Embed Size (px)
Citation preview

B-RAF and melanocytic neoplasia
Melissa Gill, MD,a and Julide Tok Celebi, MDb
New York, New York
High frequency of B-RAF gene mutations has recently been identified in benign melanocytic nevi andmelanoma. This review focuses on clinical studies that evaluate the role of B-RAF in melanocytic neoplasia.( J Am Acad Dermatol 2005;53:108-14.)
Melanoma is the fifth and seventh most com-monly diagnosed cancer in American menand women, respectively.1 Currently, it is
estimated that 1 in 55 men and 1 in 82 women in theUnited States will be diagnosedwithmelanoma in hisor her lifetime. Despite the frequency with whichmelanoma is encountered, relatively few advances inthe treatment of melanoma have been made and themortality rate continues to rise.2 Several genes havebeen implicated in the pathogenesis of melanoma;however, the molecular basis of melanoma is largelyunknown. Understanding the genetics of melano-cytic neoplasms will aid physicians in the manage-ment of patients with melanoma by improvingdiagnostic and prognostic accuracy and eventuallyallowing for molecular-targeted therapy. Recently,the identification of high-rate mutations in the B-RAFgene in melanoma has drawn attention to B-RAF andits signaling pathway, not only for its importancein melanoma development, but also as a potentialtherapeutic target.3 This review summarizes the cur-rent knowledge of the role of B-RAF in melanocyticneoplasia with an emphasis on clinical data.
B-RAF and the RAS-RAF-MEK-ERK signalingpathway
B-RAF is a proto-oncogene located on chromo-some 7 (7q34). Its protein product is a member of theRAF family of serine/threonine protein kinases,
From the Departments of Pathologya and Dermatology,b Colum-
bia University.
Supported by National Institutes of Health/National Institute
of Arthritis and Musculoskeletal and Skin Diseases grant
K08 AR050273 (to J. T. C.) and the Dermatology Foundation
(to J. T. C.).
Conflicts of interest: None.
Reprint requests: Julide Tok Celebi, MD, Columbia University,
Department of Dermatology 630 W 168th St, VC15-202,
New York, NY 10032. E-mail: [email protected].
0190-9622/$30.00
ª 2005 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2005.04.013
108
which includes A-RAF, B-RAF, and C-RAF (alsoknown as RAF-1). The RAFs are key regulatoryproteins that signal through the RAS-RAF-MEK-ERKpathway. This pathway, under physiologic condi-tions, is activated by mitogens, growth factors, andcytokines and regulates cell growth, survival, anddifferentiation (summarized in Fig 1).4 Constitutiveactivation of this signaling pathway is observed in avariety of cancers, one of which is melanoma.Activating mutations in N-RAS and B-RAF that leadto constitutive activation of the pathway are found inapproximately 10% and 66% of melanomas, respec-tively.3,5 Of the RAS (N-RAS, K-RAS, H-RAS) and RAF(A-RAF, B-RAF, C-RAF) isoforms, the majority ofmutations in melanoma are in N-RAS or B-RAF.K-RAS and H-RAS mutations are rare, and A-RAFand C-RAF mutations have not been described.6
Importantly, N-RAS and B-RAF mutations are ob-served in amutually exclusive fashion inmelanoma.7
B-RAF has 3 functional domains, one of which is thekinase domain where most activating mutations in B-RAF cluster (Fig 2). The hotspot mutation in B-RAF isthe substitution of valine to glutamine at amino acid599 (originally designated and commonly referred toas V599E mutation; however, the actual amino acidnumber was later recognized to be 600 (V600E) andaccounts for more than 90% of B-RAF mutations inmelanoma.5
B-RAF and melanomaThe majority of melanomas occur sporadically
(sporadic melanoma, 90%) and only a small percent-age show familial clustering (familial melanoma, 5%-12%). Familial melanoma has been associated withCDKN2A/ARF and CDK4 gene mutations that ac-count for 20% to 40% and 2% of familial cases,respectively.8 Although several genes and signalingpathways have been implicated in the pathogenesisof melanoma, the molecular basis of sporadic mel-anoma remains largely uncharacterized. In 2002, B-RAF gene mutations were identified in a wide rangeof human cancers, the highest frequency occurring

J AM ACAD DERMATOL
VOLUME 53, NUMBER 1
Gill and Celebi 109
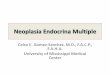
Fig 1. Schematic diagram of the RAS-RAF-MEK-ERK signaling pathway. A mitogen, growthfactor, or cytokine binds to its respective membrane receptor, causing a change in confirmationof the receptor and autophosphorylation. Attached phosphates (P) recruit the Shc-Grb2-SOScomplex to the cell membrane, where it activates RAS by exchanging GDP for GTP. ActivatedGTP-RAS binds B-RAF, recruiting it from its inactivated state in the cytoplasm to the cellmembrane, where, through a series of reactions, it can be converted to its active phosphor-ylated state. Phosphorylation and activation of B-RAF leads to phosphorylation and activationof MEK and subsequently ERK. Active, phosphorylated ERK is able to translocate into thenucleus where it can phosphorylate and thus activate transcription factors (TFs), leading totranscription of genes that regulate cellular proliferation and survival. BAY 43-9006, an orallyadministered small molecule, inhibits this signaling pathway at the level of RAF.
in melanoma (66%).3 Subsequently these findingswere confirmed, and B-RAF remains the only geneknown to date to be altered in the majority ofsporadic melanomas (summarized in Table I).Although B-RAF somatic mutations are common inmelanoma, germline B-RAF mutations are absent orrare in melanoma-prone families9,10 and patientswith sporadic melanoma.11 Surprisingly, however,commonmelanocytic nevi were also found to harbora high rate of B-RAF mutations, suggesting that B-RAF plays a role in the pathogenesis of a subset ofbenign and malignant melanocytic neoplasms.
In this article, we review clinical studies thatevaluate the mutational profile of the B-RAF genein melanocytic neoplasms. However, it is difficult tocompare these studies because of differences instudy design, small sample size, tumor types studied(primary tumor vs cell line), and differences inmutation detection techniques. The majority of thesestudies analyze primary tumors, which may under-estimate the true prevalence of B-RAF mutations.Thus it is important to interpret the results with thesevariables in mind. Readers may also refer to excellentreviews on the molecular understanding of B-RAFand its signaling pathway.6,12,13
The role of B-RAF in early versus late stagesof melanoma development. Several studies eval-uated the involvement of B-RAF during initiation andprogression of primary melanoma, as well as in
metastatic disease. Studies show no correlation withB-RAFmutation status and Breslow thickness, whichsuggests that B-RAF activation occurs early in tumor-igenesis. Evaluation of radial- versus vertical-growthphase melanoma has resulted in contradictory find-ings. One study showed a low frequency of B-RAFmutations in radial-growth phase melanoma (10%)compared with vertical-growth phase melanoma(63%), which suggests that B-RAF may be importantfor melanoma progression rather than initiation.14 Bycontrast, another study found B-RAFmutations in theradial-growth phase and in the corresponding verti-cal-growth phase of all 8 melanomas analyzed.7
Similar to primary cutaneous melanoma, a highfrequency of B-RAF mutations (44%-68%)15-17 isfound in metastatic melanomas, which implies thatB-RAF may be important for melanocyte transforma-tion but not for metastatic spread. B-RAF mutationswere not found to be associatedwith specific sites formetastases (lymphatic vs hematogenous).15,16
B-RAF and melanoma subtypes by anatomicsite, a link to UV exposure? Although cutaneous,uveal, and mucosal melanomas arise from the samecell type (the neural crestederived melanocyte),these melanoma subgroups show distinct epidemi-ologic patterns, clinical behaviors, and genetic aber-rations, which suggests that distinct molecularpathways for their development. Uveal melanomaoriginates from melanocytes of the choroid, ciliary

J AM ACAD DERMATOL
JULY 2005
110 Gill and Celebi
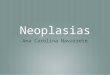
Fig 2. Schematic diagram of B-RAF protein. B-RAF protein is 765 amino acids in length andcontains 3 conserved regions. Conserved region 1 (CR1) is near the NH2-terminus and containsthe RAS-binding domain. Conserved region 2 (CR2) is located near protein’s center andcontains regulatory sites. Located toward the COOH-terminus of B-RAF is conserved region 3(CR3), the kinase domain, which contains a glycine-rich P loop and the protein’s activationsegment. Activating mutations in melanocytic tumors cluster in exon 11 of the B-RAF gene,which encodes the glycine-rich P loop (codons 461-476) and more frequently in exon 15,which encodes the activation segment (codons 578-622). Codon 599 of B-RAF, which encodesthe amino acid valine at position 599, is an oncogenic hotspot, with more than 90% of B-RAFmutations causing a change in amino acid at this location.
body, and iris. Mucosal melanoma arises frommelanocytes present in the mucosa of the conjunc-tiva, upper aerodigestive tract, female genital tract,and anorectal and urinary tracts. Ultraviolet (UV)exposure is a well-known risk factor for cutaneousmelanoma, whereas uveal structures and mucosalmembranes are generally protected from UV light.Studies demonstrated a high B-RAF mutation fre-quency in cutaneous melanoma but not in uveal18,19
or mucosal melanoma,20-22 thereby suggesting a linkbetween B-RAF mutations and UV exposure. How-ever, clinical studies show that this relationship iscomplex andmolecular studies have yet to shed lighton these observations. A study evaluating cutaneousmelanoma showed a 54% B-RAF mutation rate inmelanomas on nonchronically sun-damaged skin(trunk and extremities), but only an 8% rate onchronically sun-damaged skin (face), 15% on gla-brous skin (palmar, plantar, subungual), and 10% onmucosal sites. This study demonstrates that B-RAFmutations are low in anatomic sites that receive thelowest sun exposure (eg, mucosa) and the highestsun exposure (eg, face), whereas they are commonin sites that receive intermittent UV light (eg, trunkand extremities).22 Moreover, B-RAF mutations do
not have the typical ‘‘UV signature,’’ making thisassociation all the more complex (the most commonB-RAF mutation, V599E, results from a single base-pair substitution of a thymidine to an adenine, T[A.By contrast, the typical UV signature mutations areC[T or CC[TT). Taken together, the link betweenB-RAF and UV radiation remains unclear. Cutaneousmelanomas with distinct clinical and histopathologiccharacteristics, such as desmoplastic melanoma andSpitzoid melanoma, lack B-RAF mutations, whichsuggests distinct genetic pathways in these cutane-ous melanoma subsets.23,24 It is also possible thatmelanomas in different anatomic subgroups (uvealvs cutaneous) and similarly those in different his-topathologic subgroups (desmoplastic vs spitzoid)may have distinct genetic pathways for melanoma-genesis, that cannot be explained by UV exposure.
B-RAF and melanoma histopathologicsubtype. The association between B-RAF mutationstatus and melanoma histopathologic subtype suchas superficial spreading melanoma (SSM), nodularmelanoma (NM), acral lentiginous melanoma (ALM)and lentigo maligna melanoma has been evaluated.Several studies have suggested a positive correlationwith the SSM subtype. In one study, SSM subtypewas

J AM ACAD DERMATOL
VOLUME 53, NUMBER 1
Gill and Celebi 111
Table I. B-RAF mutations in melanoma
Melanoma subtype B-RAF mutation rates (%) References
Primary cutaneous melanoma 26-80* 3, 5, 11, 22, 25, 26, 40-42Metastatic cutaneous melanoma 44-68 15-17Uveal melanoma 0 18, 19Mucosal melanoma 0-10 20-22Desmoplastic melanoma 0 23Spitzoid melanoma (melanoma with Spitz nevus-like features) 0% 24
*The differences in mutation frequencies could be due to differences in sample size, sensitivity of the techniques, and analysis of tumor
specimens versus cell lines.
found to have a significantly higher mutation fre-quency (56%) than lentigo maligna melanoma andNM (13%).25 Similar mutation frequencies in SMM(56.1%) and NM (17%) have been reported byothers.7 Interestingly, one study suggested a linkbetween both the anatomic site and the histopatho-logic subgroup, reporting a 53%mutation rate in SSMon the trunk compared with a 13% rate in ALM on thesoles.22 SSM is the most common melanoma histo-pathologic subtype and is seen predominantly on thetrunk and extremities, whereas ALM is a less com-mon histopathologic subtype; it occurs on the palmsand soles. It is therefore difficult to interpret whetherthe observed differences in mutation frequency aredue to different anatomic sites receiving varyingamounts of UV light or due to different histopatho-logic subtypes with distinct genetic pathways formelanoma development.
B-RAF and melanoma prognostic factors. Inan attempt to evaluate whether the biologic behaviorof melanomas with B-RAF mutations differ fromthose without B-RAF mutations, studies evaluatedprognostic factors for melanoma, such as age, sex,tumor thickness, clinical stage, and clinical outcome.To date, no correlation between B-RAF mutationstatus and Breslow thickness, clinical stage, or clin-ical outcome has been demonstrated.7,17,25,26 Therelation between B-RAF mutation status and patientage is complex and as yet unclear. Two groups haveshown an association between presence of B-RAFmutation and younger age at presentation, withB-RAF mutation rates as high as 70% in patientsyounger than 40 years and as low as 10% in patientsolder than 80 years.17,26 Other groups found no suchassociation.7,22,25 Nevertheless, these studies suggestthat B-RAF mutation status is not a prognostic factorfor melanoma.
B-RAF and melanocytic neviSoon after the identification of B-RAF mutations
in melanoma, surprisingly melanocytic nevi werealso found to harbor a high rate of B-RAF alter-ations (70%-82%), suggesting that B-RAF activation
alone is not sufficient for the development ofmelanoma.
B-RAF and melanocytic nevi histopathologicsubtypes. B-RAF mutations are common in mostmelanocytic nevi; however, the frequency variesdepending on the histopathologic subtype. Com-mon acquired nevi (junctional, compound, intrader-mal) as well as congenital and dysplastic nevi areassociated with mutations in B-RAF, whereas Spitznevi and blue nevi lack or show a low frequencyof alterations in this gene, respectively (summarizedin Table II). A correlation between B-RAF muta-tion status and anatomic location, skin type, nevussize, or number has not been found for commonacquired melanocytic nevi (junctional, compound,intradermal).27
B-RAF and melanocytic nevi as precursors ofmelanoma. The majority of melanomas in the skinarise de novo. However, some occur in associationwith a melanocytic nevus, which suggests thatmelanocytic nevi may be precursors of melanoma.Nevus cells can be found histopathologically in 22%of all melanomas.28 In a recent study, 14 cases ofmelanoma associated with melanocytic nevus wereevaluated for B-RAF mutations. In 3 of these, muta-tions in both the nevus and the melanoma werefound, 10 of 14 were wild type for both, and only onecase showed mutation in the melanoma cells only.These results further suggest, but do not prove, thatmelanocytic nevi were precursors to melanoma insome of these cases.29 However, in the absence ofadditional molecular evidence, the role of nevi asprecursors for melanoma remains controversial.
B-RAF and changing melanocytic nevi. Todate, the role of B-RAF in melanocytic nevus path-ogenesis is unclear. A recent study showed anassociation between B-RAF mutation status andclinically enlarging or changing melanocytic neo-plasms.30 In this study, 49 melanocytic tumors, notsuspected to be melanoma at presentation, under-went biopsy 12 months later, because of increase insize or structural change determined by epilumines-cence microscopy, and analyzed for B-RAF V599E

J AM ACAD DERMATOL
JULY 2005
112 Gill and Celebi
Table II. B-RAF mutations in melanocytic nevi
Melanocytic nevus (histopathologic subtype) B-RAF mutation rates (%) References
Common acquired nevus (Junctional, compound, intradermal) 70-88 27, 29, 40, 43, 44Congenital nevus 46-86 29, 40Dysplastic nevus 18-80 29, 40, 43Blue nevus 0-12 29, 44Spitz nevus 0 29, 42, 44
mutation. B-RAF mutation was observed 13 timesmore frequently in lesions with increasing size and 7times more frequently in lesions showing structuralchanges by epiluminescence microscopy comparedwith unchanged lesions. Some of the changinglesions were determined to be melanoma accordingto biopsy findings, but changing nevi also showedhigher B-RAF mutation rates. These results areintriguing and suggest that B-RAF mutation may beresponsible for the sudden onset of growth inmelanocytic tumors. However, in this study, biopsyat the initial visit was not performed and thereforeB-RAF mutation status at the initial presentation wasunknown. Since histopathologic examination, notclinical features and digital epiluminescence micros-copy, is the ‘‘gold’’ standard for the diagnosis ofmelanoma, it is possible that these ‘‘unsuspect’’lesions were melanoma and had the B-RAFmutationat initial presentation. Future studies would behelpful to confirm these findings.
B-RAF as a therapeutic targetAdvances in the genomic era have led to im-
proved diagnosis, prognosis, and treatment of avariety of cancers. One such example is the discov-ery and successful application of imatinib mesylate(ST1571, Gleevec) in the treatment of chronic mye-logenous leukemia, which has opened new avenuesin molecular-based treatment of cancer. Imatinib, amolecular-targeted therapy, is currently the first-linetreatment for chronic myelogenous leukemia.31
Although the development of clinical resistancewhen imatinib is used as monotherapy has recentlyemerged as a therapeutic challenge32 and othermolecules and treatment strategies are being devel-oped, imatinib and its target tyrosine kinase Abl,represent the paradigm for molecular-based treat-ment of cancer.
To date, no treatment has been identified thatconfers a significantly improved survival rate inpatients with advanced-stage melanoma. Identifica-tion of a high rate of B-RAF mutations in melanomaalongwithmolecular studies demonstratingB-RAF asa potential therapeutic target inmelanoma has drawnsignificant attention to this molecule and its signalingpathway.33,34 Recently small-molecule RAF inhibitors
have been developed, one of which, BAY 43-9006, isorally administered and is currently being evaluatedin clinical trials. Phase I clinical and pharmacokineticstudies show that BAY 43-9006 is generally welltolerated among patients, with the majority of tox-icities limited to the gastrointestinal system and theskin.35 Efficacy data for hepatocellular carcinoma,renal cell carcinoma, and non-small-cell lung cancershow stabilization of progressive disease rather thantumor regression.35 Preliminary studies, however,show a very modest activity of BAY 43-9006 as asingle agent in melanoma.6,36 Although phase I/IIclinical trials demonstrate a favorable safety profilefor BAY 43-9006 when combined with paclitaxel andcarboplatin,37 data on its efficacy in the treatment ofmelanoma are under investigation. BAY 43-9006 isnot a specific inhibitor of RAF and has activity againstother kinases.38 While potent and specific RAFinhibitors are being developed to increase efficacy,clinical studies with BAY 43-9006 are ongoing. Inaddition to RAF inhibitors, therapeutic agents target-ing other molecules in the RAS-RAF-MEK-ERK sig-naling pathway are currently being developed andtested.39
ConclusionsSince the identification of high-rate B-RAF muta-
tions in melanoma in 2002, several groups haveattempted to delineate the implications of B-RAFin melanocytic tumorigenesis. At present, only lim-ited conclusions can be drawn from the data. Thepresence of high-frequency B-RAF mutations incommon acquired nevi in addition to similar ratesof B-RAF mutation in melanoma suggests thatB-RAF activation plays a role in both benign mela-nocytic proliferations and melanoma; however, it isnot sufficient alone for development of melanoma.In addition, the absence of germline B-RAF muta-tions in patients with familial and sporadic mela-noma suggests that B-RAFmutation does not play animportant role in susceptibility to development ofmelanoma. We can also infer that more than onegenetic pathway exists for melanocytic neoplasia,both benign and malignant, as certain subtypesof nevi (ie, Spitz and blue nevi) and melanoma(ie, uveal and mucosal melanoma) harbor no or

J AM ACAD DERMATOL
VOLUME 53, NUMBER 1
Gill and Celebi 113
rare B-RAFmutations. These genetic differences mayresult in varying responses to therapeutic agents. Asmore molecular-targeted therapies are being devel-oped, identification of molecular signatures andclassification of melanoma subtypes based on theirgenetic profiles will be crucial in determining thetherapeutic regimen.
REFERENCES
1. Jemal A, Tiwari RC, Murray T, Ghafoor A, Samuels A, Ward E,
et al. Cancer statistics, 2004. CA Cancer J Clin 2004;54:8-29.
2. Rigel DS, Carucci JA. Malignant melanoma: prevention, early
detection, and treatment in the 21st century. CA Cancer J Clin
2000;50:215-36; quiz 237-40.
3. Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S,
et al. Mutations of the BRAF gene in human cancer. Nature
2002;417:949-54.
4. Wan PT, Garnett MJ, Roe SM, Lee S, Niculescu-Duvaz D, Good
VM, et al. Mechanism of activation of the RAF-ERK signaling
pathway by oncogenic mutations of B-RAF. Cell 2004;116:
855-67.
5. Brose MS, Volpe P, Feldman M, Kumar M, Rishi I, Gerrero R,
et al. BRAF and RAS mutations in human lung cancer and
melanoma. Cancer Res 2002;62:6997-7000.
6. Gray-Schopfer VC, da Rocha Dias S, Marais R. The role of B-RAF
in melanoma. Cancer Metastasis Rev 2005;24:165-83.
7. Omholt K, Platz A, Kanter L, Ringborg U, Hansson J. NRAS and
BRAF mutations arise early during melanoma pathogenesis
and are preserved throughout tumor progression. Clin Cancer
Res 2003;9:6483-8.
8. Hayward NK. Genetics of melanoma predisposition. Oncogene
2003;22:3053-62.
9. Laud K, Kannengiesser C, Avril MF, Chompret A, Stoppa-
Lyonnet D, Desjardins L, et al. BRAF as a melanoma suscep-
tibility candidate gene? Cancer Res 2003;63:3061-5.
10. Lang J, Boxer M, MacKie R. Absence of exon 15 BRAF germ-
line mutations in familial melanoma. Hum Mutat 2003;21:
327-30.
11. Casula M, Colombino M, Satta MP, Cossu A, Ascierto PA,
Bianchi-Scarra G, et al. BRAF gene is somatically mutated but
does not make a major contribution to malignant melanoma
susceptibility: the Italian Melanoma Intergroup Study. J Clin
Oncol 2004;22:286-92.
12. Wellbrock C, Karasarides M, Marais R. The RAF proteins take
centre stage. Nat Rev Mol Cell Biol 2004;5:875-85.
13. Garnett MJ, Marais R. Guilty as charged: B-RAF is a human
oncogene. Cancer Cell 2004;6:313-9.
14. Dong J, Phelps RG, Qiao R, Yao S, Benard O, Ronai Z, et al. BRAF
oncogenic mutations correlate with progression rather than
initiation of human melanoma. Cancer Res 2003;63:3883-5.
15. Gorden A, Osman I, Gai W, He D, Huang W, Davidson A, et al.
Analysis of BRAF and N-RAS mutations in metastatic mela-
noma tissues. Cancer Res 2003;63:3955-7.
16. Kumar R, Angelini S, Czene K, Sauroja I, Hahka-Kemppinen M,
Pyrhonen S, et al. BRAF mutations in metastatic melanoma:
a possible association with clinical outcome. Clin Cancer Res
2003;9:3362-8.
17. Shinozaki M, Fujimoto A, Morton DL, Hoon DS. Incidence of
BRAF oncogene mutation and clinical relevance for primary
cutaneous melanomas. Clin Cancer Res 2004;10:1753-7.
18. Cruz F 3rd, Rubin BP, Wilson D, Town A, Schroeder A, Haley A,
et al. Absence of BRAF and NRAS mutations in uveal mela-
noma. Cancer Res 2003;63:5761-6.
19. Rimoldi D, Salvi S, Lienard D, Lejeune FJ, Speiser D, Zografos L,
et al. Lack of BRAF mutations in uveal melanoma. Cancer Res
2003;63:5712-5.
20. Cohen Y, Rosenbaum E, Begum S, Goldenberg D, Esche C,
Lavie O, et al. Exon 15 BRAF mutations are uncommon in
melanomas arising in nonsun-exposed sites. Clin Cancer Res
2004;10:3444-7.
21. Edwards RH, Ward MR, Wu H, Medina CA, Brose MS, Volpe P,
et al. Absence of BRAF mutations in UV-protected mucosal
melanomas. J Med Genet 2004;41:270-2.
22. Maldonado JL, Fridlyand J, Patel H, Jain AN, Busam K,
Kageshita T, et al. Determinants of BRAF mutations in primary
melanomas. J Natl Cancer Inst 2003;95:1878-90.
23. Davison JM, Rosenbaum E, Barrett TL, Goldenberg D, Hoque
MO, Sidransky D, et al. Absence of V599E BRAF mutations in
desmoplastic melanomas. Cancer 2005;103:788-92.
24. Gill M, Cohen J, Renwick N, Mones JM, Silvers DN, Celebi JT.
Genetic similarities between Spitz nevus and Spitzoid mela-
noma in children. Cancer 2004;101:2636-40.
25. Thomas NE, Alexander A, Edmiston SN, Parrish E, Millikan RC,
Berwick M, et al. Tandem BRAF mutations in primary invasive
melanomas. J Invest Dermatol 2004;122:1245-50.
26. Kumar R, Angelini S, Hemminki K. Activating BRAF and N-Ras
mutations in sporadic primary melanomas: an inverse associ-
ation with allelic loss on chromosome 9. Oncogene 2003;22:
9217-24.
27. Kumar R, Angelini S, Snellman E, Hemminki K. BRAF mutations
are common somatic events in melanocytic nevi. J Invest
Dermatol 2004;122:342-8.
28. Stolz W, Schmoeckel C, Landthaler M, Braun-Falco O. Associ-
ation of early malignant melanoma with nevocytic nevi.
Cancer 1989;63:550-5.
29. Yazdi AS, Palmedo G, Flaig MJ, Puchta U, Reckwerth A, Rutten
A, et al. Mutations of the BRAF gene in benign and malignant
melanocytic lesions. J Invest Dermatol 2003;121:1160-2.
30. Loewe R, Kittler H, Fischer G, Fae I, Wolff K, Petzelbauer P.
BRAF kinase gene V599E mutation in growing melanocytic
lesions. J Invest Dermatol 2004;123:733-6.
31. Wong S, Witte ON. The BCR-ABL story: bench to bedside and
back. Annu Rev Immunol 2004;22:247-306.
32. Gorre ME, Mohammed M, Ellwood K, Hsu N, Paquette R, Rao
PN, et al. Clinical resistance to STI-571 cancer therapy caused
by BCR-ABL gene mutation or amplification. Science 2001;293:
876-80.
33. Karasarides M, Chiloeches A, Hayward R, Niculescu-Duvaz D,
Scanlon I, Friedlos F, et al. B-RAF is a therapeutic target in
melanoma. Oncogene 2004;23:6292-8.
34. Tuveson DA, Weber BL, Herlyn M. BRAF as a potential
therapeutic target in melanoma and other malignancies.
Cancer Cell 2003;4:95-8.
35. Strumberg D, Richly H, Hilger RA, Schleucher N, Korfee S,
Tewes M, et al. Phase I clinical and pharmacokinetic study of
the novel Raf kinase and vascular endothelial growth factor
receptor inhibitor BAY 43-9006 in patients with advanced
refractory solid tumors. J Clin Oncol 2005;23:965-72.
36. Ahmad T, Marais R, Pyle M, James B, Shwartz M, Gore M, et al.
BAY 43-9006 in patients with advanced melanoma: the Royal
Marsden experience. J Clin Oncol 2004;22:7506.
37. Flaherty KT, Brose M, Schuchter L, Tuveson DA, Lee R,
Schwartz B, et al. Phase I/II trial of BAY 43-9006, carboplatin
and paclitaxel demonstrates preliminary antitumor activity in
the expansion cohort of patients with metastatic melanoma.
J Clin Oncol 2004;22:7507.
38. Wilhelm SM, Carter C, Tang L, Wilkie D, McNabola A, Rong H,
et al. BAY 43-9006 exhibits broad spectrum oral antitumor

J AM ACAD DERMATOL
JULY 2005
114 Gill and Celebi
activity and targets the RAF/MEK/ERK pathway and receptor
tyrosine kinases involved in tumor progression and angiogen-
esis. Cancer Res 2004;64:7099-109.
39. Sebolt-Leopold JS, Herrera R. Targeting the mitogen-activated
protein kinase cascade to treat cancer. Nat Rev Cancer 2004;4:
937-47.
40. Pollock PM, Harper UL, Hansen KS, Yudt LM, Stark M, Robbins
CM, et al. High frequency of BRAF mutations in nevi. Nat
Genet 2003;33:19-20.
41. Sasaki Y, Niu C, Makino R, Kudo C, Sun C, Watanabe H,
et al. BRAF point mutations in primary melanoma show
different prevalences by subtype. J Invest Dermatol 2004;
123:177-83.
42. Gill M, Renwick N, Silvers DN, Celebi JT. Lack of BRAF
mutations in Spitz nevi. J Invest Dermatol 2004;122:1325-6.
43. Uribe P, Wistuba, II, Gonzalez S. BRAF mutation: a frequent
event in benign, atypical, and malignant melanocytic lesions
of the skin. Am J Dermatopathol 2003;25:365-70.
44. Saldanha G, Purnell D, Fletcher A, Potter L, Gillies A,
Pringle JH. High BRAF mutation frequency does not char-
acterize all melanocytic tumor types. Int J Cancer 2004;111:
705-10.