Embed Size (px)
Citation preview

Beyond Basal Insulin: Intensification of Therapy Jennifer D’Souza, PharmD, CDE, BC-ADM

Disclosures
• Jennifer D’Souza has no conflicts of interest to disclose.
2

When Basal Insulin Is Not Enough Learning Objectives
• Categorize patient characteristics that would assist clinicians in identifying the appropriate management for intensification of insulin therapies in patients with type 2 diabetes
• Discuss the implications of adverse effects associated with various classes of antihyperglycemic medications
• Compare and contrast advantages and disadvantages of various strategies used for intensifying insulin therapy
• Employ clinical practice recommendations from practice guidelines toward the optimal use of different classes of drugs for intensification of insulin therapy in individuals with diabetes 3

Case Study: Introduction
• Mr. K, a 50-year-old Caucasian male, has had diabetes for 6 years
• He is concerned about his uncontrolled blood glucose level, a recent increase in weight (5 lbs), and that lately has been feeling anxious and sometimes confused
• Physical exam: • Height 5’9” (152 cm) • Weight 198 lbs (90 kg) • BMI 29.2 kg/m² • BP 138/84 mmHg Continued…
4

Case Study: Introduction (cont’d)
• Lab results (recent): • A1C 8.1% • FPG <130 mg/dL • 2-hour postprandial (dinner) >180 mg/dL (~200 mg/dL)
• Medication history: • Metformin 500 mg/glipizide 5 mg: 2 tabs (1000/10) BID • Started on insulin glargine last year, titrating to a current dose of 50
units at bedtime (increased by 6 units in the past week) • Consults with a registered dietitian and eats a healthy diet • Exercises three times a week Continued…
5
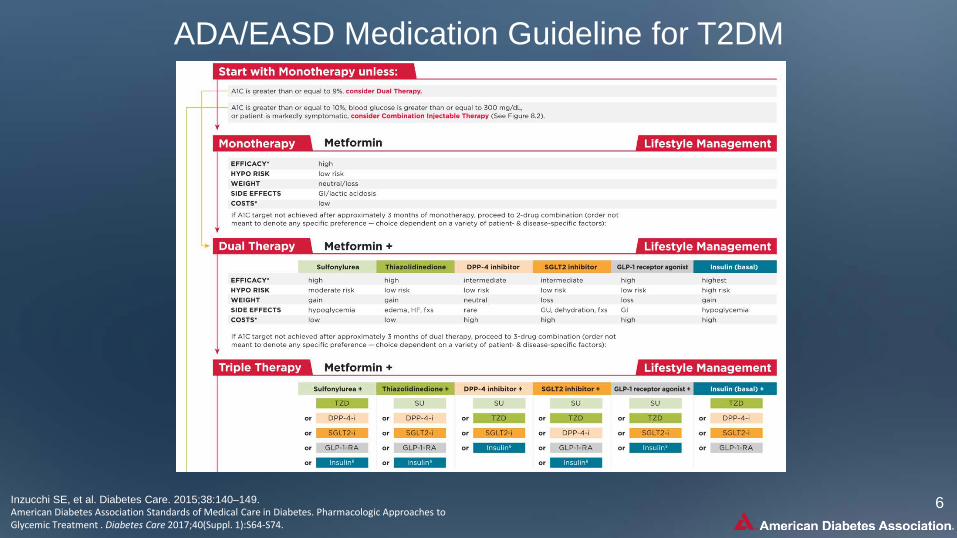
ADA/EASD Medication Guideline for T2DM
Inzucchi SE, et al. Diabetes Care. 2015;38:140–149. American Diabetes Association Standards of Medical Care in Diabetes. Pharmacologic Approaches to Glycemic Treatment . Diabetes Care 2017;40(Suppl. 1):S64-S74.
6

US FDA-Approved Therapies To Be Combined with Basal Insulin
Class Agents with FDA Approval for Use in Combination with Insulin
Thiazolidinediones (TZD)
• Pioglitazone • Rosiglitazone
US FDA. Drugs@FDA Web site. http://www.accessdata.fda.gov/Scripts/cder/DrugsatFDA/
7

US FDA-Approved Therapies To Be Combined with Basal Insulin
Class Agents with FDA Approval for Use in Combination with Insulin
DPP-4 inhibitors
• Alogliptin • Linagliptin • Saxagliptin • Sitagliptin
US FDA. Drugs@FDA Web site. http://www.accessdata.fda.gov/Scripts/cder/DrugsatFDA/
8

DPP-4 Inhibitors as Add-on Therapy to Basal Insulin (With or Without Oral Agents)
-0.6 -0.6 -0.6 -0.71
0
-0.2
0.1
-0.1
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
0.2Sitagliptin¹ Saxagliptin² Linagliptin³ Alogliptin⁴
Δ in
A1C
, %
Basal insulin, add DPP-4 inhibitor Basal insulin, add placebo
Baseline A1C = 8.5% Δ 0.6%* Δ 0.41%† Δ 0.7%† Δ 0.61%*
* p < 0.001; † p < 0.0001 1. Vilsbøll T, et al. Diabetes Obes Metab. 2010;12:167-177. 2. Barnett AH, et al. Curr Med Res Opin. 2012;28:513-523. 3. Yki-Järvinen H, et al. Diabetes Care. 2013;36:3875-3881. 4. Rosenstock J, et al. Diabetes Obes Metab. 2009;11:1145-1152.
A1C <7.0%. 13% 5% 17% 7% 20% 8%
9

DPP-4 Inhibitors and Basal Insulin: Low Risk of Severe Hypoglycemia or Weight Gain
No data
0.6
5.3
1.7 1.0
0.3
3.3
1.0 2.0
0
2
4
6Sitagliptin¹ Saxagliptin² Linagliptin³ Alogliptin⁴
Sev
ere
Hyp
ogly
cem
ia, %
Agent + INS INS + PBO
0.10 0.39
-0.30
0.60
0.10 0.18
-0.04
0.70
-0.6-0.20.20.61.0
Δ W
t, %
of
Bas
elin
e
The proportion of patients attaining A1C <7% with sitagliptin, alogliptin, or linagliptin in combination with basal insulin ranged from 8% to 20%;¹ no data for saxagliptin
1. Vilsbøll T, et al. Diabetes Obes Metab. 2010;12:167-177. 2. Barnett AH, et al. Curr Med Res Opin. 2012;28:513-523. 3. Yki-Järvinen H, et al. Diabetes Care. 2013;36:3875-3881. 4. Rosenstock J, et al. Diabetes Obes Metab. 2009;11:1145-1152.
10

US FDA. Drugs@FDA Web site. http://www.accessdata.fda.gov/Scripts/cder/DrugsatFDA/
Class Agents With FDA Approval for Use in Combination With Insulin
SGLT2 Inhibitors
• Canagliflozin • Dapagliflozin • Empagliflozin
US FDA-Approved Therapies To Be Combined with Basal Insulin
Class Agents with FDA approval for use in combination with insulin
SGLT2 inhibitors
• Canagliflozin • Dapagliflozin • Empagliflozin
11
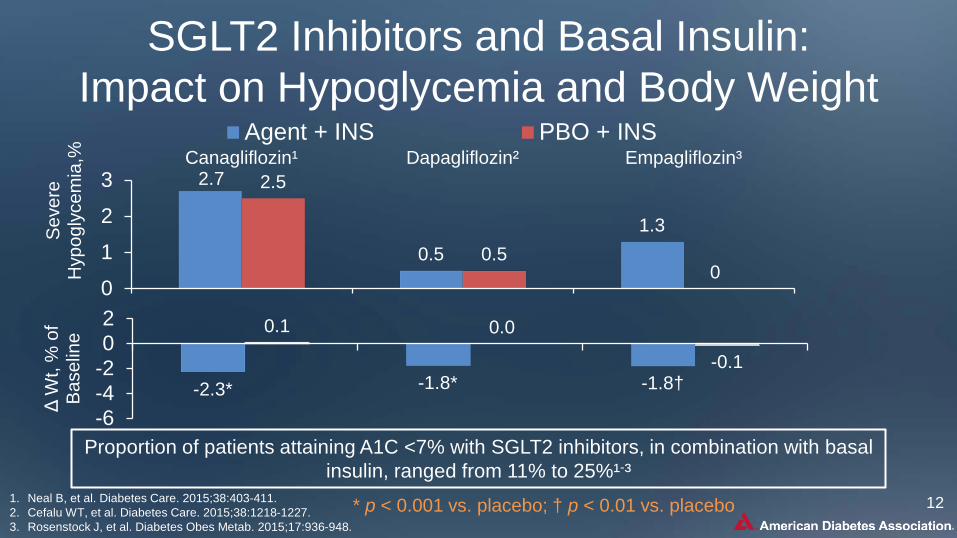
SGLT2 Inhibitors and Basal Insulin: Impact on Hypoglycemia and Body Weight
2.7
0.5 1.3
2.5
0.5 0
0
1
2
3Canagliflozin¹ Dapagliflozin² Empagliflozin³
Sev
ere
Hyp
ogly
cem
ia,%
Agent + INS PBO + INS
Proportion of patients attaining A1C <7% with SGLT2 inhibitors, in combination with basal insulin, ranged from 11% to 25%¹-³
-2.3* -1.8* -1.8†
0.1 0.0
-0.1
-6-4-202
Δ W
t, %
of
Bas
elin
e
1. Neal B, et al. Diabetes Care. 2015;38:403-411. 2. Cefalu WT, et al. Diabetes Care. 2015;38:1218-1227. 3. Rosenstock J, et al. Diabetes Obes Metab. 2015;17:936-948.
* p < 0.001 vs. placebo; † p < 0.01 vs. placebo 12

SGLT2 Inhibitors and Potential Risk of Diabetic Ketoacidosis
The EMA will review incidences of ketoacidosis in patients using SGLT2 inhibitors • The focus will be on dapagliflozin, canagliflozin,
empagliflozin, canagliflozin/metformin, and dapagliflozin/metformin
This follows a warning issued by the FDA on May 15, 2015 FDA regarding the potential risk of ketoacidosis with SGLT2 inhibitors
20 cases of diabetic acidosis, reported as diabetic ketoacidosis, ketoacidosis, or ketosis, were recorded in patients treated with SGLT2 inhibitors between March 2013 and June 2014
FDA News Release (SGLT2). Available at: http://www.fda.gov/drugs/drugsafety/ucm446845.htm. 13

• Mr. K had enjoyed good glucose control for 6 months with a metformin 500 mg/glipizide 5 mg: 2 tablets (1000/10) BID and a stable dose of basal insulin glargine 36 units at bedtime
• A few weeks ago, his post-dinner blood glucose levels increased, prompting him to increase in his basal insulin dose, which is now 50 units
• His blood glucose diary shows the following:
Day Pre-breakfast Pre-dinner 2-hr post-
dinner Bedtime Comments
Sun 138 145 195 188 Mon 132 205 196 Increased basal insulin dose by 4 units Tues 120 135 182 Forgot to inject his insulin Wed 145 168 230 198 Thurs 132 186 Increased basal insulin dose by 2 units Fri 142 175 Sat 112 128 173
Case Study: Introduction (cont’d)
14

Case Study - Discussion Question
From Mr. K’s diary, which plasma glucose patterns of hyperglycemia are present? A. Fasting B. Preprandial C.Postprandial D.Nocturnal E. B and C above
Day Pre-breakfast
Pre-dinner
2-Hr post-dinner
Bedtime Comments
Sun 138 145 195 188
Mon 132 155 205 196 Increased basal
insulin dose by 4 units
Tues 120 135 188 182 Forgot to inject
his insulin
Wed 145 168 230 198
Thurs 132 140 200 186 Increased basal
insulin dose by 2 units
Fri 125 142 175 161
Sat 112 128 185 173
15

Case Study - Discussion Question
A drug from which of the following drug classes could you consider to intensify Mr. K’s treatment beyond basal insulin to manage his dysglycemia? A. GLP-1 receptor agonist B. DPP-4 inhibitor C. SGLT2 inhibitor D. Rapid-acting insulin before the main meal E. A, B, C, or D above
19

When Basal Is Not Enough
American Diabetes Association Standards of Medical Care in Diabetes. Glycemic Targets. Diabetes Care 2017;40(Suppl. 1):S64-S74. Inzucchi SE, et al. Diabetes Care. 2015;38:140–149.
20

Basal Insulin + GLP-1 Receptor Agonists

Scientific Rationale for Combining a GLP-1RA with Basal Insulin
GLP-1 receptor agonist¹,² ●Simple to initiate ●Pronounced PPG control ●Reduced risk of hypoglycemia ●Weight reduction ●Achieve A1C targets in 40-60%
Basal insulin analogs³,⁴ ●Simple to initiate ●Control nocturnal and FPG ●Lower hypoglycemia risk vs NPH ●Modest weight gain (1-3 kg) ●Achieve A1C target in 40%
Additive effects
1. Holst JJ, et al. Mol Cell Endocrinol. 2009;297:127-136. 2. Calabrese D. Am J Manag Care. 2011;S52-S58. 3. Liebl A. Curr Med Res Opin. 2007;23:129-132. 4. Gugliano D, et al. Diabetes Care. 2011;34:510-517.
PPG = postprandial FPG = fasting plasma glucose
Complementary actions
22

Basal (long-acting) insulin daily + bolus (rapid-acting) insulin before meals

More Than 2 Daily Injections
• Temptation is to split basal dose and give it twice a day
As type 2 patients require larger doses of basal insulin (>0.5 units/kg)
• Keep basal once daily, and • Add a rapid acting insulin injection with largest meal • Follow a dosing algorithm • Follow the 90/10 rule
If going to 2 injection insulin program
Adapted from: American Diabetes Association Standards of Medical Care in Diabetes. Pharmacologic Approaches to Glycemic Treatment . Diabetes Care 2017;40(Suppl. 1):S64-S74. Inzucchi SE, et al. Diabetes Care. 2015;38:140–149.
24

90/10 Rule for Basal+1
90% basal, 10% rapid-acting (bolus)
Start with largest meal of the day
When initiating rapid-acting insulin: • Always stop the
sulfonylurea • Often stop
thiazolidinedione • Consider adjusting the
doses of other antidiabetic medications
Adapted from: American Diabetes Association Standards of Medical Care in Diabetes. Pharmacologic Approaches to Glycemic Treatment . Diabetes Care 2017;40(Suppl. 1):S64-S74. Inzucchi SE, et al. Diabetes Care. 2015;38:140–149.
25

Dosing Algorithm for Basal+1
Add 1 rapid-acting insulin injection before largest meal
Start: 4 Units, 0.1 U/kg or 10% basal dose. If A1C <8%, consider ↓ basal by same amount
Adjust: ↑ dose by 1-2 units or 10-15% once or twice weekly until SMBG target reached
For hypo: Determine & address causes; if no clear reason for hypo, ↓ corresponding dose
by 2-4 units or 10-20% Adapted from: American Diabetes Association Standards of Medical Care in Diabetes. Pharmacologic Approaches to Glycemic Treatment . Diabetes Care 2017;40(Suppl. 1):S64-S74. Inzucchi SE, et al. Diabetes Care. 2015;38:140–149.
26

Example: 90/10 Rule for Initiating Basal+1
• Patient is administering basal insulin 50 units at bedtime • Initiating the 90/10 Rule
• Reduce basal insulin by 10% (i.e., 45 units) • Administer 5 units of bolus (rapid-acting) insulin
before the largest meal ------------------------------------------ • 45 units basal insulin once daily (usually bedtime)
• Glargine, detemir, degludec, or NPH • 5 units bolus before the largest meal
• Aspart, lispro, glulisine, or regular
Adapted from: 1. American Diabetes Association Standards of Medical Care in Diabetes. Pharmacologic Approaches to Glycemic
Treatment . Diabetes Care 2017;40(Suppl. 1):S64-S74. 2. Inzucchi SE, et al. Diabetes Care. 2015;38:140–149.
27

Timing of Bolus Insulin Injections
Add rapid-acting
insulin at breakfast
Pre-lunch:
Add long-acting at
breakfast or rapid-acting
insulin at lunch
Pre-dinner:
Add rapid-acting
insulin at dinner
Pre-bedtime:
Nathan DM, et al. Diabetes Care. 2009;32:103-203.
Based on preprandial levels:
28

Types of Insulin: Prandial (Meal-Related)
Type of insulin Onset of action Peak of action Duration
of action Presentation
Rapid-acting insulin analog Insulin lispro (U100, U200) 15 min 30-90 min 3-5 hour Vial, pen/cartridge
Insulin glulisine 15 min 30-90 min 3-5 hour Vial, pen/cartridge Insulin aspart 15 min 30-90 min 3-5 hour Vial, pen Inhaled insulin 15 min 30-40 min 2-3 hour Inhaler Short-acting insulin Regular, human 30-60 min 120 min 5-8 hour Vial
Adapted from: Inzucchi S, et al. Diabetes Care. 2015;38:140-149. FDA Approved Labeling [Package Insert] for each preparation.
29

LIS 0.2 U/kg (n = 10) Regular human insulin (n = 10); mean dose, 15.4 U
0 240 360 480 300 420 Time, min
120 180 60
80 70
50
30
0 10 20
40
60
Ser
um fr
ee in
sulin
co
ncen
tratio
n, m
U/L
U-200 Lispro • Pharmacokinetics • Pharmacodynamics
http://www.prnewswire.com/news-releases/us-food-and-drug-administration-approves-humalog-200-unitsml-kwikpen-300089341.html
Potential advantage: smaller injection volume for those with high prandial insulin requirements
0 240 360 480 300 420 Time, min
120 180 60
250
200
150
100
0
Pla
sma
gluc
ose,
mg/
dL
50
LIS 0.2 U/kg (n = 10) Regular human insulin (n = 10); mean dose, 15.4 U
PK/PD data generated from a study of 10 patients with T1DM 30

Inhaled Insulin (Technosphere) in T2DM
Inhaled TI (48 units) SC RHI (24 units)
5.0
3.0
1.0 GIR
, mg/
kg/m
in
0 60 120 180 Time, min
4.0
2.0
0.0 240 300 360 420 480 540
• Duration of action for inhaled insulin is much shorter than for RHI1
• Almost complete PPG suppression has been observed in a double-blind, placebo-controlled trial in insulin-naive patients with T2DM using OADs2
1. Rave K, et al. J Diabetes Sci Technol. 2008;2:205-212. 2. Rosenstock J, et al. Diabetes Care. 2015;38:2274-2281.
31

Premixed Insulins
• Contain both a basal and prandial component, allowing coverage of both basal and prandial needs with a single injection.
• Regular human insulin and human NPH/Regular premixed formulations (70/30) are less costly alternatives to rapid-acting insulin analogs and premixed insulin analogs, respectively
32

Types of Insulin: Premixed
Type of insulin Onset of action
Peak of action
Duration of action Presentation
NPH/Regular 70/30 or 50/50 30-60 min Dual 10-16 hour Vial, pen/ cartridge
Insulin Aspart Protamine/Insulin Aspart 70/30 10-20 min Dual 15-18 hour Vial, pen
Insulin Lispro Protamine/Insulin Lispro 75/25 or 50/50 5-15 min Dual 16-18 hours Vial, pen/
cartridge Insulin Degludec/Insulin Aspart 70/30 10-20 min Dual 42 hours Pen
Adapted from: American Diabetes Association Standards of Medical Care in Diabetes. Pharmacologic Approaches to Glycemic Treatment . Diabetes Care 2017;40(Suppl. 1):S64-S74. Inzucchi SE, et al. Diabetes Care. 2015;38:140–149.
33

When Basal Insulin Is Not Enough - SUMMARY
• Inadequate control despite effectively titrated basal insulin (FBG >130 mg/dL, A1C >7%)
• Basal dose is ≥0.5 U/kg/day
Know when additional therapy beyond basal insulin is needed
• Avoid hypoglycemia • Therapies favorable to weight reduction and
blood pressure • Agents that specifically address post-prandial glucose excursions
Consider TZD, DPP-4 i, or GLP-1 RA as an additive to basal insulin
Adding a rapid-acting insulin or premixed insulin in a step-wise method before meals
34

Thank You!
35


![Basal Insulin and Combinations - jjdi.com€¦ · v Actions/Uses of Basal Insulin Basal insulin (NPH, glargine [U-100 and U-300], detemir, degludec U-100, U-200) • Controls fasting](https://img.pdfslide.us/doc/110x75/5b15fceb7f8b9a472e8c4f1d/basal-insulin-and-combinations-jjdicom-v-actionsuses-of-basal-insulin-basal.jpg)