Embed Size (px)
Citation preview

CRS-I-Treatment
Alan
Maisel
MD
Professor of
Medicine,
University of
California,
San Diego
Director
Coronary Care
Unit And Heart
Failure Program
San Diego
Veterans
Hospital


Outcomes in Patients Hospitalized
With HF
N = 38,702Aghababian RV. Rev Cardiovasc Med. 2002;3(suppl 4):S3
Jong P et al. Arch Intern Med. 2002;162:1689
0
25
50
75
100
20%
50%
30Days
6Months
Hospital Readmissions
0
25
50
75
100
12%
50%
30Days
12Months
Mortality
33%
5Years
Median LOS: 6 days
• Until recently we
didn’t really have
any effective, non-
toxic treatments for
CHF


Treatment of Acute HF
Diuretics
Fluid
volume
Vasodilators
Preload
and/or
afterload
Inotropes
Contrac
-
tility
Natriuretic
Peptides
Fluid volume
Preload
Afterload
Neuro-
hormes
Increase
lusitropy

Profiles and Therapies of Advanced Heart Failure
Yes
R. Bourge, UAB Cardiology (adapted from L. Stevenson)
Stevenson LW. Eur J Heart Failure 1999;1:251-257
No
Warm and Dry
PCW and CI
normal
Warm and Wet
PCW elevated
CI normal
Cold and Wet
PCW elevated
CI decreased
Cold and Dry
PCW low/normal
CI decreased
Vasodilators
Nitroprusside
Nitroglycerine
Nesiritide
Inotropic Drugs
Dobutamine
Milrinone
Calcium Sensitizers
Nl SVR High SVR
Congestion at Rest
Low
Perfusion
at Rest
No
Yes

Complications of Diuretic Therapy
for Heart Failure
Na = sodium; Mg = magnesium; GFR = glomerular filtration rate; PRA = plasma renin activity.Kaplan NM., Treatment of Hypertension: Drug Therapy in Clinical Hypertension (p. 203) in Clinical Hypertension, 6th. Ed. Baltimore: William and Wilkins 1994.
Distal Ca++Reabsorption
Plasma Volume
Uric AcidClearance
HypomagnesemiaDiuretic Therapy
Cardiac Output
Renal Reabsorption of Na (and Mg)
Renal Blood Flow
Hyponatremia
PRA
GFR
ProximalReabsorption
Aldosterone
Kaliuresis
Hypokalemia
Glucose IntoleranceHypocalcemiaHyperuricemia
CalciumClearance
Pre-renalAzotemia
Neurohumoral Activation

The Natriuretic Peptide System is Overwhelmed in Acute Decompensated Heart Failure
Adapted from Burnett JC, J Hypertens 1999;17(Suppl 1):S37-S43
Angiotensin II
Epinephrine
Endothelin
ANP BNP
Aldosterone

Human B-type Natriuretic
Peptide (hBNP)
Nesiritide is identical
to endogenous hBNP
Mechanism of Action:
via receptor binding
to GC-A receptor and
cGMP production (no
impact on cAMP)

rhBNPD
R I
M
K
R
G
SS
S
S
G
L
GF
CC
S S
GSGQVM
K V LR
RH
KPS
Effects of NesiritideVenous, arterial, coronary
VASODILATION
CARDIAC
INDEX
Preload
Afterload
PCWP
Dyspnea
HEMODYNAMIC
CARDIAC
No increase in HR
Not proarrhythmic
Aldosterone
Endothelin
Norepinephrine
SYMPATHETIC AND
NEUROHORMONAL SYSTEMS
NATRIURESIS
DIURESIS
Fluid volume
Preload
Diuretic
usage
RENAL
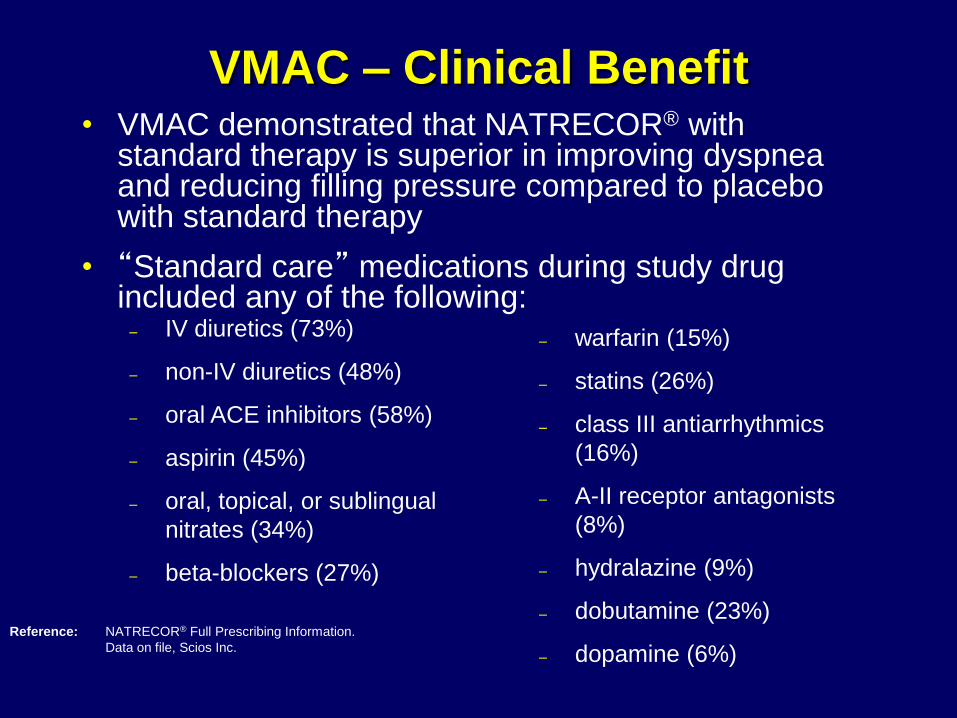
VMAC – Clinical Benefit• VMAC demonstrated that NATRECOR® with
standard therapy is superior in improving dyspnea and reducing filling pressure compared to placebo with standard therapy
• “Standard care” medications during study drug included any of the following:– IV diuretics (73%)
– non-IV diuretics (48%)
– oral ACE inhibitors (58%)
– aspirin (45%)
– oral, topical, or sublingual
nitrates (34%)
– beta-blockers (27%)
– warfarin (15%)
– statins (26%)
– class III antiarrhythmics
(16%)
– A-II receptor antagonists
(8%)
– hydralazine (9%)
– dobutamine (23%)
– dopamine (6%)Reference: NATRECOR® Full Prescribing Information.
Data on file, Scios Inc.

Hemodynamic Effects of Nesiritide
vs Placebo vs IV NTG
*†
*
†
*
†
††
†
†
*
During 3-hr placebo period
Placebo n = 62
IV NTG n = 60
Nesiritide n = 124
After 3-hr period
IV NTG n = 92
Nesiritide n = 154
Publication Committee for the VMAC Investigators. JAMA. 2002;287:1531
*P0.05 vs placebo†P0.05 vs IV NTG
PCWP – Placebo
PCWP – IV NTG
PCWP – Nesiritide
End of Placebo-Controlled Period
Time on Study Drug (hr)
0 0.25 0.5 1 2 3 6 9 12 24 36 48
–9
–8
–7
–6
–5
–4
–3
–2
–1
0
†
*
*
Ch
an
ge F
rom
Baselin
e i
n
PC
WP
(m
m H
g)

Nitroglycerin Dose and Change in
PCWP During Treatment With
Nitroglycerin
n = 9 (3 hr); n = 12 (>3 hr)
Added to standard therapy
Elkayam U et al. Am J Cardiol. 2004;93:237
0
20
40
60
80
100
120
140
160
180
0 3 6 9 12 15 18 21 24
Time (hr)
Nit
rog
lyceri
n D
ose (
mcg
/min
)
8
7
6
5
4
3
2
1
0
Ch
an
ge in
PC
WP
(mm
Hg
)
NTG dose
Change in PCWP
*
*
*
*
*
*
* P<0.05 vs baseline

Nesiritide Versus Other Vasodilators
Parameters Nitroglycerin NitroprussideNesiritide
Tachyphylaxis Yes No No
Toxic Metabolites No Yes No
Hypotension Yes Yes Yes
Special handling Glass Light No
Headache Yes Yes Yes
Action on RAAS ? Renin Aldosterone
Difficult titration No Yes No

Limitations of Current Therapies for Acute HF: Positive Inotropes
• Increased mortality1-3
– Milrinone
– Enoximone
– Imazodan
– Vesnarinone
– Dobutamine
– Xamoterol
– Ibopamine
• Increased risk of hospitalization
• Aggravation and induction of
arrhythmias (need telemetry)4
– Milrinone
– Dobutamine
– Dopamine
• Tachycardia
• Tachyphylaxis (dobutamine)
• Neurohormonal activation and/or
lack of suppression
• Physiologic effects antagonized
by -blockade (dobutamine,
dopamine)1Packer M et al. N Engl J Med. 1991;325:14682Cohn JN et al. N Engl J Med. 1998;339:18103The Xamoterol in Severe Heart Failure Study Group. Lancet. 1990;336:1 4Ewy GA. J Am Coll Cardiol. 1999;33:572

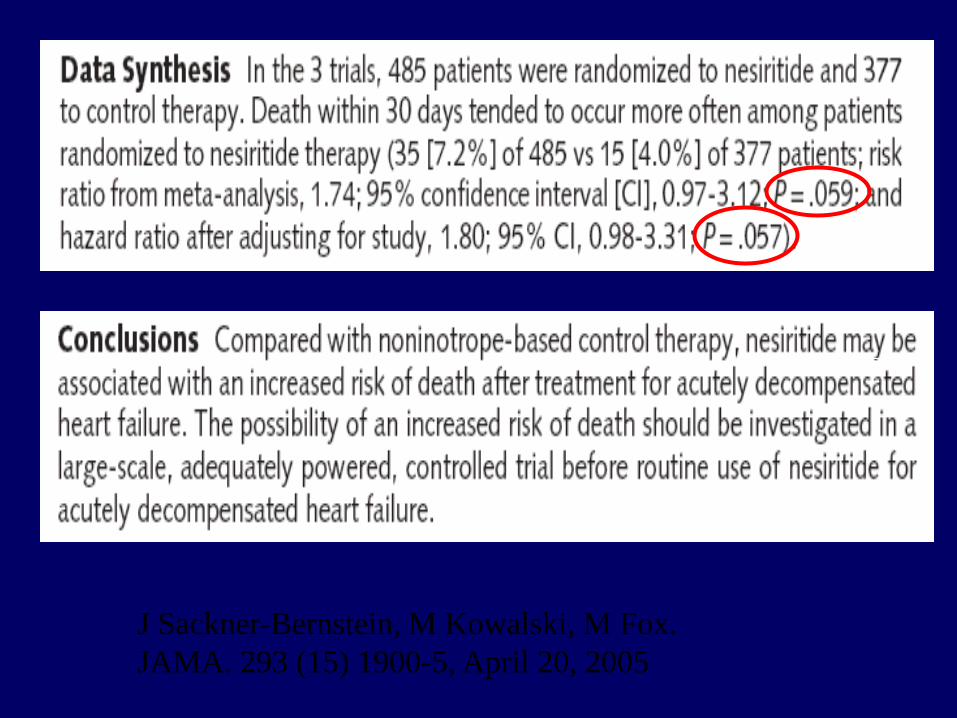
J Sackner-Bernstein,
M Kowalski, M Fox.
JAMA. 293 (15)
1900-5,
April 20, 2005

Acute Decompensated Heart Failure:
Nesiritide and Mortality
• No short-term therapy for ADHF has been proven to improve short- or long-term mortality rates.
• Nesiritide is the only approved ADHF therapy which has been shown in large, randomized trials to provide both significant symptomatic and hemodynamic improvement when added to standard care.
• Nesiritide has not been studied in a trial powered to evaluate an effect on mortality.
– 30-day mortality data available for 7 trials
– 6-month mortality data available for 4 trials
J Sackner-Bernstein, M Kowalski, M Fox.
JAMA. 293 (15) 1900-5, April 20, 2005

30-Day Mortality Hazard Ratios
VMAC
PROACTION
FUSION I
PRECEDENT
Efficacy
Comparative
Mills et al.
Note: Arrows depict studies included in JAMA publication

• A prospective, multi-center, randomized, double-blind, pilot study
– Included 279 randomized and treated heart failure patients undergoing
cardiac surgery with or without mitral valve repair/replacement
• NAPA was a Phase II, exploratory study
– No pre-specified primary endpoints; however there were pre-specified
areas of interest
– Not the labeled dose (no bolus)
– Limitations with this analysis
• 180-day mortality endpoint was added late in the study; as a result subjects
were lost to follow-up (3%), declined consent (9%) or did not respond to request
for information (13%), other* (6%) at 180 days.
• This study is too small to draw definitive mortality conclusions
– This study is not designed to demonstrate safety and effectiveness for this
use
• More robust trials are planned
NAPA TrialNesiritide Administered Peri-Anesthesia in Patients Undergoing
Cardiac Surgery
* Documented alive at days 174 to 179.

Nesiritide
(n=141)
% (n)
Placebo
(n=138)
% (n)
Hazard
Ratio
(95% CI)
P value
Kaplan-Meier rate
within 30 days
2.8%
(4/141)
5.9%
(8/138)
0.48
(0.14, 1.59)0.219
Kaplan-Meier rate
within 180 days
6.7%
(8/141)
14.7%
(17/138)
0.44
(0.19, 1.01)0.046
• 30-day mortality data were available for 132 patients
in the nesiritide group and 127 in the placebo
group.
• 180-day mortality data were available for 94 patients
treated with nesiritide and 95 patients treated with
placebo.
Reference: Luber JM, Jr., on behalf of the NAPA Investigators. J Card Fail. 2006; 12(6, suppl 1):S73-S74. Abstract 235. Scios will
submit a final report to FDA once its own internal validation of the data is complete.
NAPA Trial
30-Day and 180-Day Mortality

Reference: Luber JM, Jr., on behalf of the NAPA Investigators. J Card Fail. 2006; 12(6, suppl 1):S73-S74. Abstract 235. Scios will
submit a final report to FDA once its own internal validation of the data is complete.
In seven NATRECOR® clinical trials, through 30 days, 5.3% in the NATRECOR® treatment group died as compared with 4.3% in the
group treated with other standard medications. In four clinical trials, through 180 days, 21.7% in the NATRECOR® treatment group died as
compared with 21.5% in the group treated with other medications. There is not enough information to know about the effect of
NATRECOR® on mortality.
NAPA Trial
Kaplan-Meier Survival Curve by Treatment Goup
J Sackner-Bernstein,
HA Skopick,
KD Aronson.
Circ. 111 1487-91,
2005

Methods/Results
• 5 studies, N = 1,269
• Dose ranging from 0.01 to 0.06 g/kg/min
• “Even low-dose nesiritide (0.015 g/kg/min) significantly increased risk (p=0.012 and p=0.006 compared with non-inotrope and inotrope based controls, respectively)”
J Sackner-Bernstein, HA Skopick,
KD Aronson. Circ. 111 1487-91, 2005

SCr Increases with Nesiritide: Renal
Outcomes
• Prescribing Information, Precautions: Renal Effects
– “When NATRECOR® was initiated at doses higher than 0.01
mcg/kg/min (0.015 and 0.03 mcg/kg/min), there was an increased
rate of elevated SCr compared with standard therapies, although
the rate of acute renal failure and the need for dialysis was not
increased.”
– “In the 30-day follow-up period in VMAC, 5 patients in the NTG
group (2%) and 9 patients in the NATRECOR® group (3%) required
first-time dialysis.” (p=0.418)
Reference: NATRECOR® Full Prescribing Information.

NAPA TrialMean Change in Serum Creatinine (SCr) and Calculated Glomerular
Filtration Rate (cGFR) by Treatment Group and Baseline Renal Function
PARAMETERS OF INTEREST NESIRITIDE PLACEBO P
Peak SCr Increase (mg/dL)*
All Patients (n=266) 0.15 0.34 <0.001
Patients with baseline SCr >1.2 (n=62) 0.02 0.48 0.001
Maximum Decrease in cGFR (ml/min)*
All Patients (n=266) -10.8 -17.2 0.001
Patients with baseline SCr >1.2 (n=62) -0.2 -9.1 0.003
Postoperative SCr Increase >0.5 mg/dL*
All Patients (n=271) 7% 23% <0.001
Postoperative Urine Output (first 24 hrs.) (ml)
All Patients (n=271) 2926 2350 <0.001* Through discharge or hospital day 14, whichever came first
Reference: Hebeler RF Jr. on behalf of the NAPA investigators. Circulation May 30, 2006. Abstract 292
NATRECOR® may affect renal function in susceptible individuals. In patients with severe heart failure whose renal function may depend on the activity of the renin-angiotensin-aldosterone system, treatment with NATRECOR® may be associated with azotemia. In the VMAC trial, through day 30, the incidence of elevations in creatinine to >0.5 mg/dL above baseline was 28% and 21% in the NATRECOR® and nitroglycerin groups, respectively. When NATRECOR® was initiated at doses higher than 0.01 mcg/kg/min, there was an increased rate of elevated serum creatinine over baseline compared with standard therapies, although the rate of acute renal failure and need for dialysis were not increased.

NAPA Trial
Mean Change from Baseline in Post-Op SCr
NATRECOR® may affect renal function in susceptible individuals. In patients with severe heart failure whose renal function may depend on the activity of the renin-angiotensin-aldosterone system, treatment with NATRECOR® may be associated with azotemia. In the VMAC trial, through day 30, the incidence of elevations in creatinine to >0.5 mg/dL above baseline was 28% and 21% in the NATRECOR® and nitroglycerin groups, respectively. When NATRECOR® was initiated at doses higher than 0.01 mcg/kg/min, there was an increased rate of elevated serum creatinine over baseline compared with standard therapies, although the rate of acute renal failure and need for dialysis were not increased.
Reference: Luber JM, Jr., on behalf of the NAPA Investigators. J Card Fail. 2006; 12(6, suppl 1):S73-S74. Abstract 235. Scios will
submit a final report to FDA once its own internal validation of the data is complete.

Ideal Agent for Acute HF
• Vasodilator (venous and arterial)
• Rapidly decreases ventricular filling pressures
• Rapidly decreases symptoms of congestion
• Does not increase heart rate or directly increase contractility (decreases myocardial oxygen demand)
• Not proarrhythmic
• No tolerance
• Provides neurohormonal suppression
• Promotes diuresis/natriuresis
• Conveniently dosed (with or without PA catheterization)
• Minimal titration needed
Fonarow GC. Rev Cardiovasc Med. 2001;2(suppl 2):S7

Braunwald Panel
Recommendations
• Nesiritide is approved for inpatient management of acute HF
• Use of nesiritide should be limited to patients presenting to the hospital with acute HF who have dyspnea at rest
• Physicians considering the use of nesiritide should consider
– Its efficacy in reducing dyspnea
– Possible risks of the drug
– Availability of alternate therapies to relieve HF symptoms
Scios Inc. press release. June 13, 2005. Available at: http://www.sciosinc.com/scios/pr_1118721302.
Accessed July 13, 2005

ADHERE CART: Predictors of Mortality
SYS BP 115n = 24,933
SYS BP 115n = 7150
6.41%
n = 5102
15.28%
n = 2048
21.94%
n = 62012.42%
n = 1425
5.49%
n = 4099
2.14%
n = 20,834
BUN 43N = 33,046
Greater thanLess than
2.68%
n = 25,122
8.98%
n = 7202
Cr 2.752045
Highest to Lowest Risk Cohort
OR 12.9 (95% CI 10.4-15.9)
Fonarow GC et al. JAMA 2005. 293:572

In-Hospital Mortality Risk by Initial
BNP Levels Reduced vs. Preserved
Systolic Function HF
48,629 (63%) out of 77,467 pt episodes had BNP assessment at initial evaluation
19,544 patients with LVEF < 0.40 and 18,164 patients with LVEF > 0.40
Q2 2003 to Q4 2004
1.4
2.8
3.8
6.4
0
1
2
3
4
5
6
7
InH
os
pit
al M
ort
ality
Q1 (<622) Q2 (622-1210) Q3 (1210-2310)
Q4 (>2310)
P<0.0001
1.5
2.7 2.8
5
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
InH
os
pit
al M
ort
ali
ty
Q1 (<336) Q2 (336-630) Q3 (630-1230) Q4 (>1230)
P<0.0001
LVEF < 0.40 LVEF > 0.40

Patient Outcomes by Quartiles of
BNP Levels in the ADHERE
Registry
48,629 (63%) out of 77,467 pt episodes had BNP assessment at initial evaluation.
Q2 2003 to Q4 2004
Q1
(<430)
Q2
(430-839)
Q3
(840-
1730)
Q4
(>1730)
P Value
Ventilation 3.1 3.7 3.9 4.1 P=0.0002
CPR 0.6 0.9 1.2 1.7 P<0.0001
Ultrafiltrat 0.6 0.8 1.6 5.0 P<0.0001
LOS (days) 5.2 5.7 5.9 6.3 P<0.0001
ICU admit
%
12.8 15.4 16.6 19.6 P<0.0001
ASx at DC 48.8 49.6 48.0 43.6 P<0.0001

High risk patient:• No change or increase in BNP level• Inadequate diuresis (<500cc)• Worsening renal function
SBP ≥ 90Nesiritide 1-2 days
IV Diuretics
SBP < 90InotropesPressors
+/- Swan Ganz Catheter
BNP level 6h after Nesiritide cessationthen re-check BNP
Improvement in symptoms/ BNP
Oral vasodilators and diuretics until euvolemic.D/C BNP level
Yes No
Consider• Angiography• IABP• Transplant• LVAD
Nesiritide 1-2 days, then po Vasodilators,diuretics
Low Risk Patient:• BNP level decreased• Adequate diuresis (500-1000cc)• No deterioration in renal function
Continue diuretics/vasodilators until euvolemic
BNP < 400Discharge
BNP ≥ 400Re-evaluate
Volume status
Discharge withearly follow-up
Nesiritide plus
diuretics
Euvolemic
Yes No
ALGORITHM FOR USE IN BNP TESTING IN PATIENTS WITH CHF
Yes
IV diuretic for 6 to 12 hoursNo
Initial BNP > 600&
Initial BUN > 40
Draw BNP, BUN

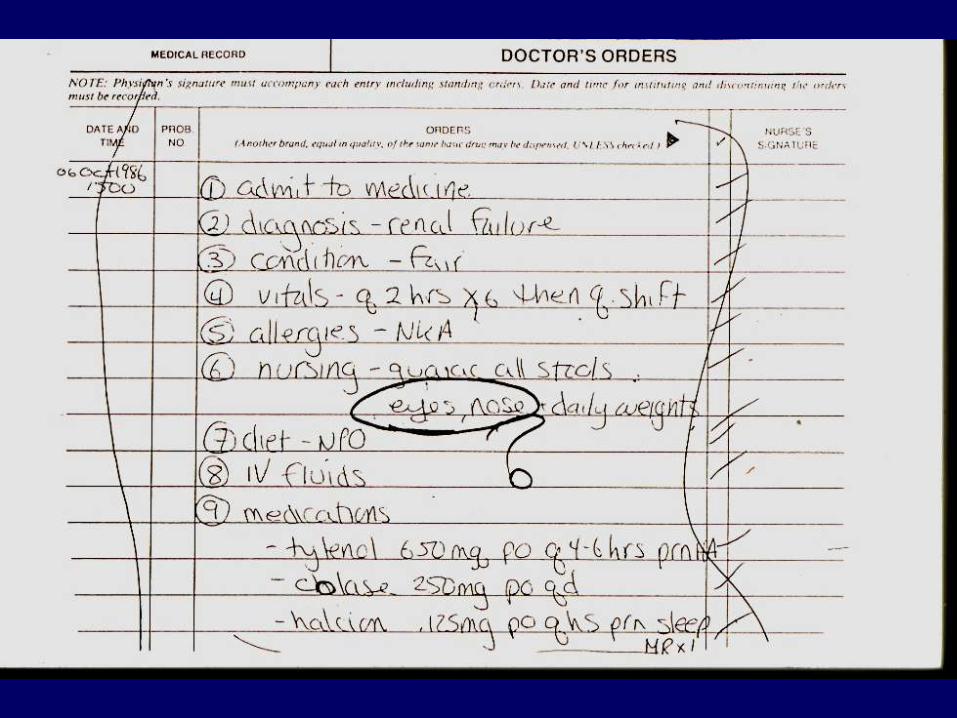
Write orders carefully


Continuous Aortic Flow
AugmentationOrqis® Cancion®
Ax – Fem graft
Cath : Fem:Fem
single Fem
• a – inflow (fem artery)
• b – pump
• c – pump motor
• d – controller
• e – flow sensor
• f – outflow (desc
a
b
c
d
e
f

Mechanism of Action
Continuous Aortic Flow Augmentation
Ventricular
UnloadingVasodilation Renal Effects
DiuresisHemodynamic improvement
Clinical Benefit
Nitric Oxide
Other mediators
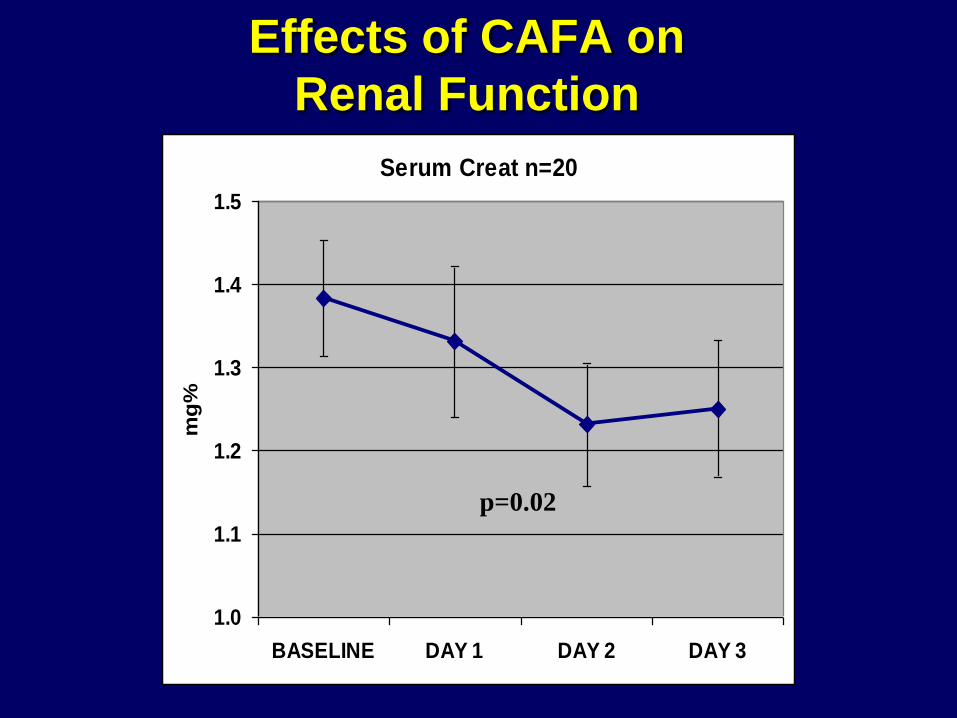
Effects of CAFA on
Renal Function
Serum Creat n=20
1.0
1.1
1.2
1.3
1.4
1.5
BASELINE DAY 1 DAY 2 DAY 3
mg
%
p=0.02

Mechanical Therapy
Smaller devices
Less infection?
Opportunity
for explant

REMATCH Trial: All Cause Mortality
LV Assist
Device (n=68)
Control
(n=61)
P=0.001
6 12 18 240
100
80
60
40
20
0
30
Months
% E
ve
nt
Fre
e S
urv
iva
l
RR 0.52 (0.34,0.78)N Engl J Med 2001; 345: 1435

Limitations of Current LVAD Therapy
• Very expensive.
• Major commitment on the part of
physicians, nurses and hospitals for
continuing care.
• Small increase in survival rates after 2
years.
• Substantial risk of bleeding, infection and
device malfunction requiring in-hospital
care.

Limitations of Current LVAD Therapy
• Very expensive.
• Major commitment on the part of
physicians, nurses and hospitals for
continuing care.
• Small increase in survival rates after 2
years.
• Substantial risk of bleeding, infection and
device malfunction requiring in-hospital
care.

Donor Myocytes
Dilated CMP
Post LVAD
Mechanical Unloading Reverses The
Heart Failure Phenotype

Cell Transplantation For Treating
HF
• neonatal/adult CM
• embryonic stem cell
• bone marrow stem cell
• skeletal myoblast
• others
GM fibroblast
cardiac stem cells
Possible Graft
End
stage
heart
failureNew Myocytes
Functional recovery
of diseased hearts
Undefined mechanisms
animals, human
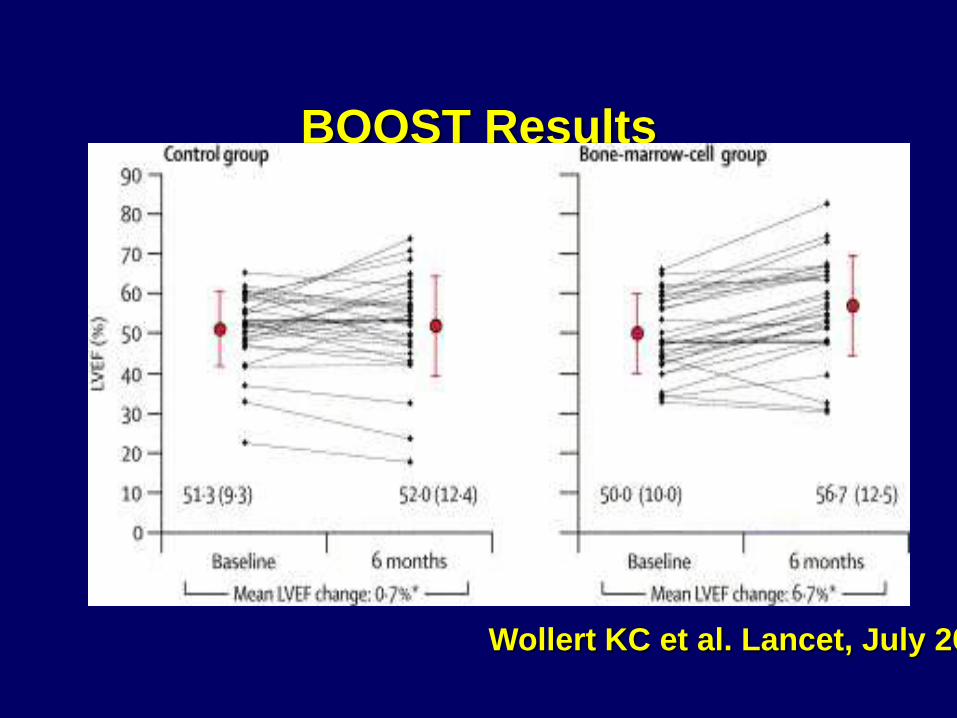
BOOST Results
Wollert KC et al. Lancet, July 2004

Titrating therapy by Natriuretic
peptide levels
• NP levels above baseline
usually mean volume
overload
• NP levels can help one
achieve euvolemia and
monitor treatment
• NP levels can help
determine appropriate
discharge from the hospital

Changes in BNP and PAW* Levels
During 24 Hours of Treatment
Msaisel, A. et al. J Cardiac Failure, Vol. 7, No. 1, 2001
N = 15 (responders)
PA
W (
mm
Hg
)
Hours
BN
P (p
g/m
l)
15
17
19
21
23
25
27
29
31
33
baseline 4 8 12 16 20 24600
700
800
900
1000
1100
1200
1300
PAWBNP
*Pulmonary artery wedge.

250500
800
1750
500
1000
1500
2000
2500
I II III IV
Dry ( NYHA Euvolemic state)
In volume overloaded patients: BNP level = baseline BNP(dry)
plus change due to increased volume(wet)B
NP
lev
el (
pg/m
l)
NYHA Class - Euvolemic (Dry) BNP
Wet (Change due to volume overload)

28
17
14
6
3
kDaRec. A B C D E blank Rec.
Clinical BNP Results pg/ mL: A B C D E
Maisel 3920 3720 4010 2090 127
in-house Triage 1140 1440 1260 1570 584
Major form of BNP in patients with CHF is proBNP
proBNP
BNP
5 CHF patients:
Liang, Maisel et al., JACC 2007

Serial BNP for Guiding Treatment
During Hospitalization?
Courtesy of Damien Logeart.

BNP:
It’s About Improving Patient Care
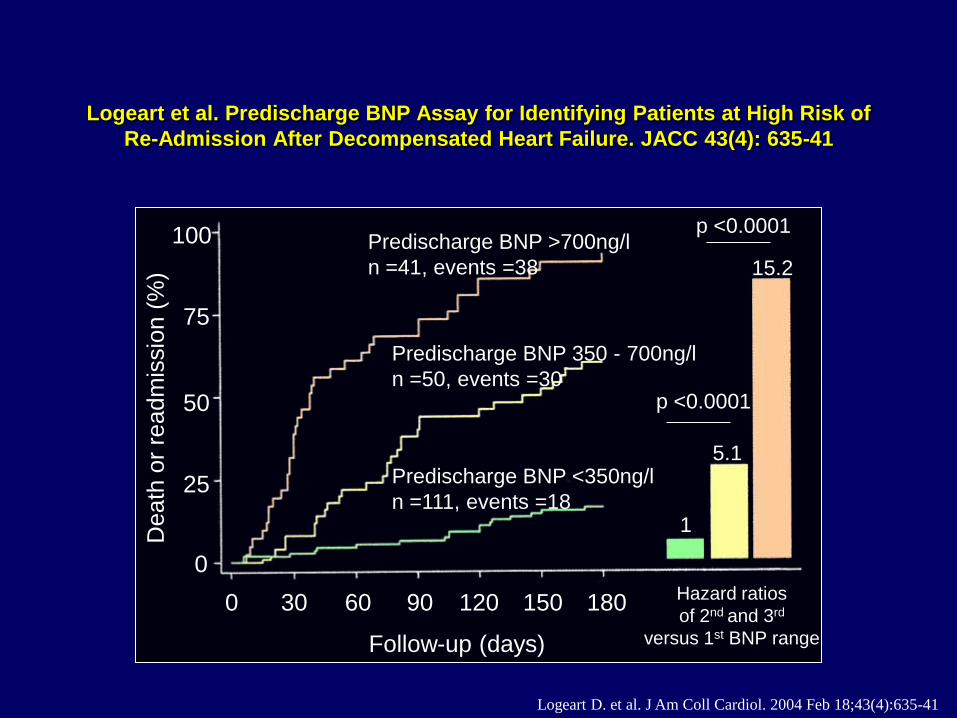
Logeart et al. Predischarge BNP Assay for Identifying Patients at High Risk of
Re-Admission After Decompensated Heart Failure. JACC 43(4): 635-41
Logeart D. et al. J Am Coll Cardiol. 2004 Feb 18;43(4):635-41
Follow-up (days)
Hazard ratios
of 2nd and 3rd
versus 1st BNP range
Death
or
readm
issio
n (
%)
100
75
50
25
0
0 30 60 90 120 150 180
Predischarge BNP >700ng/l
n =41, events =38
Predischarge BNP 350 - 700ng/l
n =50, events =30
Predischarge BNP <350ng/l
n =111, events =18
p <0.0001
p <0.0001
15.2
5.1
1

Bringing BNP Into the Clinic —or Bringing the Clinic to BNP
Needs to be interpreted in context
• Does not take the place of history, physical exam
• To interpret value must have understanding of BNP and heart failure syndrome
• Must have previous BNP values to which to refer

BN
P (
pg/m
l)
262248
1180
1050
275
0
200
400
600
800
1000
1200
1400
A B C D E
A. Decompensated CHF (IV)
B. After treatment (II)
C. Clinic - 2 months later (II)
D. Stopped Meds - 3 months later (IV)
E. After treatment (II)
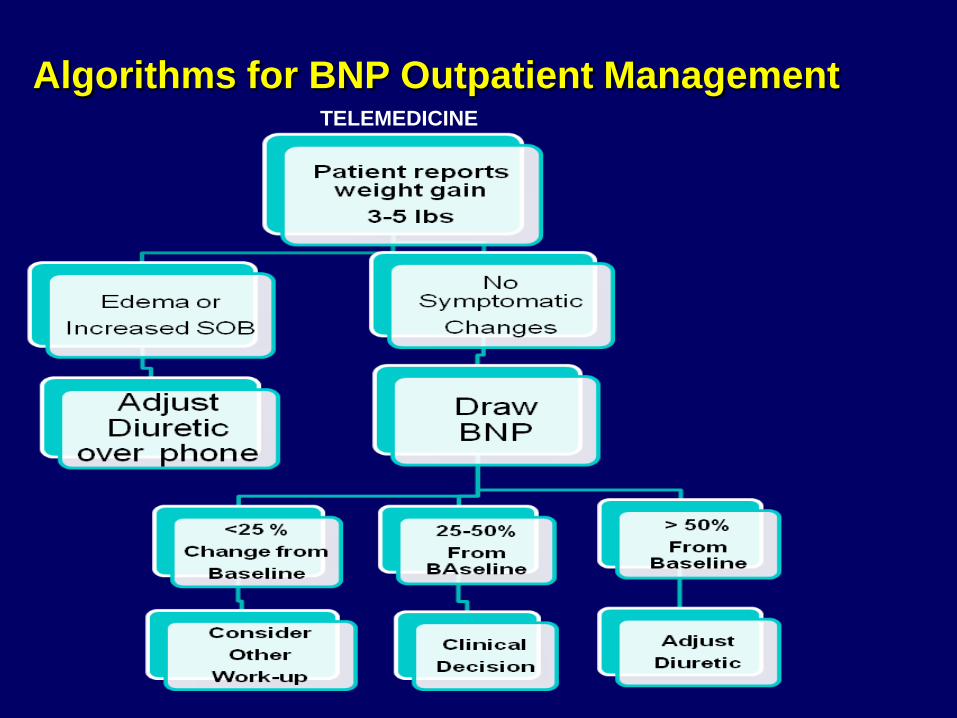
Algorithms for BNP Outpatient ManagementTELEMEDICINE

Algorithms for BNP Outpatient ManagementOUTPATIENT CLINC

The Holy Grail
• Can BNP levels be
used to titrate
outpatient therapy?

Targets in Treatment
• In many conditions treatment
can be titrated against a
target :
Hypertension Blood Pressure
Diabetes glucose, HbA1c
Lipids Cholesterol

Heart Failure Treatment Targets
There is currently
no target for treatment
of heart failure that is:
– Objective
– Reliable
– Practical
– Inexpensive


Neurohormones in Heart Failure
• Neurohumoral activation
– Marker of severity and prognosis in CHF
• BNP levels
– Reflect LV wall stress/ filling pressure
– Correlate with LV ejection fraction
– Indicate prognosis in CHF and after MI
– Fall with effective ACEI / diuretic therapy

Benefit of BNP plasma levels for optimising
therapy in patients with systolic heart failure :
The Systolic hearT fAilure tReatment Supported
by BNP trial (STARS-BNP) multicenter
randomised study.
For STARS-BNP Investigators on behalf of the working group on Heart failure of the
French Society of Cardiology
STARS
BNP


BNP group Clinical group p
all causes hospitalizations N: 52 60 NS
Hospitalizations related to HF N 22 48 P<0,001
Death all causes N: 7 11 NS
Death related to HF N: 3 9 P<0,05
HF related death and hospitalizations N: 25 57 P<0,001
End Points
STARS
BNP

Patient
Doctor
Our patients
really love
the BNP test!

And
they
live
longer!
People
feel
better
when
their
BNP
levels
are
lower

Patient
compliance
often improves
when patients
also have an
objective way
to monitor their
condition

BNP on Every Street Corner?


Some
would
like
Nothing
better
than
To burst
the
bubble

BNP and Guidelines
• As with every new diagnostic
or treatment modality,
guidelines often lag behind
state-of-the-art practice
• It is very encouraging to see
that after only several years
of introduction into clinical
practice, the use of BNP
is already recommended
by all major guidelines
Suspected Acute Heart
Failure
Assess Symptoms and
SignsHeart Disease?
ECG / BNP/ X-
ray?
Nor
mal
Evaluate function
byEchocardiography / other
imaging
Nor
mal
Abnorm
al
Abnorm
alHeart Failure, assess
by
Echocardiography Selected tests(angio, hemodynamic
monitoring, PAC)Characterize type and
severity
Consider other diagnosis
European Heart J. 2005;26:385-6.NEED MORE
COMPLETE CITATION

Diagnostic Tests Alone Will Not
Accomplish Our Goals…

Being an MD at a distanceAirport get phone calls
foot ball game
Or just relaxing
What’s his
BNP ?

We Need to Be Good Clinicians
at the Bedside First!

Modern
technology
is not always
available
to us

It takes longer
to use history,
physical exam
skills AND
technology…


Thank You!