Embed Size (px)
Citation preview
Balazs Halmos, M.D.
Division of Hematology/Oncology
Columbia University Medical Center
Eli-Lilly
Pfizer
Astellas
Daiichi-Sankyo
Oncothyreon
Astex
Astra-Zeneca
Bristol-Myers-Squibb
Novartis
Roche
Boehringer-Ingelheim
Merck
I will discuss off-label use of compounds
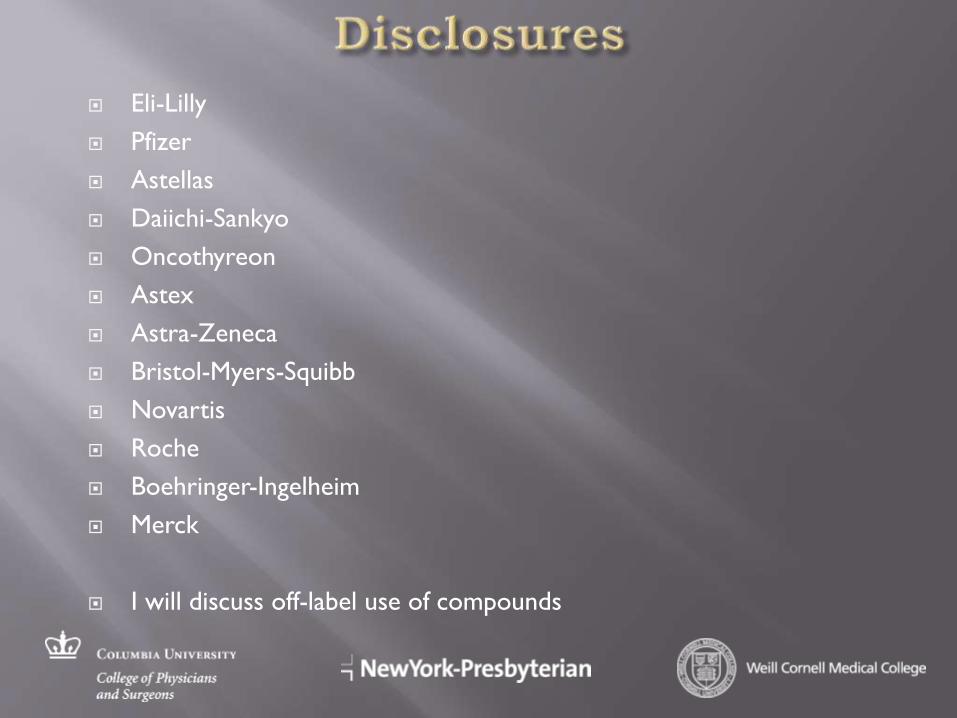
Member of HER family of cell surface TK receptors
Downstream signaling via Ras/MAPK, STAT and PI3K/AKT pathways
Present at high levels in many cancers, including majority of all lung cancers
• Drugs (EGFR TKI- tyrosine kinase inhibitor:
gefitinib, erlotinib) that bind to its “active”
pocket and thereby block its function had been
developed 2nd or 3rd-line therapy
• JBR21 study of erlotinib vs placebo in 2nd/3rd
line
• Median survival 6.7 vs 4.7 months
• 8.8% response rate
• Benefit seemed to be modest but across the board
• Main side effects- skin rash, diarrhea, rare incidence of
pneumonitis, liver dysfunction
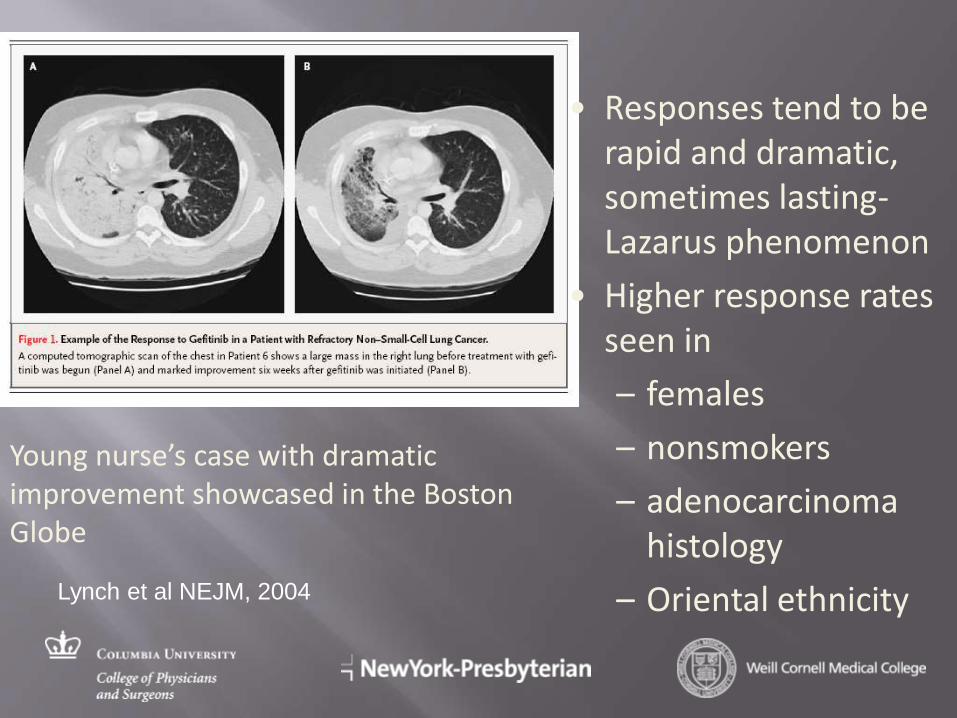
Young nurse’s case with dramatic improvement showcased in the Boston Globe
• Responses tend to be rapid and dramatic, sometimes lasting- Lazarus phenomenon
• Higher response rates seen in
– females
– nonsmokers
– adenocarcinoma histology
– Oriental ethnicity
Lynch et al NEJM, 2004
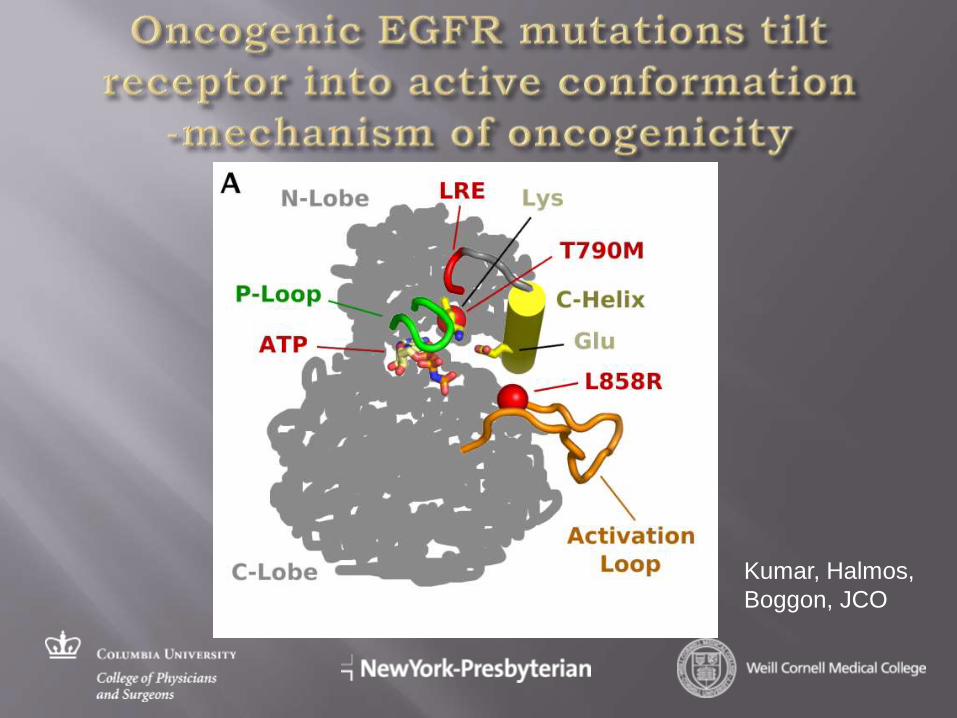
Kumar, Halmos,
Boggon, JCO
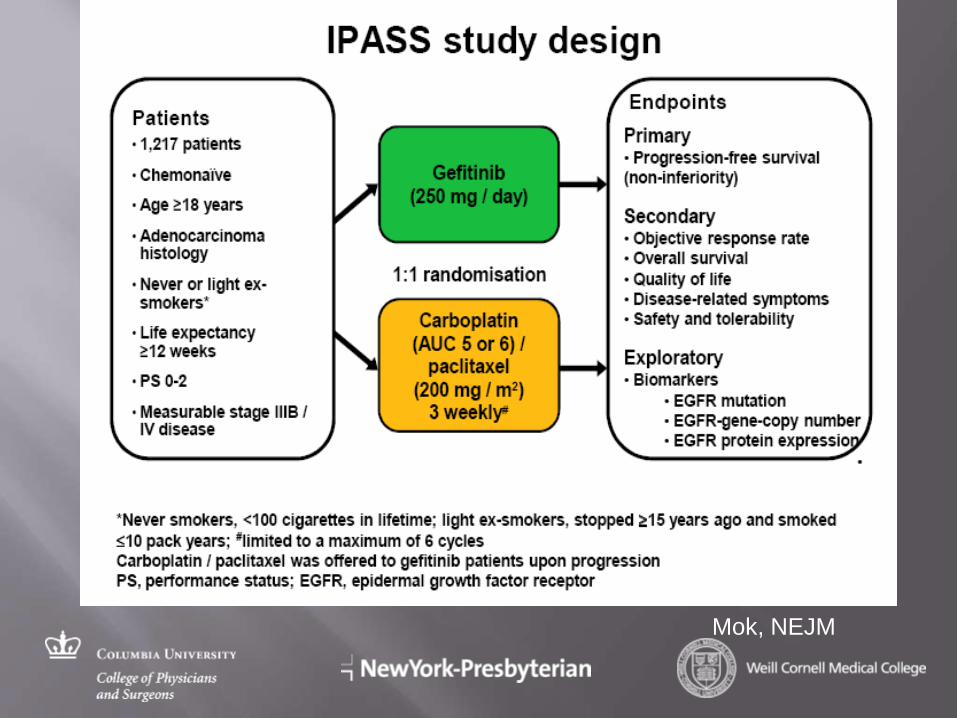
Mok, NEJM
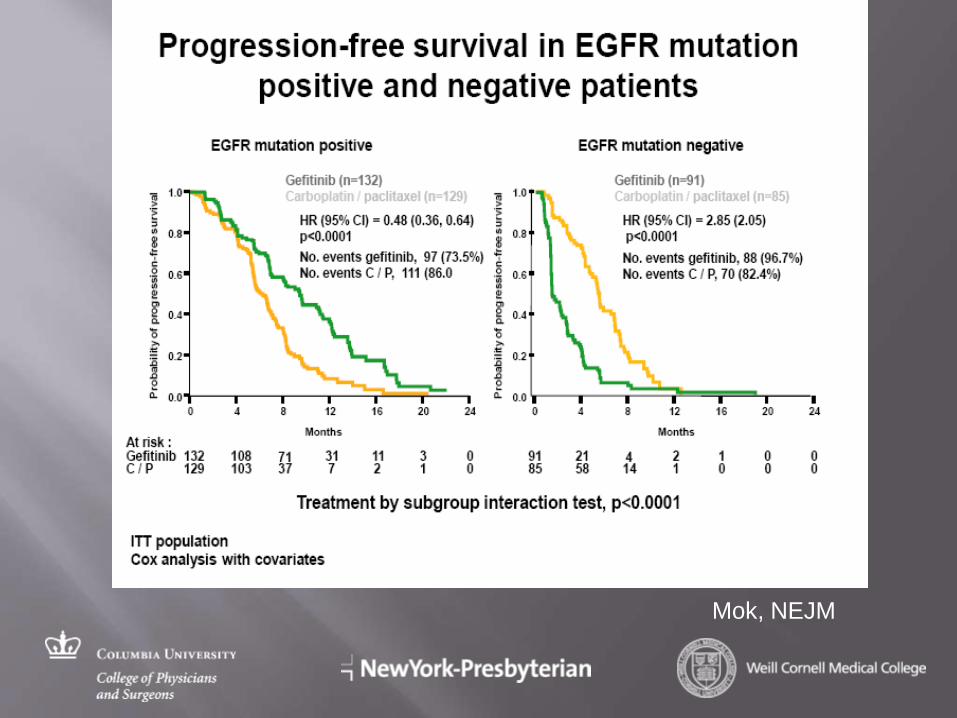
Mok, NEJM
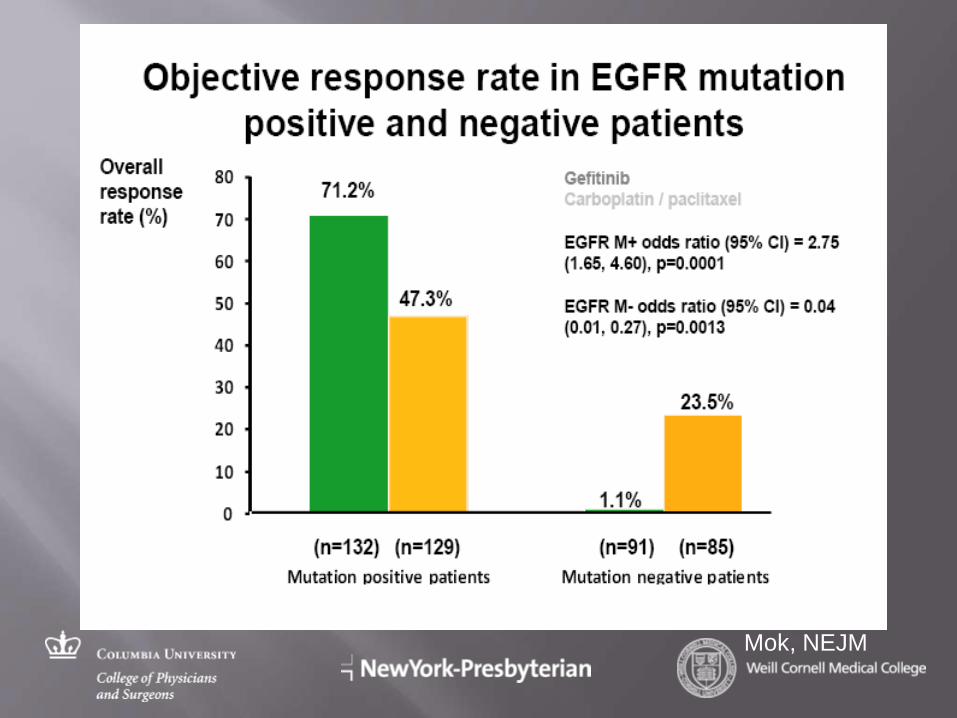
Mok, NEJM
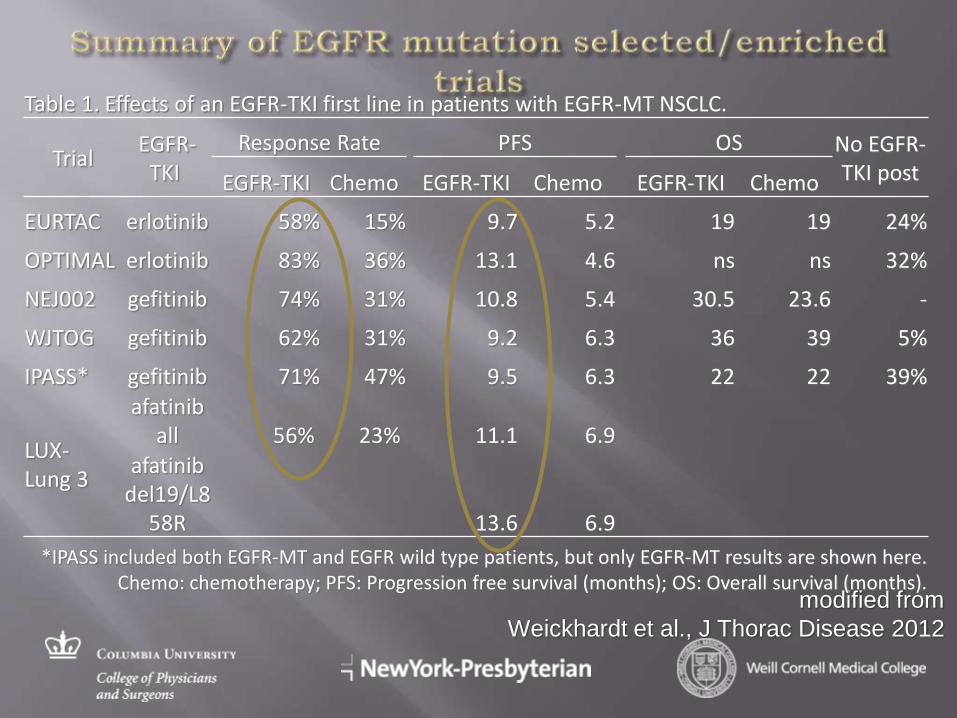
modified from
Weickhardt et al., J Thorac Disease 2012
Table 1. Effects of an EGFR-TKI first line in patients with EGFR-MT NSCLC.
Trial EGFR-
TKI
Response Rate PFS OS No EGFR-TKI post EGFR-TKI Chemo EGFR-TKI Chemo EGFR-TKI Chemo
EURTAC erlotinib 58% 15% 9.7 5.2 19 19 24%
OPTIMAL erlotinib 83% 36% 13.1 4.6 ns ns 32%
NEJ002 gefitinib 74% 31% 10.8 5.4 30.5 23.6 -
WJTOG gefitinib 62% 31% 9.2 6.3 36 39 5%
IPASS* gefitinib 71% 47% 9.5 6.3 22 22 39%
LUX- Lung 3
afatinib all 56% 23% 11.1 6.9
afatinib del19/L8
58R 13.6 6.9
*IPASS included both EGFR-MT and EGFR wild type patients, but only EGFR-MT results are shown here. Chemo: chemotherapy; PFS: Progression free survival (months); OS: Overall survival (months).
OS is 18.8 months with gefitinib and 17.4 months with doublet chemotherapy
Median OS for EGFR mutant pts- 21 months- same with gefinitib vs chemo
52% of pts in chemo arm received gefitinib
Major reasons why a drug that leads to an 80%+ RR does not yield a survival benefit
Cross-over
Development of acquired resistance
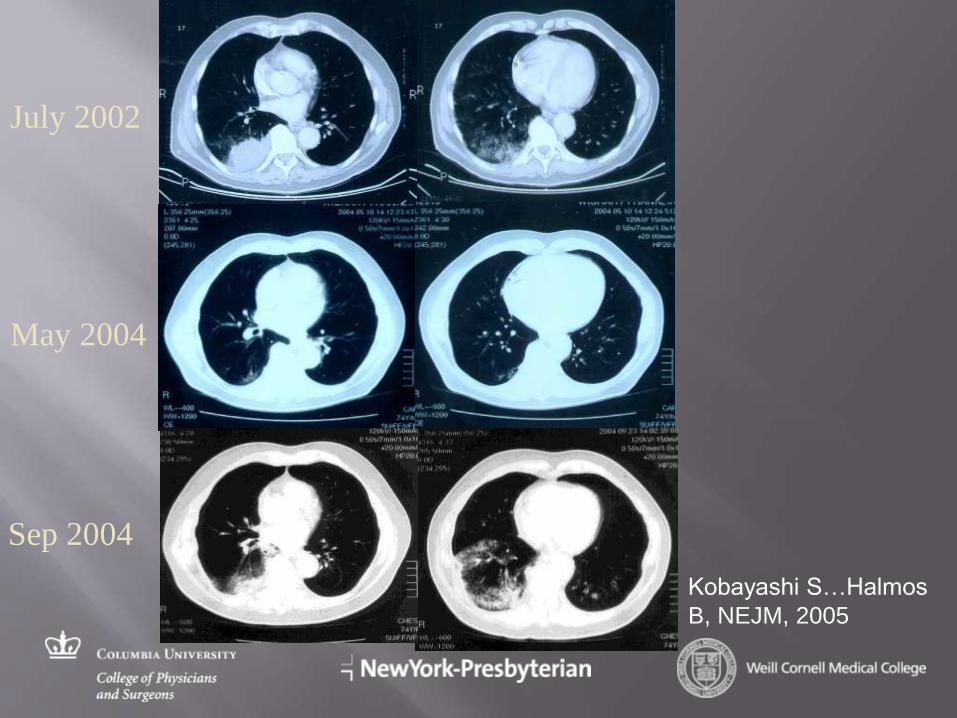
July 2002
May 2004
Sep 2004
Kobayashi S…Halmos
B, NEJM, 2005
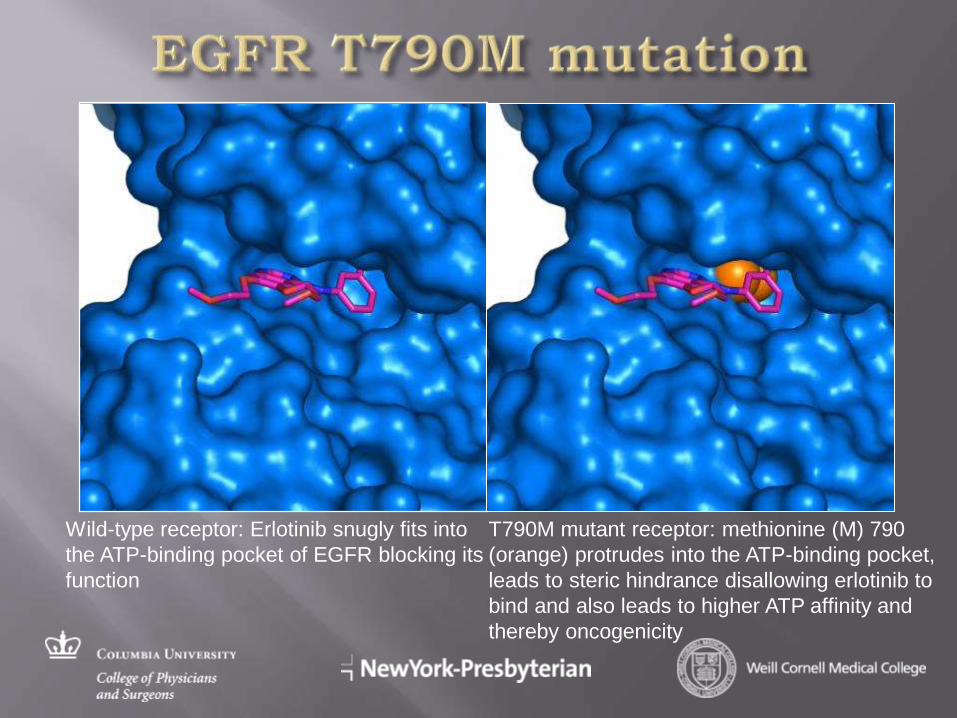
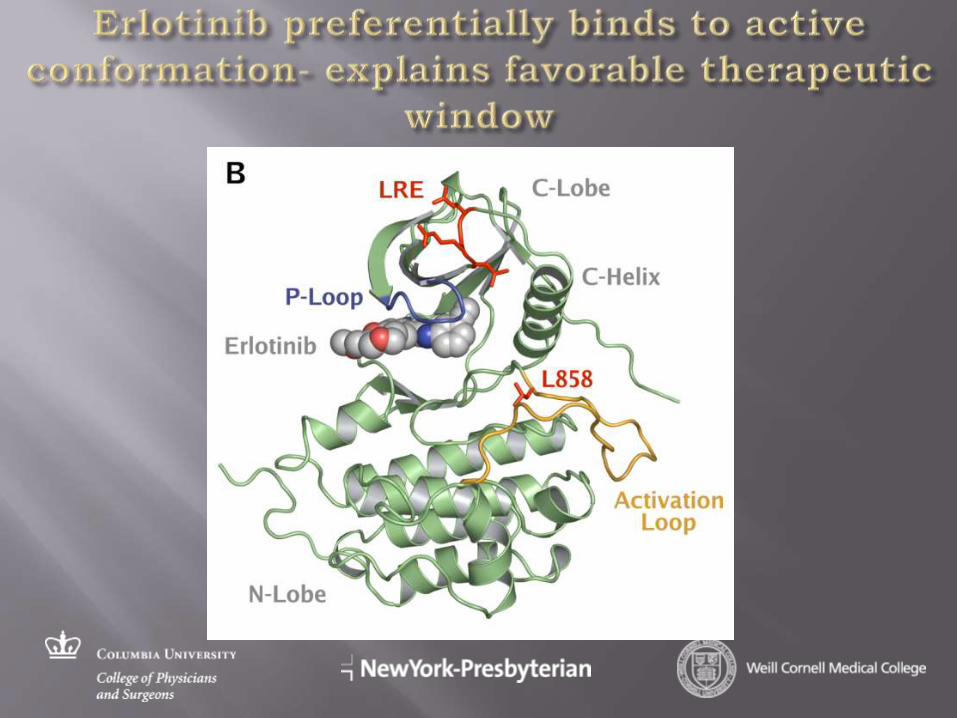
Wild-type receptor: Erlotinib snugly fits into
the ATP-binding pocket of EGFR blocking its
function
T790M mutant receptor: methionine (M) 790
(orange) protrudes into the ATP-binding pocket,
leads to steric hindrance disallowing erlotinib to
bind and also leads to higher ATP affinity and
thereby oncogenicity
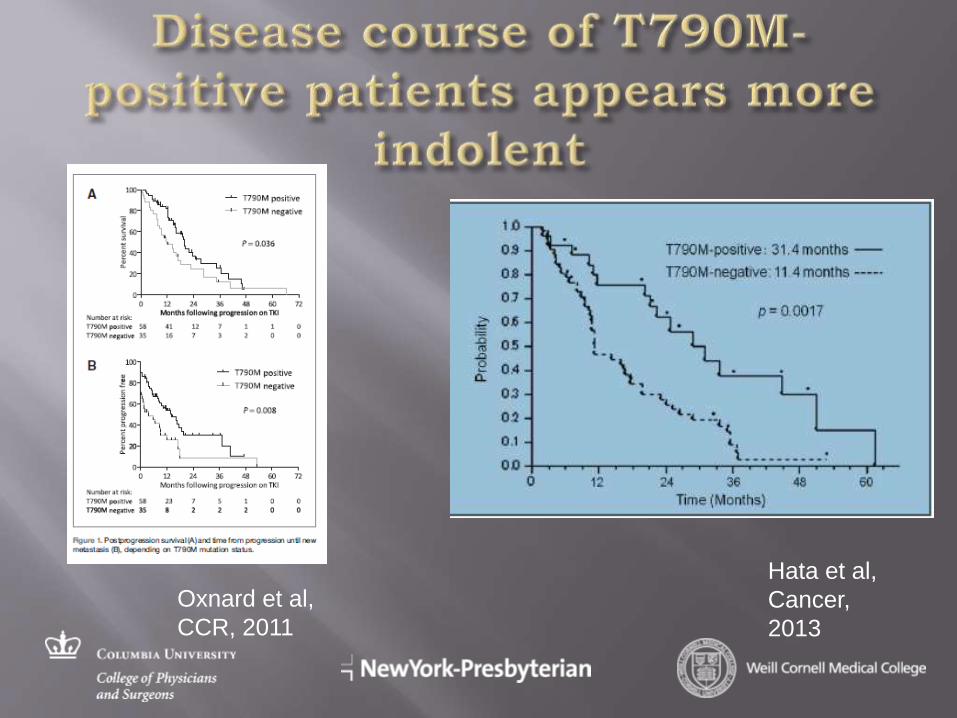
Hata et al,
Cancer,
2013
Oxnard et al,
CCR, 2011
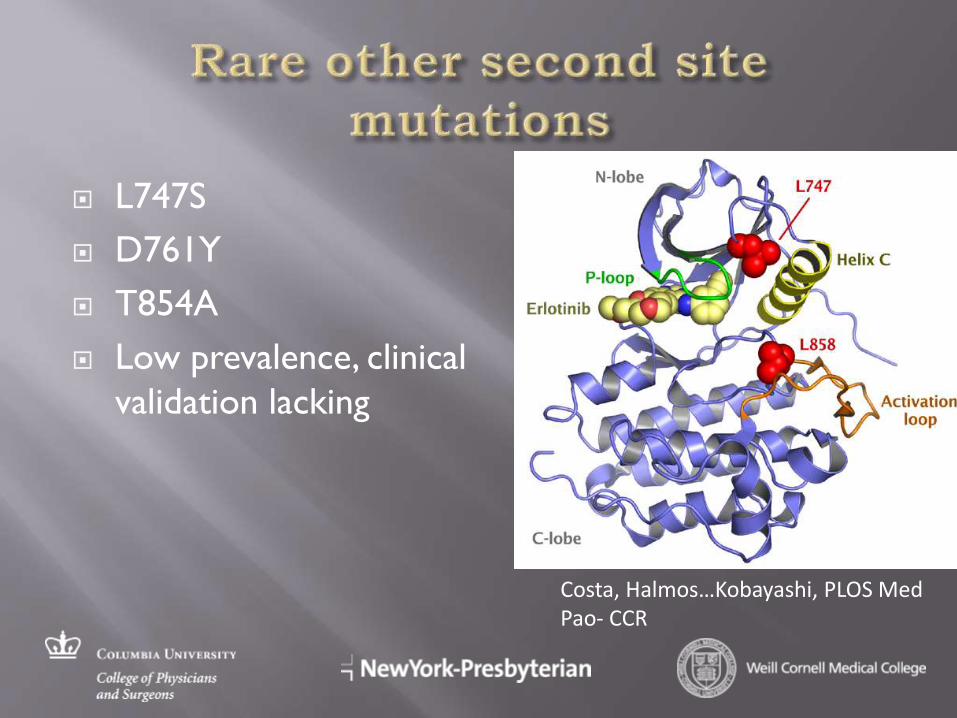
L747S
D761Y
T854A
Low prevalence, clinical
validation lacking
Costa, Halmos…Kobayashi, PLOS Med Pao- CCR
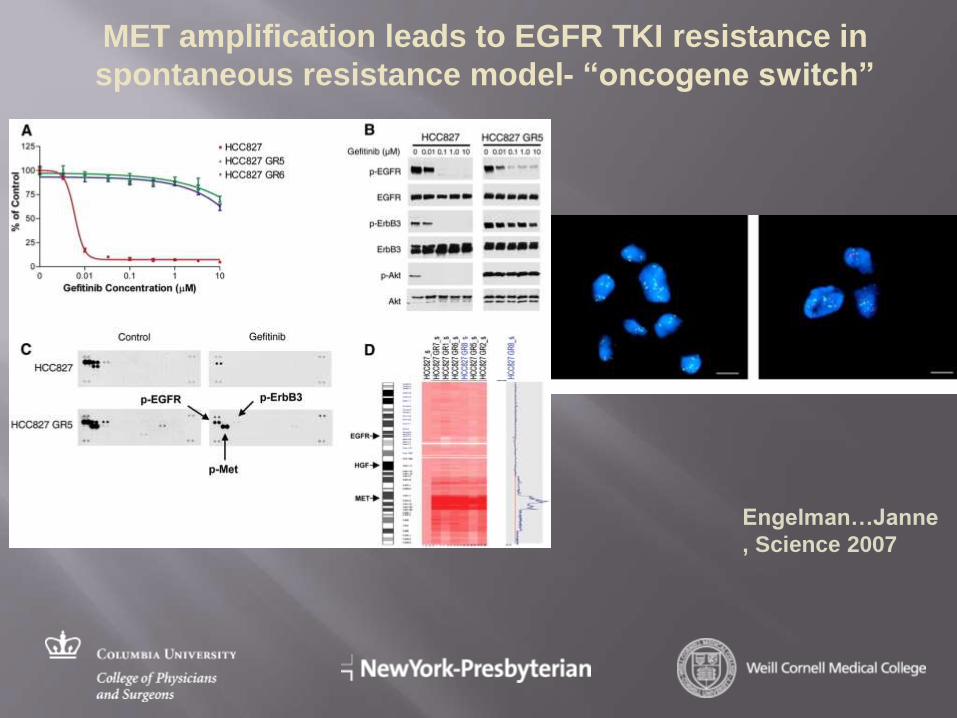
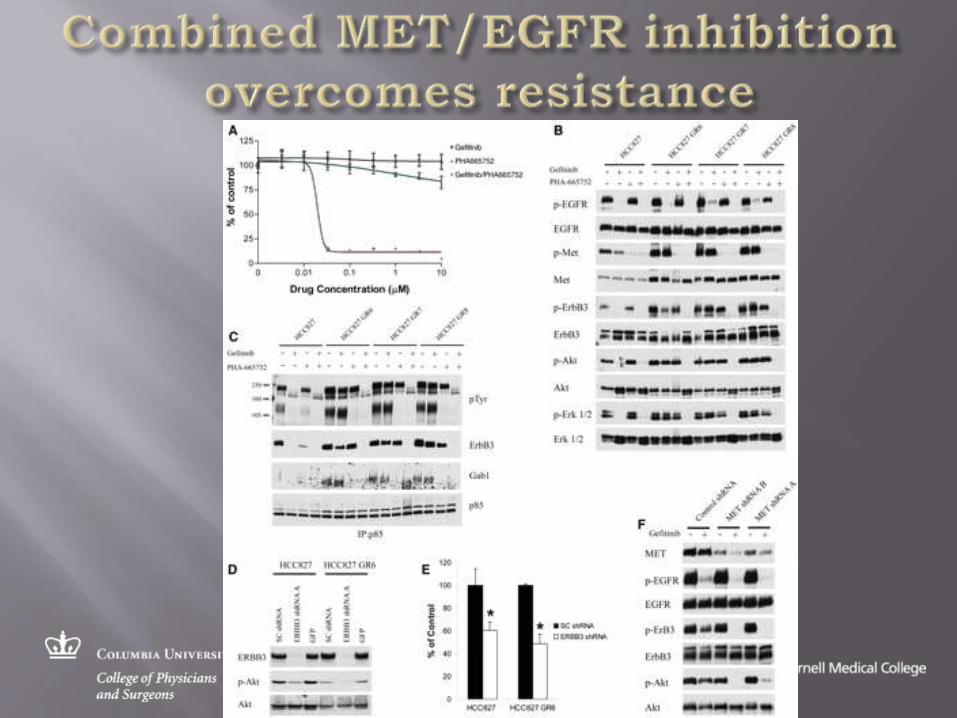
MET amplification leads to EGFR TKI resistance in
spontaneous resistance model- “oncogene switch”
Engelman…Janne
, Science 2007
37 patients with acquired resistance with repeated biopsies
Phenotype change from NSCLC to SCLC in 14%- histological transformation
Adaptive change- EMT noted in some samples (high vimentin, low E-cadherin)
Original EGFR gene mutation retained in all (in SCLC as well)
49% with EGFR T790M, 5% PI3K mutations, 5% MET amplification
3 of 4 pts treated with SCLC-like regimen responded Sequist, 2011
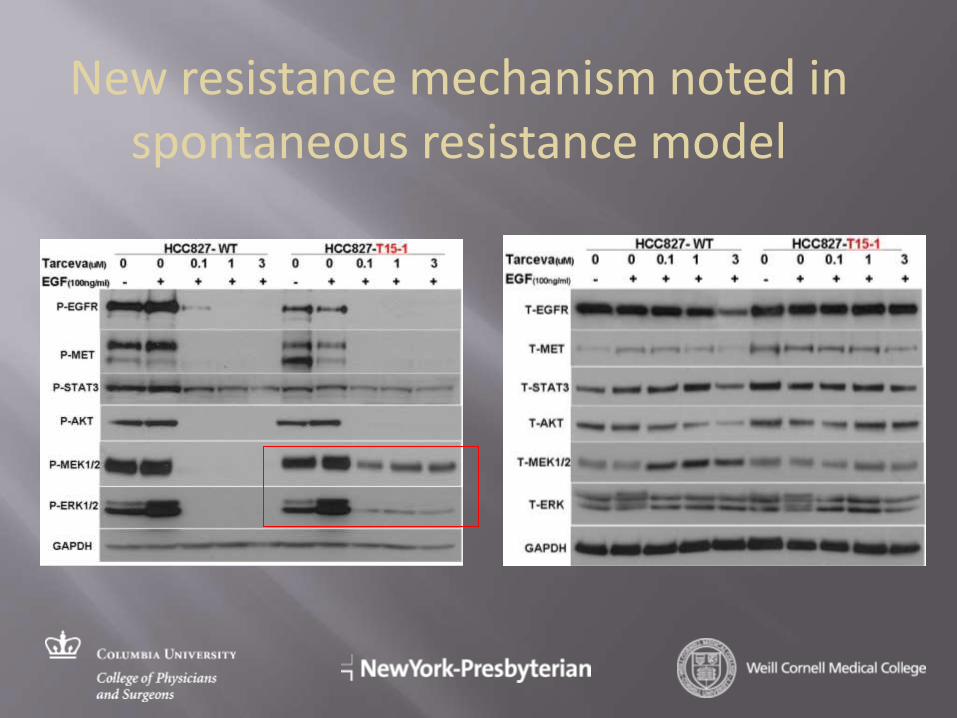
New resistance mechanism noted in spontaneous resistance model
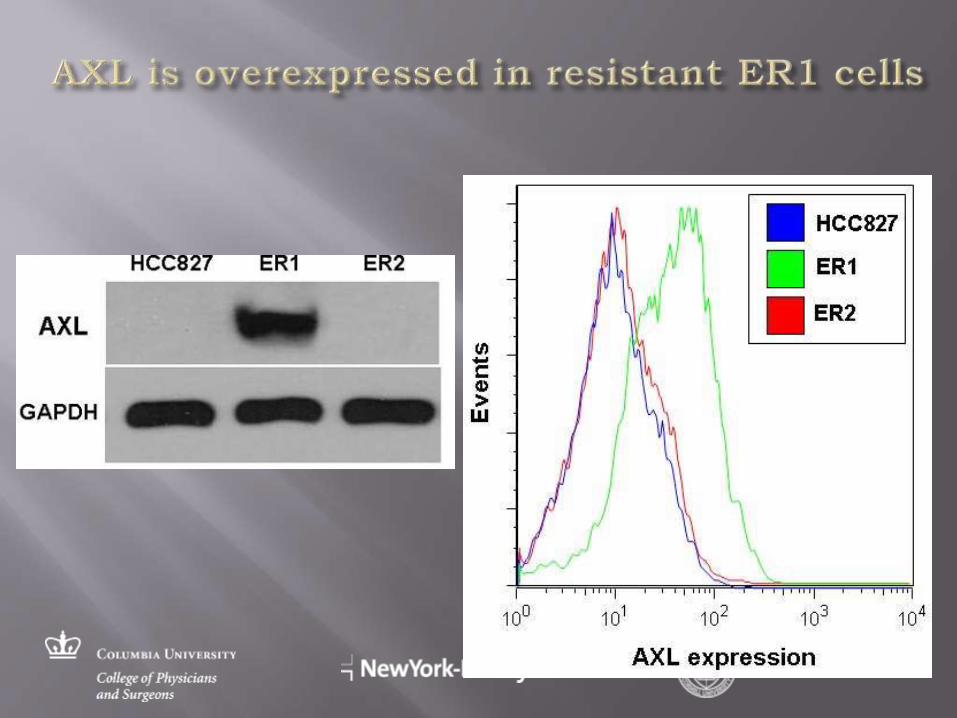
HCC827
ER1
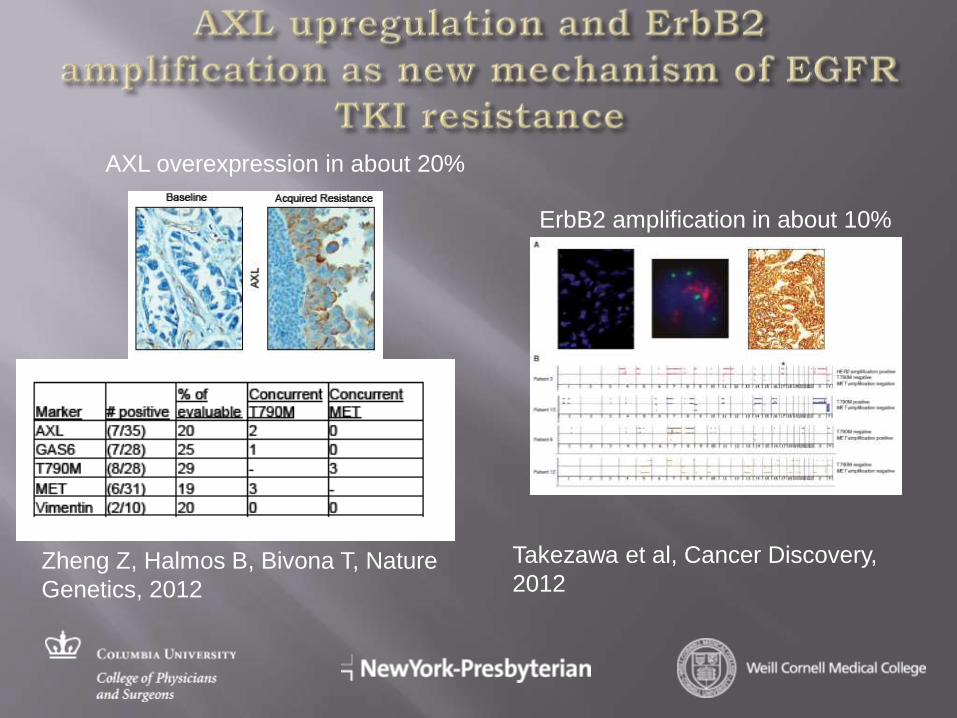
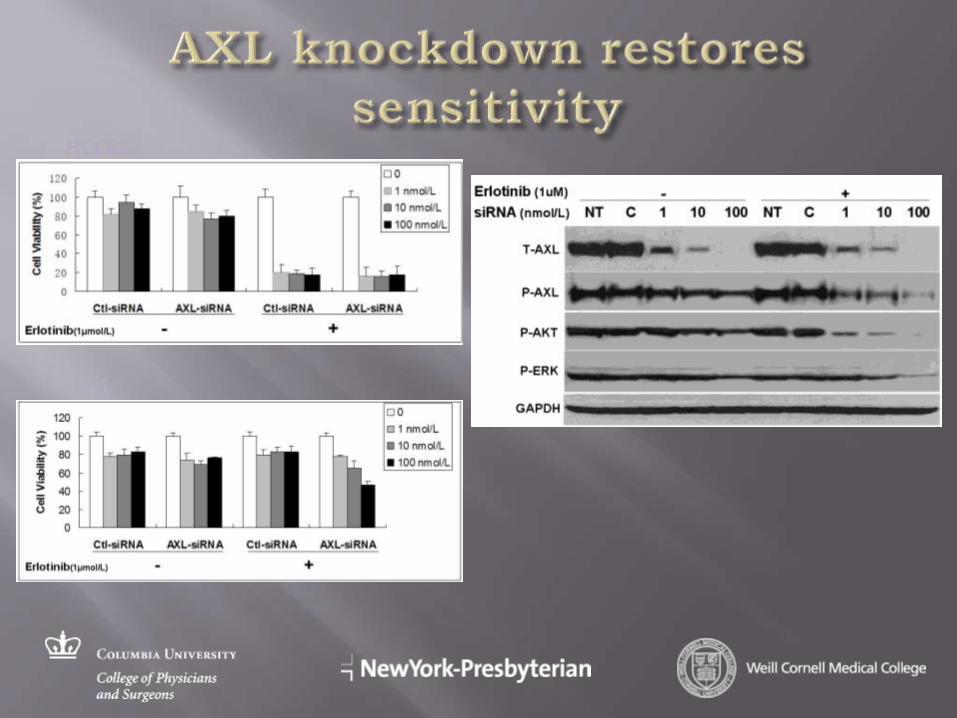
Zheng Z, Halmos B, Bivona T, Nature
Genetics, 2012
ErbB2 amplification in about 10%
Takezawa et al, Cancer Discovery,
2012
AXL overexpression in about 20%
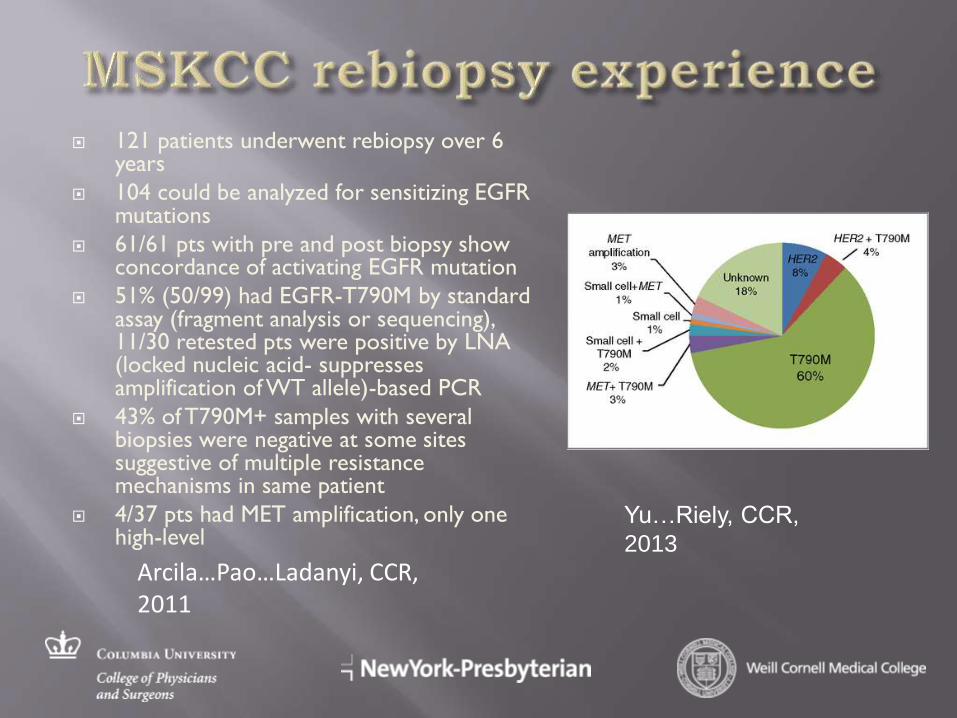
121 patients underwent rebiopsy over 6 years
104 could be analyzed for sensitizing EGFR mutations
61/61 pts with pre and post biopsy show concordance of activating EGFR mutation
51% (50/99) had EGFR-T790M by standard assay (fragment analysis or sequencing), 11/30 retested pts were positive by LNA (locked nucleic acid- suppresses amplification of WT allele)-based PCR
43% of T790M+ samples with several biopsies were negative at some sites suggestive of multiple resistance mechanisms in same patient
4/37 pts had MET amplification, only one high-level
Arcila…Pao…Ladanyi, CCR, 2011
Yu…Riely, CCR,
2013
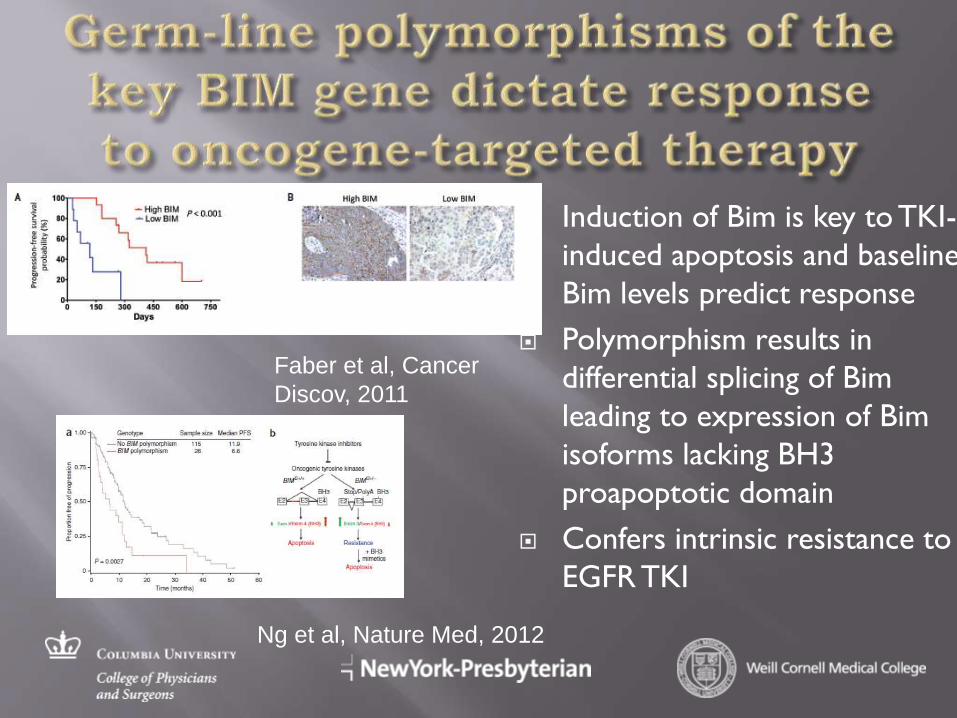
Induction of Bim is key to TKI-
induced apoptosis and baseline
Bim levels predict response
Polymorphism results in
differential splicing of Bim
leading to expression of Bim
isoforms lacking BH3
proapoptotic domain
Confers intrinsic resistance to
EGFR TKI
Faber et al, Cancer
Discov, 2011
Ng et al, Nature Med, 2012
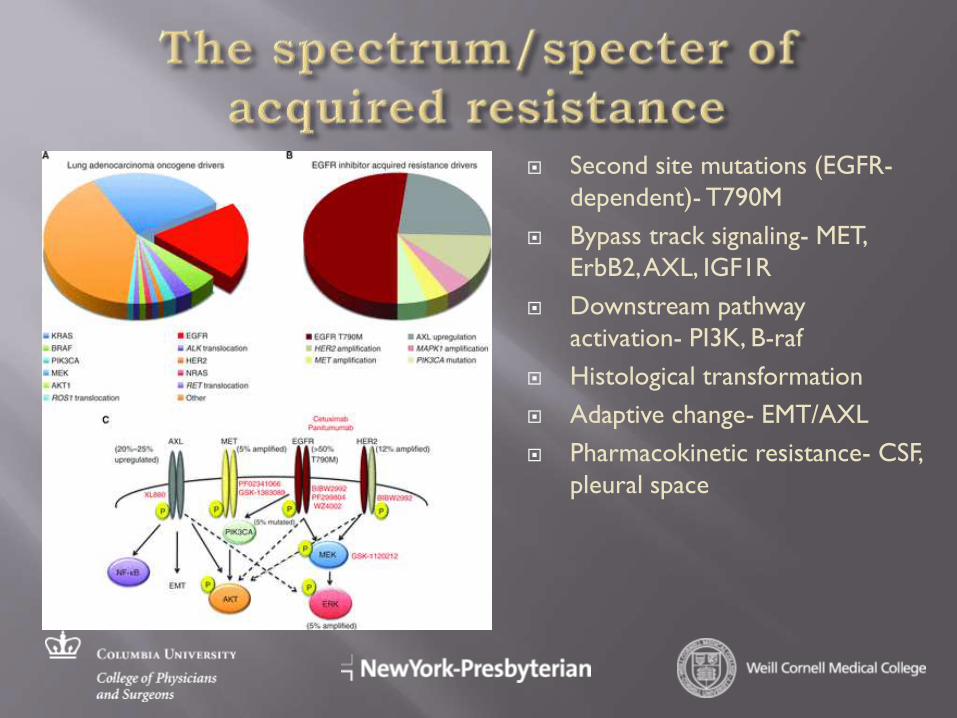
Second site mutations (EGFR-
dependent)- T790M
Bypass track signaling- MET,
ErbB2, AXL, IGF1R
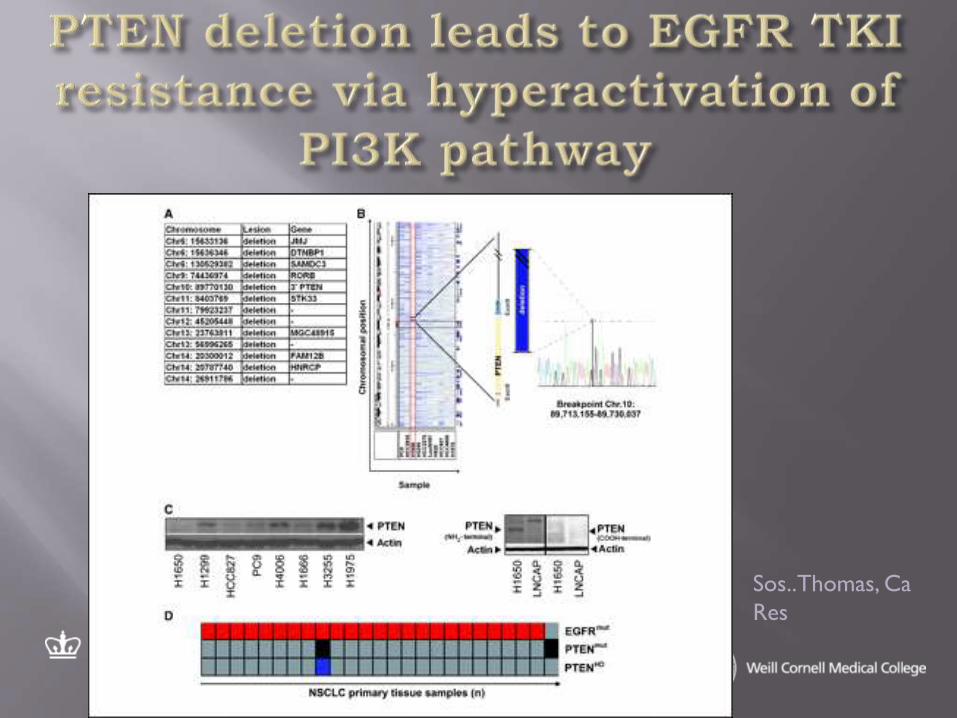
Downstream pathway
activation- PI3K, B-raf
Histological transformation
Adaptive change- EMT/AXL
Pharmacokinetic resistance- CSF,
pleural space
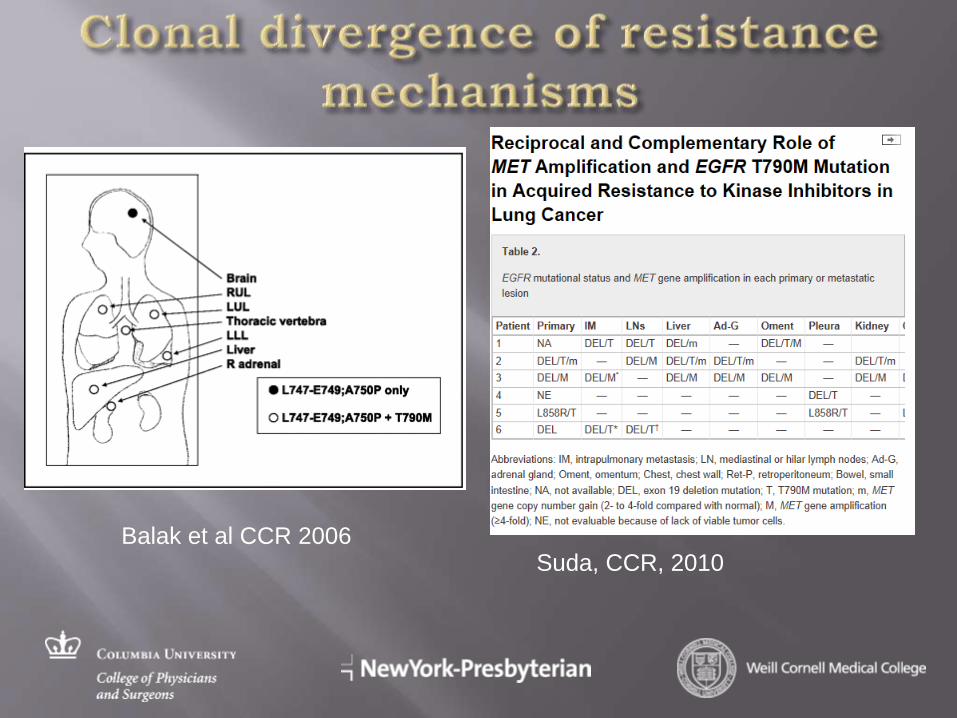
Suda, CCR, 2010 Balak et al CCR 2006

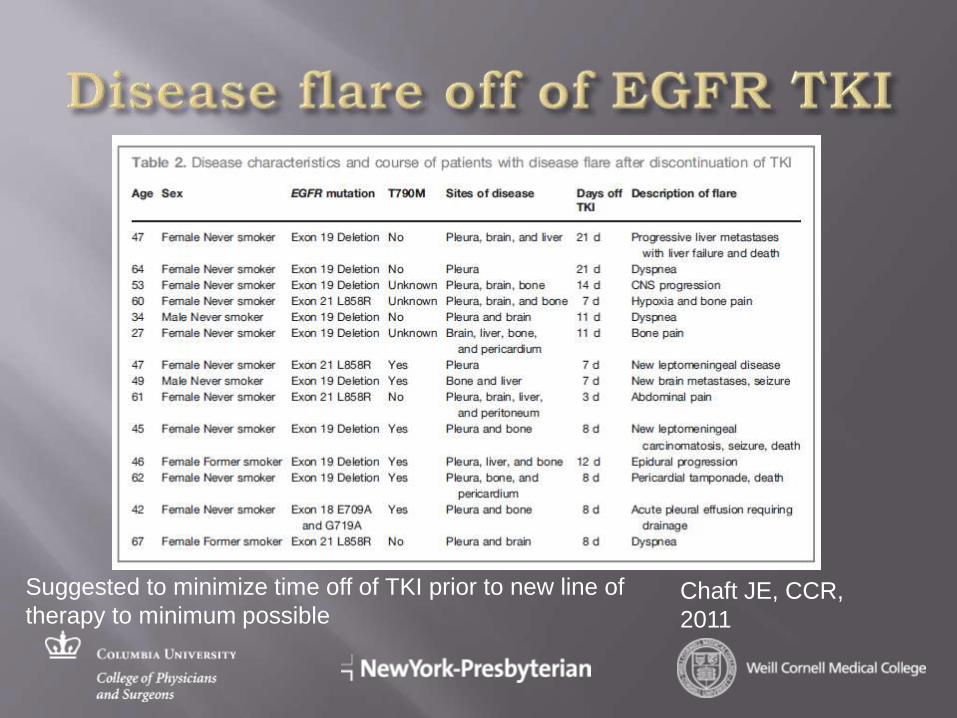
Chaft JE, CCR,
2011
Suggested to minimize time off of TKI prior to new line of
therapy to minimum possible
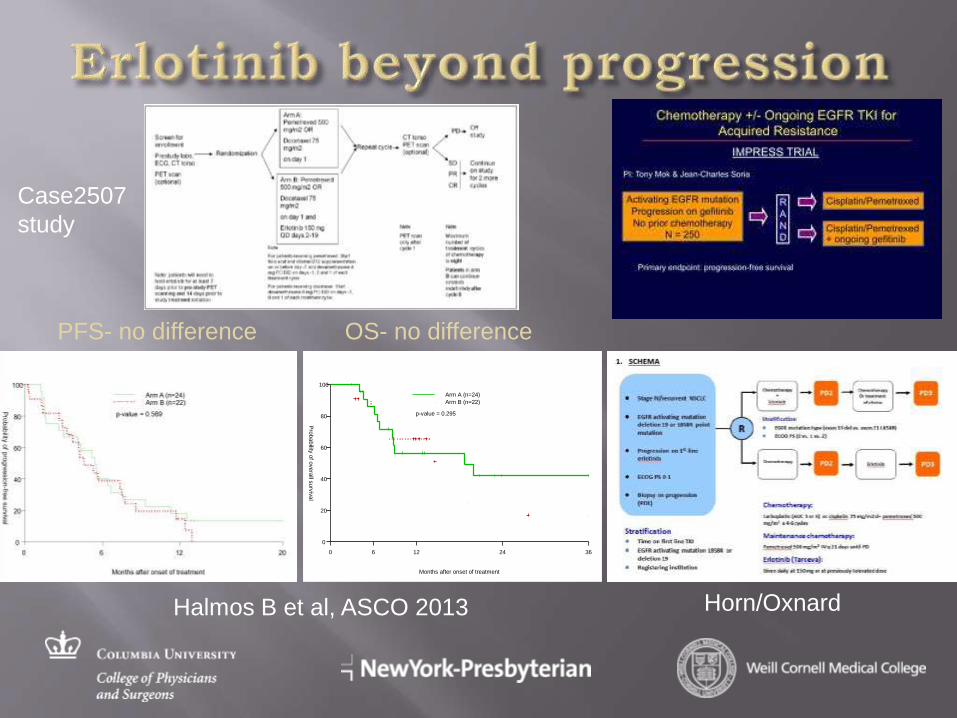
Months after onset of treatment
Pro
ba
bility
of o
ve
rall s
urv
iva
l
0 6 12 24 36
0
20
40
60
80
100
Arm A (n=24)
Arm B (n=22)
p-value = 0.295
PFS- no difference OS- no difference
Case2507
study
Halmos B et al, ASCO 2013 Horn/Oxnard
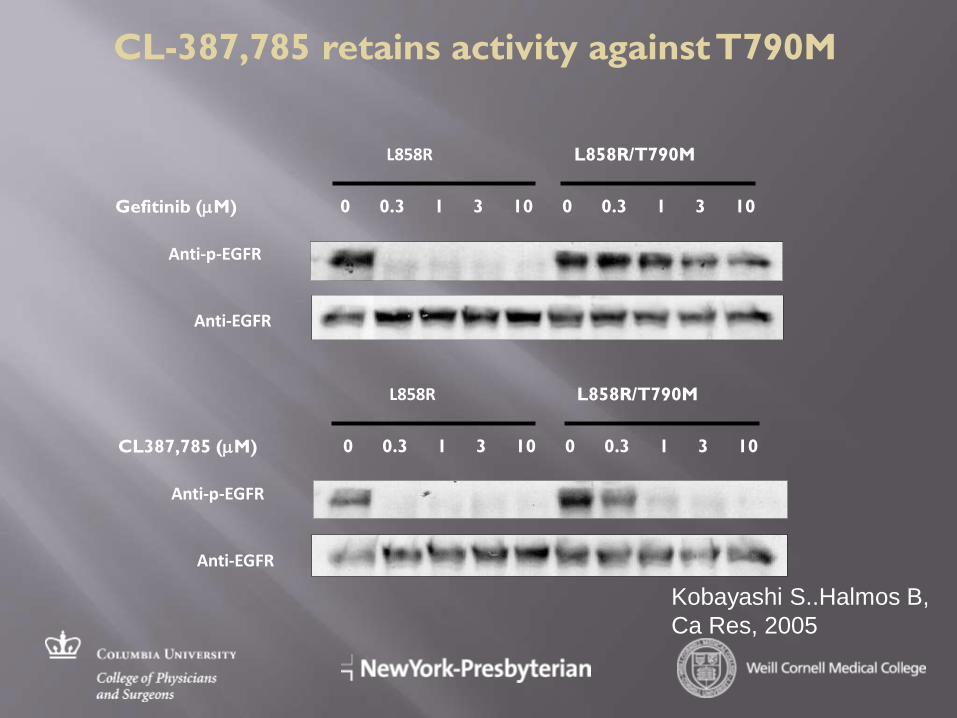
Anti-p-EGFR
Anti-EGFR
0 0.3 1 3 10 Gefitinib (mM)
L858R L858R/T790M
0 0.3 1 3 10
Anti-p-EGFR
Anti-EGFR
0 0.3 1 3 10 CL387,785 (mM)
L858R L858R/T790M
0 0.3 1 3 10
CL-387,785 retains activity against T790M
Kobayashi S..Halmos B,
Ca Res, 2005
• Irreversibly bind EGFR C797 residue- ATP-competitive inhibitors
• Most also inhibit ErbB2/ErbB4 by binding to critical Cysteine residue near ATP-binding site
• Potential advantage is that new synthesis of EGFR/ErbB2 is required for function
• Partially capable of overcoming T790M-mediated resistance in vitro
• Also in vitro activity against exon 20 mutations of EGFR and ErbB2
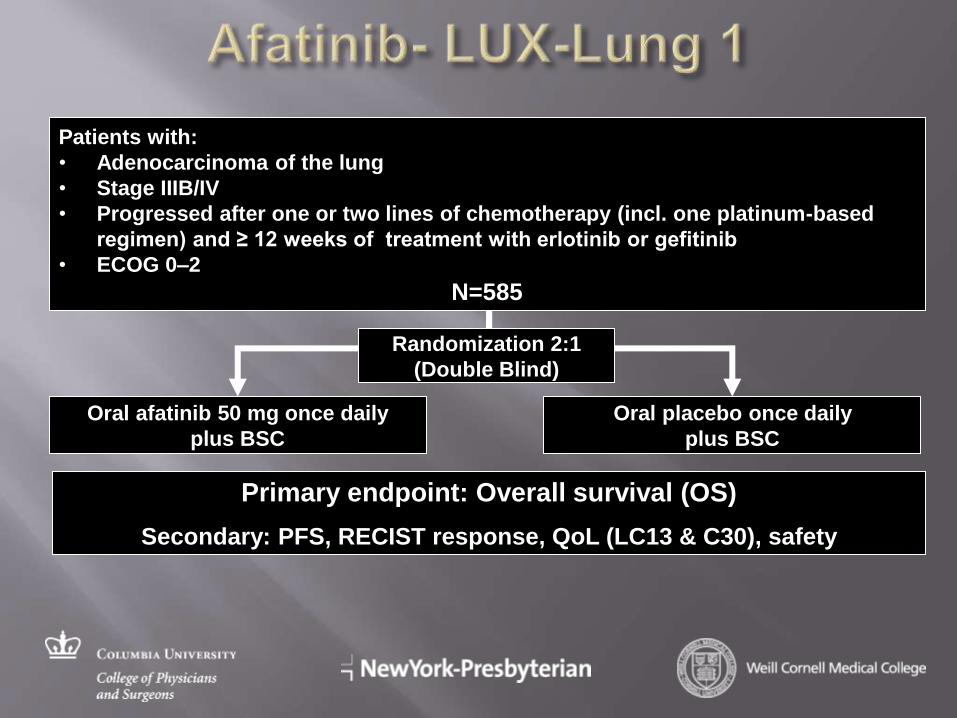
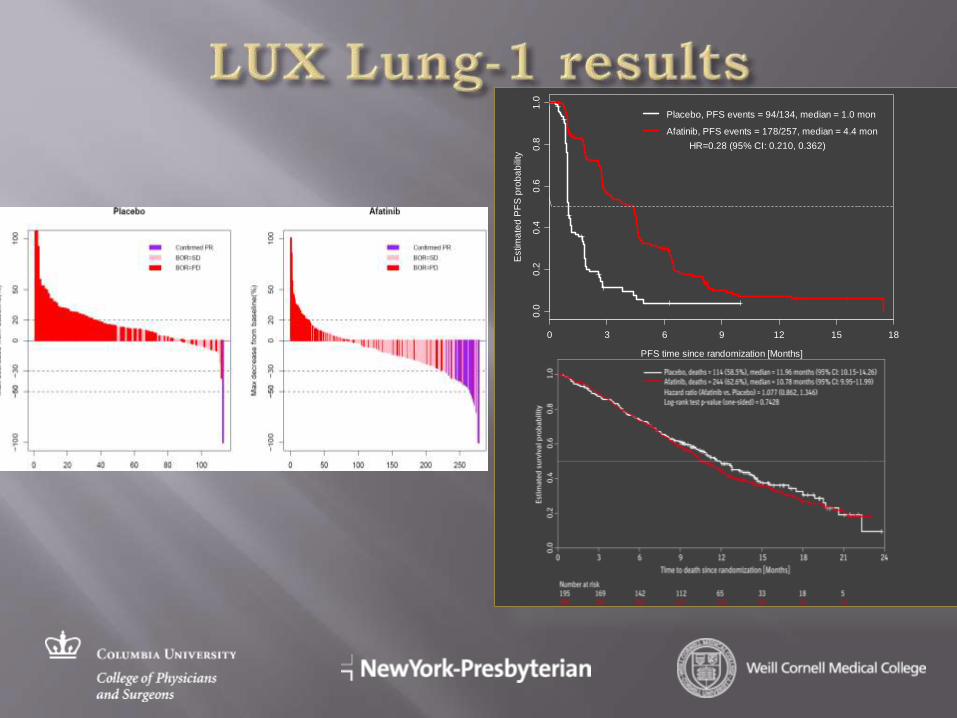
Randomization 2:1
(Double Blind)
Oral afatinib 50 mg once daily
plus BSC
Oral placebo once daily
plus BSC
Primary endpoint: Overall survival (OS)
Secondary: PFS, RECIST response, QoL (LC13 & C30), safety
Patients with:
• Adenocarcinoma of the lung
• Stage IIIB/IV
• Progressed after one or two lines of chemotherapy (incl. one platinum-based
regimen) and ≥ 12 weeks of treatment with erlotinib or gefitinib
• ECOG 0–2
N=585

Jackman, JCO 2010
0.0
0.2
0.4
0.6
0.8
1.0
PFS time since randomization [Months]
Estim
ate
d P
FS
pro
ba
bili
ty
0 3 6 9 12 15 18
Placebo, PFS events = 94/134, median = 1.0 mon
Afatinib, PFS events = 178/257, median = 4.4 mon
HR=0.28 (95% CI: 0.210, 0.362)
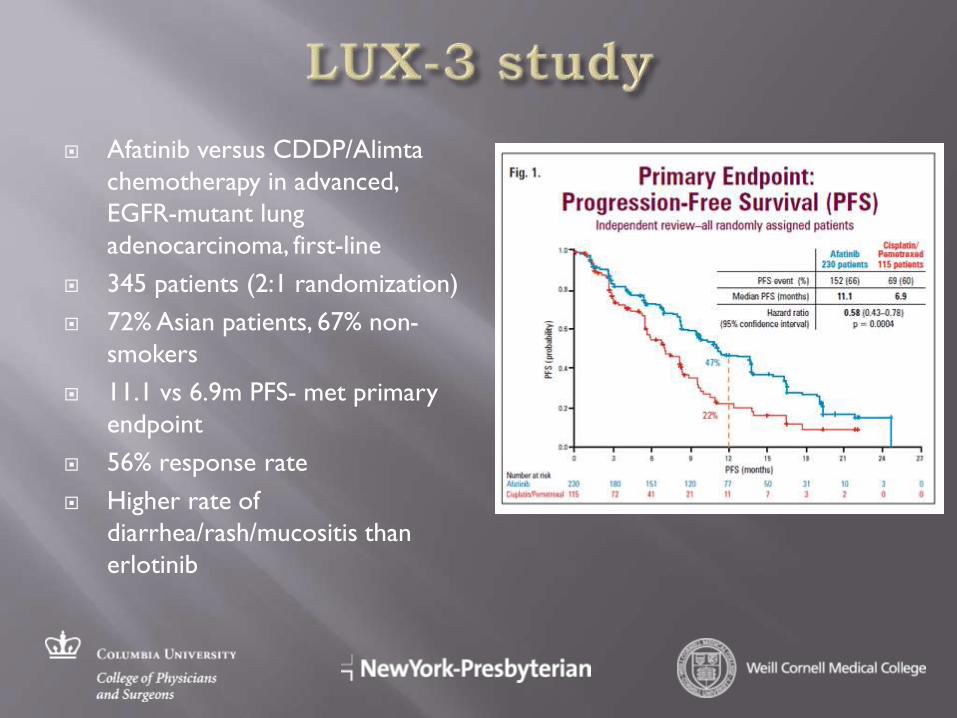
Afatinib versus CDDP/Alimta
chemotherapy in advanced,
EGFR-mutant lung
adenocarcinoma, first-line
345 patients (2:1 randomization)
72% Asian patients, 67% non-
smokers
11.1 vs 6.9m PFS- met primary
endpoint
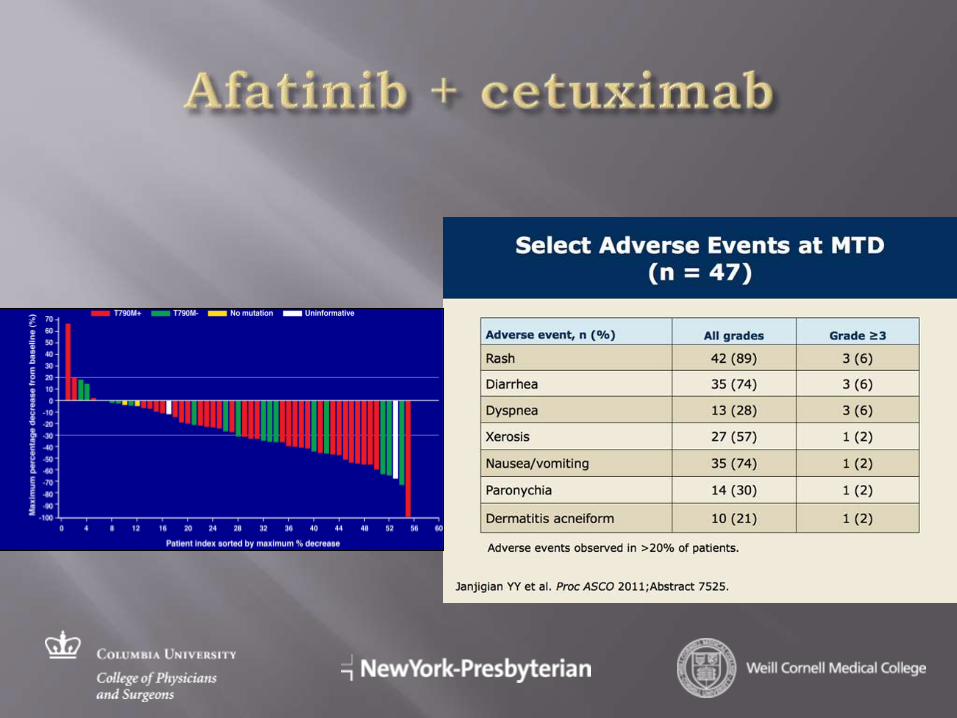
56% response rate
Higher rate of
diarrhea/rash/mucositis than
erlotinib
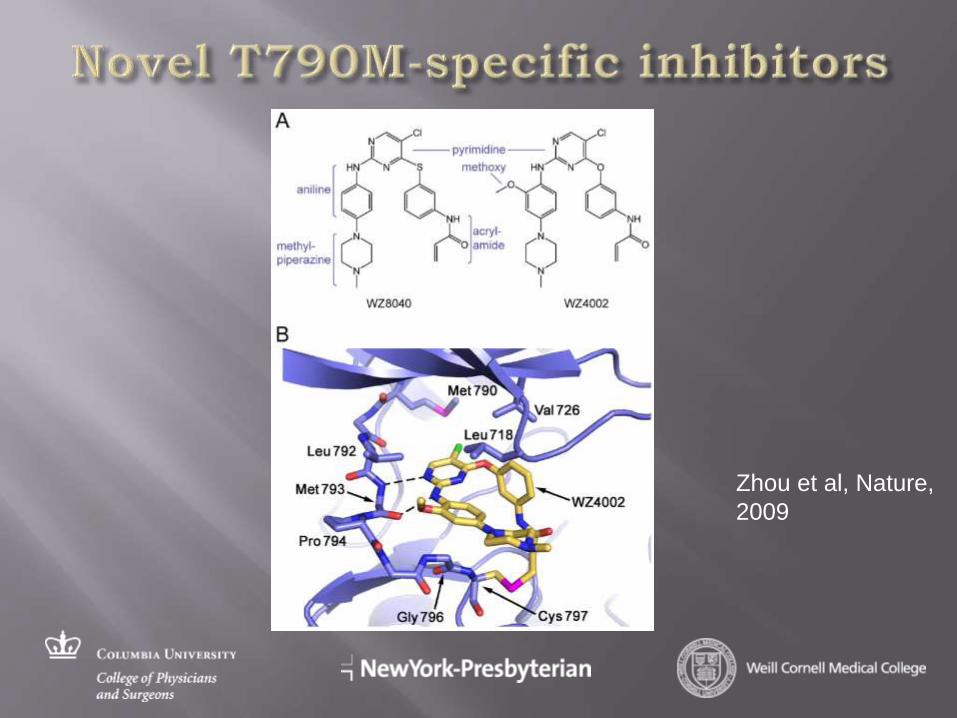
Zhou et al, Nature,
2009
These novel and highly promising drugs largely
spare EGFR WT signaling and preferentially block
mutant/T790M signaling leading to potentially wider
therapeutic indices
WZ4002
CO-1686- 67% (6/9) response rate in phase I of
T790M patients, no rash or diarrhea
AZD9291- 56% (7/12) response rate in phase I in
T790M patients, well-tolerated, some rash
AP26113
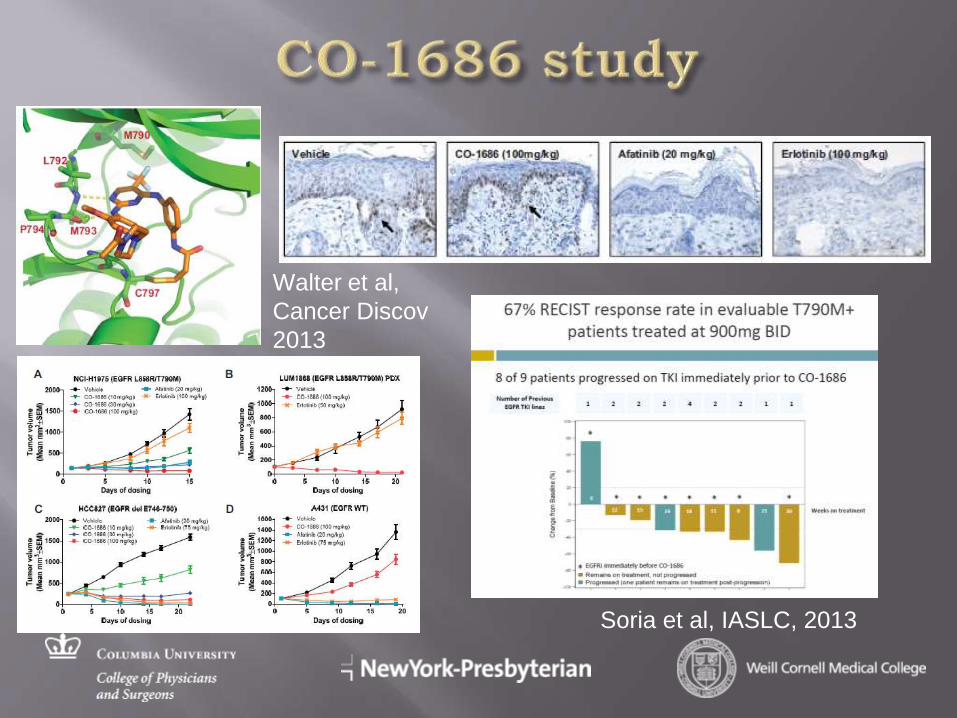
Soria et al, IASLC, 2013
Walter et al,
Cancer Discov
2013
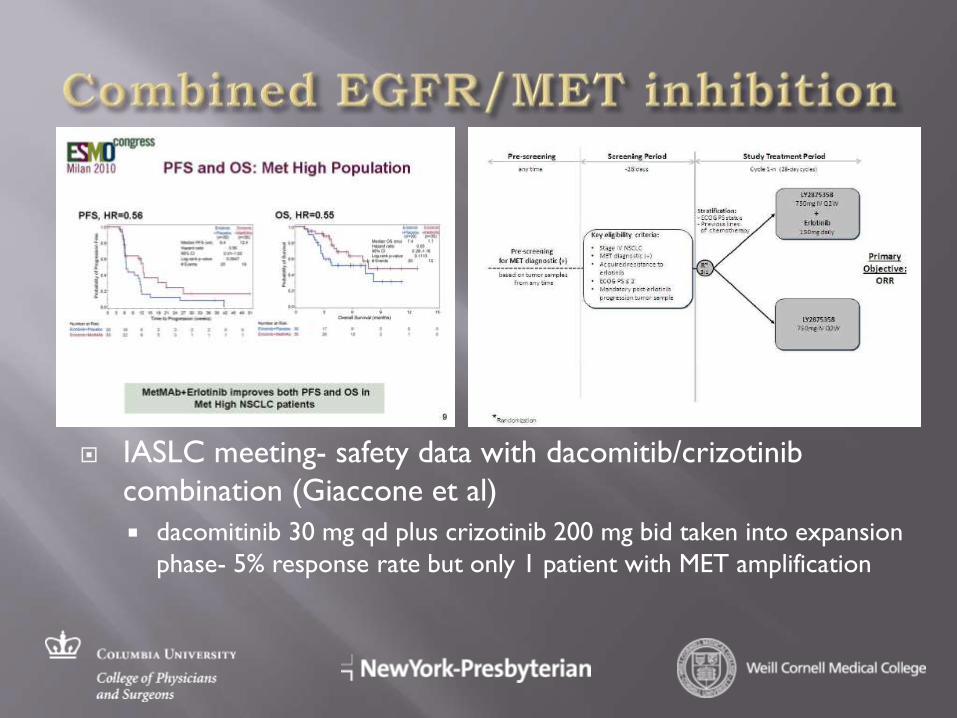
IASLC meeting- safety data with dacomitib/crizotinib
combination (Giaccone et al)
dacomitinib 30 mg qd plus crizotinib 200 mg bid taken into expansion
phase- 5% response rate but only 1 patient with MET amplification
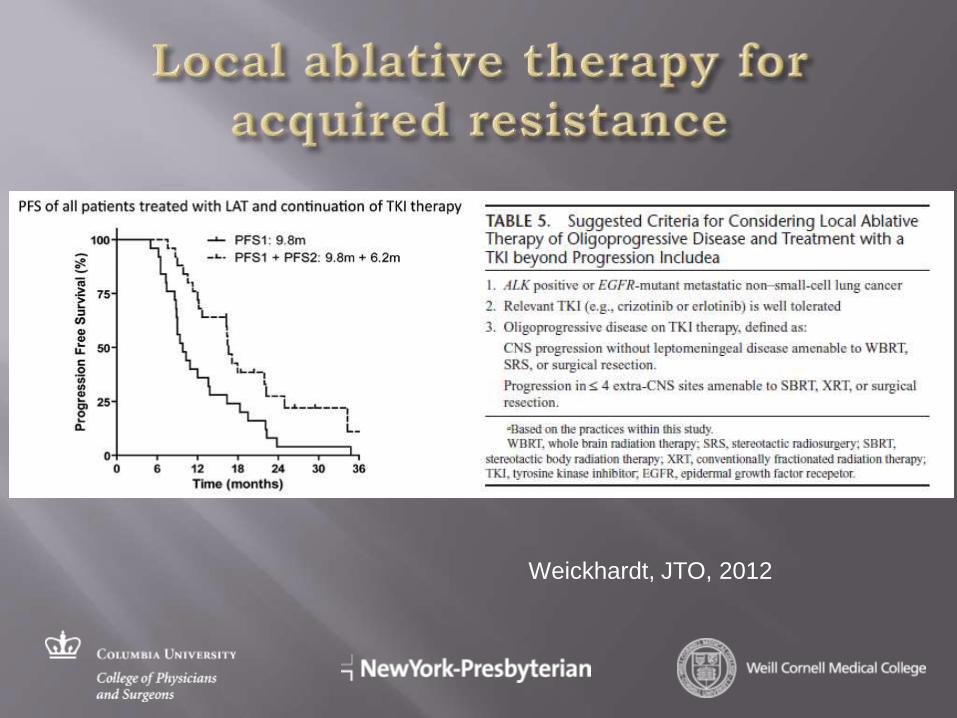
Weickhardt, JTO, 2012
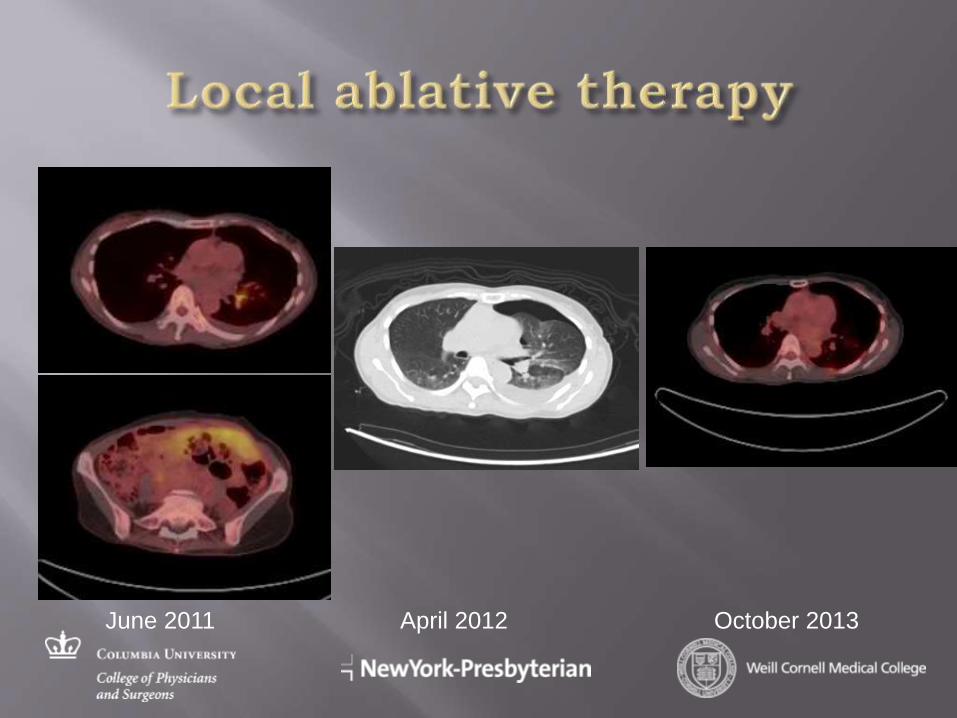
June 2011 April 2012 October 2013
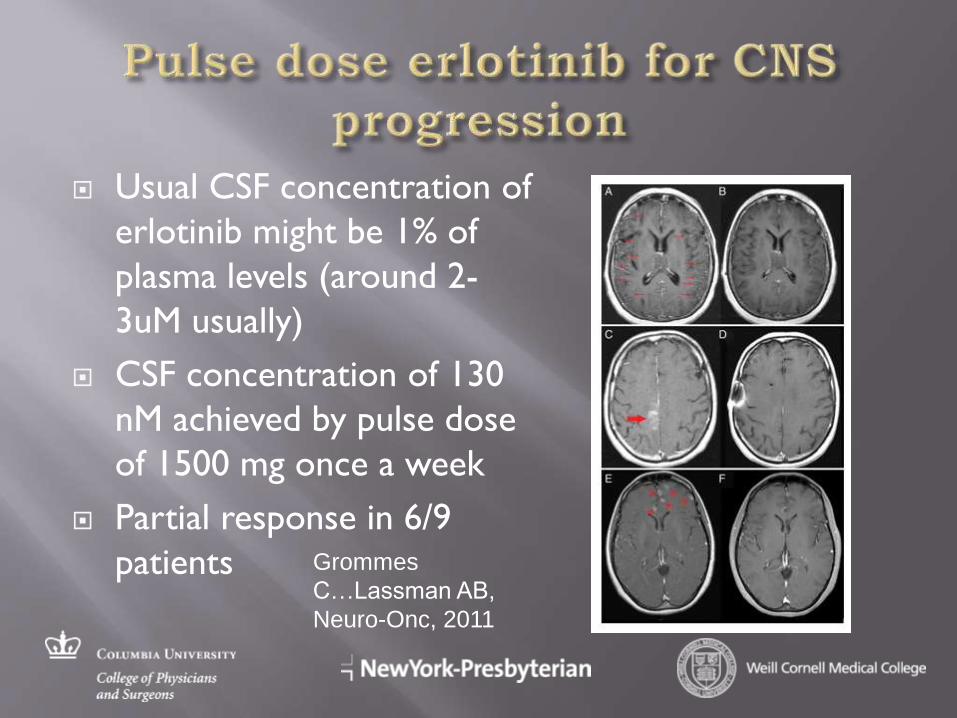
Usual CSF concentration of
erlotinib might be 1% of
plasma levels (around 2-
3uM usually)
CSF concentration of 130
nM achieved by pulse dose
of 1500 mg once a week
Partial response in 6/9
patients Grommes
C…Lassman AB,
Neuro-Onc, 2011
Second site mutations (EGFR-dependent)- T790M
Mutation-selective EGFR inhibitor
Bypass track signaling (EGFR-co-dependent)- MET, ErbB2, AXL, IGF1R
Combined inhibition
Downstream pathway activation- PI3K, B-raf
EGFR/mTOR inhibition
Histological transformation
Small cell therapy
Adaptive change- EMT/AXL
Unclear/ combined inhibition
Apoptotic resistance
BH3-mimetics
Pharmacokinetic resistance- CSF, pleural space
Pulse dose erlotinib, local therapy
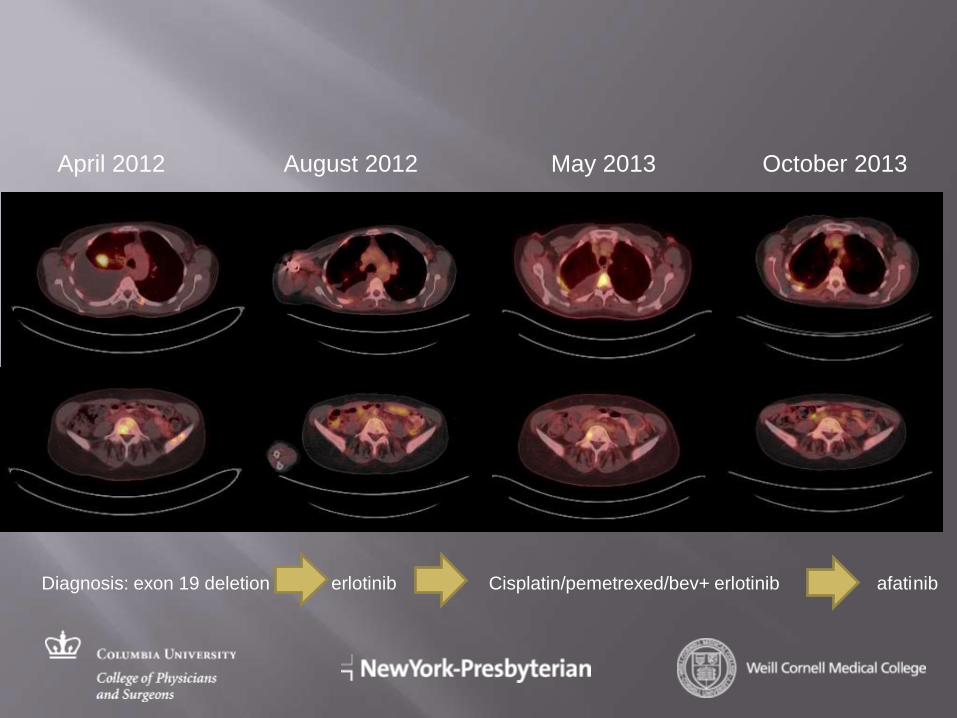
April 2012 August 2012 May 2013 October 2013
Diagnosis: exon 19 deletion erlotinib Cisplatin/pemetrexed/bev+ erlotinib afatinib
EGFR-T790M is dominant and challenging resistance mechanism
Irreversible inhibitors clearly have some in vivo activity- but enough to be clinically meaningful?
Specific T790M inhibitors- clear signals of activity
Would combination of inhibitors be a good strategy? For which patients?
EGFR/MET co-inhibition?
Other strategies- AXL, ErbB2/3, HSP90, PI3K, mTOR etc..
Biopsies at progression should be more and more routine
How to design clinical studies? Selection of patients/ enrichment likely paramount for success Molecular testing/selection upfront
Molecular monitoring/ imaging
Multiplex testing, next generation sequencing, CTC studies
Combination studies
Strategies to prevent resistance will be pivotal Adjuvant therapy
Early combination therapy
Targeted + immunotherapy
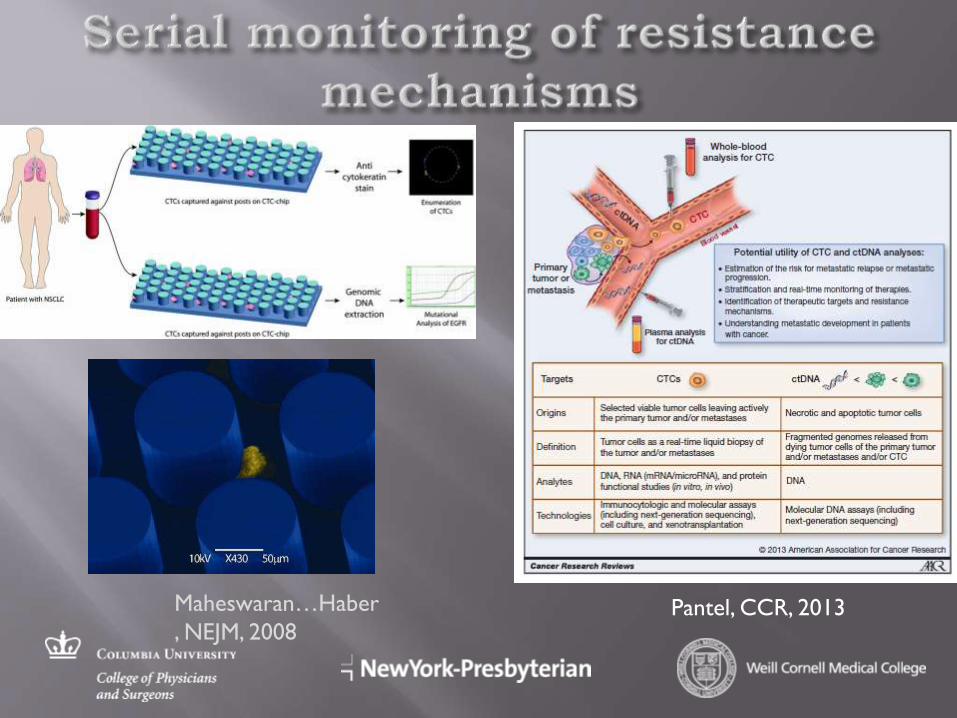
Maheswaran…Haber
, NEJM, 2008 Pantel, CCR, 2013
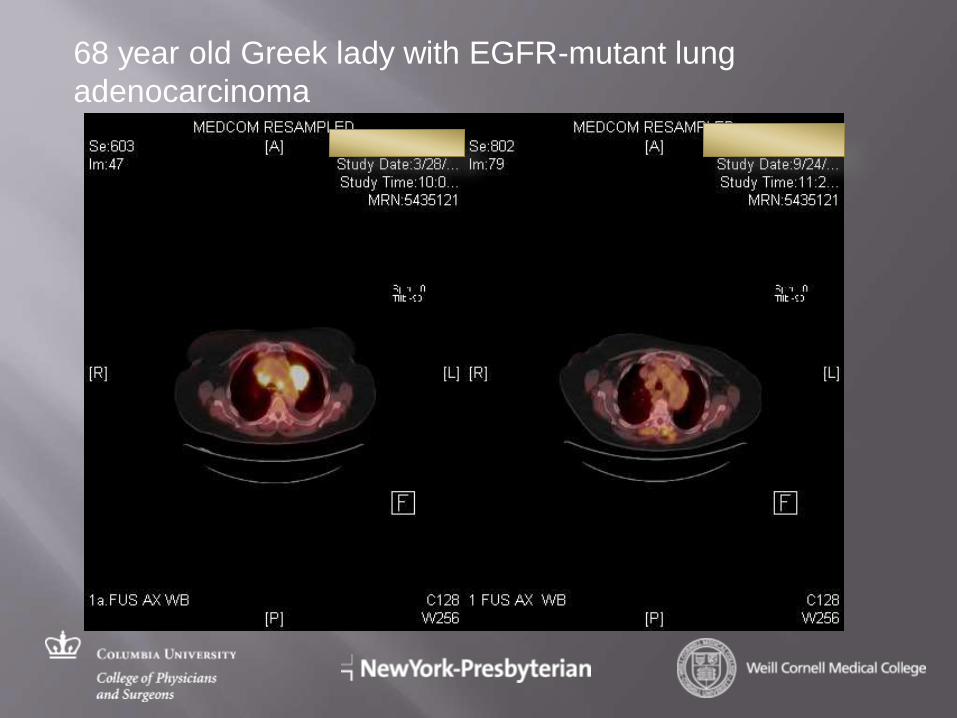
68 year old Greek lady with EGFR-mutant lung
adenocarcinoma
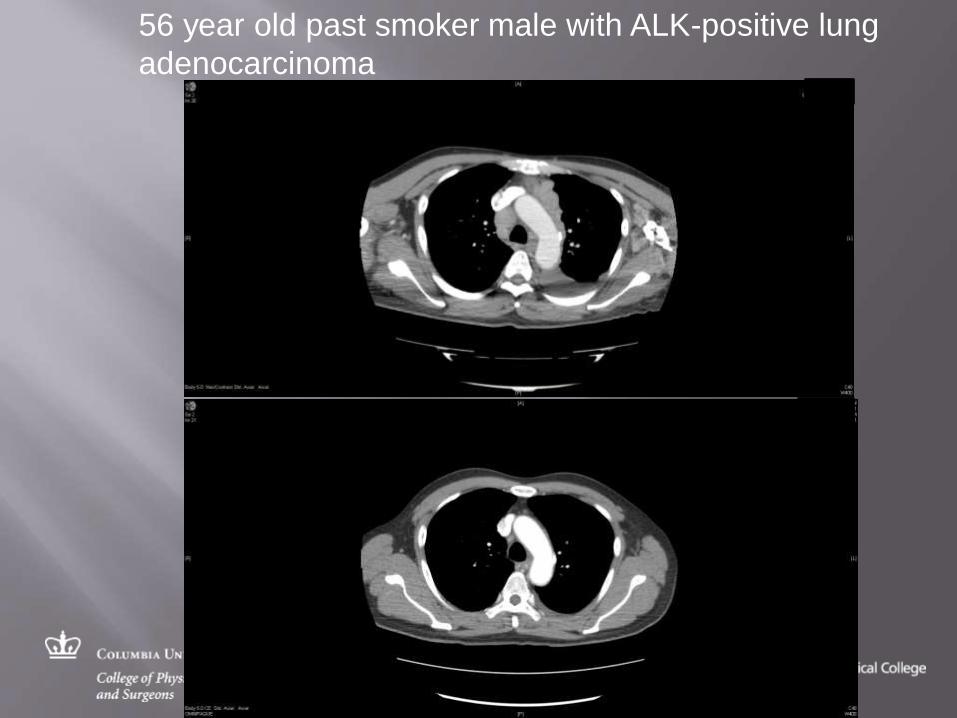
56 year old past smoker male with ALK-positive lung
adenocarcinoma
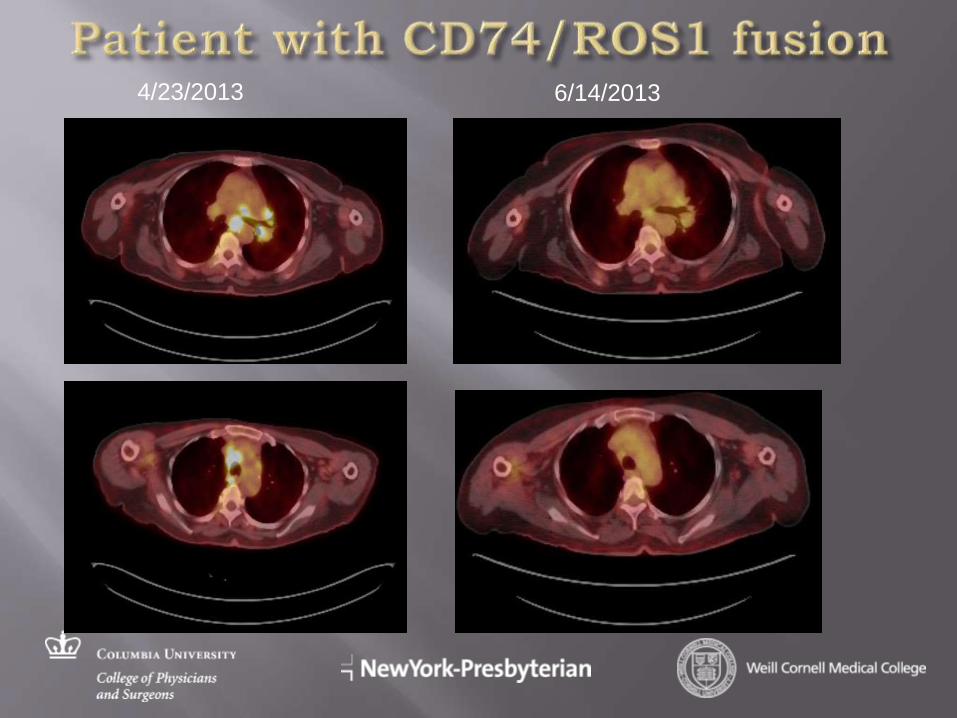
4/23/2013 6/14/2013

January 2013 August 2013
Patient with dual EGFR/ErbB2 mutation on afatinib
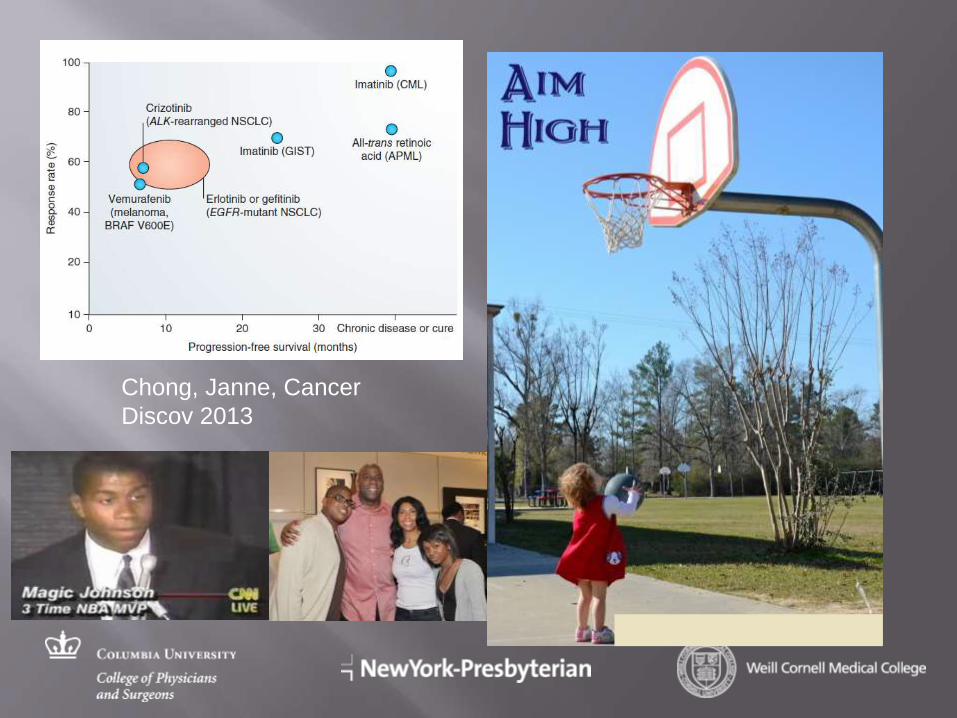
Chong, Janne, Cancer
Discov 2013