Embed Size (px)
Citation preview

Meaningful Use: What Does it Mean?Barbara Klepfer, MSN, RN-BC
Anne Mamiya, MT(ASCP) Lisa Votti, MSN, RN-BC
Austin, TXNovember 21, 2014
© Seton Healthcare Family 1

Review requirements of the 3 stages of the American Recovery and Reinvestment Act (ARRA).
Identify at least 4 innovations related to ARRA which must occur to achieve meaningful use (MU).
2
Objectives
© Seton Healthcare Family

United States Department of Health and Human Services (HHS) implements and manages ARRA programs
Healthcare Information Technology (HIT) infrastructure being built
Centers for Medicare & Medicaid Services (CMS) provides reimbursement incentives to those successful in achieving Meaningful Use (MU)
Overview
http://www.hhs.gov/recovery/
American Recovery and Reinvestment Act (ARRA) of 2009
© Seton Healthcare Family 3

Preserve/create jobs; promote economic recovery
Assist those most impacted by recessionProvide investments needed to increase
technological advances in science and health
Invest in long-term economic profits Stabilize state and local government
budgets
4
Purpose of ARRA
© Seton Healthcare Family

DIVISION A—APPROPRIATIONS PROVISIONS TITLE I—AGRICULTURE, RURAL DEVELOPMENT, FOOD AND DRUG ADMINISTRATION,AND RELATED
AGENCIES TITLE II—COMMERCE, JUSTICE, SCIENCE, AND RELATED AGENCIES TITLE III—DEPARTMENT OF DEFENSE TITLE IV—ENERGY AND WATER DEVELOPMENT TITLE V—FINANCIAL SERVICES AND GENERAL GOVERNMENT TITLE VI—DEPARTMENT OF HOMELAND SECURITY TITLE VII—INTERIOR, ENVIRONMENT, AND RELATED AGENCIES TITLE VIII—DEPARTMENTS OF LABOR, HEALTH AND HUMAN SERVICES,AND EDUCATION, AND RELATED
AGENCIES TITLE IX—LEGISLATIVE BRANCH TITLE X—MILITARY CONSTRUCTION AND VETERANS AFFAIRS AND RELATED AGENCIES TITLE XI—STATE, FOREIGN OPERATIONS, AND RELATED PROGRAMS TITLE XII—TRANSPORTATION, HOUSING AND URBAN DEVELOPMENT, AND RELATED AGENCIES TITLE XIII—HEALTH INFORMATION TECHNOLOGY TITLE XIV—STATE FISCAL STABILIZATION FUND TITLE XV—ACCOUNTABILITY AND TRANSPARENCY TITLE XVI—GENERAL PROVISIONS—THIS ACT
DIVISION B—TAX, UNEMPLOYMENT, HEALTH, STATE FISCAL RELIEF, AND OTHER PROVISIONS TITLE I—TAX PROVISIONS TITLE II—ASSISTANCE FOR UNEMPLOYED WORKERS AND STRUGGLING FAMILIES TITLE III—PREMIUM ASSISTANCE FOR COBRA BENEFITS TITLE IV—MEDICARE AND MEDICAID HEALTH INFORMATION TECHNOLOGY; MISCELLANEOUS MEDICARE
PROVISIONS TITLE V—STATE FISCAL RELIEF TITLE VI—BROADBAND TECHNOLOGY OPPORTUNITIES PROGRAM TITLE VII—LIMITS ON EXECUTIVE COMPENSATION
5
Table of Contents for ARRA
© Seton Healthcare Family
http://www.gpo.gov/fdsys/pkg/BILLS-111hr1enr/pdf/BILLS-111hr1enr.pdf

A part of the ARRA legislationHealth Information Technology for Economic and
Clinical Health (HITECH)HITECH allocates $19 billion to hospitals and
physicians who demonstrate “meaningful use” of electronic medical records
HHS regulates and guides development of interoperable, private and secure nationwide health information technology infrastructures
HITECH Act
6
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Basics.html
© Seton Healthcare Family

EHR Final Rule Incentives for MUProvides guidelines for EHR adoption Provides guidelines on qualifying for incentives
Standards & Certification CriteriaIdentifies certification process of EHRs
Privacy & SecurityIncrease privacy during health information
exchangeGuidelines for encryption & destruction of health
information
HITECH – 3 Areas of Focus
7© Seton Healthcare Family

Utilization of EHRs for meaningful use to achieve 5 health care goals:Improve quality, safety, and efficiency of
care while reducing disparitiesEngage patients and families in their carePromote public and population health &
improve outcomesImprove care coordinationPromote the privacy and security of EHRs
Why is This Important?
8© Seton Healthcare Family

Meaningful Use is defined by the use of certified EHR technology in a meaningful manner (for example electronic prescribing); ensuring that the certified EHR technology is connected in a manner that provides for the electronic exchange of health information to improve the quality of care; and that in using certified EHR technology the provider must submit to the Secretary of Health & Human Services (HHS) information on quality of care and other measures.
Definition of Meaningful Use
9© Seton Healthcare Family
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Meaningful_Use.html
http://www.nejm.org/doi/full/10.1056/NEJMp0912825

Stage 1
• 5 Domains:• D1: Improve Quality, Safety, Efficiency• D2: Engage Patients and Families• D3: Improve Care Coordination• D4: Improve Public and Population Health• D5: Ensure Privacy and Security for Personal Health Information
Stage 2
• Stage 1 + Stage 2• Objective is to increase health information exchange between
providers and promote patient engagement by giving patients secure online access to their health information.
Stage 3
• From lessons learned (Final Rule is not out)• Simplify and reduce reporting• Promote innovative approach, reward good behavior• Consolidate
Stages of Meaningful Use
10© Seton Healthcare Family
http://www.healthit.gov/providers-professionals/national-learning-consortiumhttp://www.healthit.gov/providers-professionals/step-5-achieve-meaningful-use-stage-1

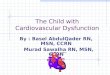
ARRA Meaningful Use TimelineEH: Eligible Hospital – Follow Federal Fiscal Year (October – September)
EP: Eligible Professional –Follow Calendar Year (January – December)
12

Incentive PaymentsPayment years under the EHR Incentive Programs
follow the federal fiscal year (Oct – Sept)Hospitals can begin receiving payments in any year
from FFY 2011 to FFY 2015Incentive payments decrease for hospitals that start
receiving payments in 2014 and laterHospitals that are not meaningful users of certified
EHR technology will be subject to payment adjustments beginning in FFY 2015
Product of 3 factors with complex formulas:1. An Initial Amount 2. The Medicare Share 3. A Transition Factor applicable to the payment year
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/MLN_TipSheet_MedicareHospitals.pdf
13

Adjustments (aka Penalties) Adjustments will be applied:
At the start of the 2015 fiscal year (FY) for eligible hospitals and CAHs (October 1, 2014)
At the start of the calendar year (CY) for EPs (January 1, 2015)
EPs, eligible hospitals, and CAHs must continue to demonstrate meaningful use every year to avoid payment adjustments in subsequent years.
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/How_Payment_Adj_Affect_ProvidersTipsheet.pdf
14

How are Adjustments Applied? For Eligible Hospitals
Applied to the % increase to the Inpatient Prospective Payment System (IPPS) payment rate
Hospitals receive a reduced update to the IPPS standardized amount Payment adjustments are cumulative for every consecutive year the
hospital is not a meaningful user For CAHs
Applied to the Medicare reimbursement for inpatient services during the cost reporting period in which they failed to demonstrate meaningful use
For a cost reporting period that begins in FY 2015, a CAH reimbursement would be reduced from 101 percent of its reasonable costs to 100.66 percent
To Avoid Adjustments Eligible Hospitals must:
Demonstrate meaningful use prior to the 2015 calendar/fiscal payment adjustment year (and every year after)
2013 participation will avoid the 2015 adjustment for those that participate in 2013 2014 participation will avoid the 2015 adjustment for those that begin participation
in 2014 CAHs must:
Demonstrate meaningful use during the same FY the payment adjustments take place to avoid the adjustments (starting in 2015, and beyond)
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/How_Payment_Adj_Affect_ProvidersTipsheet.pdf 15

15
Stage 1 MU
© Seton Healthcare Family

Final rule for requirements for 2014 Stage 1 were released with Stage 2 Final rules
Eligible hospitals (EH) and Critical Access Hospitals (CAH)must meet:11 Required Core Objectives5 Menu Objectives from a list of 10 (at least
one must be a public health measure)16 out of 29 Clinical Quality Measures
Stage 1 Meaningful Use 2014
16© Seton Healthcare Family
http://www.gpo.gov/fdsys/pkg/FR-2014-09-04/pdf/2014-21021.pdf
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Meaningful_Use.html

MU ObjectiveStage 1 2014
Core/Menu Threshold
CPOE Core 30% Meds
Drug-Drug/Drug-Allergy Checks Core ImplementProblem List Core 80%Medication List Core 80%Medication Allergy List Core 80%Demographics Core 50%Vital Signs Core 50%Smoking Status Core 50%
Clinical Decision Support Core Implement 1 rule
View, Download, and Transmit Core 50%-Provide Ability
Protect Electronic Health Information Core Security Risk Assessment
Stage 1 2014 – Eligible Hospitals and CAHs
http://www.healthit.gov/sites/default/files/2014editionehrcertificationcriteria_mustage1.pdf
17

MU ObjectiveStage 1 2014
Core/Menu ThresholdImmunization Registry (public health) Menu 1 testReportable Labs (public health) Menu 1 testSyndromic Surveillance (public health) Menu 1 testDrug formulary checks Menu ImplementAdvance Directives Menu 50%Incorporate Lab Results Menu 40%Generate Patient List by Condition Menu 1 reportPatient-Specific Education Menu 10%Medication Reconciliation Menu 50%
Summary of Care at Transition Menu 50%
Clinical Quality Measures CQM 16 of 29 across 3 domains
Stage 1 2014 – Eligible Hospitals and CAHs
19

Reporting period is 90 consecutive days for first year.
If you have previously attested to Stage 1 then you must report for an entire federal fiscal year.
Exception for FFY 2014. (allows for a 90 day or 1 quarter reporting period)
Stage 1 Reporting
19
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Hospital_Attestation_Stage1Worksheet_2014Edition.pdf
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/MU_Stage1_ReqOverview.pdf© Seton Healthcare Family

Objectives and Clinical Quality MeasuresReporting may be yes/no or
numerator/denominator attestationReporting through attestationReference worksheet for Stage 1
Stage 1 Reporting
20
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/MU_Stage1_ReqOverview.pdf
© Seton Healthcare Family

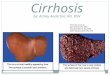
Meaningful Use Clinical Quality Measures Beginning FY14CMS
eMeasure ID NQF # Version # Measure TitleNational Quality Strategy Domain
55 0495 3Emergency Department (ED)-1 Emergency Department Throughput – Median time from ED arrival to ED departure for admitted ED patients
Patient and Family Engagement
111 0497 3ED-2 Emergency Department Throughput – admitted patients – Admit decision time to ED departure time for admitted patients
Patients and Family Engagement
104 0435 3 Stroke-2 Ischemic stroke – Discharged on anti- thrombotic therapy.
Clinical Process/ Effectiveness
71 0436 4 Stroke-3 Ischemic stroke – Anticoagulation Therapy for Atrial Fibrillation/Flutter
Clinical Process/ Effectiveness
91 0437 4 Stroke-4 Ischemic stroke – Thrombolytic Therapy Clinical Process/ Effectiveness
72 0438 3 Stroke-5 Ischemic stroke – Antithrombotic therapy by end of
Clinical Process/ Effectiveness
105 0439 3 Stroke-6 Ischemic stroke – Discharged on Statin Medication
Clinical Process/ Effectiveness
107 N/A 3 Stroke-8 Ischemic or hemorrhagic stroke – Stroke education
Patient and Family Engagement
102 0441 3 Stroke-10 Ischemic or hemorrhagic stroke – Assessed for Rehabilitation Care Coordination
108 0371 3 Venous Thromboembolism (VTE)-1 VTE prophylaxis Patient Safety190 0372 3 VTE-2 Intensive Care Unit (ICU) VTE prophylaxis Patient Safety
73 0373 3 VTE-3 VTE Patients with Anticoagulation Overlap Therapy
Clinical Process/ Effectiveness
109 N/A 3VTE-4 VTE Patients Receiving Unfractionated Heparin (UFH) with Dosages/Platelet Count Monitoring by Protocol (or Nomogram)
Clinical Process/ Effectiveness
110 N/A 3 VTE-5 VTE discharge instructions Patient and Family Engagement
114 N/A 3 VTE-6 Incidence of potentially preventable VTE Patient Safety22

Meaningful Use Clinical Quality Measures Beginning FY14CMS
eMeasure ID NQF # Version # Measure TitleNational Quality Strategy Domain
100 0142 3 AMI-2-Aspirin Prescribed at Discharge for AMI Clinical Process/ Effectiveness
113 0469 3 PC-01 Elective Delivery Prior to 39 Completed Weeks Gestation
Clinical Process/ Effectiveness
60 0164 3 AMI-7a Fibrinolytic Therapy Received Within 30 minutes of Hospital Arrival
Clinical Process/ Effectiveness
53 0163 3 AMI-8a Primary PCI Received Within 90 Minutes of Hospital Arrival
Clinical Process/ Effectiveness
30 0639 4 AMI-10 Statin Prescribed at Discharge Clinical Process/ Effectiveness
188 147 4PN-6 Initial Antibiotic Selection for Community- Acquired Pneumonia (CAP) in Immunocompetent Patients
Efficient Use of Healthcare Resources
171 527 4 SCIP-INF-1 Prophylactic Antibiotic Received within 1 Hour Prior to Surgical Incision Patient safety
172 528 4 SCIP-INF-2 Prophylactic Antibiotic Selection for Surgical Patients
Efficient Use of Healthcare Resources
178 453 4SCIP-INF-9 Urinary catheter removed on Postoperative Day 1 (POD1) or Postoperative Day 2 (POD2) with day of surgery being day zero
Patient Safety
32 496 4 ED-3 Median time from ED arrival to ED departure for discharged ED patients Care Coordination
26 N/A 2 Home Management Plan of Care (HMPC) Document Given to Patient/Caregiver (CAC-3)
Patient and Family Engagement
9 480 3 Exclusive Breast Milk Feeding (PC-05) Clinical Process/ Effectiveness
185 716 3 Healthy Term Newborn Patient Safety
31 1354 3 Hearing screening before hospital dischargeClinical Process/ Effectiveness
23

23
Stage 2 MU
© Seton Healthcare Family

Meet 16 Core Objectives
Meet 3 out of 6 Menu Objectives
Report 16 of 29 Clinical Quality Measures
© Seton Healthcare Family 24
Stage 2 2014 – Eligible Hospitals and CAHs

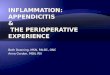
Stage 1 and 2 Comparison for Eligible Hospitals and CAHs
MU Objective
Stage 1 2014 Stage 2 2014
Core/Menu Threshold Core/Menu Threshold
CPOE Core 30% Meds Core60% Meds30% Lab30% Rad
Drug-Drug/Drug-Allergy Checks Core Implement Incorporated into the CDS objective
Problem List Core 80% Incorporated into the Summary of Care at Transition as required elements
Medication List Core 80%
Medication Allergy List Core 80%
Demographics Core 50% Core 80%
Vital Signs Core 50% Core 80%
Smoking Status Core 50% Core 80%
Clinical Decision Support Core Implement 1 rule Core1) 5 interventions 2) Drug-Drug/Drug-Allergy Checks
View, Download, and Transmit Core 50%-Provide Ability Core
1) 50%-Provide Ability2) 5%-View, Download or Transmit
Protect Electronic Health Information Core Security Risk Assessment Core Security Risk
Assessment 26

Stage 1 and 2 Comparison for Eligible Hospitals and CAHs
MU ObjectiveStage 1 2014 Stage 2 2014
Core/Menu Threshold Core/Menu ThresholdImmunization Registry (public health) Menu 1 test Core Ongoing submissionReportable Labs (public health) Menu 1 test Core Ongoing submissionSyndromic Surveillance (public health) Menu 1 test Core Ongoing submissionDrug formulary checks Menu Implement Incorporated into ePrescriptionsAdvance Directives Menu 50% Menu 50%Incorporate Lab Results Menu 40% Core 55%Generate Patient List by Condition Menu 1 report Core 1 reportPatient-Specific Education Menu 10% Core 10%Medication Reconciliation Menu 50% Core 50%
Summary of Care at Transition Menu 50% Core
1) 50%-any method2) 10%-electronic3) 1 exchange with different EHR technology
Med Administration Using Assistive Technology with eMAR Core 10%
Electronic Progress Notes Menu 30%Imaging results Menu 10%Family Health History Menu 20%Electronic Prescriptions Menu 10%
Electronic Lab Results to Ambulatory Providers Menu 20%
Clinical Quality Measures CQM 16 of 29 across 3 domains CQM 16 of 29 across 3
domains 27

In August 2014, CMS released a final rule that grants flexibility to providers who are unable to fully implement 2014 Edition CEHRT for an EHR reporting period in 2014 due to delays in 2014 Edition CEHRT availabilityProviders scheduled to demonstrate Stage 2 of meaningful use for an EHR reporting period in 2014 that have not fully implemented 2014 Edition CEHRT can:
Demonstrate 2013 Stage 1 objectives and 2013 CQMs with 2011 Edition CEHRT or a combination of 2011 and 2014 Edition CEHRT
Demonstrate 2014 Stage 1 objectives and 2014 CQMs with 2014 Edition CEHRT or a combination of 2011 and 2014 Edition CEHRT
Demonstrate Stage 2 objectives and 2014 CQMs with 2014 Edition CEHRT or a combination of 2011 and 2014 Edition CEHRT
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Stage_2.html
CMS 2014 CEHRT Flexibility
28

ARRA Meaningful Use TimelineEH: Eligible Hospital – Follow Federal Fiscal Year (October – September)
EP: Eligible Professional –Follow Calendar Year (January – December)
29

H.R.5481 - To continue the use of a 3-month quarter EHR reporting period for health care providers to demonstrate meaningful use for 2015 under the Medicare and Medicaid EHR incentive payment programs, and for other purposes.
https://www.congress.gov/bill/113th-congress/house-bill/5481
2015 Reporting Period
30

Begins in 2017
NPRM for Stage 3 expected in first quarter of 2015
Draft areas of focusClinical Decision Support (CDS)Patient engagementCare coordinationPopulation management
© Seton Healthcare Family 30
Stage 3

31
Innovations to Achieve Meaningful Use
© Seton Healthcare Family

Transmit prescriptions to local pharmacies
Report data to state or national health department(s) &/or CMS Smoking status of pts 13 yrs or olderClinical Quality Measures Immunization registriesLab resultsSyndromic surveillance data (monitor for
outbreaks/epidemics)Texting results or orders
Health Information Exchange
32© Seton Healthcare Family

Exchange clinical information w/ next provider of care or referral to a consultantPatient demographicsAllergies Height/WeightLab & other test resultsProcedure listProblem & Diagnosis listMedication listAdvance DirectivesReferralsSummary of care
Pt Care Summary at Transition of Care
33© Seton Healthcare Family

Electronic copy of record to patients within 3 business days
Electronic copy of discharge instructionsPatient portals for patients to enter
home medications, health history information, update Advance Directives information, etc.
Identify education resources for patient and provide information to patient to access electronically
Patient Access to EHR
34© Seton Healthcare Family

Electronic orders – legible, dated, signedElectronic medication reconciliationDuplicate order checkingStandardization of order sets aligned
withEvidence-based medicineFormulariesClinical preferences Quality improvement efforts
Computerized Provider Order Entry (CPOE)
35© Seton Healthcare Family

Closed Loop Medication Administration
Bar Code Scanning (Positive Pt ID)
Patient education via television or computer
Clinical Device InterfacesPhysiologic MonitorsPulse OximetersSmart IV PumpsSmart BedsVentilatorsPatient Call LightsEmergency Call Lights
Utilization of social media for reminders, check-ins, etc.
Technology Adoption
36© Seton Healthcare Family

Drug-Drug, Drug-Allergy, Drug-Food, Drug-Formulary checks
Duplicate ordering alerts
Clinical quality measures rules
Real-time monitoring of patients meeting quality measure criteria
Plan of Care rules
Evidence-based support
An Order Set
Clinical Decision Support (CDS) – Interventions
37© Seton Healthcare Family
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/ClinicalDecisionSupport_Tipsheet-.pdf

38
Attestation Process
© Seton Healthcare Family

To attest for the Medicare EHR Incentive Program in your first year of participation, you will need to have met meaningful use for a consecutive 90-day reporting period.
Submit intent to attest on CMS website: Successfully register for the Medicare EHR Incentive Program; Meet meaningful use criteria using certified EHR technology; and Successfully attest, using CMS' Web-based system, that you have
met meaningful use criteria using certified EHR technology.
Meet reporting requirements for attestation
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/RegistrationandAttestation.html
http://www.cms.gov/apps/stage-1-meaningful-use-attestation-calculator/
Attestation Process
39© Seton Healthcare Family

Questions
41© Seton Healthcare Family

Blumenthal, D. (February 4, 2010). “Launching HITECH”. New England Journal of Medicine. 362(5): 382-385. Retrieved September 22, 2010 from: http://www.nejm.org/doi/full/10.1056/NEJMp0912825
Centers for Medicare and Medicaid Services (2014) . Medicare and Medicaid EHR Incentive Program Basics. Retrieved from http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Basics.html
Centers for Medicare and Medicaid Services (2014) . 2014 Definition Stage 1 of Meaningful Use. Retrieved from http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Meaningful_Use.html
Centers for Medicare and Medicaid Services (2014) . Medicare EHR Incentive Program Payment Adjustments: What Providers Need to Know Retrieved from https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/How_Payment_Adj_Affect_ProvidersTipsheet.pdf
Centers for Medicare and Medicaid Services (2013). EHR Incentive Program for Medicare Hospitals: Calculating Payments Retrieved from http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/MLN_TipSheet_MedicareHospitals.pdf
Centers for Medicare and Medicaid Services (2014). Registration User Guide for Eligible Hospitals. Retrieved November 2014 from https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/EHRHospital_RegistrationUserGuide.pdf
References
42© Seton Healthcare Family

Center for Medicare and Medicaid Services (2014). Stage 2. Retrieved from http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Stage_2.html
Center for Medicare and Medicaid Services (2014). Clinical Decision Support: More Than Just ‘Alerts’ Tipsheet. Retrieved from http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/ClinicalDecisionSupport_Tipsheet-.pdf
Center for Medicare and Medicaid Registration & Attestation. (2014). Retrieved from http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/RegistrationandAttestation.html
Congress.gov (2014). H.R.5481 - To continue the use of a 3-month quarter EHR reporting period for health care providers to demonstrate meaningful use for 2015 under the Medicare and Medicaid EHR incentive payment programs, and for other purposes. Retrieved from https://www.congress.gov/bill/113th-congress/house-bill/5481
References
43

HealthIT.gov (2014). National Health Consortium. Retrieved from http://www.healthit.gov/providers-professionals/national-learning-consortium
HealthIT.gov (2014). Retrieved from http://www.healthit.gov/sites/default/files/2014editionehrcertificationcriteria_mustage1.pdf
HealthIT.gov (2014). How to implement EHRs. Retrieved from http://www.healthit.gov/providers-professionals/ehr-implementation-steps/step-5-achieve-meaningful-use
HealthIT.gov. Federal Advisory Committees. Draft recommendations for stage 3. retrieved November 18, 2014 from http://www.healthit.gov/FACAS/sites/faca/files/muwg_stage3_draft_rec_07_aug_13_.v3.pdf
HITECH Answers (2014). Meaningful Use. Retrieved from http://www.hitechanswers.net/ehr-adoption-2/meaningful-use/
One Hundred Eleventh Congress of the United States of America (January 6, 2009). American Recovery and Reinvestment Act of 2009. Retrieved September 2010 from: http://fdsys.gpo.gov/fdsys/pkg/BILLS-111hr1ENR/pdf/BILLS-111hr1ENR.pdf
U.S. Department of Health & Human Services (2010, September). HHS Home > Recovery > Overview. Retrieved September 9. 2010, from HHS.gov/Recovery: http://www.hhs.gov/recovery/overview/index.html
References
© Seton Healthcare Family 43