/3 of BDI VASCULAR INJURYVASCULAR INJURY
risk factors for late stricture
3030--50%50%type IV : 60 %type IV : 60 %
Stewart et al. Ann Surg 2003; 237: 460Stewart et al. Ann Surg 2003; 237: 460
Patients Patients Mortality Biliary Reinterv. FU (mo)Mortality Biliary Reinterv. FU (mo) RecurrentRecurrentcomplic.complic. median median StrictureStricture
. Perop. detect. :. Perop. detect. : 7 %7 % 24 %24 % 14 %14 % 4646
. Peritonitis :. Peritonitis : 50 %50 % 23 %23 % 535345 %45 %
34 %34 %20 %20 %
29 %29 %
47 %47 %
Laparoscopic cholecystectomy Laparoscopic cholecystectomy = = minimallyminimally invasiveinvasive procedureprocedure
BDIBDI = = maximallymaximally invasiveinvasive situationsituation→→ change your philosophychange your philosophy→→ treat properly treat properly →→ medicomedico‐‐legal consequencelegal consequencess
PHILOSOPHY of TREATMENT

Bile Duct Injury during Lap.Chole.
MANAGEMENT of BILE DUCT INJURY DIAGNOSED MANAGEMENT of BILE DUCT INJURY DIAGNOSED EARLY EARLY after LAPAROSCOPIC CHOLECYSTECTOMYafter LAPAROSCOPIC CHOLECYSTECTOMY
•• external biliary fistulaexternal biliary fistula•• bile peritonitisbile peritonitis•• obstructive jaundice from biliary strictureobstructive jaundice from biliary stricture
3 types of postoperative clinical presentations :3 types of postoperative clinical presentations :
1. Postoperative Biliary FistulaRADIOLOGICAL EVALUATIONRADIOLOGICAL EVALUATION
AVOID to REOPERATE AVOID to REOPERATE …… before complete evaluationbefore complete evaluationPURPOSEPURPOSE
1. to define site and severity of BDI 2. to evaluate the intraabdominal bile leakage 3. to detect coexistent injury
TYPE of IMAGING STUDIESTYPE of IMAGING STUDIES
1. CT with contrast injection is superior to US 2. MRI is a “all-in” exam (cholangio + angio-MRI) to define lesions3. ERCP is the most useful tool in partial injury
(excepted if complete obstruction or transsection)

WAIT
ERCP
CT or (MRI)CT or (MRI)
ddiffuse bileiffuse bileperitonitisperitonitis
llocalizedocalizedbilomabiloma
* * nno collectiono collection* * ggood clinical conditionood clinical condition
if if -- persistant > 1 week or worseningpersistant > 1 week or worsening-- LFTs elevated (obstruction ?)LFTs elevated (obstruction ?)-- total biliary diversiontotal biliary diversion
SURGERYSURGERY Percut.Percut.RX drainageRX drainage
-- amount of bile / 24 h.amount of bile / 24 h.-- evolution of biliary leakevolution of biliary leak
to define to define ‐‐ type / site / severitytype / site / severity
cystic, Luchka * partial injury cystic, Luchka * partial injury * complete transsection* complete transsectionducts * lat. clippinducts * lat. clippingg * resection* resection
ERCPERCP
ES + prosthesisES + prosthesis ES + prosthesisES + prosthesisoror
surgerysurgery
Efficient endoscopic managementEfficient endoscopic management
SURGERYSURGERY
ENDOSCOPIC MANAGEMENTENDOSCOPIC MANAGEMENT

2.POST- OPERATIVE BILIARY PERITONITIS
High sHigh suspicion for Buspicion for BDDI I should be maintained for should be maintained for any patient any patient who do not recover normally who do not recover normally and and quickly after LC.quickly after LC.
The mean delay for reoperation in the Belgian The mean delay for reoperation in the Belgian registry was registry was …… 11 days 11 days (1 (1 –– 21)21)
!
MANAGEMENT of BILIARY PERITONITIS
LAPAROTOMYLAPAROTOMY
•• clinical improvementclinical improvement•• no residual bile collectionsno residual bile collections
on repeat CT examinationon repeat CT examination
* peritoneal lavage* peritoneal lavage* * biliary drainagebiliary drainage
-- biliobilio-- digestivedigestive anastomosisanastomosis……. if possible. if possible
-- otherwise, otherwise, externalexternal diversiondiversion
* * septic condition ( infected bilseptic condition ( infected bile)e)** long standing peritonitislong standing peritonitis
* good clinical condition* good clinical condition* recent peritonitis* recent peritonitis
partial laceration,partial laceration,cystic or Luchka ductcystic or Luchka duct
completecompletelacerationlaceration
1.1. endoprosthesisendoprosthesis2.2. percutaneous orpercutaneous or
surgical drainagesurgical drainage(lap or open)(lap or open)
EMERGENCY TREATMENT
ERCPERCP

ssuture suture+ T tubeuture suture+ T tube HJAHJA . excise and HJA. excise and HJA+ T+ T‐‐tube HJA tube HJA . . diversiondiversion
- type- severity
classification of injuryclassification of injuryby by IOCIOC
ppartialartialinjuryinjury
ccompleteompletetranssectiontranssection
wwideideresectionresection
tthermalhermalnecrosisnecrosis
partial laceration of the choledochuspartial laceration of the choledochus

ENDEND--toto--END BILIARY REPAIREND BILIARY REPAIR
CAUSES of FAILURESCAUSES of FAILURES
* loss of ductal tissue* loss of ductal tissue* tension on the suture line* tension on the suture line* inadequate blood supply* inadequate blood supply
(thermal injury)(thermal injury)* small caliber of the ducts* small caliber of the ducts* proximal location of B* proximal location of BDDII
lateral BDI to lateral BDI to anomalous RLDanomalous RLD
during delayed LC during delayed LC for severe cholecystitisfor severe cholecystitis
primary repair primary repair by by suturesuturewith Twith T--tube tube insertioninsertion
BDI due to an ANOMALOUS R. HEPATIC DUCT

STRATEGY OF TREATMENTSTRATEGY OF TREATMENT
do a selective cholangiography !!do a selective cholangiography !!
if limited biliary sectorif limited biliary sectorand thin ductand thin duct
if large biliary sectorif large biliary sectorand large stomaand large stoma
if large biliary sectorif large biliary sectorand thin ductand thin duct
then, close it permanentlythen, close it permanently
make a repair (suture + Tube ormake a repair (suture + Tube orHJA)HJA)
clip temporary and comeclip temporary and comeback later, when dilatedback later, when dilated
BDI due to an ANOMALOUS R. HEPATIC DUCTBDI due to an ANOMALOUS R. HEPATIC DUCT
TOTAL BILIARY DIVERSIONTOTAL BILIARY DIVERSION
INDICATIONSINDICATIONS
•• when a biliary repair is impossible or unsafewhen a biliary repair is impossible or unsafe-- proximal thermal necrosisproximal thermal necrosis-- severe inflammationsevere inflammation-- tiny proximal ducttiny proximal duct
TECHNIQUETECHNIQUE•• drain into the proximal biliary stumpdrain into the proximal biliary stump•• multiples large submultiples large sub--hepatic drainshepatic drains
……. NOT too close of the hepatoduodenal. NOT too close of the hepatoduodenalligament ligament ……. risk of vascular injury !. risk of vascular injury !
•• (large sub(large sub--hepatic omentoplasty) hepatic omentoplasty)

HepaticoHepatico--jejunal anastomosis:jejunal anastomosis:The HEPPThe HEPP--COUINAUD APPROACH COUINAUD APPROACH
HepaticoHepatico--jejunal anastomosis:jejunal anastomosis:The HEPPThe HEPP--COUINAUD APPROACH COUINAUD APPROACH
«« mucosamucosa--toto--mucosamucosa »» hepaticohepatico--jejunostomyjejunostomy

LongLong--term followterm follow--up (up (at least at least 10 years) is mandatory 10 years) is mandatory before definitive conclusions before definitive conclusions aboutabout the outcome the outcome of of BBDDI.I.
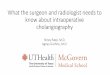
BILE DUCT INJURY during LAP. CHOLE
Female , 74y1994: ‐ type IV BDI post lap chole
Hepp‐Couinaud HJAFU once a year in outpatient clinic(biology and cholangioMRI)
Completely asymptomatic with normal follow‐up untill june 2009April and June 2009: Cholangitis Normal LFT (after cholangitis)MRI: ! Stenosis at the level of the LHD
CLINICAL CASES

Clinical case : 1
CT SCANCT SCAN
Female, 35y
D1: abdominal pain
CRP: 22WBC: 24000Normal LFT
Female, 35y
D1: abdominal pain
CRP: 22WBC: 24000Normal LFT
ERCPERCP
WHAT SHOULD YOU DO?
1.Wait and see
2.Percutaneous drain alone
3.Endoprothesis alone
4.Percutaneous drain and endoprothesis
5.Open Hepatico-jejunostomy and peritoneal lavage

Clinical case : 1
Answer:
4.Endoprothesis and percutaneous drain
Clinical case 2
* F 30 years* F 30 years--oldold* Lap chole * Lap chole
9 days ago9 days ago
Bile peritonitisBile peritonitis
Sepsis++Sepsis++ERCPERCP

1.Wait and see
2. Endoprothesis and percutaneous drain
3.Surgical exploration
Answer: 3. Surgical exploration
D9: Surgical exploration:D9: Surgical exploration:excisexcision ion of of EHBD and EHBD and mainmain biliarybiliary convergenceconvergenceDiffuse Biliary peritonitisDiffuse Biliary peritonitis

1. Peritoneal lavage and direct end to end suture
2. Peritoneal lavage and suture with T-tube insertion
3. Peritoneal lavage and hepatico-jejunal anastomosis
4.Peritoneal lavage and external biliary diversion
Clinical case : 2
Answer:
4.Peritoneal lavage and external biliary diversion