Embed Size (px)
Citation preview
Basics of Polysomnography Chitra Lal, MD, FCCP, FAASM
Assistant professor of Medicine, Pulmonary, Critical Care and Sleep,
MUSC, Charleston, SC
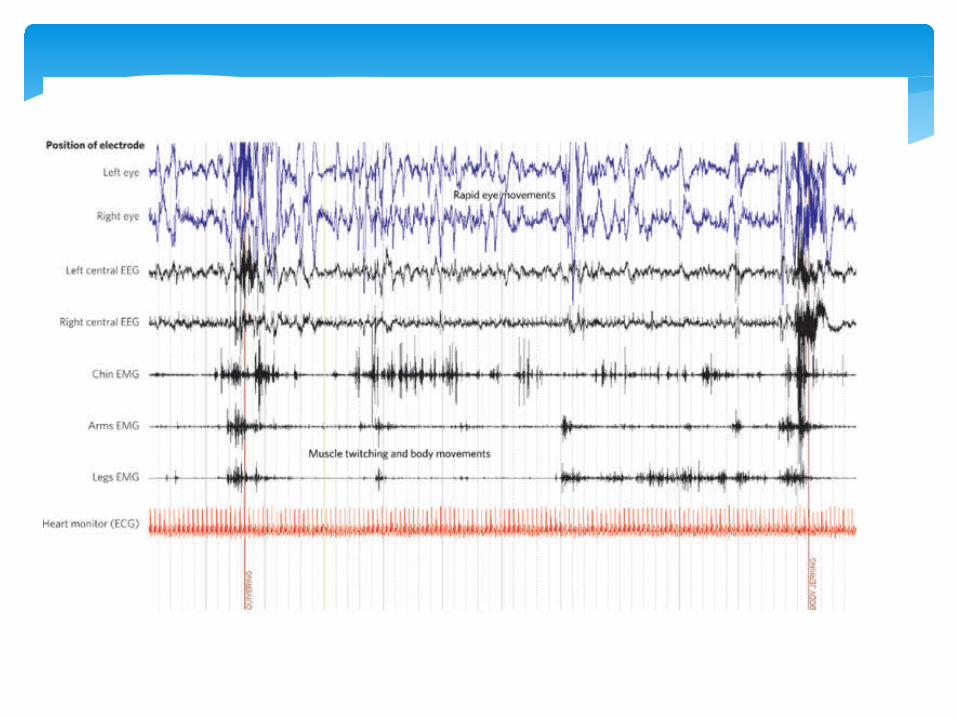
∗ Continuous and simultaneous recording of several physiologic variables during sleep
∗ EEG ∗ EOG ∗ EMG ∗ ECG ∗ Snoring ∗ Thoracic and abdominal movements ∗ SaO2 ∗ Airflow
Basics of Polysomnography
∗ Additional Channels : - End tidal Co2 (PetCo2) - Transcutaneous CO2 - PAP level - Esophageal pressure monitor - Additional EEG channels for nocturnal seizures - Video monitoring - Esophageal pH
Polysomnogram
∗ Diagnostic PSG ∗ PAP titration study ∗ Split night study
Types of Sleep Studies
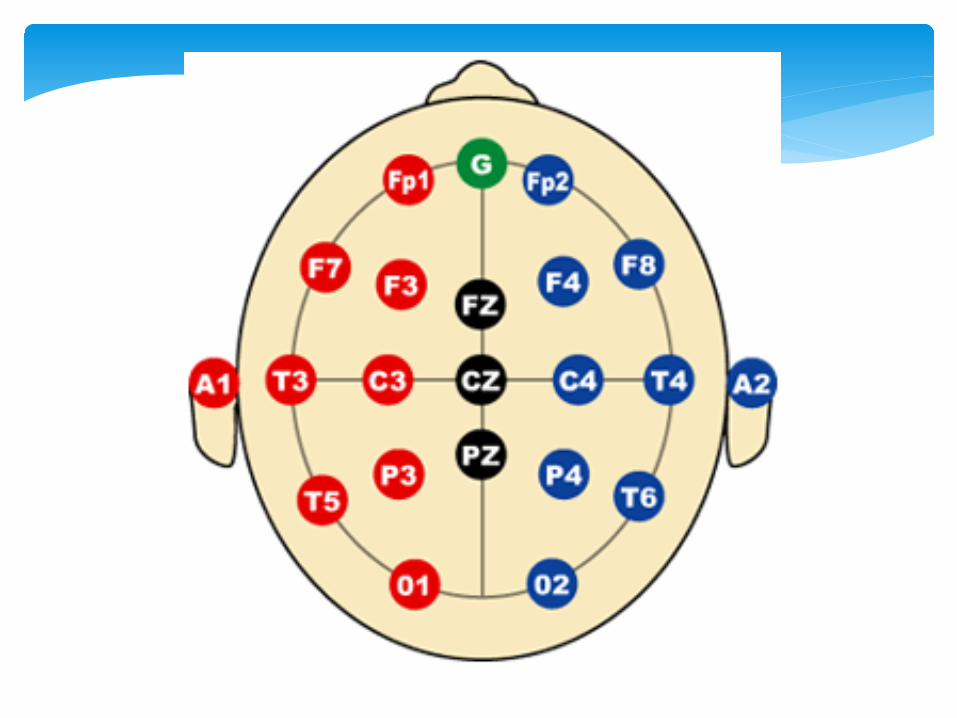
Electroencephalography
∗ International 10-20 system (10% or 20% inter-electrode distance) ∗ Electrodes are identified by letters representing brain regions
and a numeric subscript representing side of the body ∗ F is Frontal ∗ O is occipital ∗ C is central ∗ M is mastoid ∗ Odd #’s are left side, even #’s are right side, z is midline ∗ AASM recommends F4M1, C4M1 and O2M1
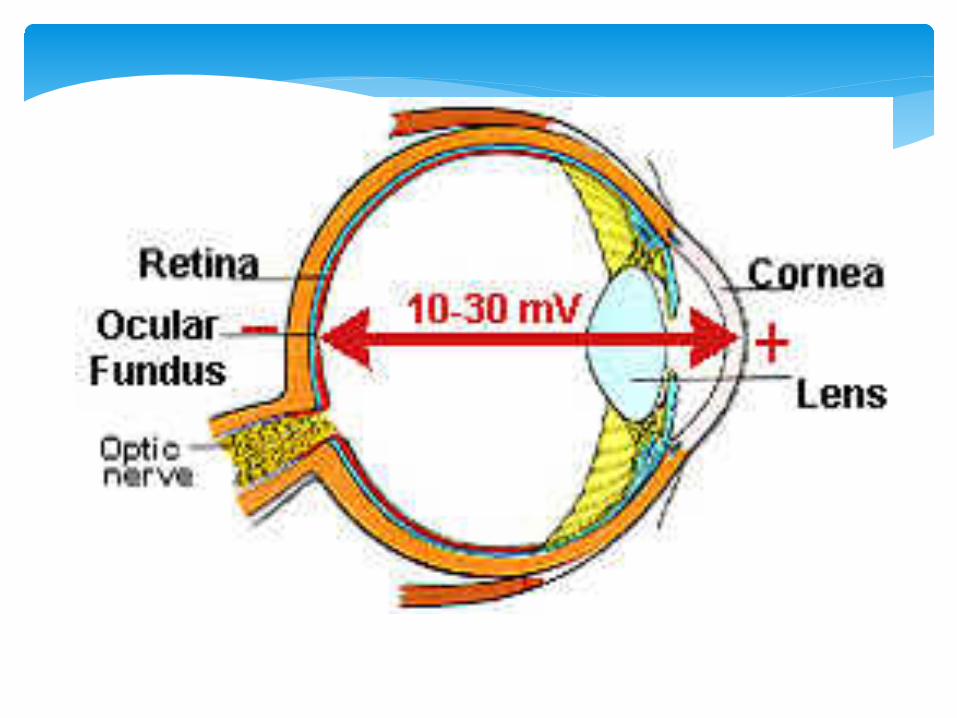
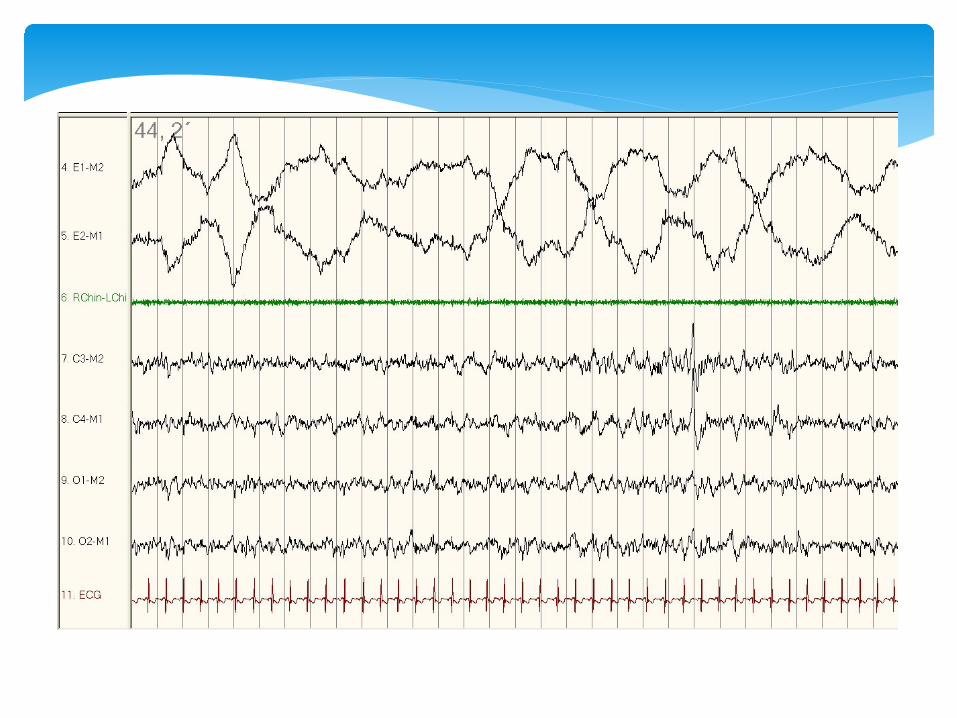
Electro-oculography(EOG)
∗ Cornea is positively charged ∗ Retina is negatively charged ∗ EOG measures the potential difference (PD) (dipole)
between the two ∗ Positive voltage (downward deflection) is when the eye
moves towards an electrode and vice-versa ∗ AASM recommends E1M2 and E2M2 ∗ E1 is 1 cm below the left outer canthus ∗ E2 is 1 cm above the right outer canthus ∗ Conjugate eye movements cause out-of-phase deflections
EMG (chin)
∗ 3 EMG leads : - midline and 1 cm above the inferior edge of the mandible - 2 cm to the right of midline and 2 cm below the inferior edge of the mandible - 2 cm to the left of midline and 2 cm below the inferior edge of the mandible ∗ 1 cm electrode distances for children ∗ Derivation consists of either electrode below the mandible
referenced to the electrode above the mandible ∗ Additional masseter electrodes for Bruxism
ECG
∗ Single modified lead II : electrodes below right clavicle near sternum and over left lateral chest wall
Airflow
∗ Apneas are scored by Oronasal thermistor (recommended) or nasal air pressure transducer (alternative)
∗ Hypopneas are scored by nasal air pressure transducer(recommended) or Oronasal thermistor (alternative)
∗ Respiratory effort related arousals are scored by nasal air pressure transducer or respiratory effort
Airflow
∗ Oronasal thermistor measures temperature change with airflow, roughly quantitative measure
∗ Nasal pressure transducer measures subtle variations in airflow
Respiratory Effort
∗ Esophageal pressure monitoring (balloon measure, very uncomfortable, recommended by AASM)
∗ Surface diaphragmatic EMG ∗ Respiratory Inductance Plethysmography (RIP) :
calibrated volumetric measure for chest and abdominal wall excursion (AASM recommended)
∗ Strain guages : use mercury, now banned in hospitals ∗ Effort belts : piezo-crystal sensors
Ventilation
∗ Pulse oximetry ∗ PetCo2 (end tidal CO2) or transcutaneous Co2 in
children for alveolar hypoventilation ∗ Snoring is recorded with a microphone
EMG (anterior tibialis)
∗ Detects periodic limb movements of sleep (PLMS) ∗ Additional electrodes over the extensor digitorum
communis to detect RBD
Interpretation of PSG
∗ 30 second periods or epochs ∗ Paper speed of 10 mm/second ∗ Original scoring criteria per Rechtshaffen & Kales (R &
K), recently revised by AASM ∗ Majority of Epoch rule ∗ Each epoch is assigned a sleep stage
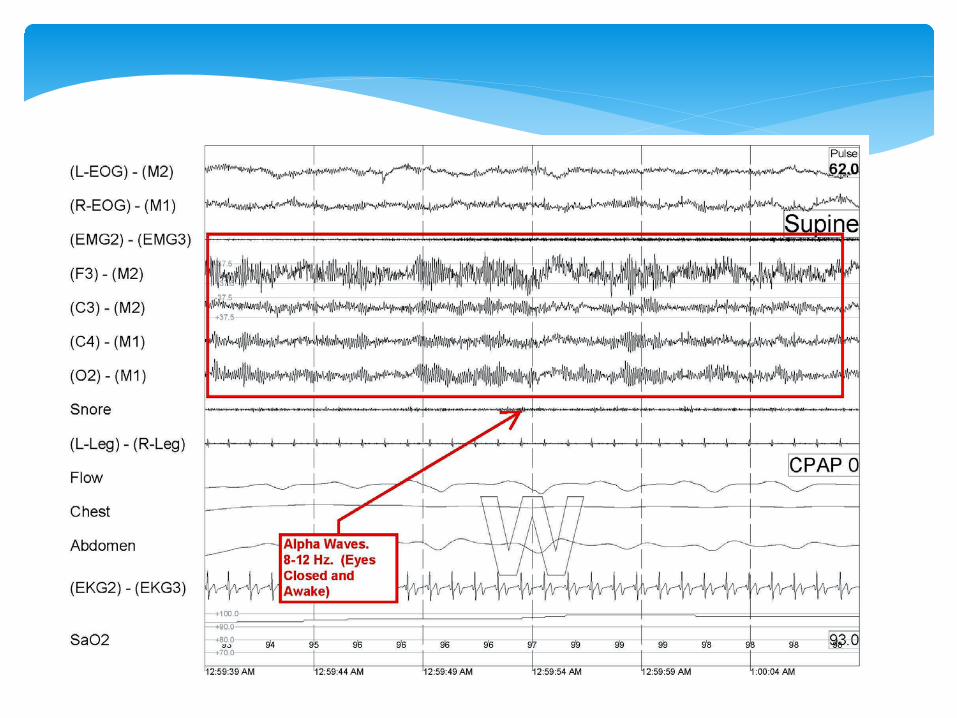
Wake
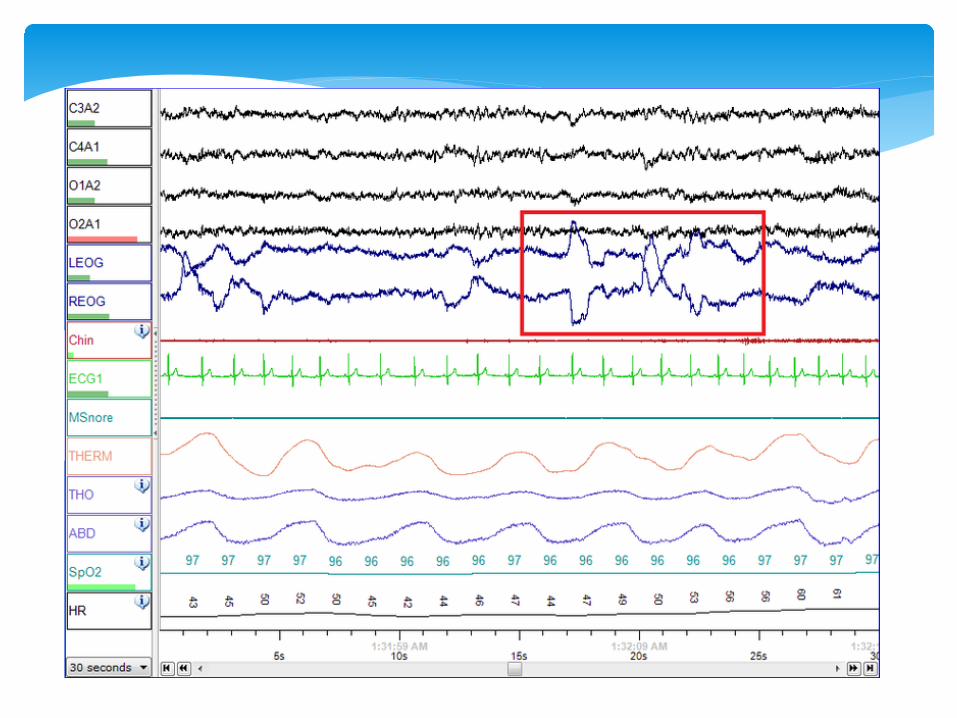
∗ Alpha rhythm over occipital region > 50% of epoch with eye closure, slow-rolling eye movements
∗ Open eyes wakefulness : beta rhythm, conjugate vertical eye blinks, reading eye movements
∗ High chin tone
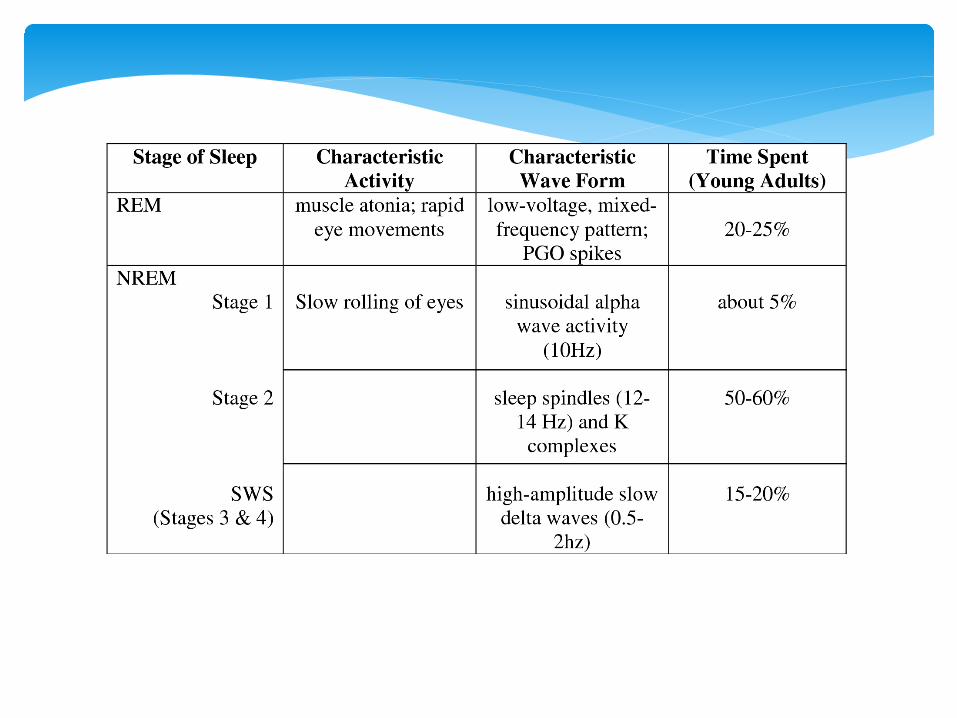
Stages of Sleep
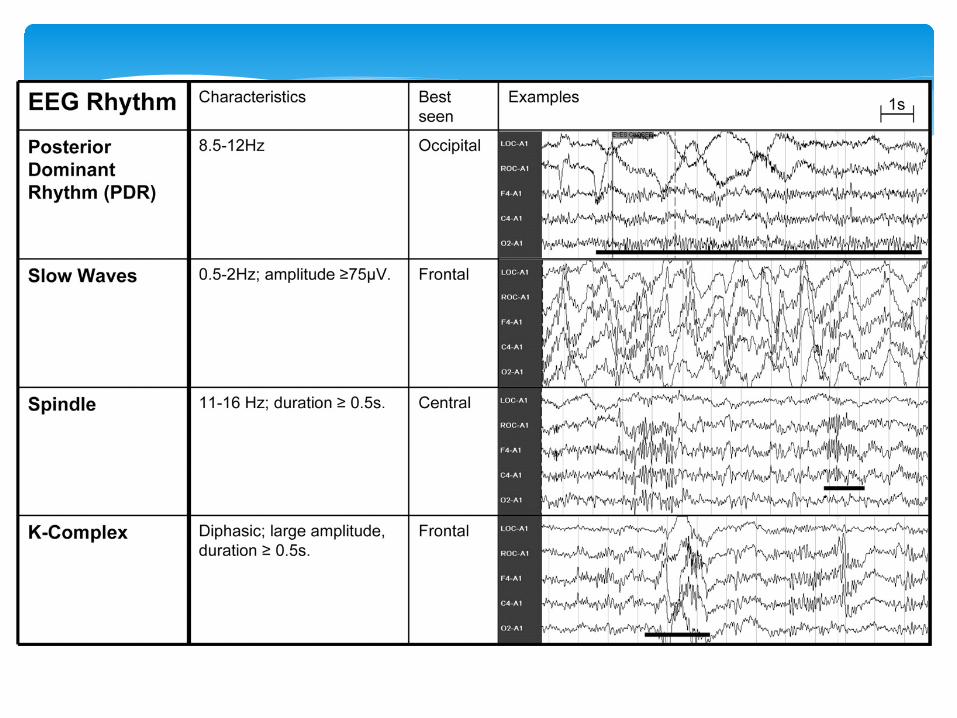
∗ N1 : Theta waves > 50% of epoch, slow-rolling eye movements, low chin tone, vertex waves (central region, < 0.5 seconds)
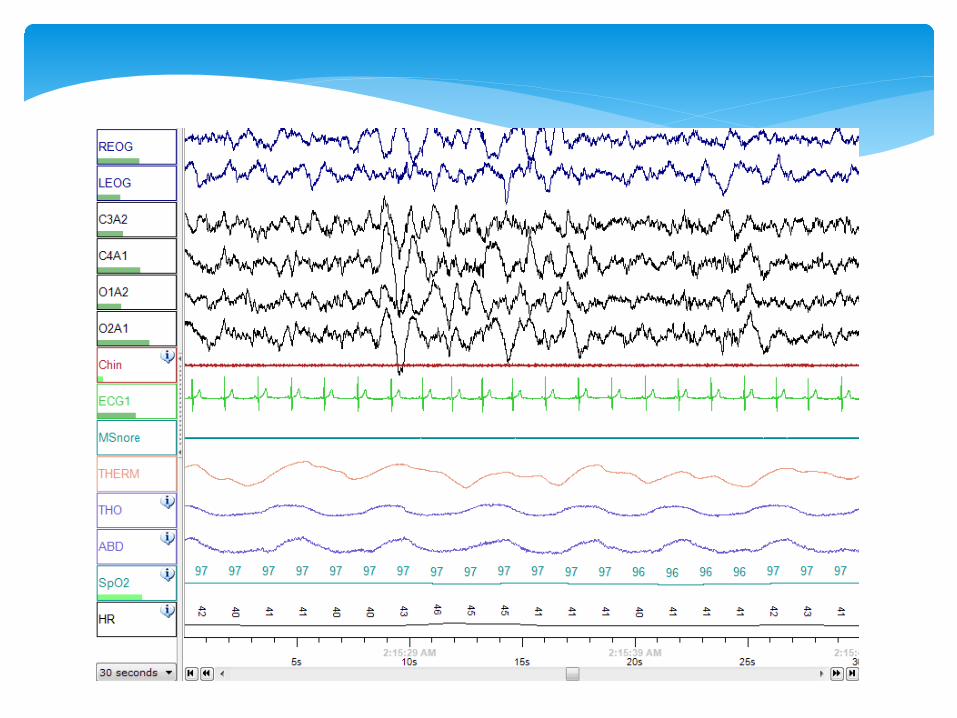
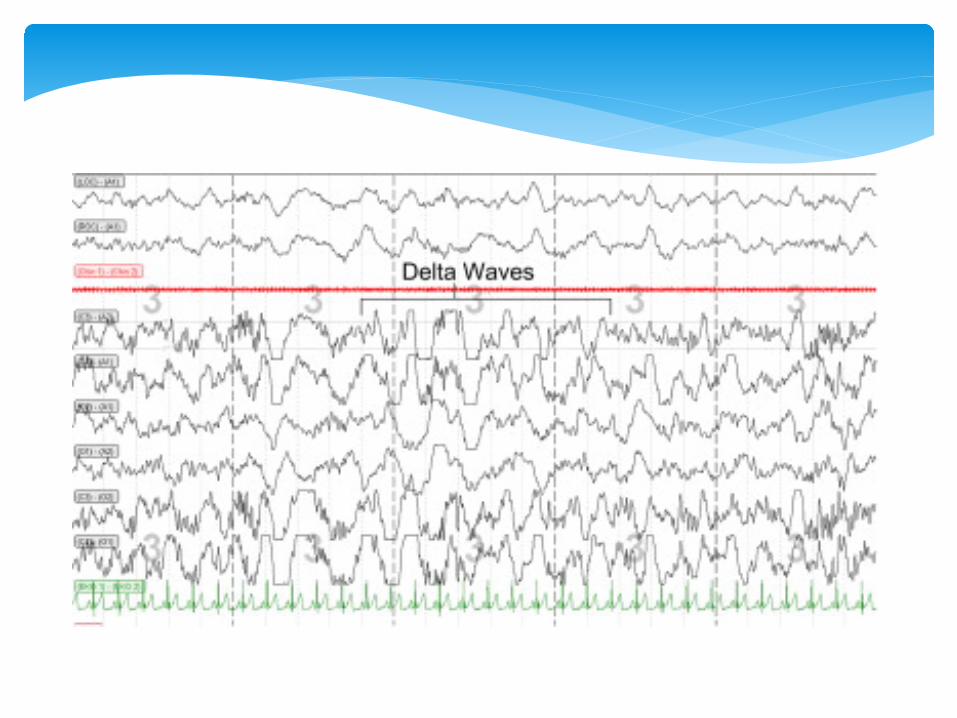
∗ N2 : K complexes and spindles, background theta rhythm, can have delta waves < 20% of epoch
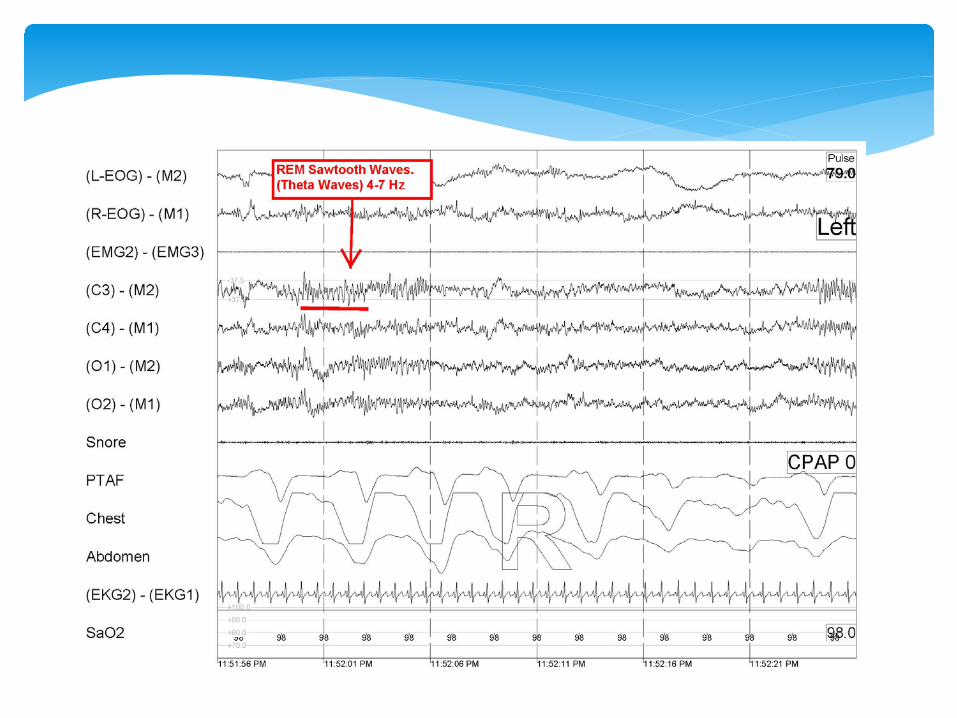
∗ N3 : Delta waves > 20% of epoch ∗ REM sleep : REM’s, lowest chin tone, saw-tooth
waves, relatively low voltage, mixed frequency EEG
∗ Alpha rhythm is attenuated and Theta waves >50% of the epoch
∗ If no alpha rhythm is generated, stage N1 if: - Vertex waves are present - EEG is 4-7 Hz frequency, and ≥ 1 Hz slower then the background rhythm in stage W - Slow eye movements
Stage N1
∗ Score N2 (in absence of criteria for N3) if either/both occur in the first ½ of that epoch or in the last ½ of the previous epoch:
- K complex without associated arousal - Sleep spindles ∗ Continue staging N2 for epochs with low-amplitude,
mixed frequency EEG without K complexes/spindles, if they are preceded by epochs with K complexes without arousals/spindles
Stage N2
∗ End stage N2 when 1 of the following occurs: - transition to stage W, N3 or R - arousal -major body movement followed by slow eye movements without non-arousal associated K complexes/spindles
Stage N2
∗ Score R if ALL of the following are met: - Low-amplitude, mixed-frequency EEG - Low chin EMG tone - Rapid eye movements ∗ REM RULES: Continue staging R even in the absence
of rapid eye movements, if EEG is low-amplitude, mixed frequency, no K/spindles, and low chin tone
Stage R
∗ Stop staging R if: - transition to W or N3 - ↑ in chin tone - arousal/major body movement followed by slow eye movements - non-arousal associated K complex/spindle occurs
Stage R
∗ Movement or muscle artifact obscuring > ½ of the epoch, so that sleep stage cannot be determined
∗ If alpha for part of the epoch (even if < 1/2 of the epoch), stage it as W
∗ If no alpha is discernible, but W epoch precedes/follows it, stage it as W
∗ Otherwise, stage it as the epoch which follows it
Major Body Movement
∗ Abrupt shift of EEG frequency, including alpha and/or frequencies > 16 Hz (not spindles) which last for ≥ 3 seconds and are preceded by ≥ 10 seconds of sleep
∗ Arousal from REM sleep also requires a concurrent ↑ in chin tone for ≥ 1 seconds
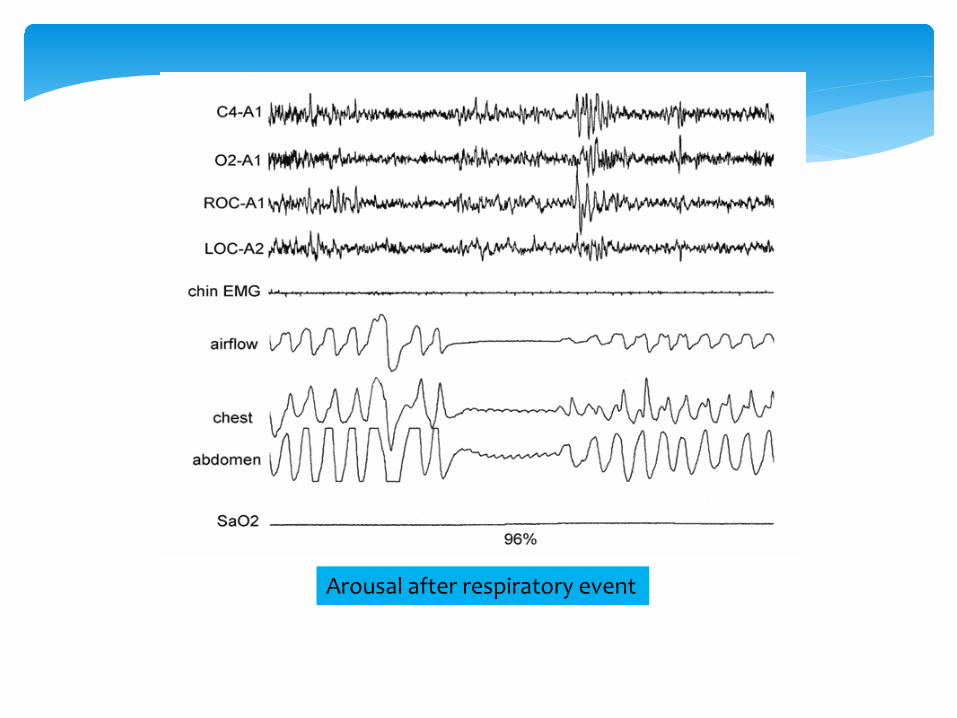
Arousal
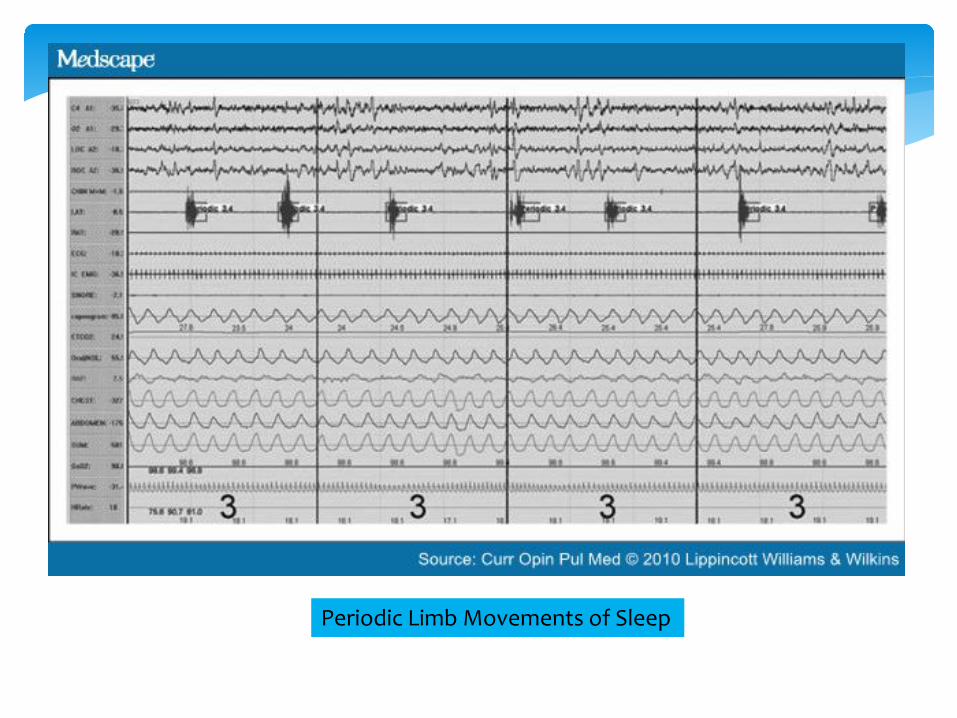
∗ Significant leg movement (LM) definition: - Duration of LM between 0.5-10 seconds - ≥ 8 microvolts increase in EMG voltage above resting EMG ∗ PLM series: - ≥ 4 consecutive LM events - Duration between LM events between 5-90 seconds - if duration between LM events is < 5 seconds, count as 1 LM
Periodic Limb Movements of Sleep (PLMS)
∗ Apneas are scored by oronasal thermistor ∗ Hypopneas are scored by nasal pressure transducer ∗ During PAP titration, use PAP device flow signal to
score respiratory events ∗ Respiratory effort is scored by esophageal
manometry (gold standard) or thoracoabdominal RIP belts
Respiratory Rules
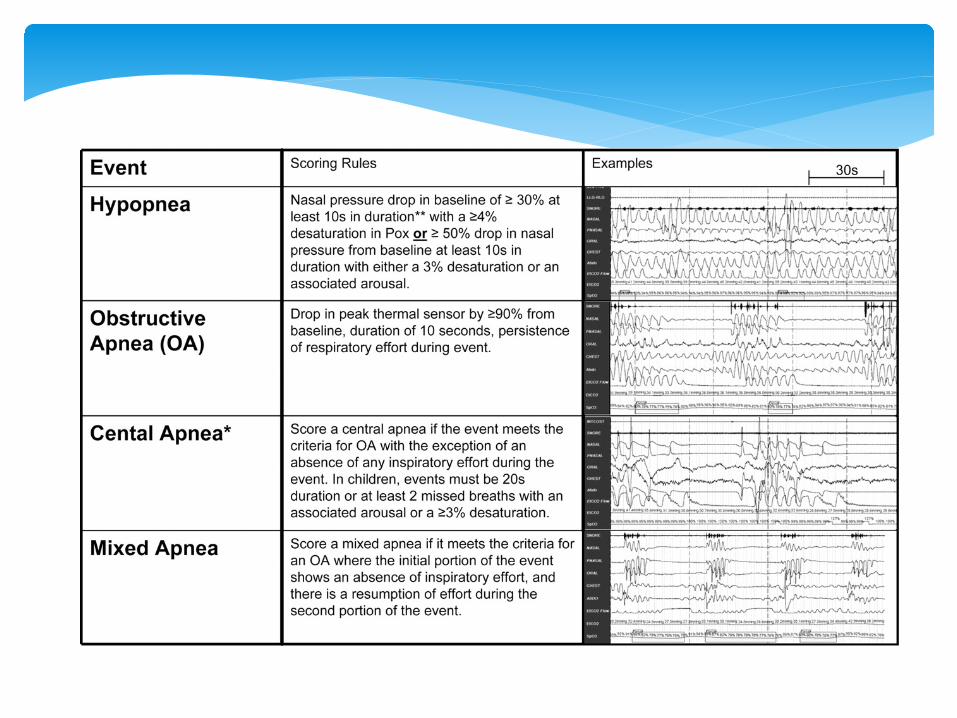
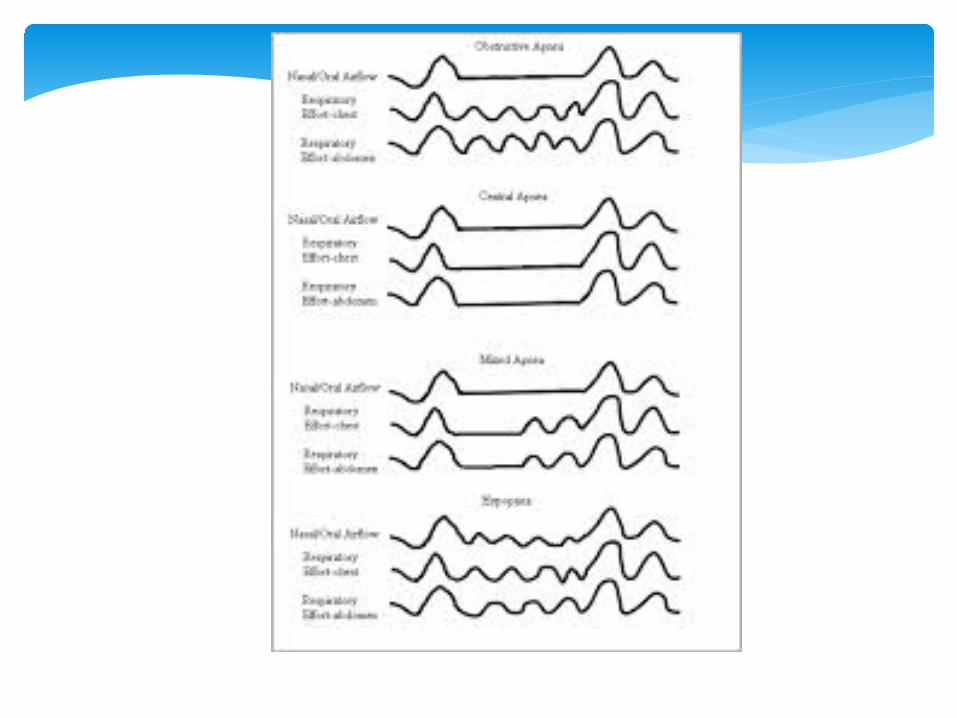
Hypopnea
∗ Peak signal excursion drops by ≥ 30% of pre-event baseline for ≥ 10 seconds with a ≥ 3% drop in oxygen saturation or arousal (current AASM recommended)
∗ Classification of hypopneas as obstructive or central is optional
Hypopnea
∗ Obstructive: - snoring - inspiratory flattening of flow signal - thoracoabdominal paradox
∗ Central: - absence of obstructive features
Respiratory Effort Related Arousal (RERA)
∗ Sequence of breaths lasting ≥ 10 seconds with increasing respiratory effort or decreasing inspiratory flow followed by an arousal, and does not meet criteria for apnea/hypopnea
∗ ↑ paCO2 (or surrogate) to > 55 mm Hg for ≥ 10 minutes OR ∗ ≥ 10 mm Hg increase in paCO2 (or surrogate) during
sleep (compared to awake supine value) to > 50 mm Hg for ≥ 10 minutes
Hypoventilation
∗ ≥ 3 consecutive central apneas and/or central hypopneas separated by crescendo-decrescendo breathing with a cycle length of ≥ 40 seconds
OR ∗ ≥ 5 central apneas and/or central hypopneas per hour
of sleep with crescendo-decrescendo breathing over ≥ 2 hours of monitoring
Cheyne-Stokes Breathing
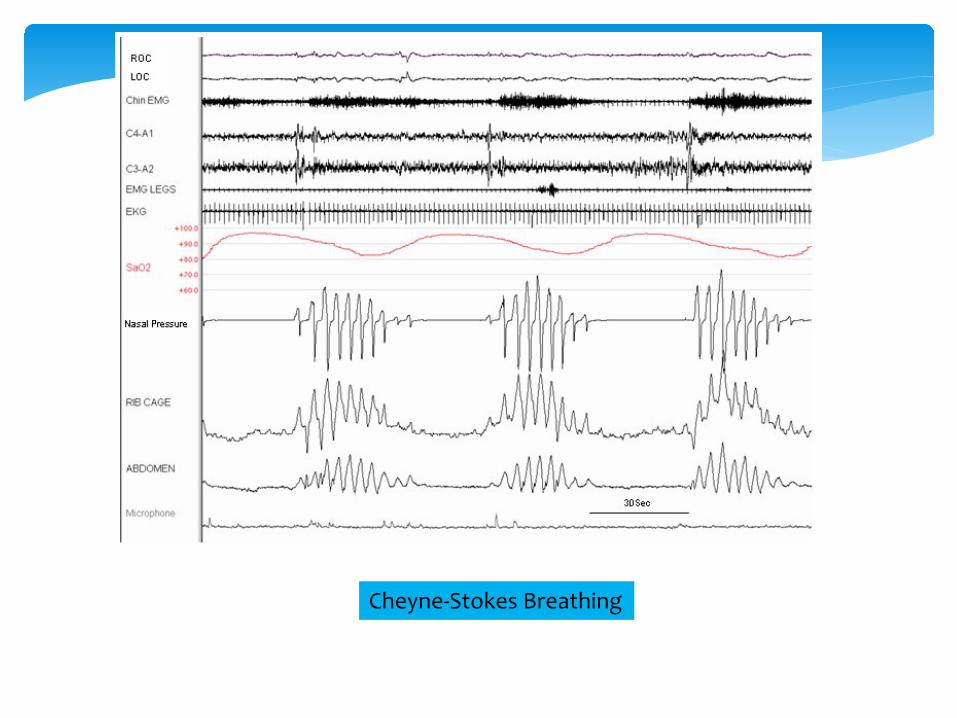
Cheyne-Stokes Breathing
∗ Lights out clock time (hr:min) ∗ Lights on clock time (hr:min) ∗ Total Sleep Time (TST) ∗ Total Recording Time (TRT; “lights out” to “lights on”
in min) ∗ Sleep latency (SL; lights out to first epoch of any
stage of sleep) ∗ REM latency (sleep onset to first epoch of REM sleep
in minutes)
Sleep Scoring Data
∗ Wake after sleep onset (WASO; TRT-SL-TST, in min) ∗ Percent sleep efficiency (TST/TRT X 100) ∗ Time in each stage in minutes ∗ Time in each stage/TST x 100 ∗ Arousal Index (ArI; # of arousals x 60/TST) ∗ Periodic limb movements of sleep index (PLMSI; PLMS x
60/TST) ∗ PLMS arousal index (PLMSArI; PLMS with arousals x
60/TST)
Sleep Scoring Data
∗ Apnea-Hypopnea Index (AHI; # of apneas + hypopneas x 60/TST)
∗ Respiratory Disturbance Index (RDI; RERA’s + apneas + hypopneas x 60/TST)
Sleep Scoring Data