Embed Size (px)
Citation preview

49
Essential Guide to Acute Care, Third Edition. Nicola Cooper, Paul Cramp, Kirsty Forrest and Rakesh Patel. © 2020 John Wiley & Sons Ltd. Published 2020 by John Wiley & Sons Ltd.
Basic Pulmonary Physiology
The main function of the respiratory system is to supply oxygenated blood and remove carbon dioxide. This process is achieved by:
● Ventilation – the delivery and removal of gas to and from the alveoli ● Gas exchange – oxygen and carbon dioxide cross the alveolar-capillary wall by diffusion ● Circulation – oxygen is transported from the lungs to the cells and carbon dioxide is
transported from the cells to the lungs. The concept of oxygen delivery was introduced in Chapter 2
When it comes to respiratory failure, there are two basic types: failure to ventilate and failure to oxygenate. An understanding of basic pulmonary physiology is important in understanding why respiratory failure occurs.
Ventilation
During inspiration, the volume of the thoracic cavity increases due to contraction of the diaphragm and movement of the ribs and air is actively drawn in to the lung. Beyond the termi-nal bronchioles is the respiratory zone, where the surface area of the lung is huge and diffusion of gas occurs. The lung is elastic and returns passively to its pre-inspiratory volume on expira-tion. The lung is also very compliant – a normal breath requires only 3 cmH2O of pressure.
Respiratory FailureBy the end of this chapter you will be able to:
● Understand basic pulmonary physiology ● Describe the mechanisms of respiratory failure ● Know when respiratory support is indicated ● Know which type of respiratory support to use ● Describe the effects of mechanical ventilation ● Apply this to your clinical practice
CHAPTER 4
c04.indd 49 7/20/2020 1:42:21 PM

Chapter 4 Respiratory Failure50
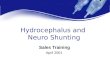
A normal breath (500 mL) is only a small proportion of total lung volume, shown dia-grammatically in Figure 4.1. Of each 500 mL inhaled, 150 mL stays in the anatomical dead space and does not take part in gas exchange. Most of the rest of the gas which enters the respiratory zone takes part in alveolar ventilation, but around 5% does not due to normal ventilation–perfusion (V/Q) mismatch and this is called the alveolar dead space. The ana-tomical plus alveolar dead space is called the physiological dead space. In health, the ana-tomical and physiological dead spaces are almost the same.
V/Q mismatch can increase in disease. If ventilation is reduced to a part of the lung and blood flow remains unchanged, alveolar O2 will fall and CO2 will rise in that area, approach-ing the values of venous blood. If blood flow is obstructed to a part of the lung and ventila-tion remains unchanged, alveolar O2 will rise and CO2 will fall in that area, approaching the values of inspired air. The ventilation–perfusion ratio therefore lies along a continuum, ranging from zero (perfusion but no ventilation i.e. shunt) to infinity (ventilation but no perfusion i.e. dead space).
When PaO2 falls and PaCO2 rises due to ventilation–perfusion mismatch, normal people increase their overall alveolar ventilation to compensate. This corrects the hypercapnia but only partially the hypoxaemia due to the different shapes of the O2 and CO2 dissociation curves. The A–a gradient is a measure of ventilation–perfusion mismatch and is discussed later.
Total lungcapacity Vital
capacity
Functional residualcapacityResidual vol
2
4
6
0
Tidal vol
Litres
CV
Figure 4.1 Normal lung volumes. The closing volume (CV) is the volume at which the dependent airways begin to collapse, or close. It is normally about 10% of the vital capacity and increases to about 40% by the age of 65.
c04.indd 50 7/20/2020 1:42:22 PM

asiic ullooary hysiolooy 51
The mechanics of ventilation are complex. Surfactant plays an important role in the elas-tic properties of the lung (and is depleted in acute respiratory distress syndrome). The lungs tend to recoil while the thoracic cage tends to expand slightly. This creates a negative intra-pleural pressure which increases during inspiration, because as the lung expands, its elastic recoil increases. Figure 4.2 shows the pressure changes which occur in the alveolus during normal breathing.
Ventilation is controlled in the brainstem respiratory centres with input from the cortex (voluntary control). The muscles which effect ventilation are the diaphragm, intercostals, abdominal muscles, and the accessory muscles (e.g. sternomastoids). Ventilation is sensed by central and peripheral chemoreceptors and other receptors in the lungs. Normally, PaCO2 is the most important factor in the control of ventilation but the sensitivity to changes in PaCO2 is reduced by sleep, old age, and airway resistance (e.g. in chronic obstructive pulmonary disease). As well as a rise in PaCO2, other factors that increase ventilation include hypoxae-mia, low arterial pH, and situations in which there is increased oxygen demand (e.g. sepsis).
Oxygenation
Oxygen tension in the air is around 20 kPa (154 mmHg) at sea level, falling to around 0.5 kPa (3.8 mmHg) in the mitochondria. This gradient is known as the ‘oxygen cascade’, illustrated in Figure 4.3. An interruption at any point along this cascade can cause hypoxia – for example, high altitude, upper or lower airway obstruction, alveolar problems, abnormal haemoglobins, circulatory failure, or mitochondrial dysfunction.
If a patient is breathing 60% oxygen and his PaO2 is 13 kPa (100 mmHg), it can be seen that there is a significant problem with gas exchange – the ‘normal’ value of 13 kPa is not
0
–1
+1
cmH20
Inspiration Expiration
Figure 4.2 Pressure changes in the alveolus during normal breathing.
c04.indd 51 7/20/2020 1:42:22 PM

Chapter 4 Respiratory Failure52
normal at all in the context of a high inspired oxygen concentration (FiO2). In a healthy person, the predicted PaO2 is roughly 10 kPa (75 mmHg) below the FiO2. Problems with gas exchange can occur at the alveolar–arterial step of the oxygen cascade (D to E in Figure 4.3). Normal people have a small alveolar–arterial difference because the bronchial veins of the lung and thebesian veins of the heart carry unsaturated blood directly to the left ventricle, bypassing the alveoli. Large differences are always due to pathology.
In the example above, one can see the difference between FiO2 and PaO2 without a cal-culation. However, the difference between alveolar and arterial oxygen (the A–a gradient) can be measured using the alveolar gas equation.
Oxygen leaves the alveolus in exchange for carbon dioxide. Arterial and alveolar PCO2 are virtually the same. If we know the composition of inspired gas and the respiratory exchange ratio (R), then the alveolar oxygen concentration can be calculated. (The respira-tory exchange ratio allows for metabolism by the tissues.) To convert FiO2 in to the partial pressure of inspired O2, we have to adjust for barometric pressure, water vapour pressure, and temperature. Assuming sea level (101 kPa or 760 mmHg), inspired air which is 100% humidified (water vapour pressure 6 kPa or 47 mmHg), and 37°C, the alveolar gas equation is as follows:
PAO FiO PB PAH O PACO 0.82 2 2 2( ) /
E
F
O2
Oxygen partial pressure (vertical) in different parts of thebody (horizontal)
AirwaysAlveolus
AB
C
D20 kPa
15 kPa
10 kPa
5 kPa
0 kPaMitochondriainside cells
A = inspired dry gas, B = humidi�ed, C = mixed with expired gas,D = alveolar ventilation + oxygen consumption, E = venousmixing + V/Q mismatch, F = capillary blood, G = mitochondria
Mixedvenousoxygen
RBC’s
AB
C D E
F
G
Figure 4.3 The oxygen cascade.
c04.indd 52 7/20/2020 1:42:23 PM

The heeThanisi of heisniha iry hnilihe 53
PAO2 = alveolar PO2
FiO2 = fraction of inspired oxygenPB = barometric pressure of 101 kPaPAH2O = alveolar partial pressure of water of 6 kPaPACO2 = alveolar CO2
0.8 is the respiratory exchange ratio (or respiratory quotient)
Once PAO2 has been estimated, the A–a gradient is calculated as PAO2 – PaO2. A normal A–a gradient is up to 2 kPa (15 mmHg) or 4 kPa (30 mmHg) in smokers and older people.
For example, a person breathing air with a PaO2 of 12.0 kPa and a PaCO2 of 5.0 kPa has an A–a gradient as follows:
PAO FiO PB PAH O ACO 0.82 2 2 2( ) /P
PAO 0.21 95gradient on air, 0.
2 5 0 8/ .(When calculating the A a 221 95 is often shortened to 20.)
20 5 / 0.8 13.75
The A–a gradient is therefore 13.75 − 12 = 1.75 kPa.
The calculation of the A–a gradient illustrates the importance of always documenting the inspired oxygen concentration on an arterial blood gas report; otherwise, problems with oxygenation may not be detected. Some applications of the A–a gradient are illustrated in the case histories at the end of this chapter. However, it is important to remember the gen-eral principle that a ‘normal’ test does not necessarily exclude significant pathology.
TheMechanismsof RespiratoryFailure
Respiratory failure is said to be present when there is PaO2 of less than 8.0 kPa (60 mmHg) when breathing air at sea level without intracardiac shunting. It occurs with or without a high PaCO2.
Traditionally, respiratory failure is divided into type 1 and type 2, but these are not practi-cal terms and it is better to think instead of:
● Failure to ventilate ● Failure to oxygenate ● Failure to both ventilate and oxygenate
Failureto Ventilate
Ventilation–perfusion mismatch causes a high PaCO2, as mentioned earlier. But hypercap-nic respiratory failure occurs when a patient cannot compensate for a high PaCO2 by increasing overall alveolar ventilation and this usually occurs in conditions which cause alveolar hypoventilation.
c04.indd 53 7/20/2020 1:42:25 PM

Chapter 4 Respiratory Failure54
Figure 2.5 illustrated how respiratory muscle load and respiratory muscle strength can be affected by disease and an imbalance leads to alveolar hypoventilation. To recap, respira-tory muscle load is increased by increased resistance (e.g. upper or lower airway obstruc-tion), reduced compliance (e.g. infection, oedema, rib fractures, or obesity), and increased respiratory rate. Respiratory muscle strength can be reduced by a problem in any part of the neuro-respiratory pathway – motor neurone disease, Guillain–Barré syndrome, myasthe-nia gravis, critical illness polyneuropathy/myopathy, or electrolyte abnormalities (e.g. low potassium, magnesium, phosphate, or calcium). Drugs which act on the respiratory centre such as morphine reduce total ventilation. Oxygen therapy corrects the hypoxaemia which occurs as a result of V/Q mismatch or alveolar hypoventilation.
Failureto Oxygenate
Although there are many potential causes of hypoxaemia, as illustrated by the oxygen cas-cade, the most common causes of failure to oxygenate are:
● V/Q mismatch ● Intra-pulmonary shunt ● Diffusion problems
V/Q MismatchIf the airways are impaired by the presence of secretions or narrowed by bronchoconstric-tion, that segment will be perfused but only partially ventilated. The resulting V/Q mis-match will result in hypoxaemia and hypercapnia. The patient will increase his overall alveolar ventilation to compensate. Giving supplemental oxygen will cause the PaO2 to increase.
In normal lungs, the bases are better perfused and less well ventilated whereas the apices are better ventilated and less well perfused. Therefore, consolidation at the lung bases is more likely to cause hypoxaemia because significant shunts can occur with basal pathol-ogy. On the other hand, significant consolidation at the apices can occur (e.g. in tuberculo-sis) but this is less likely to cause hypoxaemia.
Intra-Pulmonary ShuntIf the airways are totally filled with fluid or collapsed, that segment will be perfused but not ventilated at all (see Figure 4.4). Mixed venous blood is shunted across it. Increasing the inspired oxygen in the presence of a moderate to severe shunt will not improve PaO2. Intra-pulmonary shunting as a cause of hypoxaemia is observed in pneumonia and atelectasis.
V/Q mismatch and intra-pulmonary shunting can often be distinguished by the response of the patient to supplemental oxygen. With a large shunt, hypoxaemia cannot be abolished even by giving the patient high concentration oxygen. Small reductions in inspired oxygen may lead to a large reduction in PaO2 because of the relatively steep part of the oxygen dis-sociation curve (see Figure 2.7).
c04.indd 54 7/20/2020 1:42:25 PM

The heeThanisi of heisniha iry hnilihe 55
Diffusion ProblemsSome conditions (e.g. fibrosis) affect the blood–gas barrier which is normally extremely thin, leading to ineffective diffusion of gas. The response to supplemental oxygen reduces with increasing severity of disease.
In summary, with V/Q mismatch, intra-pulmonary shunt, and diffusion problems, there is adequate ventilation but inadequate gas exchange and therefore a low PaO2 with a nor-mal or low PaCO2 is seen.
Failureto BothVentilateand Oxygenate
Postoperative respiratory failure is an example of a situation where problems with gas exchange are often accompanied by hypoventilation, leading to hypoxaemia as well as hypercapnia. In postoperative respiratory failure, the hypoxaemia may be caused by infection or atelectasis due to a combination of the effects of general anaesthesia and pain. A reduction in functional residual capacity below closing volume also contributes leading to airway collapse in the dependent parts of the lung (see Figure 4.1). The hyper-capnia is caused by excessive load from reduced compliance and decreased minute vol-ume (the volume of gas inhaled/exhaled per minute) due to pain or opiates. At-risk patients are those with pre-existing lung disease, who are obese, or who have upper abdominal or thoracic surgery. Box 4.1 outlines the measures to prevent postoperative respiratory failure.
Alveolar�ooding
Obstructiveairways disease
Interstitiallung disease
Mixed venousoxygen
V / Q MISMATCH SHUNT
Figure 4.4 V/Q mismatch versus shunt.
c04.indd 55 7/20/2020 1:42:25 PM

Chapter 4 Respiratory Failure56
RespiratorySupport
Ideally, patients with acute respiratory failure that does not rapidly reverse with medical therapy should be admitted to a respiratory care unit or other level two to three facility. Hypoxaemia is the most life-threatening facet of respiratory failure. The goal of treatment is to ensure adequate oxygen delivery to the tissues which is generally achieved with a PaO2 of at least 8.0 kPa (60 mmHg) or SpO2 of at least 93%. However, patients with chronic respiratory failure require different therapeutic targets than patients with previously nor-mal lungs. One would not necessarily aim for normal values in these patients (see Chapter 2).
Apart from oxygen therapy and treatment of the underlying cause, various forms of res-piratory support are used in the treatment of respiratory failure. There are two main types of respiratory support: non-invasive and invasive. Non-invasive respiratory support con-sists of bilevel positive airway pressure (BiPAP) or continuous positive airway pressure (CPAP), usually administered via tight fitting masks, and high flow nasal oxygen therapy (HFNOT). Invasive respiratory support requires endotracheal intubation and comes in sev-eral different modes.
‘Respiratory support’ does not necessarily mean mechanical ventilation. For example, CPAP is not ventilation, as will be explained later. The ABCDE approach is still important and should be used to assess and manage any patient with respiratory failure (see Table 4.1).
Respiratory support is indicated when:
● There is a failure to oxygenate or ventilate despite medical therapy ● There is unacceptable respiratory fatigue ● There are non-respiratory indications for tracheal intubation and ventilation (e.g. the
need for airway protection)
Once a decision has been made that a patient needs respiratory support, the next question is, what type? Failure to ventilate is treated by manoeuvres designed to increase alveolar
Box4.1 PreventingPostoperativeRespiratoryFailure
● Identify high-risk patients preoperatively: pre-existing lung disease, upper abdomi-nal or thoracic surgery, smokers (impaired ciliary transport), obesity
● Institute ‘prehabilitation’ (see Chapter 9) ● Use regional analgesia if possible ● Early postoperative chest physiotherapy ● Humidified oxygen ● Avoid drugs which may depress ventilation if possible ● Early identification of pneumonia ● Early respiratory support if indicated.
c04.indd 56 7/20/2020 1:42:26 PM

oon-onasine Respiratory upport 57
ventilation by increasing the depth and rate of breathing. Failure to oxygenate, however, is treated by restoring and maintaining lung volumes using alveolar recruitment manoeuvres such as the application of a positive end-expiratory pressure (PEEP or CPAP). Figure 4.5 summarises the different types of respiratory support.
There is considerable evidence available as to what works best in different clinical situa-tions.1 This information is important. For example, there is no good evidence that ‘trying’ non-invasive ventilation in a young person with life-threatening asthma is of any benefit. The first-line methods of respiratory support for different conditions are shown in Table 4.2.
Non-InvasiveRespiratorySupport
Non-invasive respiratory support will be more familiar to people who work outside the intensive care unit. BiPAP and CPAP are two types of non-invasive respiratory support. HFNOT is discussed further in the mini-tutorial. Non-invasive BiPAP is also referred to as NIV (non-invasive ventilation). The ventilator cycles between two different pressures trig-gered by the patient’s own breathing, the higher IPAP (inspiratory positive airway pressure) and the lower EPAP (expiratory positive airway pressure). In CPAP, a single positive pres-sure is applied throughout the patient’s respiratory cycle. The difference between non-inva-sive BiPAP and CPAP is shown in Figure 4.6.
Table 4.1 Approach to the patient with respiratory failure.
Action
A Assess and treat any upper airway obstructionAdminister oxygen if required
B Look at the chest: assess rate, depth, and symmetryMeasure SpO2
Quickly listen with a stethoscope (for air entry, wheeze, crackles)You may need to use a bag and mask if the patient has inadequate ventilationTreat wheeze, pneumothorax, fluid, collapse, infection, etc.Is a physiotherapist needed?
C Fluid challenge(s) or rehydration may be neededVasoactive drugs may be needed in sepsis (see Chapter 6)
D Assess conscious level as this affects treatment options
E Are ABCD stable? If not, go back to the top and call for helpArterial blood gasesGather more information (e.g. usual functional capacity of patient)Decide if and what type of respiratory support is neededMake ICU and CPR decisions nowDo not move an unstable patient without the right monitoring equipment and staffCall a senior colleague if not already
c04.indd 57 7/20/2020 1:42:26 PM

Chapter 4 Respiratory Failure58
Table 4.2 First-line methods of respiratory support for different causes of acute respiratory failure.
Tracheal intubation Non-invasive ventilation (NIV/BiPAP) Non-invasive CPAP
● Asthma ● Pneumonia* ● ARDS (acute respiratory
distress syndrome) ● Severe respiratory
acidosis (pH <7.25)** ● Unstable patient or
contraindications to non-invasive respiratory support
● Inability to protect airway due to reduced conscious level
Mild–moderate respiratory acidosis (pH 7.25–7.35) in the following conditions:
● Exacerbation of COPD ● Hypercapnic respiratory failure
secondary to chest wall deformity (e.g. kyphoscoliosis) or neuromuscular diseases
● Decompensated sleep apnoea ● Weaning from invasive
ventilation ● Acute cardiogenic pulmonary
oedema ● Postoperative respiratory failure ● Acute respiratory failure in
immunocompromised patients
● To treat hypoxaemia in pneumonia or postoperative respiratory failure associated with atelectasis (other methods may be used instead e.g. humidified high flow nasal oxygen therapy)
● Acute cardiogenic pulmonary oedema
* If NIV or CPAP is used as a trial of treatment in pneumonia in patients without COPD or postoperative respiratory failure, this should be done on an ICU with close monitoring and rapid access to intubation. Patients with excessive secretions may also require tracheal intubation.
** Sometimes non-invasive respiratory support is used in severe respiratory acidosis where there is a ceiling of care (e.g. in severe COPD).
RESPIRATORY SUPPORT
Non-invasive(e.g.tight-�tting mask)
Invasive(tracheal intubation)
BiPAP(a form of IPPV)
CPAPHFNOT
CPAP(usually used in weaning)
Volume controlPressure control
BiPAPSIMVPSV
(all are forms of IPPV)
Figure 4.5 Different types of respiratory support. BiPAP = bilevel positive pressure ventilation (also known as NIV: non-invasive ventilation); IPPV = intermittent positive pressure ventilation; CPAP = continuous positive pressure ventilation; HFNOT = high flow nasal oxygen therapy; SIMV = synchronised intermittent mandatory ventilation; PSV = pressure support ventilation.
c04.indd 58 7/20/2020 1:42:26 PM

oon-onasine Respiratory upport 59
Non-invasive respiratory support is contraindicated in:
● Inability to protect own airway ● Reduced conscious level ● Respiratory arrest or apnoea episodes ● Recent facial, oesophageal, or gastric surgery ● Bowel obstruction ● Copious respiratory secretions ● Other organ system failure (e.g. haemodynamic instability) ● Severe confusion/agitation
However, non-invasive BiPAP is sometimes used in drowsy patients if it is decided that the patient is not suitable for tracheal intubation because of severe chronic lung disease.
Non-Invasive BiPAP
Non-invasive ventilators have a simpler design compared with the ventilators on an ICU. This is because most were originally designed for home use. The disadvantage of this is that some older models are not adequately equipped in terms of monitoring and alarms when used in hospital.
The operator has to choose the appropriate type and size of mask and set basic ventilator controls: supplementary oxygen flow rate, the inspiratory pressure (IPAP), expiratory pres-sure (EPAP), backup respiratory rate, and inspiratory time or I:E ratio.
0
CPAP
BiPAP
0
10
20
Airway pressure (cmH2O)
Time (s)
10
20
Figure 4.6 The difference between non-invasive BiPAP and CPAP. With non-invasive BiPAP, mechanical ventilation is superimposed on spontaneous breathing. See Figure 4.9 for BiPAP in a paralysed patient.
c04.indd 59 7/20/2020 1:42:26 PM

Chapter 4 Respiratory Failure60
Non-invasive BiPAP is used in certain patients with a mild to moderate acute respiratory acidosis (see Table 4.2). In an acute exacerbation of COPD, it is usual to begin with an IPAP of 15 cmH2O and an EPAP of 5 cmH2O. The levels are then adjusted based on patient comfort, tidal volume achieved (if measured), and arterial blood gases.
The main indications for non-invasive BiPAP in the acute setting are mild–moderate res-piratory acidosis (pH 7.25–7.35) in2:
● Exacerbation of COPD ● Acute cardiogenic pulmonary oedema (when either BiPAP or CPAP can be used) ● Acute on chronic hypercapnic respiratory failure secondary to chest wall deformity or
neuromuscular diseases ● Decompensated obstructive sleep apnoea ● Weaning from invasive ventilation
There is also evidence that non-invasive BiPAP can be used in acute respiratory failure due to chest trauma (without pneumothorax), postoperative acute respira-tory failure, and acute respiratory failure in immunocompromised patients – in all these situations, treatment should be initiated by an expert and patients monitored in the ICU.
Non-invasive BiPAP is not recommended for acute respiratory failure in patients with no pre-existing lung disease, asthma, or severe acute respiratory syndrome due to viral illness.
There is a large body of evidence supporting non-invasive BiPAP in acute exacerbations of COPD (see mini-tutorial). Non-invasive BiPAP can also be used as a step-down treat-ment in patients who have been intubated and ventilated on the ICU. Weaning problems occur in at least 60% patients with COPD and this is a major cause of prolonged ICU stay. A randomised multicentre trial has shown that non-invasive BiPAP is more successful in weaning than a conventional approach in patients with COPD.3 Patients who failed a T-piece trial (breathing spontaneously with no support) 48 hours after intubation were randomly assigned to receive either non-invasive BiPAP immediately after extubation or conventional weaning (a gradual reduction in ventilator support). The non-invasive BiPAP group took a shorter time to wean, had shorter ICU stays, a lower incidence of hospital-acquired pneumonia, and increased 60 day survival. Other studies have reported similar findings.
Early trials of non-invasive BiPAP for pneumonia were discouraging, but a later prospec-tive randomised trial of non-invasive BiPAP in community-acquired pneumonia (56 patients) showed a significant fall in respiratory rate and the need for intubation.4 However, half of the patients in this study had COPD and it was carried out in an ICU. Previously well patients who require ventilation for pneumonia should be referred to an ICU as they may need tracheal intubation.
c04.indd 60 7/20/2020 1:42:26 PM

oon-onasine Respiratory upport 61
Mini-Tutorial:NIVfor Exacerbationsof COPD
Around 20% of patients admitted to hospital with COPD present with or develop hyper-capnic respiratory failure, which carries an increased mortality. There have been several randomised controlled trials of non-invasive BiPAP versus standard care in acute exac-erbations of COPD.1,5 The strongest evidence to support the use of non-invasive BiPAP is in patients with a pH of 7.25–7.35 due to an acute respiratory acidosis (i.e. in the absence of a metabolic acidosis). BiPAP reduces the sensation of breathlessness, the need for tracheal intubation, and improves survival. If patients are going to improve on BiPAP, it is almost always within the first 1–4 hours of initiating treatment.
Studies have compared non-invasive BiPAP with tracheal intubation. In one study,6 the mean pH was 7.20. Survival was similar in both groups, but in patients for whom non-invasive BiPAP was successful, they had a shorter ICU and hospital stay and fewer complications (see Table 4.3). The following were excluded from being randomised to non-invasive treatment: respiratory arrest or apnoea episodes, hypotension, agitation requiring sedation, and heart rate less than 60 per minute.
Non-invasive BiPAP should be commenced as soon as the pH falls below 7.35 because the further the degree of acidosis, the less the chances of improvement. It should be used as an adjunct to full medical therapy which treats the underlying cause of acute respiratory failure. In a one-year prevalence study of nearly 1000 patients admitted with an exacerbation of COPD in one city, around 1 in 5 were acidotic on arrival in the Emergency Department, but 20% of these had a normal pH by the time they were admitted to a ward.7 This included patients with an initial pH of less than 7.25, suggesting that bronchodilators and controlled oxygen therapy are important in the initial management of acute exacerbations of COPD.
Patients on non-invasive BiPAP require close supervision because sudden deteriora-tion can occur at any time. Simple measures such as adjusting the mask to reduce excessive air leaks can make a difference to the success or otherwise of treatment. Basic vital signs frequently measured give an indication of whether or not non-invasive BiPAP is effective. If non-invasive BiPAP does not improve the respiratory acidosis
Table 4.3 Complications of non-invasive respiratory support versus intubation.
Non-invasiverespiratorysupport Tracheal intubation
Necrosis of skin over bridge of nose Pneumonia
Aspiration Barotrauma and volutrauma
Changes in cardiac output (less) Changes in cardiac output
Complications of sedation and paralysis
Tracheal stenosis/tracheomalacia
c04.indd 61 7/20/2020 1:42:26 PM

Chapter 4 Respiratory Failure62
Non-Invasive CPAP
Non-invasive CPAP was first introduced in the 1980s as a therapy for obstructive sleep apnoea (OSA). A tight-fitting face or nasal mask delivers a single positive pressure through-out the patient’s respiratory cycle. In OSA, CPAP prevents pharyngeal collapse. CPAP can also be delivered through an endotracheal tube or tracheostomy tube in spontaneously breathing patients and is used this way during weaning from a ventilator on the ICU.
The main indications for non-invasive CPAP in the acute setting are:
● To improve oxygenation in pneumonia or postoperative respiratory failure associated with atelectasis
● Acute cardiogenic pulmonary oedema
In the spontaneously breathing patient, the application of CPAP provides positive end-expiratory pressure (PEEP) that can reverse or prevent atelectasis, improve functional residual capacity and oxygenation. These improvements may prevent the need for tracheal intubation and can sometimes reduce the work of breathing. High flow nasal oxygen ther-apy can be used as an alternative in these situations (see mini-tutorial). However, in patients with problems causing alveolar hypoventilation, mechanical ventilation rather than CPAP is more appropriate.
The inspiratory flow in a CPAP circuit needs to be high enough to match the patient’s peak inspiratory flow rate. If this is not achieved, the patient will breathe against a closed valve with the risk that the generation of significant negative intrapleural pressure will lead to the development of pulmonary oedema. Look at the expiratory valve on a CPAP circuit in use. The valve should remain slightly open during inspiration (see Figure 4.7).
within the first few hours of treatment despite adjustments to ventilator settings, tra-cheal intubation should be considered.
Predictors of failure of non-invasive BiPAP in an acute exacerbation of COPD are:
● No improvement within 2 hours ● High APACHE (acute physiological and chronic health evaluation) score ● Pneumonia ● Very underweight patient ● Neurological compromise ● pH less than 7.3 prior to starting NIV
It is recommended that non-invasive BiPAP should be administered in a dedicated area, with staff who have been trained in its application, who are experienced in its use, and who are aware of its limitations.8 All patients should have a clear plan covering what to do in the event of deterioration, including decisions about CPR and tracheal intubation.
Guidelines for COPD, including care bundles, can be found on the British Thoracic Society website.8
c04.indd 62 7/20/2020 1:42:26 PM

oon-onasine Respiratory upport 63
Non-invasive CPAP reduces respiratory distress and may reduce tracheal intubation and mortality rates in acute respiratory failure caused by cardiogenic pulmonary oedema, although data regarding mortality are less conclusive.9 CPAP is also a feasible technique in the pre-hospital setting, because it is simpler to administer than BiPAP, requiring minimal training and equipment.
In acute cardiogenic pulmonary oedema, CPAP ‘squeezes’ fluid out of the alveoli in to the circulation. There is a decline in the level of shunt because of redistribution of lung water from the alveolar space in to the perivascular cuffs. CPAP also has cardiovascular effects:
● Left ventricular function is improved because afterload is reduced (leading to an increase in stroke volume). This occurs because the increased intrathoracic pressure has a squeez-ing effect on the left ventricle. There is a subsequent reduction in the pressure gradient between the ventricle and the aorta which has the effect of reducing the work required during contraction (i.e. afterload) – see Figure 4.8
● Relief of respiratory distress leads to haemodynamic improvement and reversal of hyper-tension and tachycardia, probably through reduced sympathoadrenergic stimulation
Non-invasive CPAP in acute cardiogenic pulmonary oedema is indicated when the patient has failed to respond to medical therapy and there is an acute respiratory acidosis or hypoxaemia despite oxygen therapy. However, patients who do not respond quickly to non-invasive CPAP should be considered for tracheal intubation.
Tight-�ttingmask (nasal, facial, or hood)
CPAP valve:5, 7.5, or 10 cmH20(gas �ow adjustedto get correct valvemovement)
Humidi�er
Tubing
FiO2sensor
Three controlbuttons:OnGas �owO2 concentration
Safety valve(limitsbarotrauma)
Figure 4.7 A CPAP circuit.
c04.indd 63 7/20/2020 1:42:27 PM

Chapter 4 Respiratory Failure64
LEFT ATRIUM
LEFTVENTRICULAR(LV) CAVITY
1. Positive pressure squeezing LV
2. Leads to a reducedLV –aorta pressuregradient
3. Leads to less LVwall tension or workrequired to contract(afterload)
AORTA
Figure 4.8 How CPAP reduces afterload.
Mini-Tutorial:HighFlowNasalOxygenTherapy
High flow nasal oxygen therapy (HFNOT) is able to deliver humidified oxygen at high concentrations and at high flows that are equivalent to around 5 cmH2O of PEEP. The ability of nasal cannulae to provide a CPAP effect was first noted in neonates and is now commonly used in adults.10 HFNOT can deliver gas flows of up to 60 litres/min and its advantages are:
● Reduction in anatomical dead space ● Application of PEEP ● Delivery of an FiO2 close to 1.0 (100% oxygen) ● Delivery of humidified, warmed gas ● Ability to deal with copious secretions
The FLORALI trial11 randomised patients with non-cardiogenic acute hypoxaemic respiratory failure without hypercapnia and no contraindications (e.g. haemodynamic instability) to HFNOT, standard oxygen therapy, or NIV. Patients all had a PaO2/FiO2
c04.indd 64 7/20/2020 1:42:27 PM

-onasine Respiratory upport 65
InvasiveRespiratorySupport
In the past ‘iron lungs’ were used to apply an intermittent negative pressure to the thorax, thus inflating the lungs, but manual intermittent positive pressure ventilation (IPPV) was introduced during a large polio epidemic in Copenhagen in 1952. Mortality rates were lower than with previously used techniques. This heralded the introduction of intensive care units.
ICU ventilators are set to deliver either a certain volume or a certain pressure when inflating the lungs. This is termed ‘volume control’ or ‘pressure control’ ventilation. These different modes of ventilation have their own advantages and disadvantages (see Table 4.4).
In volume-controlled ventilation, inhalation proceeds until a preset tidal volume is deliv-ered and this is followed by passive exhalation. A feature of this mode is that gas is often delivered at a constant inspiratory flow rate, resulting in peak pressures applied to the air-ways higher than that required for lung distension. Since the volume delivered is constant, airway pressures vary with changing pulmonary compliance and airway resistance. A major disadvantage is that excessive airway pressure may be generated, resulting in baro-trauma, and so a pressure limit should be set by the operator.
In pressure-controlled ventilation, a constant inspiratory pressure is applied and the pressure difference between the ventilator and lungs results in inflation until that pressure is attained. Passive exhalation follows. The volume delivered is dependent on pulmonary
ratio (i.e. a comparison between alveolar oxygen – derived from the alveolar gas equa-tion – and FiO2) of 300 mmHg (40 kPa) or less. The use of HFNOT was associated with improved survival and there was a lower tracheal intubation rate among patients with a PaO2/FiO2 ratio of less than 200 mmHg.
The contraindications to HFNOT are the same as those for non-invasive respiratory support. Its advantages mean it is increasingly being used to treat pneumonia and postoperative respiratory failure – but as with all non-invasive respiratory support, it is important to select patients carefully, as ioappropriate perseneraoice can delay tracheal intubation when it is indicated and thus lead to worse outcomes.
In some countries, THRIVE (transnasal humidified rapid insufflation ventilatory exchange) is commonly used during anaesthesia and sedation.12 Warmed, humidified, high flow oxygen is administered through nasal cannulae at rates of 70–90 L/min. This not only provides PEEP, but also a degree of ventilation as a result of the interaction between the primary supraglottic vortex of gas from above and ‘cardiogenic oscillations’ from below. Cardiogenic oscillations result from compression and expansion of the small airways due to blood leaving and entering the thoracic cavity with each heart-beat. The amount of gas exchange that results from a ‘cardiogenic breath’ is small, but is enough to allow longer periods of apnoea or compromised ventilation during tra-cheal intubation of difficult airways and shared airway surgery, to give two examples.
c04.indd 65 7/20/2020 1:42:27 PM

Chapter 4 Respiratory Failure66
and thoracic compliance. A major advantage of pressure control is use of a decelerating inspiratory flow pattern, in which inspiratory flow tapers off as the lung inflates. This usu-ally results in a more homogenous gas distribution throughout the lungs. A disadvantage is that dynamic changes in pulmonary mechanics may result in varying tidal volumes.
Sophisticated ventilators have been manufactured which incorporate the advantages of both modes and also interact with patients. ICU ventilators can switch between modes so they can adapt to clinical circumstances and also facilitate weaning from the ventilator as the patient recovers. Ventilator modes are often described by what initiates the breath (trig-ger variable), what controls gas delivery during the breath (target or limit variable), and what terminates the breath (cycle variable). So, for example, BiPAP is machine or patient triggered, pressure targeted, and time cycled.
The most commonly used ventilator modes on the ICU are:
● BiPAP ● SIMV (synchronised intermittent mandatory ventilation) ● PSV (pressure support ventilation) also known as ASB (assisted spontaneous breaths) ● CPAP
In the ICU setting, BiPAP is considered to be a single mode of ventilation that covers the entire spectrum of mechanical ventilation to spontaneous breathing. When the patient has no spontaneous breaths, the ventilator acts as a pressure-controlled ventilator. When the patient has spontaneous breaths, the ventilator synchronises intermittently with the patient’s breathing and spontaneous breaths can occur during any phase of the respiratory cycle without increasing airway pressure above the set maximum level, as can occur with conventional pressure-controlled ventilation. When the patient is able to breathe more adequately, pressure support is used to augment every spontaneous breath.
The waveforms of these different ventilator modes are shown in Figure 4.9.
As well as the mode of ventilation, the operator of an ICU ventilator can adjust the fol-lowing main variables: FiO2, the inspiratory pressure, expiratory pressure (PEEP), backup
Table 4.4 Advantages and disadvantages of volume versus pressure control.
Volume control Pressure control
Delivery Delivers a set tidal volume no matter what pressure this requires. This can cause excessively high peak pressures and barotrauma
If airway pressures are high, only small tidal volumes will be delivered. Not good if lung compliance keeps changing
Leaks Poor compensation Compensates for leaks well (e.g. poor fitting mask or circuit fault)
PEEP Some flow/volume control ventilators cannot apply PEEP
PEEP easily added
PEEP = positive end-expiratory pressure.
c04.indd 66 7/20/2020 1:42:27 PM

-onasine Respiratory upport 67
respiratory rate, inspiratory time or I:E ratio, and alarm limits (e.g. minimum and maxi-mum tidal volumes).
PositiveEnd-ExpiratoryPressure(PEEP)
PEEP prevents the collapse of alveoli which has several benefits:
● Improvement of ventilation–perfusion matching ● Reduced lung injury from shear stresses caused by repeated opening and closing ● Prevention of surfactant breakdown in collapsing alveoli leading to improved lung
compliance
Lung disease is usually heterogeneous, so recruitment of alveoli in one part of the lung may cause over distension in another. PEEP also increases mean intrathoracic pressure which can
Airway pressure (cmH2O)
Time (s)
Mechanical ventilation
Spontaneous breathing
A
B
C
D
0
0
0
0
10
20
Patient triggeredbreath
Figure 4.9 Waveforms of different ventilator modes. A = BiPAP in a paralysed patient (i.e. no spontaneous breaths). B = SIMV. There are spontaneous breaths between mechanical breaths. The ventilator synchronises mechanical breaths so that the lungs are not inflated during inspiration. C = augmented PSV (pressure support ventilation). The ventilator assists every spontaneous breath. D = CPAP. Spontaneous ventilation plus a continuous positive airway pressure.
c04.indd 67 7/20/2020 1:42:28 PM

Chapter 4 Respiratory Failure68
reduce cardiac output. PEEP is normally set to 5 cmH2O and increased if required. ‘Best PEEP’ for a particular patient can be deduced from a ventilator’s pressure–volume loop display.
TheEffectsof MechanicalVentilation
During IPPV there is reversal of the thoracic pump – the normal negative intrathoracic pressure during spontaneous inspiration which draws blood into the chest from the vena cavae, a significant aspect of venous return. With IPPV, venous return decreases during inspiration, and if PEEP is added, venous return could be impeded throughout the respira-tory cycle. This can cause hypotension. The degree of impairment of venous return is directly proportional to the mean intrathoracic pressure. So changes in ventilatory pattern, not just pressures, can cause cardiovascular changes.
At high lung volumes, the heart may be directly compressed by lung expansion. This prevents adequate filling of the cardiac chambers. Ventricular contractility is also affected. Elevated intrathoracic pressures directly reduce the left and right ventricular ejection pres-sure which is the difference between the pressure inside and outside the ventricular wall during systole. As a result, stroke volume is reduced for a given end-diastolic volume. IPPV can also reduce renal, hepatic, and splanchnic blood flow.
These physiological changes during IPPV can be precipitously revealed when intubating critically ill patients. Marked hypotension and cardiovascular collapse can occur as a result of uncorrected volume depletion prior to tracheal intubation, compounded by the admin-istration of anaesthetic drugs which cause vasodilatation and reduce circulating catechola-mine levels as the patient loses consciousness. The effects of mechanical ventilation are not as severe when the patient is awake and breathing spontaneously.
Although mechanical ventilation can be life saving for people with respiratory failure, poorly applied ventilation techniques can not only cause cardiovascular compromise but can also damage lung tissue and lead to ventilator-induced lung injury (VILI). In particular, large tidal volumes and extreme cyclical inflation and deflation have been shown to worsen outcome in acute lung injury (see Chapter 6 for information on ventilation strategies in acute lung injury/acute respiratory distress syndrome).
An algorithm outlining the management of respiratory failure is shown in Figure 4.10.
Mini-Tutorial:TrachealIntubationin AcuteSevereAsthma
Tracheal intubation and ventilation can be a life-saving intervention in acute severe asthma. If indicated (i.e. when there is no response to maximum medical therapy), it is important that it is performed sooner rather than later. However, 10 minutes preparation beforehand is time well spent, particularly for those patients who are most unstable, as cardiovascular collapse can occur due to uncorrected volume depletion, the abolition of catecholamine responses, and vasodilatation when anaesthetic drugs are given. Patients should be volume loaded prior to induction of anaesthesia and a vasopressor (e.g. ephedrine or metaraminol)
c04.indd 68 7/20/2020 1:42:28 PM

The ooheeai of heeThanehi heaanihan a 69
kept ready to treat hypotension. Anaesthetic drugs can be given in such a way to minimise hypotension and drugs that cause histamine release should be avoided if possible. In acute severe life-threatening asthma, maximum medical therapy may mean intravenous salbuta-mol, magnesium sulphate, hydrocortisone, and nebulised or subcutaneous adrenaline.14 Therapy should be started while preparations to intubate are underway. Following tracheal intubation, the patient is ventilated with a looo expiratory tile and this may mean only 6–8 breaths per minute is possible. ‘Permissive hypercapnia’ is the term used when the PaCO2 is allowed to rise in such situations, in order to prevent ‘stacking’. This is when the next positive pressure is delivered before there has been enough time for expiration to fully occur (which is prolonged in severe lower airway obstruction). In ‘stacking’, the lung volume slowly expands, reducing venous return and leading to a progressive fall in cardiac output and blood pressure. This is corrected by disconnecting the ventilator and allowing passive expiration to occur (which can take several seconds). The updated UK asthma guidelines can be found on the British Thoracic Society website.13
RESPIRATORY FAILURE
Oxygen + maximum medical treatment (± physiotherapy)
IMPROVEMENT–observe
NO IMPROVEMENT
1. Is respiratory support appropriate? If yes,2. What type of respiratory support is indicated?
3. Make CPR and ICU decisions
Invasive ventilation on ICU
Move to an appropriatearea and start non-invasiverespiratory support
NO IMPROVEMENT
1. Adjust mask or settings2. Adjust medical treatment
if appropriate
NO IMPROVEMENT
Figure 4.10 Algorithm for the management of respiratory failure. The appropriateness of any respiratory support should be decided by a senior doctor e.g. it would not be appropriate to ventilate a patient who is imminently dying of an incurable lung disease.
c04.indd 69 7/20/2020 1:42:29 PM

Chapter 4 Respiratory Failure70
Self-Assessment: Case Histories
1 A previously well 30-year-old woman is admitted in a coma from a drug overdose and responds only to painful stimuli. Arterial blood gases on air show: pH 7.24, PaCO2 8.32 kPa (64 mmHg), st bicarbonate 29 mmol/L, BE +3, and PaO2 7.8 kPa (60 mmHg). The emergency department doctor diagnoses drug intoxication with probable aspira-tion pneumonia because of the hypoxaemia. What is your assessment?
2 Twenty-four hours later you are asked to assess the same patient for discharge as she has recovered and the hospital is in need of beds. She is alert and orientated and her repeat arterial blood gases on air show: pH 7.6, PaCO2 3.1 kPa (24 mmHg), st bicarbo-nate 22 mmol/L, BE −3, and PaO2 9.1 kPa (70 mmHg). Should you discharge this patient?
3 A 24-year-old woman is admitted with acute severe asthma. Her vital signs are as fol-lows: BP 100/60 mmHg, pulse 130 per minute, respiratory rate 40 per minute with poor respiratory effort, temperature 37°C, and she is drowsy. Her arterial blood gases on 15 litres per minute oxygen via reservoir bag mask show: pH 7.15, PaCO2 9.0 kPa (70 mmHg), st bicarbonate 22 mmol/L, BE −3, and PaO2 7 kPa (54 mmHg). What is your management?
4 Later on ICU the same patient develops hypotension (60/30 mmHg). The patient is sedated and paralysed and the ventilator is set to 12 breaths per minute. The inspiratory to expiratory ratio is 1 : 4, tidal volumes are 600 mL, and peak airway pressures are 45 cm H20. What are the possible causes of the hypotension and what is your management?
5 A 50-year-old man is admitted with an exacerbation of COPD. His arterial blood gases on a 28% Venturi mask show: pH 7.3, PaCO2 8.0 kPa (62 mmHg), st bicarbonate 29 mmol/L, BE +3, and PaO2 7 kPa (54 mmHg). What is your management?
KeyPoints – RespiratoryFailure
● Respiratory failure is due to a failure to ventilate, a failure to oxygenate, or both ● Treatment consists of oxygen therapy and treatment of the underlying cause ● If there is no improvement, respiratory support is indicated and the type of respira-tory support depends on the clinical situation
● Respiratory support can be non-invasive (e.g. via a tight-fitting mask, hood, or high flow nasal oxygen therapy) or invasive (tracheal intubation)
● Different types of respiratory support are indicated in different situations ● ICU ventilators utilise several different ventilator modes depending on the clinical situation
● Invasive mechanical ventilation is associated with cardiovascular effects and venti-lator induced lung injury.
c04.indd 70 7/20/2020 1:42:29 PM

elln-ssessleott: isicussioo 71
6 A 40-year-old man with no past medical history is admitted with severe pneumonia. His vital signs are: BP 120/70 mmHg, pulse 110 per minute, respiratory rate 40 per minute, temperature 38°C, and he is alert. His arterial blood gases on 15 litres per minute oxygen via reservoir bag mask show: pH 7.31, PaCO2 4.0 kPa (31 mmHg), PaO2 6 kPa (46 mmHg), st bicarbonate 14 mmol/L, and BE −7. What should you do?
7 You are called to see a 70-year-old man who had a laparotomy for small bowel obstruc-tion 3 days ago. He has developed a cough with green sputum and a fever. His respira-tory rate is increased (30 per minute) and his arterial blood gases on 10 litres per minute oxygen via Hudson mask show: pH 7.3, PaCO2 8.0 kPa (62 mmHg), st bicarbo-nate 29 mmol/L, BE +3, and PaO2 7.6 kPa (58 mmHg). What is your management?
8 A 60 kg 25-year-old woman diagnosed with Guillain–Barré syndrome has been under-going twice-daily forced vital capacity (FVC) measurements and treatment with intra-venous immunoglobulin therapy. Her FVC has fallen below 1 L and her arterial blood gases on air show: pH 7.3, PaCO2 7.5 kPa (58 mmHg), st bicarbonate 27 mmol/L, BE +2, and PaO2 10 kPa (77 mmHg). Her respiratory rate is 28 per minute with poor lung expansion. What should you do?
9 A 50-year-old woman is admitted to the emergency department after developing acute breathlessness. On examination, she has a blood pressure of 80 mmHg systolic. Her pulse is 110 per minute, respiratory rate 36 per minute, and she is alert but in respira-tory distress. Her chest is clear and an urgent portable chest X-ray is normal. The electrocardiogram shows sinus tachycardia with T wave inversion in leads V1–V6. Arterial blood gases on 15 litres per minute oxygen via reservoir bag mask show: pH 7.25, PaCO2 3.0 kPa (23 mmHg), st bicarbonate 10 mmol/L, BE −12, and PaO2 12 kPa (92 mmHg). What is the diagnosis and what is your management?
10 A 70-year-old man with COPD is admitted in extremis. He has been more breathless for the last few days. He responds to painful stimuli only, his blood pressure is 130/60 mmHg, pulse 120 per minute, and arterial blood gases on air show: pH 7.1, PaCO2 14.0 kPa (108 mmHg), st bicarbonate 20 mmol/L, BE −5, and PaO2 6 kPa (46 mmHg). What is your management?
Self-Assessment: Discussion
1 There is a low pH (acidaemia) due to a high PaCO2 – a respiratory acidosis. The st bicar-bonate is normal/high as expected. The PaO2 is low. In this situation, the PaO2 could be low because of upper airway obstruction, aspiration pneumonia, or hypoventilation caused by the drug overdose. The patient can be assessed clinically for signs of airway obstruction and the A–a gradient can be calculated to distinguish between a problem with gas exchange or hypoventilation. PAO2 = 0.21 × 95 − 8.32/0.8 = 9.6 kPa. The A–a gradient is therefore 9.6 − 7.8 = 1.8 kPa which is normal. This suggests hypoventilation rather than pneumonia is the cause of the low PaO2. The management in this case still starts with airway, breathing, and circulation.
c04.indd 71 7/20/2020 1:42:29 PM

Chapter 4 Respiratory Failure72
2 There is a high pH (alkalaemia) due to a low PaCO2. The st bicarbonate is normal/low as expected. The PaO2 has improved from before, but is still below the expected value. The A–a gradient can be calculated: PAO2 = 0.21 × 95 − 3.1/0.8 = 16.1 kPa. The A–a gra-dient is therefore 16.1 − 9.1 = 7 kPa which is abnormal. This arterial blood gas result could be explained by the development of aspiration pneumonia and requires further evaluation. The patient should not be discharged.
3 There is a low pH (acidaemia) due to a high PaCO2 – a respiratory acidosis. The st bicar-bonate is normal/high as expected. The PaO2 is very low when compared with the FiO2 of approximately 0.8 (or 80%). According to NHS England, three people die from asthma every day in the UK, but many of these deaths could be avoided. Previous life-threatening attacks increase the risk of death from asthma. You should have recog-nised, from the seriously abnormal vital signs, that this is a case of life-threatening asthma. Appropriate management therefore would be to call for help immediately, then assess and manage the airway, give oxygen, assess and manage breathing (nebu-lised and/or intravenous bronchodilators and exclude pneumothorax), assess and man-age circulation (give intravenous fluid – see mini-tutorial), and move on to disability and examination once A, B, C are stable or help arrives. Unless there is a dramatic improvement, this patient requires the ICU team and tracheal intubation.
4 See the mini-tutorial on tracheal intubation in acute severe asthma. Apart from ‘stack-ing’, tension pneumothorax and hypovolaemia are other possible causes. Normally, ventilators are set so that peak airway pressures do not exceed 35 cmH2O. This is slightly complicated by the fact that peak pressures in acute severe asthma do not necessarily reflect alveolar pressures but the ventilator pressures needed to overcome airway obstruction. PEEP is routinely added on ICU ventilators, but is not usually of benefit in acute severe asthma as patients already have significant intrinsic or ‘auto’-PEEP. In summary, an expert should supervise the ventilator requirements of any patient with acute severe asthma.
5 There is a low pH (acidaemia) due to a high PaCO2 – a respiratory acidosis. The st bicar-bonate is normal/high as expected. The PaO2 is low. Apart from A, B, C, prompt medi-cal management of his exacerbation of COPD may improve things. The oxygen could be increased to 35% and information about the patient’s usual function and any previ-ous spirometry results sought. A chest X-ray should be requested to exclude a pneumo-thorax and look for pneumonia. If there is no prompt improvement of his respiratory acidosis with medical therapy, non-invasive ventilation should be started. Oxygen ther-apy is given through the ventilator mask, titrated to arterial blood gases. Intravenous fluid is often required for dehydration in breathless patients.
6 There is a low pH (acidaemia) due to a low st bicarbonate. The expected PaCO2 should be lower, indicating a ‘hidden’ respiratory acidosis – he is tiring. This patient has seri-ously abnormal vital signs and marked hypoxaemia despite a high concentration of oxygen. He may well be alert and talking, but he requires immediate assessment by the ICU team. Intravenous fluid should be given for the metabolic acidosis, which is
c04.indd 72 7/20/2020 1:42:29 PM

elln-ssessleott: isicussioo 73
due to sepsis. Although some may be tempted to try non-invasive respiratory support first in this situation, this is not supported by evidence-based guidelines and should not be performed outside an ICU. This patient is likely to require tracheal intubation.
7 There is a low pH (acidaemia) due to a high PaCO2 – a respiratory acidosis. The st bicarbonate is normal/high as expected. The PaO2 is low. Postoperative respiratory failure is caused by atelectasis due to a combination of recumbency, general anaesthe-sia, and pain which prevents deep breathing and coughing. Opioid analgesia also depresses respiration and cough. Retained secretions and even lobar collapse can occur. Management in this case should prioritise good pain relief (consider epidural analgesia) and urgent chest physiotherapy. The oxygen concentration should be increased and humidified. Antibiotics and sputum culture are required. If there is no improvement, the ICU team should be contacted. Non-invasive ventilation may be tried in the first instance, but this should be administered in a level two to three area and each patient should be assessed on an individual basis by an expert.
8 There is a low pH (acidaemia) due to a high PaCO2 – a respiratory acidosis. The st bicarbonate is normal and the PaO2 is low. There is evidence of ventilatory failure (high PaCO2 and increased respiratory rate with a poor respiratory effort) as a result of increasing respiratory muscle weakness (falling FVC). Closer examination may reveal a patient who is using accessory respiratory muscles and has a cough which is bovine in nature. Neurological examination may also reveal poor bulbar function. Monitoring oxygen saturations and arterial blood gases in this situation are of little help in decid-ing when to institute respiratory support because abnormal arterial blood gases follow ventilatory failure rather than precede it. This is why the FVC is closely monitored in this condition. The usual cut-off is 15 mL per kg, below which tracheal intubation and ventilation is recommended. Up to one-third of patients with Guillain–Barré syn-drome admitted to hospital require mechanical ventilation.14 Autonomic neuropathy can accompany the syndrome, leading to tachycardia and hypotension which also require close observation especially during tracheal intubation which can precipitate asystole from profound vagal stimulation.
9 This patient is in shock. There is a low pH (acidaemia) due to a low st bicarbonate – a metabolic acidosis. The PaCO2 is low as expected. However, the PaO2 is very low com-pared with the FiO2. The A–a gradient is PAO2 = 0.8 × 95 − 3.0/0.8 = 72.25 kPa. A–a gradient = 72.25 − 12 = 60.25 kPa. What could cause such a significant problem with gas exchange, blood pressure as well as electrocardiogram changes with a normal chest X-ray? The answer is a massive pulmonary embolism. Treatment (after A, B, C, including fluid challenges) in this case includes intravenous thrombolysis which should be considered in pulmonary embolism causing shock.15
10 There is a low pH (acidaemia) due to a high PaCO2 – a respiratory acidosis. The st bicarbonate should be normal/high but it is low, indicating a ‘hidden’ metabolic acido-sis as well. The PaO2 is low. His airway should be assessed and he requires oxygen to get his PaO2 to around 8 kPa (60 mmHg). His breathing should be assessed next and
c04.indd 73 7/20/2020 1:42:29 PM

Chapter 4 Respiratory Failure74
medical therapy commenced. Non-invasive ventilation is usually contraindicated in patients with severe respiratory acidosis or who are unconscious. However, before pro-ceeding to tracheal intubation, further information should be sought if possible as to the severity of the patient’s chronic lung disease. Has a discussion already taken place about tracheal intubation and ventilation between the patient and his specialist? Do the next of kin have information (e.g. in the form of an advanced directive or ‘do not resuscitate’ order) about what should happen in the event of an acute severe illness? Sometimes, non-invasive ventilation is used as a ‘second best’ but more appropriate treatment. Each patient should be assessed individually by an experienced doctor.
References
1 Rochwerg B, Brochard L, Elliot MW et al. Official ERS/ATS clinical practice guidelines: non-invasive ventilation for acute respiratory failure. Eur Respir J 2017; 50: 1602426.
2 British Thoracic Society Standards of Care Committee. Non-invasive ventilation in acute respiratory failure. Thorax 2002; 57: 192–211.
3 Nava S, Ambrosino N, Clini E et al. Non-invasive mechanical ventilation in the weaning of patients with respiratory failure due to chronic obstructive pulmonary disease. A randomised controlled trial. Ann Intern Med 1998; 128: 721–728.
4 Confalonieri M, Potena A, Carbone G et al. Acute respiratory failure in patients with severe community-acquired pneumonia. A prospective randomised evaluation of non-invasive ventilation. Am J Respir Crit Care Med 1999; 160: 1585–1591.
5 The YONIV trial, Plant PK, Owen JL, Elliot MW. A multi-centre randomised controlled trial of the early use of non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards. Lancet 2000; 355(9219): 1931–1935.
6 Conti G, Antonelli M, Navalesi P et al. Non-invasive vs conventional mechanical ventilation in patients with chronic obstructive pulmonary disease after failure of medical treatment in the ward: a randomized trial. Intensive Care Med 2002; 28: 1701–1707.
7 Plant PK, Owen JL, Elliot MW. One year prevalence study of respiratory acidosis in acute exacerbations of COPD: implications for the provision of non-invasive ventilation and oxygen administration. Thorax 2000; 55: 550–554.
8 National Institute for Health and Care Excellence (NICE). Chronic obstructive pulmonary disease in over 16s: diagnosis and management. NG115. Last updated July 2019. https://www.nice.org.uk/guidance/ng115 (Accessed October 2019).
9 Vital FMR, Ladiera MT, Atallah AN. Non-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema. Cochrane Database Syst Rev 2013; 5: CD005351.
10 Ashraf-Kasani N, Kumar R. High-flow nasal oxygen therapy. BJA Educ 2017; 17(2): 63–67. 11 Frat J-P, Thille A, Mercat A et al. High-flow oxygen through nasal cannula in acute
hypoxaemic respiratory failure. N Engl J Med 2015; 372(23): 2185–2196. 12 Nouraei R, Shorthouse JR, Keegan J et al. What is transnasal humidified rapid insufflation
ventilatory exchange (THRIVE)?. ENT Audiol News 2018; 27(2). https://www.entandaudiologynews.com/development/spotlight-on-innovation/post/what-is-transnasal-humidified-rapid-insufflation-ventilatory-exchange-thrive (Accessed January 2020).
c04.indd 74 7/20/2020 1:42:29 PM

Further Resourices 75
13 BTS/SIGN. British guideline on the management of asthma, 2019. https://www.brit-thoracic.org.uk/quality-improvement/guidelines/asthma (Accessed October 2019).
14 Yentis SM, Hirsch NP, Smith BG (Eds). Guillain-Barré syndrome. In: Anaesthesia and Intensive Care A-Z, 3rd edition. London, Butterworth Heinemann, 2004.
15 National Institute for Health and Care Excellence (NICE). Venous thromboembolic diseases: diagnosis, management and thrombophilia testing. CG144. Last updated November 2015. https://www.nice.org.uk/guidance/cg144 (Accessed October 2019).
FurtherResources
West JB. Respiratory Physiology the Essentials, 7th edition. Philadelphia, Lippincott Williams and Wilkins, 2005.
Symonds AK (Ed). Non-Invasive Respiratory Support: A Practical Handbook, 3rd edition. New York, CRC Press, 2007.
Davidson AC, Banham S, Elliot M et al. BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults. Thorax 2016; 71: ii1–ii35.
c04.indd 75 7/20/2020 1:42:29 PM

c04.indd 76 7/20/2020 1:42:29 PM