Embed Size (px)
Citation preview

BackgroundReports of long-term survivors (≥5 years) of
locally advanced esophageal cancer (LAEC) have
focused mainly on HRQL or GI symptoms
Only a handful of studies examined long term
oncological outcomes and causes of death beyond 5
years
Are patients with LAEC “truly” cured of their
disease?
AATS 95th ANNUAL MEETING, 2015
Objectives
1.To determine overall and CSS in patients with LAEC surviving at least 5 years 2.To determine the frequency and outcome of recurrent EC in 5 year survivors 3.To determine predictors of recurrence and mortality beyond the 5 year time point4.To determine the incidence of second primary cancers5.To determine competing causes of death
AATS 95th ANNUAL MEETING, 2015
Study Design Retrospective review of prospectively collected EC
database of esophagectomy for clinical T2N0 or higher disease
(1988 - 2009)
AATS 95th ANNUAL MEETING, 2015
Methods
• Definition of recurrence:• Local if luminal or intramural • Regional if in any nodes in dissected bed• Distant visceral or nodes beyond dissected
fields
• OS and CSS calculated from the landmark time of 5th postoperative year using KM method
• Multivariable analysis performed for factors affecting recurrence and survival
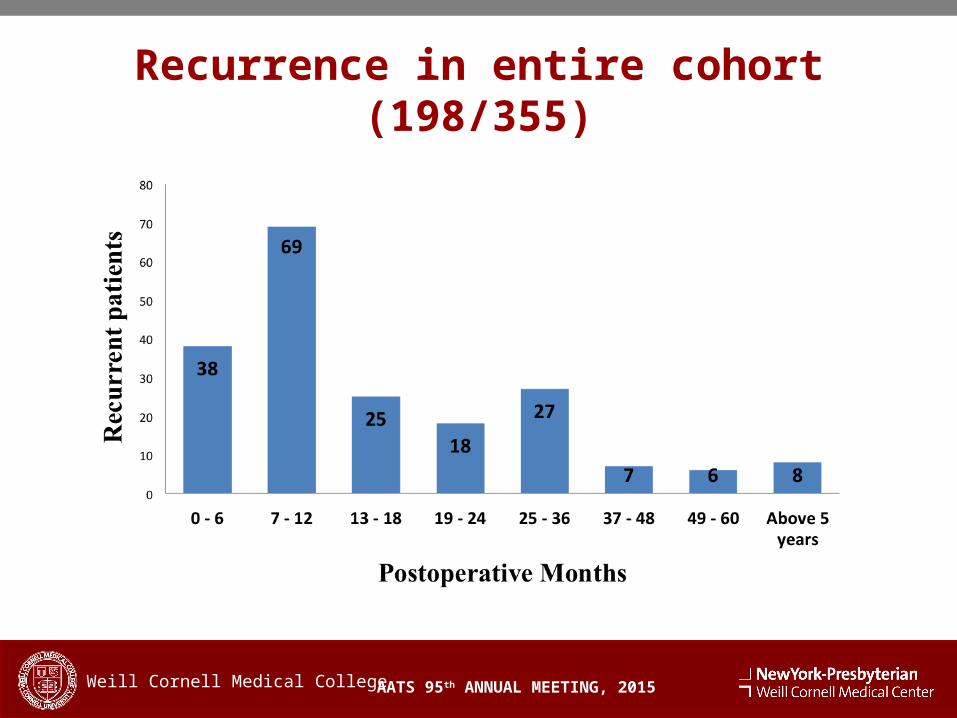
Recurrence in entire cohort (198/355)
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
AATS 95th ANNUAL MEETING, 2015
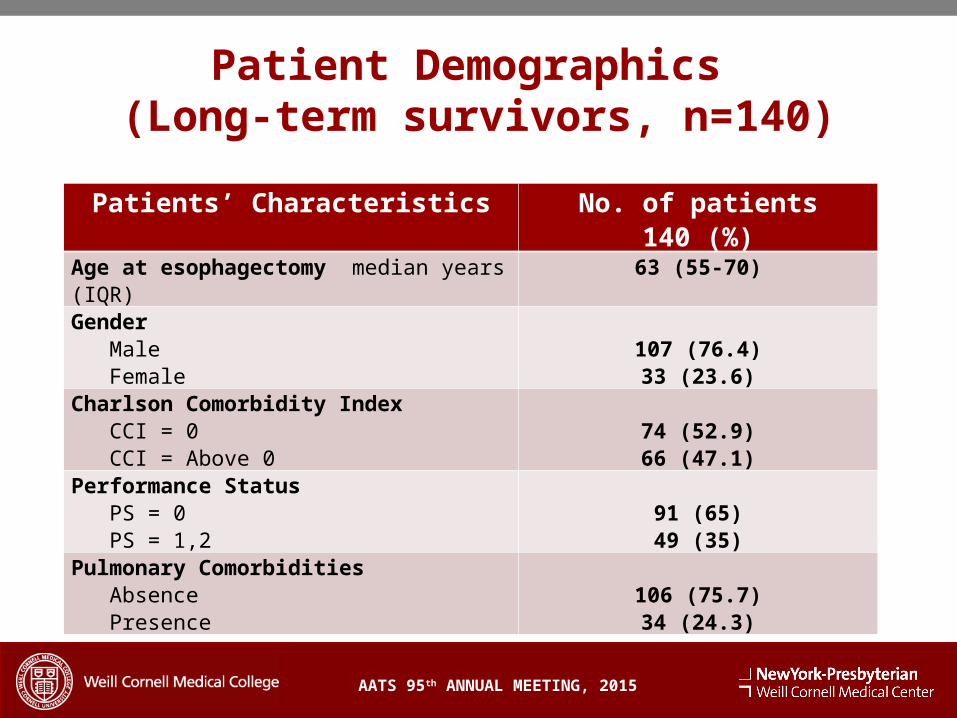
Patient Demographics (Long-term survivors, n=140)
Patients’ Characteristics No. of patients140 (%)
Age at esophagectomy median years (IQR)
63 (55-70)
Gender Male Female
107 (76.4)33 (23.6)
Charlson Comorbidity Index CCI = 0 CCI = Above 0
74 (52.9)66 (47.1)
Performance Status PS = 0 PS = 1,2
91 (65)49 (35)
Pulmonary Comorbidities Absence Presence
106 (75.7)34 (24.3)

Clinical Staging
AATS 95th ANNUAL MEETING, 2015
cTNM stages Number (%)
T1 N1 M0T1 N2 M1
2 (1.4%)1 (0.7%)
T2 N0-1 M0 39 (27.9%)
T3 N0-1 M0T3 N1 M1
86 (61.4%)8 (5.7%)
T4a N0 M0 T4a N1 M1
3 (1.2%)1 (0.7%)
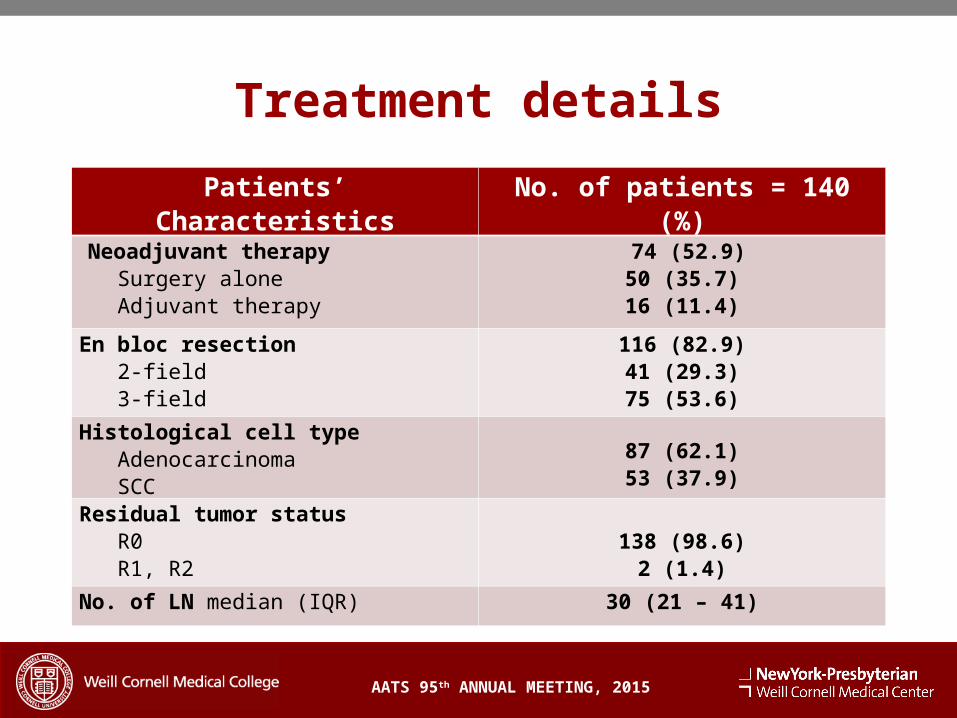
Treatment details
Patients’ Characteristics No. of patients = 140 (%)
Neoadjuvant therapy Surgery alone Adjuvant therapy
74 (52.9)50 (35.7)16 (11.4)
En bloc resection 2-field 3-field
116 (82.9)41 (29.3)75 (53.6)
Histological cell type Adenocarcinoma SCC
87 (62.1)53 (37.9)
Residual tumor status R0 R1, R2
138 (98.6)
2 (1.4)
No. of LN median (IQR) 30 (21 – 41)
AATS 95th ANNUAL MEETING, 2015
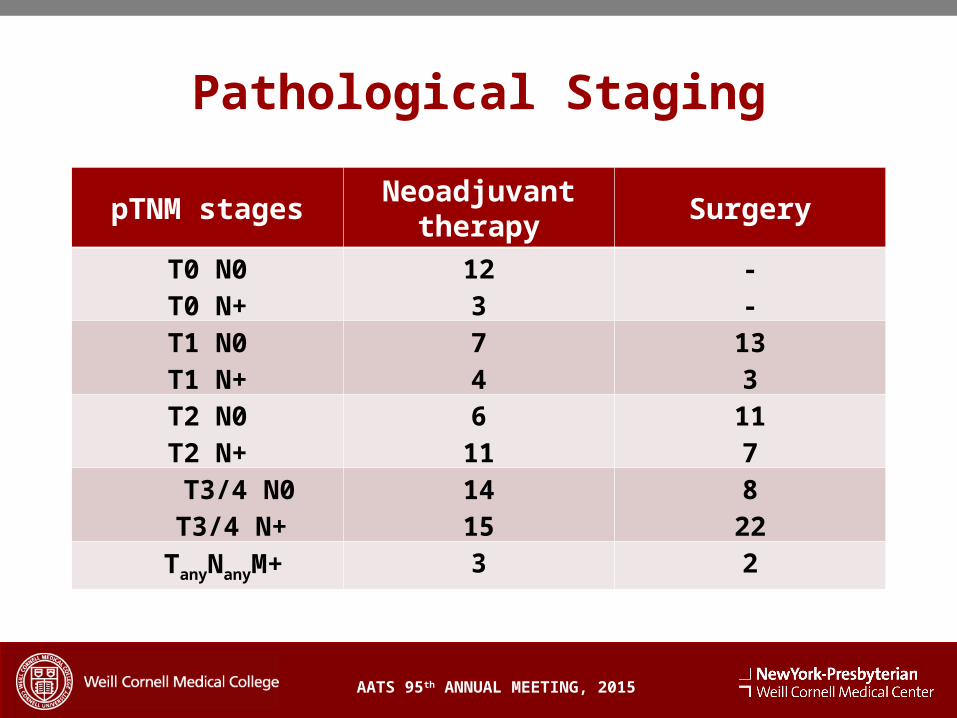
Pathological Staging
AATS 95th ANNUAL MEETING, 2015
pTNM stagesNeoadjuvant
therapySurgery
T0 N0T0 N+
123
--
T1 N0T1 N+
74
133
T2 N0T2 N+
611
117
T3/4 N0 T3/4 N+
1415
822
TanyNanyM+ 3 2
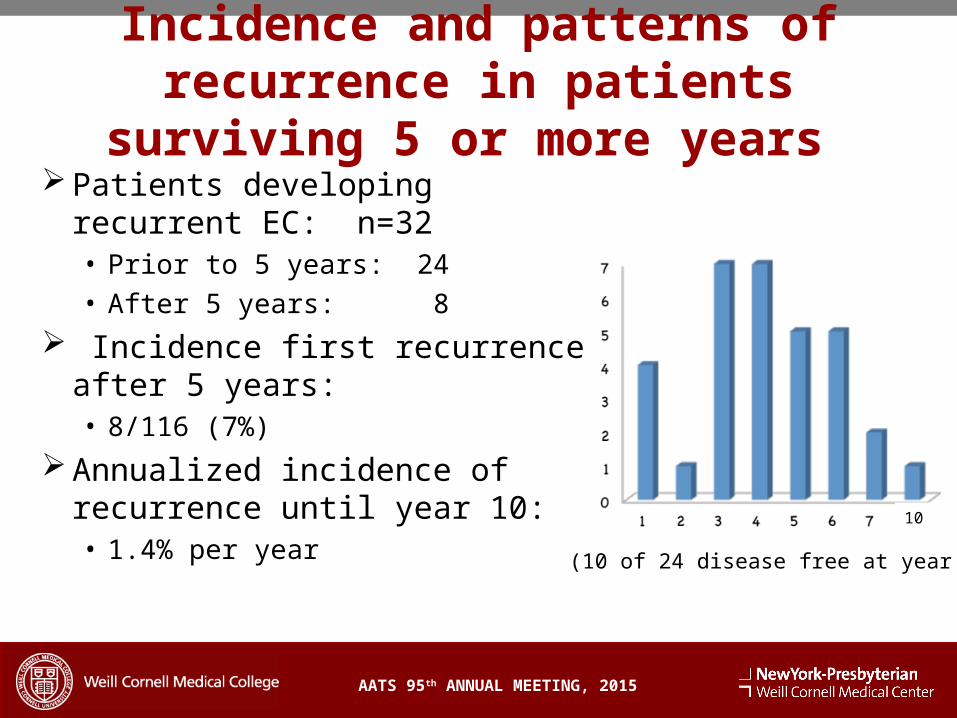
Incidence and patterns of recurrence in patients surviving
5 or more years
AATS 95th ANNUAL MEETING, 2015
Patients developing recurrent EC: n=32• Prior to 5 years: 24
• After 5 years: 8
Incidence first recurrence after 5 years: • 8/116 (7%)
Annualized incidence of recurrence until year 10:• 1.4% per year
(10 of 24 disease free at year 5)
10
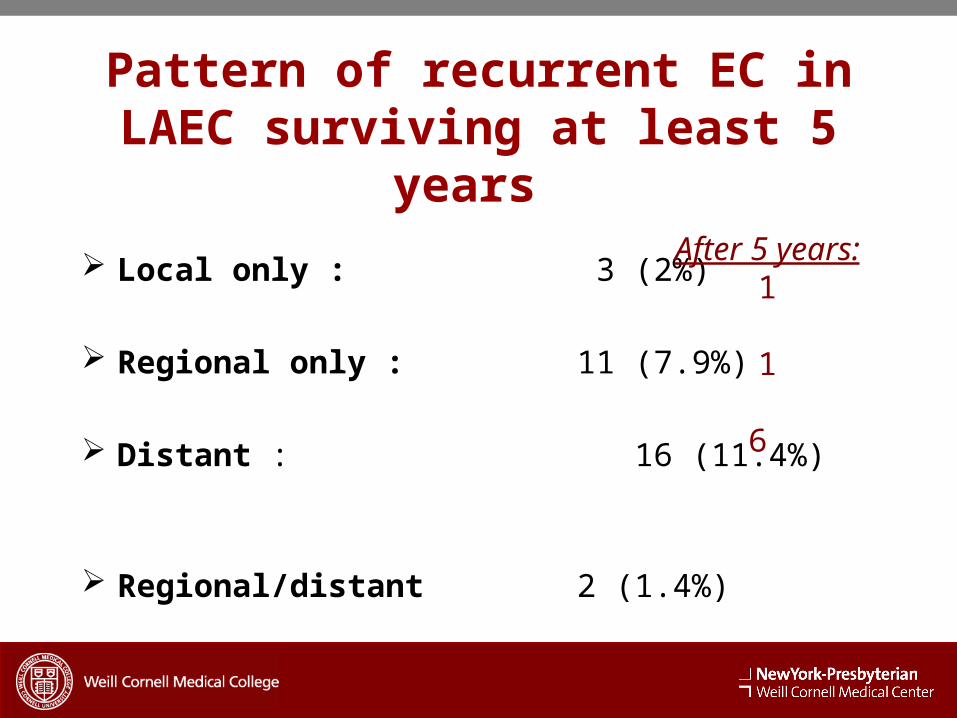
Pattern of recurrent EC in LAEC surviving at least 5
years
Local only : 3 (2%) Regional only : 11 (7.9%)
Distant : 16 (11.4%)
Regional/distant 2 (1.4%)
After 5 years:1
1
6
AATS 95th ANNUAL MEETING, 2015
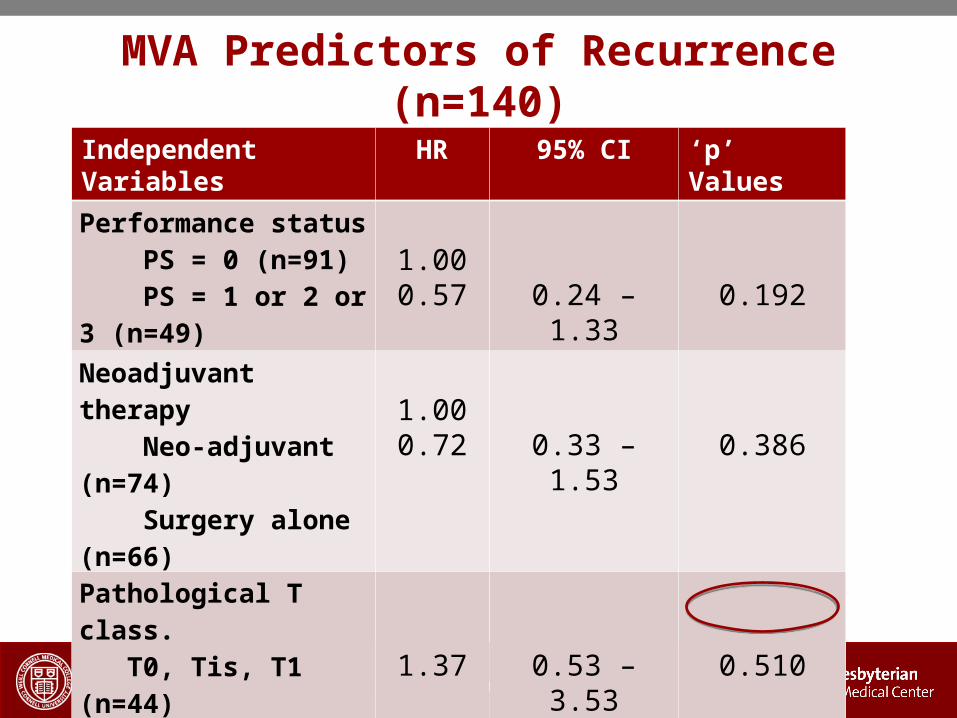
MVA Predictors of Recurrence (n=140)
Independent Variables
HR 95% CI ‘p ’ Values
Performance status PS = 0 (n=91) PS = 1 or 2 or 3 (n=49)
1.000.57 0.24 – 1.33 0.192
Neoadjuvant therapy Neo-adjuvant (n=74) Surgery alone (n=66)
1.000.72 0.33 – 1.53 0.386
Pathological T class. T0, Tis, T1 (n=44) T2, T3, T4 (N=96) 1.37 0.53 – 3.53 0.510
Pathological N class. N0 (n=71) N1, N2, N3 (n=69) 3.00 1.28 – 7.06 0.012
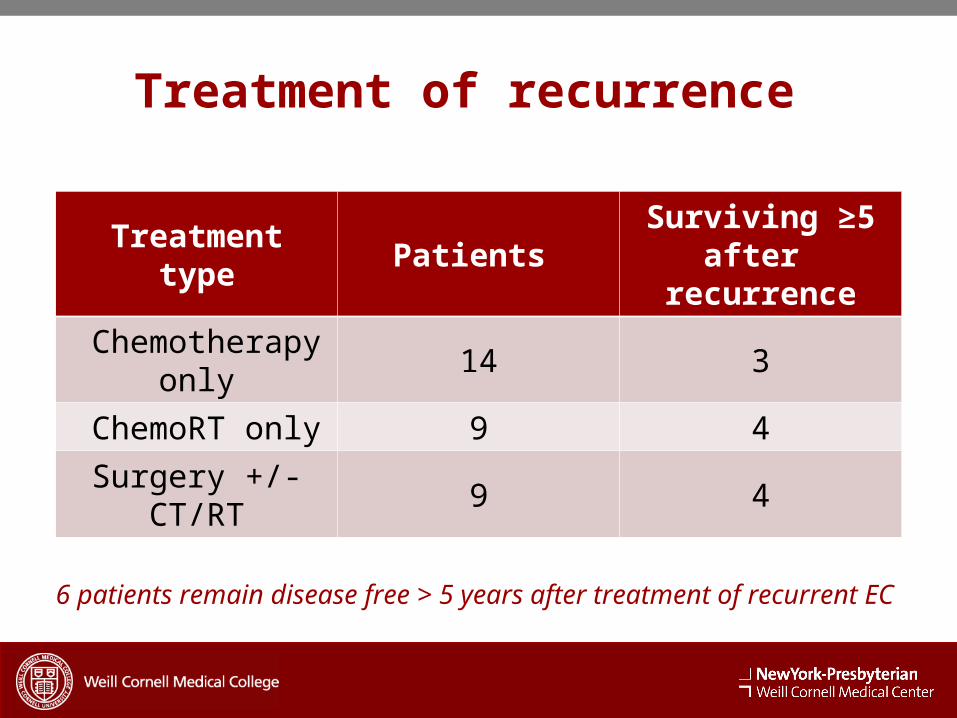
Treatment of recurrence
Treatment type Patients Surviving ≥5 after recurrence
Chemotherapy only 14 3
ChemoRT only 9 4
Surgery +/- CT/RT 9 4
6 patients remain disease free > 5 years after treatment of recurrent EC
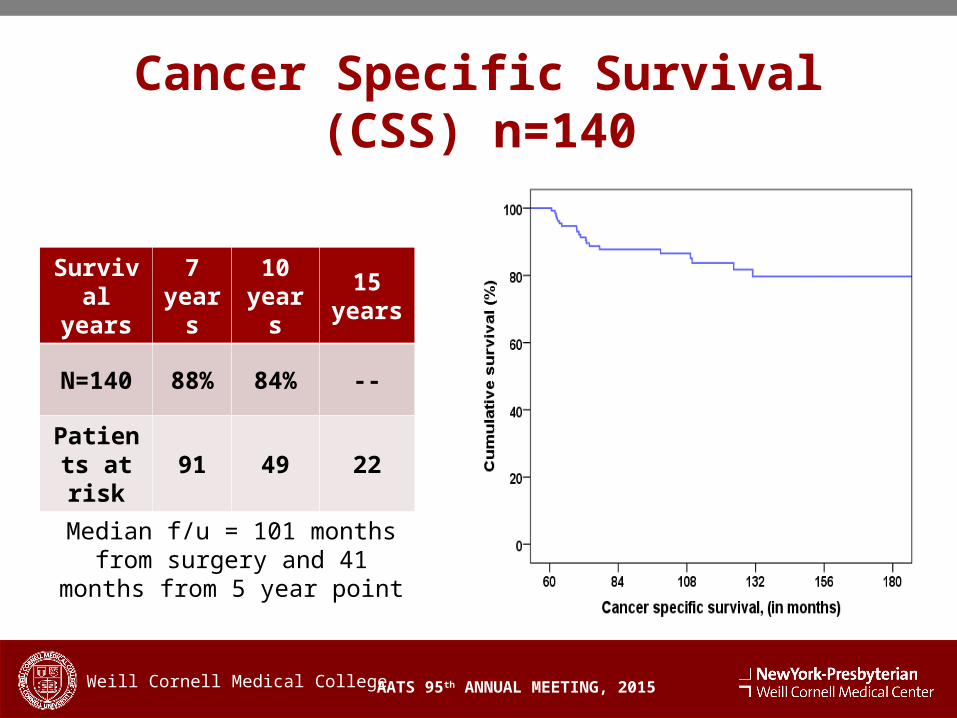
Cancer Specific Survival (CSS) n=140
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years
7 years
10 years
15 years
N=140 88% 84% --
Patients at risk
91 49 22
Median f/u = 101 months from surgery and 41 months
from 5 year point
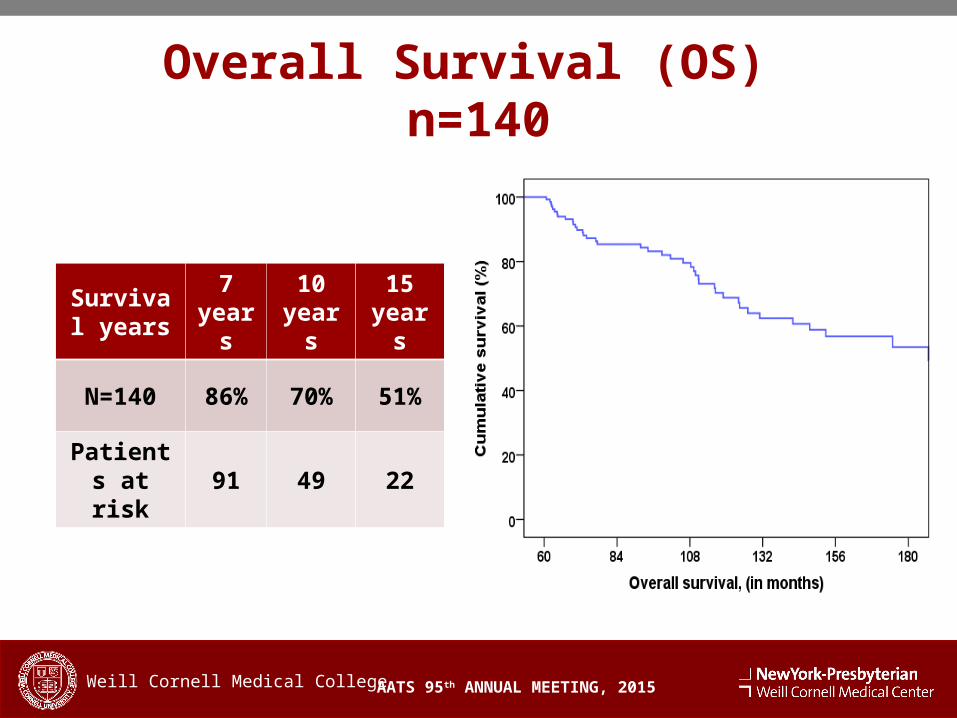
Overall Survival (OS) n=140
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years
7 years
10 years
15 years
N=140 86% 70% 51%
Patients at risk
91 49 22
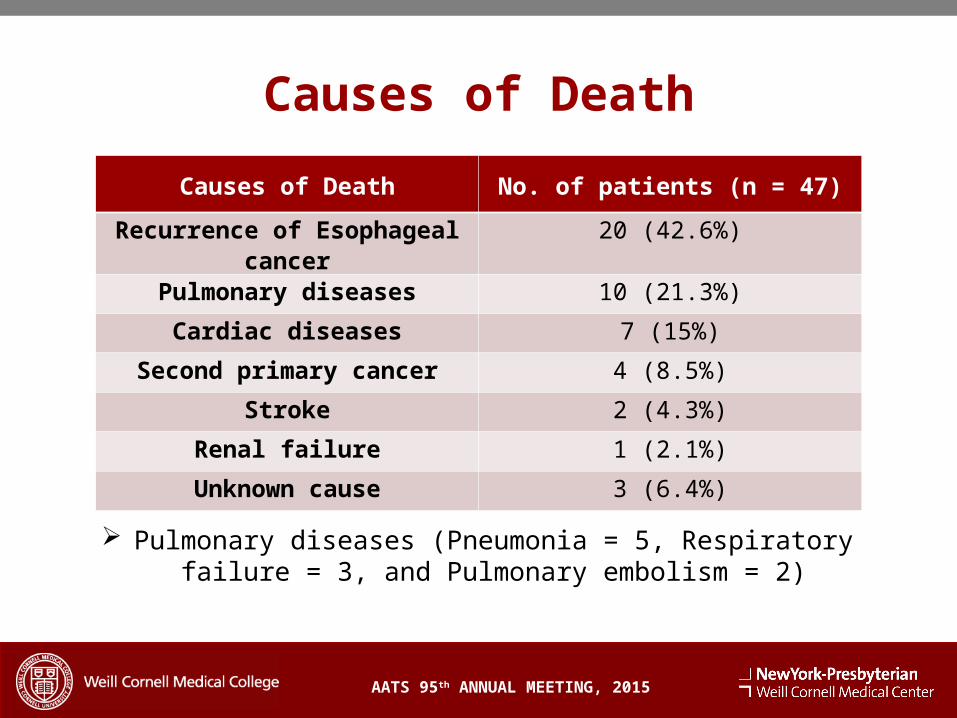
Causes of Death
Pulmonary diseases (Pneumonia = 5, Respiratory failure = 3, and Pulmonary embolism = 2)
AATS 95th ANNUAL MEETING, 2015
Causes of Death No. of patients (n = 47)
Recurrence of Esophageal cancer
20 (42.6%)
Pulmonary diseases 10 (21.3%)
Cardiac diseases 7 (15%)
Second primary cancer 4 (8.5%)
Stroke 2 (4.3%)
Renal failure 1 (2.1%)
Unknown cause 3 (6.4%)
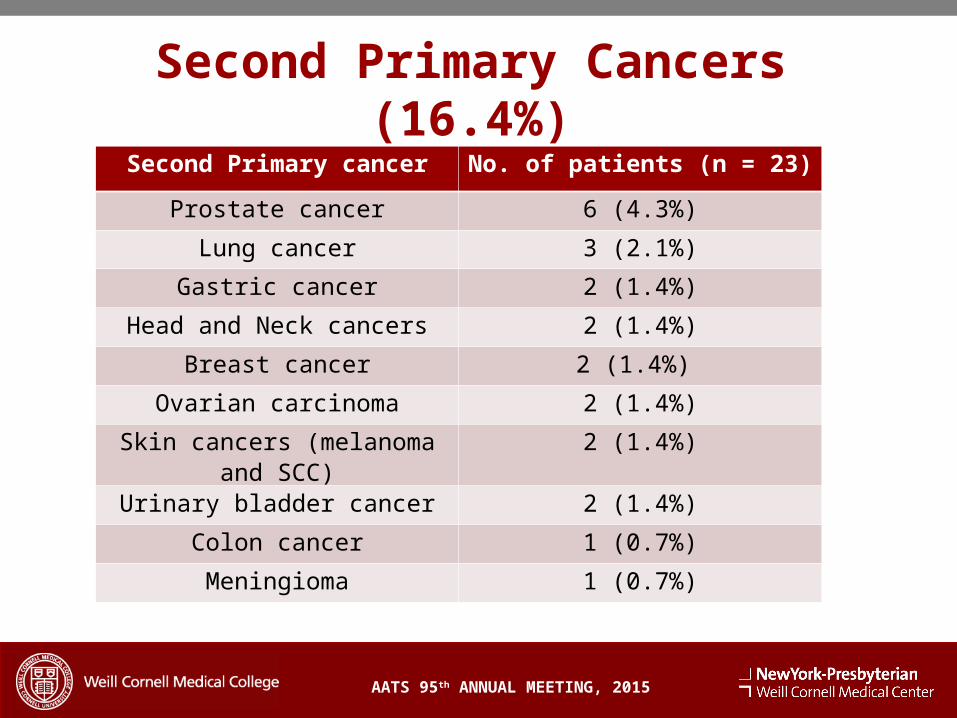
Second Primary Cancers (16.4%)
AATS 95th ANNUAL MEETING, 2015
Second Primary cancer No. of patients (n = 23)
Prostate cancer 6 (4.3%)
Lung cancer 3 (2.1%)
Gastric cancer 2 (1.4%)
Head and Neck cancers 2 (1.4%)
Breast cancer 2 (1.4%)
Ovarian carcinoma 2 (1.4%)
Skin cancers (melanoma and SCC)
2 (1.4%)
Urinary bladder cancer 2 (1.4%)
Colon cancer 1 (0.7%)
Meningioma 1 (0.7%)
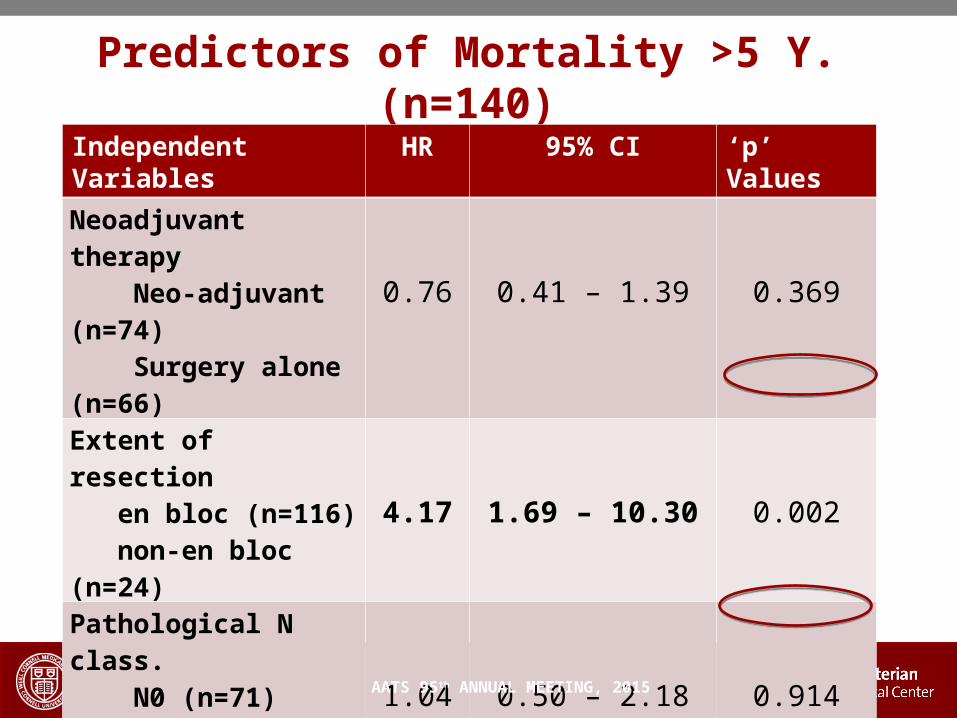
Predictors of Mortality >5 Y. (n=140)
Independent Variables
HR 95% CI ‘p ’ Values
Neoadjuvant therapy Neo-adjuvant (n=74) Surgery alone (n=66) 0.76 0.41 – 1.39 0.369
Extent of resection en bloc (n=116) non-en bloc (n=24) 4.17 1.69 – 10.30 0.002
Pathological N class. N0 (n=71) N1, N2, N3 (n=69) 1.04 0.50 – 2.18 0.914
Recurrence No recurrence (n=108) Recurrences (n=32) 4.65 2.42 – 8.93 <0.001
AATS 95th ANNUAL MEETING, 2015
Conclusions The majority of patients with LAEC who do not
recur by 5 years are, in fact, cured of their disease
A small subset of patients (<10%) remain at risk for recurrent EC Nodal disease is the only independent
variable for EC recurrence Patients cured of EC are at risk for second
primary cancers Pulmonary disease leads to at least 20% of non
–cancer deaths
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Recommendations
Careful follow up for patients with LAEC surviving 5 years should be continued due to the risk of late recurrence and second primary cancers
Therapy can be advocated for selected patients with recurrences
Because aspiration may be an important long term sequela of esophagectomy, patients need careful follow-up by physicians familiar with the management of esophageal diseases
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Thank youThank you
Conclusion
Despite surviving at least 5-years after esophagectomy for LAEC, a small subset of patients at risk for Recurrence of esophageal cancerSecond primary cancersPulmonary disease possibly related to esophagectomy
Careful follow-up and surveillance are mandatory for LAEC patients even after 5-years follow-up
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
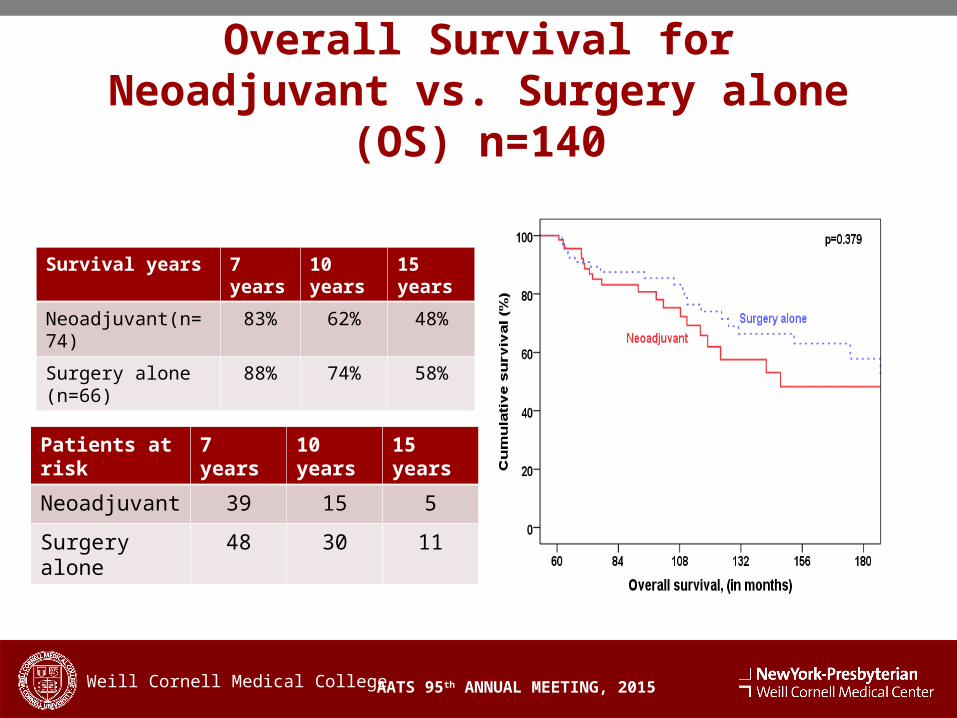
Overall Survival for Neoadjuvant vs. Surgery alone (OS) n=140
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years 7 years 10 years 15 years
Neoadjuvant(n=74) 83% 62% 48%
Surgery alone (n=66) 88% 74% 58%
Patients at risk 7 years 10 years 15 years
Neoadjuvant 39 15 5
Surgery alone 48 30 11
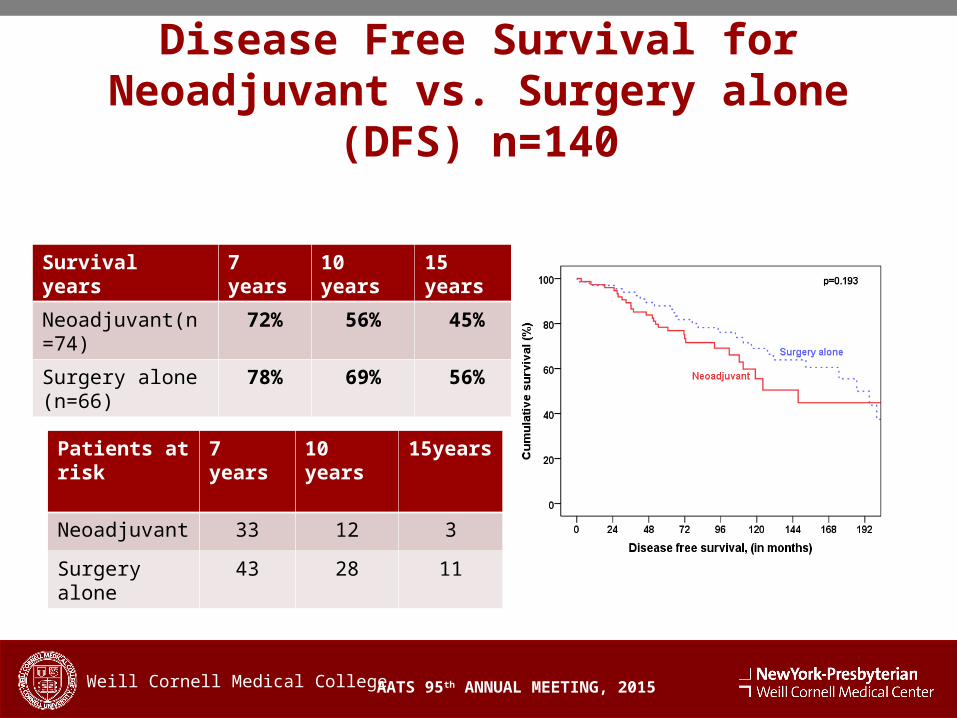
Disease Free Survival for Neoadjuvant vs. Surgery alone (DFS) n=140
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years 7 years 10 years 15 years
Neoadjuvant(n=74) 72% 56% 45%
Surgery alone (n=66)
78% 69% 56%
Patients at risk 7 years 10 years 15years
Neoadjuvant 33 12 3
Surgery alone 43 28 11
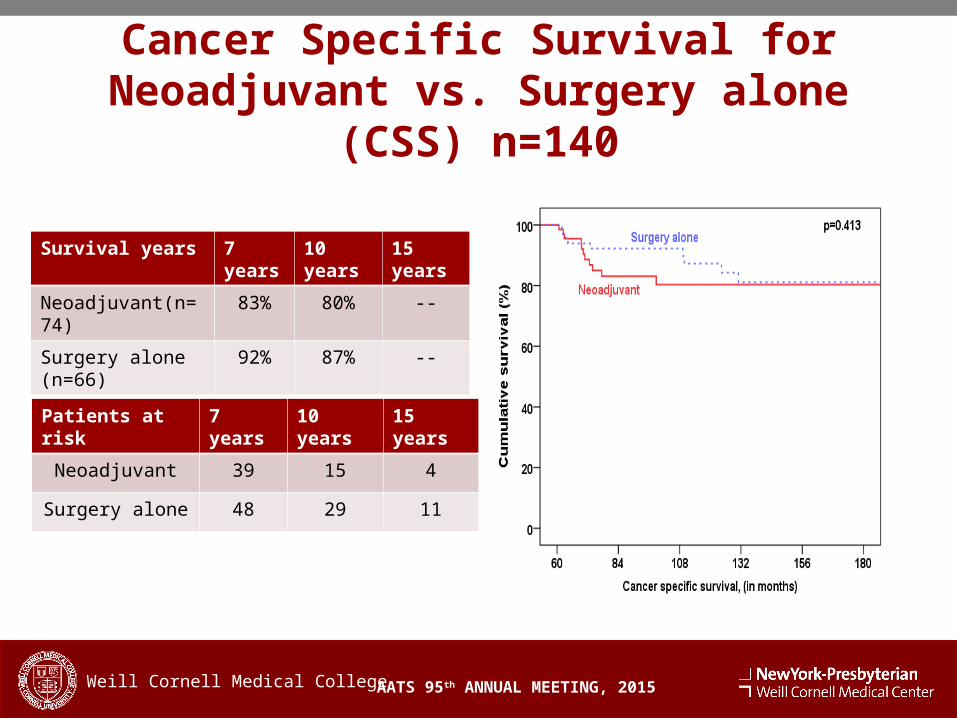
Cancer Specific Survival for Neoadjuvant vs. Surgery alone (CSS) n=140
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years 7 years 10 years 15 years
Neoadjuvant(n=74) 83% 80% --
Surgery alone (n=66) 92% 87% --
Patients at risk 7 years 10 years 15 years
Neoadjuvant 39 15 4
Surgery alone 48 29 11
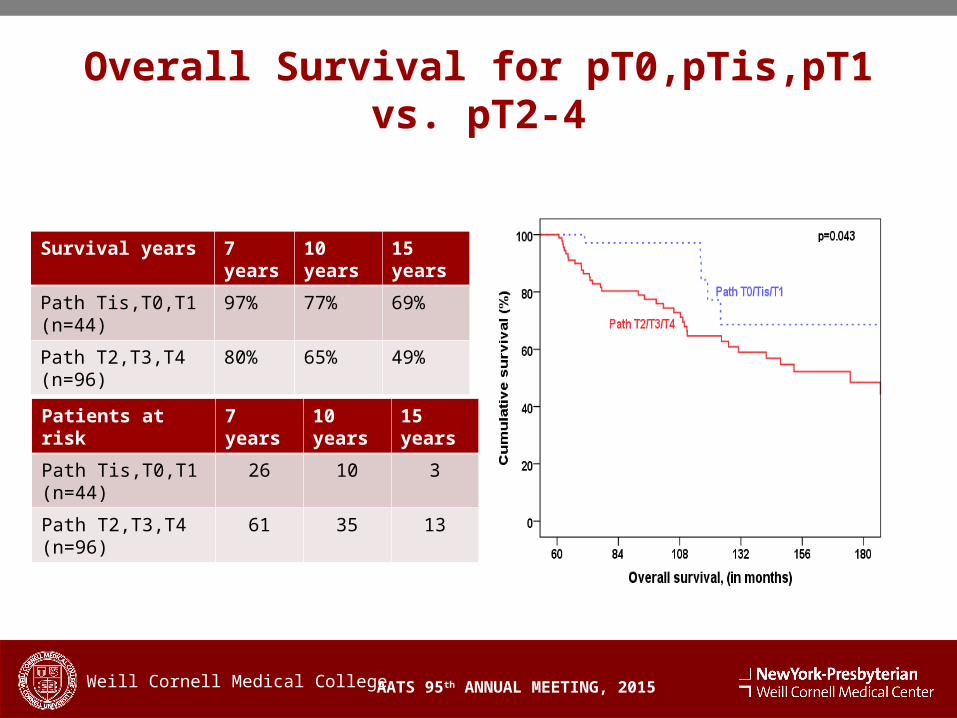
Overall Survival for pT0,pTis,pT1 vs. pT2-4
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years 7 years 10 years 15 years
Path Tis,T0,T1 (n=44) 97% 77% 69%
Path T2,T3,T4 (n=96) 80% 65% 49%
Patients at risk 7 years 10 years 15 years
Path Tis,T0,T1 (n=44) 26 10 3
Path T2,T3,T4 (n=96) 61 35 13
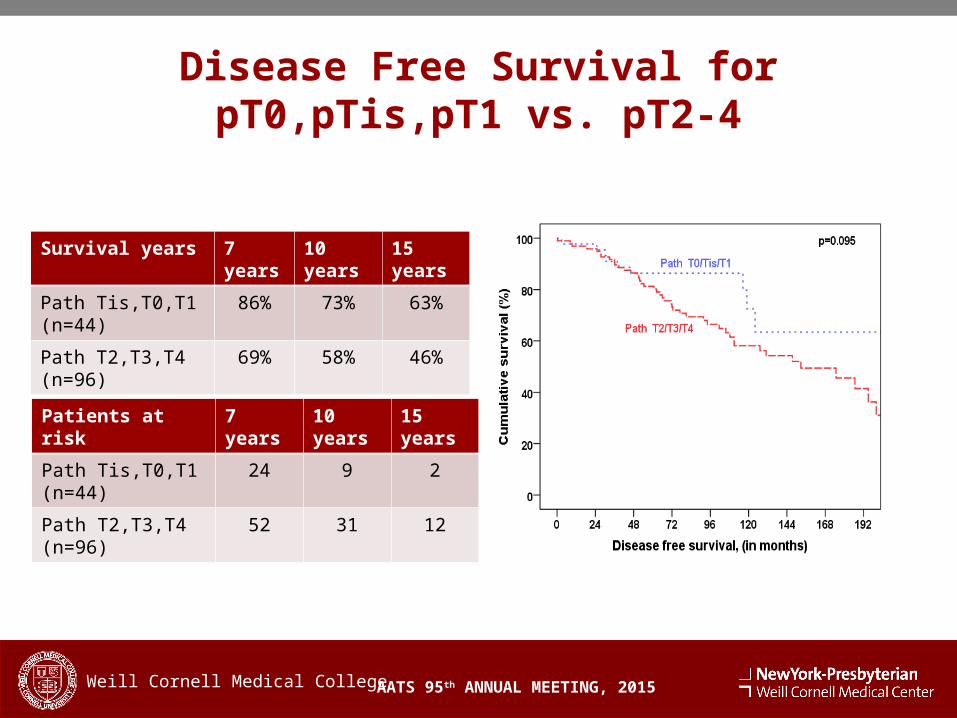
Disease Free Survival for pT0,pTis,pT1 vs. pT2-4
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years 7 years 10 years 15 years
Path Tis,T0,T1 (n=44) 86% 73% 63%
Path T2,T3,T4 (n=96) 69% 58% 46%
Patients at risk 7 years 10 years 15 years
Path Tis,T0,T1 (n=44) 24 9 2
Path T2,T3,T4 (n=96) 52 31 12
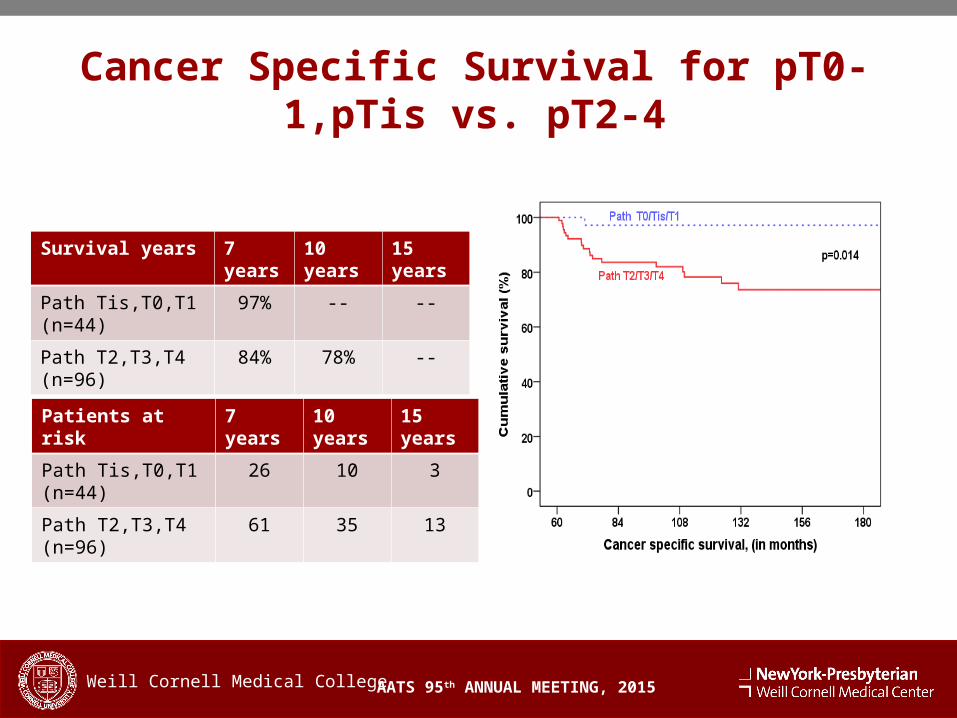
Cancer Specific Survival for pT0-1,pTis vs. pT2-4
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years 7 years 10 years 15 years
Path Tis,T0,T1 (n=44) 97% -- --
Path T2,T3,T4 (n=96) 84% 78% --
Patients at risk 7 years 10 years 15 years
Path Tis,T0,T1 (n=44) 26 10 3
Path T2,T3,T4 (n=96) 61 35 13
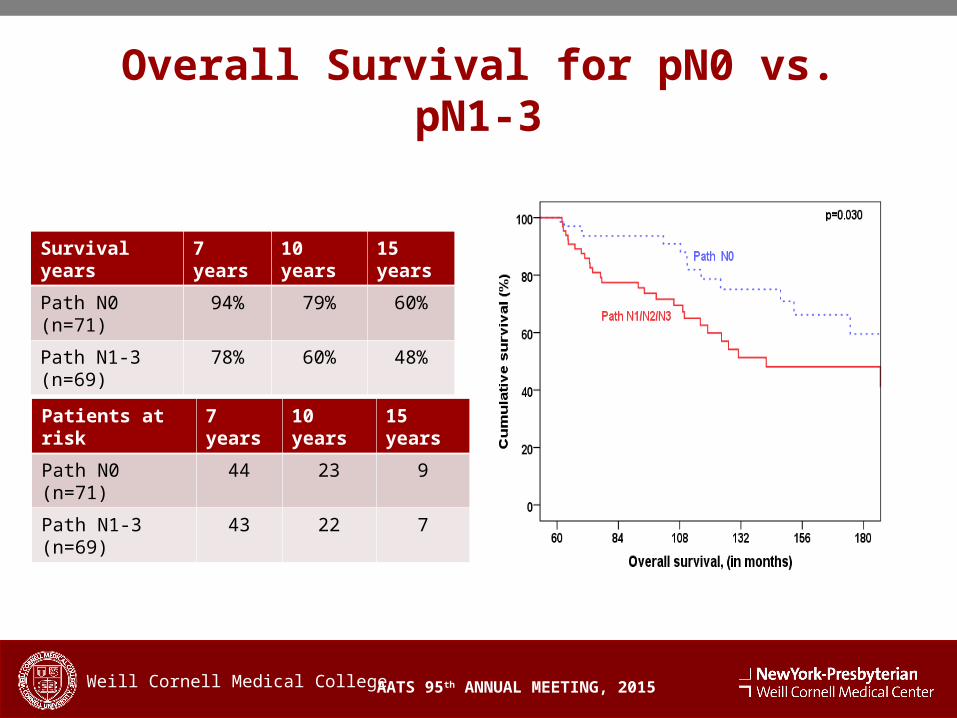
Overall Survival for pN0 vs. pN1-3
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years 7 years 10 years 15 years
Path N0 (n=71) 94% 79% 60%
Path N1-3 (n=69) 78% 60% 48%
Patients at risk 7 years 10 years 15 years
Path N0 (n=71) 44 23 9
Path N1-3 (n=69) 43 22 7
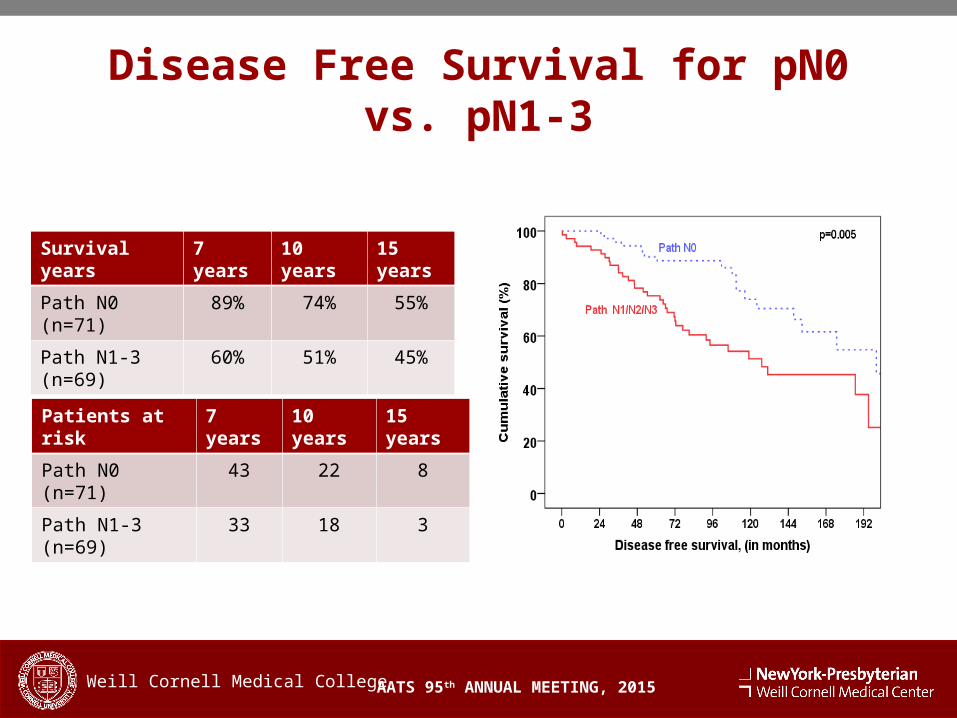
Disease Free Survival for pN0 vs. pN1-3
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years 7 years 10 years 15 years
Path N0 (n=71) 89% 74% 55%
Path N1-3 (n=69) 60% 51% 45%
Patients at risk 7 years 10 years 15 years
Path N0 (n=71) 43 22 8
Path N1-3 (n=69) 33 18 3
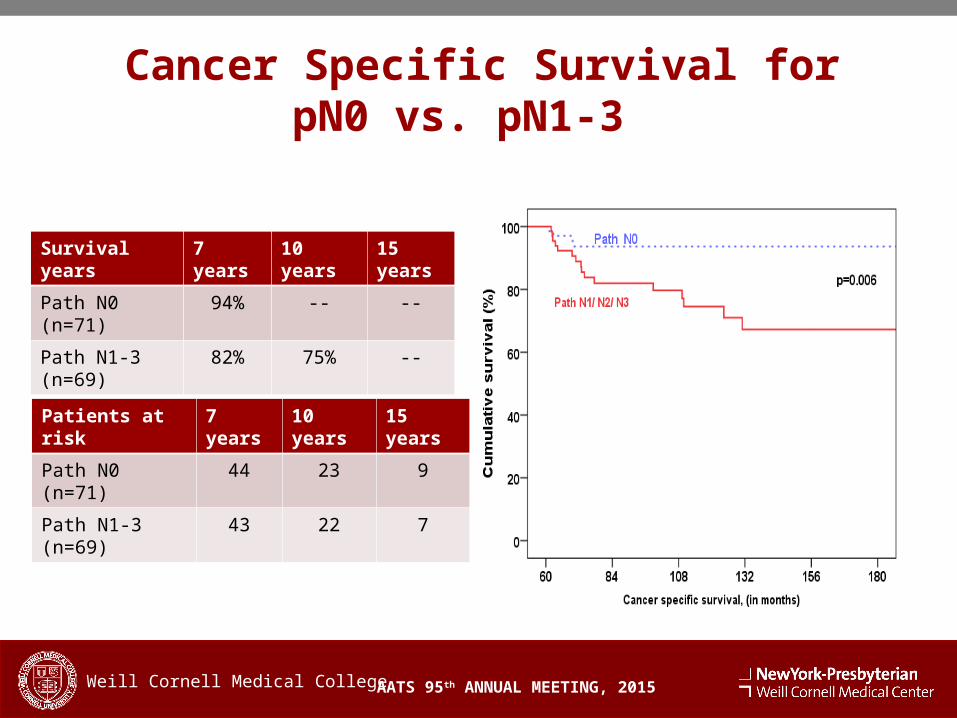
Cancer Specific Survival for pN0 vs. pN1-3
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College
Survival years 7 years 10 years 15 years
Path N0 (n=71) 94% -- --
Path N1-3 (n=69) 82% 75% --
Patients at risk 7 years 10 years 15 years
Path N0 (n=71) 44 23 9
Path N1-3 (n=69) 43 22 7
Follow-up and Recurrence
AATS 95th ANNUAL MEETING, 2015
Median follow-up for 5-year survivors was 101 months (60-270 m.)
For entire cohort (n=140): 198 developed recurrent EC in the entire cohort (n=355) 96 % occurred prior to the 5th postoperative year. 107 in the first year (54%), 43 (22%) patients in year 2, 27 (14%) in
year 3, 7 (4%) in year 4, 6 (3%) in year 5, and 8 (4%) after year 5.
In 5-year survivors (n=140): 32 (23%) developed recurrence. Local in 3 patients (2%), Regional in 11 (7.9%), Distant in 16
(11.4%) and both regional and distant in 2 (1.4%) patients. 11 patients survived at least 5 years after treatment of their recurrence.
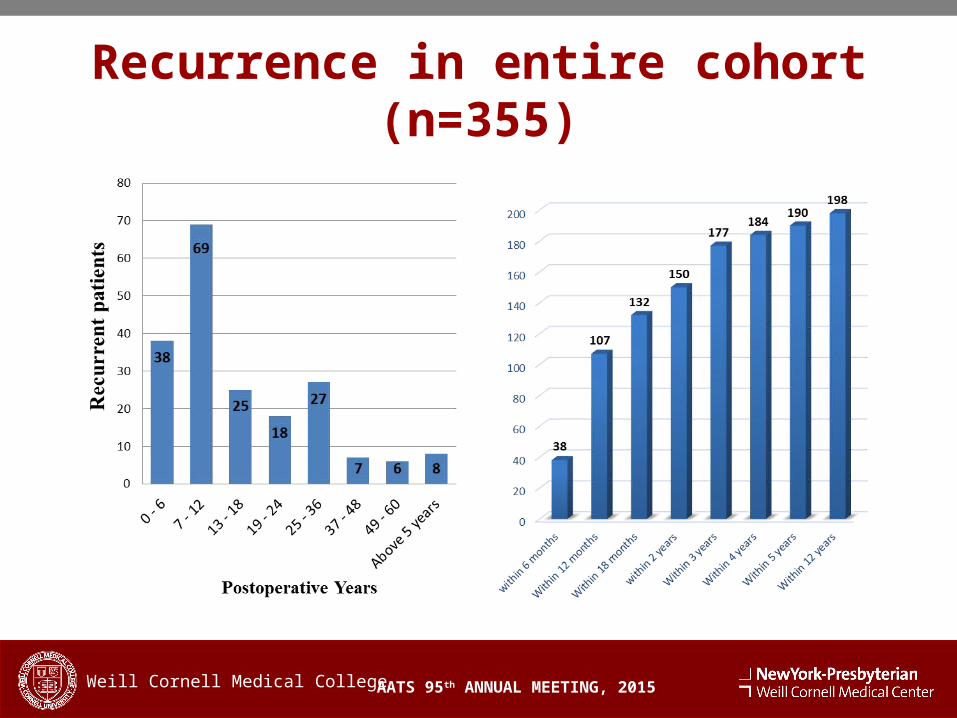
Recurrence in entire cohort (n=355)
AATS 95th ANNUAL MEETING, 2015Weill Cornell Medical College