Embed Size (px)
Citation preview

Acquired Cardiovascular Disease Svensson et al
ACD
Bicuspid aortic valve surgery with proactive ascending aorta repair
Lars G. Svensson, MD, PhD,a,b Kyung-Hwan Kim, MD,a Eugene H. Blackstone, MD,a,d
Jeevanantham Rajeswaran, MSc,d A. Marc Gillinov, MD,a Tomislav Mihaljevic, MD,a
Brian P. Griffin, MD,c Richard Grimm, DO,c William J. Stewart, MD,c Donald F. Hammer, MD,c andBruce W. Lytle, MDa,b
From th
Institu
of Ca
Quan
Ohio.
Support
(to E.
Donn
Fund
cular
Disclosu
speak
cant,
Lifesc
speak
Receive
public
Address
diova
44195
0022-52
Copyrig
doi:10.1
622
Objectives: Bicuspid aortic valves are associated with aortic catastrophes, particularly dissection.We examinedwhether proactive repair of associated dilatation would reduce risk of subsequent aortic dissection or reoperationand whether more aggressive resection is needed in patients undergoing bicuspid aortic valve surgery alone.
Methods: From January 1993 to June 2003, 1989 patients (of our total experience of 4316) underwent bicuspidaortic valve surgery. Long-term outcomes of 1810 were analyzed according to aortic size and whether bicuspidaortic valve surgery was performed alone or with aortic repair.
Results: In-hospital 30-day survival was similar (98.8% valve alone vs 98.9%with aortic repair), with no penaltyincurred for concomitant aortic repair. Bicuspid aortic valve–alone patients had worse late survival (75% vs 85%at 10 years, P¼ .0001), but in the matched cohort survival was nearly identical (85% vs 86%; P ¼ .7). With thisstrategy, freedom from late aortic events was high in both groups (99% valve alone vs 97%with aortic repair at 10years; P[log-rank] ¼ .06) and similar in the matched cohort (95% vs 97%; P ¼ .2). Approximately 95% of pa-tients undergoing valve-alone surgery had aortic diameters smaller than 4.6 cm or cross-sectional area/height ratiosless than 9.4 cm2/m; 80% undergoing valve surgery plus aortic repair had diameters larger than 4.1 cm or ratiosgreater than 7.3 cm2/m. Only 0.2% of events occurred at an aortic diameter size of less than 4.5 cm.
Conclusions:Aortic size larger than 4.5 cm or aortic cross-sectional area/height ratio greater than 8 to 10 shouldbe considered triggers for concurrent aortic repair, because there is no added risk, and late survival is better;however, more aggressive resection is unwarranted. (J Thorac Cardiovasc Surg 2011;142:622-9)
Supplemental material is available online.
Bicuspid aortic valves are present in 1% to 2% of thepopulation and are associated with aortic valve stenosisand regurgitation, resulting heart failure, valve surgery atan earlier age than in those with tricuspid valves, andsuch aortic problems as coarctation of the aorta, ascending
e Department of Thoracic and Cardiovascular Surgery,a Heart and Vascular
te; the Aortic Surgery Center,b Heart and Vascular Institute; the Department
rdiovascular Medicine,c Heart and Vascular Institute; and the Department of
titative Health Sciences,d Research Institute, Cleveland Clinic, Cleveland,
ed in part by the Kenneth Gee and Paula Shaw, PhD, Chair in Heart Research
H.B), the Judith Dion Pyle Chair in Heart Valve Research (to A.M.G.), the
a and Ken Lewis Chair in Cardiothoracic Surgery and Peter Boyle Research
(to T.M.), and the John and Rosemary Brown Endowed Chair in Cardiovas-
Medicine (to B.P.G.).
res: A.M.G. receives compensation from Edwards Lifesciences (consultant,
ers bureau, significant) and from St Jude Medical (research support, signifi-
and speakers bureau, modest). T.M. receives compensation from Edwards
iences (consultant) and from Intuitive Surgical (consultant, recipient of
er fees).
d for publication Feb 25, 2010; revisions received Sept 22, 2010; accepted for
ation Oct 24, 2010; available ahead of print Feb 4, 2011.
for reprints: Lars G. Svensson, MD, PhD, Department of Thoracic and Car-
scular Surgery, Cleveland Clinic, 9500 Euclid Ave, Desk J4-1, Cleveland, OH
(E-mail: [email protected]).
23/$36.00
ht � 2011 by The American Association for Thoracic Surgery
016/j.jtcvs.2010.10.050
The Journal of Thoracic and Cardiovascular Surg
aortic aneurysm, and aortic dissection.1-8 Aortic dissection,particularly in patients with bicuspid valves, carries a highrisk of immediate death and death during emergencysurgery and is associated with considerably reduced latesurvival.1,7,9 Of those patients with acute dissection, 15%have bicuspid aortic valves.7 Among patients with bicuspidaortic valves, aortic dissection occurs in 12%with aortic di-ameter smaller than 5.0 cm,9 which is similar to the 15%prevalence seen among patients with Marfan syndromewith aortic diameter smaller than 5.0 cm.10 Indeed, whenthe ratio of aortic cross-sectional area (square centimeters)divided by height (meters) is greater than 10, risk of dissec-tion increases for both groups.9,10 Furthermore, shorterpatients are more prone to dissection at an equivalentaortic size.9,10 Timing of surgery and procedurescontinues to be debated, with some authors advocatingsurgery at an aortic size larger than 5.5 cm and others atsmaller than 4.5 cm.9-19
The aims of this study were as follows: (1) to identify dif-ferences between patients undergoing bicuspid aortic valvesurgery alone and those for whom concomitant ascendingaortic repair was performed, with particular emphasis ondetermining whether various methods of indexing aorticvalve size to body size might differentiate these groups ofpatients, and (2) to evaluate early and late risk-adjusted out-comes of patients undergoing bicuspid aortic valve surgerywith or without a proactive approach to repairing the
ery c September 2011

Abbreviations and AcronymsCI ¼ confidence intervalCT ¼ computed tomographyMRI ¼ magnetic resonance imaging
Svensson et al Acquired Cardiovascular Disease
ascending aorta. Specifically, we examined whether con-comitant repair of the ascending aorta can be done safely,whether aortic dimensions matter, how this approach influ-ences late outcome, and whether even more aggressivesurgery is needed.
ACD
MATERIALS AND METHODSFrom January 1993 to June 2003, 1989 patients underwent bicuspid aor-
tic valve surgery at ClevelandClinic (our total experiencewith bicuspid aor-
tic valves is 4316 patients, of whom 771 underwent repair); among them,
1810 preoperative echocardiograms suitable for ascending aorta measure-
ment were available (echocardiograms in which the ascending aorta was
not adequately imaged were excluded). This interval was chosen to allow
long-term follow-up and also because during this period indications for con-
comitant aortic resectionwere not clearly defined, and thus therewas greater
heterogeneity in resecting the aorta according to size. Among the 1810 pa-
tients with suitable echocardiograms, 1449 (80%) had bicuspid aortic valve
surgery alone (valve-alone group), and 361 (20%) had bicuspid aortic valve
surgery plus concomitant ascending aortic repair (valve–aorta group). As-
cending aortic procedures performed included composite valve tube graft
in 208 cases, ascending aorta tube graft in 117, and root procedure plus aor-
tic valve repair in 36. During this time, 245 patients had bicuspid aortic
valves repaired. Since then, however, the proportion of patients undergoing
repair has increased because of improved techniques and results.1,3,4,15
Mean age in the valve-alone group was 56� 15 years (range, 18–90 years),
and 76% were men; in the valve–aorta group, mean age was 54� 14 years
(range, 20–86 years), and 82% were men (Table E1).
Patient and procedure variables were entered prospectively into the
Cleveland Clinic Cardiovascular Information Registry. Use of these regis-
try data for research was approved by the Institutional Review Board, with
patient consent waived.
Echocardiographic MeasurementsIn the preoperative parasternal long-axis transthoracic echocardio-
graphic view, the ascending aorta was measured 1 to 2 cm above the sino-
tubular junction. All echocardiograms were reviewed and measured by one
of us (K.-H.K.). We were interested to see whether various methods of
indexing aortic size to height or body surface area might differentiate
between patients who had undergone valve-alone versus combined
valve–aorta operations (Table 1). Size of the ascending aorta was analyzed
in 3 ways. The first was simply its diameter, as measured echocardiograph-
ically. The second normalized the diameter and circularized area (in square
centimeters) derived from this to patient height.9,10 The third standardized
the degree of normality of ascending aorta dimension according to the body
surface area of the patient. This was expressed as a Z value, the number of
SDs that the patient’s aortic diameter deviated from mean normal
dimension (95% of normal individuals are within �2 and þ2 Z units).
Other expressions were also examined (Table E2). Routine transesophageal
echocardiography was done intraoperatively.
Computed tomography. Computed tomography (CT) and mag-
netic resonance imaging (MRI) were done only for patients with suspected
aortic aneurysm. These data were therefore not available for all patients in
this study. Nevertheless, echocardiographic imaging was available for most
The Journal of Thoracic and Ca
of the ascending aorta and aortic root and was routinely recorded, as de-
scribed in the preceding text. Among patients who had aneurysms, most un-
derwent further imaging by CTorMRI; if aneurysms were not significantly
enlarged on echocardiography, however, further imaging may not have
been performed. We therefore used echocardiography for preoperative
assessment. CT or MRI would have shown any arch or descending aorta
involvement or coarctation. Because this was a retrospective study and
patients were followed by referring physicians, routine late CT or MRI
studies were not performed.
Surgery. Valve-alone procedures were performed on the basis of patient
symptoms or evidence of left ventricular deterioration. If the predominant le-
sion was aortic valve regurgitation, then the valve was evaluated for possible
repair according to a Commissure, Leaflet, Annulus, Sinuses, Sinotubular
(CLASS) schema.3,15 The decision to perform combined valve and aorta
resection was based on aortic size and the quality of each patient’s aorta.
The quality of the aorta was subjectively assessed by surgeons based on
wall thickness, ability to hold sutures, and whether a potential dissection
plane was visible in the media. During this period, the approach to repair
the aorta was heterogeneous and was based on the judgment of the
surgeon. This gives strength to the study in that no specific cutoff point
was used. Although many patients had ascending aorta tube grafts, if the
root was enlarged substantially, a composite valve graft was inserted or an
aortic root remodeling or modified David reimplantation procedure was
performed.3,4,8,13,15 A minimally invasive incision was preferred for both
valve-alone and combined valve–aorta repairs. The typical repair technique
for bicuspid valves was placement of Cabrol sutures at the commissures,
plication of clefts, release of raphe, and leading-edge figure-of-8 sutures,
as described previously.15
OutcomesOutcomes considered were in-hospital mortality, long-term events re-
lated to the ascending aorta, and long-term all-cause mortality. Patients
were followed up systematically at 2-year intervals, supplemented by
a cross-sectional follow-up by Institutional Review Board–approved mailed
questionnaire or telephone interview requiring patient consent, with empha-
sis on assessing events related to the aorta, including ascertaining mode of
death. Mean follow-up was 5.9 � 3.6 years for the valve-alone group and
6.7 � 3.6 years for the valve–aorta group, with 10% followed up longer
than 11 years; 8550 and 2411 patient-years of data were available for
analysis, respectively. Data on vital status were augmented with the Social
Security Death Index,20,21 yielding mean follow-up for vital status of 9.2
� 4.0 years for the valve-alone group and 9.0� 3.4 years for the valve–aorta
group. Seventy-five patients (4.1%) were unavailable for follow-up, and all
were checked for death with the Social Security Death Index.
Data AnalysisDifferences between valve-alone and valve–aortapatients. Data analysis first addressed dissimilarities between the
valve-alone and valve–aorta groups (Table E1), so that comparisons of out-
come were fair. Briefly, multivariable logistic regression analysis was used
to identify a parsimonious set of patient and procedure variables associated
with combined valve and aorta surgery versus valve surgery alone. Bagging
was used for variable selection (see Appendix for variables considered),22
with automated analysis of 1000 bootstrap samples and a P value for reten-
tion of .05. Frequency of occurrence of individual factors or clusters of
highly correlated factors in these analyses was counted (aggregation
step), and factors appearing in 50% or more of the analyses were consid-
ered reliably statistically significant at P� .05. To this parsimonious model
were added nonsignificant variables representing groups of patient, coro-
nary disease, valve pathology, and surgical procedure variables that might
be related to unrecorded selection factors (saturated propensity model).23
Because preoperative diagnostic aneurysm and dilated aorta variables act
as surrogates for group membership, they were not included in the
rdiovascular Surgery c Volume 142, Number 3 623

TABLE 1. Factors associated with higher likelihood of undergoing
bicuspid aortic valve surgery and ascending aorta repair
Factor Estimate ± SE P Reliability (%)*
Larger ascending aorta
diametery�21 � 1.3 <.0001 100
Emergency operation 1.9 � 0.59 .001 77
No LCx disease �0.63 � 0.19 .0008 95
Lower AV stenosis grade �0.15 � 0.033 <.0001 87
Nonsevere LV dysfunctionz �0.023 � 0.010 .02 54
More recent date of
operation
0.13 � 0.029 <.0001 93
AV, Aortic valve; LCx, left circumflex; LV, left ventricular; SE, standard error.
*Percentage of times factor appeared in 1000 bootstrap models. y(Height/diameter),
inverse transformation. Ascending aortia diameter normalized by patient height.
z(LV dysfunction grade)2, squared transformation.
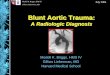
FIGURE 1. Cumulative distribution of ascending aorta size at bicuspid
aortic valve surgery. Vertical axis represents nonparametric percentile;
thus, the value for ascending aorta diameter at the 50% point on the vertical
axis is the median value (50th percentile), the values at 10% and 90% are
the 10th and 90th percentiles, and so forth. A, Diameter. B, Area/height
ratio. BAV, Bicuspid aortic valve surgery alone; BAVþAo, bicuspid aortic
valve surgery and ascending aorta repair.
Acquired Cardiovascular Disease Svensson et al
ACD
propensity model. Using this saturated model, a propensity score was cal-
culated for each patient (C ¼ .90).
Propensity matching. Using only the propensity score, patients from
the valve–aorta group were matched 1:1 with patients from the valve-alone
group with a greedy matching strategy. Patients in the valve–aorta group
whose propensity scores deviated more than approximately 0.2 from those
of patients in the valve-alone group were considered unmatched; 206 well-
matched pairs (57%) were obtained.
Comparison of early outcomes. Because there were few in-
hospital deaths or strokes, we performed focused logistic regression analysis
with treatment group and ascending aorta size variables included in the
model, along with propensity score, as covariables for risk adjustment.24
Comparison of time-related outcomes. Freedom from long-
term events related to the ascending aorta and survival estimates were ob-
tained using the Kaplan–Meier nonparametric method. A parametric
method was used to resolve the number of phases of instantaneous risk
(hazard function) and to estimate shaping parameters.25 (For additional
details, see http://my.clevelandclinic.org/professionals/software/hazards/
default.aspx.) Because this was a retrospective study, patients who had val-
vular disease alonewould have been followed up only by echocardiography
unless there was evidence of aneurysmal formation. Longitudinal CT or
MRI data were therefore not available for following any potential aortic
growth other than those detected by echocardiography or incidental CT
or MRI that in turn resulted in referral for reoperation.
Data PresentationContinuous variables are summarized as mean� SD, or equivalently as
15th, 50th, (median), and 85th percentiles when the distribution of values
was skewed. Categoric variables are summarized as frequencies and per-
centages. Continuous variables were compared using the Wilcoxon rank-
sum test. Categoric variables were compared using the c2 test when the
smallest number of individuals in a category was more than 5 and with
Fisher’s exact test otherwise. Freedom from events related to ascending
aorta and survival estimates are accompanied by asymmetric 68% confi-
dence limits, equivalent to � 1 SE.
RESULTSDifferences Between Valve-Alone and Valve–AortaPatients
Patients in the valve–aorta group were more likely thanthose in the valve-alone group to undergo emergencysurgery and were less likely to have circumflex coronary
624 The Journal of Thoracic and Cardiovascular Surg
artery disease, aortic valve stenosis, or left ventricular dys-function. They were operated on more frequently and hadlarger aortic diameters (with similar C-statistics for aorticdiameter or area normalized to height [C¼ .86] or standard-ized to Z value [C ¼ .85]; Table 1).
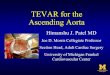
Heterogeneity of decision making resulted in wide over-lap of ascending aorta size, however expressed (Figure 1,Table E2). Nevertheless, patients with aortic diameterslarger than 4.2 cm frequently underwent aortic replacement(Figure 1, A), and at approximately 4.7 cm, 100% hadreplacement. Similarly, at an aortic cross-sectional area/height ratio of 8 to 9 cm2/m, the aorta was increasingly re-placed; at a value of 10, virtually all patients underwent aor-tic replacement (Figure 1, B). Above a Z value ofþ5, theaorta was increasingly replaced; above þ8, nearly 100%were replaced (Figure E1).
ery c September 2011

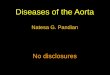
FIGURE 2. Nonparametric Kaplan–Meier estimates of freedom from
events related to ascending aorta. Note that vertical axis is greatly ex-
panded, from 90% to 100%. Each circle represents an aortic event after
bicuspid aortic valve repair alone; each square represents an aortic event
after combined valve–aorta procedure, positioned along vertical axis by
Kaplan–Meier estimator. Vertical bars represent � 1 SE, and numbers in
parentheses designate patients remaining at risk. A, Whole cohort. B,
Matched cohort. BAV, Bicuspid aortic valve surgery alone (circles); BAVþAo, bicuspid aortic valve surgery and ascending aorta repair (squares).
Svensson et al Acquired Cardiovascular Disease
ACD
Hospital Mortality and MorbidityUnadjusted hospital mortality was 1.1% (CL, 0.58%–
2.0%) for the valve–aorta group versus 1.2% (CL, 0.95%–1.6%, P>.9) for the valve-alone group. Risk of stroke wassimilar at 1.7% and 1.3%, respectively (P ¼ .6). There wasno statistically significant difference between groups with re-spect to return to the operating room for bleeding, myocardialinfarction, or renal failure (Table E3).
In propensity-matched patients, mortality and morbidityfigures were similar for both groups (P>.9). Propensity-adjusted analysis corroborated this, showing that neitherascending aorta surgery nor ascending aorta diameter influ-enced in-hospital death or risk of stroke (Table E4).
Follow-up Events Related to Ascending AortaOn follow-up, there were 14 events related to the aorta, 8
in the valve-alone group and 6 in the valve–aorta group.
The Journal of Thoracic and Ca
Valve-alone group (n¼ 1449) events were (1) 1 reoperationfor aortic dissection at 14 days, (2) 1 death from aortic dis-section 4.1 months after the patient refused reoperation,(3) 1 dissection reoperated 2.3 years after surgery, (4) 1 distalaortic aneurysm at 4.6 years, (5) 1 reoperation for ascendingaorta aneurysm at 5.5 years, (6) 1 root aneurysm at 6.3 years,(7) 1 root aneurysm at 6.4 years, and (8) 1 dilated ascendingaorta at 11.5 years. Aortic diameters, cross-sectional area/height ratios, and Z values before surgery were 4.6 cm, 5.2cm, 4.0 cm, 4.8 cm, 4.7 cm, 3.1 cm, 6.0 cm, and 4.2 cm;9.1 cm2/m, 14 cm2/m, 7.0 cm2/m, 9.7 cm2/m, 9.9 cm2/m,4.8 cm2/m, 16 cm2/m, and 7.8 cm2/m; and 6.4, 9.0, 5.3,6.1, 6.5, 3.7, 9.4, and 6.1 Z, respectively. Thus, for thevalve-alone group, nonparametric Kaplan–Meier estimatesof freedom from aortic events at 1, 5, and 10 years were, re-spectively, 99.8%, 99.7%, and 99%. Of note, only 3 of 1449patients (0.2%) in the valve-alone group had aortic eventsafter operation at an aortic diameter smaller than 4.5 cm.In the valve–aorta group (n¼ 361), aortic events were (1)
1 death from aortic dissection at 2 days, (2) 1 death fromdissection beyond an allograft 14 days after surgery, (3) 1reoperation for root aneurysm 2.4 years later, (4) 1 reopera-tion for root aneurysm 3.5 years later, (5) 1 reoperation forroot aneurysm 4.7 years later, and (6) 1 reoperation for di-lated aorta 9.5 years later. Aortic diameters, cross-sectional area/height ratios, and Z values before surgerywere 6.0 cm, 4.9 cm, 5.2 cm, 3.6 cm, 4.5 cm, and 3.2 cm;15 cm2/m, 12 cm2/m, 13 cm2/m, 5.6 cm2/m, 8.8 cm2/m,and 4.5 cm2/m; and 8.5, 9.1, 8.6, 4.1, 5.9, and 2.5 Z, respec-tively. Of note, only 3 patients developed a root aneurysm,and only 1 underwent reoperation for late arch aneurysm.Thus, for this latter group, nonparametric Kaplan–Meierestimates of freedom from aortic events at 1, 5, and 10 yearswere, respectively, 99.4%, 98.4%, and 97.1%. Risk-unadjusted comparison shows that patients in the valve–aorta group were somewhat more likely to have aorticevents than were those in the valve-alone group (P[log-rank] ¼ .06; Figure 2, A). Matched comparison, however,shows freedom from ascending aorta–related events to besimilar (P[log-rank] ¼ .2; Figure 2, B). Thus, based onthe decision making described, reintervention on the aortawas rare for both groups. That is, later reoperation for aneu-rysm repair was rare for valve-alone procedures, and falseaneurysms or late complications were also rare for com-bined valve–aorta procedures.
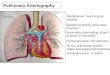
Long-Term SurvivalRisk-unadjusted survival after combined valve–aorta
procedures was better (85% 10-year survival) than aftervalve-alone surgery (75% 10-year survival, P[log-rank] ¼ .0001; Figures 3, A, and E2), probably because ofmore severe symptoms in thevalve-alone patients, associatedwith more severe aortic valve stenosis andworse left ventric-ular function (Tables 1 and E1). For the propensity-matched
rdiovascular Surgery c Volume 142, Number 3 625

FIGURE 3. Survival for both groups. Format is as in Figure 2. Solid lines
are parametric estimates enclosed within 68% confidence limits. A, Whole
cohort. B, Matched cohort. BAV, Bicuspid aortic valve surgery alone
(circles); BAVþAo, bicuspid aortic valve surgery and ascending aorta re-
pair (squares).
Acquired Cardiovascular Disease Svensson et al
ACD
cohort of 206 patients in each group, however, risk-adjustedsurvival was nearly identical (10-year survival 86% vs85% and 15-year survival 74% vs. 79%, respectively, P[log-rank] ¼ .6; Figure 3, B), including for ventricular dys-function.An important caveat is that propensitymatching ad-justed for preoperative symptoms, aortic valve disease, andventricular dysfunction differences. There were no differ-ences in survival or aortic complications according to repairor replacement of the valve, root procedure, or valve type(mechanical vs biologic).
DISCUSSIONPrincipal Findings
This study evaluated patients operated on during a periodwhen no strict guidelines existed concerning when to resectthe ascending aorta during bicuspid aortic valve procedures.Hence, there were some intersurgeon differences in the ap-proach to management of a dilated aorta that resulted ina spectrum of procedures based on the initial diameter.Our results thus show that at an absolute diameter of 4.5cm or greater or a cross-sectional area/height ratio higherthan 8 cm2/m, the aorta can be safely resected without
626 The Journal of Thoracic and Cardiovascular Surg
added penalty. However, the recent trend of recommendingmore aggressive resection of the aorta when smaller than4.5 cm, or concurrently the aortic root, or electively the aor-tic arch, cannot be justified on the basis of this study. In-deed, only 1 patient with aortic diameter smaller than 4.5cm required reoperation for aortic dissection. We thereforecannot justify the added risks of root resection with coro-nary reimplantation, or aortic arch resection with circula-tory arrest and no concurrent significant aneurysmaldilatation beyond 4.5 cm. Of interest, this study has alsoshown pari passu that patients operated on under currentvalve guidelines when they start to show symptoms orhave developed left ventricular dysfunction have poorerlate survival than less symptomatic patients (valve–aortagroup). This raises the issue of whether severe bicuspidvalve disease, as with mitral valve disease, should be ad-dressed before development of symptoms or left ventriculardysfunction.
Bicuspid aortic valve is among the most common con-genital cardiac defects.7 In this study, it was associatedwith aortic dilatation requiring proactive repair in 20% ofpatients. As the general population ages, aortic disease, in-cluding dissection and aneurysmal disease, is becomingmore common, contributing to 43,000 to 47,000 deathsannually in the United States.6 Earlier treatment of aorticdilatation has therefore become paramount in preventingaortic dissection and aneurysmal complications.
We have for a number of years proactively and aggres-sively resected and repaired aortic dilatation associatedwith bicuspid valves, but not typically at diameters smallerthan 4.5 cm. In this study, every patient with an aortic diam-eter greater than 6.1 cm underwent repair. Indeed, 83% ofthose patients with a diameter greater than approximately4.8 cm underwent repair (Figure 1, A). Similarly, we as-sessed aortic cross-sectional area/height ratio to indicatewhen surgery is required for a dilated aorta in patientswith bicuspid valves or Marfan syndrome.9,10 We notedthat approximately 95% of those who did not undergo anaortic procedure had a ratio less than 9.4 cm2/m, whereas80% of those who underwent ascending aortic repair hada ratio greater than 7.3 cm2/m. Likewise, about 95% ofpatients who did not have an aortic procedure had a Zvalue less than 6.9, whereas 80% of those who underwentascending aortic repair had a Z value greater than 5.3.
Because the aorta increases in diameter with somaticgrowth, interpretation of measurements has been facilitatedby normalizing it to height or body surface area (eg, indexedarea, Z value). Indexing aortic size to these anthropomor-phic data suggests that the cross-sectional area/height ratiodiscriminates rather well those patients who need concur-rent aortic repair. Furthermore, this ratio also takes into ac-count the greater risk of dissection in shorter patients. Weencourage the use of this ratio for timing surgery in patientswith bicuspid aortic valves or Marfan syndrome.9,10
ery c September 2011

Svensson et al Acquired Cardiovascular Disease
ACD
Currently, for patients without symptoms, we use a ratiogreater than 10 cm2/m.
With this proactive approach, 10-year freedom from as-cending aortic events was 97.1% for the valve–aorta groupversus 99% for the valve-alone group, clearly a low risk. In-deed, when we saw these results, we rechecked all patients’late outcomes to ensure that no complication had beenmissed. Although we see patients from our larger experi-ence who occasionally return for reoperation on either theaortic root or arch, this is uncommon unless aortic dissec-tion was present at the index operation. Similarly, we seepatients who have been operated on elsewhere; the denom-inator in this case is unknown, however, although with 1%to 2% of the population having bicuspid valves, it is likelylarge. Of note, in 2004, after the period of this study, Borgerand colleagues1 recommended that ascending aorta replace-ment be used more often, because in their series 22 patientsdeveloped long-term complications related to the ascendingaorta, particularly those in whom the aorta was greater than4.5 cm. Fifteen-year freedom from complications was 43%,81%, and 86% for aortic diameters of 4.5 to 4.9 cm, 4.0 to4.5 cm, and smaller than 4.0 cm, respectively (P<.001).Our study supports their hypothesis that proactive repairof the aorta, particularly when larger than 4.5 cm in diame-ter, reduces late risk of complications.
Reducing late complications related to aortic dilatation,however, would not be justified if doing so carried anincreased early risk of death, stroke, or other serious com-plications related to surgery. We therefore used severalmethods, including propensity adjustment and propensitymatching, to identify risk-adjusted differences in surgicalrisk between the groups. Despite this careful and detailedanalysis, we found no statistically significant difference inearly deaths or complications. Furthermore, the approxi-mate 99% survival and 1.5% postoperative occurrence ofstroke were gratifyingly good in both groups. There isthus no specific penalty (ie, increase in risk) associatedwith concomitant repair of the aorta.
On late follow-up, patients in the valve–aorta group hadbetter non–risk-adjusted survival than did those in thevalve-alone group. One likely explanation is that thevalve-alone patients had more symptomatic aortic valvedisease, either stenosis or regurgitation, resulting in symp-toms as an indication for surgery, and worse left ventricularfunction (Tables 1 and E2). This raises the interesting issueof whether earlier surgery for significant but asymptomaticaortic valve disease might result in better long-term sur-vival. Surgery should therefore be considered in young pa-tients with severe valvular disease even if they show neithersymptoms nor marked left ventricular dysfunction or dilata-tion. After propensity matching, the difference in long-termsurvival was not statistically significant for the 206 matchedpatient pairs. However, this propensity matching balancedsymptoms, aortic stenosis or regurgitation, and left ventric-
The Journal of Thoracic and Ca
ular dysfunction and specifically addressed whether aorticrepair affected survival. This matched analysis showedthat addition of aortic repair did not negatively affect sur-vival. Indeed, this would not be expected, unless perhaps re-lated to a risk of false aneurysms or graft infection, butneither occurred. Current American College of Cardiol-ogy/American Heart Association guidelines for aortic valvesurgery are essentially based on symptoms or measures ofleft ventricular dysfunction14; the issue of asymptomatic se-vere aortic valve disease and earlier surgery will need to beaddressed during further guideline iterations.
LimitationsThis was a clinical cohort study and not a randomized
trial. A randomized trial would be difficult because of thecontinuous nature of aortic diameter. We did, however,use various methods to analyze the data and provide a faircomparison. We found no disadvantage to concomitant as-cending aorta repair. Aortic diameter data were not col-lected prospectively; nevertheless, one of us (K.-H.K.)retrieved and reviewed every preoperative echocardiogramthat did not give precise aortic diameters. Postoperativefollow-up imaging of the aorta was not performed on a rou-tine schedule with CT or MRI, and echocardiography wasperformed at the referring cardiologist’s discretion.
RecommendationsSurgical options (based on 771 repairs) depend on the sur-
geon’s experience, but in our opinion, a regurgitant bicuspidvalve should be repaired, and if the ascending aorta is alsosignificantly dilated (diameter larger than 4.5 cm or aorticcross-sectional area/height ratio greater than 10 cm2/m), itshould be replaced.1-5,8,11,13-17,19 This study shows thatfailure to do so is associated with an increased risk of lateaortic complications, particularly aortic dissection. If theroot is enlarged, a remodeling root-sparing operation is pre-ferred, because often these are young patients in whom bio-logic valves soon fail, and mechanical valves requirelifelong anticoagulation.3,13,15,19 In our experience, 10-year freedom from reoperation for bicuspid valve repairranges from 79% to 83% for valve-alone procedures andis 91% for combined valve–aorta procedures, slightly lessthan for tricuspid valve repair and root-sparing or root-preserving procedures (96% at 10 years).3,4,11,13,15,19 Forpatients with aortic valve stenosis, the valve will requirereplacement because attempted decalcification proceduresfail within a few years.Proactive aortic repair is recommended at the time of bi-
cuspid aortic valve surgery when either the aortic diameterexceeds approximately 4.5 cm, the aortic cross-sectionalarea/height ratio exceeds approximately 8 to 9 cm2/m, orthe Z value exceeds 7. For patients with a bicuspid valvenot requiring surgery, we recommend aortic repair whenthe aortic cross-sectional area/height ratio exceeds 10
rdiovascular Surgery c Volume 142, Number 3 627

Acquired Cardiovascular Disease Svensson et al
ACD
cm2/m. Our data do not currently justify resecting the aortaif it is smaller than 4.5 cm. Consideration should be given tostress testing patients with severe bicuspid valve diseasebefore the development of symptoms or left ventricular dys-function, because left ventricular mass exceeding 180 g/m2
or a left atrium exceeding 4.5 cmmay be better predictors oflate survival than are symptoms. Furthermore, patientsshould be followed long term, preferably byMRI (to reducethe risks of CT-related radiation), for late development ofaneurysm, particularly of the aortic arch.26
References1. Borger MA, Preston M, Ivanov J, Fedak PW, Davierwala P, Armstrong S, et al.
Should the ascending aorta be replaced more frequently in patients with bicuspid
aortic valve disease? J Thorac Cardiovasc Surg. 2004;128:677-83.
2. Sundt TM III, Mora BN, Moon MR, Bailey MS, Pasque MK, Gay WA Jr.
Options for repair of a bicuspid aortic valve and ascending aortic aneurysm.
Ann Thorac Surg. 2000;69:1333-7.
3. Svensson LG, Blackstone EH, CosgroveDM III. Surgical options in young adults
with aortic valve disease. Curr Probl Cardiol. 2003;28:417-80.
4. Svensson LG, Blackstone EH, Feng J, de Oliveira D, Gillinov AM,
ThamilarasanM, et al. AreMarfan syndrome andmarfanoid patients distinguish-
able on long-term follow-up? Ann Thorac Surg. 2007;83:1067-74.
5. Svensson LG, Kim KH, Blackstone EH, Alster JM, McCarthy PM,
Greenberg RK, et al. Elephant trunk procedure: newer indications and uses.
Ann Thorac Surg. 2004;78:109-16.
6. Svensson LG, Rodriguez ER. Aortic organ disease epidemic, and why do
balloons pop? Circulation. 2005;112:1082-4.
7. Braverman AC, G€uven H, Beardslee MA, Makan M, Kates AM, Moon MR. The
bicuspid aortic valve. Curr Probl Cardiol. 2005;30:470-522.
8. Svensson LG. Sizing for modified David’s reimplantation procedure.Ann Thorac
Surg. 2003;76:1751-3.
9. Svensson LG, Kim KH, Lytle BW, Cosgrove DM. Relationship of aortic
cross-sectional area to height ratio and the risk of aortic dissection in patients
with bicuspid aortic valves. J Thorac Cardiovasc Surg. 2003;126:892-3.
10. Svensson LG, Khitin L. Aortic cross-sectional area/height ratio timing of aortic
surgery in asymptomatic patients with Marfan syndrome. J Thorac Cardiovasc
Surg. 2002;123:360-1.
11. Casselman FP, Gillinov AM, Akhrass R, Kasirajan V, Blackstone EH,
Cosgrove DM. Intermediate-term durability of bicuspid aortic valve repair for
prolapsing leaflet. Eur J Cardiothorac Surg. 1999;15:302-8.
12. Svensson LG, Labib SB, Eisenhauer AC, Butterly JR. Intimal tear without hema-
toma: an important variant of aortic dissection that can elude current imaging
techniques. Circulation. 1999;99:1331-6.
13. Svensson LG, Longoria J, Kimmel WA, Nadolny E. Management of aortic valve
disease during aortic surgery. Ann Thorac Surg. 2000;69:778-84.
628 The Journal of Thoracic and Cardiovascular Surg
14. Bonow RO, Carabello BA, et al, American College of Cardiology/American
Heart Association Task Force on Practice Guidelines, Society of Cardiovascular
Anesthesiologists, Society for Cardiovascular Angiography and Interventions,
Society of Thoracic Surgeons. ACC/AHA 2006 guidelines for the management
of patients with valvular heart disease: a report of the American College of Car-
diology/American Heart Association Task Force on Practice Guidelines (writing
committee to revise the 1998 Guidelines for the Management of Patients With
Valvular Heart Disease): developed in collaboration with the Society of Cardio-
vascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiog-
raphy and Interventions and the Society of Thoracic Surgeons: developed in
collaboration with the Society of Cardiovascular Anesthesiologists: endorsed
by the Society for Cardiovascular Angiography and Interventions and the Society
of Thoracic Surgeons. Circulation. 2006;114:e84-231.
15. Svensson LG, Deglurkar I, Ung J, Pettersson G, Gillinov AM, D’Agostino RS,
et al. Aortic valve repair and root preservation by remodeling, reimplantation,
and tailoring: technical aspects and early outcome. J Card Surg. 2007;22:
473-9.
16. Burkhart HM, Zehr KJ, Schaff HV, Daly RC, Dearani JA, Orszulak TA. Valve-
preserving aortic root reconstruction: a comparison of techniques. J Heart Valve
Dis. 2003;12:62-7.
17. Miller DC. Valve-sparing aortic root replacement in patients with the Marfan
syndrome. J Thorac Cardiovasc Surg. 2003;125:773-8.
18. Svensson LG. Acute aortic syndromes: time to talk of many things. Cleveland
Clin J Med. 2008;75:25-69.
19. Svensson LG, Crawford ES, Hess KR, Coselli JS, Safi HJ. Composite valve graft
replacement of the proximal aorta: comparison of techniques in 348 patients. Ann
Thorac Surg. 1992;54:427-39.
20. Boyle CA, Decoufl�e P. National sources of vital status information: extent of
coverage and possible selectivity in reporting. Am J Epidemiol. 1990;131:
160-8.
21. Newman TB, Brown AN. Use of commercial record linkage software and vital
statistics to identify patient deaths. J Am Med Inform Assoc. 1997;4:233-7.
22. Breiman L. Bagging predictors. Machine Learning. 1996;24:123-40.
23. Blackstone EH. Comparing apples and oranges. J Thorac Cardiovasc Surg. 2002;
123:8-15.
24. Drake C, Fisher L. Prognostic models and the propensity score. Int J Epidemiol.
1995;24:183-7.
25. Blackstone EH, Naftel DC, Turner ME Jr. The decomposition of time-varying
hazard into phases, each incorporating a separate stream of concomitant informa-
tion. J Am Stat Assoc. 1986;81:615-24.
26. Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE Jr. et al.
2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for
the diagnosis and management of patients with Thoracic Aortic Disease: a re-
port of the American College of Cardiology Foundation/American Heart Asso-
ciation Task Force on Practice Guidelines, American Association for Thoracic
Surgery, American College of Radiology, American Stroke Association, Soci-
ety of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiogra-
phy and Interventions, Society of Interventional Radiology, Society of
Thoracic Surgeons, and Society for Vascular Medicine. Circulation. 2010;
121:e266-369.
ery c September 2011

Svensson et al Acquired Cardiovascular Disease
APPENDIX. Variables Used in Propensity Model
Patient VariablesDemography. Age (years), sex, ethnicity, weight (kilo-grams), height (centimeters), body surface area (squaremeters), body mass index (kilograms per squaremeter)Symptoms. New York Heart Association functional class(I–IV), emergency operationVentricular dysfunction. Previous myocardial infarction,degree of left ventricular dysfunction (1, none; 2, mild; 3,mild to moderate; 4, moderate; 5, moderately severe; 6,severe)Valve pathology. Aortic valve regurgitation, aortic valvestenosis, tricuspid valve regurgitation, mitral valve regurgi-tationAscending aorta. Diameter (centimeters) and its normal-ized and standardized derivatives (diameter/height[centimeters per meter], diameter/body surface area [centi-meters per square meter], area [square centimeters], area/height [square centimeters per meter], area/body massindex [square centimeters], area/body surface area [squarecentimeters per square meter], Z value)
The Journal of Thoracic and Ca
Coronary anatomy. Left main trunk disease (percentagestenosis), left anterior descending coronary artery systemdisease (maximum percentage stenosis), right coronaryartery system disease (maximum percentage stenosis), leftcircumflex coronary artery system disease (maximumpercentage stenosis)Other cardiac comorbidity. Atrial fibrillation, hyperten-sion, history of cardiac disease, complete heart block/pacer,ventricular arrhythmiaNoncardiac comorbidity. Treated diabetes, insulin-treated diabetes, history of endocarditis, history of periph-eral arterial disease, history of smoking, carotid disease,popliteal disease, creatinine (milligrams per deciliter),blood urea nitrogen (milligrams per deciliter), bilirubin(milligrams per deciliter), creatinine clearance (millilitersper minute), hematocrit (percentage)Experience. Date of operation (years since January 1, 1995)
Procedure VariablesSurgery type. Coronary artery bypass grafting, mitralvalve repair, mitral valve replacement, aortic valve repair,aortic valve replacementProcedure. Internal thoracic artery graft used
rdiovascular Surgery c Volume 142, Number 3 629
ACD

FIGURE E1. Cumulative distribution of ascending aorta size at bicuspid
aortic valve surgery: Z value. Vertical axis represents nonparametric per-
centile; thus, the value for ascending aorta diameter at the 50% point on
the vertical axis is the median value (50th percentile), the values at 10%
and 90% are the 10th and 90th percentiles, and so forth. BAV,Bicuspid aor-
tic valve surgery alone;BAVþAo, bicuspid aortic valve surgery and ascend-
ing aorta repair.
FIGURE E2. Instantaneous risk of death (hazard function) enclosed
within 68% confidence limits. A, Whole cohort. B, Matched cohort.
BAV, Bicuspid aortic valve surgery alone; BAVþAo, bicuspid aortic valve
surgery and ascending aorta repair.
Acquired Cardiovascular Disease Svensson et al
629.e1 The Journal of Thoracic and Cardiovascular Surgery c September 2011
ACD

TABLEE1. Patient characteristics, procedure details, and length of stay information for patients undergoing bicuspid aortic valve surgery with or
without ascending aorta repair
BAV alone (n ¼ 1449) BAV plus aorta (n ¼ 361)
Variable N* Value N* Value P
Demographic data
Age (y, mean � SD) 1449 56 � 15 361 54 � 14 .001
Female (no.) 1449 353 (24%) 361 66 (18%) .01
Height (cm, mean � SD) 1445 173 � 10 361 176 � 10 <.0001
Body surface area (m2, mean � SD) 1445 2.01 � 0.25 361 2.1 � 0.24 .002
Clinical acuity
New York Heart Association functional class (no.) 1449 361 <.0001
I 242 (17%) 105 (29%)
II 853 (59%) 191 (53%)
III 252 (17%) 49 (14%)
IV 102 (7.0%) 16 (4.4%)
Emergency operation (no.) 1449 13 (0.9%) 361 13 (3.6%) .0001
Cardiac comorbidity
AV regurgitation grade (no.) 1416 356 <.0001
None 328 (23%) 48 (13%)
Mild 258 (18%) 41 (12%)
Moderate 224 (16%) 61 (17%)
Moderately severe 174 (12%) 71 (20%)
Severe 432 (30%) 135 (38%)
AV stenosis grade (no.) 1331 350 <.0001
None 369 (28%) 157 (45%)
Mild 33 (2.5%) 15 (4.3%)
Mild to moderate 6 (0.45%) 2 (0.57%)
Moderate 60 (4.5%) 28 (8.0%)
Moderately severe 67 (5.03%) 23 (6.6%)
Severe 796 (60%) 125 (36%)
Previous cardiac operation (no.) 1449 174 (12%) 361 47 (13%) .6
Aortic disease (no.)
Preoperative diagnosis of aortic aneurysm 1449 27 (1.9%) 361 239 (66%) <.0001
Marfan syndrome 1449 2 (0.14%) 361 8 (2.2%) <.0001
Dilated aorta 1449 510 (35%) 361 277 (77%) <.0001
Aortic dissection 1449 2 (0.14%) 361 24 (6.6%) <.0001
Noncardiac comorbidity
Smoking (no.) 1428 749 (52%) 352 177 (50%) .5
Peripheral arterial disease (no.) 1449 329 (23%) 361 62 (17%) .02
Carotid artery disease (no.) 1449 295 (20%) 361 54 (15%) .02
Chronic obstructive pulmonary disease (no.) 1133 232 (20%) 327 51 (16%) .05
Treated diabetes (no.) 1391 127 (9.1%) 352 26 (7.4%) .3
Renal disease (no.) 1449 44 (3.04%) 361 6 (1.7%) .2
Creatinine (mg/dL, mean � SD) 1406 1.1 � 0.69 354 1.1 � 1.05 .1
Procedure
Hemiarch (no.) 1449 1 (0.07%) 361 32 (8.9%) <.0001
Arch (no.) 1449 0 (0%) 361 10 (2.8%) <.0001
AV repair (no.) 1449 206 (14%) 361 39 (11%) .09
AV replacement (no.) 1449 1243 (86%) 361 322 (89%) .09
Mechanical valve 200 (16%) 68 (21%) .03
Biologic valve 1004 (81%) 250 (78%) .2
Unknown 39 (3%) 4 (1.2%) .08
Mitral valve repair (no.) 1449 102 (7.04%) 361 17 (4.7%) .1
Coronary artery bypass grafting (no.) 1449 397 (27%) 361 76 (21%) .01
Myocardial ischemic time (min, mean � SD) 1447 74 � 34 361 90 � 35 <.0001
Cardiopulmonary bypass time (min, mean � SD) 1448 98 � 45 361 119 � 49 <.0001
(Continued)
Svensson et al Acquired Cardiovascular Disease
The Journal of Thoracic and Cardiovascular Surgery c Volume 142, Number 3 629.e2
ACD

TABLE E1. Continued
BAV alone (n ¼ 1449) BAV plus aorta (n ¼ 361)
Variable N* Value N* Value P
Length of stay (dy)Intensive care unit 1446 1/1/3 361 1/1/3 .05
Postoperative 1449 4/6/9 361 5/6/9.9 .004
Total 1449 4/6/13 361 5/7/12 .1
BAV, Bicuspid aortic valve; AV, aortic valve. *Patients with data available. yData shown as 15th, 50th, and 85th percentiles.
TABLE E2. Ascending aorta size at time of bicuspid aortic valve surgery with or without ascending aorta repair
BAV alone (n ¼ 1449) BAV plus aorta (n ¼ 361)
Variable Mean ± SD 15th/50th/85th Percentiles Mean ± SD 15th/50th/85th Percentiles P
Diameter (cm) 3.6 � 0.59 3/3.6/4.2 4.8 � 0.94 3.9/4.8/5.6 <.0001
Diameter/height (cm/m)* 2.1 � 0.34 1.76/2.08/2.43 2.7 � 0.54 2.18/2.71/3.19 <.0001
Diameter/body surface area (cm/m2)* 1.82 � 0.33 1.49/1.8/2.16 2.4 � 0.52 1.84/2.3/2.8 <.0001
Area (cm2) 10 � 3.4 7.1/10/14 19 � 7.6 12/18/25 <.0001
Area/height (cm2/m)* 6.1 � 1.96 4.2/5.8/8 10 � 4.4 6.8/10/14 <.0001
Area/body mass index (cm2)* 0.39 � 0.14 0.26/0.38/0.53 0.69 � 0.3 0.43/0.65/0.94 <.0001
Area/body surface area (cm2/m2) 5.3 � 1.7 3.6/5.1/7 9.1 � 3.9 5.8/8.6/12 <.0001
Z value* 4.0 � 1.88 2.2/4.04/5.8 6.9 � 2.2 4.7/7.0/8.8 <.0001
Z value represents number of SDs by which aortic diameter deviated from mean expected normal diameter for patient’s body surface area. BAV, Bicuspid aortic valve. *Data
available for 1445 patients.
TABLEE3. Mortality andmorbidity for bicuspid aortic valve surgery
with or without ascending aorta repair
Variable
BAV alone
(n ¼ 1449)
BAV plus aorta
(n ¼ 361)
PNo. (%) No. (%)
In-hospital death 18 (1.2)* 4 (1.1)y >.9
In-hospital complications
Stroke 19 (1.3) 6 (1.7) .6
Return to operating room
for bleeding
75 (5.2) 21 (5.8) .6
Myocardial infarction 8 (0.55) 2 (0.55) >.9
Renal failure 12 (0.83) 2 (0.55) >.9
Prolonged ventilation 62 (4.3) 15 (4.2) .9
Septicemia or sepsis 31 (2.1) 5 (1.4) .4
BAV, Bicuspid aortic valve. *68% confidence limits 0.95% to 1.6%. y68% confi-
dence limits 0.58% to 2.0%.
TABLE E4. Influence of aortic procedure and diameter on death and
stroke
Variable Estimate ± SE P
In-hospital death
Ascending aortia surgery 0.47 � 0.72 .5
Ascending aortia diameter* 4.4 � 2.6 .1
Propensity score �0.59 � 1.3 .7
Intercept �5.1 � 0.66
In-hospital stroke
Ascending aortia surgery 0.27 � 0.66 .7
Ascending aortia diametery 0.23 � 0.81 .8
Propensity score �0.32 � 1.3 .8
Intercept �4.7 � 1.4
SE, Standard error. *(Height/area of ascending aorta), inverse transformation. As-
cending aortia area normalized by patient height. yLn(area of ascending aorta/height),logarithmic transformation. Ascending aortia area normalized by patient height.
Acquired Cardiovascular Disease Svensson et al
629.e3 The Journal of Thoracic and Cardiovascular Surgery c September 2011
ACD