Embed Size (px)
DESCRIPTION
Baptist Cancer Institute Annual Report 2012
Citation preview

Baptist Cancer Institute
2 0 1 2 CANCER PROGRAM A n n u a l R e p o r t

Table of Contents
2 Cancer Committee Report
6 Tumor Registry Report
18 Tumor Review: Hodgkin’s Disease
24 Tumor Review: Soft Tissue Sarcomas
30 Quality Assurance
32 Clinical Research and Education
36 Distinguished Individual in Cancer Care
38 Philanthropy
B a p t i s t C a n c e r I n s t i t u t e 2 0 1 2 A n n u a l R e p o r t

Baptist Cancer Institute (BCI) is affiliated with
Baptist Health, the only locally governed,
faith-based health system in Northeast Florida.
Baptist Health, a Magnet™ Health Care
System honored for excellence in patient
care, is comprised of Baptist Medical Center
Jacksonville, Baptist Medical Center Beaches,
Baptist Medical Center Nassau, Baptist Medical
Center South, Wolfson Children’s Hospital and
Baptist Clay Medical Campus.
Baptist Cancer Institute is one of the most
active clinical research institutes in the state
of Florida, with open studies in breast cancer,
lung cancer, gastrointestinal malignancies,
lymphoma, leukemia, head and neck cancer
and brain tumors. We work in collaboration
with physicians across the state and the
nation to conduct clinical trials that lead to
improved diagnostic approaches, reductions
in toxicities and new ways to fight these often
devastating diseases.
1

As the world progresses to electronic
information, Baptist Medical Center
and Baptist Cancer Institute (BCI) have
followed suit. This year, 2011, will be the
second year the Cancer Committee report
will be exclusively online. The Baptist
hospital systems – Baptist Jacksonville,
Baptist South, Baptist Beaches, and Baptist
Nassau – are now complete EMR hospitals.
As chairman of the Cancer Committee, we
will continue to follow the electronic medical
record impetus and make this report both
concise and informative. The Cancer program has
continued to be healthy, offering a wide breadth of
services and high-quality care for cancer patients in
Northeast Florida and Southeast Georgia. Cutting-edge
programs in neuro-oncology, breast care, and lung cancer
treatment are active in offering a high level of care which
translates into high satisfaction for patients.
Baptist Health offers a wide variety of not only cancer treatments, but
educational programs for both physicians and the public. At Baptist Jacksonville,
palliative care offers a multi-step program for our cancer patients. Close communications
with Hospice of Northeast Florida allows hospice to step in when more intensive care is
Cancer Committee
ReportTroy H. Guthrie Jr., MD, Cancer Committee Chairman
B a p t i s t C a n c e r I n s t i t u t e 2 0 1 2 A n n u a l R e p o r t

needed at the patient’s home. These programs allow
patients and their families to make every minute count
toward the highest quality of life. Clinical research
programs continue to be extremely active at BCI,
with research programs in breast cancer, lung cancer,
melanoma, neurological malignancies, prostate cancer,
hematological malignancies, and other solid tumors.
Research studies are offered through the auspices of the
National Cancer Institute clinical study groups, as well as
pharmaceutical-sponsored industry trials.
Screening programs in breast cancer, colon cancer,
prostate cancer, and skin cancers continue to expand,
offering education to the public as well as active
intervention. The genetic assessment program, under
the leadership of Melinda Fawbush, MSN, ARNP,
remains extremely active concentrating primarily on
breast cancer.
Multi-disciplinary conferences in breast cancer
are offered weekly, lung cancer bi-weekly, and
neuro-oncology monthly. These programs are
teleconferenced to satellite hospitals so that education
can be received by physicians and health care staff
in their own hospital. Psychosocial support continues
to be offered by George Royal, PhD, and
more recently, nutritional, physical therapy, and
occupational therapy programs are offered
through our multi-disciplinary cancer program.
The Cancer Committee at Baptist Medical
Center Jacksonville continues to meet
quarterly to provide leadership direction and
review of all aspects of the cancer program
and services as mandated by the American
College of Surgeons. At each meeting, the
activities of the tumor registry and current
clinical research, as well as goals of the
Cancer Committee, are reviewed.
Current leadership for the Cancer Committee
includes:
• Troy H. Guthrie, Jr., MD, Chairman, Cancer
Committee;
• Mark Augspurger, MD, Liaison to the American
College of Surgeons; Patricia Woods, RN, BSN,
OCN, Quality Improvement Coordinator;
• Paul Oberdorfer, MD, Community Outreach
Coordinator;
• Melissa McCarthan, RHT, CTR, Tumor Registrar; and
• Jan Peer, CCRP, Research Coordinator.
3

At each meeting, the Cancer Committee reviews,
revises, and reapproves current program goals to
determine whether they are being met and if they
are aligned with the latest requirements of the
American College of Surgeons.
This Annual Report, as required by the American
College of Surgeons, will include a prospective
and retrospective study of cancer disease sites,
as well as assess the quality of data provided by
the tumor registry. This year, Hodgkin’s disease
and soft tissue sarcoma will be the areas of review.
In 2011, more than 10 percent of all analytic
cases were reviewed on a prospective basis by
physician volunteers to ensure continued quality
and timeliness of data entered into the Baptist
Tumor Registry. In 2011, for the second time in
a row, there was a drop in the number of cases
accessed with the total number of analytic cases
being 1,624 compared to 1,656 the previous
year. The total number of analytic cases fell at
Baptist South, likewise, from 533 cases to 458
analytic cases. The slight drop in analytic cases
at Baptist Jacksonville appeared to be spread
out among tumor sites. Currently, the Tumor
Registry includes a total of 26,414 analytic cases
accrued since 1990. In 2011, the cancer clinical
research program included active participation in
the National Surgical Adjuvant Breast and Bowel
Project, Eastern Cooperative Oncology Group,
Radiation Therapy Oncology Group, and Mayo
Clinic Cancer Research Consortium, as well as
pharmaceutical industry sponsored research
trials. In 2011, approximately 50 percent of the
research patients participated in NCI group
studies and 50 percent were patients registered
on pharmaceutical studies.
Other Baptist Cancer Institute activities include:
• Major conferences for oncology nurses
• Prevention and community education programs
• Continued participation in the American Cancer
Society and Leukemia and Lymphoma Society
Committees
• Special oncology nursing programs for
community support of education in breast and
lung cancer
• Smoking cessation assistance programs for the
community as well as employees of Baptist
Health
• Cutting-edge prostate cancer treatment
programs, including seed implants and the state
of the art da Vinci Robotic Surgery unit
• Continued expansion of the stereotactic
radiosurgery radiation program with a marked
increase in the number of body sites being
treated
• Continued expansion of the limited breast
radiation program using the Mammosite®
technique
• Continued expansion of the digital breast
cancer-screening program with movement to
centralized diagnostic studies at the Baptist
Cancer Institute
• Participation in in-patient quality improvement
programs, including infection control
• Expansion of the chemotherapy and
radiopharmaceutical embolization programs for
treatment of liver malignancies
• Continued participation of indigent programs,
including the highly successful We Care program
• Continued expansion of a hospital-based
chemotherapy infusion unit
4

• On-site involvement of hospice and palliative
care programs for optimum support for both
the cancer patient and family
• Continued expansion of the Genetic Risk
Assessment Screening program, now focusing
on breast cancer, but also includes melanoma,
and colon cancers
• Continued active participation in the oncology
training program for the medical oncology
fellows from the University of Florida
Jacksonville and the Radiation Therapy
residents at Mayo Clinic Jacksonville
As Cancer Committee Chairman since 2005, it gives me great pleasure to see the continued expansion
of cancer services offered in Northeast Florida and Southeast Georgia in the year 2011. State-of-the-
art programs which run the entire spectrum of hematologic and solid tumor malignancies are being
offered in a multi-disciplinary approach to patients of all walks of life. A close collaboration of physicians,
hospital administrators, and allied professional staff has enabled the Baptist Cancer Institute to remain at
the forefront of care in this region for cancer patients.
Troy H. Guthrie Jr., MDCancer Committee ChairmanMedical Director, Education and ResearchBaptist Cancer Institute
• Continued expansion and utilization of the
comprehensive breast health program with
nurse coordinator at Baptist Jacksonville,
Baptist South and Baptist Beaches
• Rapid expansion of the Neuro-oncology
program, with continued expansion of the
radiosurgery program, as well as increased
sophistication of the Neurosurgery suites
and continued expansion of Neuro-oncology
clinical research studies
5

The Tumor Registry at Baptist Cancer
Institute has been approved since 1990
by the Commission on Cancer of the
American College of Surgeons. As part
of our approval, the Tumor Registry
collects data on cancer screenings
annually in terms of incidence, tumor
site, kinds of treatment provided,
and survival outcomes. Its data is then
entered into the Florida State Tumor
Registry and ultimately accumulated at the
national level as SEER data. This process
enables all American College of Surgeons
accredited cancer centers to compare their
own outcomes in terms of diagnoses, stage,
effectiveness of cancer treatment, and ultimate
outcome in terms of survival, to each other. This
enables Baptist Cancer Institute through its Tumor
Registry, as well as other accredited programs, to assess
their level of care when compared to others both within the
state of Florida, as well as at the national level and see if standards
of care are met to assess areas where quality improvement is needed to
address deficits within each program.
TumorRegistry Report
Troy H. Guthrie Jr., MD, Cancer Committee Chairman
Melissa McCarthan, RHIT, CTR
April Stebbins, RHIT, CTR
Rassy Sprouse, BSc
B a p t i s t C a n c e r I n s t i t u t e 2 0 1 2 A n n u a l R e p o r t

The registry assists the Cancer Committee with
evaluating outcomes, quality of medical care,
and assessment of treatment, recurrence, and
survival rates. Currently, the Baptist Tumor
Registry has accumulated data from both
Baptist Medical Center Jacksonville since 1990
and Baptist Medical Center South, where data
collection began in 2005. Physician volunteers
from both Baptist Jacksonville and Baptist South
assist tumor registry in assessing the accuracy of
analytic case data accumulation for each year.
Ten percent of all cases are evaluated by these
physician volunteers for accuracy of data as well
as timeliness of reporting.
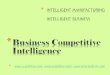
Figure 1 demonstrates the number of cases
accumulated from 1990 through 2011 at Baptist
Medical Center Jacksonville. As you can see,
for the second year in a row, there is a drop in
the number of patients seen compared to 2010.
This decrease in the number of patients is less
dramatic than the previous year, but represents
the second year in 21 years that the Tumor
Registry has seen a decline in cases. Since 1991,
the Tumor Registry at Baptist Jacksonville has
seen a total of 26,414 analytic cases. Similar
to previous years, there remains a female
predominance of analytic cases with 2011 having
943 female cases and 681 male cases (Figure
2). Table 1 demonstrates the incidence of the
most common primary sites seen at Baptist
Medical Center Jacksonville with breast cancer
accounting for 434 cases or 27 percent, prostate
cancer 199 cases or 12 percent, Lung cancer
186 cases or 11 percent and female genital
cancers 106 cases or 7 percent. Of great interest,
melanoma came in as the sixth-most common
site with 90 cases or 6 percent. Colorectal,
a much more common malignancy, had only
89 cases or 5 percent and central nervous
system malignancies or neuro-oncology had 85
cases or 5 percent. In 2011, there continued
to be a decrease in prostate cancer, although
less dramatic when compared to 2010 and a
relatively dramatic drop in lung cancer cases
was seen compared to 2010, with only 186
cases being registered in 2011. Melanoma and
urinary bladder as primary sites showed the most
substantial increase in patient numbers accrued
to the 2011 Tumor Registry. Table 2 shows the
frequency of primary sites seen at Baptist South
which has a somewhat different incidence of
primary sites than Baptist Jacksonville with an
increased percentage of lung, colorectal, thyroid,
and kidney primaries and a marked decrease in
the frequency of melanoma, brain tumor, and
7

Figure 2 Male & Female Malignancies: 2011 (Baptist Jacksonville)
1000
800
600
400
200
0
681
943
No
. of
Ma
lig
nanc
ies
Male Female
Figure 1 Baptist Cancer Institute Analytic Cases by Year
1800
1600
1400
1200
1000
800
600
400
200
01990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
688 76
4 807
1004
1102
964
928
865 96
5
972 10
41 1138
1308
1139
1265
1253
1467
1630
1656
1744 1779
No
. of
Pa
tien
ts
Year
Figure 3 Analytic Cases: 2010 - 2011 (Baptist Jacksonville and Baptist South)
2000
1600
1200
800
400
0
1656
533
No
. of
Pa
tien
ts
Baptist Jacksonvi l le
Baptist South
2010 2011 2010 2011
458
1624
1624
female genital tract incidence. These differences
between sites seen at each hospital again
references the difference in terms of referral
pattern with expertise in melanoma and neuro-
oncology being located at Baptist Jacksonville
and only a modest presence of gynecologic
oncology at Baptist South. These tables also
indicate the male and female predominance
of malignancies by the primary site at both
institutions. There was a drop for the second
year in a row of 32 analytic cases of Baptist
Jacksonville and a decrease for the first time of
total cases seen at Baptist South from 533 cases
to 458 cases (Figure 3). These decreases in total
cases seen are almost certainly multi-factorial but
recent campaigns by other hospitals to attract
cancer cases may be a factor. Table 3 compares
the incidence of the five most common primary
8

Table 1 Primary Sites : Baptist Medical Center Jacksonville (2011)
Site Total % Male Female
Breast 434 27% 3 431
Prostate 199 12% 199 0
Lung 186 11% 89 97
Female Genital 106 7% 0 106
Melanoma 90 6% 53 37
Colorectal 89 5% 50 39
Brain & CNS 85 5% 37 48
Other Sites 63 4% 37 26
Other Sites 57 4% 30 27
Blood & Bone Marrow 62 4% 36 26
Kidney 51 3% 30 21
Pancreas 51 3% 28 23
Urinary Bladder 49 3% 38 11
Lymph Node 47 3% 24 23
Stomach 21 1% 13 8
Unknown Primary 17 1% 7 10
Esophagus 11 1% 10 1
Liver 10 1% 7 3
Total 1,624 100% 681 943
sites seen at Baptist Jacksonville compared to
state and national statistics. Similar to previous
years, there is an essential doubling of the
incidence of breast cancer seen at Baptist Cancer
Institute compared to both Florida and the
United States and likewise a marked increase
in the number of female genital and melanoma
cancer cases seen compared to again the state
of Florida and the U.S. average. Offsetting
this is a modest decrease in the number of
prostate and lung cancer cases seen at Baptist
Jacksonville compared to both Florida and the U.
S. average. A 5 percent incidence of colorectal
cancer seen at Baptist Jacksonville unfavorably
compares to the overall national incidence
of 9 percent. This variance most probably
represents referral patterns of this primary site
to gastroenterologists for endoscopy and then
9

Table 2 Primary Sites : Baptist Medical Center South (2011)
Site Total % Male Female
Breast 127 27% 0 127
Lung 50 10% 24 26
Colorectal 47 10% 19 28
Thyroid 31 7% 5 26
Kidney 29 6% 18 11
Urinary Bladder 27 6% 19 8
Prostate 21 5% 21 0
UGI 19 4% 14 5
Other Sites 15 4% 7 8
Lymph Nodes 18 4% 13 5
Blood & Bone Marrow 17 4% 11 6
Melanoma 16 4% 11 5
Brain & CNS 12 3% 4 8
Pancreas 10 2% 5 5
Female Genital 9 2% 0 9
Head & Neck 6 1% 6 0
Unknown Primary 4 1% 2 2
Total 458 100% 179 279
for surgery. Baptist Jacksonville fell within the
national average percentage for other primary
sites except for melanoma and CNS tumors
which certainly represent our active neuro-
oncology program, as well as the expertise in
melanoma care at Baptist Jacksonville.
The Tumor Registry also maintains a list of
individual cases discussed and attendance at
the Tumor Board as well as that of the multi-
disciplinary breast conference, neuro-oncology
conference, and lung cancer conferences.
Participation at these conferences assures the
adequate representation of all primary sites
are discussed as mandated by the American
College of Surgeons to maintain a commission
on cancer certified tumor registry. Separate
multi-disciplinary breast conferences are held at
Baptist Jacksonville, Baptist South, and Baptist
Beaches. All multi-disciplinary conferences
10

Table 3 Comparison Data with Florida and United States
Organ SiteBaptist Cancer
InstituteFlorida United States
Breast 27% 14% 14%
Lung 11% 15% 14%
Prostate 12% 15% 15%
Female Genital 7% 3% 4%
Melanoma 6% 5% 4%
“Figures for Florida and U.S. are estimates from Cancer Facts and Figures 2011”
as well as Tumor Board are patient focused
discussions regarding diagnoses and treatment
approaches. Continued medical education (CME)
and continuing education units (CEU) credits
are available by the Baptist Health continuing
education program for these conferences. The
Tumor Registry is also available for questions
concerning treatment outcomes or any other
questions that arise from medical staff or
community.
The Tumor Registry also reviews the organization
of the weekly multi-disciplinary tumor conference
as well as assists the Cancer Committee in
evaluation outcomes, quality of medical care,
assessment of complications, recurrence, and
survival rates. Currently, the Baptist Tumor
Registry accumulates data from Baptist
Jacksonville as well as Baptist South. Baptist
Medical Center Beaches has a separate Tumor
Registry. All data is reviewed prior to entering
it into the Tumor Registry and a composite 10
percent of patients are then further reviewed by
physician volunteers for accuracy and timeliness
of data entry. Currently, Melissa McCarthan,
RHIT, CTR; April Stebbins, RHIT, CTR; and
Rassy Sprouse, BS, staff the Tumor Registry
and are supervised by Linda Huntley, Director
of Oncology Services, as well as physician
supervisors Troy Guthrie, Jr., MD, and Mark
Augsperger, MD.
11

The number of breast cancer cases which are
accrued to the Baptist Health Tumor Registry
at Baptist Jacksonville consistently exceeds the
state of Florida and national average. In 2011,
there were a total of 434 cases entered into the
tumor registry representing 27 percent of all cases
which exceeds the national and state of Florida
average of 13 percent. Similar to previous years
and similar to the national average, the majority of
these cases are early stage breast cancer (Figure
4). Seventy-nine cases or 18 percent were DCIS,
190 cases (44 percent) were Stage I and 113
or 26 percent were Stage II. These early stage
breast cancers represent 88 percent of all breast
cancers seen and we would expect that all but a
few of these women would ultimately be cured of
their breast cancer. Stage III was 33 or 8 percent
in which many of the patients would ultimately
die of their breast cancer and Stage IV was 18
patients or 4 percent and we would expect all
of the patients to ultimately die of their breast
cancer. Out of these 434 cases, only one or less
than one percent is classified as unknown stage
assessing to the tenacity of our Tumor Registry in
adequately staging the patients.
Breast cancer consistently represents a very
high percentage of the cases seen at the Baptist
Cancer Institute compared to the U.S. average.
This attests to the effective network in which
primary care physicians work with our digital
mammogram screening program to diagnose
patients at an early stage and move them into
the organized breast cancer program run through
the multi-disciplinary Hill Breast Clinic. In 2011,
the breast health program spent its first full year
in the Hill Breast Center at the Baptist Outpatient
Center. Two nurse navigators assisted patients
and physicians to optimize patient convenience as
well as patient care. A breast survivorship program
with nutrition, physical therapy and psychosocial
support is in place to enhance the overall
experience in patients seen at the Hill Breast
Center. Cutting-edge surgery programs with
intraoperative radiation began in the fall of 2012.
Limited breast radiation with the MammoSite
and more recently IntraBeam® for intraoperative
breast radiation are in place. Cutting-edge
research programs both in the adjuvant and the
more advanced metastatic setting are offered at
the Baptist Cancer Institute, through both medical
oncology with cooperative group studies as well
as pharmaceutical sponsored and the radiation
therapy through the RTOG research group. Other
assets for optimizing the care of breast health
patients at the Baptist Cancer Institute through
the Hill Breast Center program include genetic
risk assessment led by Melinda Fawbush, MSN,
ARNP, which assists patients and their families in
making decisions for both the type of surgery and
other long-term preventive programs if they are
know to have increased genetic risks. Psychosocial
support is provided by George Royal, PhD, and
an increasing involvement in breast survivorship
services include nutrition, physical therapy, and
lymphedema treatment. All of these services
continue to enhance the breast health program
and increase Baptist Cancer Institute’s share of
breast care patients within Northeast Florida and
Southeast Georgia.
Breast Cancer
12

Figure 4 Baptist Cancer Institute Breast Cancer Staging: 2011
60
50
40
30
20
10
00 1 2 3 4 Unknown
18
44
26
8
4
0
Pe
rce
nt
S tage
Figure 5 Baptist Cancer Institute Breast Cancer-DCIS Accrual
90
80
70
60
50
40
30
20
10
0
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
8
17
25
23
29 30
34
39
43
40
56
71
61
55
50
60
55
68
81
85
Nu
mb
er
of
Pa
tie
nts
80
79
Figure 5 shows the number of cases of ductal
carcinoma in situ seen at Baptist Cancer Institute
since the establishment of the Tumor Registry
in 1990. Seventy-nine cases were seen in 2011,
which is essentially the same as the previous year
in 2010. All of these cases of ductal carcinoma in
situ will be cured with local therapy and represent
a success of the wide use of screening digital
mammograms within our system.
13

Figure 6 Baptist Cancer Institute Lung Cancer Staging: 2011
50
40
30
20
10
00 1 2 3 4 Unknown
0%
32%
8%
13%
41%
6%
Pe
rce
nt
S tage
Baptist Cancer Institute saw 186 patients with
lung cancer in 2011. As in past years, the patients
who were accrued in our Tumor Registry were
predominantly advanced cases. Unfortunately, 77
cases were Stage IV, representing 41 percent of all
lung cancer seen. Twenty-five or 13 percent were
Stage III, who have approximately a 20 percent
chance of being cured. Fourteen patients were
Stage II, in which the cure rate is approximately 35
percent, and 58 or 32 percent were Stage I in which
over half the patients are cured with local therapy
(Figure 6). The proportion of patients with lung
cancer seen at Baptist Jacksonville is 11 percent,
slightly lower than the 14 percent seen nationally.
This percentage of patients, as well as total
numbers, represented a drop from the previous
years of 241 patients, which was 15 percent of
the cancer seen last year. Similar to statistics both
in Florida and the United States, the majority of
patients with lung cancer are Stage III and IV, which
are poorly curable. This presentation in advanced
stage represents no accepted screening program
for at least the patients seen in 2011. Recently,
the role of low-dose screening CT scans has been
reaffirmed at the national level, but is not widely
accepted since the number of false negatives and
unnecessary biopsies is a troublesome handicap
for its widespread use. One bright spot in lung
cancer at Baptist Health is the multi-disciplinary
lung cancer program led by Bridget Rossi, RN,
MSN, OCN, nurse navigator. She has established
a foundation to assist needy patients in all aspects
of their care from diagnosis to end of life. The role
of the stereotactic radiosurgery program at Baptist
Cancer Institute has likewise expanded since
selected patients with Stage I, particularly who are
frail, has become accepted. Research areas within
the Baptist Cancer Institute include the continued
participation in a cooperative group adjuvant
non-small cell lung cancer, as well as innovative
targeted therapies for metastatic and recurrent
non-small cell lung cancer.
Lung Cancer
14

Figure 7 Baptist Cancer Institute Prostate Cancer Staging: 2011
60
50
40
30
20
10
00 1 2 3 4 Unknown
0%
30%
62%
2% 3% 3%
Pe
rce
nt
S tage
In 2011, Baptist Cancer Institute Tumor Registry
assessed 199 prostate cancer cases, which was little
changed from 2010 when 204 cases were registered.
This still represents a dramatic drop from 2009 and
2008, when more than 300 cases were assessed each
year. This drop in prostate cancer accrual represents a
clear cut change in referral patterns in the community
where many patients are now being both biopsied
and referred to outside treatment facilities. However,
as in previous years, the vast majority of patients
are either Stage I (60 patients), which represented
30 percent of the patients seen, or Stage II (124
patients), which represented 62 percent of patients.
Thus 92 percent of patients were either Stage I or
Stage II in which the vast majority will be cured with
either surgery or some form of radiation treatment.
Only four patients or 2 percent and six patients or 3
percent were Stage III and Stage IV respectively. Five
patients or 3 percent were unknown stage which again
represents a success for our Tumor Registry which
accurately staged all but 3 percent of the patients
(Figure 7). Those patients generally were cases which
were referred outside our institute prior to completing
staging workup. The Baptist Cancer Institute continues
the prostate screening program which has been
sponsored by both Baptist Cancer Institute and
the NFL Jacksonville Jaguars for many years. The
prostate cancer prevention program trial was closed
in 2011 and unfortunately found no benefit from the
use of antioxidants either in the form of Selenium
or vitamins in decreasing the incidence of prostate
cancer. Radiation treatment at Baptist Cancer Institute
includes the state-of-the-art IMRT Radiation Therapy,
seed implants, and urologic surgeons have the da
Vinci Robotic Surgery Program. Patients entered on
an innovated immunotherapy program with the use
of Ipilimumab for advanced castrate resistant prostate
cancer continue to be followed in 2011 and 2012.
The use of innovative new treatments for patients
previously considered refractory to hormone treatment
has improved with two new drugs being approved by
the FDA for castrate resistant prostate cancer patients
seen at Baptist Cancer Institute.
Prostate Cancer
15

Figure 8 Baptist Cancer Institute Gynecological Cancer Staging: 2011
60
50
40
30
20
10
00 1 2 3 4 Unknown
6%
55%
4%
18%
10%
7%
Pe
rce
nt
S tage
In 2011, the Gynecologic Cancer Program at
Baptist Cancer Institute continued to be active in
terms of numbers of patients with 104 patients
seen in the calendar year 2011. As illustrated in
Figure 8, 59 percent or 62 patients were Stage
I and II which in general are felt to be readily
curable by surgery or surgery plus radiation. Only
28 percent of patients were Stage III and IV and
7 or 7 percent had inadequate information to
properly stage. This high percentage of patients
in early stage represents a success in American
cancer management with a high utilization by
American women of standard guidelines for
pelvic exam and Pap smear. The percentage of
female genital cancer seen at Baptist Cancer
Institute (6 percent) reflects favorably with the
5 percent average reported in other United
States tumor registries.
Female Genital Track Cancer
16

Figure 10 Melanoma Cancer Staging: 2011
50
25
0Stages 0 1 2 3 4 Unknown
0%
12%
43%
15%
6%
2%
Pe
rce
nt
S tage
12%
In 2011, Baptist Cancer Institute tumor registry
assessed 90 cases of patients diagnosed with
melanoma. This mirrors a trend which started
in 2005 with steadily increasing numbers of
melanoma patients seen at Baptist Jacksonville.
Most of those patients represented early stage
either Stage 0, which is in situ disease which
accounted for 12 patients or 13 percent, Stage I,
43 patients or 48 percent and Stage II, 15
patients or 17 percent. Overall, these Stages 0-II
represent a total of 78 percent of the patients
in early stage with an expectation of around 90
percent of those patients will be cured (Figure
10). Unfortunately, six patients or 7 percent and
two patients or 2 percent were Stages III and IV,
most of whom would not be expected to survive
five years. Another troublesome aspect is that
12 patients or 13 percent were unknown stage,
most probably representing leaving the institution
prior to completing staging and having their
treatment elsewhere.
These patients which represented 6 percent of
all cancer cases seen at Baptist Cancer Institute
and accrued into our Registry compares favorably
with the 5 percent rate for the state of Florida
and the 4 percent rate for the United States.
This high percentage of melanoma patients
seen at Baptist Cancer Institute almost certainly
represents the surgical and medical oncology
expertise in this tumor site which is recognized
throughout Northeast Florida and Southeast
Georgia. State-of- the-art surgical approaches
include lymph node mapping, and expertise in
wide local excision from melanomas occurring
in all sites of the body is present. Likewise,
medical oncology has extensive expertise in
the use of immunotherapy as both an adjuvant
treatment and a systemic treatment for metastatic
melanoma. A wide variety of research studies
including innovative adjuvant treatment protocols
through the ECOG study group and multiple
studies investigating the role of Ipilimumab
in metastatic melanoma was in place in 2011.
Multiple patients were referred from outside
the institution for involvement in those
research studies.
Melanoma
17

Tumor Review:Hodgkin’s Disease at Baptist Cancer
Institute Mark Augspurger, MD, Radiation Oncologist
Each year, approximately 7,500 new
cases of Hodgkin’s disease (HD) will
be diagnosed in the United States. In
contrast to the increase in incidence of
Non-Hodgkin’s lymphoma over the past
several decades, the annual incidence of
Hodgkin’s disease has remained stable.
There has been an increase in the accuracy of
diagnosis and staging, as well as an increasing
utilization of combination chemotherapy for the
treatment of HD. More than 75 percent of newly
diagnosed Hodgkin’s disease lymphoma cases will be
cured.
B a p t i s t C a n c e r I n s t i t u t e 2 0 1 2 A n n u a l R e p o r t

Epidemiology and Etiology
Hodgkin’s disease has a slight increased
incidence of male cases to female, approximately
1.3:1. The age of onset of Hodgkin’s disease is
a bimodal presentation with the largest group
of patients in the second and third decade of
life and a second smaller peak after age 50. The
second peak is probably an artifact of histologic
misclassification since recent studies have shown
that many of these cases diagnosed as Hodgkin’s
disease in the older age group were in fact Non-
Hodgkin’s lymphoma. In terms of race, Hodgkin’s
disease is much more common in Caucasians
than African Americans. There are no well
established etiologic factors causing HD. Case
match studies show that it’s slightly higher in a
familiar cluster pattern and is also more likely to
occur in those of higher economic status. There
has been extensive ongoing debate whether the
Epstein Barr virus is implicated in the etiology
of Hodgkin’s disease but to date this remains
unsettled. Patients infected with the Human
Immune Deficiency Virus (HIV) seem to have
a higher incidence of Hodgkin’s disease when
compared to age match control, but it is unclear
why this association occurs.
19

Figure 1 Cases by Gender (2001 - 2011)
50
40
30
20
10
0
48
39
No
. of
Ca
ses
Male Female
Figure 2 Cases by Race (2001 - 2011)
70
60
50
40
30
20
10
0
68
14
No
. of
Ca
ses
White Black Other
5
Signs, Symptoms and Diagnosis
Hodgkin’s disease is a lymph node based
malignancy and commonly presents as an
asymptomatic lymphadenopathy which may
progress to symptomatic disease. The majority
of patients, more than 80 percent, present
with lymphadenopathy above the diaphragm
involving the anterior mediastinum, cervical
and less commonly axillary and below the
diaphragm adenopathy. Only in the latest stages,
is visceral disease such as lung, liver, and bone
marrow involved. Involvement of Waldeyer’s
ring is quite uncommon. Approximately 40
percent of patients present with systemic
symptoms. Classically these B symptoms
include sweats, fever, weight loss and chronic
pruritis. These symptoms occur more frequently
in older patients and have a negative impact
on prognosis. Diagnosis is made by a biopsy
of a suitable lymph node and histopatholigic
examination by an experienced pathologist.
The diagnostic Reed-Sternberg cell is found
within the appropriate lymph node milieu and
these cells on histopathologic exam are typically
CD30+ and CD15+ by immunohistochemical
staining. Flow cytometry is generally not
helpful in making a definitive diagnosis of
Hodgkin’s disease. Staging is typically based
on the number of lymph node sites involved,
whether these lymph node sites are above or
below the diaphragm and whether or not the
patient is asymptomatic (A) or symptomatic (B.)
Typically, these cases of Hodgkin’s lymphoma
are separated into four histologic categories:
20

lymphocyte predominant, nodular sclerosing,
mixed cellularity, and lymphocyte depleted.
At one time, histopathologic subtype was
important, but more recently it has been found
that the pathologic stage trumps histologic
subtype in terms of long-term prognosis. The
staging system used is a modified Ann Arbor
staging system and consists of the following:
• Stage I is involvement of a single lymph node
region;
• Stage II is involvement of two or more
lymph node regions on the same side of the
diaphragm;
• Stage III is involvement of lymph node
regions on both sides of the diaphragm;
• and Stage IV is involvement of extra nodal
sites such as lung, liver or bone marrow and
not contiguous to a known nodal site.
The designation A means no symptoms and B
means the presence of fever, drenching sweats,
weight loss or intractable chronic pruritis. Bulky
disease is considered a maximum diameter
of a lymph node mass greater than 9cm. In
general, Hodgkin’s disease is staged clinically
with imaging studies such as CT scans or PET CT
scans rather than surgical pathologic staging.
Treatment and Outcome
Treatment of Hodgkin’s disease involves the
application of combination chemotherapy with
selective cases receiving radiation therapy
particularly for bulky disease. Currently, in 2013,
the only patients who are treated with radiation
alone are typically those who have Stage IA
disease involving high cervical nodes. For Stages
IB to Stage IVB, combination chemotherapy,
classically the ABVD (Adriamycin, Bleomycin,
Vinblastine, and Dacarbazine regimen) is
employed with radiation therapy reserved for
bulky lymphadenopathy usually given at the
completion of combination chemotherapy. For
most patients, four to six cycles of chemotherapy
is employed. Surgery other than lymph
node biopsy for diagnosis has no role in the
therapeutic management of Hodgkin’s disease.
Outcome is based on primarily stage with
obviously earlier stage disease doing significantly
better than later stage disease. Overall, for
Stage I, approximately 85-90 percent of patients
will be expected to be disease free at five years,
for Stage II 75-80 percent will be disease free
at five years, for Stage III 55-65 percent will
be alive and disease free at five years, and for
Stage IV 45-55 percent will be alive and free
of disease at five years. Adverse prognostic
factors include age greater than 50 years, bulky
disease, and advanced stage. Patients with
other immunodeficiencies such as HIV or post-
transplant, likewise, do poorer. For patients
who reoccur, combination chemotherapy with a
different chemotherapy regimen plus autologous
transplant appears to cure 25-30 percent of
those patients. A new targeted therapy is
currently available, brentuximab; a monoclonal
antibody to CD30 and appears to have high
response rates in the 70-80 percent range but
has been commercially available only for two
years and its exact role remains to be defined.
At Baptist Health, the Tumor Registry of Baptist
Cancer Institute accrued a total of 87 cases
21

Figure 3 Cases by Stage (2001 - 2011)
50
40
30
20
10
0
0 1 2 3 4 Unknown N/A
0
34
30
7 7
8Nu
mb
er
of
Ca
ses
S tage
1
between 2001 and 2011, an average of 8.7
cases were seen yearly. Out of those patients,
48 were male and 39 were female for the
expected slight male predominance of 1.3:1.0,
as seen in national databases (Figure 1). Again,
similar to national databases, there is a strong
predominance of caucasian patients with 68
being caucasian, 14 being African American
and five being other races (Figure 2). Staging
showed that predominance of patients were
early stage with 34 of 87 being Stage I, 30 of 87
being Stage II, seven were Stage III, seven were
Stage IV, eight were stage unknown and one was
non-analytic (Figure 3). In terms of treatment,
there was a major problem with our data. On the
initial data run, 50 of 89 were listed as having
received no therapy and seven of 89 were listed
as receiving surgery or biopsy only. This data
will be reviewed under our article for quality
assurance but to briefly summarize, most of these
patients listed as receiving surgery alone or no
chemotherapy actually received chemotherapy
as outpatients and were not captured by the
tumor registry. Survival was extremely good as
would be expected in more than 80 percent of
Stages I, II, and III being five year survivors and
only Stage IV dropping down to 57 percent and
as essentially expected in the national database
(Figure 4).
Thus, in summary, the information on Hodgkin’s
disease was flawed by a large number of cases
in which treatment was done outside of the
hospital and was not captured by the tumor
registry. However, all other aspects of the data
including number of cases, male to female ratio,
race, stage, and long-term survival appeared
consistent with that seen at the national level.
22

Figure 4 Survival Rates Over Five Years (Cases Diagnosed 2003 - 2005)
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
Cum
ula
tive
Sur
viva
l R
ate
s
0.0
Years from Diagnosis
1.0 2.0 3.0 4.0 5.0
Stage I Stage I I Stage I I I Stage IV
23

Soft tissue sarcomas are a group of rare,
but anatomically and histologically quite
diverse neoplasms. This is due to their
varying location within the soft tissues
of nearly all body sites. Currently, there
are more than three dozen recognizable
histological distinct subtypes occurring within
the body. Each year approximately 7,000 new
cases of soft tissue sarcoma are identified and
approximately 4,000 patients die of this disease. The
age adjusted incidence is two cases/100,000 persons.
Tumor Review: Soft Tissue
Sarcomas at Baptist Cancer
InstituteTroy Guthrie, MD, Medical Director,
Baptist Cancer Institute
B a p t i s t C a n c e r I n s t i t u t e 2 0 1 2 A n n u a l R e p o r t

Epidemiology and Etiology
In soft tissue sarcomas, there is a slight male
predominance with the male to female ratio
being approximately 1.1:1. Approximately 50
percent of soft tissue sarcomas will occur in
adults older than 60 years and 50 percent below
age 60. The vast majority of soft tissue sarcomas
occur in caucasians, 86 percent, 10 percent in
African Americans, and 4 percent in other ethnic
groups. There is no geographical distribution.
In terms of risk factors, soft tissue sarcomas
clearly have been reported to originate within
previously irradiated fields and often develop
decades after radiation. The majority of those
malignancies arising within radiation fields are
high grade lesions. Chemical exposures in certain
occupations such as those working in factories
making plastics or solvent exposure have likewise
been reported as a risk factor. There are rare
genetic syndromes such as von Recklinghausen
disease, tuberous sclerosis, and others which
have likewise been linked to specific types of soft
tissue sarcomas. In general, however, the vast
majority of soft tissue sarcomas are not linked to
any specific etiology.
Signs, Symptoms, and Diagnostic Workup
In terms of signs and symptoms, the majority
of soft tissue sarcomas present either in the
extremities or superficial trunk as a mass lesion
either exerting pressure or causing pain due to
mass expansion. Many of these malignancies are
found incidental to self-examination or physician
examination. Approximately, 15 percent of soft
tissue sarcomas arise in the retroperitoneal and
present as an abdominal mass with about half
of patients reporting pain. Physical exams of
patients with soft tissue sarcomas usually reveal
a palpable mass but little else is noted. General
laboratory testing likewise is non-diagnostic.
Imaging studies are the most important
evaluation procedures and usually include either
CTs or MRIs of the affected area as well as CT
scans, primarily of the lung looking for metastatic
lesions. Diagnosis is usually obtained either by
image guided core needle biopsy or excisional
biopsy performed by an experienced surgeon.
In general, if the lesion is on the extremity, the
pathway of the biopsy should be planned such
that it can be resected in total within a definitive
surgical procedure later since there is some risk
of seeding the tract with malignant cells and
having secondary lesions develop within the
biopsy tract if not completely excised.
25

Figure 1 Cases by Gender (2001 - 2011)
25
20
15
10
5
0
17
22
No
. of
Ca
ses
Male Female
Figure 2 Cases by Race (2001 - 2011)
35
30
25
20
15
10
5
0
26
10
White Black Other
3
No
. of
Ca
ses
Histopathology
In general, the histopathological diagnosis
is made of the tissue of origin, for example,
fibrosarcoma from fibrous tissue or
rhabdomyosarcoma from striated muscle
cells. The most important determinant of
prognosis is the grade of the tumor, with
grading being Grade I low grade, Grade II
intermediate grade, or Grade III high grade
tumors. Some histopathological types, such as
rhabdomyosarcoma or fibrous histiocytoma, are
automatically assigned a high grade status. The
staging of soft tissue sarcomas depends on four
factors: primary tumor, which is based on size
either greater than 5cm or less than 5 cm and
whether or not they are superficial a. deep, b.
grade of the tumor: being well differentiated
grade I; moderately differentiated grade II;
poorly differentiated grade III or undifferentiated
grade IV, presence or absence of lymph node
involvement, and presence or absence of
metastatic lesions. In general, early stage lesions
are low grade or intermediate lesions that are
small and advanced stage lesions are lesions
that are high grade, large lesions and may have
metastatic lesions. Because soft tissue sarcomas
tend to be asymptomatic until reaching a large
stage SEER data shows that most adult soft
tissue sarcomas present in more advanced Stage
III or Stage IV stages.
Treatment
The treatment of the primary lesion is surgical
resection with wide margins. In particular, for
soft tissue sarcomas occurring in the extremities,
it is felt when possible that the surgery should
be done by an experienced surgical oncologist
so that limb sparing when possible can be
achieved. If initial surgical resection of a soft
tissue sarcoma is impossible then preoperative
treatment with both radiation therapy and in
certain circumstances either systemic or limb
arterial perfusion of chemotherapy is advised.
Most often it is felt that patients needing this
treatment should be referred to medical centers
where a multi-disciplinary team experienced in
26

Figure 3 Cases by Stage (2001 - 2011)
20
15
10
5
0
0 1 2 3 4 Unknown N/A
0
7
3
10
1
14
Nu
mb
er
of
Ca
ses
S tage
4
managing soft tissue sarcomas is available. Thus
often soft tissue sarcomas, while diagnosed in
one institution, are referred outside for definitive
treatment particularly of the primary lesion.
In general, there is a low incidence of lymph
node involvement for soft tissue sarcomas and
routine lymph node dissection during surgical
procedures is not done.
The role of radiation therapy is both preoperative
and postoperative in the definitive management
of the primary site. In patients who have locally
advanced lesions, deployment of radiation
therapy either with or without adjuvant
chemotherapy has resulted in higher rates
of definitive resection of the primary site. In
patients who have been resected up front and
who have either positive or close margins and a
high histological grade, there have been both
retrospective and prospective studies showing
application of radiation therapy to the primary
site results in a drop in local recurrence rates.
The role of chemotherapy in soft tissue sarcomas
is much less well defined compared to surgery
and radiation. Typically, response rates to
chemotherapy are low. Complete remissions are
rarely produced and the duration of response
is quite short. Chemotherapy drugs used to
treat soft tissue sarcomas include doxorubicin,
ifosfamide, dacarbazine, and occasionally
other chemotherapy agents. Response rates
to combinations of chemotherapy agents such
as doxorubicin, ifosfamide +/- dacarbazine
are higher but do not seem to translate into
a long-term survival advantage. In general,
chemotherapy is reserved for improving local
control preoperatively and palliative treatment of
metastatic disease. Of note, some patients with
surgically resectable metastatic disease do seem
to benefit from surgical resection particularly
if the metastases are in the lungs. Targeted
therapy for certain soft tissue sarcomas, such as
dermatofibrosarcoma and certain other soft tissue
sarcomas, has an evolving role. These soft tissue
sarcomas (PDGFα) express a target such as c-KIT
or platelet derived growth factor alpha and can
be treated with targeted agents such as Imatinib
or Dasatinib.
27

Figure 4 Cases by Treatment (2001 - 2011)
20
15
10
5
0
SurgerySurgery/Radiation
None Surgery/Chemo Chemo All Others
12
11
5 4
3
4
Nu
mb
er
of
Ca
ses
The records of the Baptist Cancer Institute Tumor
Registry were reviewed from 2001 to 2011.
The cases were analyzed and compared to the
national cancer database. During this time, 39
patients with soft tissue sarcoma have been an
accession to our Tumor Registry averaging four
patients each year. Of those 39 patients, 17 were
male and 22 were female–slightly different from
the usual male/female ratio reported (Figure 1).
In terms of race, 26 were caucasian, 10 African
American, and three represented another ethnic
group (Figure 2). Staging showed seven were
Stage I, three were Stage II, 10 were Stage III,
one was Stage IV, 14 were unknown stage and
four were non-analyzable (Figure 3). This higher
proportion of non-analyzable and unknown stage
represents the fact that a large portion of patients
were referred to outside institutions, particularly
Mayo Clinic and the University of Florida
Gainesville for a specialized multi-disciplinary
team to treat these rare malignancies.
Treatment, in general, followed the same lines
as that reported in national databases (Figure 4).
Twelve of the patients or 30.8 percent received
surgery, 11 (28.2 percent) received surgery plus
radiation, and four (10.3 percent) received surgery
plus chemotherapy. A total of 27 of the 39 or
69.2 percent received some form of surgical
treatment as would be expected from national
databases. Five or (12.8 percent) were listed as
receiving no specific therapy but were referred
out and probably received standard care. Three
patients received chemotherapy alone in palliative
treatment. These percentages would be the same
as expected in national averages. Figure 5 shows
five year survival for our 39 patients and shows
81 percent of Stage I were alive at five years and
67 percent of Stage II were alive, 47 percent of
Stage III and only 14 percent of Stage IV had
survived five years. This is comparable to what is
published and shows that management of soft
tissue sarcomas is quite similar to that practiced
throughout the United States and end results
appear to be similar.
Thus this review of soft tissue sarcomas seen at
Baptist Cancer Institute from 2001 to 2011 shows
similar epidemiologic factors, similar treatments
except a higher percentage of patients referred
outside to receive specialized care. Our survival
data is likewise similar to that reported in national
SEER data.
28

Figure 5 Survival Rates Over Five Years (Cases Diagnosed 2003 - 2005)
100
95
90
85
80
75
70
65
60
55
50
45
40
35
30
25
20
15
10
5
0
Cum
ula
tive
Sur
viva
l R
ate
s
0.0
Years from Diagnosis
1.0 2.0 3.0 4.0 5.0
Stage I Stage I I Stage I I I Stage IV
29

The Tumor Registry and its database are
necessary for quality of care monitoring
provided by Baptist Cancer Institute.
The accuracy and dependability of
this essential service was evaluated
and examined as directed by the
American College of Surgeons and
the Commission on Cancer. A review of
the data that resulted in patient accrual
management and lifespan was assessed
during a 10-year period for Hodgkin’s
disease from 2001 through 2011. The
abstracts were reviewed for accuracy and
charts were pulled when deemed necessary.
Quality Assurance Troy H. Guthrie Jr., MD, Medical Director, Education and
Research, Baptist Cancer Institute, Melissa McCarthan, RHIT, CTR;
April Stebbins, RHIT, CTR;
and Rassy Sprouse, BS
B a p t i s t C a n c e r I n s t i t u t e 2 0 1 2 A n n u a l R e p o r t

The following are the results of the assessment
on the 87 patients entered by our Tumor Registry
during the above-mentioned time period. The
results are summarized as follows:
• Abstracts contained adequate information to
assess accuracy;
• There were no errors in the classification of
the Hodgkin’s patients identified in terms of
histology;
• Therapy of Hodgkin’s patients had many
problems in terms of identifying treatment.
• 50 out of 89 patients were listed as having no
therapy, and seven out of 89 patients were
listed as being treated with surgery alone.
Clearly this was inaccurate so charts were pulled
from the offices of 21st Century Oncology and
reviewed by Troy H. Guthrie, MD, and from the
office of Cancer Specialists of North Florida
and reviewed by Unni Thomas, MD. Of the
50 patients listed as having no treatments,
currently 10 have been identified as receiving
chemotherapy and three have been identified
as receiving chemotherapy plus radiation. Of
the seven patients listed as receiving surgery
alone to date, two have been listed as receiving
chemotherapy and one receiving chemotherapy
plus radiation. This is a laborious task and the
accuracy of data will continue to be reviewed
so that we can have accurate long-term follow-
up on Hodgkin’s disease patients from this time
period of 2001 to 2011; Kaplan-Meier curves
were readily available and appear to be accurate;
and demographics were available and appear to
be accurate.
Recommendations for correction include:
• Education was presented to the Tumor
Registry concerning treatment of Hodgkin’s
disease so that a red flag will be raised
if no therapy or surgery alone is listed as
treatment;
• Suggestions have been made to work
more closely with the clinicians of record
concerning any patient in whom the accuracy
of staging, treatment or survival including
phone calls would be warranted;
• Cancer physicians should be involved in
the abstraction process particularly up front
if information is missing or appears to be
inaccurate; and
• Request additional information from
physicians who refer patients for
management outside the institution so long
term follow-up can be accurate in terms of
treatment and survival.
31

In 2011, cancer research for the Baptist
Cancer Institute continued to function
at a high level on multiple sites,
including the Baptist Cancer Institute,
Florida Radiation Oncology Group,
and Cancer Specialists of Northeast
Florida. At any one time throughout
all campuses approximately 60 to
70 research protocols were available
for patients with diverse cancer sites
including breast, lung, gastrointestinal,
brain, melanoma, pancreatic, hematologic
malignancies, and other less common sites.
All protocols were available for patients at
Baptist Medical Center Jacksonville and Baptist
Medical Center South, as well as having referrals
from outside the Jacksonville area, including
Southeast Georgia. Studies were available to patients
originating from both national cooperative groups,
including the National Surgical Adjuvant Breast and Bowel
Project (NSABP), Eastern Cooperative Oncology Group (ECOG),
North Central Cancer Treatment Group (NCCTG), and Radiation
Therapy Oncology Group (RTOG), as well as many studies which came
through pharmaceutical companies and private research organizations (PRO).
Clinical Researchand Education
B a p t i s t C a n c e r I n s t i t u t e 2 0 1 2 A n n u a l R e p o r t

On campus, approximately 50 percent of the
studies were through National Cancer Institute
(NCI)-sponsored cooperative group studies
and the other half were industry sponsored
pharmaceutical studies.
All studies done on campus, either NCI-
sponsored or pharmaceutical-sponsored
were reviewed by the Baptist Medical
Center Institutional Review Board (IRB) for
appropriateness of research, conflict of interest
and protection of human rights. All studies were
then described in language understandable
by the public in an informed consent and
also published on the Baptist Cancer Institute
website. Phases of studies including phase I,
phase II, and phase III, were available in 2011.
In 2011, studies through the Baptist Cancer
Institute led to FDA approval for a number of
drugs, including Ipilimumab for the treatment
of metastatic melanoma, Aldo-herceptin for the
treatment of HER2+ breast cancer, and afatinib
for the treatment of EGFR mutation positive
non-small cell lung cancer. In addition to
treatment protocols, a number of registry
studies were done that include SystHERs
in HER2+ breast cancer that is metastatic,
treatment approaches in metastatic melanoma,
as well as studies in chronic myelocytic leukemia
and paroxysmal nocturnal hemoglobinuria. The
2011 patient accrual for all participants consisted
of 35 patients compared to the 65 patients in
2010 (Table 1). Accrual throughout the campus
has remained well below 100 patients per year
due to diverse reasons, including increasing
pressure on physicians to deal with increasing
patient volume, increasing complexity of
insurance and third party payment, as well as
reluctance of patients to participate in studies
that may cause economic pressure. Hopefully,
patient accrual will increase in 2012 to above
50 patients close to years past.
Baptist Cancer Institute continues to be an active
community cancer education program offering
CME sessions at the multi-specialty breast cancer
conference, neuro-oncology conference, and
lung cancer conference and tumor board. Table
2 lists the subjects of the annual tumor board
for 2012. Table 3 lists the active participants in
the cooperative groups at Baptist Health, as
well as those involved in the research programs
of the NSABP, and RTOG study groups. In
summary, the Baptist cancer program continues
to offer exciting clinical projects through
both cooperative group mechanisms as well
as pharmaceutical studies. A great deal of
enthusiasm on the campus exists for continuing
to increase patient accrual and increasing the
relevance of clinical trials for everyday treatment.
33

Table 2 Tumor Board : 2012
Table 1 Clinical Research BCI : 2008 – 2011
Year # of Patients
2008 88
2009 90
2010 65
2011 35
Breast Cancer Prevention Troy Guthrie, MD
Volatile Organic Compounds and the Early Detection of Lung Cancer Nir Peled, MD
Hosts of Lymphoma Troy Guthrie, MD
Melanoma Staging and Treatment Troy Guthrie, MD
Contemporary Head and Neck Oncology and Reconstructive Surgery Phillip Pirguosis, MD
Interventional Pain Management for the Spine Christopher Roberts. MD
Chronic Myeloid Leukemia Overview Troy Guthrie, MD
Melanoma Metastatic to Regional Lymph Nodes John Crump, MD
Post-mastectomy Radiation Therapy: Update and Indications Nicole Anderson, MD
Head and Neck Cancer Naeem Latif, MD
Multiple Myeloma Troy Guthrie, MD
Triple Negative Breast Cancer Dimitrios Agaliotis, MD
Non Small Cell Lung Cancer Troy Guthrie, MD
Cervix and Endometrial Cancer: Case Discussion and Brief Overview Michael Olson, MD
Prostate Cancer Naeem Latif, MD
The Management of Prostate Cancer Mark Augspurger, MD
Melanoma Update Gary Bowers, MD
Management of Anorectal Melanoma Hank Hill, MD
Neuro Oncology Tumor Board Multiple Presenters
34

Cooperative Group Trials (BCI)Dimitrios Agaliotis, MD, PhD – Medical Oncology
Jeff Bubis, DO – Medical Oncology
Stephen Buckley, MD – Gynecologic Oncology
Catherine Bush, RN, OCN, BSN – Study coordinator
Andrea Canto – Study Coordinator
Carlos Castillo, MD – Medical Oncology
Roxane Green – Regulatory Coordinator
Troy Guthrie, MD – Principal Investigator, ECOG, NSABP, Mayo Trials Group
Zhen Hou, MD, PhD – Medical Oncology
Douglas W. Johnson, MD – Sub-Investigator, Radiation Oncology
Robert A. Joyce, MD – Medical Oncology
Mohammad Khan, MD – Medical Oncology
Mathew Luke, MD – Medical Oncology
Alan Marks, MD – Medical Oncology
Joseph Mignone, MD – Medical Oncology
Yuval Naot, MD – Medical Oncology
Jeanine Richmond, RN, BSN, OCN, - Study Coordinator
Matthew Robertson, MD - Gynecologic Oncology
Mila Shteyn, MA - Study Coordinator
Alexander Moore – Study Coordinator
Unni Thomas, MD – Medical Oncology
Maria Valente – Medical Oncology
Prevention (NSABP and SWOG)Andrea Canto – STAR Program Coordinator
Troy Guthrie Jr., MD – Principal Investigator
RTOGCynthia Anderson, MD – Radiation Oncology
Mark Augspurger, MD – Radiation Oncology
Jessica Bahari, MD – Radiation Oncology
Abhijit V. Deshmukh, MD – Radiation Oncology
Kenneth Goldstein, MD – Radiation Oncology
Troy Guthrie, MD – Medical Oncology
Jeffrey Harris, MD – Medical Oncology
Douglas W. Johnson, MD – Principal Investigator
Anand Kuruvilla, MD – Radiation Oncology
Carla Malott, RN – Clinical Research Associate
Thomas Marsland, MD – Medical Oncology
Lois Morgan, RN – Clinical Research Associate
Michael Olson, MD – Radiation Oncology
Niraj Pahlajani, MD – Radiation Oncology
Shyam Paryani, MD – Radiation Oncology
Jan Peer, CCRP – Clinical Research Associate
Sonya Schoeppel, MD – Radiation Oncology
Neenad Sha, MD – Radiation Oncology
Dwelvin Simmons, MD – Radiation Oncology
Robert Still, MD – Surgeon
J. Wynn Sullivan, MD – Medical Oncology
Linda Sylvester, MD – Medical Oncology
Mitchell Terk, MD – Radiation Oncology
Carlos Vargas, MD – Radiation Oncology
John Wells, MD – Radiation Oncology
Larry Wilf, MD – Nuclear Medicine Radiologist
Michal Wolski, MD – Radiation Oncology
Cancer Risk Assessment and Genetics
Melinda Fawbush, ARNP, MSN
Troy Guthrie Jr., MD – Principal Investigator
Table 3
35

Distinguished Individual in
Cancer Care: E. Dayan Sandler, MD
Each year the Annual Report honors an
individual who has made a significant
contribution to the cancer program at
Baptist Health and to Baptist Cancer
Institute progress. In past issues, we
have honored both physicians and non-
physicians. This year we are honoring
Dayan Sandler, MD, Chief of Pathology
at Baptist Health. Dr. Sandler has made
numerous contributions to the cancer
program since joining the physician faculty in
1993.
Dayan obtained her Doctorate of Medicine from
the University of California School of Medicine San
Francisco, Calif., where she had previously obtained a
Doctor of Pharmacy. She did her post-graduate training
in the department of pathology at University of California San
Francisco from 1986-1990. She received intensive training in Cytology,
Dermopathology, and Hematopathology. After completing her pathology
residency, she received further training with a fellowship in nuclear medicine,
B a p t i s t C a n c e r I n s t i t u t e 2 0 1 2 A n n u a l R e p o r t

within the Department of Radiology again at the
University of California San Francisco in
1990-1991. She became a staff pathologist at
St. Mary’s Hospital in San Francisco from 1991
to 1992 prior to joining the clinical faculty at
Baptist Medical Center Jacksonville in 1993.
Here she has served in many positions, including
director of Immunohistochemistry, Histology,
Flow Cytometry Analysis Laboratory, and has
served as the director of Laboratory Medicine
from 1997 to the present. She also served as
the director of the Stem Cell Laboratory when
it functioned at Baptist Jacksonville from
1996-1999. She has been Chief of Pathology
since 2004 at Baptist Health. Dr. Sandler has
made numerous contributions to the cancer
program at Baptist Health, particularly in the
field of breast cancer. She has a breast cancer
consultation service and is the pathologist for the
Breast Conference. She also serves as primary
pathologist and as a major participant within the
recently established neuro-oncology
multi-disciplinary program. Dr. Sandler is widely
sought by both fellow pathologists and clinicians
for her opinions within the pathology field.
She has been an active member of the Cancer
Committee for 12 years, and more recently, has
served as committee chair of Baptist Health’s
System Breast Program Leadership.
She has been an active member of Tipping the
Scale Program, serving as both committee chair
and as a mentor. She has mentored four young
ladies, all of whom have gone to college.
On a personal note, her husband, Dr. Jeffrey
Sandler, is an Ear, Nose and Throat surgeon at
Baptist Medical Center South. They have three
children, Jonathan, Laura and Zachary, all of
whom are in college. Her greatest passion is
being with her family; all of them are outdoor
enthusiasts, and she loves kayaking, photography
and traveling.
E. Dayan Sandler, MD
37

Baptist Cancer Institute Donors | Calendar Year 2012
Ms. Julie K. Abbott
Mrs. Mary W. Ackerly
Acosta Sales and Marketing Co., Inc.
Adelante Group, Inc
Mrs. Letitia R. Aitken
All About Blinds
Mrs. Lucile W. Allsopp
Amanda Morrow LLC
Anonymous
Arlington Toyota
Mr. and Mrs. John Arnold
Mr. Sheridan T. Arnold
Mr. and Mrs. Paul M. Arvia
Mr. and Mrs. Douglas C. Asper
Atlantic Companies
Mr. and Mrs. Steven E. Austin
Mr. and Mrs. Stephen E. Bachand
Mr. Robert B. Bailey
Ms. Kathy Baker
Mr. and Mrs. Thompson S. Baker II
Ms. Purisima Balgos
Ms. Jacquelyn D. Bates
Ms. Cathy Battreall
Ms. Joan M. Bauer
Ms. Beverly R. Beck
Mrs. Beverly J. Behrens
Benchmark Custom Luxury Homes, Inc
Benchmark Homes Realty, Inc.
Mr. and Mrs. Gerald Bertisch
Mr. Robert E. Berwick
Mr. Otto J. Betz, Jr.
Mrs. Lucy Boesel
Mr. Robert Bon Durant
Ms. Connie Bones
Mr. Mac Bracewell
Ms. Kari M. Bracy
Ms. Lauren Braren
Mrs. Kay Brooks
Mr. John E. Buckey
Mr. and Mrs. Malcolm A. Buckey, Jr.
Mrs. Shirley J. Budden
Ms. Margaret A. Bulin
Mr. and Mrs. Phillip Burnaman
Ms. Lynn Y. Cabrera
Mrs. Gretchen H. Calvert
Cambridge Prep Academy
Mrs. Anastasia Cameron
Mr. Michael D. Cantrell
Ms. Esther F. Cantus
Dr. and Mrs. Perry G. Carlos
Ms. Marge Cash
Ms. Debbie Castroverde
Mr. and Mrs. George Catallo
Dr. and Mrs. Michael A. Chanatry
Ms. Robin C. Chandler
Claude Nolan Cadillac, Inc.
Mr. and Mrs. Gary A. Close
Coldwell Banker Walter Williams Realty, Inc.
Mr. C. Randolph Coleman
Mr. and Mrs. Douglas Coleman
Mr. and Mrs. Donald Cox
Ms. Esther G. Cruikshank
Ms. Sarah B. Dann
Mr. Earle Mauldin, III and Ms. Debbie L. Davidoff
Mr. and Mrs. John C. Davis
Ms. Carol DeGregorio
Mr. and Mrs. Greg Delaney
Mrs. Susan S. Delfs
Ms. Michelle Denbesten
Mr. and Mrs. Derek E. Dewan
Ms. Elana Dietz
Mr. and Mrs. Patrick S. Doran
Mrs. Robin Doyle
Drs. Mori, Bean & Brooks, PA
Mr. and Mrs. Charles N. Dunn, Jr.
Mrs. Lillian D. Durden
Mr. and Mrs. Gary Ehlig
Mr. Tucker W. Elliott
Mrs. Sharon A. Ellis
Mr. and Mrs. John H. Erstling
Mr. Gerard R. Evan
Mr. Lawrence W. Evans
Mr. and Mrs. William S. Fellner
Mr. and Mrs. Paul S. Ferber
Ferguson Enterprises
Fernandina Beach High School
Ms. Donna M. Fiedorowicz
First Coast Supply, Inc.
First Radiation & Oncology Group
Mr. and Mrs. Thomas J. Flanigan
Florida Blue
Florida Propane Partners, LLC
Ms. Judith Y. Flynn
Ms. Kathleen Foley
Fore In One Golf Services, Inc
Ms. Susan E. Forster
Mrs. Marie E. Frankiewicz
Ms. Virginia M. Fritz
Mr. and Mrs. Jim Furyk
Jim and Tabitha Furyk Foundation
Mr. and Mrs. James R. Gabrielsen
Mrs. Mary Louise Gallagher
Mrs. Charlene K. Gamewell
Mrs. Jane W. Gamewell
Gannett Foundation
Mrs. Margaret Gates
Georgia Xpress Lubes, Inc
Mr. and Mrs. Robert T. Golitz
Goodall Family Foundation
Mrs. Helene C. Gorab
Ms. Mary Ann Graham
Mr. and Mrs. Michael J. Grebe
Ms. J. A. Grunther
Mrs. Melody T. Gurney
Mrs. Pauline W. Guzek
Ms. Dorothy E. Hall
Mr. and Mrs. Y. E. “Chipper” Hall
Hamilton Family Foundation
Hanaya Enterprises LLC
Mrs. Maureen L. Hannan
Ms. Millie G. Harrison
Ms. April Hart
Ms. Elizabeth L. Harther
Mr. Greg Hartley
Dr. and Mrs. Gregory W. Hartley
Mr. John Haswell
Ms. Lisa Hathaway
Ms. Marion D. Haynes
Mrs. Shonda J. Heath
Major General Patricia P. Hickerson
Major General Patricia Hickerson
Mr. and Mrs. Robert E. Hill, Jr.
Mr. Hal Hitch
Ms. Susan Hitch
Mr. and Mrs. Howard I. Hodor
Mr. John J. Hofstetter
Mrs. Jill I. Hornsby
Mr. David K. Hunt
Mrs. Sharon Hunt
In the Pink Boutique, Inc
Innovations By Shelley
Ms. Melissa Intemann
Iridium Holding, Inc.
Ms. Roxanne Isaacs
J. McLaughlin
Jacksonville Jaguars Booster Club, Inc
Ms. Patricia A. Jensen
38

Mr. and Mrs. Walter Jewett
Mr. and Mrs. Richard O. Jones
Ms. Lucinda Jordan
K. Fehling & Associates
Mr. and Mrs. Ralph O. Kaufman, Jr.
Mr. Raphael M. Kelly
Ms. Shirley Ketchum Patterson
Mrs. Gail A. Killion
Ms. Beverly A. Koerner
Ms. Nancy Koob
Ms. Duffy M. Kopriva
Ms. Jennifer Lada
Ms. Shelley Laird
Mrs. Margaret V. Lehman
Mr. and Mrs. Herb LeMoyne
Lender Processing Services
Mr. and Mrs. Paul Lichlyter
Lilly USA, LLC
Ms. Lynda Linforth
Mr. Jeffrey Locke
Mrs. Jenny H. Lockett
Ms. Julia E. Lord
LuLu’s Waterfront Grille
Mr. and Mrs. William B. Lynch
Ms. Susan E. Mack
Ms. Diana Mackoul
Magnolia Point Women’s Club
Mrs. Virginia B. Maloney
Mr. and Mrs. James T. Mann
Ms. Barbara S. Maple
Marchese Communications
Mr. Randy Marshall
Ms. Beth McCague
Ms. Alison McCallum
Mr. and Mrs. Donald C. McGraw III
Mr. and Mrs. Rodney A. McLauchlan
Mrs. Christin McManus
Mr. and Mrs. Jeffrey G. McNeill
Mr. and Mrs. C. Keith Meiser
Mrs. Damara F. Merten
Ms. Marzena Mignone
Mrs. Barbara P. Miller
Ms. Betsy A. Miller
Mr. and Mrs. James R. Miller
Mr. Phillip Mills, CPA
Mr. John Minor
Mr. and Mrs. Michael Monaghan
Mrs. Melissa Morgan
Ms. Shelley Morgan
Mr. and Mrs. Eric B. Morris
Mr. and Mrs. Richard G. Morrison
Ms. Amanda Morrow
Mr. Charles A. Morrow, Jr.
Mrs. Christine C. Moyer
Mrs. Mary Murphy
Mr. and Mrs. Randal P. Nader
ND Industrial Corp
Dr. Kevin L. Neal, DDS
NFL Affiliate of the Susan G. Komen Foundation, Inc.
Mrs. Barbara Orr
Parker & Pennington, PA
Mrs. Ann Patsiga
Ms. Danielle Payne
Ms. Sharon Peacock
Mr. and Mrs. Joseph Pearce
Mrs. Gigi Pelletier
Dr. Patricia B. Pereira
Mrs. Marie C. Perry
PGA Tour, Inc.
PhRMA
Ms. Gussie D. Pokorny
Ponte Vedra Properties Realty LLC
Ms. Jane D. Porter
Mrs. Rose Puleo
Ms. Leigh Quijano
Mr. and Mrs. Brady L. Rackley
Ms Selina Rainey
Mr. Bernard E. Reidy
Ms. Barbara Resnick
Mr. and Mrs. Raymond S. Rizzo
Robert Williams Design, LLC
Ms. Cathleen Roden
Mr. A.C. Roemhild
Mr. and Mrs. Jack P. Rothacker
Ms. Nancy C. Rowe
Mr. and Mrs. William T. Roy
S.R.F.
Mrs. Robin Saltman
Dr. Brenda M. Samara, PhD
Mr. and Mrs. James R. Scielzo
Mr. and Mrs. Francis Seabrook
Seaside National Bank & Trust
Mr. Donald C. Shaffer
Mrs. Gail W. Shave
Mr. and Mrs. John H. Shields II
Mrs. Theodora P. Siragusa
Ms. Kerrie J. Slattery and Mr. Paul Lambert
Mr. and Mrs. James P. Smith, Jr.
Mr. and Mrs. Shepard C. Spink
Mrs. Martha Stachitas
Mrs. L. Elaine Stallings
Ms. Kimberly A. Steedman
Mr. and Mrs. C. L. Strickland
Mr. and Mrs. Thornton M. Swisher
Swisher International, Inc.
Mr. and Mrs. John Tancredi
Mrs. Cathleen C. Taylor
Mr. Joe T. Taylor
Mrs. Cynthia L. Thatcher
The Edna Sproull Williams Foundation
The Haskell Company
The Jacksonville Jewish Foundation
The RITA Foundation Inc.
Mr. and Mrs. Joseph A. Thompson
Mr. Kerry Tobin
Mr. Randolph Totten
Underwood Jewelers Corporation
Valentine Sales
Mrs. Julie Van Voorhis
Mrs. Julie Vermeulen
Ms. Tilghman H. Waesche
Mr. Ralph D. Wagoner
Mrs. Amy F. Wallman
Mr. and Mrs. Christopher W. Ware
Ms. Suzannah Warren
Ms. Elizabeth B. Watkins
Mr. Charles R. Weed
Mrs. Barbara T. Welch-Salmon
Mrs. Janette O. Wells
Ms. Donna WeMett
Mrs. Nancy M. Wertheimer
Mrs. Frances W. West
Dr. and Mrs. Robert E. Wharen, Jr.
Ms. Peggy A. Widicus
Ms. Debra H. Widner
Mr. and Mrs. John F. Wilbanks
Ms. Lisa J. Williamson
Mr. and Mrs. James T. (Tylee) Wilson
Ms. Tane M. Wilson
Ms. Janis A. Wotiz
Mr. Richard Yocolano
Mr. and Mrs. Richard Zanard
39

1235 San Marco BoulevardJacksonville, Florida 32207
904.202.2273
baptistjax.com