Embed Size (px)
DESCRIPTION
Ben Edwards 14 th March 2014. Damage Control Resuscitation. Damage control resuscitation. Term used to describe key concepts Permissive hypotension Haemostatic resuscitation Damage control surgery (DCS). Jansen J et al. Damage control resuscitation for patients with major trauma. - PowerPoint PPT Presentation
Citation preview

Ben Edwards14th March 2014
Damage Control Resuscitation

Term used to describe key concepts
Permissive hypotension
Haemostatic resuscitation
Damage control surgery (DCS)
Jansen J et al. Damage control resuscitation for patients with major trauma. BMJ 2009;338:b1778

“A strategy of deferring or restricting fluid administration until haemorrhage is controlled, while accepting a limited period of suboptimum end organ perfusion”
Aim for Systolic BP 70-80
Recommend use for up to 60 minutes Aim to get control of bleeding within this
time

Should not be used in those with isolated/concurrent head injuries Aim Systolic BP>90 “Normotension”
Therefore most applicable to penetrating trauma BUT 40% polytrauma patients have traumatic
brain injury! Other terminology
Hypotensive resuscitationDelayed resuscitation

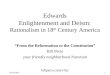
Randomised 2 groups with penetrating trauma and BP <90 Immediate Delayed
BP raised to >100 post anaesthesia
Bickell WH et al, NEJM 1994; 331:1105-9Bickell WH et al, NEJM 1994; 331:1105-9

Statistically significant findings: Survival higher in delayed group Stay shorter in delayed group
Trend towards Higher intra-op blood loss in the
immediate group ? More complications in immediate group
Not statistically significant
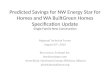
Bickell WH et al, NEJM 1994; 331:1105-9Bickell WH et al, NEJM 1994; 331:1105-9

Outcome of Patients with Penetrating Torso Injuries, According to Treatment Group

Early use of blood and blood products as primary resuscitation fluids
Trauma induced coagulopathy causes• mortality• incidence of multi organ failure
• Renal • Acute lung injury
• ICU length of stay


Damage control resuscitation: Correct coagulopathy Limit duration of shock Reduce haemodilution
Use high ratio blood component therapy Limit use of crystalloids
Reduce hypothermia Tranexamic acid Factor VIIa
role remains unproven

Each hospital should have oneSTH massive transfusion pack
4 units packed red cells 3 bags FFP 2 bags cryoprecipitate 1 adult dose platelets
Give empirically Use clinical judgement, don’t wait for the
clotting result

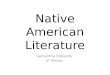
Holcomb J et al. Annals of Surgery 2008;248:477-458 Holcomb J et al. Annals of Surgery 2008;248:477-458
Increased Plasma and Platelet to Red Blood Cell Ratios Improves Outcome in 466 Massively Transfused Civilian Trauma Patients

Increased number of coagulation products in relationship to red blood cell products transfused improves mortality in trauma patients
Shaz BH et al. Transfusion 2010;50:493-500Shaz BH et al. Transfusion 2010;50:493-500


Over 20,000 patients ‘with or at risk of significant bleeding’
1g of Tranexamic acid over 10 minutes followed by a further 1 g over 8 hours reduced all cause mortality and deaths due to bleeding
Further analysis showed that must be given within 3 hours of injury
Independent standard for achieving best practice tariff (BPT) payment

“Temporary sacrifice of anatomy to preserve vital physiology”
Do only what is needed to stabilise and address life threatening injuries
Major surgery worsens the immune hit from trauma

DCS only if Temp <35°C INR >1.5 Platelets <120 BE> -5 pH <7.25
Critical care for further resuscitation
Serum lactate useful to assess adequacy of resuscitation

Damage control resuscitation practices are in evolution As studies and evidence develop guidance
will change Military principles applied to a civilian
population Hybrid approach probably the future
Permissive hypotension, haemostatic resuscitation, DCS
Attention to detail vital