Embed Size (px)
Citation preview
Beth Israel Deaconess Medical Center:
How Patient Cost Estimates Will
Improve Patient Satisfaction and
Reduce Hospital Costs
June 17, 2013
• About Beth Israel Deaconess Medical Center
• Healthcare Industry Challenges
• Goals - Getting to the Ideal State
• Our Journey
• Workflows
• Best Practices and Lessons Learned
• Questions and Answers
Today’s Discussion
2
About Beth Israel Deaconess Medical Center
• One of the nation's preeminent academic medical centers in Boston
• A major teaching hospital of Harvard Medical School, BIDMC is ranked
each year as a "Best Hospital" by U.S. News & World Report in multiple
specialties
• Home to a renowned academic research program
• Level 1 Trauma Center, Transplant center
• Recognized for cardiac and vascular programs
l
3
• One of 15 hospitals in the Boston area
• 649 licensed beds: 440 of which are medical/surgical, 77
critical care and 60 OB/GYN beds
• 1,250 physicians, 8,000 employees
• Wide network of growing partnerships and affiliations
– Comprised of multiple community hospitals, physician groups
and community based practices and health centers
– Well over 25 different divisions, each with multiple
departments and clinics including satellites
The Complexity of BIDMC
4
Employers Shift More of the Healthcare Cost to Employees
• Backlash to providers
• Emergence of healthcare consumerism
• Driven by increased costs
Goal: Provide pricing transparency
Healthcare Industry
5
Managed Care Contracting
• Payer contracts require accepting all plans including:
– Tiered contracts
– High deductible plans
– Increased patient responsibility
Goal: Educate on payer benefits and requirements
Healthcare Industry
6

Patient Satisfaction
• Economic environment
• Payment responsibility shift to the consumer
• Uninformed public
• Sticker shock
• Patients taking responsibility for own health
• Increase in self-pay population and bad debt
Goal: Provide accurate estimates prior to service
Healthcare Industry
7
8
Healthcare Industry
Trends in High-Deductible Health Plans
• Upfront deductibles apply to everything except routine
• Patient cost sharing for both hospital and professional
services
• Payer counter strategy for no patient cost for routine
services
Goal: Reduce patient dissatisfaction directed at provider

9
Providing a Holistic View of Out-of-Pocket Services
• No means of accurately determining payer allowances
prior to treatment
• Payers are very careful about how they communicate what
is and is not covered
• Best-guess estimates provided upon patient request
• No collection of co-insurance and deductibles at time of
service
Goal: Increase self pay collections
Healthcare Industry
10
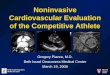
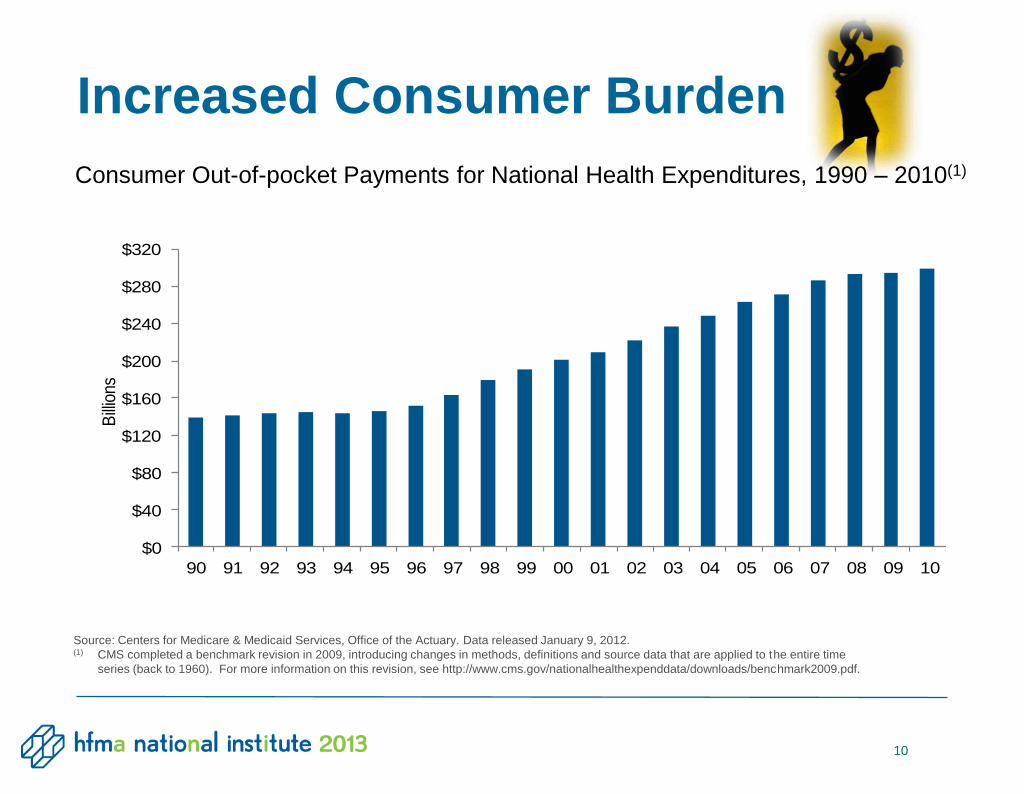
Consumer Out-of-pocket Payments for National Health Expenditures, 1990 – 2010(1)
$0
$40
$80
$120
$160
$200
$240
$280
$320
90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08 09 10
Bill
ions
Source: Centers for Medicare & Medicaid Services, Office of the Actuary. Data released January 9, 2012. (1) CMS completed a benchmark revision in 2009, introducing changes in methods, definitions and source data that are applied to the entire time
series (back to 1960). For more information on this revision, see http://www.cms.gov/nationalhealthexpenddata/downloads/benchmark2009.pdf.
Increased Consumer Burden
11
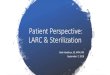
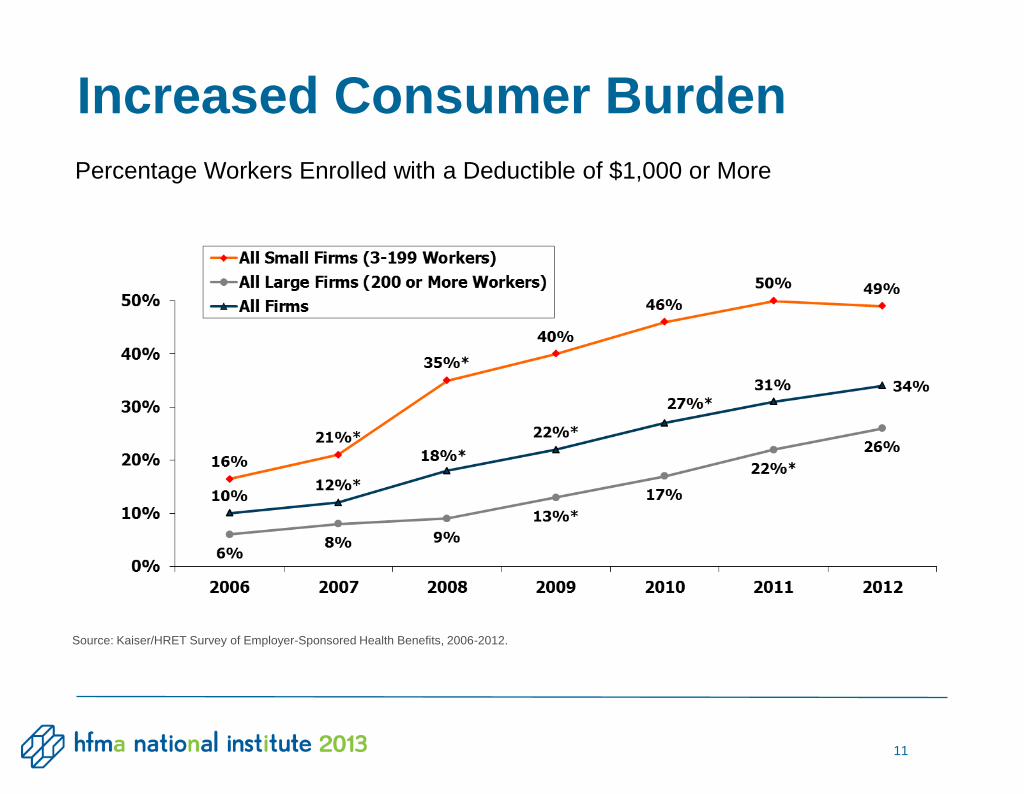
Percentage Workers Enrolled with a Deductible of $1,000 or More
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2006-2012.
Increased Consumer Burden
12
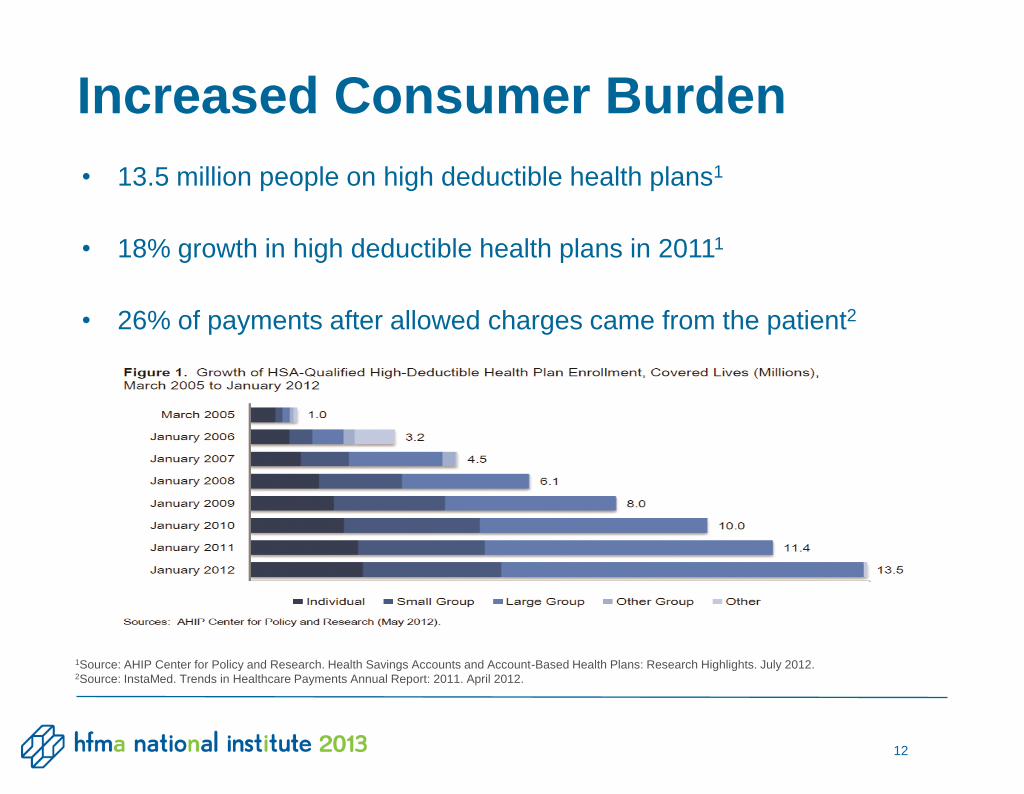
• 13.5 million people on high deductible health plans1
• 18% growth in high deductible health plans in 20111
• 26% of payments after allowed charges came from the patient2
1Source: AHIP Center for Policy and Research. Health Savings Accounts and Account-Based Health Plans: Research Highlights. July 2012. 2Source: InstaMed. Trends in Healthcare Payments Annual Report: 2011. April 2012.
Increased Consumer Burden
Getting To An Ideal State
• Provide pricing transparency
• Educate on payer requirements and benefits
• Provide estimates prior to service
• Reduce patient dissatisfaction directed at provider
• Increase self pay collections and decrease bad debt
Goals
13
Initial Steps
• Gain strategic support at top levels of the organization
– Champion/s, Physicians
• Engage
– Department / practice liaisons, other billing companies
• Create
– Infrastructure to support project
– Project team
Getting Started
14
Decide on the Direction
• Create an Estimate Tool or Purchase?
– Internal discussion to create a tool
– Review and compare available tools
• Enterprise or Phase In?
– Determine the scope of both
• Communicate and or Collect?
– Identify the value and the impact of each
First Decisions
15
Purchase a Solution
• Why?
– Time to build and price
– Lack of in-house resources
– Packaged solution came with necessary features
Specialty Areas First
• Why?
– Enterprise too large and complex in scope
– Limited resources
Our Decisions
16
Communicate Estimates Initially
• Why?
– Time to obtain and review impact
– Gather and improve from feedback
– Time to prepare for collection roll out
Our Decisions
17
Identify and Select “Best” Practices/Departments to Start
• Some key considerations:
– Highest out of pocket expenses
– Who has the most predictable service?
– Lead time to time of service
– Who is interested in doing estimates
First Adopters
18
Introduce the Project to the Key Departments
• Review the need
• Explain the benefits
• Provide an overview of product and features
• Engage the physicians
Attract Interest
19
Analyze User Workflow
• Which services?
• Who will produce estimates?
• Who has the skills?
• How will estimates be delivered?
Identify Payers for Estimates
• Initially single payers only (no secondary insurers)
• Exclude Medicare, Masshealth (Medicaid)
Customization
20
Communication Strategy
• Collaborate with practice physicians
– Prepare patient
– Provide an introductory letter
– Not a collection notice
Customization
21
Setting Up the Tool
• Charge masters
• Payer contracts
• Matching the tool with the practice
• Provider procedure sets
• DRG or by charges
Set Up
22
Conduct Extensive Testing
• Verify against payments
• Verify against contracts
Provide Training
• On the estimator tool
• Additional necessary training
Milestones
23
Go Live
• Provide support
• Conduct QA
• Provide feedback
Milestones
24
25 25 25 25 25
Obstetrics Selected to Pilot the Tool
• 1st to roll out in May 2013
• Provides the most lead time to the service
• Most predictable service
Pilot Department
Two Estimates
• 1st at the time of scheduling
– Performed by Fiscal Clearance
– Sent with informational package to patient
• 2nd estimate sent at 32 weeks
– Authorization unit re-verifies eligibility, generates new
estimate and mails
– 1st deliveries in June
Workflow
26
Results
• 80 patient estimates sent out the first week
– Estimates produced for the entire month of
August
• Project 40 obstetric estimates weekly going
forward
Workflow
27
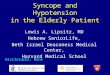
• Detail of proposed service
• Financial obligations
• Easy to follow numeric system
• English or Spanish
• Patient Portion Explanation
– Total due and why
– Verbiage - it is an estimate only
Patient Friendly Care Estimate
28
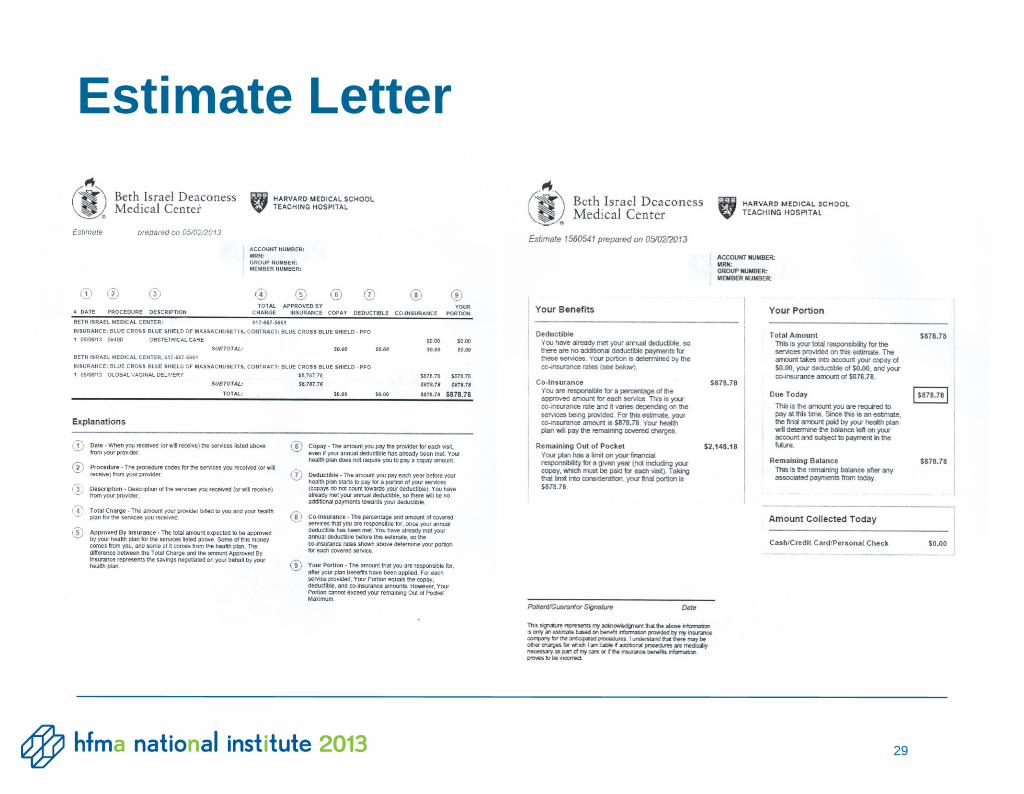
Estimate Letter
29
• Feedback to date from department, patients and
physicians
• Confirm estimate to actual
• Enhance training
• Continuous engagement with department
Continuous Improvement
30
31 31 31 31 31
Radiology
• Two areas
– Diagnostic Breast Imaging
– Mobile Radiology
• Roll out - work in progress
On Deck
Diagnostic Breast Imaging
• Requested by department head because of patient
complaints
• Quick turnaround after routine showed findings
• Estimate to be sent electronically to be delivered in
advance
• Patient responsibility is in stark contrast to routine
• No resource to produce estimates
Workflows
32
Mobile Radiology
• Lower volume
• Scheduled in advance (generally 5 days)
• MR staff have the most flexibility with workload to perform
estimates
Workflows
33
Expand to Other Areas
• Orthopedics, Surgery, Clinics
• Create estimates for additional procedures and payers
Improve the Product
• Identify issues and continue to enhance the product
• Provide training on new features, as necessary
Set Goals
• Identify, measure and monitor results
• Set strategy for collection
Next Steps
34
35 35 35 35
Foster Organizational Commitment
• Get leadership buy in – especially physicians
• Promote patient satisfaction and revenue cycle
optimization
Engage Departments throughout Healthcare System
• Start small with a predictable service
• Support the department to find where it fits in their
workflow
• Provide training
Best Practices and Lessons Learned
Provide Real Time Support to Departments
• On site for start up
• Remote support on-going
• Accuracy counts – spend time to QA
Prepare Patients & Staff for What is Coming and Why
• Publicize the new policy and when it will start
• Post notifications in office and facility
• Include notification in billing statements
Best Practices and Lessons Learned
36
Set Intermediate and Long Term Goals
• Consider education and communication as first step
• Consider partial collections if 100% is too big a step
• Internally celebrate progress
• Solicit and incorporate patient feedback
• Measure success
Best Practices and Lessons Learned
37
Questions?

Thank you!
39
Charles Messinger
Training and QA Director
www.bidmc.org
Beth O’Toole
Senior Director, Revenue Cycle
www.bidmc.org