Embed Size (px)
Citation preview
Bell’s Palsy
Diah Mustika HW
RSAL dr Ramelan Surabaya
History
- Sir Charles Bell, Scottish Surgeon
- First described in early 1800s based on trauma to facial nerves
- Definition of Bell’s Palsy: Acute peripheral CN VII (facial nerve) palsy of unknown cause
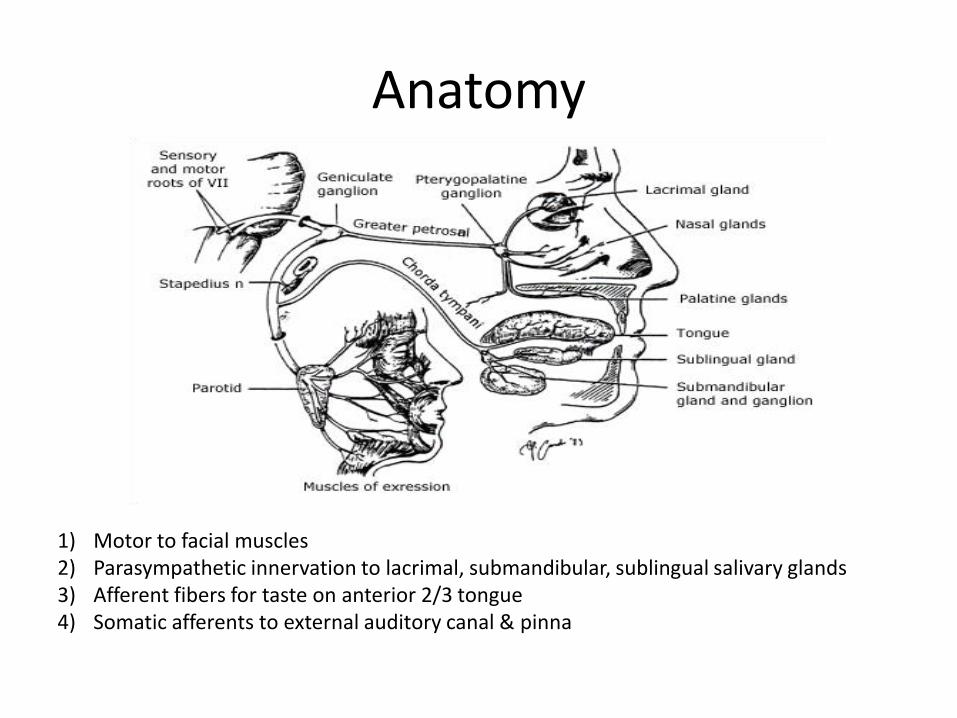
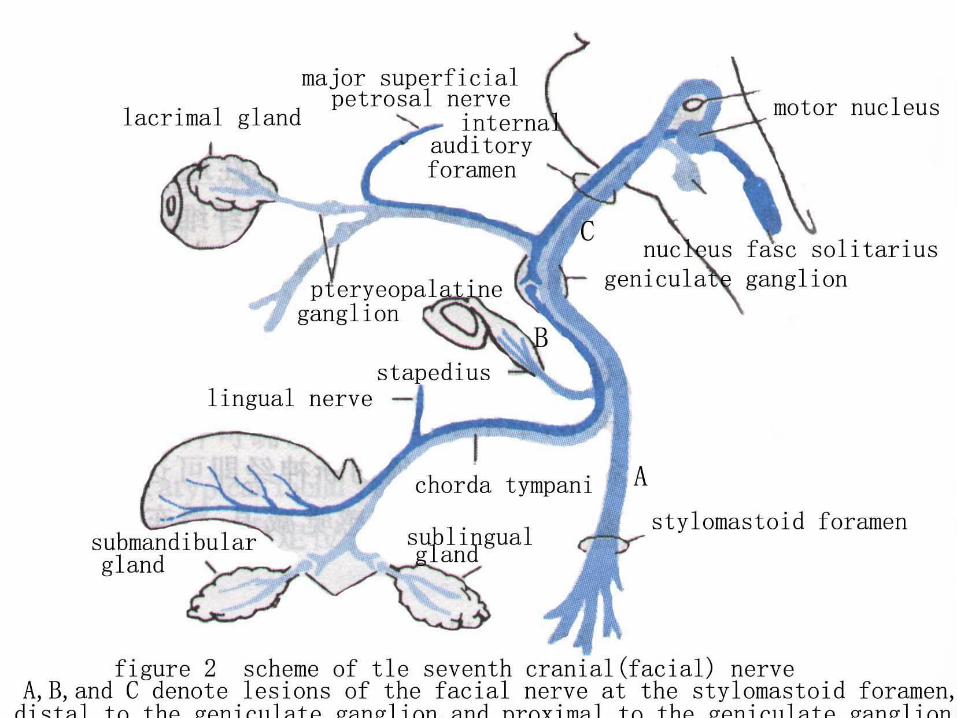
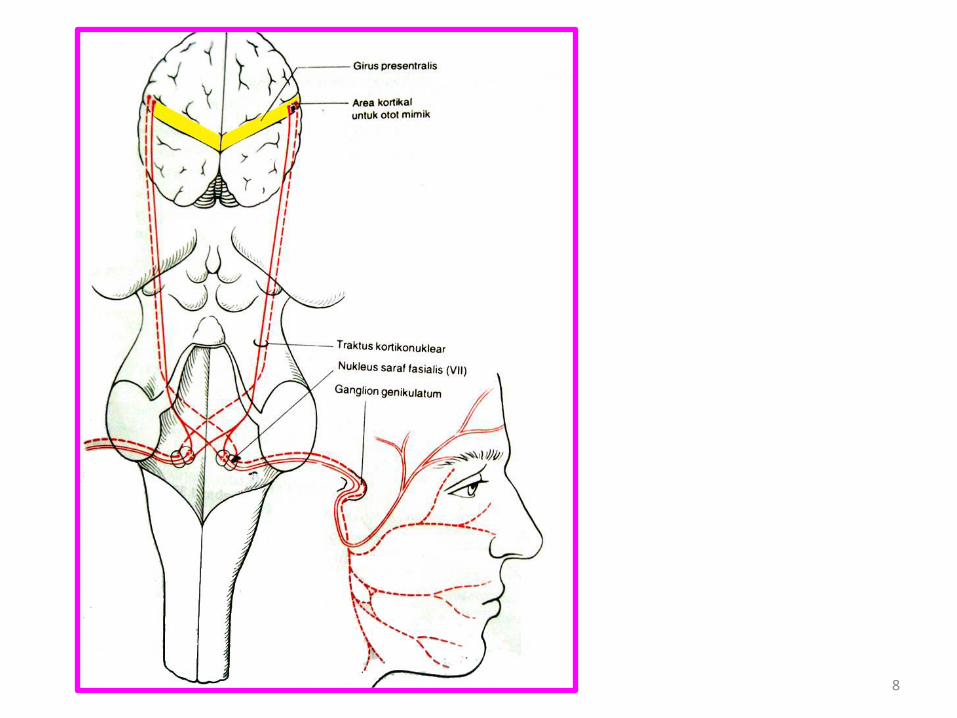
Anatomy
1) Motor to facial muscles2) Parasympathetic innervation to lacrimal, submandibular, sublingual salivary glands3) Afferent fibers for taste on anterior 2/3 tongue4) Somatic afferents to external auditory canal & pinna
Epidemiology
• ½ of all facial palsy’s qualify as “Bell’s Palsy”
• Annual Incidence 10-40/100,000
• Lifetime incidence 1:60
• Risk is 3xs greater in pregnancy, especially 3rd
trimester
• Increased risk with diabetes
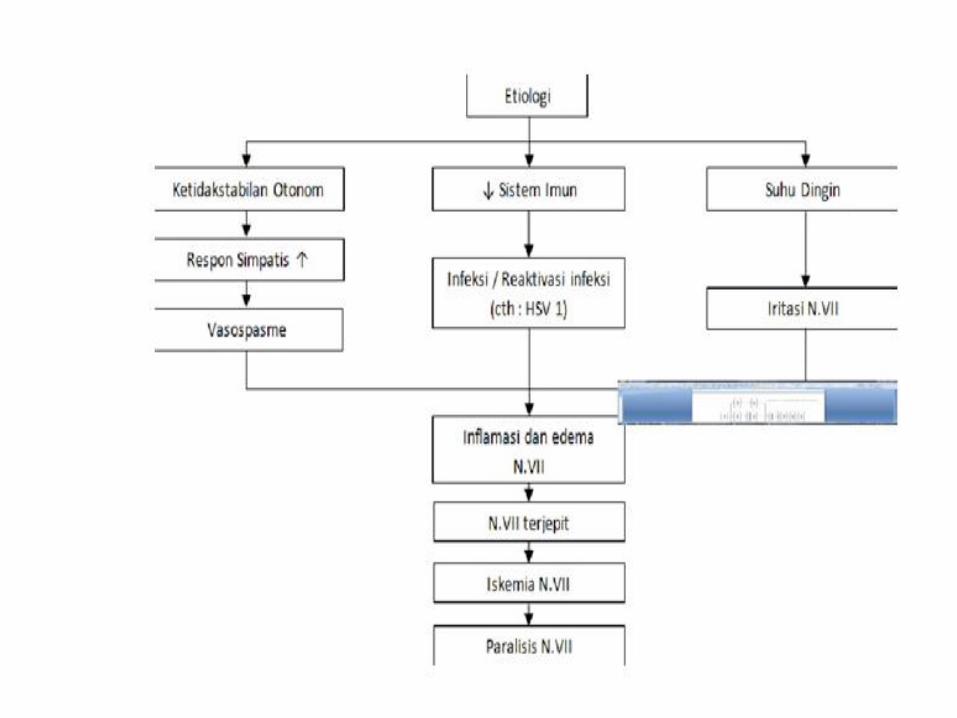
Etiology and pathology
• the cause is unclear
• exposure to chill
• a viral infection
• edema
• degeneration.
Etiology pathology
7
8
Clinical features
• Occurs at any age and any time.
• unilateral
• The onset is acute. attain maximum paralysisin 48h --5 days.
• pain behind the ear.
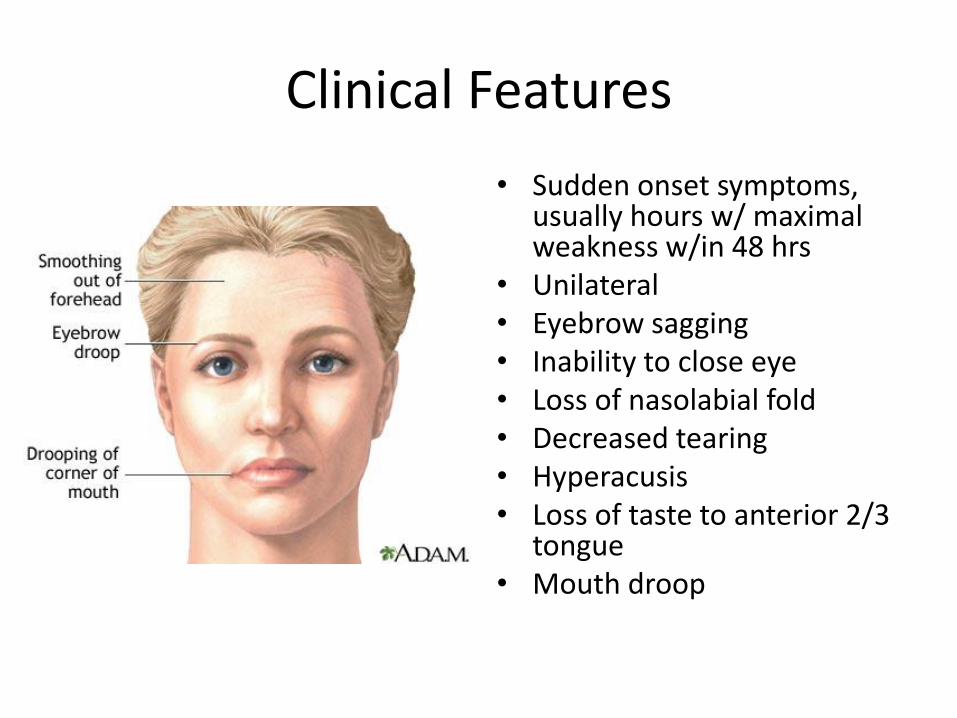
Clinical Features
• Sudden onset symptoms, usually hours w/ maximal weakness w/in 48 hrs
• Unilateral• Eyebrow sagging• Inability to close eye• Loss of nasolabial fold• Decreased tearing• Hyperacusis• Loss of taste to anterior 2/3
tongue• Mouth droop
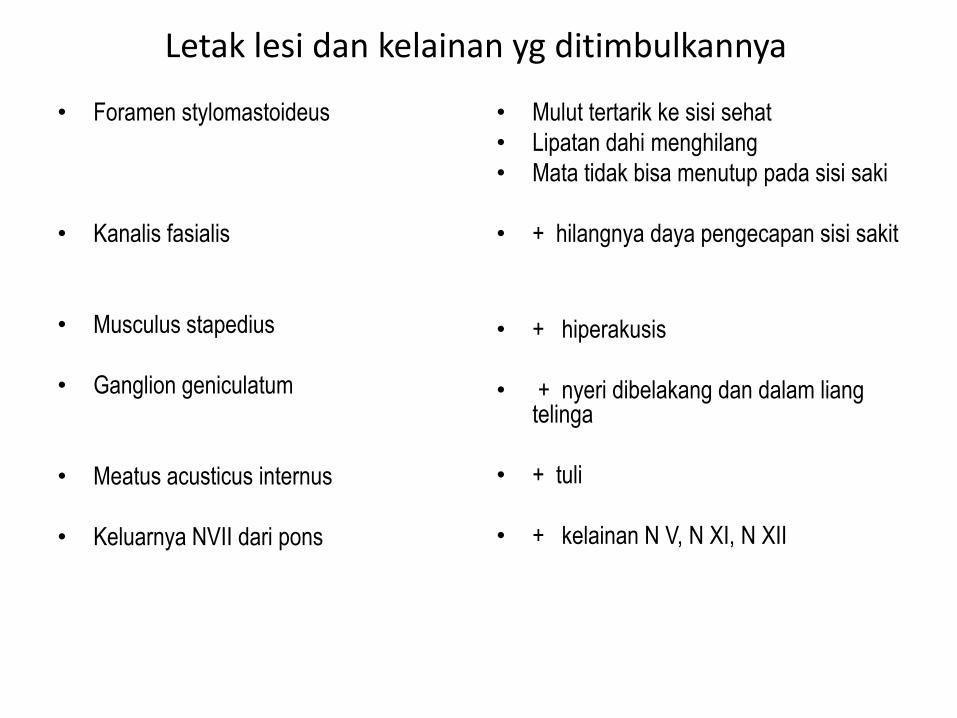
Letak lesi dan kelainan yg ditimbulkannya
• Foramen stylomastoideus
• Kanalis fasialis
• Musculus stapedius
• Ganglion geniculatum
• Meatus acusticus internus
• Keluarnya NVII dari pons
• Mulut tertarik ke sisi sehat
• Lipatan dahi menghilang
• Mata tidak bisa menutup pada sisi saki
• + hilangnya daya pengecapan sisi sakit
• + hiperakusis
• + nyeri dibelakang dan dalam liangtelinga
• + tuli
• + kelainan N V, N XI, N XII
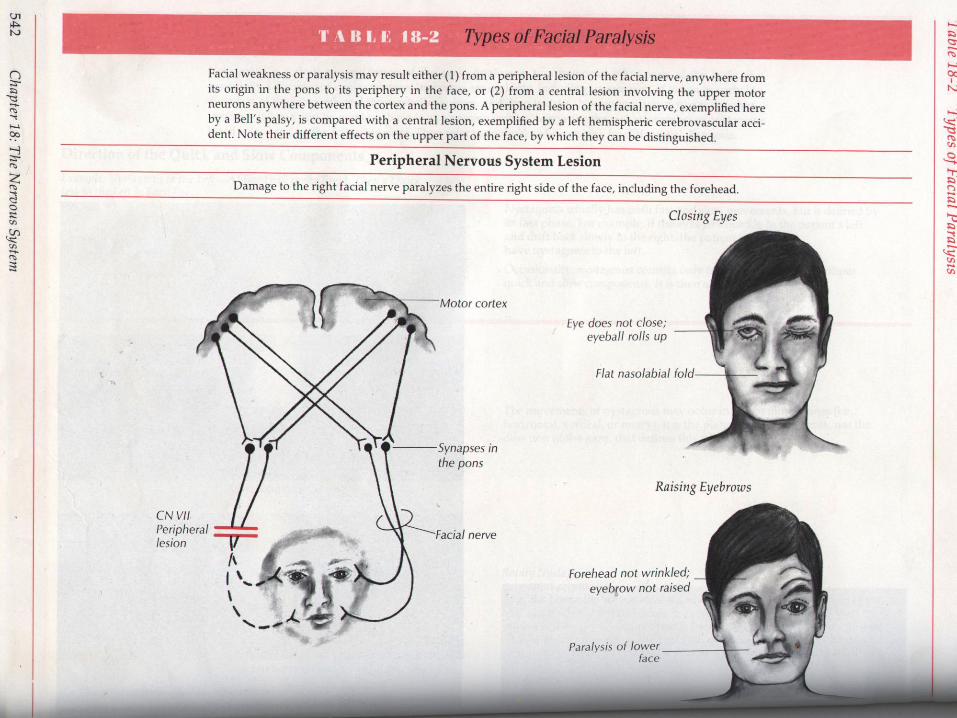
Diagnosis
• based on the acute onset and theperipheral facial palsy.
• distinguished from facial paralysis due toother causes
• distinguished from the supranuclear one(such as in a stroke)
14
2. PEMERIKSAAN KLINIS
- Test Lakrimasi ( shimmer test )
- Fungsi sensorik : glukosa 5 % --- manis
as sitrat 1 % ---- asam
sod kloride 2.5 % ---- asin
quinine HCl 0,075 % ----- pahit
- Test refleks stapedius/hiperakusis
- Pemeriksaan fungsi motorik
15
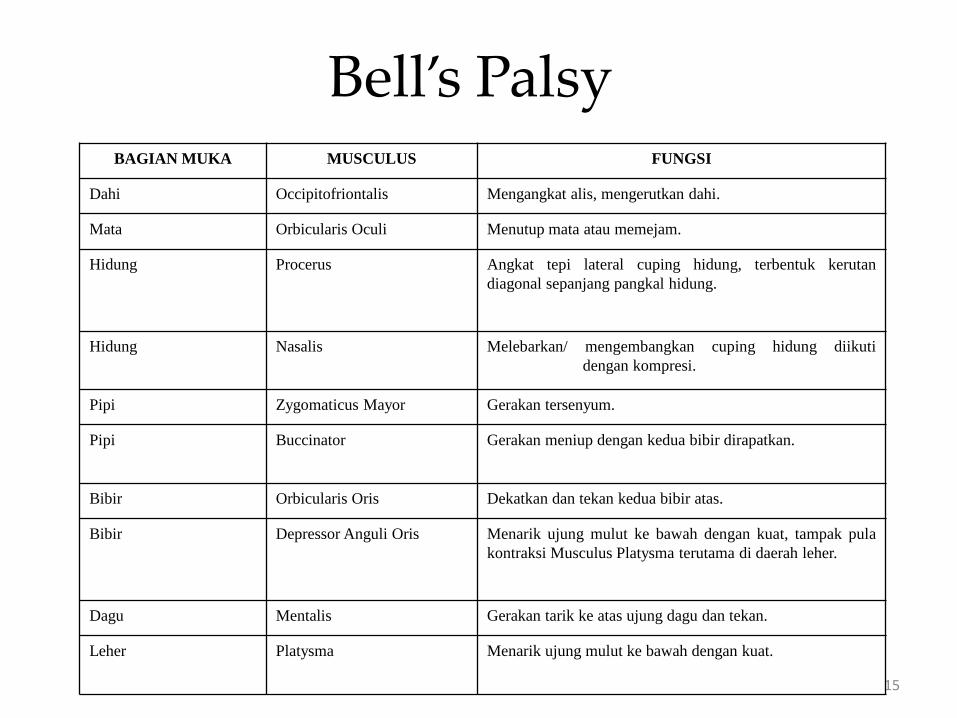
Bell’s PalsyBAGIAN MUKA MUSCULUS FUNGSI
Dahi Occipitofriontalis Mengangkat alis, mengerutkan dahi.
Mata Orbicularis Oculi Menutup mata atau memejam.
Hidung Procerus Angkat tepi lateral cuping hidung, terbentuk kerutan
diagonal sepanjang pangkal hidung.
Hidung Nasalis Melebarkan/ mengembangkan cuping hidung diikuti
dengan kompresi.
Pipi Zygomaticus Mayor Gerakan tersenyum.
Pipi Buccinator Gerakan meniup dengan kedua bibir dirapatkan.
Bibir Orbicularis Oris Dekatkan dan tekan kedua bibir atas.
Bibir Depressor Anguli Oris Menarik ujung mulut ke bawah dengan kuat, tampak pula
kontraksi Musculus Platysma terutama di daerah leher.
Dagu Mentalis Gerakan tarik ke atas ujung dagu dan tekan.
Leher Platysma Menarik ujung mulut ke bawah dengan kuat.
Prognosis
• usually good. recover within a few weeks orin a month or two.
• But if there is evidence of denervation after10 days, one may expect a long delay in theonset of recovery.
Treatment
• surgical decompression may be harmful.
• take some corticosteroids, such asprednisone (40 to 60mg/day).
• Vitamin B
• antiviral agents may be useful.
• physiatrics and acupuncture therapy
• a shield to protect the eye.






![EfficacyofManipulativeAcupunctureTherapyMonitoredbyLSCI ...Bell’s palsy is an acute peripheral facial nerve palsy of un-knowncauseandaccountsfor50%ofallcasesoffacialnerve palsy [1]](https://img.pdfslide.us/doc/110x75/60a4deb9e0003e748e568e41/efficacyofmanipulativeacupuncturetherapymonitoredbylsci-bellas-palsy-is-an.jpg)