Embed Size (px)
Citation preview

Bilaterally Cleft Lip, Limb Defects, andHaematological Manifestations: Roberts SyndromeVersus TAR Syndrome
Maik Urban,1* Charlotte Opitz,2 Christiane Bommer,1 Herbert Enders,3 Sigrid Tinschert,1 andRegine Witkowski1
1Institut fur Medizinische Genetik, Universitatsklinikum Charite, Humboldt-Universitat zu Berlin, Berlin, Germany2Zentrum fur Zahnmedizin, Abteilung fur Kieferorthopadie und Orthodontie, Universitatsklinikum Charite,Humboldt-Universitat zu Berlin, Berlin, Germany
3Institut fur Anthropologie und Humangenetik, Eberhard-Karls-Universitat Tubingen, Tubingen, Germany
We report on a 13-year-old patient followedsince birth. He is the only offspring ofyoung, non-consanguineous German par-ents. His mother has an isolated left cleft oflip and a cleft palate. At birth, our patientpresented with bilaterally cleft lip/cleft pal-ate, phocomelia of upper limbs with normalhands, and mild symmetrical deficiencies ofthe long bones of the lower limbs. Haemato-logical evaluation demonstrated a leukae-moid reaction during a urinary tract infec-tion as well as intermittent thrombocytope-nia and episodes of marked eosinophiliaduring the first two years of life. Intellectualdevelopment has been normal. Comparisonwith two similar cases from the literaturesuggests a non-random phenotypic overlapof Roberts syndrome (MIM 268300) and TARsyndrome (MIM 274000). Such clinical con-stellations may be key observations to un-derstand the genetic relationship of Robertssyndrome and TAR syndrome in future phe-notype–genotype correlations. Am. J. Med.Genet. 79:155–160, 1998. © 1998 Wiley-Liss, Inc.
KEY WORDS: TAR syndrome; thrombocyto-penia absent radius syn-drome; Roberts syndrome;pseudothalidomide syn-drome; SC phocomel ia ;t h r o m b o c y t o p e n i a ;haematology
INTRODUCTION
Thrombocytopenia with radial aplasia (TAR) syn-drome and Roberts syndrome are rare autosomal re-cessive conditions. TAR syndrome comprises absent ra-dii with thumbs present and hypomegakaryocyticthrombocytopenia in patients without cleft palate. Rob-erts syndrome is characterised by facial clefts, limb de-ficiencies resulting in tetraphocomelia in most cases,and genital hyperplasia [for reviews, see Hedberg andLipton, 1988; Van Den Berg and Francke, 1993].
The basic genetic defect of these two syndromes hasnot yet been mapped or characterised. The rate of con-sanguinity is high in Roberts syndrome [Van den Bergand Francke, 1993]. In contrast, most TAR syndromepatients have non-consanguineous parents [Hall et al.,1969; Hedberg and Lipton, 1988]; consanguinity of par-ents is rare [Shalev et al., 1983; Teufel et al., 1983;Giuffre et al., 1988; Ceballos-Quintal et al., 1992].Therefore, the underlying genetic mechanism of TARsyndrome is speculated to result from compound het-erozygosity involving mutations resulting in Robertssyndrome or in Fanconi anaemia [Hall, 1987]. Alden-hoff and Waldenmaier [1979] assumed an ‘‘analogous’’relationship between Roberts syndrome, TAR syn-drome, and SC phocomelia. Interestingly, in TAR syn-drome, some families with unusual pedigree constella-tions have been observed. Hall et al. [1969] reportedTAR syndrome in a paternal aunt and uncle of theindex case. Schnur et al. [1987] found an uncle of hispatient to be affected. Edelberg et al. [1977] publisheda report of a patient whose mother had a first cousinwith two affected children. There is also an instance ofparent-to-child transmission [Ward et al., 1986]. In ad-dition, McKusick reported a case of Roberts syndromein which an aunt had the TAR syndrome [McKusick,1994]. We present a patient without mental retarda-tion, who has a phenotype between the TAR and theRoberts syndrome and compare his findings to those oftwo similar observations [Waldenmaier et al., 1978;Midro et al., 1993].
*Correspondence to: Maik Urban, UniversitatsklinikumCharite, Institut fur Medizinische Genetik, Luisenstraße 13a, D -10098 Berlin, Germany.
Received 9 July 1997; Accepted 17 November 1997
American Journal of Medical Genetics 79:155–160 (1998)
© 1998 Wiley-Liss, Inc.

CLINICAL REPORTThe propositus, a 13-year-old boy, is the only live-
born child of young, non-consanguineous parents.Mother and father are of German ancestry and were 21and 23 years old at the time of birth of this child. Hismother had a left cleft lip and a cleft palate, and hadhad 2 spontaneous abortions during the first half ofgestation. There was no history of alcohol or drug in-take, infectious illness, or maternal diabetes duringthese 3 pregnancies. This patient was delivered at termby caesarian section after an uneventful pregnancy. Hepresented with facial clefts and defects of all four limbs.He weighed 2,240 g, measured 43 cm, and had an OFCof 33 cm. The Apgar score was 4-8-9-9. In addition tothe clefts, he had silvery blond, sparse hair, a neonatalmidline facial haemangioma resolving with age, mildhypertelorism, a left lachrymal duct stenosis requiringcorrection, mildly ‘‘dysplastic’’ ear helices, hypoplasticalae nasi, an additional incisor, mandibular hypopla-sia, bilateral inguinal hernias, phimosis, a right mal-descensus testis, upper limb phocomelia, and shortnessof femora, tibiae, and fibulae. Borderline enlargementof the phallus was noted at age 7. Unfortunately, this
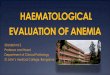
was not commented on in infancy, when it tends to bemost obvious. Testicular volumes were normal. Therewas no history of cow’s milk intolerance. Cloudy cor-neae were not present (Fig. 1).
A short rudimentary bone between the scapulae andthe hands was seen on radiographs. The hands and feetwere normal with 5 rays each. Our patient has bilat-eral hip ‘‘dysplasia,’’ varus deformity of the knees, andclubfeet. The knee deformity results from aplasia of themedial portions of the epiphyses and hypoplastic me-dial metaphyses of the upper tibiae. Fusion of the sec-ond and the third cervical vertebrae was noted on alateral skull film. A brain CT scan performed neona-tally was normal. Echocardiography and abdominal ul-trasound findings were within normal limits. Our pa-tient is of normal intelligence with average perfor-mance at school (Fig. 2). He is attending a school forphysically disabled children.
Haematological Findings
Neonatally, the boy had a leukaemoid reaction (WBC36,600/mm3 with a shift to the left), which did not re-solve despite effective treatment of an underlying uri-
Fig. 1. Continued.
156 Urban et al.

nary tract infection. Repeated blood investigationsdemonstrated intermittent thrombocytopenia (plateletcounts of 38,000/mm3, 158,000/mm3, 161,000/mm3,67,000/mm3, 96,000/mm3, in the first 2 years of life)and episodes of eosinophilia (up to 27%). There is nohistory of anaemia. A bone marrow biopsy was not car-ried out during infancy. The haematological abnormali-ties resolved with age. A recent investigation of hisperipheral blood showed a normal WBC, normal differ-ential blood count, and an almost normal platelet count(148,000/mm3). According to his parents, their sonnever had any petechiae or bleeding problems, al-though he had frequent operations in the first year oflife and several major orthopaedic procedures for cor-rection on his limbs in later infancy.
Cytogenetic Results
Neonatal prometaphase chromosome study (46,XY)demonstrated premature separation of centromeresand heterochromatin repulsion. However, at age 13,these findings had disappeared. Chromosomes of bothparents were normal. The chromosome analysis of thefoetus of his mother’s first abortion failed because ofinfection of the sample. No cytogenetic abnormalitieswere found in the prenatal cytogenetic investigation ofthe third pregnancy. Eventually the foetus was aborted
spontaneously in the 14th week of gestation. No mal-formations were seen.
DISCUSSION
Our patient has findings of the Roberts and the TARsyndrome. Phocomelia of the upper limbs and mild de-fects of the lower limbs are seen in both conditions.More severe deficiencies of the legs would suggest Rob-erts syndrome, but a few TAR patients with tetrapho-comelia have been reported [Anyane-Yeboa et al.,1985]. The presence of the thumbs despite absent radiiis a characteristic of TAR syndrome; normal or hypo-plastic thumbs were reported in all 100 cases of TARsyndrome reviewed by Hedberg and Lipton [1988]. Ab-sence of radii was present in 99 cases reviewed. How-ever, preserved thumbs and absent radii may also beseen in Roberts syndrome. Eleven cases listed in a re-view of 100 patients [Van den Berg and Francke, 1993]have this finding including one patient with thrombo-cytopenia [Waldenmaier et al., 1978]. All of these pa-tients had tetraphocomelia, a common finding in Rob-erts syndrome. Some patients (3/11) had consanguine-ous parents and affected sibs without that finding[Zergollern and Hitrec, 1982; da Silva and Bezerra,1982]. Further patients (3/11) were mentally retarded[Herrmann et al., 1969; Grosse et al., 1975; Tomkins et
Fig. 1. A: The propositus in the neonatal period. Note midline facial haemangioma, mild hypertelorism, bilaterally cleft lip, phocomelia of upper limbs.B,C: Age 7. Note facial anomalies and sparse, light hair. The size of the phallus appears to be at the upper limit of normal. Flexion contracture and varusdeformity are present at both knees. D: Age 13. Note light hair, hypoplastic alae nasi, mandibular hypoplasia, and mildly ‘‘dysplastic’’ ear helices.
Roberts Syndrome Versus TAR Syndrome 157

al., 1979]. Orofacial clefting was not present in 4 ofthese 11 patients [Herrmann et al., 1969; Lenz et al.,1974; Tomkins et al., 1979].
Fusion of the second and third vertebrae was re-ported in one of two patients with TAR syndrome, theother one having cervical spina bifida [Hall et al.,1969]. Thrombocytopenia, eosinophilia and leukaemoidreactions are cardinal manifestations of TAR-syndrome. In a TAR syndrome patient, normal intel-lectual development is to be expected. In Roberts syn-drome, mental retardation is a common, but inconstantabnormality. Remarkably, the propositus does in manyrespects resemble the JMO patient with SC phocome-lia/Roberts syndrome who did not suffer mental retar-dation either [Herrmann and Opitz, 1977; Opitz, 1982](Opitz, personal communication), although the TARsyndrome is excluded in JMO because of absence ofthumbs. However, severe facial clefts virtually rule outTAR syndrome and suggest Roberts syndrome.
Difficulty of differential diagnosis in our case is il-lustrated by data available from the literature. McKu-sick [1994] stated ‘‘The occurrence of cleft lip and pal-ate in association with skeletal changes such as absentradius suggests Roberts syndrome or SC phocomelia
rather than TAR syndrome. Clefting must be rare inTAR syndrome.’’ Hedberg and Lipton [1988] sum-marised their review of 100 patients of TAR syndrome:‘‘The dyad of thrombocytopenia and absent radii withthumbs present, and the absence of cleft palate in TAR,allows phenotypic discrimination.’’
The maternal facial cleft raises the possibility of acoincidental combination of polygenic clefts and TARsyndrome. Clearly, this cannot be ruled out. However,facial clefts were reported in relatives of patients withRoberts syndrome [Freeman et al., 1974]. Stroer [1939]assumed that facial clefting may be a heterozygousmanifestation in the family he studied. The index pa-tient was an 8-year-old boy with evident Roberts syn-drome, who was born to second cousin parents withoutfacial clefts. A younger sister of that boy had mild cleft-ing. Interestingly, bilaterally cleft lip and cleft palatewere present in the common ancestor of both parentsfour generations before the index case. In addition, afirst cousin of his mother and a niece of his father hada bilaterally cleft lip and a cleft palate [Stroer, 1939].Orofacial clefting was seen in two non-consanguineousrelatives (in a maternal uncle and in a paternal secondcousin) of a patient with well-defined TAR syndrome,including phocomelia of the upper limbs, who had noclefts [Aldenhoff and Waldenmaier, 1979].
Two reports of patients with bilaterally cleft lip, cleftpalate, virtually identical skeletal malformations butwith normal thumbs, and thrombocytopenia were pub-lished by Waldenmaier et al. [1978] and Midro et al.[1993]. The former diagnosed their patient as ‘‘Robertssyndrome with thrombocytopenia’’; the infant had aplatelet count ranging from 39,000 to 70,000/mm3,ASD, absence of gallbladder, and a horseshoe kidney.He died at 15 days because of pneumonia and enteritis.The patient of Midro et al. [1993] was evaluated at theage of 6 months. The platelet count was 42,000/mm3;bone marrow biopsy showed a decreased number ofmegacaryocytes. No penile enlargement was seen. Cy-togenetic signs of Roberts syndrome were reported tobe absent. The diagnosis suggested by Midro et al.[1993] was ‘‘TAR syndrome with orofacial clefting.’’Both groups were aware of the fact that it was virtuallyimpossible to exclude the alternative diagnosis in theirpatients. Waldenmaier et al. [1978] stated that Robertssyndrome and TAR syndrome cannot be consideredseparate entities, but only different degrees of Robertssyndrome. Midro et al. [1993] argued a coincidentaloccurrence of TAR syndrome and polygenic facial clefts.
These two cases illustrate an overlap of the Robertsand TAR syndrome similar to that seen in our patient.Clinical differentiation of the two conditions seems tobe impossible. However, in general the clinical differ-entiation is of some importance for prognostic counsel-ling, since the diagnosis of TAR syndrome usually im-plies normal intellectual development. Hall et al.[1969] reported mental retardation in 3 out of 40 TARsyndrome patients and attributed this to intracranialhaemorrhage during infancy. There is only an isolatedobservation of a brain malformation (hypoplasia of thecerebellar vermis and corpus callosum) in a patientwith TAR syndrome so far [MacDonald et al., 1994]. Itis tempting to speculate, that haematological signs
Fig. 2. An examination sheet from school. The document was given tous by our patient, who was asked for a handwritten document. Note ex-cellent handwriting and drawing of a young man with Mohawk hair style,pierced cheeks, and smoking a cigarette. Such doodles on examinationssheets are normal for a German boy of that age and, in our opinion, doreflect satisfactory social integration.
158 Urban et al.

typical of TAR syndrome in the presence of thumbsmight indicate a normal intellectual development de-spite facial clefting. However, further observations arerequired to confirm this suggestion.
In patients diagnosed as Roberts syndrome, an ex-tensive inquiry into blood results from infancy mightbe helpful in counselling the parents. The absence of ahistory of bleeding problems is not sufficient to excludeassociated haematological manifestations of TAR syn-drome. Therefore, the TAR syndrome is a diagnosis tobe considered in the famous historical patient MarcoCatone (Fig. 3). However, without having any haema-tological details it would be questionable to make anyclinical diagnosis in retrospect.
To our knowledge, our patient is the third case of thisparticular phenotype reported so far. He is virtuallythe first who grew old enough to warrant a comment onfurther intellectual development. Taking into consider-ation the two most similar patients mentioned above, acoincidental combination appears unlikely to us. Thephenotype observed in our patient may be a key obser-vation for the understanding of the genetic relationshipof Roberts syndrome and TAR syndrome in future phe-notype–genotype correlations.
ACKNOWLEDGMENTSThe authors are grateful to Prof. John M. Opitz, Uni-
versity of Utah, Salt Lake City, Utah, for his valuable
comments. The authors thank Drs. Gabriele du Bois(Leinefelde-Echterdingen), Ekkehart Weber (AsklepiosKlinik Birkenwerder), and Michael Ruland (Moglin-gen) for their kind support of this study.
REFERENCES
Aldenhoff P, Waldenmaier C (1979): Das TAR-Syndrom. In Tolksdorf M,Spranger J (eds.): ‘‘Klinische Genetik in der Padiatrie; 1. Symposium inKiel, Juli 1978.’’ Stuttgart: Thieme, pp 66–69.
Anyane-Yeboa K, Jaramillo S, Nagel C (1985): Brief clinical report: Tetra-phocomelia in the syndrome of thrombocytopenia with absent radii. AmJ Med Genet 20:571–576.
Ceballos-Quintal JM, Pinto-Escalante D, Gongora-Biachi RA (1992): TAR-like syndrome in a consanguineous Mayan girl. Am J Med Genet 43:805–807.
da Silva EO, Bezerra LHG (1982): The Roberts syndrome. Hum Genet61:372–374.
Edelberg SB, Cohn J, Brandt NJ (1977): Congenital hypomegakaryocyticthrombocytopenia associated with bilateral absence of the radius: TheTAR syndrome. Hum Hered 27:147–152.
Freeman MVR, Williams DW, Schimke RN, Temtamy SA, Vachier E, Ger-man J (1974): The Roberts syndrome. Clin Genet 5:1–16.
Giuffre L, Cammarata M, Corsello G, Vitaliti SM (1988): Two new cases ofthrombocytopenia absent radius (TAR) syndrome: Clinical, genetic andnosologic features. Klin Padiatr 200:10–14.
Grosse FR, Pandel C, Wiedemann HR (1975): The tetraphocomelia-cleftpalate syndrome. Description of a new case. Humangenetik 28:353–356.
Hall JG, Levin J, Kuhn JP, Ottenheimer EJ, Van Berkum KAP, McKusick
Fig. 3. The circus artist Marco Catone. He died in Paris in 1800 at an age of 62 years [already mentioned as phocomelic by Virchow, 1896, and others].Wiedemann diagnosed Catozze as having tetraphocomelia [Kunze and Nippert, 1986]. TAR syndrome is a possible diagnosis. Note bilateral presence ofthumbs. A: Portrait by F. Regnault in about 1775. B: Scientific figure by Vrolik [reproduced from Wepler, 1937], which is apparently a rather crude copyof Regnault’s portrait.
Roberts Syndrome Versus TAR Syndrome 159

VA (1969): Thrombocytopenia with absent radius (TAR). Medicine(Baltimore) 48:411–439.
Hall JG (1987): Thrombocytopenia and absent radius (TAR) syndrome. JMed Genet 24:79–83.
Hedberg VA, Lipton JM (1988): Thrombocytopenia with absent radii. Am JPediatr Hematol Oncol 10:51–64.
Herrmann J, Feingold M, Tuffli GA, Opitz JM (1969): A familial dysmor-phogenetic syndrome of limb deformities, characteristic facial appear-ance and associated anomalies: The ‘‘pseudothalidomide’’ or ‘‘SC syn-drome.’’ BD:OAS 5:81–89.
Herrmann J, Opitz JM (1977): The SC phocomelia and the Roberts syn-drome: Nosologic aspects. Eur J Pediatr 125:117–134.
Kunze J, Nippert I (1986): ‘‘Genetics and Malformations in Art.’’ Berlin:Grosse Verlag, p. 40.
Lenz WD, Marquardt E, Weicker H (1974): Pseudothalidomide syndrome.BD:OAS 10:97–107.
MacDonald MR, Schaefer GB, Olney AH, Patton DF (1994): Hypoplasia ofthe cerebellar vermis and corpus callosum in thrombocytopenia withabsent radius syndrome on MRI studies. Am J Med Genet 50:46–50.
McKusick VA (1994): ‘‘Mendelian Inheritance in Man. A Catalog of HumanGenes and Genetic Disorders,’’ 11th ed. Baltimore: Johns Hopkins Uni-versity Press.
Midro A, Hubert E, Preferansow J, Iwaszkiewicz-Pawlowska A (1993):TAR syndrome with orofacial clefting. Genet Counsel 4:187–192.
Opitz JM (1982): Comment [on SC phocomelia syndrome]. In PapadatosCJ, Bartsocas CS (eds): ‘‘Skeletal Dysplasias.’’ New York: Alan R. Liss,pp 357–358.
Schnur RE, Eunpu DL, Zackai EH (1987): Thrombocytopenia with absentradius in a boy and his uncle. Am J Med Genet 28:117–123.
Shalev E, Weiner E, Feldman E, Cohen H, Zuckerman H (1983): Micro-gnathia-prenatal ultrasonographic diagnosis. Int J Gynaecol Obstet21:343–345.
Stroer WFH (1939): Uber das Zusammentreffen von Hasenscharte miternsten Extremitatenmißbildungen. Erbarzt 7:101–104.
Teufel M, Enders H, Dopfer R (1983): Consanguinity in a Turkish familywith thrombocytopenia with absent radii (TAR) syndrome. Hum Genet64:94–96.
Tomkins D, Hunter A, Roberts M (1979): Cytogenetic findings in Roberts-SC phocomelia syndrome(s). Am J Med Genet 4:17–26.
Van Den Berg DJ, Francke U (1993): Roberts syndrome: A review of 100cases and a new rating system for severity. Am J Med Genet 47:1104–1123.
Virchow R (1898): Uber die Phokomelen und das Barenweib. Verh Berl GesEthnol Urgeschichte 30:55–61.
Waldenmaier C, Aldenhoff P, Klemm T (1978): The Roberts’ syndrome.Hum Genet 40:345–349.
Ward RE, Bixler D, Provisor AJ, Bader P (1986): Parent to child transmis-sion of the thrombocytopenia absent radius (TAR) syndrome. Am J MedGenet Suppl 2:207–214.
Wepler W (1937): Die sogenannte Phokomelie. Dtsch Med Wochenschr63:1302–1305.
Zergollern L, Hitrec V (1982): Four siblings with Roberts syndrome. ClinGenet 21:1–6.
160 Urban et al.