Embed Size (px)
Citation preview

BAP GUIDELINES FOR TREATING
BIPOLAR DISORDER
• Guy Goodwin, Oxford University, UK
• For a Consensus Meeting endorsed by the British Association for Psychopharmacology
• traduction française partielle sans garantie.

http://www.bap.org.uk/

Recommandations
• Les recommendations s’appliquent sur un patient moyen
• Recommendations peuvent s’appliquer environ 70% du temps aussi nous avons utilisés des expressions comme “Cliniciens peuvent considérer…..”
• Cependant, il y aura des occasions où appliquer une recommendation sans réflechir peut faire plus de mal que de bien

Guidelines
• Options provide a summary of up-to-date evidence and may highlight current uncertainties
• Standards of care are intended to apply rigidly. Many standards are driven by ethical consensus rather than evidence

Methodology
• Meeting on 24th May 2002
• Brief presentations on key areas– Emphasis on systematic reviews and
randomised controlled trials (RCTs) – Discussion to identify consensus and
uncertainty
• Review and recommendations circulated to participants (2 iterations, Nov, 2002, Feb 2003)
• Feedback as far as possible incorporated into the final version of the guidelines (Feb 2003)

Strength of evidence andrecommendations
Treatment• Ia: meta-analysis of RCTs • Ib: at least one RCT• IIa-b: at least one
controlled or exptl. study (no R)
• III: descriptive studies• IV: expert committee
reports, opinions and/or clinical experience
Observational• I: large representative
population samples• II: small, limited samples• III: non-representative
surveys, case reports• IV: expert committee reports,
opinions and/or clinical experience

Outline
• Fundamentals of patient management– Diagnosis – Access to services and the safety of the patient
and others – Enhanced care
• Treatment of different phases of bipolar illness – Acute Manic or Mixed Episodes – Acute Depressive episode – Long term treatment – Treatment in special situations

Diagnosis is good (S)
• Mania and mixed states
• Hypomania should be used as defined inDSM IV = elated states without significant functional impairment
• Consider the identification of the core symptoms of mania or depression against a check list as in DSM IV to improve confidence in, and the reliability of diagnosis

Early diagnosis
• Only reliable after a clear-cut episode of mania
• Too soon: Bipolar symptoms such as irritability or aggression may appear, with the benefit of hindsight, to be misdiagnosed by clinicians when a patient is first seen
• Too late: In the presence of mood elevation, disturbed behaviour should not be attributed solely to personality problems or situational disturbance (B)

Differential diagnosis
• Stimulant drugs may mimic manic symptoms (II) – A drug-induced psychosis should wane with the clearance of
the offending drug (II) – L-Dopa and corticosteroids are the most common prescribed
medications associated with secondary mania (I)
• More commonly, drug and/or alcohol misuse is co-morbid with manic or depressive mood change (I)
– The mood state will significantly outlast the drugged state and a diagnosis of bipolar disorder should be made (S)
– Significant alcohol or substance misuse worsens the outlook for bipolar patients (I) and merits assessment and treatment in its own right (A)

Outline
• Fundamentals of patient management
– Diagnosis
– Access to services and the safety of the patient and others
– Enhanced care
• Treatment of different phases of bipolar illness
– Acute manic or mixed episodes
– Acute depressive episode
– Long term treatment
– Treatment in special situations

Enhanced care
• Education
• Promote awareness of stressors, sleep disturbance and early signs of relapse, and regular patterns of activity
– Sleep disruption is often the final common pathway triggering manic episodes (II)
• Promote regular patterns of daily activities (D)
• Since alcohol and substance misuse are associated with a poor outcome, they require assessment, and appropriate advice and treatment (A)

Enhanced care
• Enhanced treatment adherence
• Optimal patterns of activity
• Enhanced awareness of prodromes
• Action plan
– Self-medication
– Behaviour
– Advice

Outline
• Fundamentals of patient management– Diagnosis – Access to services and the safety of the
patient and others – Enhanced care
• Treatment of different phases of bipolar illness – Acute manic or mixed episodes – Acute depressive episode – Long term treatment – Treatment in special situations

Traitement des differentes phases
du trouble bipolaire
• Les AMM sont faites pour limiter l’action des firmes pharmaceutiques, PAS celle des cliniciens. Préconiser, ‘Hors AMM’ des médicaments est implicite dans quelques recommendations
• Cpendant, demandez l’avis d’un expert si vous n’êtes pas sûr de l’efficacité ou de l’inocuité d’un médicament isolé ou de son usage en combination (S)

Manie aigüe ou états mixtes
Pour les patients qui n’ont pas de traitement à long terme pour le trouble bipolaire
• Administration orale d’un neuroleptiqueou du depakote
• Les plus basses doses nécessaires doivent être employées (A). N’augmentez pas la dose de neuroleptiques simplement pout obtenir un effet sedatif (S)

Choix d’un neuroleptique
• Les neuroleptiques atypiques doivent être envisagés, ayant moins d’effets secondaires à court terme et leur efficacité pour traiter la phase d’exaltation étant confirmée (A)

‘Valproate’
• Sodium Valproate (Epilim)
• Divalproex = Valproate semisodium = Divalproate
• DEPAKOTE = Valproate semisodium contains a higher fraction (about 30%) of the valproate moiety
• For hospitalised patients divalproate semisodium: 750 mg on day 1 and 20mg/kg+ on day 2.Levels of 50–125 microg/mL

For less ill manic patients
• Valproate, lithium or carbamazepine may be considered as a short term treatment (A)
• To promote sleep for agitated overactive patients in the short term, consider adjunctive treatment with a benzodiazepine such as clonazepam or lorazepam (B)

If symptoms uncontrolledand/or mania is very
severe
• Add another first-line medicine
– Consider the combination of lithium or valproate with an antipsychotic (A)
– Consider clozapine in more refractory illness (B)
– Electro convulsive therapy (ECT) may be considered for manic patients who are severely ill and/or whose mania is treatment resistant and patients with severe mania during pregnancy (C)

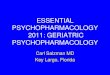
YMRS score (USA study):Double-blind and open-label periods
*p<0.05**p<0.01 risperidone vs placebo
All scores are the mean change from study entry. MS=mood stabiliser
0
10
20
30
YM
RS
sco
re
Entry Week1
Week2
Week3
Endpoint(LOCF)
Week1
Week2
Week6
Week10
Endpoint(LOCF)
Double-blind Open-label(all patients received risperidone)
*
* **
Placebo + MSRisperidone + MSHaloperidol + MS
Sachs et al., Am J Psych 2002

Acute depression
• Treat with an antidepressant and an anti-manic drug (e.g. lithium, valproate or an antipsychotic) together (B)
• Antidepressant monotherapy is not recommended for patients with a history of mania (B)
• Consider ECT for patients with high suicidal risk, psychosis, severe depression during pregnancy or life-threatening inanition (A)

Traitement à long terme
• Envisagez un traitement à long terme après un seul épisode maniaque sévère : prévenir une rechute rapide conduit à une évolution moins sévère de la maladie (D)
• Considerer un traitement élargi comprenant un soutien psycho-social (A)
• Quand un patient est stabilisé, il doit être fermement avisé que le traitement doit être continué à vie, les risques de rechute restant élevés (A)

Choix d’un traitement à long terme
• Le lithium comme monothérapie initiale (A)(Ia)
• Si le lithium est inefficace ou mal supporté:– Valproate previent probablement les récidives
maniaques et dépressives (Ia) – Olanzapine (Zyprexa) previent plus les
récidives maniaques que les dépressives (Ib)– Carbamazepine (tegretol)– Lamotrigine (lamictal)

If the patient fails monotherapy
• Consider long term combination treatment (C)– Where the burden is mania, combine
predominantly anti-manic agents (e.g. lithium, valproate, an antipsychotic) (D)
– Where the burden is depressive, lamotrigine oran antidepressant may be more appropriate in combination with an anti-manic long-term agent (D)
• Consider clozapine in treatment resistant patients (C)

Trial or error
• Need for pragmatic clinical trials
• Balance– Compares lithium, valproate semisodium
and their combination– Any bipolar patient eligible for long term
treatment– Simple records, telephone randomization– Open treatment

BALANCE: current networkBALANCE: current network
• 54 active investigators• 200 registered investigators• Most active investigators have recruited 1 patient
• Increase to 5/6 over next 2 years• Convert “registered” to “active”• Should result in 500+ participants over next 2
years
• www.psychiatry.ox.ac.uk/balance

Arrêt d’un traitement àlong terme
• Après arrêt du traitement, le risque de rechute reste élevé, même après des années de stabilisation (I)
• L’arrêt d’un médicament doit normallement être étalée sur au moins 2 semaines et si possible plus longtemps (A and S). Une rechute rapide en manie est le premier risque d’un arrêt abrupt du lithium (Ia)
• L’arrêt d’un traitement médicamentaux ne doit pas signifier l’arrêt des services aux patients (S)

Conclusions
• La plupart des traitements sont basés sur des preuves issues d’essais cliniques
• La stratégie détaillée reste pragmatique
• Des soins élargis à des éducation psycho-sociales améliore les résultats
• La participation aux essais cliniques améliore la santé du patient

Thanks• Ian Anderson• Jules Angst • David Baldwin• Zubin Bhagwagar• John Cookson • Nicol Ferrier• Sophia Frangou• John Geddes• Heinz Grunze• Peter Haddad• Amanda Harris • Neil Hunt• Robin Jacoby• Peter Jones• Rob Kerwin
• Dominic Lam • Anne Lingford-Hughes • Stuart Montgomery • Richard Morris• Willem Nolen• Gary Sachs• Barbara Sahakian • Jan Scott • Allan Young
Observers from Royal College of PsychiatrySpecial Interest Group• Thomas Barnes• Vivienne Curtis
Observers from AstraZeneca,Bristol Myers Squibb, GSK, Janssen-Cilag, Lilly, sanofi-Synthelabo