Embed Size (px)
Citation preview

Basic Concepts in Bladder Cancer Immunotherapy
Leonard G. Gomella, MD Chairman, Department of Urology Sidney Kimmel Cancer Center Thomas Jefferson University Philadelphia, PA

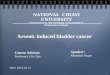
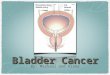
BCG Intravesical Immunotherapy • BCG immunotherapy standard of care NMIBC • Mechanism is s:ll under inves:ga:on,is recognized as immunotherapy
• BCG is internalized by both urothelial cancer cells and immune cells – Causes secre:on of cytokines and chemokines, and presenta:on of BCG and/or cancer cell an:gens to ac:vate T cells
• Safety: < 5% serious complica:ons – Common SE: fever, hematuria, granulomatous prosta::s
Redelman-Sidi, G et al. Nature Reviews Urology 2014; 11: 153–162 Lamm DL. Clin Infect Dis. 2000;31 Suppl 3:S86

Intravesical BCG Immunotherapy
BCG
Bladder cancer cells
CD8+ T cell HLA class I DC
Processing and antigen presentation
HLA class II
apoptosis BCG or cancer antigen
phagocytosis
CD4+ T cell
inflammation side effects
Macrophage
NK cell
Th-1 response IL-2, IL-12, IFN-γ, TNF-β
Cell-mediated immune response
DC CD8+
T cell Processing and antigen presentation
phagocytosis
Cytokine production

Overview of Cancer Immunology and Immunotherapy

Hallmarks of Cancer
Hanahan D, Weinberg RA. Cell. 2011;144:646-674. Hanahan D, Weinberg RA. Cell. 2000;100:57-70.
Sustaining prolifera:ve signaling
Deregula:ng cellular
energe:cs
Avoiding immune
destruc0on
Enabling replica:ve immortality
Inducing angiogenesis
Resis:ng cell death
Evading growth
suppressors Ac:va:ng invasion and metastasis
Hallmarks of Cancer
Pathogenesis
The immune system has a major role in cancer pathogenesis

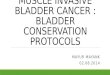
Increased Incidence of Cancer in Immunocompromised Individuals
• Malignant tumors develop in individuals with compromised immune systems1-‐3
1. Kasiske BL, Wang C, et al. Am J Transplant. 2004;4(6):905-‐913. 2. Le Mire L, Wojnarowska F, et al. Br J Dermatol. 2006;154(3):472-‐477. 3. Abbas AK, Lichtman AH. Basic Immunology. 3rd ed. 2011.
Tes:cular cancer
Breast cancer
Prostate cancer
Colon cancer
Bladder cancer
Hepatobiliary cancer
Melanoma
Kidney cancer
Non-‐Hodgkin’s lymphoma
Non-‐melanoma skin cancer
Tumor / cancer risk in transplant pa0ents compared with general popula0on1-‐3
0 5 10 15 20 Fold-‐increase in tumor / cancer risk
20-‐fold and beyond
15-‐fold
8-‐fold
3-‐fold
5-‐fold
2-‐fold

Basics: Immune system and cancer
interac:ons • Immune system and cancer interact in a
dynamic process known as “Immunoedi:ng” or “the 3 E’s” – Elimina:on: ini:al tumor development, low tumor volume immune system can eradicate cancer cells
– Equilibrium: immune system controls cancer growth
– Escape: con:nued growth; gene:c instability tumor heterogeneity takes place and overwhelms the immune system
Dunn GP, et al. Nat Rev Immunol. 2006;6(11):836-848. Mittal D, et al. Curr Opin Immunol. 2014;27:16-25

Immune Evasion of Cancer Progressive metasta:c cancer represents a failure of immune surveillance
Kalbasi A, et al. J Clin Invest. 2013;123(7):2756

An:cancer Immunity is Mediated Through a Mul:-‐step Process
Chen DS, et al. Immunity. 2013;39(1):1-10.
1. An:gens released by cancer cells
2. An:gens presented to T cells 3. T cell priming and ac:va:on 4. T cell trafficking to tumors 5. T cell infiltra:on into tumors 6. T cell recogni:on of cancer cells 7. Killing of cancer cells

Immune Checkpoints Lead to Promo:on or Inhibi:on of Immune Response
Chen DS, et al. Immunity. 2013;39(1):1-10.
Ac:va:ng:
CD28; CD137; OX40; GITR;IL-‐2
Inhibitory:
CTLA-‐4; PD-‐L1/PD-‐1;
PD-‐L1/B7.1

Principles of Cancer Immunotherapy • Immune response to cancer both s:mulatory and inhibitory
factors • Inhibitory immune checkpoints include CTLA-‐4, PD-‐1, PDL-‐1
– Limit immune response to protect self – Oien upregulated in tumors and in immune cells invading tumors – Results in inhibi:on of the T cell immune response – Allows tumors to more easily “hide” from the immune system
• Checkpoint inhibitors – An:bodies block the immune checkpoint to enhance T-‐cell and other immune cell func:ons
– Allow the immune response to expand – Examples of FDA-‐approved inhibitors include:
• CTLA-‐4: Ipilimumab • PD-‐1: Nivolumab, Pembrolizumab • PD-‐L1: Atezolizumab
Sharma P, et al. Nat Rev Cancer. 2011;11:805-812 Pardoll D. Nat Rev Cancer. 2012;12:252-264

Clinical Cancer Immunotherapy • Passive Immunotherapy:
o Monoclonal an:bodies directed against growth factors such as bevacizumab (VGEF), cetuximab (EGFR)
o Chronically administered, no sustainable an:-‐tumor response • Ac:ve Immunotherapy: induce host response to tumor by T-‐cell cascade -‐> CTL
o Need T-‐cell for solid tumor kill (cytotoxic T lymphocyte or CTL) o T cell cannot respond to naked or circula:ng an:gens o Require an:gens to be “presented” to T cells on APC (an:gen presen:ng
cells) o Dendri:c cells, Langerhans cells, monocytes, macrophages are APC o APC internalize an:gens, couple to HLA molecules to “present” on the
surface to ac:vate T-‐cell o Immune response depends on s:mulatory signals and inhibitory
“checkpoints” to avoid excessive produc:on of immune cells such s T cells that could be detrimental to normal :ssue

Selected Immunotherapies in Oncology • Vaccine based therapies: T cell ac:va:on to seek out tumor cells
– Eg, Sipuleucel-‐T, BCG • Cytokines: naturally occurring, modulate immune response
– Eg, IL-‐2, interferon-‐alpha • Monoclonal an0bodies: block specific growth factors, etc causing cell
death cascade – Eg, bevacizumab targe:ng VGEF
NEWEST THERAPIES • Checkpoint inhibitors: monoclonal an:bodies block the immune
checkpoint response; “take the brakes off” immune system – Eg, CTLA-‐4, PD-‐1, PD-‐L1 inhibitors
• Chimeric An0gen Receptor (Car) T-‐cell Therapy – Pa:ent’s T cells are reengineered to recognize cancer (experimental)
Dinarello CA Eur J Immunol. 2007 Nov; 37(Suppl 1): S34–S45. Weiner LM, et al. Nat Rev Immunol. 2010;10:317-327. Kantoff PW, et al. N Engl J Med. 2010;363:411-422. Pardoll D. Nat Rev Cancer. 2012;12:252-264.

hnp://www.ny:mes.com/2016/12/03/health/immunotherapy-‐cancer.html

Immune Checkpoint Inhibi:on
• Pembrolizumab: PD-‐1 monoclonal an:body • Nivolumab: PD-‐1 monoclonal an:body • Atezolizumab: monoclonal an:body to programmed death ligand 1 (PD-‐L1)
• Avelumab: an:-‐PD-‐L1 monoclonal • Durvalumab: an:-‐PD-‐L1 monoclonal Homet Moreno B, et al. Br J Cancer. 2015 Apr 28;112(9):1421-7 Markham A. Drugs. 2016 Aug;76(12):1227-32
PD-‐1 T cell receptor PDL-‐1 tumor ligand PD-‐1/PD-‐L1 inhibitors result in higher response rates across a wide range of tumors than most other immunotherapies

PD-‐1/PD-‐L1 Ac:vity
Suppression of T-‐cell response….. “Taking the brakes off”
http://www.pharmaceutical-journal.com/news-and-analysis/feature/immune-checkpoint-inhibitors-bring-new-hope-to-cancer-patients/20067127.article Accessed October 24, 2016

Why is Bladder Cancer A Good Target for Immunotherapy?

Urothelial bladder cancer (UBC) as an target for immunotherapy
• Pa:ents with UBC have a high rate of soma:c muta:ons similar to tumors associated with tobacco use or environmental carcinogen exposure
• Host immune system can recognize tumor an:gens. An:gens detected seen as foreign, s:mula:ng an immune an: tumor response
Lawrence MS, et al. Nature Jul 11;499(7457):214-8, 2013; Bellmunt. Ann Oncol. 2013; Cancer Genome Atlas Research Network. Comprehensive molecular characterization of urothelial bladder carcinoma. Nature 507, 315–322 (2014)

Basis of Urothelial Cancer Immunotherapy
• High rates of soma:c muta:ons – May enhance immune response
• Urothelial cancers may express compounds that suppress the immune system such as programmed death-‐ligand 1 (PD-‐L1)
• CD4+ and CD8+ T cells express inhibitory PD-‐1 to prevent overs:mula:on of the immune response
• PD-‐L1/and PD-‐1 are the immune checkpoints • Check point inhibitors enhance an:-‐tumor effects by allowing a more robust immune response
Powles, T, et al. Nature 2014; 515: 558–562. Hafez N, Petrylak DP. Immunotherapy. 2015;7(1):1-2

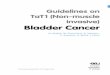
Immune Cells Within Tumors Predict Overall Survival: MIBC Example
• Higher immune cell density (T cells) predic:ve of survival of pa:ents with MIBC • Suggests importance of immune response in MIBC
1. Sharma P, et al. Proc Natl Acad Sci U S A. 2007;104(10):3967-3972. 2. Galon J, Pagès F, et al. Science. 2006;313(5795):1960-1964.
Prop
. Surviving W
ithou
t Disease
Time in Months 40 20 0 60 80
0.0
0.2
0.4
0.6
0.8
1.0
P<0.001
T cells (CD8) <8 (median survival=13 months) T cells (CD8) ≥8 (median survival >80 months)

Checkpoint Inhibitors and Biomarkers • FDA approved complementary diagnos:c, the PD-‐L1 (SP142) assay with atezolizumab – detects PD-‐L1 expression on tumor-‐infiltra:ng immune cells
• Phase 1 study of atezolizumab: higher response rates were with higher tumor levels of PD-‐L1 expression in tumor-‐infiltra:ng lymphocytes, not tumor cells.
• While promising, many other PD-‐L1 an:bodies exist limi:ng generalizability
• Genomic and other tes:ng being u:lized to determine best response to a given checkpoint inhibitor
Petrylak DP, et al. J Clin Oncol. 2015;33(suppl): abstract 4501 Tsiatas M, et al. Ann Transl Med. 2016 Jul;4(14):270

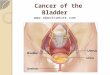
mRNA expression levels of PD1/PDL1 and CTLA4 genes in a series of 155 bladder tumors.
Pignot, et al. J Clin Oncol 34, 2016 (suppl; abstr 4523)

PD-‐L1 Diagnos0c Tes0ng Clinical Experience at the Thomas Jefferson University Hospital
23
Urothelial Carcinoma Tumor Cells
Urothelial Carcinoma Tumor-‐infiltra0ng Immune Cells
PD-‐L1 IHC Staining Using Ventana SP142
Magnifica0on x10 Magnifica0on x10
Courtesy of Charalambos C. Solomides, MD, Director of Cytopathology

Generic/Dosing Brand Manufacturer Target Comp. Biomarker
Urothelial Carcinoma Approval
Date(s) of UC Approval
Approval in Other Malignancies
Atezolizumab 3wk TECENTRIQ Genentech PD-‐L1 VENTANA PD-‐L1 (SP142)*
1, 2, 3 5/18/20161,2 4/17/20173
NSLC
Avelumab 2wk BAVENCIO Pfizer PD-‐L1 DAKO 73-‐10
1, 2 5/9/2017 Merckel Cell
Durvalumab 2wk IMFINZI AstraZeneca PD-‐L1 VETANA PD-‐L1 (SP263)*
1, 2 5/1/2017 -‐-‐
Nivolumab 2wk OPDIVO Bristol-‐Myers Squibb
PD-‐1 DAKO 28-‐8$ 1, 2 2/2/2017 Melanoma, NSLC,RCC, others
Pembrolizumab 3wk KEYTRUDA Merck PD-‐1 DAKO 22C3$
1, 2, 3 5/18/2017 Melanoma, NSCLC, Microsatellite Instability-‐High Cancer, others
Checkpoint inhibitors for systemic use in advanced UC (7/2017)
(Mark R et al In press American J Hematology Onc)
1. Locally advanced or metasta:c UC with progression during or aier treatment w/pla:num chemo. 2. Locally advanced or metasta:c UC progressing within 12 mo of neoadjuvant/ adjuvant pla:num chemo. 3. Locally advanced or metasta:c UC if pla:num ineligible. * Indicates FDA approved companion biomarker
$ FDA approved biomarker in other malignancies

Why did early BCG studies use 6 weeks of therapy?
n Because BCG was packaged in 6 packs.
Why does beer come in 6 packs?


![Women and Bladder Cancer - Oncoscan yellow 8-20_.pdf · bladder cancer [18,170] than cervical cancer [11,270] > 500,000 people in the U.S. have/had bladder cancer – highest recurrent](https://img.pdfslide.us/doc/110x75/5f694c18ea002e289e4b0db0/women-and-bladder-cancer-yellow-8-20pdf-bladder-cancer-18170-than-cervical.jpg)