Embed Size (px)
Citation preview
03/07/2016
1
Baby, you are HOT! Febrile illnesses in the
pediatric population
Susan Wood RN Paramedic NWC EMSS Educator
February 2016
Pediatric Patients
System CE in last 2 years reviewed:
general assessment abuse,asthma
seizures and cardiac arrest.
Assessment
A systematic approach is important, so throughout the encounter, a paramedic should be assessing for
causative factors…
Such as? Hypoxemia
Acidosis
Hypovolemia
Hypoglycemia
Hypothermia
Trauma
Infection
SOP p. 60
Goals 1. Create a greater awareness of childhood
illnesses encountered pre-hospital with unusual presentations
2. Gain insight regarding modes of transmission and level of protection for disease specific illnesses
3. Prioritize prehospital care for individuals with a presentation of a febrile illness and/or rash
Class Outline
• Power Point presentation
• Case studies
• Handout outline:
– Article, “Fever in the Neonate and young infant”
– p. 8 Grid for note taking throughout lecture
– p. 9-14 Case study rubrics
EMS is called to a single family house for the “sick child.” Upon arrival further information reveals a 14 day premature infant who is now 4 days old in the care of a 19 year old mother who states he felt hot and had a fever. Grandmother also present.
Information received reveals that the neonate came home 2 days ago and due for follow up physician appt. tomorrow.
03/07/2016
2
What should EMS be thinking about with this limited initial
information?
Is this a concern that can wait until the doctors visit tomorrow morning or should they go back to the hospital now?
Fever in the neonate
• It is one of the most common chief complaints for peds pts presenting to the ED
• Approximately up to 20%
• Fever is clinically more important for those 0-3 months of age
Alpern ER, Henretig FM. Fever. In: Fleisher GR, Ludwg S, Henretig FM, eds, Textbook of Pediatric Emergency Medicine 5th ed.
Philadelphia, PA: Lippincott Williams & Wilkins, pp. 295–306, 2006.
EMS has seen it all
Thoughts on this scenario can include:
young mom, not knowledgeable…
is she just afraid?
is the fever accurate?
Next steps for EMS…
Next steps…general impression
PAT-Pediatric Assessment Triangle
includes:
general appearance
work of breathing
circulation
(SKIN tells all)
Bottom line…
Do they look sick or not?
And if they do, intervention follows quickly.
If they don’t, what is next?
History is important
Because of this given situation in which the information may not come freely flowing, it is up
to EMS to ask the right questions, in the right way, to appreciate the severity of illness
Children < 3 mos old have unique risks for serious bacterial infections (SBI)
03/07/2016
3
Serious bacterial infections (SBI)
Neonates (less than 28 days old)
Young infants (28-90 days old)
Traditionally thought of as a subset of infants because of the potential for severity level with
infections
Serious bacterial infections (SBI)
Most common:
UTI
Bacteremia (infection w/o a focused source)
Meningitis
*While the current practice of immunizing has ↓ the risk, the
trend is changing and vaccination is not guaranteed.
Back to that fever
• Often only indication for concern is a fever
– Body temp is regulated by the thermosensitive neurons in the hypothalamus
• While an infants body temperature can vary based on age and even time of day, a fever is considered something of concern.
What then defines a fever?
Baby you are hot tonight!
Physicians will generally agree that a fever is defined for the child appropriately dressed at rest is:
• Rectal temp of 38°C (100.4°F)
• Oral temp of 37.2°C (99°F) (used only when >5 yo)
American Academy of Pediatrics
Where does that fever come from and how can EMS discover
the origin?
perhaps investigation is needed as to…
…where the infant came from?
HUH?
03/07/2016
4
This adorable bundle of (sick) joy came from:
A galaxy far, far away….
But perhaps…
Did/does mom have any medical illnesses?
Did mom have any/all prenatal care?
Did mom allow immunizations?
Is mom breastfeeding?
It’s complicated
The maturing immune system is a work in progress
Immunity is either innate (within) or acquired
Acquired immunity is either active or passive
How does one acquire passive immunity?
Active immunity?
History and Physical
Important information to ask about:
“is the child going to be immunized?”
If not, at greater risk for infection…
“Is the child breastfeeding?”
In addition to Immunoglobulin G (IgG), mother’s breast milk contains IgD, IgE, IgM.
So now that fever is not…”just a fever.”
Bottom line….any child less than 3 months of age with a fever should be
transported to the hospital for further evaluation or clear instruction
to the parent of risk
Fever = Infection (until proven otherwise)
• First week of life
– Maternal acquired pathogens
• Second week
– Hospital acquired
What should EMS recommend be done with the infant in the opening
scenario?
It is always prudent to encourage treatment
Transport is important due to nature of illness in a high risk population
Waiting is not recommended as the underlying problem is NOT able to be understood without further evaluation.
The very young infants that do not eat can become dehydrated, added to that a fever and they can deteriorate rapidly!
03/07/2016
5
What else does EMS want to evaluate?
What questions should be asked to appreciate a child’s hydration status?
Additional history components
Any hx of previous hospitalization or ICU stay?
Did child have any prior use of antibiotics?
Any prior use of antipyretics?
If so, what time?
↓ fever after Tylenol should not exclude a SBI.
Fevers to be concerned about
When they look sick…
When they appear in pain
Difficulty breathing
Appear dehydrated
Airway and breathing
Increased WOB includes:
retractions
nasal flaring
grunting
Noises kids make
In addition to fever, kids make all sorts of noises
Noises heard while breathing include:
Hoarse or raspy cry (croup)
Muffled voice or ᴓ talking (epiglottitis)
Snoring (upper airway obst.)
Wheezing on expiration (lower airway obst.)
Crackles (pneumonia/bronciolitis)
STRIDOR (croup ~ 90%; epiglottitis ~ 10%)
FEVER + Noise + AMS
This is never a good sign
One can assume pt distress
Supportive care
TRANSPORT
03/07/2016
6
So many things
Croup
Meningitis
Bronchiolitis
Epiglottitis
Asthma
RSV
What is highest priority?
Flu
Chicken pox
Rubella
Abuse
Everything cannot be covered
Today: Concentrated effort will be on communicable
illnesses seen in children with fevers
Rashes, whoops and weird stuff!
Scenario 3
Arrive at a single family home for the child who parent states, “just had a seizure.”
EMS finds a 13 month old child in the care of parents.
Two older school aged children are also in the home and crying in concern for their sibling.
Child is limp, appears post-ictal lying on floor.
Child is on floor with blanket underneath body. Diaper wet. Mom states that the child has had a cold for the last 4 days & developed a fever last night to 38.7°C/ 101.6°F.
laying on floor, eyes closed, no movement of extremities
labored deep breathing
very pink, flushed & hot to touch. Also noted is a red petechial rash over chest, abdomen & extremities.
no FBAO
deep breathing noted with intermittent
snoring respirations
as noted above; fast and regular distal
pulse
bGL 96; pupils are slow but reactive
03/07/2016
7
Treatment priorities? EMS (self) protection/priorities?
T: 40°C/104.0°F, HR: 120, R 22, Pox: 94%
Lungs clear, adequate air movement.
Parent states that the infant has been irritable and had difficulty taking in normal fluids by mouth or eating regular meals.
There is bulging at fontanel noted.
Meningitis “Meningococcal disease refers to an illness caused by type of bacteria known as meningococcus….
May develop in response to # of causes, bacteria or viruses, physical injury, cancer or certain drugs
Illnesses are often severe & include infections of the protective membranes covering the brain known as meninges, spinal cord (meningitis) & bloodstream infections (bacteremia or septicemia).”
CDC
Mode of transmission
Severity of illness & treatment for meningitis differ depending on cause
Thus, it is important to know the specific cause
“Spread through exchange of respiratory & throat secretions …
…can be treated w/ antibiotics, but quick medical attention is extremely important.”
• CDC
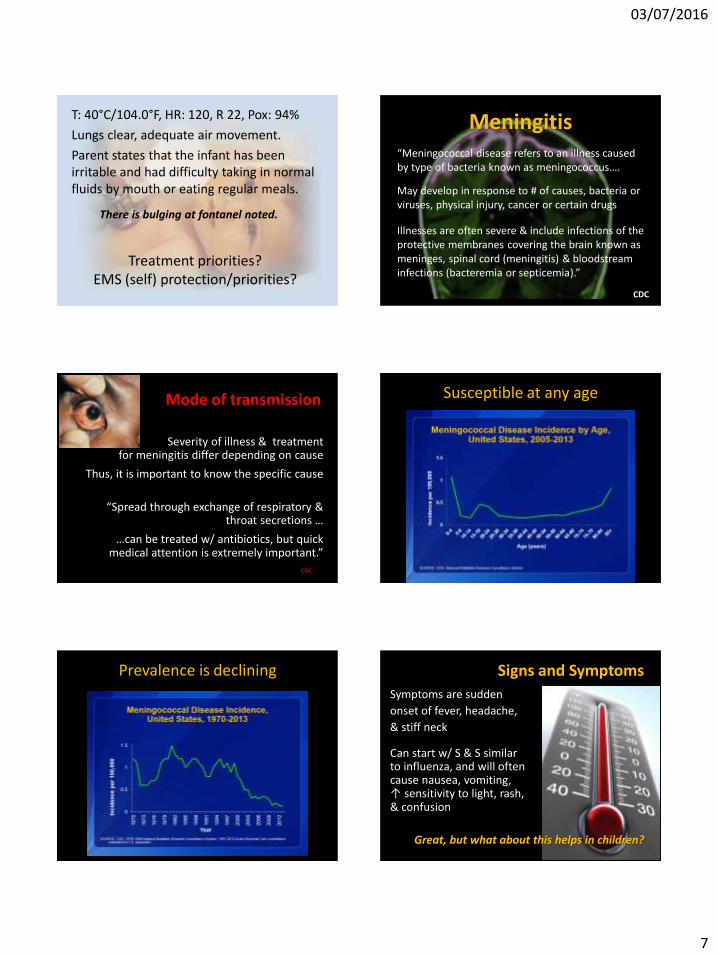
Susceptible at any age
Prevalence is declining Signs and Symptoms
Symptoms are sudden
onset of fever, headache,
& stiff neck
Can start w/ S & S similar to influenza, and will often cause nausea, vomiting, ↑ sensitivity to light, rash, & confusion
Great, but what about this helps in children?
03/07/2016
8
Fever we know, but…
Headache How is this seen with children? Stiff neck …Completely unreliable w/ infants Confusion What will be noticed? No oral intake, irritable, crying all the time, hx. of infection or prolonged hospital stay. The symptoms of meningococcal meningitis can appear quickly or over several days. Sx. develop w/in 3-7 d after exposure.
Greatest concern is
potential to rapidly
deteriorate
Description, & Presentation
Viral more common, also called aseptic meningitis
Caused by enterovirus
Incubation period 3-7 d
In newborns, bacterial concern from maternal transmission - more severe; treatment with antibiotics
Sudden: less common but more likely to progress to shock, rash noted, poor prognosis (septicaemia)
Gradual: more common presents w/ fever & URI or GI
While most people recover, serious complications such as brain damage, hearing loss, or learning disabilities can occur.
There are several pathogens (types of germs) that can cause bacterial meningitis including haemophilus influenzae (most often caused by type b, Hib), & others
In the US, about 4,100 cases of bacterial meningitis, including 500 deaths from 2003–2007
Viral Most common type
Often less severe and people usually get better on their own
EXCEPT for Infants younger than 1 month & people with weakened immune systems are more likely to have severe illness
There is a fungal meningitis although rare
Usually spread of fungus through blood to the spinal cord~ people with weakened immune systems ; not contagious
Primary amebic meningoencephalitis (PAM) is a very rare form of parasitic meningitis that causes a brain infection that is usually fatal
03/07/2016
9
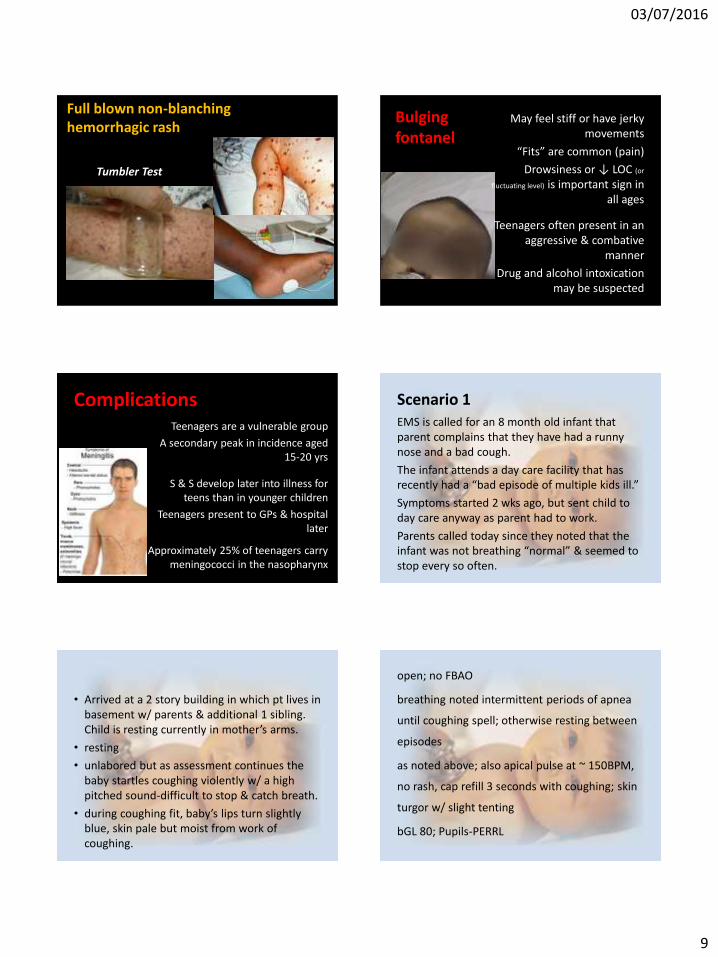
Full blown non-blanching hemorrhagic rash
Tumbler Test
Bulging fontanel
May feel stiff or have jerky movements
“Fits” are common (pain)
Drowsiness or ↓ LOC (or
fluctuating level) is important sign in all ages
Teenagers often present in an aggressive & combative
manner
Drug and alcohol intoxication may be suspected
Complications Teenagers are a vulnerable group
A secondary peak in incidence aged 15-20 yrs
S & S develop later into illness for teens than in younger children
Teenagers present to GPs & hospital later
Approximately 25% of teenagers carry meningococci in the nasopharynx
Scenario 1 EMS is called for an 8 month old infant that parent complains that they have had a runny nose and a bad cough.
The infant attends a day care facility that has recently had a “bad episode of multiple kids ill.”
Symptoms started 2 wks ago, but sent child to day care anyway as parent had to work.
Parents called today since they noted that the infant was not breathing “normal” & seemed to stop every so often.
• Arrived at a 2 story building in which pt lives in basement w/ parents & additional 1 sibling. Child is resting currently in mother’s arms.
• resting
• unlabored but as assessment continues the baby startles coughing violently w/ a high pitched sound-difficult to stop & catch breath.
• during coughing fit, baby’s lips turn slightly blue, skin pale but moist from work of coughing.
open; no FBAO
breathing noted intermittent periods of apnea
until coughing spell; otherwise resting between
episodes
as noted above; also apical pulse at ~ 150BPM,
no rash, cap refill 3 seconds with coughing; skin
turgor w/ slight tenting
bGL 80; Pupils-PERRL
03/07/2016
10
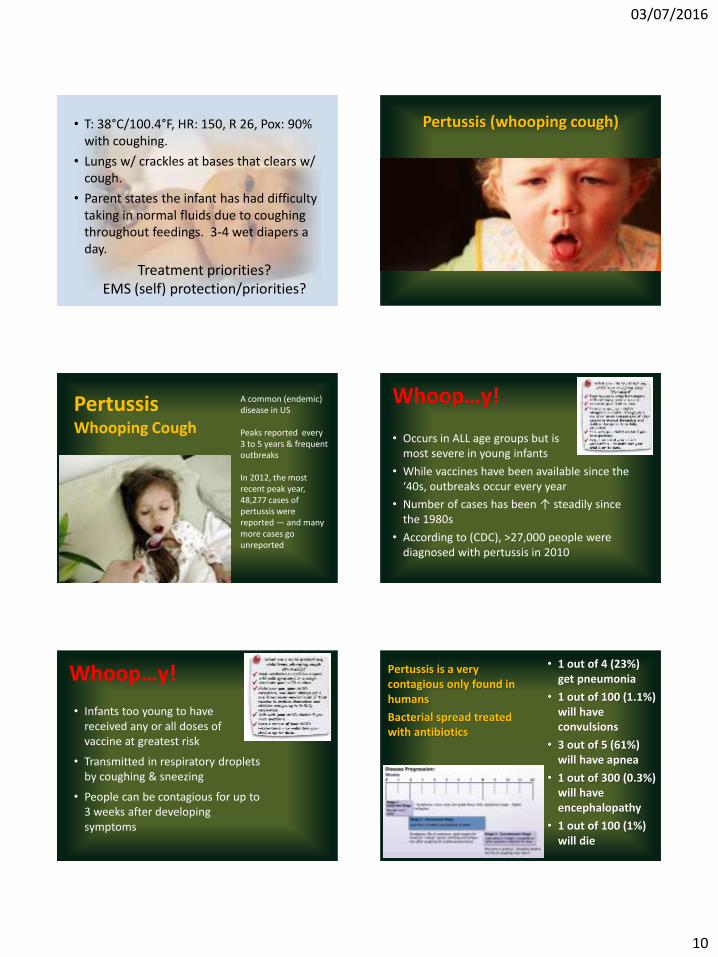
Treatment priorities? EMS (self) protection/priorities?
• T: 38°C/100.4°F, HR: 150, R 26, Pox: 90% with coughing.
• Lungs w/ crackles at bases that clears w/ cough.
• Parent states the infant has had difficulty taking in normal fluids due to coughing throughout feedings. 3-4 wet diapers a day.
Pertussis (whooping cough)
Pertussis Whooping Cough
A common (endemic) disease in US Peaks reported every 3 to 5 years & frequent outbreaks In 2012, the most recent peak year, 48,277 cases of pertussis were reported — and many more cases go unreported
Whoop…y!
• Occurs in ALL age groups but is most severe in young infants
• While vaccines have been available since the ‘40s, outbreaks occur every year
• Number of cases has been ↑ steadily since the 1980s
• According to (CDC), >27,000 people were diagnosed with pertussis in 2010
Whoop…y!
• Infants too young to have received any or all doses of vaccine at greatest risk
• Transmitted in respiratory droplets by coughing & sneezing
• People can be contagious for up to 3 weeks after developing symptoms
Pertussis is a very contagious only found in humans
Bacterial spread treated with antibiotics
• 1 out of 4 (23%) get pneumonia
• 1 out of 100 (1.1%) will have convulsions
• 3 out of 5 (61%) will have apnea
• 1 out of 300 (0.3%) will have encephalopathy
• 1 out of 100 (1%) will die
03/07/2016
11
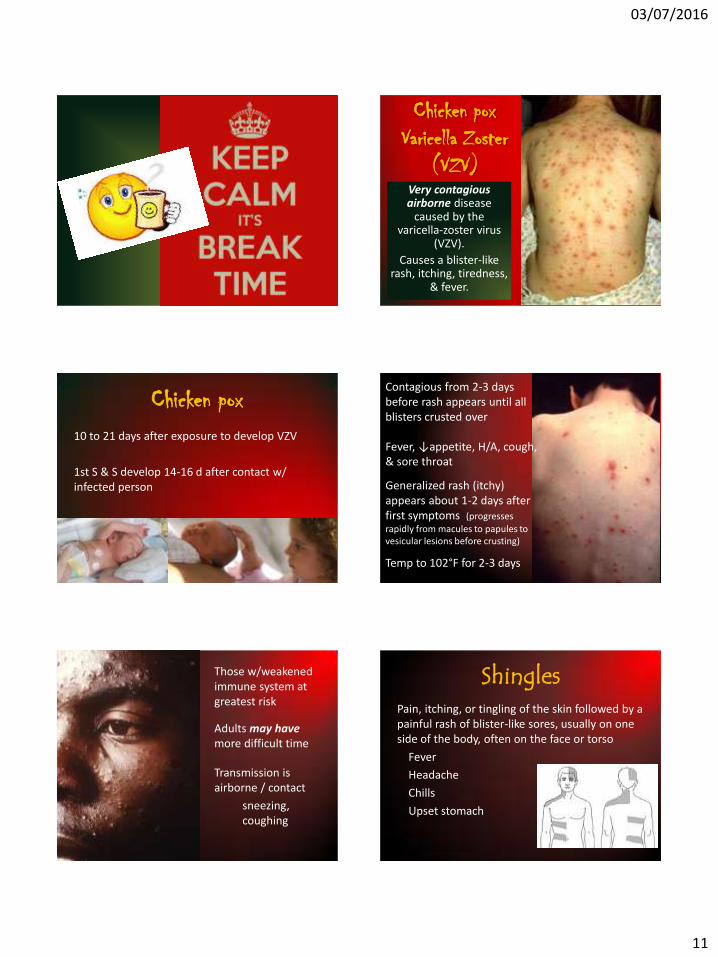
BREAK Chicken pox
Varicella Zoster (VZV)
Very contagious airborne disease
caused by the varicella-zoster virus
(VZV).
Causes a blister-like rash, itching, tiredness,
& fever.
Chicken pox 10 to 21 days after exposure to develop VZV
1st S & S develop 14-16 d after contact w/ infected person
Contagious from 2-3 days before rash appears until all blisters crusted over
Fever, ↓appetite, H/A, cough, & sore throat
Generalized rash (itchy) appears about 1-2 days after first symptoms (progresses
rapidly from macules to papules to vesicular lesions before crusting)
Temp to 102°F for 2-3 days
Those w/weakened immune system at greatest risk
Adults may have more difficult time
Transmission is airborne / contact
sneezing, coughing
Shingles Pain, itching, or tingling of the skin followed by a painful rash of blister-like sores, usually on one side of the body, often on the face or torso
Fever
Headache
Chills
Upset stomach
03/07/2016
12
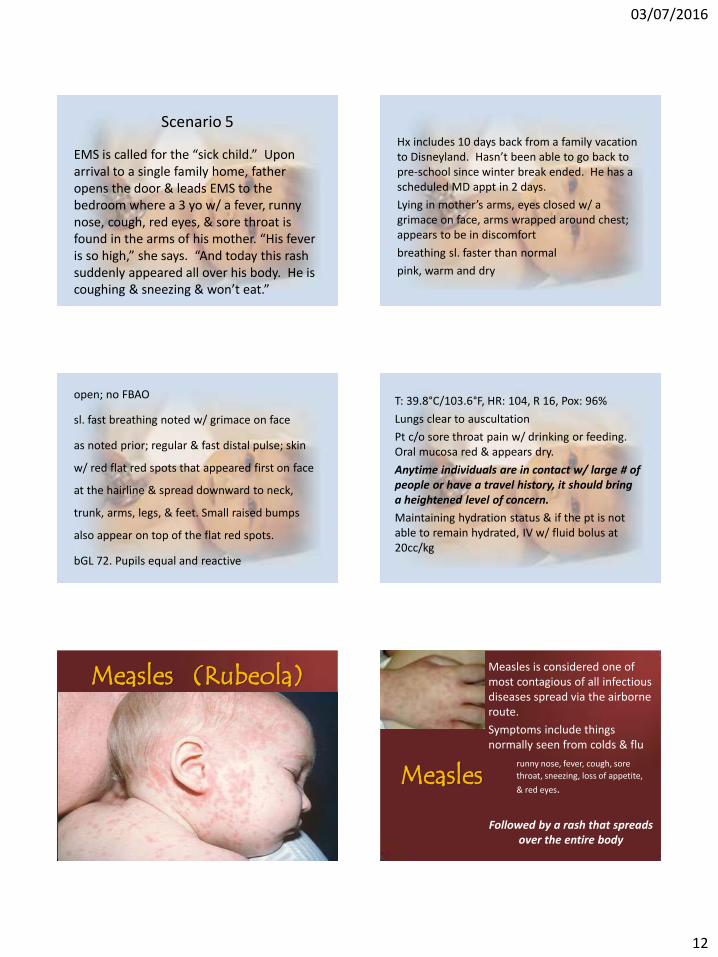
Scenario 5
EMS is called for the “sick child.” Upon arrival to a single family home, father opens the door & leads EMS to the bedroom where a 3 yo w/ a fever, runny nose, cough, red eyes, & sore throat is found in the arms of his mother. “His fever is so high,” she says. “And today this rash suddenly appeared all over his body. He is coughing & sneezing & won’t eat.”
Hx includes 10 days back from a family vacation to Disneyland. Hasn’t been able to go back to pre-school since winter break ended. He has a scheduled MD appt in 2 days.
Lying in mother’s arms, eyes closed w/ a grimace on face, arms wrapped around chest; appears to be in discomfort
breathing sl. faster than normal
pink, warm and dry
open; no FBAO
sl. fast breathing noted w/ grimace on face
as noted prior; regular & fast distal pulse; skin
w/ red flat red spots that appeared first on face
at the hairline & spread downward to neck,
trunk, arms, legs, & feet. Small raised bumps
also appear on top of the flat red spots.
bGL 72. Pupils equal and reactive
T: 39.8°C/103.6°F, HR: 104, R 16, Pox: 96%
Lungs clear to auscultation
Pt c/o sore throat pain w/ drinking or feeding. Oral mucosa red & appears dry.
Anytime individuals are in contact w/ large # of people or have a travel history, it should bring a heightened level of concern.
Maintaining hydration status & if the pt is not able to remain hydrated, IV w/ fluid bolus at 20cc/kg
Measles (Rubeola)
Measles
Measles is considered one of most contagious of all infectious diseases spread via the airborne route.
Symptoms include things normally seen from colds & flu
runny nose, fever, cough, sore
throat, sneezing, loss of appetite,
& red eyes.
Followed by a rash that spreads over the entire body

03/07/2016
13
Measles Rash begins 3-5 days after symptoms start
Begins as flat red spots appearing on face (hairline) & spread to neck, trunk, arms, legs, & feet
Small raised bumps may also appear on top of flat red spots
The spots may become joined together as they spread from the head to the rest of the body.
When rash appears, fever may spike to ↑ 104°F.
*July 2, 2015, Washington State DoH confirmed a measles-related death.
Measles Before measles vaccination program started ~ 1963, estimates about 3 - 4 M/yr got measles in the US.
Of those, 400-500 died, 48,000 were hospitalized, & 4,000 got encephalitis (brain swelling)
In 2013, national coverage for MMR vaccine among children aged 19—35 months was 91.9%.
Measles In 2000, the United States declared that measles was eliminated from this country.
People who receive 2 vaccine doses are considered protected for life & do not need booster.
Koplik Spots
2-3 days after symptoms begin, tiny
white spots with redness may appear
inside mouth
• To ↓ risk, EMS transporting pts with S & S should wear masks
• U.S. experienced a record # of cases during 2014, 644 cases in 27 states — more than 3 X # of reported cases in 2013 & over 10 X # of cases reported in 2012 to CDC
• ↑est # of cases since elimination documented in 2000
What now?
03/07/2016
14
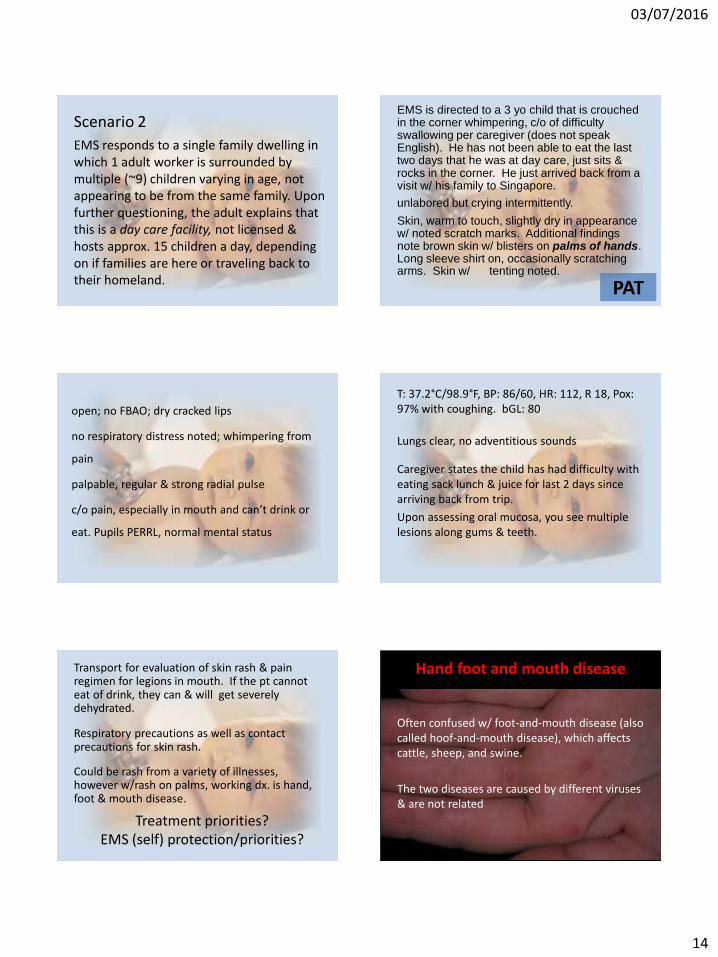
Scenario 2
EMS responds to a single family dwelling in which 1 adult worker is surrounded by multiple (~9) children varying in age, not appearing to be from the same family. Upon further questioning, the adult explains that this is a day care facility, not licensed & hosts approx. 15 children a day, depending on if families are here or traveling back to their homeland. PAT
EMS is directed to a 3 yo child that is crouched in the corner whimpering, c/o of difficulty swallowing per caregiver (does not speak English). He has not been able to eat the last two days that he was at day care, just sits & rocks in the corner. He just arrived back from a visit w/ his family to Singapore.
unlabored but crying intermittently.
Skin, warm to touch, slightly dry in appearance w/ noted scratch marks. Additional findings note brown skin w/ blisters on palms of hands. Long sleeve shirt on, occasionally scratching arms. Skin w/ tenting noted.
open; no FBAO; dry cracked lips
no respiratory distress noted; whimpering from
pain
palpable, regular & strong radial pulse
c/o pain, especially in mouth and can’t drink or
eat. Pupils PERRL, normal mental status
T: 37.2°C/98.9°F, BP: 86/60, HR: 112, R 18, Pox: 97% with coughing. bGL: 80
Lungs clear, no adventitious sounds
Caregiver states the child has had difficulty with eating sack lunch & juice for last 2 days since arriving back from trip.
Upon assessing oral mucosa, you see multiple lesions along gums & teeth.
Treatment priorities? EMS (self) protection/priorities?
Transport for evaluation of skin rash & pain regimen for legions in mouth. If the pt cannot eat of drink, they can & will get severely dehydrated.
Respiratory precautions as well as contact precautions for skin rash.
Could be rash from a variety of illnesses, however w/rash on palms, working dx. is hand, foot & mouth disease.
Hand foot and mouth disease
Often confused w/ foot-and-mouth disease (also called hoof-and-mouth disease), which affects cattle, sheep, and swine.
The two diseases are caused by different viruses & are not related

03/07/2016
15
Hand foot and mouth disease
Outbreaks not common in United States; more so in Asia, with 1000’s infected
Occurs particularly in young children, may be severe enough to require hospitalization
As of August 15, Singapore reported more than 18,000 cases of HFMD in 2015
Who cares?
Remember, people travel!
Hand foot & mouth disease
Viral illness
Affects infants & children younger than 5 years old but can occur in adults
Starts with a fever, ↓ appetite, sore throat, malaise
1-2 d after fever, painful sores develop in mouth, then on palms of hands & soles of feet May also appear on knees, elbows, buttocks or genital area
Small red blisters / ulcers
Hand foot and mouth disease
Some people, especially young children, may get dehydrated if they are not able to swallow
because of painful mouth sores
Hand foot and mouth disease
Caused by viruses that belong to the Enterovirus genus (group), including polioviruses, coxsackieviruses, echoviruses, and enteroviruses.
Same virus that causes meningitis so could cause it as well
Hand foot and mouth disease
Virus found in:
nose & throat secretions, blister fluid, & feces
Mode of transmission:
Respiratory and contact precautions
There is no specific treatment except over-the-counter medications to relieve pain
Scenario 6
EMS is called for abdominal pain. Upon arrival, a caregiver opens the door, explaining that the 4 year old child has had nausea, vomiting & explosive diarrhea for 2 days.
Every time an attempt is made to eat, it is met with resistance as it just keeps coming back up.
03/07/2016
16
Found on the couch, an obviously fatigued,
lethargic child wrapped in a blanket holding
their stomach
breathing normal
pale, dry & cool to touch.
T: 37.1°C/98.8°F, BP: 70/54, HR: 130, R22, Pox: 99%
Lungs clear to auscultation
Oral mucosa dry, skin turgor poor; unable to maintain oral intake for 2 days.
Do you start an IV? When is it indicated in the dehydrated child?
Fluid bolus for rehydration?
Contact precautions; do not touch anything that may have come in contact with fecal matter! Gowns are needed….and Good luck
Acute gastroenteritis (AGE) Norovirus
Norovirus Most common cause of AGE in the US
Each year, it causes 19-21 million illnesses & contributes to 56,000-71,000 hospitalizations & 570-800 deaths
Norovirus is also most common cause of foodborne-disease outbreaks in US
Norovirus Very contagious & can infect anyone
Mode of transmission from infected person, contaminated food, water, or by touching contaminated surfaces
Contact precautions should be taken
Prevention: practice proper hand washing
03/07/2016
17
A person usually develops symptoms 12 to 48 hours after being exposed
Most people get better within 1 - 3 days
Causes inflammation of stomach / intestines resulting in pain, N/V, diarrhea, low grade fever & generalized aching
Risk for dehydration especially in young children and older adults...
Information sent system
wide on Jan. 20th, 16
As a reminder…
From CE 2013
3 Ds and some Bs DNR (POLST) form
D10 for hypoglycemia
Dopamine documentation
Be safe
Be smart
Be current EMS CE May, 2013
D D D B
Turn the corner to some infection control issues
Just out
We’re not immune to infection control challenges
In handout

03/07/2016
18
Norovirus gastroenteritis
Outbreaks in
System areas
Norovirus gastroenteritis
It is extremely important that EMS use Contact and Standard precautions when responding to and transporting pts with vomiting and diarrhea
Contact precautions
Be safe
Hand Hygiene
During outbreaks, wash hands with soap and water immediately after removing gloves instead of only using the alcohol-based waterless sanitizer if suspected or confirmed norovirus gastroenteritis.
For all other hand hygiene indications refer to the 2002 HICPAC Guideline for Hand Hygiene in Health-Care Settings:
http://www.cdc.gov/mmwr/PDF/rr/rr5116.pdf ).
Increase frequency of cleaning and disinfection of pt care areas and frequently touched surfaces during outbreaks of norovirus
Cleaning and disinfecting of ambulance should be done before transporting another pt.
Procedures for cleaning:
Spray all surfaces with EPA-approved disinfectant; hold cleaning agent dispenser 10” from surface and atomize with quick short strokes, spraying evenly on (potentially) contaminated areas of equipment and affected interior pt compartment or other affected portions of vehicle until wet. Wait 30 seconds and wipe dry with paper towel.
To kill staph, strep, and other virus and bacteria strains, repeat as above, wait 10 minutes, and wipe dry
Blood and other body fluids must be thoroughly cleaned from surfaces and objects before applying disinfectant
Use Standard Precautions for handling soiled pt-service items or linens, including appropriate use of PPE
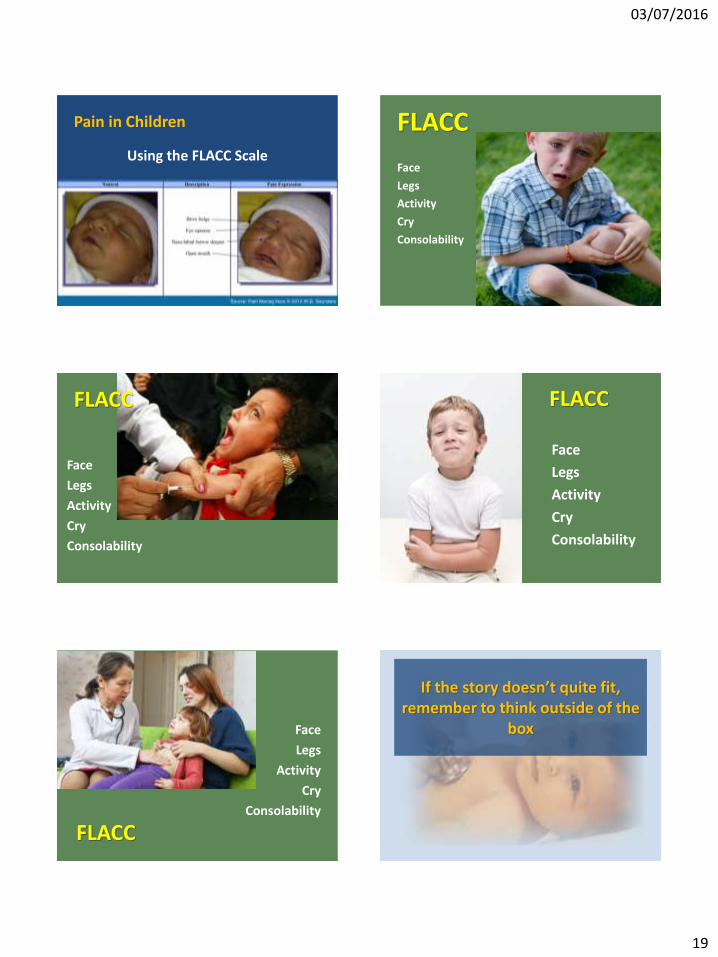
The Pain Factor
As a reminder for
pediatric patients,
assessment should also
include monitoring
pain
03/07/2016
19
Pain in Children
Using the FLACC Scale
FLACC
Face
Legs
Activity
Cry
Consolability
FLACC
Face
Legs
Activity
Cry
Consolability
Face
Legs
Activity
Cry
Consolability
FLACC
Face
Legs
Activity
Cry
Consolability
FLACC
If the story doesn’t quite fit, remember to think outside of the
box
03/07/2016
20
Scenario 4
Dispatched for the “sick child.”
Information of a 5 yo unresponsive.
It’s a warm, sunny summer day; EMS arrives at an apt complex, escorted to an apt in which 3 families live together. 5 adults & 6 children reside in a 2 br apt. There are 2 teens present, 2 school aged children & 2 babies in only diapers in a playpen crying. The teen explains that the 5 yo brother was sleeping on the bed when they heard a “thud.”
“He must have fallen off the top bunk bed,” he explained, “then started shaking all over.”
Found a small, underdeveloped child slow to respond on the couch.
Within 2 min of arrival, pt has a generalized complex seizure again.
laying on couch, eyes staring up and to the right, no movement of extremities
irregular deep breathing
pink, warm and dry.
snoring respirations; no FBAO
deep breathing noted with intermittent snoring after seizure
as noted above; regular distal pulse; skin w/ noted small round shaped marks (~2cm in
diameter) & multiple bruises on body & back of legs
bGL 74; Pupils are dilated & slow to respond
T: 37.1°C / 98.8°F, BP: 130/86, HR: 90, R 15, Pox: 97%
Lungs clear to auscultation
With no other history found, never let your guard down to the possibility of abuse.
Transport necessary to a L1 trauma center; and report suspicions to DCFS per policy.
Unknown origin; standard precautions
*Great JOB*
Any questions?


























