Embed Size (px)
Citation preview

[CANCER RESEARCH 46, 3225-3238, July 1986]
Basic Principles and Applications of Monoclonal Antibodies in the Management ofCarcinomas: The Richard and Hinda Rosenthal Foundation Award Lecture1
Jeffrey SchlomLaboratory of Tumor Immunology and Biology, National Cancer Institute, NIH, Bethesda, Maryland 20892
Introduction
The advent of hybridoma technology in 1975 (1) representeda quantum leap in the field of tumor immunology. For the firsttime, B-lymphocytes from immunized hosts could be immortalized by means of fusion with drug selected non-immunoglob-ulin secretor murine myeloma cells. These fused cell productscould then be cloned and propagated indefinitely. The supernatant fluids of cultures from literally thousands of these clonedcell populations (termed hybridomas) could then be assayed toselect for homogeneous populations of immunoglobulins withthe desired reactivity. As a result of this technology, numerousMAbs2 have been generated that have led to the identification
and/or characterization of TAAs from various human carcinomas, melanomas, leukemias, and lymphomas. To date, morethan 100 MAbs against human carcinomas have been reportedin the literature (see Ref. 2 for review); most have been characterized as unique with respect to range of reactivity andreactive antigen or epitope. Some of the more extensivelycharacterized MAbs to carcinoma associated antigens are listedin Table 1. Many of these MAbs have already been used invarious aspects of patient management or in better defining thebiology of carcinoma cell populations.
The potential applications of MAbs in the management ofhuman carcinomas are outlined in Table 2. They can be dividedinto three major categories: diagnosis, prognosis, and treatment. The principles and applications governing each of thesecategories will be discussed in detail below.
MAbs to Carcinoma Associated Antigens
The development and characterization of MAbs to tumorassociated antigens, differentiation antigens, proteins associated with the metastatic process, and oncogene products are allthe subject of active investigations. This article, however, willdeal primarily with MAbs directed against tumor associatedantigens. For reasons of succinctness, studies involving only afew of these MAbs will be described in detail. Several basicprinciples, however, appear to pertain to the vast majority ofTAAs that have been defined by most anticarcinoma MAbs.These are:
(a) A given carcinoma associated antigen is usually expressedon more than one type of carcinoma. For example, a MAbgenerated with the use of a breast tumor extract as immunogenmay react not only with breast carcinomas but also with at leastone other, or several other, carcinoma types, such as ovarian,colorectal, or lung carcinoma.
(b) Not all tumors within a given tumor type will express agiven TAA. For example, a given MAb may react with 80% ofcolorectal cancers.
(c) Not all cells within a given tumor lesion will express a
Received 2/19/86; accepted 3/25/86.1Presented on May 22, 1985, at the Seventy-sixth Annual Meeting of the
American Association for Cancer Research, Houston, TX.2The abbreviations used are: MAb, monoclonal antibody; TAA, tumor asso
ciated antigen; TAG-72, tumor associated glycoprotein 72; CEA, carcinoem-bryonic antigen; RIA, radioimmunoassay; p21, M, 21,000 protein; RI, radiolo-calization index; IFN-aA, clone A a-interferon.
particular TAA. This is also carried over into metastatic lesions;i.e., various metastatic lesions from one patient will express agiven TAA to varying degrees.
(d) There is not only antigenic heterogeneity among carcinoma cell populations but also a temporal modulation of tumorantigens.
(e) Many carcinoma associated antigens are stable components of the cell membrane. This is quite different from observations of lymphoid antigens which, when complexed with anantibody, are usually internalized, capped, or shed. In contrast,it has been shown that when MAbs to some carcinoma associated antigens bind to the cell surface, no internalization, capping, or shedding occurs.
(/) Carcinoma associated antigens can be categorized as"private" or "public." The more public an antigen, the more
likely it is to be expressed on most cells of most carcinomas ofa given type; however, these determinants are usually alsoexpressed on some normal adult cell populations. The moreprivate antigens are either not expressed or weakly expressedon normal adult cells; generally, however, a lower percentageof tumors or cells within a given tumor express the privateantigen as compared to the public antigen. Many of theseprinciples will be exemplified and further detailed in this report.
Characterization of a Novel Tumor Associated Glycoprotein(TAG-72)
Whereas many MAbs have been generated to known tumorantigens, several novel TAAs have been discovered by MAbsgenerated using relatively crude tumor extract as immunogen.MAb B72.3 (3) exemplifies one such antibody. It has beenextensively studied in several laboratories and it recognizes anovel tumor associated glycoprotein (termed TAG-72). TAG-72 represents a prototype of a more private TAA.
We have recently reported (4) the partial purification andcharacterization of TAG-72 from xenograft tumors [from thehuman carcinoma cell line (LS-174T)] which expresses highlevels of this antigen. The tumor homogenate was initiallyfractionated by Sepharose CL-4B chromatography and thensubjected to two sequential passages through B72.3 antibodyaffinity columns. The three step procedure produced a purification of TAG-72 with minimal contamination by other proteins as shown by polyacrylamide gel electrophoresis followedby staining with Coomassie blue or periodic acid-Schiff reagent.The density of affinity purified TAG-72, as determined bycesium chloride gradient ultracentrifugation, was found to be1.45 g/ml. This density determination, together with the highmolecular weight of TAG-72, its resistance to chondroitinasedigestion, the presence of blood group related oligosaccharides,and sensitivity to shearing into lower molecular weight formssuggest that TAG-72 is a novel mucin-like molecule with amolecular weight of >106. TAG-72 can clearly be distinguished
from the M, 180,000 carcinoembryonic antigen.MAb B72.3 is a murine IgGl which was prepared using a
membrane enriched extract of human metastatic breast carcinoma as antigen (3). It has been reacted with a spectrum of
3225
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
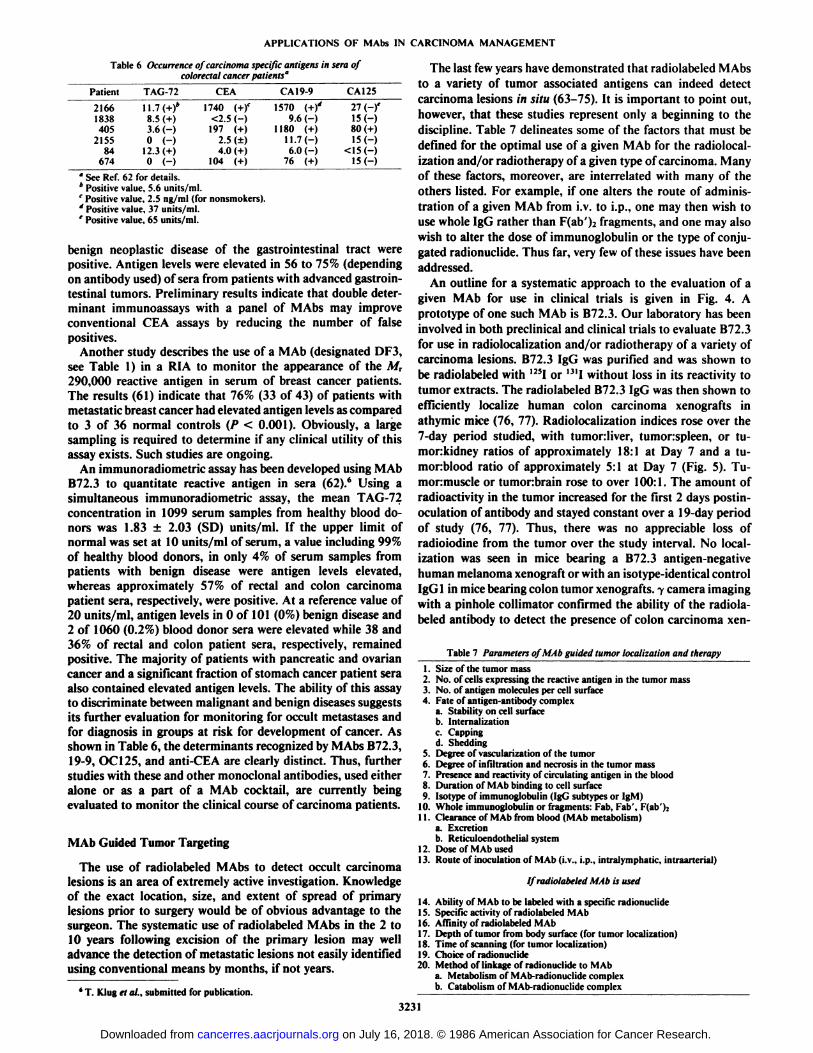
Table 1 Monoclonal antibodies' reactive with human carcinomas Table 3 MAb B72.ÃŒreactivity with human neoplasia"
ImmunogenBreast
carcinomaHuman
milkColon
carcinomaOvarian
carcinomaPancreaticMAbB72.3
DF3HMFG1,
HMFG219-917-1A
NPI-435,73COL1-15OC
125DU-PAN-2Reactive
antigenM,>10*mucin(TAG-72)
M,290.000High
molecularweight
glycoproteinGlycoprotein
(~M, 200,000)*
Unknown proteinCEA (M, 180,000)CEA. (M, 180.000)CEA (M,180,000)M,
750,000High
molecularRef.3,
5, 88
2689,9055-57,
91,9291,
93, 9418,209512996
weightglycoprotein
" Selected MAbs are listed in Table I as examples; see the article of Schlom
and Weeks (2) for a more comprehensive review.* T. Klug, personal communication.
Table 2 Potential clinical applications of MAbs with Human carcinomas
I. DiagnosisA. Screening of body fluids (serum, sputum, effusions, urine, cerebrospinal
fluid) for the presence of TAAB. Nuclear scanning with radiolabeled MAb
1. Detection of primary or metastatic lesions (i.V., subepidermal, or i.p.administration of radiolabeled MAb)
2. Lymphoscintigraphy to detect lymph node involvementC. Immunopathology
1. The diagnostic dilemma: malignant vs. benign2. Differential diagnosis of tumor type3. Subclassification of tumor based on TAA expression
a. Melastatic potentialb. Specific favored sites of metastasisc. Predicted response (or lack thereof) to specific therapeutic regi
mensd. Prognosis
II. Monitoring of disease progressionA. Screening of body fluids (see IA) for TAAB. Nuclear scanning with radiolabeled MAb to detect or quantitate tumor
recurrence (see IB)C. Immunopalhology for detection of occult métastases
1. Aspiration cytology2. Lymph node or bone marrow biopsy3. Cytology of body fluids
HI. TherapyA. Direct cytotoxicity of MAb
1. Complement mediated2. Cell mediated
B. Drug conjugation of MAb (e.g., Adriamycin)C. Toxin conjugation of MAb (e.g., ricin)D. Radionuclide conjugation of MAb (e.g., a or ßemitters)E. Ex vivo tumor removal from harvested bone marrowF. Inhibition of receptors for growth factorsG. Administration of anti-idiotype MAbs to induce specific active immunity
to tumor antigens
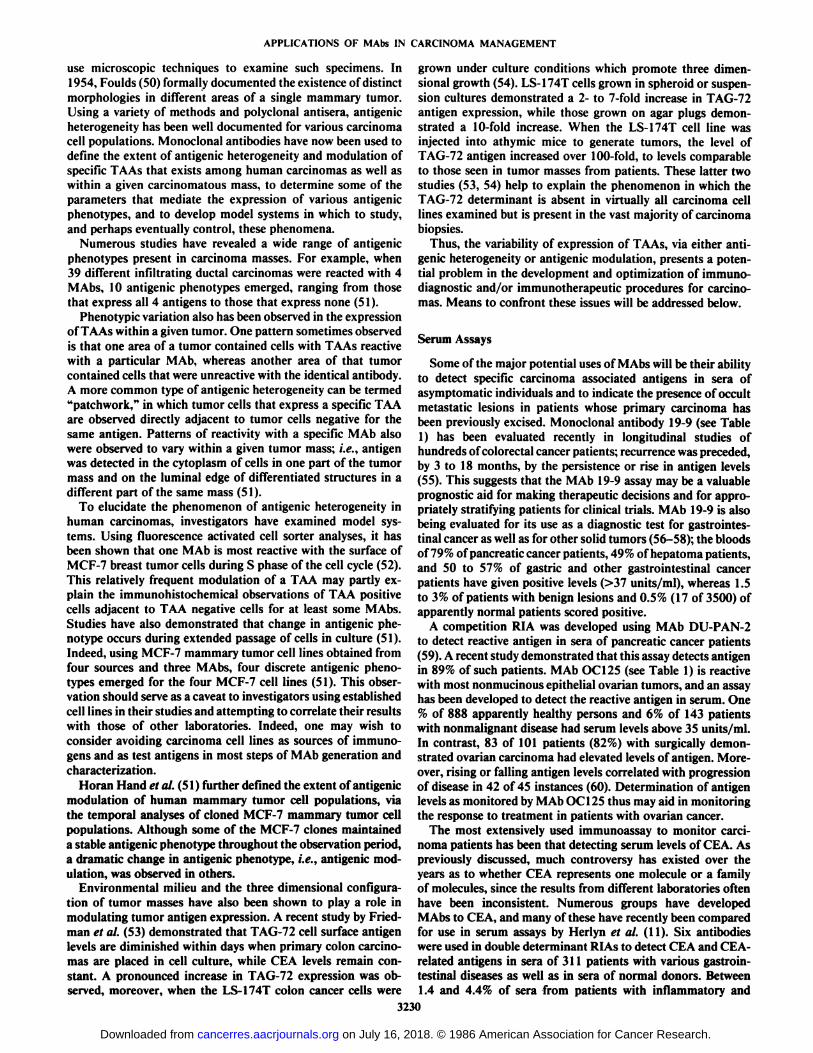
adult and fetal human tissues using avidin-biotin complex im-munohistochemical techniques to evaluate the expression ofthe reactive TAG-72 antigen (5-7). TAG-72 has been shown tobe expressed in several epithelial derived malignancies includingthe vast majority of colonie adenocarcinomas, invasive ductalcarcinomas of the breast, non-small cell lung carcinomas, common epithelial histological types of ovarian carcinomas (Table3), as well as the majority of pancreatic, gastric, and esophagealcancer evaluated. TAG-72 expression has not been detected,however, in tumors of neural, hematopoietic, or sarcomatousderivation, suggesting that the TAG-72 antigen is "pancarci-noma" in nature. No or only trace MAb B72.3 reactivity has
been observed with a wide range of adult normal tissues, withlimited reactivity noted in a few benign lesions of the breastand colon. The one exception thus far noted is the expressionof TAG-72 in secretory phase endometrium (but not the prolif-
OrganOvaryLungColonBreastHistológica!tumortypeSerous
cystadenocarcinomaMucinouscystadenocarcinomaAdenocarcinoma
Squamous cell carcinomaLarge cellcarcinomaAdenocarcinomaInvasive
ductal carcinomaNo.
ofreactive
tumors/no.tested30/30
10/1028/29
(97)3/3
1/151/54(94)37/44
(84)>20%
reactivemalignantcells14/30(47)*
6/10(60)20/29
(69)1/30/123/54
(43)12/44(27)
•See Ref. 6 for details.* Numbers in parentheses, percentage.
80in_jLUOLU
60F<ce
40j-L1J
UDCS
20A.—
•..*...
....a
Ä.
••••••.....B..-fAW O^
^ V V ¿i**•
••
••**•-•
••*•*••* ••*•*•*•.
v>. .D._-•-«7•
•O O OO* wvMALIGNANT BENIGN
COLONMALIGNANT BENIGN
BREAST
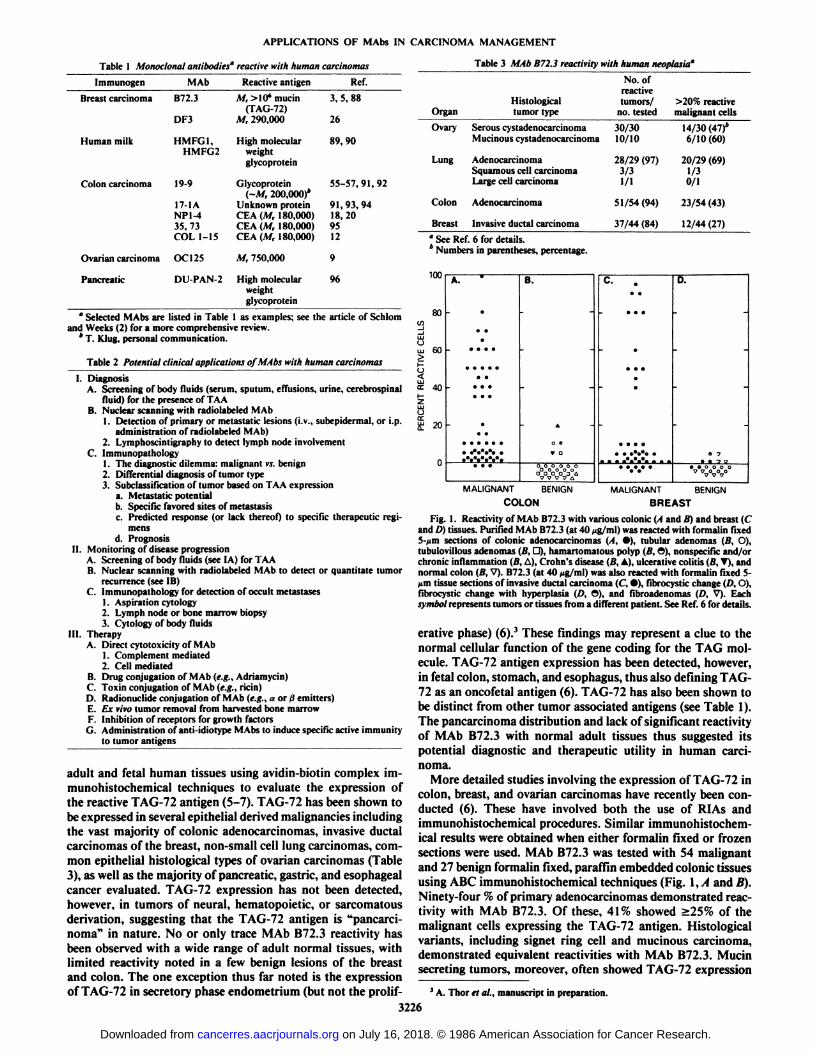
Fig. I. Reactivity of MAb B72.3 with various colonie (A and B) and breast (Cand /') tissues. Purified MAb B72.3 (at 40 ^g/ml) was reacted with formalin fixed5-/im sections of colonie adenocarcinomas (A, •),tubular adenomas (B, O),tubulovillous adenomas (B, O), hamartomatous polyp (B, O), nonspecific and/orchronic inflammation (B, A), Crohn's disease (/>'.A), ulcerative colitis (I!, T), andnormal colon (B, V). B72.3 (at 40 jig/ml) was also reacted with formalin fixed 5-um tissue sections of invasive ductal carcinoma (C, •),fibrocystic change (D, O),fibrocystic change with hyperplasia i/>, O), and fibroadenomas (/', V). Eachsymbol represents tumors or tissues from a different patient. See Ref. 6 for details.
erative phase) (6).3 These findings may represent a clue to the
normal cellular function of the gene coding for the TAG molecule. TAG-72 antigen expression has been detected, however,in fetal colon, stomach, and esophagus, thus also denning TAG-72 as an oncofetal antigen (6). TAG-72 has also been shown tobe distinct from other tumor associated antigens (see Table 1).The pancarcinoma distribution and lack of significant reactivityof MAb B72.3 with normal adult tissues thus suggested itspotential diagnostic and therapeutic utility in human carcinoma.
More detailed studies involving the expression of TAG-72 incolon, breast, and ovarian carcinomas have recently been conducted (6). These have involved both the use of RIAs andimmunohistochemical procedures. Similar immunohistochem-ical results were obtained when either formalin fixed or frozensections were used. MAb B72.3 was tested with 54 malignantand 27 benign formalin fixed, paraffin embedded colonie tissuesusing ABC immunohistochemical techniques (Fig. I, A and B).Ninety-four % of primary adenocarcinomas demonstrated reactivity with MAb B72.3. Of these, 41% showed >25% of themalignant cells expressing the TAG-72 antigen. Histologicalvariants, including signet ring cell and mucinous carcinoma,demonstrated equivalent reactivities with MAb B72.3. Mucinsecreting tumors, moreover, often showed TAG-72 expression
3A. Thor et al., manuscript in preparation.
3226
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
within secreted mucinous material and glandular lumina. Heterogeneity of TAG-72 expression was observed between cellsof primary tumors, as well as between and among primary,regional, and distant colon carcinoma tumor métastases.MAbB72.3 demonstrated minimal reactivity with benign colon tissues, although a single specimen from a patient with activeCrohn's disease demonstrated 20% of the epithelial cells to be
reactive. Colon specimens examined without histological abnormalities were negative for TAG-72 expression.
MAb B72.3 was also tested for reactivity with formalin fixed,paraffin embedded primary invasive ductal carcinomas (n =44), as well as a variety of benign breast lesions (Fig. 1, C andD). Eighty-four % of primary breast carcinomas demonstratedexpression of the TAG-72 antigen, although only 27% contained >25% of the malignant epithelial cells reactive withMAb B72.3. No correlation was observed between histologicaltumor grade, lymph node status, the presence of estrogenreceptor, and the expression of the TAG-72 antigen. Heterogeneity was also observed in both primary as well as metastaticlesions in a manner similar to that noted for colon carcinoma.Despite a prolonged MAb B72.3 incubation time and relativelyhigh concentrations of MAb used, a variety of benign breastlesions failed to demonstrate enhanced levels of TAG-72expression (Fig. ID). Reactivity with apocrine metaplasia wasoccasionally noted; however, this epithelial alteration has acharacteristic histological appearance and can be easily differentiated from carcinomas.
Thor et al. (8) have recently shown B72.3 to be reactive witha variety of malignant and borderline ovarian tumor types usingthe immunoperoxidase technique and surgically resected tissues. TAG-72 is expressed in >5% of malignant epithelial cellsin 77% of human primary and 71% of metastatic ovariancancers of the common epithelial histological subtypes (Fig. 2).Serous and mucinous cystadenocarcinomas and undifferen-tiated, endometrioid, and clear cell carcinomas were all shownto express the TAG-72 antigen. In contrast, normal ovariantissues and 26 of 27 benign ovarian tumors of various histological subtypes failed to express similar levels of TAG-72; ofinterest was one benign tumor which demonstrated unusualglandular complexity, as well as 3 tumors designated borderlinemalignancy, which contained elevated TAG-72 expression (Fig.
ÃŽ3100O
90>
80?
70050£
40mR
3°;»i
io0A.
Malignant.Primary-
..•-
:"iV:»«••••,B.
MalignantMetastatic•V••,•.*.*.*.•
•C.
BenignOvary«aO
3.O
b.o
a.00000
ODOOO00000000000oooooooD.
NormalOvary_----00
DO
Fig. 2. Purified MAb B72.3 (at a concentration of 40 ng/ml) reactivity withformalin fixed paraffin embedded sections of ovarian tissue. Each symbol represents tumors or tissues from a different patient. . I. malignant primary tumors(•);B, malignant metastatic tumors (•);( . benign tumors (O), tumors ofborderline malignant potential (O a.). Tumor b. represents a mucinous cystade-iionia noted to have "epithelial complexity with no cytological atypia"; D, normal
ovary (D). See Ref. 8 for details.
2). This suggests that expression of the TAG-72 antigen mayhave prognostic significance in that it may reflect a moremalignant phenotype of ovarian epithelium. MAb B72.3 hasalso been used to successfully detect ovarian carcinoma cells incytological preparations of human serous effusions and peritoneal washings (see below). In addition, the reactivity of MAbB72.3 was shown (8) to be quite distinct from that of MAbOC 125 (9). Potential applications of MAb B72.3 in the studyof human ovarian cancer cell populations, as well as in severalaspects of the management of human ovarian cancer, will bediscussed below.
MAbs Define a Repertoire of Epitopes on CEA
CEA is among the most extensively studied oncofetal antigens. It has been described as a M, 180,000 complex glycopro-tein which is highly expressed by both embryonic colonie mucosa and carcinomas of the gastrointestinal tract (10). Therehave been numerous reports, however, that indicate that CEAmay actually be a family of isoantigens and that anti-CEAantibodies may indeed differ dramatically in their reactivity(11).
There are several areas in which MAbs to CEA are beingused in the management of carcinoma patients. These includeblood assays to monitor tumor burden, immunohistopatholog-ical analyses of tissue samples to detect or further characterizetumor cells, and in situ detection of carcinomatous lesions(either at primary sites, in regional lymph nodes, or at distalsites) using radiolabeled antibody. One of the major drawbacksof the use of anti-CEA antibodies for the above purposes hasbeen the cross-reactivity of some of these reagents with severalnormal adult tissues. Using purified CEA, colon and gastriccarcinoma cell lines, and extracts of human breast carcinomasas immunogens, anti-CEA MAbs have been generated whichcross-react with CEA-related antigens on normal colonie mucosa, spleen, liver, lung, sweat glands, polymorphonuclear leukocytes, and/or monocytes (see Ref. 12 for review). The CEAcross-reacting antigens most commonly described are normalcross-reacting antigen (NCA) (13), NCA-2 (14), normal fecalantigen (IS), met-on ¡urnantigen (16), and biliary glycoprotein
(17). At present, the degree of differential expression of CEAin carcinomas versus normal tissues is not resolved. A well-characterized group of anti-CEA MAbs (18,19), some of whichare currently being used in radioimaging of colon cancer patients, has been shown to have at least some degree of reactivityto normal polymorphonuclear leukocytes. Perhaps the mostwell-characterized anti-CEA MAbs, in terms of range of reactivities to tumor and nontumorous tissues, are those recentlyreported by Primus et al. (18, 20) and designated NP-1 to NP-4. MAb NP-1 was shown to react with polymorphonuclearleukocytes, and MAbs NP-1 to NP-3 were shown to react withnormal colon. One of the most highly selective anti-CEA MAbsthus far reported in terms of differential reactivity for coloncarcinoma versus normal adult tissues is MAb NP-4. Oneinteresting finding of these studies, however, was that the NP-4 epitope is principally expressed on primary colon carcinomasand not in regional or distal métastases.
Muraro et al. (12) have recently described 15 anti-CEAmonoclonal antibodies (termed COL 1 through COL 15), obtained from mice immunized with several different preparationsfrom human colon carcinoma biopsy material. These MAbswere selected early in the screening process for lack of reactivityto polymorphonuclear leukocytes, the most common cross-reactive normal tissue of anti-CEA antibodies. These MAbs
3227
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
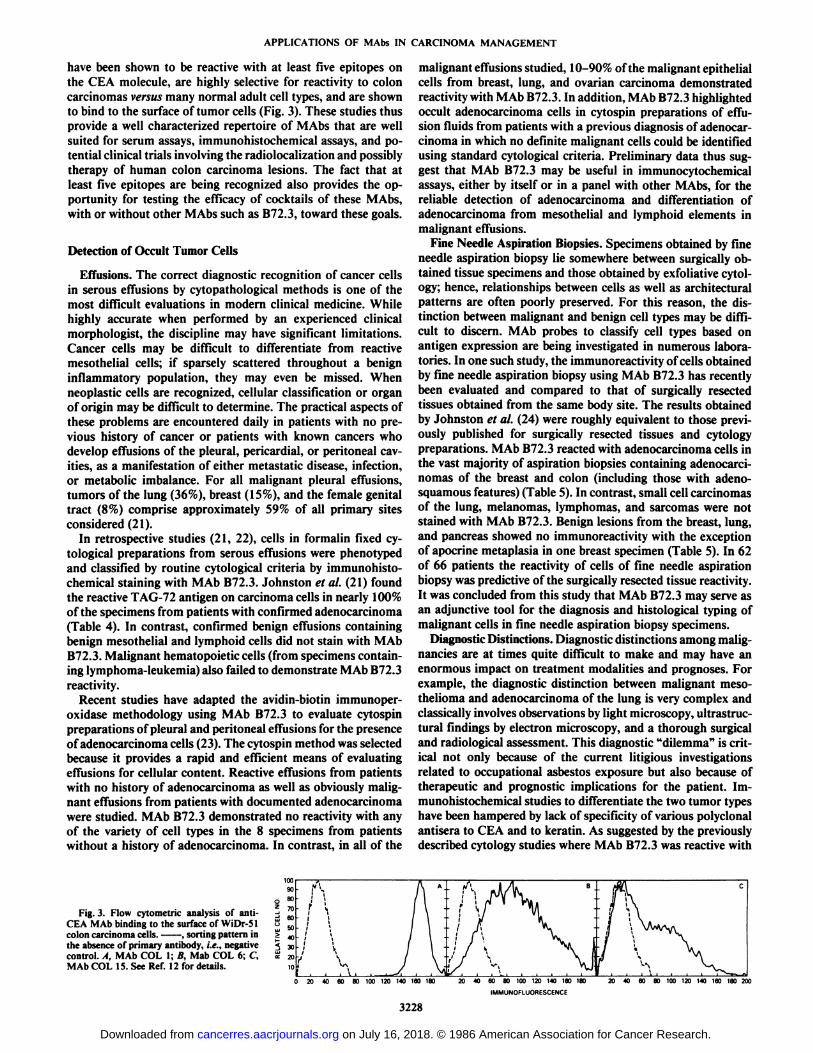
have been shown to be reactive with at least five epitopes onthe CEA molecule, are highly selective for reactivity to coloncarcinomas versus many normal adult cell types, and are shownto bind to the surface of tumor cells (Fig. 3). These studies thusprovide a well characterized repertoire of MAbs that are wellsuited for serum assays, immunohistochemical assays, and potential clinical trials involving the radiolocalization and possiblytherapy of human colon carcinoma lesions. The fact that atleast five epitopes are being recognized also provides the opportunity for testing the efficacy of cocktails of these MAbs,with or without other MAbs such as B72.3, toward these goals.
Detection of Occult Tumor Cells
Effusions. The correct diagnostic recognition of cancer cellsin serous effusions by cytopathological methods is one of themost difficult evaluations in modern clinical medicine. Whilehighly accurate when performed by an experienced clinicalmorphologist, the discipline may have significant limitations.Cancer cells may be difficult to differentiate from reactivemesothelial cells; if sparsely scattered throughout a benigninflammatory population, they may even be missed. Whenneoplastic cells are recognized, cellular classification or organof origin may be difficult to determine. The practical aspects ofthese problems are encountered daily in patients with no previous history of cancer or patients with known cancers whodevelop effusions of the pleural, pericardia!, or peritoneal cavities, as a manifestation of either metastatic disease, infection,or metabolic imbalance. For all malignant pleural effusions,tumors of the lung (36%), breast (15%), and the female genitaltract (8%) comprise approximately 59% of all primary sitesconsidered (21).
In retrospective studies (21, 22), cells in formalin fixed cy-tological preparations from serous effusions were phenotypedand classified by routine cytological criteria by immunohistochemical staining with M Ab B72.3. Johnston et al. (21) foundthe reactive TAG-72 antigen on carcinoma cells in nearly 100%of the specimens from patients with confirmed adenocarcinoma(Table 4). In contrast, confirmed benign effusions containingbenign mesothelial and lymphoid cells did not stain with MAbB72.3. Malignant hematopoietic cells (from specimens containing lymphoma-leukemia) also failed to demonstrate MAb B72.3reactivity.
Recent studies have adapted the avidin-biotin immunoper-oxidase methodology using MAb B72.3 to evaluate cytospinpreparations of pleural and peritoneal effusions for the presenceof adenocarcinoma cells (23). The cytospin method was selectedbecause it provides a rapid and efficient means of evaluatingeffusions for cellular content. Reactive effusions from patientswith no history of adenocarcinoma as well as obviously malignant effusions from patients with documented adenocarcinomawere studied. MAb B72.3 demonstrated no reactivity with anyof the variety of cell types in the 8 specimens from patientswithout a history of adenocarcinoma. In contrast, in all of the
malignant effusions studied, 10-90% of the malignant epithelialcells from breast, lung, and ovarian carcinoma demonstratedreactivity with MAb B72.3. In addition, MAb B72.3 highlightedoccult adenocarcinoma cells in cytospin preparations of effusion fluids from patients with a previous diagnosis of adenocarcinoma in which no definite malignant cells could be identifiedusing standard cytological criteria. Preliminary data thus suggest that MAb B72.3 may be useful in immunocytochemicalassays, either by itself or in a panel with other MAbs, for thereliable detection of adenocarcinoma and differentiation ofadenocarcinoma from mesothelial and lymphoid elements inmalignant effusions.
Fine Needle Aspiration Biopsies. Specimens obtained by fineneedle aspiration biopsy lie somewhere between surgically obtained tissue specimens and those obtained by exfoliative cytology; hence, relationships between cells as well as architecturalpatterns are often poorly preserved. For this reason, the distinction between malignant and benign cell types may be difficult to discern. MAb probes to classify cell types based onantigen expression are being investigated in numerous laboratories. In one such study, the immunoreactivity of cells obtainedby fine needle aspiration biopsy using MAb B72.3 has recentlybeen evaluated and compared to that of surgically resectedtissues obtained from the same body site. The results obtainedby Johnston et al. (24) were roughly equivalent to those previously published for surgically resected tissues and cytologypreparations. MAb B72.3 reacted with adenocarcinoma cells inthe vast majority of aspiration biopsies containing adenocarci-nomas of the breast and colon (including those with adeno-squamous features) (Table 5). In contrast, small cell carcinomasof the lung, melanomas, lymphomas, and sarcomas were notstained with MAb B72.3. Benign lesions from the breast, lung,and pancreas showed no immunoreactivity with the exceptionof apocrine metaplasia in one breast specimen (Table 5). In 62of 66 patients the reactivity of cells of fine needle aspirationbiopsy was predictive of the surgically resected tissue reactivity.It was concluded from this study that MAb B72.3 may serve asan adjunctive tool for the diagnosis and histological typing ofmalignant cells in fine needle aspiration biopsy specimens.
Diagnostic Distinctions. Diagnostic distinctions among malignancies are at times quite difficult to make and may have anenormous impact on treatment modalities and prognoses. Forexample, the diagnostic distinction between malignant meso-thelioma and adenocarcinoma of the lung is very complex andclassically involves observations by light microscopy, ultrastructural findings by electron microscopy, and a thorough surgicaland radiological assessment. This diagnostic "dilemma" is crit
ical not only because of the current litigious investigationsrelated to occupational asbestos exposure but also because oftherapeutic and prognostic implications for the patient. Immunohistochemical studies to differentiate the two tumor typeshave been hampered by lack of specificity of various polyclonalantisera to CEA and to keratin. As suggested by the previouslydescribed cytology studies where MAb B72.3 was reactive with
Fig. 3. Flow cytometric analysis of anti-CEA MAb binding to the surface of WiDr-51colon carcinoma cells. , sorting pattern inthe absence of primary antibody, i.e., negativecontrol. A, MAb COL 1; B, Mab COL 6; C,MAb COL 15. See Ref. 12 for details.
0 20 40 60 80 100 120 140 160 1. 20 40 60 80 100 120 140 160 ISO
IMMUNOFLUORESCENCE
20 40 60 80 100 120 140 160 180 200
3228
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
Table 4 Reactivity ofMAb B72.3 to formalin fixed paraffin embeddedserous effusions
Specimensreactive/no, tested
Type ofeffusionBenign"Lymphoma-leukemiaBreast
carcinomaOvarianadenocarcinomaLungAdenocarcinomaAdenosquamous
carcinomaSmallcellcarcinomaPoorlydifferentiatedsquamouscell
carcinomaWelldifferentiatedsquamouscellcarcinomaTumor
cellsNA0/922/2328/2819/191/10/32/20/2Mesothelium0/410/90/230/190/190/10/30/20/2
°From patients without cancer (n = 24), and patients with prior or extantcancer in other body sites (n = 17). See Ref. 21 for details.
Table 5 Reactivity affine needle aspiration biopsies with MAb B72.3
No. antigenTissuetypeLungBenign
lesionsAdenocarcinomaSquamous
carcinomaLargecellcarcinomaSmallcellcarcinomaCarcinoidBreastBenign
lesionsAdenocarcinomaColonAdenocarcinomaPancreasBenignAdenocarcinomaMelanomaLymphomaSarcomaNo.
tested102731136110216181322positive02725700I«17605000
" Confined to apocrine metaplasia. See Ref. 24 for details.
adenocarcinoma and nonreactive with mesothelial cells, TAG-72 antigen expression was evaluated via MAb B72.3 immuno-histochemical assays with these two tumor types. Szpak et al.(25) reacted MAb B72.3 with both malignant mesotheliomas(diagnosed according to strict pathological criteria) and ade-nocarcinornas of the lung using avidin-biotin complex inimunohistochemical techniques and formalin fixed, paraffin embedded tissues. No expression of the TAG-72 antigen wasdetectable in 10 of 19 mesotheliomas, while < 1% of tumor cellswere focally immunoreactive in the remaining 8 cases. Conversely, 19 of 22 adenocarcinomas of the lung demonstrated atleast 10% of the malignant cells to be reactive with MAb B72.3.Thus, the presence of TAG-72 was significant in distinguishingmalignant mesothelioma from adenocarcinoma (P < 0.0001).Recent studies have also demonstrated that MAb B72.3 isextremely useful in the differential diagnosis of small cell versusnon-small cell carcinoma of the lung.4
Prognostic Studies
One future prospect concerns the use of a series of monoclonal antibodies to assay tissue sections of carcinoma from anindividual patient to help define the likelihood of metastasis ofthat tumor. There is a large body of evidence supporting thehypothesis that less differentiated tumor cells are more likely
to metastasize. At this time, however, the degree of differentiation of a tumor is for the most part determined on the basis ofmorphological criteria such as nuclear and histológica! grade,with estrogen receptor status showing some minor prognosticindication for breast carcinoma. It would appear, however, thatmore subtle changes in levels of individual proteins, or theglycoprotein determinants (i.e., degree or type of glycosylationof individual proteins), would eventually provide a more accurate assessment as to the degree of (or lack of) differentiationof cells within a given tumor mass. The monoclonal antibodieseventually used in this situation may be directed against (a)tumor associated antigens, (b) oncogene or protooncogeneproducts, (c) differentiation antigens, (d) proteins associatedwith the metastatic process (such as laminin receptor or typeIV collagenase), or (e) normal cellular proteins or glycoproteinsthat are increased or decreased in levels during the processes ofdedifferentiation and early disease progression.
One example of the direction of this research is the recentfinding that the expression of the determinant defined by monoclonal antibody DF3 (Table 1) has been shown to correlate withnuclear grade, histológica! grade, and estrogen receptor statusamong breast carcinomas but is an independent marker ofdifferentiation (26, 27). Since monoclonal antibody DF3 alsoreacts strongly with lactating mammary epithelial cells, it canbe hypothesized at this point to be reactive with a novel differentiation determinant.
Another area of investigation concerns the use of MAbs tospecific oncogene and protooncogene translational products.For example, with the use of immunohistochemical and RIAassays using MAbs to ras p21 (see Ref. 28 for review), thefollowing have recently been shown, (a) Certain inflammatorybowel disease tissues demonstrate less ras p21 expression thanadjacent carcinoma (29). (¿>)Increased ras p21 expression isprogressively increased in breast lesions as follows: nonatypicalhyperplasia, atypical hyperplasia, carcinoma in situ, and carcinoma, respectively.5 (e) ras p21 expression generally correlates
with nuclear anaplasia of prostatic cancer and is inverselyrelated to the degree of glandular differentiation (30). (d) Increased ras p21 expression has been observed in dysplastic andin situ bladder lesions and in high grade bladder carcinoma(31).
These and other studies, however, seem to be pointing outseveral important concepts concerning the role of oncogenes orprotooncogenes in carcinoma pathogenesis. For example, as inthe case of the ras family, less than 10% and, more likely, lessthan 5% of various carcinoma lesions contain the point mutatedras oncogene (32-48), enhanced ras p21 expression is observed
in approximately 50% of several types of carcinomas, andenhanced ras p21 expression does not seem to be necessary forthe maintenance of the transformed phenotype; i.e., many metastatic lesions do not contain enhanced ras p21 (29,49). Unlikeexperiments involving selected cell lines, many experimentsinvolving human carcinoma biopsy material thus point to thefollowing concept: if a given oncogene or protooncogene product is involved in the pathogenesis of a given carcinoma, it isbut one factor of many in a multistep process, perhaps actingmore like a "progressor gene" than an "oncogene."
Antigenic Heterogeneity and Modulation within Human Carcinoma Cell Populations
Heterogeneity among tumor cells within carcinoma massesmust have been noticed by those who were among the first to
4 W. W. Johnston et al., personal communication. 9 N. Ohuchi el al., accepted for publication.
3229
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
use microscopic techniques to examine such specimens. In1954, Foulds (50) formally documented the existence of distinctmorphologies in different areas of a single mammary tumor.Using a variety of methods and polyclonal antisera, antigenicheterogeneity has been well documented for various carcinomacell populations. Monoclonal antibodies have now been used todefine the extent of antigenic heterogeneity and modulation ofspecific TAAs that exists among human carcinomas as well aswithin a given carcinomatous mass, to determine some of theparameters that mediate the expression of various antigenicphenotypes, and to develop model systems in which to study,and perhaps eventually control, these phenomena.
Numerous studies have revealed a wide range of antigenicphenotypes present in carcinoma masses. For example, when39 different infiltrating ductal carcinomas were reacted with 4MAbs, 10 antigenic phenotypes emerged, ranging from thosethat express all 4 antigens to those that express none (51).
Phenotypic variation also has been observed in the expressionof TAAs within a given tumor. One pattern sometimes observedis that one area of a tumor contained cells with TAAs reactivewith a particular MAb, whereas another area of that tumorcontained cells that were unreactive with the identical antibody.A more common type of antigenic heterogeneity can be termed"patchwork," in which tumor cells that express a specific TAA
are observed directly adjacent to tumor cells negative for thesame antigen. Patterns of reactivity with a specific MAb alsowere observed to vary within a given tumor mass; i.e., antigenwas detected in the cytoplasm of cells in one part of the tumormass and on the luminal edge of differentiated structures in adifferent part of the same mass (51 ).
To elucidate the phenomenon of antigenic heterogeneity inhuman carcinomas, investigators have examined model systems. Using fluorescence activated cell sorter analyses, it hasbeen shown that one MAb is most reactive with the surface ofMCF-7 breast tumor cells during S phase of the cell cycle (52).This relatively frequent modulation of a TAA may partly explain the immunohistochemical observations of TAA positivecells adjacent to TAA negative cells for at least some MAbs.Studies have also demonstrated that change in antigenic phe-notype occurs during extended passage of cells in culture (51).Indeed, using MCF-7 mammary tumor cell lines obtained fromfour sources and three MAbs, four discrete antigenic phenotypes emerged for the four MCF-7 cell lines (51). This observation should serve as a caveat to investigators using establishedcell lines in their studies and attempting to correlate their resultswith those of other laboratories. Indeed, one may wish toconsider avoiding carcinoma cell lines as sources of immuno-gens and as test antigens in most steps of MAb generation andcharacterization.
Horan Hand et al. (51 ) further defined the extent of antigenicmodulation of human mammary tumor cell populations, viathe temporal analyses of cloned MCF-7 mammary tumor cellpopulations. Although some of the MCF-7 clones maintaineda stable antigenic phenotype throughout the observation period,a dramatic change in antigenic phenotype, i.e., antigenic modulation, was observed in others.
Environmental milieu and the three dimensional configuration of tumor masses have also been shown to play a role inmodulating tumor antigen expression. A recent study by Friedman et al. (53) demonstrated that TAG-72 cell surface antigenlevels are diminished within days when primary colon carcinomas are placed in cell culture, while CEA levels remain constant. A pronounced increase in TAG-72 expression was observed, moreover, when the LS-174T colon cancer cells were
grown under culture conditions which promote three dimensional growth (54). LS-174T cells grown in spheroid or suspension cultures demonstrated a 2- to 7-fold increase in TAG-72antigen expression, while those grown on agar plugs demonstrated a 10-fold increase. When the LS-174T cell line wasinjected into athymic mice to generate tumors, the level ofTAG-72 antigen increased over 100-fold, to levels comparableto those seen in tumor masses from patients. These latter twostudies (53, 54) help to explain the phenomenon in which theTAG-72 determinant is absent in virtually all carcinoma celllines examined but is present in the vast majority of carcinomabiopsies.
Thus, the variability of expression of TAAs, via either antigenic heterogeneity or antigenic modulation, presents a potential problem in the development and optimization of immuno-diagnostic and/or immunotherapeutic procedures for carcinomas. Means to confront these issues will be addressed below.
Serum Assays
Some of the major potential uses of MAbs will be their abilityto detect specific carcinoma associated antigens in sera ofasymptomatic individuals and to indicate the presence of occultmetastatic lesions in patients whose primary carcinoma hasbeen previously excised. Monoclonal antibody 19-9 (see Table1) has been evaluated recently in longitudinal studies ofhundreds of colorectal cancer patients; recurrence was preceded,by 3 to 18 months, by the persistence or rise in antigen levels(55). This suggests that the MAb 19-9 assay may be a valuableprognostic aid for making therapeutic decisions and for appropriately stratifying patients for clinical trials. MAb 19-9 is alsobeing evaluated for its use as a diagnostic test for gastrointestinal cancer as well as for other solid tumors (56-58); the bloodsof 79% of pancreatic cancer patients, 49% of hepatoma patients,and 50 to 57% of gastric and other gastrointestinal cancerpatients have given positive levels (>37 units/ml), whereas 1.5to 3% of patients with benign lesions and 0.5% (17 of 3500) ofapparently normal patients scored positive.
A competition RIA was developed using MAb DU-PAN-2to detect reactive antigen in sera of pancreatic cancer patients(59). A recent study demonstrated that this assay detects antigenin 89% of such patients. MAb OC125 (see Table 1) is reactivewith most nonmucinous epithelial ovarian tumors, and an assayhas been developed to detect the reactive antigen in serum. One% of 888 apparently healthy persons and 6% of 143 patientswith nonmalignant disease had serum levels above 35 units/ml.In contrast, 83 of 101 patients (82%) with surgically demonstrated ovarian carcinoma had elevated levels of antigen. Moreover, rising or falling antigen levels correlated with progressionof disease in 42 of 45 instances (60). Determination of antigenlevels as monitored by MAb OC 125 thus may aid in monitoringthe response to treatment in patients with ovarian cancer.
The most extensively used immunoassay to monitor carcinoma patients has been that detecting serum levels of CEA. Aspreviously discussed, much controversy has existed over theyears as to whether CEA represents one molecule or a familyof molecules, since the results from different laboratories oftenhave been inconsistent. Numerous groups have developedMAbs to CEA, and many of these have recently been comparedfor use in serum assays by Herlyn et al. (11). Six antibodieswere used in double determinant RIAs to detect CEA and CEA-related antigens in sera of 311 patients with various gastrointestinal diseases as well as in sera of normal donors. Between1.4 and 4.4% of sera from patients with inflammatory and
3230
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
ANTIBODY CHARACTERIZATION
1) Solid Phase Radioimmunoassay2) Immunohistochemistry3) Live Cell Radioimmunoassay
\FRAGMENTATION
USDS-PAGE
2) CompetitionRadioimmunoassay
ANTIBODY RADIOLABELING
11SDS-PAGE - Autoradiography
21 Solid Phase Radioimmunoassay
IN VIVO ANALYSIS MODELS
1) Biodistribution2) Clearance3) Scanning
\RADIOIMMUNOLOCALIZATION
-CLINICAL TRIALSl ) Biodistribution2) Clearance3) Scanning
RADIOIMMUNOTHERAPY- MODEL SYSTEMS
1) Tumor Growth21 Toxicity
\ ZRADIOIMMUNOTHERAPY
-CLINICAL TRIALS
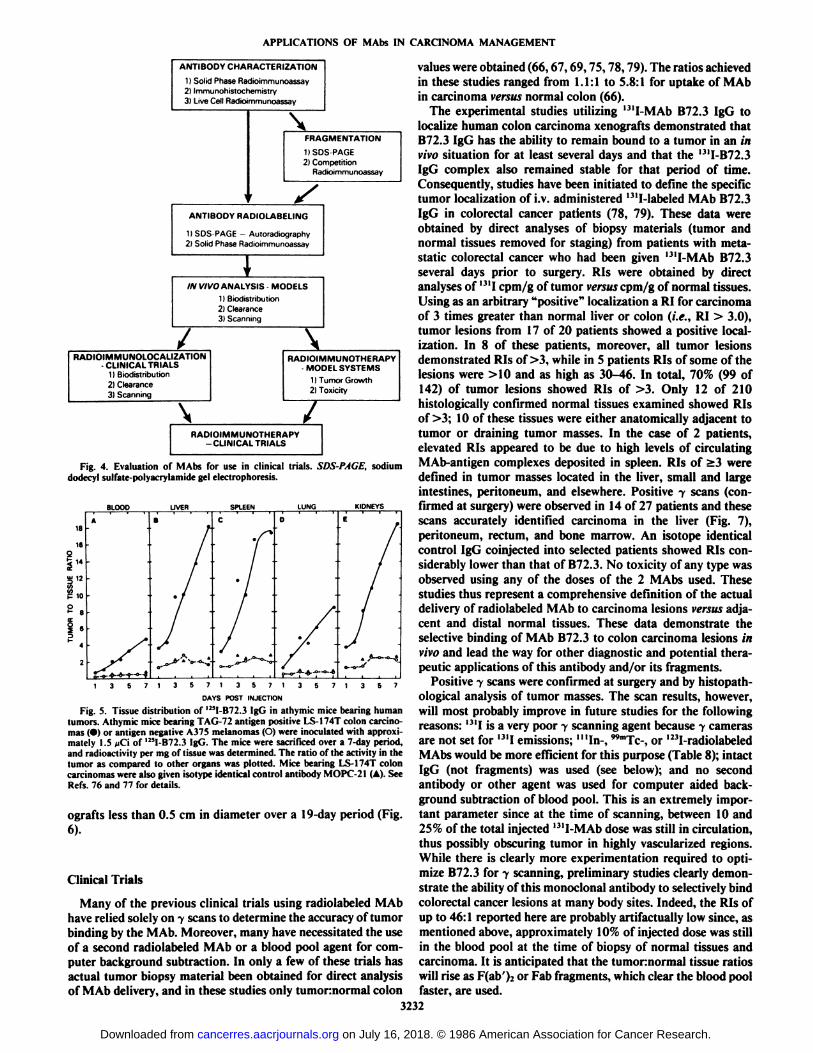
Fig. 4. Evaluation of MAbs for use in clinical trials. SDS-PAGE, sodiumdodecyl sulfate-polyacrylamide gel electrophoresis.
13571357136713571357
DAYS POST INJECTION
Fig. 5. Tissue distribution of '"I-B72.3 IgG in athymic mice bearing humantumors. Athymic mice bearing TAG-72 antigen positive LS-174T colon carcinomas (•)or antigen negative A37S melanomas (O) were inoculated with approximately 1.5 iiC\ of '"I-B72.3 IgG. The mice were sacrificed over a 7-day period,and radioactivity per mg of tissue was determined. The ratio of the activity in thetumor as compared to other organs was plotted. Mice bearing LS-174T coloncarcinomas were also given isotype identical control antibody MOPC-21 (A). SeeRefs. 76 and 77 for details.
ografts less than 0.5 cm in diameter over a 19-day period (Fig.
6).
Clinical Trials
Many of the previous clinical trials using radiolabeled MAbhave relied solely on y scans to determine the accuracy of tumorbinding by the MAb. Moreover, many have necessitated the useof a second radiolabeled MAb or a blood pool agent for computer background subtraction. In only a few of these trials hasactual tumor biopsy material been obtained for direct analysisof MAb delivery, and in these studies only tumornormal colon
values were obtained (66,67,69,75,78,79). The ratios achievedin these studies ranged from 1.1:1 to 5.8:1 for uptake of MAbin carcinoma versus normal colon (66).
The experimental studies utilizing l3'I-MAb B72.3 IgG to
localize human colon carcinoma xenografts demonstrated thatB72.3 IgG has the ability to remain bound to a tumor in an invivo situation for at least several days and that the I3II-B72.3
IgG complex also remained stable for that period of time.Consequently, studies have been initiated to define the specifictumor localization of i.v. administered 13ll-labeled MAb B72.3
IgG in colorectal cancer patients (78, 79). These data wereobtained by direct analyses of biopsy materials (tumor andnormal tissues removed for staging) from patients with metastatic colorectal cancer who had been given 13lI-MAb B72.3
several days prior to surgery. RIs were obtained by directanalyses of I31Icpm/g of tumor vm«scpm/g of normal tissues.Using as an arbitrary "positive" localization a RI for carcinoma
of 3 times greater than normal liver or colon (i.e., RI > 3.0),tumor lesions from 17 of 20 patients showed a positive localization. In 8 of these patients, moreover, all tumor lesionsdemonstrated RIs of >3, while in 5 patients RIs of some of thelesions were >10 and as high as 30-46. In total, 70% (99 of142) of tumor lesions showed RIs of >3. Only 12 of 210histologically confirmed normal tissues examined showed RIsof >3; 10 of these tissues were either anatomically adjacent totumor or draining tumor masses. In the case of 2 patients,elevated RIs appeared to be due to high levels of circulatingMAb-antigen complexes deposited in spleen. RIs of >3 weredefined in tumor masses located in the liver, small and largeintestines, peritoneum, and elsewhere. Positive y scans (confirmed at surgery) were observed in 14 of 27 patients and thesescans accurately identified carcinoma in the liver (Fig. 7),peritoneum, rectum, and bone marrow. An isotope identicalcontrol IgG coinjected into selected patients showed RIs considerably lower than that of B72.3. No toxicity of any type wasobserved using any of the doses of the 2 MAbs used. Thesestudies thus represent a comprehensive definition of the actualdelivery of radiolabeled MAb to carcinoma lesions versus adjacent and distal normal tissues. These data demonstrate theselective binding of MAb B72.3 to colon carcinoma lesions invivo and lead the way for other diagnostic and potential therapeutic applications of this antibody and/or its fragments.
Positive 7 scans were confirmed at surgery and by histopath-ological analysis of tumor masses. The scan results, however,will most probably improve in future studies for the followingreasons: I31Iis a very poor y scanning agent because y camerasare not set for 13IIemissions; "'In-, "Tc-, or I23l-radiolabeled
MAbs would be more efficient for this purpose (Table 8); intactIgG (not fragments) was used (see below); and no secondantibody or other agent was used for computer aided background subtraction of blood pool. This is an extremely important parameter since at the time of scanning, between 10 and25% of the total injected 13lI-MAb dose was still in circulation,
thus possibly obscuring tumor in highly vascularized regions.While there is clearly more experimentation required to optimize B72.3 for y scanning, preliminary studies clearly demonstrate the ability of this monoclonal antibody to selectively bindcolorectal cancer lesions at many body sites. Indeed, the RIs ofup to 46:1 reported here are probably art ¡factuallylow since, asmentioned above, approximately 10% of injected dose was stillin the blood pool at the time of biopsy of normal tissues andcarcinoma. It is anticipated that the tumonnormal tissue ratioswill rise as F(ab' ).-.or Fab fragments, which clear the blood pool
faster, are used.3232
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
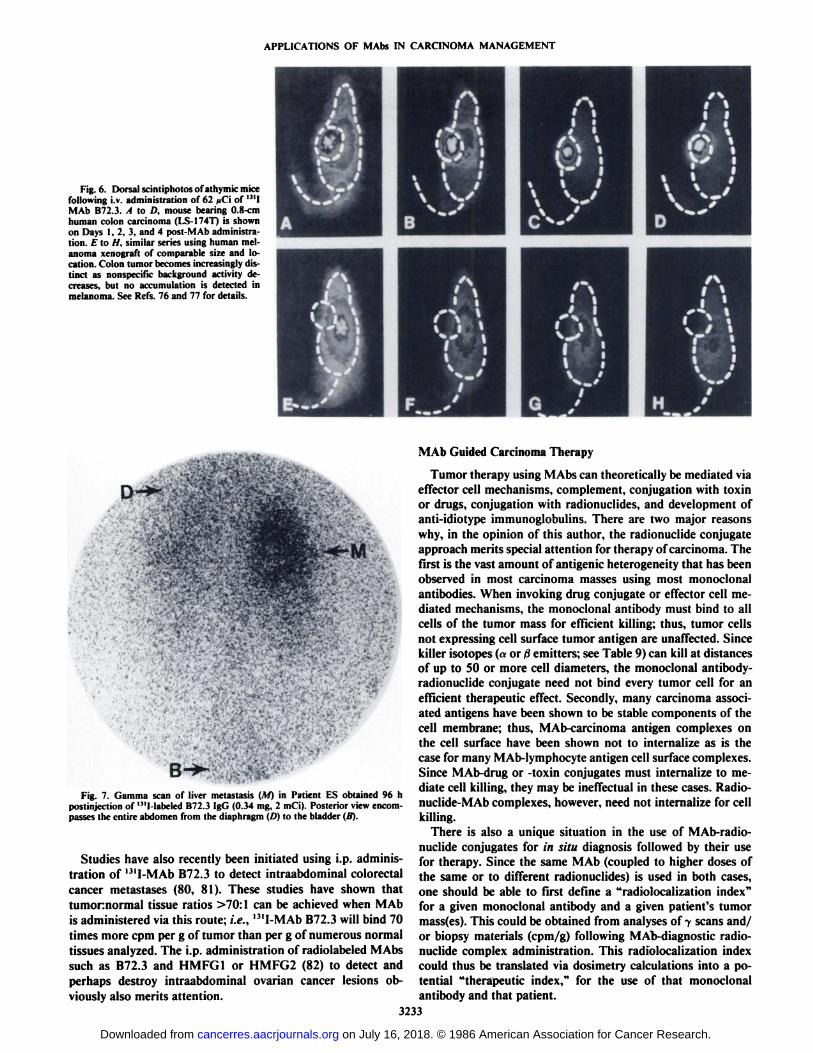
Fig. 6. Dorsal scintiphotos of athymic micefollowing i.v. administration of 62 /iCi of ' "IMAb B72.3. A to D, mouse bearing 0.8-cmhuman colon carcinoma (LS-I74T) is shownon Days 1, 2, 3, and 4 post-MAb administration. E to //, similar series using human melanoma xenograft of comparable size and location. Colon tumor becomes increasingly distinct as nonspecific background activity decreases, but no accumulation is detected inmelanoma. See Refs. 76 and 77 for details.
sas
Fig. 7. Gamma scan of liver metastasis (A/) in Patient ES obtained 96 hpostinjection of '"l-labeled B72.3 IgG (0.34 mg, 2 mCi). Posterior view encompasses the entire abdomen from the diaphragm (D) to the bladder (/?).
Studies have also recently been initiated using i.p. administration of '"I-MAb B72.3 to detect intraabdominal colorectal
cancer métastases(80, 81). These studies have shown thattumornormal tissue ratios >70:1 can be achieved when MAbis administered via this route; i.e., l3'I-MAb B72.3 will bind 70
times more cpm per g of tumor than per g of numerous normaltissues analyzed. The i.p. administration of radiolabeled MAbssuch as B72.3 and HMFG1 or HMFG2 (82) to detect andperhaps destroy intraabdominal ovarian cancer lesions obviously also merits attention.
MAb Guided Carcinoma Therapy
Tumor therapy using MAbs can theoretically be mediated viaeffector cell mechanisms, complement, conjugation with toxinor drugs, conjugation with radionuclides, and development ofanti-idiotype immunoglobulins. There are two major reasons
why, in the opinion of this author, the radionuclide conjugateapproach merits special attention for therapy of carcinoma. Thefirst is the vast amount of antigenic heterogeneity that has beenobserved in most carcinoma masses using most monoclonalantibodies. When invoking drug conjugate or effector cell mediated mechanisms, the monoclonal antibody must bind to allcells of the tumor mass for efficient killing; thus, tumor cellsnot expressing cell surface tumor antigen are unaffected. Sincekiller isotopes (a or ßemitters; see Table 9) can kill at distancesof up to 50 or more cell diameters, the monoclonal antibody-radionuclide conjugate need not bind every tumor cell for anefficient therapeutic effect. Secondly, many carcinoma associated antigens have been shown to be stable components of thecell membrane; thus, MAb-carcinoma antigen complexes onthe cell surface have been shown not to internalize as is thecase for many MAb-lymphocyte antigen cell surface complexes.Since MAb-drug or -toxin conjugates must internalize to mediate cell killing, they may be ineffectual in these cases. Radio-nuclide-MAb complexes, however, need not internalize for cellkilling.
There is also a unique situation in the use of MAb-radio-nuclide conjugates for in situ diagnosis followed by their usefor therapy. Since the same MAb (coupled to higher doses ofthe same or to different radionuclides) is used in both cases,one should be able to first define a "radiolocalization index"for a given monoclonal antibody and a given patient's tumor
mass(es). This could be obtained from analyses of 7 scans and/or biopsy materials (cpm/g) following MAb-diagnostic radionuclide complex administration. This radiolocalization indexcould thus be translated via dosimetry calculations into a potential "therapeutic index," for the use of that monoclonal
antibody and that patient.3233
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
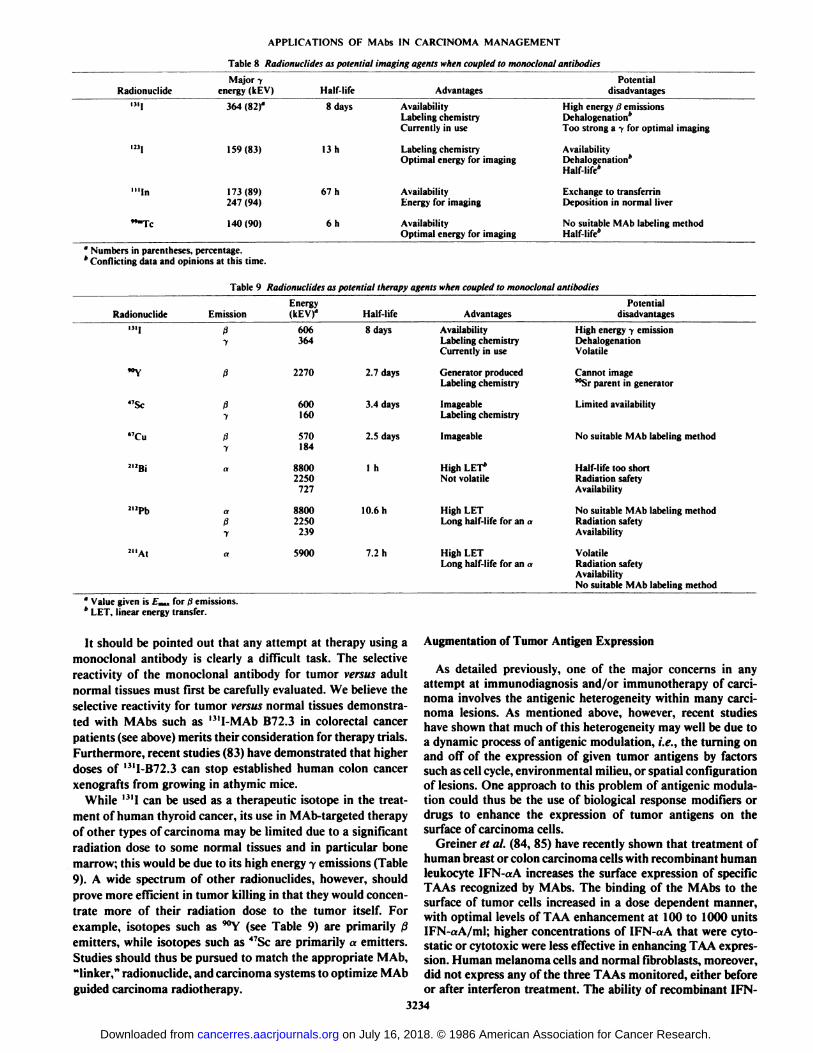
Table 8 Radionuclides as potential imaging agents when coupled to monoclonal antibodies
RadionuclideDi]m,'"InTeMajory
energy(kEV)364(82)°159(83)173(89)
247(94)140(90)Half-life8
days13
h67
h6hAdvantagesAvailability
Labeling chemistryCurrently inuseLabeling
chemistryOptimal energy forimagingAvailability
Energy forimagingAvailability
Optimal energy for imagingPotential
disadvantagesHigh
energy .; emissionsDehalogenation*
Too strong a y for optimalimagingAvailability
Dehalogenation*Half-life*Exchange
to transferrinDeposition in normalliverNo
suitable MAb labeling methodHalf-life*
* Numbers in parentheses, percentage.* Conflicting data and opinions at this time.
Table 9 Radionuclides as potential therapy agents when coupled to monoclonal antibodies
RadionuclideDI,"Y47Sc"Cu21JBi212PbEmissionß
1ßß
7ß
yaaßyEnergy
(kEVf606
3642270600
160570
1848800
22507278800
2250239Half-life8
days2.7
days3.4
days2.5
days1
h10.6hAdvantagesAvailability
Labeling chemistryCurrently inuseGenerator
producedLabelingchemistryImageable
LabelingchemistryImageableHigh
LET*
NotvolatileHigh
LETLong half-life for an aPotential
disadvantagesHighenergy -. emission
DehalogenationVolatileCannot
image""Sr parent ingeneratorLimited
availabilityNo
suitable MAb labelingmethodHalf-life
too shortRadiation safetyAvailabilityNo
suitable MAb labeling methodRadiation safetyAvailability
At 5900 7.2 h High LETLong half-life for an a
VolatileRadiation safetyAvailabilityNo suitable MAb labeling method
" Value given is /„„,for .; emissions.* LET, linear energy transfer.
It should be pointed out that any attempt at therapy using a Augmentation of Tumor Antigen Expressionmonoclonal antibody is clearly a difficult task. The selectivereactivity of the monoclonal antibody for tumor versus adultnormal tissues must first be carefully evaluated. We believe theselective reactivity for tumor versus normal tissues demonstrated with MAbs such as "'I-MAb B72.3 in colorectal cancer
patients (see above) merits their consideration for therapy trials.Furthermore, recent studies (83) have demonstrated that higherdoses of '-"I-B72.3 can stop established human colon cancer
xenografts from growing in athymic mice.While '•"!can be used as a therapeutic isotope in the treat
ment of human thyroid cancer, its use in MAb-targeted therapy
of other types of carcinoma may be limited due to a significantradiation dose to some normal tissues and in particular bonemarrow; this would be due to its high energy y emissions (Table9). A wide spectrum of other radionuclides, however, shouldprove more efficient in tumor killing in that they would concentrate more of their radiation dose to the tumor itself. Forexample, isotopes such as '"Y (see Table 9) are primarily ßemitters, while isotopes such as 47Sc are primarily a emitters.
Studies should thus be pursued to match the appropriate MAb,"linker," radionuclide, and carcinoma systems to optimize MAb
guided carcinoma radiotherapy.
As detailed previously, one of the major concerns in anyattempt at immunodiagnosis and/or immunotherapy of carcinoma involves the antigenic heterogeneity within many carcinoma lesions. As mentioned above, however, recent studieshave shown that much of this heterogeneity may well be due toa dynamic process of antigenic modulation, i.e., the turning onand off of the expression of given tumor antigens by factorssuch as cell cycle, environmental milieu, or spatial configurationof lesions. One approach to this problem of antigenic modulation could thus be the use of biological response modifiers ordrugs to enhance the expression of tumor antigens on thesurface of carcinoma cells.
Greiner et al. (84, 85) have recently shown that treatment ofhuman breast or colon carcinoma cells with recombinant humanleukocyte IFN-aA increases the surface expression of specificTAAs recognized by MAbs. The binding of the MAbs to thesurface of tumor cells increased in a dose dependent manner,with optimal levels of TAA enhancement at 100 to 1000 unitsIFN-aA/ml; higher concentrations of IFN-aA that were cyto-static or cytotoxic were less effective in enhancing TAA expression. Human melanoma cells and normal fibroblasts, moreover,did not express any of the three TAAs monitored, either beforeor after interferon treatment. The ability of recombinant IFN-
3234
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
«Ato increase the expression of TAAs on human carcinomacells showed temporal dependency, with optimal enhancementoccurring after 16 to 24 h. The enhancement of specific TAAsat the surface of the carcinoma cells by IFN-aA was also
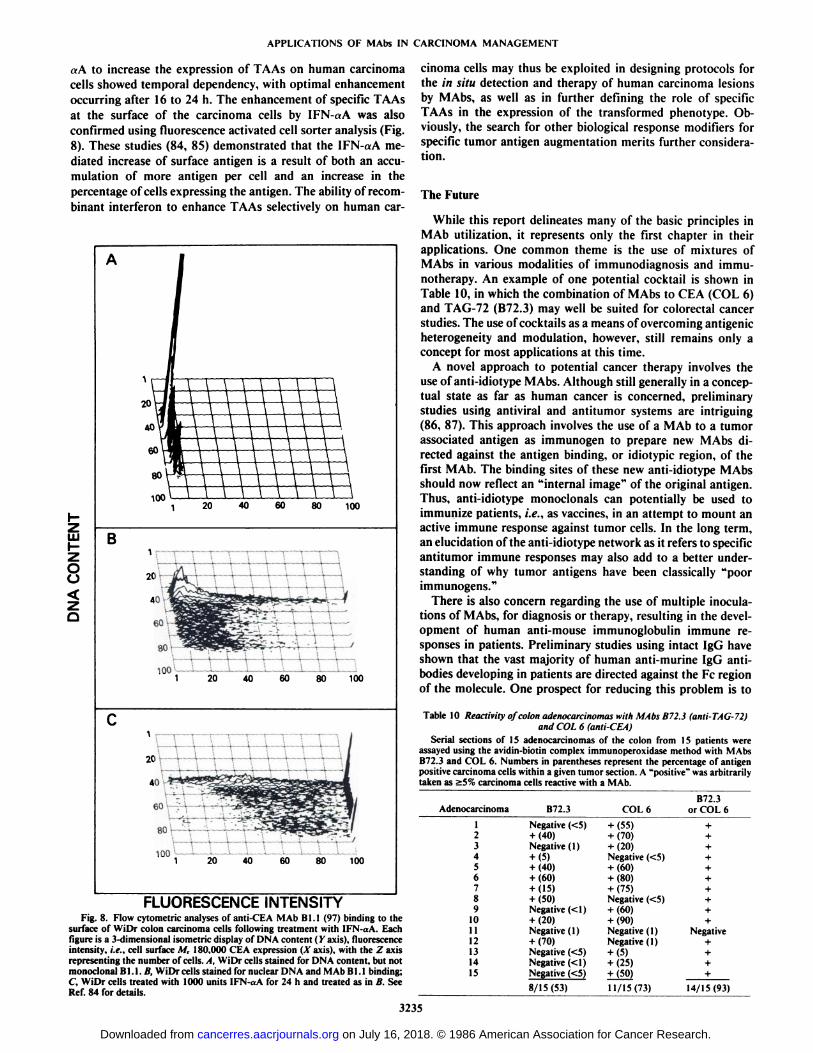
confirmed using fluorescence activated cell sorter analysis (Fig.8). These studies (84, 85) demonstrated that the IFN-aA me
diated increase of surface antigen is a result of both an accumulation of more antigen per cell and an increase in thepercentage of cells expressing the antigen. The ability of recombinant interferon to enhance TAAs selectively on human car-
UI
OO
B
20 40 60 80 100
100 '
FLUORESCENCE INTENSITYFig. 8. Flow cytometric analyses of anti-CEA MAb BI.I (97) binding to the
surface of WiDr colon carcinoma cells following treatment with IFN-aA. Eachfigure is a 3-dimensional isometric display of DNA content ( Y axis), fluorescenceintensity, i.e., cell surface M, 180,000 CEA expression (A"axis), with the Z axis
representing the number of cells. A, WiDr cells stained for DNA content, but notmonoclonal B1.1. B, WiDr cells stained for nuclear DNA and MAb Bl. l binding;C, WiDr cells treated with 1000 units IFN-aA for 24 h and treated as in B. SeeRef. 84 for details.
cinoma cells may thus be exploited in designing protocols forthe in situ detection and therapy of human carcinoma lesionsby MAbs, as well as in further defining the role of specificTAAs in the expression of the transformed phenotype. Obviously, the search for other biological response modifiers forspecific tumor antigen augmentation merits further consideration.
The Future
While this report delineates many of the basic principles inMAb utilization, it represents only the first chapter in theirapplications. One common theme is the use of mixtures ofMAbs in various modalities of immunodiagnosis and immu-notherapy. An example of one potential cocktail is shown inTable 10, in which the combination of MAbs to CEA (COL 6)and TAG-72 (B72.3) may well be suited for colorectal cancerstudies. The use of cocktails as a means of overcoming antigenicheterogeneity and modulation, however, still remains only aconcept for most applications at this time.
A novel approach to potential cancer therapy involves theuse of anti-idiotype MAbs. Although still generally in a conceptual state as far as human cancer is concerned, preliminarystudies usirtg antiviral and antitumor systems are intriguing(86, 87). This approach involves the use of a MAb to a tumorassociated antigen as immunogen to prepare new MAbs directed against the antigen binding, or idiotypic region, of thefirst MAb. The binding sites of these new anti-idiotype MAbsshould now reflect an "internal image" of the original antigen.
Thus, anti-idiotype monoclonals can potentially be used toimmunize patients, i.e., as vaccines, in an attempt to mount anactive immune response against tumor cells. In the long term,an elucidation of the anti-idiotype network as it refers to specificantitumor immune responses may also add to a better understanding of why tumor antigens have been classically "poorimmunogens."
There is also concern regarding the use of multiple inoculations of MAbs, for diagnosis or therapy, resulting in the development of human anti-mouse immunoglobulin immune responses in patients. Preliminary studies using intact IgG haveshown that the vast majority of human anti-murine IgG antibodies developing in patients are directed against the Fc regionof the molecule. One prospect for reducing this problem is to
Table 10 Reactivity of colon adenocarcinomas with MAbs B72.3 (anti-TAG-72)and COL 6 (anti-CEA)
Serial sections of 15 adenocarcinomas of the colon from 15 patients wereassayed using the avidin-biotin complex immunoperoxidase method with MAbsB72.3 and COL 6. Numbers in parentheses represent the percentage of antigenpositive carcinoma cells within a given tumor section. A "positive" was arbitrarily
taken as 25% carcinoma cells reactive with a MAb.
Adenocarcinoma123456789101112131415B72.3Negative
(<5)+(40)Negative(1)+(5)+(40)+(60)+(15)+(50)Negative(<1)+(20)Negative
( 1)+(70)Negative(<5)Negative(<1)Negative(<5)8/15(53)COL
6+
(55)+(70)+(20)Negative(<5)+(60)+(80)+(75)Negative(<5)+(60)+(90)Negative
( 1)Negative(1)+(5)+(25)+(50)11/15(73)B72.3
or COL6++++++++++Negative++++14/15(93)
3235
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
fractionate MAbs to very small fragments to obtain the minimum antigen binding component available. This would mostprobably eliminate the more immunogenic constant regions onthe immunoglobulin molecule. Another approach would be toclone the genes coding for individual MAbs, reduce them insize via restriction endonuclease methodology and, if necessary,insert or lÃgatehuman immunoglobulin constant regions. Suchrecombinant chimeric molecules have already been generated.Their efficiency of binding, affinity, and avidity, however, hasnot yet been demonstrated in any antitumor systems. A spin-off of this technology would also be the ligation of efficientmetal binding or drug binding regions to recombinant immunoglobulin molecules. Thus, recombinant DNA technology willbe most likely to play a larger role in MAb research anddevelopment. Thus, while several potential obstacles have beenclearly defined, the utility of MAbs in numerous aspects of themanagement of carcinoma patients now appears much closerto realization.
Acknowledgments
I wish to thank the Rosenthal Award Subcommittee of the AmericanAssociation for Cancer Research Awards Committee, and Dr. and Mrs.Rosenthal for the honor of receiving the Ninth Rosenthal FoundationAward. I also wish to thank the following present and previous membersof my Laboratory, A. Caruso, D. Colcher, J. Esteban, J. Greiner, P.Hand, V. Johnson, R. Muraro, M. Nuti, N. Ohuchi, A. Paterson, D.Salomon, A. Thor, M. Weeks, and D. Wunderlich; and our collaborators, J. Carrasquillo, R. Cunningham, P. B. Fisher, E. Friedman, F.Gorstein, M. Herlyn, W. Johnston, A. Keenan, H. Koprowski, D. Kufe,S. Larson, J. L. Magnani, S. E. Martin, P. Noguchi, S. Pestka, H.Sears, Z. Steplewski, P. Sugarbaker, C. Szpak, and M. Viola, for theiroutstanding contributions to many of the studies outlined in thismanuscript.
References
1. Kohler, M., and Milstein. C. Continuous cultures of fused cells secretingantibody of predefined specificity. Nature (Lond.), 256:494-497, 1975.
2. Schlom. J., and Weeks, M. O. Potential clinical utility of monoclonalantibodies in the management of human carcinomas. In: V. J. DeVita, Jr.,S. Hellman, and S. A. Rosenberg (eds.). Important Advances in Oncology1985, pp. 170-192. Philadelphia: J. B. Lippincott. 1985.
3. Colcher. D., Horan Hand. P., Nuti. M.. and Schlom, J. A spectrum ofmonoclonal antibodies reactive with mammary tumor cells. Proc. Nati. Acad.Sci. USA, 78: 3199-3203, 1981.
4. Johnson. V., Schlom, J., Paterson, A. J., Bennett. J., Magnani, J. L., andColcher, D. Analysis of a human tumor associated glycoprotein (TAG-72)identified by monoclonal antibody B72.3. Cancer Res., 46: 850-857. 1986.
5. Nuti, M.. Teramoto, Y. A., Mariani-Constantini, R.. Horan Hand. P.,Colcher, D., and Schlom, J. A monoclonal antibody (B72.3) defines patternsof distribution of a novel tumor-associated antigen in human mammarycarcinoma cell populations. Int. J. Cancer, 29: 539-545, 1982.
6. Thor, A., Ohuchi. N., and Schlom, J. Distribution of oncofetal antigentumor-associated glycoprotein-72 defined by monoclonal antibody B72.3.Cancer Res., 46: 3II8-3124, 1986.
7. Stramignoni. D., Bowen, R., Atkinson, B., and Schlom. J. Differentialreactivity of monoclonal antibodies with human colon adenocarcinomas andadenomas. Int. J. Cancer, 31: 543-552, 1983.
8. Thor, A.. Gorstein, F., Ohuchi. N., Szpak, C. A., Johnston, W. W., andSchlom, J. Tumor-associated glycoprotein (TAG-72) in ovarian carcinomasdefined by a monoclonal antibody B72.3. J. Nati. Cancer Inst., in press,1986.
9. Bast. R. C., Feeney, M., Lazarus, H., Nadler, L. M., Colvin, R. B., andKnapp, R. C. Reactivity of a monoclonal antibody with human ovariancarcinoma. J. Clin. Invest., 68: 1331-1337. 1981.
10. Gold. P., and Freedman, S. O. Demonstration of tumor-specific antigens inhuman colonie carcinomata by immunological tolerance and adsorptiontechniques. J. Exp. Med., ¡21.:439-462, 1965.
11. Herlyn, M., Blaszczyk, M., Sears, H. F., Verrill, H., Lindgren, J., Colcher,D., Steplewski, Z., Schlom, J., and Koprowski, H. Detection of a carcinoem-bryonic antigen and related antigens in sera of patients with gastrointestinaltumors using monoclonal antibodies in double determinant radioimmunoas-says. Hybridoma, 2: 329-339, 1983.
12. Muraro, R., Wunderlich, D., Thor, A., Lundy, J., Noguchi, P., Cunningham,R., and Schlom, J. Definition by monoclonal antibodies of a repertoire of
epitopes on carcinoembryonic antigen differentially expressed in humancolon carcinomas versus normal adult tissues. Cancer Res., 45: 5769-5780,1985.
13. Von Kleist, S., Chavanel, G., and Bur tin, P. Identification of an antigen fromnormal human tissue that cross reacts with the carcinoembryonic antigen.Proc. Nati. Acad. Sci. USA, 69: 2492-2494, 1972.
14. Von Kleist, S., and Burliti. P. Antigens cross reacting with CEA. ¡n:R. B.Herberman and K. R. Mclntire (eds.), Immunodiagnosis of Cancer, Vol. 9,Part 1, pp. 322-341. New York: Marcel Dekker, Inc., 1979.
15. Kuroki, M., Koga, Y., and Matsuoka, Y. Purification and characterizationof carcinoembryonic antigen-related antigens in normal adult feces. CancerRes., 41:113-720, 1981.
16. Primus, F. J., Freeman, J. W., and Goldenberg, D. M. Immunologicalheterogeneity of carcinoembryonic. antigen: purification from meconium ofan antigen related to carcinoembryonic antigen. Cancer Res., 43: 679-685,1983.
17. Svenberg, T., l laminarst nini. S., and Hedin, A. Purification and propertiesof biliary glycoprotein l (BGP1). Immunochemical relationship to carcinoembryonic antigen. Mol. Immunol., 16: 245-252, 1979.
18. Primus, F. J., Newell, K. D., Blue, N., and Goldenberg, D. M. Immunologicalheterogeneity of carcinoembryonic antigen: antigenic determinants on carcinoembryonic antigen distinguished by monoclonal antibodies. Cancer Res.,«.•686-692,1983.
19. Kuroki, M., Kuroki, M., Koga, Y., and Matsuoka, Y. Monoclonal antibodiesto carcinoembryonic antigen: a systematic analysis of antibody specificitiesusing related normal antigens and evidence for allotypic determinants oncarcinoembryonic antigen. J. Immunol., 133: 2090-2097, 1984.
20. Primus, F. J., Kuhns, J. K., and Goldenberg, D. M. Immunological heterogeneity of carcinoembryonic antigen determinants in colonie tumors withmonoclonal antibodies. Cancer Res., 43: 693-701, 1983.
21. Johnston, W. W., Szpak, C. A., Lottich, S. C.. Thor, A., and Schlom, J. Useof a monoclonal antibody (B72.3) as an immunocytochemical adjunct todiagnosis of adenocarcinoma in human effusions. Cancer Res., 45: 1894-1900, 1985.
22. Szpak, C. A., Johnston, W. W., Lottich. S. C., Kufe, D., Thor, A., andSchlom, J. Patterns of reactivity of four novel monoclonal antibodies (B72.3,DF3, Bl.l. B6.2) with cells in human malignant and benign effusions: ahighly selective recognition of adenocarcinoma over other neoplasms andmesothelium. Acta Cytol., 28: 356-367, 1984.
23. Martin, S. E., Moshiri, S., Thor, A., and Schlom, J. Identification ofadenocarcinoma in cytospin preparations of effusions using monoclonalantibody B72.3. Am. J. Clin. Pathol., in press, 1986.
24. Johnston, W. W., Szpak, C. A., Lottich, S. C., Thor, A., and Schlom, J. Theuse of a monoclonal antibody (B72.3) as a novel immunohistochemicaladjunct for the diagnosis of carcinomas in fine needle aspiration biopsies.Hum. Pathol., in press, 1986.
25. Szpak, C. A., Johnston, W. W., Roggli. V., Kolbeck, J Lottich, S. C.,Vollmer, R., Thor, A., and Schlom, J. The diagnostic distinction betweenmalignant mesothelioma of the pleura and adenocarcinoma of the lung asdefined by a monoclonal antibody (B72.3). Am. J. Clin. Pathol., in press,1986.
26. Kufe, D., Inghirami, G., Abe, M., Hayes, D., Justi-Wheeler, H., and Schlom,J. Differential reactivity of a novel monoclonal antibody (DF3) with humanmalignant versus benign breast tumors. Hybridoma, 3: 223-232, 1984.
27. Lundy, J., Thor, A., Maenza, R., Schlom, J., Forouhar, F., Testa, M., andKufe, D. Monoclonal antibody DF3 correlates with tumor differentiationand hormone receptor status in breast cancer patients. Breast Cancer Res.Treat., 5: 269-276, 1985.
28. Shih, T. Y., and Weeks, M. O. Oncogenes and cancer: the p21 ras genes.Cancer Invest., 2: 109-123, 1984.
29. Thor, A., Horan Hand, P., Wunderlich, D., Caruso, A., Muraro, R., andSchlom, J. Monoclonal antibodies define differential ra* gene expression inmalignant and benign colonie diseases. Nature (Lond.), 311: 562-565, 1984.
30. Viola, M., Fromowitz, F., Oravez, S., Deb, S., Finkel, G., Lundy, J., Hand,P., Thor, A., and Schlom, J. Expression of raj oncogene in prostate cancer.N. Engl. J. Med., 314: 133-137, 1986.
31. Viola, M. V., Fromowitz, F., Oravez, S., Deb, S., Horan Hand, P., andSchlom, J. ras oncogene expression is increased in premalignant lesions andhigh grade bladder carcinomas. J. Exp. Med., 161: 1213-1218, 1985.
32. Der, C. J.. and Cooper, G. M. Altered gene products are associated withactivation of cellular ra\ genes in human lung and colon carcinoma. Cell, 32:201-208, 1983.
33. Fujita, J., Yoshida, O., Yuasa, Y., Rhim. J. S., Hatanaka, M., and Aaronson,S. A. Ha-ras oncogenes are activated by somatic alterations in human urinarytract tumours. Nature (Lond.), 309: 464-466, 1984.
34. Pulciani, S., Santos, E., Lauver, A. V., Long, L. K., Aaronson, S. A., andBarbacid, M. Oncogenes in solid human tumours. Nature (Lond.), 300:539-542, 1982.
35. Feig, L. A., Bast, R. C., Knapp, R. C.. and Cooper, G. M. Somatic activationof ras gene in a human ovarian carcinoma. Science (Wash. DC), 223: 698-700, 1984.
36. McCoy, M. S., Toóle,J. J., Cunningham, J. M., Chang, E. H., Lowy, D. R.,and Weinberg, R. A. Characterization of a human colon/lung carcinomaoncogene. Nature (Lond.), 302: 79-81, 1983.
37. Nakano, H., Yamamoto, T., Neville, C., Evans, D., Mizuno, T., and Perucho,M. Isolation of transforming sequences of two human lung carcinomas:structural and functional analysis of c-k-ruv oncogenes. Proc. Nati. Acad.Sci. USA, 81:71-75, 1984.
3236
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
38. Gambke, C, Signer, E., and Moroni, C. Activation of fi-ras gene in bonemarrow cells from a patient with acute myeloblastic leukemia. Nature(Lond.), 307:476-478, 1984.
39. Eva, A., Tronick, S. R., Gol, R. A., Pierce, J. H., and Aaronson, S. A.Transforming genes of human hematopoietic tumors: frequent detection ofrus -relateci oncogenes whose activation appears independent of tumor type.Proc. Nati. Acad. Sci. USA, 80:4926-4930, 1983.
40. Albino, A. P., Le Strange, R., Oliff, A. I., Furth, M. E., and Old, L. J.Transforming rax genes from human melanoma: a manifestation of tumourheterogeneity? Nature (Lond.), 308:69-72, 1984.
41. Tainsky, M. A., Cooper, C. S., Giovanella, B. C., and Vande Woude, G. F.An activated ras" gene: detected in late but not early passage human PAIteratocarcinoma cells. Science (Wash. DC), 225:643-645, 1984.
42. Capon, D. J., Seeburg, P. H., McGrath, J. P., Hayfleck, J. S., Edman, U.(Levinson, A. D., and Goeddel, D. V. Activation of Ki ra,v: gene in human
colon and lung carcinomas by two different point mutations. Nature (Lond.),304: 507-513, 1983.
43. Santos, E., Reddy, E. P., Pulciani, S., Feldmann, R. J., and Barbacid, M.Spontaneous activation of a human proto-oncogene. Proc. Nati. Acad. Sci.USA, 80:4679-4683, 1983.
44. Yuasa, Y., Srivastava, S. K., Dunn, C. Y., Rhim, J. S., Reddy, E. P., andAaronson, S. A. Acquisition of transforming properties by alternative pointmutations within c-bas/has human proto-oncogene. Nature (Lond.), 303:775-779, 1983.
45. Padua, R. A., Barrass, N. C., and Currie, G. A. Activation of N-r<w in ahuman melanoma cell line. Mol. Cell. Biol., 5:582-585, 1985.
46. Santos, E., Martin-Zanca, D., Reddy, E. P., Pierotti, M. A., Della Porta, G.,and Barbacid, M. Malignant activation of a ìt-rasoncogene in lung carcinomabut not in normal tissue of the same patient. Science (Wash. DC), 223:661-664, 1984.
47. Kraus, M. H., Yuasa, Y., and Aaronson, S. A. A position 12-activated H-rasoncogene in all HS578T mammary carcinosarcoma cells but not normalmammary cells of the same patient. Proc. Nati. Acad. Sci. USA, 81: 5384-5388, 1984.
48. Hall, A., Marshall, C. J., Spurr, N. K., and Weiss, R. A. Identification of atransforming gene in two human sarcoma lines as a member of the ras genefamily located on chromosome 1. Nature (Lond.), 303: 396-400, 1983.
49. Horan Hand, P., Thor, A., Wunderlich, D., Munirò. R., Caruso, A., andSchlom, }. Monoclonal antibodies of predefined specificity detect activatedrus gene expression in human mammary and colon carcinomas. Proc. Nati.Acad. Sci. USA, 81: 5227-5231, 1984.
50. Foulds, L. The experimental study of tumor progression: a review. CancerRes., 14: 327-339, 1954.
51. Horan Hand, P., Nuti, M., Colcher, D., and Schlom, J. Definition ofantigenic heterogeneity and modulation among human mammary carcinomacell populations using monoclonal antibodies to tumor associated antigens.Cancer Res., 43: 728-735, 1983.
52. Kufe, D. W., Nadler, L., Sargent, L., Shapiro, H., Hand, P., Austin, F.,Colcher, D., and Schlom, J. Biological behavior of human breast carcinoma-associated antigens expressed during cellular proliferation. Cancer Res., 43:851-857, 1983.
53. Friedman, E., Thor, A., Horan Hand, P., and Schlom, J. Surface expressionof tumor-associated antigens in primary cultured human colonie epithelialcells from carcinomas, benign tumors, and normal tissues. Cancer Res., 45:5648-5655, 1985.
54. Horan Hand, P., Colcher, D., Salomon, D., Ridge, J., Noguchi, P., andSchlom, J. Influence of spatial configuration of carcinoma cell populationson the expression of a tumor-associated glycoprotein. Cancer Res., 45: 833-840, 1985.
55. Herlyn, M., Sears, H. F., Steplewski, Z., and Koprowski, H. Monoclonalantibody detection of a circulating tumor associated antigen: I. Presence ofantigen in sera of patients with colorectal, gastric, and pancreatic carcinoma.J. Clin. Immunol., 2:135-140, 1982.
56. Magnani, J. L., Nilsson, B., Brockhaus, M., Zopf, D., Steplewski, Z.,Koprowski, H., and Ginsberg, V. A monoclonal antibody-defined antigenassociated with gastrointestinal cancer is a ganglioside containing sialylatedlacto-W-fuco-pentaose. J. Biol. Chem., 257:14365-14369, 1982.
57. Magnani, J. L., Steplewski, Z., Koprowski, H., and Ginsberg, V. Identification of the gastrointestinal and pancreatic cancer-associated antigen detectedby monoclonal antibody 19-9 in the sera of patients as a mucin. Cancer Res.,^3:5489-5492, 1983.
58. Devillano, B., Sears, H. J., Barnes, J., Space, S., Brennan, S., Rake, B.,Bucher, C., Liu, V., Schoemaker, H., and Zurawski, V. ¡KThe Centocor CA19-9°"RIA. Proceedings of the 34th Annual Meeting, American Association
for Clinical Chemistry, 1982.59. Metzgar, R. S., Rodriquez, N., Finn, O. J., Lan, M. S., Daasch, V. N.,
Fernsten, P. D., Meyers, W. C, Sindelar, W. F., Sandler, R. S., and Seigier,H. F. Detection of a pancreatic cancer-associated antigen (DU-PAN-2 antigen) in serum and ascites of patients with adenocarcinoma. Proc. Nati. Acad.Sci. USA, 81: 5242-5246, 1984.
60. Niloff, J. M., Klug, T. L., Schaetzl, E., Zurawski, V. R., Knapp, R. C., andBast, R. C. Elevation of serum CAI25 in carcinomas of the fallopian tube,endometrium, and endocervix. Am. J. Obstet. Gynecol., 148: 1057-1062,1984.
61. Hayes, D. F., Sekine, H., Ohno, T., Abe, M., Keefe, K., and Kufe, D. W.Use of a murine monoclonal antibody for detection of circulating plasmaDF3 antigen levels in breast cancer patients. J. Clin. Invest., 75:1671-1678,1985.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
Paterson, A. J., Schlom, J., Sears, H. F., Bennett, J., and Colcher, D. Aradioimmunoassay for detection of a human tumor-associated glycoprotein(TAG-72) using monoclonal antibody B72.3. Int. J. Cancer, in press, 1986.Larson, S. M. Radiolabeled monoclonal antitumor antibodies in diagnosisand therapy. J. NucÃ.Med., 26: 538-545, 1985.Rainsbury, R. M. The localization of human breast carcinomas by radiola-beled monoclonal antibodies. Br. J. Surg., 71:805-812, 1984.Bradwell, A. R., Fairweather, D. S., and Dukes, P. W. Localization oftumours using radiolabeled antibodies. Med. Lab. Sci., 41: 267-278, 1984.Farrands, P. A., Pimm, M. V., Embleton, M. J., Perkins, A. C., Hardy, J.D., Baldwin, R. W., and Hardcastle, J. D. Radioimmunodetection of humancolorectal cancers by an antitumor monoclonal antibody. Lancet, 2: 397-400, 1982.Armitage, N. C., Perkins, A. C., Pirn, M. V., Farrands, P. A., Baldwin, R.W., and Hardcastle, J. D. The localization of an anti-tumour monoclonalantibody (791T/36) in gastrointestinal tumors. Br. J. Surg., 74: 407-412,1984.Epenetos, A. A., Shepherd, J., Bretton, K. E., Hawkins, L., and Nimmon, C.C. Radioimmunodiagnosis of ovarian cancer using '-'I labelled, tumor-associated monoclonal antibodies. Cancer Detect. Prevent., 7:45-9, 1984.Chatal, J.-F., Saccavini, J.-C, Fumoleau, P., Douillard, J.-Y., Curtet, C.,Kremer, M., Le Mevel, B., and Koprowski, H. Immunoscintigraphy of coloncarcinoma. J. NucÃ.Med., 25:307-314, 1984.Carrasquillo, J. A., Krohn, K. A., Beaumier, P., McGuffm, R. W., Brown, J.P., Hellstrom, K. E., Hellström,I., and Larson, S. M. Diagnosis and therapyfor solid tumors with radiolabeled antibodies and immune fragments. CancerTreat. Rep., 68: 317-328, 1984.Zalcberg, J. R., Thompson, C. H., Lichtensein, M., Leyden, M. J., Andrews,J. T., Sullivan, J. R., and McKenzie, I. F. C. Tumour visualization using aradiolabelled monoclonal antibody. Aust. N. Z. J. Med., 13:571-577, 1983.Rainsbury, R. M., Westwood, J. H., Coombes, R. C., Neville, A. M., Ott, R.J., Kalirai, T. S., McCready, V. R., and Gazet, J. C. Location of metastaticbreast carcinoma by a monoclonal antibody chelate labelled with indium111. Lancet, 2:934-938, 1983.Moldofsky, P. J., Powe, J., Mulherne, C. B., Hammond, U., Sears, H. F.,Gatenby, P. A., Steplewski, Z., and Koprowski, H. Metastatic colon carcinoma detected with radiolabeled F(ab')2 monoclonal antibody fragments.Radiology, 149: 549-555, 1983.Mach, J. P., Chatal, J. F., Lumbroso, J. D., Buchegger, F., Forni, M.,Ritschard, J., Berche, C., Douillard, J-Y., Carrel, S., Herlyn, M., Steplewski,Z., and Koprowski, II. Tumor localization in patients by radiolabeled monoclonal antibodies against colon carcinoma. Cancer Res., 43: 5593-5600,1983.Mach, J-P., Buchegger, F., Forni, M., Ritschard, J., Berche, C., Lumbroso,J-D., Schreyer, M., Giradet, C., Accolla, R. S., and Carrel, S. Use of aradiolabeled monoclonal anti-CEA antibodies for the detection of humancarcinomas by external photoscanning and tomoscintigraphy. Immunol. Today, Dec.: 239-249, 1981.Colcher, D., Keenan, A. M., Larson, S. M., and Schlom, J. Prolonged bindingof a radiolabeled monoclonal antibody (B72.3) used for the in situ radioim-munodetection of human colon carcinoma xenografts. Cancer Res., 44:5744—5751, 1984.Keenan, A. M., Colcher, D., Larson, S. M., and Schlom, J. Radioimmuno-scintigraphy of human colon cancer xenografts in mice with radioiodinatedmonoclonal antibody B72.3. J. NucÃ.Med., 25:1197-1203, 1984.Carrasquillo, J. A., Colcher, D., Sugarbaker, P., Reynolds, J. R., Keenan, A.M., Simpson, D., Bryant, G., Thor, A., Perentesis, P., Esteban, J., Horowitz,M., Schlom, J., and Larson, S. M. Radiolocalization of colon cancer with 1131 B72.3 monoclonal antibody. In: Proceedings of the 32nd Annual Meetingof the Society of Nuclear Medicine, No. 51, 1985.Colcher, D. C., Carrasquillo, J. A., Sugarbaker, P., Bryant, G., Esteban, J.,Simpson, D., Thor, A., Reynolds, J., Horowitz, M., Keenan, A. M., Larson,S. M., and Schlom, J. Biodistribution of monoclonal antibody B72.3 (1-131)in colon cancer patients. In: Proceedings of the 32nd Annual Meeting of theSociety of Nuclear Medicine, No. 52, 1985.Colcher, D., Esteban, J., Carrasquillo, J. A., Sugarbaker, P., Reynolds, J. C,Bryant, G., Larson, S. M., and Schlom, J. Comparison of routes of administration of radiolabeled monoclonal antibodies in patients with colorectalcancer. ¡H:Proceedings of the 33rd Annual Meeting of the Society of NuclearMedicine, 1986(abstr.).Carrasquillo, J. A., Colcher, D., Sugarbaker, P., Esteban, J., Reynolds, J. C.,Bryant, G., Perentesis, P., Yokoyama, K., Schlom, J., and Larson, S. M.Intraperitoneal infusion with 1-131 B72.3 monoclonal antibody in patientswith peritoneal carcinomatosis from colon cancer. In: Proceedings of the33rd Annual Meeting of the Society of Nuclear Medicine, 1986 (abstr.).Epenetos, A. A. Clinical results with regional antibody-guided irradiation.In: Advances in the Application of Monoclonal Antibodies in Clinical Oncology, May, 1985 (abstr.).Colcher, D., Mornex, F., Esteban, J., Minelli, M. F., and Schlom, J. Radioim-munotherapy of human colon carcinoma xenografts. In: Proceedings of the33rd Annual Meeting of the Society of Nuclear Medicine, 1986 (abstr.).Greiner, J. W., Horan Hand, P., Noguchi, P., Fisher, P., Pestka, S., andSchlom, J. Enhanced expression of surface tumor associated antigens onhuman breast and colon tumor cells after recombinant leukocyte a-interferontreatment. Cancer Res., 44: 3208-3214, 1984.Greiner, J. W., Tobi, M., Fisher, P. B., Langer, J. A., and Pestka, S.Differential responsiveness to cloned mammary carcinoma cell populations
3237
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

APPLICATIONS OF MAbs IN CARCINOMA MANAGEMENT
to the human recombinant leukocyte interferon enhancement of tumor antigen expression. Int. J. Cancer, 36:159-166, 1985.
86. Koprowski, H., Herlyn, I)., Lübeck,M., DeFreitas, E., and Sears, H. F.Human anti-idiotype antibodies in cancer patients: is the modulation of theimmune response beneficial for the patient? Proc. Nati. Acad. Sci. USA, HI:216-219, 1984.
87. Nepom, G. T., Nelson, K. A., Holbeck, S. L., Hellstrom, I., and Hellström,K. E. Induction of immunity to a human rumor marker by in vim administration of anti-idiotype antibodies in mice. Proc. Nati. Acad. Sci. USA, 81:2864-2867,1984.
88. Colcher, D., Hand, P., Wunderlich, D., Nuli, M., Teramoto, Y. A., Kufe, D.,and Schlom, J. Potential diagnosis and prognostic applications of monoclonal antibodies to human mammary cancer. In: G. L. Wright, Jr. (ed.),Monoclonal Antibodies and Cancer, pp. 121-159. New York: Marcel Dek-
ker, Inc., 1983.89. Taylor-Papadimitriou, J., Peterson, J. A., Arklie, J., Burchell, J., Ceriani, R.
L., and Bodmer, W. I . Monoclonal antibodies to epithelium-specific components of human milk fat globule membrane: production and reaction withcells in culture. Int. J. Cancer, 28:17-21, 1981.
90. Arklie, J., Taylor-Papadimitriou, J., Bodmer, W., Egan, M., and Mollis, R.Differentiation antigens expressed by epithelial cells in lactating breast arealso detectable in breast cancers. Int. J. Cancer, 2fi: 23-29,1981.
91. Herlyn, M., Steplewski, /.. Herlyn, D., and Koprowski, H. Colorectal
carcinoma specific antigen: detection by means of monoclonal antibodies.Proc. Nati. Acad. Sci. USA, 76:1438-1442, 1979.
92. Arends, J. W., Wiggers, T., Schutte, B., Thijs, C. T., Verstijnen, C., Hilgers,J., Blijham, G. H., and Bosnian. F. T. Monoclonal antibody (1116-NS-19-9) defined monosialoganglioside (GICA) in colorectal carcinoma in relationto stage, histopathology and DNA flow cytometry. Int. J. Cancer, 32: 289-293, 1983.
93. Mach, J. P., Chatal, J. F., I-umbroso, J. D., Buchegger, F., Forni, M.,Ritschard, J., Berche, C, Douillard, J. Y., Carrel, S., Herlyn, M., Steplewski,/,., and Koprowski, H. Tumor localization in patients by radiolabeled monoclonal antibodies against colon cancer. Cancer Res., 43:5593-5600, 1983.
94. Atkinson, B. F., Ernst, C. S., Herlyn, M., Steplewski, /., Sears, H. F., andKoprowski, H. Gastrointestinal cancer-associated antigen in immunoperox-idase assay. Cancer Res., 42:4820-4823,1982.
95. Buchegger, F., Schreyer, M., Carrel, S., and Mach, J. P. Monoclonal antibodies to identify a CEA crossreacting antigen of 95 KI) (NCA-95) distinctin antigenicity and tissue distribution from the previously described NCA of55 KD. Int. J. Cancer, 33:643-649,1984.
96. Metzgar, R. S., Gaillard, M. T., Levine, S. J., Tuck, F. L. Bossen, E. H., andBorowitz, M. J. Antigens of human pancreatic adenocarcinoma cells definedby murine monoclonal antibodies. Cancer Res., 42:601-608,1982.
97. Colcher, D., lloran Hand, P., ÑutÃ,M., and Schlom, J. Differential bindingto human mammary and non-mammary tumors of monoclonal antibodiesreactive with carcinoembryonic antigen. Cancer Invest., /.- 127-138, 1983.
3238
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
1986;46:3225-3238. Cancer Res Jeffrey Schlom Rosenthal Foundation Award Lecturethe Management of Carcinomas: The Richard and Hinda Basic Principles and Applications of Monoclonal Antibodies in
Updated version
http://cancerres.aacrjournals.org/content/46/7/3225.citation
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/46/7/3225.citationTo request permission to re-use all or part of this article, use this link
on July 16, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from













![Characterization of the Blood Lymphocyte …cancerres.aacrjournals.org/content/canres/45/7/3225.full.pdf[CANCER RESEARCH 45, 3225-3230, July 1985] Characterization of the Blood Lymphocyte](https://img.pdfslide.us/doc/110x75/5aa6a05c7f8b9a1d728eac65/characterization-of-the-blood-lymphocyte-cancer-research-45-3225-3230-july.jpg)















